Application of Neutron Capture Therapy to Widespread Tumours Saverio Altieri 1,2 Silva Bortolussi 1,2 1 Department of Nuclear and Theoretical Physics, University of Pavia, Italy 2 INFN (National Institute of Nuclear Physics), section of Pavia, Italy. [email protected]Abstract. The neutron Capture Therapy (NCT) is a new Radiation Therapy technique characterized by very high tumour selectivity. Elements with large neutron capture cross sections, as 10 B, concentrate in tumoral cells 4-5 times more than in healthy ones. The 10 B(n,α) 7 Li reaction induced by thermal neutron irradiation is lethal only for cells with high 10 B concentrations. This is due to the very short range of α particles and 7 Li nuclei. BNCT is particularly powerful in the treatment of tumours that are widespread in an entire organ, as lung or liver. For the first time in the world BNCT was applied to the cure of liver metastases at pavia University. After Boro-Phenylalanine administration, the organ was removed from the patient body, irradiated inside the thermal column of a nuclear reactor, and re-implanted (autotrasplantation). Presently we are studying the possibility to extend BNCT application to the cure of lung tumours in a rat model. Results of both researches are presented. 1. Basic Principles of BNCT Neutron Capture Therapy (NCT) is made up of two phases. The first one consists in infusing the patient with a solution that selectively concentrates in the tumoral cells a proper element wich has high neutron capture cross section ( 10 B or Gd); in the second phase the interested zone is irradiated by thermal or epithermal neutrons. During the irradiation, charged particles originate from neutron capture; their range in tissues is of the same order of a cell diameter. This fact allows to deliver a lethal dose to tumoral cells, that are rich in Boron or Gadolinium concentration, and to spare healthy ones. The rection used in the therapy is the following: 10 B(n,α) 7 Li, and in this case the technique is called BNCT (Boron Neutron Capture Therapy). This reaction has some characteristics that make it particularly suitable to the therapy: • the cross section for thermal neutron capture is very high (3840 barn at 0.025 eV), and the Q- value is positive (Q=2.792 MeV); • the reaction products deposit all their energy in 10 μm from the point where they are created, that is, substantially inside the cell in wich the reaction takes place; • the dose is delivered only during neutron irradiation because the reaction products are not radioactive; if an explanted organ is irradiated, the whole body is spared from undesired dose. The selective Boron uptake in the tumour with respect to healthy tissues, makes BNCT an extremely advantageous technique to cure tumours that affect whole vital organs and that are not surgically operable. In this case the treatment can be performed by neutron irradiation of the entire organ without
Transcript
Application of Neutron Capture Therapy to Widespread Tumours
Saverio Altieri1,2 Silva Bortolussi1,2
1 Department of Nuclear and Theoretical Physics, University of Pavia, Italy 2 INFN (National Institute of Nuclear Physics), section of Pavia, Italy.
Abstract. The neutron Capture Therapy (NCT) is a new Radiation Therapy technique characterized by very high tumour selectivity. Elements with large neutron capture cross sections, as 10B, concentrate in tumoral cells 4-5 times more than in healthy ones. The 10B(n,α)7Li reaction induced by thermal neutron irradiation is lethal only for cells with high 10B concentrations. This is due to the very short range of α particles and 7Li nuclei. BNCT is particularly powerful in the treatment of tumours that are widespread in an entire organ, as lung or liver. For the first time in the world BNCT was applied to the cure of liver metastases at pavia University. After Boro-Phenylalanine administration, the organ was removed from the patient body, irradiated inside the thermal column of a nuclear reactor, and re-implanted (autotrasplantation). Presently we are studying the possibility to extend BNCT application to the cure of lung tumours in a rat model. Results of both researches are presented.
1. Basic Principles of BNCT Neutron Capture Therapy (NCT) is made up of two phases. The first one consists in infusing the patient with a solution that selectively concentrates in the tumoral cells a proper element wich has high neutron capture cross section (10B or Gd); in the second phase the interested zone is irradiated by thermal or epithermal neutrons. During the irradiation, charged particles originate from neutron capture; their range in tissues is of the same order of a cell diameter. This fact allows to deliver a lethal dose to tumoral cells, that are rich in Boron or Gadolinium concentration, and to spare healthy ones.
The rection used in the therapy is the following: 10B(n,α)7Li, and in this case the technique is called BNCT (Boron Neutron Capture Therapy). This reaction has some characteristics that make it particularly suitable to the therapy:
• the cross section for thermal neutron capture is very high (3840 barn at 0.025 eV), and the Q-value is positive (Q=2.792 MeV);
• the reaction products deposit all their energy in 10 μm from the point where they are created, that is, substantially inside the cell in wich the reaction takes place;
• the dose is delivered only during neutron irradiation because the reaction products are not radioactive; if an explanted organ is irradiated, the whole body is spared from undesired dose.
The selective Boron uptake in the tumour with respect to healthy tissues, makes BNCT an extremely advantageous technique to cure tumours that affect whole vital organs and that are not surgically operable. In this case the treatment can be performed by neutron irradiation of the entire organ without
the precise knowledge of number and position of metastatic nodules. An example is represented by liver colon-adenocarcinoma metastases that invade the whole organ after a successful surgical resection of primitive tumour. The autotransplant technique, consisting in the irradiation of the explanted liver in a thermal neutron field, was developed in Pavia, and to date has been applied on two terminal patients. Recently we have started a feasibility study to extend BNCT to cure diffuse lung tumours by external neutron beams.
2. Liver metastases Starting from an idea proposed by Pinelli, a long term research program to study the possibility to apply BNCT to explantable organs began at university of Pavia in 1987. In TAOrMINA project (Advanced Treatment of Organs by Means of Neutron Irradiation and Auto-transplant), the INFN section of Pavia, the Department of Nuclear and Theoretical Physics, the Depatment of Surgery (Division of Hepato-pancreatic Surgery) and the Department of Animal Biology of the Pavia University, the Centre of study for Histochemistry (CNR) and the IRCCS S. Matteo Policlinic of Pavia, were involved. The physical and surgical activities were coordinated by T. Pinelli and A. Zonta respectively. [1]
The therapeutic concept is based on the neutron irradiation of the isolated organs in a thermal neutron field produced in the Thermal column of the reactor Triga Mark II of Pavia University. The column was modified in order to realize a 100 cm long channel with graphite walls, with trasversal dimensions of 40 x 20 cm2. The γ background coming from the reactor core was drastically lowered by inserting two Bismuth screens, both 10 cm thick. The study of the irradiation field was performed using the Monte Carlo transport code MCNP [2].
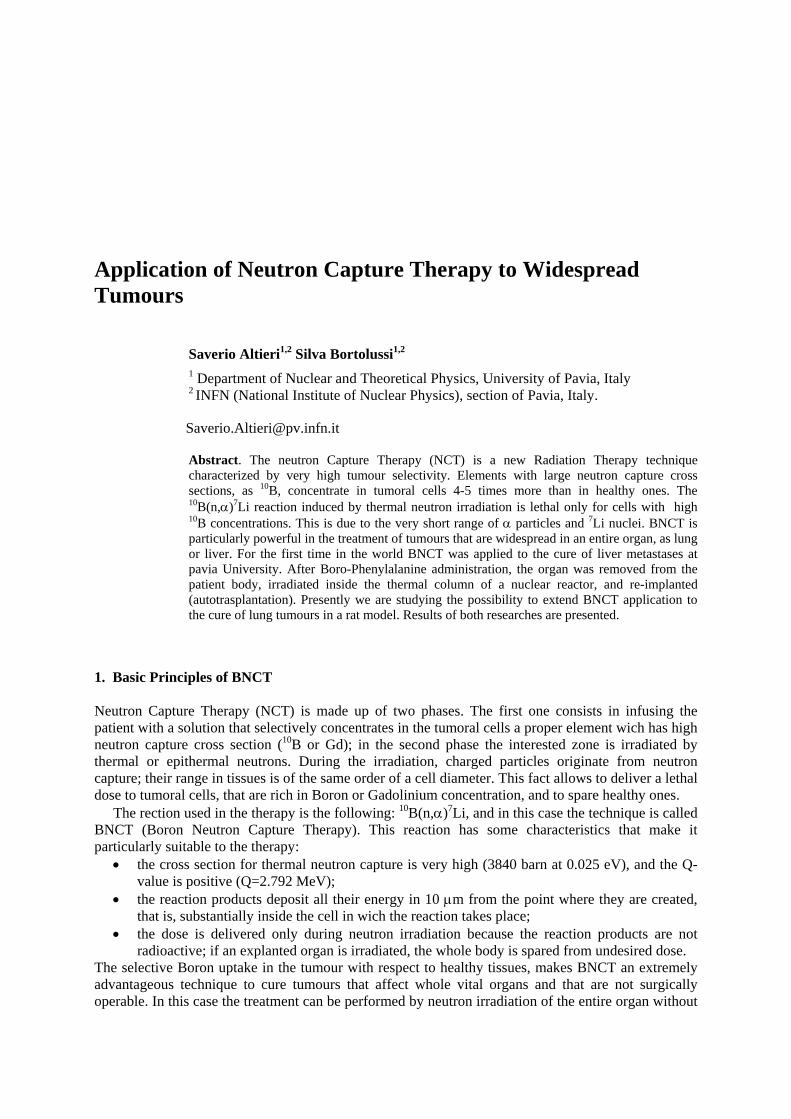
In the irradiation position, the thermal flux in air is 1.4.1010cm-2s-1 (±7%), while the epithermal component with energy higher than 0.2 eV is about three orders of magnitude lower. The behaviour of the thermal neutron flux in the irradiation position was studied both experimentally (by Copper wires activation) and by MCNP simulations. A teflon phantom of the human liver was realized for experimental measures in the right position inside the Thermal Column, and a model of the same phantom was built thanks to geometry capabilities of MCNP for calculation (fig.1) [3].
Fig.1 Liver model used to measure and simulate the neutron flux distribution in the irradiation position. On the left a particular of the thermal column is reported, in wich the Bismuth screens and the irradiation channel with the phantom can be seen.
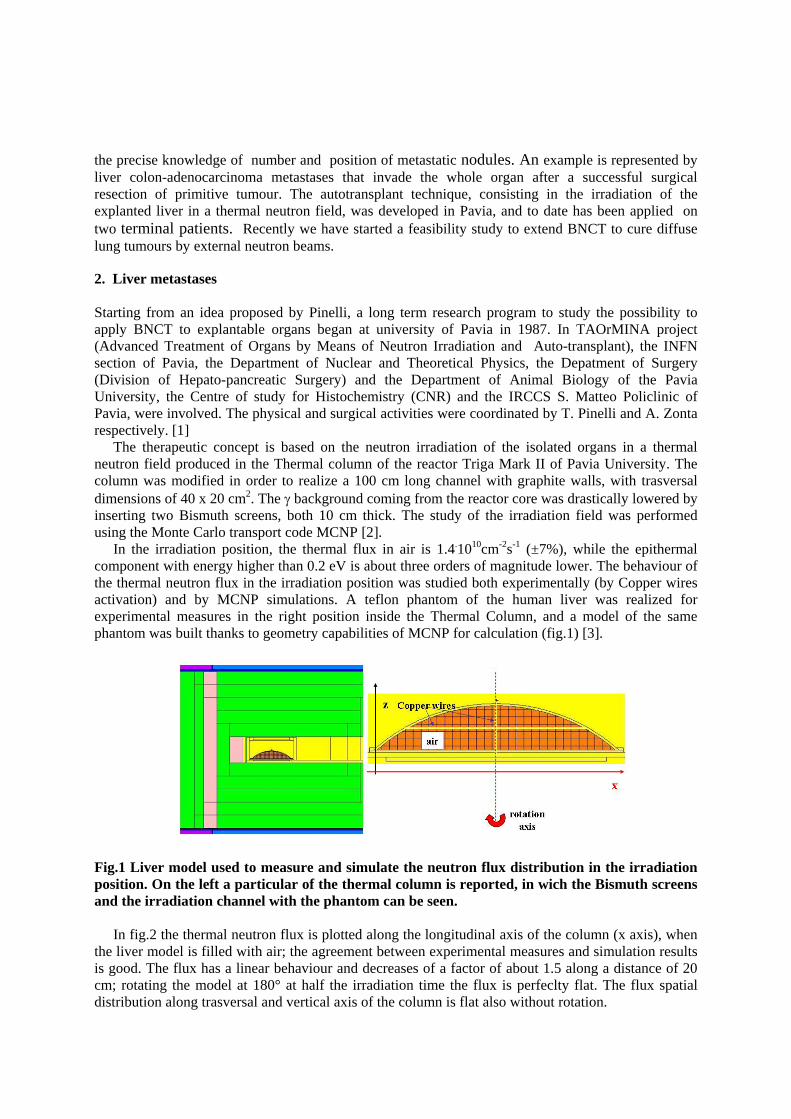
In fig.2 the thermal neutron flux is plotted along the longitudinal axis of the column (x axis), when
the liver model is filled with air; the agreement between experimental measures and simulation results is good. The flux has a linear behaviour and decreases of a factor of about 1.5 along a distance of 20 cm; rotating the model at 180° at half the irradiation time the flux is perfeclty flat. The flux spatial distribution along trasversal and vertical axis of the column is flat also without rotation.
Fig.2 Spatial behaviour of the neutron flux in the liver simplified model, filled with air. The experimental and simulated results are overlapped for comparison.
To study the distortion caused by the liver to the neutron flux distribution, an hepatic-equivalent
solution was realized, wich composition and percentage in weight of each element is reported in tab.1 and tab.2.
compound H2O CH4N2O CH4N2O KCl H3PO3 H3BO3 Total mass (g) 909.2 64.3 11.2 4.2 9.5 1.6 1000
Tab. 1 Compounds of the hepathic-equivalent solution with 50 ppm of 10B
Tab. 2 Elemental composition of the hepathic-equivalent solution with 50 ppm of 10B compared with ICRU 46 [4]
The introduction of the hepatic solution modifies the flux distribution in a way that the ratio
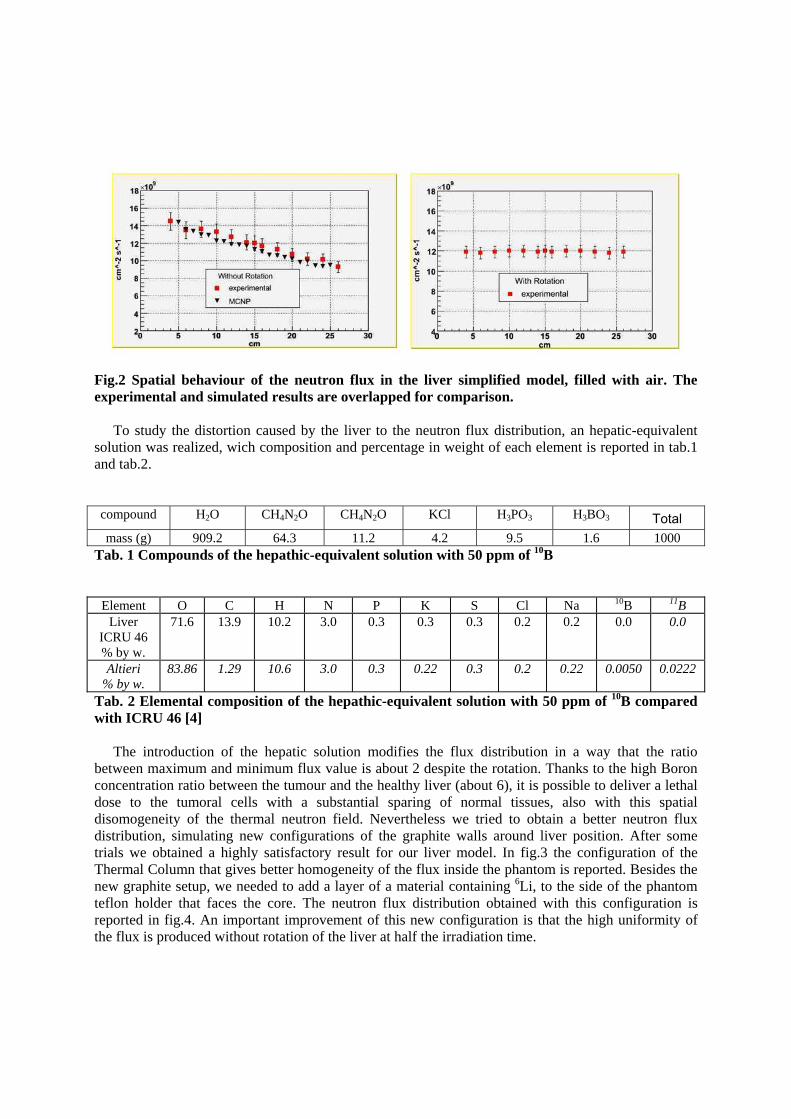
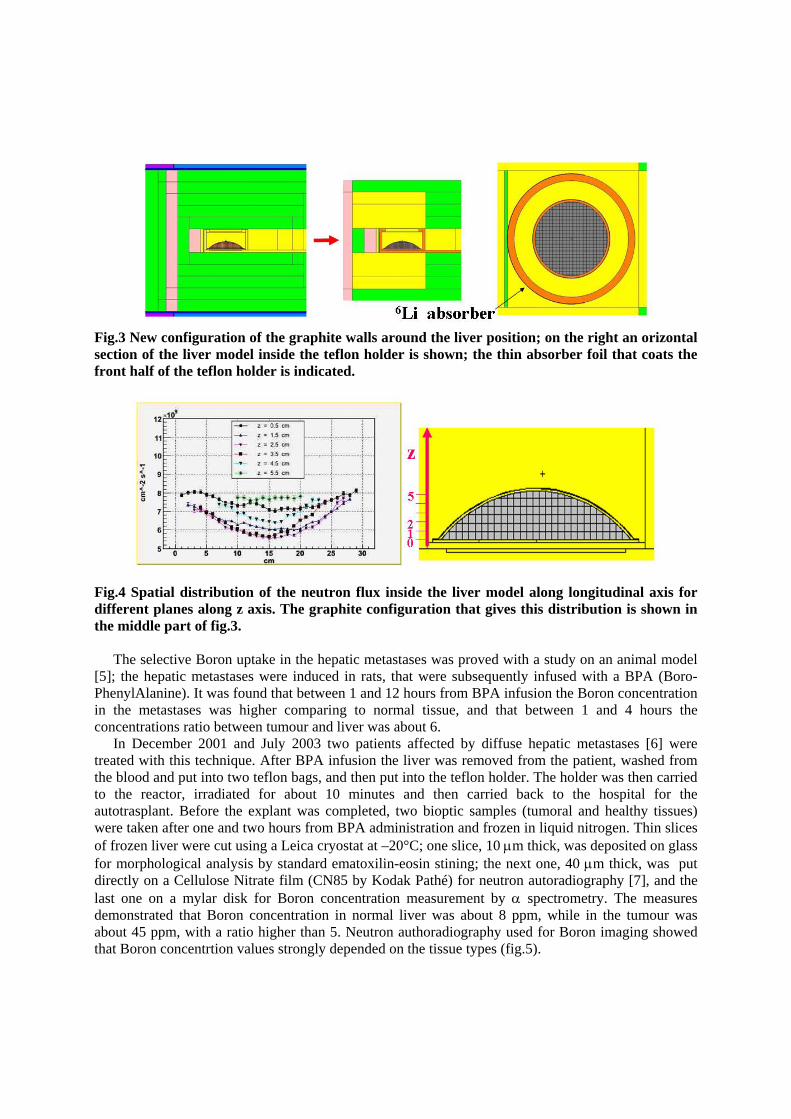
between maximum and minimum flux value is about 2 despite the rotation. Thanks to the high Boron concentration ratio between the tumour and the healthy liver (about 6), it is possible to deliver a lethal dose to the tumoral cells with a substantial sparing of normal tissues, also with this spatial disomogeneity of the thermal neutron field. Nevertheless we tried to obtain a better neutron flux distribution, simulating new configurations of the graphite walls around liver position. After some trials we obtained a highly satisfactory result for our liver model. In fig.3 the configuration of the Thermal Column that gives better homogeneity of the flux inside the phantom is reported. Besides the new graphite setup, we needed to add a layer of a material containing 6Li, to the side of the phantom teflon holder that faces the core. The neutron flux distribution obtained with this configuration is reported in fig.4. An important improvement of this new configuration is that the high uniformity of the flux is produced without rotation of the liver at half the irradiation time.
Fig.3 New configuration of the graphite walls around the liver position; on the right an orizontal section of the liver model inside the teflon holder is shown; the thin absorber foil that coats the front half of the teflon holder is indicated.
Fig.4 Spatial distribution of the neutron flux inside the liver model along longitudinal axis for different planes along z axis. The graphite configuration that gives this distribution is shown in the middle part of fig.3.
The selective Boron uptake in the hepatic metastases was proved with a study on an animal model
[5]; the hepatic metastases were induced in rats, that were subsequently infused with a BPA (Boro-PhenylAlanine). It was found that between 1 and 12 hours from BPA infusion the Boron concentration in the metastases was higher comparing to normal tissue, and that between 1 and 4 hours the concentrations ratio between tumour and liver was about 6.
In December 2001 and July 2003 two patients affected by diffuse hepatic metastases [6] were treated with this technique. After BPA infusion the liver was removed from the patient, washed from the blood and put into two teflon bags, and then put into the teflon holder. The holder was then carried to the reactor, irradiated for about 10 minutes and then carried back to the hospital for the autotrasplant. Before the explant was completed, two bioptic samples (tumoral and healthy tissues) were taken after one and two hours from BPA administration and frozen in liquid nitrogen. Thin slices of frozen liver were cut using a Leica cryostat at –20°C; one slice, 10 μm thick, was deposited on glass for morphological analysis by standard ematoxilin-eosin stining; the next one, 40 μm thick, was put directly on a Cellulose Nitrate film (CN85 by Kodak Pathé) for neutron autoradiography [7], and the last one on a mylar disk for Boron concentration measurement by α spectrometry. The measures demonstrated that Boron concentration in normal liver was about 8 ppm, while in the tumour was about 45 ppm, with a ratio higher than 5. Neutron authoradiography used for Boron imaging showed that Boron concentrtion values strongly depended on the tissue types (fig.5).
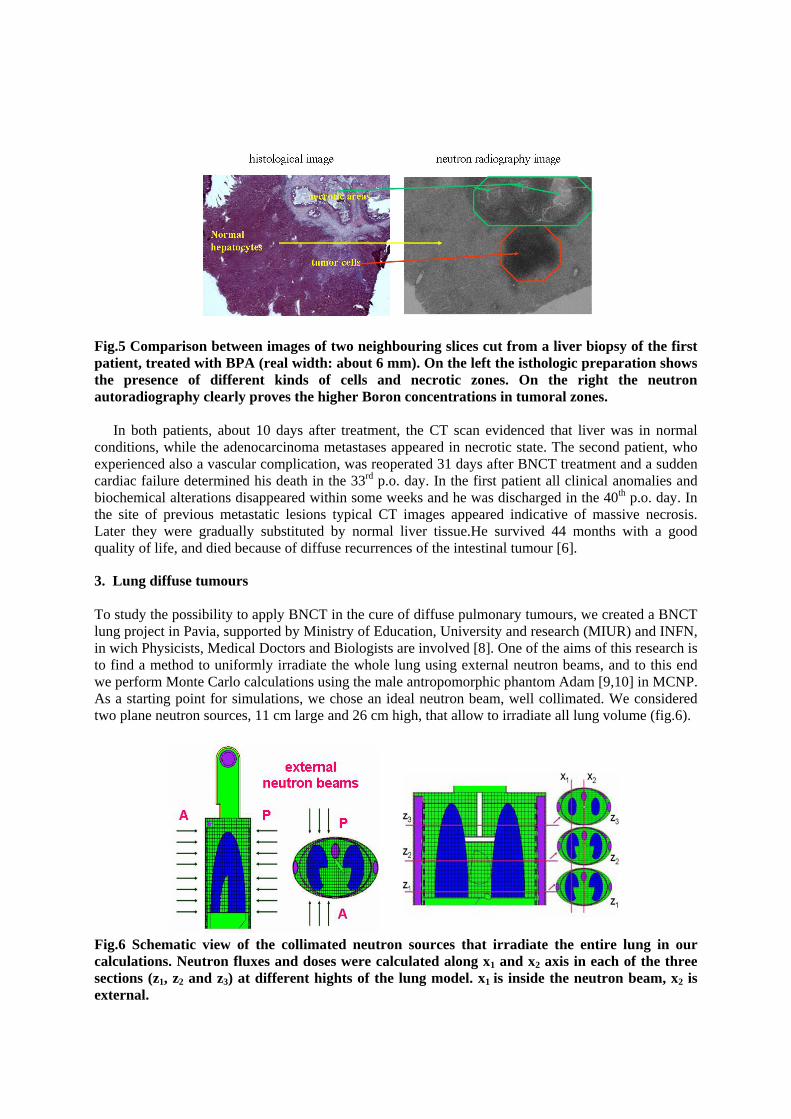
Fig.5 Comparison between images of two neighbouring slices cut from a liver biopsy of the first patient, treated with BPA (real width: about 6 mm). On the left the isthologic preparation shows the presence of different kinds of cells and necrotic zones. On the right the neutron autoradiography clearly proves the higher Boron concentrations in tumoral zones.
In both patients, about 10 days after treatment, the CT scan evidenced that liver was in normal conditions, while the adenocarcinoma metastases appeared in necrotic state. The second patient, who experienced also a vascular complication, was reoperated 31 days after BNCT treatment and a sudden cardiac failure determined his death in the 33rd p.o. day. In the first patient all clinical anomalies and biochemical alterations disappeared within some weeks and he was discharged in the 40th p.o. day. In the site of previous metastatic lesions typical CT images appeared indicative of massive necrosis. Later they were gradually substituted by normal liver tissue.He survived 44 months with a good quality of life, and died because of diffuse recurrences of the intestinal tumour [6].
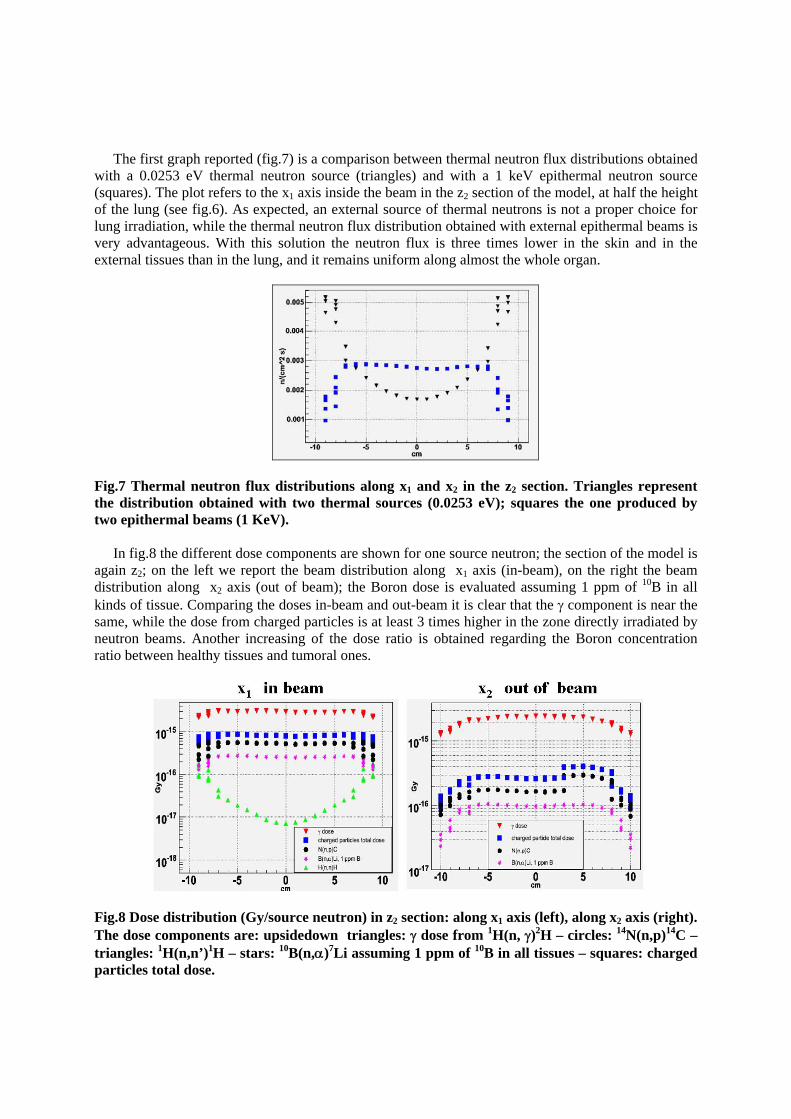
3. Lung diffuse tumours To study the possibility to apply BNCT in the cure of diffuse pulmonary tumours, we created a BNCT lung project in Pavia, supported by Ministry of Education, University and research (MIUR) and INFN, in wich Physicists, Medical Doctors and Biologists are involved [8]. One of the aims of this research is to find a method to uniformly irradiate the whole lung using external neutron beams, and to this end we perform Monte Carlo calculations using the male antropomorphic phantom Adam [9,10] in MCNP. As a starting point for simulations, we chose an ideal neutron beam, well collimated. We considered two plane neutron sources, 11 cm large and 26 cm high, that allow to irradiate all lung volume (fig.6).
Fig.6 Schematic view of the collimated neutron sources that irradiate the entire lung in our calculations. Neutron fluxes and doses were calculated along x1 and x2 axis in each of the three sections (z1, z2 and z3) at different hights of the lung model. x1 is inside the neutron beam, x2 is external.
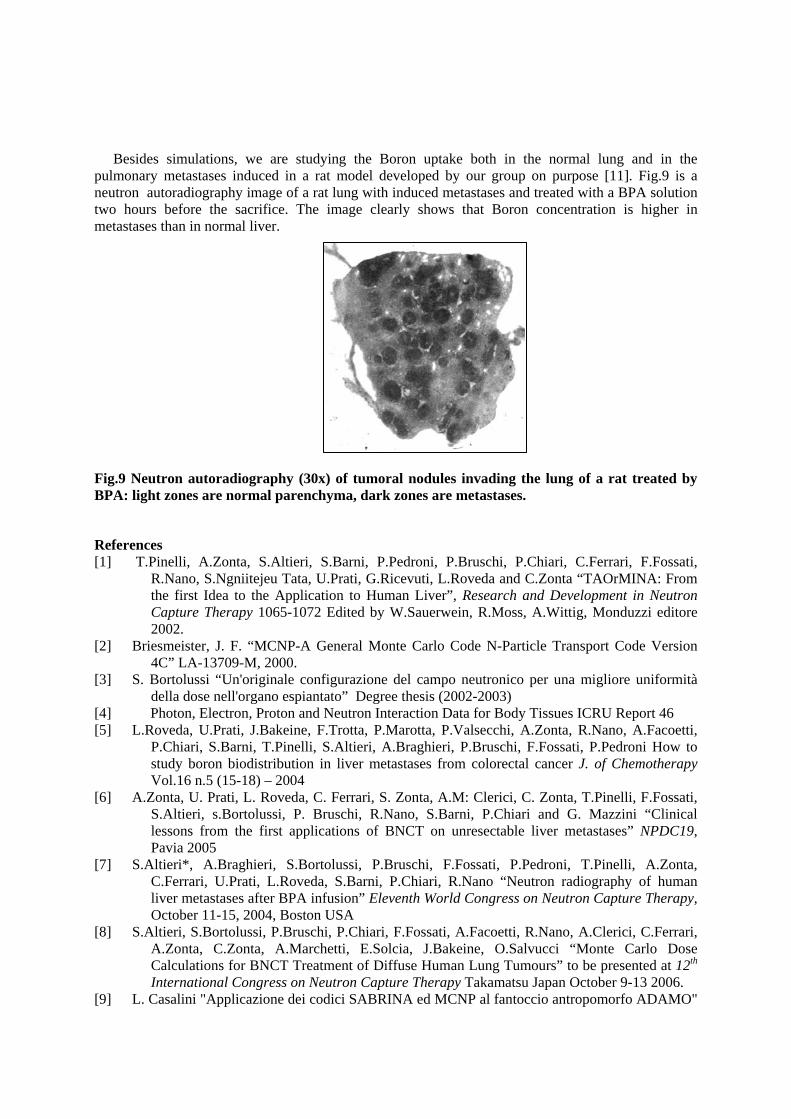
The first graph reported (fig.7) is a comparison between thermal neutron flux distributions obtained with a 0.0253 eV thermal neutron source (triangles) and with a 1 keV epithermal neutron source (squares). The plot refers to the x1 axis inside the beam in the z2 section of the model, at half the height of the lung (see fig.6). As expected, an external source of thermal neutrons is not a proper choice for lung irradiation, while the thermal neutron flux distribution obtained with external epithermal beams is very advantageous. With this solution the neutron flux is three times lower in the skin and in the external tissues than in the lung, and it remains uniform along almost the whole organ.
Fig.7 Thermal neutron flux distributions along x1 and x2 in the z2 section. Triangles represent the distribution obtained with two thermal sources (0.0253 eV); squares the one produced by two epithermal beams (1 KeV).
In fig.8 the different dose components are shown for one source neutron; the section of the model is
again z2; on the left we report the beam distribution along x1 axis (in-beam), on the right the beam distribution along x2 axis (out of beam); the Boron dose is evaluated assuming 1 ppm of 10B in all kinds of tissue. Comparing the doses in-beam and out-beam it is clear that the γ component is near the same, while the dose from charged particles is at least 3 times higher in the zone directly irradiated by neutron beams. Another increasing of the dose ratio is obtained regarding the Boron concentration ratio between healthy tissues and tumoral ones.
Fig.8 Dose distribution (Gy/source neutron) in z2 section: along x1 axis (left), along x2 axis (right). The dose components are: upsidedown triangles: γ dose from 1H(n, γ)2H – circles: 14N(n,p)14C – triangles: 1H(n,n’)1H – stars: 10B(n,α)7Li assuming 1 ppm of 10B in all tissues – squares: charged particles total dose.
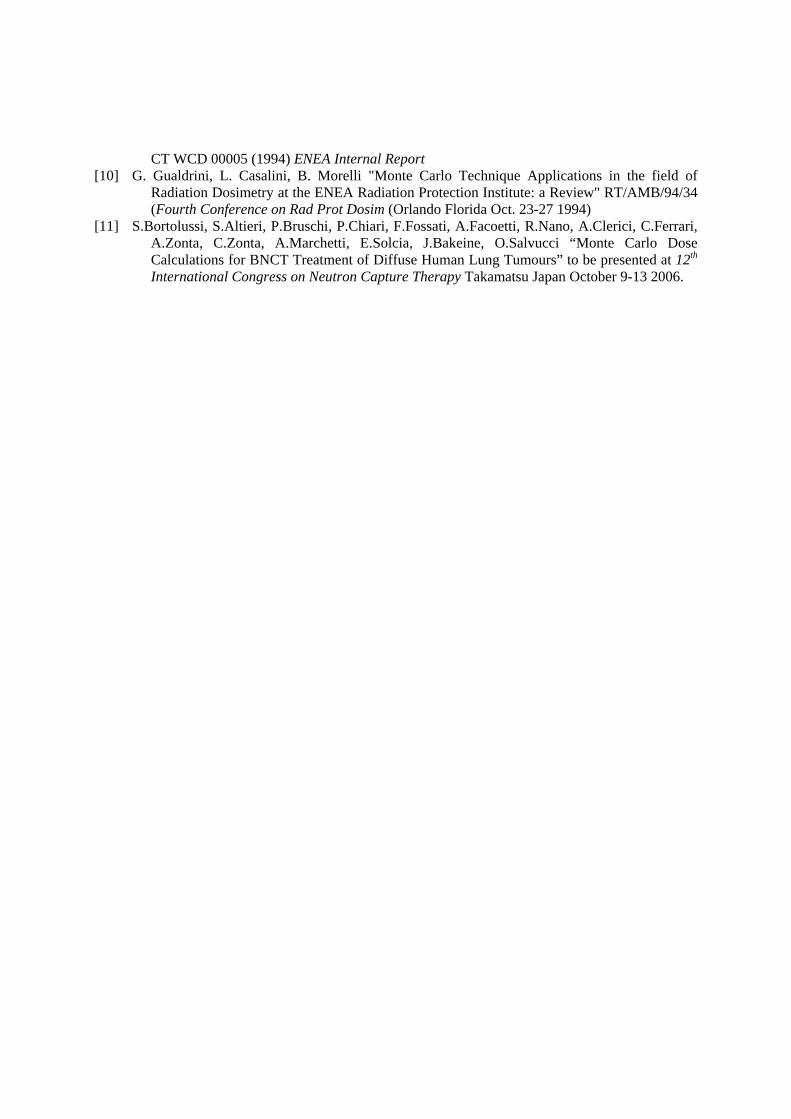
Besides simulations, we are studying the Boron uptake both in the normal lung and in the pulmonary metastases induced in a rat model developed by our group on purpose [11]. Fig.9 is a neutron autoradiography image of a rat lung with induced metastases and treated with a BPA solution two hours before the sacrifice. The image clearly shows that Boron concentration is higher in metastases than in normal liver.
Fig.9 Neutron autoradiography (30x) of tumoral nodules invading the lung of a rat treated by BPA: light zones are normal parenchyma, dark zones are metastases.
R.Nano, S.Ngniitejeu Tata, U.Prati, G.Ricevuti, L.Roveda and C.Zonta “TAOrMINA: From the first Idea to the Application to Human Liver”, Research and Development in Neutron Capture Therapy 1065-1072 Edited by W.Sauerwein, R.Moss, A.Wittig, Monduzzi editore 2002.
[2] Briesmeister, J. F. “MCNP-A General Monte Carlo Code N-Particle Transport Code Version 4C” LA-13709-M, 2000.
[3] S. Bortolussi “Un'originale configurazione del campo neutronico per una migliore uniformità della dose nell'organo espiantato” Degree thesis (2002-2003)
[4] Photon, Electron, Proton and Neutron Interaction Data for Body Tissues ICRU Report 46 [5] L.Roveda, U.Prati, J.Bakeine, F.Trotta, P.Marotta, P.Valsecchi, A.Zonta, R.Nano, A.Facoetti,
P.Chiari, S.Barni, T.Pinelli, S.Altieri, A.Braghieri, P.Bruschi, F.Fossati, P.Pedroni How to study boron biodistribution in liver metastases from colorectal cancer J. of Chemotherapy Vol.16 n.5 (15-18) – 2004
[6] A.Zonta, U. Prati, L. Roveda, C. Ferrari, S. Zonta, A.M: Clerici, C. Zonta, T.Pinelli, F.Fossati, S.Altieri, s.Bortolussi, P. Bruschi, R.Nano, S.Barni, P.Chiari and G. Mazzini “Clinical lessons from the first applications of BNCT on unresectable liver metastases” NPDC19, Pavia 2005
[7] S.Altieri*, A.Braghieri, S.Bortolussi, P.Bruschi, F.Fossati, P.Pedroni, T.Pinelli, A.Zonta, C.Ferrari, U.Prati, L.Roveda, S.Barni, P.Chiari, R.Nano “Neutron radiography of human liver metastases after BPA infusion” Eleventh World Congress on Neutron Capture Therapy, October 11-15, 2004, Boston USA
[8] S.Altieri, S.Bortolussi, P.Bruschi, P.Chiari, F.Fossati, A.Facoetti, R.Nano, A.Clerici, C.Ferrari, A.Zonta, C.Zonta, A.Marchetti, E.Solcia, J.Bakeine, O.Salvucci “Monte Carlo Dose Calculations for BNCT Treatment of Diffuse Human Lung Tumours” to be presented at 12th International Congress on Neutron Capture Therapy Takamatsu Japan October 9-13 2006.
[9] L. Casalini "Applicazione dei codici SABRINA ed MCNP al fantoccio antropomorfo ADAMO"
CT WCD 00005 (1994) ENEA Internal Report [10] G. Gualdrini, L. Casalini, B. Morelli "Monte Carlo Technique Applications in the field of
Radiation Dosimetry at the ENEA Radiation Protection Institute: a Review" RT/AMB/94/34 (Fourth Conference on Rad Prot Dosim (Orlando Florida Oct. 23-27 1994)
[11] S.Bortolussi, S.Altieri, P.Bruschi, P.Chiari, F.Fossati, A.Facoetti, R.Nano, A.Clerici, C.Ferrari, A.Zonta, C.Zonta, A.Marchetti, E.Solcia, J.Bakeine, O.Salvucci “Monte Carlo Dose Calculations for BNCT Treatment of Diffuse Human Lung Tumours” to be presented at 12th International Congress on Neutron Capture Therapy Takamatsu Japan October 9-13 2006.


![[Tumours of testis]](https://static.documents.pub/doc/80x56/635022e42630aed50008c845/tumours-of-testis.jpg)













