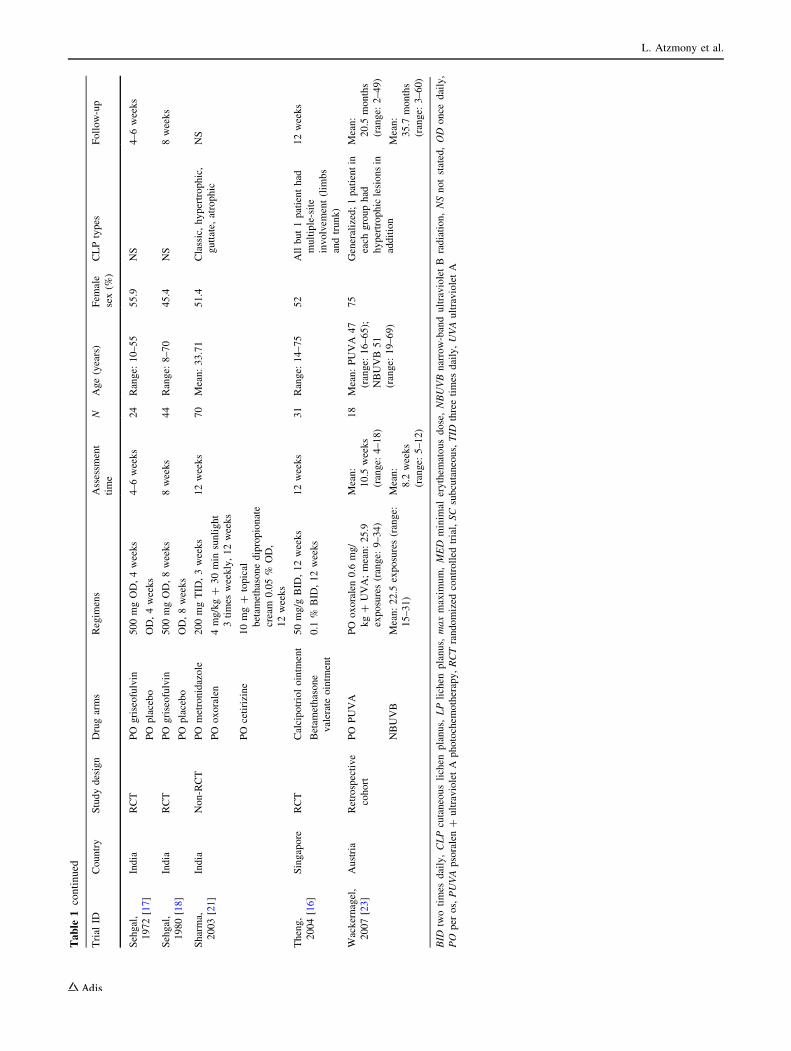
EVIDENCE-BASED REVIEW Treatments for Cutaneous Lichen Planus: A Systematic Review and Meta-Analysis Lihi Atzmony 1 • Ofer Reiter 1 • Emmilia Hodak 1,2 • Michael Gdalevich 3 • Daniel Mimouni 1,2 Ó Springer International Publishing Switzerland 2015 Abstract Background Cutaneous lichen planus (CLP) is an inflammatory dermatosis. Its chronic relapsing course and frequently spontaneous regression hamper the assessment of treatment effectiveness. Objective To evaluate the efficacy of available treatment modalities for CLP. Data Sources PubMed, Cochrane Central Register of Controlled Trials (CENTRAL), ClinicalTrials.gov registry. Methods We performed a systematic review of the cur- rent literature. All randomized controlled trials, nonran- domized case–control studies, and cohort studies with more than one treatment arm were included. The primary out- comes were complete response and time to complete response. The secondary outcomes were partial response, relapse, time to relapse, reduction of itch, the adverse event rate, and withdrawal due to adverse events. Data Synthesis Sixteen studies met the inclusion criteria, of which 11 were randomized controlled trials. Most trials had a small sample size. In the rare studies in which variants other than generalized or classic lichen planus were included, they could not be analyzed separately. Body-of-evidence quality ranged from very low to mod- erate. Acitretin, sulfasalazine, and griseofulvin were associated with increased overall response rates in com- parison with placebo. Narrow-band ultraviolet B radiation (NBUVB) was more effective than 6 weeks’ low-dose prednisolone in achieving a complete response, and prednisolone was more effective than enoxaparin. Hydroxychloroquine was more effective than griseofulvin in achieving an overall response. Betamethasone valerate 0.1 % ointment had comparable efficacy to calcipotriol ointment. Methotrexate was effective, with a nonsignifi- cant difference in the complete response rate in compar- ison with oral betamethasone. In nonrandomized controlled trials, oral psoralen plus ultraviolet A pho- tochemotherapy (PUVA) had comparable efficacy to a PUVA bath and NBUVB. Psoralen plus sunlight exposure (PUVASOL) and betamethasone dipropionate 0.05 % cream were effective relative to a short course of oral metronidazole. Conclusions Several effective treatment options are available for CLP. Further well-designed studies are war- ranted to investigate the efficacy of topical glucocorti- coids—the current first-line therapy—as well as other treatment modalities, and the treatment of different variants of CLP. L. Atzmony and O. Reiter contributed equally to this work. Electronic supplementary material The online version of this article (doi:10.1007/s40257-015-0160-6) contains supplementary material, which is available to authorized users. & Daniel Mimouni [email protected]1 Department of Dermatology, Rabin Medical Center, Beilinson Hospital, 39 Jabotinski Street, 49100 Petach Tikva, Israel 2 Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel 3 Faculty of Health Sciences, Ben-Gurion University of the Negev and South District Health Office, Ministry of Health, Beer Sheva, Israel Am J Clin Dermatol DOI 10.1007/s40257-015-0160-6
Transcript
EVIDENCE-BASED REVIEW
Treatments for Cutaneous Lichen Planus: A Systematic Reviewand Meta-Analysis
Lihi Atzmony1 • Ofer Reiter1 • Emmilia Hodak1,2 • Michael Gdalevich3 • Daniel Mimouni1,2
� Springer International Publishing Switzerland 2015
Abstract
Background Cutaneous lichen planus (CLP) is an
inflammatory dermatosis. Its chronic relapsing course and
frequently spontaneous regression hamper the assessment
of treatment effectiveness.
Objective To evaluate the efficacy of available treatment
Methods We performed a systematic review of the cur-
rent literature. All randomized controlled trials, nonran-
domized case–control studies, and cohort studies with more
than one treatment arm were included. The primary out-
comes were complete response and time to complete
response. The secondary outcomes were partial response,
relapse, time to relapse, reduction of itch, the adverse event
rate, and withdrawal due to adverse events.
Data Synthesis Sixteen studies met the inclusion criteria,
of which 11 were randomized controlled trials. Most trials
had a small sample size. In the rare studies in which
variants other than generalized or classic lichen planus
were included, they could not be analyzed separately.
Body-of-evidence quality ranged from very low to mod-
erate. Acitretin, sulfasalazine, and griseofulvin were
associated with increased overall response rates in com-
parison with placebo. Narrow-band ultraviolet B radiation
(NBUVB) was more effective than 6 weeks’ low-dose
prednisolone in achieving a complete response, and
prednisolone was more effective than enoxaparin.
Hydroxychloroquine was more effective than griseofulvin
in achieving an overall response. Betamethasone valerate
0.1 % ointment had comparable efficacy to calcipotriol
ointment. Methotrexate was effective, with a nonsignifi-
cant difference in the complete response rate in compar-
ison with oral betamethasone. In nonrandomized
controlled trials, oral psoralen plus ultraviolet A pho-
tochemotherapy (PUVA) had comparable efficacy to a
PUVA bath and NBUVB. Psoralen plus sunlight exposure
(PUVASOL) and betamethasone dipropionate 0.05 %
cream were effective relative to a short course of oral
metronidazole.
Conclusions Several effective treatment options are
available for CLP. Further well-designed studies are war-
ranted to investigate the efficacy of topical glucocorti-
coids—the current first-line therapy—as well as other
treatment modalities, and the treatment of different variants
of CLP.
L. Atzmony and O. Reiter contributed equally to this work.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s40257-015-0160-6) contains supplementarymaterial, which is available to authorized users.
* A statistically significant difference was observed (P\ 0.05)a A detailed definition of ‘‘response’’ was not supplied in the original articleb Overall response = clinical improvement defined as a range of responses from a mild decrease in symptoms and in lesion size and number to
complete disappearance of symptoms and lesions; clinical improvement was significantly greater with PUVASOL or betamethasone than with
metronidazolec Overall response = lesion flatteningd The risk of bias was assessed using the Downs and Black checklist [6]; the total achievable maximum score was 27e ITT/modified-ITT
Treatments for Cutaneous Lichen Planus
1/14, RR 4 [95 % CI 0.51–31.46]), although improvement,
graded by a linear analog severity scale, was significantly
greater in the prednisolone group (the median score at entry
minus the score at 6 weeks: 2.5 versus 0.85, P\ 0.05).
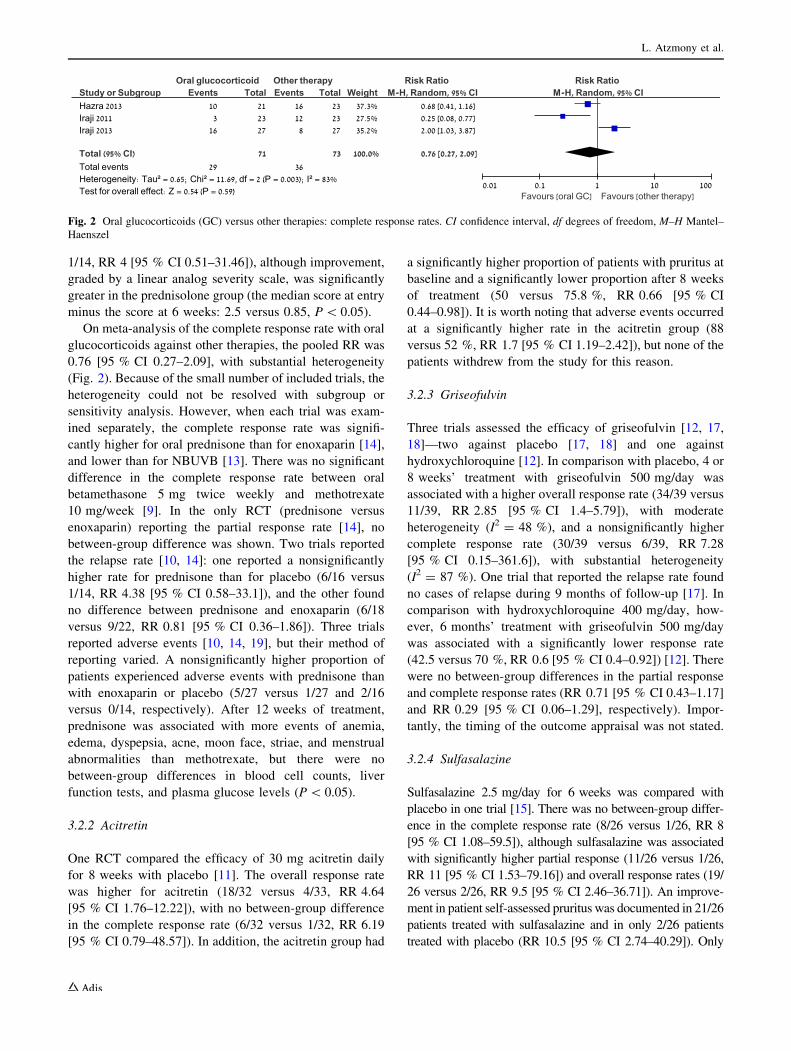
On meta-analysis of the complete response rate with oral
glucocorticoids against other therapies, the pooled RR was
0.76 [95 % CI 0.27–2.09], with substantial heterogeneity
(Fig. 2). Because of the small number of included trials, the
heterogeneity could not be resolved with subgroup or
sensitivity analysis. However, when each trial was exam-
ined separately, the complete response rate was signifi-
cantly higher for oral prednisone than for enoxaparin [14],
and lower than for NBUVB [13]. There was no significant
difference in the complete response rate between oral
betamethasone 5 mg twice weekly and methotrexate
10 mg/week [9]. In the only RCT (prednisone versus
enoxaparin) reporting the partial response rate [14], no
between-group difference was shown. Two trials reported
the relapse rate [10, 14]: one reported a nonsignificantly
higher rate for prednisone than for placebo (6/16 versus
1/14, RR 4.38 [95 % CI 0.58–33.1]), and the other found
no difference between prednisone and enoxaparin (6/18
versus 9/22, RR 0.81 [95 % CI 0.36–1.86]). Three trials
reported adverse events [10, 14, 19], but their method of
reporting varied. A nonsignificantly higher proportion of
patients experienced adverse events with prednisone than
with enoxaparin or placebo (5/27 versus 1/27 and 2/16
versus 0/14, respectively). After 12 weeks of treatment,
prednisone was associated with more events of anemia,
edema, dyspepsia, acne, moon face, striae, and menstrual
abnormalities than methotrexate, but there were no
between-group differences in blood cell counts, liver
function tests, and plasma glucose levels (P\ 0.05).
3.2.2 Acitretin
One RCT compared the efficacy of 30 mg acitretin daily
for 8 weeks with placebo [11]. The overall response rate
was higher for acitretin (18/32 versus 4/33, RR 4.64
[95 % CI 1.76–12.22]), with no between-group difference
in the complete response rate (6/32 versus 1/32, RR 6.19
[95 % CI 0.79–48.57]). In addition, the acitretin group had
a significantly higher proportion of patients with pruritus at
baseline and a significantly lower proportion after 8 weeks
of treatment (50 versus 75.8 %, RR 0.66 [95 % CI
0.44–0.98]). It is worth noting that adverse events occurred
at a significantly higher rate in the acitretin group (88
versus 52 %, RR 1.7 [95 % CI 1.19–2.42]), but none of the
patients withdrew from the study for this reason.
3.2.3 Griseofulvin
Three trials assessed the efficacy of griseofulvin [12, 17,
18]—two against placebo [17, 18] and one against
hydroxychloroquine [12]. In comparison with placebo, 4 or
8 weeks’ treatment with griseofulvin 500 mg/day was
associated with a higher overall response rate (34/39 versus
11/39, RR 2.85 [95 % CI 1.4–5.79]), with moderate
heterogeneity (I2 = 48 %), and a nonsignificantly higher
complete response rate (30/39 versus 6/39, RR 7.28
[95 % CI 0.15–361.6]), with substantial heterogeneity
(I2 = 87 %). One trial that reported the relapse rate found
no cases of relapse during 9 months of follow-up [17]. In
comparison with hydroxychloroquine 400 mg/day, how-
ever, 6 months’ treatment with griseofulvin 500 mg/day
was associated with a significantly lower response rate
(42.5 versus 70 %, RR 0.6 [95 % CI 0.4–0.92]) [12]. There
were no between-group differences in the partial response
and complete response rates (RR 0.71 [95 % CI 0.43–1.17]
and RR 0.29 [95 % CI 0.06–1.29], respectively). Impor-
tantly, the timing of the outcome appraisal was not stated.
3.2.4 Sulfasalazine
Sulfasalazine 2.5 mg/day for 6 weeks was compared with
placebo in one trial [15]. There was no between-group differ-
ence in the complete response rate (8/26 versus 1/26, RR 8
[95 % CI 1.08–59.5]), although sulfasalazine was associated
with significantly higher partial response (11/26 versus 1/26,
RR 11 [95 % CI 1.53–79.16]) and overall response rates (19/
26 versus 2/26, RR 9.5 [95 % CI 2.46–36.71]). An improve-
ment in patient self-assessed pruritus was documented in 21/26
patients treated with sulfasalazine and in only 2/26 patients
treated with placebo (RR 10.5 [95 % CI 2.74–40.29]). Only
Fig. 2 Oral glucocorticoids (GC) versus other therapies: complete response rates. CI confidence interval, df degrees of freedom, M–H Mantel–
Haenszel
L. Atzmony et al.
patients treated with sulfasalazine experienced adverse events
(8/26 versus 0/26, RR 17 [95 % CI 1.03–280.07]). Neverthe-
less, although the sulfasalazine group had a higher rate of
withdrawal due to adverse events, the difference in comparison
with the placebo group was not significant (3/26 versus 0/26,
RR 7 [95 % CI 0.38–280.07]).
3.2.5 Enoxaparin
One trial assessed the efficacy of subcutaneous enoxaparin
5 mg/week against oral prednisone 0.5 mg/kg/day for up to
8 weeks [14]. The complete response rate was significantly
lower for enoxaparin (8/27 versus 16/27, RR 0.95
[95 % CI 0.26–0.97]). Accordingly, the enoxaparin group
had a lesser reduction in itch (rated by a visual analog
scale) after treatment (2.84 versus 0.83, P = 0.005).
However, there were no significant between-group differ-
ences in the partial and overall response rates (10/27 versus
6/27, RR 1.67 [95 % CI 0.71–3.94] and 18/27 versus
22/27, RR 0.5 [95 % CI 0.13–1.91], respectively) or the
relapse rates (6/18 versus 9/22, RR 0.81 [95 % CI
0.36–1.86]). The number of patients with adverse events
was nonsignificantly lower in the enoxaparin group (1/27
versus 5/27, RR 0.2 [95 % CI 0.02–1.6]).
3.2.6 Methotrexate
One trial tested the efficacy and safety of oral methotrexate
10 mg/week against oral betamethasone for 12 weeks [9,
19]. As mentioned above, there was no between-group
difference in the complete response rate. The rates of some
adverse events were higher with betamethasone.
3.2.7 Metronidazole
A lower proportion of patients achieved overall ‘‘clinical
improvement’’ after 3 weeks of treatment with metron-
idazole than with PUVASOL and topical glucocorticoids
[21]. However, the planned intervention was not compa-
rable in terms of treatment duration. These results are
discussed in the section on phototherapy.
3.2.8 Hydroxychloroquine
A comparison of hydrochloroquine 400 mg/day with
griseofulvin 500 mg/day for 6 months yielded overall
response rates of 70 and 42.5 %, respectively [12]. These
results are discussed in the section on griseofulvin.
3.2.9 Dapsone
A nonrandomized case–control study comparing dapsone
150 mg/day with topical betamethasone 0.1 % reported a
nonsignificant between-group difference in the ‘‘good
response’’ rate after 3 months’ treatment (29/59 versus
10/25, RR 1.28 [95 % CI 0.75–2.12]) [22]. The authors
did not mention the type of betamethasone used. Of note,
most of the patients had classic lichen planus, but the
cohort also included patients with lichen actinicus, linear
lichen planus, lichen planus pigmentosus, and mucosal
lichen planus. Their responses were not analyzed sepa-
rately, so the possible effect of the different variants on
treatment in terms of direction and size could not be
determined.
3.3 Topical Therapy
Although topical glucocorticoids are used as a first-line
therapy in CLP, their efficacy has not been tested in a well-
designed RCT. Only three of the trials that were eligible for
the present review included topical glucocorticoids as a
treatment arm [16, 21, 22]. One assessed the efficacy of
calcipotriol 0.05 % against betamethasone valerate 0.1 %
ointment and found no difference between the groups in
‘‘lesion flattening’’ after 12 weeks (7/15 versus 8/16, RR 0.93
[95 % CI 0.45–1.94]) [16]. It is worth noting that the rate of
adverse events (irritation and increased pruritus severity) was
higher for calcipotriol, but the difference in comparison with
betamethasone dipropionate did not reach statistical signifi-
cance (3/15 versus 0/16, RR 7.43 [95 % CI 0.42–132.96]).
The second study of topical glucocorticoids reported a high
‘‘clinical improvement’’ rate for betamethasone dipropionate
0.05 % cream in comparison with oral metronidazole [21] at
12 weeks. However, this trial was subject to a high risk of
bias (see the sections on phototherapy and metronidazole).
The third study compared dapsone with topical betametha-
sone and showed a comparable ‘‘good response’’ (see section
on dapsone) [22].
One group examined the efficacy of KH 1060 ointment
(lexacalcitol)—a vitamin D3 analog—which had been
found to be approximately as effective as calcipotriol
ointment in the treatment of psoriasis [24], in comparison
with placebo [8]. After 8 weeks of treatment, there was no
between-group difference in the partial response rate (14/
49 versus 15/43, RR 0.95 [95 % CI 0.72–1.26]).
3.4 Strength of Body of Evidence
Table 3 details the results of the body-of-evidence analysis.
4 Discussion
In this systematic review, we aimed to evaluate the efficacy
of different treatment modalities for CLP. In contrast to
previous reviews, which included only small numbers of
Treatments for Cutaneous Lichen Planus
RCTs [2–4], our review included 16 trials, of which 11
were RCTs. The overall quality of evidence was very low
to moderate in terms of treatment efficacy. Acitretin, sul-
fasalazine, and griseofulvin were associated with higher
overall response rates than placebo. Acitretin and sul-
fasalazine caused significantly more adverse events than
placebo, but griseofulvin did not. NBUVB was more
effective than prednisolone in achieving a complete
Table 3 Quality of evidence for reviewed treatments
Intervention No. of
trials
Quality of
evidence
Effects
Oral prednisone 3 Moderate 10-day course did not significantly increase response and relapse rates versus placebo;
small sample size [10]
Medium dose for 8 weeks was more effective in achieving CR than enoxaparin [14]
Low dose for 6 weeks was less effective in achieving CR than NBUVB [13]
Topical GC 1 Moderate Flattening of lesions with betamethasone valerate 0.1 % ointment comparable to
calcipotriol ointment at 12 weeks (50 %); low PR rate; lichen planus type not
mentioned [16]
1 Low High and comparable ‘‘clinical improvement’’ rates with PUVASOL or betamethasone
dipropionate cream ? oral cetirizine for 12 weeks; permissive definition of
‘‘response’’ [21]
1 Very low Comparable ‘‘clinical improvement’’ rates with betamethasone 0.1 % (type not
mentioned) and dapsone [22]
Acitretin 30 mg/day for
8 weeks
1 Moderate More effective than placebo in achieving OR and reducing pruritus [11]
PO griseofulvin 500 mg/day
for 8 weeks
3 Moderate High response rate; more effective than placebo in achieving OR (not CR) [17, 18]
No relapses during 9 months’ follow-up [17]
In one low-quality RCT, response rate significantly lower than with hydroxychloroquine
[12]
Metronidazole 200 mg TID
for 3 weeks
1 Low Lower proportion of patients achieved overall ‘‘clinical improvement’’ after 3 weeks of
treatment with metronidazole than with PUVASOL or betamethasone dipropionate
0.1 % cream ? oral cetirizine [21]; short treatment duration compared with other
treatment arms
Sulfasalazine 2.5 mg/day for
6 weeks
1 Moderate More effective than placebo in achieving OR (not CR) and reducing pruritus [15]
Hydroxychloroquine
400 mg/day for 6 months
1 Low More effective than griseofulvin in achieving OR (not CR) [12]
SC enoxaparin 5 mg/week
for 8 weeks
1 Moderate Less effective than medium-dose prednisolone in achieving CR; comparable OR [14]
Dapsone 150 mg/day for
3 months
1 Very low ‘‘Clinical improvement’’ rates comparable to betamethasone 0.1 % (type not mentioned)
[22]
Methotrexate 10 mg/week
for 12 weeks
1 Low Nonsignificant difference in response rates and better safety profile compared with oral
betamethasone; quality downgraded to low because of inconclusiveness of results and
small sample size [9]
NBUVB 1 Moderate More effective than low-dose prednisone for 6 weeks in achieving CR [13]
1 Low OR rates comparable to PUVA; small sample size [23]
Topical PUVA 1 Low OR rate nonsignificantly higher with PUVA bath than with oral PUVA; small sample
size [20]
Oral PUVA 2 Low Effectiveness comparable to NBUVB; see above [23]
PUVASOL for 12 weeks 1 Low High and comparable ‘‘clinical improvement’’ rates with PUVASOL or betamethasone
dipropionate cream ? oral cetirizine for 12 weeks [21]
Topical vitamin D
derivatives
2 Moderate Comparable efficacy of calcipotriol 0.05 % and betamethasone valerate 0.1 % ointment
for 12 weeks [16]
Similar efficacy of KH 1060 and placebo for 8 weeks [8]
Quality assessment refers to OR/PR/CR/other reported response outcomes
CR complete response, GC glucocorticoid, NBUVB narrow-band ultraviolet B radiation, OR overall response, PO per os, PR partial response,