University of Zurich Zurich Open Repository and Archive Winterthurerstr. 190 CH-8057 Zurich http://www.zora.uzh.ch Year: 2008 Temporary transarticular stabilization with a locking plate for medial shoulder luxation in a dog Post, C; Guerrero, T; Voss, K; Montavon, P M Post, C; Guerrero, T; Voss, K; Montavon, P M (2008). Temporary transarticular stabilization with a locking plate for medial shoulder luxation in a dog. Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T), 21(2):166-170. Postprint available at: http://www.zora.uzh.ch Posted at the Zurich Open Repository and Archive, University of Zurich. http://www.zora.uzh.ch Originally published at: Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T) 2008, 21(2):166-170.
Transcript
University of ZurichZurich Open Repository and Archive
Winterthurerstr. 190
CH-8057 Zurich
http://www.zora.uzh.ch
Year: 2008
Temporary transarticular stabilization with a locking plate formedial shoulder luxation in a dog
Post, C; Guerrero, T; Voss, K; Montavon, P M
Post, C; Guerrero, T; Voss, K; Montavon, P M (2008). Temporary transarticular stabilization with a locking platefor medial shoulder luxation in a dog. Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T),21(2):166-170.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T) 2008, 21(2):166-170.
Post, C; Guerrero, T; Voss, K; Montavon, P M (2008). Temporary transarticular stabilization with a locking platefor medial shoulder luxation in a dog. Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T),21(2):166-170.Postprint available at:http://www.zora.uzh.ch
Posted at the Zurich Open Repository and Archive, University of Zurich.http://www.zora.uzh.ch
Originally published at:Veterinary and Comparative Orthopaedics and Traumatology (V.C.O.T) 2008, 21(2):166-170.
Temporary transarticular stabilization with a locking plate formedial shoulder luxation in a dog
Abstract
This report describes the temporary fixation of a traumatic shoulder luxation in a large-breed dog usinga 3.5-mm Locking Round-Hole Reconstruction Plate (LRHRP) to provide stable internal splinting,allowing healing of the injured ligaments, joint capsule, glenohumeral ligaments, tendons, and musclesfor restoration of joint stability. The use of a temporary plate with a locking system should beconsidered as an option in the treatment of canine shoulder joint luxations with severe tissue damage.
Received July 3, 2007 Vet Comp Orthop Traumatol 2/2008 Accepted August 3, 2007
Temporary transarticular stabilization with a locking plate for medial shoulder luxation in a dog C. Post, T. Guerrero, K. Voss, P. M. Montavon Vetsuisse Faculty, University of Zurich, Clinic for Small Animal Surgery, Zurich, Switzerland
Summary This report describes the temporary fixation of a trau-matic shoulder luxation in a large-breed dog using a 3.5-mm Locking Round-Hole Reconstruction Plate (LRHRP) to provide stable internal splinting, allowing healing of the injured ligaments, joint capsule, gleno-humeral ligaments, tendons, and muscles for restora-tion of joint stability. The use of a temporary plate with a locking system should be considered as an option in the treatment of canine shoulder joint luxations with severe tissue damage.
Prepublished online November 13, 2007 doi:10.3415/VCOT-07-07-0066
Introduction
The stability of the glenohumeral joint is imparted by both static and dynamic mech-anisms. Static stabilisers are the medial and lateral glenohumeral ligaments, and the joint capsule. Dynamic stabilisers consist of five periarticular (cuff) muscles that span the joint. They include the infraspintus, su-praspinatus, subscapularis, and teres minor muscles, and to a lesser extent, the biceps brachii muscle. Injury to the static or dy-namic stabilisers may cause joint laxity, subluxation or, in severe cases, luxation of the joint (1, 2).
Trauma is the most common cause of medial shoulder luxation in large-breed dogs (3). Closed reduction and temporary immobilization with a Spica splint is mostly performed in acute cases in the absence of articular fractures. Open reduction and sur-gical stabilisation is indicated if closed re-duction under anaesthesia fails or if relu-xation occurs (3). Several surgical methods have been described, including transposi-tion of the bicipital or supraspinatus tendon, suture stabilisation, and prosthetic ligament repair (3–6). Postoperative external immo-bilization is advised after all of these pro-cedures. Tendon transposition can be effec-tive in stabilising the joint, but altered joint mechanics may lead to articular incongruity and degenerative joint disease (DJD) (4, 6, 7). Arthrodesis has also been described as a salvage procedure for intractable gleno-humeral joint instability, and chronic lux-ations (8).
The purpose of this clinical communi-cation is to report the successful manage-ment of a traumatic medial glenohumeral luxation in a large dog with contralateral elbow luxation, using a Locking Round-
Hole Reconstruction Platea (LRHRP) for temporary transarticular immobilization.
Case presentation Preoperative findings and treatment
A 32 kg, 11-year-old, male, Golden Retriev-er was referred to our clinic four hours after a road traffic accident with suspected left shoulder and right elbow injuries. The dog was admitted in ventral recumbency, and was unable to walk. Clinical examination revealed a heart rate of 140 beats/min, a re-spiratory rate of 98 breaths/min, a capillary refill time of 2 sec, and a rectal temperature of 38.9°C. An intravenous catheter was placed, and infusion therapy was initiated (lactated Ringer’s Solutionb 40 ml/kg and HAES-Sterilb 10% 10 ml/kg). Analgesia was provided with buprenorphinec (0.014 mg/kg IV). Results of routine haematologi-cal and serum biochemical analyses were within reference intervals. Lateromedial and ventrodorsal survey radiographs of the chest and abdomen revealed three broken ribs and mild evidence of lung contusions.
Both of the forelimbs were held in outer rotation. The left shoulder and the right elbow were swollen, and appeared to be painful during manipulation. Luxation of the left shoulder and the right elbow was suspected from clinical findings. A neuro-logical examination was considered unre-markable. Mediolateral and craniocaudal radiographs of both forelimbs were taken under general anaesthesia (induction with
a Synthes Gmbh & Co KG, Umkirch, Germany. b Fresenius Kabi AG, Stans, Switzerland. c Temgesic®, Essex Chemie AG, Luzern, Switzer-
midazolamd 0.1 mg/kg and fentanyle 5 mg/kg, maintenance with inhaled isofluranef in oxygen), revealing lateral luxation of the right elbow, medial luxation of the left shoulder and a minimally displaced fracture of the left acromion (Fig. 1). The right elbow joint was reduced in a closed manner using a Lewin bone clamp (9), and the joint was considered stable enough for conservative treatment. However, the left shoulder relu-xated readily following closed reduction. Open reduction and internal fixation of the left shoulder was therefore indicated.
Surgical treatment
The dog was placed in right lateral recum-bency, and a hanging-leg orthopaedic prep-aration was performed with a craniolateral approach to the left shoulder (10). The in-fraspinatus muscle was found to be torn at the musculotendinous junction. The lateral glenohumeral ligament and the caudolateral portion of the joint capsule were disrupted, and the shoulder joint seemed highly un-stable. Additional incisions and retractions of the brachiocephalicus and superficial and deep pectoralis muscles were performed in order to access the medial aspect of the shoulder joint. The articular capsule on the medial aspect and the medial glenohumeral ligament were also found to be completely ruptured, the subscapular muscle was intact. The joint was reduced and the capsule was closed on the medial and caudolateral as-pect, using simple interrupted sutures (poly-dioxaneg, 0 metric), which were all placed prior to tying. A 3.5-mm LRHRP (Synthes Companya) with 13 holes was contoured to an angle of 110° and slightly twisted. A part of the supraspinatus muscle was bluntly elevated at its origin from the distocranial scapular spine and the distal supraspinous fossa. The deltoid muscle was reflected caudally and the plate was placed under the partially elevated supraspinatus muscle along the base of the spine of the scapula, and the craniolateral side of the humerus.
The suprascapular nerve was identified and protected. The LRHRP was then fixed in the cranial angle between the spine and the body of the scapula with four 3.5 mm self-taping locking screws (screw length from proximal to distal: 8, 12, 16, and 26 mm) di-rected caudomedially through the junction of the spine and body. The plate was an-chored to the humerus with four 3.5 mm selftaping locking screws (length from proximal to distal: 30, 22, 12 and 10 mm) (Fig. 2). The locking mechanism between screw heads and plate allowed maintaining a distance between plate and shoulder joint (Fig. 2). Because the acromion fracture was only minimally displaced and shoulder movement was restricted due to internal fix-ation, no surgical treatment of the acromion fracture was deemed necessary. The infra-spinatus muscle was reconstructed with two locking loop tension sutures (polydioxaneg, 3.5 metric). The fascia and subcutis were closed in a simple interrupted pattern (poly-dioxaneg, 3 metric and 2 metric), respect-ively. The skin was closed in a simple inter-
Fig. 1 A) Radiographs of the left shoulder showing superimposition of the scapular neck and humerus in the mediolateral view and, B) mediodorsal displacement of the humerus in the caudocranial view, as well as an avulsion fracture (arrow) of the acromion.
A) B)
Fig. 2 The 3.5 mm LRH reconstruction plate fixed to the scapula and humerus with four self-taping locking screws in each bone.
d Dormicum®, Roche Pharma AG, Reinach, Swit-zerland.
e Sintenyl®, Sintetica SA, Mendrisio, Switzerland. f Isoflo®, Abbot AG, Baar, Switzerland. g PDS®, Ethicon, Provet AG, Lyssach, Switzerland.
Vet Comp Orthop Traumatol 2/2008
167
Temporary fixation of a medial shoulder luxation
rupted pattern (polyamide pseudomonofila-menth, 1.5 metric). A Spica splint was ap-plied to the right forelimb to stabilize the re-duced elbow but external coaptation was not applied for the left shoulder.
Postoperative findings and treatment
Postoperative radiographs (Fig. 3) showed that the left shoulder was reduced and fixed at an angle of 113° with a distended and slightly incongruent joint space. The right elbow was anatomically reduced. Postoper-ative analgesia was provided with a fentanyl skin patchi (100 µg/kg) and morphinej (0.2 mg/kg every four hours for 24 hours). Cefa-zolink (22 mg/kg) was given perioperatively and continued for the next six days because
of concomitant lung contusions and skin wounds. The dog was able to walk with as-sistance the next day. Unassisted walking with the Spica splint on the right forelimb was possible one week after surgery.
Gentle physiotherapy with passive cran-ial movements of the fixed left shoulder, and extension and flexion of the left elbow joint, applied daily with increasing intensity, was performed one day after surgery and con-tinued for a total of 12 weeks. The Spica splint on the right forelimb was changed one day after surgery, and then every third day until removal 14 days after surgery. The LRHRP across the left shoulder joint was surgically removed 25 days after implan-tation. This required a limited craniolateral approach to the scapular spine and the proximal aspect of the humerus. The joint appeared stable then during passive testing of craniocaudal drawer movements, abduc-tion and adduction.
The range of motion (ROM) of the af-fected and healthy shoulder and elbow joints were measured weekly with a goniometer (11) for a period of 12 weeks. The ROM of
the affected left shoulder was 34° one day after implant removal, 58° after two days, and 84° two weeks after implant removal (normal value 108° [11]). Twelve weeks after implant removal, ROM had decreased from 84° to 72°. The ROM in the contralat-eral shoulder was 90° two weeks after im-plant removal and 102° 12 weeks after im-plant removal. The ROM of the right elbow increased from 95° on the day after removal of the Spica splint to 120° 12 weeks later (normal value 129° [11]). Pronation and supination were within normal limits at the final examination.
Postoperative mediolateral and cranio-caudal radiographs of the right elbow and left shoulder were taken nine and 42 days after surgery, as well as immediately follow-ing implant removal (Fig. 4). These con-firmed maintenance of joint reduction in all of the images, and signs of callus formation without any displacement of the left acro-mion fracture 42 days after surgery. Radio-graphs of both shoulder joints in forced flexion and extension 26 and 42 days after the first surgery confirmed stable joint re-duction.
The clinical outcome was considered to be ‘good’. The dog showed a grade II out of V lameness ten weeks after surgery, and a grade I out of V lameness sixteen weeks after surgery. Force plate gait analysis was performed 10 weeks after surgery using the model OR6–7 from AMTIl. Five valid trials per limb were ob-tained at a velocity of 2 m/s (± 0.15), with an acceleration/deceleration < ± 0.3m/s2.
Peak vertical forces (PVFs) of the left forelimb were 94.74% body weight (BW), and those of the right forelimb were 90.75% BW. Vertical impulse of the left forelimb was 13.27% BW x sec, and VI of the right forelimb was 14.43% BW x sec. Stance time was shorter in the left forelimb (134.5 msec), compared to the right forelimb (and 149.83 msec), respectively. The dog loaded the forelimbs with 53%, and the hindlimbs with 47% of total force.
h Supramid®, Aesculap AG & Co., Tuttlingen, Ger-many.
i Durogesic®, Janssen-Cilag AG, Baar, Switzer-land.
j Morphin HCL®, Sintetica SA, Mendrisio, Swit-zerland.
k Kefzol®, Medika AG, Aesch, Switzerland.
Fig. 3 A) Mediolateral and B) caudocranial radiographs immediately after surgery showing the LRHRP applied to the cranial angle between the spine and body of the scapula and to the craniolateral side of the humerus. The reduction of the shoulder joint is suboptimal in a slightly incongruent position.
A) B)
l Model OR6–7, AMTI Advanced Medical Tech-nologies Inc., Watertown, MA, USA.
Vet Comp Orthop Traumatol 2/2008
168
Post et al.
Discussion
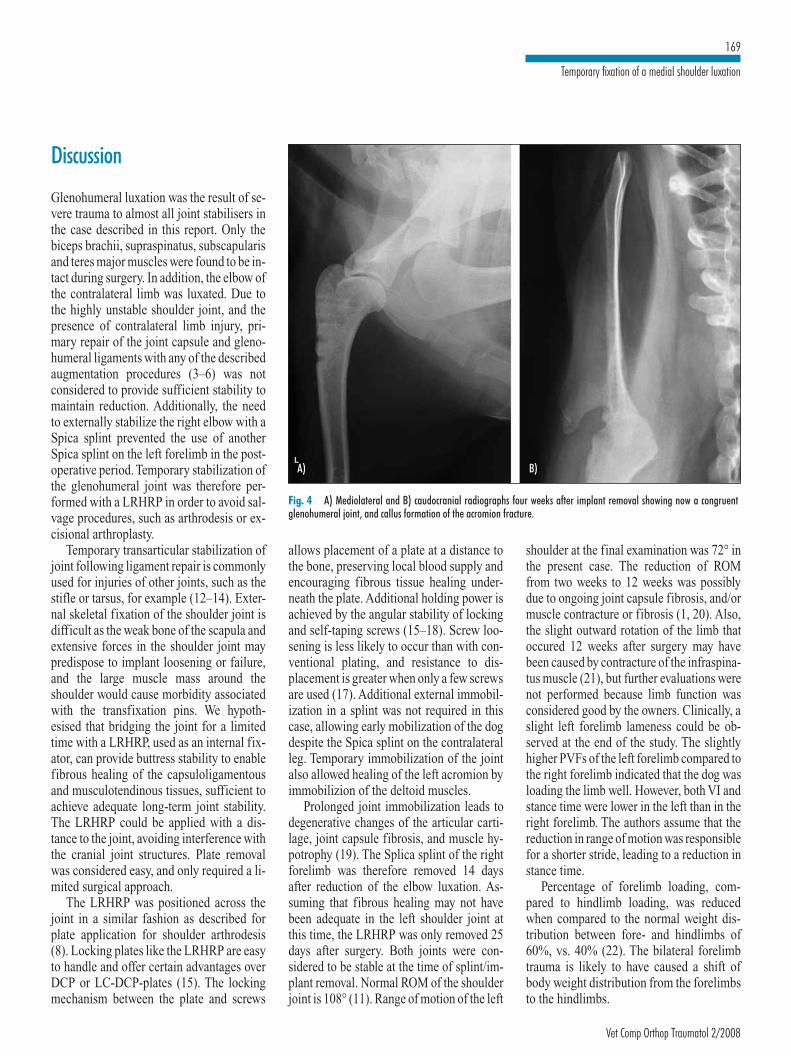
Glenohumeral luxation was the result of se-vere trauma to almost all joint stabilisers in the case described in this report. Only the biceps brachii, supraspinatus, subscapularis and teres major muscles were found to be in-tact during surgery. In addition, the elbow of the contralateral limb was luxated. Due to the highly unstable shoulder joint, and the presence of contralateral limb injury, pri-mary repair of the joint capsule and gleno-humeral ligaments with any of the described augmentation procedures (3–6) was not considered to provide sufficient stability to maintain reduction. Additionally, the need to externally stabilize the right elbow with a Spica splint prevented the use of another Spica splint on the left forelimb in the post-operative period. Temporary stabilization of the glenohumeral joint was therefore per-formed with a LRHRP in order to avoid sal-vage procedures, such as arthrodesis or ex-cisional arthroplasty.
Temporary transarticular stabilization of joint following ligament repair is commonly used for injuries of other joints, such as the stifle or tarsus, for example (12–14). Exter-nal skeletal fixation of the shoulder joint is difficult as the weak bone of the scapula and extensive forces in the shoulder joint may predispose to implant loosening or failure, and the large muscle mass around the shoulder would cause morbidity associated with the transfixation pins. We hypoth-esised that bridging the joint for a limited time with a LRHRP, used as an internal fix-ator, can provide buttress stability to enable fibrous healing of the capsuloligamentous and musculotendinous tissues, sufficient to achieve adequate long-term joint stability. The LRHRP could be applied with a dis-tance to the joint, avoiding interference with the cranial joint structures. Plate removal was considered easy, and only required a li-mited surgical approach.
The LRHRP was positioned across the joint in a similar fashion as described for plate application for shoulder arthrodesis (8). Locking plates like the LRHRP are easy to handle and offer certain advantages over DCP or LC-DCP-plates (15). The locking mechanism between the plate and screws
allows placement of a plate at a distance to the bone, preserving local blood supply and encouraging fibrous tissue healing under-neath the plate. Additional holding power is achieved by the angular stability of locking and self-taping screws (15–18). Screw loo-sening is less likely to occur than with con-ventional plating, and resistance to dis-placement is greater when only a few screws are used (17). Additional external immobil-ization in a splint was not required in this case, allowing early mobilization of the dog despite the Spica splint on the contralateral leg. Temporary immobilization of the joint also allowed healing of the left acromion by immobilizion of the deltoid muscles.
Prolonged joint immobilization leads to degenerative changes of the articular carti-lage, joint capsule fibrosis, and muscle hy-potrophy (19). The Splica splint of the right forelimb was therefore removed 14 days after reduction of the elbow luxation. As-suming that fibrous healing may not have been adequate in the left shoulder joint at this time, the LRHRP was only removed 25 days after surgery. Both joints were con-sidered to be stable at the time of splint/im-plant removal. Normal ROM of the shoulder joint is 108° (11). Range of motion of the left
shoulder at the final examination was 72° in the present case. The reduction of ROM from two weeks to 12 weeks was possibly due to ongoing joint capsule fibrosis, and/or muscle contracture or fibrosis (1, 20). Also, the slight outward rotation of the limb that occured 12 weeks after surgery may have been caused by contracture of the infraspina-tus muscle (21), but further evaluations were not performed because limb function was considered good by the owners. Clinically, a slight left forelimb lameness could be ob-served at the end of the study. The slightly higher PVFs of the left forelimb compared to the right forelimb indicated that the dog was loading the limb well. However, both VI and stance time were lower in the left than in the right forelimb. The authors assume that the reduction in range of motion was responsible for a shorter stride, leading to a reduction in stance time.
Percentage of forelimb loading, com-pared to hindlimb loading, was reduced when compared to the normal weight dis-tribution between fore- and hindlimbs of 60%, vs. 40% (22). The bilateral forelimb trauma is likely to have caused a shift of body weight distribution from the forelimbs to the hindlimbs.
Fig. 4 A) Mediolateral and B) caudocranial radiographs four weeks after implant removal showing now a congruent glenohumeral joint, and callus formation of the acromion fracture.
A) B)
Vet Comp Orthop Traumatol 2/2008
169
Temporary fixation of a medial shoulder luxation
In conclusion, temporary internal fix-ation of a medial luxated glenohumeral joint in this polytraumatized dog with a locking plate yielded satisfactory functional results, and allowed the avoidance of salvage pro-cedures. The use of temporary locking plates may therefore be an alternative method for transarticular stabilization of joints. Further investigations are warranted to establish the optimal duration and effect on joint motion of temporary locking plate fixation for canine shoulder luxations.
xation in the dog. Vet Comp Orthop Traumatol 2001; 14: 196–200.
6. Vasseur PB. Clinical results of surgical correction of shoulder luxation in dogs. J Am Vet Med Assoc 1983; 182: 503–505.
7. Vasseur PB, Pool RR, Klein K. Effects of tendon transfer on the canine scapulohumeral joint. Am J Vet Res 1983; 44: 811–815.
8. Johnson A. Arthrodesis of the shoulder. In: Johnson A, Houlton J, Vannini R, editors. AO Prin-ciples of Fracture Management in the Dog and Cat. Stuttgart: Thieme Verlag 2005; pp. 434–440.
9. Savoldelli D, Montavon PM, Suter PF. Traumatic elbow joint luxation in the dog and cat: perioper-ative findings. Schweiz Arch Tierheilkd 1996; 138: 387–391.
10. Piermattei D, Johnson K. An atlas of surgical ap-proaches to the bones and joints of the dog and cat. 4th ed. Philadelphia: Saunders; 2004.
11. Jaegger G, Marcellin-Little DJ, Levine D. Relia-bility of goniometry in Labrador Retrievers. Am J Vet Res 2002; 63: 979–986.
12. Keller M, Voss K, Montavon PM. The ComPad UniLock 2.0/2.4 system and its clinical appli-cation in small animal orthopedic. Vet Comp Or-thop Traumatol 2005; 18: 83–93.
13. Montavon P, Pohler Ortrun E et al. The mini in-strument and implant set and its clinical appli-cation. Vet Comp Orthop Traumatol 1988; 1: 44–51.
14. Voss K, Keller M, Montavon PM. Internal splint-ing of dorsal intertarsal and tarsometatarsal insta-bilities in dogs and cats with the ComPact Unilock 2.0/2.4 (TM) system. Vet Comp Orthop Traumatol 2004; 17: 125–130.
15. Aguila AZ, Manos JM, Orlansky AS et al. In vitro biomechanical comparison of limited contat dy-namic compression plate and locking compres-
sion plate. Vet Comp Orthop Traumatol 2005; 18: 220–226.
16. Gautier E, Sommer C. Guidelines for the clinical application of the LCP. Injury 2003; 34(Suppl 2): B63–76.
17. Sikes JW, Jr., Smith BR, Mukherjee DP et al. Comparison of fixation strengths of locking head and conventional screws, in fracture and recon-struction models. J Oral Maxillofac Surg 1998; 56: 468–473.
18. Wagner M. General principles for the clinical use of the LCP. Injury 2003; 34(Suppl 2): B31–42.
19. Salter RB, Simmonds DF, Malcolm BW et al. The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage. An experimental investigation in the rabbit. J Bone Joint Surg Am 1980; 62: 1232–1251.
20. Montgomery R, Fitch R. Muscle and tendon dis-orders. In: Slatter D, editor. Textbook of small ani-mal surgery. third ed. Philadelphia: Saunders; 2003 pp. 2264–2271.
21. Devor M, Sorby R. Fibrotic contracture of the ca-nine infraspinatus muscle: pathophysiology and prevention by early surgical intervention. Vet Comp Orthop Traumatol 2006; 19: 117–121.
22. Budsberg SC, Verstraete MC, Soutas-Little RW. Force plate analysis of the walking gait in healthy dogs. Am J Vet Res 1987; 48: 915–918.
References 1. Gray MJ, Lambrechts NE, Maritz NG et al. A bio-
mechanical investigation of the static stabilisers of the glenohumeral joint in the dog. Vet Comp Or-thop Traumatol 2005; 18: 55–61.
2. Sidaway BK, McLaughlin RM, Elder SH et al. Role of the tendons of the biceps brachii and in-fraspinatus muscles and the medial glenohumeral ligament in the maintenance of passive shoulder joint stability in dogs. Am J Vet Res 2004; 65: 1216–1222.
3. Engen M. Surgical Treatments of Shoulder Lu-xations. In: Bojrab M, editor. Current Techniques in Small Animal Surgery. 4th ed. Maryland: Wil-liams & Wilkins 1998; pp. 1260–1261.
4. Craig E. Surgical Stabilization of traumatic medi-al shoulder dislocation. J Am Anim Hosp Assoc 1980; 16: 93–102.
5. Ringwood P. Medial glenohumeral ligament re-construction for ex-vivo medial glenohumeral lu-
Correspondence to: Constantin J. Post, Dr. med vet Vetsuisse Faculty, University of Zurich Clinic for Small Animal Surgery Winterthurerstraße 260 8057 Zurich, Switzerland Phone: +41 446358745, Fax: +41 446358944 E-mail: [email protected]














![Series FXS Solar Injection System...1/8" Plunger Min Flow Rate: 0.34 [GPO] Max Pressure: 12,000 [PSIG] 3/16" Plunger Min Flow Rate: 0.78 Max Pressure: 7,500 [PSIG] 1/4" Plunger Min](https://static.documents.pub/doc/80x56/5f3501e166994a531e4f54ad/series-fxs-solar-injection-system-18-plunger-min-flow-rate-034-gpo.jpg)
![1 Min Flow Rate Maximization for Software Defined Radio Access … · 2013-12-20 · arXiv:1312.5345v1 [cs.IT] 18 Dec 2013 1 Min Flow Rate Maximization for Software Defined Radio](https://static.documents.pub/doc/80x56/5e98fc6726025b21e1204574/1-min-flow-rate-maximization-for-software-deined-radio-access-2013-12-20-arxiv13125345v1.jpg)






