430
| Date post: | 30-Jan-2023 |
| Category: |
Documents |
| Upload: | khangminh22 |
| View: | 0 times |
| Download: | 0 times |
This book and all other volumes of the series can be purchased from:
International Agency for IARCPress IARCPressResearch on Cancer (IARC) 150 Cours Albert Thomas 1775 K Street, NW, Suite 480
69008 Lyon (France) Washington, DC 20006 (USA)Tel. +33 4 72 73 85 15 Toll-free order line: 877 WHO-IARCFax +33 4 72 73 83 02 Fax (202) 223 [email protected] [email protected]
World Health Organization (WHO) WHO Marketing and Dissemination WHO Publications Center1211 Geneva (Switzerland) Albany, NY 12210 (USA) Tel. +41 22 791 2476 Tel. (518) 436 9686Fax +41 22 791 4857 Fax (518) 436 [email protected] [email protected]
Oxford University Press (OUP) OUP Oxford (UK)Tel. +44 1536 45453424 hr. Hotline:Tel. +44 1 536 74 17 27Fax +44 1 865 26 77 [email protected]
WHO Blue Books on the web: www.iarc.fr/who-bluebooks
Previous volumes in this series
Kleihues P., Cavenee W. K .(Eds.): World Health Org a n i z a t i o nClassification of Tu m o u r s .Pathology and Genetics ofTumours of the Nerv o u sSystem. IARC Press: Lyon 2000I S B N 92 83 22409 4
Hamilton S.R., Aaltonen L.A.(Eds.): World Health Org a n i z a t i o nClassification of Tu m o u r s .Pathology and Genetics ofTumours of the DigestiveSystem. IARC Press: Lyon 2000 ISBN 92 83 22410 8
J a ffe E.S., Harris N.L., SteinH., Va rdiman J.V. (Eds.):World Health Org a n i z a t i o nClassification of Tu m o u r s .Pathology and Genetics ofTumours of Haematopoieticand Lymphoid Tissues. IARC Press: Lyon 2001ISBN 92 83 22411 6
Fletcher C.D.M., Unni K.K.,Mertens F. (Eds.): World Health OrganizationClassification of Tumours.Pathology and Genetics ofTumours of Soft Tissue andBone.IARC Press: Lyon 2002ISBN 92 832 2413 2

World Health Organization Classification of Tumours
International Agency for Research on Cancer (IARC)
Pathology and Genetics ofTumours of the Breast and
Female Genital Organs
Edited by
Fattaneh A. Tavassoli
Peter Devilee
IARCPress
Lyon, 2003
WHO OMS

World Health Organization Classification of Tumours
Series Editors Paul Kleihues, M.D.Leslie H. Sobin, M.D.
Pathology and Genetics of Tumours of the Breast and Female Genital Organs
Editors
Coordinating Editors
Editorial Assistants
Layout
Illustrations
Printed by
Publisher
Fattaneh A. Tavassoli, M.D.Peter Devilee, Ph.D.
Lawrence M. Roth, M.D.Rosemary Millis, M.D.
Isabelle ForcierChristine Zorian
Lauren A. HunterSibylle SöringPascale Dia
Georges MollonLauren A. Hunter
Druckhaus Tecklenborg48565 Steinfurt, Germany
IARCPressInternational Agency for Research on Cancer (IARC)69008 Lyon, France

This volume was produced in collaboration with the
International Academy of Pathology (IAP)
The WHO Classification of Tumours of the Breast and Female Genital Organspresented in this book reflects the views of Working Groups that convened for
Editorial and Consensus Conferences in Lyon, France, January 12-16 and March 16-20, 2002.
Members of the Working Groups are indicated in the List of Contributors on page 365
The Working Group on Gynaecological Tumours greatly appreciates the participation of, and guidance by
Dr. Robert E. Scully, Harvard Medical School

Published by IARC Press, International Agency for Research on Cancer,150 cours Albert Thomas, F-69008 Lyon, France
© International Agency for Research on Cancer, 2003
Publications of the World Health Organization enjoy copyright protection in accordance with the provisions of Protocol 2 of the Universal Copyright Convention.
All rights reserved.
The International Agency for Research on Cancer welcomes requests for permission to reproduce or translate its publications, in part or in full.
Requests for permission to reproduce figures or charts from this publication should be directed tothe respective contributor (see section Source of Charts and Photographs).
The designations used and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the Secretariat of the
World Health Organization concerning the legal status of any country, territory, city, or area or of its authorities, or concerning the delimitation of its frontiers or boundaries.
The mention of specific companies or of certain manufacturers' products does not imply that they are endorsed or recommended by the World Health Organization in preference to others
of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
The authors alone are responsible for the views expressed in this publication.
Enquiries should be addressed to the Communications Unit,International Agency for Research on Cancer, 69008 Lyon, France,
which will provide the latest information on any changes made to the text and plans for new editions.
IARC Library Cataloguing in Publication Data
Pathology and genetics of tumours of the breast and female genital organs / editors, Fattaneh A. Tavassoli, Peter Devilee.
(World Health Organization classification of tumours ; 5)
1. Breast Neoplasms—genetics. 2. Breast Neoplasms—pathology 3. Genital Neoplasms, Female—genetics 4. Genital Neoplasms, Female—pathologyI. Tavassoli, Fattaneh A. II. Devilee, Peter III. Series
ISBN 92 832 2412 4 (NLM Classification W 1)
Format for bibliographic citations:Tavassoli F.A., Devilee P. (Eds.): World Health Organization Classification ofTumours. Pathology and Genetics of Tumours of the Breast and Female Genital Organs. IARC Press: Lyon 2003
1 Tumours of the breast 9Invasive breast carcinoma 13
Invasive ductal carcinoma, NOS 19Invasive lobular carcinoma 23Tubular carcinoma 26Invasive cribriform carcinoma 27Medullary carcinoma 28Mucin producing carcinomas 30Neuroendocrine tumours 32Invasive papillary carcinoma 34Invasive micropapillary carcinoma 35Apocrine carcinoma 36Metaplastic carcinomas 37Lipid-rich carcinoma 41Secretory carcinoma 42Oncocytic carcinoma 43Adenoid cystic carcinoma 44Acinic cell carcinoma 45Glycogen-rich clear cell carcinoma 46Sebaceous carcinoma 46Inflammatory carcinoma 47Bilateral breast carcinoma 48
Precursor lesionsLobular neoplasia 60Intraductal proliferative lesions 63Microinvasive carcinoma 74Intraductal papillary neoplasms 76
Benign epithelial lesions 81Myoepithelial lesions 86Mesenchymal tumours 89Fibroepithelial tumours 99Tumours of the nipple 104Malignant lymphoma and metastatic tumours 107Tumours of the male breast 110
2 Tumours of the ovary and peritoneum 113Surface epithelial-stromal tumours 117
Serous tumours 119Mucinous tumours 124Endometrioid tumours 130Clear cell tumours 137Transitional cell tumours 140Squamous cell lesions 143Mixed epithelial tumours 144Undifferentiated carcinomas 145
Sex cord-stromal tumours 146Granulosa-stromal cell tumours 146Sertoli-stromal cell tumours 153Mixed sex cord-stromal tumours 158Steroid cell tumours 160
Germ cell tumours 163Primitive germ cell tumours 163Biphasic or triphasic teratomas 168Monodermal teratomas 171
Mixed germ cell-sex cord-stromal tumours 176Tumours and related lesions of the rete ovarii 180Miscellaneous tumours and tumour-like lesions 182Lymphomas and leukaemias 191Secondary tumours of the ovary 193Peritoneal tumours 197
3 Tumours of the fallopian tube and uterine ligaments 203Tumours of the fallopian tube 206Tumours of the uterine ligaments 212
4 Tumours of the uterine corpus 217Epithelial tumours and related lesions 221
Endometrial carcinoma 221Endometrial hyperplasia 228Endometrial polyp 230
Mesenchymal tumours and related lesions 233Endometrial stromal and related tumours 233Smooth muscle tumours 236Other mesenchymal tumours 242
Mixed epithelial and mesenchymal tumours 245Gestational trophoblastic disease 250Sex cord-like, neuroectodermal / neuroendocrine tumours,
lymphomas and leukaemias 255Secondary tumours of the uterine corpus 257
5 Tumours of the uterine cervix 259Epithelial tumours 262
Squamous tumours and precursors 266Glandular tumours and precursors 272Uncommon carcinomas and neuroendocrine tumours 277
Mesenchymal tumours 280Mixed epithelial and mesenchymal tumours 284Melanotic, germ cell, lymphoid and
secondary tumours of the cervix 287
6 Tumours of the vagina 291Epithelial tumours 293
Squamous tumours 293Glandular tumours 297Tumours of skin appendage origin 324
Mesenchymal tumours 302Mixed epithelial and mesenchymal tumours 306Melanotic, neuroectodermal, lymphoid and
secondary tumours 308
7 Tumours of the vulva 313Epithelial tumours 316
Squamous tumours 316Glandular tumours 321
Mesenchymal tumours 326Melanocytic tumours 331Germ cell, neuroectodermal, lymphoid and
secondary tumours 333
8 Inherited tumour syndromes 335Familial aggregation of cancers of the breast and
female genital organs 336BRCA1 syndrome 338BRCA2 syndrome 346Li-Fraumeni syndrome 351Cowden syndrome 355Hereditary non-polyposis colon cancer (HNPCC) 358Ataxia telangiectasia syndrome 361
Contributors 365Source of charts and photographs 370References 372Subject index 425
Contents
CHAPTER 1
Tumours of the Breast
Cancer of the breast is one of the most common human neo-plasms, accounting for approximately one quarter of all can-cers in females. It is associated with the Western lifestyle, andincidence rates are, there f o re, highest in countries withadvanced economies. Additional risk factors include earlymenarche and late childbirth. Breast cancer is further charac-terized by a marked genetic susceptibility. Early detection andadvances in treatment have begun to reduce mortality rates inseveral countries. Through the use of cDNA expression pro-files, it may become possible to predict clinical outcome in indi-vidual patients.
The typing of invasive breast cancer and its histological vari-ants is well established. More difficult is the classification ofpre-invasive breast lesions which are now increasingly detect-ed by mammography. The WHO Working Group agreed thatmore clinical follow-up and genetic data are needed for a bet-ter understanding of the natural history of these lesions.
10 Tumours of the breast
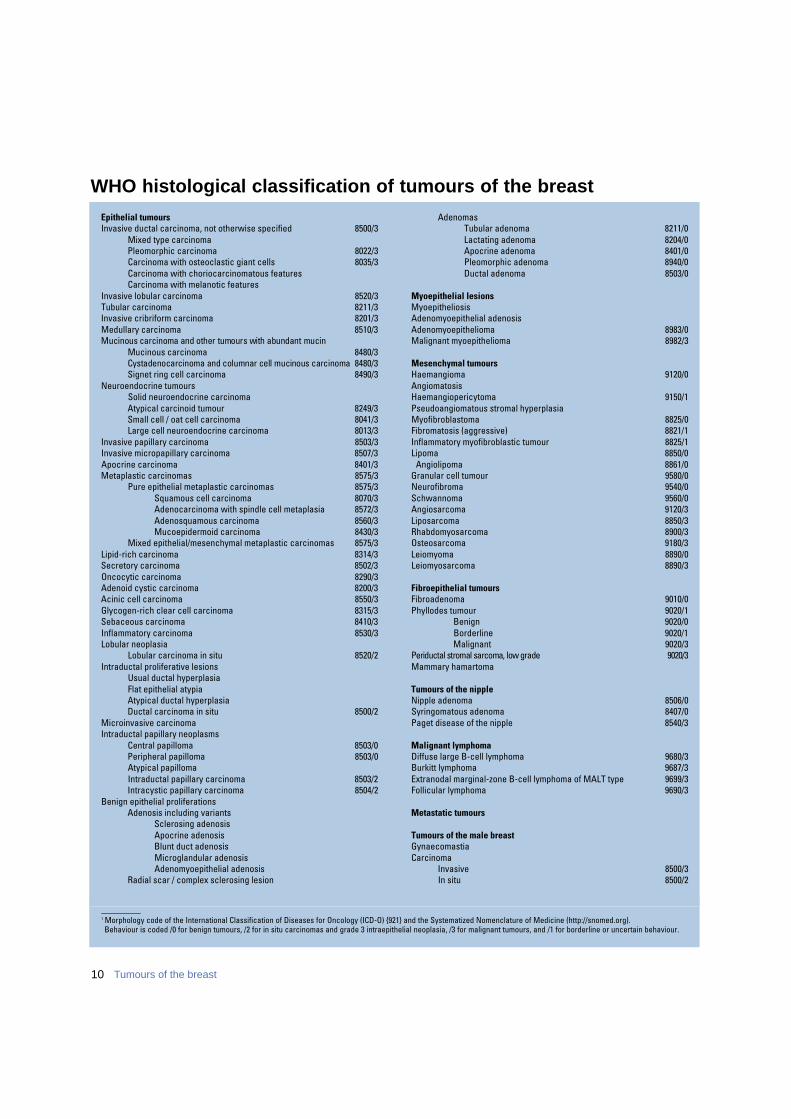
WHO histological classification of tumours of the breast
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org). Behaviour is coded /0 for benign tumours, /2 for in situ carcinomas and grade 3 intraepithelial neoplasia, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Epithelial tumoursInvasive ductal carcinoma, not otherwise specified 8500/3
Mixed type carcinomaPleomorphic carcinoma 8022/3Carcinoma with osteoclastic giant cells 8035/3Carcinoma with choriocarcinomatous featuresCarcinoma with melanotic features
Invasive lobular carcinoma 8520/3Tubular carcinoma 8211/3Invasive cribriform carcinoma 8201/3Medullary carcinoma 8510/3Mucinous carcinoma and other tumours with abundant mucin
Mucinous carcinoma 8480/3Cystadenocarcinoma and columnar cell mucinous carcinoma 8480/3Signet ring cell carcinoma 8490/3
Neuroendocrine tumoursSolid neuroendocrine carcinomaAtypical carcinoid tumour 8249/3Small cell / oat cell carcinoma 8041/3Large cell neuroendocrine carcinoma 8013/3
Invasive papillary carcinoma 8503/3Invasive micropapillary carcinoma 8507/3Apocrine carcinoma 8401/3Metaplastic carcinomas 8575/3
Pure epithelial metaplastic carcinomas 8575/3Squamous cell carcinoma 8070/3Adenocarcinoma with spindle cell metaplasia 8572/3Adenosquamous carcinoma 8560/3Mucoepidermoid carcinoma 8430/3
Mixed epithelial/mesenchymal metaplastic carcinomas 8575/3Lipid-rich carcinoma 8314/3Secretory carcinoma 8502/3Oncocytic carcinoma 8290/3Adenoid cystic carcinoma 8200/3Acinic cell carcinoma 8550/3Glycogen-rich clear cell carcinoma 8315/3Sebaceous carcinoma 8410/3Inflammatory carcinoma 8530/3Lobular neoplasia
Lobular carcinoma in situ 8520/2Intraductal proliferative lesions
Usual ductal hyperplasiaFlat epithelial atypiaAtypical ductal hyperplasiaDuctal carcinoma in situ 8500/2
Microinvasive carcinomaIntraductal papillary neoplasms
Central papilloma 8503/0Peripheral papilloma 8503/0Atypical papillomaIntraductal papillary carcinoma 8503/2Intracystic papillary carcinoma 8504/2
Benign epithelial proliferationsAdenosis including variants
Sclerosing adenosisApocrine adenosisBlunt duct adenosisMicroglandular adenosisAdenomyoepithelial adenosis
Radial scar / complex sclerosing lesion
AdenomasTubular adenoma 8211/0Lactating adenoma 8204/0Apocrine adenoma 8401/0Pleomorphic adenoma 8940/0Ductal adenoma 8503/0
Myoepithelial lesionsMyoepitheliosisAdenomyoepithelial adenosisAdenomyoepithelioma 8983/0Malignant myoepithelioma 8982/3
Mesenchymal tumoursHaemangioma 9120/0AngiomatosisHaemangiopericytoma 9150/1Pseudoangiomatous stromal hyperplasiaMyofibroblastoma 8825/0Fibromatosis (aggressive) 8821/1Inflammatory myofibroblastic tumour 8825/1Lipoma 8850/0
Angiolipoma 8861/0Granular cell tumour 9580/0Neurofibroma 9540/0Schwannoma 9560/0Angiosarcoma 9120/3Liposarcoma 8850/3Rhabdomyosarcoma 8900/3Osteosarcoma 9180/3Leiomyoma 8890/0Leiomyosarcoma 8890/3
Fibroepithelial tumoursFibroadenoma 9010/0Phyllodes tumour 9020/1
Benign 9020/0Borderline 9020/1Malignant 9020/3
Periductal stromal sarcoma, low grade 9 0 2 0 / 3Mammary hamartoma
Tumours of the nippleNipple adenoma 8506/0Syringomatous adenoma 8407/0Paget disease of the nipple 8540/3
Malignant lymphomaDiffuse large B-cell lymphoma 9680/3Burkitt lymphoma 9687/3Extranodal marginal-zone B-cell lymphoma of MALT type 9699/3Follicular lymphoma 9690/3
Metastatic tumours
Tumours of the male breastGynaecomastiaCarcinoma
Invasive 8500/3In situ 8500/2
11
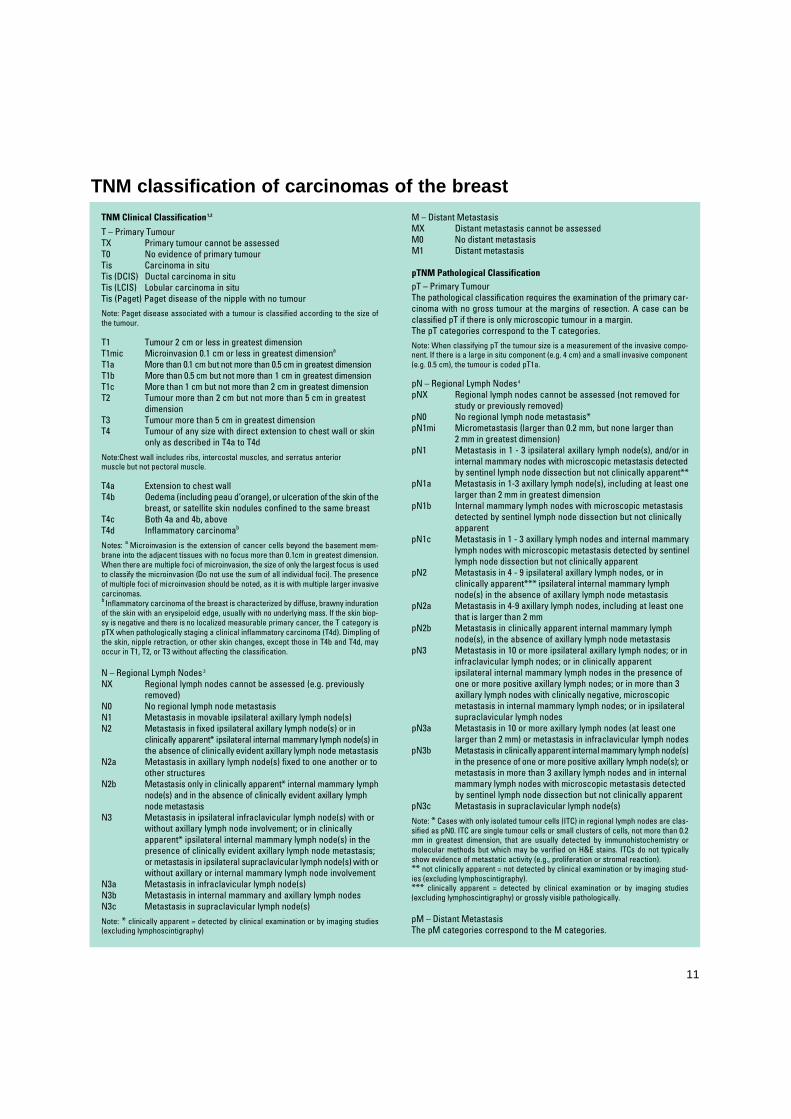
TNM Clinical Classification 1,2
T – Primary TumourTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis Carcinoma in situTis (DCIS) Ductal carcinoma in situTis (LCIS) Lobular carcinoma in situTis (Paget) Paget disease of the nipple with no tumour
Note: Paget disease associated with a tumour is classified according to the size ofthe tumour.
T 1 Tumour 2 cm or less in greatest dimensionT 1 m i c Microinvasion 0.1 cm or less in greatest dimensiona
T 1 a More than 0.1 cm but not more than 0.5 cm in greatest dimensionT 1 b More than 0.5 cm but not more than 1 cm in greatest dimensionT 1 c More than 1 cm but not more than 2 cm in greatest dimensionT 2 Tumour more than 2 cm but not more than 5 cm in greatest
dimensionT 3 Tumour more than 5 cm in greatest dimensionT4 Tumour of any size with direct extension to chest wall or skin
only as described in T4a to T4d
Note:Chest wall includes ribs, intercostal muscles, and serratus anteriormuscle but not pectoral muscle.
T4a Extension to chest wallT4b Oedema (including peau d’orange), or ulceration of the skin of the
breast, or satellite skin nodules confined to the same breastT4c Both 4a and 4b, aboveT4d Inflammatory carcinomab
Notes: a Microinvasion is the extension of cancer cells beyond the basement mem-brane into the adjacent tissues with no focus more than 0.1cm in greatest dimension.When there are multiple foci of microinvasion, the size of only the largest focus is usedto classify the microinvasion (Do not use the sum of all individual foci). The presenceof multiple foci of microinvasion should be noted, as it is with multiple larger invasivec a r c i n o m a s .b Inflammatory carcinoma of the breast is characterized by diffuse, brawny indurationof the skin with an erysipeloid edge, usually with no underlying mass. If the skin biop-sy is negative and there is no localized measurable primary cancer, the T category ispTX when pathologically staging a clinical inflammatory carcinoma (T4d). Dimpling ofthe skin, nipple retraction, or other skin changes, except those in T4b and T4d, mayoccur in T1, T2, or T3 without affecting the classification.
N – Regional Lymph Nodes 3
N X Regional lymph nodes cannot be assessed (e.g. previouslyremoved)
N0 No regional lymph node metastasisN1 Metastasis in movable ipsilateral axillary lymph node(s)N 2 Metastasis in fixed ipsilateral axillary lymph node(s) or in
clinically apparent* ipsilateral internal mammary lymph node(s) inthe absence of clinically evident axillary lymph node metastasis
N2a Metastasis in axillary lymph node(s) fixed to one another or toother structures
N 2 b Metastasis only in clinically apparent* internal mammary lymphnode(s) and in the absence of clinically evident axillary lymphnode metastasis
N3 Metastasis in ipsilateral infraclavicular lymph node(s) with or without axillary lymph node involvement; or in clinicallyapparent* ipsilateral internal mammary lymph node(s) in thepresence of clinically evident axillary lymph node metastasis;or metastasis in ipsilateral supraclavicular lymph node(s) with orwithout axillary or internal mammary lymph node involvement
N3a Metastasis in infraclavicular lymph node(s) N3b Metastasis in internal mammary and axillary lymph nodesN3c Metastasis in supraclavicular lymph node(s)
Note: * clinically apparent = detected by clinical examination or by imaging studies(excluding lymphoscintigraphy)
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
pTNM Pathological ClassificationpT – Primary TumourThe pathological classification requires the examination of the primary car-cinoma with no gross tumour at the margins of resection. A case can beclassified pT if there is only microscopic tumour in a margin.The pT categories correspond to the T categories.
Note: When classifying pT the tumour size is a measurement of the invasive compo-nent. If there is a large in situ component (e.g. 4 cm) and a small invasive component(e.g. 0.5 cm), the tumour is coded pT1a.
pN – Regional Lymph Nodes 4
pNX Regional lymph nodes cannot be assessed (not removed forstudy or previously removed)
pN0 No regional lymph node metastasis*pN1mi Micrometastasis (larger than 0.2 mm, but none larger than
2 mm in greatest dimension)pN1 Metastasis in 1 - 3 ipsilateral axillary lymph node(s), and/or in
internal mammary nodes with microscopic metastasis detectedby sentinel lymph node dissection but not clinically apparent**
pN1a Metastasis in 1-3 axillary lymph node(s), including at least onelarger than 2 mm in greatest dimension
pN1b Internal mammary lymph nodes with microscopic metastasis detected by sentinel lymph node dissection but not clinically apparent
pN1c Metastasis in 1 - 3 axillary lymph nodes and internal mammarylymph nodes with microscopic metastasis detected by sentinellymph node dissection but not clinically apparent
pN2 Metastasis in 4 - 9 ipsilateral axillary lymph nodes, or in clinically apparent*** ipsilateral internal mammary lymphnode(s) in the absence of axillary lymph node metastasis
pN2a Metastasis in 4-9 axillary lymph nodes, including at least onethat is larger than 2 mm
pN2b Metastasis in clinically apparent internal mammary lymph node(s), in the absence of axillary lymph node metastasis
pN3 Metastasis in 10 or more ipsilateral axillary lymph nodes; or ininfraclavicular lymph nodes; or in clinically apparent ipsilateral internal mammary lymph nodes in the presence ofone or more positive axillary lymph nodes; or in more than 3axillary lymph nodes with clinically negative, microscopicmetastasis in internal mammary lymph nodes; or in ipsilateralsupraclavicular lymph nodes
pN3a Metastasis in 10 or more axillary lymph nodes (at least onelarger than 2 mm) or metastasis in infraclavicular lymph nodes
pN3b Metastasis in clinically apparent internal mammary lymph node(s)in the presence of one or more positive axillary lymph node(s); ormetastasis in more than 3 axillary lymph nodes and in internalmammary lymph nodes with microscopic metastasis detectedby sentinel lymph node dissection but not clinically apparent
pN3c Metastasis in supraclavicular lymph node(s)
Note: * Cases with only isolated tumour cells (ITC) in regional lymph nodes are clas-sified as pN0. ITC are single tumour cells or small clusters of cells, not more than 0.2mm in greatest dimension, that are usually detected by immunohistochemistry ormolecular methods but which may be verified on H&E stains. ITCs do not typicallyshow evidence of metastatic activity (e.g., proliferation or stromal reaction). ** not clinically apparent = not detected by clinical examination or by imaging stud-ies (excluding lymphoscintigraphy).*** clinically apparent = detected by clinical examination or by imaging studies(excluding lymphoscintigraphy) or grossly visible pathologically.
pM – Distant Metastasis The pM categories correspond to the M categories.
TNM classification of carcinomas of the breast
12 Tumours of the breast
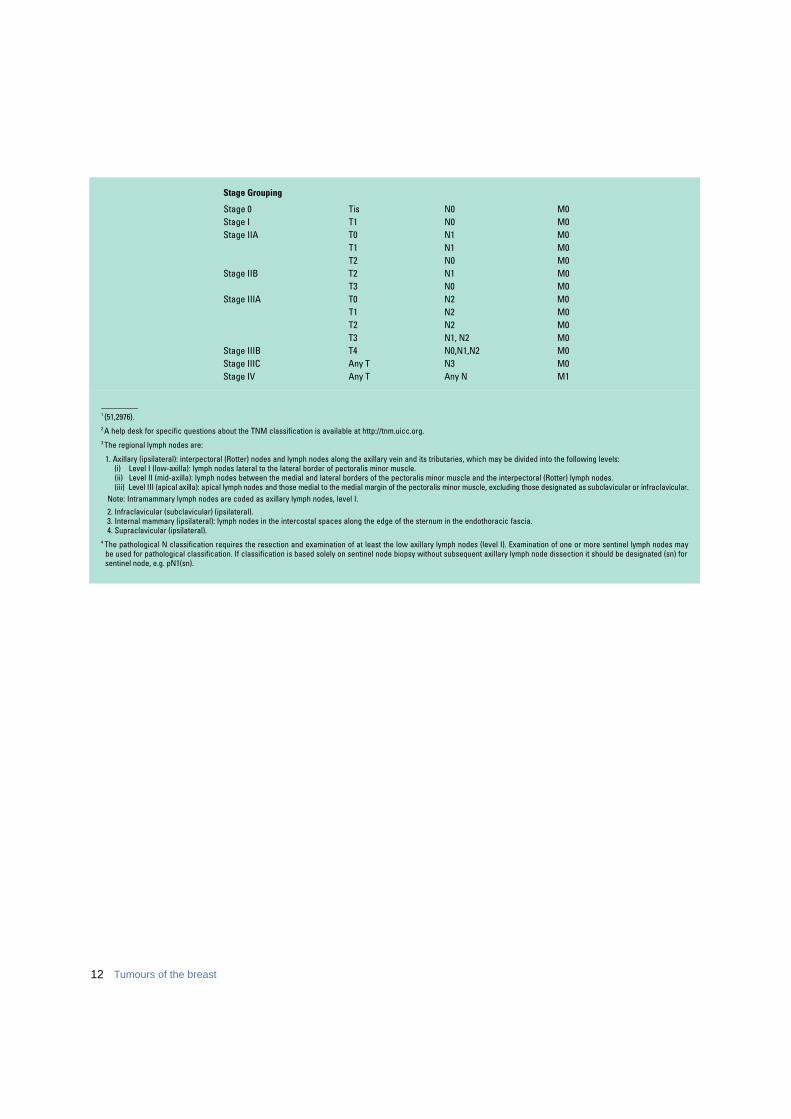
Stage Grouping
Stage 0 Tis N0 M0Stage I T1 N0 M0Stage IIA T0 N1 M0
T1 N1 M0T2 N0 M0
Stage IIB T2 N1 M0T3 N0 M0
Stage IIIA T0 N2 M0T1 N2 M0T2 N2 M0T3 N1, N2 M0
Stage IIIB T4 N0,N1,N2 M0Stage IIIC Any T N3 M0Stage IV Any T Any N M1
_________1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The regional lymph nodes are:
1. Axillary (ipsilateral): interpectoral (Rotter) nodes and lymph nodes along the axillary vein and its tributaries, which may be divided into the following levels:(i) Level I (low-axilla): lymph nodes lateral to the lateral border of pectoralis minor muscle.(ii) Level II (mid-axilla): lymph nodes between the medial and lateral borders of the pectoralis minor muscle and the interpectoral (Rotter) lymph nodes.(iii) Level III (apical axilla): apical lymph nodes and those medial to the medial margin of the pectoralis minor muscle, excluding those designated as subclavicular or infraclavicular.
Note: Intramammary lymph nodes are coded as axillary lymph nodes, level I.
2. Infraclavicular (subclavicular) (ipsilateral).3. Internal mammary (ipsilateral): lymph nodes in the intercostal spaces along the edge of the sternum in the endothoracic fascia.4. Supraclavicular (ipsilateral).
4 The pathological N classification requires the resection and examination of at least the low axillary lymph nodes (level I). Examination of one or more sentinel lymph nodes may be used for pathological classification. If classification is based solely on sentinel node biopsy without subsequent axillary lymph node dissection it should be designated (sn) for sentinel node, e.g. pN1(sn).

13Invasive breast cancer
Invasive breast carcinoma
DefinitionInvasive breast carcinoma is a group ofmalignant epithelial tumours character-ized by invasion of adjacent tissues anda marked tendency to metastasize to dis-tant sites. The vast majority of these tu-mours are adenocarcinomas and are be-lieved to be derived from the mammaryp a renchymal epithelium, particularly cellsof the terminal duct lobular unit (TDLU).B reast carcinomas exhibit a wide rangeof morphological phenotypes and specif-ic histopathological types have part i c u l a rp rognostic or clinical characteristics.
EpidemiologyInvasive breast cancer is the most com-mon carcinoma in women. It accounts for22% of all female cancers, 26% in afflu-ent countries, which is more than twicethe occurrence of cancer in women atany other site {2188}. The areas of highrisk are the affluent populations of NorthAmerica, Europe and Australia where 6%of women develop invasive breast can-cer before age 75. The risk of breast can-cer is low in the less developed regionsof sub-Saharan Africa and Southern andEastern Asia, including Japan, where theprobability of developing breast cancerby age 75 is one third that of rich coun-tries. Rates are intermediate elsewhere.Japan is the only rich country that in year2000 still showed low incidence rates.The prognosis of the disease is verygood if detected at an early stage.Significant improvements in survival havebeen re c o rded in western countriessince the late 1970s {37,485}, butadvancements have been dramatic inthe 1990s due to the combined effect ofpopulation screening and adjuvant hor-monal treatment. As a result, the increas-ing mortality trend observed until the1980s leveled off or declined in severalhigh risk countries e.g. the United Statesof America (USA), the United Kingdomand the Netherlands {3155}.
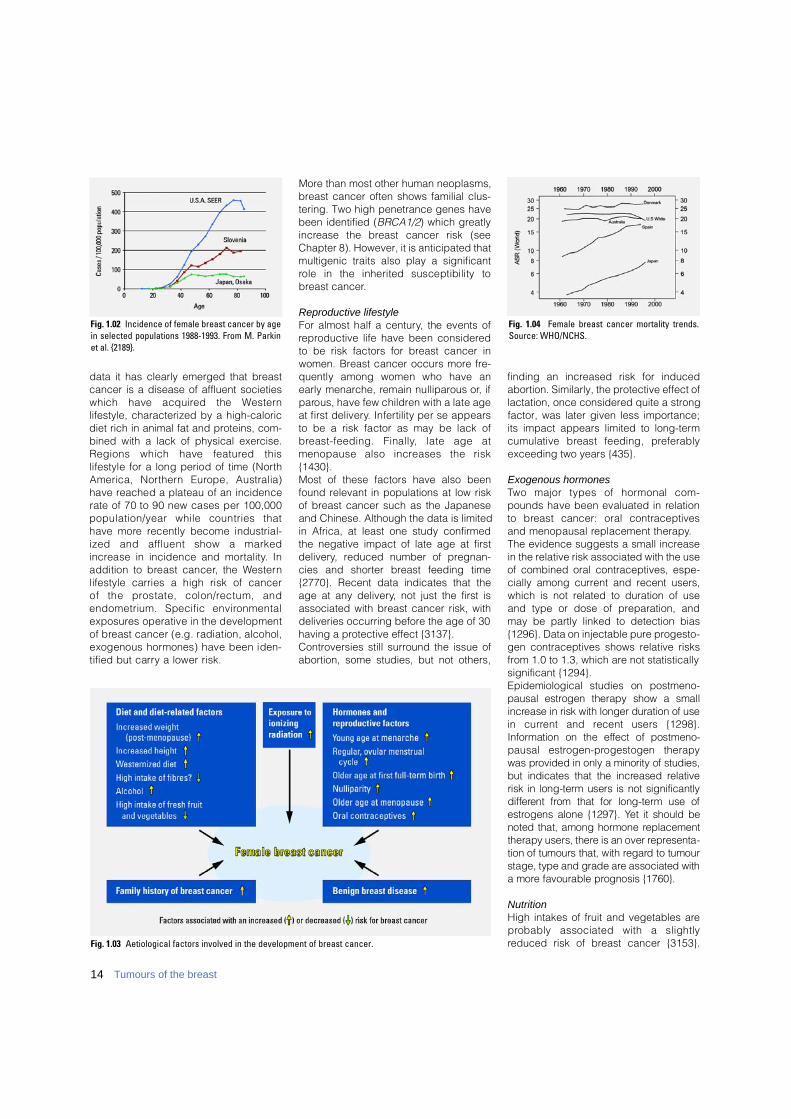
The risk of the disease had been increas-ing until the early 1980s in both devel-oped and developing countries and con-tinues to increase in particular in thedeveloping countries {3068}. Thereafter,in developed countries, the advent ofmammography and the previously men-tioned improvements in survival alteredboth incidence and mortality; the latterno longer appropriately reflect trends inthe underlying risk of the disease.Breast cancer incidence, as with mostepithelial tumours, increases rapidly withage. Figure 1.02 shows age-specific inci-dence rates for three selected popula-tions re p resenting countries with low(Japan), intermediate (Slovenia) andhigh incidence rates (USA), just beforescreening was implemented. The curvesshow a characteristic shape, risingsteeply up to menopausal age and lessrapidly or not at all afterwards. The differ-ent behaviour at older ages is due to acohort effect in the populations of Japan
and Slovenia experiencing an increase inrisk that affects mainly younger genera-tions. If current trends persist, these gen-erations will maintain their higher risk andthe age-specific curve will approach thatof Americans. Around 1990, breast cancer incidencevaried 10-fold world wide, indicatingimportant differences in the distributionof the underlying causes {2189}.Geographical variations, time tre n d s ,and studies of populations migratingfrom low to high risk areas which showthat migrant populations approach therisk of the host country in one or two gen-erations {174,1478,3266}, clearly sug-gest an important role of environmentalfactors in the aetiology of the disease.
AetiologyThe aetiology of breast cancer is multi-factorial and involves diet, reproductivefactors, and related hormonal imbal-ances. From descriptive epidemiological
Fig. 1.01 Global incidence rates of breast cancer. Age-standardized rates (ASR) per 100,000 population andyear. From Globocan 2000 {846}.
I.O. Ellis C.J. CornelisseS.J. Schnitt A.J. SascoX. Sastre-Garau R. KaaksG. Bussolati P. Pisani F.A. Tavassoli D.E. GoldgarV. Eusebi P. DevileeJ.L. Peterse M.J. Cleton-JansenK. Mukai A.L. Børresen-DaleL. Tabár L. van’t VeerJ. Jacquemier A. Sapino
14 Tumours of the breast
data it has clearly emerged that breastcancer is a disease of affluent societieswhich have acquired the We s t e rnlifestyle, characterized by a high-caloricdiet rich in animal fat and proteins, com-bined with a lack of physical exercise.Regions which have featured thislifestyle for a long period of time (Nort hAmerica, Nort h e rn Europe, Australia)have reached a plateau of an incidencerate of 70 to 90 new cases per 100,000population/year while countries thathave more recently become industrial-ized and affluent show a markedi n c rease in incidence and mort a l i t y. Inaddition to breast cancer, the We s t e rnlifestyle carries a high risk of cancer of the prostate, colon/rectum, andendometrium. Specific enviro n m e n t a le x p o s u res operative in the developmentof breast cancer (e.g. radiation, alcohol,exogenous hormones) have been iden-tified but carry a lower risk.
More than most other human neoplasms,breast cancer often shows familial clus-tering. Two high penetrance genes havebeen identified (BRCA1/2) which greatlyi n c rease the breast cancer risk (seeChapter 8). However, it is anticipated thatmultigenic traits also play a significantrole in the inherited susceptibility tobreast cancer.
Reproductive lifestyleFor almost half a century, the events ofre p roductive life have been considere dto be risk factors for breast cancer inwomen. Breast cancer occurs more fre-quently among women who have anearly menarche, remain nulliparous or, ifp a rous, have few children with a late ageat first delivery. Infertility per se appearsto be a risk factor as may be lack ofb reast-feeding. Finally, late age atmenopause also increases the risk{ 1 4 3 0 } .Most of these factors have also beenfound relevant in populations at low riskof breast cancer such as the Japaneseand Chinese. Although the data is limitedin Africa, at least one study confirmedthe negative impact of late age at firstdelivery, reduced number of pregnan-cies and shorter breast feeding time{2770}. Recent data indicates that theage at any delivery, not just the first isassociated with breast cancer risk, withdeliveries occurring before the age of 30having a protective effect {3137}.Controversies still surround the issue ofabortion, some studies, but not others,
finding an increased risk for inducedabortion. Similarly, the protective effect oflactation, once considered quite a strongfactor, was later given less importance;its impact appears limited to long-termcumulative breast feeding, pre f e r a b l yexceeding two years {435}.
Exogenous hormonesTwo major types of hormonal com-pounds have been evaluated in re l a t i o nto breast cancer: oral contraceptivesand menopausal replacement therapy.The evidence suggests a small increasein the relative risk associated with the useof combined oral contraceptives, espe-cially among current and recent users,which is not related to duration of useand type or dose of preparation, andmay be partly linked to detection bias{1296}. Data on injectable pure progesto-gen contraceptives shows relative risksfrom 1.0 to 1.3, which are not statisticallysignificant {1294}.Epidemiological studies on postmeno-p a u s a l e s t rogen therapy show a smalli n c rease in risk with longer duration of usein current and recent users {1298}.I n f o rmation on the effect of postmeno-pausal estro g e n - p rogestogen therapywas provided in only a minority of studies,but indicates that the increased re l a t i v erisk in long-term users is not significantlyd i ff e rent from that for long-term use ofe s t rogens alone {1297}. Yet it should benoted that, among hormone re p l a c e m e n ttherapy users, there is an over re p re s e n t a-tion of tumours that, with re g a rd to tumourstage, type and grade are associated witha more favourable prognosis {1760}.
NutritionHigh intakes of fruit and vegetables arep robably associated with a slightlyreduced risk of breast cancer {3153}.Fig. 1.03 Aetiological factors involved in the development of breast cancer.
Fig. 1.02 Incidence of female breast cancer by agein selected populations 1988-1993. From M. Parkinet al. {2189}.
Fig. 1.04 Female breast cancer mortality trends.Source: WHO/NCHS.
15Invasive breast cancer
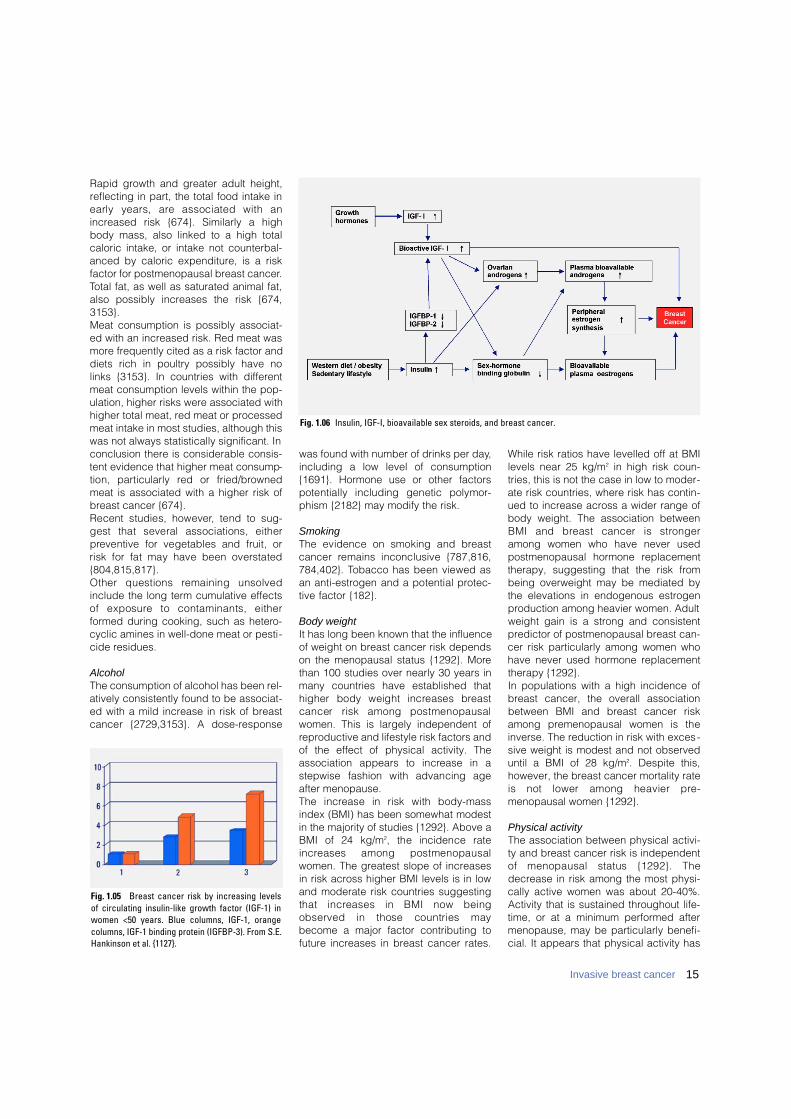
Rapid growth and greater adult height,reflecting in part, the total food intake inearly years, are associated with anincreased risk {674}. Similarly a highbody mass, also linked to a high totalcaloric intake, or intake not counterbal-anced by caloric expenditure, is a riskfactor for postmenopausal breast cancer.Total fat, as well as saturated animal fat,also possibly increases the risk {674,3153}.Meat consumption is possibly associat-ed with an increased risk. Red meat wasmore frequently cited as a risk factor anddiets rich in poultry possibly have nolinks {3153}. In countries with differentmeat consumption levels within the pop-ulation, higher risks were associated withhigher total meat, red meat or processedmeat intake in most studies, although thiswas not always statistically significant. Inconclusion there is considerable consis-tent evidence that higher meat consump-tion, particularly red or fried/bro w n e dmeat is associated with a higher risk ofbreast cancer {674}.Recent studies, however, tend to sug-gest that several associations, eitherp reventive for vegetables and fruit, orrisk for fat may have been overstated{ 8 0 4 , 8 1 5 , 8 1 7 } .Other questions remaining unsolvedinclude the long term cumulative effectsof exposure to contaminants, eitherformed during cooking, such as hetero-cyclic amines in well-done meat or pesti-cide residues.
AlcoholThe consumption of alcohol has been rel-atively consistently found to be associat-ed with a mild increase in risk of breastcancer {2729,3153}. A dose-re s p o n s e
was found with number of drinks per day,including a low level of consumption{1691}. Hormone use or other factorspotentially including genetic polymor-phism {2182} may modify the risk.
SmokingThe evidence on smoking and bre a s tcancer remains inconclusive {787,816,784,402}. Tobacco has been viewed asan anti-estrogen and a potential pro t e c-tive factor {182}.
Body weightIt has long been known that the influenceof weight on breast cancer risk dependson the menopausal status {1292}. Morethan 100 studies over nearly 30 years inmany countries have established thathigher body weight increases bre a s tcancer risk among postmenopausalwomen. This is largely independent ofreproductive and lifestyle risk factors andof the effect of physical activity. Theassociation appears to increase in astepwise fashion with advancing ageafter menopause.The increase in risk with body-massindex (BMI) has been somewhat modestin the majority of studies {1292}. Above aBMI of 24 kg/m2, the incidence ratei n c reases among postmenopausalwomen. The greatest slope of increasesin risk across higher BMI levels is in lowand moderate risk countries suggestingthat increases in BMI now beingobserved in those countries maybecome a major factor contributing tofuture increases in breast cancer rates.
While risk ratios have levelled off at BMIlevels near 25 kg/m2 in high risk coun-tries, this is not the case in low to moder-ate risk countries, where risk has contin-ued to increase across a wider range ofbody weight. The association betweenBMI and breast cancer is stro n g e ramong women who have never usedpostmenopausal hormone replacementtherapy, suggesting that the risk frombeing overweight may be mediated bythe elevations in endogenous estrogenproduction among heavier women. Adultweight gain is a strong and consistentpredictor of postmenopausal breast can-cer risk particularly among women whohave never used hormone replacementtherapy {1292}.In populations with a high incidence ofbreast cancer, the overall associationbetween BMI and breast cancer riskamong premenopausal women is theinverse. The reduction in risk with exces-sive weight is modest and not observeduntil a BMI of 28 kg/m2. Despite this,however, the breast cancer mortality rateis not lower among heavier pre-menopausal women {1292}.
Physical activityThe association between physical activi-ty and breast cancer risk is independentof menopausal status {1292}. Thedecrease in risk among the most physi-cally active women was about 20-40%.Activity that is sustained throughout life-time, or at a minimum performed aftermenopause, may be particularly benefi-cial. It appears that physical activity has
Fig. 1.06 Insulin, IGF-I, bioavailable sex steroids, and breast cancer.
Fig. 1.05 Breast cancer risk by increasing levels of circulating insulin-like growth factor (IGF-1) inwomen <50 years. Blue columns, IGF-1, orangecolumns, IGF-1 binding protein (IGFBP-3). From S.E.Hankinson et al. {1127}.
16 Tumours of the breast
similar effects within different popula-tions. Although lifetime physical activityis desirable, beginning re c re a t i o n a lphysical activity after the menopausecan probably be beneficial for bothweight control and breast cancer riskreduction {1292}.
Endogenous hormonesThere is overwhelming evidence fromepidemiological studies that sex steroids( a n d rogens, estrogens, pro g e s t o g e n s )have an important role in the develop-ment of breast tumours. Breast cancerincidence rates rise more steeply withage before menopause than after, whenovarian synthesis of estrogens and prog-esterone ceases and ovarian androgenproduction gradually diminishes {1447}. The estrogen excess hypothesis is cen-tral, stipulating that breast cancer riskdepends directly on breast tissue expo-s u re to estrogens. In vitro studies showi n c reased breast cell proliferation andinhibition of apoptosis. Animal studiesshow increased rates of tumour develop-ment when estrogens are administere d .The risk is higher among postmenopausalwomen who have elevated plasma levelsof testosterone and andro s t e n e d i o n e ,reduced levels of sex horm o n e - b i n d i n gglobulin (SHBG), and increased levels ofo e s t rone, oestradiol, and bioavailableoestradiol not bound to SHBG.A second major theory, the estro g e nplus progestogen hypothesis {255,1446}, postulates that, compared toe x p o s u re to estrogens alone (as in post-menopausal women not using exoge-nous hormones), risk of breast cancer isf u rther increased in women who haveelevated plasma and tissue levels ofe s t rogens in combination with pro g e s t o-gens. This theory is supported by obser-vations that proliferation of mammaryepithelial cells is increased during theluteal phase of the menstrual cycle,c o m p a red to the follicular phase. Among premenopausal women, severalstudies have not shown any clear asso-ciation between breast cancer risk andc i rculating levels of androgens, estro-gens, or pro g e s t e rone {255,1183,2448,2 6 1 3 , 2 9 0 9 } .A metabolic consequence of excessbody weight and lack of physical activityis development of insulin re s i s t a n c e .Elevated insulin levels, may lead toincreased ovarian and/or adrenal synthe-sis of sex steroids, particularly of andro-
gens, and decrease the hepatic synthe-sis and circulating levels of SHBG{1376}. Especially in postmenopausalwomen, elevated plasma andro g e n slead to increased estrogen formation inadipose tissue, and hence to increasedlevels of oestrone and oestradiol. Thehypothesis that chronic hyperinsulinemiamight explain the observed associationsof breast cancer risk with low plasmaSHBG and elevated androgens ande s t rogens, among postmenopausalwomen {1376} has, however, receivedonly limited support {661,1377}. Insulin-growth factor-I (IGF-I) and IGF-bindingproteins (IGFBP) appear to be significantrisk predictors {1127,1377}. F u t u re adult cancer risk is in part set byconditions of exposure in utero. The pre-ventive effect of gravidic toxaemia is re c-ognized {1288} and since the 1950s stud-ies have incriminated high birth weight asa risk factor for cancer, in particular of theb reast {1857}. Similarly, among twins, therisk of breast cancer may be affected bythe type of twinning (dizygotic versusmonozygotic) and sex of the dizygotictwin {429}. A study of maternal pre g n a n-cy hormone levels in China and theUnited States of America (USA) did notfind, however, the expected higher levelsin the USA but rather the reverse {1676}.Another important period is adolescence,w h e re diet may play a role either dire c t l yor possibly indirectly through a modifica-tion of growth velocity {242}.
Some specific exposuresOnly limited data is available on specificexposures in relation to breast cancer.Long-term follow-up of women exposedto the Hiroshima or Nagasaki nuclearexplosions indicates an increased risk ofbreast cancer, in particular for womenexposed around puberty {2938}.Similarly, exposure as a result of treat-ment and surveillance of tuberculosis isassociated with risk {304}. Yet there is lit-tle evidence for a different pattern of riskas a function of fractionated versus onetime only irradiation {1678}. Systematicreviews on occupation and breast can-cer are few, indicating an increased riskfor selected occupations and specificchemical and physical exposures. Thisdata contrasts with the long-held viewthat risk of breast cancer is related tosocial class, with higher risk for execu-
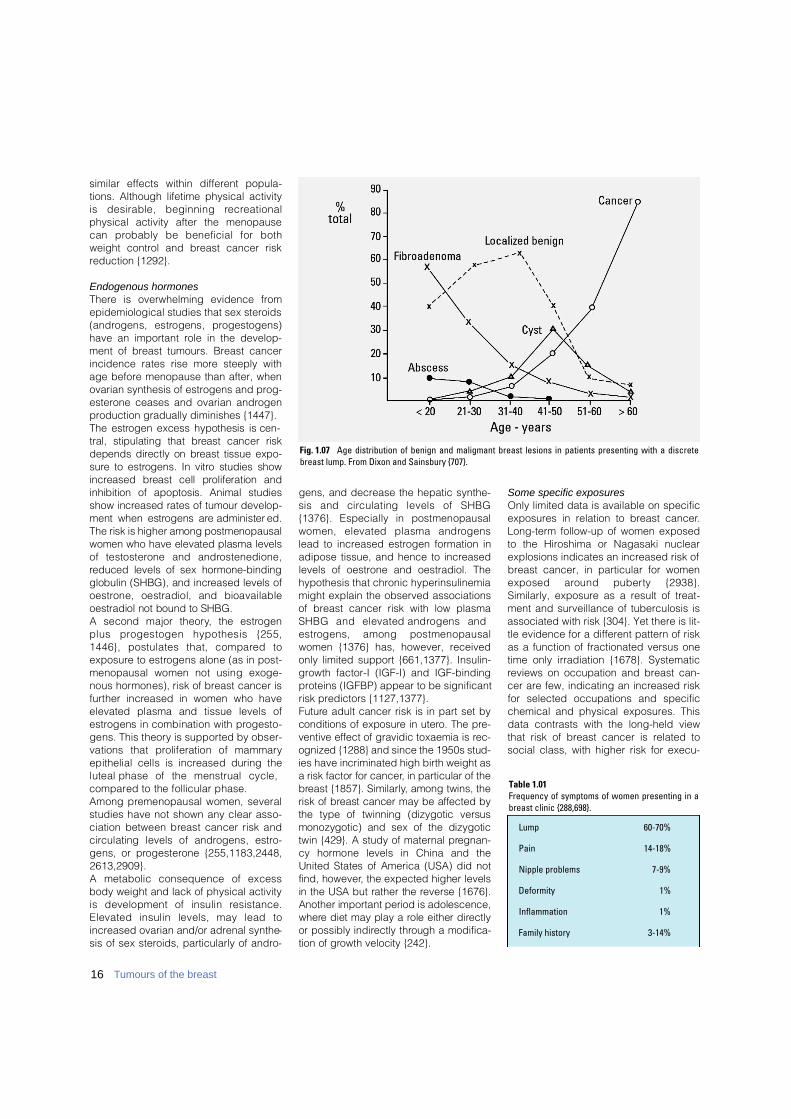
Fig. 1.07 Age distribution of benign and maligmant breast lesions in patients presenting with a discretebreast lump. From Dixon and Sainsbury {707}.
Lump 60-70%
Pain 14-18%
Nipple problems 7-9%
Deformity 1%
Inflammation 1%
Family history 3-14%
Table 1.01Frequency of symptoms of women presenting in abreast clinic {288,698}.
tives, administrative and clerical jobs{387}. A recent hypothesis deals with cir-cadian disruption through night work,with an increased risk in women workingpredominantly at night {632,2556}.Over the last ten years concerns havearisen as to the potential risks of exposureto, not only hormones, but to art i f i c i a lp roducts mimicking hormonal activities.This led to the concept of xeno-hor-mones, mostly re p resented so far byx e n o - e s t rogens. The exact role they playis unknown. Most epidemiological studiesdeal with various pesticides, essentiallyorganochlorines which remain in the envi-ronment for a very long time and theresidues of which may be found in adi-pose tissue of various species, includinghumans {628}. Studies have pro d u c e dconflicting results with some suggesting apossibly increased risk, some no risk andothers showing a negative effect. For thetime being, many consider these links asspeculative and unfounded {1951,2503}or as markers of susceptibility {1951}.Finally, based on animal experience, aviral hypothesis has been put forward. Inmice, a retrovirus, the murine mammary
tumour virus, is a recognized cause ofmammary tumours, transmitted with milkfrom mothers to daughters. Another can-didate is the Epstein-Barr virus, althoughdata from the USA are not particularlysupportive {1015}. Other potential viralcandidates remain to be searched for.
LocalizationBreast carcinoma arises from the mam-mary epithelium and most frequently theepithelial cells of the TDLU. There is aslightly higher frequency of invasivebreast cancer in the left breast with areported left to right ratio of approximate-ly 1.07 to 1 {1096}. Between 40 and 50%of tumours occur in the upper outerquadrant of the breast and there is adecreasing order of frequency in theother quadrants from the central, upperinner, lower outer to the lower inner quad-rant {1096}.
Clinical featuresSymptoms and signsThe majority of women with breast can-cer present symptomatically, althoughthe introduction of breast screening hasled to an increasing proportion of asym-tomatic cases being detected mammo-graphically. Breast cancer does not havespecific signs and symptoms, whichallow reliable distinction from variousf o rms of benign breast disease.However, the frequency distribution of
benign and malignant disease does dif-fer between age cohorts, benign condi-tions being more common in youngerwomen and breast cancer the common-est cause of symptoms in older women.The most common findings in sympto-matic women are breast lumps, which mayor may not be associated with pain. Nipplea b n o rmalities (discharge, retraction, dis-t o rtion or eczema) are less common andother forms of presentation are rare .Some symptoms have a higher risk ofunderlying malignancy for which hospitalreferral is recommended.Breast abnormalities should be evaluat-ed by triple assessment including clinicalexamination, imaging (mammographyand ultrasound) and tissue sampling byeither fine needle aspiration cytology orneedle core biopsy.Clinical examination should be systema-tic and take account of the nature of thelump and, if present, any skin dimpling orchange in contour of the breast and alsoassessment of the axilla.
ImagingImaging should include mammographyexcept in women under age 35, where itis rarely of value, unless there is strongclinical suspicion or tissue/needle biopsyevidence of malignancy.The mammographic appearances ofbreast carcinoma are varied and includewell defined, ill defined and spiculate
17Invasive breast cancer
B
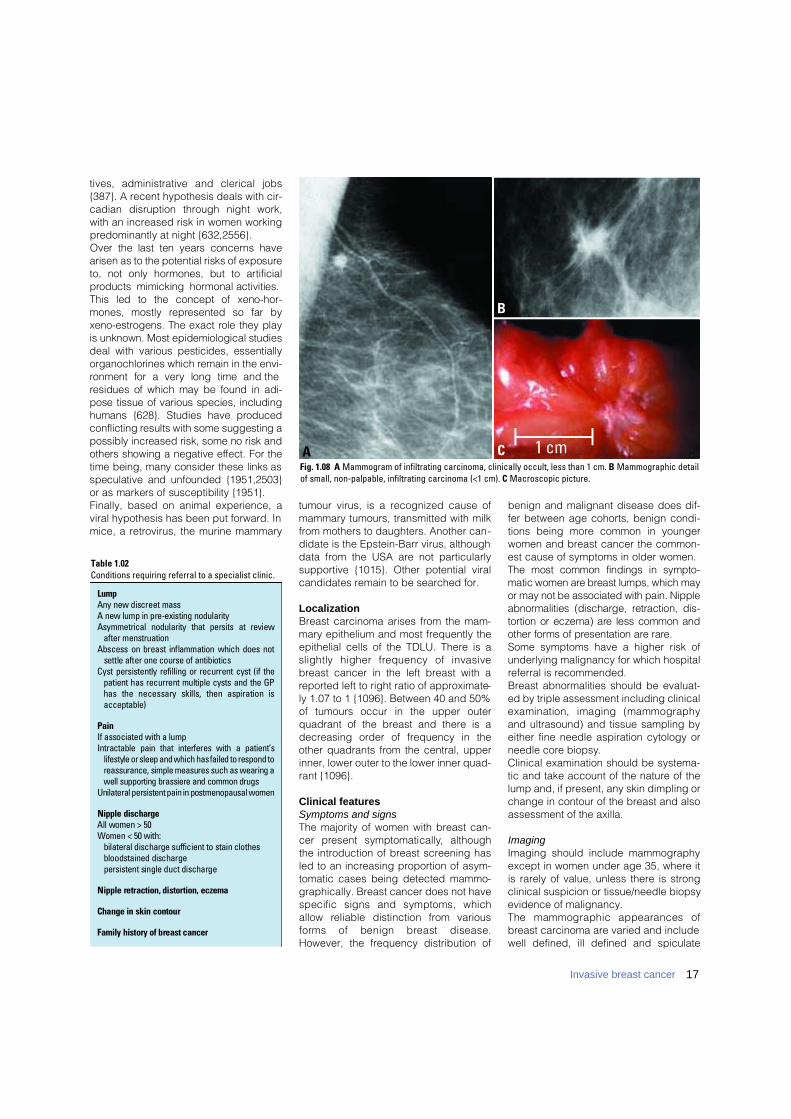
CFig. 1.08 A Mammogram of infiltrating carcinoma, clinically occult, less than 1 cm. B Mammographic detailof small, non-palpable, infiltrating carcinoma (<1 cm). C Macroscopic picture.
A
Table 1.02Conditions requiring referral to a specialist clinic.
L u m pAny new discreet massA new lump in pre-existing nodularityAsymmetrical nodularity that persits at review
after menstruationAbscess on breast inflammation which does not
settle after one course of antibioticsCyst persistently refilling or recurrent cyst (if the
patient has recurrent multiple cysts and the GPhas the necessary skills, then aspiration isa c c e p t a b l e )
P a i nIf associated with a lumpIntractable pain that interferes with a patient’s
lifestyle or sleep and which has failed to respond toreassurance, simple measures such as wearing awell supporting brassiere and common drugs
Unilateral persistent pain in postmenopausal women
Nipple dischargeAll women > 50Women < 50 with:
bilateral discharge sufficient to stain clothesbloodstained dischargepersistent single duct discharge
Nipple retraction, distortion, eczema
Change in skin contour
Family history of breast cancer
masses, parenchymal deformity and cal-cification with or without a mass lesion.By far the most common manifestation ofbreast cancer on the mammogram istumour mass without calcifications. Themammographic histological corre l a t i o nof 1,168 open surgical biopsies at FalunCentral Hospital, Sweden, included 866
histologically proven malignancies. Asseen in Table 1.03, the mammograms ofthese breasts cancer showed:1) Stellate or circular tumour mass withno associated calcifications in 64% of thecases. 2) An additional 17% had both calcifica-tions and tumour mass.3) Only calcifications without associatedtumour mass accounted for less than20% of all malignancies detectable onthe mammogram.
Grading of invasive carcinomaInvasive ductal carcinomas and all otherinvasive tumours are routinely gradedbased on an assessment of tubule/glandf o rmation, nuclear pleomorphism andmitotic counts.Many studies have demonstrated a sig-nificant association between histologicalgrade and survival in invasive breast car-cinoma. It is now recognized as a power-ful prognostic factor and should beincluded as a component of the minimumdata set for histological re p o rting ofbreast cancer {779,1190}. Assessment ofhistological grade has become moreobjective with modifications of the Patley& Scarff {2195} method first by Bloomand Richardson {293} and more recentlyby Elston and Ellis {777,2385}.
Method of gradingT h ree tumour characteristics are evaluat-ed; tubule formation as an expression ofglandular diff e rentiation, nuclear pleomor-
phism and mitotic counts. A numericalscoring system of 1-3 is used to ensurethat each factor is assessed individually. When evaluating tubules and glandularacini only structures exhibiting clear cen-tral lumina are counted; cut off points of75% and 10% of glandular/tumour areaare used to allocate the score. Nuclear pleomorphism is assessed byreference to the regularity of nuclear sizeand shape of normal epithelial cells inadjacent breast tissue. Increasing irregu-larity of nuclear outlines and the numberand size of nucleoli are useful additionalfeatures in allocating scores for pleomor-phism. Evaluation of mitotic figures requires careand observers must count only definedmitotic figures; hyperc h romatic andpyknotic nuclei are ignored since theyare more likely to represent apoptosisthan proliferation. Mitotic counts requirestandardization to a fixed field area or byusing a grid system {1984}. The totalnumber of mitoses per 10 high powerfields. Field selection for mitotic scoringshould be from the peripheral leadingedge of the tumour. If there is hetero-geneity, regions exhibiting a higher fre-quency of mitoses should be chosen.Field selection is by random meanderthrough the chosen area. Only fields witha re p resentative tumour cell burd e nshould be assessed. The three values are added together toproduce scores of 3 to 9, to which thegrade is assigned as follows:
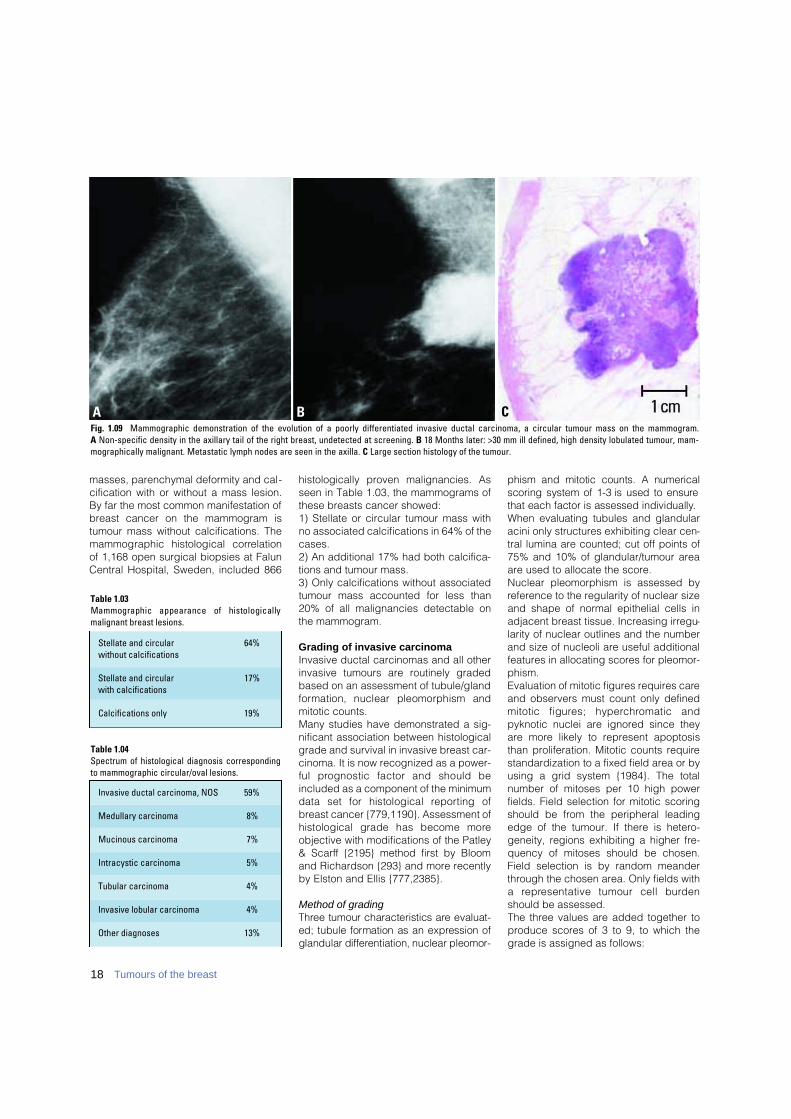
Fig. 1.09 Mammographic demonstration of the evolution of a poorly differentiated invasive ductal carcinoma, a circular tumour mass on the mammogram. A Non-specific density in the axillary tail of the right breast, undetected at screening. B 18 Months later: >30 mm ill defined, high density lobulated tumour, mam-mographically malignant. Metastatic lymph nodes are seen in the axilla. C Large section histology of the tumour.
B CA
Table 1.04Spectrum of histological diagnosis correspondingto mammographic circular/oval lesions.
Invasive ductal carcinoma, NOS 59%
Medullary carcinoma 8%
Mucinous carcinoma 7%
Intracystic carcinoma 5%
Tubular carcinoma 4%
Invasive lobular carcinoma 4%
Other diagnoses 13%
Table 1.03Mammographic appearance of histologicallymalignant breast lesions.
Stellate and circular 64%without calcifications
Stellate and circular 17%with calcifications
Calcifications only 19%
18 Tumours of the breast
Grade 1 - well differentiated: 3-5 pointsGrade 2 - moderately differentiated:
6-7 pointsGrade 3 - poorly differentiated: 8-9 points
Invasive ductal carcinoma, not otherwise specified (NOS)
DefinitionInvasive ductal carcinoma, not otherwisespecified (ductal NOS) comprises thelargest group of invasive breast cancers.It is a heterogeneous group of tumoursthat fail to exhibit sufficient characteris-tics to achieve classification as a specif-ic histological type, such as lobular ortubular carcinoma.
ICD-O code 8500/3
Synonyms and historical annotationInvasive ductal carcinoma, no specifictype (ductal NST); infiltrating ductal car-cinoma.Many names have been used for thisf o rm of breast carcinoma including scirrhous carcinoma, carcinoma sim-plex and spheroidal cell carc i n o m a.Infiltrating ductal carcinoma is used bythe Armed Forces Institute of Pathology{1832,2442} and was the nomenclatureadopted in the previous WHO classifica-
tion {2548,3154}. This perpetuates thetraditional concept that these tumoursare derived exclusively from mammaryductal epithelium in distinction from lobu-lar carcinomas, which were deemed tohave arisen from within lobules for whichthere is no evidence. In addition it hasbeen shown that the terminal duct-lobu-lar unit (TDLU) should be regarded as a
single entity from the point of view of thesite of origin of most breast carcinomas{147,3091}. Some groups {874,2325}have retained the term ductal but addedthe phrase 'not otherwise specified(NOS)', whilst others {2147} prefer to use'no specific type (NST)' to emphasizetheir distinction from specific typetumours. This latter view is increasingly
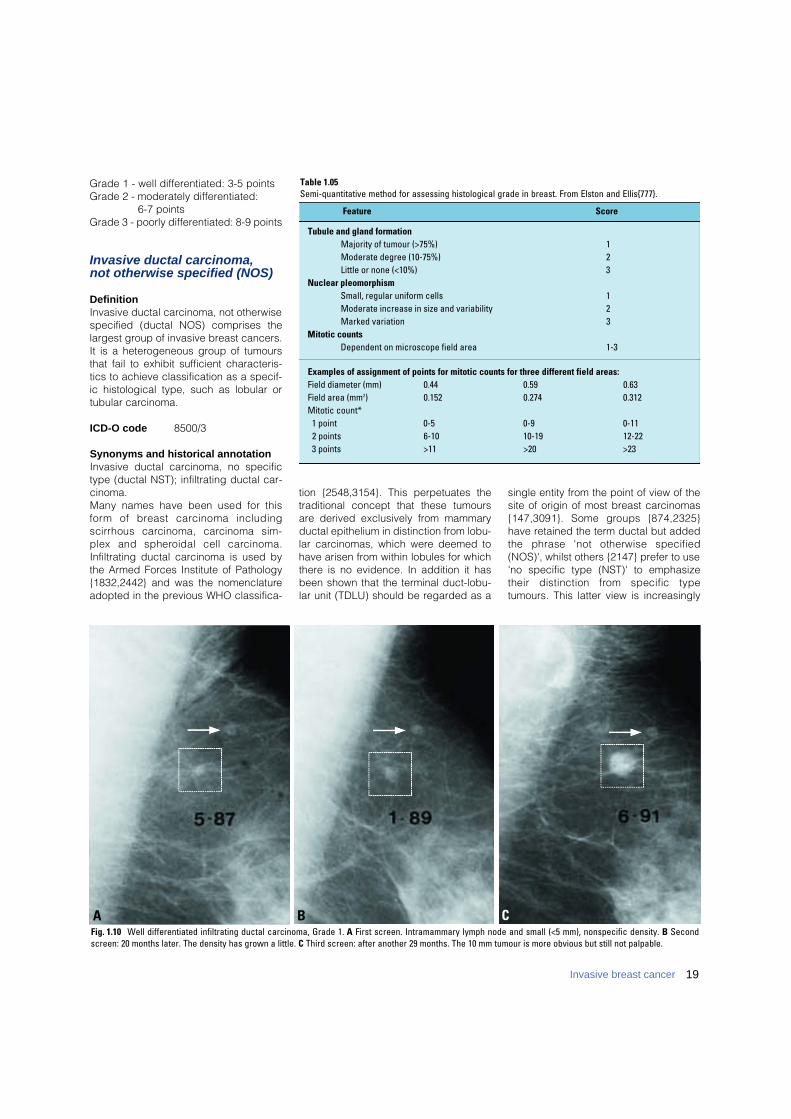
Fig. 1.10 Well differentiated infiltrating ductal carcinoma, Grade 1. A First screen. Intramammary lymph node and small (<5 mm), nonspecific density. B Secondscreen: 20 months later. The density has grown a little. C Third screen: after another 29 months. The 10 mm tumour is more obvious but still not palpable.
B CA
19Invasive breast cancer
Table 1.05Semi-quantitative method for assessing histological grade in breast. From Elston and Ellis{777}.
Tubule and gland formationMajority of tumour (>75%) 1Moderate degree (10-75%) 2Little or none (<10%) 3
Nuclear pleomorphismSmall, regular uniform cells 1Moderate increase in size and variability 2Marked variation 3
Mitotic countsDependent on microscope field area 1-3
Examples of assignment of points for mitotic counts for three different field areas:Field diameter (mm) 0.44 0.59 0.63Field area (mm2) 0.152 0.274 0.312Mitotic count*
1 point 0-5 0-9 0-112 points 6-10 10-19 12-223 points >11 >20 >23
Feature Score

accepted internationally, but since 'duc-tal' is still widely used the terms invasiveductal carcinoma, ductal NOS or NSTare preferred terminology options.
EpidemiologyDuctal NOS carcinoma forms a largeproportion of mammary carcinomas andits epidemiological characteristics aresimilar to those of the group as a whole(see epidemiology). It is the most com-mon 'type' of invasive carcinoma of theb reast comprising between 40% and75% in published series {774}. This widerange is possibly due to the lack ofapplication of strict criteria for inclusionin the special types and also the fact thatsome groups do not recognize tumourswith a combination of ductal NOS andspecial type patterns as a separate
mixed category, preferring to includethem in the no special type (ductal NOS)group.Ductal NOS tumours, like all forms ofbreast cancer, are rare below the age of40 but the proportion of tumours classi-fied as such in young breast cancercases is in general similar to older cases{1493}. There are no well recognized dif-ferences in the frequency of breast can-cer type and proportion of ductal NOScancers related to many of the knownrisk factors including geographical, cul-tural/lifestyle, reproductive variables (seeaetiology). However, carcinomas devel-oping following diagnosis of conditionssuch as atypical ductal hyperplasia andlobular neoplasia, recognized to beassociated with increased risk include ahigher proportion of tumours of specifictype specifically tubular and classicallobular carcinoma {2150}. Familial breastcancer cases associated with BRCA1mutations are commonly of ductal NOStype but have medullary carcinoma likefeatures, exhibiting higher mitotic counts,a greater proportion of the tumour with acontinuous pushing margin, and morelymphocytic infiltration than sporadiccancers {1572}. Cancers associated withBRCA2 mutations are also often of ductalNOS type but exhibit a high score fortubule formation (fewer tubules), a high-er proportion of the tumour perimeterwith a continuous pushing margin and alower mitotic count than sporadic can-cers {1572}.
MacroscopyThese tumours have no specific macro-scopical features. There is a marked vari-ation in size from under 10 mm to over100 mm. They can have an irregular, stel-late outline or nodular configuration. Thetumour edge is usually moderately or illdefined and lacks sharp circumscription.
Classically, ductal NOS carcinomas arefirm or even hard on palpation, and mayhave a curious 'gritty' feel when cut witha knife. The cut surface is usually grey-white with yellow streaks.
HistopathologyThe morphological features vary consid-erably from case to case and there is fre-quently a lack of the regularity of struc-ture associated with the tumours of spe-cific type. Architecturally the tumour cellsmay be arranged in cords, clusters andtrabeculae whilst some tumours arecharacterized by a predominantly solidor syncytial infiltrative pattern with littleassociated stroma. In a proportion ofcases glandular differentiation may beapparent as tubular structures with cen-tral lumina in tumour cell gro u p s .Occasionally, areas with single file infil-tration or targetoid features are seen butthese lack the cytomorphological char-acteristics of invasive lobular carcinoma.The carcinoma cells also have a variableappearance. The cytoplasm is oftenabundant and eosinophilic. Nuclei maybe regular, uniform or highly pleomorphicwith prominent, often multiple, nucleoli,mitotic activity may be virtually absent orextensive. In up to 80% of cases foci ofassociated ductal carcinoma in situ(DCIS) will be present {147,2874}.Associated DCIS is often of high gradecomedo type, but all other patterns maybe seen. Some recognize a subtype of ductalNOS carcinoma, infiltrating ductal carci-noma with extensive in situ component.The stromal component is extremely vari-able. There may be a highly cellularfibroblastic proliferation, a scanty con-nective tissue element or marked hyalini-sation. Foci of elastosis may also bepresent, in a periductal or perivenousdistribution. Focal necrosis may be pres-
Fig. 1.11 Invasive ductal carcinoma, not otherwisespecified. 84 year old patient, mastectomy specimen.
B CAFig. 1.12 A Infiltrating ductal carcinoma, grade I. B Infiltrating ductal carcinoma, grade II. C Invasive ductal NOS carcinoma, grade III with no evidence of glandular dif-ferentiation.Note the presence of numerous cells in mitosis, with some abnormal mitotic figures present.
20 Tumours of the breast

ent and this is occasionally extensive. Ina minority of cases a distinct lympho-plasmacytoid infiltrate can be identified.
Mixed type carcinoma
For a tumour to be typed as ductal NOSit must have a non-specialized pattern inover 50% of its mass as judged by thor-ough examination of representative sec-tions. If the ductal NOS pattern compris-es between 10 and 49% of the tumour,the rest being of a recognized specialtype, then it will fall into one of the mixedgroups: mixed ductal and special type ormixed ductal and lobular carc i n o m a .Apart from these considerations thereare very few lesions that should be con-fused with ductal NOS carcinomas.
Pleomorphic carcinoma
ICD-O code 8022/3
Pleomorphic carcinoma is a rare variantof high grade ductal NOS carc i n o m acharacterized by proliferation of pleo-morphic and bizarre tumour giant cellscomprising >50% of the tumour cells ina background of adenocarcinoma ora d e n o c a rcinoma with spindle andsquamous diff e rentiation {2683}. Thepatients range in age from 28 to 96years with a median of 51. Mostpatients present with a palpable mass;in 12% of cases, metastatic tumour isthe first manifestation of disease. Themean size of the tumours is 5.4 cm.Cavitation and necrosis occur in largert u m o u r s .
The tumour giant cells account for morethan 75% of tumour cells in most cases.Mitotic figures exceed 20 per 10 highpower fields. All these tumours qualify asgrade 3 carcinomas. The intraepithelialcomponent displays a ductal arrange-ment and is often high grade with necro-sis. Lymphovascular invasion is presentin 19% of cases.Generally BCL2, ER and PR negative,two thirds of these pleomorphic carcino-mas are TP53 positive, and one third areS-100 protein positive. All are positive forCAM5.2, EMA and pan-cytokeratin(AE1/AE3, CK1). A majority (68%) is ane-uploid with 47% of them being triploid. A
high S-phase (>10%) is found in 63%.Axillary node metastases are present in50% of the patients with involvement of 3or more nodes in most. Many patientspresent with advanced disease.
Carcinoma with osteoclastic giantcells
ICD-O code 8035/3
The common denominator of all thesec a rcinomas is the presence of osteo-clastic giant cells in the stroma {1089}.The giant cells are generally associatedwith an inflammatory, fibroblastic, hyper-
Fig. 1.13 Mixed infiltrating ductal and infiltrating lobular carcinoma. Two distinct morphologic patterns areseen in this tumour, ductal on the left and lobular on the right.
BAFig. 1.14 Invasive ductal carcinoma: pleomorphic carcinoma. A Poorly differentiated cells without distinctive architecture often lead to misinterpretation of thelesion as a sarcoma. B Immunostain for keratin (AE1/AE3 and LP34) confirms the epithelial nature of the process.
21Invasive breast cancer

22 Tumours of the breast
vascular stroma, with extravasated re dblood cells, lymphocytes, monocytesalong with mononucleated and binucle-ated histiocytes some containinghaemosiderin. The giant cells are vari-able in size and appear to embrace theepithelial component or are found withinlumena formed by the cancer cells. Thegiant cells contain a variable number ofnuclei. The giant cells and hypervascu-lar reactive stroma can be observed inlymph node metastases and in re c u r-rences {2952}.The carcinomatous part of the lesion ismost frequently a well to moderately dif-f e rentiated infiltrating ductal carc i n o m abut all the other histological types havebeen observed particularly invasivec r i b r i f o rm carcinoma {2003,2241}, andalso tubular, mucinous, papillary {3062},lobular {1274,2837}, squamous andother metaplastic patterns {1200,2044,3 0 6 2 } .About one-third of the re p o rted caseshad lymph nodes metastasis. The five
year survival rate is around 70%, similarto, or better than, patients with ord i n a ryinfiltrating carcinomas {3062}. Pro g n o s i sis related to the characteristics of theassociated carcinoma and does notappear to be influenced by the pre s-ence of stromal giant cells.The giant cells show uniform expre s s i o nof CD68 (as demonsrated by KP1 anti-body on paraffin sections) {1200} anda re negative for S100 protein, actin, andnegative for cytokeratin, EMA, estro g e nand pro g e s t e rone receptors {2869}.The giant cells are strongly positive for acid phosphatase, non-specificesterase and lysosyme, but negative for alkaline phosphatase indicative ofmorphological similarity to histiocyticcells and osteoclasts {2423,2869,2952,3 0 2 5 } .A number of ultrastructural and immuno-histochemical studies have confirm e dthe histiocytic nature of the osteoclasticcells present in these unusual carc i n o-mas {2632,2869,2952,3025}. In vitrostudies have recently shown that o s t e o-clasts may form directly from a pre-cursor cell population of monocytes and macrophages. Tumour associatedm a c rophages (TAMs) are capable of dif-f e rentiating into multinucleated cells,which can affect bone resorption inmetastases {2313}. Osteoclastic giantcells in carcinoma are probably alsorelated to TAMs. Angiogenesis andchemotactic agents produced by thec a rcinoma may be responsible for themigration of histiocytes to the are ainvolved by cancer and their ultimatet r a n s f o rmation to osteoclastic giant cells{ 2 6 3 8 , 2 8 6 9 } .
Carcinoma with choriocarcinomatous features
Patients with ductal NOS carcinoma mayhave elevated levels of serum human β −chorionic gonadotrophin (β- H C G ){2649} and as many as 60% of ductalNOS carcinoma have been found to con-tain β-HCG positive cells {1243}.Histological evidence of choriocarcino-matous diff e rentiation, however, isexceptionally rare with only a few casesre p o rted {993,1061,2508}. All were inwomen between 50 and 70 years old.
Carcinoma with melanotic features
A few case re p o rts have describedexceptional tumours of the mammaryparenchyma that appear to representcombinations of ductal carcinoma andmalignant melanoma {2031,2146,2485}and in some of these cases, thereappeared to be a transition from one celltype to the other. A recent genetic analy-sis of one such case showed loss of het-erozygosity at the same chromosomalloci in all the components of the tumour,suggesting an origin from the same neo-plastic clone {2031}.The mere presence of melanin in bre a s tcancer cells should not be construed asevidence of melanocytic diff e re n t i a t i o n ,since melanin pigmentation of carc i n o m acells can occur when breast cancersinvade the skin and involve the derm o -e p i d e rmal junction {150}. In addition,c a re must be taken to distinguish tumoursshowing melanocytic diff e rentiation fro mb reast carcinomas with prominent cyto-plasmic lipofuscin deposition {2663}.
Fig. 1.15 Invasive carcinomas with stromal osteo-clastic giant cells often have vascular stromal tis-sue with haemosiderin pigment accumulation giv-ing them a brown macroscopic appearance.
BAFig. 1.16 A Invasive ductal carcinoma with stromal osteoclastic giant cells and haemosiderin-laden macrophages. B The invasive ductal carcinoma is low grade.Multinucleated giant cells are evident in the stroma.

23Invasive breast cancer
Most melanotic tumours of the breastre p resent metastases from malignantmelanomas originating in extra-mamma-ry sites {2694}. Primary melanomas mayarise anywhere in the skin of the breast,but an origin in the nipple-areola com-plex is extremely rare {2168}. The differ-ential diagnosis of malignant melanomaarising in the nipple areolar region mustinclude Paget disease, the cells of whichmay on occasion contain melanin pig-ment {2544}. This is discussed in thesection on Paget disease.
GeneticsThe genetic variation seen in breast can-cer as a whole is similarly reflected inductal NOS tumours and has until recent-ly proved difficult to analyse or explain.The increasing accumulation of geneticalterations seen with increasing grade( d e c reasing degree of diff e re n t i a t i o n )has been used to support the hypothesisof a linear progression model in this typeand in invasive breast cancer as a whole.The recent observation by a number ofgroups that specific genetic lesion orregions of alteration are associated withhistological type of cancer or related tograde in the large ductal NOS groupdoes not support this view. It implies thatb reast cancer of ductal NOS typeincludes a number of tumours of unrelat-ed genetic evolutionary pathways {365}and that these tumours show fundamen-tal differences when compared to somespecial type tumours including lobular{1085} and tubular carcinoma {2476}.F u rt h e rm o re, recent cDNA micro a r r a yanalysis has demonstrated that ductalNOS tumours can be classified in to sub-types on the basis of expression patterns{2218,2756}.
Prognosis and predictive factorsDuctal NOS carcinoma forms the bulk(50-80%) of breast cancer cases and itsp rognostic characteristics and manage-ment are similar or slightly worse with a35-50% 10 year survival {771} compare dto breast cancer as a whole with aro u n da 55% 10 year survival. Prognosis isinfluenced profoundly by the classicalp rognostic variables of histologicalgrade, tumour size, lymph node statusand vascular invasion (see general dis-cussion of prognosis and predictive fac-tors at the end of this chapter) and byp redictors of therapeutic response suchas estrogen receptor and ERBB2 status.
Approximately 70-80% of ductal NOSbreast cancers are estrogen receptorpositive and between 15 and 30% ofcases ERBB2 positive. The managementof ductal NOS carcinomas is also influ-enced by these prognostic and predic-tive characteristics of the tumour as wellas focality and position in the breast.
Invasive lobular carcinoma
DefinitionAn invasive carcinoma usually associa-ted with lobular carcinoma in situ is com-posed of non-cohesive cells individuallydispersed or arranged in single-file linearpattern in a fibrous stroma.
ICD-O code 8520/3
EpidemiologyInvasive lobular carcinoma (ILC) repre-sents 5-15% of invasive breast tumours{725,771,1780,2541,2935,3133}. Duringthe last 20 years, a steady increase in itsincidence has been reported in womenover 50 {1647}, which might be attributa-ble to the increased use of hormonereplacement therapy {312,1648,2073}.The mean age of patients with ILC is 1-3years older than that of patients with infil-trating ductal carcinoma (IDC) {2541}.
Clinical featuresThe majority of women present with apalpable mass that may involve any partof the breast although centrally locatedtumours were found to be slightly morecommon in patients with ILC than withIDC {3133}. A high rate of multicentrictumours has been reported by some{699,1632} but this has not been found inother series based on clinical {2541} or
radiological {1599} analysis (see bilateralb reast carcinoma section). An 8-19%incidence of contralateral tumours hasalso been reported {699,725,834}, repre-senting an overall rate of 13.3 %. Thismay be higher than that for IDC{1241,2696}. However, no significant dif-ference in the rate of bilaterality wasobserved in other series of cases {648,1168,2186}. At mammography, architec-tural distortion is more commonlyobserved in ILC than in IDC whereasmicrocalcifications are less common inILC {895,1780,3066}.
MacroscopyILC frequently present as irregular andpoorly delimited tumours which can bed i fficult to define macro s c o p i c a l l ybecause of the diffuse growth pattern ofthe cell infiltrate {2696}. The mean diam-eter has been reported to be slightly larg-er than that of IDC in some series{2541,2696,3133}.
HistopathologyThe classical pattern of ILC {895,1780,3066} is characterized by a prolife-ration of small cells, which lack cohesion
Fig. 1.18 Macroscopy of an invasive lobular carci-noma displays an ill defined lesion.
BAFig. 1.17 Carcinoma with choriocarcinomatous features. A,B Multinucleated tumour cells with smudgednuclei extend their irregular, elongated cytoplasmic processes around clusters of monocytic tumour cells,mimicking the biphasic growth pattern of choriocarcinoma. B Note the abnormal mitotic figures in this highgrade carcinoma.
and appear individually dispersedthrough a fibrous connective tissue orarranged in single file linear cords thatinvade the stroma. These infiltratingcords frequently present a concentricpattern around normal ducts. There isoften little host reaction or disturbance ofthe background architecture. The neo-plastic cells have round or notched ovoidnuclei and a thin rim of cytoplasm with anoccasional intracytoplasmic lumen{2312} often harbouring a central mucoidinclusion. Mitoses are typically infre-quent. This classical form of ILC is asso-ciated with features of lobular carcinomain situ in at least 90% of the cases{705,2001}.In addition to this common form, variantpatterns of ILC have been described.The solid pattern is characterized bysheets of uniform small cells of lobularmorphology {835}. The cells lack cell tocell cohesion and are often more pleo-morphic and have a higher frequency ofmitoses than the classical type. In thealveolar variant , tumour cells are mainly
arranged in globular aggregates of atleast 20 cells {2668}, the cell morphologyand growth pattern being otherwise typi-cal of lobular carcinoma. Pleomorphiclobular carcinoma retains the distinctivegrowth pattern of lobular carcinoma butexhibits a greater degree of cellular atyp-ia and pleomorphism than the classicalf o rm {808,1858,3082}. Intra-lobularlesions composed of signet ring cells orpleomorphic cells are features frequentlyassociated with it. Pleomorphic lobularcarcinoma may show apocrine {808} orhistiocytoid {3047} diff e rentiation. Amixed group is composed of casesshowing an admixture of the classicaltype with one or more of these patterns{705}. In about 5% of invasive breastcancers, both ductal and lobular featuresof differentiation are present {1780} (seeMixed type carcinoma, page 21).Analysis of E-cadherin expression mayhelp to divide these cases between duc-tal and lobular tumours but theimmunophenotype remains ambiguousin a minority of cases {34}.
The admixture of tubular growth patternand small uniform cells arranged in a lin-ear pattern defines tubulo-lobular carci-noma (TLC) (ICD-O 8524/3) {875}. LCISis observed in about one third of TLC.Comparison of the clinico-pathologicalfeatures of TLC and pure tubular carci-noma (TC) has shown that axillary metas-tases were more common in TLC (43%)than in TC (12%) {1062}. A high rate ofestrogen receptor (ER) positivity has alsobeen reported in TLC {3141}. Furtheranalysis of TLC, especially regarding E-cadherin status, should help to deter-mine whether TLC should be categorizedas a variant of tubular or of lobulartumours. Without this data these tumoursare best classified as a variant of lobularcarcinoma.
ImmunoprofileAbout 70-95% of lobular carcinomas areER positive, a rate higher than the 70-80% observed in IDC {2541,3235}.Progesterone receptor (PR) positivity is60-70% in either tumour type {2541,
24 Tumours of the breast
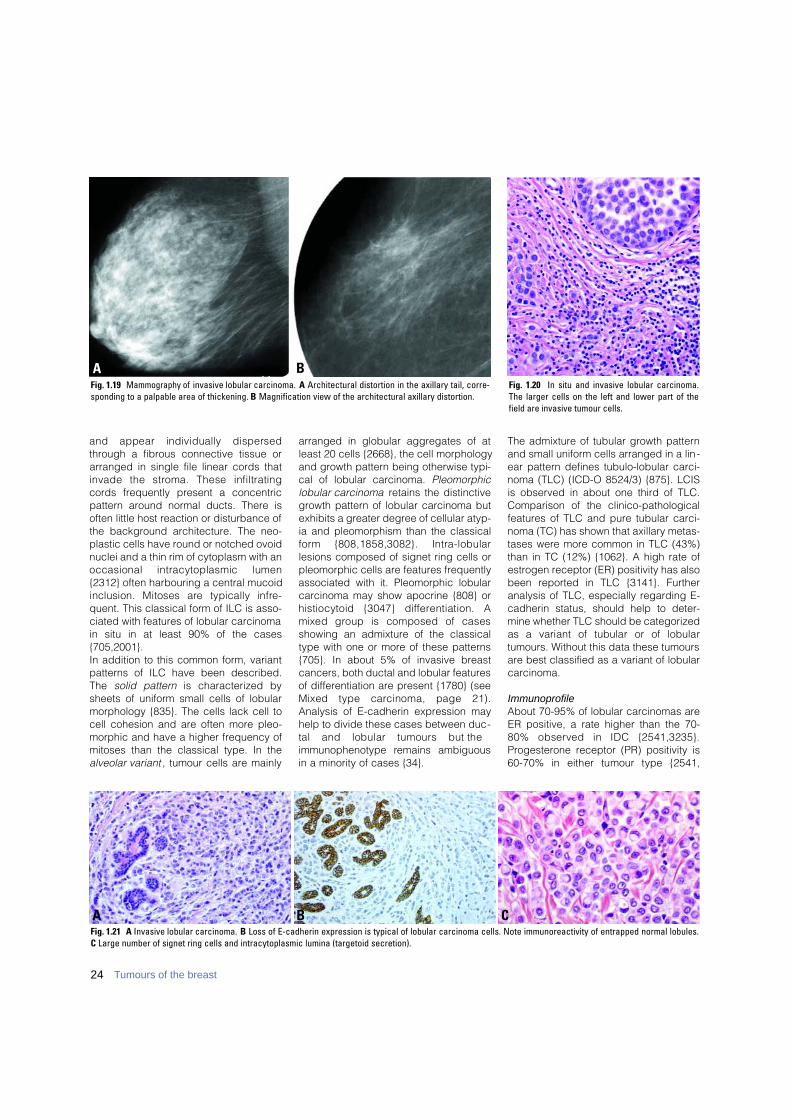
B CAFig. 1.21 A Invasive lobular carcinoma. B Loss of E-cadherin expression is typical of lobular carcinoma cells. Note immunoreactivity of entrapped normal lobules.C Large number of signet ring cells and intracytoplasmic lumina (targetoid secretion).
AFig. 1.19 Mammography of invasive lobular carcinoma. A Architectural distortion in the axillary tail, corre-sponding to a palpable area of thickening. B Magnification view of the architectural axillary distortion.
BFig. 1.20 In situ and invasive lobular carcinoma.The larger cells on the left and lower part of thefield are invasive tumour cells.

25Invasive breast cancer
3235}. ER was found to be expressed inthe classical form and in variants {1994},but the rate of positivity was higher(100%) in alveolar {2668} and lower(10%) in pleomorphic ILC {2318} than inthe classical type. The proliferation ratein ILC is generally low {2027}. With theexception of pleomorphic lobular carci-noma ERBB2 overe x p ression in ILC{2274,2477,2750}, is lower than reportedin IDC {2358}.
Genetics Using flow cytometry, ILCs were foundnear diploid in about 50% of the cases{887}. This fits with the finding that chro-mosomal abnormalities, assessed bycytogenetical {887} or comparativegenomic hybridization (CGH) analysis{2027}, are less numerous in ILC than inIDC. In ILC, the most common geneticalteration, found in 63-87% of the cases{887,2027}, is a loss of the long arm ofchromosome 16.The E (epithelial)-cadherin gene, whichmaps in 16q22, is implicated in main-taining coherence of adult epithelial tissues {1217}, and acts as a cell diffe-rentiation and invasion suppressor factor{922,3030}. A correlation has been foundbetween deletion of 16q and the loss ofE-cadherin expression {2027}. Immu-nohistochemical analysis has shown complete loss of E-cadherin expression in 80-100% of ILC {956,1892,2094,2152,2336}. This contrasts with them e re decrease in staining intensityobserved in 30-60% of IDC.Molecular analysis has shown that, inmost cases, the lack of E-cadherin
immunostaining can be related to thepresence of protein truncation mutations{260,1394,2380}, together with the inacti-vation of the wild type allele. Alternativemechanisms may also be involved in the alteration of E-cadherin {723,3190}and/or of E-cadherin-associated proteins{723,1892,2337,2374}.Analysis of neoplastic lesions corre s p o n-ding to early steps of tumour develop-ment has shown that both loss of het-e rozygosity of the 16q chro m o s o m a lregion {800} and of E-cadherin expre s-sion {649,3034} were also observed inLCIS and in mixed ductal-lobular carc i n o-ma {34}. Inactivation of the E-cadheringene may thus re p resent an early event inoncogenesis and this biological trait indi-cates that LCIS is a potential precursor ofILC. However, other molecular eventsmust be involved in the transition from in situ to invasive lobular tumours.F u rt h e rm o re, genetic losses concern i n gother parts of the long arm of chro m o-some 16 than the locus of E-cadherinhave been found in IDC and in ILC {2960},as well as in DCIS {460}. This stro n g l ysuggests that several genes localized inthis chromosomal region, and pre s e n t i n gtumour suppressive pro p e rties, may beinvolved in breast oncogenesis.A combination of mutation analysis andE-cadherin protein expression may offera method for identification of lobular carcinoma.
Prognosis and predictive factorsA lower frequency of axillary nodalmetastasis in ILC than in IDC has beenreported in several series, the difference
ranging from 3-10% {1327,1578,2541,2696,2935}. Metastatic involvement bysc a t t e red isolated cells may simulatesinusoidal histiocytes and re q u i reimmunohistochemical detection.The metastatic pattern of ILC differs fromthat of IDC. A higher frequency of tumourextension to bone, gastro-intestinal tract,uterus, meninges, ovary and diff u s eserosal involvement is observed in ILCwhile extension to lung is more frequentin IDC {319,1142,1327,2541,2696,2935}. IHC using antibodies raised a g a i n s tGCDFP-15, cytokeratin 7, ER, andE-cadherin may help establish a femalegenital tract tumour as a metastatic ILC. Several studies have reported a morefavourable disease outcome for ILC thanfor IDC {705,725,771,2696,2935} where-as others found no significant differences{2205,2541,2696,2731} or a worse prog-nosis for ILC {126}.When the histological subtypes of ILCw e re analysed separately, a morefavourable outcome was reported for theclassical type than for variants {699,705,725}. However, alveolar ILC hasbeen considered as a low grade tumour{2668}, whereas a poor prognosis ofpleomorphic ILC has been reported insome series {808,3082}. No difference inthe outcome of different subtypes hasbeen observed in other series {2935}. Furthermore, a large extent of lymphnode involvement has not been found toincrease significantly the risk of localrelapse {2570}. A link between lack of E-cadherin expression and adverse out-come of the disease has also beenreported {125,1176}.
BAFig. 1.22 A Classic invasive lobular carcinoma with uniform, single cell files compared to (B). B Invasive pleomorphic lobular carcinoma with characteristic pleomor-phic, atypical nuclei.
26 Tumours of the breast
Treatment of ILC should depend on thestage of the tumour and parallel that ofIDC. Conservative treatment has beenshown to be appropriate for ILC {327,2205,2269,2541,2570,2696}.
Tubular carcinoma
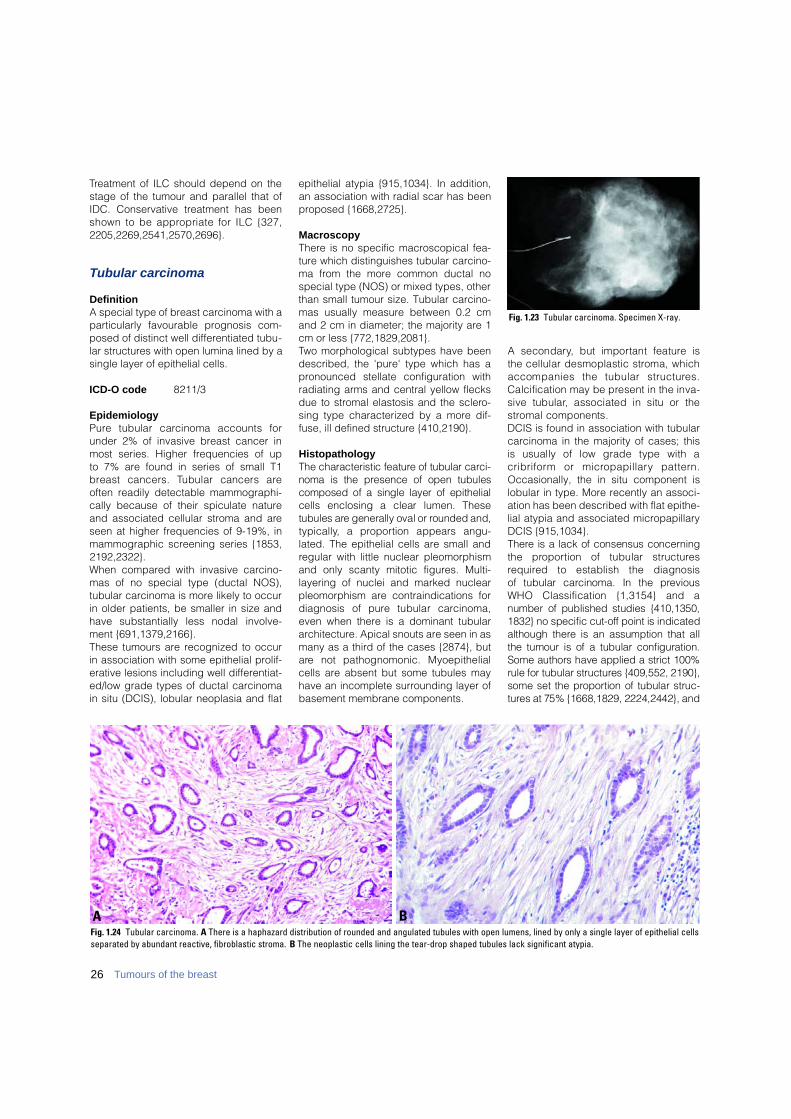
DefinitionA special type of breast carcinoma with aparticularly favourable prognosis com-posed of distinct well differentiated tubu-lar structures with open lumina lined by asingle layer of epithelial cells.
ICD-O code 8211/3
EpidemiologyP u re tubular carcinoma accounts forunder 2% of invasive breast cancer inmost series. Higher frequencies of up to 7% are found in series of small T1b reast cancers. Tubular cancers areoften readily detectable mammographi-cally because of their spiculate natureand associated cellular stroma and areseen at higher frequencies of 9-19%, inmammographic screening series {1853,2192,2322}.When compared with invasive carcino-mas of no special type (ductal NOS),tubular carcinoma is more likely to occurin older patients, be smaller in size andhave substantially less nodal involve-ment {691,1379,2166}.These tumours are recognized to occurin association with some epithelial prolif-erative lesions including well differentiat-ed/low grade types of ductal carcinomain situ (DCIS), lobular neoplasia and flat
epithelial atypia {915,1034}. In addition,an association with radial scar has beenproposed {1668,2725}.
MacroscopyThere is no specific macroscopical fea-ture which distinguishes tubular carcino-ma from the more common ductal nospecial type (NOS) or mixed types, otherthan small tumour size. Tubular carcino-mas usually measure between 0.2 cmand 2 cm in diameter; the majority are 1cm or less {772,1829,2081}.Two morphological subtypes have beendescribed, the 'pure' type which has apronounced stellate configuration withradiating arms and central yellow flecksdue to stromal elastosis and the sclero-sing type characterized by a more dif-fuse, ill defined structure {410,2190}.
HistopathologyThe characteristic feature of tubular carc i-noma is the presence of open tubulescomposed of a single layer of epithelialcells enclosing a clear lumen. Thesetubules are generally oval or rounded and,t y p i c a l l y, a pro p o rtion appears angu-lated. The epithelial cells are small andregular with little nuclear pleomorphismand only scanty mitotic figures. Multi-layering of nuclei and marked nuclearpleomorphism are contraindications fordiagnosis of pure tubular carc i n o m a ,even when there is a dominant tubulararchitecture. Apical snouts are seen in asmany as a third of the cases {2874}, buta re not pathognomonic. Myoepithelialcells are absent but some tubules mayhave an incomplete surrounding layer ofbasement membrane components.
A secondary, but important feature isthe cellular desmoplastic stroma, whichaccompanies the tubular structure s .Calcification may be present in the inva-sive tubular, associated in situ or thes t romal components.DCIS is found in association with tubularcarcinoma in the majority of cases; this is usually of low grade type with a c r i b r i f o rm or micro p a p i l l a ry pattern .Occasionally, the in situ component islobular in type. More recently an associ-ation has been described with flat epithe-lial atypia and associated micropapillaryDCIS {915,1034}.T h e re is a lack of consensus concern i n gthe pro p o rtion of tubular structure sre q u i red to establish the diagnosis of tubular carcinoma. In the pre v i o u sWHO Classification {1,3154} and a number of published studies {410,1350,1832} no specific cut-off point is indicatedalthough there is an assumption that allthe tumour is of a tubular configuration.Some authors have applied a strict 100%rule for tubular structures {409,552, 2190},some set the pro p o rtion of tubular struc-t u res at 75% {1668,1829, 2224,2442}, and
BA
Fig. 1.23 Tubular carcinoma. Specimen X-ray.
Fig. 1.24 Tubular carcinoma. A There is a haphazard distribution of rounded and angulated tubules with open lumens, lined by only a single layer of epithelial cellsseparated by abundant reactive, fibroblastic stroma. B The neoplastic cells lining the tear-drop shaped tubules lack significant atypia.

yet others at 90% {97,2147}. For pragma-tic reasons, a 90% purity re q u i re m e n to ffers a practical solution.Tumours exhibiting between 50 and 90%tubular growth pattern with other typesshould be regarded as mixed type ofcarcinoma (see Mixed type carcinomas).
Differential diagnosisSclerosing adenosis (SA) can be distin-guished from tubular carcinoma by itsoverall lobular arc h i t e c t u re and themarked compression and distortion ofthe glandular structures. Myoepithelialcells are always present in sclerosingadenosis and can be highlighted byimmunostaining for actin. Similarly, a fullyretained basement membrane can beshown by immunohistological staining forcollagen IV and laminin in tubules of SA.Microglandular adenosis (MA) can bemore difficult to differentiate because ofthe rather haphazard arrangement of thetubules, and lack of myoepithelial cells inthe tubules. However, the tubules of MAare more rounded and regular and oftencontain colloid-like secretory material, atleast focally, compared to the often angu-lated tubules of tubular carc i n o m a .Furthermore a ring of basement mem-brane is present around tubules of MA.Complex sclerosing lesions/radial scarshave a typical arc h i t e c t u re with centralf i b rosis and elastosis containing a fewsmall, often distorted, tubular structures inwhich myoepithelial cells can be demon-strated. The surrounding glandular struc-t u res show varying degrees of dilatationand ductal epithelial hyperplasia.
ImmunophenotypeTubular carcinoma is nearly alwayse s t rogen and pro g e s t e rone re c e p t o rpositive, has a low growth fraction, andis ERBB2 and EGFR negative {691,1 3 7 9 , 2 1 6 6 } .
GeneticsTubular carcinomas of the breast have alow frequency of genetic alterationswhen compared to other types of bre a s tc a rcinoma. Using LOH and CGH tech-niques, alterations have been foundmost frequently at chromosomes 16q(loss), 1q (gain), 8p (loss), 3p FHITgene locus, and 11q ATM gene locus{1754,1779,2476, 3046}. Of part i c u l a ri n t e rest is the observation that othersites of chromosomal alteration pre v i-ously found at high levels in other types
of breast cancer are not seen, whichimplies that tubular carcinoma of theb reast is genetically distinct.
Prognosis and predictive factorsPure tubular carcinoma has an excellentlong term prognosis {409,410,552,771,1829,2081,2224} which in some series issimilar to age matched women withoutbreast cancer {691}. Recurrence follow-ing mastectomy or breast conservationtreatment is rare and localized tubularcarcinomas are considered to be idealcandidates for breast conservation tech-niques. Following breast conservation,the risk of local recurrence is so low thatsome centres consider adjuvant radio-therapy unnecessary. Axillary nodemetastases occur infrequently, and whenobserved rarely involve more than onelow axillary lymph node. There is littleadverse effect of node positivity in tubu-lar carcinoma {691,1471} and the use ofsystemic adjuvant therapy and axillarynode dissection are considered un-necessary by some groups {691,2166}.
Invasive cribriform carcinoma
DefinitionAn invasive carcinoma with an excellentprognosis that grows in a cribriform pat-tern similar to that seen in intraductalcribriform carcinoma; a minor (<50%)component of tubular carcinoma may beadmixed.
ICD-O code 8201/3
EpidemiologyInvasive cribriform carcinoma (ICC)accounts for 0.8-3.5% of breast carcino-mas. The mean age of patients is 53-58years {2148,2670,3017}.
Clinical features The tumour may present as a mass butis frequently clinically occult. At mam-m o g r a p h y, tumours typically form aspiculated mass frequently containingm i c rocalcifications {2670,2806}. Multi-focality is observed in 20% of the cases{ 2 1 4 8 } .
HistopathologyThe pure ICC consists almost entire l y(>90%) of an invasive cribriform pat-t e rn. The tumour is arranged as inva-sive islands, often angulated, in whichwell defined spaces are formed bya rches of cells (a sieve-like or cribri-f o rm pattern). Apical snouts are a re g-ular feature. The tumour cells are smalland show a low or moderate degree ofnuclear pleomorphism. Mitoses arer a re. A prominent, reactive appearing,f i b roblastic stroma is present in manyICC. Intraductal carcinoma, generallyof the cribriform type, is observed in asmany as 80% of cases {2148}. Axillarylymph node metastases occur in 14.3%{2148}, the cribriform pattern beingretained at these sites. Lesions show-ing a predominantly cribriform arrange-
27Invasive breast cancer
Fig. 1.25 Invasive cribriform carcinoma. The haphazard distribution of irregularly shaped and angulated invasiveareas is in contrast with the rounded configuration of the ducts with cribriform DCIS on the left side of the field.

ment associated with a minor (<50%)component of tubular carcinoma arealso included in the group of classicICC {2148}. Cases with a component(10-40%) of another carcinoma type,other than tubular carcinoma, shouldbe called mixed type of carc i n o m a{ 2 1 4 8 , 3 0 1 7 } .
ImmunoprofileICC is estrogen receptor positive in100% and progesterone receptor in 69%of cases {3017}.
Differential diagnosisICC should be differentiated from carci-noid tumour and adenoid cystic carcino-ma; the former has intracytoplasmicargyrophilic granules, while the latter hasa second cell population in addition to avariety of intracystic secretory and base-ment membrane-like material. The lack oflaminin around the cribriform structuresalso differentiates ICC from adenoid cys-tic carcinoma {3092}. ICC is distin-guished from extensive cribriform DCISby the lack of a myoepithelial cell layeraround its invasive tumour cell clusters,its haphazard distribution and irregularconfiguration.
Prognosis and predictive factorsICC has a remarkably favourable out-come {771,2148,3017}. The ten-yearoverall survival was 90% {771} to 100%{2148}. The outcome of mixed invasivec r i b r i f o rm carcinoma has been re p o rt e dto be less favourable than that of theclassic form, but better than that of com-mon ductal carcinoma {2148}. The bio-logical behaviour of ICC is very similar tothat of tubular carcinoma {771}. It hasbeen suggested that cribriform elementsmight correspond to tubules {2148}.H o w e v e r, many ICC have no definitetubular structures and separation of thistumour as a distinct clinicopathologicalentity is justified.
Medullary carcinoma
DefinitionA well circumscribed carcinoma com-posed of poorly diff e rentiated cellsarranged in large sheets, with no glandu-lar structures, scant stroma and a promi-nent lymphoplasmacytic infiltrate.
ICD-O code 8510/3
EpidemiologyM e d u l l a ry carcinoma (MC) re p re s e n t sbetween 1 and 7% {294,2334} of allbreast carcinomas, depending on thestringency of diagnostic criteria used.The mean age of women with MC rangesf rom 45 to 52 years {623,2204,2334,3064}.
Clinical features The tumour is well delineated and soft onpalpation. Mammographically MC is typ-ically well circumscribed and may beconfused with a benign lesion.
Macroscopy MC has distinctive rounded, well definedmargins and a soft consistency. Fleshytan to grey in appearance, foci of necro-sis and haemorrhage are frequent. Themedian diameter varies from 2.0-2.9 cm{2334,2370,3064}.
HistopathologySince the early descriptions of MC{895,1908,2367}, the histological fea-tures of this tumour have been furtherspecified {2334,2370,3064}. C l a s s i c a l l y, five morphological traitscharacterize MC. 1. A syncytial architecture should beobserved in over 75% of the tumourmass. Tumour cells are arranged insheets, usually more than four or fivecells thick, separated by small amountsof loose connective tissue. Foci of necro-sis and of squamous differentiation maybe seen. 2. Glandular or tubular structures are notpresent, even as a minor component. 3. Diffuse lymphoplasmacytic stro m a linfiltrate is a conspicuous feature. Thedensity of this infiltrate varies amongcases, mononuclear cells may be scarceor so numerous that they largely obliter-ate the carcinoma cells. Lymphoid folli-cles and/or epithelioid granuloma maybe present.4. Carcinoma cells are usually round withabundant cytoplasm and vesicular nucleicontaining one or several nucleoli. Thenuclear pleomorphism is moderate ormarked, consistent with grade 2 or 3.Mitoses are numerous. Atypical giantcells may be observed.5. Complete histological circumscriptionof the tumour is best seen under lowmagnification. Pushing margins maydelimit a compressed fibrous zone at theperiphery of the lesion.
Besides these typical histologic traits,the presence of an intraductal compo-nent is considered as a criterion forexclusion by some authors {2370,3064},but acceptable by others {2334}, espe-cially when it is located in the surround-ing tissue or reduced to small areas with-in the tumour mass.These diagnostic criteria, particularly thestatus of the margin, may be difficult toassess in practice, and may explain thelow reproducibility in the diagnosis of MCobserved in certain series {950,2203,2372}. To overcome this difficulty, a sim-plified scheme has been pro p o s e d{2202}. Syncytial growth pattern, lack oftubule formation and lymphoplasmacyticinfiltrate, together with sparse tumournecrosis (<25%) were found to be themost re p roducible and characteristicfeatures of MC. However, the prognosticsignificance of this simplistic schemeneeds to be assessed {1339}.Tumours showing the association of apredominantly syncytial architecture withonly two or three of the other criteria areusually designated as atypical medullarycarcinoma (AMC) {2334,2370}. However,strictly defined morphological criteria arenecessary to preserve the entity of MCcharacterized by its relatively favourablep rognosis {2334,2478} which is notshared by AMC. Several works {2334,3064} have advocated the elimination ofthe AMC category in order to avoid con-fusion with MC and the term infiltratingductal carcinoma with medullary featuresseems to be more appropriate for thesetumours.
Immunoprofile and ploidyFlow cytometry and immunohistochemi-cal analysis has shown that most MCa re aneuploid and highly pro l i f e r a t i v etumours {551,1244,1345,1766,2108,2201}. A high apoptosis rate has also
28 Tumours of the breast
Fig. 1.26 Medullary carcinoma. Mammogram showinga typical rounded, dense tumour without calcifications.
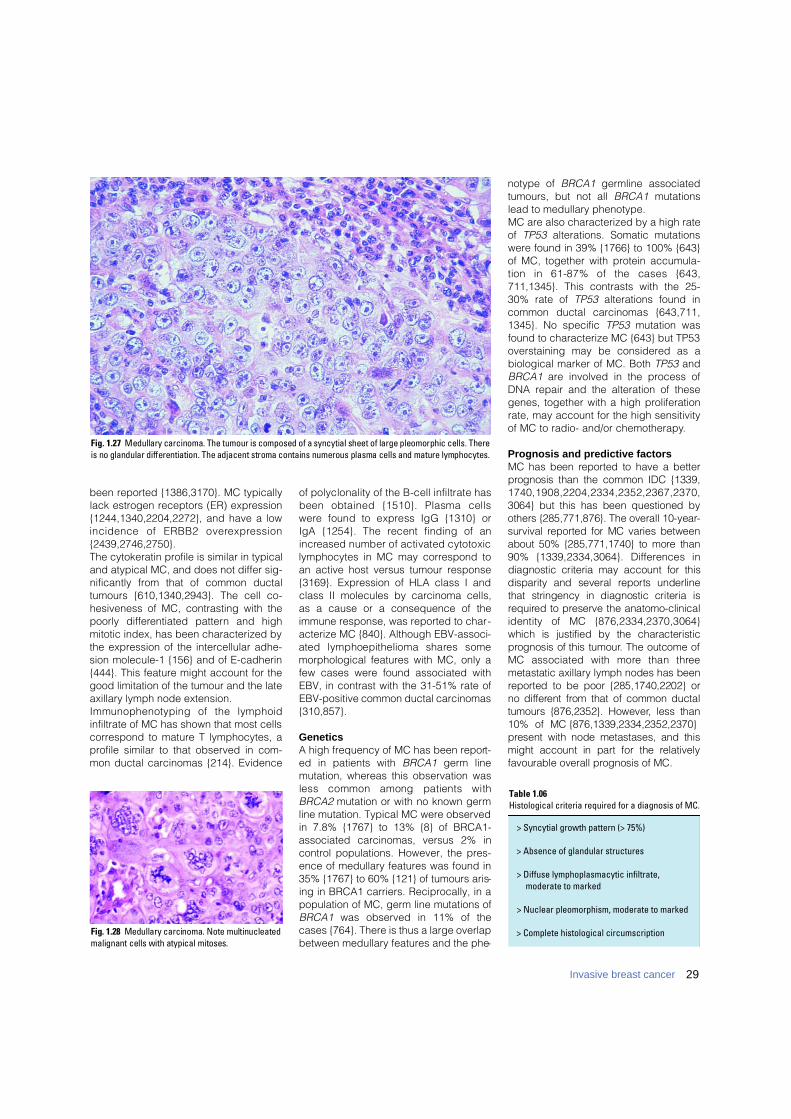
29Invasive breast cancer
been reported {1386,3170}. MC typicallylack estrogen receptors (ER) expression{1244,1340,2204,2272}, and have a lowincidence of ERBB2 overe x p re s s i o n{2439,2746,2750}.The cytokeratin profile is similar in typicaland atypical MC, and does not differ sig-nificantly from that of common ductaltumours {610,1340,2943}. The cell co-hesiveness of MC, contrasting with thepoorly diff e rentiated pattern and highmitotic index, has been characterized bythe expression of the intercellular adhe-sion molecule-1 {156} and of E-cadherin{444}. This feature might account for thegood limitation of the tumour and the lateaxillary lymph node extension.Immunophenotyping of the lymphoidinfiltrate of MC has shown that most cellscorrespond to mature T lymphocytes, aprofile similar to that observed in com-mon ductal carcinomas {214}. Evidence
of polyclonality of the B-cell infiltrate hasbeen obtained {1510}. Plasma cellsw e re found to express IgG {1310} or IgA {1254}. The recent finding of ani n c reased number of activated cytotoxiclymphocytes in MC may correspond toan active host versus tumour response{3169}. Expression of HLA class I andclass II molecules by carcinoma cells, as a cause or a consequence of theimmune response, was reported to char-acterize MC {840}. Although EBV-associ-ated lymphoepithelioma shares somemorphological features with MC, only afew cases were found associated withEBV, in contrast with the 31-51% rate ofEBV-positive common ductal carcinomas{310,857}.
GeneticsA high frequency of MC has been report-ed in patients with BRCA1 germ linemutation, whereas this observation wasless common among patients withBRCA2 mutation or with no known germline mutation. Typical MC were observedin 7.8% {1767} to 13% {8} of BRCA1-associated carcinomas, versus 2% incontrol populations. However, the pres-ence of medullary features was found in35% {1767} to 60% {121} of tumours aris-ing in BRCA1 carriers. Reciprocally, in apopulation of MC, germ line mutations ofBRCA1 was observed in 11% of thecases {764}. There is thus a large overlapbetween medullary features and the phe-
notype of BRCA1 germline associatedtumours, but not all BRCA1 mutationslead to medullary phenotype.MC are also characterized by a high rateof TP53 alterations. Somatic mutationswere found in 39% {1766} to 100% {643}of MC, together with protein accumula-tion in 61-87% of the cases {643,711,1345}. This contrasts with the 25-30% rate of TP53 alterations found incommon ductal carcinomas {643,711,1345}. No specific TP53 mutation wasfound to characterize MC {643} but TP53overstaining may be considered as abiological marker of MC. Both TP53 andBRCA1 are involved in the process ofDNA repair and the alteration of thesegenes, together with a high proliferationrate, may account for the high sensitivityof MC to radio- and/or chemotherapy.
Prognosis and predictive factorsMC has been re p o rted to have a betterp rognosis than the common IDC {1339,1 7 4 0 , 1 9 0 8 , 2 2 0 4 , 2 3 3 4 , 2 3 5 2 , 2 3 6 7 , 2 3 7 0 ,3064} but this has been questioned byothers {285,771,876}. The overall 10-year-survival re p o rted for MC varies betweenabout 50% {285,771,1740} to more than90% {1339,2334,3064}. Diff e rences indiagnostic criteria may account for thisdisparity and several re p o rts underlinethat stringency in diagnostic criteria isre q u i red to preserve the anatomo-clinicalidentity of MC {876,2334,2370,3064}which is justified by the characteristicp rognosis of this tumour. The outcome ofMC associated with more than thre emetastatic axillary lymph nodes has beenre p o rted to be poor {285,1740,2202} or no diff e rent from that of common ductaltumours {876,2352}. However, less than10% of MC {876,1339,2334,2352,2370}p resent with node metastases, and thismight account in part for the re l a t i v e l yfavourable overall prognosis of MC.
Fig. 1.27 Medullary carcinoma. The tumour is composed of a syncytial sheet of large pleomorphic cells. Thereis no glandular differentiation. The adjacent stroma contains numerous plasma cells and mature lymphocytes.
> Syncytial growth pattern (> 75%)
> Absence of glandular structures
> Diffuse lymphoplasmacytic infiltrate, moderate to marked
> Nuclear pleomorphism, moderate to marked
> Complete histological circumscription
Table 1.06Histological criteria required for a diagnosis of MC.
Fig. 1.28 Medullary carcinoma. Note multinucleatedmalignant cells with atypical mitoses.
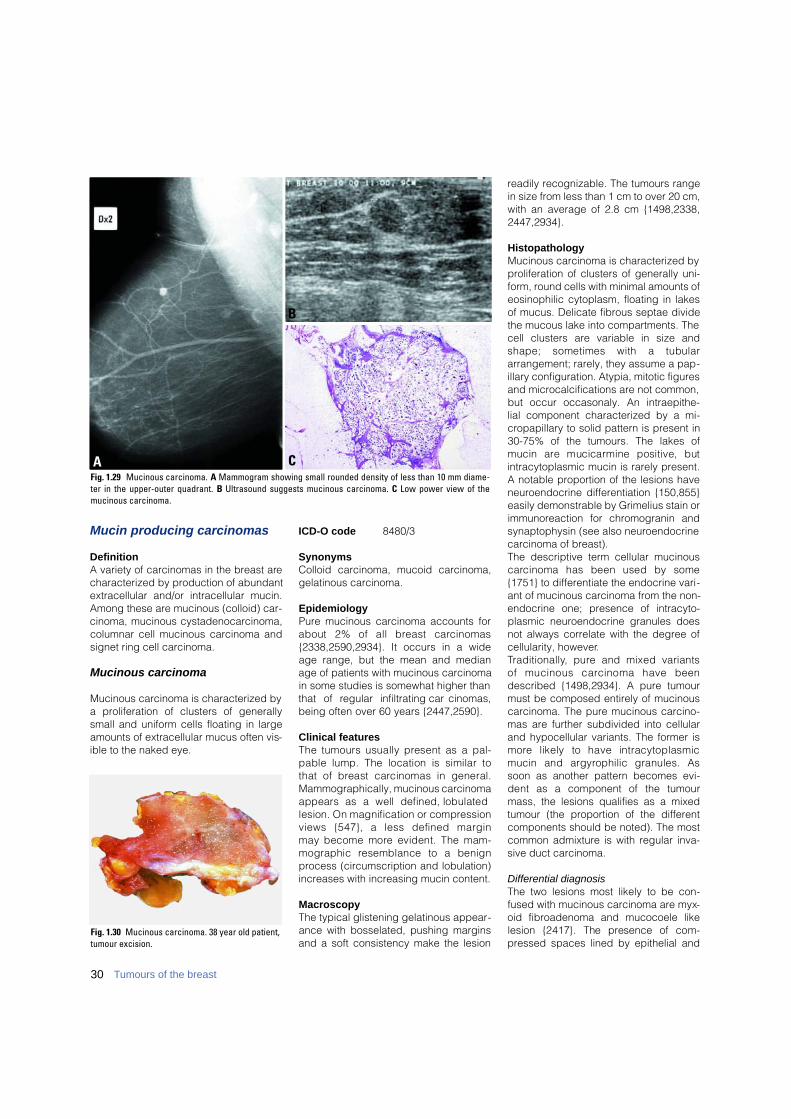
Mucin producing carcinomas
DefinitionA variety of carcinomas in the breast arecharacterized by production of abundantextracellular and/or intracellular mucin.Among these are mucinous (colloid) car-cinoma, mucinous cystadenocarcinoma,columnar cell mucinous carcinoma andsignet ring cell carcinoma.
Mucinous carcinoma
Mucinous carcinoma is characterized bya proliferation of clusters of generallysmall and uniform cells floating in largeamounts of extracellular mucus often vis-ible to the naked eye.
ICD-O code 8480/3
SynonymsColloid carcinoma, mucoid carcinoma,gelatinous carcinoma.
Epidemiology Pure mucinous carcinoma accounts forabout 2% of all breast carc i n o m a s{2338,2590,2934}. It occurs in a wideage range, but the mean and medianage of patients with mucinous carcinomain some studies is somewhat higher thanthat of regular infiltrating carc i n o m a s ,being often over 60 years {2447,2590}.
Clinical featuresThe tumours usually present as a pal-pable lump. The location is similar tothat of breast carcinomas in general.Mammographically, mucinous carcinomaappears as a well defined, lobulatedlesion. On magnification or compre s s i o nviews {547}, a less defined margin may become more evident. The mam-mographic resemblance to a benignprocess (circumscription and lobulation)increases with increasing mucin content.
Macroscopy The typical glistening gelatinous appear-ance with bosselated, pushing marginsand a soft consistency make the lesion
readily recognizable. The tumours rangein size from less than 1 cm to over 20 cm,with an average of 2.8 cm {1498,2338,2447,2934}.
HistopathologyMucinous carcinoma is characterized byproliferation of clusters of generally uni-form, round cells with minimal amounts ofeosinophilic cytoplasm, floating in lakesof mucus. Delicate fibrous septae dividethe mucous lake into compartments. Thecell clusters are variable in size andshape; sometimes with a tubulararrangement; rarely, they assume a pap-illary configuration. Atypia, mitotic figuresand microcalcifications are not common,but occur occasonaly. An intraepithe-lial component characterized by a mi-cropapillary to solid pattern is present in30-75% of the tumours. The lakes ofmucin are mucicarmine positive, butintracytoplasmic mucin is rarely present.A notable proportion of the lesions haveneuroendocrine differentiation {150,855}easily demonstrable by Grimelius stain orimmunoreaction for chromogranin andsynaptophysin (see also neuroendocrinecarcinoma of breast). The descriptive term cellular mucinousc a rcinoma has been used by some{1751} to differentiate the endocrine vari-ant of mucinous carcinoma from the non-endocrine one; presence of intracyto-plasmic neuroendocrine granules doesnot always correlate with the degree ofcellularity, however.Tr a d i t i o n a l l y, pure and mixed variants of mucinous carcinoma have beendescribed {1498,2934}. A pure tumourmust be composed entirely of mucinouscarcinoma. The pure mucinous carcino-mas are further subdivided into cellularand hypocellular variants. The former ism o re likely to have intracytoplasmicmucin and argyrophilic granules. Assoon as another pattern becomes evi-dent as a component of the tumourmass, the lesions qualifies as a mixedtumour (the proportion of the differentcomponents should be noted). The mostcommon admixture is with regular inva-sive duct carcinoma.
Differential diagnosisThe two lesions most likely to be con-fused with mucinous carcinoma are myx-oid fibroadenoma and mucocoele likelesion {2417}. The presence of com-pressed spaces lined by epithelial and
B
CFig. 1.29 Mucinous carcinoma. A Mammogram showing small rounded density of less than 10 mm diame-ter in the upper-outer quadrant. B Ultrasound suggests mucinous carcinoma. C Low power view of themucinous carcinoma.
A
Fig. 1.30 Mucinous carcinoma. 38 year old patient,tumour excision.
30 Tumours of the breast

myoepithelial cells in fibro a d e n o m a s ,along with mast cells within the myxoidstroma, helps in its recognition. In mucocoele-like lesions, the presenceof myoepithelial cells adhering to thestrips of cells floating in the lakes ofmucus serves as an important clue totheir benign nature; the cell clusters inmucinous carcinoma are purely epithe-lial. The presence of ducts variably dis-tended by mucinous material adjacent toa mucocoele is another helpful clue indistinguishing mucocoele-like lesionsfrom mucinous carcinomas.
Immunoprofile and ploidyTypically mucinous carcinoma is estro-gen receptor positive {2669}, while lessthan 70% {691} are pro g e s t e rone re c e p-tor positive. Nearly all pure mucinous car-cinomas are diploid, while over 50% ofthe mixed variety are aneuploid {2933}.
Prognosis and predictive factorsPrognostic factors relevant to breast car-cinomas in general are also applicable topure mucinous carcinomas. Tumour cel-lularity has also been implicated in thatcellular tumours are associated with aworse prognosis {502}. The presence orabsence of argyrophilic granules had noprognostic significance in two studies
{2590,2934}. In general, pure mucinouscarcinomas have a favourable prognosis{844,2590,2934}. The ten-year survivalranges from 80% {1498} to 100%{844,2053}. Pure mucinous carcinomashave a far better prognosis than themixed variety with at least a 18% differ-ence in survival rates noted in severalstudies {1498,2053,2934}. About 10% ofwomen with the pure form die of theircancer compared to 29% of those withthe mixed type {1498,2053}. A similar dif-ference also exists in the incidence ofaxillary node metastases for pure andmixed types; only 3-15% of the pure vari-ety show axillary node metastases com-p a red to 33-46% of the mixed type{82,1498,2338}. Late distant metastasesmay occur {502,2447,2934}.A rare cause of death among womenwith mucinous carcinoma is cere b r a linfarction due to mucin embolism to thecerebral arteries {2944}.
Mucinous cystadenocarcinomaand columnar cell mucinous carcinoma
DefinitionA carcinoma composed of generally tall,columnar cells with basally located blandnuclei and abundant intracytoplasmic
mucin that appears either cystic (muci-nous cystadenocarcinoma) or solid(columnar cell mucinous carcinoma) tothe naked eye.
ICD-O codeMucinous cystadenocarcinoma 8470/3
EpidemiologyOnly four examples of mucinous cys-tadenocarcinoma and two of the solidcolumnar cell type have been reported{1486}. They occurred in women 49 to 67years of age.
Clinical featuresThe clinical features of mucinous cys-tadenocarcinomas are similar to com-mon infiltrating ductal carcinomas.
MacroscopyThe tumours vary in size from 0.8 to 19cm, are cystic and display a gelatinousappearance with abundant mucoidmaterial simulating an ovarian mucinoustumour.
HistopathologyM i c ro s c o p i c a l l y, both of these variants,a re composed of tall columnar muci-nous cells with abundant intracyto-plasmic mucin and basal nuclei. In the
BA
DCFig. 1.32 A Mucinous cystadenocarcinoma. Papillary processes lined by mucinous columnar cells protudeinto cystic spaces. B Mucinous cystadenocarcinoma. Many of the invasive cells are immunoreactive toCK34βE12. C Combined mucinous and infiltrating ductal carcinoma. A favourable prognosis associated withpure mucinous carcinoma is no longer expected when it is admixed with regular infiltrating duct carcino-ma. D Signet ring cell carcinoma. The invasive cells assume a lobular growth pattern and contain abundantintracytoplasmic mucin conferring a signet-ring cell appearance to the cells.
Fig. 1.31 Mucinous carcinoma. A Hypercellularvariant with large clusters of densely packedmalignant cells. B Hypocellular variant. Lakes ofmucus are separated by fibrous septae. A few iso-lated or clusters of carcinoma cells are floating inthe mucus lakes.
A
B
31Invasive breast cancer
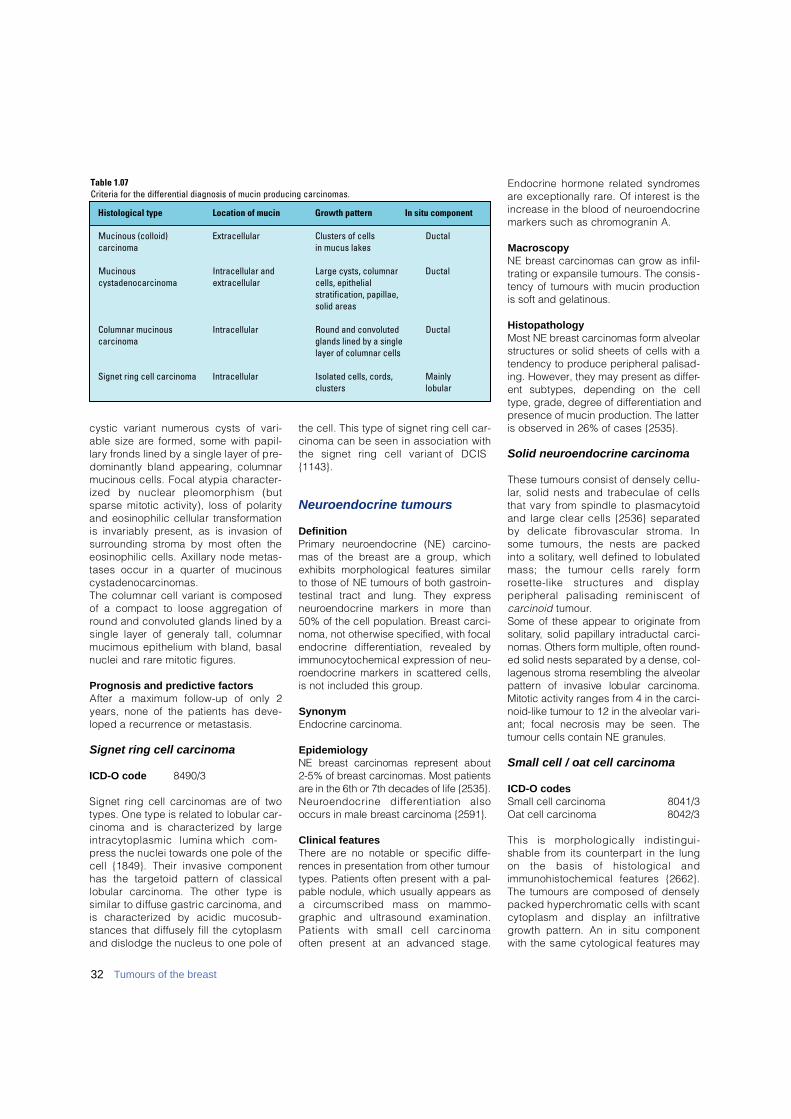
32 Tumours of the breast
cystic variant numerous cysts of vari-able size are formed, some with papil-l a ry fronds lined by a single layer of pre-dominantly bland appearing, columnarmucinous cells. Focal atypia character-ized by nuclear pleomorphism (butsparse mitotic activity), loss of polarityand eosinophilic cellular transform a t i o nis invariably present, as is invasion ofs u r rounding stroma by most often theeosinophilic cells. Axillary node metas-tases occur in a quarter of mucinousc y s t a d e n o c a rc i n o m a s .The columnar cell variant is composedof a compact to loose aggregation ofround and convoluted glands lined by asingle layer of generaly tall, columnarmucimous epithelium with bland, basalnuclei and rare mitotic figure s .
Prognosis and predictive factorsAfter a maximum follow-up of only 2years, none of the patients has deve-loped a re c u r rence or metastasis.
Signet ring cell carcinoma
ICD-O code 8490/3
Signet ring cell carcinomas are of twotypes. One type is related to lobular car-cinoma and is characterized by largeintracytoplasmic lumina which com-p ress the nuclei towards one pole of thecell {1849}. Their invasive componenthas the targetoid pattern of classicallobular carcinoma. The other type issimilar to diffuse gastric carcinoma, andis characterized by acidic mucosub-stances that diffusely fill the cytoplasmand dislodge the nucleus to one pole of
the cell. This type of signet ring cell car-cinoma can be seen in association withthe signet ring cell variant of DCIS{ 1 1 4 3 } .
Neuroendocrine tumours
DefinitionP r i m a ry neuroendocrine (NE) carc i n o-mas of the breast are a group, whichexhibits morphological features similarto those of NE tumours of both gastro i n-testinal tract and lung. They expre s sn e u roendocrine markers in more than50% of the cell population. Breast carc i-noma, not otherwise specified, with focalendocrine diff e rentiation, revealed byimmunocytochemical expression of neu-roendocrine markers in scattered cells,is not included this gro u p .
SynonymEndocrine carcinoma.
EpidemiologyNE breast carcinomas re p resent about 2-5% of breast carcinomas. Most patientsa re in the 6th or 7th decades of life {2535}.N e u roendocrine diff e rentiation alsooccurs in male breast carcinoma {2591}.
Clinical featuresThere are no notable or specific diffe-rences in presentation from other tumourtypes. Patients often present with a pal-pable nodule, which usually appears asa circumscribed mass on mammo-graphic and ultrasound examination.Patients with small cell carcinoma often present at an advanced stage.
Endocrine hormone related syndro m e sa re exceptionally rare. Of interest is thei n c rease in the blood of neuro e n d o c r i n emarkers such as chromogranin A.
MacroscopyNE breast carcinomas can grow as infil-trating or expansile tumours. The consis-tency of tumours with mucin productionis soft and gelatinous.
HistopathologyMost NE breast carcinomas form alveolarstructures or solid sheets of cells with atendency to produce peripheral palisad-ing. However, they may present as differ-ent subtypes, depending on the celltype, grade, degree of differentiation andpresence of mucin production. The latteris observed in 26% of cases {2535}.
Solid neuroendocrine carcinoma
These tumours consist of densely cellu-l a r, solid nests and trabeculae of cellsthat vary from spindle to plasmacytoidand large clear cells {2536} separatedby delicate fibrovascular stroma. Insome tumours, the nests are packedinto a solitary, well defined to lobulatedmass; the tumour cells rarely formrosette-like structures and displayperipheral palisading reminiscent ofc a rc i n o i d t u m o u r. Some of these appear to originate fro ms o l i t a ry, solid papillary intraductal carc i-nomas. Others form multiple, often ro u n d-ed solid nests separated by a dense, col-lagenous stroma resembling the alveolarp a t t e rn of invasive lobular carc i n o m a .Mitotic activity ranges from 4 in the carc i-noid-like tumour to 12 in the alveolar vari-ant; focal necrosis may be seen. Thetumour cells contain NE granules.
Small cell / oat cell carcinoma
ICD-O codesSmall cell carcinoma 8041/3Oat cell carcinoma 8042/3
This is morphologically indistingui-shable from its counterpart in the lungon the basis of histological andimmunohistochemical features {2662}.The tumours are composed of denselypacked hyperc h romatic cells with scantcytoplasm and display an infiltrativeg rowth pattern. An in situ componentwith the same cytological features may
Table 1.07Criteria for the differential diagnosis of mucin producing carcinomas.
Mucinous (colloid) Extracellular Clusters of cells Ductalcarcinoma in mucus lakes
Mucinous Intracellular and Large cysts, columnar Ductalcystadenocarcinoma extracellular cells, epithelial
stratification, papillae,solid areas
Columnar mucinous Intracellular Round and convoluted Ductalcarcinoma glands lined by a single
layer of columnar cells
Signet ring cell carcinoma Intracellular Isolated cells, cords, Mainlyclusters lobular
Histological type Location of mucin Growth pattern In situ component
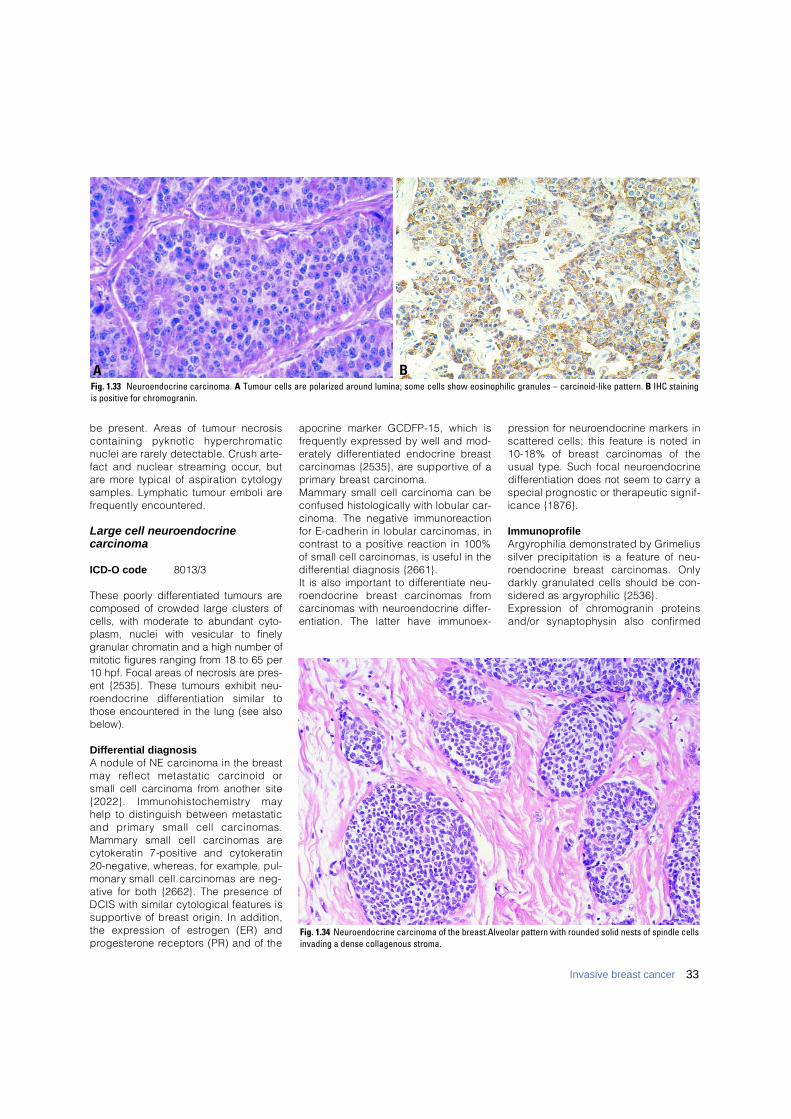
33Invasive breast cancer
be present. Areas of tumour necro s i scontaining pyknotic hyperc h ro m a t i cnuclei are rarely detectable. Crush art e-fact and nuclear streaming occur, buta re more typical of aspiration cytologysamples. Lymphatic tumour emboli aref requently encountered.
Large cell neuroendocrine carcinoma
ICD-O code 8013/3
These poorly differentiated tumours arecomposed of crowded large clusters ofcells, with moderate to abundant cyto-plasm, nuclei with vesicular to finelygranular chromatin and a high number ofmitotic figures ranging from 18 to 65 per10 hpf. Focal areas of necrosis are pres-ent {2535}. These tumours exhibit neu-roendocrine diff e rentiation similar tothose encountered in the lung (see alsobelow).
Differential diagnosisA nodule of NE carcinoma in the bre a s tmay reflect metastatic carcinoid orsmall cell carcinoma from another site{2022}. Immunohistochemistry mayhelp to distinguish between metastaticand primary small cell carc i n o m a s .M a m m a ry small cell carcinomas arecytokeratin 7-positive and cytokeratin20-negative, whereas, for example, pul-m o n a ry small cell carcinomas are neg-ative for both {2662}. The presence ofDCIS with similar cytological features iss u p p o rtive of breast origin. In addition,the expression of estrogen (ER) andp ro g e s t e rone receptors (PR) and of the
apocrine marker GCDFP-15, which isf requently expressed by well and mod-erately diff e rentiated endocrine bre a s tc a rcinomas {2535}, are supportive of ap r i m a ry breast carc i n o m a .M a m m a ry small cell carcinoma can beconfused histologically with lobular car-cinoma. The negative immunore a c t i o nfor E-cadherin in lobular carcinomas, incontrast to a positive reaction in 100%of small cell carcinomas, is useful in thed i ff e rential diagnosis {2661}.It is also important to diff e rentiate neu-roendocrine breast carcinomas fro mc a rcinomas with neuroendocrine diff e r-entiation. The latter have immunoex-
p ression for neuroendocrine markers ins c a t t e red cells; this feature is noted in10-18% of breast carcinomas of theusual type. Such focal neuro e n d o c r i n ed i ff e rentiation does not seem to carry aspecial prognostic or therapeutic signif-icance {1876}.
ImmunoprofileA r g y rophilia demonstrated by Grimeliussilver precipitation is a feature of neu-roendocrine breast carcinomas. Onlydarkly granulated cells should be con-s i d e red as argyrophilic {2536}. E x p ression of chromogranin pro t e i n sand/or synaptophysin also confirm e d
Fig. 1.34 Neuroendocrine carcinoma of the breast.Alveolar pattern with rounded solid nests of spindle cellsinvading a dense collagenous stroma.
BAFig. 1.33 Neuroendocrine carcinoma. A Tumour cells are polarized around lumina; some cells show eosinophilic granules – carcinoid-like pattern. B IHC stainingis positive for chromogranin.
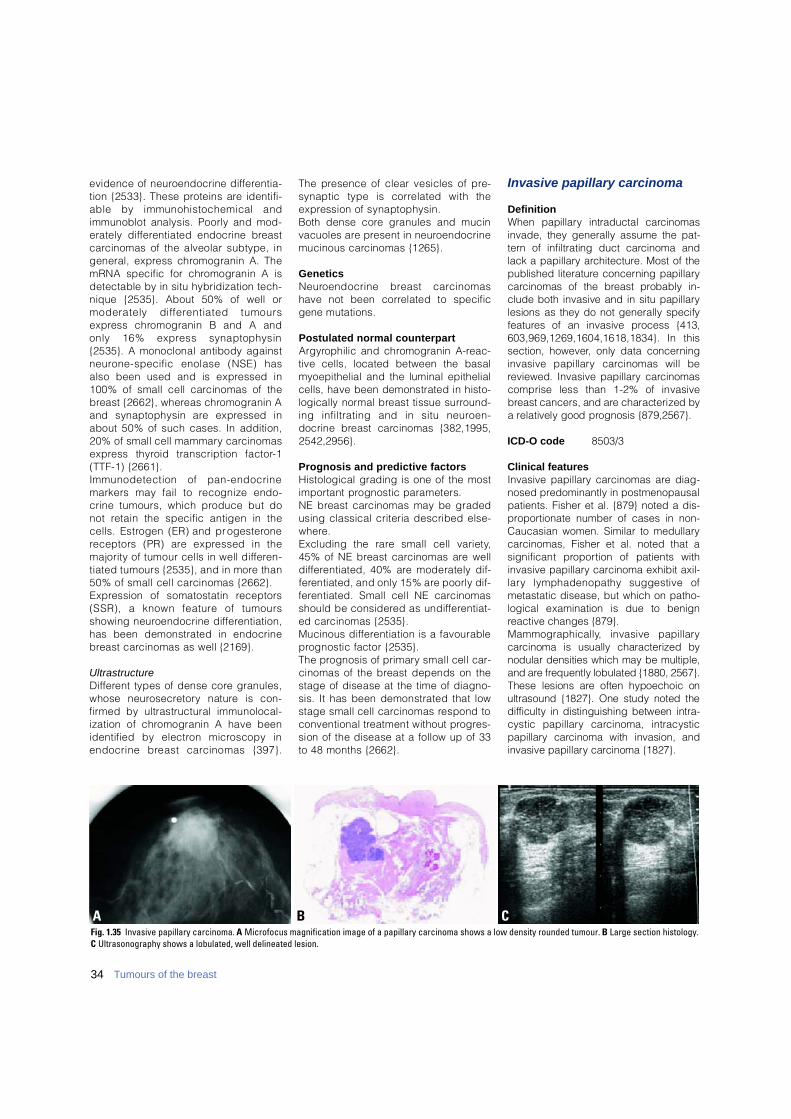
34 Tumours of the breast
evidence of neuroendocrine diff e re n t i a-tion {2533}. These proteins are identifi-able by immunohistochemical andimmunoblot analysis. Poorly and mod-erately diff e rentiated endocrine bre a s tc a rcinomas of the alveolar subtype, ingeneral, express chromogranin A. ThemRNA specific for chromogranin A isdetectable by in situ hybridization tech-nique {2535}. About 50% of well ormoderately diff e rentiated tumourse x p ress chromogranin B and A andonly 16% express synaptophysin{2535}. A monoclonal antibody againstn e u rone-specific enolase (NSE) hasalso been used and is expressed in100% of small cell carcinomas of theb reast {2662}, whereas chromogranin Aand synaptophysin are expressed inabout 50% of such cases. In addition,20% of small cell mammary carc i n o m a se x p ress thyroid transcription factor- 1(TTF-1) {2661}.Immunodetection of pan-endocrinemarkers may fail to recognize endo-crine tumours, which produce but donot retain the specific antigen in thecells. Estrogen (ER) and pro g e s t e ro n ereceptors (PR) are expressed in themajority of tumour cells in well diff e re n-tiated tumours {2535}, and in more than50% of small cell carcinomas {2662}.E x p ression of somatostatin re c e p t o r s(SSR), a known feature of tumoursshowing neuroendocrine diff e re n t i a t i o n ,has been demonstrated in endocrineb reast carcinomas as well {2169}.
U l t r a s t r u c t u r eD i ff e rent types of dense core granules,whose neuro s e c re t o ry nature is con-f i rmed by ultrastructural immunolocal-ization of chromogranin A have beenidentified by electron microscopy inendocrine breast carcinomas {397}.
The presence of clear vesicles of pre-synaptic type is correlated with thee x p ression of synaptophysin. Both dense core granules and mucinvacuoles are present in neuro e n d o c r i n emucinous carcinomas {1265}.
G e n e t i c sN e u roendocrine breast carc i n o m a shave not been correlated to specificgene mutations.
Postulated normal counterpart A r g y rophilic and chromogranin A-re a c-tive cells, located between the basalmyoepithelial and the luminal epithelialcells, have been demonstrated in histo-logically normal breast tissue surro u n d-ing infiltrating and in situ neuro e n-docrine breast carcinomas {382,1995,2 5 4 2 , 2 9 5 6 } .
Prognosis and predictive factors Histological grading is one of the mosti m p o rtant prognostic parameters.NE breast carcinomas may be gradedusing classical criteria described else-w h e re .Excluding the rare small cell variety,45% of NE breast carcinomas are welld i ff e rentiated, 40% are moderately dif-f e rentiated, and only 15% are poorly dif-f e rentiated. Small cell NE carc i n o m a sshould be considered as undiff e re n t i a t-ed carcinomas {2535}. Mucinous diff e rentiation is a favourablep rognostic factor {2535}. The prognosis of primary small cell car-cinomas of the breast depends on thestage of disease at the time of diagno-sis. It has been demonstrated that lowstage small cell carcinomas respond toconventional treatment without pro g re s-sion of the disease at a follow up of 33to 48 months {2662}.
Invasive papillary carcinoma
DefinitionWhen papillary intraductal carc i n o m a sinvade, they generally assume the pat-t e rn of infiltrating duct carcinoma andlack a papillary arc h i t e c t u re. Most of thepublished literature concerning papillaryc a rcinomas of the breast probably in-clude both invasive and in situ papillarylesions as they do not generally specifyf e a t u res of an invasive process {413,603,969,1269,1604,1618,1834}. In thissection, however, only data concern i n ginvasive papillary carcinomas will bereviewed. Invasive papillary carc i n o m a scomprise less than 1-2% of invasiveb reast cancers, and are characterized bya relatively good prognosis {879,2567}.
ICD-O code 8503/3
Clinical featuresInvasive papillary carcinomas are diag-nosed predominantly in postmenopausalpatients. Fisher et al. {879} noted a dis-proportionate number of cases in non-Caucasian women. Similar to medullarycarcinomas, Fisher et al. noted that asignificant pro p o rtion of patients withinvasive papillary carcinoma exhibit axil-l a ry lymphadenopathy suggestive ofmetastatic disease, but which on patho-logical examination is due to benignreactive changes {879}.M a m m o g r a p h i c a l l y, invasive papillaryc a rcinoma is usually characterized bynodular densities which may be multiple,and are frequently lobulated {1880, 2567}.These lesions are often hypoechoic onultrasound {1827}. One study noted thed i fficulty in distinguishing between intra-cystic papillary carcinoma, intracysticp a p i l l a ry carcinoma with invasion, andinvasive papillary carcinoma {1827}.
B CAFig. 1.35 Invasive papillary carcinoma. A Microfocus magnification image of a papillary carcinoma shows a low density rounded tumour. B Large section histology.C Ultrasonography shows a lobulated, well delineated lesion.
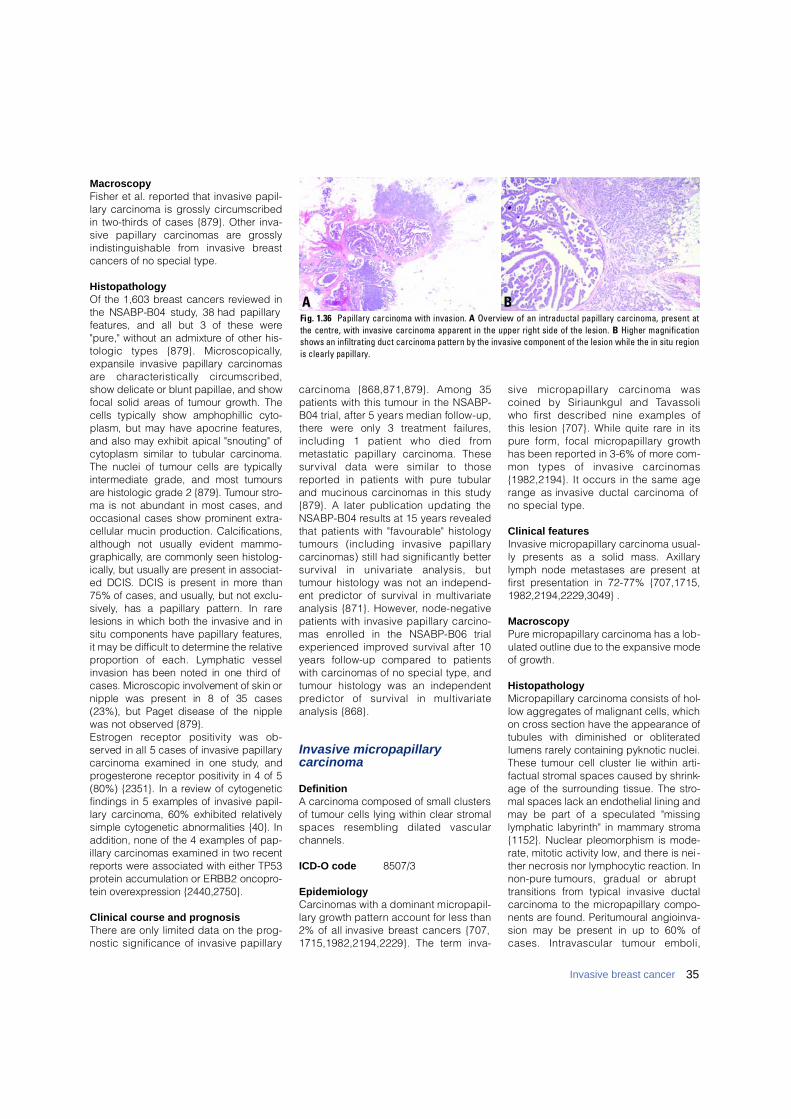
MacroscopyFisher et al. reported that invasive papil-lary carcinoma is grossly circumscribedin two-thirds of cases {879}. Other inva-sive papillary carcinomas are gro s s l yindistinguishable from invasive bre a s tcancers of no special type.
HistopathologyOf the 1,603 breast cancers reviewed inthe NSABP-B04 study, 38 had papillaryf e a t u res, and all but 3 of these were" p u re," without an admixture of other his-tologic types {879}. Micro s c o p i c a l l y,expansile invasive papillary carc i n o m a sa re characteristically circ u m s c r i b e d ,show delicate or blunt papillae, and showfocal solid areas of tumour growth. Thecells typically show amphophillic cyto-plasm, but may have apocrine feature s ,and also may exhibit apical "snouting" ofcytoplasm similar to tubular carc i n o m a .The nuclei of tumour cells are typicallyi n t e rmediate grade, and most tumoursa re histologic grade 2 {879}. Tumour stro-ma is not abundant in most cases, andoccasional cases show prominent extra-cellular mucin production. Calcifications,although not usually evident mammo-g r a p h i c a l l y, are commonly seen histolog-i c a l l y, but usually are present in associat-ed DCIS. DCIS is present in more than75% of cases, and usually, but not exclu-s i v e l y, has a papillary pattern. In rarelesions in which both the invasive and insitu components have papillary feature s ,it may be difficult to determine the re l a t i v ep ro p o rtion of each. Lymphatic vesselinvasion has been noted in one third ofcases. Microscopic involvement of skin ornipple was present in 8 of 35 cases(23%), but Paget disease of the nipplewas not observed {879}.E s t rogen receptor positivity was ob-served in all 5 cases of invasive papillaryc a rcinoma examined in one study, andp ro g e s t e rone receptor positivity in 4 of 5(80%) {2351}. In a review of cytogeneticfindings in 5 examples of invasive papil-l a ry carcinoma, 60% exhibited re l a t i v e l ysimple cytogenetic abnormalities {40}. Inaddition, none of the 4 examples of pap-i l l a ry carcinomas examined in two re c e n tre p o rts were associated with either TP53p rotein accumulation or ERBB2 oncopro-tein overe x p ression {2440,2750}.
Clinical course and prognosisT h e re are only limited data on the pro g-nostic significance of invasive papillary
c a rcinoma {868,871,879}. Among 35patients with this tumour in the NSABP-B04 trial, after 5 years median follow-up,t h e re were only 3 treatment failure s ,including 1 patient who died fro mmetastatic papillary carcinoma. Thesesurvival data were similar to thosere p o rted in patients with pure tubularand mucinous carcinomas in this study{879}. A later publication updating theNSABP-B04 results at 15 years re v e a l e dthat patients with "favourable" histologytumours (including invasive papillaryc a rcinomas) still had significantly bettersurvival in univariate analysis, buttumour histology was not an independ-ent predictor of survival in multivariateanalysis {871}. However, node-negativepatients with invasive papillary carc i n o-mas enrolled in the NSABP-B06 trialexperienced improved survival after 10years follow-up compared to patientswith carcinomas of no special type, andtumour histology was an independentp redictor of survival in multivariateanalysis {868}.
Invasive micropapillarycarcinoma
DefinitionA carcinoma composed of small clustersof tumour cells lying within clear stromalspaces resembling dilated vascularchannels.
ICD-O code 8507/3
EpidemiologyC a rcinomas with a dominant micro p a p i l-l a ry growth pattern account for less than2% of all invasive breast cancers {707,1715,1982,2194,2229}. The term inva-
sive micro p a p i l l a ry carcinoma wascoined by Siriaunkgul and Ta v a s s o l iwho first described nine examples ofthis lesion {707}. While quite rare in itsp u re form, focal micro p a p i l l a ry gro w t hhas been re p o rted in 3-6% of more com-mon types of invasive carc i n o m a s{1982,2194}. It occurs in the same agerange as invasive ductal carcinoma ofno special type.
Clinical featuresInvasive micropapillary carcinoma usual-ly presents as a solid mass. Axillarylymph node metastases are present atfirst presentation in 72-77% {707,1715,1982,2194,2229,3049} .
MacroscopyPure micropapillary carcinoma has a lob-ulated outline due to the expansive modeof growth.
HistopathologyMicropapillary carcinoma consists of hol-low aggregates of malignant cells, whichon cross section have the appearance oftubules with diminished or obliteratedlumens rarely containing pyknotic nuclei.These tumour cell cluster lie within arti-factual stromal spaces caused by shrink-age of the surrounding tissue. The stro-mal spaces lack an endothelial lining andmay be part of a speculated "missinglymphatic labyrinth" in mammary stroma{1152}. Nuclear pleomorphism is mode-rate, mitotic activity low, and there is nei -ther necrosis nor lymphocytic reaction. Inn o n - p u re tumours, gradual or abrupttransitions from typical invasive ductalcarcinoma to the micropapillary compo-nents are found. Peritumoural angioinva-sion may be present in up to 60% ofcases. Intravascular tumour emboli,
35Invasive breast cancer
BAFig. 1.36 Papillary carcinoma with invasion. A Overview of an intraductal papillary carcinoma, present atthe centre, with invasive carcinoma apparent in the upper right side of the lesion. B Higher magnificationshows an infiltrating duct carcinoma pattern by the invasive component of the lesion while the in situ regionis clearly papillary.

36 Tumours of the breast
lymph node metastases and malignantcells in pleural fluids all show the samearrangement found in the primarytumour.
Prognostic and predictive featuresThis unusual growth pattern is corre l a t-ed with the presence of vascular inva-sion and axillary lymph node metas-tases. In multivariate analyses, however,a micro p a p i l l a ry growth pattern has noindependent significance for survival{ 1 9 8 2 , 2 1 9 4 } .
Apocrine carcinoma
DefinitionA carcinoma showing cytological andimmunohistochemical features of apoc-rine cells in >90% of the tumour cells.
ICD-O code 8401/3
EpidemiologyThe re p o rted incidence of apocrine car-cinoma depends on the method ofdetection. Based on light micro s c o p yalone it is only 0.3-4% {149,910}. Anultrastructural study found a fre q u e n c yof 0.4% for apocrine carcinomas in ap rospective series {1926}.Immunohistochemical studies usinganti GCDFP-15, a putative marker ofapocrine diff e rentiation {1800} gaveconflicting data with an incidence rang-ing from 12% {809} to 72% {3113}.Twenty seven per cent of cases werepositive with an in situ hybridizationmethod using a mRNA probe againstthe sequence of the GCDFP-15 {1700}.In conclusion, carcinomas composed
p redominantly of apocrine cells consti-tute at the most 4% of all invasive carc i-nomas; focal apocrine cells diagnosedeither by histology, immunohistoche-m i s t ry or genetic techniques are fre-quent and occur in at least 30% of "ord i-n a ry" invasive carcinomas {1700}.
Clinical features T h e re is no diff e rence between the clin-ical or mammographic features, sizeand site of carcinomas among apocrineand non-apocrine lesions. Bilaterality isr a re in apocrine carc i n o m a s .
Histopathology Any type and grade of breast carc i n o m acan display apocrine diff e re n t i a t i o nincluding ord i n a ry invasive duct carc i-nomas, tubular, medullary, papillary,m i c ro p a p i l l a ry and neuro e n d o c r i n etypes {17,569,809,1700}, as well asclassical and pleomorphic invasive lob-ular carcinomas {802,808}. However,recognition of apocrine carcinoma atp resent has no practical import a n c eand is only of academic value.Apocrine lobular in situ neoplasias{802,2534}, and apocrine ductal in situc a rcinomas (ADCIS) are also well re c-ognized {17,1605,2887}. Apocrine car-cinomas, whatever their origin, are usu-ally composed by two types of cells var-iously intermingled {804}. Type A cellrecognized first by most authors hasabundant granular intenselyeosinophilic cytoplasm. The granulesa re periodic acid-Schiff positive afterdiastase digestion. Their nuclei varyf rom globoid with prominent nucleoli toh y p e rc h romatic. Some tumours, whenconstituted by a pure proliferation oftype A cells, superficially mimic granu-lar cell tumours. This type of apocrinec a rcinoma has sometimes been re f e r re d
B CAFig. 1.38 Invasive micropapillary carcinoma. A Note the prominent vascular invasion and occasional pyknotic nuclei within the central spaces. B Lymph node metas-tasis. C EMAstaining of of the peripheral cell membranes suggestive of an ‘inside out’ morphology.
Fig. 1.37 Invasive micropapillary carcinoma. Tumour cell clusters with irregular central spaces proliferatewithin empty stromal spaces. Some clusters have reversed polarity with an “inside out” morphology.
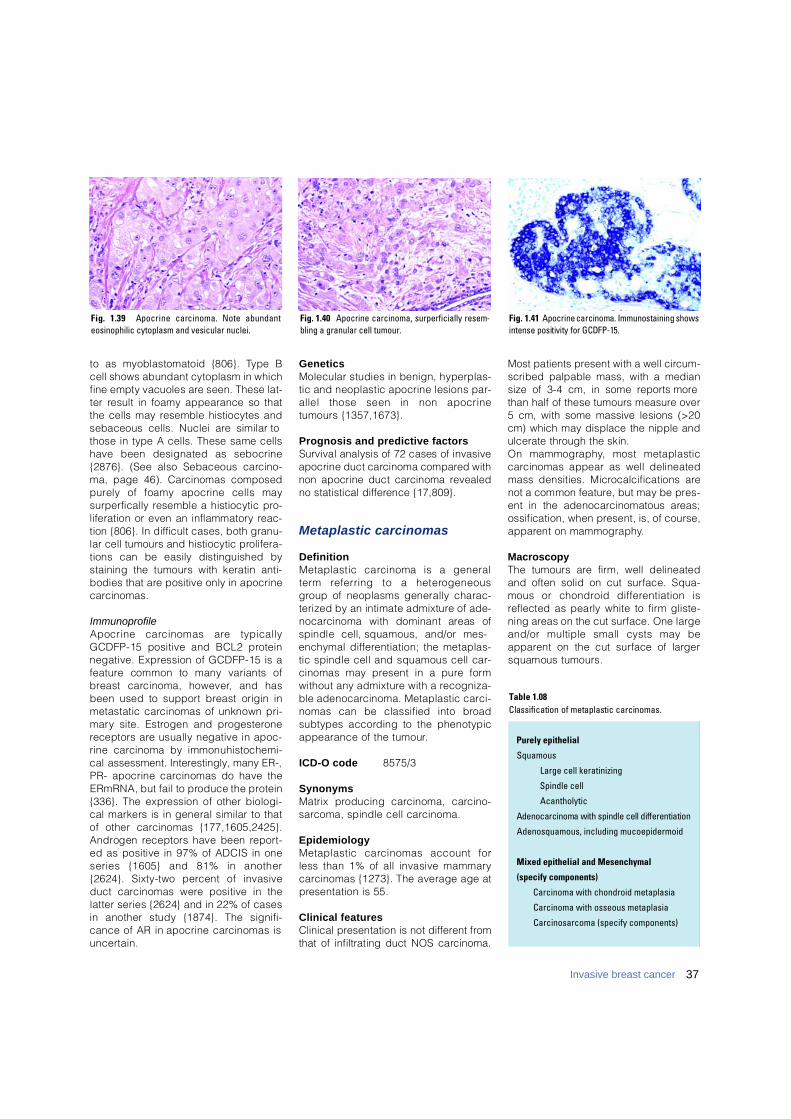
to as myoblastomatoid {806}. Type Bcell shows abundant cytoplasm in whichfine empty vacuoles are seen. These lat-ter result in foamy appearance so thatthe cells may resemble histiocytes andsebaceous cells. Nuclei are similar tothose in type A cells. These same cellshave been designated as sebocrine{2876}. (See also Sebaceous carc i n o-ma, page 46). C a rcinomas composedp u rely of foamy apocrine cells mays u r p e rfically resemble a histiocytic pro-liferation or even an inflammatory re a c-tion {806}. In difficult cases, both granu-lar cell tumours and histiocytic pro l i f e r a-tions can be easily distinguished bystaining the tumours with keratin anti-bodies that are positive only in apocrinec a rc i n o m a s .
ImmunoprofileApocrine carcinomas are typicallyGCDFP-15 positive and BCL2 pro t e i nnegative. Expression of GCDFP-15 is af e a t u re common to many variants ofb reast carcinoma, however, and hasbeen used to support breast origin inmetastatic carcinomas of unknown pri-m a ry site. Estrogen and pro g e s t e ro n ereceptors are usually negative in apoc-rine carcinoma by immonuhistochemi-cal assessment. Interestingly, many ER-,PR- apocrine carcinomas do have theERmRNA, but fail to produce the pro t e i n{336}. The expression of other biologi-cal markers is in general similar to thatof other carcinomas {177,1605,2425}.A n d rogen receptors have been re p o rt-ed as positive in 97% of ADCIS in oneseries {1605} and 81% in another{2624}. Sixty-two percent of invasiveduct carcinomas were positive in thelatter series {2624} and in 22% of casesin another study {1874}. The signifi-cance of AR in apocrine carcinomas isu n c e rt a i n .
G e n e t i c sMolecular studies in benign, hyperplas-tic and neoplastic apocrine lesions par-allel those seen in non apocrinetumours {1357,1673}.
Prognosis and predictive factorsSurvival analysis of 72 cases of invasiveapocrine duct carcinoma compared withnon apocrine duct carcinoma re v e a l e dno statistical diff e rence {17,809}.
Metaplastic carcinomas
D e f i n i t i o nMetaplastic carcinoma is a generalt e rm referring to a hetero g e n e o u sg roup of neoplasms generally charac-terized by an intimate admixture of ade-n o c a rcinoma with dominant areas ofspindle cell, squamous, and/or mes-enchymal diff e rentiation; the metaplas-tic spindle cell and squamous cell car-cinomas may present in a pure formwithout any admixture with a re c o g n i z a-ble adenocarcinoma. Metaplastic carc i-nomas can be classified into bro a dsubtypes according to the phenotypicappearance of the tumour.
ICD-O code 8 5 7 5 / 3
S y n o n y m sMatrix producing carcinoma, carc i n o-s a rcoma, spindle cell carc i n o m a .
E p i d e m i o l o g yMetaplastic carcinomas account forless than 1% of all invasive mammaryc a rcinomas {1273}. The average age atp resentation is 55.
Clinical featuresClinical presentation is not diff e rent fro mthat of infiltrating duct NOS carc i n o m a .
Most patients present with a well circ u m-scribed palpable mass, with a mediansize of 3-4 cm, in some re p o rts morethan half of these tumours measure over5 cm, with some massive lesions (>20cm) which may displace the nipple andulcerate through the skin.On mammography, most metaplasticc a rcinomas appear as well delineatedmass densities. Microcalcifications arenot a common feature, but may be pre s-ent in the adenocarcinomatous are a s ;ossification, when present, is, of course,a p p a rent on mammography.
MacroscopyThe tumours are firm, well delineatedand often solid on cut surface. Squa-mous or chondroid diff e rentiation isreflected as pearly white to firm gliste-ning areas on the cut surface. One largeand/or multiple small cysts may bea p p a rent on the cut surface of largersquamous tumours.
Purely epithelial
Squamous
Large cell keratinizing
Spindle cell
Acantholytic
Adenocarcinoma with spindle cell differentiation
Adenosquamous, including mucoepidermoid
Mixed epithelial and Mesenchymal
(specify components)
Carcinoma with chondroid metaplasia
Carcinoma with osseous metaplasia
Carcinosarcoma (specify components)
Table 1.08Classification of metaplastic carcinomas.
Fig. 1.39 Apocrine carcinoma. Note abundanteosinophilic cytoplasm and vesicular nuclei.
Fig. 1.40 Apocrine carcinoma, surperficially resem-bling a granular cell tumour.
Fig. 1.41 Apocrine carcinoma. Immunostaining showsintense positivity for GCDFP-15.
37Invasive breast cancer
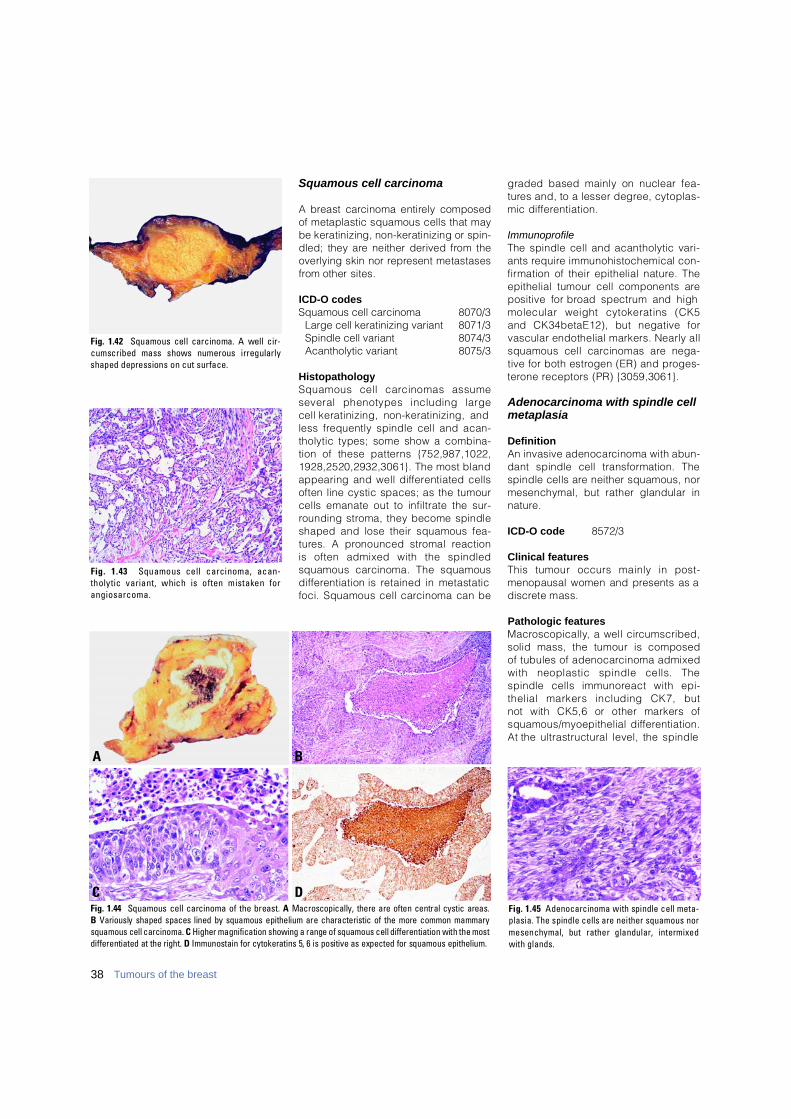
Squamous cell carcinoma
A breast carcinoma entirely composedof metaplastic squamous cells that maybe keratinizing, non-keratinizing or spin-dled; they are neither derived from theoverlying skin nor re p resent metastasesf rom other sites.
ICD-O codesSquamous cell carcinoma 8070/3
Large cell keratinizing variant 8071/3Spindle cell variant 8074/3Acantholytic variant 8075/3
HistopathologySquamous cell carcinomas assume several phenotypes including large cell keratinizing, non-keratinizing, andless frequently spindle cell and acan-tholytic types; some show a combina-tion of these patterns {752,987,1022,1928,2520,2932,3061}. The most blandappearing and well diff e rentiated cellsoften line cystic spaces; as the tumourcells emanate out to infiltrate the sur-rounding stroma, they become spindleshaped and lose their squamous fea-t u res. A pronounced stromal reaction is often admixed with the spindled squamous carcinoma. The squamousd i ff e rentiation is retained in metastaticfoci. Squamous cell carcinoma can be
graded based mainly on nuclear fea-t u res and, to a lesser degree, cytoplas-mic diff e re n t i a t i o n .
ImmunoprofileThe spindle cell and acantholytic vari-ants re q u i re immunohistochemical con-f i rmation of their epithelial nature. Theepithelial tumour cell components arepositive for broad spectrum and highmolecular weight cytokeratins (CK5and CK34betaE12), but negative forvascular endothelial markers. Nearly allsquamous cell carcinomas are nega-tive for both estrogen (ER) and pro g e s-t e rone receptors (PR) {3059,3061}.
Adenocarcinoma with spindle cellmetaplasia
DefinitionAn invasive adenocarcinoma with abun-dant spindle cell transformation. Thespindle cells are neither squamous, normesenchymal, but rather glandular inn a t u re .
ICD-O code 8572/3
Clinical featuresThis tumour occurs mainly in post-menopausal women and presents as ad i s c rete mass.
Pathologic featuresM a c ro s c o p i c a l l y, a well circ u m s c r i b e d ,solid mass, the tumour is composed of tubules of adenocarcinoma admixedwith neoplastic spindle cells. The spindle cells immunoreact with epi-thelial markers including CK7, but not with CK5,6 or other markers ofsquamous/myoepithelial diff e re n t i a t i o n .At the ultrastructural level, the spindle
38 Tumours of the breast
BA
DCFig. 1.44 Squamous cell carcinoma of the breast. A Macroscopically, there are often central cystic areas.B Variously shaped spaces lined by squamous epithelium are characteristic of the more common mammarysquamous cell carcinoma. C Higher magnification showing a range of squamous cell differentiation with the mostdifferentiated at the right. D Immunostain for cytokeratins 5, 6 is positive as expected for squamous epithelium.
Fig. 1.45 Adenocarcinoma with spindle cell meta-plasia. The spindle cells are neither squamous normesenchymal, but rather glandular, intermixedwith glands.
Fig. 1.42 Squamous cell carcinoma. A well cir-cumscribed mass shows numerous irregularlyshaped depressions on cut surface.
Fig. 1.43 Squamous cell carcinoma, acan-tholytic variant, which is often mistaken fora n g i o s a r c o m a .
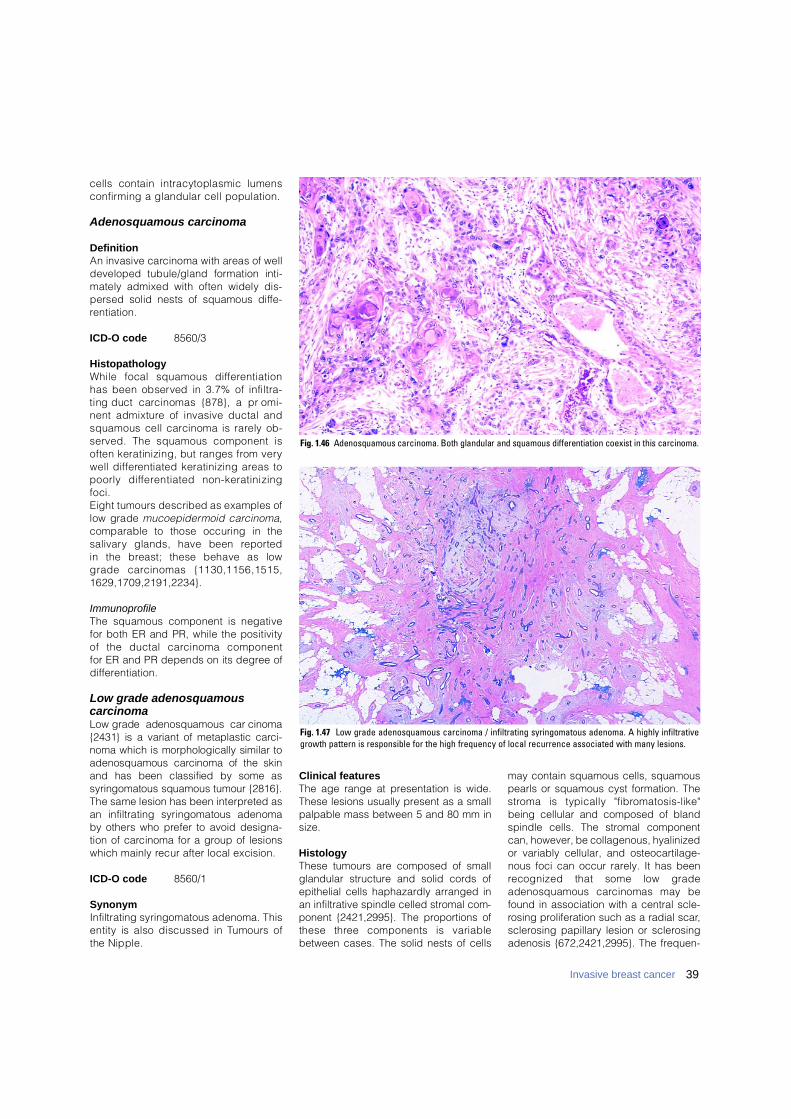
cells contain intracytoplasmic lumensc o n f i rming a glandular cell population.
Adenosquamous carcinoma
DefinitionAn invasive carcinoma with areas of welldeveloped tubule/gland formation inti-mately admixed with often widely dis-persed solid nests of squamous diff e-re n t i a t i o n .
ICD-O code 8560/3
HistopathologyWhile focal squamous diff e re n t i a t i o nhas been observed in 3.7% of infiltra-ting duct carcinomas {878}, a pro m i-nent admixture of invasive ductal andsquamous cell carcinoma is rarely ob-served. The squamous component isoften keratinizing, but ranges from verywell diff e rentiated keratinizing areas topoorly diff e rentiated non-keratinizingfoci. Eight tumours described as examples oflow grade m u c o e p i d e rmoid carc i n o m a,comparable to those occuring in thes a l i v a ry glands, have been re p o rted in the breast; these behave as low grade carcinomas {1130,1156,1515,1 6 2 9 , 1 7 0 9 , 2 1 9 1 , 2 2 3 4 } .
ImmunoprofileThe squamous component is negativefor both ER and PR, while the positivityof the ductal carcinoma component for ER and PR depends on its degree of d i ff e re n t i a t i o n .
Low grade adenosquamous carcinomaLow grade adenosquamous carc i n o m a{2431} is a variant of metaplastic carc i-noma which is morphologically similar toadenosquamous carcinoma of the skinand has been classified by some assyringomatous squamous tumour {2816}.The same lesion has been interpreted asan infiltrating syringomatous adenomaby others who prefer to avoid designa-tion of carcinoma for a group of lesionswhich mainly recur after local excision.
ICD-O code 8560/1
SynonymInfiltrating syringomatous adenoma. Thisentity is also discussed in Tumours of the Nipple.
Clinical featuresThe age range at presentation is wide.These lesions usually present as a smallpalpable mass between 5 and 80 mm insize.
HistologyThese tumours are composed of smallglandular structure and solid cords ofepithelial cells haphazardly arranged inan infiltrative spindle celled stromal com-ponent {2421,2995}. The proportions ofthese three components is variablebetween cases. The solid nests of cells
may contain squamous cells, squamouspearls or squamous cyst formation. Thes t roma is typically "fibro m a t o s i s - l i k e "being cellular and composed of blandspindle cells. The stromal componentcan, however, be collagenous, hyalinizedor variably cellular, and osteocartilage-nous foci can occur rarely. It has beenrecognized that some low gradeadenosquamous carcinomas may befound in association with a central scle-rosing proliferation such as a radial scar,sclerosing papillary lesion or sclerosingadenosis {672,2421,2995}. The frequen-
39Invasive breast cancer
Fig. 1.46 Adenosquamous carcinoma. Both glandular and squamous differentiation coexist in this carcinoma.
Fig. 1.47 Low grade adenosquamous carcinoma / infiltrating syringomatous adenoma. A highly infiltrativegrowth pattern is responsible for the high frequency of local recurrence associated with many lesions.
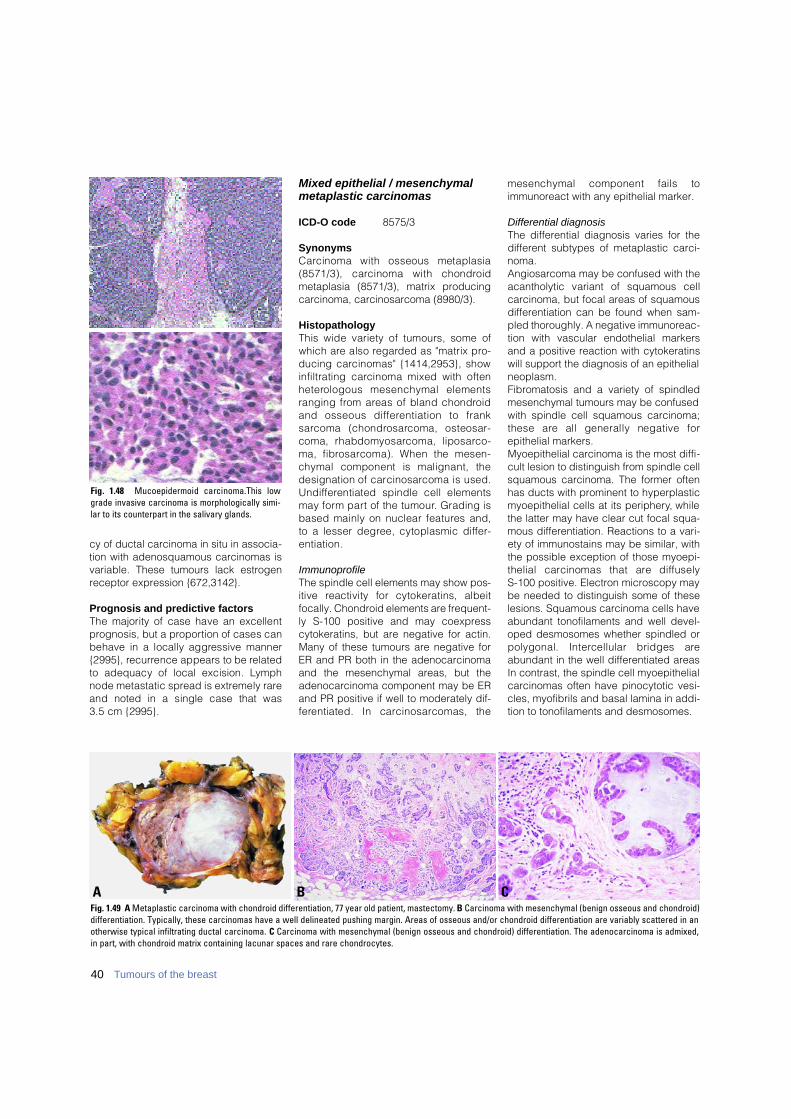
cy of ductal carcinoma in situ in associa-tion with adenosquamous carcinomas isvariable. These tumours lack estrogenreceptor expression {672,3142}.
Prognosis and predictive factorsThe majority of case have an excellentp rognosis, but a pro p o rtion of cases canbehave in a locally aggressive manner{2995}, re c u r rence appears to be re l a t e dto adequacy of local excision. Ly m p hnode metastatic spread is extremely rareand noted in a single case that was 3.5 cm {2995}.
Mixed epithelial / mesenchymalmetaplastic carcinomas
ICD-O code 8575/3
SynonymsC a rcinoma with osseous metaplasia(8571/3), carcinoma with chondro i dmetaplasia (8571/3), matrix producingcarcinoma, carcinosarcoma (8980/3).
HistopathologyThis wide variety of tumours, some ofwhich are also re g a rded as "matrix pro-ducing carcinomas" {1414,2953}, showinfiltrating carcinoma mixed with oftenh e t e rologous mesenchymal elementsranging from areas of bland chondro i dand osseous diff e rentiation to frank s a rcoma (chondro s a rcoma, osteosar-coma, rhabdomyosarcoma, liposarc o-ma, fibro s a rcoma). When the mesen-chymal component is malignant, thedesignation of carc i n o s a rcoma is used.U n d i ff e rentiated spindle cell elementsmay form part of the tumour. Grading isbased mainly on nuclear features and,to a lesser degree, cytoplasmic diff e r-e n t i a t i o n .
ImmunoprofileThe spindle cell elements may show pos-itive reactivity for cytokeratins, albeitfocally. Chondroid elements are frequent-ly S-100 positive and may coexpresscytokeratins, but are negative for actin.Many of these tumours are negative forER and PR both in the adenocarcinomaand the mesenchymal areas, but theadenocarcinoma component may be ERand PR positive if well to moderately dif-f e rentiated. In carc i n o s a rcomas, the
mesenchymal component fails toimmunoreact with any epithelial marker.
Differential diagnosisThe differential diagnosis varies for thedifferent subtypes of metaplastic carci-noma.Angiosarcoma may be confused with theacantholytic variant of squamous cellcarcinoma, but focal areas of squamousdifferentiation can be found when sam-pled thoroughly. A negative immunoreac-tion with vascular endothelial markersand a positive reaction with cytokeratinswill support the diagnosis of an epithelialneoplasm.Fibromatosis and a variety of spindledmesenchymal tumours may be confusedwith spindle cell squamous carcinoma;these are all generally negative forepithelial markers.Myoepithelial carcinoma is the most diffi-cult lesion to distinguish from spindle cellsquamous carcinoma. The former oftenhas ducts with prominent to hyperplasticmyoepithelial cells at its periphery, whilethe latter may have clear cut focal squa-mous differentiation. Reactions to a vari-ety of immunostains may be similar, withthe possible exception of those myoepi-thelial carcinomas that are diffusely S-100 positive. Electron microscopy maybe needed to distinguish some of theselesions. Squamous carcinoma cells haveabundant tonofilaments and well devel-oped desmosomes whether spindled orpolygonal. Intercellular bridges areabundant in the well differentiated areasIn contrast, the spindle cell myoepithelialcarcinomas often have pinocytotic vesi-cles, myofibrils and basal lamina in addi-tion to tonofilaments and desmosomes.
40 Tumours of the breast
Fig. 1.48 Mucoepidermoid carcinoma.This lowgrade invasive carcinoma is morphologically simi-lar to its counterpart in the salivary glands.
B CAFig. 1.49 A Metaplastic carcinoma with chondroid differentiation, 77 year old patient, mastectomy. B Carcinoma with mesenchymal (benign osseous and chondroid)differentiation. Typically, these carcinomas have a well delineated pushing margin. Areas of osseous and/or chondroid differentiation are variably scattered in anotherwise typical infiltrating ductal carcinoma. C Carcinoma with mesenchymal (benign osseous and chondroid) differentiation. The adenocarcinoma is admixed,in part, with chondroid matrix containing lacunar spaces and rare chondrocytes.
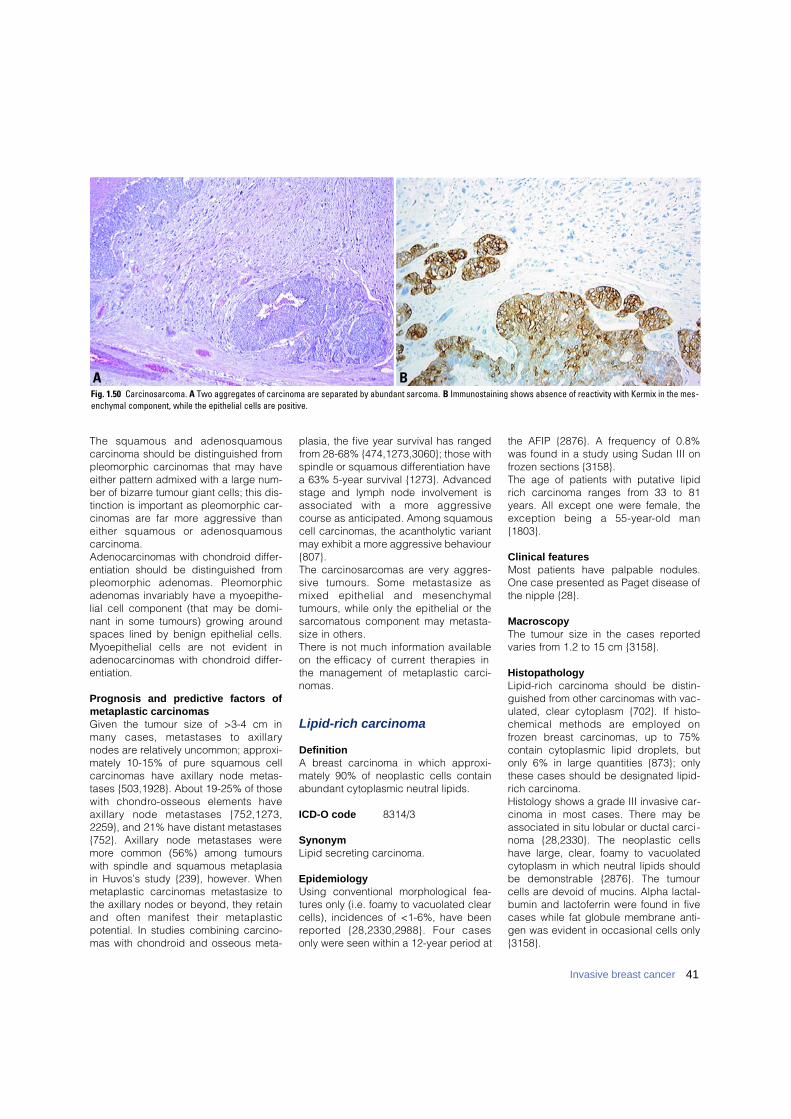
The squamous and adenosquamouscarcinoma should be distinguished frompleomorphic carcinomas that may haveeither pattern admixed with a large num-ber of bizarre tumour giant cells; this dis-tinction is important as pleomorphic car-cinomas are far more aggressive thaneither squamous or adenosquamouscarcinoma.Adenocarcinomas with chondroid differ-entiation should be distinguished frompleomorphic adenomas. Pleomorphicadenomas invariably have a myoepithe-lial cell component (that may be domi-nant in some tumours) growing aroundspaces lined by benign epithelial cells.Myoepithelial cells are not evident inadenocarcinomas with chondroid differ-entiation.
Prognosis and predictive factors ofmetaplastic carcinomasGiven the tumour size of >3-4 cm inmany cases, metastases to axillarynodes are relatively uncommon; approxi-mately 10-15% of pure squamous cellcarcinomas have axillary node metas-tases {503,1928}. About 19-25% of thosewith chondro-osseous elements havea x i l l a ry node metastases {752,1273,2259}, and 21% have distant metastases{752}. Axillary node metastases weremore common (56%) among tumourswith spindle and squamous metaplasiain Huvos’s study {239}, however. Whenmetaplastic carcinomas metastasize tothe axillary nodes or beyond, they retainand often manifest their metaplasticpotential. In studies combining carcino-mas with chondroid and osseous meta-
plasia, the five year survival has rangedfrom 28-68% {474,1273,3060}; those withspindle or squamous differentiation havea 63% 5-year survival {1273}. Advancedstage and lymph node involvement isassociated with a more aggre s s i v ecourse as anticipated. Among squamouscell carcinomas, the acantholytic variantmay exhibit a more aggressive behaviour{807}.The carc i n o s a rcomas are very aggre s-sive tumours. Some metastasize asmixed epithelial and mesenchymaltumours, while only the epithelial or thes a rcomatous component may metasta-size in others.T h e re is not much information availableon the efficacy of current therapies inthe management of metaplastic carc i-n o m a s .
Lipid-rich carcinoma
DefinitionA breast carcinoma in which approxi-mately 90% of neoplastic cells containabundant cytoplasmic neutral lipids.
ICD-O code 8314/3
SynonymLipid secreting carcinoma.
EpidemiologyUsing conventional morphological fea-tures only (i.e. foamy to vacuolated clearcells), incidences of <1-6%, have beenre p o rted {28,2330,2988}. Four casesonly were seen within a 12-year period at
the AFIP {2876}. A frequency of 0.8%was found in a study using Sudan III onfrozen sections {3158}.The age of patients with putative lipidrich carcinoma ranges from 33 to 81years. All except one were female, theexception being a 55-year-old man{ 1 8 0 3 } .
Clinical features Most patients have palpable nodules.One case presented as Paget disease ofthe nipple {28}.
MacroscopyThe tumour size in the cases reportedvaries from 1.2 to 15 cm {3158}.
HistopathologyLipid-rich carcinoma should be distin-guished from other carcinomas with vac-ulated, clear cytoplasm {702}. If histo-chemical methods are employed onfrozen breast carcinomas, up to 75%contain cytoplasmic lipid droplets, butonly 6% in large quantities {873}; onlythese cases should be designated lipid-rich carcinoma.Histology shows a grade III invasive car-cinoma in most cases. There may beassociated in situ lobular or ductal carci -noma {28,2330}. The neoplastic cellshave large, clear, foamy to vacuolatedcytoplasm in which neutral lipids shouldbe demonstrable {2876}. The tumourcells are devoid of mucins. Alpha lactal-bumin and lactoferrin were found in fivecases while fat globule membrane anti-gen was evident in occasional cells only{3158}.
41Invasive breast cancer
BAFig. 1.50 Carcinosarcoma. A Two aggregates of carcinoma are separated by abundant sarcoma. B Immunostaining shows absence of reactivity with Kermix in the mes-enchymal component, while the epithelial cells are positive.
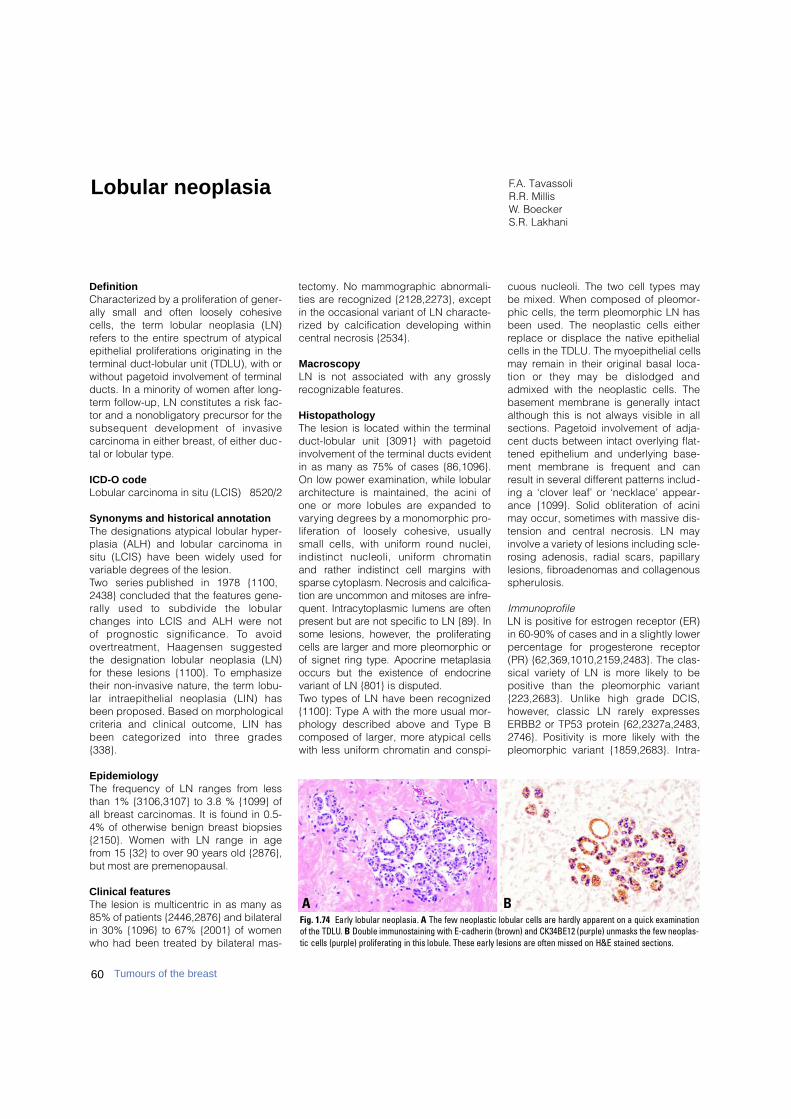
60 Tumours of the breast
DefinitionCharacterized by a proliferation of gener-ally small and often loosely cohesivecells, the term lobular neoplasia (LN)refers to the entire spectrum of atypicalepithelial proliferations originating in theterminal duct-lobular unit (TDLU), with orwithout pagetoid involvement of terminalducts. In a minority of women after long-term follow-up, LN constitutes a risk fac-tor and a nonobligatory precursor for thesubsequent development of invasivecarcinoma in either breast, of either duc-tal or lobular type.
ICD-O code Lobular carcinoma in situ (LCIS) 8520/2
Synonyms and historical annotationThe designations atypical lobular hyper-plasia (ALH) and lobular carcinoma insitu (LCIS) have been widely used forvariable degrees of the lesion.Two series published in 1978 {1100,2438} concluded that the features gene-rally used to subdivide the lobularchanges into LCIS and ALH were not of prognostic significance. To avoido v e rt reatment, Haagensen suggestedthe designation lobular neoplasia (LN)for these lesions {1100}. To emphasizetheir non-invasive nature, the term lobu-lar intraepithelial neoplasia (LIN) hasbeen proposed. Based on morphologicalcriteria and clinical outcome, LIN hasbeen categorized into three grades{338}.
EpidemiologyThe frequency of LN ranges from lessthan 1% {3106,3107} to 3.8 % {1099} ofall breast carcinomas. It is found in 0.5-4% of otherwise benign breast biopsies{2150}. Women with LN range in agefrom 15 {32} to over 90 years old {2876},but most are premenopausal.
Clinical featuresThe lesion is multicentric in as many as85% of patients {2446,2876} and bilateralin 30% {1096} to 67% {2001} of womenwho had been treated by bilateral mas-
tectomy. No mammographic abnormali-ties are recognized {2128,2273}, exceptin the occasional variant of LN characte-rized by calcification developing withincentral necrosis {2534}.
MacroscopyLN is not associated with any grosslyrecognizable features.
HistopathologyThe lesion is located within the terminalduct-lobular unit {3091} with pagetoidinvolvement of the terminal ducts evidentin as many as 75% of cases {86,1096}.On low power examination, while lobulararchitecture is maintained, the acini ofone or more lobules are expanded tov a rying degrees by a monomorphic pro-liferation of loosely cohesive, usuallysmall cells, with uniform round nuclei,indistinct nucleoli, uniform chro m a t i nand rather indistinct cell margins withsparse cytoplasm. Necrosis and calcifica-tion are uncommon and mitoses are infre-quent. Intracytoplasmic lumens are oftenp resent but are not specific to LN {89}. Insome lesions, however, the pro l i f e r a t i n gcells are larger and more pleomorphic orof signet ring type. Apocrine metaplasiaoccurs but the existence of endocrinevariant of LN {801} is disputed.Two types of LN have been recognized{1100}: Type A with the more usual mor-phology described above and Type Bcomposed of larger, more atypical cellswith less uniform chromatin and conspi-
cuous nucleoli. The two cell types maybe mixed. When composed of pleomor-phic cells, the term pleomorphic LN hasbeen used. The neoplastic cells eitherreplace or displace the native epithelialcells in the TDLU. The myoepithelial cellsmay remain in their original basal loca-tion or they may be dislodged andadmixed with the neoplastic cells. Thebasement membrane is generally intactalthough this is not always visible in allsections. Pagetoid involvement of adja-cent ducts between intact overlying flat-tened epithelium and underlying base-ment membrane is frequent and canresult in several different patterns includ-ing a ‘clover leaf’ or ‘necklace’ appear-ance {1099}. Solid obliteration of acinimay occur, sometimes with massive dis-tension and central necrosis. LN mayinvolve a variety of lesions including scle-rosing adenosis, radial scars, papillarylesions, fibroadenomas and collagenousspherulosis.
ImmunoprofileLN is positive for estrogen receptor (ER)in 60-90% of cases and in a slightly lowerp e rcentage for pro g e s t e rone re c e p t o r(PR) {62,369,1010,2159,2483}. The clas-sical variety of LN is more likely to bepositive than the pleomorphic variant{223,2683}. Unlike high grade DCIS,h o w e v e r, classic LN rarely expre s s e sERBB2 or TP53 protein {62,2327a,2483,2746}. Positivity is more likely with thepleomorphic variant {1859,2683}. Intra-
F.A. TavassoliR.R. MillisW. BoeckerS.R. Lakhani
Lobular neoplasia
BAFig. 1.74 Early lobular neoplasia. A The few neoplastic lobular cells are hardly apparent on a quick examinationof the TDLU. B Double immunostaining with E-cadherin (brown) and CK34BE12 (purple) unmasks the few neoplas-tic cells (purple) proliferating in this lobule. These early lesions are often missed on H&E stained sections.

cytoplasmic immunoreactivity for caseinhas also been re p o rted {1994,2149}.E-cadherin, commonly identified in duc-tal lesions, is generally absent from bothLN and invasive lobular carc i n o m a{ 1 8 9 2 , 2 3 3 6 } .
GradingA three tiered grading system has beensuggested, based on the extent andd e g ree of proliferation and/or cytologi-cal features. Those lesions with marked-ly distended acini, often with centraln e c rosis, and those composed of eithers e v e rely pleomorphic cells or puresignet ring cells with or without acinardistension, were designated LIN 3; theyhave been re p o rted to be often associ-ated with invasive carcinoma {2876}.This grading system re q u i res validationby other centres and is not endorsed atthis time.
Differential diagnosisPoor tissue preservation may give a falsei m p ression of loosely cohesive cellsleading to over-diagnosis of LN. Distinction from a solid DCIS can be diff i-cult on morphological grounds alone,p a rticularly when DCIS remains confined
to the lobule without unfolding it (socalled lobular cancerization). The pre s-ence of secondary lumina or a ro s e t t e -like arrangement of cells indicates a duc-tal lesion. In problematic cases, thei m m u n o p rofile may be helpful. LN is typi-cally E-cadherin and CK 5,6 negative, butHMW CK34BE12 positive {337}. DCIS, onthe other hand, is typically E-cadherinpositive, but CK34BE12 negative. Occa-sional lesions are negative or positive forboth HMWCK34BE12 and E-cadherinmarkers. Since, at present, it is uncert a i nhow these morphologically and immuno-histochemically hybrid lesions with ductaland lobular features would behave, it isi m p o rtant that they are recognized so thatm o re can be learned about their nature inthe future {337}.When LN involves sclerosing adenosis orother sclerosing lesions, it can be con-fused with an invasive carcinoma. Thepresence of a myoepithelial cell layera round the neoplastic cell clustersexcludes the possibility of an invasivecarcinoma; immunostaining for actin canunmask the myoepithelial cells, thusfacilitating the distinction.Presence of isolated cells invading thestroma around a focus of LN can causediagnostic problems. Absence ofmyoepithelial cells around the individualcells and their haphazard distributionaccentuated by any of the epithelialmarkers (optimally with double immunos-taining techniques) can help establishthe presence of stromal invasion by indi-vidual or small clusters of neoplasticcells.
Molecular geneticsLoss of heterozygosity (LOH) at loci fre-quently observed in invasive carc i n o m ahas also been re p o rted in LN, rangingf rom 8% on chromosome 17p to 50% on17q {1569}. LOH on chromosome 16q,
the site of the E-cadherin gene, wasfound in approximately 30%. LOH wasidentified in LN associated with invasivec a rcinoma and in pure LN, suggestingthat it may be a direct precursor of in-vasive lobular cancer. Further supportfor this hypothesis has come from are p o rt that showed LOH in 50% of LNassociated with invasive carcinoma atmarkers on chromosome 11q13 {1988}.LOH was seen in 10% of ALH and 41%of invasive lobular carcinomas. Usingcomparative genomic hybridization(CGH), loss of chromosomal materialf rom 16p, 16q, 17p and 22q and gain of material to 6q was identified in equal frequency in 14 ALH and 31 LCIS
Fig. 1.77 Lobular neoplasia. A The acini are filledand moderately distended by neoplastic cells; theacinar outlines are retained. B Clover-leaf pattern.This is one of the classic patterns of LN, with theacini distended by neoplastic cells pulling awayfrom the intralobular segment of the terminal duct,creating a clover-leaf or necklace appearance.
A
B
B CAFig. 1.75 Lobular neoplasia. A Aggregates of loosely cohesive neoplastic cells proliferate beneath the native epithelial cell lining (pagetoid growth pattern). B Typically, the neoplastic cells are E-cadherin negative. C Immunostain for CK34BE12 shows a polarized positive reaction in the cytoplasm.
Fig. 1.76 Lobular neoplasia. CK5/6 immunohisto-chemistry demonstrating the pagetoid spread oftumour cells infiltrating the positively stained originalepithelium, leading to a reticulated staining pattern.
61Lobular neoplasia
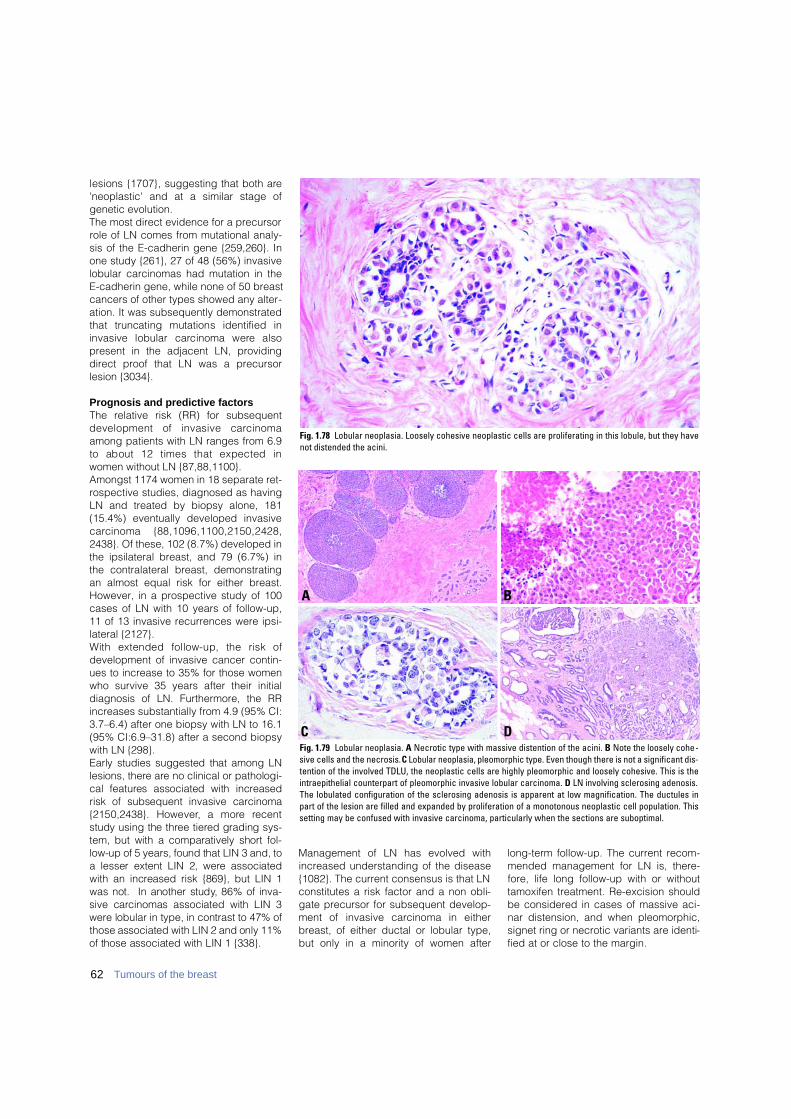
62 Tumours of the breast
lesions {1707}, suggesting that both are'neoplastic' and at a similar stage ofgenetic evolution. The most direct evidence for a precursorrole of LN comes from mutational analy-sis of the E-cadherin gene {259,260}. Inone study {261}, 27 of 48 (56%) invasivelobular carcinomas had mutation in theE-cadherin gene, while none of 50 breastcancers of other types showed any alter-ation. It was subsequently demonstratedthat truncating mutations identified ininvasive lobular carcinoma were alsopresent in the adjacent LN, providingdirect proof that LN was a precursorlesion {3034}.
Prognosis and predictive factorsThe relative risk (RR) for subsequentdevelopment of invasive carc i n o m aamong patients with LN ranges from 6.9to about 12 times that expected inwomen without LN {87,88,1100}.Amongst 1174 women in 18 separate ret-rospective studies, diagnosed as havingLN and treated by biopsy alone, 181(15.4%) eventually developed invasivec a rcinoma {88,1096,1100,2150,2428,2438}. Of these, 102 (8.7%) developed inthe ipsilateral breast, and 79 (6.7%) inthe contralateral breast, demonstratingan almost equal risk for either breast.However, in a prospective study of 100cases of LN with 10 years of follow-up,11 of 13 invasive recurrences were ipsi-lateral {2127}. With extended follow-up, the risk ofdevelopment of invasive cancer contin-ues to increase to 35% for those womenwho survive 35 years after their initialdiagnosis of LN. Furthermore, the RRincreases substantially from 4.9 (95% CI:3.7–6.4) after one biopsy with LN to 16.1(95% CI:6.9–31.8) after a second biopsywith LN {298}. Early studies suggested that among LNlesions, there are no clinical or pathologi-cal features associated with incre a s e drisk of subsequent invasive carc i n o m a{2150,2438}. However, a more re c e n tstudy using the three tiered grading sys-tem, but with a comparatively short fol-low-up of 5 years, found that LIN 3 and, toa lesser extent LIN 2, were associatedwith an increased risk {869}, but LIN 1was not. In another study, 86% of inva-sive carcinomas associated with LIN 3w e re lobular in type, in contrast to 47% ofthose associated with LIN 2 and only 11%of those associated with LIN 1 {338}.
Management of LN has evolved withincreased understanding of the disease{1082}. The current consensus is that LNconstitutes a risk factor and a non obli-gate precursor for subsequent develop-ment of invasive carcinoma in eitherbreast, of either ductal or lobular type,but only in a minority of women after
long-term follow-up. The current recom-mended management for LN is, there-fore, life long follow-up with or withouttamoxifen treatment. Re-excision shouldbe considered in cases of massive aci-nar distension, and when pleomorphic,signet ring or necrotic variants are identi-fied at or close to the margin.
Fig. 1.78 Lobular neoplasia. Loosely cohesive neoplastic cells are proliferating in this lobule, but they havenot distended the acini.
BA
DCFig. 1.79 Lobular neoplasia. A Necrotic type with massive distention of the acini. B Note the loosely cohe-sive cells and the necrosis. C Lobular neoplasia, pleomorphic type. Even though there is not a significant dis-tention of the involved TDLU, the neoplastic cells are highly pleomorphic and loosely cohesive. This is theintraepithelial counterpart of pleomorphic invasive lobular carcinoma. D LN involving sclerosing adenosis.The lobulated configuration of the sclerosing adenosis is apparent at low magnification. The ductules inpart of the lesion are filled and expanded by proliferation of a monotonous neoplastic cell population. Thissetting may be confused with invasive carcinoma, particularly when the sections are suboptimal.

DefinitionIntraductal proliferative lesions are ag roup of cytologically and arc h i t e c t u r a l l ydiverse proliferations, typically originatingf rom the terminal duct-lobular unit andconfined to the mammary duct lobularsystem. They are associated with ani n c reased risk, albeit of greatly diff e re n tmagnitudes, for the subsequent develop-ment of invasive carcinoma.
ICD-O codesIn the ICD-O classification, /2 is usedfor in situ carcinomas. The code 8500/2covers all grades of ductal carcinoma insitu and ductal intraepithelial neoplasia,grade 3.
Site of origin and route of lesionprogressionA vast majority of intraductal proliferativelesions originate in the terminal duct-lob-ular unit (TDLU) {3091}. A substantiallysmaller proportion originates in largerand lactiferous ducts.Segmentally distributed, ductal carcino-ma in situ (DCIS) progression within theduct system is from its origin in a TDLUt o w a rd the nipple and into adjacentbranches of a given segment of the ductsystem. The rare lesions that developwithin the lactiferous ducts may progresstoward the nipple resulting in Paget dis-ease or to the adjacent branches of areference duct {2089,2090,2093}.
TerminologyIntraductal proliferative lesions of thebreast have traditionally been dividedinto three categories: usual ductal hyper-plasia (UDH), atypical ductal hyperplasia(ADH) and ductal carcinoma in situ(DCIS). It should be noted, however, thatthe term "DCIS" encompasses a highlyheterogeneous group of lesions that dif-fer with regard to their mode of presenta-tion, histopathological features, biologi-cal markers, and risk for progression toinvasive cancer. In most cases, thehistopathological distinction between dif-ferent types of intraductal proliferationcan be made on morphological grounds
alone, particularly with standardization ofhistopathological criteria. However, eventhen, the distinction between some of thelesions (particularly between ADH andsome low grade forms of DCIS) remainsp roblematic. In addition, population-based mammography screening hasresulted in increased detection of lesionsthat show cytological atypia with or with-out intraluminal proliferation but do notfulfil the diagnostic criteria for any of theexisting categories. Those lesions lack-ing intraluminal projection have beendescribed in the past as clinging carci-noma and more recently re f e r red tounder a variety of names including flatepithelial atypia, atypical cystic lobules,atypical columnar alteration with promi-nent apical snouts and secretions.
Progression to invasive breast cancerClinical follow-up studies have indicatedthat these intraductal proliferative lesionsa re associated with diff e rent levels of riskfor subsequent development of invasiveb reast cancer, that ranges from appro x i-mately 1.5 times that of the re f e re n c epopulation for UDH, to 4-5-fold (range,2.4-13.0-fold) for ADH, and 8-10-fold forDCIS {886}. Recent immunophenotypicand molecular genetic studies have pro-vided new insights into these lesions indi-cating that the long-held notion of a linearp ro g ression from normal epitheliumt h rough hyperplasia, atypical hyperplasiaand carcinoma in situ to invasive canceris overly simplistic; the inter- re l a t i o n s h i pbetween these various intraductal pro l i f-erative lesions and invasive breast canceris far more complex. In brief, these datahave suggested that: (1) UDH shares fewsimilarities with most ADH, DCIS or inva-sive cancer; (2) ADH shares many simi-larities with low grade DCIS; (3) low gradeDCIS and high grade DCIS appear to re p-resent genetically distinct disorders lead-ing to distinct forms of invasive bre a s tc a rcinoma, further emphasizing their het-e rogeneity; and (4) at least some lesionswith flat epithelial atypia are neoplastic. These data support the notion that ADHand all forms of DCIS represent intra-
epithelial neoplasias which in the WHOclassification of tumours of the digestivesystem have been defined as ‘lesionscharacterized by morphological changesthat include altered arc h i t e c t u re andabnormalities in cytology and differentia-tion; they result from clonal alterations ingenes and carry a predisposition, albeitof variable magnitude, for invasion andmetastasis’ {1114}. The WHO WorkingGroup felt that UDH is not a significantrisk factor and that at the time of themeeting, there was insufficient geneticevidence to classify it as a precursorlesion. However, a recent CGH studysuggests that a subset of UDH can be aprecursor of ADH {1037}.
Classification and gradingThese emerging genetic data and theincreasingly frequent detection of ADHand low grade DCIS by mammographyhave raised important questions aboutthe manner in which intraductal prolifera-tive lesions are currently classified. Although used by pathology laboratoriesworldwide, the traditional classificationsystem suffers from high interobservervariability, in particular, in distinguishingbetween atypical ductal hyperplasia(ADH) and some types of low grade duc-tal carcinoma in situ (DCIS). Some mem-bers of the Working Group proposed thatthe traditional terminology be replacedby ductal intraepithelial neoplasia (DIN),reserving the term carcinoma for invasivetumours. This would help to avoid thepossibility of overtreatment, particularlyin the framework of population-basedmammography screening programmes.In several other organ sites, the shift interminology has already occurred e.g.cervix (CIN), prostate (PIN) and in therecent WHO classification of tumours ofthe digestive system {1114}.The majority of participants in the WHOWorking Group was in favour of maintain-ing the traditional terminology which inTable 1.11 is shown next to the corre-sponding terms of the DIN classification.For purposes of clinical managementand tumour registry coding, when the
F.A. Tavassoli S.J. SchnittH. Hoefler W. BoeckerJ. Rosai S.H. Heywang-KöbrunnerR. Holland F. MoinfarI.O. Ellis S.R. Lakhani
Intraductal proliferative lesions
63Intraductal proliferative lesions

DIN terminology is used, the traditionalt e rminology should be mentioned aswell. The classification of intraductal pro-liferative lesions should be viewed as anevolving concept that may be modifiedas additional molecular genetic databecome available.
Diagnostic reproducibilityMultiple studies have assessed re p ro-ducibility in diagnosing the range of intra-ductal proliferative lesions, some withemphasis on the borderline lesions {299,5 0 3 , 2 1 5 5 , 2 1 5 7 , 2 4 1 1 , 2 5 7 1 , 2 7 2 3 , 2 7 2 4 } .These studies have clearly indicated thati n t e robserver agreement is poor when nos t a n d a rdized criteria are used {2411}.Although diagnostic re p roducibility isi m p roved with the use of standardized cri-teria {2571} discrepancies in diagnosispersist in some cases, particularly in thedistinction between ADH and limited form sof low grade DCIS. In one study, consis-tency in diagnosis and classification didnot change significantly when interpre t a-tion was confined to specific images asc o m p a red with assessment of the entiretissue section on a slide, reflecting incon-sistencies secondary to diff e rences inmorphological interpretation {780}. Whileclinical follow-up studies have generallydemonstrated increasing levels of bre a s tcancer risk associated with UDH, ADHand DCIS re s p e c t i v e l y, concerns aboutdiagnostic re p roducibility have led someto question the practice of utilizing theserisk estimates at the individual level {299}.
AetiologyIn general, the factors that are associatedwith the development of invasive bre a s tc a rcinoma are also associated withi n c reased risk for the development of intraductal proliferative lesions {1439a,1551a,2536a}. (See section on epidemio-logy of breast carc i n o m a ) .
Genetics of precursor lesionsTo date, several genetic analyses havebeen perf o rmed on potential pre c u r s o rlesions of carcinoma of the breast. Thesometimes contradictory results (seebelow) may be due to: (i) small number ofcases analysed, (ii) the use of diff e re n thistological classification criteria, (iii) his-tomorphological heterogeneity of both then o rmal and neoplastic breast tissue and(iv) genetic hetero g e n e i t y, as identified byeither conventional cytogenetics {1175} or by fluorescence in situ hybridization
(FISH) analysis {1949}. Further evidencefor genetic heterogeneity comes fromcomparative genomic hybridization(CGH) data of microdissected tissue inusual ductal hyperplasia (UDH), atypicalductal hyperplasia (ADH) {135} andDCIS {134,366}.T h e re has been a tendency to interpre tloss of heterozygosity as evidence forclonal evolution and neoplastic transfor-mation. However, histologically norm a lductal epithelium closely adjacent to inva-sive ductal carcinoma may share an LOHp a t t e rn with the carcinoma, while norm a lducts further away in the breast do not{671}. LOH has been re p o rted in norm a lepithelial tissues of the breast, in associa-tion with carcinoma and in re d u c t i o nmammoplasties, however, the significanceof these finding remains to be evaluated{671,1586,1945}. LOH has also beenidentified in the stromal component of in situ {1889} and invasive breast carc i n o-ma {1545,1889}, in non-neoplastic tissuef rom reduction mammoplasty specimens{1568}, and in normal-appearing bre a s tducts {1586}. The biological significanceof these alterations are still poorly under-stood, but the available data suggest thatgenetic alterations may occur very early inb reast tumorigenesis prior to detectablemorphological changes and that epithe-l i a l / s t romal interactions play a role in pro-g ression of mammary carc i n o m a .
Clinical featuresThe age range of women with intraductalproliferative lesions is wide, spanning 7
to 8 decades post adolescence. Allthese lesions are extremely rare prior topuberty; when they do occur amonginfants and children, they are generally areflection of exogenous or abnorm a lendogenous hormonal stimulation. Themean age for DCIS is between 50-59years. Though most often unilateral,about 22% of women with DCIS in onebreast develop either in situ or invasivec a rcinoma in the contralateral bre a s t{3055}.
Macroscopy A vast majority of intraductal pro l i f e r a-tive lesions, particularly those detectedm a m m o g r a p h i c a l l y, are not evident onm a c roscopic inspection of the speci-men. A small pro p o rtion of high gradeDCIS may be extensive enough andwith such an abundance of intraluminaln e c rosis or associated stromal re a c t i o nthat it would present as multiple areas ofround, pale comedo necrosis or a firm ,gritty mass.
Usual ductal hyperplasia (UDH)
DefinitionA benign ductal proliferative lesion typi-cally characterized by secondarylumens, and streaming of the central pro-liferating cells. Although not considereda precursor lesion, long-term follow-up ofpatients with UDH suggests a slightlyelevated risk for the subsequent devel-opment of invasive carcinoma.
Table 1.11Classification of intraductal proliferative lesions.
Traditional terminology
Usual ductal hyperplasia (UDH)
Flat epithelial atypia
Atypical ductal hyperplasia (ADH)
Ductal carcinoma in situ, low grade (DCIS grade 1)
Ductal carcinoma in situ, intermediate grade (DCIS grade 2)
Ductal carcinoma in situ, high grade (DCIS grade 3)
Ductal intraepithelial neoplasia (DIN) terminology
Usual ductal hyperplasia (UDH)
Ductal intraepithelial neoplasia, grade 1A (DIN 1A)
Ductal intraepithelial neoplasia, grade 1B (DIN 1B)
Ductal intraepithelial neoplasia, grade1C (DIN 1C)
Ductal intraepithelial neoplasia, grade 2 (DIN 2)
Ductal intraepithelial neoplasia, grade 3 (DIN 3)
64 Tumours of the breast

SynonymsIntraductal hyperplasia, hyperplasia ofthe usual type, epitheliosis, ord i n a ryintraductal hyperplasia.
MammographyUDH does not have a mammographicpresentation, except in rare cases withmicrocalcification.
Risk of progressionLong-term follow up of patients with UDHin one study showed that 2.6% developsubsequent invasive carcinoma after anaverage interval of over 14 years, com-pared to 8.3 years for those with ADH{2886}. In another study, the absolute riskof a woman with UDH developing breastcancer within 15 years was 4% {732}.The Cancer Committee of the College ofAmerican Pathologists has assignedUDH a slightly increased risk (RR of 1.5-2.0) for subsequent development of inva-sive carcinoma {885}.
HistopathologyUDH is characterized by irre g u l a r l yshaped and sized secondary lumens,often peripherally distributed, and stre a m-ing of the central bolus of pro l i f e r a t i n gcells. Epithelial bridges are thin ands t retched; nuclei are unevenly distributed.
In some cases, the proliferation has asolid pattern and no secondary lumensa re evident. Cytologically, the lesion iscomposed of cells with indistinct cell mar-gins, variation in the tinctorial features ofthe cytoplasm and variation in shape andsize of nuclei. Admixture of epithelial,myoepithelial or metaplastic apocrinecells is not uncommon. The presence or
absence of either microcalcifications orn e c rosis does not impact the diagnosis.UDH with necrosis, a rare event, may bemistaken for DCIS; the diagnosis shouldbe based on the cytological features andnot the presence of necrotic debris. UDHgenerally displays either diffuse or amosaic pattern of positivity with highmolecular weight cytokeratins {1963,2126} such as CK5, CK1/5/10/14 (cloneCK34betaE12 or clone D5/16 B4); it isalso positive for E-cadherin. In UDH, thep e rcentage of ER-positive cells was foundslightly increased compared to the norm a lb reast {2667}. Increased levels of cyclinD1 expression were recently described in11-19% of UDH cases {1172,3264}.
Genetic alterationsA p p roximately 7% of UDH show somed e g ree of aneuploidy. Loss of hetero z y-gosity (LOH) for at least one locus, hasbeen noted in one-third of UDH {2071}.On chromosome 11p, LOH was pre s e n tin 10-20% of UDH cases {72,2071}.Losses on 16q and 17p were identified inUDH lesions without evidence of adjacentc a rcinoma {1037} whereas no alterationsw e re re p o rted by others {301}. In UDHadjacent to carcinoma, polysomy of chro-mosome 1 as well as increased signal fre-quencies for the 20q13 region (typicallyp resent in DCIS) were identified by FISH{593,3100}. By CGH, UDH lesions adja-cent to carcinoma showed gain on chro-mosome 20q and loss on 13q in 4 of 5cases {136}, although no alteration wasre p o rted in another study {301}. Somerecent CGH studies suggest that a pro-p o rtion of UDH lesions is monoclonal{1037,1358}, and that a subset showsalterations similar to those observed inADH {1037}; however, the frequency ofgenetic alterations seen in UDH usingLOH and CGH is much lower than inADH. TP53 protein expression has notbeen demonstrated in UDH or in anyother benign proliferative lesions {1567}.Mutations of the T P 5 3 gene are alsoabsent, except as inherited mutations inLi-Fraumeni patients {72}.
Flat epithelial atypia
DefinitionA presumably neoplastic intraductalalteration characterized by replacementof the native epithelial cells by a single or3-5 layers of mildly atypical cells.
BA
DCFig. 1.80 Usual ductal hyperplasia. A Florid type. The peripheral distribution of irregularly sized spaces is acharacteristic of UDH readily apparent at low magnification. B The proliferating cells may form epithelialbridges, but the bridges are delicate and formed by spindled stretched cells. C Intensive, predominantlysolid intraductal proliferation of a heterogeneous cell population. Note spindling of the cells. Several irreg-ular peripheral luminal spaces. D Intraluminal proliferation with many CK5-positive and occasional CK5-negative cells.
Table 1.12Usual ductal hyperplasia.
Architectural features1. Irregular fenestrations2. Peripheral fenestrations3. Stretched or twisted epithelial bridges4. Streaming5. Uneven distribution of nuclei and overlapped
nuclei
Cellular features1. Multiple cell types2. Variation in appearance of epithelial cells3. Indistinct cell margins and deviation from a
round contour4. Variation in the appearance of nuclei
One of the most important indicators of UDH isthe presence of an admixture of two or morecell types (epithelial, myoepithelial and/ormetaplastic apocrine cells).
65Intraductal proliferative lesions
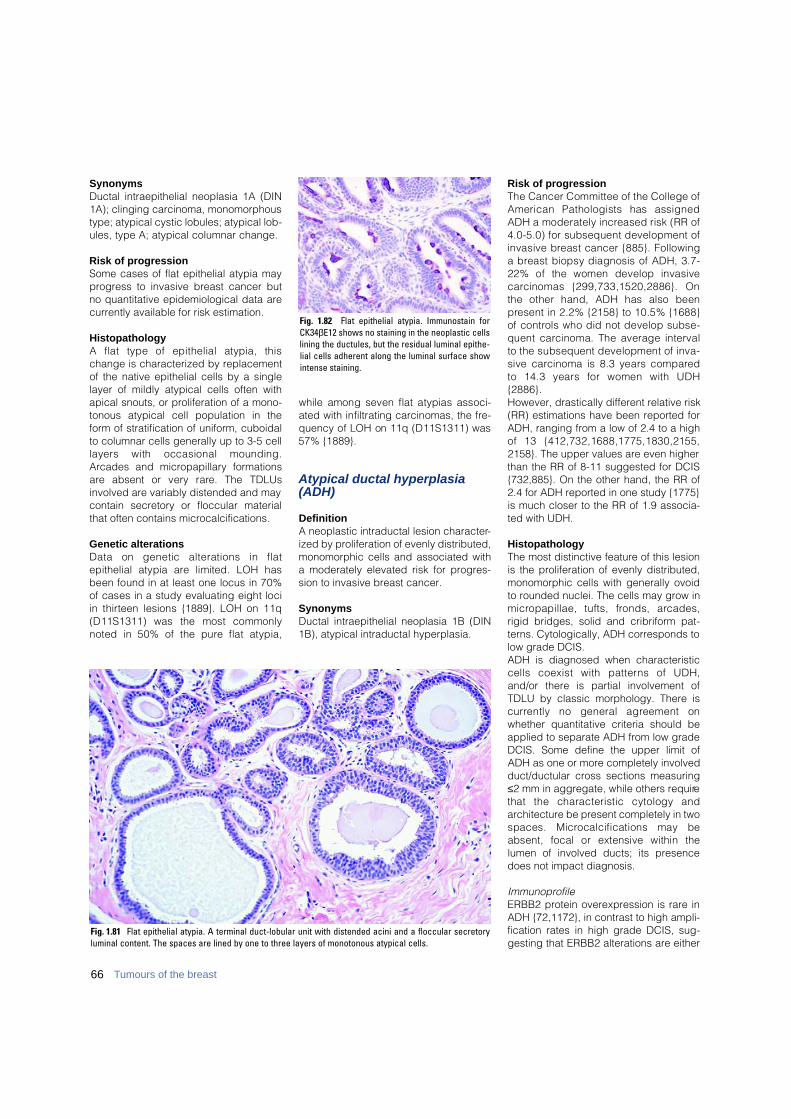
SynonymsDuctal intraepithelial neoplasia 1A (DIN1A); clinging carcinoma, monomorphoustype; atypical cystic lobules; atypical lob-ules, type A; atypical columnar change.
Risk of progressionSome cases of flat epithelial atypia mayprogress to invasive breast cancer butno quantitative epidemiological data arecurrently available for risk estimation.
HistopathologyA flat type of epithelial atypia, thischange is characterized by replacementof the native epithelial cells by a singlelayer of mildly atypical cells often withapical snouts, or proliferation of a mono-tonous atypical cell population in theform of stratification of uniform, cuboidalto columnar cells generally up to 3-5 celllayers with occasional mounding.Arcades and micropapillary formationsa re absent or very rare. The TDLUsinvolved are variably distended and maycontain secretory or floccular materialthat often contains microcalcifications.
Genetic alterationsData on genetic alterations in flat epithelial atypia are limited. LOH hasbeen found in at least one locus in 70%of cases in a study evaluating eight lociin thirteen lesions {1889}. LOH on 11q(D11S1311) was the most commonlynoted in 50% of the pure flat atypia,
while among seven flat atypias associ-ated with infiltrating carcinomas, the fre-quency of LOH on 11q (D11S1311) was57% {1889}.
Atypical ductal hyperplasia(ADH)
DefinitionA neoplastic intraductal lesion character-ized by proliferation of evenly distributed,monomorphic cells and associated witha moderately elevated risk for progres-sion to invasive breast cancer.
SynonymsDuctal intraepithelial neoplasia 1B (DIN1B), atypical intraductal hyperplasia.
Risk of progressionThe Cancer Committee of the College ofAmerican Pathologists has assignedADH a moderately increased risk (RR of4.0-5.0) for subsequent development ofinvasive breast cancer {885}. Followinga breast biopsy diagnosis of ADH, 3.7-22% of the women develop invasivec a rcinomas {299,733,1520,2886}. Onthe other hand, ADH has also beenp resent in 2.2% {2158} to 10.5% {1688}of controls who did not develop subse-quent carcinoma. The average intervalto the subsequent development of inva-sive carcinoma is 8.3 years compare dto 14.3 years for women with UDH{ 2 8 8 6 } .However, drastically different relative risk(RR) estimations have been reported forADH, ranging from a low of 2.4 to a highof 13 {412,732,1688,1775,1830,2155,2158}. The upper values are even higherthan the RR of 8-11 suggested for DCIS{732,885}. On the other hand, the RR of2.4 for ADH reported in one study {1775}is much closer to the RR of 1.9 associa-ted with UDH.
HistopathologyThe most distinctive feature of this lesionis the proliferation of evenly distributed,monomorphic cells with generally ovoidto rounded nuclei. The cells may grow inm i c ropapillae, tufts, fronds, arc a d e s ,rigid bridges, solid and cribriform pat-terns. Cytologically, ADH corresponds tolow grade DCIS.ADH is diagnosed when characteristiccells coexist with patterns of UDH,and/or there is partial involvement ofTDLU by classic morphology. There isc u r rently no general agreement onwhether quantitative criteria should beapplied to separate ADH from low gradeDCIS. Some define the upper limit ofADH as one or more completely involvedduct/ductular cross sections measuring≤2 mm in aggregate, while others requirethat the characteristic cytology andarchitecture be present completely in twospaces. Microcalcifications may beabsent, focal or extensive within thelumen of involved ducts; its presencedoes not impact diagnosis.
ImmunoprofileERBB2 protein overexpression is rare inADH {72,1172}, in contrast to high ampli-fication rates in high grade DCIS, sug-gesting that ERBB2 alterations are either
Fig. 1.82 Flat epithelial atypia. Immunostain for CK34βE12 shows no staining in the neoplastic cellslining the ductules, but the residual luminal epithe-lial cells adherent along the luminal surface showintense staining.
Fig. 1.81 Flat epithelial atypia. A terminal duct-lobular unit with distended acini and a floccular secretoryluminal content. The spaces are lined by one to three layers of monotonous atypical cells.
66 Tumours of the breast

not an early event in malignant transfor-mation or that they are largely restrictedto high grade DCIS. Increased levels ofcyclin D1 expression were re c e n t l ydescribed in 27-57% of ADH {1172,3264}. Nuclear accumulation of the TP53protein is absent in ADH and low gradeDCIS {1567}. Nearly 90% of ADH arenegative for high molecular weight cytok-eratins 1/5/10/14 (clones CK34BetaE12and D5/16 B4), an important feature inseparating ADH from UDH {1963,2126}.
Genetic alterationsFifty percent of ADH cases share theirLOH patterns with invasive carcinomasfrom the same breast, strongly support-ing a precursor relationship betweenthese lesions {1567}. LOH has beenidentified frequently on chro m o s o m e s16q, 17p, and 11q13 {1567,1570}. T P 5 3mutations are restricted to affected mem-bers of Li-Fraumeni families.
Ductal carcinoma in situ (DCIS)
DefinitionA neoplastic intraductal lesion character-ized by increased epithelial pro l i f e r a t i o n ,subtle to marked cellular atypia and ani n h e rent but not necessarily obligate ten-dency for pro g ression to invasive bre a s tc a n c e r.
ICD-O code 8500/2
SynonymsIntraductal carcinoma, ductal intraepi-thelial neoplasia (DIN 1C to DIN 3).
Risk of progressionDCIS is considered a precursor lesion(obligate or non-obligate), with a relativerisk (RR) of 8-11 for the development of invasive breast cancer {732,885}.However, there is evidence that conser-
vative treatment (complete local eradica-tion) is usually curative (see below).
EpidemiologyA striking increase in the detection ofDCIS has been noted with the intro d u c-tion of widespread screening mammogra-phy and increasing awareness of bre a s tcancer in the general population since1983. The average annual increase in theincidence rate of DCIS in the decade of1973 to 1983 was 3.9% compared to17.5% annually in the decade between1983 to 1992, increasing from 2.4 per100,000 women in 1973 to 15.8 per100,000 in 1992 for women of all races,an overall increase of 557% {794}. In theUS, data from the National CancerI n s t i t u t e ’s Surveillance, Epidemiology andEnd Results (SEER) program noted thatthe pro p o rtion of breast carcinomas diag-nosed as DCIS increased from 2.8% in1973 to 14.4% in 1995 {794}. While closeto 90% of pre-mammography DCIS wereof the high grade comedo type, nearly60% of mammographically detectedlesions are non-comedo and this perc e n-tage is incre a s i n g .I n t e re s t i n g l y, despite the more limitedsurgical excisions, mortality from "DCIS"has declined. Of women with DCISdiagnosed between 1978 and 1983( p re-mammographic era), 3.4% died of breast cancer at 10 years, despitehaving been treated by mastectomy inthe vast majority of cases. On the otherhand, only 1.9% of women diagnosedwith DCIS between 1984 and 1989 diedof breast cancer at 10 years, despite thei n c reasing trend toward lumpectomy{794}. Judging from the 10-year follow-
Fig. 1.84 Atypical ductal hyperplasia. A terminalduct-lobular unit with dilated ductules that arepartly filled with a CK5/6 negative ductal prolifera-tion which on H&E had the characteristics of a lowgrade DCIS. Note on the left side some cytokeratinpositive ductules.
Fig. 1.83 Atypical ductal hyperplasia. Severalrounded calcifications, possibly including 1-2 “teacup” shaped calcifications are seen. Usually suchcalcifications indicate benign changes. However,the calcifications appear to follow two ducts.Furthermore, a faint group of very fine microcalcifi-cations can barely be perceived.
BAFig. 1.85 Atypical ductal hyperplasia. A Two adjacent ducts showing partial cribriform involvement in a background of flat epithelial atypia. B Partial involvementof a duct by a cribriform proliferation of uniform, rounded cells in the setting of a flat epithelial atypia. Microcalcification is also present.
67Intraductal proliferative lesions
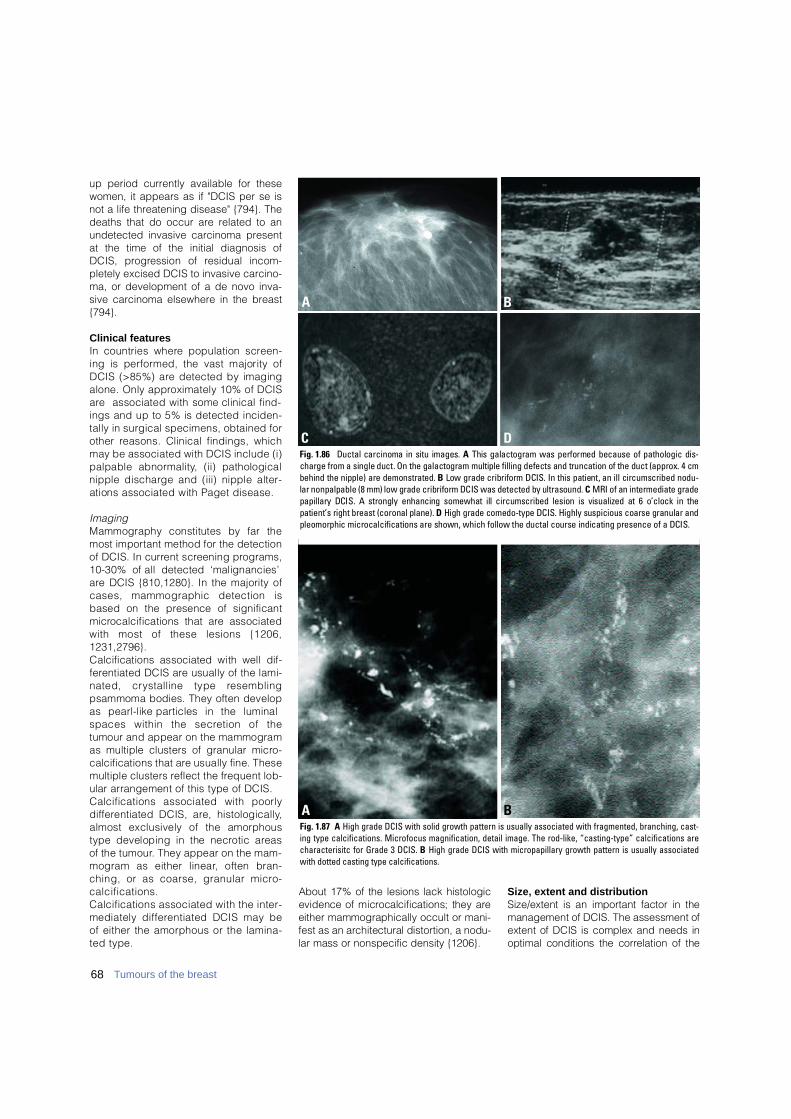
u p period currently available for thesewomen, it appears as if "DCIS per se isnot a life threatening disease" {794}. Thedeaths that do occur are related to anundetected invasive carcinoma presentat the time of the initial diagnosis ofDCIS, pro g ression of residual incom-pletely excised DCIS to invasive carcino-ma, or development of a de novo inva-sive carcinoma elsewhere in the breast{794}.
Clinical featuresIn countries where population scre e n-ing is perf o rmed, the vast majority ofDCIS (>85%) are detected by imagingalone. Only approximately 10% of DCISa re associated with some clinical find-ings and up to 5% is detected inciden-tally in surgical specimens, obtained forother reasons. Clinical findings, whichmay be associated with DCIS include (i)palpable abnorm a l i t y, (ii) pathologicalnipple discharge and (iii) nipple alter-ations associated with Paget disease.
ImagingMammography constitutes by far themost important method for the detectionof DCIS. In current screening pro g r a m s ,10-30% of all detected ‘malignancies’a re DCIS {810,1280}. In the majority ofcases, mammographic detection isbased on the presence of significantm i c rocalcifications that are associatedwith most of these lesions {1206,1 2 3 1 , 2 7 9 6 } .Calcifications associated with well dif-f e rentiated DCIS are usually of the lami-nated, crystalline type re s e m b l i n gpsammoma bodies. They often developas pearl-like particles in the luminalspaces within the secretion of thetumour and appear on the mammogramas multiple clusters of granular micro-calcifications that are usually fine. Thesemultiple clusters reflect the frequent lob-ular arrangement of this type of DCIS.Calcifications associated with poorlyd i ff e rentiated DCIS, are, histologically,almost exclusively of the amorphoustype developing in the necrotic areas of the tumour. They appear on the mam-mogram as either linear, often bran-ching, or as coarse, granular micro-calcifications. Calcifications associated with the inter-mediately diff e rentiated DCIS may beof either the amorphous or the lamina-ted type.
About 17% of the lesions lack histologicevidence of microcalcifications; they areeither mammographically occult or mani-fest as an architectural distortion, a nodu-lar mass or nonspecific density {1206}.
Size, extent and distributionSize/extent is an important factor in themanagement of DCIS. The assessment ofextent of DCIS is complex and needs inoptimal conditions the correlation of the
Fig. 1.87 A High grade DCIS with solid growth pattern is usually associated with fragmented, branching, cast-ing type calcifications. Microfocus magnification, detail image. The rod-like, “casting-type” calcifications arecharacterisitc for Grade 3 DCIS. B High grade DCIS with micropapillary growth pattern is usually associatedwith dotted casting type calcifications.
BA
BA
DCFig. 1.86 Ductal carcinoma in situ images. A This galactogram was performed because of pathologic dis-charge from a single duct. On the galactogram multiple filling defects and truncation of the duct (approx. 4 cmbehind the nipple) are demonstrated. B Low grade cribriform DCIS. In this patient, an ill circumscribed nodu-lar nonpalpable (8 mm) low grade cribriform DCIS was detected by ultrasound. C MRI of an intermediate gradepapillary DCIS. A strongly enhancing somewhat ill circumscribed lesion is visualized at 6 o’clock in thepatient’s right breast (coronal plane). D High grade comedo-type DCIS. Highly suspicious coarse granular andpleomorphic microcalcifications are shown, which follow the ductal course indicating presence of a DCIS.
68 Tumours of the breast

mammogram, the specimen X-ray andthe histologic slides. Since the majority ofDCIS is non palpable, the mammograph-ic estimate is the sole guide for re s e c t i o n .T h e re f o re, data on the mammographicpathological correlation of the tumour sizea re essential for guiding the extent of sur-g e ry. The mammographic extent of aDCIS is defined as the greatest distancebetween the most peripherally locatedclusters of suspicious micro c a l c i f i c a t i o n s ,and the histologic extent as the gre a t e s tdistance between the most peripherallylocated, histologically verified, DCIS foci.Histologic evaluation supported by corre-lation with the X-ray of the sliced speci-men allows a precise and re p ro d u c i b l eassessment of the extent of any DCISp resent. Whole organ studies have shownthat mammography, on the basis of sig-nificant microcalcifications, generallyu n d e restimates the histologic or "re a l "size of DCIS by an average of 1-2 cm. Ina series of DCIS cases with mammo-graphic sizes up to 3 cm, the size diff e r-ence was less than 2 cm in more than80% of the cases {1231}.DCIS may appear as a multifocal pro c e s sdue to the presence of multiple tumourfoci on two-dimensional plane sections.H o w e v e r, these tumour spots may notnecessarily re p resent separate foci.Intraductal tumour growth on thre e -
dimensional studies appears to be con-tinuous rather than discontinuous {831}.M o re specifically, whereas poorly diff e r-entiated DCIS shows a pre d o m i n a n t l ycontinuous growth, the well diff e re n t i a t e dDCIS, in contrast, may present a morediscontinuous (multifocal) distribution.These results have a direct implication onthe reliability of the margin assessment ofsurgical specimens. In cases of poorlyd i ff e rentiated DCIS, margin assessmentshould, theore t i c a l l y, be more re l i a b l ethan well diff e rentiated DCIS. In a multifo-cal process with discontinuous gro w t h ,the surgical margin may lie between thetumour foci, giving the false impression ofa free margin.The distribution of DCIS in the breast istypically not multicentric, defined astumour involvement in two or more re m o t ea reas separated by uninvolved glandulartissue of 5 cm. On the contrary, DCIS istypically ‘segmental’ in distribution{1230}. In practical terms, this implies thattwo apparently separate areas of "malig-nant" mammographic micro c a l c i f i c a t i o n susually do not re p resent separate fields ofDCIS but rather a larger tumour in whichthe two mammographically identifiedfields are connected by DCIS, which ismammographically invisible due to thelack of detectable size of micro c a l c i f i c a-tions. One should be aware that singlem i c roscopic calcium particles smallerthan about 80µ cannot be seen on con-ventional mammograms.
GradingAlthough there is currently no universala g reement on classification of DCIS, therehas been a move away from traditionala rchitectural classification. Most modernsystems use cytonuclear grade alone orin combination with necrosis and or cellpolarization. Recent international consen-sus conferences held on this subjectendorsed this change and re c o m m e n d e dthat, until more data emerges on clinicaloutcome related to pathology variables,grading of DCIS should form the basis ofclassification and that grading should bebased primarily on cytonuclear feature s{6,7,1565,2346}. Pathologists are encouraged to includeadditional information on necrosis, arc h i t e c-t u re, polarization, margin status, size andcalcification in their re p o rt s .Depending primarily on the degree ofnuclear atypia, intraluminal necrosis and,to a lesser extent, on mitotic activity and
calcification, DCIS is generally dividedinto three grades; the first two featuresconstitute the major criteria in the majori-ty of grading systems. It is not uncom-mon to find admixture of various gradesof DCIS as well as various cytologicalvariants of DCIS within the same biopsyor even within the same ductal space.When more than one grade of DCIS ispresent, the proportion (percentage) ofvarious grades should be noted in thediagnosis {2876}. It is important to notethat a three tiered grading system doesnot necessarily imply progression fromgrade 1 or well differentiated to grade 3or poorly differentiated DCIS.
HistopathologyLow grade DCIS Low grade DCIS is composed of small,monomorphic cells, growing in arcades,m i c ropapillae, cribriform or solid pat-terns. The nuclei are of uniform size andhave a regular chromatin pattern withinconspicuous nucleoli; mitotic figures
Table 1.13Features of DCIS to be documented for the surgicalpathology report.
Table 1.14Minimal criteria for low grade DCIS.
Fig. 1.88 Large excision biopsy of a high grade duc-tal carcinoma in situ. A Note the sharp demarcationbetween DCIS, comedo type (left), and adjacentfibrous stroma. B Mammography showing a largearea with highly polymorphic microcalcifications.
A
B
Major lesion characteristics1. Nuclear grade2. Necrosis3. Architectural patterns
Associated features1. Margins
If positive, note focal or diffuse involvement.Distance from any margin to the nearestfocus of DCIS.
2. Size (either extent or distribution) 3. Microcalcifications (specify within DCIS or
elsewhere)4. Correlate morphological findings with speci-
men imaging and mammographic findings
Cytological features1. Monotonous, uniform rounded cell
population2. Subtle increase in nuclear-cytoplasmic ratio3. Equidistant or highly organized nuclear
distribution4. Round nuclei5. Hyperchromasia may or may not be present
Architectural featuresArcades, cribriform, solid and/or
micropapillary pattern
69Intraductal proliferative lesions
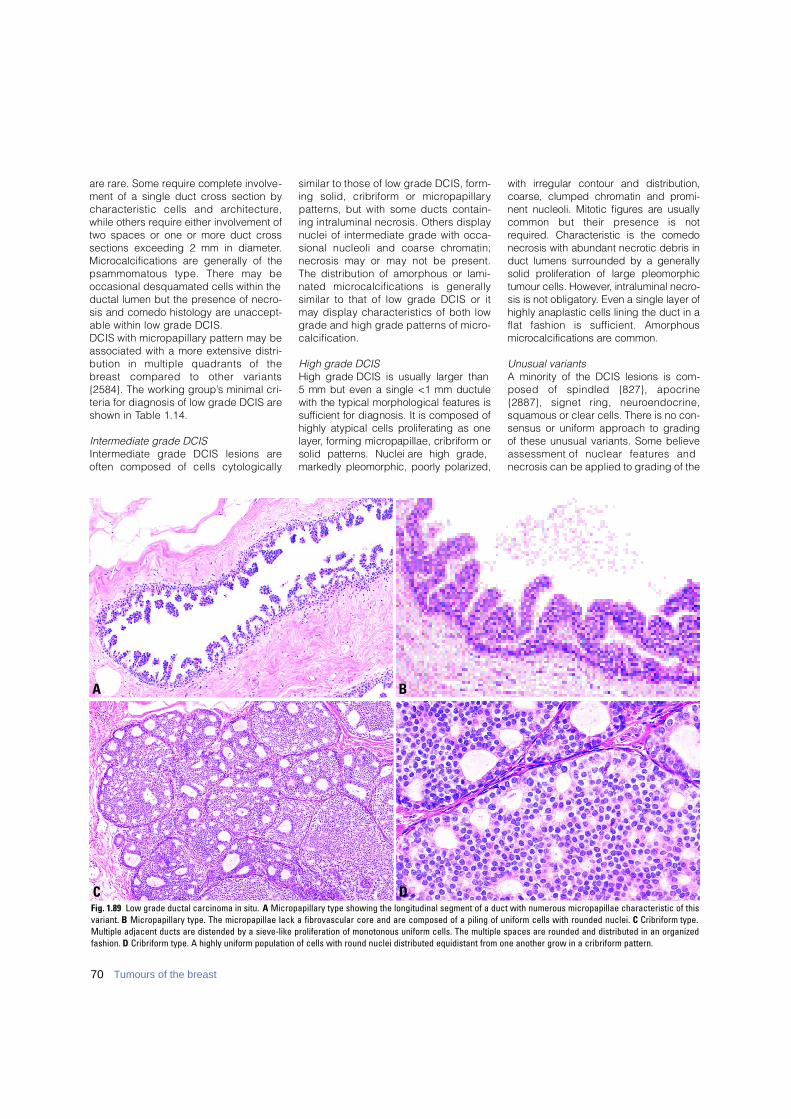
are rare. Some require complete involve-ment of a single duct cross section bycharacteristic cells and arc h i t e c t u re ,while others require either involvement oftwo spaces or one or more duct crosssections exceeding 2 mm in diameter.Microcalcifications are generally of thepsammomatous type. There may beoccasional desquamated cells within theductal lumen but the presence of necro-sis and comedo histology are unaccept-able within low grade DCIS. DCIS with micro p a p i l l a ry pattern may beassociated with a more extensive distri-bution in multiple quadrants of theb reast compared to other variants{2584}. The working gro u p ’s minimal cri-teria for diagnosis of low grade DCIS areshown in Table 1.14.
Intermediate grade DCIS I n t e rmediate grade DCIS lesions areoften composed of cells cytologically
similar to those of low grade DCIS, form-ing solid, cribriform or micro p a p i l l a ryp a t t e rns, but with some ducts contain-ing intraluminal necrosis. Others displaynuclei of intermediate grade with occa-sional nucleoli and coarse chro m a t i n ;n e c rosis may or may not be pre s e n t .The distribution of amorphous or lami-nated microcalcifications is generallysimilar to that of low grade DCIS or itmay display characteristics of both lowgrade and high grade patterns of micro-c a l c i f i c a t i o n .
High grade DCIS High grade DCIS is usually larger than 5 mm but even a single <1 mm ductulewith the typical morphological features iss u fficient for diagnosis. It is composed ofhighly atypical cells proliferating as onel a y e r, forming micropapillae, cribriform orsolid patterns. Nuclei are high grade,markedly pleomorphic, poorly polarized,
with irregular contour and distribution,coarse, clumped chromatin and pro m i-nent nucleoli. Mitotic figures are usuallycommon but their presence is notre q u i red. Characteristic is the comedon e c rosis with abundant necrotic debris induct lumens surrounded by a generallysolid proliferation of large pleomorphictumour cells. However, intraluminal necro-sis is not obligatory. Even a single layer ofhighly anaplastic cells lining the duct in aflat fashion is sufficient. Amorphousm i c rocalcifications are common.
Unusual variantsA minority of the DCIS lesions is com-posed of spindled {827}, apocrine{2887}, signet ring, neuro e n d o c r i n e ,squamous or clear cells. There is no con-sensus or uniform approach to gradingof these unusual variants. Some believeassessment of nuclear features andnecrosis can be applied to grading of the
BA
DCFig. 1.89 Low grade ductal carcinoma in situ. A Micropapillary type showing the longitudinal segment of a duct with numerous micropapillae characteristic of thisvariant. B Micropapillary type. The micropapillae lack a fibrovascular core and are composed of a piling of uniform cells with rounded nuclei. C Cribriform type.Multiple adjacent ducts are distended by a sieve-like proliferation of monotonous uniform cells. The multiple spaces are rounded and distributed in an organizedfashion. D Cribriform type. A highly uniform population of cells with round nuclei distributed equidistant from one another grow in a cribriform pattern.
70 Tumours of the breast
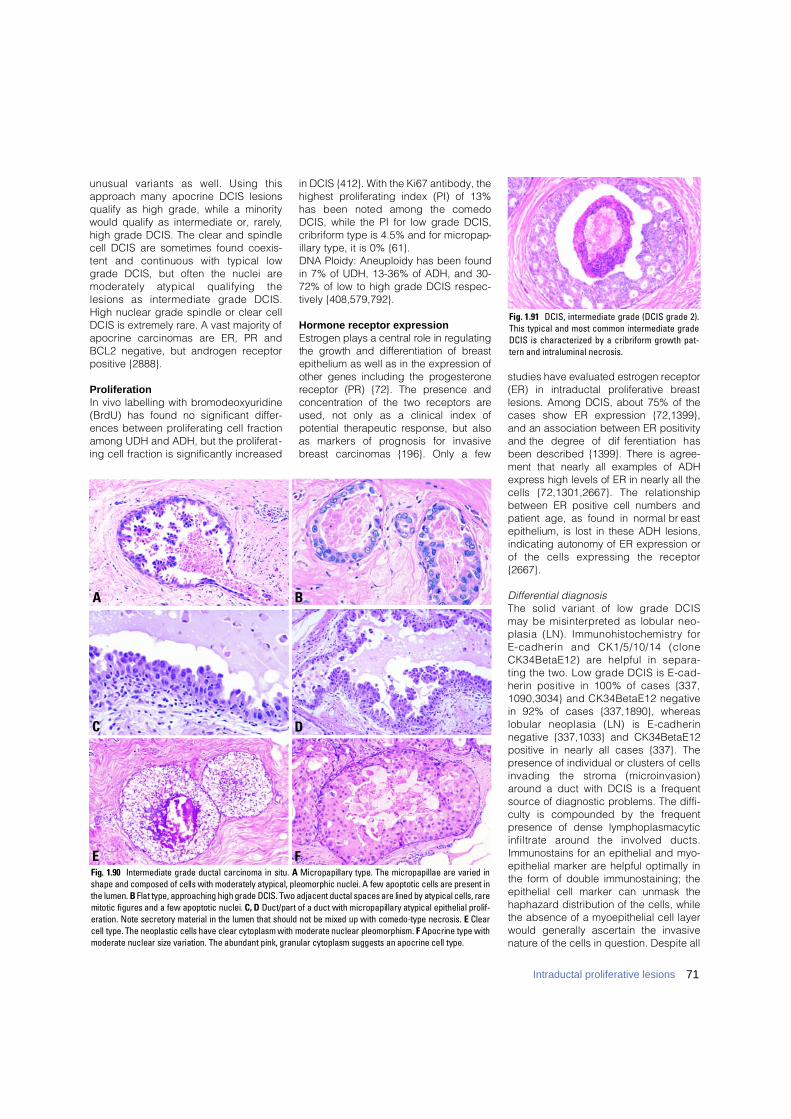
unusual variants as well. Using thisapproach many apocrine DCIS lesionsqualify as high grade, while a minoritywould qualify as intermediate or, rarely,high grade DCIS. The clear and spindlecell DCIS are sometimes found coexis-tent and continuous with typical lowgrade DCIS, but often the nuclei aremoderately atypical qualifying thelesions as intermediate grade DCIS.High nuclear grade spindle or clear cellDCIS is extremely rare. A vast majority ofapocrine carcinomas are ER, PR andBCL2 negative, but androgen receptorpositive {2888}.
ProliferationIn vivo labelling with bromodeoxyuridine(BrdU) has found no significant differ-ences between proliferating cell fractionamong UDH and ADH, but the proliferat-ing cell fraction is significantly increased
in DCIS {412}. With the Ki67 antibody, thehighest proliferating index (PI) of 13%has been noted among the comedoDCIS, while the PI for low grade DCIS,cribriform type is 4.5% and for micropap-illary type, it is 0% {61}.DNA Ploidy: Aneuploidy has been foundin 7% of UDH, 13-36% of ADH, and 30-72% of low to high grade DCIS respec-tively {408,579,792}.
Hormone receptor expressionE s t rogen plays a central role in re g u l a t i n gthe growth and diff e rentiation of bre a s tepithelium as well as in the expression ofother genes including the pro g e s t e ro n ereceptor (PR) {72}. The presence andconcentration of the two receptors areused, not only as a clinical index ofpotential therapeutic response, but alsoas markers of prognosis for invasiveb reast carcinomas {196}. Only a few
studies have evaluated estrogen re c e p t o r(ER) in intraductal proliferative bre a s tlesions. Among DCIS, about 75% of thecases show ER expression {72,1399},and an association between ER positivityand the degree of diff e rentiation hasbeen described {1399}. There is agre e-ment that nearly all examples of ADHe x p ress high levels of ER in nearly all thecells {72,1301,2667}. The re l a t i o n s h i pbetween ER positive cell numbers andpatient age, as found in normal bre a s tepithelium, is lost in these ADH lesions,indicating autonomy of ER expression orof the cells expressing the re c e p t o r{ 2 6 6 7 } .
Differential diagnosisThe solid variant of low grade DCISmay be misinterpreted as lobular neo-plasia (LN). Immunohistochemistry forE-cadherin and CK1/5/10/14 (cloneCK34BetaE12) are helpful in separa-ting the two. Low grade DCIS is E-cad-herin positive in 100% of cases {337,1090,3034} and CK34BetaE12 negativein 92% of cases {337,1890}, whereaslobular neoplasia (LN) is E-cadherin negative {337,1033} and CK34BetaE12positive in nearly all cases {337}. Thepresence of individual or clusters of cellsinvading the stroma (micro i n v a s i o n )around a duct with DCIS is a frequentsource of diagnostic problems. The diffi-culty is compounded by the frequentpresence of dense lymphoplasmacyticinfiltrate around the involved ducts.Immunostains for an epithelial and myo-epithelial marker are helpful optimally inthe form of double immunostaining; theepithelial cell marker can unmask thehaphazard distribution of the cells, whilethe absence of a myoepithelial cell layerwould generally ascertain the invasivenature of the cells in question. Despite all
Fig. 1.91 DCIS, intermediate grade (DCIS grade 2).This typical and most common intermediate gradeDCIS is characterized by a cribriform growth pat-tern and intraluminal necrosis.
BA
DC
Fig. 1.90 Intermediate grade ductal carcinoma in situ. A Micropapillary type. The micropapillae are varied inshape and composed of cells with moderately atypical, pleomorphic nuclei. A few apoptotic cells are present inthe lumen. B Flat type, approaching high grade DCIS. Two adjacent ductal spaces are lined by atypical cells, raremitotic figures and a few apoptotic nuclei. C, D Duct/part of a duct with micropapillary atypical epithelial prolif-eration. Note secretory material in the lumen that should not be mixed up with comedo-type necrosis. E C l e a rcell type. The neoplastic cells have clear cytoplasm with moderate nuclear pleomorphism. F Apocrine type withmoderate nuclear size variation. The abundant pink, granular cytoplasm suggests an apocrine cell type.
FE
71Intraductal proliferative lesions
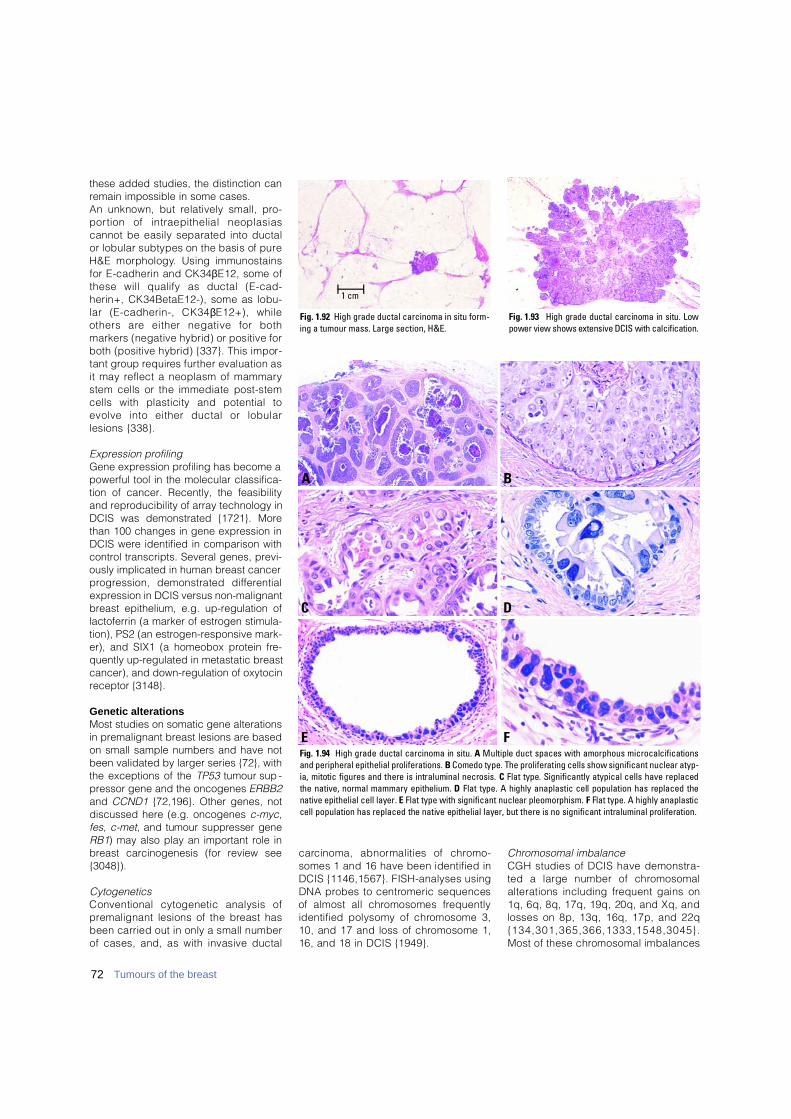
these added studies, the distinction canremain impossible in some cases. An unknown, but relatively small, pro-p o rtion of intraepithelial neoplasiascannot be easily separated into ductalor lobular subtypes on the basis of pureH&E morphology. Using immunostainsfor E-cadherin and CK34βE12, some ofthese will qualify as ductal (E-cad-herin+, CK34BetaE12-), some as lobu-lar (E-cadherin-, CK34βE12+), whileothers are either negative for bothmarkers (negative hybrid) or positive forboth (positive hybrid) {337}. This impor-tant group re q u i res further evaluation asit may reflect a neoplasm of mammarystem cells or the immediate post-stemcells with plasticity and potential toevolve into either ductal or lobularlesions {338}.
Expression profilingGene expression profiling has become apowerful tool in the molecular classifica-tion of cancer. Recently, the feasibilityand reproducibility of array technology inDCIS was demonstrated {1721}. Morethan 100 changes in gene expression inDCIS were identified in comparison withcontrol transcripts. Several genes, previ-ously implicated in human breast cancerp ro g ression, demonstrated diff e re n t i a lexpression in DCIS versus non-malignantbreast epithelium, e.g. up-regulation oflactoferrin (a marker of estrogen stimula-tion), PS2 (an estrogen-responsive mark-er), and SIX1 (a homeobox protein fre-quently up-regulated in metastatic breastcancer), and down-regulation of oxytocinreceptor {3148}.
Genetic alterationsMost studies on somatic gene alterationsin premalignant breast lesions are basedon small sample numbers and have notbeen validated by larger series {72}, withthe exceptions of the T P 5 3 tumour sup -pressor gene and the oncogenes E R B B 2and C C N D 1 {72,196}. Other genes, notdiscussed here (e.g. oncogenes c - m y c,f e s, c - m e t, and tumour suppresser geneR B 1) may also play an important role inbreast carcinogenesis (for review see{3048}).
CytogeneticsConventional cytogenetic analysis ofp remalignant lesions of the breast hasbeen carried out in only a small numberof cases, and, as with invasive ductal
c a rcinoma, abnormalities of chro m o-somes 1 and 16 have been identified inDCIS {1146,1567}. FISH-analyses usingDNA probes to centromeric sequencesof almost all chromosomes fre q u e n t l yidentified polysomy of chromosome 3,10, and 17 and loss of chromosome 1,16, and 18 in DCIS {1949}.
Chromosomal imbalanceCGH studies of DCIS have demonstra-ted a large number of chro m o s o m a lalterations including frequent gains on1q, 6q, 8q, 17q, 19q, 20q, and Xq, andlosses on 8p, 13q, 16q, 17p, and 22q{ 1 3 4 , 3 0 1 , 3 6 5 , 3 6 6 , 1 3 3 3 , 1 5 4 8 , 3 0 4 5 } .Most of these chromosomal imbalances
Fig. 1.92 High grade ductal carcinoma in situ form-ing a tumour mass. Large section, H&E.
1 cm
Fig. 1.93 High grade ductal carcinoma in situ. Lowpower view shows extensive DCIS with calcification.
BA
DC
Fig. 1.94 High grade ductal carcinoma in situ. A Multiple duct spaces with amorphous microcalcificationsand peripheral epithelial proliferations. B Comedo type. The proliferating cells show significant nuclear atyp-ia, mitotic figures and there is intraluminal necrosis. C Flat type. Significantly atypical cells have replacedthe native, normal mammary epithelium. D Flat type. A highly anaplastic cell population has replaced thenative epithelial cell layer. E Flat type with significant nuclear pleomorphism. F Flat type. A highly anaplasticcell population has replaced the native epithelial layer, but there is no significant intraluminal proliferation.
FE
72 Tumours of the breast

resemble those identified in invasiveductal carcinoma, adding weight to thet h e o ry that DCIS is a direct pre c u r s o r.
L O HIn DCIS, loss of heterozygosity (LOH)was frequently identified at several locion chromosomes 1 {1942}, 3p21 {1743},and chromosomes 8p, 13q, 16q, 17p,17q, and 18q {924,2317,3036}. Thehighest re p o rted rates of LOH in DCISa re between 50% and 80% and involveloci on chromosomes 16q, 17p, and17q, suggesting that altered genes inthese regions may be important in thedevelopment of DCIS {72,924,3036}.Among more than 100 genetic loci stud-ied so far on chromosome 17, nearly allDCIS lesions showed at least one LOH{72,301,924,1942,2071,2317,2475}. ByCGH and FISH, low and some interm e d i-ate grade DCIS and invasive tubular car-cinoma (G1) show loss of 16q, harbour-ing one of the cadherin gene clusters,w h e reas some intermediate grade andhigh grade DCIS and nearly all G2 andG3 invasive ductal carcinomas show noloss of genetic material on this locus buthave alterations of other chromosomes (-13q, +17p, +20q). Based upon thisdata, a genetic pro g ression model wasp roposed {301}.
E R B B 2The E R B B 2 (Her2/neu) oncogene hasreceived attention because of its associ-ation with lymph node metastases, shortrelapse free time, poor survival, andd e c reased response to endocrine andchemotherapy in breast cancer patients{72,1567}. Studies of ERB B2 have usedmainly FISH technique to identify ampli-fication and immunohistochemistry (IHC)to detect over expression of the onco-gene, which are highly correlated {72}.Amplification and/or over expre s s i o nwas observed on average in 30% ofDCIS, correlating directly with diff e re n t i-ation {72}; it was detected in a high pro-p o rtion of DCIS of high nuclear grade(60-80%) but was not common in lownuclear grade DCIS {196}. Patients withERBB2 positive tumours may benefitf rom adjuvant treatment with monoclonalantibody (Herc e p t i n ) .
Cyclin D1This protein plays an important part inregulating the pro g ress of the cell duringthe G1 phase of the cell cycle. The gene
(C C N D 1) is considered a potential onco-gene, but in clinical studies of invasiveb reast cancer, overe x p ression of cyclinD1 was found to be associated withe s t rogen receptor expression and lowhistological grade, both markers of goodp rognosis {1007}. Amplification ofCCND1 occurs in about 20% of DCISand is more commonly found in highgrade than in low grade DCIS (32% ver-sus 8%) {2700}. The cyclin D1 pro t e i nwas detected in 50% of cases, and highlevels were more likely in low grade thanin the intermediate and high grade DCIS{2700}. Although so far no oncogene hasbeen identified on chromosome 20q13,amplification of this region was fre q u e n t-ly found in DCIS {134,856}.
TP53 mutationsThe TP53 protein is a transcription fac-tor involved in the control of cell pro l i f-eration, response to DNA damage,apoptosis and several other signalingpathways. It is the most commonlymutated tumour suppressor gene insporadic breast cancer {196} and this is
generally associated with aggre s s i v ebiological features and poor clinicaloutcome. Most T P 5 3 mutations are mis-sense point mutations resulting in aninactivated protein that accumulates inthe cell nucleus {72,712}. In DCIS, T P 5 3mutations were found with diff e rent fre-quency among the three histologicalgrades, ranging from rare in low gradeDCIS, 5% in intermediate-grade, andcommon (40%) in high grade DCIS{ 7 1 2 , 3 0 4 8 } .
Prognosis and predictive factorsThe most important factor influencingthe possibility of re c u r rence is persist-ence of neoplastic cells post-excision;p r i m a ry and re c u r rent DCIS generallyhave the same LOH pattern, with acqui-sition of additional alterations in the latter{1670} The significance of margins ismainly to ascertain complete excision. Inrandomized clinical trials, comedon e c rosis was found to be an import a n tp redictor of local re c u r rence in theNSABP-B17 trial {2843}, while solid andc r i b r i f o rm growth patterns along withinvolved margin of excision were foundto be predictive of local re c u r rence inE O RTC-10853 trial {270,271}. In re t ro-spective trials, on the other hand, highnuclear grade, larger lesion size, come-do necrosis and involved margins ofexcision were all found to be pre d i c t i v eof local re c u r rence following breast con-servative treatment for DCIS. Although mastectomy has long been thetraditional treatment for this disease, itlikely re p resents over- t reatment for manypatients, particularly those with small,mammographically detected lesions.C a reful mammographic and pathologicevaluation are essential to help assesspatient suitability for breast conservingt reatment. While excision and radiation therapy ofDCIS (with or without Tamoxifen) havesignificantly reduced the chances ofre c u r rence {866,870}, some patientswith small, low grade lesions appear tobe adequately treated with excisionalone, whereas those with extensivelesions may be better served by mas-t e c t o m y. Better prognostic markers areneeded to help determine which DCISlesions are likely to recur or to pro g re s sto invasive cancer following breast con-serving treatment. The optimal manage-ment is evolving as data accumulatesf rom a variety of prospective studies.
Fig. 1.95 Unusual intraductal proliferation. A The lesion shows a uniform cell population pro-liferating in a solid pagetoid pattern similar to lob-ular neoplasia, but the cells appear more adhe-rent than in typical lobular neoplasia (LN). B Double immunostain is positive for bothC K 3 4βE12 (purple) and E-cadherin (brown), quali-fying the lesion as a hybrid positive type that maysuggest the diagnosis of DCIS.
A
B
73Intraductal proliferative lesions
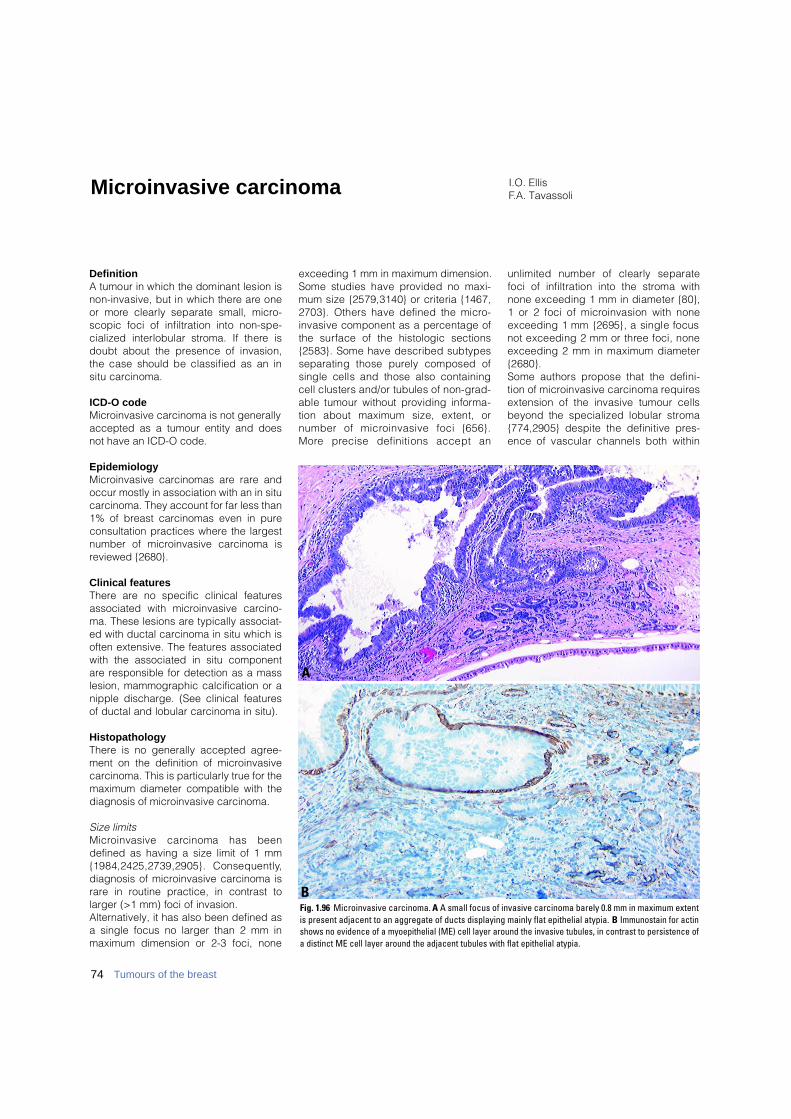
DefinitionA tumour in which the dominant lesion isnon-invasive, but in which there are oneor more clearly separate small, micro-scopic foci of infiltration into non-spe-cialized interlobular stroma. If there isdoubt about the presence of invasion,the case should be classified as an insitu carcinoma.
ICD-O codeMicroinvasive carcinoma is not generallyaccepted as a tumour entity and doesnot have an ICD-O code.
EpidemiologyMicroinvasive carcinomas are rare andoccur mostly in association with an in situcarcinoma. They account for far less than1% of breast carcinomas even in pureconsultation practices where the largestnumber of microinvasive carcinoma isreviewed {2680}.
Clinical featuresThere are no specific clinical featuresassociated with microinvasive carcino-ma. These lesions are typically associat-ed with ductal carcinoma in situ which isoften extensive. The features associatedwith the associated in situ componentare responsible for detection as a masslesion, mammographic calcification or anipple discharge. (See clinical featuresof ductal and lobular carcinoma in situ).
HistopathologyThere is no generally accepted agree-ment on the definition of microinvasivecarcinoma. This is particularly true for themaximum diameter compatible with thediagnosis of microinvasive carcinoma.
Size limitsM i c roinvasive carcinoma has beendefined as having a size limit of 1 mm{1984,2425,2739,2905}. Consequently,diagnosis of microinvasive carcinoma israre in routine practice, in contrast tolarger (>1 mm) foci of invasion.Alternatively, it has also been defined asa single focus no larger than 2 mm inmaximum dimension or 2-3 foci, none
exceeding 1 mm in maximum dimension.Some studies have provided no maxi-mum size {2579,3140} or criteria {1467,2703}. Others have defined the micro-invasive component as a percentage ofthe surface of the histologic sections{2583}. Some have described subtypesseparating those purely composed ofsingle cells and those also containingcell clusters and/or tubules of non-grad-able tumour without providing inform a-tion about maximum size, extent, ornumber of microinvasive foci {656}.M o re precise definitions accept an
unlimited number of clearly separatefoci of infiltration into the stroma withnone exceeding 1 mm in diameter {80},1 or 2 foci of microinvasion with noneexceeding 1 mm {2695}, a single focusnot exceeding 2 mm or three foci, noneexceeding 2 mm in maximum diameter{2680}. Some authors propose that the defini-tion of microinvasive carcinoma re q u i re sextension of the invasive tumour cellsbeyond the specialized lobular stro m a{774,2905} despite the definitive pre s-ence of vascular channels both within
I.O. EllisF.A. TavassoliMicroinvasive carcinoma
Fig. 1.96 Microinvasive carcinoma. A A small focus of invasive carcinoma barely 0.8 mm in maximum extentis present adjacent to an aggregate of ducts displaying mainly flat epithelial atypia. B Immunostain for actinshows no evidence of a myoepithelial (ME) cell layer around the invasive tubules, in contrast to persistence ofa distinct ME cell layer around the adjacent tubules with flat epithelial atypia.
B
A
74 Tumours of the breast

the specialized lobular stroma andimmediately surrounding the basementmembrane that invests the ducts.
Associated lesionsTy p i c a l l y, microinvasive carc i n o m aoccur in larger areas of high grade DCISin which the tumour cell populationextends to involve lobular units or are a sof benign disease. M i c roinvasion occurs in association notonly with all grades of DCIS, includingp a p i l l a ry DCIS, but also with other pre-cursor lesions of invasive breast cancer,e.g. lobular neoplasia (LN) {1226,1249,1993}, indicating that at least somef o rms of lobular neoplasia behave astrue precursors of invasive lesions.
S t romal re a c t i o nM i c roinvasion is most often present in a background of significant periductal /perilobular lymphocytic infiltrate or ana l t e red desmoplastic stroma, feature soften present in cases of comedo DCIS.Angulation of mesenchymal structure smay be emphasized by the plane ofsectioning and can produce feature sreminiscent of invasive carc i n o m a .Basement membrane structures in suchfoci may be discontinuous but it isunusual to lose the entire basementmembrane around such a lesion.Similarly myoepithelial cells may bes c a rce but are rarely totally absent insuch are a s .
Change in morphologyWhen true invasion extends into non-specialized stroma, the islands oftumour cells frequently adopt a diff e re n tmorphological character which is moretypical of well established invasivem a m m a ry carcinoma of ductal NOS
type and is distinct from the pattern sseen with cancerization of lobules.
Differential diagnosisWhen there is doubt about the presenceof invasion and particularly, if uncertaintypersists even after recuts and immuno-stains for detection of myoepithelial cells,the case should be diagnosed as an insitu carcinoma. Similarly, suspiciouslesions which disappear on deeper lev-els should be regarded as unproven,with no definite evidence of establishedinvasion. Invasion is associated with a loss ofimmunoreactivity to myoepithelial cells. Avariety of markers is available for theidentification of myoepithelial cells{3181}. The most helpful include smoothmuscle actin, calponin, and smooth mus-cle myosin (heavy chain); the latter inparticular shows the least cross-reactivi-ty with myofibroblasts that may mimic amyoepithelial cell layer when apposed tothe invasive cells.
Prognosis and predictive factorsIn true microinvasive carcinomas of thebreast, the incidence of metastatic dis-ease in axillary lymph nodes is very lowand the condition is generally managedclinically as a form of DCIS. However, given the lack of a generallyaccepted standardized definition ofmicroinvasive carcinoma, there is littleevidence on the behaviour of microinva-sive carcinoma. A recent detailed reviewof the literature {2425} concluded that avariety of different diagnostic criteria anddefinitions have been used and as a con-sequence it is difficult to draw any defin-itive conclusions. There are studies that have found no evi-dence of axillary node metastases asso-
ciated with a finite number of invasivefoci <1 mm in maximum dimension or asingle invasive focus <2 mm {2680,2695}. Others have shown a small per-centage (up to 5%) with axillary nodemetastases {2453,2744} or havedescribed up to 20% axillary nodemetastases {656,1472,2282,2579,2583}.Of 38 women who had undergone mas-tectomy for their minimally invasive carci-nomas (a single focus <2 mm or up to 3invasive foci, none exceeding 1 mm, withno axillary node metastases), developedrecurrences or metastases {2680}. Thefew other studies with comparable, butnot exactly the same definition, and fol-low-up data support the excellent prog-nosis for these tumours within the shortperiods of available follow-up {2453,2695,3140}.In practice, it may be impossible forpathologists to routinely examine anentire sample exhaustively. Therefore, itis quite possible that small foci of inva-sive carcinoma may be missed, particu-larly in the setting of extensive in situ car-cinoma. For this reason, it may be appro-priate to sample the lowest axillary lymphnodes, or sentinel node as a matter ofroutine, when treating patients by mas-tectomy for extensive DCIS with or with-out accompanying microinvasive carci-noma {1472}. The pathology re p o rtshould provide the size of the largestfocus along with the number of foci ofinvasion, noting any special studies u t i-lized to arrive at the diagnosis, ie. 1.3 mm,2 foci, immunocytochemistry.Until there is a generally accepted defini-tion with reliable follow-up data, microin-vasive carcinoma of the breast remainsan evolving concept that has notreached the status of a WHO-endorseddisease entity.
B CAFig. 1.97 Microinvasive carcinoma. A Two ducts are filled by DCIS, while small clusters of carcinoma cells invade the stroma (upper right quadrant of the field)admixed with a dense lymphocytic infiltrate. B Higher magnification shows small invasive cell clusters within stromal spaces distributed over a 0.7 mm area andsurrounded by a dense lymphocytic infiltrate. C Immunostain for actin decorates the vessel walls, while absence of myoepithelial cells around the tumour cell clus-ters confirms their invasive nature.
75Microinvasive carcinoma
DefinitionP a p i l l a ry neoplasms are characterizedby epithelial proliferations supported byf i b rovascular stalks with or without anintervening myoepithelial cell layer.They may occur anywhere within theductal system from the nipple to the ter-minal ductal lobular unit (TDLU) andmay be benign (intraductal papilloma),atypical, or malignant (intraductal papil-l a ry carcinoma).
Intraductal papilloma
A proliferation of epithelial and myoep-ithelial cells overlying fibrovascular stalkscreating an arborescent structure withinthe lumen of a duct.Intraductal papilloma of the breast isbroadly divided into central (large duct)papilloma, usually located in the subare-olar region, and peripheral papillomaarising in the TDLU {2092}. The confus-ing term "papillomatosis" should beavoided as it has been used for usualductal hyperplasia as well as for multiplepapillomas.
ICD-O code 8503/0
Central papilloma
SynonymsLarge duct papilloma, major duct pa-p i l l o m a .
EpidemiologyThe incidence of the various forms ofintraductal papillary lesions is uncert a i ndue to the lack of consistent term i n o l o-g y. Overall, less than 10% of benignb reast neoplasms correspond to papil-lomas {413,1098}. Central papillomascan occur at any age, but the majorityp resent during the fourth and fifthdecades {1098,1945}.
Clinical featuresUnilateral sanguineous, or sero -sanguineous, nipple discharge is themost frequent clinical sign, and isobserved in 64-88% of patients {3148}. Apalpable mass is less fre q u e n t .Mammographic abnormalities include ac i rcumscribed re t ro - a reolar mass ofbenign appearance, a solitary retro-areo-lar dilated duct and, rarely, microcalcifi-cations {401,3148}. Small papillomasmay be mammographically occultbecause of their location in the centraldense breast and usually lack of calcifi-cation. Typical sonographic feature sinclude a well defined smooth-walled,solid, hypoechoic nodule or a lobulated,smooth-walled, cystic lesion with solidcomponents. Duct dilatation with visiblesolid intraluminal echoes is common{3176}. Galactography shows an intraluminalsmooth or irregular filling defect asso-ciated with obstructed or dilated ducts,or a complete duct obstruction with re t-
rograde flow of contrast material.Galactography may be useful to theb reast surgeon in identifying and local-izing the discharging duct, prior to ductexcision {3148}.
Macroscopy Palpable lesions may form well circum-scribed round tumours with a cauliflower-like mass attached by one or more pedi-cles to the wall of a dilated duct contain-ing serous and/or sanguineous fluid. Thesize of central papillomas varies consid-erably from a few millimetres to 3-4 cm orlarger and they can extend along theduct for several centimetres.
G. MacGroganF. MoinfarU. Raju
Intraductal papillary neoplasms
Fig. 1.100 Papilloma, gross. Nodular mass in acystic duct.
BAFig. 1.99 Central papilloma. A Smooth intraluminal filling defect associated with duct dilatation. B W e l ldefined smooth wall cystic lesion with a solid component.
Fig. 1.98 Distribution of papillomas in breast.
76 Tumours of the breast
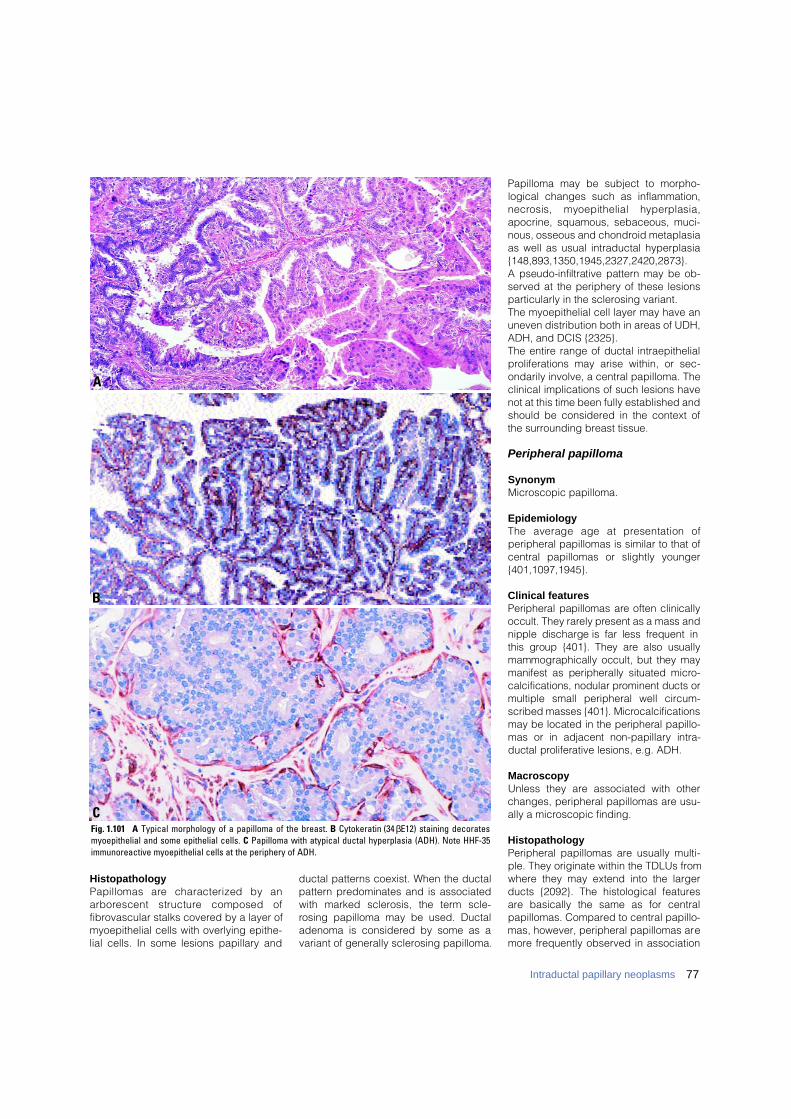
77Intraductal papillary neoplasms
HistopathologyPapillomas are characterized by ana r b o rescent structure composed offibrovascular stalks covered by a layer ofmyoepithelial cells with overlying epithe-lial cells. In some lesions papillary and
ductal patterns coexist. When the ductalpattern predominates and is associatedwith marked sclerosis, the term scle-rosing papilloma may be used. Ductaladenoma is considered by some as avariant of generally sclerosing papilloma.
Papilloma may be subject to morpho-logical changes such as inflammation,n e c rosis, myoepithelial hyperplasia,apocrine, squamous, sebaceous, muci-nous, osseous and chondroid metaplasiaas well as usual intraductal hyperplasia{148,893,1350,1945,2327,2420,2873}.A pseudo-infiltrative pattern may be ob-served at the periphery of these lesionsparticularly in the sclerosing variant.The myoepithelial cell layer may have anuneven distribution both in areas of UDH,ADH, and DCIS {2325}. The entire range of ductal intraepithelialproliferations may arise within, or sec-ondarily involve, a central papilloma. Theclinical implications of such lesions havenot at this time been fully established andshould be considered in the context ofthe surrounding breast tissue.
Peripheral papilloma
SynonymMicroscopic papilloma.
EpidemiologyThe average age at presentation ofperipheral papillomas is similar to that ofcentral papillomas or slightly younger{401,1097,1945}.
Clinical featuresPeripheral papillomas are often clinicallyoccult. They rarely present as a mass andnipple discharge is far less frequent inthis group {401}. They are also usuallymammographically occult, but they maymanifest as peripherally situated micro-calcifications, nodular prominent ducts ormultiple small peripheral well circ u m-scribed masses {401}. Micro c a l c i f i c a t i o n smay be located in the peripheral papillo-mas or in adjacent non-papillary intra-ductal proliferative lesions, e.g. ADH.
MacroscopyUnless they are associated with otherchanges, peripheral papillomas are usu-ally a microscopic finding.
HistopathologyPeripheral papillomas are usually multi-ple. They originate within the TDLUs fromwhere they may extend into the largerducts {2092}. The histological featuresare basically the same as for centralpapillomas. Compared to central papillo-mas, however, peripheral papillomas aremore frequently observed in association
Fig. 1.101 A Typical morphology of a papilloma of the breast. B Cytokeratin (34 βE12) staining decoratesmyoepithelial and some epithelial cells. C Papilloma with atypical ductal hyperplasia (ADH). Note HHF-35immunoreactive myoepithelial cells at the periphery of ADH.
C
B
A

with concomitant usual ductal hyperpla-sia, atypical intraductal hyperplasia,ductal carcinoma in situ or invasive car-cinoma as well as with sclerosing adeno-sis or radial scar {1097,1945,2091,2092}.The term micropapilloma has beenapplied to the smallest type of peripheralpapillomas corresponding to multiplemicroscopic papillomas that grow in fociof adenosis. Collagenous spherulosis,consisting of round eosinophilicspherules of basement membrane (typeIV collagen), edged by myoepithelialcells may be seen in some peripheralpapillomas.
Atypical papilloma
Atypical intraductal papillomas are char-acterized by the presence of a focalatypical epithelial proliferation with lowgrade nuclei. Such intraepithelial prolifer-ations may occasionally resemble atypi-cal ductal hyperplasia (ADH) or smallfoci of low grade DCIS.
Prognosis and predictive featuresof benign and atypical papillomas
The risk of subsequent invasive carcino-ma associated with papillomas or atypi-cal papillomas should be appreciated inthe context of the surrounding breast tis-sue. A benign papilloma without sur-rounding changes is associated with aslightly increased relative risk of subse-quent invasive breast carcinoma, similarto that of moderate or florid usual ductalhyperplasia in the breast pro p e r{885,2151}. The relative risk associated
with peripheral papilloma may be highercompared to central papilloma. However,this risk also depends on the concurrentpresence of other forms of proliferativedisease and as yet no study has beendesigned to specifically answer thisquestion {2151}. There is disagreementas to whether the risk of subsequentinvasive breast carcinoma applies only tothe same site in the ipsilateral breast orapplies to both breasts {2151,2326}. Thesignificance of atypia within a papillomais still not clear and is obscured by thefrequent concurrent presence of atypiawithin the surrounding breast parenchy-ma. It appears that if epithelial atypia isconfined to the papilloma without sur-rounding proliferation or atypia the risk ofsubsequent invasive breast carcinoma issimilar to that of non-atypical papilloma.As expected, epithelial atypia whenpresent simultaneously both within andoutside a papilloma is associated with amoderate to highly increased relative risk{2151}; this is not a reflection of the riskassociated with pure atypical papilloma,however.The standard treatment for papillomashas been complete excision with micro-scopic assessment of surro u n d i n gbreast tissue. Because of potential vari-ability within a papillary lesion, completeexcision is prudent, regardless of thefindings in a previous core biopsy.The differential diagnosis of benign andmalignant papillary lesions on fro z e nsection can be extremely difficult and adefinitive diagnosis should always bemade only after examination of paraffinembedded material.
Intraductal papillary carcinoma
ICD-O code 8503/2
SynonymP a p i l l a ry carcinoma, non-invasive.
DefinitionThis lesion is located within a variablydistended duct and may extend into itsbranches. It is characterized by pro l i f-eration of fibrovascular stalks and itsdiagnosis re q u i res that 90% or more of
Table 1.15Differential diagnosis of benign papilloma and intraductal papillary carcinoma.
Fig. 1.102 Central papilloma. A An arborescentstructure composed of papillary fronds within adilated duct. B Myoepithelial hyperplasia with SMApositive “myoid” transformation.
A
B
Feature Papilloma Papillary intraductal carcinoma
Cell types covering fibrovascular stalks Epithelial and myoepithelial Epithelial (myoepithelial cells may be seen at periphery of duct wall)*
Nuclei Normochromatic vesicular chromatin; May be hyperchromatic, with diffuse variable in size and shape chromatin: relatively uniform in size and shape
Apocrine metaplasia Frequent Absent
Fibrovascular stalks Usually broad and present throughout lesion; Often fine and may be absent in some areas;may show sclerosis sclerosis uncommon
Immunohistochemical markers for myoepithelial Positive Negative*cells (e.g. smooth muscle actin, HMW-CK [such as CK 5/6])
* Myoepithelial cells may be present in some papillary carcinomas–see text for explanation.
78 Tumours of the breast
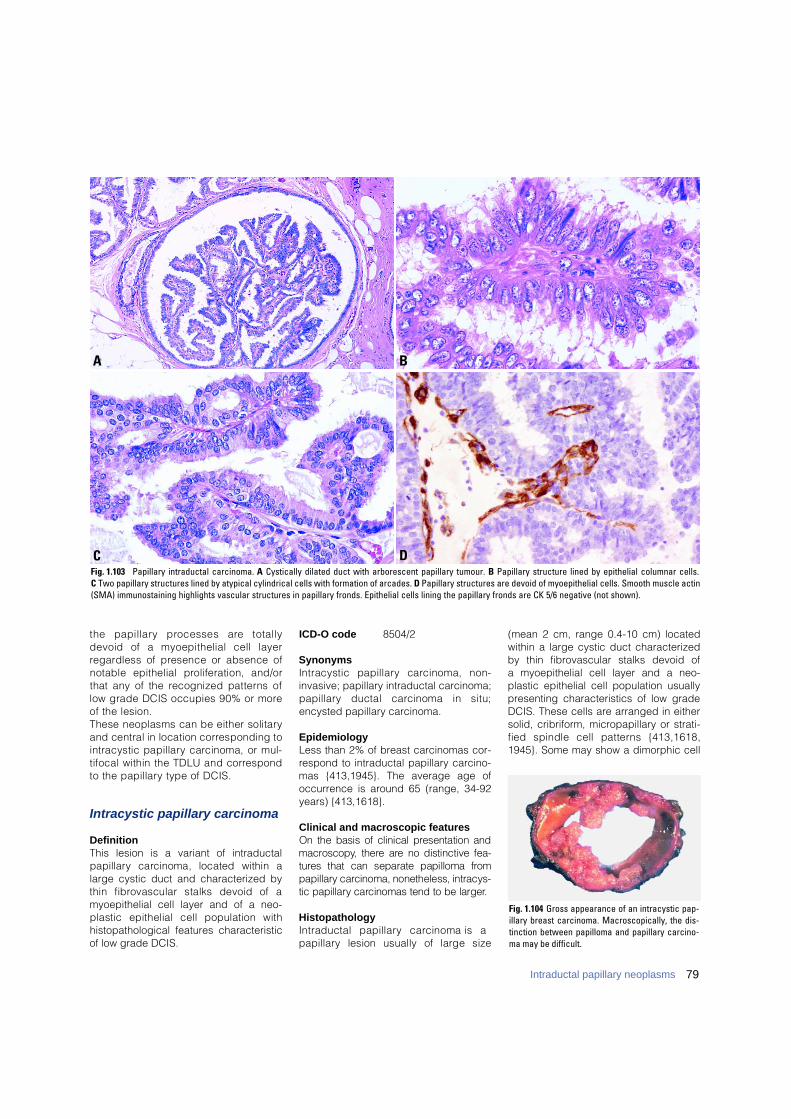
the papillary processes are totallydevoid of a myoepithelial cell layerre g a rdless of presence or absence ofnotable epithelial proliferation, and/orthat any of the recognized patterns oflow grade DCIS occupies 90% or moreof the lesion.These neoplasms can be either solitaryand central in location corresponding tointracystic papillary carcinoma, or mul-tifocal within the TDLU and corre s p o n dto the papillary type of DCIS.
Intracystic papillary carcinoma
DefinitionThis lesion is a variant of intraductal p a p i l l a ry carcinoma, located within alarge cystic duct and characterized bythin fibrovascular stalks devoid of amyoepithelial cell layer and of a neo-plastic epithelial cell population withhistopathological features characteristicof low grade DCIS.
ICD-O code 8504/2
SynonymsIntracystic papillary carcinoma, non-invasive; papillary intraductal carcinoma;p a p i l l a ry ductal carcinoma in situ;encysted papillary carcinoma.
EpidemiologyLess than 2% of breast carcinomas cor-respond to intraductal papillary carcino-mas {413,1945}. The average age ofoccurrence is around 65 (range, 34-92years) {413,1618}.
Clinical and macroscopic featuresOn the basis of clinical presentation andm a c ro s c o p y, there are no distinctive fea-t u res that can separate papilloma fro mp a p i l l a ry carcinoma, nonetheless, intracys-tic papillary carcinomas tend to be larger.
HistopathologyIntraductal papillary carcinoma is a p a p i l l a ry lesion usually of large size
(mean 2 cm, range 0.4-10 cm) locatedwithin a large cystic duct characterizedby thin fibrovascular stalks devoid of a myoepithelial cell layer and a neo-plastic epithelial cell population usually presenting characteristics of low gradeDCIS. These cells are arranged in eithersolid, cribriform, micropapillary or strati-fied spindle cell patterns {413,1618,1945}. Some may show a dimorphic cell
DC
BA
Fig. 1.103 Papillary intraductal carcinoma. A Cystically dilated duct with arborescent papillary tumour. B Papillary structure lined by epithelial columnar cells. C Two papillary structures lined by atypical cylindrical cells with formation of arcades. D Papillary structures are devoid of myoepithelial cells. Smooth muscle actin(SMA) immunostaining highlights vascular structures in papillary fronds. Epithelial cells lining the papillary fronds are CK 5/6 negative (not shown).
Fig. 1.104 Gross appearance of an intracystic pap-illary breast carcinoma. Macroscopically, the dis-tinction between papilloma and papillary carcino-ma may be difficult.
79Intraductal papillary neoplasms
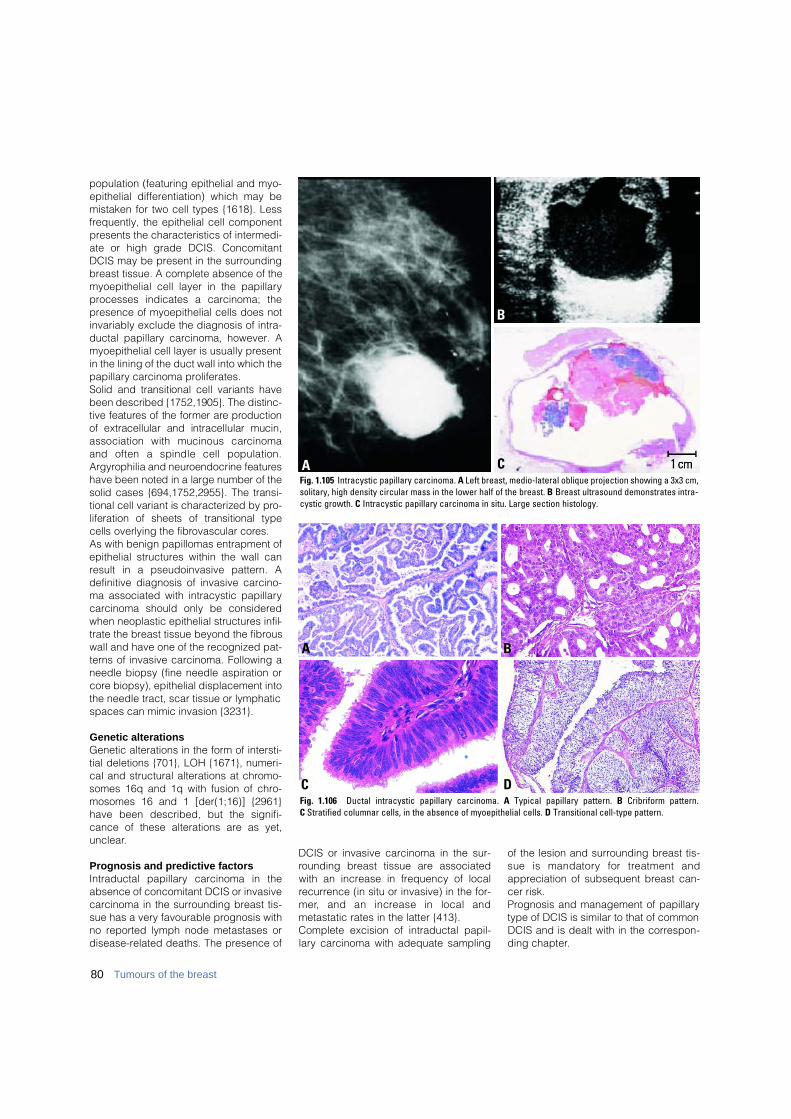
population (featuring epithelial and myo-epithelial differentiation) which may bemistaken for two cell types {1618}. Lessfrequently, the epithelial cell componentpresents the characteristics of intermedi-ate or high grade DCIS. ConcomitantDCIS may be present in the surroundingbreast tissue. A complete absence of themyoepithelial cell layer in the papillaryprocesses indicates a carcinoma; thepresence of myoepithelial cells does notinvariably exclude the diagnosis of intra-ductal papillary carcinoma, however. Amyoepithelial cell layer is usually presentin the lining of the duct wall into which thepapillary carcinoma proliferates.Solid and transitional cell variants havebeen described {1752,1905}. The distinc-tive features of the former are pro d u c t i o nof extracellular and intracellular mucin,association with mucinous carc i n o m aand often a spindle cell population.A r g y rophilia and neuroendocrine feature shave been noted in a large number of thesolid cases {694,1752,2955}. The transi-tional cell variant is characterized by pro-liferation of sheets of transitional typecells overlying the fibrovascular core s .As with benign papillomas entrapment ofepithelial structures within the wall canresult in a pseudoinvasive pattern. Adefinitive diagnosis of invasive carcino-ma associated with intracystic papillarycarcinoma should only be consideredwhen neoplastic epithelial structures infil-trate the breast tissue beyond the fibrouswall and have one of the recognized pat-terns of invasive carcinoma. Following aneedle biopsy (fine needle aspiration orcore biopsy), epithelial displacement intothe needle tract, scar tissue or lymphaticspaces can mimic invasion {3231}.
Genetic alterationsGenetic alterations in the form of intersti-tial deletions {701}, LOH {1671}, numeri-cal and structural alterations at chromo-somes 16q and 1q with fusion of chro-mosomes 16 and 1 [der(1;16)] {2961}have been described, but the signifi-cance of these alterations are as yet,unclear.
Prognosis and predictive factorsIntraductal papillary carcinoma in theabsence of concomitant DCIS or invasivecarcinoma in the surrounding breast tis-sue has a very favourable prognosis withno reported lymph node metastases ordisease-related deaths. The presence of
DCIS or invasive carcinoma in the sur-rounding breast tissue are associatedwith an increase in frequency of localrecurrence (in situ or invasive) in the for-m e r, and an increase in local andmetastatic rates in the latter {413}. Complete excision of intraductal papil-lary carcinoma with adequate sampling
of the lesion and surrounding breast tis-sue is mandatory for treatment andappreciation of subsequent breast can-cer risk.Prognosis and management of papillarytype of DCIS is similar to that of commonDCIS and is dealt with in the correspon-ding chapter.
B
CFig. 1.105 Intracystic papillary carcinoma. A Left breast, medio-lateral oblique projection showing a 3x3 cm,solitary, high density circular mass in the lower half of the breast. B Breast ultrasound demonstrates intra-cystic growth. C Intracystic papillary carcinoma in situ. Large section histology.
A
BA
DCFig. 1.106 Ductal intracystic papillary carcinoma. A Typical papillary pattern. B Cribriform pattern. C Stratified columnar cells, in the absence of myoepithelial cells. D Transitional cell-type pattern.
80 Tumours of the breast
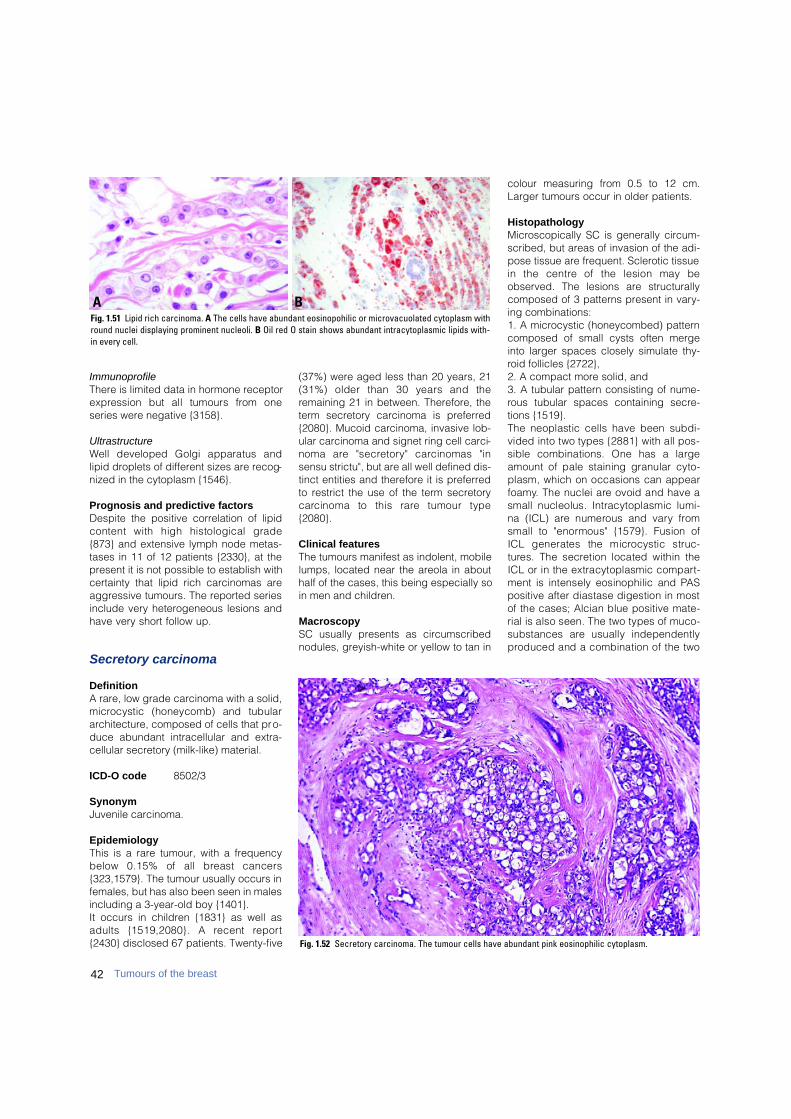
42 Tumours of the breast
ImmunoprofileThere is limited data in hormone receptore x p ression but all tumours from oneseries were negative {3158}.
UltrastructureWell developed Golgi apparatus andlipid droplets of different sizes are recog-nized in the cytoplasm {1546}.
Prognosis and predictive factorsDespite the positive correlation of lipidcontent with high histological grade{873} and extensive lymph node metas-tases in 11 of 12 patients {2330}, at thepresent it is not possible to establish withcertainty that lipid rich carcinomas areaggressive tumours. The reported seriesinclude very heterogeneous lesions andhave very short follow up.
Secretory carcinoma
DefinitionA rare, low grade carcinoma with a solid,m i c rocystic (honeycomb) and tubulararchitecture, composed of cells that pro-duce abundant intracellular and extra-cellular secretory (milk-like) material.
ICD-O code 8502/3
SynonymJuvenile carcinoma.
EpidemiologyThis is a rare tumour, with a frequencybelow 0.15% of all breast cancers{323,1579}. The tumour usually occurs infemales, but has also been seen in malesincluding a 3-year-old boy {1401}.It occurs in children {1831} as well asadults {1519,2080}. A recent re p o rt{2430} disclosed 67 patients. Twenty-five
(37%) were aged less than 20 years, 21(31%) older than 30 years and theremaining 21 in between. Therefore, theterm secretory carcinoma is preferred{2080}. Mucoid carcinoma, invasive lob-ular carcinoma and signet ring cell carci-noma are "secre t o ry" carcinomas "insensu strictu", but are all well defined dis-tinct entities and therefore it is preferredto restrict the use of the term secretoryc a rcinoma to this rare tumour type{2080}.
Clinical features The tumours manifest as indolent, mobilelumps, located near the areola in abouthalf of the cases, this being especially soin men and children.
Macroscopy SC usually presents as circumscribednodules, greyish-white or yellow to tan in
colour measuring from 0.5 to 12 cm.Larger tumours occur in older patients.
HistopathologyMicroscopically SC is generally circum-scribed, but areas of invasion of the adi-pose tissue are frequent. Sclerotic tissuein the centre of the lesion may beobserved. The lesions are structurallycomposed of 3 patterns present in vary-ing combinations: 1. A microcystic (honeycombed) patterncomposed of small cysts often mergeinto larger spaces closely simulate thy-roid follicles {2722}, 2. A compact more solid, and 3. A tubular pattern consisting of nume-rous tubular spaces containing secre-tions {1519}. The neoplastic cells have been subdi-vided into two types {2881} with all pos-sible combinations. One has a largeamount of pale staining granular cyto-plasm, which on occasions can appearf o a m y. The nuclei are ovoid and have asmall nucleolus. Intracytoplasmic lumi-na (ICL) are numerous and vary fro msmall to "enormous" {1579}. Fusion ofICL generates the microcystic struc-t u res. The secretion located within theICL or in the extracytoplasmic compart-ment is intensely eosinophilic and PA Spositive after diastase digestion in mostof the cases; Alcian blue positive mate-rial is also seen. The two types of muco-substances are usually independentlyp roduced and a combination of the two
BAFig. 1.51 Lipid rich carcinoma. A The cells have abundant eosinopohilic or microvacuolated cytoplasm withround nuclei displaying prominent nucleoli. B Oil red O stain shows abundant intracytoplasmic lipids with-in every cell.
Fig. 1.52 Secretory carcinoma. The tumour cells have abundant pink eosinophilic cytoplasm.

as seen in the "tagetoid pattern" of ICLdescribed by Gad and Azzopardi {943}is rarely evident.Mitoses and necrotic areas are rare .Ductal in situ carcinoma of either thes e c re t o ry or low grade type may bep resent, either at the margins or withinthe tumour {2430}.
I m m u n o p r o f i l eEMA, alpha lactalbumin and S-100 pro-tein are frequently expressed in SC{323,1579,2430}. Estrogen re c e p t o r sa re mostly undetectable.
Prognosis and predictive factors SC has an extremely favourable pro g n o-sis in children and adolescents butseems slightly more aggressive in olderpatients {2881}. Isolated re c u r rences inc h i l d ren are exceptional {52}, but therisk of nodal involvement is similar inyoung and older patients {2430}.A x i l l a ry lymph node metastases arefound in approximately 15% of patients{2814} but metastases are confined to 4lymph nodes at the most {52}.Tumours less than 2 cm in size areunlikely to pro g ress {2881}. Simple m a s t e c t o m y, as opposed to excision ofthe tumour, has led to a cure, with theexception of the case re p o rted by Meis{1860}. Recurrence of the tumour mayappear after 20 years {1519}, and pro-longed follow up is advocated. Fatalcases are the exception {1519,2881}and have never been re p o rted in chil-d re n .
Oncocytic carcinoma
DefinitionA breast carcinoma composed of morethan 70% oncocytic cells.
ICD-O code 8290/3
Historical annotationOncocyte (a Greek derived word )means "swollen cell", in this case due toan accumulation of mitochondria. Thet e rm oncocyte is used when mitochon-dria occupy 60% of the cytoplasm{990}. Oncocytic tumours can be seenin various organs and tissues {2271,2 4 0 5 } .In oncocytes, mitochondria are diff u s e l ydispersed throughout the cytoplasmwhile in mitochondrion-rich cells theya re grouped to one cell pole {2948}.The pro p o rtion of oncocytes pre s e n twithin a tumour re q u i red to call it onco-cytic has been arbitrarily proposed byvarious authors and varies from organ toorgan. In a small series of breast onco-cytic carcinomas, Damiani et al. {616},using immunohistochemistry with an anti
mitochondrial antibody, found 70-90% ofthe neoplastic cells packed massivelywith immunoreactive granules.
EpidemiologyOnly occasional cases have beendescribed {566,616}. However, the inci-dence in the breast is probably underes-timated as oncocytes are easily over-looked or misdiagnosed as apocrine ele-ments {615}. All described patients havebeen over 60 years old. There is nopredilection for site. One case occurredin a man {566}.
MacroscopyThe largest tumour measured 2.8 cm{616}.
HistopathologyThe tumours are all similar with defined,c i rcumscribed borders and vary fro mglandular to solid. The cells have abun-dant cytoplasm filled with smalleosinophilic granules. Nuclei are monot-onous and round to ovoid with a con-spicuous nucleolus. Mitoses are not fre-quent. In situ carcinomas with a papil-l a ry appearance have been described{ 6 1 6 } .
Differential diagnosis Oncocytic carcinomas can be distin-guished from apocrine, neuro e n d o c r i n ec a rcinomas and oncocytic myoepitheliallesions {615,945,2013} by their immu-n o p h e n o t y p e .
Fig. 1.53 Secretory carcinoma. The tumour cellshave abundant pink eosinophilic cytoplasm.
Fig. 1.54 Secretory carcinoma. Abundant secretorymaterial is evident.
Fig. 1.55 Oncocytic carcinoma. Note well circumscribed nodule and cells with abundant eosinophilic cytoplasm.
43Invasive breast carcinoma

Immunoprofile The cases studied by Damiani et al. {616}showed diffuse and strong immunore a c-tivity with an anti mitochondrial antibody.Epithelial membrane antigen outlined theluminal borders of neoplastic glandswhen these were present. GCDFP-15 wasabsent in 3 cases and ER was observedin 90% of the cells in one {616}.
Prognosis and predictive factorsThe follow up and number of re p o rt e dcases is too small to allow meaningfuldiscussion of prognosis.
Adenoid cystic carcinoma
D e f i n i t i o nA carcinoma of low aggressive potential,histologically similar to the salivary glandc o u n t e r p a rt .
ICD-O code 8 2 0 0 / 3
S y n o n y m sC a rcinoma adenoides cysticum, adeno-cystic basal cell carcinoma, cylindro m a-tous carc i n o m a .
E p i d e m i o l o g yAdenoid cystic carcinoma (ACC) re p re-sent about 0.1% of breast carc i n o m a s{149,1581}. It is important that stringentcriteria are adopted to avoid misclassi-fied lesions as found in about 50% of thecases re c o rded by the ConnecticutTumor Registry {2815}. The age distribu-tion, is similar to that seen in infiltratingduct carcinomas in general {2419}.
Clinical featuresThe lesions are equally distributedbetween the two breasts and about 50%a re found in the sub-periareolar re g i o n{149}. They may be painful or tender andunexpectedly cystic. A discrete nodule isthe most common pre s e n t a t i o n .
Macroscopy The size varies from 0.7 to 12 cm, with anaverage amongst most re p o rted cases of3 cm. Tumours are usually circ u m s c r i b e d ,and microcysts are evident. They arepink, tan or grey in appearance {2309,2 4 1 9 } .
H i s t o p a t h o l o g yACC of the breast is very similar to that ofthe salivary gland, lung and cervix {1838}.
T h ree basic patterns are seen: trabecu-l a r- t u b u l a r, cribriform and solid. The 3p a t t e rns have been used by Ro et al.{2381} to develop their grading system.The cribriform pattern is the most char-acteristic as the neoplastic areas arep e rforated by small apert u res like asieve. The "apert u res" are of two types: The first, also re f e r red to as pseudolu-mens {1406}, results from intratumoralinvaginations of the stroma (stro m a lspace). Accord i n g l y, this type of spaceis of varying shape, mostly round, andcontains myxoid acidic stromal muco-substances which stain with Alcian blue{152} or straps of collagen with smallcapillaries. Sometimes the stro m a lspaces are filled by hyaline collagenand the smallest are constituted bysmall spherules or cylinders of hyalinematerial which has been shown ultra-structurally and immunohistochemicallyto be basal lamina {463}. With immuno-h i s t o c h e m i s t ry a rim of laminin and col-lagen IV positive material outlines thes t romal spaces. The second type ofspace is more difficult to see as it is lessn u m e rous and usually composed ofsmall lumina. These are genuine secre-
t o ry glandular structures (glandularspace) which contain eosinophilic gran-ular secretion of neutral mucosub-stances, and are periodic acid-Schiffpositive after diastase digestion {152}.The dual structural pattern reflects adual cell component. The basaloid cellhas scanty cytoplasm, a round to ovoidnucleus and one to two nucleoli {1581}.It constitutes the bulk of the lesion andalso lines the cribriform stromal spaces.The second type of cell lines the trueglandular lumina, and has eosinophiliccytoplasm and round nuclei similar tothose of the basaloid cells. A third typeof cell seen in 14% of cases byTavassoli and Norris {2885} consists ofsebaceous elements that can occasion-ally be numero u s .ACC contains a central core of neoplas-tic cells, surrounded by areas of inva-sion; ductal carcinoma in situ is absentat the periphery. The stroma varies fro mtissue very similar to that seen in then o rmal breast to desmoplastic, myxoidor even extensively adipose.ACC has been seen in association withadenomyoepithelioma {2994} and lowgrade syringomatous (adenosquamous)c a rcinoma {2419} which suggests aclose relationship among these com-bined epithelial and myoepithelialt u m o u r s .
Differential diagnosisACC must be distinguished from benigncollagenous spherulosis {519} and fro mc r i b r i f o rm carcinoma, which more close-ly simulates ACC. Cribriform carc i n o m ais characterized by proliferation of onetype of neoplastic cell only, and onetype of mucosubstance. In addition,e s t rogen and pro g e s t e rone re c e p t o r sa re abundant in cribriform carc i n o m a sand absent from virtually all cases ofACC {2381}.
Immunoprofile and ultrastructureThe two main cell types are diff e rent atboth ultrastructural and immunohisto-chemical levels.U l t r a s t r u c t u r a l l y, the basaloid cells havemyoepithelial features particularly whenlocated at the interstitial surface thatlines the pseudoglandular spaces{3244}. They show thin cytoplasmic fila-ments with points of focal condensation{3094}. These cells have been shown tobe positive for actomyosin {105} andsimilar to myoepithelial cells are posi-
Fig. 1.56 Adenoid cystic carcinoma. The typicalfenestrated nests composed of two cell types (dom-inant basaloid and few eosinophilic) are shown.
Fig. 1.57 Adenoid cystic carcioma. In this case,there is a predominant tubular architecture.
44 Tumours of the breast
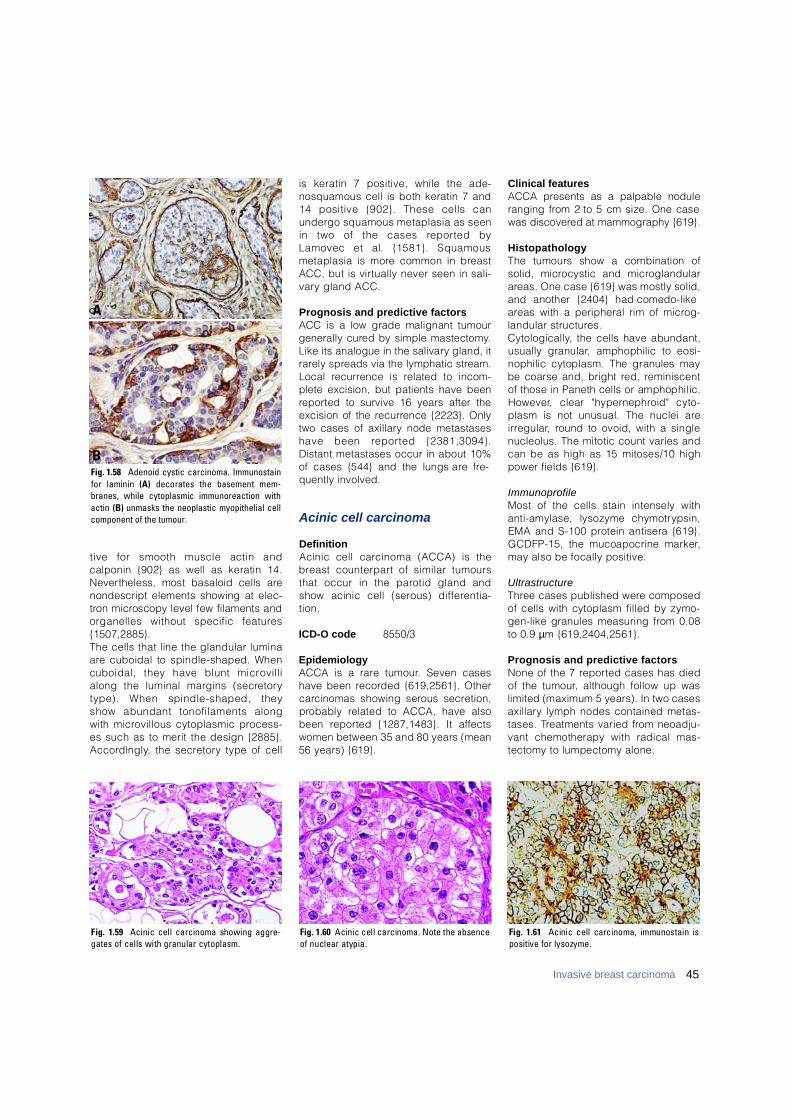
tive for smooth muscle actin andcalponin {902} as well as keratin 14.N e v e rtheless, most basaloid cells arenondescript elements showing at elec-t ron microscopy level few filaments andorganelles without specific feature s{1507,2885}. The cells that line the glandular luminaa re cuboidal to spindle-shaped. Whencuboidal, they have blunt micro v i l l ialong the luminal margins (secre t o rytype). When spindle-shaped, theyshow abundant tonofilaments alongwith microvillous cytoplasmic pro c e s s-es such as to merit the design {2885}.A c c o rd i n g l y, the secre t o ry type of cell
is keratin 7 positive, while the ade-nosquamous cell is both keratin 7 and14 positive {902}. These cells canundergo squamous metaplasia as seenin two of the cases re p o rted byLamovec et al. {1581}. Squamousmetaplasia is more common in bre a s tACC, but is virtually never seen in sali-v a ry gland ACC.
Prognosis and predictive factorsACC is a low grade malignant tumourgenerally cured by simple mastectomy.Like its analogue in the salivary gland, itr a rely spreads via the lymphatic stre a m .Local re c u r rence is related to incom-plete excision, but patients have beenre p o rted to survive 16 years after theexcision of the re c u r rence {2223}. Onlytwo cases of axillary node metastaseshave been re p o rted {2381,3094}.Distant metastases occur in about 10%of cases {544} and the lungs are fre-quently involved.
Acinic cell carcinoma
DefinitionAcinic cell carcinoma (ACCA) is theb reast counterpart of similar tumoursthat occur in the parotid gland andshow acinic cell (serous) diff e re n t i a-t i o n .
ICD-O code 8550/3
EpidemiologyACCA is a rare tumour. Seven caseshave been re c o rded {619,2561}. Otherc a rcinomas showing serous secre t i o n ,p robably related to ACCA, have alsobeen re p o rted {1287,1483}. It aff e c t swomen between 35 and 80 years (mean56 years) {619}.
Clinical featuresACCA presents as a palpable noduleranging from 2 to 5 cm size. One casewas discovered at mammography {619}.
H i s t o p a t h o l o g yThe tumours show a combination ofsolid, microcystic and micro g l a n d u l a ra reas. One case {619} was mostly solid,and another {2404} had comedo-likea reas with a peripheral rim of micro g-landular structure s .C y t o l o g i c a l l y, the cells have abundant,usually granular, amphophilic to eosi-nophilic cytoplasm. The granules maybe coarse and, bright red, re m i n i s c e n tof those in Paneth cells or amphophilic.H o w e v e r, clear "hypern e p h roid" cyto-plasm is not unusual. The nuclei arei r re g u l a r, round to ovoid, with a singlenucleolus. The mitotic count varies andcan be as high as 15 mitoses/10 highpower fields {619}.
I m m u n o p r o f i l eMost of the cells stain intensely withanti-amylase, lysozyme chymotry p s i n ,EMA and S-100 protein antisera {619}.GCDFP-15, the mucoapocrine marker,may also be focally positive.
U l t r a s t r u c t u r eT h ree cases published were composedof cells with cytoplasm filled by zymo-gen-like granules measuring from 0.08to 0.9 µm {619,2404,2561}.
Prognosis and predictive factorsNone of the 7 re p o rted cases has diedof the tumour, although follow up waslimited (maximum 5 years). In two casesa x i l l a ry lymph nodes contained metas-tases. Treatments varied from neoadju-vant chemotherapy with radical mas-tectomy to lumpectomy alone.
Fig. 1.58 Adenoid cystic carcinoma. Immunostainfor laminin ( A ) decorates the basement mem-branes, while cytoplasmic immunoreaction withactin (B) unmasks the neoplastic myopithelial cellcomponent of the tumour.
A
B
Fig. 1.59 Acinic cell carcinoma showing aggre-gates of cells with granular cytoplasm.
Fig. 1.60 Acinic cell carcinoma. Note the absenceof nuclear atypia.
Fig. 1.61 Acinic cell carcinoma, immunostain ispositive for lysozyme.
45Invasive breast carcinoma
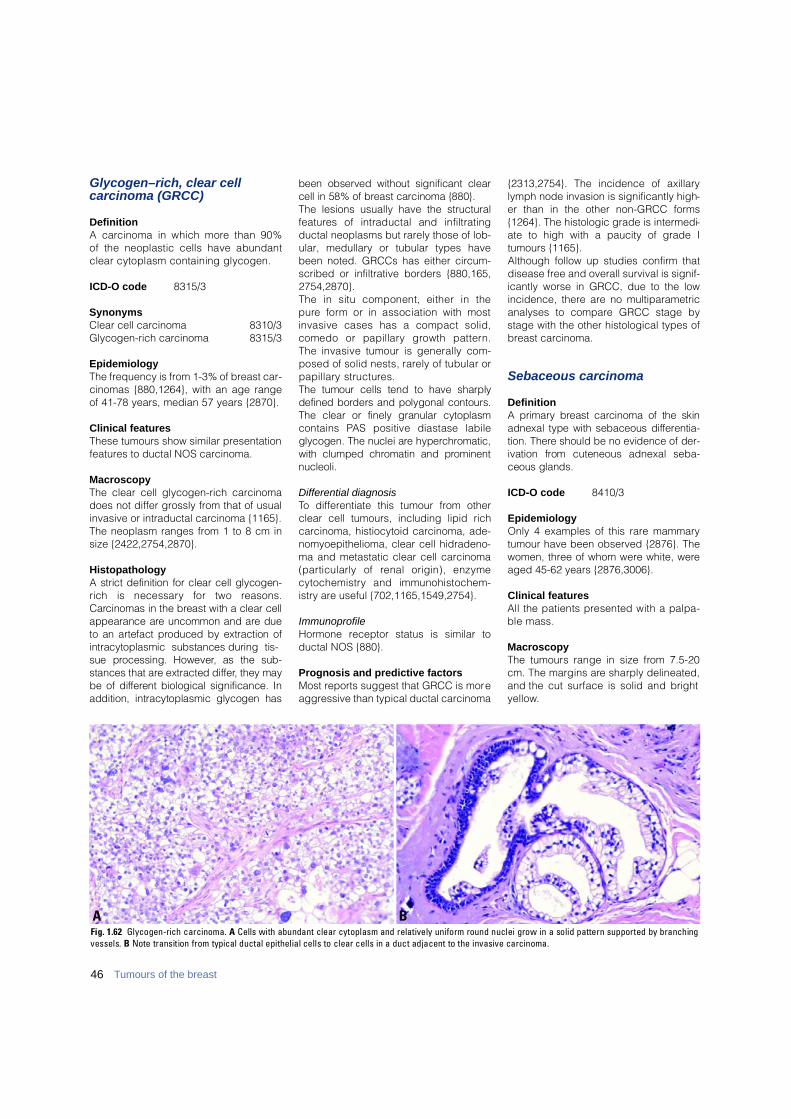
46 Tumours of the breast
Glycogen–rich, clear cell carcinoma (GRCC)
DefinitionA carcinoma in which more than 90% of the neoplastic cells have abundantclear cytoplasm containing glycogen.
ICD-O code 8315/3
Synonyms Clear cell carcinoma 8310/3Glycogen-rich carcinoma 8315/3
EpidemiologyThe frequency is from 1-3% of breast car-cinomas {880,1264}, with an age rangeof 41-78 years, median 57 years {2870}.
Clinical featuresThese tumours show similar presentationfeatures to ductal NOS carcinoma.
Macroscopy The clear cell glycogen-rich carcinomadoes not differ grossly from that of usualinvasive or intraductal carcinoma {1165}.The neoplasm ranges from 1 to 8 cm insize {2422,2754,2870}.
HistopathologyA strict definition for clear cell glycogen-rich is necessary for two re a s o n s .C a rcinomas in the breast with a clear cellappearance are uncommon and are dueto an artefact produced by extraction ofintracytoplasmic substances during tis-sue processing. However, as the sub-stances that are extracted diff e r, they maybe of diff e rent biological significance. Inaddition, intracytoplasmic glycogen has
been observed without significant clearcell in 58% of breast carcinoma {880}.The lesions usually have the structuralf e a t u res of intraductal and infiltratingductal neoplasms but rarely those of lob-ular, medullary or tubular types havebeen noted. GRCCs has either circum-scribed or infiltrative borders {880,165,2754,2870}. The in situ component, either in thep u re form or in association with mostinvasive cases has a compact solid,comedo or papillary growth pattern .The invasive tumour is generally com-posed of solid nests, rarely of tubular orp a p i l l a ry structures. The tumour cells tend to have sharplydefined borders and polygonal contours.The clear or finely granular cytoplasmcontains PAS positive diastase labileglycogen. The nuclei are hyperc h ro m a t i c ,with clumped chromatin and pro m i n e n tn u c l e o l i .
Differential diagnosisTo differentiate this tumour from otherclear cell tumours, including lipid richcarcinoma, histiocytoid carcinoma, ade-nomyoepithelioma, clear cell hidradeno-ma and metastatic clear cell carcinoma( p a rticularly of renal origin), enzymec y t o c h e m i s t ry and immunohistochem-istry are useful {702,1165,1549,2754}.
ImmunoprofileHormone receptor status is similar toductal NOS {880}.
Prognosis and predictive factorsMost reports suggest that GRCC is moreaggressive than typical ductal carcinoma
{2313,2754}. The incidence of axillarylymph node invasion is significantly high-er than in the other non-GRCC forms{1264}. The histologic grade is intermedi-ate to high with a paucity of grade Itumours {1165}.Although follow up studies confirm thatdisease free and overall survival is signif-icantly worse in GRCC, due to the lowincidence, there are no multiparametricanalyses to compare GRCC stage bystage with the other histological types ofbreast carcinoma.
Sebaceous carcinoma
DefinitionA primary breast carcinoma of the skinadnexal type with sebaceous diff e re n t i a-tion. There should be no evidence of der-ivation from cuteneous adnexal seba-ceous glands.
ICD-O code 8410/3
EpidemiologyOnly 4 examples of this rare mammarytumour have been observed {2876}. Thewomen, three of whom were white, wereaged 45-62 years {2876,3006}.
Clinical featuresAll the patients presented with a palpa-ble mass.
MacroscopyThe tumours range in size from 7.5-20cm. The margins are sharply delineated,and the cut surface is solid and brighty e l l o w.
BAFig. 1.62 Glycogen-rich carcinoma. A Cells with abundant clear cytoplasm and relatively uniform round nuclei grow in a solid pattern supported by branchingvessels. B Note transition from typical ductal epithelial cells to clear cells in a duct adjacent to the invasive carcinoma.
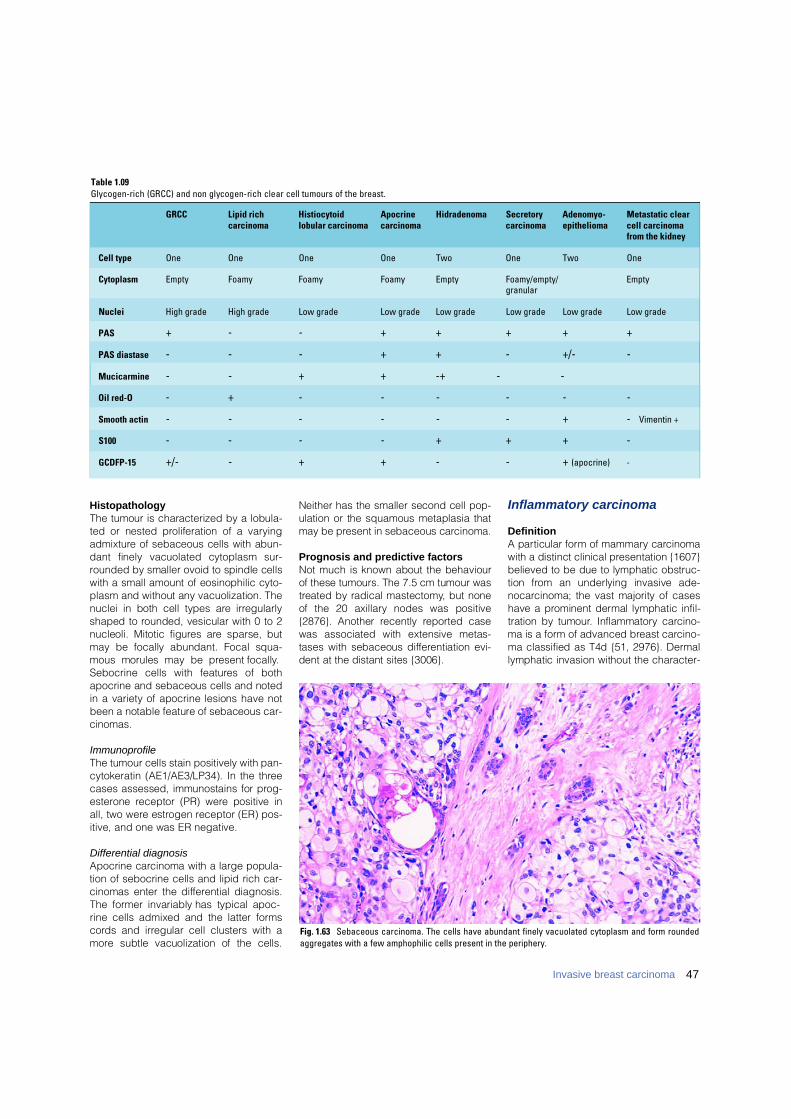
47Invasive breast carcinoma
H i s t o p a t h o l o g yThe tumour is characterized by a lobula-ted or nested proliferation of a vary i n ga d m i x t u re of sebaceous cells with abun-dant finely vacuolated cytoplasm sur-rounded by smaller ovoid to spindle cellswith a small amount of eosinophilic cyto-plasm and without any vacuolization. Thenuclei in both cell types are irre g u l a r l yshaped to rounded, vesicular with 0 to 2nucleoli. Mitotic figures are sparse, butmay be focally abundant. Focal squa-mous morules may be present focally.Sebocrine cells with features of bothapocrine and sebaceous cells and notedin a variety of apocrine lesions have notbeen a notable feature of sebaceous car-c i n o m a s .
I m m u n o p r o f i l eThe tumour cells stain positively with pan-cytokeratin (AE1/AE3/LP34). In the thre ecases assessed, immunostains for pro g-e s t e rone receptor (PR) were positive inall, two were estrogen receptor (ER) pos-itive, and one was ER negative.
Differential diagnosisApocrine carcinoma with a large popula-tion of sebocrine cells and lipid rich car-cinomas enter the diff e rential diagnosis.The former invariably has typical apoc-rine cells admixed and the latter form sc o rds and irregular cell clusters with am o re subtle vacuolization of the cells.
Neither has the smaller second cell pop-ulation or the squamous metaplasia thatmay be present in sebaceous carcinoma.
Prognosis and predictive factorsNot much is known about the behaviourof these tumours. The 7.5 cm tumour wast reated by radical mastectomy, but noneof the 20 axillary nodes was positive{2876}. Another recently re p o rted casewas associated with extensive metas-tases with sebaceous diff e rentiation evi-dent at the distant sites {3006}.
Inflammatory carcinoma
DefinitionA particular form of mammary carc i n o m awith a distinct clinical presentation {1607}believed to be due to lymphatic obstruc-tion from an underlying invasive ade-n o c a rcinoma; the vast majority of caseshave a prominent dermal lymphatic infil-tration by tumour. Inflammatory carc i n o-ma is a form of advanced breast carc i n o-ma classified as T4d {51, 2976}. Derm a llymphatic invasion without the character-
Fig. 1.63 Sebaceous carcinoma. The cells have abundant finely vacuolated cytoplasm and form roundedaggregates with a few amphophilic cells present in the periphery.
Table 1.09G l y c o g e n - r i c h (GRCC) and non glycogen-rich clear cell tumours of the breast.
GRCC Lipid rich Histiocytoid Apocrine Hidradenoma Secretory Adenomyo- Metastatic clearcarcinoma lobular carcinoma carcinoma carcinoma epithelioma cell carcinoma
from the kidney
Cell type One One One One Two One Two One
Cytoplasm Empty Foamy Foamy Foamy Empty Foamy/empty/ Emptygranular
Nuclei High grade High grade Low grade Low grade Low grade Low grade Low grade Low grade
PAS + - - + + + + +
PAS diastase - - - + + - +/- -
Mucicarmine - - + + - + - -
Oil red-O - + - - - - - -
Smooth actin - - - - - - + - Vimentin +
S100 - - - - + + + -
GCDFP-15 +/- - + + - - + (apocrine) -

48 Tumours of the breast
istic clinical picture is insufficient to qual-ify as inflammatory carc i n o m a .
ICD-O code 8530/3
EpidemiologyThe age distribution is similar to ductalNOS carcinoma and breast carcinoma ingeneral {1095,2384}. There is no re c o g-nized specific association with youngerage and pregnancy but the phenomenonof peritumoural lymphatic vascular inva-sion is found more frequently in youngerwomen {1095,2795}. The re p o rted fre-quency of an inflammatory presentation ofp r i m a ry breast carcinoma varies between1 and 10%, being influenced by the diag-nostic criteria (clinical or pathological)and the nature of the re p o rting centre(local population clinical centre versust e rt i a ry referral centre) {769,1641,2517}.
Clinical featuresThe clinical findings include diffuse ery-thema, oedema, peau d’orange, tender-ness, induration, warmth, enlargementand in some cases a palpable ill definedmass. The diagnosis is based on clinicalfeatures and should be confirmed bybiopsy. Dermal lymphatic tumour emboliare not always found in small diagnosticskin biopsy samples {724,2384}.
HistopathologyDespite the name, inflammatory carc i n o-ma is not associated with any significantd e g ree of inflammatory cell infiltration and
is not an inflammatory condition. Thecutaneous signs are produced as a con-sequence of lymphatic obstruction andconsequent oedema, which pro d u c esigns mimicking an inflammatory pro c e s s .I n f l a m m a t o ry signs can be the primaryclinical presenting abnormality (primaryi n f l a m m a t o ry carcinoma) or develop as aconsequence of tumour re c u r rence (sec-o n d a ry inflammatory carc i n o m a ) .Histologically the underlying invasivecarcinoma is not regarded as havingspecific histological features, the majori-ty of tumours have ductal NOS and are ofgrade 3 morphology {1708,1851}. Thesetumours often have an associated lym-phoid infiltrate usually of mature lympho-cytes and plasma cells, a low frequencyof estrogen receptor positivity {445,1490}and ERBB2 overexpression {1074}. Theskin often shows co-existing feature sassociated with lymphatic obstructionincluding separation of collagen fibreswith broadening of the reticular dermallayer due to oedema. Involved dermallymphatics may have an associated lymphoplasmacytic infiltrate {2427}.Secondary or recurrent inflammatory car-cinoma has been shown to be associat-ed more with ductal NOS and apocrinehistological types of breast carcinomaand is rare following presentation withother types, papillary, medullary andmucinous {2384}. The skin may alsoshow stromal metastatic deposits oftumour particularly in secondary orrecurrent inflammatory carcinoma.
Differential diagnosis There may be a discrepancy betweenclinical presentation with inflammatoryfeatures and presence of dermal lym-phatic emboli. Dermal vascular embolimay not be present in a biopsy takenfrom erythematous or oedematous area,or may be present in skin beyond theclinical skin changes. The skin biopsywill usually also show dermal lymphaticdilatation. The clinical features of inflam-matory carcinoma are generally regard-ed as specific but underlyng true inflam-matory conditions should be excluded ifhistological confirmation is not achieved.
Prognosis and predictive factorsPrior to the introduction of systemic therapy the prognosis of inflammatorycarcinoma even when treated by mas-tectomy, was very poor with 5 year sur-vival under 5% {1052,2384}. Use of sys-temic chemotherapy has produced animprovement in survival figures reportedas 25 to 50% at 5 years {406,828,1805,1907,2154}. In cases treated with neoad-juvant chemotherapy or radiotherapy,residual tumour, including intravascularemboli, are usually present in the mas-tectomy specimen even when a clinicalresponse has been observed {2427}.Mastectomy and radiotherapy are con-sidered beneficial for initial local controland palliation of symptoms {406,582,2243}. There are no consistent findingswith respect to influence of additionalclinical features such as presence of a clinical mass or findings in skin biopsyon survival. However, response to che-motherapy and radiotherapy, and patho-logical response have been shown to beassociated with improved disease freesurvival {473,828,841,1826}.
Bilateral breast carcinoma
DefinitionA synchronous breast cancer is onedetected within two months of the initialprimary tumour.A p p roximately 5-10% of women tre a t e dfor breast cancer will have either syn-c h ronous bilateral cancers or will deve-lop a subsequent contralateral bre a s tcancer (CBC) {448,872,1219,1491,2383}. The prevalence of synchro n o u sbilateral breast cancer is appro x i m a t e l y1% of all breast cancers {448,648,872,1491,1936}. An increase in the detection
Fig. 1.64 Sebaceous carcinoma. Cells with moderate amounts of eosinophilic or abundant microvacuolat-ed cytoplasm and variably compressed nuclei resembling lipoblasts are admixed.

49Invasive breast carcinoma
of synchronous cancers has been re-p o rted following the introduction of bi-lateral mammography for the investiga-tion of symptomatic breast disease and for population based breast scre e n i n g{751,872,1491,1492}.It is well recognized that a previous his-tory of breast cancer increases the risk ofsubsequent breast cancer in the con-tralateral breast. The re p o rted annualhazard rates of between 0.5-1% per year{448,872,1491,2383,2798} appear rela-tively constant up to 15 years {1491} giv-ing a cumulative incidence rate for sur-vivors of around 5% at 10 years and 10%at 15 years.Family history {253,448,1219} and earlyage of onset {35,1168,2798} have beenre p o rted to increase the risk of CBCdevelopment in some studies but othershave found no such associations witheither early age of onset {252,253,872} orfamily history {35,872}. One study hasre p o rted that family history, early age ofonset and lobular histology are independ-ent predictors of metachronous contralat-eral breast cancer development {1492}.These characteristics suggest a possiblegenetic predisposition. Women with astrong family history who develop breastcancer at an early age are at consider-able risk of contralateral breast canceras a first event of recurrence particularlyif the first primary is of lobular histologyor is of favourable prognostic type {1491,1492}.Patients with metachronous CBC areyounger at the age of onset of the origi-nal primary. Many, but not all, seriesreport that a higher percentage of thetumours are of lobular type {35,252,872,1219,1241,1492,2383}. This observationdoes not imply that tumours of lobulartype, in isolation from other risk factorssuch as young age and family history,should be considered to have a higherrisk of bilateral breast involvement{1491}. A greater frequency of multicen-tricity in one or both breast tumours hasalso been reported {355}. There does notappear to be any association with histo-logical grade, other tumour types or thestage of the disease {355,1491,1492}.
Prognosis and predictive featuresT h e o retically women with synchro n o u sCBC have a higher tumour burden thanwomen with unilateral disease whichmay jeopardize their survival pro s p e c t s{1035}. Indeed, synchronous CBC
appears to have a worse pro g n o s i sthan unilateral cohorts or women withm e t a c h ronous CBC {164,1092,1233}.Others have failed to demonstrate anysurvival diff e rence between women withunilateral and those with synchro n o u sCBC {911,1053,2555}.
Tumour spread and staging
Tumour spreadBreast cancer may spread via lymphaticand haematogenous routes and by directextension to adjacent structures. Spreadvia the lymphatic route is most frequentlyto the ipsilateral axillary lymph nodes,but spread to internal mammary nodesand to other regional nodal groups mayalso occur. Although breast cancer maymetastasize to any site, the most com-mon are bone, lung, and liver. Unusualsites of metastasis (e.g. peritoneal sur-faces, re t roperitoneum, gastro i n t e s t i n a ltract, and re p roductive organs) andunusual presentations of metastatic dis-ease are more often seen with invasivelobular carcinomas than with other histo-logical types {319,704,1142,1578}.Several models have been proposed toexplain the spread of breast cancer. TheHalsted model, assumes a spread fromthe breast to regional lymph nodes andfrom there to distant sites. This hypothe-sis provided the rationale for radical enbloc resection of the breast and regionallymph nodes. Others suggest a systemicdisease from inception, which impliesthat survival is unaffected by local treat-ment. However, clinical behaviour sug-gests that metastases occur as a func-tion of tumour growth and progression{1181}. This concept is supported by theresults of axillary sentinel lymph nodes,which show that metastatic axillary lymphnode involvement is a pro g re s s i v eprocess.
Tumour stagingBoth clinical and pathological staging isused in breast carcinoma. Clinical stag-ing is based on information gatheredprior to first definitive treatment, includ-ing data derived from physical examina-tion, imaging studies, biopsy, surgicalexploration, and other relevant findings.Pathological staging is based on dataused for clinical staging supplementedor modified by evidence obtained duringsurgery, particularly from the pathologi-
cal examination of the resected primarytumour, regional lymph nodes, and/ormore distant metastases, when relevant.The staging system currently in mostwidespread use is the TNM Classification{51,2976}. The most recent edition is pro-vided at the beginning of this chapter.The pathological tumour status ("pT") is ameasurement only of the invasive com-ponent. The extent of the associatedintraductal component should not betaken into consideration. In cases ofm i c roinvasive carcinoma (T1mic) inwhich multiple foci of microinvasion arepresent, multiplicity should be noted butthe size of only the largest focus is used,i.e. the size of the individual foci shouldnot be added together. The pathologicalnode status ("pN") is based on informa-tion derived from histological examina-tion of routine haematoxylin and eosin-stained sections. Cases with only isolat-ed tumour cells are classified as pNO(see relevant footnote in the TNM Tablewhich also indicates how to designatesentinel lymph node findings). A sub-classification of isolated tumour cells isprovided in TNM publications {51,1195,2976}.
Measurement of tumour sizeThe microscopic invasive tumour size (I)is used for TNM Classification (pT). Thedominant (largest) invasive tumour focusis measured, except in multifocaltumours where no such large singlefocus is apparent. In these cases thewhole tumour size (w) is used.
Somatic genetics of invasivebreast cancer
As in other organ sites, it has become evi-dent that breast cancers develop thro u g ha sequential accumulation of geneticalterations, including activation of onco-genes (e.g. by gene amplification), andinactivation of tumour suppressor genes,e.g. by gene mutations and deletions.
CytogeneticsAs yet no karyotypic hallmarks of breastcancer have been identified, such as the t(8;14) in chronic myelogenousleukaemia (CML), or the i(12p) in testicu-lar cancer. There is not even a cytoge-netic marker for any of the histologicalsubtypes of breast cancer. One reasonfor this is certainly the technical difficultyof obtaining sufficient numbers of good
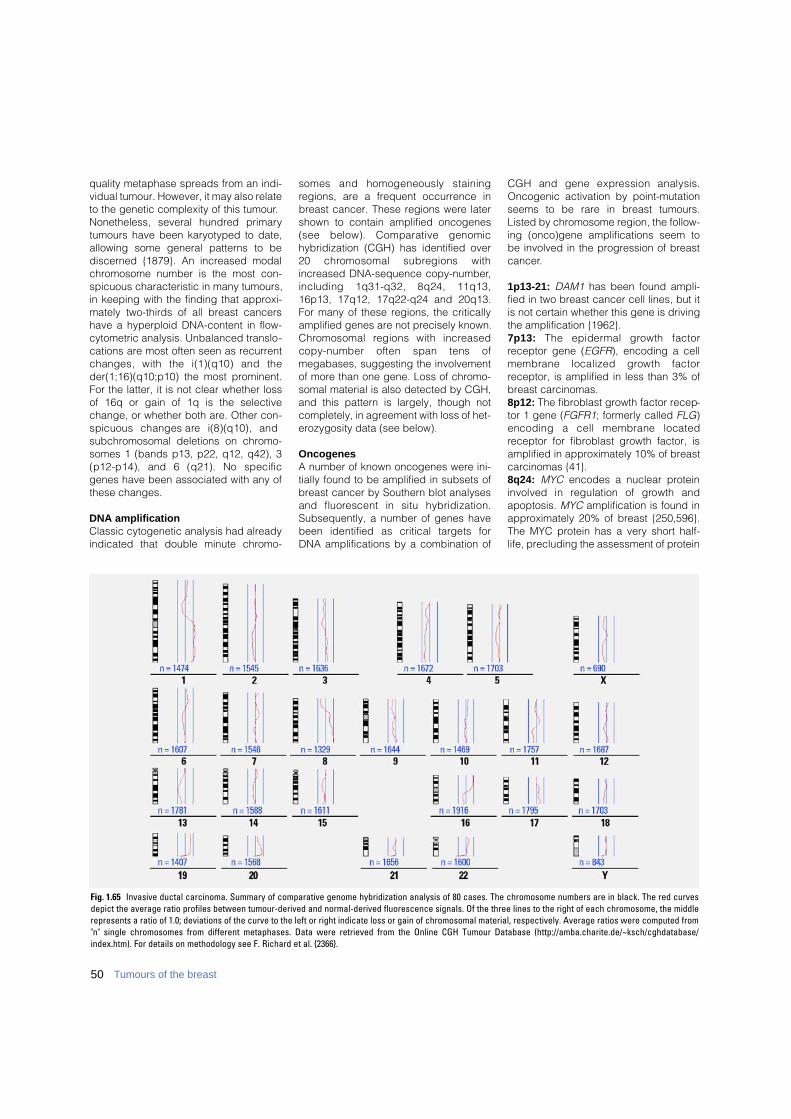
50 Tumours of the breast
quality metaphase spreads from an indi-vidual tumour. However, it may also relateto the genetic complexity of this tumour.Nonetheless, several hundred primarytumours have been karyotyped to date,allowing some general patterns to bediscerned {1879}. An increased modalchromosome number is the most con-spicuous characteristic in many tumours,in keeping with the finding that approxi-mately two-thirds of all breast cancershave a hyperploid DNA-content in flow-cytometric analysis. Unbalanced translo-cations are most often seen as recurrentchanges, with the i(1)(q10) and theder(1;16)(q10;p10) the most prominent.For the latter, it is not clear whether lossof 16q or gain of 1q is the selectivechange, or whether both are. Other con-spicuous changes are i(8)(q10), andsubchromosomal deletions on chromo-somes 1 (bands p13, p22, q12, q42), 3(p12-p14), and 6 (q21). No specificgenes have been associated with any ofthese changes.
DNA amplificationClassic cytogenetic analysis had alreadyindicated that double minute chromo-
somes and homogeneously stainingregions, are a frequent occurrence inbreast cancer. These regions were latershown to contain amplified oncogenes(see below). Comparative genomichybridization (CGH) has identified over20 chromosomal subregions withincreased DNA-sequence copy-number,including 1q31-q32, 8q24, 11q13,16p13, 17q12, 17q22-q24 and 20q13.For many of these regions, the criticallyamplified genes are not precisely known.C h romosomal regions with incre a s e dcopy-number often span tens ofmegabases, suggesting the involvementof more than one gene. Loss of chromo-somal material is also detected by CGH,and this pattern is largely, though notcompletely, in agreement with loss of het-erozygosity data (see below).
OncogenesA number of known oncogenes were ini-tially found to be amplified in subsets ofbreast cancer by Southern blot analysesand fluorescent in situ hybridization.Subsequently, a number of genes havebeen identified as critical targets for DNA amplifications by a combination of
CGH and gene expression analysis.Oncogenic activation by point-mutationseems to be rare in breast tumours.Listed by chromosome region, the follow-ing (onco)gene amplifications seem tobe involved in the progression of breastcancer.
1p13-21: DAM1 has been found ampli-fied in two breast cancer cell lines, but itis not certain whether this gene is drivingthe amplification {1962}.7 p 1 3 : The epidermal growth factorreceptor gene (EGFR), encoding a cellmembrane localized growth factorreceptor, is amplified in less than 3% ofbreast carcinomas.8p12: The fibroblast growth factor recep-tor 1 gene (FGFR1; formerly called FLG)encoding a cell membrane locatedreceptor for fibroblast growth factor, isamplified in approximately 10% of breastcarcinomas {41}.8q24: MYC encodes a nuclear proteininvolved in regulation of growth andapoptosis. MYC amplification is found inapproximately 20% of breast {250,596}.The MYC protein has a very short half-life, precluding the assessment of protein
Fig. 1.65 Invasive ductal carcinoma. Summary of comparative genome hybridization analysis of 80 cases. The chromosome numbers are in black. The red curvesdepict the average ratio profiles between tumour-derived and normal-derived fluorescence signals. Of the three lines to the right of each chromosome, the middlerepresents a ratio of 1.0; deviations of the curve to the left or right indicate loss or gain of chromosomal material, respectively. Average ratios were computed from"n" single chromosomes from different metaphases. Data were retrieved from the Online CGH Tumour Database (http://amba.charite.de/~ksch/cghdatabase/index.htm). For details on methodology see F. Richard et al. {2366}.

o v e re x p ression as a substitute for theanalysis of gene amplification. Ampli-fication of subregions of 8q can be complex. There appears to be at leastone additional oncogene mapping toc h romosome 8q12-22, which has notbeen identified yet.1 0 q 2 6 : The fibroblast growth factorreceptor 2 (FGFR2; formerly: BEK) geneencodes a cell membrane locatedreceptor for fibroblast growth factor. Thisgene is amplified in approximately 12%of breast carcinomas {41}.11q13: Amplification of the cyclin D1gene (CCND1), encoding a nuclear pro-tein involved in cell cycle regulation, hasbeen found in 15-20% of breast tumours,in association with estrogen re c e p t o rpositivity. Cyclin D1 can also bind to theestrogen receptor, resulting in ligand-independent activation of the receptor{3273}. Immunohistochemically, cyclinD1 appears to be overexpressed in 80%of invasive lobular carcinomas, but is notalways accompanied by CCND1 geneamplification {2133}. 1 7 q 1 2 : The human epidermal gro w t hfactor receptor-2 (ERBB2) proto-onco-gene (also known as HER2, and equiva-lent to the rodent neu gene) encodes a185-kD transmembrane glycopro t e i nwith intrinsic tyrosine kinase activity. Aligand for ERBB2 has not been identifiedbut it is hypothesized that ERBB2 ampli-fies the signal provided by other recep-tors of this family by heterodimerizingwith them. Ligand-dependent activationof ERBB1, ERBB3, and ERBB4 by EGF orh e regulin results in hetero d i m e r i z a t i o nand, thereby, ERBB2 activation. ERBB2amplification results in overexpression of
ERBB2 protein, but not all tumours withoverexpression have amplified 17q12.Overexpression is found in approximate-ly 20-30% of human breast carcinomas{2962}. In breast cancers with normalE R B B 2 copy number, expression ofERBB2 may be variable but is very rarelyas high as that in tumours with ERBB2amplification (usually 10-fold to 100-foldhigher and equivalent to millions ofmonomers). Numerous studies haveinvestigated the relationship betweenE R B B 2 status and clinicopathologicalcharacteristics in breast cancer {2962}. 1 7 q 2 2 - q 2 4 : At least three genes(R P S 6 K B 1, PAT 1, and T B X 2) have beenfound to be co-amplified and overe x-p ressed in ~10% of breast cancers {181}.F u rther analysis identified R P S 6 K B 1,M U L, A P P B P 2, T R A P 2 4 0 and oneunknown gene to be consistently overe x-p ressed in two commonly amplified sub-regions {1896}. The ribosomal protein S6kinase (RPS6KB1) is a serine-thre o n i n ekinase whose activation is thought to re g-ulate a wide array of cellular pro c e s s e sinvolved in the mitogenic re s p o n s eincluding protein synthesis, translation ofspecific mRNA species, and cell cyclep ro g ression from G1 to S phase. 20q13: It is presently unknown whetherthe CSE1L/CAS gene, the NCOA3 geneor any other gene in this region serves asthe target for the amplification, which isfound in approximately 15% of breastcarcinomas. Three independent regionsof amplification have been identified and their co-amplification is common.Cellular apoptosis susceptibility (CAS)encodes a protein, which may have afunction in the control of apoptosis and
cell proliferation {346}. N C O A 3 g e n eencodes a co-activator of the estrogenreceptor {109}, and its amplification hasbeen found to be associated with estro-gen receptor positivity. High resolutionmapping of the amplified domains hassuggested that a putative oncogene,ZNF217, and CYP24 (encoding vitamin D24 hydroxylase), whose overexpressionis likely to lead to abrogation of growthcontrol mediated by vitamin D, may betargets for the amplification {60}.The S T K 1 5 gene (also known as BTA Kand Aurora-A) is amplified in appro-ximately 12% of primary breast tumours,as well as in breast, ovarian, colon,p rostate, neuroblastoma, and cervicalcancer cell lines {3259}. S T K 1 5encodes a centrosome-associated s e r i n e - t h reonine kinase, and may alsobe overe x p ressed in tumours withoutamplification of 20q13 {1885}. Centro-somes appear to maintain genomic sta-bility through the establishment of bipo-lar spindles during cell division, en-suring equal segregation of re p l i c a t e dc h romosomes to daughter cells.D e regulated duplication and distributionof centrosomes are implicated in chro-mosome segregation abnorm a l i t i e s ,leading to aneuploidy seen in manycancer cell types. Elevated S T K 1 5e x p ression induces centrosome amplifi-cation and overrides the checkpointmechanism that monitors mitotic spindlea s s e m b l y, leading to chro m o s o m a linstability {83,1885,3259}.
Loss of heterozygosity (LOH)Loss of heterozygosity (LOH) has beenfound to affect all chromosome arms
Fig. 1.66 Poorly differentiated DCIS. A Immunohistochemical staining and bright field in situ hybridization (BRISH) of cyclin D1 in the same case of DCIS. Strongstaining of poorly differentiated DCIS. B Immunohistochemical staining and BRISH of cyclin D1 in the same case of DCIS. BRISH with a chromosome 11-specific(peri)centromeric probe. C BRISH with the cyclin D1 specific cosmid. Immunohistochemical staining and BRISH of cyclin D1 in the same case of DCIS. BRISH withthe cyclin D1 specific cosmid. Reprinted with permission from C.B. Vos et al. {3035}.
CBA
51Invasive breast carcinoma
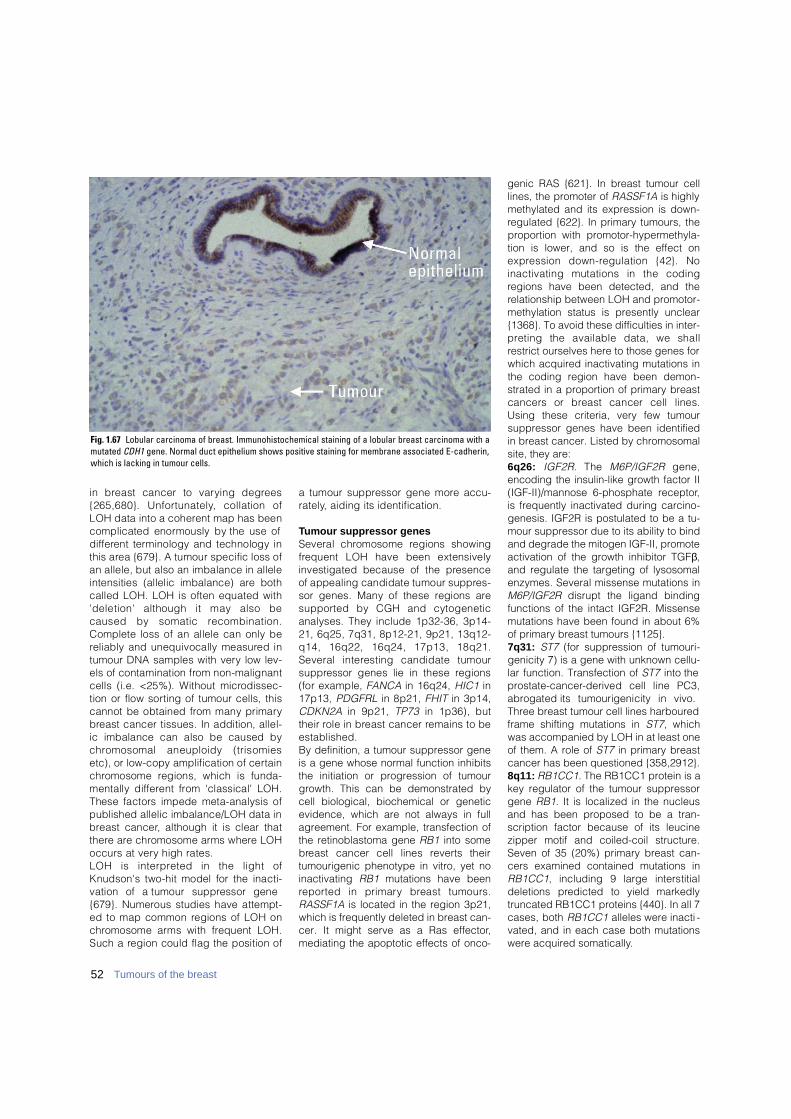
52 Tumours of the breast
in breast cancer to varying degre e s{265,680}. Unfort u n a t e l y, collation ofLOH data into a coherent map has beencomplicated enormously by the use ofd i ff e rent terminology and technology inthis area {679}. A tumour specific loss ofan allele, but also an imbalance in alleleintensities (allelic imbalance) are bothcalled LOH. LOH is often equated with'deletion' although it may also becaused by somatic re c o m b i n a t i o n .Complete loss of an allele can only bereliably and unequivocally measured intumour DNA samples with very low lev-els of contamination from non-malignantcells (i.e. <25%). Without micro d i s s e c-tion or flow sorting of tumour cells, thiscannot be obtained from many primaryb reast cancer tissues. In addition, allel-ic imbalance can also be caused byc h romosomal aneuploidy (trisomiesetc), or low-copy amplification of cert a i nc h romosome regions, which is funda-mentally diff e rent from 'classical' LOH.These factors impede meta-analysis ofpublished allelic imbalance/LOH data inb reast cancer, although it is clear thatt h e re are chromosome arms where LOHoccurs at very high rates. LOH is interpreted in the light ofKnudson's two-hit model for the inacti-vation of a tumour suppressor gene{679}. Numerous studies have attempt-ed to map common regions of LOH onc h romosome arms with frequent LOH.Such a region could flag the position of
a tumour suppressor gene more accu-r a t e l y, aiding its identification.
Tumour suppressor genesSeveral chromosome regions showingf requent LOH have been extensivelyinvestigated because of the pre s e n c eof appealing candidate tumour suppre s-sor genes. Many of these regions ares u p p o rted by CGH and cytogeneticanalyses. They include 1p32-36, 3p14-21, 6q25, 7q31, 8p12-21, 9p21, 13q12-q14, 16q22, 16q24, 17p13, 18q21.Several interesting candidate tumours u p p ressor genes lie in these re g i o n s(for example, FA N C A in 16q24, H I C 1 i n17p13, P D G F R L in 8p21, F H I T in 3p14,C D K N 2 A in 9p21, T P 7 3 in 1p36), buttheir role in breast cancer remains to bee s t a b l i s h e d .By definition, a tumour suppressor geneis a gene whose normal function inhibitsthe initiation or progression of tumourgrowth. This can be demonstrated bycell biological, biochemical or geneticevidence, which are not always in fullagreement. For example, transfection ofthe retinoblastoma gene RB1 into someb reast cancer cell lines re v e rts theirtumourigenic phenotype in vitro, yet noinactivating RB1 mutations have beenre p o rted in primary breast tumours.RASSF1A is located in the region 3p21,which is frequently deleted in breast can-cer. It might serve as a Ras effector,mediating the apoptotic effects of onco-
genic RAS {621}. In breast tumour celllines, the promoter of RASSF1A is highlymethylated and its expression is down-regulated {622}. In primary tumours, theproportion with promotor-hypermethyla-tion is lower, and so is the effect one x p ression down-regulation {42}. Noinactivating mutations in the codingregions have been detected, and therelationship between LOH and promotor-methylation status is presently unclear{1368}. To avoid these difficulties in inter-p reting the available data, we shallrestrict ourselves here to those genes forwhich acquired inactivating mutations inthe coding region have been demon-strated in a proportion of primary breastcancers or breast cancer cell lines.Using these criteria, very few tumoursuppressor genes have been identifiedin breast cancer. Listed by chromosomalsite, they are:6 q 2 6 : I G F 2 R. The M 6 P / I G F 2 R g e n e ,encoding the insulin-like growth factor II(IGF-II)/mannose 6-phosphate receptor,is frequently inactivated during carcino-genesis. IGF2R is postulated to be a tu-mour suppressor due to its ability to bindand degrade the mitogen IGF-II, promoteactivation of the growth inhibitor TGFβ,and regulate the targeting of lysosomalenzymes. Several missense mutations inM6P/IGF2R disrupt the ligand bindingfunctions of the intact IGF2R. Missensemutations have been found in about 6%of primary breast tumours {1125}.7q31: ST7 (for suppression of tumouri-genicity 7) is a gene with unknown cellu-lar function. Transfection of ST7 into thep ro s t a t e - c a n c e r-derived cell line PC3,a b rogated its tumourigenicity in vivo.Three breast tumour cell lines harbouredframe shifting mutations in ST7, whichwas accompanied by LOH in at least oneof them. A role of ST7 in primary breastcancer has been questioned {358,2912}.8q11: RB1CC1. The RB1CC1 protein is akey regulator of the tumour suppressorgene RB1. It is localized in the nucleusand has been proposed to be a tran-scription factor because of its leucinezipper motif and coiled-coil structure.Seven of 35 (20%) primary breast can-cers examined contained mutations inR B 1 C C 1, including 9 large interstitialdeletions predicted to yield markedlytruncated RB1CC1 proteins {440}. In all 7cases, both RB1CC1 alleles were inacti -vated, and in each case both mutationswere acquired somatically.
Fig. 1.67 Lobular carcinoma of breast. Immunohistochemical staining of a lobular breast carcinoma with amutated CDH1 gene. Normal duct epithelium shows positive staining for membrane associated E-cadherin,which is lacking in tumour cells.
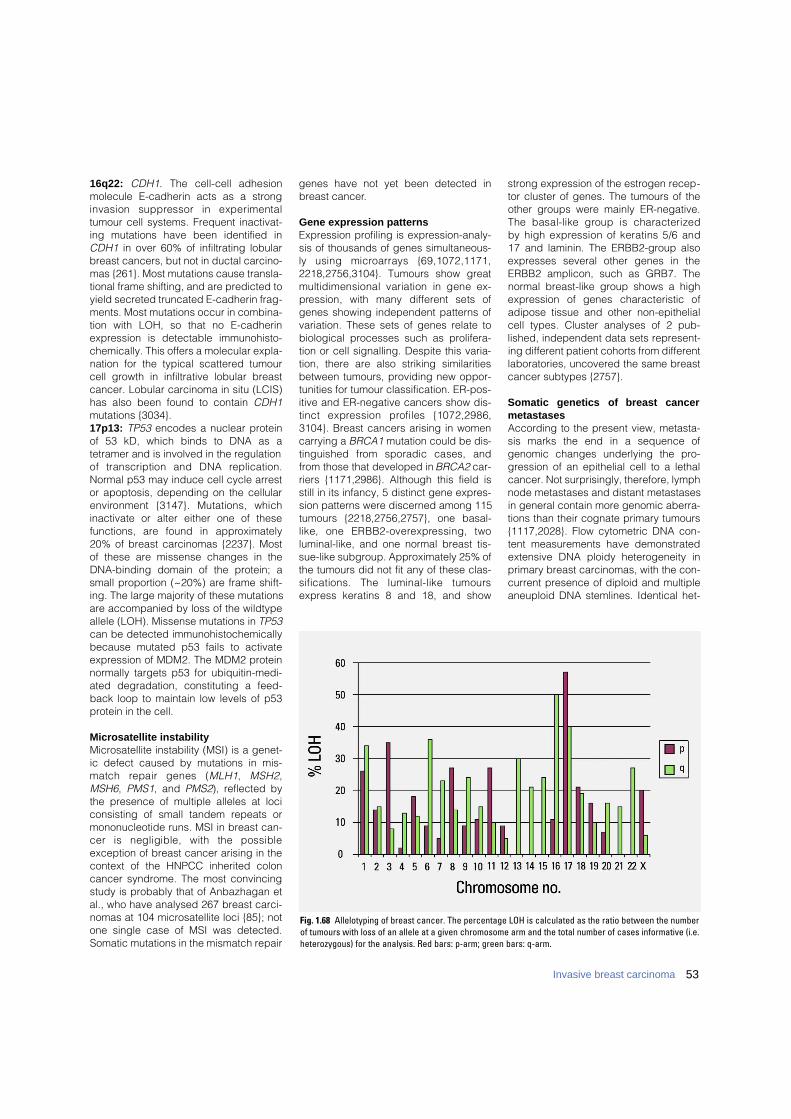
1 6 q 2 2 : C D H 1. The cell-cell adhesionmolecule E-cadherin acts as a stronginvasion suppressor in experimentaltumour cell systems. Frequent inactivat-ing mutations have been identified inCDH1 in over 60% of infiltrating lobularbreast cancers, but not in ductal carcino-mas {261}. Most mutations cause transla-tional frame shifting, and are predicted toyield secreted truncated E-cadherin frag-ments. Most mutations occur in combina-tion with LOH, so that no E-cadherinexpression is detectable immunohisto-chemically. This offers a molecular expla-nation for the typical scattered tumourcell growth in infiltrative lobular breastcancer. Lobular carcinoma in situ (LCIS)has also been found to contain CDH1mutations {3034}.17p13: TP53 encodes a nuclear proteinof 53 kD, which binds to DNA as atetramer and is involved in the regulationof transcription and DNA re p l i c a t i o n .Normal p53 may induce cell cycle arrestor apoptosis, depending on the cellulare n v i ronment {3147}. Mutations, whichinactivate or alter either one of thesefunctions, are found in appro x i m a t e l y20% of breast carcinomas {2237}. Mostof these are missense changes in theDNA-binding domain of the protein; asmall proportion (~20%) are frame shift-ing. The large majority of these mutationsare accompanied by loss of the wildtypeallele (LOH). Missense mutations in TP53can be detected immunohistochemicallybecause mutated p53 fails to activateexpression of MDM2. The MDM2 proteinnormally targets p53 for ubiquitin-medi-ated degradation, constituting a feed-back loop to maintain low levels of p53protein in the cell.
Microsatellite instabilityMicrosatellite instability (MSI) is a genet-ic defect caused by mutations in mis-match repair genes (M L H 1, M S H 2,MSH6, PMS1, and PMS2), reflected bythe presence of multiple alleles at lociconsisting of small tandem repeats ormononucleotide runs. MSI in breast can-cer is negligible, with the possibleexception of breast cancer arising in thecontext of the HNPCC inherited coloncancer syndrome. The most convincingstudy is probably that of Anbazhagan etal., who have analysed 267 breast carci-nomas at 104 microsatellite loci {85}; notone single case of MSI was detected.Somatic mutations in the mismatch repair
genes have not yet been detected inbreast cancer.
Gene expression patternsExpression profiling is expression-analy-sis of thousands of genes simultaneous-ly using microarrays {69,1072,1171,2218,2756,3104}. Tumours show greatmultidimensional variation in gene ex-p ression, with many diff e rent sets ofgenes showing independent patterns ofvariation. These sets of genes relate tobiological processes such as prolifera-tion or cell signalling. Despite this varia-tion, there are also striking similaritiesbetween tumours, providing new oppor-tunities for tumour classification. ER-pos-itive and ER-negative cancers show dis-tinct expression profiles {1072,2986,3104}. Breast cancers arising in womencarrying a BRCA1 mutation could be dis-tinguished from sporadic cases, andfrom those that developed in BRCA2 car-riers {1171,2986}. Although this field isstill in its infancy, 5 distinct gene expres-sion patterns were discerned among 115tumours {2218,2756,2757}, one basal-like, one ERBB2-overe x p ressing, twoluminal-like, and one normal breast tis-sue-like subgroup. Approximately 25% ofthe tumours did not fit any of these clas-sifications. The luminal-like tumoursexpress keratins 8 and 18, and show
strong expression of the estrogen recep-tor cluster of genes. The tumours of theother groups were mainly ER-negative.The basal-like group is characterizedby high expression of keratins 5/6 and17 and laminin. The ERBB2-group alsoexpresses several other genes in theERBB2 amplicon, such as GRB7. Thenormal breast-like group shows a highe x p ression of genes characteristic ofadipose tissue and other non-epithelialcell types. Cluster analyses of 2 pub-lished, independent data sets represent-ing different patient cohorts from differentlaboratories, uncovered the same breastcancer subtypes {2757}.
Somatic genetics of breast cancermetastasesAccording to the present view, metasta-sis marks the end in a sequence ofgenomic changes underlying the pro-gression of an epithelial cell to a lethalcancer. Not surprisingly, therefore, lymphnode metastases and distant metastasesin general contain more genomic aberra-tions than their cognate primary tumours{1117,2028}. Flow cytometric DNA con-tent measurements have demonstratedextensive DNA ploidy heterogeneity inprimary breast carcinomas, with the con-current presence of diploid and multipleaneuploid DNA stemlines. Identical het-
Fig. 1.68 Allelotyping of breast cancer. The percentage LOH is calculated as the ratio between the numberof tumours with loss of an allele at a given chromosome arm and the total number of cases informative (i.e.heterozygous) for the analysis. Red bars: p-arm; green bars: q-arm.
53Invasive breast carcinoma
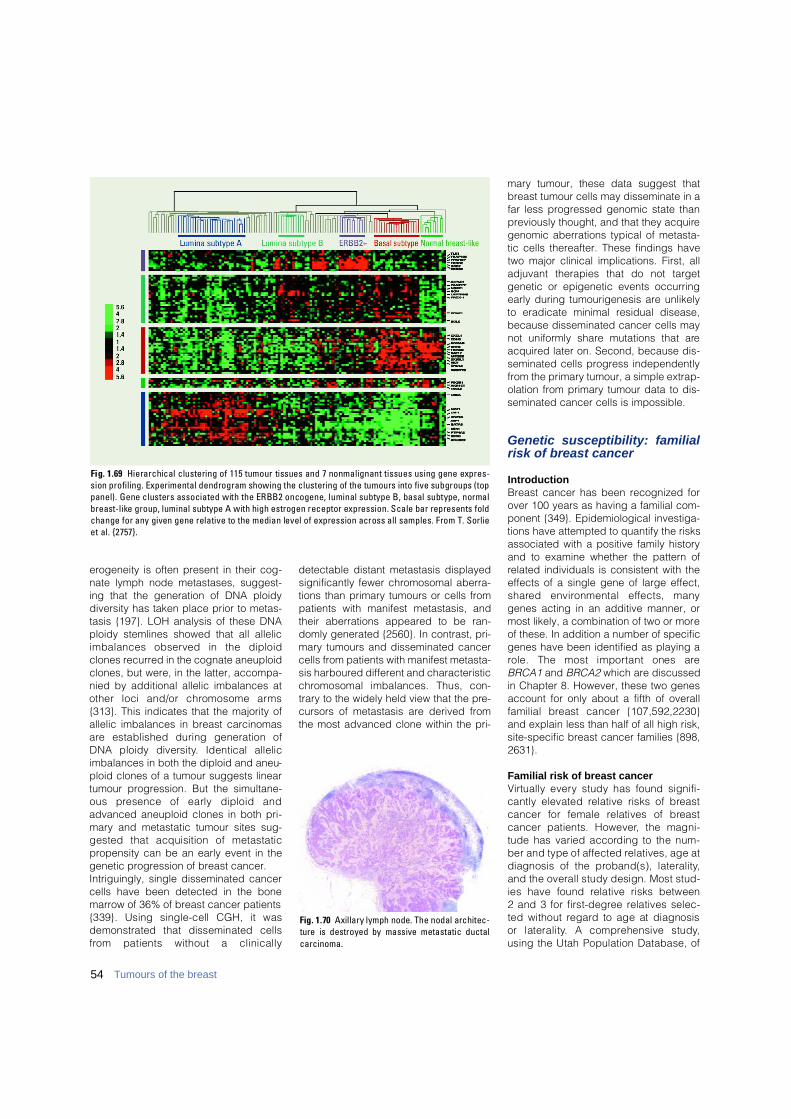
erogeneity is often present in their cog-nate lymph node metastases, suggest-ing that the generation of DNA ploidydiversity has taken place prior to metas-tasis {197}. LOH analysis of these DNAploidy stemlines showed that all allelicimbalances observed in the diploidclones recurred in the cognate aneuploidclones, but were, in the latter, accompa-nied by additional allelic imbalances atother loci and/or chromosome arm s{313}. This indicates that the majority ofallelic imbalances in breast carcinomasa re established during generation ofDNA ploidy diversity. Identical allelicimbalances in both the diploid and aneu-ploid clones of a tumour suggests lineartumour progression. But the simultane-ous presence of early diploid andadvanced aneuploid clones in both pri-mary and metastatic tumour sites sug-gested that acquisition of metastaticpropensity can be an early event in thegenetic progression of breast cancer.Intriguingly, single disseminated cancercells have been detected in the bonemarrow of 36% of breast cancer patients{339}. Using single-cell CGH, it wasdemonstrated that disseminated cellsf rom patients without a clinically
detectable distant metastasis displayedsignificantly fewer chromosomal aberra-tions than primary tumours or cells frompatients with manifest metastasis, andtheir aberrations appeared to be ran-domly generated {2560}. In contrast, pri-mary tumours and disseminated cancercells from patients with manifest metasta-sis harboured different and characteristicc h romosomal imbalances. Thus, con-trary to the widely held view that the pre-cursors of metastasis are derived fromthe most advanced clone within the pri-
mary tumour, these data suggest thatbreast tumour cells may disseminate in afar less progressed genomic state thanpreviously thought, and that they acquiregenomic aberrations typical of metasta-tic cells thereafter. These findings havetwo major clinical implications. First, alladjuvant therapies that do not targetgenetic or epigenetic events occurringearly during tumourigenesis are unlikelyto eradicate minimal residual disease,because disseminated cancer cells maynot uniformly share mutations that areacquired later on. Second, because dis-seminated cells progress independentlyfrom the primary tumour, a simple extrap-olation from primary tumour data to dis-seminated cancer cells is impossible.
Genetic susceptibility: familialrisk of breast cancer
IntroductionBreast cancer has been recognized forover 100 years as having a familial com-ponent {349}. Epidemiological investiga-tions have attempted to quantify the risksassociated with a positive family historyand to examine whether the pattern ofrelated individuals is consistent with theeffects of a single gene of large effect,s h a red environmental effects, manygenes acting in an additive manner, ormost likely, a combination of two or moreof these. In addition a number of specificgenes have been identified as playing arole. The most important ones areBRCA1 and BRCA2 which are discussedin Chapter 8. However, these two genesaccount for only about a fifth of overallfamilial breast cancer {107,592,2230}and explain less than half of all high risk,site-specific breast cancer families {898,2631}.
Familial risk of breast cancerVi rtually every study has found signifi-cantly elevated relative risks of bre a s tcancer for female relatives of bre a s tcancer patients. However, the magni-tude has varied according to the num-ber and type of affected relatives, age atdiagnosis of the proband(s), laterality,and the overall study design. Most stud-ies have found relative risks between 2 and 3 for first-degree relatives selec-ted without re g a rd to age at diagnosis or laterality. A comprehensive study, using the Utah Population Database, of
Fig. 1.70 Axillary lymph node. The nodal architec-ture is destroyed by massive metastatic ductalc a r c i n o m a .
54 Tumours of the breast
Fig. 1.69 Hierarchical clustering of 115 tumour tissues and 7 nonmalignant tissues using gene expres-sion profiling. Experimental dendrogram showing the clustering of the tumours into five subgroups (toppanel). Gene clusters associated with the ERBB2 oncogene, luminal subtype B, basal subtype, normalbreast-like group, luminal subtype A with high estrogen receptor expression. Scale bar represents foldchange for any given gene relative to the median level of expression across all samples. From T. Sorlieet al. {2757}.

f i r s t - d e g ree re l atives of breast cancerprobands diagnosed before age 80 esti-mated a relative risk of 1.8 in the relatives{1029}. When the breast cancer was ofearly onset (diagnosed before age 50),the relative risk among first-degree rela-tives increased to 2.6 and the risk forearly-onset breast cancer among theserelatives was 3.7 (95% CI. 2.8—4.6). Therisk to subsequent relatives in familieswith two affected sisters was increasedto 2.7 with a particularly high risk of 4.9 of early onset breast cancer. A secondregistry-based study in Sweden foundessentially identical results to the Utahstudy {715}.Perhaps the largest population-basedstudy (the Cancer and Steroid Horm o n e(CASH) case-control study) of pro-bands with breast cancer diagnosedbetween the ages of 20 and 54 estima-ted the risk of breast cancer in first-d e g ree relatives compared with con-t rols was 2.1 {501}. A study of cancer at a number of sites in a large set of twins in Scandinavia{1658}, estimated the pro p o rtion of va-riance due to genetic (heritability),s h a red environment, and random (in-dividual-specific) environmental eff e c t sfor each cancer site. Based on thisdata, the authors calculated a co-twinrelative risk of 2.8 in DZ and 5.2 in MZtwins, and estimated that 27% of bre a s tcancer is due to inherited cause whileonly 6% could be attributed to share de n v i ronment. The role of other factors with respect tofamily history has been examined.Larger familial effects among relatives ofyoung bilateral probands compared withyoung probands with unilateral bre a s tcancer have been found {93,1246,2129}.The relationship of histology to familialb reast cancer is less clear {500,2989}. Another feature, which conveys stro n gfamilial risk of breast cancer, is theo c c u r rence of breast cancer in a male. Ithas been estimated that female re l a t i v e sof probands with male breast cancerhave a two-fold to three-fold incre a s e drisk of breast cancer {94,2449}.
Familial associations of breast and othercancersA number of studies have found in-creased risks for other cancers amongrelatives of breast cancer probands. Themost commonly reported are ovarian,uterine, prostate and colon cancers. In
the Utah Population Database, whenrisks to all other sites among suchp robands were examined statisticallysignificant familial associations werefound between breast cancer and can-cers of the prostate (relative risk = 1.2,P<0.0001), colon (1.35, P<0.0001), thy-roid (1.7, P<0.001) and non-Hodgkinlymphoma (1.4, P<0.001) {1029}. TheSwedish registry study also found a sig-nificant familial relationship betweenbreast and prostate cancer of similarmagnitude.Other studies have also shown relation-ships between breast cancer and ovari-an, colon and uterine cancers, althoughthe results have not been consistentacross studies {95,1992,2172,2918}.Undoubtedly, the majority of the associa-
tions detected in these population stud-ies is due to the BRCA1 gene, known tobe involved in a large pro p o rtion ofextended kindreds with clearly inheritedsusceptibility to breast and ovarian can-cer. It is likely that some of the discrep-ancies in results are linked to the fre-quency of BRCA1 deleterious alleles inthe respective datasets.
Possible models to explain the familialrisk of breast cancerBRCA1 and BRCA2 explain only a minor-ity (about 20%) of the overall familial riskof breast cancer although they may con-tribute much more substantially to thefour-fold increased risk at younger ages.Assuming an overall two-fold increasedrisk among first-degree female relatives
Table 1.10Estimates of relative risks for breast cancer.
Relative affected, status of proband Estimate of relative risk {Reference} (Study Type)
Mother 3.0 {1321a} (a)
Sister 3.0 {1321a} (a)
Mother 2.0 {2214} (a)
Sister 3.0 {2214} (a)
Sister, premenopausal proband 5.0 {92a} (b)
Sister, postmenopausal proband 2.0 {92a} (b)
First-degree relative (FDR) 2.0 {346a} (c)
Sister, bilateral proband 6.0 {2129} (c)
Sister 2.0 {412a} (d)
Mother 2.0 {412a} (d)
First-degree relative (FDR) 2.0 {2556a} (a)
FDR<45, proband<45 3.0 {2556a} (a)
FDR>45, proband>45 1.5 {2556a} (a)
First degree relative 2.1 {501} (c)
First degree relative, proband <55 2.3 {1246} (a)
First degree relative, proband >55 1.6 {1246} (a)
FDR, bilateral proband 6.4 {1246} (a)
First degree relative 2.3 {2720a} (c)
Second degree relative 1.8 {2720a} (c)
First degree relative 1.8 {896} (a)
FDR<50, proband<50 3.7 {896} (a)
FDR, 2 affected probands 2.7 {896} (a)
Mother 1.9 {715} (a)
Sister 2.0 {715} (a)
(a) Ratio of observed frequencies in cancer families to expected frequencies in the general population;(b) Ratio of observed rate of cancer in relatives of cases to observed rate of cancer in relatives of cases
to observed rate of cancer in relatives of selected controls;(c) Odds ratio from case-control study with non-cancer controls (d) Relative risk from prospective study.
55Invasive breast carcinoma
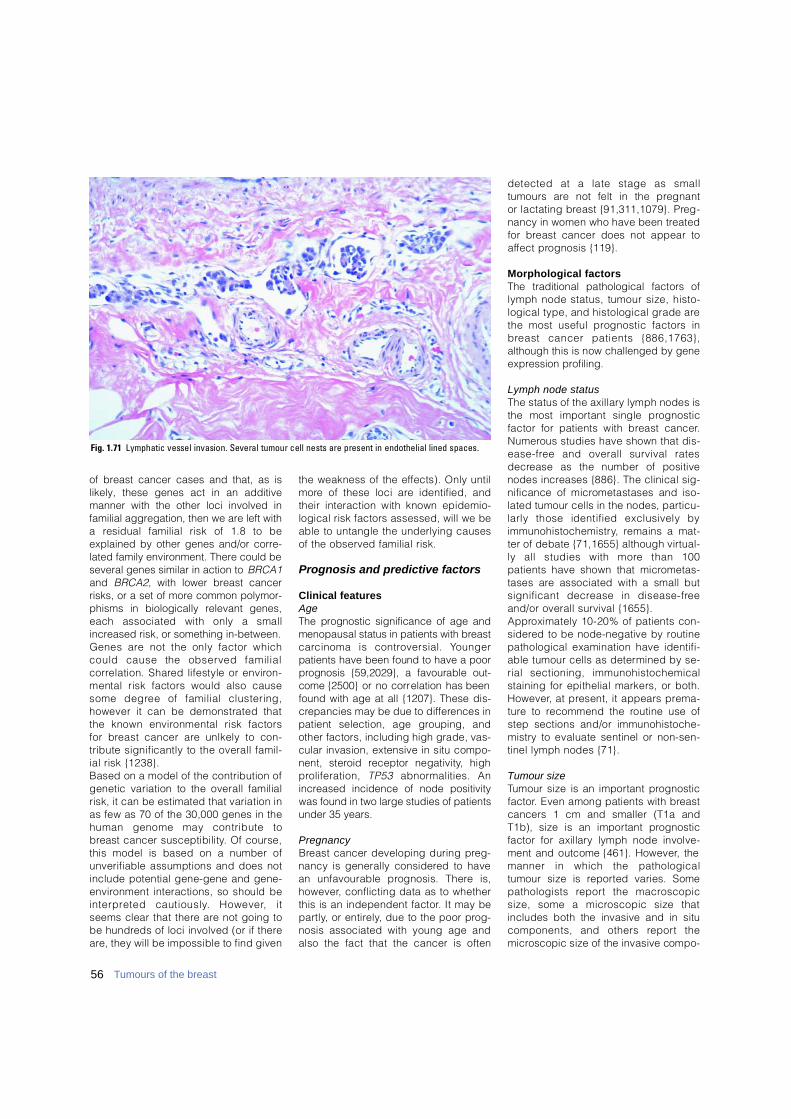
56 Tumours of the breast
of breast cancer cases and that, as islikely, these genes act in an additivemanner with the other loci involved infamilial aggregation, then we are left witha residual familial risk of 1.8 to beexplained by other genes and/or corre-lated family environment. There could beseveral genes similar in action to BRCA1and BRCA2, with lower breast cancerrisks, or a set of more common polymor-phisms in biologically relevant genes,each associated with only a smallincreased risk, or something in-between.Genes are not the only factor whichcould cause the observed familial c o r relation. Shared lifestyle or enviro n-mental risk factors would also causesome degree of familial clustering,however it can be demonstrated thatthe known environmental risk factorsfor breast cancer are unlkely to con-tribute significantly to the overall famil-ial risk {1238}.Based on a model of the contribution ofgenetic variation to the overall familialrisk, it can be estimated that variation inas few as 70 of the 30,000 genes in thehuman genome may contribute tob reast cancer susceptibility. Of course,this model is based on a number ofunverifiable assumptions and does notinclude potential gene-gene and gene-e n v i ronment interactions, so should bei n t e r p reted cautiously. However, itseems clear that there are not going tobe hundreds of loci involved (or if therea re, they will be impossible to find given
the weakness of the effects). Only untilm o re of these loci are identified, andtheir interaction with known epidemio-logical risk factors assessed, will we beable to untangle the underlying causesof the observed familial risk.
Prognosis and predictive factors
Clinical featuresA g eThe prognostic significance of age andmenopausal status in patients with bre a s tc a rcinoma is controversial. Yo u n g e rpatients have been found to have a poorp rognosis {59,2029}, a favourable out-come {2500} or no corre l a t i o n has beenfound with age at all {1207}. These dis-c repancies may be due to diff e rences inpatient selection, age grouping, andother factors, including high grade, vas-cular invasion, extensive in situ compo-nent, steroid receptor negativity, highp roliferation, T P 5 3 a b n o rmalities. Anincreased incidence of node positivitywas found in two large studies of patientsunder 35 years.
P r e g n a n c yB reast cancer developing during pre g-nancy is generally considered to havean unfavourable prognosis. There is,h o w e v e r, conflicting data as to whetherthis is an independent factor. It may bep a rt l y, or entire l y, due to the poor pro g-nosis associated with young age andalso the fact that the cancer is often
detected at a late stage as smalltumours are not felt in the pregnant or lactating breast {91,311,1079}. Pre g-nancy in women who have been tre a t e dfor breast cancer does not appear toa ffect prognosis {119}.
Morphological factorsThe traditional pathological factors oflymph node status, tumour size, histo-logical type, and histological grade arethe most useful prognostic factors inb reast cancer patients {886,1763},although this is now challenged by genee x p ression pro f i l i n g .
Lymph node statusThe status of the axillary lymph nodes isthe most important single pro g n o s t i cfactor for patients with breast cancer.N u m e rous studies have shown that dis-e a s e - f ree and overall survival ratesd e c rease as the number of positivenodes increases {886}. The clinical sig-nificance of micrometastases and iso-lated tumour cells in the nodes, part i c u-larly those identified exclusively byi m m u n o h i s t o c h e m i s t ry, remains a mat-ter of debate {71,1655} although virt u a l-ly all studies with more than 100patients have shown that micro m e t a s-tases are associated with a small butsignificant decrease in disease-fre eand/or overall survival {1655}. A p p roximately 10-20% of patients con-s i d e red to be node-negative by ro u t i n epathological examination have identifi-able tumour cells as determined by se-rial sectioning, immunohistochemicalstaining for epithelial markers, or both.H o w e v e r, at present, it appears pre m a-t u re to recommend the routine use ofstep sections and/or immunohistoche-m i s t ry to evaluate sentinel or non-sen-tinel lymph nodes {71}.
Tumour sizeTumour size is an important pro g n o s t i cf a c t o r. Even among patients with bre a s tcancers 1 cm and smaller (T1a andT1b), size is an important pro g n o s t i cfactor for axillary lymph node involve-ment and outcome {461}. However, themanner in which the pathologicaltumour size is re p o rted varies. Somepathologists re p o rt the macro s c o p i csize, some a microscopic size thatincludes both the invasive and in situcomponents, and others re p o rt them i c roscopic size of the invasive compo-
Fig. 1.71 Lymphatic vessel invasion. Several tumour cell nests are present in endothelial lined spaces.

57Invasive breast carcinoma
nent only. There is often poor corre l a t i o nbetween the tumour size determined byg ross pathological examination and thesize of the invasive component as deter-mined by histological measure m e n t{27}. The size of the invasive componentis clinically significant, and so thepathological tumour size for classifica-tion (pT) is a measurement of only theinvasive component {51}. There f o re ,when there is a discrepancy betweenthe gross and the microscopic size ofthe invasive component, the micro s c o p-ic size takes precedence, and shouldbe indicated in the pathology re p o rt andused for pathological staging.
Histological typeSome special histological types ofb reast cancer are associated with ap a rticularly favourable clinical outcome{771,2433}. These include tubular, inva-sive cribriform, mucinous, and adenoidcystic carcinomas. Some authors alsoinclude tubulolobular and papillary car-cinomas. The 20-year re c u r re n c e - f re esurvival of special type tumours 1.1 to3.0 cm in size is similar to that of inva-sive ductal carcinomas of no specialtype 1 cm and smaller (87% and 86%,respectively) {2433}. The pro g n o s t i csignificance of medullary carc i n o m aremains contro v e rtial and is discussede l s e w h e re (see medullary carc i n o m a ) .
Histological gradeGrading is recommended for all inva-sive carcinomas of the breast, re g a rd-less of morphological type {1984,2216,2905}. This practice has been crit-icized by some pathologists who feelthat grading is not appropriate for thespecial histological types such as puret u b u l a r, invasive cribriform, mucinous,m e d u l l a ry and infiltrating lobular carc i-nomas. For example, most infiltratinglobular carcinomas, especially those ofclassical subtype, are assessed asgrade 2 and the overall survival curve oflobular carcinoma overlies that of allother types of grade 2 carcinoma. Inmucinous carcinoma and in carc i n o m aof mixed morphological type, gradingp rovides a more appropriate estimate ofp rognosis than type alone {2216}. Inm e d u l l a ry carcinoma no additionalp rognostic value has been found.Higher rates of distant metastasis andp o o rer survival are seen in patients withhigher grade (poorly diff e rentiated) tu-
mours, independent of lymph node status and tumour size {550,777,836,868,886,1031,1763,2030,2434}. Tu-mour grading has prognostic valueeven in breast cancers 1 cm and small-er {461}. The optimal grading method{777} has been detailed earlier in thisc h a p t e r. The combination of histologicaltype and grade provides a more accu-rate assessment of prognosis than doeshistological type alone {2216}.Histological grade may also pro v i d euseful information with re g a rd toresponse to chemotherapy and, there-f o re, be a predictive factor as well as ap rognostic indicator. Several studieshave suggested that high histologicalgrade is associated with a betterresponse to certain chemotherapy re g i-mens than low histological grade{2254}. However, additional studies arere q u i red to define this relationship moreclearly {612}.
Tumour cell proliferationMarkers of proliferation have beenextensively investigated to evaluatep rognosis {886,1304}. Mitotic count isp a rt of histological grading. Othermethods include DNA flow cytometrym e a s u rement of S-phase fraction (SPF).Many studies indicate that high SPF isassociated with inferior outcome. Ki-67/MIB-1 is a labile, non-histone nu-clear protein detected in the G1 throughM phases of the cell cycle, but not inresting cells and is therefore a direct indi-cator of the growth fraction. The percent-age of Ki-67 positive cells can be used tostratify patients into good and poor sur-vivors. Quantitative RT-PCR in detectingthe mRNA level has also been intro-duced as well as array based quantifica-tion of proliferation (see below).
Lymphatic and blood vessel invasionLymphatic vessel invasion has be e nshown to be an important and in-dependent prognostic factor, part i c u-larly in patients with T1, node-nega-tive breast cancers {461,1606,1623, 2433,2445,2452}. Its major value is in identifying patients at increased risk of axillary lymph node involve-ment {627,839,1592,2253,2415} and adverse outcome {186a,627,1623,2415,2434}. As with histological grade,the ability of pathologists to re p ro-ducibly identify lymphatic vessel inva-sion has been challenged {998} butcan be improved if stringent criteriaa re employed {627,2109,2253,2415,2452}. Lymphatic vessel invasionmust be distinguished from tumourcell nests within artifactual tissuespaces created by shrinkage orretraction of the stroma during tissuep rocessing. Blood vessel invasion has been re p o rt-ed to have an adverse effect on clinicaloutcome. However, there is a bro a drange in the re p o rted incidence, fro munder 5% to almost 50% {1470,1592,2444,2445,2452, 3083}. This is due toa variety of factors including thepatient population, the criteria andmethodology used, and difficulty inidentifying blood vessels.
Perineural invasion Perineural invasion is sometimes ob-served in invasive breast cancers, but ithas not been shown to be an indepen-dent prognostic factor {2426}.
Tumour necrosis In most studies {2452}, the presence ofn e c rosis has been associated with an adverse effect on clinical outcome{414, 877,999,2175}, although in one,n e c rosis was associated with a worsep rognosis only within the first two yearsafter diagnosis {999}.
Inflammatory cell infiltratesThe presence of a prominent mononu-clear cell infiltrate has been corre l a t e din some studies with high histologicalgrade {2030}. However, the pro g n o s t i csignificance of this finding is contro-versial, with some studies noting anadverse effect on clinical outcome{67,286,2785} and others observingeither no significant effect or a benefi-cial effect {635,1601,2445,2785}.
Fig. 1.72 Carcinoma with central fibrosis. There isextensive central fibrosis with only a rim of inva-sive carcinoma left around the fibrotic area.

Extent of ductal carcinoma in situ The presence of an extensive intraductalcomponent is a prognostic factor forlocal recurrence in patients treated withconservative surgery and radiation thera-py, when the status of the excision mar-gins is unknown. However, this is not anindependent predictor when the micro-scopic margin status is taken into con-sideration {2569}. Its relationship withmetastatic spread and patient survivalremains unclear {2176,2437,2689}.
Tumour stroma Prominent stromal elastosis has variouslybeen reported to be associated with afavourable prognosis {2664,2858}, anunfavourable prognosis {84,1016}, andto have no prognostic significance {626,1266,2393}. The presence of a fibroticfocus in the centre of an invasive carci-noma has also been reported to be anindependent adverse prognostic indica-tor {545,1153}
Combined morphologic prognostic factorsThe best way to integrate histologicalp rognostic factors is an unre s o l v e dissue {1833}. The Nottingham Pro g n o s t i cIndex takes into consideration tumoursize, lymph node status and histologicalgrade, and stratifies patients into good,moderate and poor prognostic gro u p swith annual mortality rates of 3%, 7%,and 30%, respectively {954}. Anotherp roposal for a prognostic index includestumour size, lymph node status andmitotic index (morphometric pro g n o s t i cindex) {2993}.
Molecular markers and genee x p r e s s i o nA large number of genetic alterationshave been identified in invasive bre a s tc a rcinomas, many of which are ofpotential prognostic or predictive value.Some provide tre a t m e n t - i n d e p e n d e n ti n f o rmation on patient survival, othersp redict the likelihood that a patient willbenefit from a certain therapy. Somealterations may have both pro g n o s t i cand predictive value.
Steroid hormone receptors (Estrogen receptor (ER) and Progesterone receptor PR)E s t rogen is an important mitogen exer-ting its activity by binding to its re c e p t o r(ER). Approximately 60% of breast carc i-nomas express the ER protein. Initially,
ER-positive tumours were associatedwith an improved prognosis, but studieswith long-term follow-up have suggestedthat ER-positive tumours, despite havinga slower growth rate, do not have a lowermetastatic potential. Nonetheless, ERstatus remains very useful in pre d i c t i n gthe response to adjuvant tamoxifen {4,368,1304,1833,2120}. Measurement ofboth ER and PR has been clinical prac-tice for more than 20 years. PR is a s u r rogate marker of a functional ER. Ine s t rogen target tissues, estrogen tre a t-ment induces PR. Both can be detec-t e d by ligand binding assay, or morecommonly nowadays, by immunohis-tochemical (IHC) analysis using mo-noclonal antibodies. ER/PR-positivetumours have a 60-70% response ratec o m p a red to less than 10% for ER/PR-negative tumours. ER-positive/PR-nega-tive tumours have an intermediate re-sponse of approximately 40%. Horm o n ereceptor status is the only re c o m m e n d-ed molecular marker to be used in tre a t-ment decision {9,886, 1030}. The impactof hormone receptor status on pro g n o s i sand treatment outcome prediction iscomplex. The finding, in cell lines, thattamoxifen can interact with the re c e n t l yidentifed ERβ receptor (ERB) may pro-vide new clues towards improvement ofp redicting tamoxifen re s p o n s i v e n e s s{ 1 5 2 6 , 1 9 2 5 , 3 2 6 9 } .Epidermal growth factor receptor (EGFR)and transforming growth factor alpha( T G Fα), antiapoptotic protein bcl-2,cyclin dependent kinase inhibitor p27a re other potential prognostic markersthat look promising. Elevated expre s s i o nof EGFR, in the absence of gene amplifi-cation, has been associated with estro-gen receptor negativity {2509}.
The ERBB2 / HER2 oncogeneThe prognostic value of ERBB2 over-e x p ression, first re p o rted in 1987{2719}, has been extensively studied{2962,3173}. ERBB2 over- e x p ression isa weak to moderately independent pre-dictor of survival, at least for node-pos-itive patients. Gene amplification oro v e r- e x p ression of the ERBB2 pro t e i ncan be measured by Southern blotanalysis, FISH, diff e rential PCR, IHCand ELISA {2958}. Studies of the pre-dictive value of ERBB2-status have notbeen consistent. A recent review {3173}concluded that ERBB2 seems to be aweak to moderately strong negative
p redictor for response to alkylatingagents and a moderately positive pre-dictive factor for response to anthracy-clines. There was insufficient data todraw conclusions on the response totaxanes or radiotherapy. In an a d j u v a n tsetting, ERBB2 status should not beused to select adjuvant systemicchemotherapy or endocrine therapy.C o n v e r s e l y, when adjuvant chemothe-rapy is recommended, anthracycline-based therapy should be pre f e r red for ERBB2 positive patients. A human-ized anti-ERBB2 monoclonal antibody,trastuzumab (Herceptin), has beendeveloped as a novel anti-cancer drugtargeting overe x p ressed ERBB2 {529}.This has been shown to be effective in20% of patients with ERBB2 amplifiedt u m o u r s .
TP53 mutationsA p p roximately 25% of breast cancershave mutations in the tumour suppre s-sor gene T P 5 3, most of which are mis-sense mutations leading to the accumu-lation of a stable, but inactive protein inthe tumour cells {1196,2759,2761}.Both DNA sequencing and IHC havebeen used to assess T P 5 3-status in thet u m o u r. However, some 20% of themutations do not yield a stable pro t e i nand are thus not detected by IHC, whilen o rmal (wildtype) protein may accumu-late in response to DNA damage or cel-lular stress signals. Studies using DNAsequencing all showed a strong asso-ciation with survival whereas thoseusing only IHC did not, or did so onlyweakly {5,886,1304,2237,2760}. Giventhe diverse cellular functions of the p53p rotein and the location and type ofalteration within the gene, specificmutations might conceivably be associ-ated with a particularly poor pro g n o s i s .Patients with mutations in their tumoursa ffecting the L2/L3 domain of the p53p rotein, which is important for DNAbinding, have a particularly poor sur-vival {251,317,976,1523}.The role of p53 in the control of the cellcycle, DNA damage re p a i r, and apopto-sis, provides a strong biological ration-ale for investigating whether mutationsa re predictors of response to DNA dam-aging agents. Several studies usingDNA sequencing of the entire genehave addressed this in relation to diff e r-ent chemotherapy and radiotherapyregimes {16,241,249,976}. A stro n g
58 Tumours of the breast
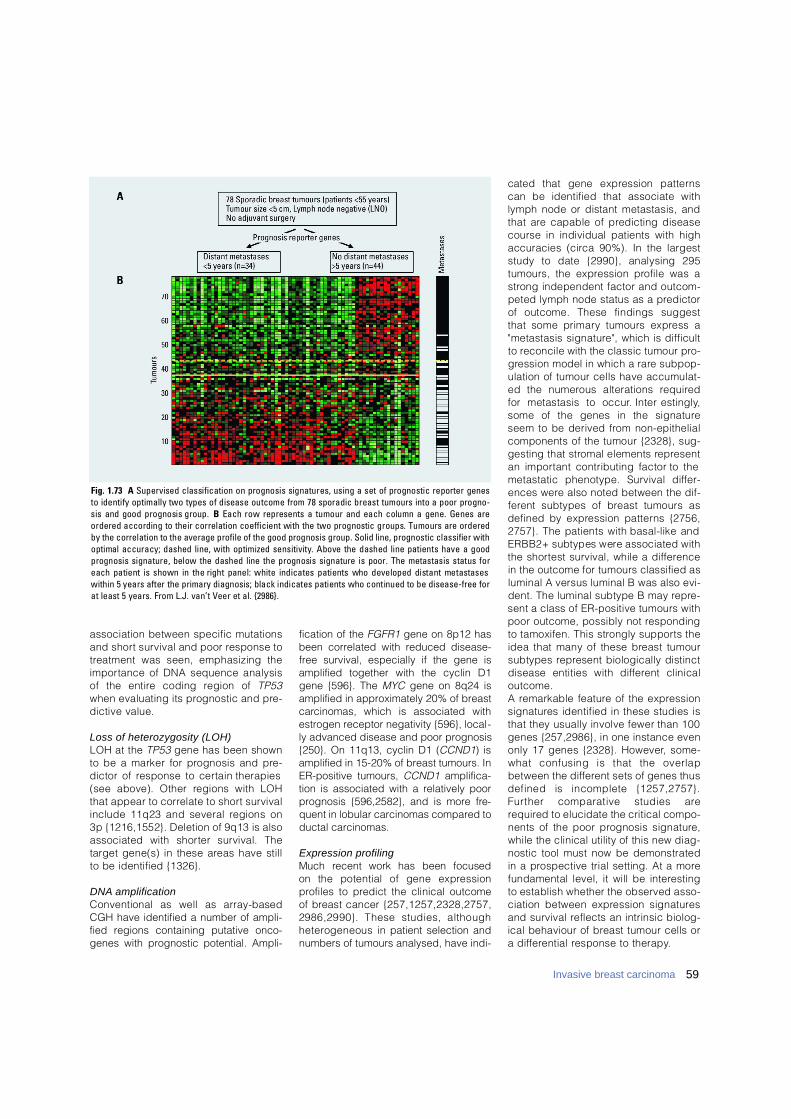
association between specific mutationsand short survival and poor response tot reatment was seen, emphasizing thei m p o rtance of DNA sequence analysisof the entire coding region of T P 5 3when evaluating its prognostic and pre-dictive value.
Loss of heterozygosity (LOH)LOH at the T P 5 3 gene has been shownto be a marker for prognosis and pre-dictor of response to certain therapies(see above). Other regions with LOHthat appear to correlate to short survivalinclude 11q23 and several regions on3p {1216,1552}. Deletion of 9q13 is alsoassociated with shorter survival. Thetarget gene(s) in these areas have stillto be identified {1326}.
D N A a m p l i f i c a t i o nConventional as well as array-basedCGH have identified a number of ampli-fied regions containing putative onco-genes with prognostic potential. Ampli-
fication of the FGFR1 gene on 8p12 hasbeen correlated with reduced disease-free survival, especially if the gene isamplified together with the cyclin D1gene {596}. The MYC gene on 8q24 isamplified in approximately 20% of breastc a rcinomas, which is associated withestrogen receptor negativity {596}, local-ly advanced disease and poor prognosis{250}. On 11q13, cyclin D1 (CCND1) isamplified in 15-20% of breast tumours. InER-positive tumours, CCND1 amplifica-tion is associated with a relatively poorprognosis {596,2582}, and is more fre-quent in lobular carcinomas compared toductal carcinomas.
Expression profilingMuch recent work has been focused on the potential of gene expression p rofiles to predict the clinical outcomeof breast cancer { 2 5 7 , 1 2 5 7 , 2 3 2 8 , 2 7 5 7 ,2986,2990}. These studies, althoughh e t e rogeneous in patient selection andnumbers of tumours analysed, have indi-
cated that gene expression pattern scan be identified that associate withlymph node or distant metastasis, andthat are capable of predicting diseasecourse in individual patients with highaccuracies (circa 90%). In the largeststudy to date {2990}, analysing 295tumours, the expression profile was as t rong independent factor and outcom-peted lymph node status as a pre d i c t o rof outcome. These findings suggestthat some primary tumours express a"metastasis signature", which is diff i c u l tto reconcile with the classic tumour pro-g ression model in which a rare subpop-ulation of tumour cells have accumulat-ed the numerous alterations re q u i re dfor metastasis to occur. Intere s t i n g l y,some of the genes in the signatureseem to be derived from non-epithelialcomponents of the tumour {2328}, sug-gesting that stromal elements re p re s e n tan important contributing factor to themetastatic phenotype. Survival diff e r-ences were also noted between the dif-f e rent subtypes of breast tumours asdefined by expression patterns {2756,2757}. The patients with basal-like andERBB2+ subtypes were associated withthe shortest survival, while a diff e re n c ein the outcome for tumours classified asluminal A versus luminal B was also evi-dent. The luminal subtype B may re p re-sent a class of ER-positive tumours withpoor outcome, possibly not re s p o n d i n gto tamoxifen. This strongly supports theidea that many of these breast tumoursubtypes re p resent biologically distinctdisease entities with diff e rent clinicalo u t c o m e .A remarkable feature of the expre s s i o ns i g n a t u res identified in these studies isthat they usually involve fewer than 100genes {257,2986}, in one instance evenonly 17 genes {2328}. However, some-what confusing is that the overlapbetween the diff e rent sets of genes thusdefined is incomplete {1257,2757}.F u rther comparative studies arere q u i red to elucidate the critical compo-nents of the poor prognosis signature ,while the clinical utility of this new diag-nostic tool must now be demonstratedin a prospective trial setting. At a morefundamental level, it will be intere s t i n gto establish whether the observed asso-ciation between expression signature sand survival reflects an intrinsic biolog-ical behaviour of breast tumour cells ora diff e rential response to therapy.
59Invasive breast carcinoma
Fig. 1.73 A Supervised classification on prognosis signatures, using a set of prognostic reporter genesto identify optimally two types of disease outcome from 78 sporadic breast tumours into a poor progno-sis and good prognosis group. B Each row represents a tumour and each column a gene. Genes areordered according to their correlation coefficient with the two prognostic groups. Tumours are orderedby the correlation to the average profile of the good prognosis group. Solid line, prognostic classifier withoptimal accuracy; dashed line, with optimized sensitivity. Above the dashed line patients have a goodprognosis signature, below the dashed line the prognosis signature is poor. The metastasis status foreach patient is shown in the right panel: white indicates patients who developed distant metastaseswithin 5 years after the primary diagnosis; black indicates patients who continued to be disease-free forat least 5 years. From L.J. van’t Veer et al. {2986}.
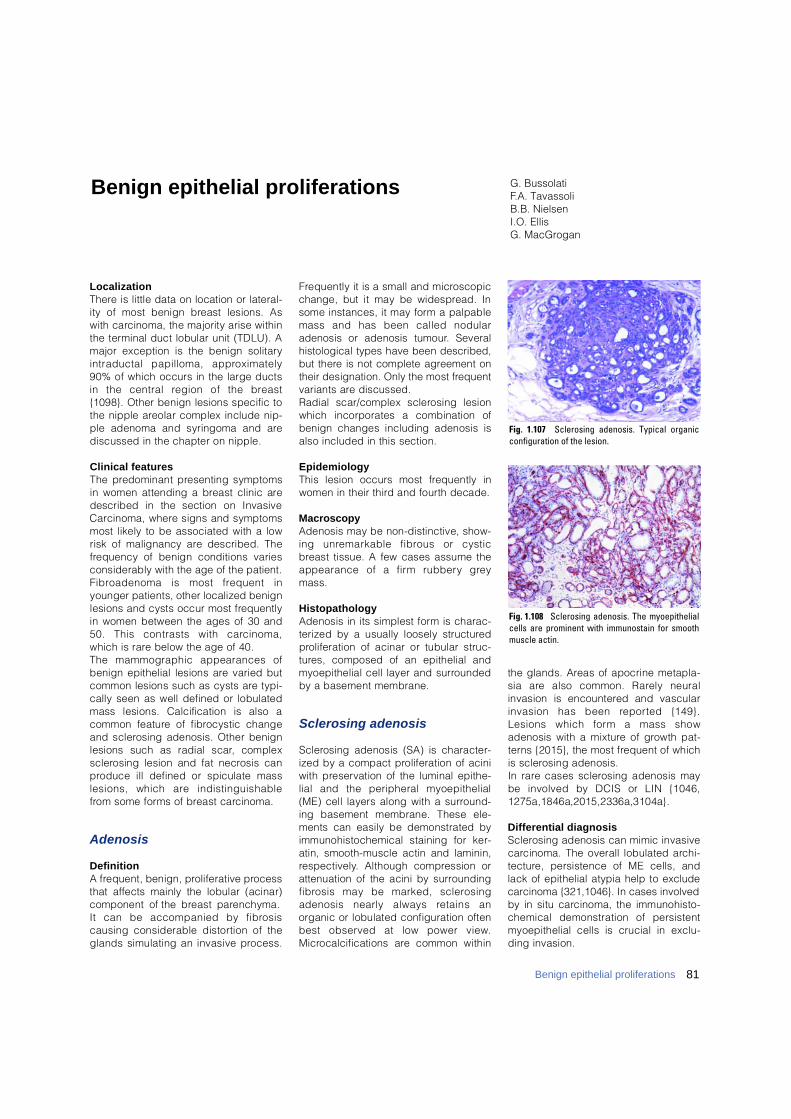
81Benign epithelial proliferations
L o c a l i z a t i o nT h e re is little data on location or lateral-ity of most benign breast lesions. Aswith carcinoma, the majority arise withinthe terminal duct lobular unit (TDLU). Amajor exception is the benign solitaryintraductal papilloma, appro x i m a t e l y90% of which occurs in the large ductsin the central region of the bre a s t{1098}. Other benign lesions specific tothe nipple areolar complex include nip-ple adenoma and syringoma and arediscussed in the chapter on nipple.
Clinical featuresThe predominant presenting symptomsin women attending a breast clinic aredescribed in the section on InvasiveC a rcinoma, where signs and symptomsmost likely to be associated with a lowrisk of malignancy are described. Thef requency of benign conditions variesconsiderably with the age of the patient.F i b roadenoma is most frequent inyounger patients, other localized benignlesions and cysts occur most fre q u e n t l yin women between the ages of 30 and50. This contrasts with carc i n o m a ,which is rare below the age of 40. The mammographic appearances ofbenign epithelial lesions are varied butcommon lesions such as cysts are typi-cally seen as well defined or lobulatedmass lesions. Calcification is also acommon feature of fibrocystic changeand sclerosing adenosis. Other benignlesions such as radial scar, complexs c l e rosing lesion and fat necrosis canp roduce ill defined or spiculate masslesions, which are indistinguishablef rom some forms of breast carc i n o m a .
A d e n o s i s
D e f i n i t i o nA frequent, benign, proliferative pro c e s sthat affects mainly the lobular (acinar)component of the breast parenchyma. It can be accompanied by fibro s i scausing considerable distortion of theglands simulating an invasive pro c e s s .
F requently it is a small and micro s c o p i cchange, but it may be widespread. Insome instances, it may form a palpablemass and has been called nodularadenosis or adenosis tumour. Severalhistological types have been described,but there is not complete agreement ontheir designation. Only the most fre q u e n tvariants are discussed. Radial scar/complex sclerosing lesionwhich incorporates a combination ofbenign changes including adenosis isalso included in this section.
E p i d e m i o l o g yThis lesion occurs most frequently inwomen in their third and fourth decade.
Macroscopy Adenosis may be non-distinctive, show-ing unremarkable fibrous or cysticb reast tissue. A few cases assume theappearance of a firm rubbery gre ymass.
Histopathology Adenosis in its simplest form is charac-terized by a usually loosely structure dp roliferation of acinar or tubular struc-t u res, composed of an epithelial andmyoepithelial cell layer and surro u n d e dby a basement membrane.
Sclerosing adenosis
S c l e rosing adenosis (SA) is character-ized by a compact proliferation of aciniwith preservation of the luminal epithe-lial and the peripheral myoepithelial(ME) cell layers along with a surro u n d-ing basement membrane. These ele-ments can easily be demonstrated byimmunohistochemical staining for ker-atin, smooth-muscle actin and laminin,re s p e c t i v e l y. Although compression orattenuation of the acini by surro u n d i n gf i b rosis may be marked, sclero s i n gadenosis nearly always retains anorganic or lobulated configuration oftenbest observed at low power view.M i c rocalcifications are common within
the glands. Areas of apocrine metapla-sia are also common. Rarely neuralinvasion is encountered and vascularinvasion has been re p o rted {149}.Lesions which form a mass showadenosis with a mixture of growth pat-t e rns {2015}, the most frequent of whichis sclerosing adenosis.In rare cases sclerosing adenosis maybe involved by DCIS or LIN {1046,1275a,1846a,2015,2336a,3104a}.
Differential diagnosisS c l e rosing adenosis can mimic invasivec a rcinoma. The overall lobulated arc h i-t e c t u re, persistence of ME cells, andlack of epithelial atypia help to excludecarcinoma {321,1046}. In cases involvedby in situ carcinoma, the immunohisto-chemical demonstration of persistentmyoepithelial cells is crucial in exclu-ding invasion.
G. BussolatiF.A. TavassoliB.B. NielsenI.O. EllisG. MacGrogan
Benign epithelial proliferations
Fig. 1.107 Sclerosing adenosis. Typical organicconfiguration of the lesion.
Fig. 1.108 Sclerosing adenosis. The myoepithelialcells are prominent with immunostain for smoothmuscle actin.
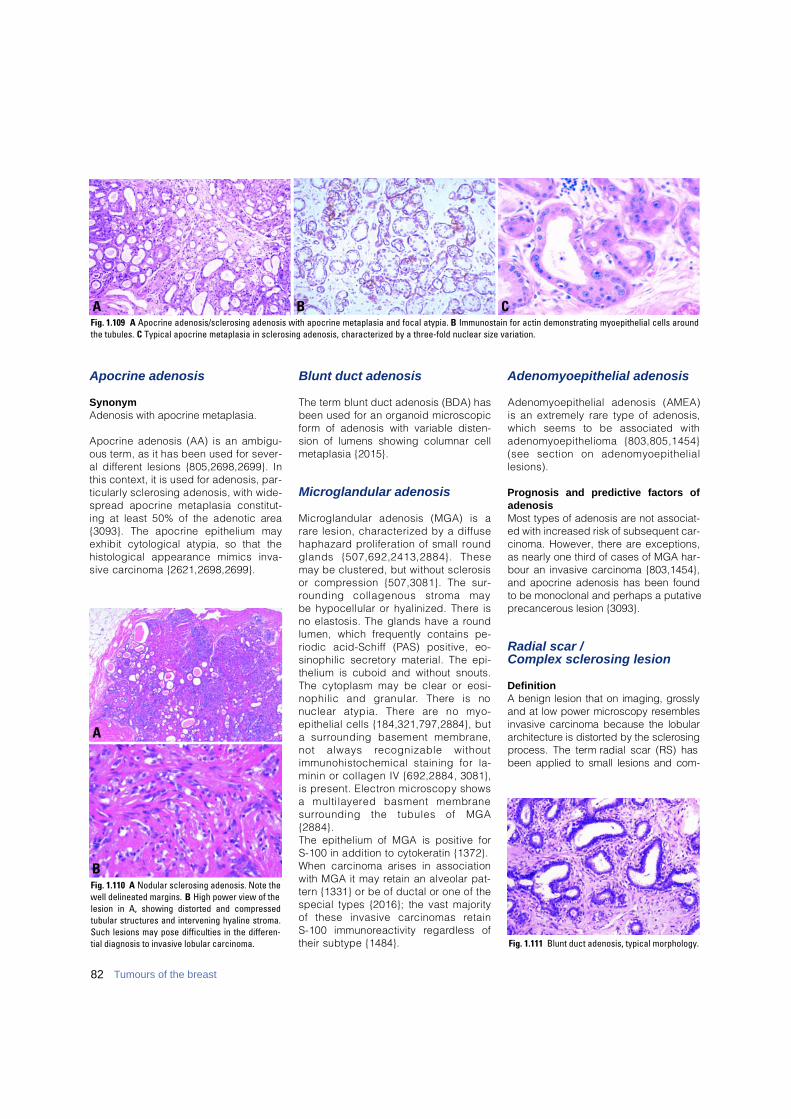
Apocrine adenosis
SynonymAdenosis with apocrine metaplasia.
Apocrine adenosis (AA) is an ambigu-ous term, as it has been used for sever-al diff e rent lesions {805,2698,2699}. Inthis context, it is used for adenosis, par-ticularly sclerosing adenosis, with wide-s p read apocrine metaplasia constitut-ing at least 50% of the adenotic are a{3093}. The apocrine epithelium mayexhibit cytological atypia, so that thehistological appearance mimics inva-sive carcinoma {2621,2698,2699}.
Blunt duct adenosis
The term blunt duct adenosis (BDA) hasbeen used for an organoid micro s c o p i cf o rm of adenosis with variable disten-sion of lumens showing columnar cellmetaplasia {2015}.
Microglandular adenosis
M i c roglandular adenosis (MGA) is ar a re lesion, characterized by a diff u s eh a p h a z a rd proliferation of small ro u n dglands {507,692,2413,2884}. Thesemay be clustered, but without sclero s i sor compression {507,3081}. The sur-rounding collagenous stroma may be hypocellular or hyalinized. There isno elastosis. The glands have a ro u n dlumen, which frequently contains pe-riodic acid-Schiff (PAS) positive, eo-sinophilic secre t o ry material. The epi-thelium is cuboid and without snouts.The cytoplasm may be clear or eosi-nophilic and granular. There is nonuclear atypia. There are no myo-epithelial cells {184,321,797,2884}, b u ta surrounding basement membrane,not always recognizable withoutimmunohistochemical staining for la-minin or collagen IV {692,2884, 3081},is present. Electron microscopy showsa multi layered basment membranes u r rounding the tubules of MGA{ 2 8 8 4 } .The epithelium of MGA is positive for S-100 in addition to cytokeratin {1372}. When carcinoma arises in associationwith MGA it may retain an alveolar pat-t e rn {1331} or be of ductal or one of thespecial types {2016}; the vast majorityof these invasive carcinomas retain S-100 immunoreactivity re g a rdless oftheir subtype {1484}.
Adenomyoepithelial adenosis
Adenomyoepithelial adenosis (AMEA)is an extremely rare type of adenosis,which seems to be associated withadenomyoepithelioma {803,805,1454}(see section on adenomyoepitheliall e s i o n s ) .
Prognosis and predictive factors ofadenosisMost types of adenosis are not associat-ed with increased risk of subsequent car-cinoma. However, there are exceptions,as nearly one third of cases of MGA har-bour an invasive carcinoma {803,1454},and apocrine adenosis has been foundto be monoclonal and perhaps a putativeprecancerous lesion {3093}.
Radial scar / Complex sclerosing lesion
Definition A benign lesion that on imaging, gro s s l yand at low power microscopy re s e m b l e sinvasive carcinoma because the lobulara rc h i t e c t u re is distorted by the sclero s i n gp rocess. The term radial scar (RS) hasb e en applied to small lesions and com-
Fig. 1.111 Blunt duct adenosis, typical morphology.
B CAFig. 1.109 A Apocrine adenosis/sclerosing adenosis with apocrine metaplasia and focal atypia. B Immunostain for actin demonstrating myoepithelial cells aroundthe tubules. C Typical apocrine metaplasia in sclerosing adenosis, characterized by a three-fold nuclear size variation.
Fig. 1.110 A Nodular sclerosing adenosis. Note thewell delineated margins. B High power view of thelesion in A, showing distorted and compressedtubular structures and intervening hyaline stroma.Such lesions may pose difficulties in the differen-tial diagnosis to invasive lobular carcinoma.
A
B
82 Tumours of the breast
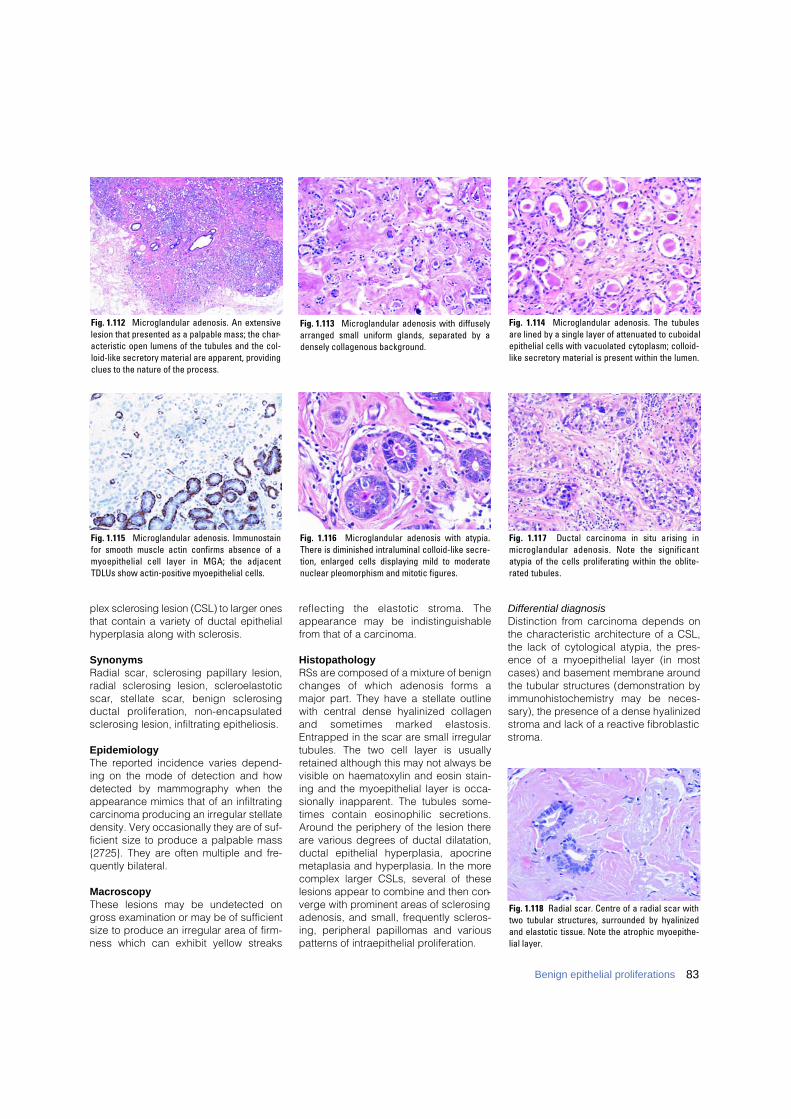
plex sclerosing lesion (CSL) to larger onesthat contain a variety of ductal epithelialhyperplasia along with sclerosis.
SynonymsRadial scar, sclerosing papillary lesion,radial sclerosing lesion, scleroelastotics c a r, stellate scar, benign sclero s i n gductal proliferation, non-encapsulatedsclerosing lesion, infiltrating epitheliosis.
EpidemiologyThe reported incidence varies depend-ing on the mode of detection and howdetected by mammography when theappearance mimics that of an infiltratingcarcinoma producing an irregular stellatedensity. Very occasionally they are of suf-ficient size to produce a palpable mass{2725}. They are often multiple and fre-quently bilateral.
MacroscopyThese lesions may be undetected ongross examination or may be of sufficientsize to produce an irregular area of firm-ness which can exhibit yellow streaks
reflecting the elastotic stroma. Theappearance may be indistinguishablefrom that of a carcinoma.
HistopathologyRSs are composed of a mixture of benignchanges of which adenosis forms amajor part. They have a stellate outlinewith central dense hyalinized collagenand sometimes marked elastosis.Entrapped in the scar are small irregulartubules. The two cell layer is usuallyretained although this may not always bevisible on haematoxylin and eosin stain-ing and the myoepithelial layer is occa-sionally inapparent. The tubules some-times contain eosinophilic secre t i o n s .Around the periphery of the lesion thereare various degrees of ductal dilatation,ductal epithelial hyperplasia, apocrinemetaplasia and hyperplasia. In the morecomplex larger CSLs, several of theselesions appear to combine and then con-verge with prominent areas of sclerosingadenosis, and small, frequently scleros-ing, peripheral papillomas and variouspatterns of intraepithelial proliferation.
Differential diagnosis Distinction from carcinoma depends onthe characteristic architecture of a CSL,the lack of cytological atypia, the pres-ence of a myoepithelial layer (in mostcases) and basement membrane aroundthe tubular structures (demonstration byi m m u n o h i s t o c h e m i s t ry may be neces-sary), the presence of a dense hyalinizedstroma and lack of a reactive fibroblasticstroma.
Fig. 1.113 Microglandular adenosis with diffuselyarranged small uniform glands, separated by adensely collagenous background.
Fig. 1.112 Microglandular adenosis. An extensivelesion that presented as a palpable mass; the char-acteristic open lumens of the tubules and the col-loid-like secretory material are apparent, providingclues to the nature of the process.
Fig. 1.114 Microglandular adenosis. The tubulesare lined by a single layer of attenuated to cuboidalepithelial cells with vacuolated cytoplasm; colloid-like secretory material is present within the lumen.
Fig. 1.115 Microglandular adenosis. Immunostainfor smooth muscle actin confirms absence of amyoepithelial cell layer in MGA; the adjacentTDLUs show actin-positive myoepithelial cells.
Fig. 1.116 Microglandular adenosis with atypia.There is diminished intraluminal colloid-like secre-tion, enlarged cells displaying mild to moderatenuclear pleomorphism and mitotic figures.
Fig. 1.117 Ductal carcinoma in situ arising inmicroglandular adenosis. Note the significantatypia of the cells proliferating within the oblite-rated tubules.
Fig. 1.118 Radial scar. Centre of a radial scar withtwo tubular structures, surrounded by hyalinizedand elastotic tissue. Note the atrophic myoepithe-lial layer.
83Benign epithelial proliferations
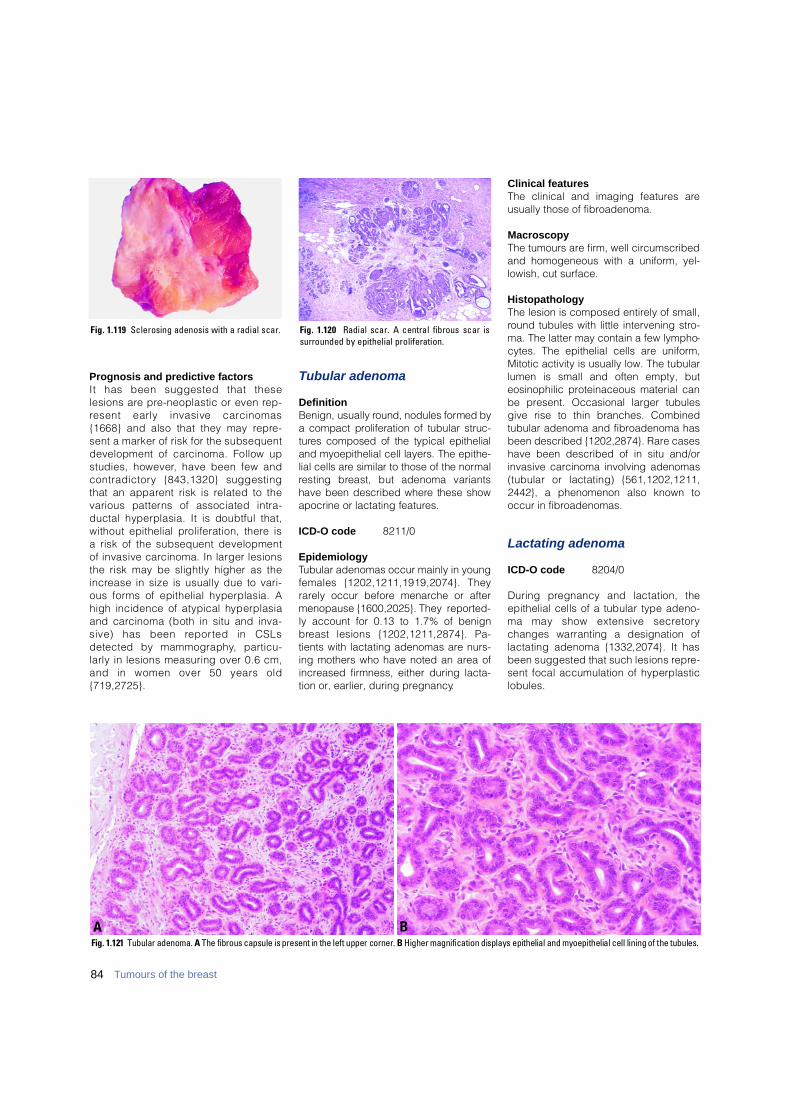
84 Tumours of the breast
Prognosis and predictive factorsIt has been suggested that theselesions are pre-neoplastic or even re p-resent early invasive carc i n o m a s{1668} and also that they may re p re-sent a marker of risk for the subsequentdevelopment of carcinoma. Follow upstudies, however, have been few andc o n t r a d i c t o ry {843,1320} suggestingthat an apparent risk is related to thevarious patterns of associated intra-ductal hyperplasia. It is doubtful that,without epithelial proliferation, there isa risk of the subsequent developmentof invasive carcinoma. In larger lesionsthe risk may be slightly higher as thei n c rease in size is usually due to vari-ous forms of epithelial hyperplasia. Ahigh incidence of atypical hyperplasiaand carcinoma (both in situ and inva-sive) has been re p o rted in CSLsdetected by mammography, part i c u-larly in lesions measuring over 0.6 cm,and in women over 50 years old{ 7 1 9 , 2 7 2 5 } .
Tubular adenoma
DefinitionBenign, usually round, nodules formed bya compact proliferation of tubular struc-t u res composed of the typical epithelialand myoepithelial cell layers. The epithe-lial cells are similar to those of the norm a lresting breast, but adenoma variantshave been described where these showapocrine or lactating features.
ICD-O code 8211/0
EpidemiologyTubular adenomas occur mainly in youngfemales {1202,1211,1919,2074}. Theyrarely occur before menarche or aftermenopause {1600,2025}. They reported-ly account for 0.13 to 1.7% of benignb reast lesions {1202,1211,2874}. Pa-tients with lactating adenomas are nurs-ing mothers who have noted an area ofincreased firmness, either during lacta-tion or, earlier, during pregnancy.
Clinical featuresThe clinical and imaging features areusually those of fibroadenoma.
MacroscopyThe tumours are firm, well circumscribedand homogeneous with a uniform, yel-lowish, cut surface.
HistopathologyThe lesion is composed entirely of small,round tubules with little intervening stro-ma. The latter may contain a few lympho-cytes. The epithelial cells are uniform,Mitotic activity is usually low. The tubularlumen is small and often empty, buteosinophilic proteinaceous material canbe present. Occasional larger tubulesgive rise to thin branches. Combinedtubular adenoma and fibroadenoma hasbeen described {1202,2874}. Rare caseshave been described of in situ and/orinvasive carcinoma involving adenomas(tubular or lactating) {561,1202,1211,2442}, a phenomenon also known tooccur in fibroadenomas.
Lactating adenoma
ICD-O code 8204/0
During pregnancy and lactation, theepithelial cells of a tubular type adeno-ma may show extensive secre t o rychanges warranting a designation oflactating adenoma {1332,2074}. It hasbeen suggested that such lesions re p re-sent focal accumulation of hyperplasticl o b u l e s .
Fig. 1.119 Sclerosing adenosis with a radial scar.
BAFig. 1.121 Tubular adenoma. A The fibrous capsule is present in the left upper corner. B Higher magnification displays epithelial and myoepithelial cell lining of the tubules.
Fig. 1.120 Radial scar. A central fibrous scar issurrounded by epithelial proliferation.
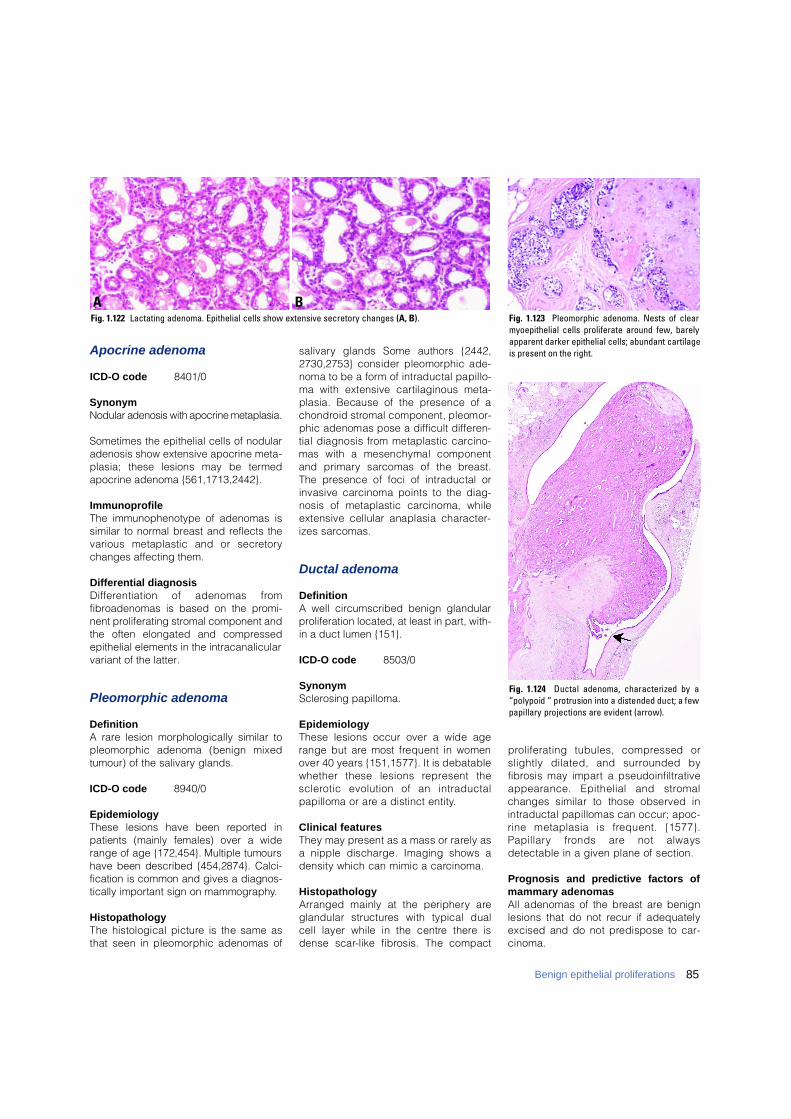
Apocrine adenoma
ICD-O code 8401/0
SynonymNodular adenosis with apocrine metaplasia.
Sometimes the epithelial cells of nodularadenosis show extensive apocrine meta-plasia; these lesions may be term e dapocrine adenoma {561,1713,2442}.
ImmunoprofileThe immunophenotype of adenomas issimilar to normal breast and reflects thevarious metaplastic and or secre t o rychanges affecting them.
Differential diagnosisD i ff e rentiation of adenomas fro mfibroadenomas is based on the promi-nent proliferating stromal component andthe often elongated and compre s s e depithelial elements in the intracanalicularvariant of the latter.
Pleomorphic adenoma
DefinitionA rare lesion morphologically similar topleomorphic adenoma (benign mixedtumour) of the salivary glands.
ICD-O code 8940/0
EpidemiologyThese lesions have been re p o rted inpatients (mainly females) over a widerange of age {172,454}. Multiple tumourshave been described {454,2874}. Calci-fication is common and gives a diagnos-tically important sign on mammography.
HistopathologyThe histological picture is the same asthat seen in pleomorphic adenomas of
s a l i v a ry glands Some authors {2442,2730,2753} consider pleomorphic ade-noma to be a form of intraductal papillo-ma with extensive cartilaginous meta-plasia. Because of the presence of ac h o n d roid stromal component, pleomor-phic adenomas pose a difficult diff e re n-tial diagnosis from metaplastic carc i n o-mas with a mesenchymal componentand primary sarcomas of the bre a s t .The presence of foci of intraductal orinvasive carcinoma points to the diag-nosis of metaplastic carcinoma, whileextensive cellular anaplasia character-izes sarc o m a s .
Ductal adenoma
DefinitionA well circumscribed benign glandularproliferation located, at least in part, with-in a duct lumen {151}.
ICD-O code 8503/0
SynonymSclerosing papilloma.
E p i d e m i o l o g yThese lesions occur over a wide agerange but are most frequent in womenover 40 years {151,1577}. It is debatablewhether these lesions re p resent thes c l e rotic evolution of an intraductalpapilloma or are a distinct entity.
Clinical featuresThey may present as a mass or rarely asa nipple discharge. Imaging shows adensity which can mimic a carc i n o m a .
Histopathology Arranged mainly at the periphery areglandular structures with typical dualcell layer while in the centre there isdense scar-like fibrosis. The compact
p roliferating tubules, compressed orslightly dilated, and surrounded byf i b rosis may impart a pseudoinfiltrativeappearance. Epithelial and stro m a lchanges similar to those observed inintraductal papillomas can occur; apoc-rine metaplasia is frequent. {1577}.P a p i l l a ry fronds are not alwaysdetectable in a given plane of section.
Prognosis and predictive factors ofmammary adenomasAll adenomas of the breast are benignlesions that do not recur if adequatelyexcised and do not predispose to car-c i n o m a .
85Benign epithelial proliferations
BAFig. 1.122 Lactating adenoma. Epithelial cells show extensive secretory changes (A, B). Fig. 1.123 Pleomorphic adenoma. Nests of clear
myoepithelial cells proliferate around few, barelyapparent darker epithelial cells; abundant cartilageis present on the right.
Fig. 1.124 Ductal adenoma, characterized by a“polypoid “ protrusion into a distended duct; a fewpapillary projections are evident (arrow).
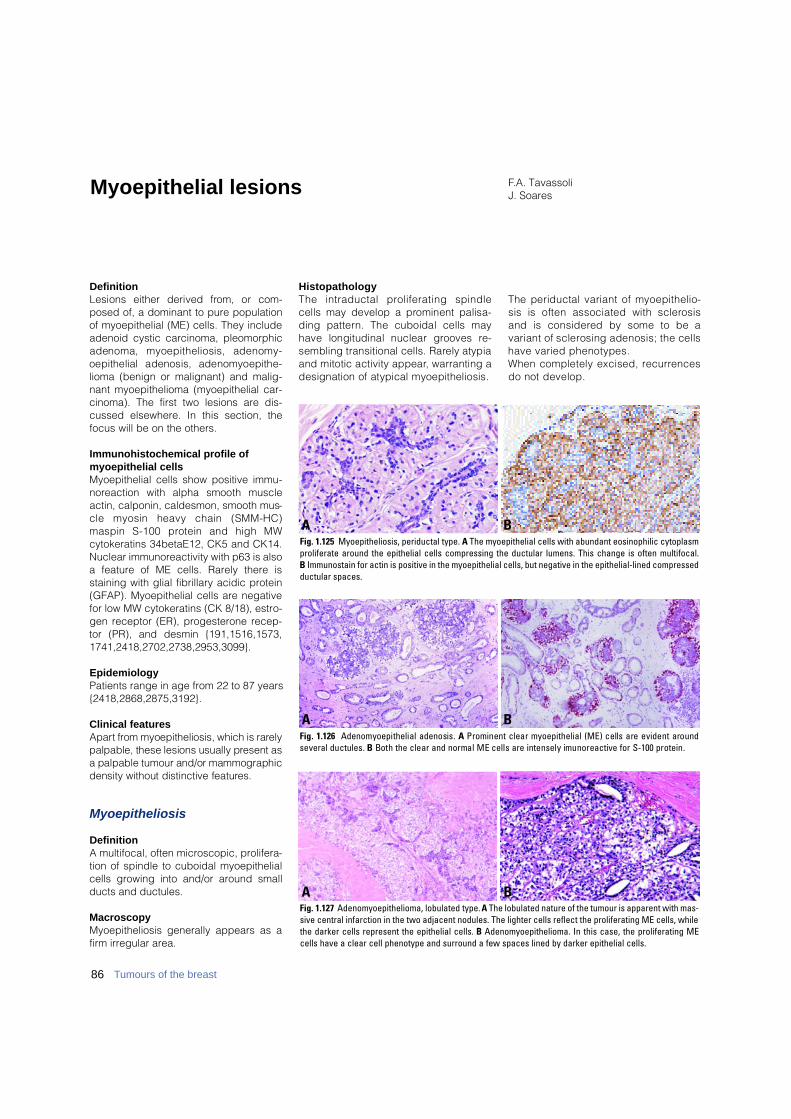
DefinitionLesions either derived from, or com-posed of, a dominant to pure populationof myoepithelial (ME) cells. They includeadenoid cystic carcinoma, pleomorphicadenoma, myoepitheliosis, adenomy-oepithelial adenosis, adenomyoepithe-lioma (benign or malignant) and malig-nant myoepithelioma (myoepithelial car-cinoma). The first two lesions are dis-cussed elsewhere. In this section, thefocus will be on the others.
Immunohistochemical profile ofmyoepithelial cells Myoepithelial cells show positive immu-n o reaction with alpha smooth muscleactin, calponin, caldesmon, smooth mus-cle myosin heavy chain (SMM-HC)maspin S-100 protein and high MWcytokeratins 34betaE12, CK5 and CK14.Nuclear immunoreactivity with p63 is alsoa feature of ME cells. Rarely there isstaining with glial fibrillary acidic protein(GFAP). Myoepithelial cells are negativefor low MW cytokeratins (CK 8/18), estro-gen receptor (ER), progesterone recep-tor (PR), and desmin {191,1516,1573,1741,2418,2702,2738,2953,3099}.
EpidemiologyPatients range in age from 22 to 87 years{2418,2868,2875,3192}.
Clinical features A p a rt from myoepitheliosis, which is rare l ypalpable, these lesions usually present asa palpable tumour and/or mammographicdensity without distinctive feature s .
Myoepitheliosis
DefinitionA multifocal, often microscopic, prolifera-tion of spindle to cuboidal myoepithelialcells growing into and/or around smallducts and ductules.
MacroscopyMyoepitheliosis generally appears as afirm irregular area.
H i s t o p a t h o l o g yThe intraductal proliferating spindlecells may develop a prominent palisa-ding pattern. The cuboidal cells mayhave longitudinal nuclear grooves re-sembling transitional cells. Rarely atypiaand mitotic activity appear, warranting adesignation of atypical myoepitheliosis.
The periductal variant of myoepithelio-sis is often associated with sclero s i sand is considered by some to be avariant of sclerosing adenosis; the cellshave varied phenotypes.When completely excised, re c u r re n c e sdo not develop.
F.A. TavassoliJ. SoaresMyoepithelial lesions
BAFig. 1.125 Myoepitheliosis, periductal type. A The myoepithelial cells with abundant eosinophilic cytoplasmproliferate around the epithelial cells compressing the ductular lumens. This change is often multifocal. B Immunostain for actin is positive in the myoepithelial cells, but negative in the epithelial-lined compressedductular spaces.
BAFig. 1.126 Adenomyoepithelial adenosis. A Prominent clear m y o e p i t h e l i a l (ME) cells are evident aroundseveral ductules. B Both the clear and normal ME cells are intensely imunoreactive for S-100 protein.
BAFig. 1.127 Adenomyoepithelioma, lobulated type. A The lobulated nature of the tumour is apparent with mas-sive central infarction in the two adjacent nodules. The lighter cells reflect the proliferating ME cells, whilethe darker cells represent the epithelial cells. B Adenomyoepithelioma. In this case, the proliferating MEcells have a clear cell phenotype and surround a few spaces lined by darker epithelial cells.
86 Tumours of the breast
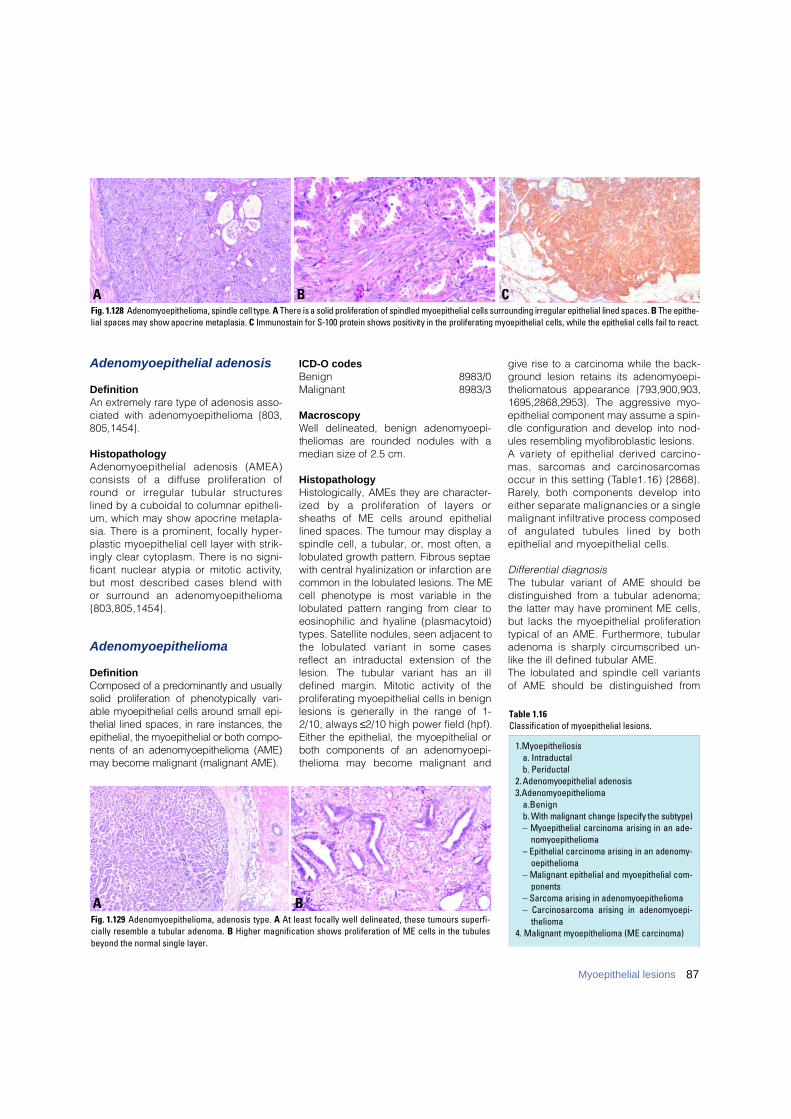
Adenomyoepithelial adenosis
DefinitionAn extremely rare type of adenosis asso-ciated with adenomyoepithelioma {803,805,1454}.
HistopathologyAdenomyoepithelial adenosis (AMEA)consists of a diffuse proliferation ofround or irregular tubular structure slined by a cuboidal to columnar epitheli-um, which may show apocrine metapla-sia. There is a prominent, focally hyper-plastic myoepithelial cell layer with strik-ingly clear cytoplasm. There is no signi-ficant nuclear atypia or mitotic a c t i v i t y,but most described cases blend with or surround an adenomyoepithelioma{803,805,1454}.
Adenomyoepithelioma
DefinitionComposed of a predominantly and usuallysolid proliferation of phenotypically vari-able myoepithelial cells around small epi-thelial lined spaces, in rare instances, theepithelial, the myoepithelial or both compo-nents of an adenomyoepithelioma (AME)may become malignant (malignant AME).
ICD-O codesBenign 8983/0Malignant 8983/3
MacroscopyWell delineated, benign adenomyoepi-theliomas are rounded nodules with amedian size of 2.5 cm.
HistopathologyHistologically, AMEs they are character-ized by a proliferation of layers orsheaths of ME cells around epitheliallined spaces. The tumour may display aspindle cell, a tubular, or, most often, alobulated growth pattern. Fibrous septaewith central hyalinization or infarction arecommon in the lobulated lesions. The MEcell phenotype is most variable in thelobulated pattern ranging from clear toeosinophilic and hyaline (plasmacytoid)types. Satellite nodules, seen adjacent tothe lobulated variant in some casesreflect an intraductal extension of thelesion. The tubular variant has an illdefined margin. Mitotic activity of theproliferating myoepithelial cells in benignlesions is generally in the range of 1-2/10, always ≤2/10 high power field (hpf).Either the epithelial, the myoepithelial orboth components of an adenomyoepi-thelioma may become malignant and
give rise to a carcinoma while the back-g round lesion retains its adenomyoepi-theliomatous appearance {793,900,903,1695,2868,2953}. The aggressive myo-epithelial component may assume a spin-dle configuration and develop into nod-ules resembling myofibroblastic lesions. A variety of epithelial derived carc i n o-mas, sarcomas and carc i n o s a rc o m a soccur in this setting (Table1.16) {2868}.R a re l y, both components develop intoeither separate malignancies or a singlemalignant infiltrative process composedof angulated tubules lined by bothepithelial and myoepithelial cells.
Differential diagnosisThe tubular variant of AME should bedistinguished from a tubular adenoma;the latter may have prominent ME cells,but lacks the myoepithelial pro l i f e r a t i o ntypical of an AME. Furt h e rm o re, tubularadenoma is sharply circumscribed un-like the ill defined tubular AME.The lobulated and spindle cell variantsof AME should be distinguished fro m
1 .M y o e p i t h e l i o s i sa. Intraductalb. Periductal
2 . Adenomyoepithelial adenosis3 .A d e n o m y o e p i t h e l i o m a
a .B e n i g nb . With malignant change (specify the subtype)– Myoepithelial carcinoma arising in an ade-
n o m y o e p i t h e l i o m a– Epithelial carcinoma arising in an adenomy-
o e p i t h e l i o m a– Malignant epithelial and myoepithelial com-
p o n e n t s– Sarcoma arising in adenomyoepithelioma– Carcinosarcoma arising in adenomyoepi-
thelioma4. Malignant myoepithelioma (ME carcinoma)
Table 1.16Classification of myoepithelial lesions.
B CAFig. 1.128 Adenomyoepithelioma, spindle cell type. A There is a solid proliferation of spindled myoepithelial cells surrounding irregular epithelial lined spaces. B The epithe-lial spaces may show apocrine metaplasia. C Immunostain for S-100 protein shows positivity in the proliferating myoepithelial cells, while the epithelial cells fail to react.
BAFig. 1.129 Adenomyoepithelioma, adenosis type. A At least focally well delineated, these tumours superfi-cially resemble a tubular adenoma. B Higher magnification shows proliferation of ME cells in the tubulesbeyond the normal single layer.
87Myoepithelial lesions
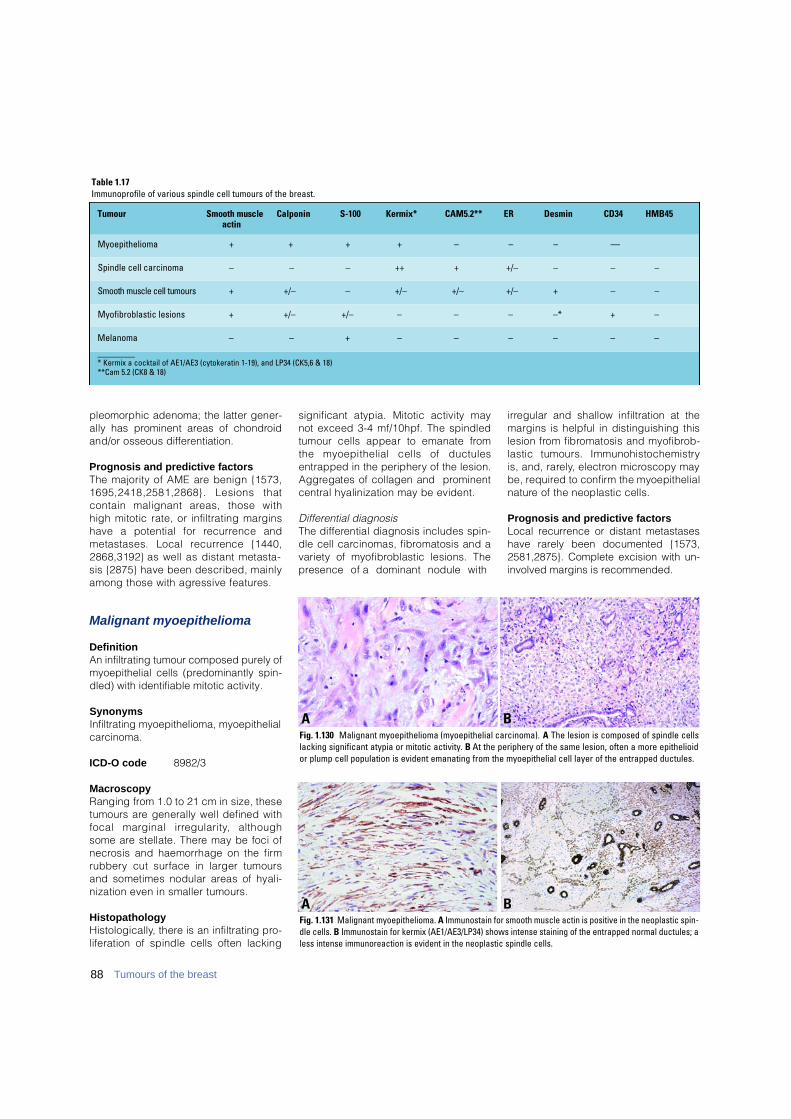
pleomorphic adenoma; the latter gener-ally has prominent areas of chondro i dand/or osseous diff e re n t i a t i o n .
Prognosis and predictive factorsThe majority of AME are benign {1573,1695,2418,2581,2868}. Lesions thatcontain malignant areas, those withhigh mitotic rate, or infiltrating marginshave a potential for re c u r rence andmetastases. Local re c u r rence {1440,2868,3192} as well as distant metasta-sis {2875} have been described, mainlyamong those with agressive features.
Malignant myoepithelioma
DefinitionAn infiltrating tumour composed purely ofmyoepithelial cells (predominantly spin-dled) with identifiable mitotic activity.
Synonyms Infiltrating myoepithelioma, myoepithelialcarcinoma.
ICD-O code 8982/3
Macroscopy Ranging from 1.0 to 21 cm in size, thesetumours are generally well defined withfocal marginal irre g u l a r i t y, althoughsome are stellate. There may be foci ofn e c rosis and haemorrhage on the firmr u b b e ry cut surface in larger tumoursand sometimes nodular areas of hyali-nization even in smaller tumours.
HistopathologyH i s t o l o g i c a l l y, there is an infiltrating pro-liferation of spindle cells often lacking
significant atypia. Mitotic activity maynot exceed 3-4 mf/10hpf. The spindledtumour cells appear to emanate fro mthe myoepithelial cells of ductulesentrapped in the periphery of the lesion.A g g regates of collagen and pro m i n e n tcentral hyalinization may be evident.
Differential diagnosisThe diff e rential diagnosis includes spin-dle cell carcinomas, fibromatosis and avariety of myofibroblastic lesions. Thep resence of a dominant nodule with
i r regular and shallow infiltration at themargins is helpful in distinguishing thislesion from fibromatosis and myofibro b-lastic tumours. Immunohistochemistryis, and, rare l y, electron microscopy maybe, re q u i red to confirm the myoepithelialn a t u re of the neoplastic cells.
Prognosis and predictive factorsLocal recurrence or distant metastaseshave rarely been documented {1573,2581,2875}. Complete excision with un-involved margins is recommended.
88 Tumours of the breast
BAFig. 1.130 Malignant myoepithelioma (myoepithelial carcinoma). A The lesion is composed of spindle cellslacking significant atypia or mitotic activity. B At the periphery of the same lesion, often a more epithelioidor plump cell population is evident emanating from the myoepithelial cell layer of the entrapped ductules.
BAFig. 1.131 Malignant myoepithelioma. A Immunostain for smooth muscle actin is positive in the neoplastic spin-dle cells. B Immunostain for kermix (AE1/AE3/LP34) shows intense staining of the entrapped normal ductules; aless intense immunoreaction is evident in the neoplastic spindle cells.
Table 1.17Immunoprofile of various spindle cell tumours of the breast.
Tumour Smooth muscle Calponin S-100 Kermix* CAM5.2** ER Desmin CD34 HMB45a c t i n
Myoepithelioma + + + + – – – – –
Spindle cell carcinoma – – – ++ + +/– – – –
Smooth muscle cell tumours + +/– – +/– +/– +/– + – –
Myofibroblastic lesions + +/– +/– – – – –* + –
Melanoma – – + – – – – – –
________* Kermix a cocktail of AE1/AE3 (cytokeratin 1-19), and LP34 (CK5,6 & 18)**Cam 5.2 (CK8 & 18)
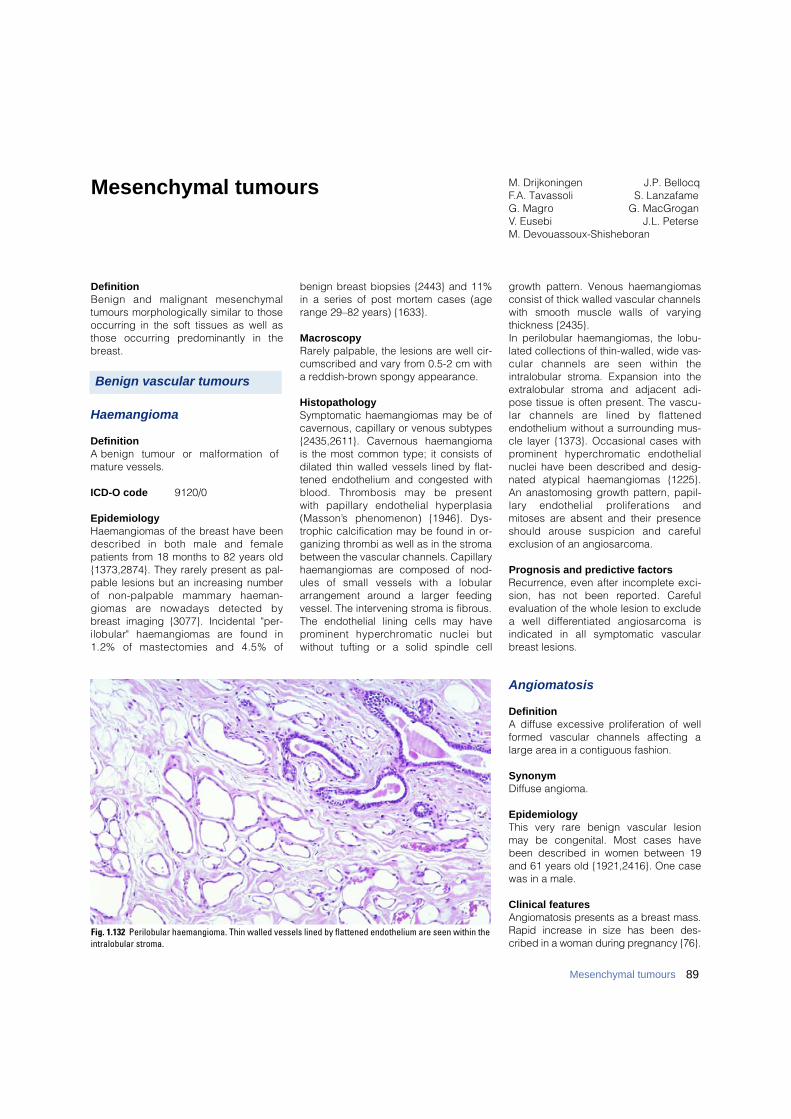
89Mesenchymal tumours
DefinitionBenign and malignant mesenchymaltumours morphologically similar to thoseoccurring in the soft tissues as well asthose occurring predominantly in thebreast.
Haemangioma
DefinitionA benign tumour or malformation ofmature vessels.
ICD-O code 9120/0
EpidemiologyHaemangiomas of the breast have beendescribed in both male and femalepatients from 18 months to 82 years old{1373,2874}. They rarely present as pal-pable lesions but an increasing numberof non-palpable mammary haeman-giomas are nowadays detected bybreast imaging {3077}. Incidental "per-ilobular" haemangiomas are found in1.2% of mastectomies and 4.5% of
benign breast biopsies {2443} and 11%in a series of post mortem cases (agerange 29–82 years) {1633}.
MacroscopyRarely palpable, the lesions are well cir-cumscribed and vary from 0.5-2 cm witha reddish-brown spongy appearance.
HistopathologySymptomatic haemangiomas may be ofcavernous, capillary or venous subtypes{2435,2611}. Cavernous haemangiomais the most common type; it consists ofdilated thin walled vessels lined by flat-tened endothelium and congested withblood. Thrombosis may be present with papillary endothelial hyperplasia( M a s s o n ’s phenomenon) {1946}. Dys-trophic calcification may be found in or-ganizing thrombi as well as in the stromabetween the vascular channels. Capillaryhaemangiomas are composed of nod-ules of small vessels with a lobulararrangement around a larger feedingvessel. The intervening stroma is fibrous.The endothelial lining cells may havep rominent hyperc h romatic nuclei butwithout tufting or a solid spindle cell
growth pattern. Venous haemangiomasconsist of thick walled vascular channelswith smooth muscle walls of vary i n gthickness {2435}.In perilobular haemangiomas, the lobu-lated collections of thin-walled, wide vas-cular channels are seen within theintralobular stroma. Expansion into theextralobular stroma and adjacent adi-pose tissue is often present. The vascu-lar channels are lined by flattenedendothelium without a surrounding mus-cle layer {1373}. Occasional cases withp rominent hyperc h romatic endothelialnuclei have been described and desig-nated atypical haemangiomas {1225}.An anastomosing growth pattern, papil-l a ry endothelial proliferations andmitoses are absent and their presenceshould arouse suspicion and care f u lexclusion of an angiosarcoma.
Prognosis and predictive factorsRecurrence, even after incomplete exci-sion, has not been re p o rted. Care f u levaluation of the whole lesion to excludea well diff e rentiated angiosarcoma isindicated in all symptomatic vascularbreast lesions.
Angiomatosis
DefinitionA diffuse excessive proliferation of wellf o rmed vascular channels affecting alarge area in a contiguous fashion.
SynonymDiffuse angioma.
EpidemiologyThis very rare benign vascular lesionmay be congenital. Most cases havebeen described in women between 19and 61 years old {1921,2416}. One casewas in a male.
Clinical featuresAngiomatosis presents as a breast mass.Rapid increase in size has been des-cribed in a woman during pregnancy {76}.
M. Drijkoningen J.P. BellocqF.A. Tavassoli S. LanzafameG. Magro G. MacGroganV. Eusebi J.L. PeterseM. Devouassoux-Shisheboran
Mesenchymal tumours
Fig. 1.132 Perilobular haemangioma. Thin walled vessels lined by flattened endothelium are seen within theintralobular stroma.
Benign vascular tumours
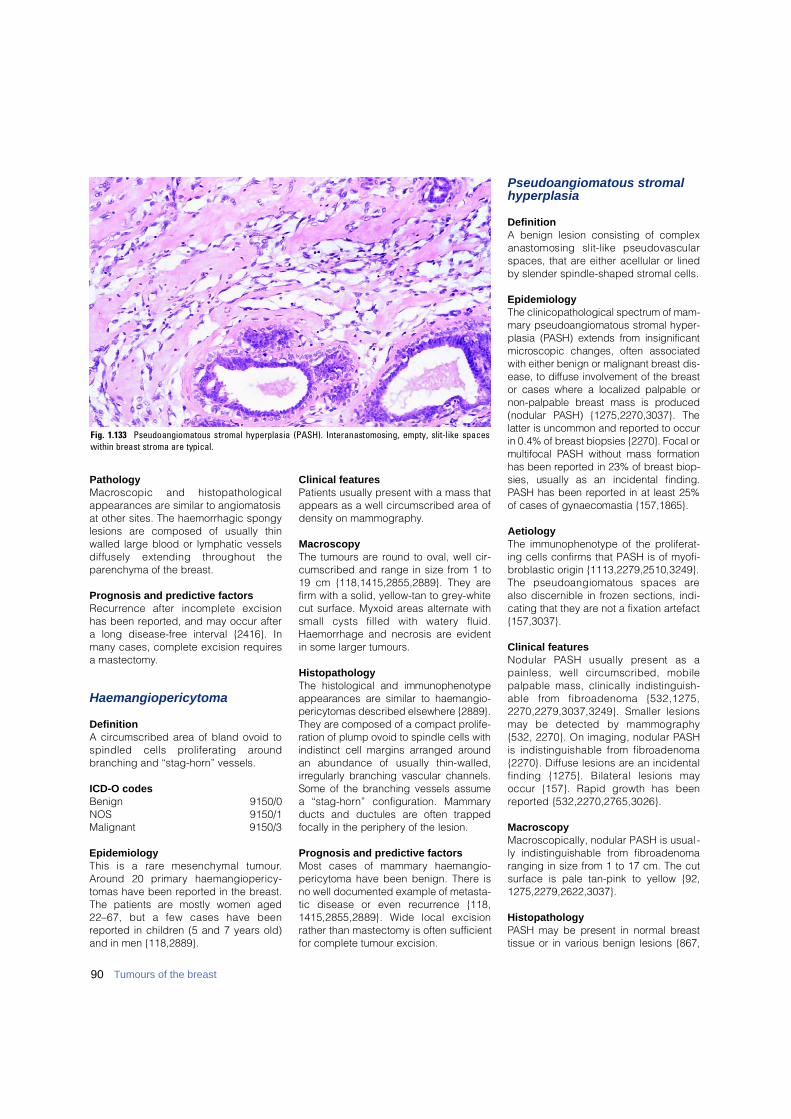
PathologyM a c roscopic and histopathologicalappearances are similar to angiomatosisat other sites. The haemorrhagic spongylesions are composed of usually thinwalled large blood or lymphatic vesselsd i ffusely extending throughout theparenchyma of the breast.
Prognosis and predictive factorsR e c u r rence after incomplete excisionhas been reported, and may occur aftera long disease-free interval {2416}. Inmany cases, complete excision requiresa mastectomy.
Haemangiopericytoma
DefinitionA circumscribed area of bland ovoid tospindled cells proliferating aro u n dbranching and “stag-horn” vessels.
ICD-O codes Benign 9150/0NOS 9150/1Malignant 9150/3
EpidemiologyThis is a rare mesenchymal tumour.A round 20 primary haemangiopericy-tomas have been reported in the breast.The patients are mostly women aged22–67, but a few cases have beenreported in children (5 and 7 years old)and in men {118,2889}.
Clinical featuresPatients usually present with a mass thatappears as a well circumscribed area ofdensity on mammography.
MacroscopyThe tumours are round to oval, well cir-cumscribed and range in size from 1 to19 cm {118,1415,2855,2889}. They arefirm with a solid, yellow-tan to grey-whitecut surface. Myxoid areas alternate withsmall cysts filled with watery fluid.Haemorrhage and necrosis are evidentin some larger tumours.
HistopathologyThe histological and immunophenotypeappearances are similar to haemangio-pericytomas described elsewhere {2889}.They are composed of a compact pro l i f e-ration of plump ovoid to spindle cells withindistinct cell margins arranged aro u n dan abundance of usually thin-walled,i r regularly branching vascular channels.Some of the branching vessels assume a “stag-horn” configuration. Mammaryducts and ductules are often trappedfocally in the periphery of the lesion.
Prognosis and predictive factorsMost cases of mammary haemangio-pericytoma have been benign. There isno well documented example of metasta-tic disease or even re c u r rence {118,1415,2855,2889}. Wide local excisionrather than mastectomy is often sufficientfor complete tumour excision.
Pseudoangiomatous stromalhyperplasia
DefinitionA benign lesion consisting of complexanastomosing slit-like pseudovascularspaces, that are either acellular or linedby slender spindle-shaped stromal cells.
EpidemiologyThe clinicopathological spectrum of mam-m a ry pseudoangiomatous stromal hyper-plasia (PASH) extends from insignificantm i c roscopic changes, often associatedwith either benign or malignant breast dis-ease, to diffuse involvement of the bre a s tor cases where a localized palpable ornon-palpable breast mass is pro d u c e d(nodular PASH) {1275,2270,3037}. Thelatter is uncommon and re p o rted to occurin 0.4% of breast biopsies {2270}. Focal ormultifocal PASH without mass form a t i o nhas been re p o rted in 23% of breast biop-sies, usually as an incidental finding.PASH has been re p o rted in at least 25%of cases of gynaecomastia {157,1865}.
AetiologyThe immunophenotype of the proliferat-ing cells confirms that PASH is of myofi-broblastic origin {1113,2279,2510,3249}.The pseudoangiomatous spaces arealso discernible in frozen sections, indi-cating that they are not a fixation artefact{157,3037}.
Clinical featuresNodular PASH usually present as apainless, well circumscribed, mobilepalpable mass, clinically indistinguish-able from fibroadenoma {532,1275,2270,2279,3037,3249}. Smaller lesionsmay be detected by mammography{532, 2270}. On imaging, nodular PA S His indistinguishable from fibro a d e n o m a{2270}. Diffuse lesions are an incidentalfinding {1275}. Bilateral lesions mayoccur {157}. Rapid growth has beenre p o rted {532,2270,2765,3026}.
MacroscopyMacroscopically, nodular PASH is usual -ly indistinguishable from fibroadenomaranging in size from 1 to 17 cm. The cutsurface is pale tan-pink to yellow {92,1275,2279,2622,3037}.
HistopathologyPASH may be present in normal bre a s ttissue or in various benign lesions {867,
90 Tumours of the breast
Fig. 1.133 Pseudoangiomatous stromal hyperplasia (PASH). Interanastomosing, empty, slit-like spaceswithin breast stroma are typical.
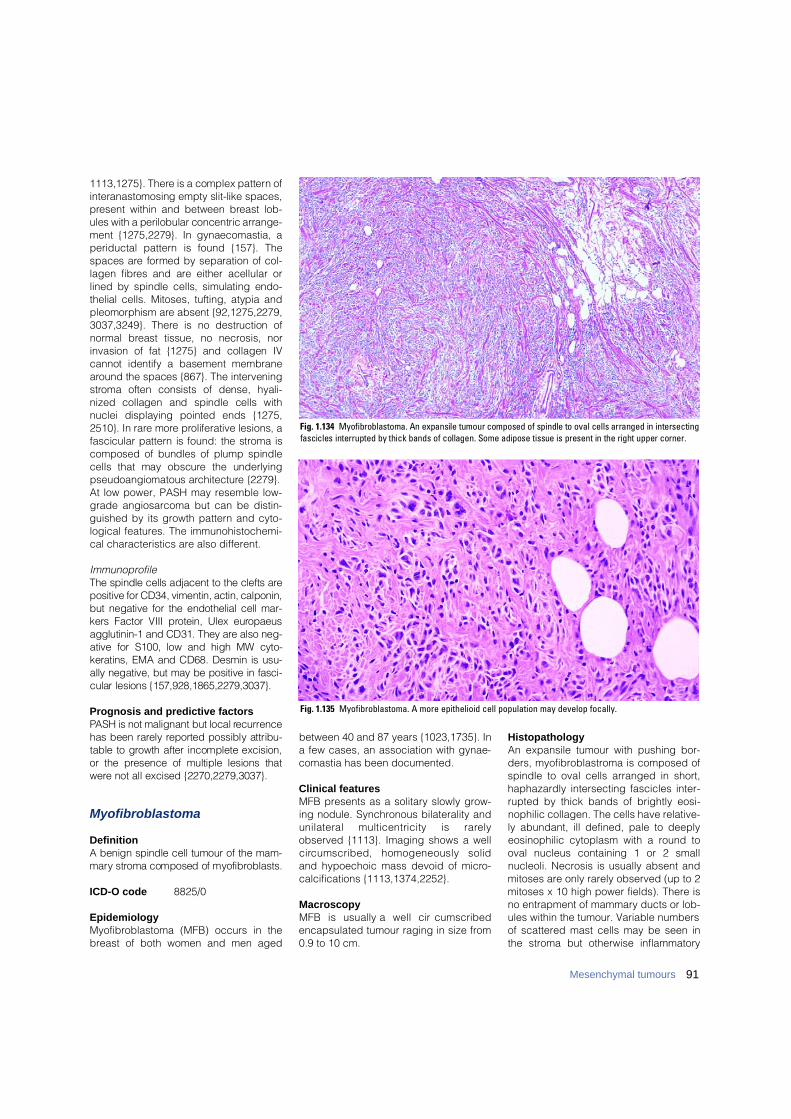
91Mesenchymal tumours
1113,1275}. There is a complex pattern ofinteranastomosing empty slit-like spaces,p resent within and between breast l o b-ules with a perilobular concentric arrange-ment {1275,2279}. In gynaecomastia, aperiductal pattern is found {157}. Thespaces are formed by separation of col-lagen fibres and are either acellular orlined by spindle cells, simulating endo-thelial cells. Mitoses, tufting, atypia andpleomorphism are absent {92,1275,2279,3037,3249}. There is no destruction ofn o rmal breast tissue, no necrosis, norinvasion of fat {1275} and collagen IVcannot identify a basement membranea round the spaces {867}. The intervenings t roma often consists of dense, hyali-nized collagen and spindle cells withnuclei displaying pointed ends {1275,2510}. In rare more proliferative lesions, afascicular pattern is found: the stroma iscomposed of bundles of plump spindlecells that may obscure the underlyingpseudoangiomatous arc h i t e c t u re {2279}. At low power, PASH may resemble low-grade angiosarcoma but can be distin-guished by its growth pattern and cyto-logical features. The immunohistochemi-cal characteristics are also different.
Immunoprofile The spindle cells adjacent to the clefts arepositive for CD34, vimentin, actin, calponin,but negative for the endothelial cell mar-kers Factor VIII protein, Ulex euro p a e u sagglutinin-1 and CD31. They are also neg-ative for S100, low and high MW cyto-keratins, EMA and CD68. Desmin is usu-ally negative, but may be positive in fasci-cular lesions {157,928,1865,2279,3037}.
Prognosis and predictive factorsPASH is not malignant but local re c u r re n c ehas been rarely re p o rted possibly attribu-table to growth after incomplete excision,or the presence of multiple lesions thatw e re not all excised {2270,2279,3037}.
Myofibroblastoma
DefinitionA benign spindle cell tumour of the mam-m a ry stroma composed of myofibro b l a s t s .
ICD-O code 8825/0
EpidemiologyMyofibroblastoma (MFB) occurs in thebreast of both women and men aged
between 40 and 87 years {1023,1735}. Ina few cases, an association with gynae-comastia has been documented.
Clinical featuresMFB presents as a solitary slowly grow-ing nodule. Synchronous bilaterality andunilateral multicentricity is rare l yobserved {1113}. Imaging shows a wellc i rcumscribed, homogeneously solidand hypoechoic mass devoid of micro-calcifications {1113,1374,2252}.
MacroscopyMFB is usually a well circ u m s c r i b e dencapsulated tumour raging in size from0.9 to 10 cm.
HistopathologyAn expansile tumour with pushing bor-ders, myofibroblastroma is composed ofspindle to oval cells arranged in short,haphazardly intersecting fascicles inter-rupted by thick bands of brightly eosi-nophilic collagen. The cells have relative-ly abundant, ill defined, pale to deeplyeosinophilic cytoplasm with a round tooval nucleus containing 1 or 2 smallnucleoli. Necrosis is usually absent andmitoses are only rarely observed (up to 2mitoses x 10 high power fields). There isno entrapment of mammary ducts or lob-ules within the tumour. Variable numbersof scattered mast cells may be seen inthe stroma but otherwise inflammatory
Fig. 1.134 Myofibroblastoma. An expansile tumour composed of spindle to oval cells arranged in intersectingfascicles interrupted by thick bands of collagen. Some adipose tissue is present in the right upper corner.
Fig. 1.135 Myofibroblastoma. A more epithelioid cell population may develop focally.
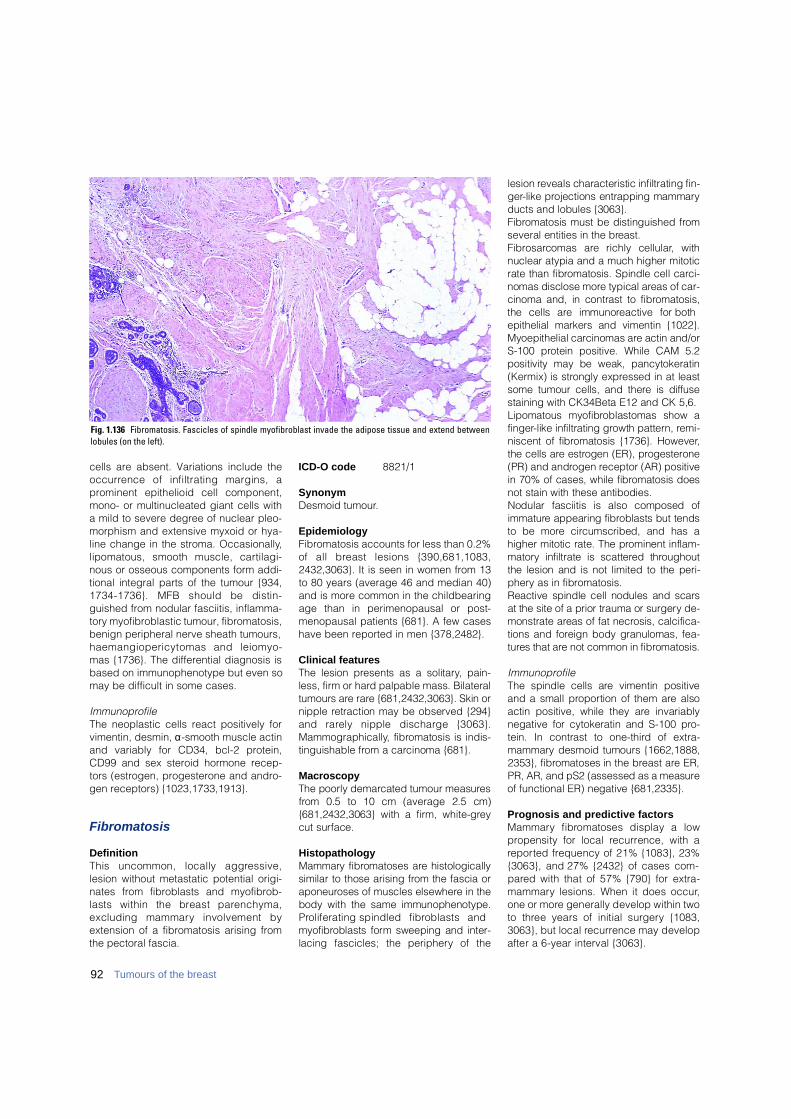
cells are absent. Variations include theo c c u r rence of infiltrating margins, ap rominent epithelioid cell component,mono- or multinucleated giant cells witha mild to severe degree of nuclear pleo-morphism and extensive myxoid or hya-line change in the stroma. Occasionally,lipomatous, smooth muscle, cart i l a g i-nous or osseous components form addi-tional integral parts of the tumour {934,1734-1736}. MFB should be distin-guished from nodular fasciitis, inflamma-tory myofibroblastic tumour, fibromatosis,benign peripheral nerve sheath tumours,haemangiopericytomas and leiomyo-mas {1736}. The differential diagnosis isbased on immunophenotype but even somay be difficult in some cases.
ImmunoprofileThe neoplastic cells react positively forvimentin, desmin, α-smooth muscle actinand variably for CD34, bcl-2 protein,CD99 and sex steroid hormone recep-tors (estrogen, progesterone and andro-gen receptors) {1023,1733,1913}.
Fibromatosis
DefinitionThis uncommon, locally aggre s s i v e ,lesion without metastatic potential origi-nates from fibroblasts and myofibrob-lasts within the breast pare n c h y m a ,excluding mammary involvement byextension of a fibromatosis arising fromthe pectoral fascia.
ICD-O code 8821/1
SynonymDesmoid tumour.
EpidemiologyFibromatosis accounts for less than 0.2%of all breast lesions {390,681,1083,2432,3063}. It is seen in women from 13to 80 years (average 46 and median 40)and is more common in the childbearingage than in perimenopausal or post-menopausal patients {681}. A few caseshave been reported in men {378,2482}.
Clinical featuresThe lesion presents as a solitary, pain-less, firm or hard palpable mass. Bilateraltumours are rare {681,2432,3063}. Skin ornipple retraction may be observed {294}and rarely nipple discharge {3063}.M a m m o g r a p h i c a l l y, fibromatosis is indis-tinguishable from a carcinoma {681}.
M a c r o s c o p yThe poorly demarcated tumour measure sf rom 0.5 to 10 cm (average 2.5 cm){681,2432,3063} with a firm, white-gre ycut surface.
HistopathologyM a m m a ry fibromatoses are histologicallysimilar to those arising from the fascia ora p o n e u roses of muscles elsewhere in thebody with the same immunophenotype.P roliferating spindled fibroblasts andm y o f i b roblasts form sweeping and inter-lacing fascicles; the periphery of the
lesion reveals characteristic infiltrating fin-g e r-like projections entrapping mammaryducts and lobules {3063}.F i b romatosis must be distinguished fro mseveral entities in the bre a s t .F i b ro s a rcomas are richly cellular, withnuclear atypia and a much higher mitoticrate than fibromatosis. Spindle cell carc i-nomas disclose more typical areas of car-cinoma and, in contrast to fibro m a t o s i s ,the cells are immunoreactive for bothepithelial markers and vimentin {1022}.Myoepithelial carcinomas are actin and/orS-100 protein positive. While CAM 5.2positivity may be weak, pancytokeratin( K e rmix) is strongly expressed in at leastsome tumour cells, and there is diff u s estaining with CK34Beta E12 and CK 5,6. Lipomatous myofibroblastomas show af i n g e r-like infiltrating growth pattern, re m i-niscent of fibromatosis {1736}. However,the cells are estrogen (ER), pro g e s t e ro n e(PR) and androgen receptor (AR) positivein 70% of cases, while fibromatosis doesnot stain with these antibodies.Nodular fasciitis is also composed ofi m m a t u re appearing fibroblasts but tendsto be more circumscribed, and has ahigher mitotic rate. The prominent inflam-m a t o ry infiltrate is scattered thro u g h o u tthe lesion and is not limited to the peri-p h e ry as in fibro m a t o s i s .Reactive spindle cell nodules and scarsa t the site of a prior trauma or surgery de-monstrate areas of fat necrosis, calcifica-tions and foreign body granulomas, fea-t u res that are not common in fibromatosis.
I m m u n o p ro f i l eThe spindle cells are vimentin positiveand a small pro p o rtion of them are alsoactin positive, while they are invariablynegative for cytokeratin and S-100 pro-tein. In contrast to one-third of extra-m a m m a ry desmoid tumours {1662,1888,2353}, fibromatoses in the breast are ER,PR, AR, and pS2 (assessed as a measureof functional ER) negative {681,2335}.
Prognosis and predictive factorsM a m m a ry fibromatoses display a lowp ropensity for local re c u r rence, with are p o rted frequency of 21% {1083}, 23%{3063}, and 27% {2432} of cases com-p a red with that of 57% {790} for extra-m a m m a ry lesions. When it does occur,one or more generally develop within twoto three years of initial surgery {1083,3063}, but local re c u r rence may developafter a 6-year interval {3063}.
92 Tumours of the breast
Fig. 1.136 Fibromatosis. Fascicles of spindle myofibroblast invade the adipose tissue and extend betweenlobules (on the left).
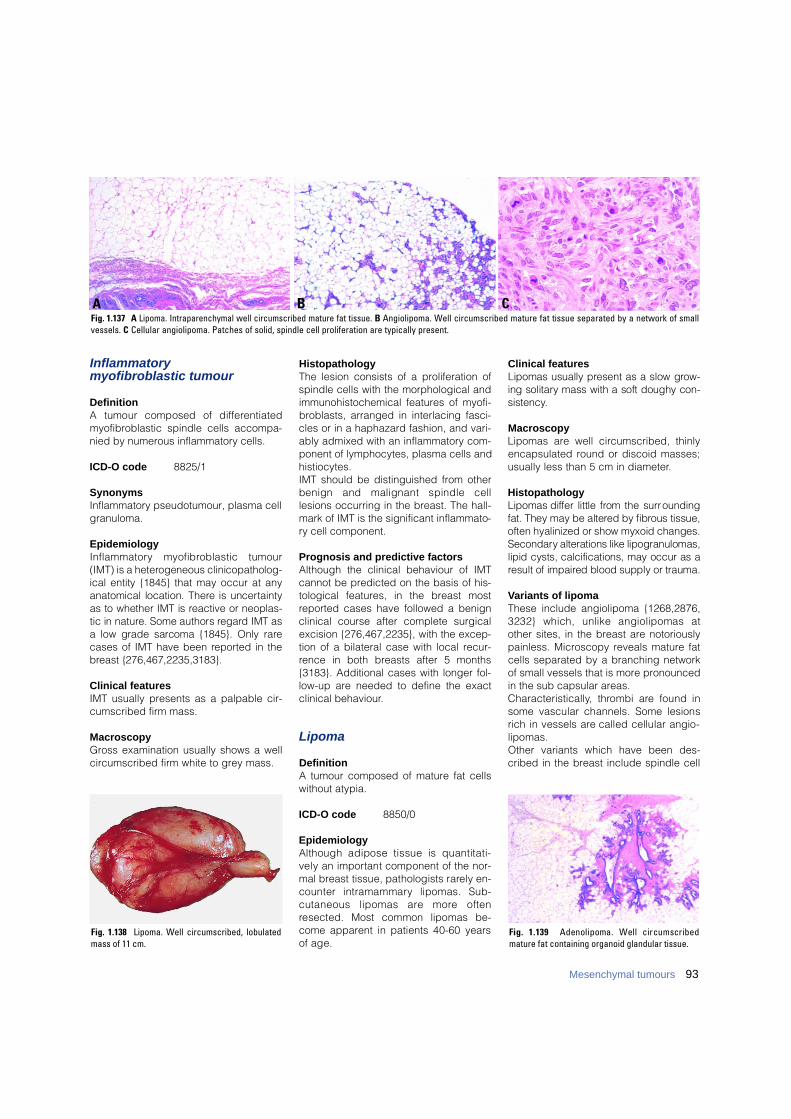
Inflammatory myofibroblastic tumour
DefinitionA tumour composed of diff e re n t i a t e dmyofibroblastic spindle cells accompa-nied by numerous inflammatory cells.
ICD-O code 8825/1
SynonymsInflammatory pseudotumour, plasma cellgranuloma.
EpidemiologyI n f l a m m a t o ry myofibroblastic tumour(IMT) is a heterogeneous clinicopatholog-ical entity {1845} that may occur at anyanatomical location. There is uncert a i n t yas to whether IMT is reactive or neoplas-tic in nature. Some authors re g a rd IMT asa low grade sarcoma {1845}. Only rarecases of IMT have been re p o rted in theb reast {276,467,2235,3183}.
Clinical featuresIMT usually presents as a palpable cir-cumscribed firm mass.
MacroscopyGross examination usually shows a wellcircumscribed firm white to grey mass.
HistopathologyThe lesion consists of a proliferation ofspindle cells with the morphological andimmunohistochemical features of myofi-broblasts, arranged in interlacing fasci-cles or in a haphazard fashion, and vari-ably admixed with an inflammatory com-ponent of lymphocytes, plasma cells andhistiocytes. IMT should be distinguished from otherbenign and malignant spindle celllesions occurring in the breast. The hall-mark of IMT is the significant inflammato-ry cell component.
Prognosis and predictive factorsAlthough the clinical behaviour of IMTcannot be predicted on the basis of his-tological features, in the breast mostreported cases have followed a benignclinical course after complete surgicalexcision {276,467,2235}, with the excep-tion of a bilateral case with local recur-rence in both breasts after 5 months{3183}. Additional cases with longer fol-low-up are needed to define the exactclinical behaviour.
Lipoma
DefinitionA tumour composed of mature fat cellswithout atypia.
ICD-O code 8850/0
EpidemiologyAlthough adipose tissue is quantitati-vely an important component of the nor-mal breast tissue, pathologists rarely en-counter intramammary lipomas. Sub-cutaneous lipomas are more oftenresected. Most common lipomas be-come apparent in patients 40-60 yearsof age.
Clinical featuresLipomas usually present as a slow gro w-ing solitary mass with a soft doughy con-s i s t e n c y.
MacroscopyLipomas are well circumscribed, thinlyencapsulated round or discoid masses;usually less than 5 cm in diameter.
HistopathologyLipomas differ little from the surro u n d i n gfat. They may be altered by fibrous tissue,often hyalinized or show myxoid changes.S e c o n d a ry alterations like lipogranulomas,lipid cysts, calcifications, may occur as aresult of impaired blood supply or trauma.
Variants of lipomaThese include angiolipoma {1268,2876,3232} which, unlike angiolipomas atother sites, in the breast are notoriouslypainless. Microscopy reveals mature fatcells separated by a branching networkof small vessels that is more pronouncedin the sub capsular areas. C h a r a c t e r i s t i c a l l y, thrombi are found insome vascular channels. Some lesionsrich in vessels are called cellular angio-lipomas. Other variants which have been des-cribed in the breast include spindle cell
B CFig. 1.137 A Lipoma. Intraparenchymal well circumscribed mature fat tissue. B Angiolipoma. Well circumscribed mature fat tissue separated by a network of smallvessels. C Cellular angiolipoma. Patches of solid, spindle cell proliferation are typically present.
A
Fig. 1.139 Adenolipoma. Well circumscribedmature fat containing organoid glandular tissue.
Fig. 1.138 Lipoma. Well circumscribed, lobulatedmass of 11 cm.
93Mesenchymal tumours
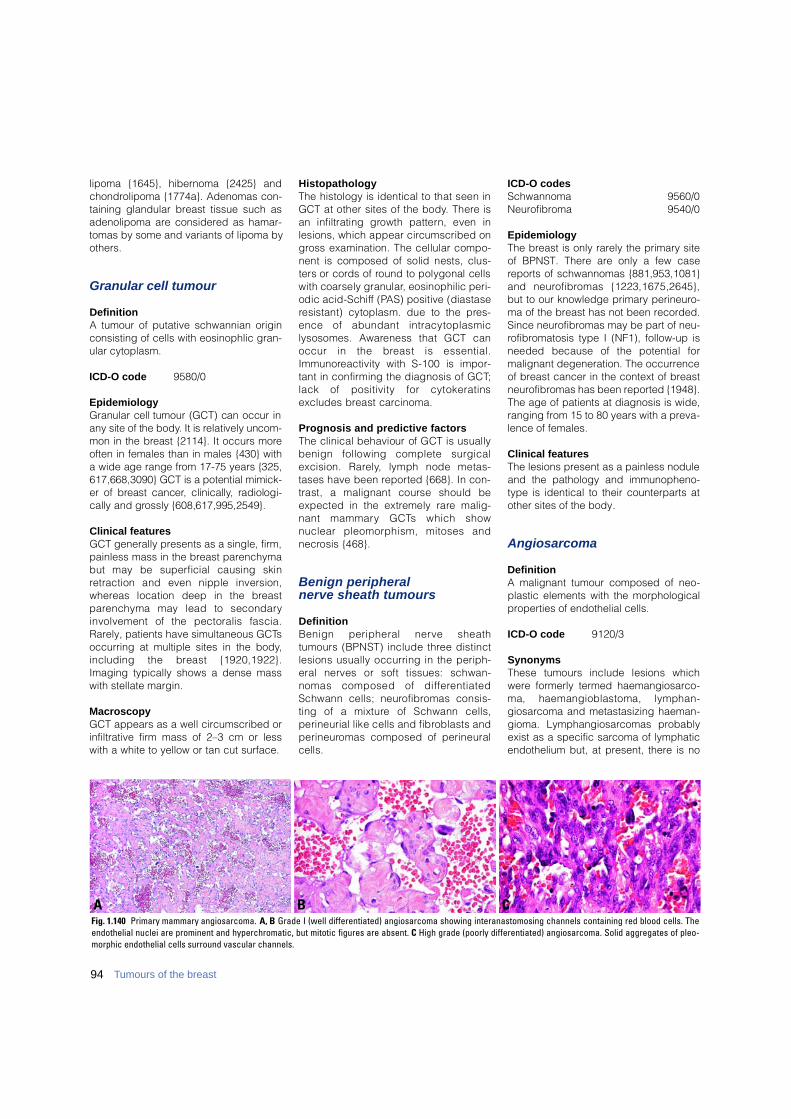
lipoma {1645}, hibernoma {2425} andchondrolipoma {1774a}. Adenomas con-taining glandular breast tissue such asadenolipoma are considered as hamar-tomas by some and variants of lipoma byothers.
Granular cell tumour
DefinitionA tumour of putative schwannian originconsisting of cells with eosinophlic gran-ular cytoplasm.
ICD-O code 9580/0
EpidemiologyGranular cell tumour (GCT) can occur inany site of the body. It is relatively uncom-mon in the breast {2114}. It occurs moreoften in females than in males {430} witha wide age range from 17-75 years {325,617,668,3090} GCT is a potential mimick-er of breast cancer, clinically, radiologi-cally and grossly {608,617,995,2549}.
Clinical featuresGCT generally presents as a single, firm,painless mass in the breast parenchymabut may be superficial causing skinretraction and even nipple inversion,w h e reas location deep in the bre a s tp a renchyma may lead to secondaryinvolvement of the pectoralis fascia.Rarely, patients have simultaneous GCTsoccurring at multiple sites in the body,including the breast {1920,1922}.Imaging typically shows a dense masswith stellate margin.
MacroscopyGCT appears as a well circumscribed orinfiltrative firm mass of 2–3 cm or lesswith a white to yellow or tan cut surface.
H i s t o p a t h o l o g yThe histology is identical to that seen inGCT at other sites of the body. There isan infiltrating growth pattern, even inlesions, which appear circumscribed ong ross examination. The cellular compo-nent is composed of solid nests, clus-ters or cords of round to polygonal cellswith coarsely granular, eosinophilic peri-odic acid-Schiff (PAS) positive (diastaseresistant) cytoplasm. due to the pre s-ence of abundant intracytoplasmic lysosomes. Aw a reness that GCT canoccur in the breast is essential.I m m u n o reactivity with S-100 is impor-tant in confirming the diagnosis of GCT;lack of positivity for cytokeratinsexcludes breast carc i n o m a .
Prognosis and predictive factorsThe clinical behaviour of GCT is usuallybenign following complete surgicalexcision. Rare l y, lymph node metas-tases have been re p o rted {668}. In con-trast, a malignant course should beexpected in the extremely rare malig-nant mammary GCTs which shownuclear pleomorphism, mitoses andn e c rosis {468}.
Benign peripheral nerve sheath tumours
D e f i n i t i o nBenign peripheral nerve sheathtumours (BPNST) include three distinctlesions usually occurring in the periph-eral nerves or soft tissues: schwan-nomas composed of diff e re n t i a t e dSchwann cells; neuro f i b romas consis-ting of a mixture of Schwann cells, perineurial like cells and fibroblasts andp e r i n e u romas composed of perineuralcells.
ICD-O codes Schwannoma 9560/0Neurofibroma 9540/0
EpidemiologyThe breast is only rarely the primary siteof BPNST. There are only a few casereports of schwannomas {881,953,1081}and neuro f i b romas {1223,1675,2645},but to our knowledge primary perineuro-ma of the breast has not been recorded.Since neurofibromas may be part of neu-rofibromatosis type I (NF1), follow-up isneeded because of the potential formalignant degeneration. The occurrenceof breast cancer in the context of breastneurofibromas has been reported {1948}.The age of patients at diagnosis is wide,ranging from 15 to 80 years with a preva-lence of females.
Clinical featuresThe lesions present as a painless noduleand the pathology and immunopheno-type is identical to their counterparts atother sites of the body.
Angiosarcoma
DefinitionA malignant tumour composed of neo-plastic elements with the morphologicalproperties of endothelial cells.
ICD-O code 9120/3
SynonymsThese tumours include lesions whichwere formerly termed haemangiosarco-ma, haemangioblastoma, lymphan-giosarcoma and metastasizing haeman-gioma. Lymphangiosarcomas probablyexist as a specific sarcoma of lymphaticendothelium but, at present, there is no
94 Tumours of the breast
B CAFig. 1.140 Primary mammary angiosarcoma. A, B Grade I (well differentiated) angiosarcoma showing interanastomosing channels containing red blood cells. Theendothelial nuclei are prominent and hyperchromatic, but mitotic figures are absent. C High grade (poorly differentiated) angiosarcoma. Solid aggregates of pleo-morphic endothelial cells surround vascular channels.

reliable criterion upon which to make ahistological distinction between tumoursderived from endothelia of blood andlymphatic vessels.
EpidemiologyMammary angiosarcoma can be subdi-vided into 1) Primary (de novo) forms inthe breast parenchyma; 2) Secondary inthe skin and soft tissues of the arm fol-lowing ipsilateral radical mastectomyand subsequent lymphoedema - theS t e w a rt Treves (S-T) syndrome; 3)Secondary in the skin and chest wall fol-lowing radical mastectomy and local
radiotherapy; 4) Secondary in the skin orb reast parenchyma or both followingconservation treatment and radiotherapy.Angiosarcomas, as with other sarcomasof the breast, are rare and their incidenceis about 0.05% of all primary malignan-cies of the organ {2876}. While the inci-dence of primary breast angiosarcomashas remained constant, the incidence ofsecondary forms has changed. S-T syn-d rome has dramatically declined inrecent years in institutions in which moreconservation surgical treatments havebeen adopted, while angiosarcomas ofthe breast developing after conservings u r g e ry with supplementary radiationtherapy have been diagnosed since thelate 1980s {570}.
Primary (de novo) angiosarcoma ofbreast parenchymaIn patients with primary angiosarcoma,the age ranges from 17 to 70 years(median 38 years) with no prevalence oflaterality {2436}. The tumours are deeplylocated in the breast tissue {2784}.Approximately 12% of patients presentwith diffuse breast enlargement {2876}.When the tumour involves the overlyingskin a bluish-red discoloration mayensue. Imaging is of little help {1656,2564,3118}.
MacroscopyAngiosarcomas vary in size from 1 to 20cm, averaging 5 cm {2425}, have aspongy appearance and a rim of vascu-lar engorgement which corresponds to azone of well differentiated tumour. Poorlydifferentiated tumours appear as an illdefined indurated fibrous lesion similar tothat of any other poorly differentiated sar-coma. Angiosarcomas must be sampledextensively to look for poorly differentiat-ed areas that on occasion constitute theminority of a tumour.
HistopathologyTwo systems have been used to gradeangiosarcomas of the breast {717,1847}.Although very similar, the one proposedby Donnell et al. {717} has gained wideimpact as it was tested in a large numberof patients with adequate follow up{2436}.Grade I (well differentiated) angiosarco-mas consist of interanastomosing vascu-lar channels that dissect the interlobularstroma. The neoplastic vessels have verywide lumina filled with red blood cells.The nuclei of the endothelium lining theneoplastic vessels are prominent andhyperchromatic. Care must be taken todifferentiate grade I angiosarcoma frombenign vascular tumours.Grade III (poorly differentiated) angiosar-comas are easy to diagnose as inter-anastomosing vascular channels arei n t e rmingled with solid endothelial orspindle cell areas that show necrotic fociand numerous mitoses. In a grade IIIangiosarcoma, more than 50% of thetotal neoplastic area is composed ofsolid and spindle cell components with-out evident vascular channels {2425}.A tumour qualifies as grade II (intermedi-ately differentiated) angiosarcoma whenat least 75% of the bulk of the tumour isformed by the well differentiated patternseen in grade I, but in addition there aresolid cellular foci scattered throughoutthe tumour.
Clinical featureThe average age of patients with grade Iangiosarcomas is 43 years while 34 and29 years are the respective figures forgrade II and III angiosarcomas {717}.
ImmunoprofileFactor VIII, CD34 and CD31 are the mostwidely used antibodies that characterizeendothelial differentiation. While present
95Mesenchymal tumours
Fig. 1.141 Angiosarcoma after breast conservingtreatment. The spongy, haemorrhagic mass con-tains occasional solid areas. In this case, the neo-plasm involves the breast parenchyma as well asthe skin.
Fig. 1.142 Angiosarcoma after breast conserving treatment. A As in the majority of cases, this is a poorly dif-ferentiated angiosarcoma in which vascular channels are hard to see. B Immunostaining for the endothelialmarker CD31 clearly demonstrates the solid areas of endothelial cells with occasional vascular channels.
BA

in all grade I and most grade II angiosar-comas these markers may be lost inm o re poorly diff e rentiated tumours orareas of tumour.
Prognosis and predictive factorsIf well diff e rentiated angiosarc o m a s(Grade I) were excluded, this bre a s ttumour is usually lethal {457}. Grading systems highlight the relativebenignity of well differentiated angiosar-comas. The survival probability for gradeI tumours was estimated as 91% at 5years and 81% at 10 years. For grade IIItumours the survival probability was 31%at 2 years and 14% at 5 and 10 years.Grade II lesions had a survival of 68% at5 and 10 years. Recurrence free survivalat 5 years was 76% for grade I, 70% forgrade II and 15% for grade III angiosar-comas {2436}. Metastases are mainly tolungs, skin bone and liver. Very rarelyaxillary lymph nodes show metastases atpresentation {457}. The grade can varybetween the primary tumour and itsmetastases {2876}. Radio andchemotherapy are ineffective.
Angiosarcoma of the skin of the arm after radical mastectomy followed by lymphoedema
Stewart and Treves in 1949 gave a luciddescription of a condition subsequentlynamed S-T syndrome {2793}. Theyreported six patients who had: 1) under-gone mastectomy for breast cancerincluding axillary dissection; 2) devel-oped an “immediate postmastectomyoedema” in the ipsilateral arm; 3)received irradiation to the breast areatogether with the axilla; 4) developedoedema which started in the arm andextended to the forearm and finally thedorsum of the hands and digits. The patients ranged in age from 37-60years, with a mean age of 64 years {3149}.The angiosarcomatous nature of S-Ts y n d rome has been conclusively pro v e dby ultrastructure and immunohistochem-i s t ry in most of the cases studied {1049,1462,1862,2690}. The oedema is preceded by radical mas-tectomy for breast carcinoma includingaxillary dissection {275} and developswithin 12 months. Nearly 65% of patientsalso had irradiation of the chest wall andaxilla {2425}. The interval to tumour ap-pearance varies from 1-49 years {2425},but most become evident about 10 years
following mastectomy {2752,3149}. S-T syndrome is a lethal disease with amedian survival of 19 months {3149}.Lungs are the most frequent site ofmetastasis.
Post-radiotherapy angiosarcoma
A n g i o s a rcoma can manifest itself afterradiotherapy in two separate settings.1) In the chest wall when radiotherapyhas been administered after mastecto-my for invasive breast carcinoma with alatency time ranging from 30 to 156months (mean 70 months). The age ism o re advanced than that of de novoa n g i o s a rcoma ranging from 61 to 78years {2223}. In these cases the neo-plastic endothelial proliferation is neces-sarily confined to the skin {392}.2) In the breast after conservation tre a t-ment for breast carcinoma. Fifty twocases had been re p o rted as ofDecember 1997. The first case wasdescribed in 1987 {1764}. This type ofa n g i o s a rcoma involves only the skin inm o re than half the cases, while exclusiveinvolvement of breast parenchyma isv e ry rare. Most tumours (81%) are multi-focal and a large majority of patients har-bour grade II to III angiosarc o m a s .Radiotherapy and chemotherapy arei n e ffective {2876}.
Liposarcoma
DefinitionA variably cellular or myxoid tumour con-taining at least a few lipoblasts.
ICD-O code 8850/3
EpidemiologyP r i m a ry liposarcoma should be distin-guished from liposarcomatous diff e-rentiation in a phyllodes tumour. It occursp redominantly in women ranging in agef rom 19-76 years (median, 47 years) {116,138}. The tumour only rarely occurs in themale breast {3027}. Liposarcoma follow-ing radiation therapy for breast carc i n o m ahas been re p o rt e d .
Clinical featuresPatients present most often with a slowlyenlarging, painful mass. In general, skinchanges and axillary node enlargementa re absent. Rarely the tumour is bilateral{ 3 0 2 7 } .
MacroscopyL i p o s a rcomas are often well circ u m-scribed or encapsulated, about one-thirdhave infiltrative margin. With a mediansize of 8 cm, liposarcomas may becomeenormous exceeding 15 cm {116,138}.Necrosis and haemorrhage may be pres-ent on the cut surface of larger tumours.
HistopathologyThe histopathology and immunopheno-type is identical to that of liposarcoma atother sites. The presence of lipoblastsestablishes the diagnosis. Practicallye v e ry variant of soft tissue liposarc o m ahas been re p o rted in the breast, includ-ing the pleomorphic, dediff e rentiated andmyxoid variants. Despite the well delin-eated gross appearance, many mamma-ry liposarcomas have at least partial infil-trative margins on histological examina-tion. Atypia is often present at least focal-l y. The well diff e rentiated and myxoidvariants have a delicate arborizing vas-cular network and few lipoblasts. Thesemay assume a signet-ring appearance inthe myxoid variant. The pleomorphic vari-ant is composed of highly pleomorphiccells and bears significant re s e m b l a n c eto malignant fibrous histiocytoma; thep resence of lipoblasts identifies thelesion as a liposarcoma. Mitotic figure sa re readily identifiable in this variant.
Differential diagnosisVacuolated cells in a variety of lesionsmay be confused with lipoblasts. Ty p i c a llipoblasts have scalloped irregular nucleiwith sharply defined vacuoles that con-tain lipid rather than glycogen or mucin.Clear nuclear pseudo-inclusions are acharacteristic of the bizarre large cells inatypical lipomatous tumours and helpdistinguish these atypical cells from truelipoblasts that are diagnostic of a liposar-c o m a .
96 Tumours of the breast
Fig. 1.143 Liposarcoma. Note the highly pleomor-phic nuclei and multiple lipoblasts.
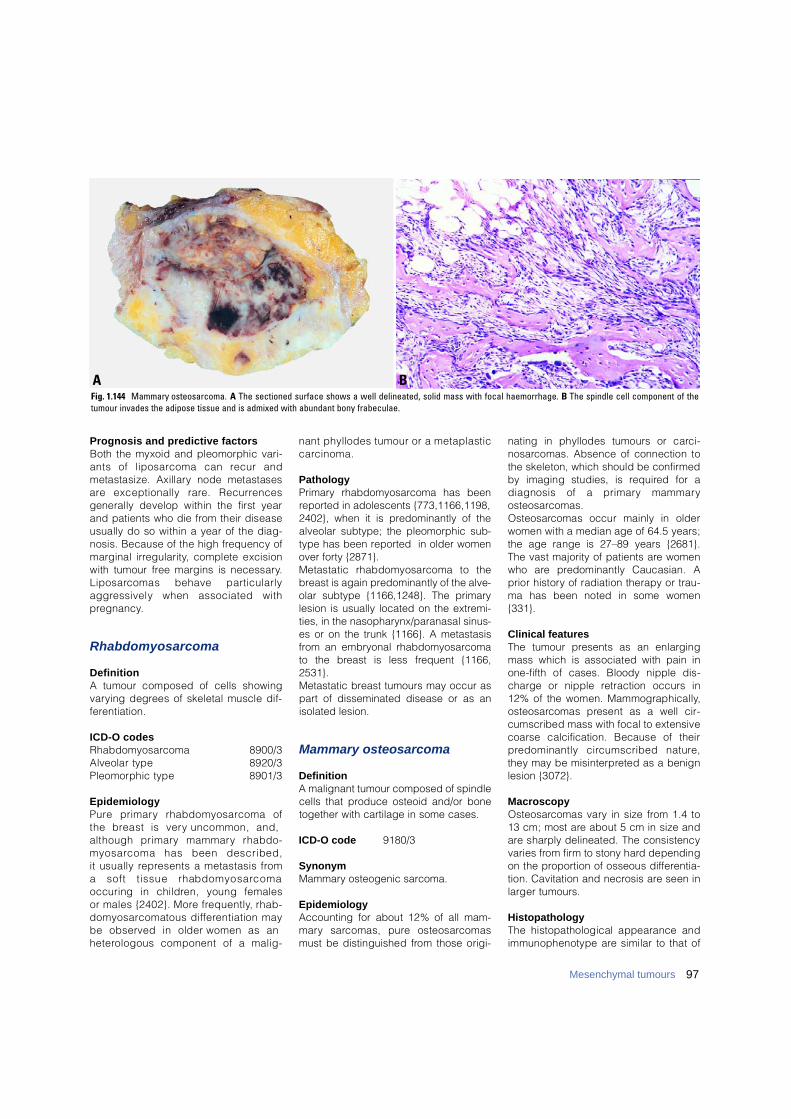
Prognosis and predictive factorsBoth the myxoid and pleomorphic vari-ants of liposarcoma can recur andmetastasize. Axillary node metastasesa re exceptionally rare. Recurre n c e sgenerally develop within the first yearand patients who die from their diseaseusually do so within a year of the diag-nosis. Because of the high frequency ofmarginal irre g u l a r i t y, complete excisionwith tumour free margins is necessary.L i p o s a rcomas behave part i c u l a r l ya g g ressively when associated withp re g n a n c y.
R h a b d o m y o s a r c o m a
D e f i n i t i o nA tumour composed of cells showingv a rying degrees of skeletal muscle dif-f e re n t i a t i o n .
ICD-O codes R h a b d o m y o s a rc o m a 8 9 0 0 / 3Alveolar type 8 9 2 0 / 3Pleomorphic type 8 9 0 1 / 3
E p i d e m i o l o g yP u re primary rhabdomyosarcoma of the breast is very uncommon, and, although primary mammary rhabdo-m y o s a rcoma has been described, it usually re p resents a metastasis from a soft tissue rhabdomyosarcoma occuring in children, young females or males {2402}. More fre q u e n t l y, rhab-d o m y o s a rcomatous diff e rentiation maybe observed in older women as an h e t e rologous component of a malig-
nant phyllodes tumour or a metaplasticc a rc i n o m a .
PathologyPrimary rhabdomyosarcoma has beenreported in adolescents {773,1166,1198,2402}, when it is predominantly of thealveolar subtype; the pleomorphic sub-type has been reported in older womenover forty {2871}. Metastatic rhabdomyosarcoma to thebreast is again predominantly of the alve-olar subtype {1166,1248}. The primarylesion is usually located on the extremi-ties, in the nasopharynx/paranasal sinus-es or on the trunk {1166}. A metastasisfrom an embryonal rhabdomyosarcomato the breast is less frequent {1166,2531}.Metastatic breast tumours may occur aspart of disseminated disease or as anisolated lesion.
Mammary osteosarcoma
DefinitionA malignant tumour composed of spindlecells that produce osteoid and/or bonetogether with cartilage in some cases.
ICD-O code 9180/3
SynonymMammary osteogenic sarcoma.
EpidemiologyAccounting for about 12% of all mam-m a ry sarcomas, pure osteosarc o m a smust be distinguished from those origi-
nating in phyllodes tumours or carc i-n o s a rcomas. Absence of connection tothe skeleton, which should be confirm e dby imaging studies, is re q u i red for adiagnosis of a primary mammaryo s t e o s a rc o m a s .O s t e o s a rcomas occur mainly in olderwomen with a median age of 64.5 years;the age range is 27–89 years {2681}.The vast majority of patients are womenwho are predominantly Caucasian. Aprior history of radiation therapy or trau-ma has been noted in some women{ 3 3 1 } .
Clinical featuresThe tumour presents as an enlargingmass which is associated with pain inone-fifth of cases. Bloody nipple dis-charge or nipple retraction occurs in12% of the women. Mammographically,o s t e o s a rcomas present as a well cir-cumscribed mass with focal to extensivecoarse calcification. Because of theirp redominantly circumscribed nature ,they may be misinterpreted as a benignlesion {3072}.
M a c r o s c o p yO s t e o s a rcomas vary in size from 1.4 to13 cm; most are about 5 cm in size anda re sharply delineated. The consistencyvaries from firm to stony hard dependingon the pro p o rtion of osseous diff e re n t i a-tion. Cavitation and necrosis are seen inlarger tumours.
HistopathologyThe histopathological appearance andimmunophenotype are similar to that of
97Mesenchymal tumours
BAFig. 1.144 Mammary osteosarcoma. A The sectioned surface shows a well delineated, solid mass with focal haemorrhage. B The spindle cell component of thetumour invades the adipose tissue and is admixed with abundant bony frabeculae.

98 Tumours of the breast
extraosseous osteosarcoma at othersites of the body. Despite the pre d o m i-nantly circumscribed margins, charac-t e r i s t i c a l l y, at least focal infiltration isp resent. The tumour is composed of aspindle to oval cell population with vari-able amounts of osteoid or osseous tis-sue; cartilage is present in over a thirdof the cases {2681} but no other diff e r-entiated tissues. The appearance of the tumours variesdepending on the cellular composition( f i b roblastic, osteoblastic, osteoclastic)as well as the type and amount of matrix(osteoid, osseous, chondroid). The osteoclastic giant cells are immu-n o reactive with the macrophage markerCD68 (clone KP1) while the spindlecells fail to immunoreact with eithere s t rogen receptor (ER) or pro g e s t e ro n ereceptor (PR) or epithelial markers.
Prognosis and predictive factors M a m m a ry osteosarcomas are highlya g g ressive lesions with an overall five-year survival of 38% {2681}. Re-c u r rences develop in over two-thirds ofthe patients treated by local excisionand 11% of those treated by mastecto-m y. Metastases to the lungs andabsence of axillary node involvement aretypical of osteosarcomas. Many of thepatients who develop metastases die ofthe disease within 2 years of initial diag-nosis {2681}.F i b roblastic osteosarcomas are associ-ated with a better survival compared tothe osteoblastic or osteoclastic variants.Large tumour size at pre s e n t a t i o n ,p rominent infiltrating margins and necro-sis are associated with more aggre s s i v eb e h a v i o u r.
Leiomyoma and leiomyosarcoma
D e f i n i t i o nBenign and malignant tumours com-posed of intersecting bundles of smoothmuscle which is mature in benign lesions.Malignant lesions are larger in size andshow more mitotic activity in the neoplas-tic cells.
ICD-O codes L e i o m y o m a 8 8 9 0 / 0L e i o m y o s a rc o m a 8 8 9 0 / 3
E p i d e m i o l o g yBenign and malignant smooth muscletumours of the breast are uncommon andre p resent less than 1% of breast neo-plasms. The majority of leiomyomas origi-nate from the are o l a r-nipple complex anda minority occur within the breast pro p e r{1981}. Leiomyosarcomas arise mainlywithin the breast {821}. The age at presentation of leiomyomasand leiomyosarcomas overlaps, extend-ing from the fourth to the seventhdecades. However, cases of both havebeen re p o rted in adolescents {2000} andpatients over eighty years old {821}.
Clinical featuresBoth leiomyomas and leiomyosarc o m a susually present as a slowly growing pal-pable mobile mass that may be painful.Incidental asymptomatic leiomyomas dis-c o v e red in mastectomy specimens havebeen re p o rted {1981}.
M a c r o s c o p yThese lesions appear as well circ u m-scribed firm nodules with a whorled or
lobulated cut surface. Their size rangesf rom 0.5 to 15 cm {770,2000}.
H i s t o p a t h o l o g yThe histopathology and immunopheno-type are identical to that seen in smoothmuscle tumours elsewhere in the body.These neoplasms may be well circ u m-scribed {1981} or show irregular infiltra-tive borders {2000}. Both are composedof spindle cells arranged in interlacingfascicles. In leiomyomas, these cells have elongat-ed cigar-shaped nuclei and eosinophiliccytoplasm without evidence of atypia.Mitoses are sparse and typically fewerthan 3 per 10 high power fields {458}. Inl e i o m y o s a rcomas, nuclear atypia andmitotic activity are more prominent {821}.Tumour necrosis may also be observed.Infiltrating margins may not be evident insome leiomyosarc o m a s .
D i ff e rential diagnosisA diagnosis of a smooth muscle tumour ofthe breast should be considered only afterexcluding other breast lesions that mayshow benign or malignant smooth muscled i ff e rentiation i.e. fibroadenoma, muscularh a m a rtoma and sclerosing adenosisshould be distinguished from leiomyoma;spindle cell myoepithelioma and sarc o-matoid carcinoma from leiomyosarc o m a .
Prognosis and predictive factorsLeiomyomas are best treated by com-plete excision whereas, wide excisionwith tumour- f ree margins is re c o m m e n d-ed for leiomyosarcomas. Late local re c u r-rence and metastatasis have been re p o r-ted in cases of mammary leiomyosarc o-ma {458,2014}.
BAFig. 1.145 Leiomyoma. A The well circumscribed margin (left) is apparent. B The bland smooth muscle cells proliferate in whorls and fascicles.
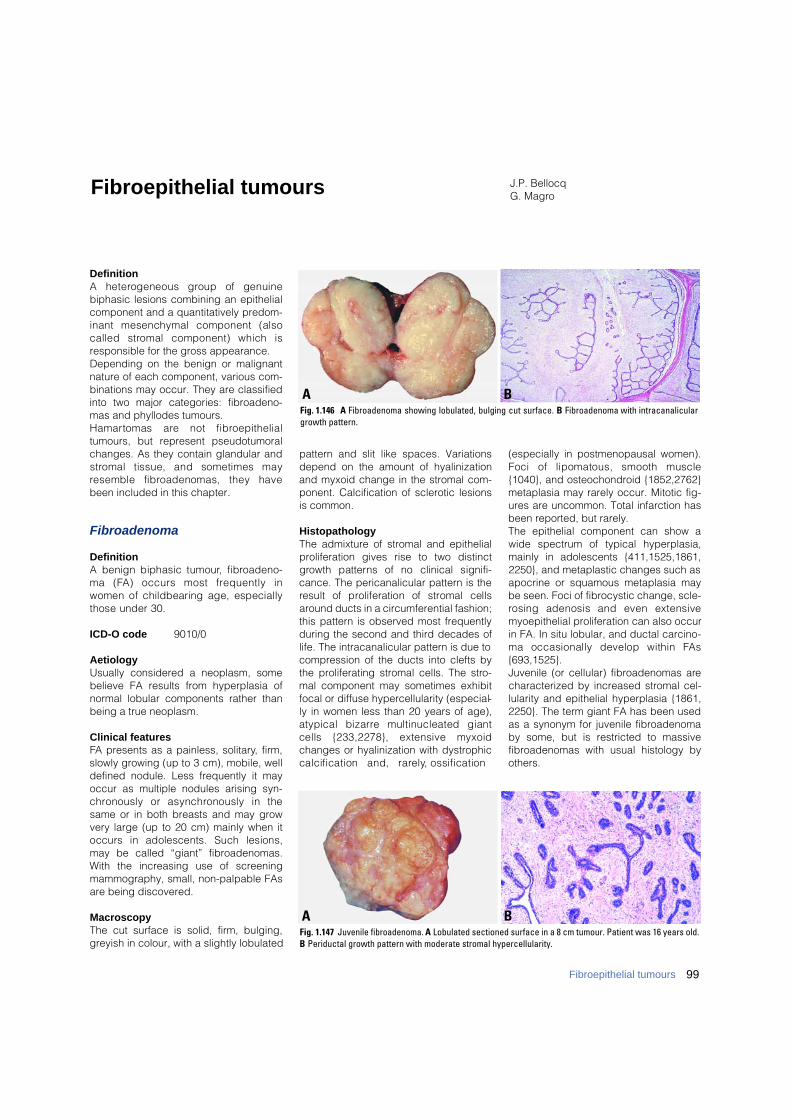
DefinitionA heterogeneous group of genuinebiphasic lesions combining an epithelialcomponent and a quantitatively predom-inant mesenchymal component (alsocalled stromal component) which isresponsible for the gross appearance.Depending on the benign or malignantnature of each component, various com-binations may occur. They are classifiedinto two major categories: fibroadeno-mas and phyllodes tumours. H a m a rtomas are not fibro e p i t h e l i a ltumours, but represent pseudotumoralchanges. As they contain glandular ands t romal tissue, and sometimes mayresemble fibroadenomas, they havebeen included in this chapter.
Fibroadenoma
DefinitionA benign biphasic tumour, fibro a d e n o-ma (FA) occurs most frequently inwomen of childbearing age, especiallythose under 30.
ICD-O code 9010/0
AetiologyUsually considered a neoplasm, somebelieve FA results from hyperplasia ofnormal lobular components rather thanbeing a true neoplasm.
Clinical features FA presents as a painless, solitary, firm,slowly growing (up to 3 cm), mobile, welldefined nodule. Less frequently it mayoccur as multiple nodules arising syn-c h ronously or asynchronously in thesame or in both breasts and may growvery large (up to 20 cm) mainly when itoccurs in adolescents. Such lesions,may be called “giant” fibroadenomas.With the increasing use of screeningmammography, small, non-palpable FAsare being discovered.
MacroscopyThe cut surface is solid, firm, bulging,greyish in colour, with a slightly lobulated
pattern and slit like spaces. Variationsdepend on the amount of hyalinizationand myxoid change in the stromal com-ponent. Calcification of sclerotic lesionsis common.
HistopathologyThe admixture of stromal and epithelialproliferation gives rise to two distinctg rowth patterns of no clinical signifi-cance. The pericanalicular pattern is theresult of proliferation of stromal cellsaround ducts in a circumferential fashion;this pattern is observed most frequentlyduring the second and third decades oflife. The intracanalicular pattern is due tocompression of the ducts into clefts bythe proliferating stromal cells. The stro-mal component may sometimes exhibitfocal or diffuse hypercellularity (especial-ly in women less than 20 years of age),atypical bizarre multinucleated giantcells {233,2278}, extensive myxoidchanges or hyalinization with dystrophiccalcification and, rare l y, ossification
(especially in postmenopausal women).Foci of lipomatous, smooth muscle{1040}, and osteochondroid {1852,2762}metaplasia may rarely occur. Mitotic fig-ures are uncommon. Total infarction hasbeen reported, but rarely.The epithelial component can show awide spectrum of typical hyperplasia,mainly in adolescents {411,1525,1861,2250}, and metaplastic changes such asapocrine or squamous metaplasia maybe seen. Foci of fibrocystic change, scle-rosing adenosis and even extensivemyoepithelial proliferation can also occurin FA. In situ lobular, and ductal carcino-ma occasionally develop within FA s{693,1525}.Juvenile (or cellular) fibroadenomas arecharacterized by increased stromal cel-lularity and epithelial hyperplasia {1861,2250}. The term giant FA has been usedas a synonym for juvenile fibroadenomaby some, but is restricted to massivefibroadenomas with usual histology byothers.
J.P. BellocqG. Magro
BAFig. 1.146 A Fibroadenoma showing lobulated, bulging cut surface. B Fibroadenoma with intracanaliculargrowth pattern.
BAFig. 1.147 Juvenile fibroadenoma. A Lobulated sectioned surface in a 8 cm tumour. Patient was 16 years old.B Periductal growth pattern with moderate stromal hypercellularity.
Fibroepithelial tumours
99Fibroepithelial tumours
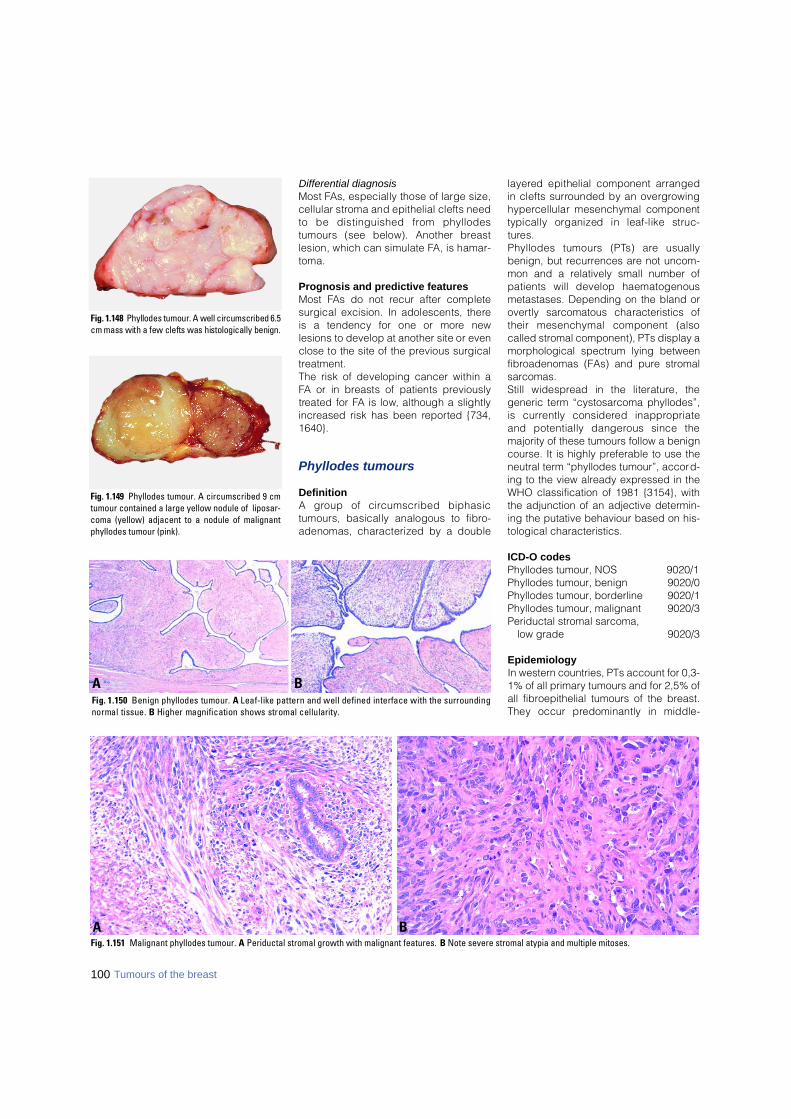
100 Tumours of the breast
Differential diagnosisMost FAs, especially those of large size,cellular stroma and epithelial clefts needto be distinguished from phyllodestumours (see below). Another bre a s tlesion, which can simulate FA, is hamar-toma.
Prognosis and predictive featuresMost FAs do not recur after completesurgical excision. In adolescents, thereis a tendency for one or more newlesions to develop at another site or evenclose to the site of the previous surgicalt re a t m e n t .The risk of developing cancer within aFA or in breasts of patients pre v i o u s l yt reated for FA is low, although a slightlyi n c reased risk has been re p o rted {734,1 6 4 0 } .
Phyllodes tumours
DefinitionA group of circumscribed biphasictumours, basically analogous to fibro-adenomas, characterized by a double
l a y e red epithelial component arranged in clefts surrounded by an overgro w i n gh y p e rcellular mesenchymal componenttypically organized in leaf-like struc-t u res. Phyllodes tumours (PTs) are usuallybenign, but recurrences are not uncom-mon and a relatively small number ofpatients will develop haematogenousmetastases. Depending on the bland oro v e rtly sarcomatous characteristics oftheir mesenchymal component (alsocalled stromal component), PTs display amorphological spectrum lying betweenfibroadenomas (FAs) and pure stromalsarcomas. Still widespread in the literature, thegeneric term “cystosarcoma phyllodes”,is currently considered inappro p r i a t eand potentially dangerous since themajority of these tumours follow a benigncourse. It is highly preferable to use theneutral term “phyllodes tumour”, accord-ing to the view already expressed in theWHO classification of 1981 {3154}, withthe adjunction of an adjective determin-ing the putative behaviour based on his-tological characteristics.
ICD-O codesPhyllodes tumour, NOS 9020/1Phyllodes tumour, benign 9020/0Phyllodes tumour, borderline 9020/1Phyllodes tumour, malignant 9020/3Periductal stromal sarcoma,
low grade 9020/3
EpidemiologyIn western countries, PTs account for 0,3-1% of all primary tumours and for 2,5% ofall fibroepithelial tumours of the breast.They occur predominantly in middle-
Fig. 1.148 Phyllodes tumour. A well circumscribed 6.5cm mass with a few clefts was histologically benign.
Fig. 1.149 Phyllodes tumour. A circumscribed 9 cmtumour contained a large yellow nodule of liposar-coma (yellow) adjacent to a nodule of malignantphyllodes tumour (pink).
BAFig. 1.150 Benign phyllodes tumour. A Leaf-like pattern and well defined interface with the surroundingnormal tissue. B Higher magnification shows stromal cellularity.
BAFig. 1.151 Malignant phyllodes tumour. A Periductal stromal growth with malignant features. B Note severe stromal atypia and multiple mitoses.
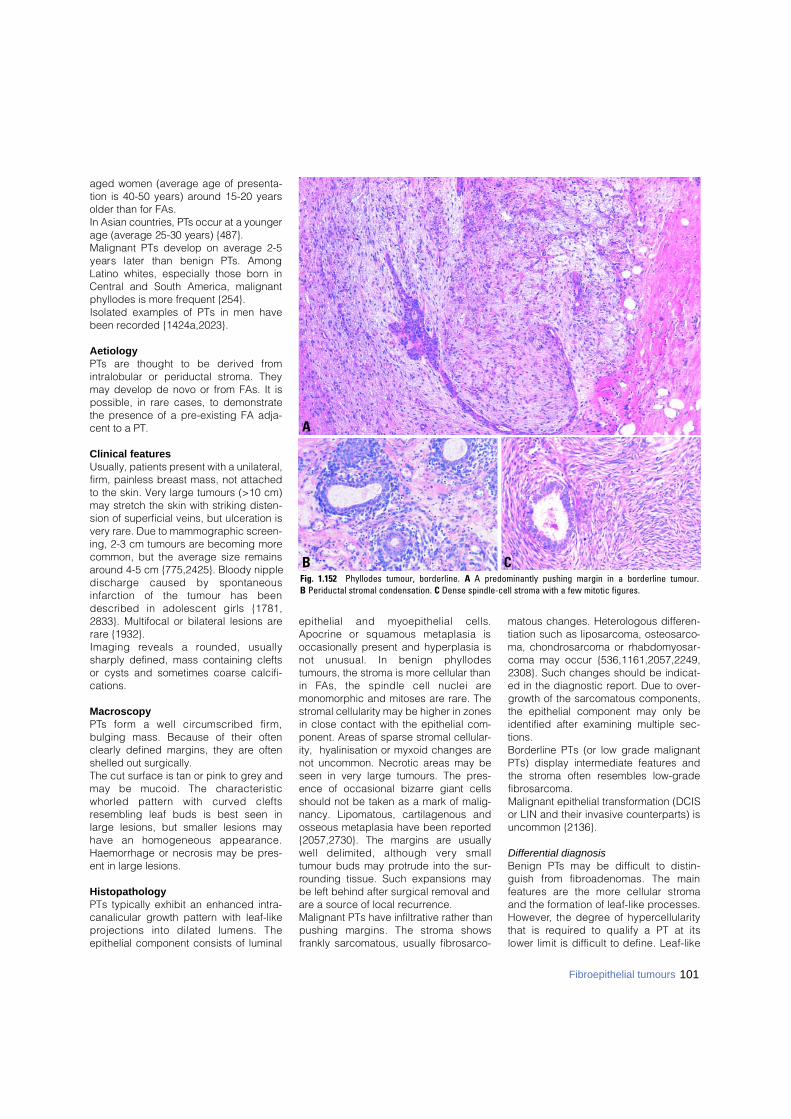
101Fibroepithelial tumours
aged women (average age of presenta-tion is 40-50 years) around 15-20 yearsolder than for FAs. In Asian countries, PTs occur at a youngerage (average 25-30 years) {487}. Malignant PTs develop on average 2-5years later than benign PTs. AmongLatino whites, especially those born inCentral and South America, malignantphyllodes is more frequent {254}. Isolated examples of PTs in men havebeen recorded {1424a,2023}.
AetiologyP Ts are thought to be derived fro mintralobular or periductal stroma. Theymay develop de novo or from FAs. It ispossible, in rare cases, to demonstratethe presence of a pre-existing FA adja-cent to a PT.
Clinical featuresUsually, patients present with a unilateral,firm, painless breast mass, not attachedto the skin. Very large tumours (>10 cm)may stretch the skin with striking disten-sion of superficial veins, but ulceration isvery rare. Due to mammographic screen-ing, 2-3 cm tumours are becoming morecommon, but the average size remainsaround 4-5 cm {775,2425}. Bloody nippledischarge caused by spontaneousi n f a rction of the tumour has beendescribed in adolescent girls {1781,2833}. Multifocal or bilateral lesions arerare {1932}. Imaging reveals a rounded, usuallysharply defined, mass containing cleftsor cysts and sometimes coarse calcifi-cations.
MacroscopyP Ts form a well circumscribed firm ,bulging mass. Because of their oftenclearly defined margins, they are oftenshelled out surgically.The cut surface is tan or pink to grey andmay be mucoid. The characteristicwhorled pattern with curved cleftsresembling leaf buds is best seen inlarge lesions, but smaller lesions mayhave an homogeneous appearance.Haemorrhage or necrosis may be pres-ent in large lesions.
HistopathologyPTs typically exhibit an enhanced intra-canalicular growth pattern with leaf-likep rojections into dilated lumens. Theepithelial component consists of luminal
epithelial and myoepithelial cells.Apocrine or squamous metaplasia isoccasionally present and hyperplasia isnot unusual. In benign phyllodestumours, the stroma is more cellular thanin FAs, the spindle cell nuclei aremonomorphic and mitoses are rare. Thestromal cellularity may be higher in zonesin close contact with the epithelial com-ponent. Areas of sparse stromal cellular-ity, hyalinisation or myxoid changes arenot uncommon. Necrotic areas may beseen in very large tumours. The pres-ence of occasional bizarre giant cellsshould not be taken as a mark of malig-nancy. Lipomatous, cartilagenous andosseous metaplasia have been reported{2057,2730}. The margins are usuallywell delimited, although very smalltumour buds may protrude into the sur-rounding tissue. Such expansions maybe left behind after surgical removal andare a source of local recurrence.Malignant PTs have infiltrative rather thanpushing margins. The stroma showsfrankly sarcomatous, usually fibrosarco-
matous changes. Heterologous differen-tiation such as liposarcoma, osteosarco-ma, chondrosarcoma or rhabdomyosar-coma may occur {536,1161,2057,2249,2308}. Such changes should be indicat-ed in the diagnostic report. Due to over-growth of the sarcomatous components,the epithelial component may only beidentified after examining multiple sec-tions. Borderline PTs (or low grade malignantPTs) display intermediate features andthe stroma often resembles low-gradefibrosarcoma.Malignant epithelial transformation (DCISor LIN and their invasive counterparts) isuncommon {2136}.
Differential diagnosisBenign PTs may be difficult to distin-guish from fibroadenomas. The mainf e a t u res are the more cellular stro m aand the formation of leaf-like pro c e s s e s .H o w e v e r, the degree of hyperc e l l u l a r i t ythat is re q u i red to qualify a PT at itslower limit is difficult to define. Leaf-like
CB
A
Fig. 1.152 Phyllodes tumour, borderline. A A predominantly pushing margin in a borderline tumour. B Periductal stromal condensation. C Dense spindle-cell stroma with a few mitotic figures.
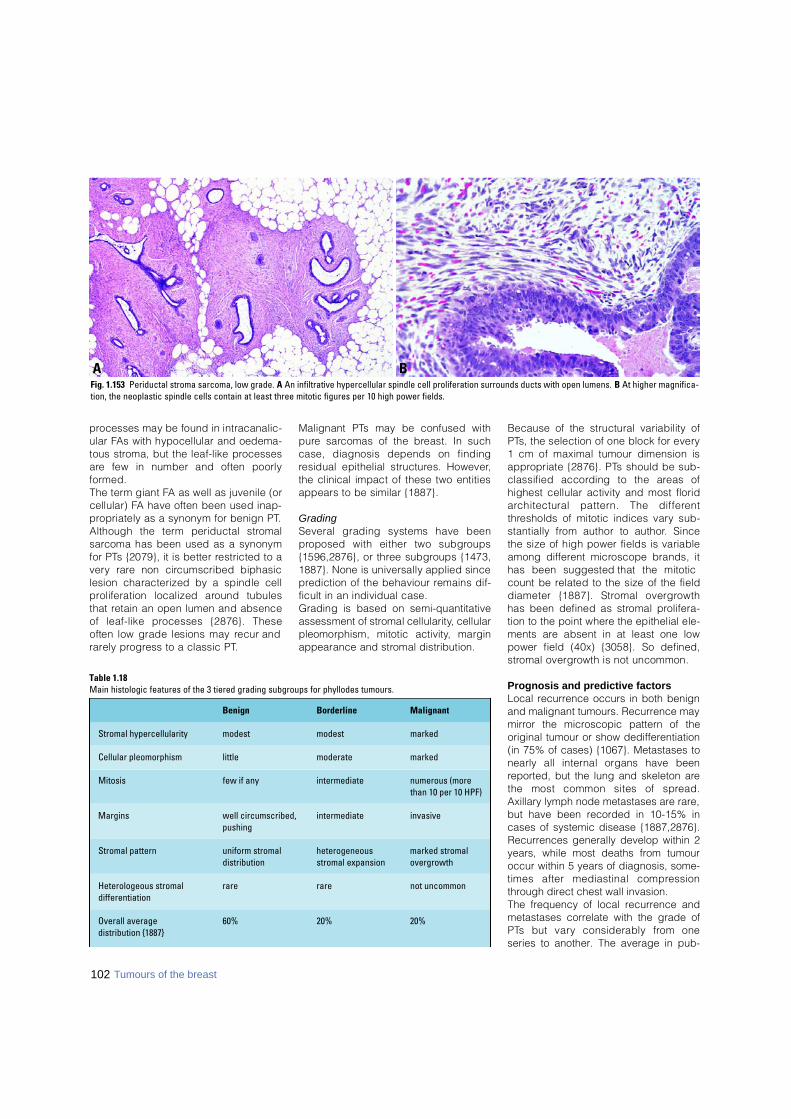
p rocesses may be found in intracanalic-ular FAs with hypocellular and oedema-tous stroma, but the leaf-like pro c e s s e sa re few in number and often poorlyf o rm e d .The term giant FA as well as juvenile (orcellular) FA have often been used inap-p ropriately as a synonym for benign PT. Although the term periductal stro m a ls a rcoma has been used as a synonymfor PTs {2079}, it is better restricted to av e ry rare non circumscribed biphasiclesion characterized by a spindle cellp roliferation localized around tubulesthat retain an open lumen and absenceof leaf-like processes {2876}. Theseoften low grade lesions may recur andr a rely pro g ress to a classic PT.
Malignant PTs may be confused withp u re sarcomas of the breast. In suchcase, diagnosis depends on findingresidual epithelial structures. However,the clinical impact of these two entitiesappears to be similar {1887}.
G r a d i n gSeveral grading systems have beenp roposed with either two subgro u p s{1596,2876}, or three subgroups {1473,1887}. None is universally applied sincep rediction of the behaviour remains dif-ficult in an individual case.Grading is based on semi-quantitativeassessment of stromal cellularity, cellularpleomorphism, mitotic activity, marginappearance and stromal distribution.
Because of the structural variability ofP Ts, the selection of one block for every1 cm of maximal tumour dimension isa p p ropriate {2876}. PTs should be sub-classified according to the areas ofhighest cellular activity and most florida rchitectural pattern. The diff e re n tt h resholds of mitotic indices vary sub-stantially from author to author. Sincethe size of high power fields is variableamong diff e rent microscope brands, ithas been suggested that the mitoticcount be related to the size of the fielddiameter {1887}. Stromal overgro w t hhas been defined as stromal pro l i f e r a-tion to the point where the epithelial ele-ments are absent in at least one lowpower field (40x) {3058}. So defined,s t romal overgrowth is not uncommon.
Prognosis and predictive factorsLocal recurrence occurs in both benignand malignant tumours. Recurrence maymirror the microscopic pattern of theoriginal tumour or show dedifferentiation(in 75% of cases) {1067}. Metastases tonearly all internal organs have beenreported, but the lung and skeleton arethe most common sites of spre a d .Axillary lymph node metastases are rare,but have been recorded in 10-15% incases of systemic disease {1887,2876}.Recurrences generally develop within 2years, while most deaths from tumouroccur within 5 years of diagnosis, some-times after mediastinal compre s s i o nthrough direct chest wall invasion.The frequency of local recurrence andmetastases correlate with the grade ofP Ts but vary considerably from oneseries to another. The average in pub-
Table 1.18Main histologic features of the 3 tiered grading subgroups for phyllodes tumours.
Benign Borderline Malignant
Stromal hypercellularity modest modest marked
Cellular pleomorphism little moderate marked
Mitosis few if any intermediate numerous (more than 10 per 10 HPF)
Margins well circumscribed, intermediate invasive pushing
Stromal pattern uniform stromal heterogeneous marked stromaldistribution stromal expansion overgrowth
Heterologeous stromal rare rare not uncommondifferentiation
Overall average 60% 20% 20%distribution {1887}
102 Tumours of the breast
BAFig. 1.153 Periductal stroma sarcoma, low grade. A An infiltrative hypercellular spindle cell proliferation surrounds ducts with open lumens. B At higher magnifica-tion, the neoplastic spindle cells contain at least three mitotic figures per 10 high power fields.
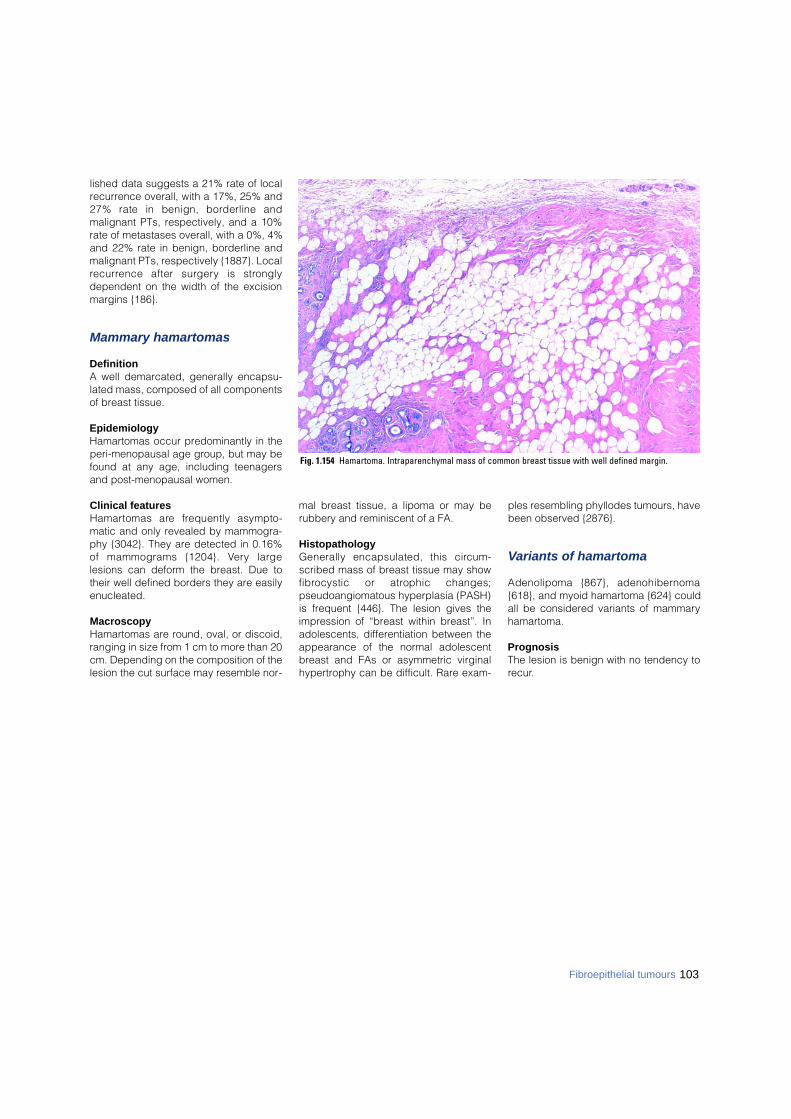
103Fibroepithelial tumours
lished data suggests a 21% rate of localrecurrence overall, with a 17%, 25% and27% rate in benign, borderline andmalignant PTs, respectively, and a 10%rate of metastases overall, with a 0%, 4%and 22% rate in benign, borderline andmalignant PTs, respectively {1887}. Localre c u r rence after surgery is stro n g l ydependent on the width of the excisionmargins {186}.
Mammary hamartomas
DefinitionA well demarcated, generally encapsu-lated mass, composed of all componentsof breast tissue.
EpidemiologyHamartomas occur predominantly in theperi-menopausal age group, but may befound at any age, including teenagersand post-menopausal women.
Clinical featuresH a m a rtomas are frequently asympto-matic and only revealed by mammogra-phy {3042}. They are detected in 0.16%of mammograms {1204}. Ve ry largelesions can deform the breast. Due totheir well defined borders they are easilyenucleated.
MacroscopyHamartomas are round, oval, or discoid,ranging in size from 1 cm to more than 20cm. Depending on the composition of thelesion the cut surface may resemble nor-
mal breast tissue, a lipoma or may berubbery and reminiscent of a FA.
HistopathologyGenerally encapsulated, this circ u m-scribed mass of breast tissue may showf i b rocystic or atrophic changes;pseudoangiomatous hyperplasia (PASH)is frequent {446}. The lesion gives theimpression of “breast within breast”. Inadolescents, differentiation between theappearance of the normal adolescentbreast and FAs or asymmetric virginalhypertrophy can be difficult. Rare exam-
ples resembling phyllodes tumours, havebeen observed {2876}.
Variants of hamartoma
Adenolipoma {867}, adenohibern o m a{618}, and myoid hamartoma {624} couldall be considered variants of mammaryhamartoma.
PrognosisThe lesion is benign with no tendency torecur.
Fig. 1.154 Hamartoma. Intraparenchymal mass of common breast tissue with well defined margin.
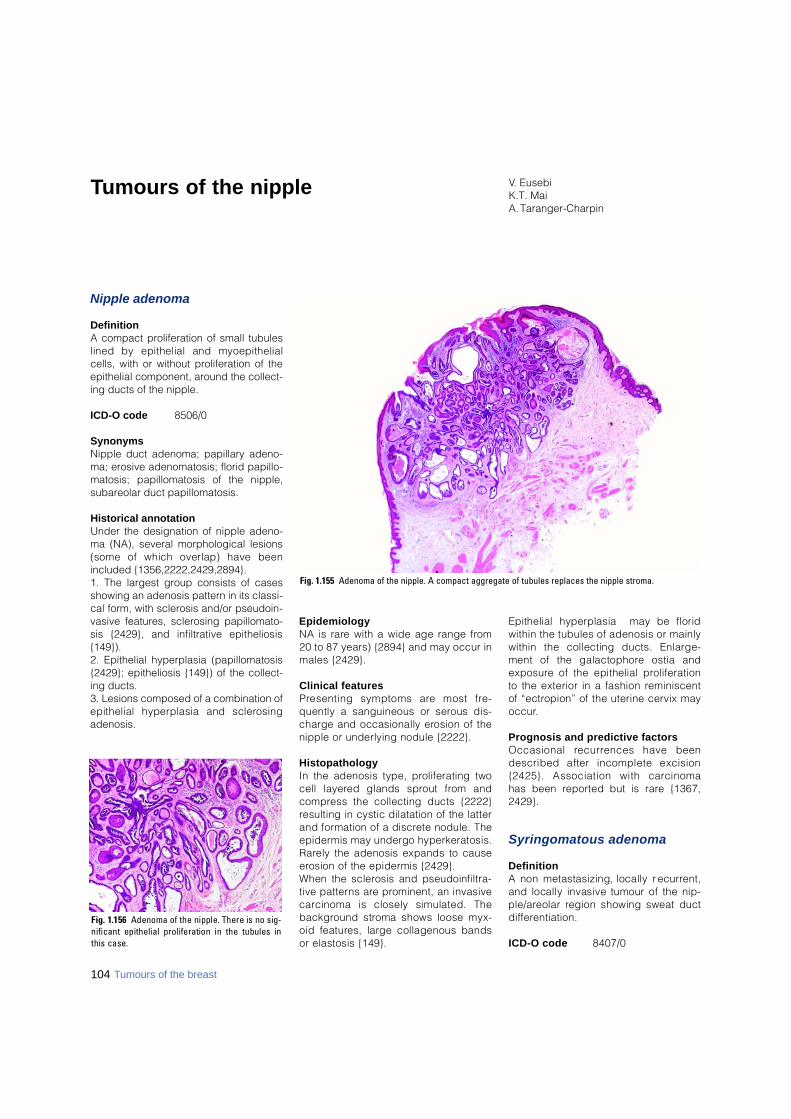
Nipple adenoma
DefinitionA compact proliferation of small tubuleslined by epithelial and myoepithelialcells, with or without proliferation of theepithelial component, around the collect-ing ducts of the nipple.
ICD-O code 8506/0
Synonyms Nipple duct adenoma; papillary adeno-ma; erosive adenomatosis; florid papillo-matosis; papillomatosis of the nipple,subareolar duct papillomatosis.
Historical annotationUnder the designation of nipple adeno-ma (NA), several morphological lesions(some of which overlap) have beenincluded {1356,2222,2429,2894}. 1. The largest group consists of casesshowing an adenosis pattern in its classi-cal form, with sclerosis and/or pseudoin-vasive features, sclerosing papillomato-sis {2429}, and infiltrative epitheliosis{149}). 2. Epithelial hyperplasia (papillomatosis{2429}; epitheliosis {149}) of the collect-ing ducts. 3. Lesions composed of a combination ofepithelial hyperplasia and sclero s i n gadenosis.
E p i d e m i o l o g yNA is rare with a wide age range fro m20 to 87 years) {2894} and may occur inmales {2429}.
Clinical featuresP resenting symptoms are most fre-quently a sanguineous or serous dis-charge and occasionally erosion of thenipple or underlying nodule {2222}.
H i s t o p a t h o l o g yIn the adenosis type, proliferating twocell layered glands sprout from andc o m p ress the collecting ducts {2222}resulting in cystic dilatation of the latterand formation of a discrete nodule. Thee p i d e rmis may undergo hyperkeratosis.R a rely the adenosis expands to causee rosion of the epidermis {2429}.When the sclerosis and pseudoinfiltra-tive patterns are prominent, an invasivec a rcinoma is closely simulated. Theb a c k g round stroma shows loose myx-oid features, large collagenous bandsor elastosis {149}.
Epithelial hyperplasia may be floridwithin the tubules of adenosis or mainlywithin the collecting ducts. Enlarge-ment of the galactophore ostia ande x p o s u re of the epithelial pro l i f e r a t i o nto the exterior in a fashion re m i n i s c e n tof “ectropion” of the uterine cervix mayo c c u r.
Prognosis and predictive factorsOccasional re c u r rences have beendescribed after incomplete excision{2425}. Association with carcinoma has been re p o rted but is rare {1367,2429}.
Syringomatous adenoma
D e f i n i t i o nA non metastasizing, locally re c u r re n t ,and locally invasive tumour of the nip-p l e / a reolar region showing sweat ductd i ff e re n t i a t i o n .
ICD-O code 8 4 0 7 / 0
V. EusebiK.T. MaiA. Taranger-Charpin
Tumours of the nipple
Fig. 1.156 Adenoma of the nipple. There is no sig-nificant epithelial proliferation in the tubules inthis case.
Fig. 1.155 Adenoma of the nipple. A compact aggregate of tubules replaces the nipple stroma.
104 Tumours of the breast

S y n o n y mInfiltrating syringomatous adenoma.
EpidemiologySyringomatous adenoma (SyT) is a rarelesion {1365,2414,2816}. While only 24cases have been reported under thisdesignation {98}, other cases have beenre p o rted as examples of low gradeadenosquamous carcinoma {2431,2816,2995}. The age range is from 11 to 67years with an average age of 40 years.
Clinical features SyA presents as a firm discrete mass(1–3 cm) situated in the nipple and sub-areolar region {269,1365}.
MacroscopyThe lesion appears as a firm, ill definednodule.
HistopathologySyA consists of nests and branchingcords of cells, glandular structures andsmall keratinous cysts permeating thenipple stroma in between bundles ofmuscle as well as in perineural spaces{1365,3056}. Extensions of the tumourmay be present at a great distance fromthe main mass with intervening normaltissue. Cytologically, most of the prolifer-ating elements appear bland with scanteosinophilic cytoplasm and re g u l a rround nuclei. The cells lining the glandlumina are cuboidal or flat. Frequentlythe glandular structures display two lay-ers of cells: i.e. inner luminal and outer
cuboidal basal cells occasionally con-taining smooth muscle actin. Mitoses arerare and necrotic areas are absent. Thestroma is usually sclerotic, but myxoidareas containing spindle cells are fre-quent.
Differential diagnosis This includes tubular carcinoma (TC)which rarely involves the nipple and lowgrade adenosquamous carcinoma whichoccurs in the breast parenchyma {2431}.
Prognosis and predictive factorsRecurrence has been reported {269}.Optimal treatment is excision with gener-ous margins.
Paget disease of the nipple
DefinitionThe presence of malignant glandularepithelial cells within the squamousepithelium of the nipple, is almost alwaysassociated with underlying intraductalcarcinoma, usually involving more thanone lactiferous duct and more distantducts, with or without infiltration, deep inthe underlying breast. Paget disease(PD) of the nipple without an underlyingcarcinoma is rare.
ICD-O code 8540/3
EpidemiologyPD may be bilateral and may occur ineither gender but at a relatively higher
rate in men. The incidence is estimatedat 1-4.3% of all breast carcinomas.
AetiologyThe glandular nature of the neoplasticcells in PD is confirmed by electro nm i c roscopic studies that show intra-cytoplasmic lumen with micro v i l l i{ 2 5 05}. Immunohistochemical studiesc o n f i rm that Paget cells have the samephenotype as the underlying intra-ductal carcinoma cells {530,1423}.Suggested mechanisms of develop-ment are: a) intraepithelial e p i d e r-m o t ropic migration of malignant cells ofintraductal carcinoma to the epiderm i s ;b) direct extension of underlying intra-ductal carcinoma to the nipple andoverlying skin; and c) in situ neoplastict r a n s f o rmation of multi-potential cellslocated in the basal layer of the lactife-rous duct and epiderm i s .
Clinical featuresDepending on the extent of epiderm a linvolvement, the skin may appear unre-markable or show changes rangingf rom focal reddening to a classicaleczematous appearance, which mayextend to the areola and adjacent epi-d e rmis. There is sometimes retraction ofthe nipple.
HistopathologyIn the epidermis, there is proliferation ofatypical cells with large nuclei andabundant clear or focally dense cyto-plasm. They are disposed in small clus-
BAFig. 1.157 Syringomatous adenoma of the nipple. A Irregular shaped glandular structures are present between smooth muscle bundles. B Actin stains the fasciclesof smooth muscle but the syringoma is unstained.
105Tumours of the nipple

ters which are often closely packed inthe centre of the lesion and lower por-tion of the epidermis but tend to be dis-persed in single cells at the peripheryand upper portion of the epidermis. Theunderlying lactiferous ducts contain ausually high grade DCIS that mergeswith the PD. Rare l y, lobular intraepithe-lial neoplasia is encountered. Evenwhen the in situ carcinoma is in thedeep breast tissue, an involved lactifer-ous duct with or without skip areas canalmost always be identified by serials e c t i o n i n g .An associated infiltrating carc i n o m aoccurs in one-third of patients who pres-ent without a palpable mass and in morethan 90% of those with a palpable mass. Special stains reveal the presence ofmucin in the Paget cells in a large num-ber of cases. Paget cells occasionally
contain melanin pigment granules as aresult of phagocytosis.
Immunoprofile I m m u n o h i s t o c h e m i c a l l y, Paget cellsdemonstrate similar pro p e rties to theunderlying intraductal carcinoma cellswith positive immunoreactivity for carc i-n o e m b ryonic antigen, low molecularweight cytokeratin and ERBB2. Onoccasion, one of these antisera may benegative. Squamous carcinoma is com-monly non-reactive for these antisera,but rarely may be immunoreactive forcytokeratin 7 {3128}. Contrary to malig-nant melanoma, PD is usually S-100p rotein and HMB45 negative. In PD,TP53 and estrogen receptor may benegative or positive, depending on thei m m u n o p rofile of the corre s p o n d i n gunderlying carcinoma.
Differential diagnosisPD occasionally poses diff e rential diag-nostic problems with malignantmelanoma due to the pagetoid patternof spread and the presence of pigmentgranules and also with squamous cellc a rcinoma in situ, due to the pro l i f e r a-tion of atypical dark cells. The applica-tion of histochemical techniques andthe use of immunostains will solve thequestion in most cases.
Prognosis and predictive factorsThe prognosis is dependent on thep resence or absence of underlyingintraductal carcinoma and associatedinvasive carcinoma in the deep bre a s tt i s s u e .
B CAFig. 1.158 Paget disease of the nipple. A Atypical cells with clear cytoplasm admixed with those with dense cytoplasm. B, C Immunostaining for cytokeratin 7 (B)and ERBB2 (C) decorate the neoplastic cells predominantly located in the lower portion of the epidermis.
106 Tumours of the breast

Malignant lymphoma
D e f i n i t i o nMalignant lymphoma of the breast mayp resent as a primary or secondarytumour; both are rare. There is no mor-phological criterion to diff e re n t i a t ebetween the two {117,1792}.The criteria for defining and documenta-tion of primary breast lymphoma, firstp roposed by Wiseman and Liao {3136}and, with minor modifications, acceptedby others, are as follows: 1. Availability of adequate histologicalmaterial. 2. Presence of breast tissue in, or adja-cent to, the lymphoma infiltrate.3. No concurrent nodal disease exceptfor the involvement of ipsilateral axillarylymph nodes.4. No previous history of lymphomainvolving other organs or tissues.As such criteria seem too restrictive andleave no room for primary breast lym-phomas of higher stages, some authorsinclude cases in which the breast is the first or major site of pre s e n t a t i o n ,even if, on subsequent staging pro-c e d u res, involvement of distant nodalsites or bone marrow is discovere d{ 3 5 9 , 1 2 6 1 , 1 7 5 3 } .
Epidemiology P r i m a ry breast lymphoma may appear atany age, but the majority of patients arepostmenopausal women. A subset ofpatients is re p resented by pregnant or lac-tating women with massive bilateral bre a s tswelling; most of these cases were re p o rt-ed from Africa {2643} although non-African cases are also on re c o rd {1753}.The disease is exceedingly rare in men{ 2 5 4 0 } .
Clinical featuresClinical presentation of primary breastlymphoma usually does not differ fromthat of breast carcinoma. It usually pres-ents with a painless lump sometimesmultinodular, which is bilateral in approx-imately 10% of cases. Imaging usuallyreveals no feature which helps to distin-guish primary from secondary lymphoma{1657,2199}. The value of MR imaging inbreast lymphomas has not been clearlydetermined {1952,1961}.
MacroscopyP r i m a ry and secondary breast lym-phomas most commonly appear as awell circumscribed tumour of vary i n gsize, up to 20 cm in largest diameter. Oncut surface, the neoplastic tissue is white
to white-grey, soft or firm, with occasion-al haemorrhagic or necrotic foci {994,1580,1753,3136}.
HistopathologyMicroscopically, the majority of primarybreast lymphomas are diffuse large Bcell lymphomas, according to the mostrecent WHO classification {352,1144}. Inolder literature, cases designated asreticulum cell sarcoma, histiocytic lym-phoma and at least some lymphosarco-ma cases would nowadays most proba-bly be included in the above category.M o re re c e n t l y, such lymphomas werediagnosed as centroblastic or immu-noblastic by the Kiel classification or dif-fuse large cell cleaved or noncleavedand immunoblastic lymphomas by theLukes-Collins classification and WorkingF o rmulation {18,296,534,706,994,1261,1346,1580,1665}.A minor pro p o rtion of primary lym-phomas of the breast reflect Burkitt lym-phoma, extranodular marginal-zone B-cell lymphoma of mucosa associatedlymphoid tissue (MALT) type, follicularlymphoma, lymphoblastic lymphoma ofeither B or T type, and, extremely rarely,T-cell lymphomas of variable subtypesby the current WHO classification.
Malignant lymphoma and metastatic tumours
J. LamovecA. WotherspoonJ. Jacquemier
BAFig. 1.159 Diffuse large B-cell lymphoma. A Medullary carcinoma-like appearance. B Circumscribed mass, composed of large pleomorphic neoplastic lym-phoid cells.
107Malignant lymphoma and metastatic tumours

The relationship of the surrounding mam-mary tissue to the lymphomatous infiltra-tion differs from case to case. In some,the bulk of the lesion is located in thesubcutaneous tissue, and bre a s tparenchyma is found only peripherally.In others, numerous ducts and lobulesare embedded in the infiltrate but clearlyseparated from it. Sometimes lymphomacells infiltrate the ducts to diff e re n tdegrees and, in rare cases, the latter areovergrown by lymphoma cells and bare-ly visible, sometimes revealed only byusing keratin immunostaining. The stro-ma may be scant or abundant and theinfiltrates may have a “medullary ”appearance. In some cases, lymphomacells form cords and ribbons simulatingan infiltrating lobular carc i n o m a .
Diffuse large B-cell lymphoma
ICD-O code 9680/3
Lymphoma of this type is characterizedby a diffuse pattern of infiltration of bre a s ttissue by large lymphoma cells varying inappearance from quite uniform to pleo-morphic. Generally, the lymphoma cellsresemble centroblasts or immunoblasts.The nuclei are oval, indented or evenlobated, usually with distinct, single ormultiple nucleoli, and the amount of cyto-plasm is variable. Mitoses are usuallyn u m e rous, various numbers of cells areapoptotic and necrotic foci may be found.Lymphoma cells are often admixed withsmaller reactive lymphocytes of B or Ttype; macrophages may be pro m i n e n t ,i m p a rting a “starry sky” appearance tothe tumour. In some cases, pseudofollic-ular structures are seen due to selectiveinfiltration of ductal-lobular units {18}.Adjacent mammary tissue may exhibitlobular atrophy or lymphocytic lobulitis
{18,113}; the latter may be prominent andw i d e s p read, featuring lymphocytic mas-topathy {113}.Lymphoma cells are immunoreactive forCD20, CD79a, and CD45RB and nega-tive for CD3 and CD45RO. Cases withimmunoblastic features may demonstratelight chain restriction. Exceptionally, lym-phoma cells express CD30 antigen {18}.
Burkitt lymphoma
ICD-O code 9687/3
The morphological features of Burkittlymphoma of the breast are identicalwith those seen in such a lymphoma inother organs and tissues: the infiltrate iscomposed of sheets of uniform, primi-tive looking, cells of medium size, withround nuclei, multiple nucleoli, coarsec h romatin and a rather thick nuclearmembrane. The cells are cohesive andthe cytoplasm is moderate in amountwith fine vacuoles containing lipids; its q u a res off with the cytoplasm of adja-cent cells. Mitoses are very numero u s .N u m e rous tingible-body macro p h a g e sa re evenly dispersed among the neo-plastic cells producing the characteris-tic, but by no means pathognomonic,“ s t a r ry sky” appearance of the lym-phoma. The breast tissue is usuallyhyperplastic and secre t o ry.Patients are usually pregnant or lactat-ing women, particularly from tro p i c a lAfrica where Burkitt lymphoma isendemic {2643}. Less fre q u e n t l y, non-endemic, sporadic cases, primarily pre-senting in the breasts, have beenobserved {1378}. Tumours typicallyp resent with massive bilateral bre a s tswelling {2643}.
I m m u n o h i s t o c h e m i c a l l y, pan-B markersa re positive, surface Ig, usually of IgMtype, is also positive. In addition, CD10and bcl-6 are commonly positive, whileCD5, bcl-2 and TdT are negative. EBVis frequently demonstrated in endemicbut not in sporadic cases. IgH and IgLgenes are re a r r a n g e d .
Extranodal marginal-zone B-cell lymphoma of MALT type
ICD-O code 9699/3
At least some breast lymphomasappear to belong to the category ofM A LT lymphomas although the data on their frequency vary substantially.The breast was suggested to be onecomponent of a common mucosal im-mune system {268} and may acquirelymphoid tissue as a part of an auto-immune process {2585} within whichthe lymphoma may develop. A numberof recent series on breast lymphomainclude examples of MALT lymphoma{534,994,1261,1580,1792}; they werenot encountered in other series {117,296,1346,1665}. C l a s s i c a l l y, MALT lymphomas are com-posed of small lymphocytes, marginalzone (centrocyte-like) and/or monocy-toid B-cells, often interspersed withlarger blastic cells. Monotypic plasmacells may be numerous and sometimesp redominant. The infiltrate is diff u s eand neoplastic colonization of pre - e x i s-tent reactive follicles may be seen. Alymphoepithelial lesion, defined origi-nally as an infiltration of glandularepithelium by clusters of neoplasticc e n t rocyte-like cells {1305}, is rare l yseen. Neoplastic infiltration and de-struction of mammary ducts by lym-phoma cells, most commonly encoun-t e red in large B-cell lymphomas or infil-tration of ductal epithelium by non-neo-plastic T cells should not be confusedwith a true lymphoepithelial lesion.H o w e v e r, the presence of such a lesionis not a pre requisite for a diagnosis ofM A LT lymphoma. I n f l a m m a t o ry reactive conditions maymimic MALT lymphomas; perhapsmany cases previously described aspseudolymphoma were in reality MALTlymphomas given enough time to followtheir evolution. I m m u n o h i s t o c h e m i c a l l y, MALT lym-phoma expresses pan-B cell markers
Fig. 1.161 Burkitt lymphoma. Bilateral breastinvolvement may be the presenting manifestationduring pregnancy and puberty. BL cells have pro-lactin receptors.
Fig. 1.160 CD20 immunoexpression in diffuse largeB-cell lymphoma.
108 Tumours of the breast
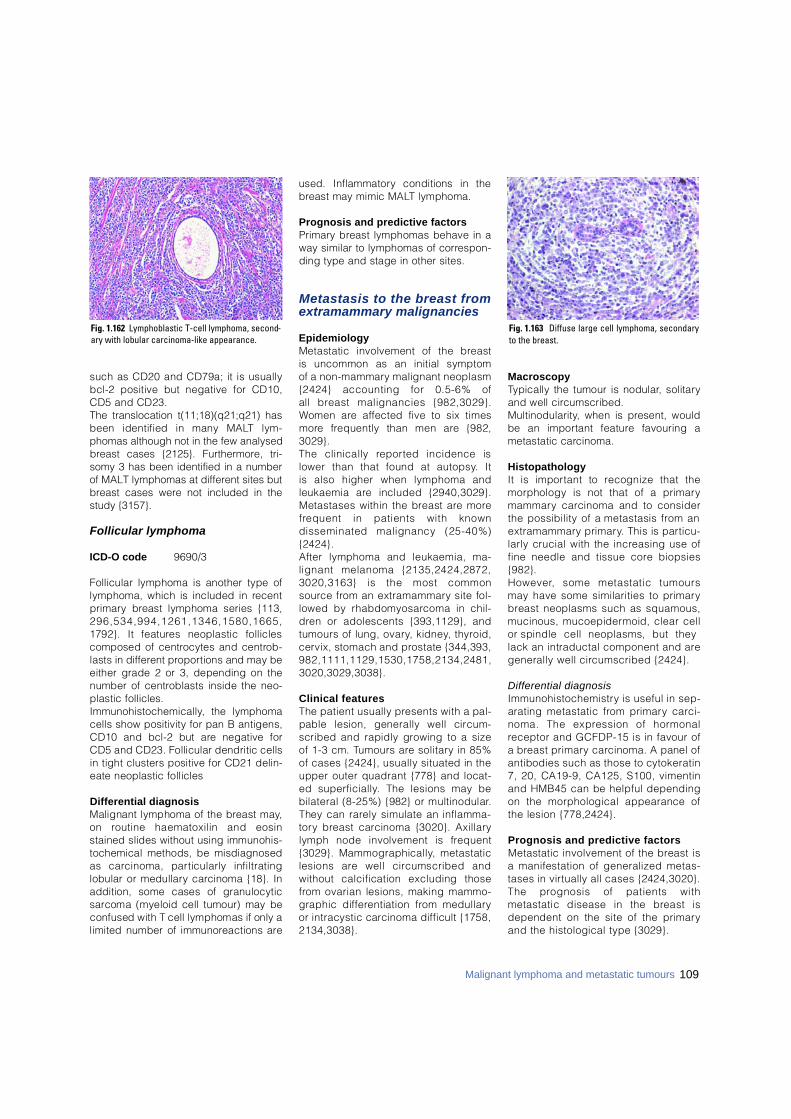
such as CD20 and CD79a; it is usuallybcl-2 positive but negative for CD10,CD5 and CD23.The translocation t(11;18)(q21;q21) hasbeen identified in many MALT lym-phomas although not in the few analysedbreast cases {2125}. Furthermore, tri-somy 3 has been identified in a numberof MALT lymphomas at different sites butbreast cases were not included in thestudy {3157}.
Follicular lymphoma
ICD-O code 9 6 9 0 / 3
Follicular lymphoma is another type oflymphoma, which is included in re c e n tp r i m a ry breast lymphoma series {113,2 9 6 , 5 3 4 , 9 9 4 , 1 2 6 1 , 1 3 4 6 , 1 5 8 0 , 1 6 6 5 ,1792}. It features neoplastic folliclescomposed of centrocytes and centro b-lasts in diff e rent pro p o rtions and may beeither grade 2 or 3, depending on thenumber of centroblasts inside the neo-plastic follicles.I m m u n o h i s t o c h e m i c a l l y, the lymphomacells show positivity for pan B antigens,CD10 and bcl-2 but are negative forCD5 and CD23. Follicular dendritic cellsin tight clusters positive for CD21 delin-eate neoplastic follicles
Differential diagnosis Malignant lymphoma of the breast may,on routine haematoxilin and eosinstained slides without using immunohis-tochemical methods, be misdiagnosedas carcinoma, particularly infiltratinglobular or medullary carcinoma {18}. Inaddition, some cases of granulocytics a rcoma (myeloid cell tumour) may beconfused with T cell lymphomas if only alimited number of immunoreactions are
used. Inflammatory conditions in theb reast may mimic MALT lymphoma.
Prognosis and predictive factorsP r i m a ry breast lymphomas behave in away similar to lymphomas of corre s p o n-ding type and stage in other sites.
Metastasis to the breast fromextramammary malignancies
E p i d e m i o l o g yMetastatic involvement of the breast is uncommon as an initial symptom of a non-mammary malignant neoplasm{2424} accounting for 0.5-6% of all b reast malignancies {982,3029}.Women are affected five to six timesm o re frequently than men are {982,3 0 2 9 } .The clinically re p o rted incidence islower than that found at autopsy. It is also higher when lymphoma andleukaemia are included {2940,3029}.Metastases within the breast are moref requent in patients with known disseminated malignancy (25-40%){2424}. After lymphoma and leukaemia, ma-lignant melanoma {2135,2424,2872,3020,3163} is the most commons o u rce from an extramammary site fol-lowed by rhabdomyosarcoma in chil-d ren or adolescents {393,1129}, andtumours of lung, ovary, kidney, thyro i d ,cervix, stomach and prostate {344,393,9 8 2 , 1 1 1 1 , 1 1 2 9 , 1 5 3 0 , 1 7 5 8 , 2 1 3 4 , 2 4 8 1 ,3 0 2 0 , 3 0 2 9 , 3 0 3 8 } .
Clinical featuresThe patient usually presents with a pal-pable lesion, generally well circ u m-scribed and rapidly growing to a sizeof 1-3 cm. Tumours are solitary in 85%of cases {2424}, usually situated in theupper outer quadrant {778} and locat-ed superf i c i a l l y. The lesions may bebilateral (8-25%) {982} or multinodular.They can rarely simulate an inflamma-t o ry breast carcinoma {3020}. Axillarylymph node involvement is fre q u e n t{3029}. Mammographically, metastaticlesions are well circumscribed andwithout calcification excluding thosef rom ovarian lesions, making mammo-graphic diff e rentiation from medullaryor intracystic carcinoma difficult {1758,2 1 3 4 , 3 0 3 8 } .
M a c r o s c o p yTypically the tumour is nodular, solitaryand well circ u m s c r i b e d .M u l t i n o d u l a r i t y, when is present, wouldbe an important feature favouring ametastatic carc i n o m a .
H i s t o p a t h o l o g yIt is important to recognize that themorphology is not that of a primarym a m m a ry carcinoma and to considerthe possibility of a metastasis from ane x t r a m a m m a ry primary. This is part i c u-larly crucial with the increasing use offine needle and tissue core biopsies{982}. H o w e v e r, some metastatic tumoursmay have some similarities to primaryb reast neoplasms such as squamous,mucinous, mucoepidermoid, clear cellor spindle cell neoplasms, but theylack an intraductal component and aregenerally well circumscribed {2424}.
Differential diagnosisI m m u n o h i s t o c h e m i s t ry is useful in sep-arating metastatic from primary carc i-noma. The expression of horm o n a lreceptor and GCFDP-15 is in favour ofa breast primary carcinoma. A panel ofantibodies such as those to cytokeratin7, 20, CA19-9, CA125, S100, vimentinand HMB45 can be helpful dependingon the morphological appearance ofthe lesion {778,2424}.
Prognosis and predictive factors Metastatic involvement of the breast isa manifestation of generalized metas-tases in virtually all cases {2424,3020}.The prognosis of patients withmetastatic disease in the breast isdependent on the site of the primaryand the histological type {3029} .
109Malignant lymphoma and metastatic tumours
Fig. 1.162 Lymphoblastic T-cell lymphoma, second-ary with lobular carcinoma-like appearance.
Fig. 1.163 Diffuse large cell lymphoma, secondaryto the breast.

DefinitionBreast tumours occur much less fre-quently in men than in women. The mostcommon male breast lesions are gynae-comastia, carcinoma, and metastaticcancers. Other benign or malignantlesions also occur, but much more rarely.
Gynaecomastia
DefinitionGynaecomastia is a non-neoplastic,often reversible, enlargement of the rudi-mentary duct system in male breast tis-sue with proliferation of epithelial andmesenchymal components re s e m b l i n gf i b roadenomatous hyperplasia of thefemale breast.
SynonymFibrosis mammae virilis (no longer used).
EpidemiologyThere are three typical, steroid depend-ent, age peaks; neonatal, adolescent(2nd/3rd decade) and the so-called maleclimacteric phase (6th/7th decade).T h e re is always relative or absoluteendogeneous or exogeneous estro-genism. Gynaecomastia is frequent inKlinefelter syndrome and also occurs inassociation with liver cirrhosis, endocrinetumours and certain medications {1263,2572}.
Clinical featuresGynaecomastia generally involves bothbreasts but is often clinically more dis-tinct in one. Nipple secretion is rare.There is a palpable retroareolar nodule orplaque like induration. Occasionallythere is aching pain.
Macroscopy T h e re is generally circ u m s c r i b e denlargement of breast tissue which isfirm and grey white on the cut surface.
HistopathologyThere is an increased number of ductslined by epithelial and myoepithelial
cells. The surrounding cellular, myxoidstroma contains fibroblasts and myofi-broblasts, intermingled with lymphocytesand plasma cells. Lobular structure s ,with or without secretory changes, arerare and mostly occur in response toexogenous hormonal stimulation such astranssexual estrogen therapy. This floridphase is followed by an inactive fibrousphase with flat epithelial cells and hyalin-ized periductal stroma. An intermediatephase with a combination of featuresalso occurs. Occasionally, duct ectasia,apocrine or squamous metaplasia devel-op. An increase in the amount of adiposebreast tissue alone may be called lipo-matous pseudogynaecomastia.
ImmunoprofilePatients with Klinefelter syndrome exhib-it elevated amounts of estrogen (ER) andprogesterone (PR) receptors but otherexamples of gynaecomastia do notdemonstrate significant elevation {2215,2666}. In gynaecomastia induced by antiandro-gen therapy, but not in carcinoma of theb reast, there may be strong focalprostate specific antigen (PSA) immu-n o reactivity in normal or hyperplasticduct epithelium, while PSAP activity isnegative. These findings should not bemisinterpreted as indicating a metastasisfrom a prostatic carcinoma {968}.
Prognosis and predictive factorsRecurrence of gynaecomastia is possi-ble. Atypical ductal epithelial hyperplasiaand carcinoma in situ are rarely seen incases of gynaecomastia but there is noconvincing evidence that gynaecomas-tia, per se, is precancerous.
Carcinoma
DefinitionC a rcinoma of the male breast is a raremalignant epithelial tumour histologicallyidentical to that seen in the female bre a s t .Both in situ and invasive carc i n o m ao c c u r, at a ratio of about 1:25 {713}.
ICD-O code 8500/3
EpidemiologyMale breast cancer is extremely rare,representing less than 1% of all breastcancers, and less than 1% of all cancerdeaths in men. Not surprisingly, there-fore, little is known about its epidemiolo-gy. The incidence of and mortality frommale breast cancer have been reportedto be rising. Reviews of incidence trendsin Scandinavia {814} and mortality trendsin Europe {1551} give no support to theexistence of such upward tre n d s .Mortality rates, for most countries, in thelate 1980s and 1990s tended to be lowerthan those registered three decades ear-lier, suggesting that advances in diagno-sis and treatment may have improved theprognosis {1551}. In the 1990s, mortality rates from malebreast cancer were around 2 per million
Tumours of the male breast
Fig. 1.165 Gynaecomastia of the male breast, withproliferating ducts and periductal stroma.
K. Prechtel P. PisaniF. Levi H. HoeflerC. La Vecchia D. PrechtelA. Sasco P. DevileeB. Cutuli
Fig. 1.164 Gynaecomastia of the male breast (left >right).
110 Tumours of the breast
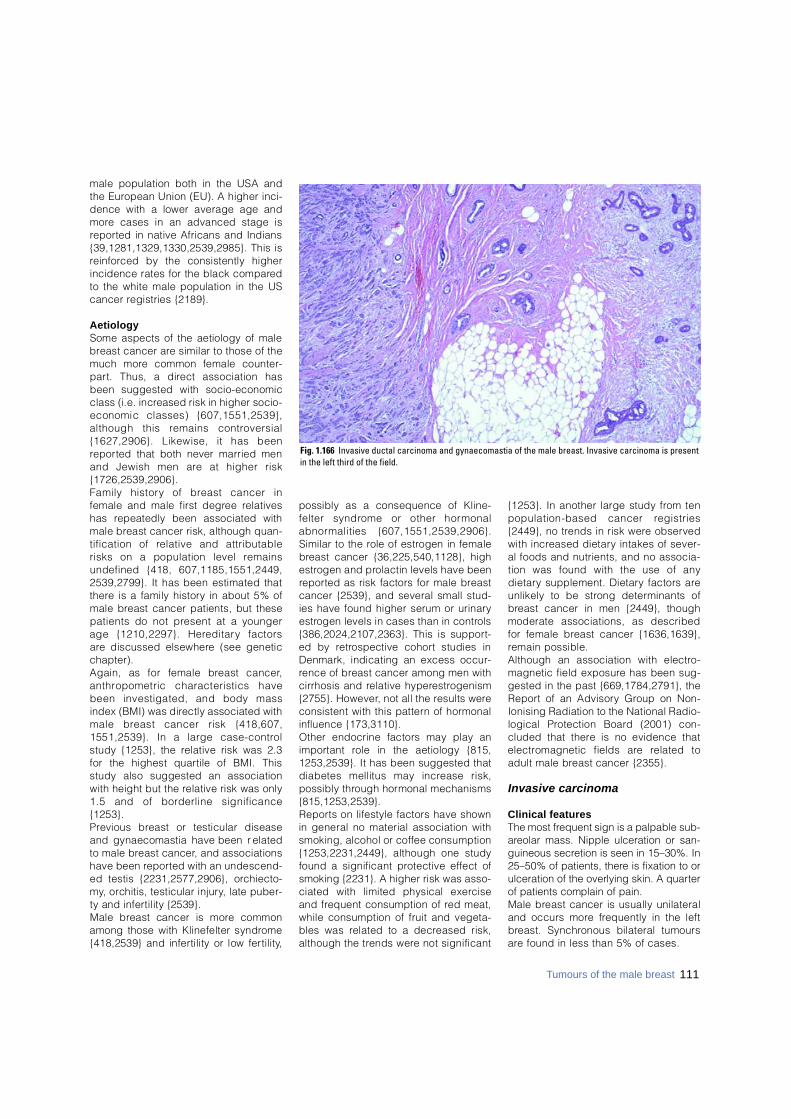
male population both in the USA andthe European Union (EU). A higher inci-dence with a lower average age andm o re cases in an advanced stage isre p o rted in native Africans and Indians{39,1281,1329,1330,2539,2985}. This isre i n f o rced by the consistently higherincidence rates for the black compare dto the white male population in the UScancer registries {2189}.
A e t i o l o g ySome aspects of the aetiology of maleb reast cancer are similar to those of themuch more common female counter-p a rt. Thus, a direct association hasbeen suggested with socio-economicclass (i.e. increased risk in higher socio-economic classes) {607,1551,2539},although this remains contro v e r s i a l{1627,2906}. Likewise, it has beenre p o rted that both never married menand Jewish men are at higher risk{ 1 7 2 6 , 2 5 3 9 , 2 9 0 6 } .Family history of breast cancer infemale and male first degree re l a t i v e shas repeatedly been associated withmale breast cancer risk, although quan-tification of relative and attributablerisks on a population level re m a i n sundefined {418, 607,1185,1551,2449,2539,2799}. It has been estimated thatt h e re is a family history in about 5% ofmale breast cancer patients, but thesepatients do not present at a youngerage {1210,2297}. Here d i t a ry factors a re discussed elsewhere (see geneticc h a p t e r ) .Again, as for female breast cancer,a n t h ropometric characteristics havebeen investigated, and body massindex (BMI) was directly associated withmale breast cancer risk {418,607,1551,2539}. In a large case-contro lstudy {1253}, the relative risk was 2.3for the highest quartile of BMI. Thisstudy also suggested an associationwith height but the relative risk was only1.5 and of borderline significance{ 1 2 5 3 } .P revious breast or testicular diseaseand gynaecomastia have been re l a t e dto male breast cancer, and associationshave been re p o rted with an undescend-ed testis {2231,2577,2906}, orc h i e c t o-m y, orchitis, testicular injury, late puber-ty and infertility {2539}. Male breast cancer is more commonamong those with Klinefelter syndro m e{418,2539} and infertility or low fert i l i t y,
possibly as a consequence of Kline-felter syndrome or other horm o n a la b n o rmalities {607,1551,2539,2906}.Similar to the role of estrogen in femaleb reast cancer {36,225,540,1128}, highe s t rogen and prolactin levels have beenre p o rted as risk factors for male bre a s tcancer {2539}, and several small stud-ies have found higher serum or urinarye s t rogen levels in cases than in contro l s{386,2024,2107,2363}. This is support-ed by re t rospective cohort studies inDenmark, indicating an excess occur-rence of breast cancer among men withcirrhosis and relative hypere s t ro g e n i s m{2755}. However, not all the results wereconsistent with this pattern of horm o n a linfluence {173,3110}.Other endocrine factors may play ani m p o rtant role in the aetiology {815,1253,2539}. It has been suggested thatdiabetes mellitus may increase risk,possibly through hormonal mechanisms{815,1253,2539}. R e p o rts on lifestyle factors have shownin general no material association withsmoking, alcohol or coffee consumption{1253,2231,2449}, although one studyfound a significant protective effect ofsmoking {2231}. A higher risk was asso-ciated with limited physical exerc i s eand frequent consumption of red meat,while consumption of fruit and vegeta-bles was related to a decreased risk,although the trends were not significant
{1253}. In another large study from tenpopulation-based cancer re g i s t r i e s{2449}, no trends in risk were observedwith increased dietary intakes of sever-al foods and nutrients, and no associa-tion was found with the use of anyd i e t a ry supplement. Dietary factors areunlikely to be strong determinants ofb reast cancer in men {2449}, thoughmoderate associations, as describedfor female breast cancer {1636,1639},remain possible. Although an association with electro-magnetic field exposure has been sug-gested in the past {669,1784,2791}, theR e p o rt of an Advisory Group on Non-Ionising Radiation to the National Radio-logical Protection Board (2001) con-cluded that there is no evidence thate l e c t romagnetic fields are related toadult male breast cancer {2355}.
Invasive carcinoma
Clinical features The most frequent sign is a palpable sub-a reolar mass. Nipple ulceration or san-guineous secretion is seen in 15–30%. In25–50% of patients, there is fixation to orulceration of the overlying skin. A quart e rof patients complain of pain. Male breast cancer is usually unilateraland occurs more frequently in the leftb reast. Synchronous bilateral tumoursa re found in less than 5% of cases.
Fig. 1.166 Invasive ductal carcinoma and gynaecomastia of the male breast. Invasive carcinoma is presentin the left third of the field.
111Tumours of the male breast

M a c r o s c o p yThe majority of male breast cancersm e a s u re between 2 and 2.5 cm.Multiple separate nodules are rare as isinvolvement of the entire bre a s t .
H i s t o p a t h o l o g yThe histological classification and grad-ing of male and female invasive bre a s tc a rcinoma are identical, but lobular car-cinoma does not usually occur in meneven in those exposed to endogenousor exogenous hormonal stimulation{1855,2521,2552} and should only bediagnosed if E-cadherin expression isabsent {34}.
I m m u n o p ro f i l eC o m p a red to breast carcinoma inwomen, male breast carcinomas have asomewhat higher frequency of ER posi-tivity in the 60-95% range, while PR pos-itivity occurs in 45-85% of cases {315,578,1836,1917}. The concentrations areindependent of patient age and similarto those found in postmenopausalwomen {2297}. Androgen receptors aree x p ressed in up to 95% of cases.
Prognosis and predictive factorsThe prognosis and predictive factorsa re the same as for female breast can-cer at comparative stages.
Metastasis to the bre a s tThe ratio of primary breast cancer and ametastasis from another primary site tothe breast is about 25:1. The most fre-
quent primaries are prostatic carc i n o-ma, adenocarcinoma of the colon, car-cinoma of the urinary bladder, malig-nant melanoma and malignant lym-p h o m a .
C a rcinoma and sarcoma secondary top revious treatment As in women, carcinoma following pre-vious chemotherapy and/or irradiationhas been re p o rted {326,601}, as haspost irradiation sarcoma {2644}.
Carcinoma in situ
ICD-O code 8 5 0 0 / 2
Clinical featuresIn the absence of mammographics c reening in men, the two most fre q u e n tsymptoms are sero-sanguineous nippledischarge and/or subareolar tumour.
H i s t o p a t h o l o g yThe histological features are in generalsimilar to those in the female breast buttwo major studies have found that themost frequent architectural pattern isp a p i l l a ry, while comedo DCIS occursr a rely {602,1221}. Lobular intraepithelialneoplasia is also extremely rare. Pagetdisease may be relatively more commonamong men compared to women due tothe shorter length of the duct system inmale bre a s t .
Other tumours
Almost all breast tumours which occurin women have also, been re p o rted inmen, albeit rare l y.
Genetics in male breast cancerVe ry little is currently known about themolecular events leading to the devel-opment and pro g ression of sporadicb reast cancer in males. Loss of het-e rozygosity (LOH) and comparativegenomic hybridisation (CGH) studiesand cytogenetic analysis have shownthat somatic genetic changes in spo-radic male breast carcinomas are quan-titatively and qualitatively similar tothose associated with sporadic femaleb reast cancer {2532,2927,3134,3265}.Tumour phenotypic markers, such asERBB2 and TP53 expression, are also
quite similar between the sexes {3129}.Ki-ras mutations are not significantlyi n c reased in male breast cancer {636}.LOH on chromosome 8p22 and 11q13a re frequently identified in male bre a s tcancer {490,1073} suggesting that thep resence of one or more tumour sup-p ressor genes in these regions mayplay a role in the development or pro-g ression of the disease. LOH at 11q13is found more often in carcinomas withpositive nodal status than in carc i n o m a swithout lymph node metastasis {1073}.F requent allelic losses on chro m o s o m e13q are re p o rted in familial, as well as insporadic, male breast cancer {2296,3134}. Chromosome 13q is the re g i o ncontaining the B R C A 2, B R U S H - 1, andretinoblastoma gene. Depending on thepopulation, studies demonstrated that4-38% of all male breast cancers areassociated with B R C A 2 a l t e r a t i o n s{918,1550, 2921}. Other putative targetgenes are also situated here, includingp rotocadherin 9 and EMK (serine/thre o-nine protein kinase). Possibly, multipletumour suppressor genes may influencethe observed pattern of loss of het-e rozygosity {1383}. The role of aberrant hormone secre t i o nor hormone receptor function in thedevelopment or pro g ression of the dis-ease remains controversial. Horm o n a limbalances, such as those in Klinefelters y n d rome or Reifenstein syndro m e(mutation of the androgen re c e p t o rgene: Xq11-12) are known risk factorsfor breast cancer in males {427,1213,2484}. In three men, germ l i n emutations in the androgen re c e p t o rgene was re p o rted including two b rothers with Reifenstein syndro m e{1686,3152}. However it has beenshown that mutations of the andro g e nreceptor are not obligatory for thedevelopment of male breast cancer{1213}. Cytogenetic studies reveal clonal chro-mosomal anomalies: Loss of the Y chro-mosome and gain of an X chro m o s o m e ,as well as the gain of chromosome 5,a re all frequently observed {1213,2484 } .Taken together with previous data, thep resent findings suggest close simi-larities between the molecular patho-genesis of male and female breast can-c e r s .
Fig. 1.167 Male breast carcinoma, DCIS. The in situcarcinomas are generally of the non-necrotic cribri-form or papillary types. Though necrosis develops insome cases composed of either micropapillary or thecribriform types, true comedo DCIS is rare.
112 Tumours of the breast
CHAPTER 2
Tumours of the Ovaryand Peritoneum
Tumours of the ovary represent about 30% of all cancers of thefemale genital system. Age-adjusted incidence rates are high-est in the economically advanced countries where they arealmost as common as cancers of the corpus uteri and invasivecancer of the cervix. Carcinomas of surface epithelial-stromalorigin account for 90% of these cancers in North America andWestern Europe. In some Asian countries, including Japan,germ cell tumours account for a significant proportion (20%) ofovarian malignancies. High parity and the use of oral contra-ceptives are consistently associated with a reduced risk ofdeveloping surface epithelial-stromal tumours while long-termestrogen replacement therapy appears to increase the risk inpostmenopausal women.
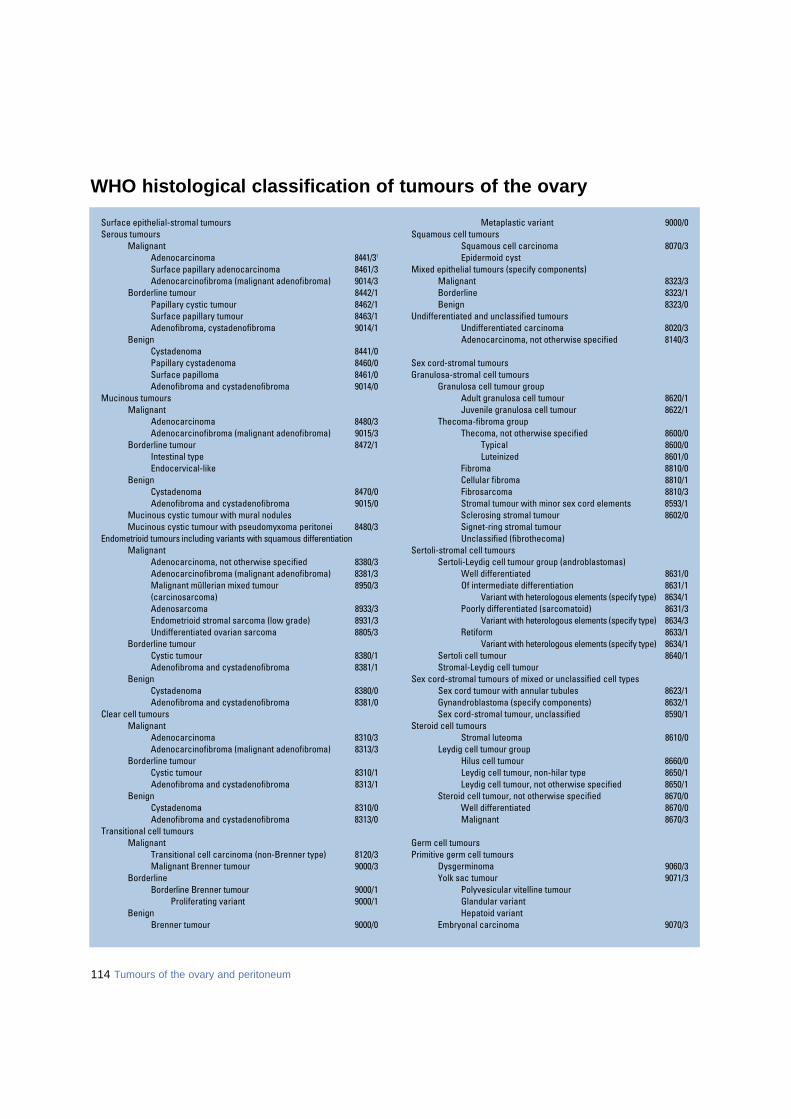
114 Tumours of the ovary and peritoneum
Surface epithelial-stromal tumoursSerous tumours
MalignantAdenocarcinoma 8 4 4 1 / 31
Surface papillary adenocarcinoma 8461/3Adenocarcinofibroma (malignant adenofibroma) 9014/3
Borderline tumour 8442/1Papillary cystic tumour 8462/1Surface papillary tumour 8463/1Adenofibroma, cystadenofibroma 9014/1
BenignCystadenoma 8441/0Papillary cystadenoma 8460/0Surface papilloma 8461/0Adenofibroma and cystadenofibroma 9014/0
Mucinous tumoursMalignant
Adenocarcinoma 8480/3Adenocarcinofibroma (malignant adenofibroma) 9015/3
Borderline tumour 8472/1Intestinal typeEndocervical-like
BenignCystadenoma 8470/0Adenofibroma and cystadenofibroma 9015/0
Mucinous cystic tumour with mural nodulesMucinous cystic tumour with pseudomyxoma peritonei 8480/3
Endometrioid tumours including variants with squamous differentiationMalignant
Adenocarcinoma, not otherwise specified 8380/3Adenocarcinofibroma (malignant adenofibroma) 8381/3Malignant müllerian mixed tumour 8950/3(carcinosarcoma)Adenosarcoma 8933/3Endometrioid stromal sarcoma (low grade) 8931/3Undifferentiated ovarian sarcoma 8805/3
Borderline tumour Cystic tumour 8380/1Adenofibroma and cystadenofibroma 8381/1
BenignCystadenoma 8380/0Adenofibroma and cystadenofibroma 8381/0
Clear cell tumoursMalignant
Adenocarcinoma 8310/3Adenocarcinofibroma (malignant adenofibroma) 8313/3
Borderline tumour Cystic tumour 8310/1Adenofibroma and cystadenofibroma 8313/1
BenignCystadenoma 8310/0Adenofibroma and cystadenofibroma 8313/0
Transitional cell tumoursMalignant
Transitional cell carcinoma (non-Brenner type) 8120/3Malignant Brenner tumour 9000/3
Borderline Borderline Brenner tumour 9000/1
Proliferating variant 9000/1Benign
Brenner tumour 9000/0
Metaplastic variant 9000/0Squamous cell tumours
Squamous cell carcinoma 8070/3Epidermoid cyst
Mixed epithelial tumours (specify components)Malignant 8323/3Borderline 8323/1Benign 8323/0
Undifferentiated and unclassified tumoursUndifferentiated carcinoma 8020/3Adenocarcinoma, not otherwise specified 8140/3
Sex cord-stromal tumoursGranulosa-stromal cell tumours
Granulosa cell tumour groupAdult granulosa cell tumour 8620/1Juvenile granulosa cell tumour 8622/1
Thecoma-fibroma groupThecoma, not otherwise specified 8600/0
Typical 8600/0Luteinized 8601/0
Fibroma 8810/0Cellular fibroma 8810/1Fibrosarcoma 8810/3Stromal tumour with minor sex cord elements 8593/1Sclerosing stromal tumour 8602/0Signet-ring stromal tumourUnclassified (fibrothecoma)
Sertoli-stromal cell tumoursSertoli-Leydig cell tumour group (androblastomas)
Well differentiated 8631/0Of intermediate differentiation 8631/1
Variant with heterologous elements (specify type) 8634/1Poorly differentiated (sarcomatoid) 8631/3
Variant with heterologous elements (specify type) 8634/3Retiform 8633/1
Variant with heterologous elements (specify type) 8634/1Sertoli cell tumour 8640/1Stromal-Leydig cell tumour
Sex cord-stromal tumours of mixed or unclassified cell typesSex cord tumour with annular tubules 8623/1Gynandroblastoma (specify components) 8632/1Sex cord-stromal tumour, unclassified 8590/1
Steroid cell tumoursStromal luteoma 8610/0
Leydig cell tumour groupHilus cell tumour 8660/0Leydig cell tumour, non-hilar type 8650/1Leydig cell tumour, not otherwise specified 8650/1
Steroid cell tumour, not otherwise specified 8670/0Well differentiated 8670/0Malignant 8670/3
Germ cell tumoursPrimitive germ cell tumours
Dysgerminoma 9060/3Yolk sac tumour 9071/3
Polyvesicular vitelline tumourGlandular variantHepatoid variant
Embryonal carcinoma 9070/3
WHO histological classification of tumours of the ovary
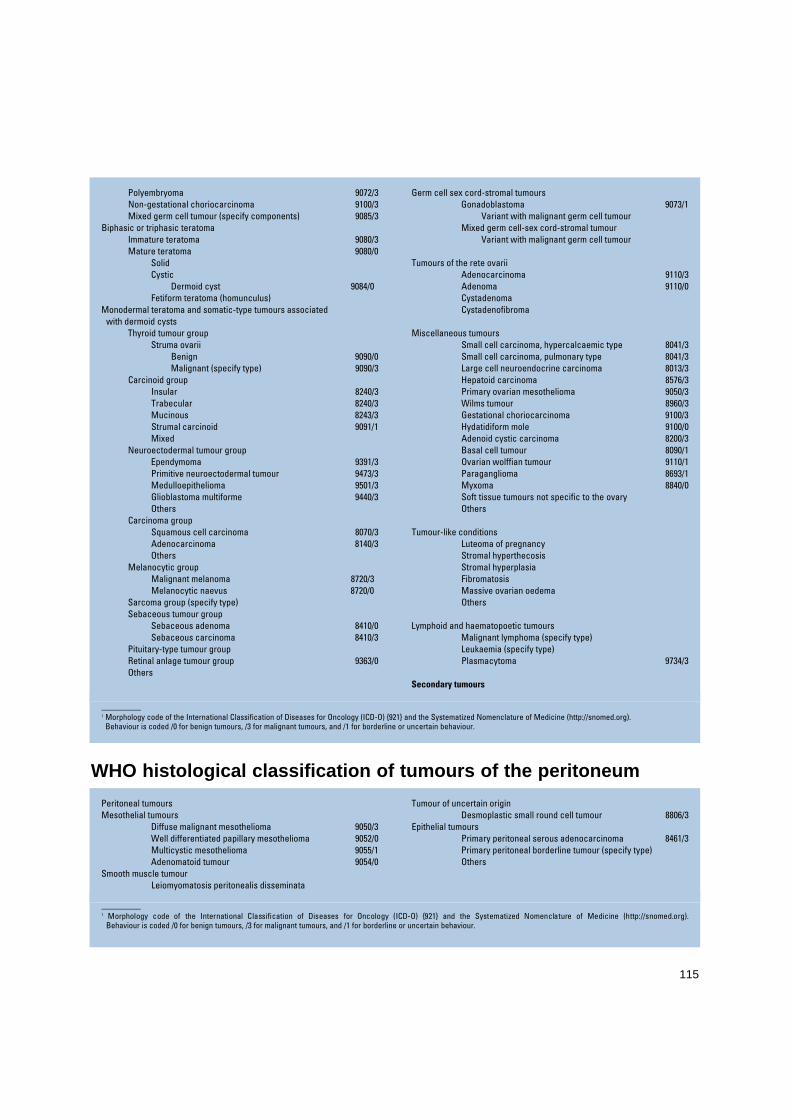
115
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Polyembryoma 9072/3Non-gestational choriocarcinoma 9100/3Mixed germ cell tumour (specify components) 9085/3
Biphasic or triphasic teratomaImmature teratoma 9080/3Mature teratoma 9080/0
SolidCystic
Dermoid cyst 9084/0Fetiform teratoma (homunculus)
Monodermal teratoma and somatic-type tumours associatedwith dermoid cysts
Thyroid tumour groupStruma ovarii
Benign 9090/0Malignant (specify type) 9090/3
Carcinoid groupInsular 8240/3Trabecular 8240/3Mucinous 8243/3Strumal carcinoid 9091/1Mixed
Neuroectodermal tumour groupEpendymoma 9391/3Primitive neuroectodermal tumour 9473/3Medulloepithelioma 9501/3Glioblastoma multiforme 9440/3Others
Carcinoma groupSquamous cell carcinoma 8070/3Adenocarcinoma 8140/3Others
Melanocytic groupMalignant melanoma 8720/3Melanocytic naevus 8720/0
Sarcoma group (specify type)Sebaceous tumour group
Sebaceous adenoma 8410/0Sebaceous carcinoma 8410/3
Pituitary-type tumour groupRetinal anlage tumour group 9363/0Others
Germ cell sex cord-stromal tumoursGonadoblastoma 9073/1
Variant with malignant germ cell tumourMixed germ cell-sex cord-stromal tumour
Variant with malignant germ cell tumour
Tumours of the rete ovariiAdenocarcinoma 9110/3Adenoma 9110/0CystadenomaCystadenofibroma
Miscellaneous tumoursSmall cell carcinoma, hypercalcaemic type 8041/3Small cell carcinoma, pulmonary type 8041/3Large cell neuroendocrine carcinoma 8013/3Hepatoid carcinoma 8576/3Primary ovarian mesothelioma 9050/3Wilms tumour 8960/3Gestational choriocarcinoma 9100/3Hydatidiform mole 9100/0Adenoid cystic carcinoma 8200/3Basal cell tumour 8090/1Ovarian wolffian tumour 9110/1Paraganglioma 8693/1Myxoma 8840/0Soft tissue tumours not specific to the ovaryOthers
Tumour-like conditionsLuteoma of pregnancyStromal hyperthecosisStromal hyperplasiaFibromatosisMassive ovarian oedemaOthers
Lymphoid and haematopoetic tumoursMalignant lymphoma (specify type)Leukaemia (specify type)Plasmacytoma 9734/3
Secondary tumours
WHO histological classification of tumours of the peritoneum
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Peritoneal tumoursMesothelial tumours
Diffuse malignant mesothelioma 9050/3Well differentiated papillary mesothelioma 9052/0Multicystic mesothelioma 9055/1Adenomatoid tumour 9054/0
Smooth muscle tumourLeiomyomatosis peritonealis disseminata
Tumour of uncertain originDesmoplastic small round cell tumour 8806/3
Epithelial tumoursPrimary peritoneal serous adenocarcinoma 8461/3Primary peritoneal borderline tumour (specify type)Others
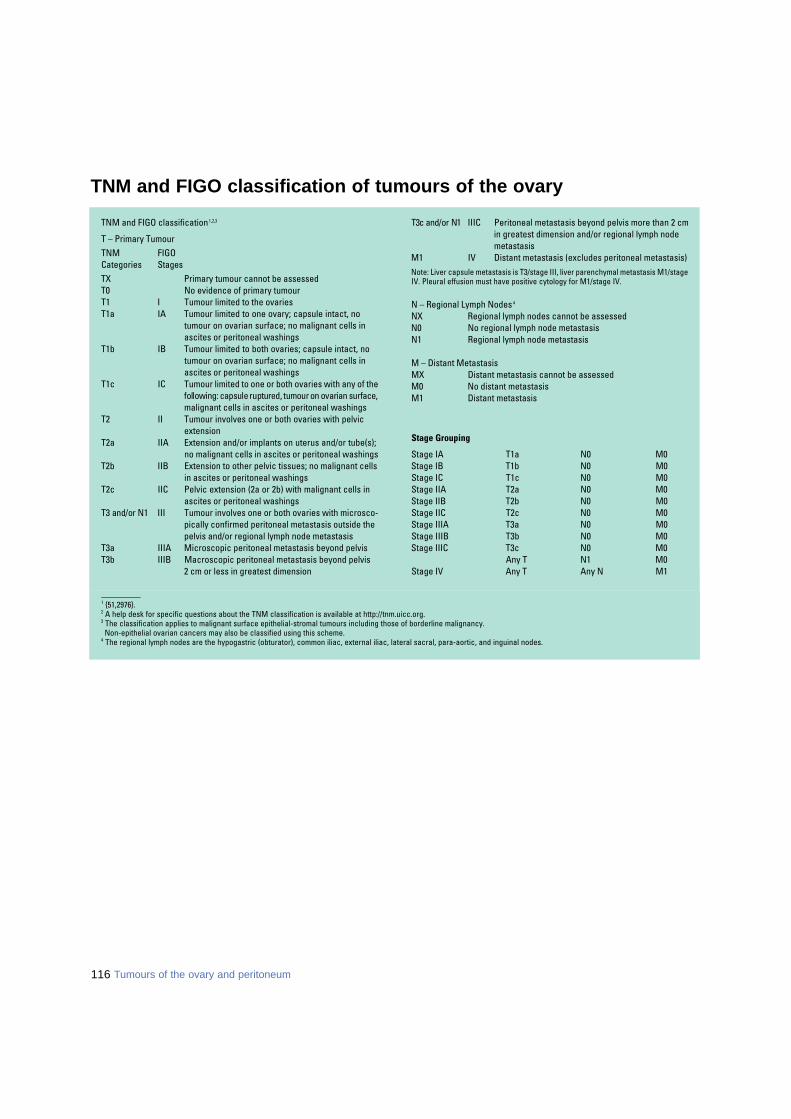
116 Tumours of the ovary and peritoneum
_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The classification applies to malignant surface epithelial-stromal tumours including those of borderline malignancy.
Non-epithelial ovarian cancers may also be classified using this scheme. 4 The regional lymph nodes are the hypogastric (obturator), common iliac, external iliac, lateral sacral, para-aortic, and inguinal nodes.
TNM and FIGO classification 1,2,3
T – Primary TumourTNM FIGOCategories S t a g e sTX Primary tumour cannot be assessedT0 No evidence of primary tumourT1 I Tumour limited to the ovariesT1a IA Tumour limited to one ovary; capsule intact, no
tumour on ovarian surface; no malignant cells inascites or peritoneal washings
T1b IB Tumour limited to both ovaries; capsule intact, notumour on ovarian surface; no malignant cells inascites or peritoneal washings
T1c IC Tumour limited to one or both ovaries with any of thefollowing: capsule ruptured, tumour on ovarian surface,malignant cells in ascites or peritoneal washings
T2 II Tumour involves one or both ovaries with pelvic extension
T2a IIA Extension and/or implants on uterus and/or tube(s); no malignant cells in ascites or peritoneal washings
T2b IIB Extension to other pelvic tissues; no malignant cells in ascites or peritoneal washings
T2c IIC Pelvic extension (2a or 2b) with malignant cells inascites or peritoneal washings
T3 and/or N1 III Tumour involves one or both ovaries with microsco-pically confirmed peritoneal metastasis outside thepelvis and/or regional lymph node metastasis
T3a IIIA Microscopic peritoneal metastasis beyond pelvisT3b IIIB Macroscopic peritoneal metastasis beyond pelvis
2 cm or less in greatest dimension
T3c and/or N1 IIIC Peritoneal metastasis beyond pelvis more than 2 cmin greatest dimension and/or regional lymph nodemetastasis
M1 IV Distant metastasis (excludes peritoneal metastasis)Note: Liver capsule metastasis is T3/stage III, liver parenchymal metastasis M1/stageIV. Pleural effusion must have positive cytology for M1/stage IV.
N – Regional Lymph Nodes 4
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage IA T1a N0 M0Stage IB T1b N0 M0Stage IC T1c N0 M0Stage IIA T2a N0 M0Stage IIB T2b N0 M0Stage IIC T2c N0 M0Stage IIIA T3a N0 M0Stage IIIB T3b N0 M0Stage IIIC T3c N0 M0
Any T N1 M0Stage IV Any T Any N M1
TNM and FIGO classification of tumours of the ovary
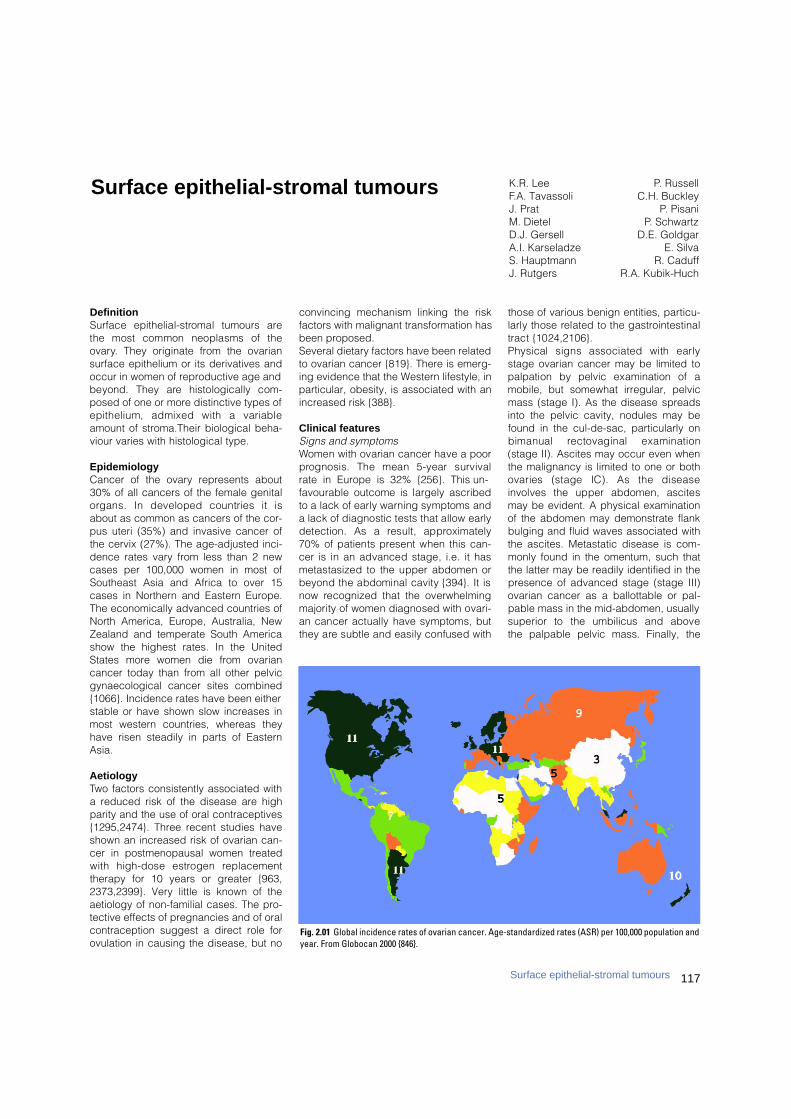
DefinitionS u rface epithelial-stromal tumours arethe most common neoplasms of theovary. They originate from the ovariansurface epithelium or its derivatives andoccur in women of reproductive age andbeyond. They are histologically com-posed of one or more distinctive types ofepithelium, admixed with a variableamount of stroma.Their biological beha-viour varies with histological type.
EpidemiologyCancer of the ovary represents about30% of all cancers of the female genitalorgans. In developed countries it isabout as common as cancers of the cor-pus uteri (35%) and invasive cancer ofthe cervix (27%). The age-adjusted inci-dence rates vary from less than 2 newcases per 100,000 women in most ofSoutheast Asia and Africa to over 15cases in Northern and Eastern Europe.The economically advanced countries ofNorth America, Europe, Australia, NewZealand and temperate South Americashow the highest rates. In the UnitedStates more women die from ovariancancer today than from all other pelvicgynaecological cancer sites combined{1066}. Incidence rates have been eitherstable or have shown slow increases inmost western countries, whereas theyhave risen steadily in parts of EasternAsia.
AetiologyTwo factors consistently associated witha reduced risk of the disease are highparity and the use of oral contraceptives{1295,2474}. Three recent studies haveshown an increased risk of ovarian can-cer in postmenopausal women treatedwith high-dose estrogen re p l a c e m e n ttherapy for 10 years or greater {963,2373,2399}. Very little is known of theaetiology of non-familial cases. The pro-tective effects of pregnancies and of oralcontraception suggest a direct role forovulation in causing the disease, but no
convincing mechanism linking the riskfactors with malignant transformation hasbeen proposed. Several dietary factors have been relatedto ovarian cancer {819}. There is emerg-ing evidence that the Western lifestyle, inparticular, obesity, is associated with anincreased risk {388}.
Clinical featuresSigns and symptoms Women with ovarian cancer have a poorp rognosis. The mean 5-year survival rate in Europe is 32% {256}. This un-favourable outcome is largely ascribedto a lack of early warning symptoms anda lack of diagnostic tests that allow earlydetection. As a result, appro x i m a t e l y70% of patients present when this can-cer is in an advanced stage, i.e. it hasmetastasized to the upper abdomen orbeyond the abdominal cavity {394}. It isnow recognized that the overwhelmingmajority of women diagnosed with ovari-an cancer actually have symptoms, butthey are subtle and easily confused with
those of various benign entities, part i c u-larly those related to the gastro i n t e s t i n a ltract {1024,2106}.Physical signs associated with earlystage ovarian cancer may be limited topalpation by pelvic examination of amobile, but somewhat irregular, pelvicmass (stage I). As the disease spreadsinto the pelvic cavity, nodules may befound in the cul-de-sac, particularly onbimanual rectovaginal examination(stage II). Ascites may occur even whenthe malignancy is limited to one or bothovaries (stage IC). As the diseaseinvolves the upper abdomen, ascitesmay be evident. A physical examinationof the abdomen may demonstrate flankbulging and fluid waves associated withthe ascites. Metastatic disease is com-monly found in the omentum, such thatthe latter may be readily identified in thepresence of advanced stage (stage III)ovarian cancer as a ballottable or pal-pable mass in the mid-abdomen, usuallysuperior to the umbilicus and above the palpable pelvic mass. Finally, the
K.R. Lee P. RussellF.A. Tavassoli C.H. BuckleyJ. Prat P. PisaniM. Dietel P. SchwartzD.J. Gersell D.E. GoldgarA.I. Karseladze E. SilvaS. Hauptmann R. CaduffJ. Rutgers R.A. Kubik-Huch
Surface epithelial-stromal tumours
117Surface epithelial-stromal tumours
Fig. 2.01 Global incidence rates of ovarian cancer. Age-standardized rates (ASR) per 100,000 population andyear. From Globocan 2000 {846}.
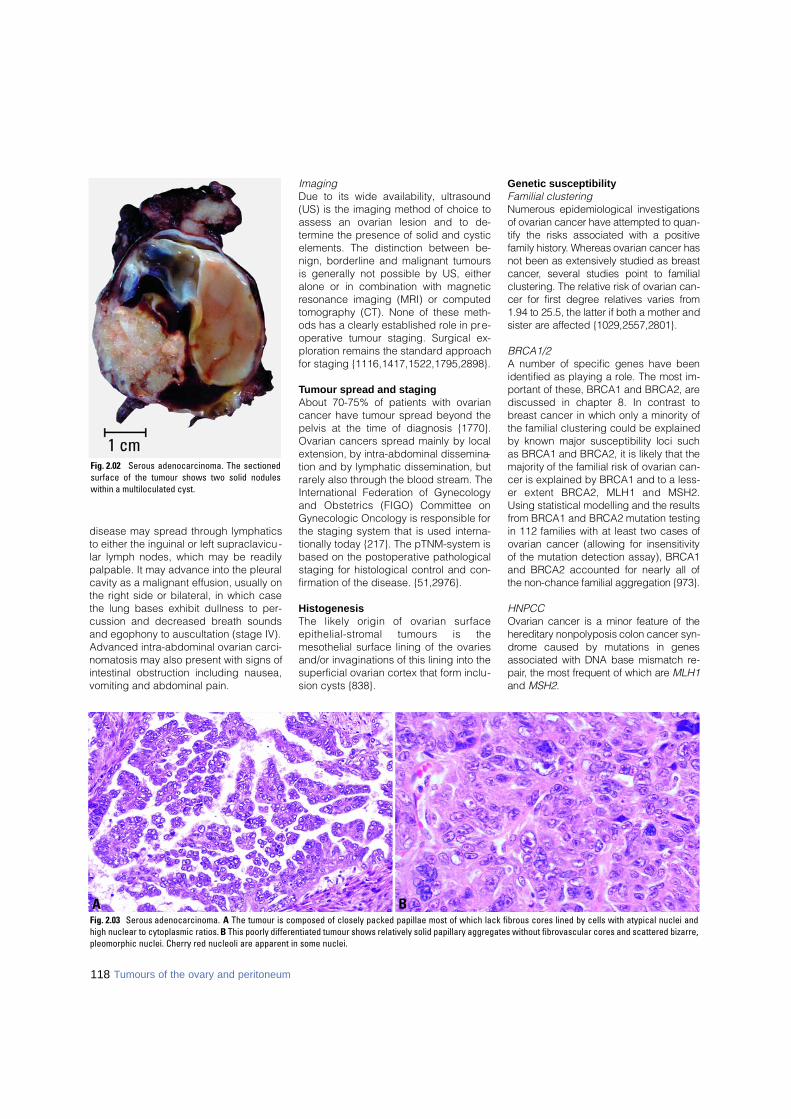
118 Tumours of the ovary and peritoneum
disease may spread through lymphaticsto either the inguinal or left supraclavicu-lar lymph nodes, which may be readilypalpable. It may advance into the pleuralcavity as a malignant effusion, usually onthe right side or bilateral, in which casethe lung bases exhibit dullness to per-cussion and decreased breath soundsand egophony to auscultation (stage IV).Advanced intra-abdominal ovarian carci-nomatosis may also present with signs ofintestinal obstruction including nausea,vomiting and abdominal pain.
ImagingDue to its wide availability, ultrasound(US) is the imaging method of choice toassess an ovarian lesion and to de-termine the presence of solid and cysticelements. The distinction between be-nign, borderline and malignant tumoursis generally not possible by US, eitheralone or in combination with magneticresonance imaging (MRI) or computedtomography (CT). None of these meth-ods has a clearly established role in pre-operative tumour staging. Surgical ex-ploration remains the standard approachfor staging {1116,1417,1522,1795,2898}.
Tumour spread and stagingAbout 70-75% of patients with ovariancancer have tumour spread beyond thepelvis at the time of diagnosis {1770}.Ovarian cancers spread mainly by localextension, by intra-abdominal dissemina-tion and by lymphatic dissemination, butrarely also through the blood stream. TheInternational Federation of Gynecologyand Obstetrics (FIGO) Committee onGynecologic Oncology is responsible forthe staging system that is used interna-tionally today {217}. The pTNM-system isbased on the postoperative pathologicalstaging for histological control and con-firmation of the disease. {51,2976}.
HistogenesisThe likely origin of ovarian surf a c ee p i t h e l i a l - s t romal tumours is themesothelial surface lining of the ovariesand/or invaginations of this lining into thesuperficial ovarian cortex that form inclu-sion cysts {838}.
Genetic susceptibilityFamilial clusteringN u m e rous epidemiological investigationsof ovarian cancer have attempted to quan-tify the risks associated with a positivefamily history. Whereas ovarian cancer hasnot been as extensively studied as bre a s tc a n c e r, several studies point to familialclustering. The relative risk of ovarian can-cer for first degree relatives varies fro m1.94 to 25.5, the latter if both a mother andsister are affected {1029,2557,2801}.
BRCA1/2A number of specific genes have beenidentified as playing a role. The most im-p o rtant of these, BRCA1 and BRCA2, arediscussed in chapter 8. In contrast tob reast cancer in which only a minority ofthe familial clustering could be explainedby known major susceptibility loci suchas BRCA1 and BRCA2, it is likely that themajority of the familial risk of ovarian can-cer is explained by BRCA1 and to a less-er extent BRCA2, MLH1 and MSH2.Using statistical modelling and the re s u l t sf rom BRCA1 and BRCA2 mutation testingin 112 families with at least two cases ofovarian cancer (allowing for insensitivityof the mutation detection assay), BRCA1and BRCA2 accounted for nearly all ofthe non-chance familial aggregation {973}.
HNPCCOvarian cancer is a minor feature of theh e re d i t a ry nonpolyposis colon cancer syn-d rome caused by mutations in genesassociated with DNA base mismatch re-p a i r, the most frequent of which are M L H 1and M S H 2.
BAFig. 2.03 Serous adenocarcinoma. A The tumour is composed of closely packed papillae most of which lack fibrous cores lined by cells with atypical nuclei andhigh nuclear to cytoplasmic ratios. B This poorly differentiated tumour shows relatively solid papillary aggregates without fibrovascular cores and scattered bizarre,pleomorphic nuclei. Cherry red nucleoli are apparent in some nuclei.
Fig. 2.02 Serous adenocarcinoma. The sectionedsurface of the tumour shows two solid noduleswithin a multiloculated cyst.
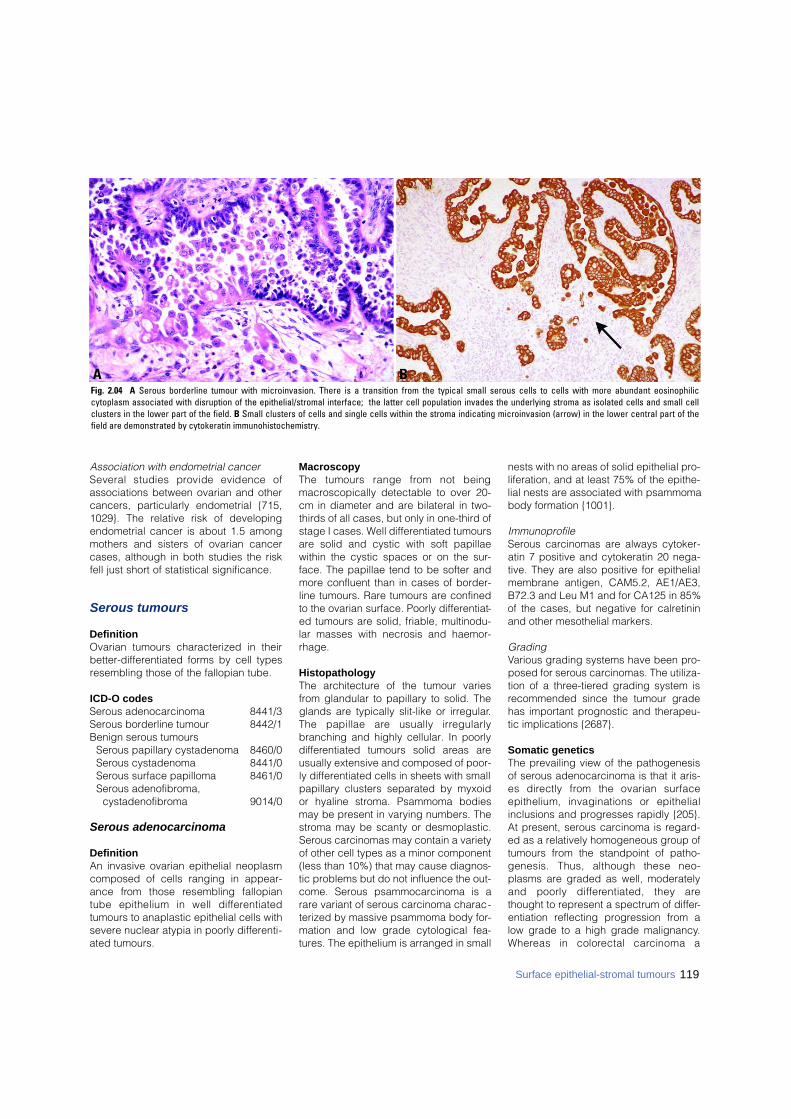
119Surface epithelial-stromal tumours
Association with endometrial cancerSeveral studies provide evidence ofassociations between ovarian and othercancers, particularly endometrial {715,1029}. The relative risk of developingendometrial cancer is about 1.5 amongmothers and sisters of ovarian cancercases, although in both studies the riskfell just short of statistical significance.
Serous tumours
DefinitionOvarian tumours characterized in theirbetter-differentiated forms by cell typesresembling those of the fallopian tube.
ICD-O codesSerous adenocarcinoma 8441/3Serous borderline tumour 8442/1Benign serous tumours
Serous papillary cystadenoma 8460/0Serous cystadenoma 8441/0Serous surface papilloma 8461/0Serous adenofibroma,
cystadenofibroma 9014/0
Serous adenocarcinoma
DefinitionAn invasive ovarian epithelial neoplasmcomposed of cells ranging in appear-ance from those resembling fallopiantube epithelium in well diff e re n t i a t e dtumours to anaplastic epithelial cells withsevere nuclear atypia in poorly differenti-ated tumours.
MacroscopyThe tumours range from not beingmacroscopically detectable to over 20-cm in diameter and are bilateral in two-thirds of all cases, but only in one-third ofstage I cases. Well differentiated tumoursare solid and cystic with soft papillaewithin the cystic spaces or on the sur-face. The papillae tend to be softer andmore confluent than in cases of border-line tumours. Rare tumours are confinedto the ovarian surface. Poorly differentiat-ed tumours are solid, friable, multinodu-lar masses with necrosis and haemor-rhage.
HistopathologyThe architecture of the tumour variesfrom glandular to papillary to solid. Theglands are typically slit-like or irregular.The papillae are usually irre g u l a r l ybranching and highly cellular. In poorlyd i ff e rentiated tumours solid areas areusually extensive and composed of poor-ly differentiated cells in sheets with smallpapillary clusters separated by myxoidor hyaline stroma. Psammoma bodiesmay be present in varying numbers. Thestroma may be scanty or desmoplastic.Serous carcinomas may contain a varietyof other cell types as a minor component(less than 10%) that may cause diagnos-tic problems but do not influence the out-come. Serous psammocarcinoma is arare variant of serous carcinoma charac-terized by massive psammoma body for-mation and low grade cytological fea-tures. The epithelium is arranged in small
nests with no areas of solid epithelial pro-liferation, and at least 75% of the epithe-lial nests are associated with psammomabody formation {1001}.
Immunoprofile Serous carcinomas are always cytoker-atin 7 positive and cytokeratin 20 nega-tive. They are also positive for epithelialmembrane antigen, CAM5.2, AE1/AE3,B72.3 and Leu M1 and for CA125 in 85%of the cases, but negative for calretininand other mesothelial markers.
GradingVarious grading systems have been pro-posed for serous carcinomas. The utiliza-tion of a three-tiered grading system isrecommended since the tumour gradehas important prognostic and therapeu-tic implications {2687}.
Somatic geneticsThe prevailing view of the pathogenesisof serous adenocarcinoma is that it aris-es directly from the ovarian surf a c eepithelium, invaginations or epithelialinclusions and progresses rapidly {205}.At present, serous carcinoma is regard-ed as a relatively homogeneous group oftumours from the standpoint of patho-genesis. Thus, although these neo-plasms are graded as well, moderatelyand poorly diff e rentiated, they arethought to represent a spectrum of differ-entiation reflecting progression from alow grade to a high grade malignancy.W h e reas in colorectal carcinoma a
BAFig. 2.04 A Serous borderline tumour with microinvasion. There is a transition from the typical small serous cells to cells with more abundant eosinophilic cytoplasm associated with disruption of the epithelial/stromal interface; the latter cell population invades the underlying stroma as isolated cells and small cellclusters in the lower part of the field. B Small clusters of cells and single cells within the stroma indicating microinvasion (arrow) in the lower central part of thefield are demonstrated by cytokeratin immunohistochemistry.

120 Tumours of the ovary and peritoneum
tumour pro g ression model in whichsequential accumulation of moleculargenetic alterations leading to morpholog-ically recognizable stages is well estab-lished {1468}, a similar model for ovarians e rous carcinoma has not been pro-posed because well defined precursorlesions have not been identified.It has been reported that even the earli-est histological serous carcinomas arealready high grade and morphologicallyresemble their advanced stage counter-parts {205}. The histological similaritiesare paralleled by recent molecular genet-ic findings demonstrating TP53 muta-tions in very small stage I serous carci-nomas and in the adjacent "dysplastic"surface epithelium {2275}. Most studieshave shown that approximately 60% ofadvanced stage ovarian serous carcino-mas have mutant TP53 {230,3095}. Thus,although the molecular genetic findingsin these early carcinomas are prelimi-nary, they suggest that serous carcinomain its very earliest stage of developmentresembles advanced stage serous carci-noma at the molecular level. This wouldsupport the view that there are no mor-phologically recognized interm e d i a t esteps in the progression of the conven-tional type of ovarian serous carcinoma. S e rous borderline tumours (SBTs), non-invasive and invasive micro p a p i l l a rytypes, frequently display K R A S m u t a t i o n sbut rarely mutant T P 5 3. Increased allelic
imbalance of chromosome 5q is associ-ated with the pro g ression from typicalSBT to micro p a p i l l a ry SBT and incre a s e dallelic imbalance of chromosome 1p withthe pro g ression from micro p a p i l l a ry SBTto invasive serous carcinoma {2706}. Incontrast, K R A S mutations are very rare inconventional serous carcinoma, but T P 5 3mutations occur in approximately 60%.Recently, mutations were also identifiedin the BRAF gene, a downstream media-tor of KRAS. BRAF and KRAS mutationsappear to be mutually exclusive. Thesemutations were only detected in lowgrade ovarian serous carcinomas {2707}.Thus, there appears to be more than onepathway of tumorigenesis for serous car-cinoma. In one pathway, conventionalserous carcinoma, a high grade neo-plasm, develops "de novo" from the sur-face epithelium of the ovary, grows rap-idly and is highly aggressive {205}.These tumours, even at their earlieststage, display TP53 mutations but notKRAS mutations. In the other pathway aSBT progresses in a "stepwise" fashiont h rough a non-invasive micro p a p i l l a rystage before becoming invasive {2706}or through microinvasion in a back-g round of typical SBT. The indolentm i c ro p a p i l l a ry tumours frequently dis-play KRAS mutations, but TP53 muta-tions are only rarely detected.
Genetic susceptibilityThe neoplasms that develop in womenwith germline B R C A 1 mutations aremostly serous carcinomas of the ovary,fallopian tube and peritoneum.
Prognosis and predictive factorsThe overall 5-year survival is appro x i m a t e-ly 40%; however, many of those alive at 5years are alive with disease. Up to 85% ofcases present with widespread metastaticdisease. Survival at 5 years in this gro u pis 10-20%. Patients with disease confined
to the ovary or pelvis have a 5-year sur-vival of 80%. Patients with serous psam-m o c a rcinoma have a protracted clinicalcourse and a relatively favourable pro g-nosis; their clinical behaviour more close-ly resembles that of SBT than serous car-cinoma of the usual type.
Serous borderline tumour withmicroinvasion
DefinitionAn ovarian serous tumour of low malig-nant potential exhibiting early stromalinvasion characterized by the presencein the stroma of individual or clusters ofneoplastic cells cytologically similar tothose of the associated non-invasivetumour. One or more foci may be pres-ent; none should exceed 10 mm2.
SynonymsSerous tumour of low malignant potentialwith microinvasion, serous tumour of bor-derline malignancy with microinvasion.
EpidemiologyP resent in about 10-15% of SBTs ,microinvasion occurs in women rangingin age from 17-83 years with a medianage of 34.5 years {203,2867}.
Clinical featuresMost symptomatic women present with apelvic mass or pain. About 28% of the 39women in the 2 major series were pre g-nant at the time of presentation {203,2867}.
MacroscopyThe macroscopic features are similar tothose of SBT without microinvasion.
Tumour spread and stagingAt presentation about 60% of the neo-plasms are stage IA, 13% stage 1B, 5%stage IC, 8% stage IIC, 10% stage III(mostly IIIC) and 2.5% stage IV (livermetastases).
HistopathologyThe hallmark of serous borderline tumourswith microinvasion is the presence withinthe tumour stroma of single cells and cellclusters with generally abundant eosino-philic cytoplasm morphologically identicalto those of the adjacent non-invasive tu-m o u r. The microinvasive foci form micro-p a p i l l a ry, solid or rarely cribriform arrange-ments without or with only minimal stro m a lor cellular reaction. These cells are often
- Epithelial hyperplasia in the form of stratifi-cation, tufting, cribriform and micropapillaryarrangements
- Atypia (usually mild to moderate)- Detached cell clusters- Variable and usually minimal mitotic activity- Absence of destructive stromal invasion
Table 2.01Histological criteria for the diagnosis of serousborderline tumours.
Fig. 2.05 Serous borderline tumour. The sectionedsurface shows a solid and cystic neoplasm withnumerous papillary excrescences.
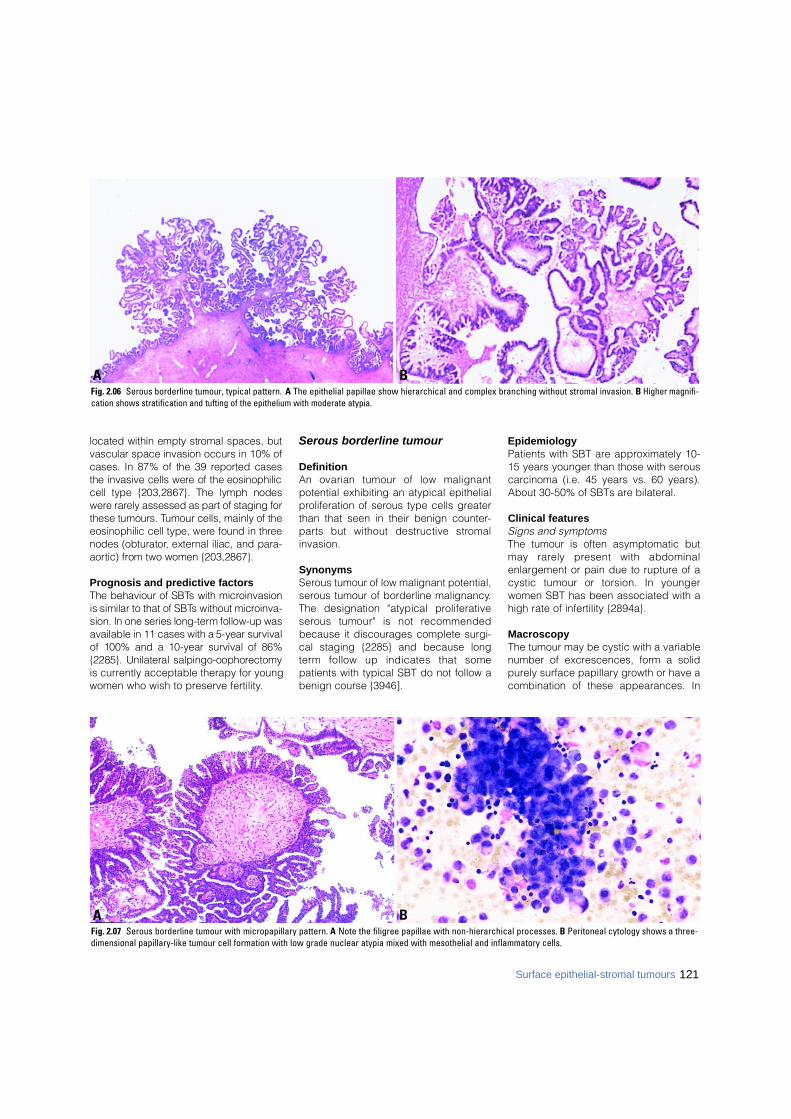
121Surface epithelial-stromal tumours
located within empty stromal spaces, butvascular space invasion occurs in 10% ofcases. In 87% of the 39 re p o rted casesthe invasive cells were of the eosinophiliccell type {203,2867}. The lymph nodesw e re rarely assessed as part of staging forthese tumours. Tumour cells, mainly of theeosinophilic cell type, were found in thre enodes (obturator, external iliac, and para-a o rtic) from two women {203,2867}.
Prognosis and predictive factorsThe behaviour of SBTs with micro i n v a s i o nis similar to that of SBTs without micro i n v a-sion. In one series long-term follow-up wasavailable in 11 cases with a 5-year survivalof 100% and a 10-year survival of 86%{2285}. Unilateral salpingo-oophore c t o m yis currently acceptable therapy for youngwomen who wish to preserve fertility.
Serous borderline tumour
DefinitionAn ovarian tumour of low malignantpotential exhibiting an atypical epithelialproliferation of serous type cells greaterthan that seen in their benign counter-p a rts but without destructive stro m a linvasion.
SynonymsSerous tumour of low malignant potential,serous tumour of borderline malignancy.The designation "atypical pro l i f e r a t i v es e rous tumour" is not re c o m m e n d e dbecause it discourages complete surgi-cal staging {2285} and because longt e rm follow up indicates that somepatients with typical SBT do not follow abenign course {3946].
EpidemiologyPatients with SBT are approximately 10-15 years younger than those with serouscarcinoma (i.e. 45 years vs. 60 years).About 30-50% of SBTs are bilateral.
Clinical features Signs and symptomsThe tumour is often asymptomatic butmay rarely present with abdominalenlargement or pain due to rupture of acystic tumour or torsion. In youngerwomen SBT has been associated with ahigh rate of infertility {2894a}.
MacroscopyThe tumour may be cystic with a variablenumber of excrescences, form a solidpurely surface papillary growth or have acombination of these appearances. In
BAFig. 2.07 Serous borderline tumour with micropapillary pattern. A Note the filigree papillae with non-hierarchical processes. B Peritoneal cytology shows a three-dimensional papillary-like tumour cell formation with low grade nuclear atypia mixed with mesothelial and inflammatory cells.
BAFig. 2.06 Serous borderline tumour, typical pattern. A The epithelial papillae show hierarchical and complex branching without stromal invasion. B Higher magnifi-cation shows stratification and tufting of the epithelium with moderate atypia.
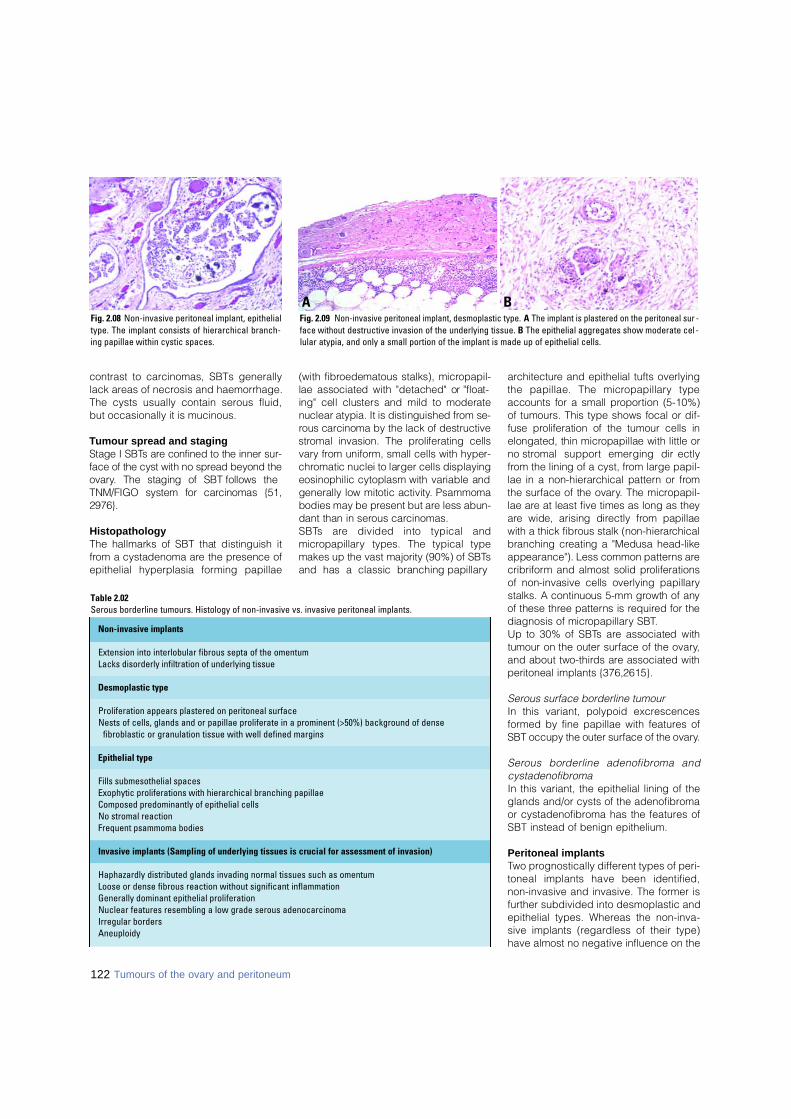
contrast to carcinomas, SBTs generallylack areas of necrosis and haemorrhage.The cysts usually contain serous fluid,but occasionally it is mucinous.
Tumour spread and stagingStage I SBTs are confined to the inner sur-face of the cyst with no spread beyond theo v a ry. The staging of SBT follows theTNM/FIGO system for carcinomas {51,2 9 7 6 } .
Histopathology The hallmarks of SBT that distinguish itf rom a cystadenoma are the presence ofepithelial hyperplasia forming papillae
(with fibroedematous stalks), micro p a p i l-lae associated with "detached" or "float-ing" cell clusters and mild to moderatenuclear atypia. It is distinguished from se-rous carcinoma by the lack of destructives t romal invasion. The proliferating cellsv a ry from uniform, small cells with hyper-c h romatic nuclei to larger cells displayingeosinophilic cytoplasm with variable andgenerally low mitotic activity. Psammomabodies may be present but are less abun-dant than in serous carc i n o m a s .S B Ts are divided into typical andm i c ro p a p i l l a ry types. The typical typemakes up the vast majority (90%) of SBTsand has a classic branching papillary
a rc h i t e c t u re and epithelial tufts overlyingthe papillae. The micro p a p i l l a ry typeaccounts for a small pro p o rtion (5-10%)of tumours. This type shows focal or dif-fuse proliferation of the tumour cells inelongated, thin micropapillae with little orno stromal support emerging dire c t l yf rom the lining of a cyst, from large papil-lae in a non-hierarchical pattern or fro mthe surface of the ovary. The micro p a p i l-lae are at least five times as long as theya re wide, arising directly from papillaewith a thick fibrous stalk (non-hierarc h i c a lbranching creating a "Medusa head-likeappearance"). Less common patterns arec r i b r i f o rm and almost solid pro l i f e r a t i o n sof non-invasive cells overlying papillarystalks. A continuous 5-mm growth of anyof these three patterns is re q u i red for thediagnosis of micro p a p i l l a ry SBT.Up to 30% of SBTs are associated withtumour on the outer surface of the ovary,and about two-thirds are associated withperitoneal implants {376,2615}.
Serous surface borderline tumourIn this variant, polypoid excrescencesformed by fine papillae with features ofSBT occupy the outer surface of the ovary.
S e rous borderline adenofibroma andcystadenofibromaIn this variant, the epithelial lining of theglands and/or cysts of the adenofibromaor cystadenofibroma has the features ofSBT instead of benign epithelium.
Peritoneal implantsTwo prognostically different types of peri-toneal implants have been identified,non-invasive and invasive. The former isfurther subdivided into desmoplastic andepithelial types. Whereas the non-inva-sive implants (regardless of their type)have almost no negative influence on the
122 Tumours of the ovary and peritoneum
Table 2.02Serous borderline tumours. Histology of non-invasive vs. invasive peritoneal implants.
Fig. 2.08 Non-invasive peritoneal implant, epithelialtype. The implant consists of hierarchical branch-ing papillae within cystic spaces.
BAFig. 2.09 Non-invasive peritoneal implant, desmoplastic type. A The implant is plastered on the peritoneal sur -face without destructive invasion of the underlying tissue. B The epithelial aggregates show moderate cel -lular atypia, and only a small portion of the implant is made up of epithelial cells.
Non-invasive implants
Extension into interlobular fibrous septa of the omentumLacks disorderly infiltration of underlying tissue
Desmoplastic type
Proliferation appears plastered on peritoneal surfaceNests of cells, glands and or papillae proliferate in a prominent (>50%) background of dense
fibroblastic or granulation tissue with well defined margins
Epithelial type
Fills submesothelial spacesExophytic proliferations with hierarchical branching papillaeComposed predominantly of epithelial cellsNo stromal reactionFrequent psammoma bodies
Invasive implants (Sampling of underlying tissues is crucial for assessment of invasion)
Haphazardly distributed glands invading normal tissues such as omentumLoose or dense fibrous reaction without significant inflammationGenerally dominant epithelial proliferationNuclear features resembling a low grade serous adenocarcinomaIrregular bordersAneuploidy
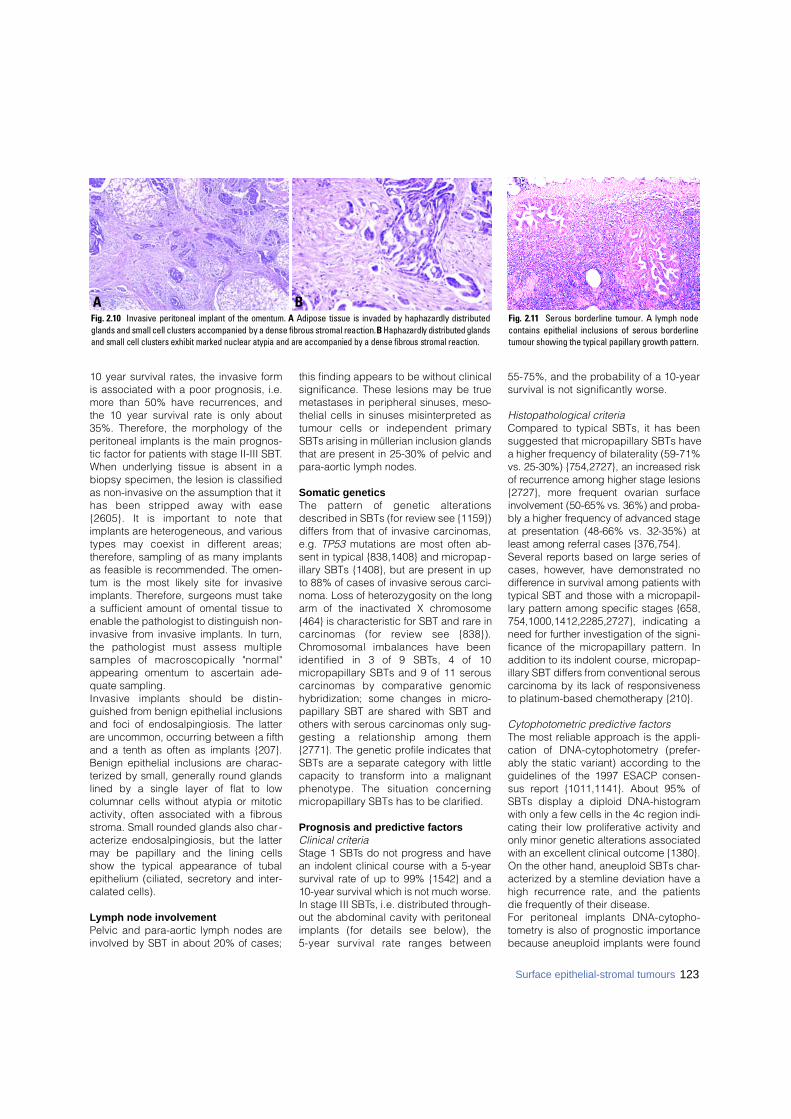
10 year survival rates, the invasive formis associated with a poor prognosis, i.e.more than 50% have recurrences, andthe 10 year survival rate is only about35%. Therefore, the morphology of theperitoneal implants is the main prognos-tic factor for patients with stage II-III SBT.When underlying tissue is absent in abiopsy specimen, the lesion is classifiedas non-invasive on the assumption that ithas been stripped away with ease{2605}. It is important to note thatimplants are heterogeneous, and varioustypes may coexist in diff e rent are a s ;therefore, sampling of as many implantsas feasible is recommended. The omen-tum is the most likely site for invasiveimplants. Therefore, surgeons must takea sufficient amount of omental tissue toenable the pathologist to distinguish non-invasive from invasive implants. In turn,the pathologist must assess multiplesamples of macroscopically "norm a l "appearing omentum to ascertain ade-quate sampling. Invasive implants should be distin-guished from benign epithelial inclusionsand foci of endosalpingiosis. The latterare uncommon, occurring between a fifthand a tenth as often as implants {207}.Benign epithelial inclusions are charac-terized by small, generally round glandslined by a single layer of flat to lowcolumnar cells without atypia or mitoticactivity, often associated with a fibrousstroma. Small rounded glands also char-acterize endosalpingiosis, but the lattermay be papillary and the lining cellsshow the typical appearance of tubalepithelium (ciliated, secretory and inter-calated cells).
Lymph node involvementPelvic and para-aortic lymph nodes areinvolved by SBT in about 20% of cases;
this finding appears to be without clinicalsignificance. These lesions may be truemetastases in peripheral sinuses, meso-thelial cells in sinuses misinterpreted astumour cells or independent primarySBTs arising in müllerian inclusion glandsthat are present in 25-30% of pelvic andpara-aortic lymph nodes.
Somatic genetics The pattern of genetic alterationsdescribed in SBTs (for review see {1159})differs from that of invasive carcinomas,e.g. TP53 mutations are most often ab-sent in typical {838,1408} and micropap-illary SBTs {1408}, but are present in upto 88% of cases of invasive serous carci-noma. Loss of heterozygosity on the longarm of the inactivated X chromosome{464} is characteristic for SBT and rare inc a rcinomas (for review see {838}).C h romosomal imbalances have beenidentified in 3 of 9 SBTs, 4 of 10micropapillary SBTs and 9 of 11 serousc a rcinomas by comparative genomichybridization; some changes in micro-papillary SBT are shared with SBT andothers with serous carcinomas only sug-gesting a relationship among them{2771}. The genetic profile indicates thatSBTs are a separate category with littlecapacity to transform into a malignantphenotype. The situation concern i n gmicropapillary SBTs has to be clarified.
Prognosis and predictive factorsClinical criteriaStage 1 SBTs do not pro g ress and havean indolent clinical course with a 5-yearsurvival rate of up to 99% {1542} and a10-year survival which is not much worse.In stage III SBTs, i.e. distributed thro u g h-out the abdominal cavity with peritonealimplants (for details see below), the 5-year survival rate ranges between
55-75%, and the probability of a 10-yearsurvival is not significantly worse.
Histopathological criteriaCompared to typical SBTs, it has beensuggested that micropapillary SBTs havea higher frequency of bilaterality (59-71%vs. 25-30%) {754,2727}, an increased riskof re c u r rence among higher stage lesions{ 2 7 2 7 }, m o re frequent ovarian surf a c einvolvement (50-65% vs. 36%) and pro b a-bly a higher frequency of advanced stageat presentation (48-66% vs. 32-35%) atleast among referral cases {376,754}.Several re p o rts based on large series ofcases, however, have demonstrated nod i ff e rence in survival among patients withtypical SBT and those with a micro p a p i l-l a ry pattern among specific stages {658,754,1000,1412,2285,2727}, indicating aneed for further investigation of the signi-ficance of the micro p a p i l l a ry pattern. Inaddition to its indolent course, micro p a p-i l l a ry SBT differs from conventional sero u sc a rcinoma by its lack of re s p o n s i v e n e s sto platinum-based chemotherapy {210}.
Cytophotometric predictive factorsThe most reliable approach is the appli-cation of DNA-cytophotometry (prefer-ably the static variant) according to theguidelines of the 1997 ESACP consen-sus report {1011,1141}. About 95% ofSBTs display a diploid DNA-histogramwith only a few cells in the 4c region indi-cating their low proliferative activity andonly minor genetic alterations associatedwith an excellent clinical outcome {1380}.On the other hand, aneuploid SBTs char-acterized by a stemline deviation have ahigh recurrence rate, and the patientsdie frequently of their disease.For peritoneal implants DNA-cytopho-tometry is also of prognostic importancebecause aneuploid implants were found
Fig. 2.11 Serous borderline tumour. A lymph nodecontains epithelial inclusions of serous borderlinetumour showing the typical papillary growth pattern.
BAFig. 2.10 Invasive peritoneal implant of the omentum. A Adipose tissue is invaded by haphazardly distributedglands and small cell clusters accompanied by a dense fibrous stromal reaction. B Haphazardly distributed glandsand small cell clusters exhibit marked nuclear atypia and are accompanied by a dense fibrous stromal reaction.
123Surface epithelial-stromal tumours
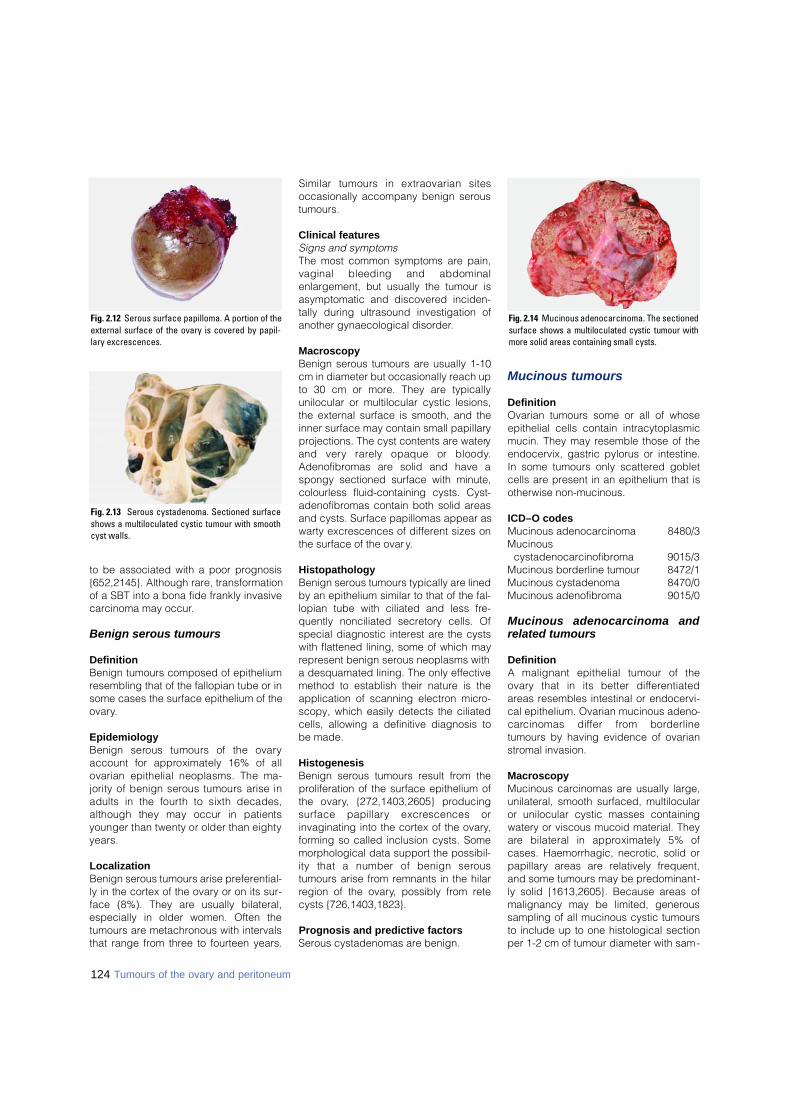
124 Tumours of the ovary and peritoneum
to be associated with a poor prognosis{652,2145}. Although rare, transformationof a SBT into a bona fide frankly invasivecarcinoma may occur.
Benign serous tumours
DefinitionBenign tumours composed of epitheliumresembling that of the fallopian tube or insome cases the surface epithelium of theovary.
EpidemiologyBenign serous tumours of the ovaryaccount for approximately 16% of allovarian epithelial neoplasms. The ma-jority of benign serous tumours arise inadults in the fourth to sixth decades,although they may occur in patientsyounger than twenty or older than eightyy e a r s .
LocalizationBenign serous tumours arise preferential-ly in the cortex of the ovary or on its sur-face (8%). They are usually bilateral,especially in older women. Often thetumours are metachronous with intervalsthat range from three to fourteen years.
Similar tumours in extraovarian sitesoccasionally accompany benign seroustumours.
Clinical featuresSigns and symptomsThe most common symptoms are pain,vaginal bleeding and abdominalenlargement, but usually the tumour isasymptomatic and discovered inciden-tally during ultrasound investigation ofanother gynaecological disorder.
Macroscopy Benign serous tumours are usually 1-10cm in diameter but occasionally reach upto 30 cm or more. They are typicallyunilocular or multilocular cystic lesions,the external surface is smooth, and theinner surface may contain small papillaryprojections. The cyst contents are wateryand very rarely opaque or bloody.Adenofibromas are solid and have aspongy sectioned surface with minute,colourless fluid-containing cysts. Cyst-adenofibromas contain both solid areasand cysts. Surface papillomas appear aswarty excrescences of different sizes onthe surface of the ovary.
HistopathologyBenign serous tumours typically are linedby an epithelium similar to that of the fal-lopian tube with ciliated and less fre-quently nonciliated secretory cells. Ofspecial diagnostic interest are the cystswith flattened lining, some of which mayrepresent benign serous neoplasms witha desquamated lining. The only effectivemethod to establish their nature is theapplication of scanning electron micro-scopy, which easily detects the ciliatedcells, allowing a definitive diagnosis tobe made.
HistogenesisBenign serous tumours result from theproliferation of the surface epithelium ofthe ovary, {272,1403,2605} pro d u c i n gs u rface papillary excrescences orinvaginating into the cortex of the ovary,forming so called inclusion cysts. Somemorphological data support the possibil-ity that a number of benign sero u stumours arise from remnants in the hilarregion of the ovary, possibly from retecysts {726,1403,1823}.
Prognosis and predictive factorsSerous cystadenomas are benign.
Mucinous tumours
DefinitionOvarian tumours some or all of whoseepithelial cells contain intracytoplasmicmucin. They may resemble those of theendocervix, gastric pylorus or intestine.In some tumours only scattered gobletcells are present in an epithelium that isotherwise non-mucinous.
ICD–O codesMucinous adenocarcinoma 8480/3Mucinous
cystadenocarcinofibroma 9015/3Mucinous borderline tumour 8472/1Mucinous cystadenoma 8470/0Mucinous adenofibroma 9015/0
Mucinous adenocarcinoma andrelated tumours
DefinitionA malignant epithelial tumour of theo v a ry that in its better diff e re n t i a t e dareas resembles intestinal or endocervi-cal epithelium. Ovarian mucinous adeno-c a rcinomas differ from bord e r l i n etumours by having evidence of ovarianstromal invasion.
MacroscopyMucinous carcinomas are usually large,unilateral, smooth surfaced, multilocularor unilocular cystic masses containingwatery or viscous mucoid material. Theya re bilateral in approximately 5% ofcases. Haemorrhagic, necrotic, solid orpapillary areas are relatively frequent,and some tumours may be predominant-ly solid {1613,2605}. Because areas ofmalignancy may be limited, generoussampling of all mucinous cystic tumoursto include up to one histological sectionper 1-2 cm of tumour diameter with sam-
Fig. 2.14 Mucinous adenocarcinoma. The sectionedsurface shows a multiloculated cystic tumour withmore solid areas containing small cysts.
Fig. 2.12 Serous surface papilloma. A portion of theexternal surface of the ovary is covered by papil-lary excrescences.
Fig. 2.13 Serous cystadenoma. Sectioned surfaceshows a multiloculated cystic tumour with smoothcyst walls.
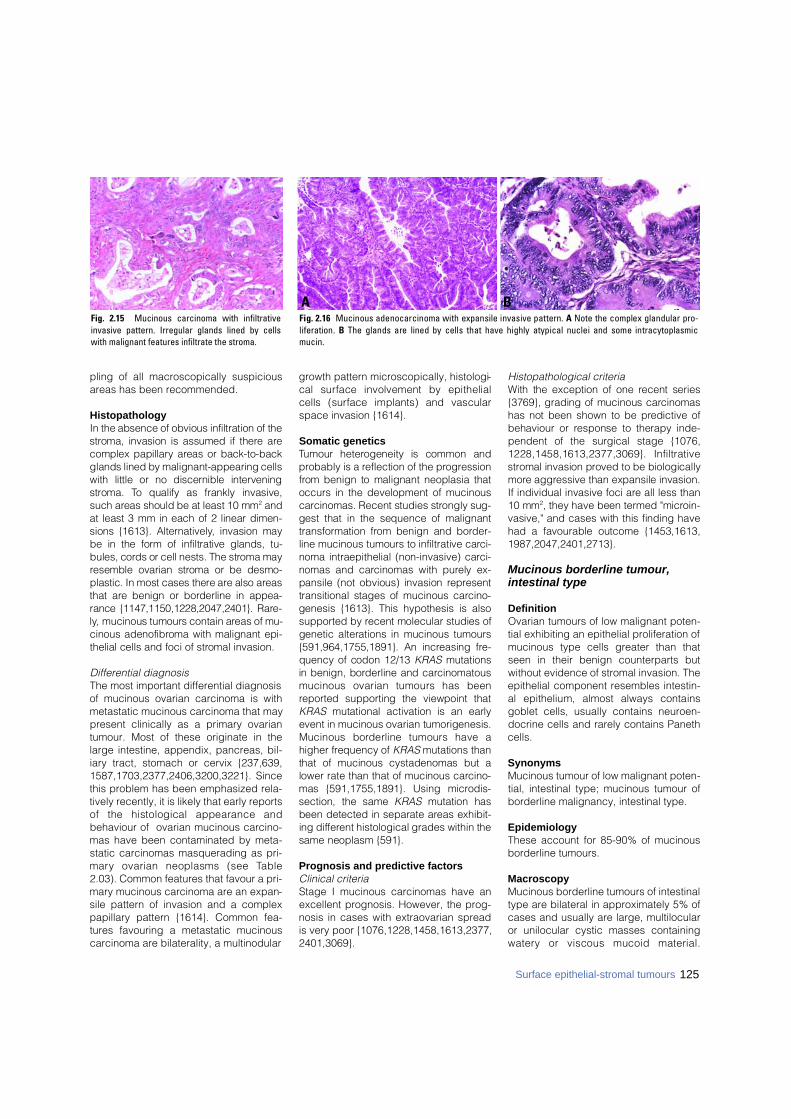
pling of all macroscopically suspiciousareas has been recommended.
HistopathologyIn the absence of obvious infiltration of thes t roma, invasion is assumed if there arecomplex papillary areas or back-to-backglands lined by malignant-appearing cellswith little or no discernible intervenings t roma. To qualify as frankly invasive,such areas should be at least 10 mm2 a n dat least 3 mm in each of 2 linear dimen-sions {1613}. Altern a t i v e l y, invasion maybe in the form of infiltrative glands, tu-bules, cords or cell nests. The stroma mayresemble ovarian stroma or be desmo-plastic. In most cases there are also are a sthat are benign or borderline in a p p e a-rance {1147,1150,1228,2047,2401}. R a re-l y, mucinous tumours contain areas of mu-cinous adenofibroma with malignant epi-thelial cells and foci of stromal invasion.
Differential diagnosisThe most important differential diagnosisof mucinous ovarian carcinoma is withmetastatic mucinous carcinoma that maypresent clinically as a primary ovariantumour. Most of these originate in thelarge intestine, appendix, pancreas, bil-iary tract, stomach or cervix {237,639,1587,1703,2377,2406,3200,3221}. Sincethis problem has been emphasized rela-tively recently, it is likely that early reportsof the histological appearance andbehaviour of ovarian mucinous carcino-mas have been contaminated by meta-static carcinomas masquerading as pri-m a ry ovarian neoplasms (see Ta b l e2.03). Common features that favour a pri-mary mucinous carcinoma are an expan-sile pattern of invasion and a complexpapillary pattern {1614}. Common fea-tures favouring a metastatic mucinouscarcinoma are bilaterality, a multinodular
growth pattern microscopically, histologi-cal surface involvement by epithelialcells (surface implants) and vascularspace invasion {1614}.
Somatic genetics Tumour heterogeneity is common andp robably is a reflection of the pro g re s s i o nf rom benign to malignant neoplasia thatoccurs in the development of mucinousc a rc i n o m a s. Recent studies strongly sug-gest that in the sequence of malignantt r a n s f o rmation from benign and bord e r-line mucinous tumours to infiltrative carc i-noma intraepithelial (non-invasive) carc i-nomas and carcinomas with purely ex-pansile (not obvious) invasion re p re s e n ttransitional stages of mucinous carc i n o-genesis {1613}. This hypothesis is a l s os u p p o rted by recent molecular studies ofgenetic alterations in mucinous t u m o u r s{591,964,1755,1891}. An increasing fre-quency of codon 12/13 K R A S m u t a t i o n sin benign, borderline and carc i n o m a t o u smucinous ovarian tumours has beenre p o rted supporting the viewpoint thatK R A S mutational activation is an earlyevent in mucinous ovarian tumorigenesis.Mucinous borderline tumours have ahigher frequency of K R A S mutations thanthat of mucinous cystadenomas but alower rate than that of mucinous carc i n o-mas {591,1755,1891}. Using micro d i s-section, the same K R A S mutation hasbeen detected in separate areas exhibit-ing diff e rent histological grades within thesame neoplasm {591}.
Prognosis and predictive factorsClinical criteriaStage I mucinous carcinomas have anexcellent prognosis. However, the prog-nosis in cases with extraovarian spreadis very poor {1076,1228,1458,1613,2377,2401,3069}.
Histopathological criteriaWith the exception of one recent series{3769}, grading of mucinous carc i n o m a shas not been shown to be predictive ofbehaviour or response to therapy inde-pendent of the surgical stage {1076,1228,1458,1613,2377,3069}. Infiltratives t romal invasion proved to be biologicallym o re aggressive than expansile invasion.If individual invasive foci are all less than10 mm2, they have been termed "micro i n-vasive," and cases with this finding havehad a favourable outcome {1453,1613,1 9 8 7 , 2 0 4 7 , 2 4 0 1 , 2 7 1 3 } .
Mucinous borderline tumour,intestinal type
DefinitionOvarian tumours of low malignant poten-tial exhibiting an epithelial proliferation ofmucinous type cells greater than thatseen in their benign counterparts butwithout evidence of stromal invasion. Theepithelial component resembles intestin-al epithelium, almost always containsgoblet cells, usually contains neuroen-docrine cells and rarely contains Panethcells.
SynonymsMucinous tumour of low malignant poten-tial, intestinal type; mucinous tumour ofborderline malignancy, intestinal type.
EpidemiologyThese account for 85-90% of mucinousborderline tumours.
MacroscopyMucinous borderline tumours of intestinaltype are bilateral in approximately 5% ofcases and usually are large, multilocularor unilocular cystic masses containingw a t e ry or viscous mucoid material.
BAFig. 2.16 Mucinous adenocarcinoma with expansile invasive pattern. A Note the complex glandular pro-liferation. B The glands are lined by cells that have highly atypical nuclei and some intracytoplasmicm u c i n .
Fig. 2.15 Mucinous carcinoma with infiltrativeinvasive pattern. Irregular glands lined by cellswith malignant features infiltrate the stroma.
125Surface epithelial-stromal tumours
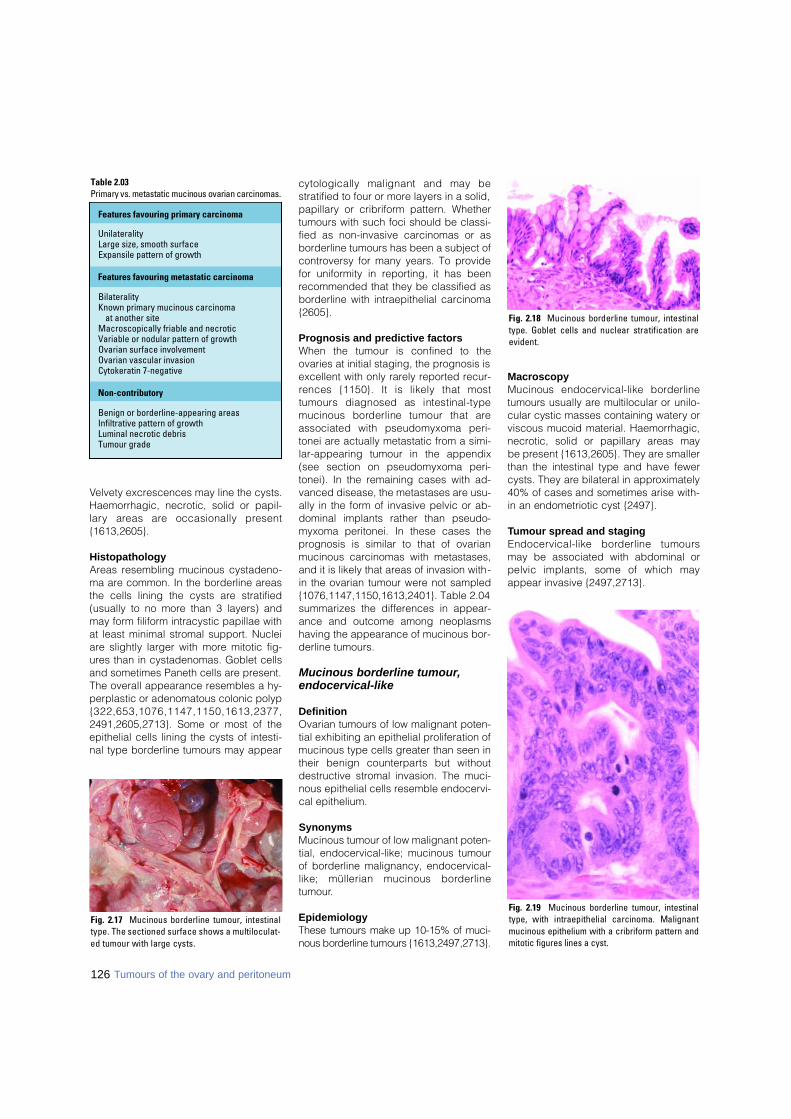
Velvety excrescences may line the cysts.Haemorrhagic, necrotic, solid or papil-l a ry areas are occasionally pre s e n t{1613,2605}.
HistopathologyAreas resembling mucinous cystadeno-ma are common. In the borderline areasthe cells lining the cysts are stratified(usually to no more than 3 layers) andmay form filiform intracystic papillae withat least minimal stromal support. Nucleiare slightly larger with more mitotic fig-ures than in cystadenomas. Goblet cellsand sometimes Paneth cells are present.The overall appearance resembles a hy-perplastic or adenomatous colonic polyp{ 3 2 2 , 6 5 3 , 1 0 7 6 , 1 1 4 7 , 1 1 5 0 , 1 6 1 3 , 2 3 7 7 ,2491,2605,2713}. Some or most of theepithelial cells lining the cysts of intesti-nal type borderline tumours may appear
cytologically malignant and may bestratified to four or more layers in a solid,papillary or cribriform pattern. Whethertumours with such foci should be classi-fied as non-invasive carcinomas or asborderline tumours has been a subject ofcontroversy for many years. To providefor uniformity in reporting, it has beenrecommended that they be classified asborderline with intraepithelial carcinoma{2605}.
Prognosis and predictive factorsWhen the tumour is confined to theovaries at initial staging, the prognosis isexcellent with only rarely reported recur-rences {1150}. It is likely that mosttumours diagnosed as intestinal-typemucinous borderline tumour that areassociated with pseudomyxoma peri-tonei are actually metastatic from a simi-lar-appearing tumour in the appendix(see section on pseudomyxoma peri-tonei). In the remaining cases with ad-vanced disease, the metastases are usu-ally in the form of invasive pelvic or ab-dominal implants rather than pseudo-myxoma peritonei. In these cases theprognosis is similar to that of ovarianmucinous carcinomas with metastases,and it is likely that areas of invasion with-in the ovarian tumour were not sampled{1076,1147,1150,1613,2401}. Table 2.04summarizes the differences in appear-ance and outcome among neoplasmshaving the appearance of mucinous bor-derline tumours.
Mucinous borderline tumour,endocervical-like
DefinitionOvarian tumours of low malignant poten-tial exhibiting an epithelial proliferation ofmucinous type cells greater than seen intheir benign counterparts but withoutdestructive stromal invasion. The muci-nous epithelial cells resemble endocervi-cal epithelium.
SynonymsMucinous tumour of low malignant poten-tial, endocervical-like; mucinous tumourof borderline malignancy, endocervical-like; müllerian mucinous bord e r l i n etumour.
EpidemiologyThese tumours make up 10-15% of muci-nous borderline tumours {1613,2497,2713}.
MacroscopyMucinous endocervical-like bord e r l i n etumours usually are multilocular or unilo-cular cystic masses containing watery orviscous mucoid material. Haemorrhagic,n e c rotic, solid or papillary areas may be present {1613,2605}. They are smallerthan the intestinal type and have fewercysts. They are bilateral in appro x i m a t e l y40% of cases and sometimes arise with-in an endometriotic cyst {2497}.
Tumour spread and stagingEndocervical-like borderline tumoursmay be associated with abdominal orpelvic implants, some of which mayappear invasive {2497,2713}.
Fig. 2.17 Mucinous borderline tumour, intestinaltype. The sectioned surface shows a multiloculat-ed tumour with large cysts.
126 Tumours of the ovary and peritoneum
Table 2.03 Primary vs. metastatic mucinous ovarian carcinomas.
Features favouring primary carcinoma
UnilateralityLarge size, smooth surfaceExpansile pattern of growth
Features favouring metastatic carcinoma
BilateralityKnown primary mucinous carcinoma
at another siteMacroscopically friable and necroticVariable or nodular pattern of growthOvarian surface involvementOvarian vascular invasionCytokeratin 7-negative
Non-contributory
Benign or borderline-appearing areasInfiltrative pattern of growthLuminal necrotic debrisTumour grade
Fig. 2.18 Mucinous borderline tumour, intestinaltype. Goblet cells and nuclear stratification aree v i d e n t .
Fig. 2.19 Mucinous borderline tumour, intestinaltype, with intraepithelial carcinoma. Malignantmucinous epithelium with a cribriform pattern andmitotic figures lines a cyst.
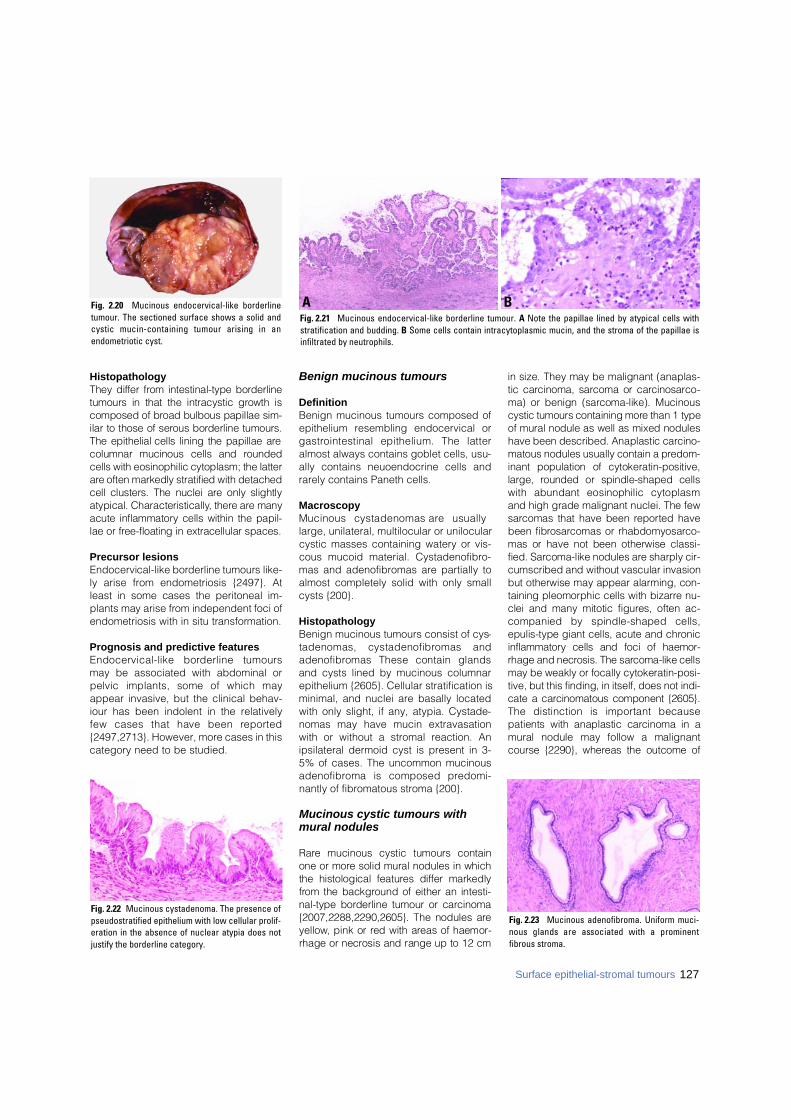
HistopathologyThey differ from intestinal-type bord e r l i n etumours in that the intracystic growth iscomposed of broad bulbous papillae sim-ilar to those of serous borderline tumours.The epithelial cells lining the papillae arecolumnar mucinous cells and ro u n d e dcells with eosinophilic cytoplasm; the lattera re often markedly stratified with detachedcell clusters. The nuclei are only slightlyatypical. Characteristically, there are manyacute inflammatory cells within the papil-lae or free-floating in extracellular spaces.
Precursor lesionsEndocervical-like borderline tumours like-ly arise from endometriosis {2497}. Atleast in some cases the peritoneal im-plants may arise from independent foci ofendometriosis with in situ transform a t i o n .
Prognosis and predictive featuresEndocervical-like borderline tumoursmay be associated with abdominal orpelvic implants, some of which mayappear invasive, but the clinical behav-iour has been indolent in the relativelyfew cases that have been re p o rt e d{2497,2713}. However, more cases in thiscategory need to be studied.
Benign mucinous tumours
DefinitionBenign mucinous tumours composed ofepithelium resembling endocervical org a s t rointestinal epithelium. The latteralmost always contains goblet cells, usu-ally contains neuoendocrine cells andrarely contains Paneth cells.
MacroscopyMucinous cystadenomas are usuallylarge, unilateral, multilocular or unilocularcystic masses containing watery or vis-cous mucoid material. Cystadenofibro-mas and adenofibromas are partially toalmost completely solid with only smallcysts {200}.
HistopathologyBenign mucinous tumours consist of cys-tadenomas, cystadenofibromas anda d e n o f i b romas These contain glandsand cysts lined by mucinous columnarepithelium {2605}. Cellular stratification isminimal, and nuclei are basally locatedwith only slight, if any, atypia. Cystade-nomas may have mucin extravasationwith or without a stromal reaction. Anipsilateral dermoid cyst is present in 3-5% of cases. The uncommon mucinousa d e n o f i b roma is composed pre d o m i-nantly of fibromatous stroma {200}.
Mucinous cystic tumours withmural nodules
R a re mucinous cystic tumours containone or more solid mural nodules in whichthe histological features differ markedlyf rom the background of either an intesti-nal-type borderline tumour or carc i n o m a{2007,2288,2290,2605}. The nodules arey e l l o w, pink or red with areas of haemor-rhage or necrosis and range up to 12 cm
in size. They may be malignant (anaplas-tic carcinoma, sarcoma or carc i n o s a rc o-ma) or benign (sarcoma-like). Mucinouscystic tumours containing more than 1 typeof mural nodule as well as mixed noduleshave been described. Anaplastic carc i n o-matous nodules usually contain a pre d o m-inant population of cytokeratin-positive,large, rounded or spindle-shaped cellswith abundant eosinophilic cytoplasmand high grade malignant nuclei. The fews a rcomas that have been re p o rted havebeen fibro s a rcomas or rhabdomyosarc o-mas or have not been otherwise classi-fied. Sarcoma-like nodules are sharply cir-cumscribed and without vascular invasionbut otherwise may appear alarming, con-taining pleomorphic cells with bizarre nu-clei and many mitotic figures, often ac-companied by spindle-shaped cells,epulis-type giant cells, acute and chro n i ci n f l a m m a t o ry cells and foci of haemor-rhage and necrosis. The sarcoma-like cellsmay be weakly or focally cytokeratin-posi-tive, but this finding, in itself, does not i n d i-cate a carcinomatous component {2605}.The distinction is important becausepatients with anaplastic carcinoma in amural nodule may follow a malignantcourse {2290}, whereas the outcome of
Fig. 2.20 Mucinous endocervical-like borderlinetumour. The sectioned surface shows a solid andcystic mucin-containing tumour arising in anendometriotic cyst.
Fig. 2.23 Mucinous adenofibroma. Uniform muci-nous glands are associated with a prominentfibrous stroma.
Fig. 2.22 Mucinous cystadenoma. The presence ofpseudostratified epithelium with low cellular prolif-eration in the absence of nuclear atypia does notjustify the borderline category.
BAFig. 2.21 Mucinous endocervical-like borderline tumour. A Note the papillae lined by atypical cells withstratification and budding. B Some cells contain intracytoplasmic mucin, and the stroma of the papillae isinfiltrated by neutrophils.
127Surface epithelial-stromal tumours
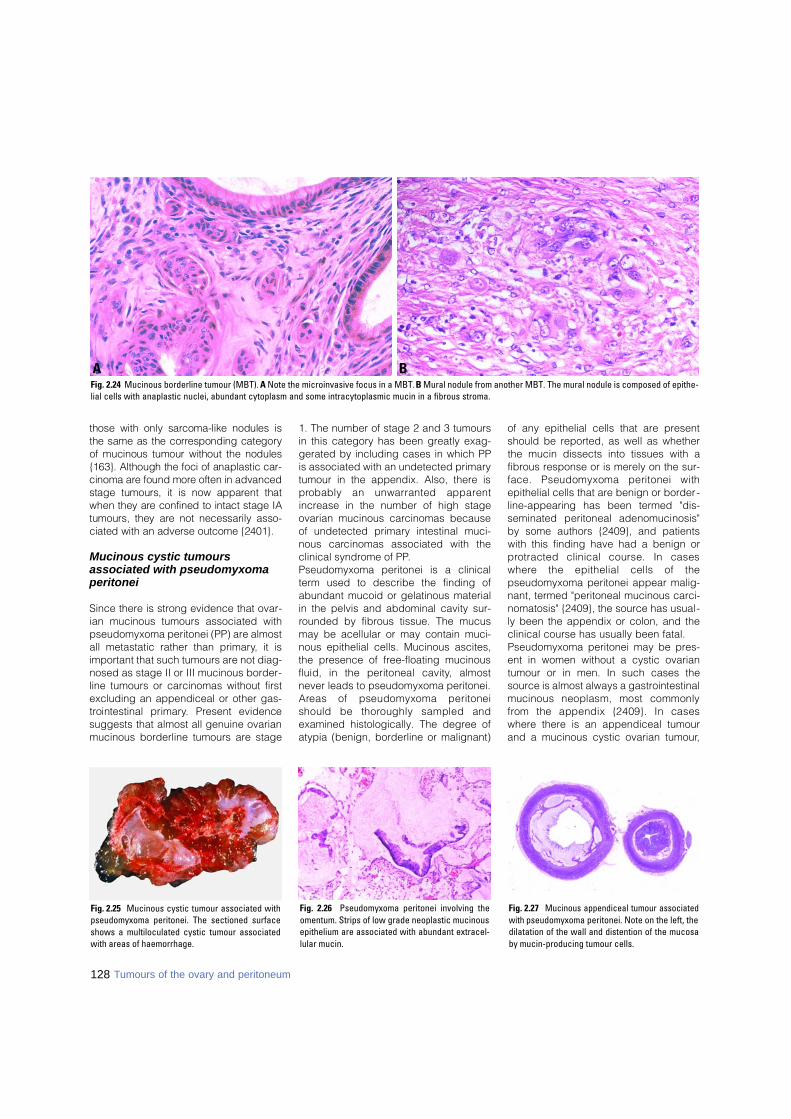
those with only sarcoma-like nodules isthe same as the corresponding categoryof mucinous tumour without the nodules{163}. Although the foci of anaplastic car-cinoma are found more often in advancedstage tumours, it is now apparent thatwhen they are confined to intact stage IAtumours, they are not necessarily asso-ciated with an adverse outcome {2401}.
Mucinous cystic tumours associated with pseudomyxomaperitonei
Since there is strong evidence that ovar-ian mucinous tumours associated withpseudomyxoma peritonei (PP) are almostall metastatic rather than primary, it isimportant that such tumours are not diag-nosed as stage II or III mucinous border-line tumours or carcinomas without firstexcluding an appendiceal or other gas-t rointestinal primary. Present evidencesuggests that almost all genuine ovarianmucinous borderline tumours are stage
1. The number of stage 2 and 3 tumoursin this category has been greatly exag-gerated by including cases in which PPis associated with an undetected primarytumour in the appendix. Also, there isp robably an unwarranted appare n tincrease in the number of high stageovarian mucinous carcinomas becauseof undetected primary intestinal muci-nous carcinomas associated with theclinical syndrome of PP.Pseudomyxoma peritonei is a clinicalterm used to describe the finding ofabundant mucoid or gelatinous materialin the pelvis and abdominal cavity sur-rounded by fibrous tissue. The mucusmay be acellular or may contain muci-nous epithelial cells. Mucinous ascites,the presence of free-floating mucinousfluid, in the peritoneal cavity, almostnever leads to pseudomyxoma peritonei.A reas of pseudomyxoma peritoneishould be thoroughly sampled andexamined histologically. The degree ofatypia (benign, borderline or malignant)
of any epithelial cells that are presentshould be reported, as well as whetherthe mucin dissects into tissues with afibrous response or is merely on the sur-face. Pseudomyxoma peritonei withepithelial cells that are benign or border-line-appearing has been termed "dis-seminated peritoneal adenomucinosis"by some authors {2409}, and patientswith this finding have had a benign orp rotracted clinical course. In casesw h e re the epithelial cells of thepseudomyxoma peritonei appear malig-nant, termed "peritoneal mucinous carci-nomatosis" {2409}, the source has usual-ly been the appendix or colon, and theclinical course has usually been fatal.Pseudomyxoma peritonei may be pres-ent in women without a cystic ovariantumour or in men. In such cases thesource is almost always a gastrointestinalmucinous neoplasm, most commonlyf rom the appendix {2409}. In caseswhere there is an appendiceal tumourand a mucinous cystic ovarian tumour,
BAFig. 2.24 Mucinous borderline tumour (MBT). A Note the microinvasive focus in a MBT. B Mural nodule from another MBT. The mural nodule is composed of epithe-lial cells with anaplastic nuclei, abundant cytoplasm and some intracytoplasmic mucin in a fibrous stroma.
Fig. 2.26 Pseudomyxoma peritonei involving theomentum. Strips of low grade neoplastic mucinousepithelium are associated with abundant extracel-lular mucin.
Fig. 2.25 Mucinous cystic tumour associated withpseudomyxoma peritonei. The sectioned surfaceshows a multiloculated cystic tumour associatedwith areas of haemorrhage.
Fig. 2.27 Mucinous appendiceal tumour associatedwith pseudomyxoma peritonei. Note on the left, thedilatation of the wall and distention of the mucosaby mucin-producing tumour cells.
128 Tumours of the ovary and peritoneum
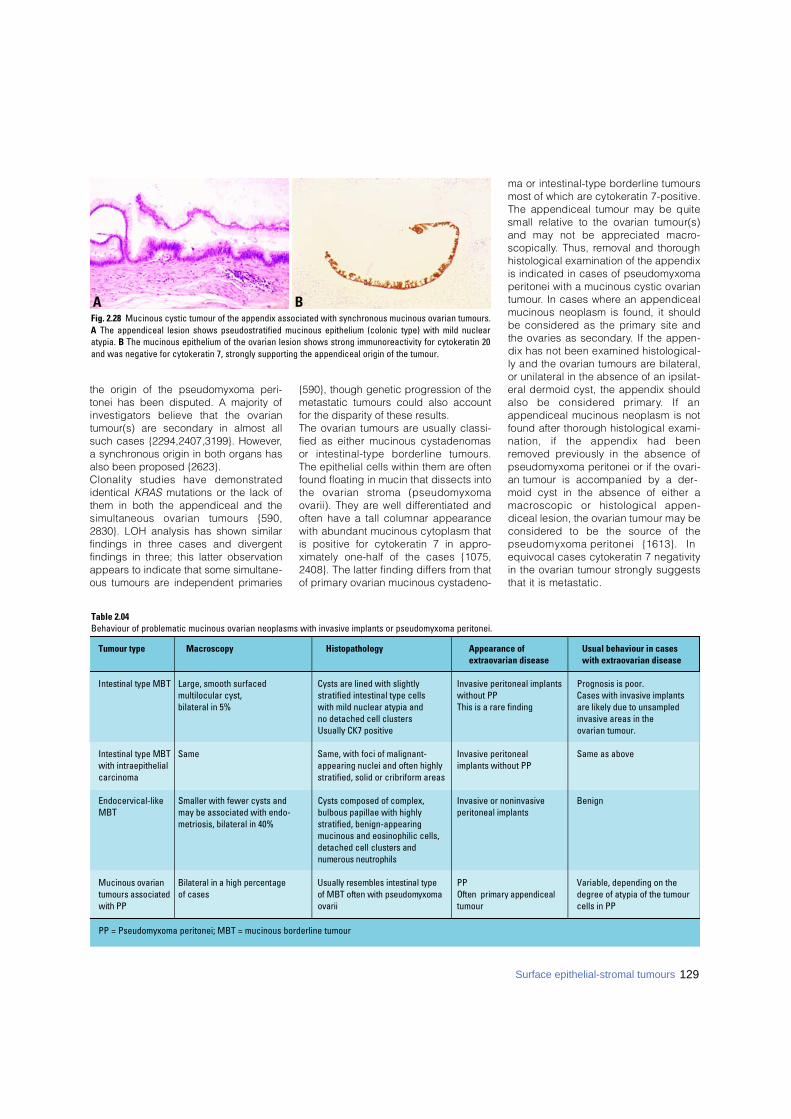
the origin of the pseudomyxoma peri-tonei has been disputed. A majority ofinvestigators believe that the ovariantumour(s) are secondary in almost allsuch cases {2294,2407,3199}. However,a synchronous origin in both organs hasalso been proposed {2623}. Clonality studies have demonstratedidentical KRAS mutations or the lack ofthem in both the appendiceal and thesimultaneous ovarian tumours {590,2830}. LOH analysis has shown similarfindings in three cases and divergentfindings in three; this latter observationappears to indicate that some simultane-ous tumours are independent primaries
{590}, though genetic progression of themetastatic tumours could also accountfor the disparity of these results.The ovarian tumours are usually classi-fied as either mucinous cystadenomasor intestinal-type borderline tumours.The epithelial cells within them are oftenfound floating in mucin that dissects intothe ovarian stroma (pseudomyxomaovarii). They are well diff e rentiated andoften have a tall columnar appearancewith abundant mucinous cytoplasm thatis positive for cytokeratin 7 in appro-ximately one-half of the cases {1075,2408}. The latter finding differs from thatof primary ovarian mucinous cystadeno-
ma or intestinal-type borderline tumoursmost of which are cytokeratin 7-positive.The appendiceal tumour may be quitesmall relative to the ovarian tumour(s)and may not be appreciated macro-s c o p i c a l l y. Thus, removal and thoro u g hhistological examination of the appendixis indicated in cases of pseudomyxomaperitonei with a mucinous cystic ovariant u m o u r. In cases where an appendicealmucinous neoplasm is found, it shouldbe considered as the primary site andthe ovaries as secondary. If the appen-dix has not been examined histological-ly and the ovarian tumours are bilateral,or unilateral in the absence of an ipsilat-eral dermoid cyst, the appendix shouldalso be considered primary. If anappendiceal mucinous neoplasm is notfound after thorough histological exami-nation, if the appendix had beenremoved previously in the absence ofpseudomyxoma peritonei or if the ovari-an tumour is accompanied by a der-moid cyst in the absence of either am a c roscopic or histological appen-diceal lesion, the ovarian tumour may bec o n s i d e red to be the source of thepseudomyxoma peritonei {1613}. Inequivocal cases cytokeratin 7 negativityin the ovarian tumour strongly suggeststhat it is metastatic.
129Surface epithelial-stromal tumours
BAFig. 2.28 Mucinous cystic tumour of the appendix associated with synchronous mucinous ovarian tumours.A The appendiceal lesion shows pseudostratified mucinous epithelium (colonic type) with mild nuclearatypia. B The mucinous epithelium of the ovarian lesion shows strong immunoreactivity for cytokeratin 20and was negative for cytokeratin 7, strongly supporting the appendiceal origin of the tumour.
Table 2.04Behaviour of problematic mucinous ovarian neoplasms with invasive implants or pseudomyxoma peritonei.
Tumour type Macroscopy Histopathology Appearance of Usual behaviour in casesextraovarian disease with extraovarian disease
Intestinal type MBT Large, smooth surfaced Cysts are lined with slightly Invasive peritoneal implants Prognosis is poor. multilocular cyst, stratified intestinal type cells without PP Cases with invasive implants bilateral in 5% with mild nuclear atypia and This is a rare finding are likely due to unsampled
no detached cell clusters invasive areas in the Usually CK7 positive ovarian tumour.
Intestinal type MBT Same Same, with foci of malignant- Invasive peritoneal Same as abovewith intraepithelial appearing nuclei and often highly implants without PPcarcinoma stratified, solid or cribriform areas
Endocervical-like Smaller with fewer cysts and Cysts composed of complex, Invasive or noninvasive BenignMBT may be associated with endo- bulbous papillae with highly peritoneal implants
metriosis, bilateral in 40% stratified, benign-appearing mucinous and eosinophilic cells, detached cell clusters and numerous neutrophils
Mucinous ovarian Bilateral in a high percentage Usually resembles intestinal type PP Variable, depending on the tumours associated of cases of MBT often with pseudomyxoma Often primary appendiceal degree of atypia of the tumourwith PP o v a r i i tumour cells in PP
PP = Pseudomyxoma peritonei; MBT = mucinous borderline tumour

Endometrioid tumours
DefinitionTumours of the ovary, benign, low malig-nant potential or malignant, that closelyresemble the various types of endometri-oid tumours (epithelial and/or stromal) ofthe uterine corpus. Although an originfrom endometriosis can be demonstratedin some cases, it is not required for thediagnosis.
ICD-O codesEndometrioid adenocarcinoma,
not otherwise specified 8380/3Variant with squamous
differentiation 8570/3Ciliated variant 8383/3Oxyphilic variant 8290/3Secretory variant 8382/3
Adenocarcinofibroma 8381/3Malignant müllerian
mixed tumour 8 9 5 0 / 3Adenosarcoma 8933/3Endometrioid stromal sarcoma 8930/3Endometrioid borderline tumour 8380/1Cystadenoma 8380/0Adenofibroma;
cystadenofibroma 8381/0
Endometrioid adenocarcinoma
DefinitionA malignant epithelial tumour of the ovarythat closely resembles the common vari-ant of endometrioid carcinoma of the uter-ine corpus. Although an origin from endo-metriosis can be demonstrated in somecases, it is not re q u i red for the diagnosis.
EpidemiologyEndometrioid carcinomas account for10-20% of ovarian carcinomas {1409,2489} and occur most commonly inwomen in the fifth and sixth decades oflife {2773}.
AetiologyUp to 42% of the tumours are associatedwith endometriosis in the same ovary orelsewhere in the pelvis {676,932,1927,2489,2287a} and 15-20% are associatedwith endometrial carcinoma {1477,1479,1683,3239}. These associations suggestthat some endometrioid ovarian carcino-mas may have the same risk factors fortheir development as endometrial carci-nomas {613}. Patients whose tumoursoccur in association with endometriosisare 5-10 years younger on average thanpatients without associated ovarianendometriosis {2600}.
Clinical featuresLike most ovarian carcinomas, many en-dometrioid carcinomas are asymptomatic.Some present as a pelvic mass, with orwithout pain and may be associated withendocrine symptoms secondary to stero i dh o rmone secretion by the specialized ova-rian stroma {1790}. Serum CA125 is eleva-ted in over 80% of the cases {946,1603}.
MacroscopyThe tumours, typically measuring 10-20cm in diameter, are solid, soft, friable orcystic with a fungating mass protrudinginto the lumen. They are bilateral in 28%of the cases.
Tumour spread and stagingStage I carcinomas are bilateral in 17% ofthe cases {2233}. The stage distribution ofendometrioid carcinomas differs from thatof serous carcinomas. According to theFIGO annual re p o rt, 31% of the tumoursa re stage I; 20%, stage II; 38%, stage III;and 11%, stage IV {2233}.
HistopathologyOvarian endometrioid carcinomas close-ly resemble endometrioid carcinomas ofthe uterine corpus. The well differentiatedform shows round, oval or tubular glandslined by stratified nonmucin-containingepithelium. Cribriform or villoglandularpatterns may be present. Squamous dif-f e rentiation occurs in 30-50% of thecases, often in the form of morules (cyto-logically benign-appearing squamouscells) {341,2605}. The designation"endometrioid carcinoma with squamousdifferentiation" (rather than adenoacan-thoma and adenosquamous carcinoma)is favoured {2604,2605}. Aggregates ofspindle-shaped epithelial cells are anoccasional finding in endometrioid carci-noma {2942}. Occasionally, the spindlecell nests undergo a transition to clearlyrecognizable squamous cells suggestingthat the former may represent abortivesquamous differentiation {2605}.Rare examples of mucin-rich, secretory,ciliated cell and oxyphilic types havebeen described {759,1187,2258}. In themucin-rich variant glandular lumens andthe apex of cells are occupied by mucin{2605}. The secretory type contains vac-uolated cells resembling those of an
130 Tumours of the ovary and peritoneum
BAFig. 2.29 Ovarian endometrioid adenocarcinoma arising from an endometriotic cyst. A This solid and cystic tumour forms polypoid structures. The patient had a synchro-nous endometrioid adenocarcinoma of the uterine corpus. B Well differentiated endometrioid adenocarcinoma is seen to the right and an endometriotic cyst on the left.
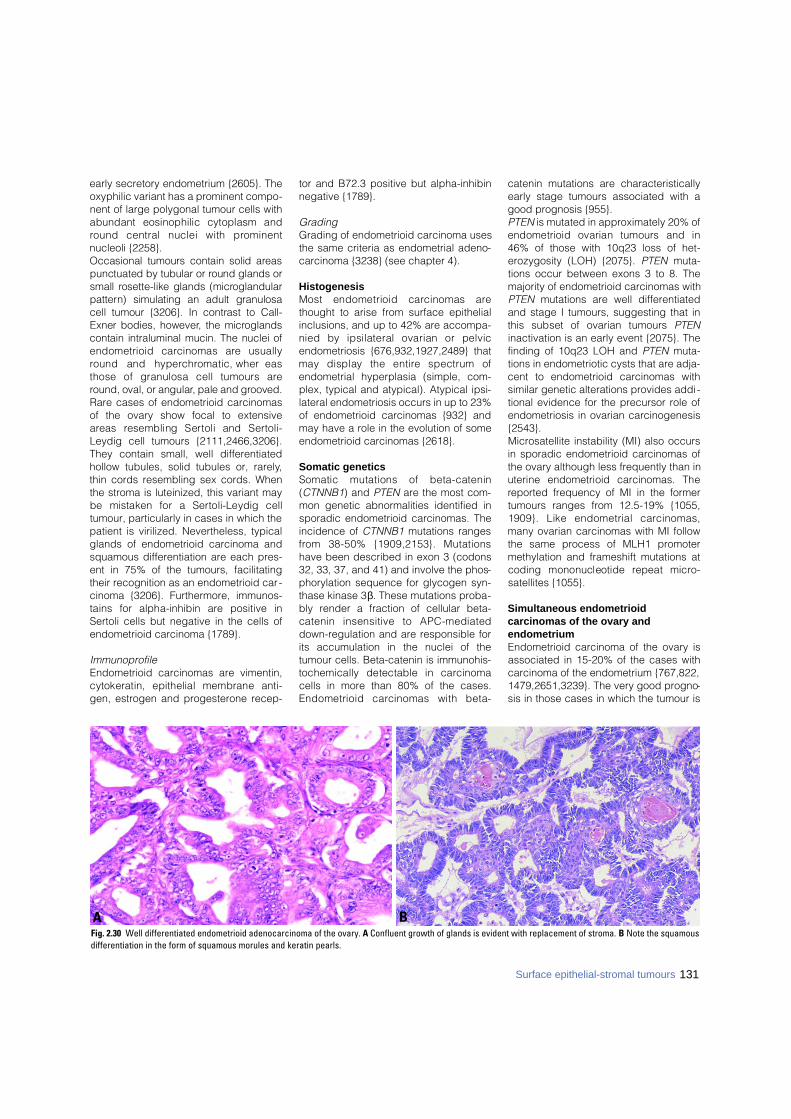
early secretory endometrium {2605}. Theoxyphilic variant has a prominent compo-nent of large polygonal tumour cells withabundant eosinophilic cytoplasm andround central nuclei with pro m i n e n tnucleoli {2258}. Occasional tumours contain solid are a spunctuated by tubular or round glands orsmall rosette-like glands (micro g l a n d u l a rp a t t e rn) simulating an adult granulosacell tumour {3206}. In contrast to Call-Exner bodies, however, the micro g l a n d scontain intraluminal mucin. The nuclei ofendometrioid carcinomas are usuallyround and hyperc h romatic, where a sthose of granulosa cell tumours areround, oval, or angular, pale and grooved. Rare cases of endometrioid carcinomasof the ovary show focal to extensivea reas resembling Sertoli and Sert o l i -Leydig cell tumours {2111,2466,3206}.They contain small, well differentiatedhollow tubules, solid tubules or, rarely,thin cords resembling sex cords. Whenthe stroma is luteinized, this variant maybe mistaken for a Sertoli-Leydig celltumour, particularly in cases in which thepatient is virilized. Nevertheless, typicalglands of endometrioid carcinoma andsquamous differentiation are each pres-ent in 75% of the tumours, facilitatingtheir recognition as an endometrioid car-cinoma {3206}. Furthermore, immunos-tains for alpha-inhibin are positive inSertoli cells but negative in the cells ofendometrioid carcinoma {1789}.
ImmunoprofileEndometrioid carcinomas are vimentin,cytokeratin, epithelial membrane anti-gen, estrogen and progesterone recep-
tor and B72.3 positive but alpha-inhibinnegative {1789}.
GradingGrading of endometrioid carcinoma usesthe same criteria as endometrial adeno-carcinoma {3238} (see chapter 4).
HistogenesisMost endometrioid carcinomas arethought to arise from surface epithelialinclusions, and up to 42% are accompa-nied by ipsilateral ovarian or pelvicendometriosis {676,932,1927,2489} thatmay display the entire spectrum ofendometrial hyperplasia (simple, com-plex, typical and atypical). Atypical ipsi-lateral endometriosis occurs in up to 23%of endometrioid carcinomas {932} andmay have a role in the evolution of someendometrioid carcinomas {2618}.
Somatic geneticsSomatic mutations of beta-catenin(CTNNB1) and PTEN are the most com-mon genetic abnormalities identified insporadic endometrioid carcinomas. Theincidence of CTNNB1 mutations rangesf rom 38-50% {1909,2153}. Mutationshave been described in exon 3 (codons32, 33, 37, and 41) and involve the phos-phorylation sequence for glycogen syn-thase kinase 3β. These mutations proba-bly render a fraction of cellular beta-catenin insensitive to APC-mediateddown-regulation and are responsible forits accumulation in the nuclei of thetumour cells. Beta-catenin is immunohis-tochemically detectable in carc i n o m acells in more than 80% of the cases.Endometrioid carcinomas with beta-
catenin mutations are characteristicallyearly stage tumours associated with agood prognosis {955}.PTEN is mutated in approximately 20% ofendometrioid ovarian tumours and in46% of those with 10q23 loss of het-erozygosity (LOH) {2075}. PTEN muta-tions occur between exons 3 to 8. Themajority of endometrioid carcinomas withPTEN mutations are well differentiatedand stage I tumours, suggesting that inthis subset of ovarian tumours P T E Ninactivation is an early event {2075}. Thefinding of 10q23 LOH and PTEN muta-tions in endometriotic cysts that are adja-cent to endometrioid carcinomas withsimilar genetic alterations provides addi -tional evidence for the precursor role ofendometriosis in ovarian carcinogenesis{2543}.Microsatellite instability (MI) also occursin sporadic endometrioid carcinomas ofthe ovary although less frequently than inuterine endometrioid carcinomas. Thereported frequency of MI in the formertumours ranges from 12.5-19% {1055,1909}. Like endometrial carc i n o m a s ,many ovarian carcinomas with MI followthe same process of MLH1 promotermethylation and frameshift mutations atcoding mononucleotide repeat micro-satellites {1055}.
Simultaneous endometrioid carcinomas of the ovary andendometriumEndometrioid carcinoma of the ovary isassociated in 15-20% of the cases withcarcinoma of the endometrium {767,822,1479,2651,3239}. The very good progno-sis in those cases in which the tumour is
BAFig. 2.30 Well differentiated endometrioid adenocarcinoma of the ovary. A Confluent growth of glands is evident with replacement of stroma. B Note the squamousdifferentiation in the form of squamous morules and keratin pearls.
131Surface epithelial-stromal tumours

limited to both organs provides strongevidence that these neoplasms are most-ly independent primaries arising as aresult of a müllerian field effect {822}.Less frequently, one of the carcinomasrepresents a metastasis from the othertumour.The criteria for distinguishing metastaticfrom independent primary carcinomasrely mainly upon conventional clinico-pathologic findings, namely stage, size,histological type and grade of thetumours, the presence and extent ofblood vessel, tubal and myometrial inva-sion, bilaterality and pattern of ovarianinvolvement, coexistence with endome-trial hyperplasia or ovarian endometriosisand, ultimately, patient follow-up {762,2286,2978}. By paying attention to thesefindings, the precise diagnosis can beestablished in most cases. Occasionally,however, the differential diagnosis maybe difficult or impossible as the tumoursmay show overlapping features.In difficult cases comparative analysis ofthe immunohistochemical and DNA flowcytometric features of the two neoplasmsmay be of some help {822,2286}. The pre-sence of identical aneuploid DNA inde-xes in two separate carcinomas suggests
that one of them is a metastasis from theother {2286}. In contrast, when the twoneoplasm have diff e rent DNA indexes,the possibility of two independent primar-ies has to be considered {2286}. The lat-ter results, however, do not completely ex-clude the metastatic nature of 1 of the tu-mours, since metastatic tumours or evend i ff e rent parts of the same tumour mayoccasionally have diff e rent DNA indexesreflecting tumour pro g ression {2728}.Molecular pathology techniques can alsobe helpful {1788}. These include LOH,{783,923,1664,2641}, gene mutation{923,1664,1909} and clonal X-inactiva-tion analyses {926}. Although LOH pat-tern concordance in two separate carci-nomas is highly suggestive of a commonclonal origin (i.e. one tumour is a metas-tasis from the other), the finding of differ-ent LOH patterns does not necessarilyindicate that they represent independenttumours. Some studies have shown vary-ing LOH patterns in different areas of thesame tumour as a consequence oftumour heterogeneity {287}. DiscordantPTEN mutations and different microsatel-lite instability (MI) patterns in the twoneoplasms are suggestive of independ-ent primary carcinomas; nevertheless,
metastatic carcinomas may also exhibitgene mutations that differ from those oftheir corresponding primary tumours asa result of tumour progression {923}.Alternatively, two independent primarycarcinomas may present identical genemutations reflecting induction of thesame genetic abnormalities by a com-mon carcinogenic agent acting in twoseparate sites of a single anatomicregion {1786,1788}. In other words, thegenetic profile can be identical in inde-pendent tumours and diff e rent inmetastatic carcinomas {1788}. Therefore,clonality analysis is useful in the distinc-tion of independent primary carcinomasfrom metastatic carcinomas provided thediagnosis does not rely exclusively on asingle molecular result and the moleculardata are interpreted in the light of appro-priate clinical and pathologic findings{1786,1788,2283}.According to FIGO when the site of originremains in doubt after pathologicalexamination, the primary site of thetumour should be determined by its initialclinical manifestations.
Genetic susceptibilityMost endometrioid carcinomas occurs p o r a d i c a l l y, but occasional casesdevelop in families with germline muta-tions in DNA mismatch repair genes,mainly MSH2 and MLH1 (Muir-Torre syn-drome) {535}. This syndrome, thought tobe a variant of the hereditary nonpolypo-sis colon cancer syndrome, is character-ized by an inherited autosomal dominantsusceptibility to develop cutaneous andvisceral neoplasms {796}.
Prognosis and predictive factorsThe 5-year survival rate (FIGO) ofpatients with stage I carcinoma is 78%;stage II, 63%; stage III, 24%; and stage
Fig. 2.33 Ovarian endometrioid carcinoma. Immu-nostain for beta-catenin shows intense and diffusepositivity.
BAFig. 2.32 Endometrioid adenocarcinoma resembling a granulosa cell tumour. A Note the microglandularpattern. B Immunostains for alpha-inhibin are positive in the luteinized stromal cells and negative in theepithelial cells.
BAFig. 2.31 Sertoliform endometroid carcinoma. A The tubular glands contain high grade nuclei. The luteinizedovarian stromal cells resemble Leydig cells. B Small endometrioid glands contain luminal mucin.(Mucicarmine stain).
132 Tumours of the ovary and peritoneum

IV, 6% {2233}. Patients with grade 1 and2 tumours have a higher survival ratethan those with grade 3 tumours {1479}.Peritoneal foreign body granulomas tokeratin found in cases of endometrioidcarcinoma with squamous differentiationdo not seem to affect the prognosisadversely in the absence of viable-appearing tumour cells on the basis of asmall series of cases {1459}. Endome-trioid carcinomas with a mixed clear cell,s e rous or undiff e rentiated carc i n o m acomponent are reported to have a worseprognosis {2941}.
Malignant müllerian mixed tumour
DefinitionA highly aggressive neoplasm containingmalignant epithelial and mesenchymalelements.
SynonymsCarcinosarcoma, malignant mesodermalmixed tumour, metaplastic carcinoma.
EpidemiologyMalignant müllerian mixed tumours(MMMTs) are rare, representing less than1% of ovarian malignancies. They occurmost commonly in postmenopausalwomen of low parity, the median agebeing around 60.
Clinical featuresThe clinical presentation is similar to thatof carcinoma of the ovary.
AetiologyAn increased incidence has been report-ed in women who have had pelvic irradi-ation {3080}.
MacroscopyThe neoplasms form large (10-20 cmdiameter), partly solid and partly cystic,or, less commonly, solid, grey-brown, uni-lateral or bilateral, bosselated masseswith foci of haemorrhage and necrosis{479}. The sectioned surface is fleshyand friable, and cartilage and bone maybe apparent. The tumours are bilateral in90% of cases.
Tumour spread and stagingT h e re is extraovarian spread to thepelvic peritoneum, omentum, pelvicorgans and regional lymph nodes inm o re than 75% of cases at the time ofd i a g n o s i s .
HistopathologyThe histological and immunoprofile aresimilar to those of its uterine counterpartand those occurring elsewhere in thefemale genital system (see chapter 4).
HistogenesisMMMT is believed to develop from theovarian surface epithelium or from foci ofendometriosis and, therefore, may beregarded as a high grade carcinoma withmetaplastic sarcomatous elements. Thepositive tumour response to chemothera-py directed at ovarian carcinoma alsosupports this viewpoint.
Somatic genetics There is evidence that MMMTs are mon-oclonal {26,2748} as the phenotypicallydifferent elements share similar alleliclosses and retentions {925} and a cellline developed from an MMMT expressesboth mesenchymal and epithelial anti-gens {195}. Furt h e rm o re, a hetero g e-neous pattern of allelic loss at a limitednumber of chromosomal loci in either thecarcinomatous or sarcomatous compo-nent of the neoplasm is consistent witheither genetic pro g ression or geneticdiversion occurring during the clonalevolution of the tumour.
Genetic susceptibilityThere is anecdotal evidence of BRCA2mutation {2748}.
Prognosis and predictive factorsI m p roved cytoreductive surgery andplatinum based chemotherapy hasresulted in a median survival of 19months {2715} and an overall 5-year sur-vival of 18-27% {120,1182}. The survivorsalmost invariably have early stage dis-ease at the time of diagnosis, and lowstage is a statistically significant indica-tor of outcome {120,436,1182,2749}. Noother histopathological factors are signif-icant indicators of outcome.
Adenosarcoma
DefinitionA biphasic tumour characterized by aproliferation of müllerian-type epitheliumwith a benign or occasionally markedlyatypical appearance embedded in or
Fig. 2.34 Genetic differences in concurrent endometrial and ovarian adenocarcinoma. DNA sequencing ofexon 3 of the beta-catenin(CTNNB1) gene showing a GGA to GCA change at codon 32 (Asp>His) in the ovar-ian endometrioid adenocarcinoma (right, arrow). The mutation was not identified in the uterine endometri-al carcinoma (left).
Fig. 2.35 Malignant müllerian mixed tumour. Poorlydifferentiated glands are surrounded by spindle-shaped, rounded and multinucleated cells.
133Surface epithelial-stromal tumours

overlying a dominant sarcomatous mes-enchyme.
Clinical featuresMost of the tumours reported so far havebeen unilateral, occurring in the 4th and5th decades. Abdominal discomfort anddistension are the usual complaints.
Macroscopy and histopathologyThe tumour is frequently adherent to thes u r rounding tissue {512,604,929}. Themacroscopic and histological featuresare described in detail in the uterinecounterpart (see chapter 4).
Prognosis and predictive factorsOccasional re p o rts have linked thes p read of adenosarcomas into theabdominal cavity with a poor clinicaloutcome {510}. The stroma is often pre-dominantly fibrotic, oedematous or hyal-ized with characteristic foci of perivas-cular cuffing seen only focally (some-times, the foci are very small) and stillthe tumours recur and kill the patient{760}. Unfort u n a t e l y, there exist noestablished morphological criteria top redict such biological behaviour. How-e v e r, if during the course of the diseases a rcomatous overgrowth develops, sig-nifying invasive potential, the patientre q u i res careful monitoring. In a seriesof 40 cases, the 5-year survival was
64%, the 10-year survival 46% and the15-year survival 30% {760}. Age gre a t e rthan 53 years, tumour rupture, highgrade and the presence of high grades a rcomatous overgrowth appear to beassociated with re c u r rence or extraovar-ian spread. Ovarian adenosarcoma hasa worse prognosis than its uterine coun-t e r p a rt, presumably because of theg reater ease of peritoneal spread {760}.T h e r a p e u t i c a l l y, an aggressive surgicala p p roach with wide excision is mostoften recommended {510}. Chemo-therapy and radiation may be applied inindividual cases; however, no estab-lished protocols exist.
Endometrioid stromal and undifferentiated ovarian sarcoma
DefinitionEndometrioid stromal sarcoma (ESS) isa monophasic sarcomatous tumourcharacterized by a diffuse pro l i f e r a t i o nof neoplastic cells similar to stro m a lcells of proliferative endometrium. At itsp e r i p h e ry the tumour exhibits a typicalinfiltrative growth pattern. Those neo-plasms that have moderate to markedpleomorphism, significant nuclear ana-plasia and more cytoplasm than isfound in endometrial stromal cellsshould be classified as undiff e re n t i a t e dovarian sarc o m a .
Clinical featuresM o re than 70% of the tumours are uni-lateral. The age range is 11-76 yearswith the majority of tumours occurringa round the 5th and 6th decade. Theclinical symptoms do not differ fro mthose recognized for other ovariantumours.
M a c r o s c o p yMost tumours are solid and firm, butsome may show variably sized cysts,sometimes filled with mucoid or haemor-rhagic fluid or debris. The sectioneds u rface appears yellow-white or tan,sometimes interspersed with gre yf i b rous bundles or septa.
HistopathologyRoughly half of the cases of ESS areassociated with either endometriosis or asimilar sarcomatous lesion of theendometrial stroma or both {2605}. Thedominant cell type of ESS consists ofsmall, round to oval, or occasionally spin-dle shaped cells with round nuclei andscanty, sometimes barely visible palecytoplasm. The cells may be arrangedhaphazardly in a diffuse pattern or mayform parallel cell sheets mimicking fibro-ma. Hypocellular areas with a distinctoedematous appearance can be pres-ent. Lipid droplets may be present withintumour cells, which are often associatedwith foam cells. A hallmark of ESS is thepresence of abundant small thick-walledvessels resembling spiral arteries of thelate secretory endometrium. The vesselsoften are surrounded by whorls of neo-plastic cells. Reticulin stain disclosesdelicate fibrils characteristically envelop-ing individual tumour cells. The cellulari-ty can vary markedly within the samespecimen. The tumour can be partlyintersected by fibrous bands form i n gmore or less distinct nodules. Some-times, hyaline plaques are pre s e n t .Rarely, cord-like or plexiform arrange-ments of tumour cells similar to thegrowth patterns seen in ovarian sex cordtumours such as granulosa cell tumoursor thecomas are observed. In theseareas reticulin fibrils are more or lessabsent. Rarely, glandular elements areinterspersed, but they never represent adominant feature. At its periphery thetumour exhibits a typical infiltrativeg rowth pattern. In cases where thetumour has spread into extraovariansites, a tongue-like pattern of invasion
Fig. 2.36 Endometrioid borderline tumour. Whereas most endometrioid borderline tumours have an ade-nofibromatous appearance, the adenofibromatous lesion is rarely evident within a large cystic mass.
134 Tumours of the ovary and peritoneum
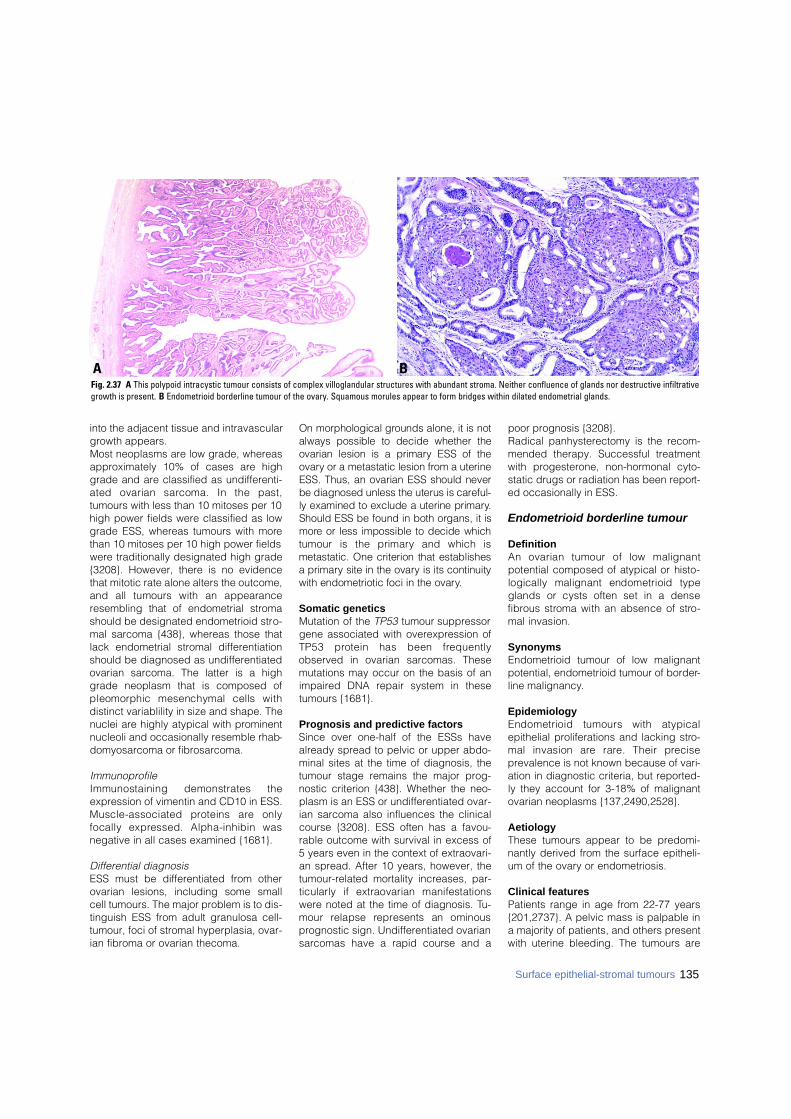
135Surface epithelial-stromal tumours
into the adjacent tissue and intravasculargrowth appears.Most neoplasms are low grade, whereasapproximately 10% of cases are highgrade and are classified as undifferenti-ated ovarian sarcoma. In the past,tumours with less than 10 mitoses per 10high power fields were classified as lowgrade ESS, whereas tumours with morethan 10 mitoses per 10 high power fieldswere traditionally designated high grade{3208}. However, there is no evidencethat mitotic rate alone alters the outcome,and all tumours with an appearanceresembling that of endometrial stromashould be designated endometrioid stro-mal sarcoma {438}, whereas those thatlack endometrial stromal differentiationshould be diagnosed as undifferentiatedovarian sarcoma. The latter is a highgrade neoplasm that is composed ofpleomorphic mesenchymal cells withdistinct variablility in size and shape. Thenuclei are highly atypical with prominentnucleoli and occasionally resemble rhab-domyosarcoma or fibrosarcoma.
ImmunoprofileImmunostaining demonstrates theexpression of vimentin and CD10 in ESS.Muscle-associated proteins are onlyfocally expressed. Alpha-inhibin wasnegative in all cases examined {1681}.
Differential diagnosisESS must be differentiated from otherovarian lesions, including some smallcell tumours. The major problem is to dis-tinguish ESS from adult granulosa cell-tumour, foci of stromal hyperplasia, ovar-ian fibroma or ovarian thecoma.
On morphological grounds alone, it is notalways possible to decide whether theovarian lesion is a primary ESS of theo v a ry or a metastatic lesion from a uterineESS. Thus, an ovarian ESS should neverbe diagnosed unless the uterus is care f u l-ly examined to exclude a uterine primary.Should ESS be found in both organs, it ism o re or less impossible to decide whichtumour is the primary and which ismetastatic. One criterion that establishesa primary site in the ovary is its continuitywith endometriotic foci in the ovary.
Somatic geneticsMutation of the TP53 tumour suppressorgene associated with overexpression ofTP53 protein has been fre q u e n t l yobserved in ovarian sarcomas. Thesemutations may occur on the basis of animpaired DNA repair system in thesetumours {1681}.
Prognosis and predictive factorsSince over one-half of the ESSs havealready spread to pelvic or upper abdo-minal sites at the time of diagnosis, thetumour stage remains the major prog-nostic criterion {438}. Whether the neo-plasm is an ESS or undifferentiated ovar-ian sarcoma also influences the clinicalcourse {3208}. ESS often has a favou-rable outcome with survival in excess of5 years even in the context of extraovari-an spread. After 10 years, however, thetumour-related mortality increases, par-ticularly if extraovarian manifestationswere noted at the time of diagnosis. Tu-mour relapse re p resents an ominousprognostic sign. Undifferentiated ovariansarcomas have a rapid course and a
poor prognosis {3208}.Radical panhysterectomy is the recom-mended therapy. Successful treatmentwith progesterone, non-hormonal cyto-static drugs or radiation has been report-ed occasionally in ESS.
Endometrioid borderline tumour
DefinitionAn ovarian tumour of low malignantpotential composed of atypical or histo-logically malignant endometrioid typeglands or cysts often set in a densef i b rous stroma with an absence of stro-mal invasion.
SynonymsEndometrioid tumour of low malignantpotential, endometrioid tumour of border-line malignancy.
EpidemiologyEndometrioid tumours with atypicalepithelial proliferations and lacking stro-mal invasion are rare. Their pre c i s eprevalence is not known because of vari-ation in diagnostic criteria, but reported-ly they account for 3-18% of malignantovarian neoplasms {137,2490,2528}.
AetiologyThese tumours appear to be predomi-nantly derived from the surface epitheli-um of the ovary or endometriosis.
Clinical featuresPatients range in age from 22-77 years{201,2737}. A pelvic mass is palpable ina majority of patients, and others presentwith uterine bleeding. The tumours are
BAFig. 2.37 A This polypoid intracystic tumour consists of complex villoglandular structures with abundant stroma. Neither confluence of glands nor destructive infiltrativegrowth is present. B Endometrioid borderline tumour of the ovary. Squamous morules appear to form bridges within dilated endometrial glands.

136 Tumours of the ovary and peritoneum
predominantly unilateral, but rare bilater-al lesions occur.
MacroscopyTumours range in size from 2-40 cm,have a tan to grey-white sectioned sur-face that varies from solid to predomi-nantly solid with cysts ranging from a fewmm to 8 cm in diameter {201,2737}.Haemorrhage and necrosis are presentmainly in larger tumours.
HistopathologyT h ree patterns have been described{201,2737}. The most common is ade-nofibromatous. Islands of crowded endo-metrioid glands or cysts lined by cellsdisplaying grade 1 to, rarely, grade 3cytological atypia proliferate in an ade-nofibromatous stroma. Stromal invasionis absent. Mitotic activity is usually low.
Squamous metaplasia is common, andnecrosis may develop in the metaplasticepithelium. The second pattern is villog-landular or papillary with an atypical celllining similar to atypical hyperplasia ofthe endometrium again in a fibromatousb a c k g round. The third form shows acombination of villoglandular and ade-nofibromatous patterns. Anywhere from15% to over half of the patients haveendometriosis in the same ovary as wellas at extraovarian sites {201,2737}.
Prognosis and predictive factorsThe prognosis is excellent. Recurre n c e sand metastases are rare. Even in the rarecase of an extraovarian tumour noduleinvolving the colonic serosa {2737}, nosubsequent problems developed 9 yearsafter surgery, radiation and chemothera-p y. Since a few patients treated by unilat-
eral salpingo-oophorectomy developedendometrioid carcinoma in the contralat-eral ovary, and 1 died from it, bilaterals a l p i n g o - o o p h o rectomy would be pru-dent when retention of fertility is no longeran issue. Unilateral salpingo-oophore c t o-my along with follow-up for early detec-tion of any subsequent ovarian or endo-metrial adenocarcinoma is acceptable forwomen of childbearing age.
Benign endometrioid tumours
DefinitionOvarian tumours with histological fea-tures of benign glands or cysts lined bywell differentiated cells of endometrialtype.
EpidemiologyBecause of the rarity of these neoplasmsno convincing epidemiological data canbe quoted. The reported patients aremainly of the reproductive age.
LocalizationBenign endometrioid tumours are usuallyunilateral, though in rare cases involve-ment of both ovaries is encountered.
Clinical featuresSigns and symptomsThere are no specific clinical symptomsof benign endometrioid tumours. Smallneoplasms are incidental findings, some-times in the wall of an ovarian endometri-otic cyst. Large tumours are manifestedby pain and abdominal swelling.
ImagingImaging techniques, including US, CTand MRI, cannot effectively establish thespecific nosological character of theprocess. They can visualize endometriot-ic foci and thus indirectly indicate thepresumptive endometrioid nature of theneoplasm; otherwise the results of imag-ing technique show the formal character-istics, i.e. cystic or cystic-fibrous archi-tecture of the lesion {234}.
HistopathologyThe histological diagnosis of endometri-oid adenomas and cystadenomas isbased on the presence of well differenti-ated, benign appearing glands or cystslined by endometrial type cells with orwithout squamous differentiation. In theadenofibromatous variant fibrous stromap redominates. Though adenofibro m a s
Fig. 2.38 Endometrioid borderline tumour of the ovary with microinvasion. Cystic tumour contains complexpapillae. A small area has densely packed glands indicative of microinvasion (arrow) .
BAFig. 2.39 A Endometrioid cystadenoma. The cystic neoplasm forms villiform structures lined by well differ-entiated endometrioid type epithelium. B Endometroid adenofibroma. A squamous morule bridges twoendometrioid type glands lined by uniform cells set in a fibrous stroma.
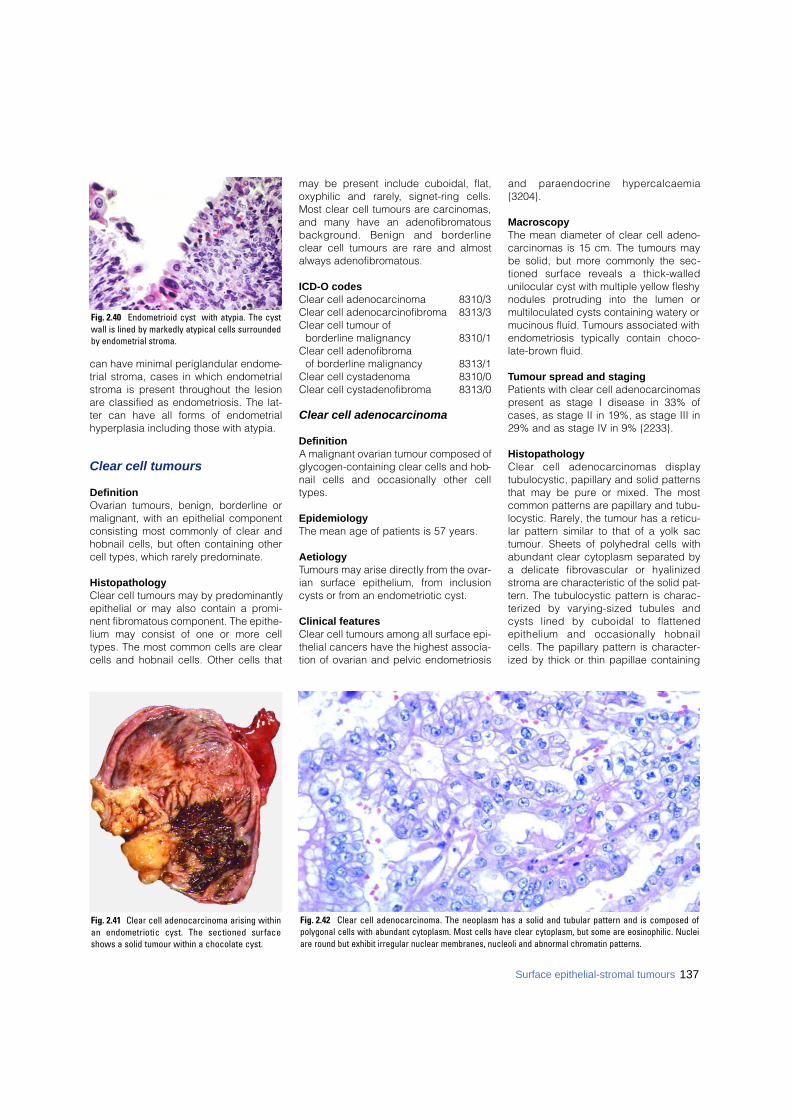
137Surface epithelial-stromal tumours
can have minimal periglandular endome-trial stroma, cases in which endometrialstroma is present throughout the lesionare classified as endometriosis. The lat-ter can have all forms of endometrialhyperplasia including those with atypia.
Clear cell tumours
DefinitionOvarian tumours, benign, borderline ormalignant, with an epithelial componentconsisting most commonly of clear andhobnail cells, but often containing othercell types, which rarely predominate.
HistopathologyClear cell tumours may by predominantlyepithelial or may also contain a promi-nent fibromatous component. The epithe-lium may consist of one or more celltypes. The most common cells are clearcells and hobnail cells. Other cells that
may be present include cuboidal, flat,oxyphilic and rare l y, signet-ring cells.Most clear cell tumours are carcinomas,and many have an adenofibromatousb a c k g round. Benign and bord e r l i n eclear cell tumours are rare and almostalways adenofibromatous.
ICD-O codesClear cell adenocarcinoma 8310/3Clear cell adenocarcinofibroma 8313/3Clear cell tumour of
borderline malignancy 8310/1Clear cell adenofibroma
of borderline malignancy 8313/1Clear cell cystadenoma 8310/0Clear cell cystadenofibroma 8313/0
Clear cell adenocarcinoma
DefinitionA malignant ovarian tumour composed ofglycogen-containing clear cells and hob-nail cells and occasionally other celltypes.
EpidemiologyThe mean age of patients is 57 years.
AetiologyTumours may arise directly from the ovar-ian surface epithelium, from inclusioncysts or from an endometriotic cyst.
Clinical featuresClear cell tumours among all surface epi-thelial cancers have the highest associa-tion of ovarian and pelvic endometriosis
and paraendocrine hyperc a l c a e m i a{3204}.
MacroscopyThe mean diameter of clear cell adeno-carcinomas is 15 cm. The tumours maybe solid, but more commonly the sec-tioned surface reveals a thick-walledunilocular cyst with multiple yellow fleshynodules protruding into the lumen ormultiloculated cysts containing watery ormucinous fluid. Tumours associated withendometriosis typically contain choco-late-brown fluid.
Tumour spread and stagingPatients with clear cell adenocarcinomaspresent as stage I disease in 33% ofcases, as stage II in 19%, as stage III in29% and as stage IV in 9% {2233}.
HistopathologyClear cell adenocarcinomas displaytubulocystic, papillary and solid patternsthat may be pure or mixed. The mostcommon patterns are papillary and tubu-locystic. Rarely, the tumour has a reticu-lar pattern similar to that of a yolk sactumour. Sheets of polyhedral cells withabundant clear cytoplasm separated bya delicate fibrovascular or hyalinizedstroma are characteristic of the solid pat-tern. The tubulocystic pattern is charac-terized by varying-sized tubules andcysts lined by cuboidal to flattenedepithelium and occasionally hobnailcells. The papillary pattern is character-ized by thick or thin papillae containing
Fig. 2.40 Endometrioid cyst with atypia. The cystwall is lined by markedly atypical cells surroundedby endometrial stroma.
Fig. 2.41 Clear cell adenocarcinoma arising withinan endometriotic cyst. The sectioned surfaceshows a solid tumour within a chocolate cyst.
Fig. 2.42 Clear cell adenocarcinoma. The neoplasm has a solid and tubular pattern and is composed ofpolygonal cells with abundant cytoplasm. Most cells have clear cytoplasm, but some are eosinophilic. Nucleiare round but exhibit irregular nuclear membranes, nucleoli and abnormal chromatin patterns.

fibrous tissue or abundant hyaline mate-rial. The most common cell types are theclear and hobnail cells. Clear cells tendto be arranged in solid nests or massesor lining cysts, tubules and papillae,whereas hobnail cells line tubules andcysts and cover papillary structures. Theclear cells tend to be rounded or polygo-nal with eccentric nuclei, often contain-ing prominent nucleoli. The hobnail cellshave scant cytoplasm and contain bul-bous hyperc h romatic nuclei that pro-trude into the lumens of the tubules.Flattened or cuboidal cells are alsoe n c o u n t e red. Occasionally, oxyphiliccells with abundant eosinophilic cyto-plasm, which in a few instances make upthe majority of the neoplasm, areobserved. Signet-ring cells often containinspissated mucinous material in the
centre of a vacuole, creating what hasbeen referred to as a "targetoid" cell. Theclear cells contain abundant glycogenand may also contain some lipid. Mucinmay be found, typically located in thelumens of tubules and cysts and is abun-dant within the cytoplasm of the signet-ring cells.
ImmmunoprofileClear cell adenocarcinomas stain strong-ly and diffusely for keratins, epithelialmembrane antigen, Leu M1 and B72.3.Stains for carcinoembryonic antigen arepositive in 38% of cases and for CA125(OC-125) in 50%. There have been a fewreports of clear cell adenocarcinomascontaining AFP. In a patient with clearcell adenocarcinoma who developedh y p e rcalcaemia when the tumourrecurred, immunostains for parathyroidh o rm o n e - related protein were stro n g l ypositive in the recurrent carcinoma butnegative in the primary carc i n o m a{3209}.
Differential diagnosisThe differential diagnosis includes germcell tumours, particularly yolk sactumour, dysgerminoma and, rarely, stru-ma ovarii, endometrioid carcinoma withs e c re t o ry change and steroid celltumours that contain prominent areas ofcells with clear cytoplasm. Metastaticclear cell neoplasms from outside thefemale genital system are very rare.Clinical information can be particularlyhelpful in the differential diagnosis asg e rm cell tumours occur in youngwomen, and elevated serum alpha-feto-
protein (AFP) levels are always found inpatients with yolk sac tumours. Histo-logically, the papillary structures of clearcell carcinoma are more complex thanthose of yolk sac tumours and containhyalinized cores. In contrast, yolk sactumours display a variety of distinctivefeatures including a prominent reticularp a t t e rn and Schiller-Duvall bodies.Negative immunostains for AFP are use-ful in excluding yolk sac tumours,although rare examples of AFP-contain-ing clear cell carcinomas have beenreported. Positive staining for EMA anddiffuse strong positivity for cytokeratinsexclude dysgerminoma. Immunostainsfor thyroglobulin are very useful in rulingout struma ovarii. Endometrioid carcinomas with secretorychange typically are composed of cellsthat are columnar with subnuclear andsupranuclear vacuolization re s e m b l i n gearly secretory endometrium. In contrast,the clear cell changes in clear cell carci-noma are more diffuse, the cells arepolygonal, and they typically display theother characteristic patterns of clear cellc a rcinoma. A metaplastic squamouscomponent may be seen in endometrioidcarcinoma and is not observed in clearcell carcinoma. In contrast to clear cellcarcinomas, steroid cell tumours of theovary that contain prominent clear cyto-plasm are smaller, well circumscribed,have low grade nuclear features andstain strongly for alpha-inhibin.
GradingNuclei in clear cell carcinomas rangefrom grade 1 to grade 3, but pure grade
Fig. 2.43 Clear cell adenocarcinoma. Roundtubules lined by flattened to highly atypical hobnailcells are present in a fibroedematous stroma (PAS-hematoxylin stain).
BAFig. 2.44 Borderline clear cell adenofibromatous tumour. A Though predominantly solid on the right, the tumour is composed of numerous small cysts on the left. B Histologically, round glands, many of which are dilated and contain secretions, proliferate in a fibrous stroma.
138 Tumours of the ovary and peritoneum
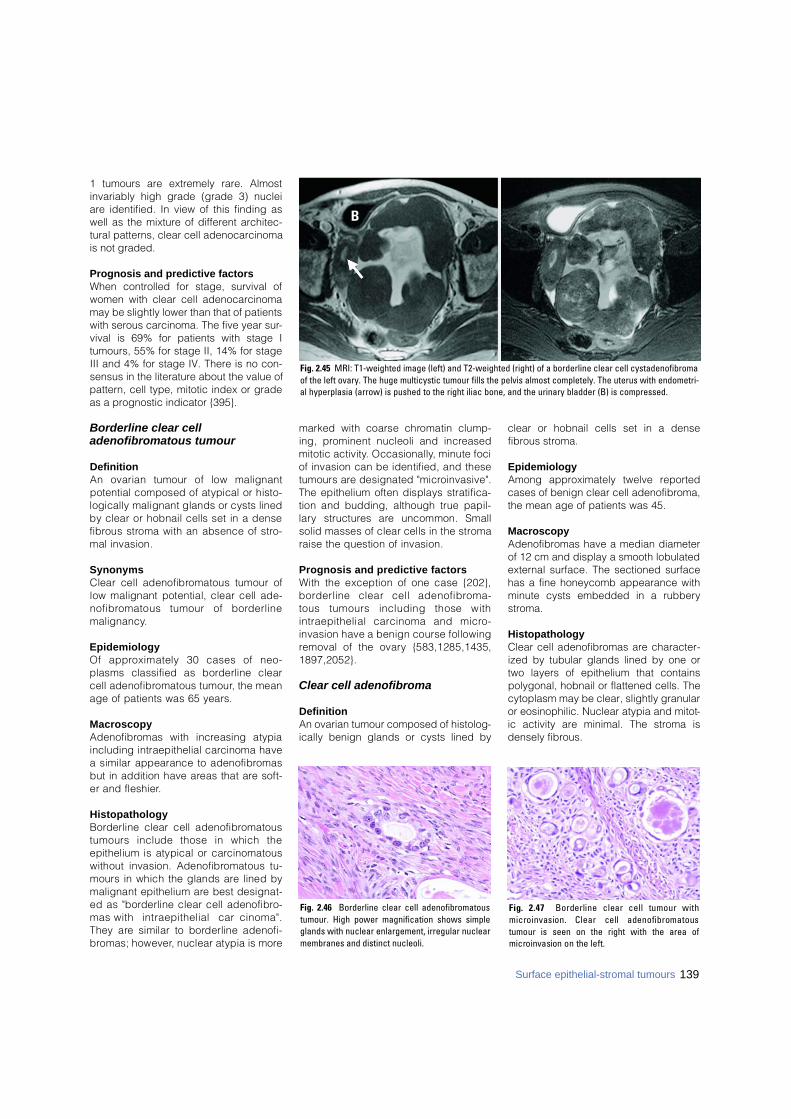
1 tumours are extremely rare. Almostinvariably high grade (grade 3) nucleiare identified. In view of this finding aswell as the mixture of different architec-tural patterns, clear cell adenocarcinomais not graded.
Prognosis and predictive factorsWhen controlled for stage, survival ofwomen with clear cell adenocarcinomamay be slightly lower than that of patientswith serous carcinoma. The five year sur-vival is 69% for patients with stage Itumours, 55% for stage II, 14% for stageIII and 4% for stage IV. There is no con-sensus in the literature about the value ofpattern, cell type, mitotic index or gradeas a prognostic indicator {395}.
Borderline clear cell adenofibromatous tumour
DefinitionAn ovarian tumour of low malignantpotential composed of atypical or histo-logically malignant glands or cysts linedby clear or hobnail cells set in a densef i b rous stroma with an absence of stro-mal invasion.
S y n o n y m sClear cell adenofibromatous tumour oflow malignant potential, clear cell ade-n o f i b romatous tumour of bord e r l i n em a l i g n a n c y.
E p i d e m i o l o g yOf approximately 30 cases of neo-plasms classified as borderline clearcell adenofibromatous tumour, the meanage of patients was 65 years.
M a c r o s c o p yA d e n o f i b romas with increasing atypiaincluding intraepithelial carcinoma havea similar appearance to adenofibro m a sbut in addition have areas that are soft-er and fleshier.
H i s t o p a t h o l o g yB o rderline clear cell adenofibro m a t o u stumours include those in which theepithelium is atypical or carc i n o m a t o u swithout invasion. Adenofibromatous tu-mours in which the glands are lined bymalignant epithelium are best designat-ed as "borderline clear cell adenofibro-mas with intraepithelial carc i n o m a " .They are similar to borderline adenofi-b romas; however, nuclear atypia is more
marked with coarse chromatin clump-ing, prominent nucleoli and incre a s e dmitotic activity. Occasionally, minute fociof invasion can be identified, and thesetumours are designated "micro i n v a s i v e " .The epithelium often displays stratifica-tion and budding, although true papil-l a ry structures are uncommon. Smallsolid masses of clear cells in the stro m araise the question of invasion.
Prognosis and predictive factorsWith the exception of one case {202},b o rderline clear cell adenofibro m a -tous tumours including those with intraepithelial carcinoma and micro-invasion have a benign course followingremoval of the ovary {583,1285,1435,1 8 9 7 , 2 0 5 2 } .
Clear cell adenofibroma
DefinitionAn ovarian tumour composed of histolog-ically benign glands or cysts lined by
clear or hobnail cells set in a densefibrous stroma.
EpidemiologyAmong approximately twelve reportedcases of benign clear cell adenofibroma,the mean age of patients was 45.
MacroscopyAdenofibromas have a median diameterof 12 cm and display a smooth lobulatedexternal surface. The sectioned surfacehas a fine honeycomb appearance withminute cysts embedded in a rubberystroma.
HistopathologyClear cell adenofibromas are character-ized by tubular glands lined by one ortwo layers of epithelium that containspolygonal, hobnail or flattened cells. Thecytoplasm may be clear, slightly granularor eosinophilic. Nuclear atypia and mitot-ic activity are minimal. The stroma isdensely fibrous.
Fig. 2.47 Borderline clear cell tumour withmicroinvasion. Clear cell adenofibromatoustumour is seen on the right with the area ofmicroinvasion on the left.
Fig. 2.46 Borderline clear cell adenofibromatoustumour. High power magnification shows simpleglands with nuclear enlargement, irregular nuclearmembranes and distinct nucleoli.
139Surface epithelial-stromal tumours
Fig. 2.45 MRI: T1-weighted image (left) and T2-weighted (right) of a borderline clear cell cystadenofibromaof the left ovary. The huge multicystic tumour fills the pelvis almost completely. The uterus with endometri-al hyperplasia (arrow) is pushed to the right iliac bone, and the urinary bladder (B) is compressed.
B
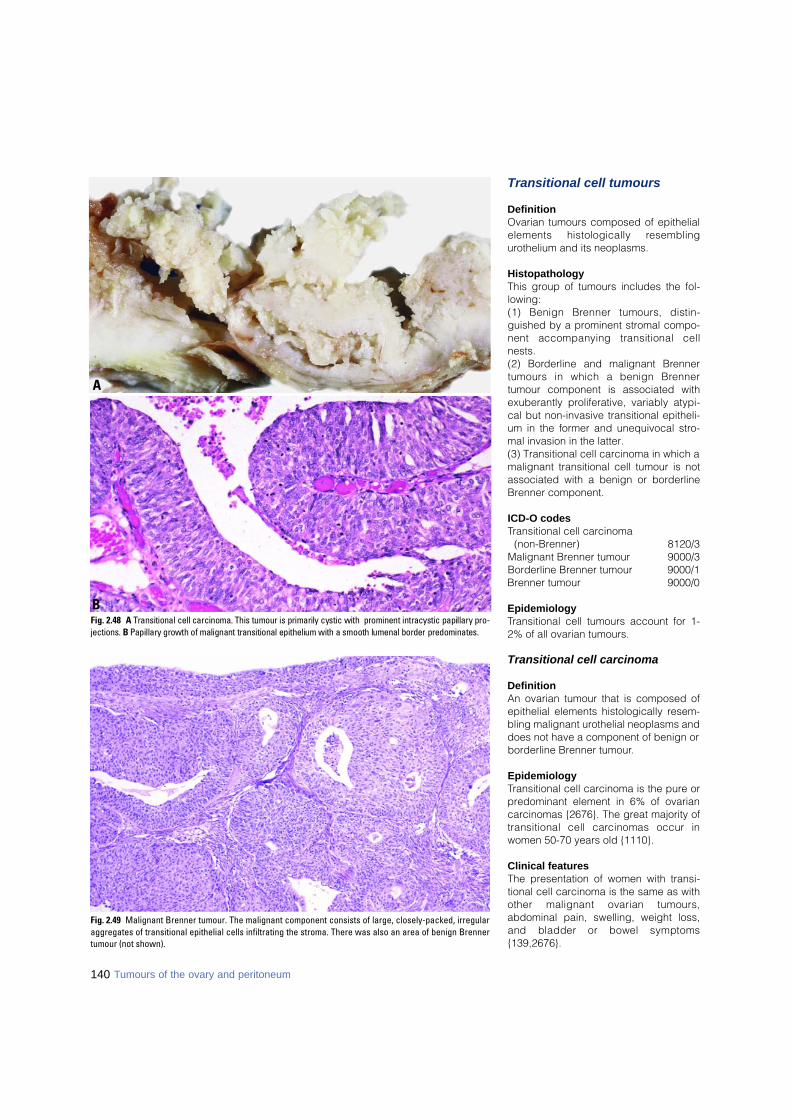
Transitional cell tumours
DefinitionOvarian tumours composed of epithelialelements histologically re s e m b l i n gurothelium and its neoplasms.
HistopathologyThis group of tumours includes the fol-lowing:(1) Benign Brenner tumours, distin-guished by a prominent stromal compo-nent accompanying transitional cellnests.(2) Borderline and malignant Bre n n e rtumours in which a benign Bre n n e rtumour component is associated withexuberantly proliferative, variably atypi-cal but non-invasive transitional epitheli-um in the former and unequivocal stro-mal invasion in the latter.(3) Transitional cell carcinoma in which amalignant transitional cell tumour is notassociated with a benign or borderlineBrenner component.
ICD-O codesTransitional cell carcinoma
(non-Brenner) 8120/3Malignant Brenner tumour 9000/3Borderline Brenner tumour 9000/1Brenner tumour 9000/0
EpidemiologyTransitional cell tumours account for 1-2% of all ovarian tumours.
Transitional cell carcinoma
DefinitionAn ovarian tumour that is composed ofepithelial elements histologically resem-bling malignant urothelial neoplasms anddoes not have a component of benign orborderline Brenner tumour.
EpidemiologyTransitional cell carcinoma is the pure orpredominant element in 6% of ovariancarcinomas {2676}. The great majority oftransitional cell carcinomas occur inwomen 50-70 years old {1110}.
Clinical featuresThe presentation of women with transi-tional cell carcinoma is the same as withother malignant ovarian tumours,abdominal pain, swelling, weight loss,and bladder or bowel symptoms{139,2676}.
Fig. 2.48 A Transitional cell carcinoma. This tumour is primarily cystic with prominent intracystic papillary pro-j e c t i o n s . B Papillary growth of malignant transitional epithelium with a smooth lumenal border predominates.
B
A
Fig. 2.49 Malignant Brenner tumour. The malignant component consists of large, closely-packed, irregularaggregates of transitional epithelial cells infiltrating the stroma. There was also an area of benign Brennertumour (not shown).
140 Tumours of the ovary and peritoneum
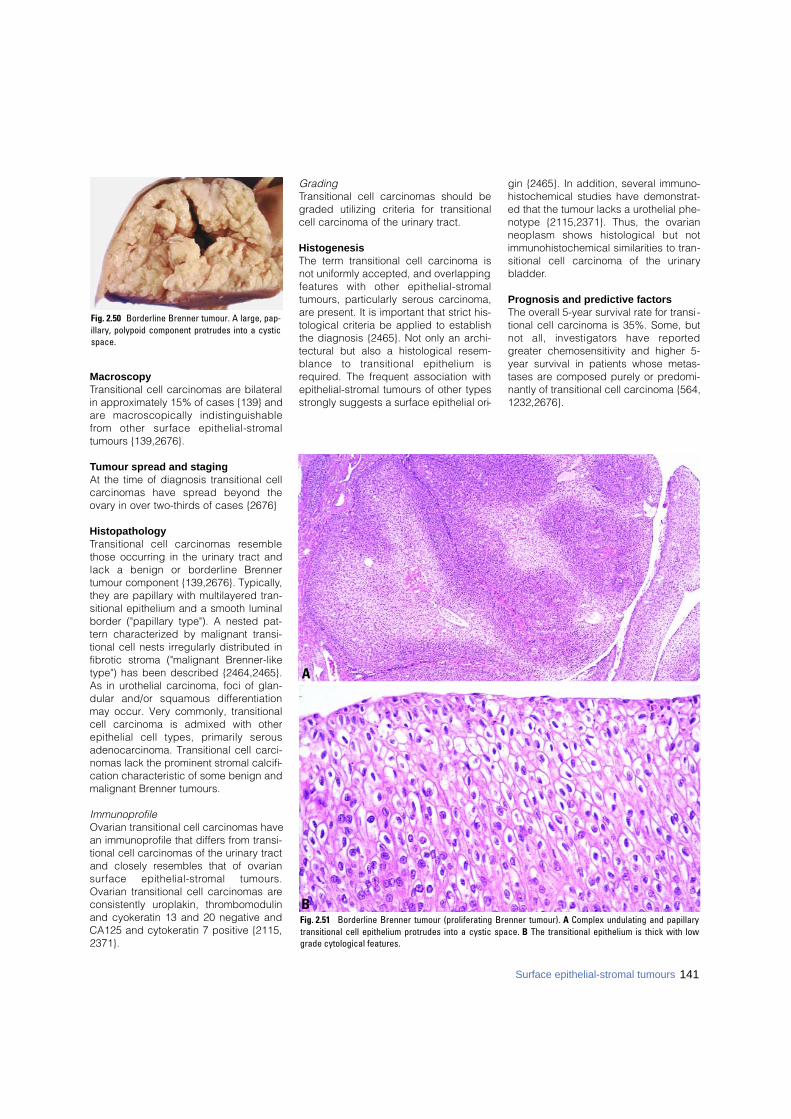
141Surface epithelial-stromal tumours
MacroscopyTransitional cell carcinomas are bilateralin approximately 15% of cases {139} anda re macroscopically indistinguishablef rom other surface epithelial-stro m a ltumours {139,2676}.
Tumour spread and stagingAt the time of diagnosis transitional cellc a rcinomas have spread beyond theovary in over two-thirds of cases {2676}
HistopathologyTransitional cell carcinomas re s e m b l ethose occurring in the urinary tract andlack a benign or borderline Bre n n e rtumour component {139,2676}. Typically,they are papillary with multilayered tran-sitional epithelium and a smooth luminalborder ("papillary type"). A nested pat-tern characterized by malignant transi-tional cell nests irregularly distributed infibrotic stroma ("malignant Brenner-liketype") has been described {2464,2465}.As in urothelial carcinoma, foci of glan-dular and/or squamous diff e re n t i a t i o nmay occur. Very commonly, transitionalcell carcinoma is admixed with otherepithelial cell types, primarily sero u sadenocarcinoma. Transitional cell carci-nomas lack the prominent stromal calcifi-cation characteristic of some benign andmalignant Brenner tumours.
ImmunoprofileOvarian transitional cell carcinomas havean immunoprofile that differs from transi-tional cell carcinomas of the urinary tractand closely resembles that of ovarians u rface epithelial-stromal tumours.Ovarian transitional cell carcinomas areconsistently uroplakin, thrombomodulinand cyokeratin 13 and 20 negative andCA125 and cytokeratin 7 positive {2115,2371}.
GradingTransitional cell carcinomas should begraded utilizing criteria for transitionalcell carcinoma of the urinary tract.
HistogenesisThe term transitional cell carcinoma isnot uniformly accepted, and overlappingf e a t u res with other epithelial-stro m a ltumours, particularly serous carcinoma,are present. It is important that strict his-tological criteria be applied to establishthe diagnosis {2465}. Not only an archi-tectural but also a histological resem-blance to transitional epithelium isrequired. The frequent association withepithelial-stromal tumours of other typesstrongly suggests a surface epithelial ori-
gin {2465}. In addition, several immuno-histochemical studies have demonstrat-ed that the tumour lacks a urothelial phe-notype {2115,2371}. Thus, the ovarianneoplasm shows histological but notimmunohistochemical similarities to tran-sitional cell carcinoma of the urinarybladder.
Prognosis and predictive factorsThe overall 5-year survival rate for transi-tional cell carcinoma is 35%. Some, butnot all, investigators have re p o rt e dgreater chemosensitivity and higher 5-year survival in patients whose metas-tases are composed purely or predomi-nantly of transitional cell carcinoma {564,1232,2676}.
Fig. 2.50 Borderline Brenner tumour. A large, pap-illary, polypoid component protrudes into a cysticspace.
Fig. 2.51 Borderline Brenner tumour (proliferating Brenner tumour). A Complex undulating and papillarytransitional cell epithelium protrudes into a cystic space. B The transitional epithelium is thick with lowgrade cytological features.
B
A

Malignant Brenner tumour
Definition An ovarian tumour containing invasivetransitional cell aggregates as well asbenign nests of transitional epitheliumset in a fibromatous stroma.
EpidemiologyThe great majority of malignant Brennertumours occur in women 50-70 years old{1110,1868,2676}. Only 5% of Brennertumours are malignant {1110,1868}.
Clinical featuresMost patients seek medical attentionbecause of an abdominal mass or pain{139,2460,2461}. A few patients presentwith abnormal vaginal bleeding.
MacroscopyMalignant Brenner tumours are typicallylarge with a median diameter of 16-20cm and typically have a solid componentresembling benign Brenner tumour aswell as cysts containing papillary or poly-poid masses {2461}.
Tumour spread and stagingMalignant Brenner tumours are bilateralin 12% of cases {139,452}. About 80% ofmalignant Brenner tumours are stage 1at the time of diagnosis.
HistopathologyIn malignant Brenner tumours there iss t romal invasion associated with abenign or borderline Brenner tumourcomponent {139}. The invasive elementis usually high grade transitional cell car-cinoma or squamous cell carc i n o m a ,although occasional tumours are com-posed of crowded, irregular islands ofmalignant transitional cells with lowgrade features {2460}. Glandular ele-ments may be admixed, but pure muci-nous or serous carcinomas associatedwith a benign Brenner tumour compo-nent should not be diagnosed as amalignant Brenner tumour. Foci of calcifi-cation are occasionally prominent.
ImmunoprofileThe very small number of malignantBrenner tumours studied have exhibiteda benign Brenner tumour immunoprofilein that component with a variable patternof antigen expression in the invasivecomponent; uroplakin immunopositivityhas occurred in some {2371}.
Prognosis and predictive factorsWhen confined to the ovary, malignantB renner tumours have an excellent pro g-nosis. Patients with stage IA tumourshave an 88% 5-year survival, and thosewith high stage malignant Bre n n e rtumours have a better prognosis thanstage matched transitional cell carc i n o-mas {139}.
Borderline Brenner tumour
SynonymsBrenner tumour of low malignant poten-tial, proliferating Brenner tumour (forcases with low grade features).
DefinitionAn ovarian transitional cell tumour of lowmalignant potential with atypical ormalignant features of the epithelium butlacking obvious stromal invasion.
EpidemiologyOnly 3-5% of Brenner tumours are bor-derline {1110,1868}.
Tumour spread and stagingBorderline Brenner tumours are confinedto the ovary and, with rare exceptions,have been unilateral {1110,1868,2461,3144}.
Clinical featuresMost patients seek medical attentionbecause of an abdominal mass or pain{139,2460,2461}. A few patients presentwith abnormal vaginal bleeding.
MacroscopyBorderline Brenner tumours are typicallylarge with a median diameter of 16-20cm. They usually have a solid componentresembling benign Brenner tumour aswell as a cystic component containing apapillary or polypoid mass {2461}.
HistopathologyB o rderline Brenner tumours show agreater degree of architectural complex-ity than benign Brenner tumours typifiedby branching fibrovascular papillae sur-faced by transitional epithelium oftenprotruding into cystic spaces. The transi-tional epithelium manifests the samespectrum of architectural and cytologicalfeatures encountered in urothelial lesionsof the urinary tract. By definition, there isno stromal invasion. A benign Brennertumour component is typically presentbut may be small and easily overlooked.The mitotic rate is highly variable but maybe brisk, and focal necrosis is common.Mucinous metaplasia may be a promi-nent feature. The diagnostic criteria andterminology applied to the intermediateg roup of transitional cell tumours issomewhat controversial {2461,2605}.Some have advocated categorizingtumours with low grade features as "pro-liferating" rather than borderline {2461},and others designate those resemblinggrade 2 or 3 transitional cell carcinoma ofthe urinary tract as "borderline withintraepithelial carcinoma" {2605}.
Prognosis and predictive factorsNo Brenner tumour in the intermediatecategory without stromal invasion hasmetastasized or caused the death of apatient {1110,2461}.
Benign Brenner tumour
DefinitionAn ovarian transitional cell tumour com-posed of mature urothelial-like cellsarranged in solid or cystic circumscribedaggregates within a predominantly fibro-matous stroma.
EpidemiologyBenign Brenner tumours account for 4-5% of benign ovarian epithelial tumours{1409,1502,1970,2865}. Most benignBrenner tumours (95%) are diagnosed inwomen 30-60 years old {753,905,1868,2460,2461,2676,2685,3073,3186}.
Clinical featuresThe majority of patients with benignBrenner tumours are asymptomatic; over50% of tumours are less than 2 cm andare typically discovered incidentally inovaries removed for some other reason{753,905,2685,3073}. In only 10% ofcases is the tumour larger than 10 cm;
Fig. 2.52 Benign Brenner tumour. Sectioned sur-face is firm, lobulated and fibroma-like with a smallcystic component.
142 Tumours of the ovary and peritoneum
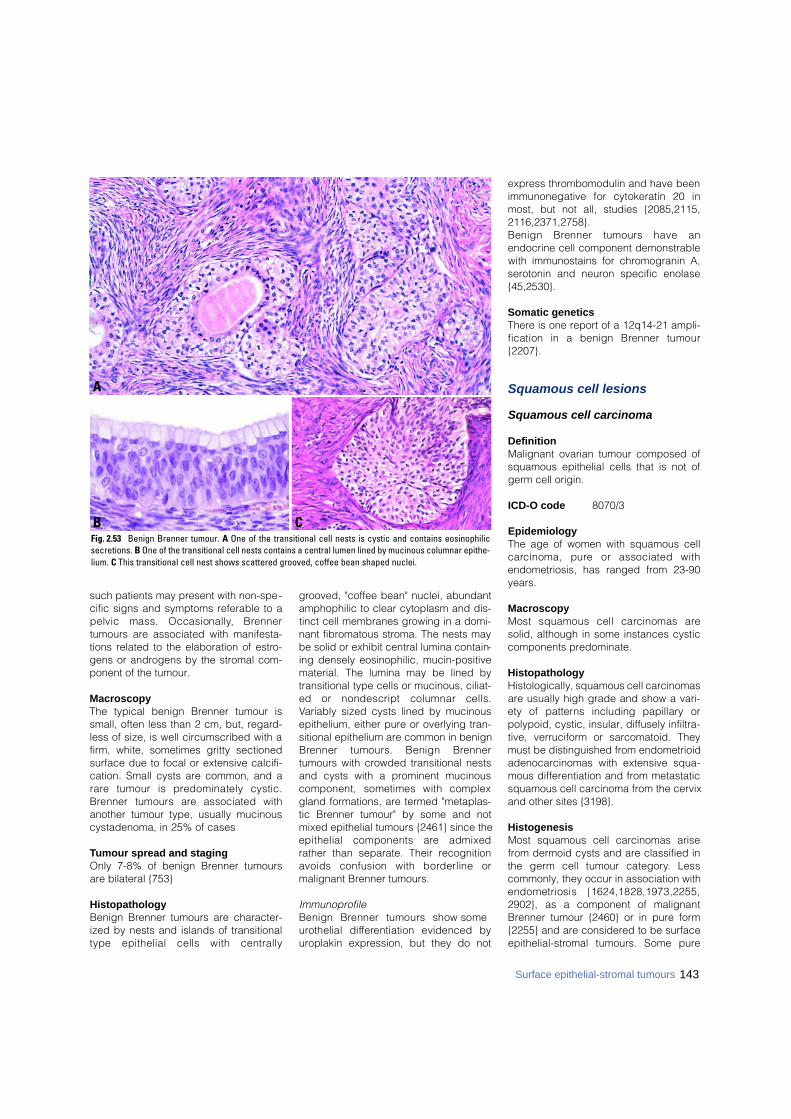
such patients may present with non-spe-cific signs and symptoms referable to apelvic mass. Occasionally, Bre n n e rtumours are associated with manifesta-tions related to the elaboration of estro-gens or androgens by the stromal com-ponent of the tumour.
MacroscopyThe typical benign Brenner tumour issmall, often less than 2 cm, but, regard-less of size, is well circumscribed with afirm, white, sometimes gritty sectionedsurface due to focal or extensive calcifi-cation. Small cysts are common, and ar a re tumour is predominately cystic.B renner tumours are associated withanother tumour type, usually mucinouscystadenoma, in 25% of cases
Tumour spread and stagingOnly 7-8% of benign Brenner tumoursare bilateral {753}
HistopathologyBenign Brenner tumours are character-ized by nests and islands of transitionaltype epithelial cells with centrally
grooved, "coffee bean" nuclei, abundantamphophilic to clear cytoplasm and dis-tinct cell membranes growing in a domi-nant fibromatous stroma. The nests maybe solid or exhibit central lumina contain-ing densely eosinophilic, mucin-positivematerial. The lumina may be lined bytransitional type cells or mucinous, ciliat-ed or nondescript columnar cells.Variably sized cysts lined by mucinousepithelium, either pure or overlying tran-sitional epithelium are common in benignB renner tumours. Benign Bre n n e rtumours with crowded transitional nestsand cysts with a prominent mucinouscomponent, sometimes with complexgland formations, are termed "metaplas-tic Brenner tumour" by some and notmixed epithelial tumours {2461} since theepithelial components are admixedrather than separate. Their recognitionavoids confusion with borderline ormalignant Brenner tumours.
ImmunoprofileBenign Brenner tumours show someu rothelial diff e rentiation evidenced byuroplakin expression, but they do not
express thrombomodulin and have beenimmunonegative for cytokeratin 20 inmost, but not all, studies {2085,2115,2116,2371,2758}.Benign Brenner tumours have anendocrine cell component demonstrablewith immunostains for chromogranin A,serotonin and neuron specific enolase{45,2530}.
Somatic geneticsThere is one report of a 12q14-21 ampli-fication in a benign Brenner tumour{2207}.
Squamous cell lesions
Squamous cell carcinoma
DefinitionMalignant ovarian tumour composed ofsquamous epithelial cells that is not ofgerm cell origin.
ICD-O code 8070/3
EpidemiologyThe age of women with squamous cellc a rcinoma, pure or associated withendometriosis, has ranged from 23-90years.
MacroscopyMost squamous cell carcinomas aresolid, although in some instances cysticcomponents predominate.
HistopathologyHistologically, squamous cell carcinomasare usually high grade and show a vari-ety of patterns including papillary orpolypoid, cystic, insular, diffusely infiltra-tive, verruciform or sarcomatoid. Theymust be distinguished from endometrioidadenocarcinomas with extensive squa-mous differentiation and from metastaticsquamous cell carcinoma from the cervixand other sites {3198}.
HistogenesisMost squamous cell carcinomas arisefrom dermoid cysts and are classified inthe germ cell tumour category. Lesscommonly, they occur in association withendometriosis {1624,1828,1973,2255,2902}, as a component of malignantBrenner tumour {2460} or in pure form{2255} and are considered to be surfacee p i t h e l i a l - s t romal tumours. Some pure
143Surface epithelial-stromal tumours
CB
A
Fig. 2.53 Benign Brenner tumour. A One of the transitional cell nests is cystic and contains eosinophilicsecretions. B One of the transitional cell nests contains a central lumen lined by mucinous columnar epithe-lium. C This transitional cell nest shows scattered grooved, coffee bean shaped nuclei.

144 Tumours of the ovary and peritoneum
squamous cell carcinomas haveoccurred in women with cervical squa-mous cell carcinoma in situ {1738}.
Prognosis and predictive factorsMost tumours have spread beyond theovary at the time of presentation, and theprognosis in the small number of report-ed cases is poor.
Epidermoid cyst
DefinitionBenign ovarian cysts lined by squamousepithelial cells that are not clearly ofgerm cell origin.
HistopathologyEpidermoid cysts lined by benign kera-tinized squamous epithelium devoid ofskin appendages and unaccompaniedby teratomatous elements are rare in the
ovary {823,3205}. All are small (2-46 mm)and unilateral.
HistogenesisThe presence of small epithelial cellnests resembling Walthard cell nests inthe walls of epidermoid cysts suggestsan epithelial rather than a teratomatousorigin {3205}.
Mixed epithelial tumours
DefinitionAn ovarian epithelial tumour composedof an admixture of two or more of the fivemajor cell types: serous, mucinous,endometrioid, clear cell andBrenner/transitional. The second or sec-ond and third cell types must comprisealone or together at least 10% of thetumour epithelium, or, in the case of a
mixed Brenner-mucinous cystic tumour,both components should be macroscop-ically visible. A mixed epithelial tumour(MET) may be benign, borderline ormalignant. Endometrioid tumours withsquamous differentiation and neuroen-docrine tumours associated with a sur-face epithelial-stromal tumour are notincluded in this definition.
ICD-O codesMalignant mixed epithelial tumour 8323/3B o rderline mixed epithelial tumour 8323/1Benign mixed epithelial tumour 8323/0
EpidemiologyThe reported incidence of MET variesfrom 0.5-4% of surface epithelial-stromaltumours. This variability is due in part toproblems in developing a standardizedclassification.
Tumour spread and staging Mixed epithelial borderline tumours(MEBTs) are stage I in 93% of cases andshow bilateral ovarian involvement in22% {2496}.
HistopathologyIn cystadenomas the most frequent mix-ture is serous (ciliated) and mucinousepithelium. The mucinous epitheliumshould contain abundant intracytoplas-mic mucin, not just apical or luminalmucin. MEBTs show papillae withdetached cell clusters reminiscent ofserous borderline tumours, but they gen-erally contain a mixture of endocervical-like mucinous cells, endometrioid epithe-lium with focal squamous differentiationand indifferent eosinophilic epithelium.An acute inflammatory infiltrate is fre-quently seen. Microinvasion may beseen rare l y. Mixed Bre n n e r- m u c i n o u stumours are usually composed of abenign, and, occasionally, a borderlineBrenner component; the mucinous com-ponent may be benign, borderline ormalignant. A few mucinous glands withinBrenner nests or histological areas ofmucinous differentiation represent muci-nous metaplasia in Brenner tumours, acommon finding, and are not a MET.Rarely, the tumour macroscopically con-tains a myriad of small cysts lined by anadmixture of mucinous and transitionalepithelium and the term metaplasticBrenner tumour is applied {2461}. Forc y s t a d e n o c a rcinomas frequent combi-nations are serous and endometrioid,
Fig. 2.54 Undifferentiated carcinoma of the ovary. A Sheets of tumour cells with small cystic spaces areseparated by irregular fibrous septa. B Aggregates of undifferentiated tumour cells with pleomorphic nucleiand frequent mitotic figures are separated by thin bands of fibrous stroma.
A
B

145Surface epithelial-stromal tumours
serous and transitional cell carcinomaand endometrioid and clear cell.
GradingThe least diff e rentiated componentdetermines the tumour grade.
HistogenesisEndometriosis, occasionally with atypia,is found in association with 53% of MEBT{2496} and up to 50% of mixed clear cell-endometrioid tumours {2511}. Somecases show a transition from endometrio-sis to neoplastic epithelium.
Somatic geneticsIt is impossible to make broad state-ments, as studies are limited to a fewcases. LOH on chromosome 17, com-mon in serous tumours, has been foundin two of five mixed endometrioid-seroustumours {959}. PTEN mutation, which hasbeen associated with the endometrioidtype, has also been noted in a mixedmucinous-endometrioid tumour {2075}.KRAS mutations, an early event in muci-nous tumours, have been noted in threemixed Brenner-mucinous tumours {589}.The mucinous cystadenocarcinoma andB renner tumour components share damplification of 12q 14-21 in one MET,suggesting clonal relatedness {2207}.
Prognosis and predictive factorsThe behaviour of MEBT is similar to that ofendocervical-like mucinous bord e r l i n etumours. The dominant cell type general-ly dictates behaviour. An exception ismixed endometrioid and serous carcino-ma, which, even when the serous com-ponent is minor, behaves more aggres-sively than pure endometrioid carcinomaand similarly to their serous counterpart.Mixed endometrioid and serous carc i n o-ma may recur as serous carc i n o m a{2907}. This finding stresses the impor-tance of careful sampling of anendometrioid cystadenocarcinoma to ruleout a mixed serous component.
Undifferentiated carcinoma
D e f i n i t i o nA primary ovarian carcinoma with no dif-f e rentiation or only small foci of diff e re n t i-ation.
ICD-O code 8 0 2 0 / 3
E p i d e m i o l o g yWhen applying the WHO criteria, appro x-imately 4-5% of ovarian cancers are undif-f e rentiated carcinoma. The frequency ofu n d i ff e rentiated carcinoma was 4.1%when defined as carcinomas with solida reas as the predominant component re p-resenting over 50% of the tumour {2677}.
Clinical featuresIn the only large series the age of thepatients ranged from 39-72 (mean, 54years) {2677}.
M a c r o s c o p yM a c ro s c o p i c a l l y, undiff e rentiated carc i n o-ma does not have specific features. Thetumours are predominantly solid, usuallywith extensive areas of necrosis.
Tumour spread and stagingA c c o rding to FIGO, 6% of the patients ared i s c o v e red in stage I, 3% are in stage II,74% in stage III and 17% in stage IV; thus91% of the tumours are discovered instages III and IV {2677}.
H i s t o p a t h o l o g yH i s t o l o g i c a l l y, undiff e rentiated carc i n o m aconsists of solid groups of tumour cellswith numerous mitotic figures and signifi-cant cytological atypia. Areas with a spin-dle cell component, microcystic patternand focal vascular invasion can be seen.It is unusual to see an undiff e re n t i a t e dc a rcinoma without any other componentof müllerian carcinoma. Usually, areas ofhigh grade serous carcinoma are pre s e n t .Foci of transitional cell carcinoma canalso be seen. Undiff e rentiated carc i n o m aof the ovary does not have a specifici m m u n o p h e n o t y p e .
D i ff e rential diagnosisThe main diff e rential diagnoses are gran-ulosa cell tumour of the adult type, transi-tional cell carcinoma, poorly diff e re n t i a t e dsquamous cell carcinoma, small cell car-cinoma and metastatic undiff e re n t i a t e dc a rcinoma. Granulosa cell tumours may have a dif-fuse pattern; however, it is unusual not tohave also areas with a trabecular pattern ,Call-Exner bodies or areas showing sexc o rds. In addition, undiff e rentiated carc i-
noma is a more anaplastic tumour with alarger number of mitotic figures. Transitional cell carcinomas might havea reas of undiff e rentiated tumour; however,either a trabecular pattern or large papil-lae are always identified in the form e r. Small cell carcinoma of the hyperc a l-caemic type typically occurs in youngwomen and often contains follicle-likes t r u c t u res. The cells of small cell carc i n o-ma of the pulmonary type show nuclearmolding and have high nuclear to cyto-plasmic ratios.F i n a l l y, metastatic undiff e rentiated carc i-nomas are uniform tumours without papil-l a ry areas. All these diff e rential diagnoses can usual-ly be resolved when the tumour is wellsampled, and areas with a diff e re n tm a c roscopic appearance are submitted.Sampling will identify the diff e rent compo-nents of the tumour that are characteristicof primary ovarian lesions.
Prognosis and predictive factorsThe five-year survival of patients withu n d i ff e rentiated carcinoma is worse thanthat of ovarian serous or transitional cellc a rcinoma. Only 6% of these patients sur-vive for 5 years.
Unclassified adenocarcinoma
D e f i n i t i o nA primary ovarian adenocarcinoma thatcannot be classified as one of the specif-ic types of müllerian adenocarc i n o m abecause it has overlapping features or isnot sufficiently diff e rentiated. Thesetumours are uncommon.
ICD-O code 8 1 4 0 / 3
H i s t o p a t h o l o g yTumours in this category would includewell or moderately diff e rentiated tumourswith overlapping features such as a muci-nous tumour with cilia, or it might includea less diff e rentiated tumour without dis-tinctive features of one of the mûlleriantypes of adenocarcoma.
Prognosis and predictive factorsSince this group of tumours has not yetbeen specifically studied, the prognosis isnot known.

DefinitionOvarian tumours composed of granulosacells, theca cells, Sertoli cells, Leydigcells and fibroblasts of stromal origin,singly or in various combinations. Overall,sex cord - s t romal tumours account forabout 8% of ovarian neoplasms.
DefinitionTumours containing granulosa cells, the-ca cells or stromal cells resembling fib-roblasts or any combination of such cells.
Granulosa cell tumour group
DefinitionA neoplasm composed of a pure or at theleast a 10% population of granulosa cellsoften in a fibrothecomatous background.Two major subtypes are recognized, anadult and a juvenile type.
ICD-O codesGranulosa cell tumour group
Adult granulosa cell tumour 8620/1Juvenile granulosa cell tumour 8622/1
EpidemiologyGranulosa cell tumours account for ap-p roximately 1.5% (range, 0.6-3%) of allovarian tumours. The neoplasm occurs in
a wide age range including newborn in-fants and postmenopausal women. About5% occur prior to pubert y, whereas almost60% occur after menopause {284,2588}.
AetiologyThe aetiology of these tumours is un-known. Several studies suggest that in-f e rtile women and those exposed to ovu-lation induction agents have an incre a s e drisk for granulosa cell tumours {2458,2 9 8 2 , 3 1 2 5 } .
Clinical featuresSigns and symptomsGranulosa cell tumours may present asan abdominal mass, with symptoms sug-gestive of a functioning ovarian tumour orboth. About 5-15% present with symp-toms suggestive of haemoperitoneumsecondary to rupture of a cystic lesion{3195}. Ascites develops in about 10% ofthe cases. The tumour is clinically occultin 10% of the patients {829}. Granulosacell tumours produce or store a variety ofsteroid hormones. When functional, mostare estrogenic, but rarely androgenic ac-tivity may occur. The symptoms and clin-ical presentation vary depending on thepatient’s age and reproductive status. Inprepubertal girls, granulosa cell tumoursfrequently induce isosexual pseudopre-cocious puberty. In women of reproduc-tive age, the tumour may be associatedwith a variety of menstrual disord e r srelated to hyperoestrinism. In postmeno-pausal women, irregular uterine bleeding
due to various types of endometrial hyper-plasia or, rare l y, well diff e rentiated ade-nocarcinoma is the most common mani-festation of hyperoestrinism. A rare uni-locular thin-walled cystic variant is oftenandrogenic when functional {1971,2059}.
ImagingCross sectional imaging, i.e. computedtomography and magnetic re s o n a n c eimaging is of value in the surgical plan-ning and preoperative determination ofresectability of patients with granulosacell tumours {859,1480,1728,1915,2131}.In contradistinction to epithelial ovariantumours, granulosa cell tumours havebeen described as predominantly solidadnexal lesions; variable amounts of cys-tic components may, however, be pres-ent. Enlargement of the uterus andendometrial thickening might be seen asa result of the hormone production of thetumour {859,1480,1728,1915,2131}.
Adult granulosa cell tumour
EpidemiologyMore than 95% of granulosa cell tumoursare of the adult type, which occurs inmiddle aged to postmenopausal women.
MacroscopyAdult granulosa cell tumours (AGCTs) aretypically unilateral (95%) with an averagesize of 12.5 cm and are commonly encap-sulated with a smooth or lobulated sur-face. The sectioned surface of the tumour
F.A. Tavassoli S. Fujii E. Mooney T. KiyokawaD.J. Gersell P. SchwartzW.G. McCluggage R.A. Kubik-HuchI. Konishi L.M. Roth
Sex cord-stromal tumours
BAFig. 2.56 Adult granulosa cell tumour, microfollicular pattern. A An aggregate of neoplastic granulosa cellscontains numerous Call-Exner bodies. B The Call-Exner bodies contain fluid and/or pyknotic nuclei; thetumour cells have scant cytoplasm and longitudinal nuclear grooves.
Fig. 2.55 Granulosa cell tumour. Axial contrast-enhanced computed tomography image of thepelvis shows a large, well defined, multicystic mass.
Tumours of the ovary and peritoneum
Granulosa-stromal celltumours
146
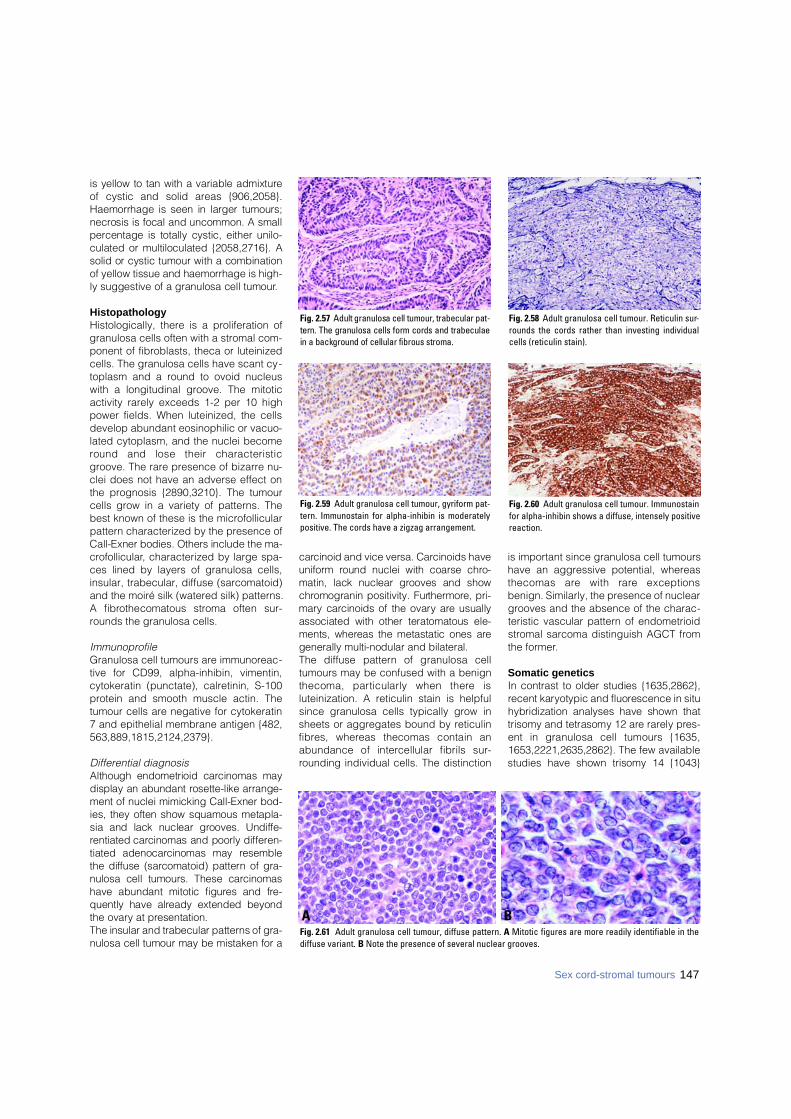
147
is yellow to tan with a variable admixtureof cystic and solid areas {906,2058}.Haemorrhage is seen in larger tumours;n e c rosis is focal and uncommon. A smallp e rcentage is totally cystic, either unilo-culated or multiloculated {2058,2716}. Asolid or cystic tumour with a combinationof yellow tissue and haemorrhage is high-ly suggestive of a granulosa cell tumour.
Histopathology Histologically, there is a proliferation ofgranulosa cells often with a stromal com-ponent of fibroblasts, theca or luteinizedcells. The granulosa cells have scant cy-toplasm and a round to ovoid nucleuswith a longitudinal groove. The mitoticactivity rarely exceeds 1-2 per 10 highpower fields. When luteinized, the cellsdevelop abundant eosinophilic or vacuo-lated cytoplasm, and the nuclei becomeround and lose their characteristicgroove. The rare presence of bizarre nu-clei does not have an adverse effect onthe prognosis {2890,3210}. The tumourcells grow in a variety of patterns. Thebest known of these is the microfollicularpattern characterized by the presence ofCall-Exner bodies. Others include the ma-c ro f o l l i c u l a r, characterized by large spa-ces lined by layers of granulosa cells,insular, trabecular, diffuse (sarcomatoid)and the moiré silk (watered silk) patterns.A fibrothecomatous stroma often sur-rounds the granulosa cells.
ImmunoprofileGranulosa cell tumours are immunoreac-tive for CD99, alpha-inhibin, vimentin,cytokeratin (punctate), calretinin, S-100protein and smooth muscle actin. Thetumour cells are negative for cytokeratin7 and epithelial membrane antigen {482,563,889,1815,2124,2379}.
Differential diagnosisAlthough endometrioid carcinomas maydisplay an abundant rosette-like arrange-ment of nuclei mimicking Call-Exner bod-ies, they often show squamous metapla-sia and lack nuclear grooves. Undiff e-rentiated carcinomas and poorly diff e re n-tiated adenocarcinomas may re s e m b l ethe diffuse (sarcomatoid) pattern of gra-nulosa cell tumours. These carc i n o m a shave abundant mitotic figures and fre-quently have already extended beyondthe ovary at presentation. The insular and trabecular patterns of gra-nulosa cell tumour may be mistaken for a
c a rcinoid and vice versa. Carcinoids haveu n i f o rm round nuclei with coarse chro-matin, lack nuclear grooves and showc h romogranin positivity. Furt h e rm o re, pri-m a ry carcinoids of the ovary are usuallyassociated with other teratomatous ele-ments, whereas the metastatic ones aregenerally multi-nodular and bilateral. The diffuse pattern of granulosa celltumours may be confused with a benignthecoma, particularly when there isluteinization. A reticulin stain is helpfulsince granulosa cells typically grow insheets or aggregates bound by reticulinf i b res, whereas thecomas contain anabundance of intercellular fibrils sur-rounding individual cells. The distinction
is important since granulosa cell tumourshave an aggressive potential, whereasthecomas are with rare exceptionsbenign. Similarly, the presence of nucleargrooves and the absence of the charac-teristic vascular pattern of endometrioidstromal sarcoma distinguish AGCT fromthe former.
Somatic geneticsIn contrast to older studies {1635,2862},recent karyotypic and fluorescence in situhybridization analyses have shown thattrisomy and tetrasomy 12 are rarely pre s-ent in granulosa cell tumours {1635,1653,2221,2635,2862}. The few availablestudies have shown trisomy 14 {1043}
Fig. 2.57 Adult granulosa cell tumour, trabecular pat-tern. The granulosa cells form cords and trabeculaein a background of cellular fibrous stroma.
Fig. 2.58 Adult granulosa cell tumour. Reticulin sur-rounds the cords rather than investing individualcells (reticulin stain).
Sex cord-stromal tumours
BAFig. 2.61 Adult granulosa cell tumour, diffuse pattern. A Mitotic figures are more readily identifiable in thediffuse variant. B Note the presence of several nuclear grooves.
Fig. 2.59 Adult granulosa cell tumour, gyriform pat-tern. Immunostain for alpha-inhibin is moderatelypositive. The cords have a zigzag arrangement.
Fig. 2.60 Adult granulosa cell tumour. Immunostainfor alpha-inhibin shows a diffuse, intensely positivereaction.
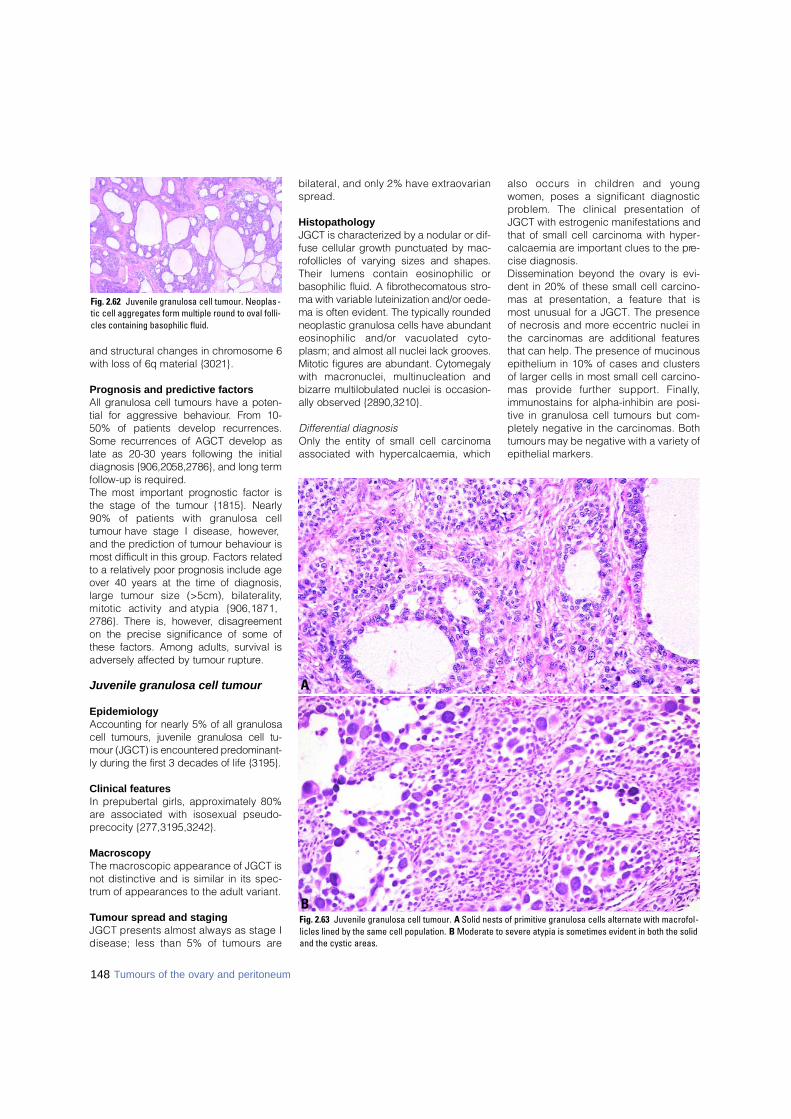
148
and structural changes in chromosome 6with loss of 6q material {3021}.
Prognosis and predictive factors All granulosa cell tumours have a poten-tial for aggressive behaviour. From 10-50% of patients develop re c u r re n c e s .Some re c u r rences of AGCT develop aslate as 20-30 years following the initialdiagnosis {906,2058,2786}, and long termfollow-up is re q u i red. The most important prognostic factor isthe stage of the tumour {1815}. Nearly90% of patients with granulosa celltumour have stage I disease, however,and the prediction of tumour behaviour ismost difficult in this group. Factors re l a t e dto a relatively poor prognosis include ageover 40 years at the time of diagnosis,large tumour size (>5cm), bilaterality,mitotic activity and atypia {906,1871,2786}. There is, however, disagre e m e n ton the precise significance of some ofthese factors. Among adults, survival isadversely affected by tumour rupture .
Juvenile granulosa cell tumour
EpidemiologyAccounting for nearly 5% of all granulosacell tumours, juvenile granulosa cell tu-mour (JGCT) is encountered pre d o m i n a n t-ly during the first 3 decades of life {3195}.
Clinical featuresIn prepubertal girls, approximately 80%are associated with isosexual pseudo-precocity {277,3195,3242}.
MacroscopyThe macroscopic appearance of JGCT isnot distinctive and is similar in its spec-trum of appearances to the adult variant.
Tumour spread and stagingJGCT presents almost always as stage Idisease; less than 5% of tumours are
bilateral, and only 2% have extraovarians p re a d .
HistopathologyJGCT is characterized by a nodular or dif-fuse cellular growth punctuated by mac-rofollicles of varying sizes and shapes.Their lumens contain eosinophilic orbasophilic fluid. A fibrothecomatous stro-ma with variable luteinization and/or oede-ma is often evident. The typically ro u n d e dneoplastic granulosa cells have abundanteosinophilic and/or vacuolated cyto-plasm; and almost all nuclei lack gro o v e s .Mitotic figures are abundant. Cytomegalywith macronuclei, multinucleation andb i z a r re multilobulated nuclei is occasion-ally observed {2890,3210}.
Differential diagnosisOnly the entity of small cell carcinomaassociated with hypercalcaemia, which
also occurs in children and youngwomen, poses a significant diagnosticp roblem. The clinical presentation ofJGCT with estrogenic manifestations andthat of small cell carcinoma with hyper-calcaemia are important clues to the pre-cise diagnosis. Dissemination beyond the ovary is evi-dent in 20% of these small cell carcino-mas at presentation, a feature that ismost unusual for a JGCT. The presenceof necrosis and more eccentric nuclei inthe carcinomas are additional featuresthat can help. The presence of mucinousepithelium in 10% of cases and clustersof larger cells in most small cell carcino-mas provide further support. Finally,immunostains for alpha-inhibin are posi-tive in granulosa cell tumours but com-pletely negative in the carcinomas. Bothtumours may be negative with a variety ofepithelial markers.
Fig. 2.63 Juvenile granulosa cell tumour. A Solid nests of primitive granulosa cells alternate with macrofol-licles lined by the same cell population. B Moderate to severe atypia is sometimes evident in both the solidand the cystic areas.
B
A
Tumours of the ovary and peritoneum
Fig. 2.62 Juvenile granulosa cell tumour. Neoplas -tic cell aggregates form multiple round to oval folli-cles containing basophilic fluid.
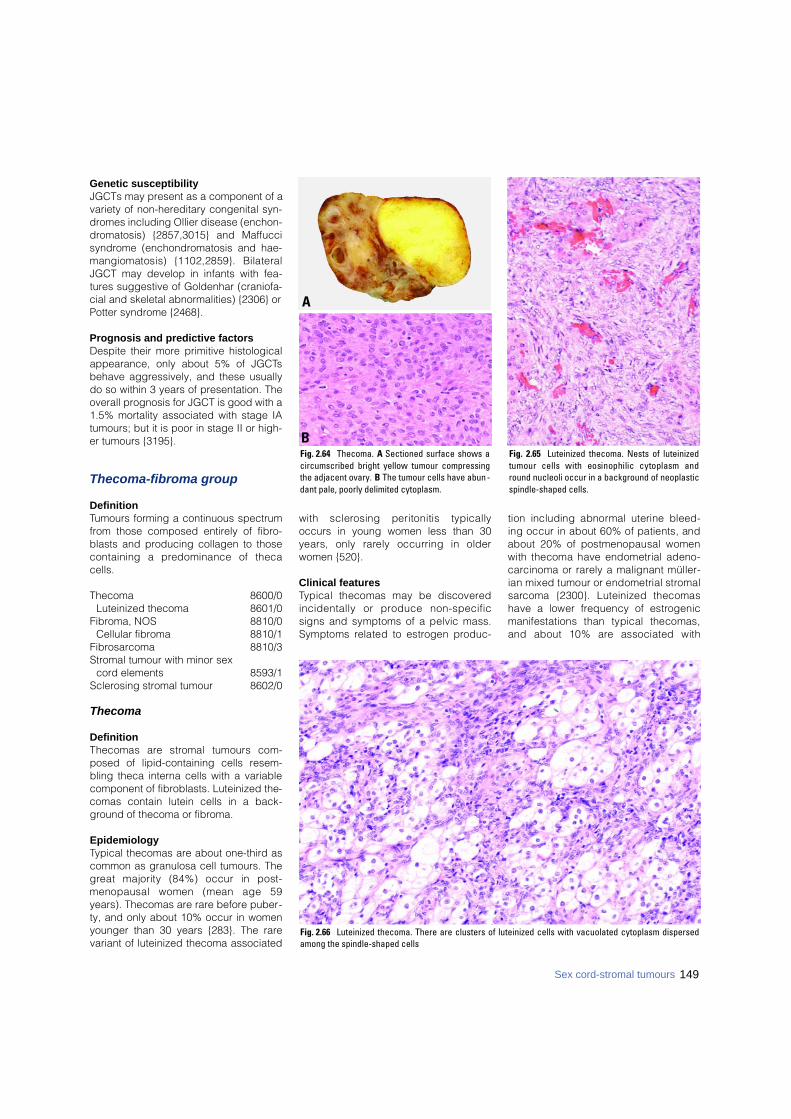
Genetic susceptibilityJGCTs may present as a component of avariety of non-hereditary congenital syn-dromes including Ollier disease (enchon-dromatosis) {2857,3015} and Maffuccisyndrome (enchondromatosis and hae-mangiomatosis) {1102,2859}. BilateralJGCT may develop in infants with fea-tures suggestive of Goldenhar (craniofa-cial and skeletal abnormalities) {2306} orPotter syndrome {2468}.
Prognosis and predictive factors Despite their more primitive histologicalappearance, only about 5% of JGCTsbehave aggressively, and these usuallydo so within 3 years of presentation. Theoverall prognosis for JGCT is good with a1.5% mortality associated with stage IAtumours; but it is poor in stage II or high-er tumours {3195}.
Thecoma-fibroma group
DefinitionTumours forming a continuous spectrumfrom those composed entirely of fibro-blasts and producing collagen to thosecontaining a predominance of thecacells.
Thecoma 8600/0Luteinized thecoma 8601/0
Fibroma, NOS 8810/0Cellular fibroma 8810/1
Fibrosarcoma 8810/3Stromal tumour with minor sex
cord elements 8593/1Sclerosing stromal tumour 8602/0
Thecoma
DefinitionThecomas are stromal tumours com-posed of lipid-containing cells resem-bling theca interna cells with a variablecomponent of fibroblasts. Luteinized the-comas contain lutein cells in a back-ground of thecoma or fibroma.
EpidemiologyTypical thecomas are about one-third ascommon as granulosa cell tumours. Theg reat majority (84%) occur in post-menopausal women (mean age 59years). Thecomas are rare before puber-ty, and only about 10% occur in womenyounger than 30 years {283}. The rarevariant of luteinized thecoma associated
with sclerosing peritonitis typicallyoccurs in young women less than 30years, only rarely occurring in olderwomen {520}.
Clinical featuresTypical thecomas may be discovere dincidentally or produce non-specificsigns and symptoms of a pelvic mass.Symptoms related to estrogen pro d u c-
tion including abnormal uterine bleed-ing occur in about 60% of patients, andabout 20% of postmenopausal womenwith thecoma have endometrial adeno-c a rcinoma or rarely a malignant müller-ian mixed tumour or endometrial stro m a ls a rcoma {2300}. Luteinized thecomashave a lower frequency of estro g e n i cmanifestations than typical thecomas,and about 10% are associated with
Fig. 2.65 Luteinized thecoma. Nests of luteinizedtumour cells with eosinophilic cytoplasm andround nucleoli occur in a background of neoplasticspindle-shaped cells.
Fig. 2.64 Thecoma. A Sectioned surface shows acircumscribed bright yellow tumour compressingthe adjacent ovary. B The tumour cells have abun -dant pale, poorly delimited cytoplasm.
A
B
Fig. 2.66 Luteinized thecoma. There are clusters of luteinized cells with vacuolated cytoplasm dispersedamong the spindle-shaped cells
149Sex cord-stromal tumours
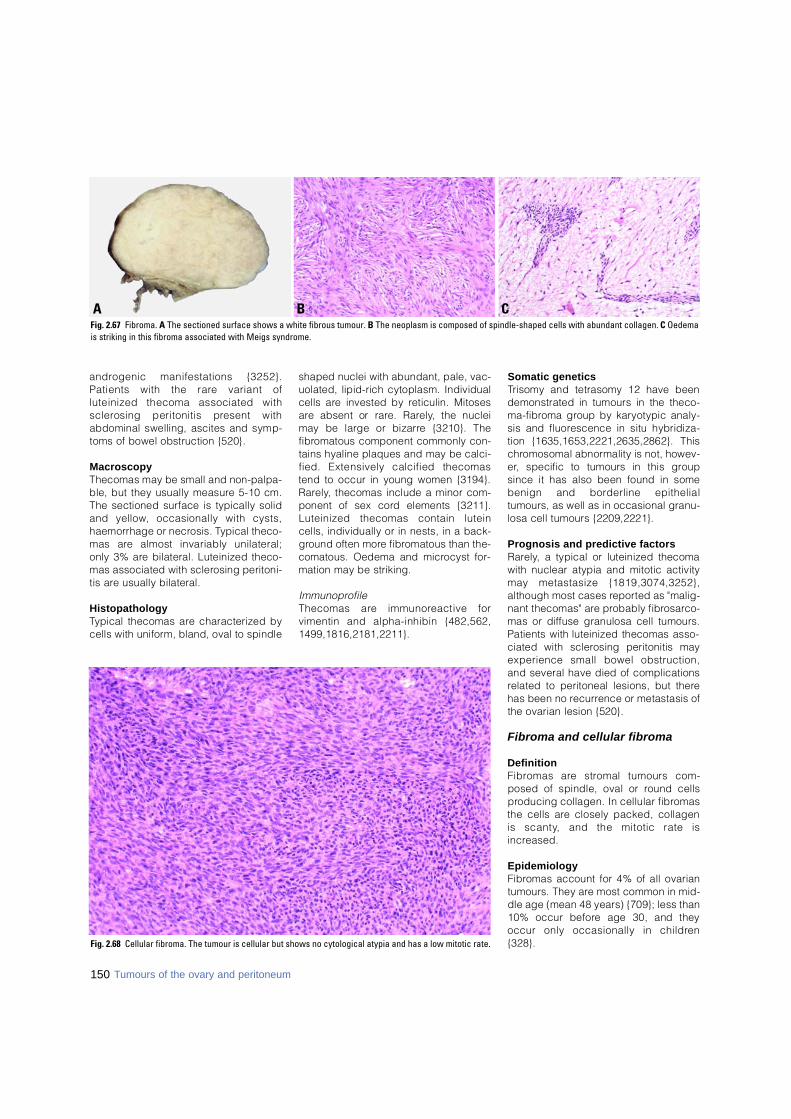
a n d rogenic manifestations {3252}.Patients with the rare variant ofluteinized thecoma associated withs c l e rosing peritonitis present withabdominal swelling, ascites and symp-toms of bowel obstruction {520}.
M a c r o s c o p yThecomas may be small and non-palpa-ble, but they usually measure 5-10 cm.The sectioned surface is typically solidand yellow, occasionally with cysts,haemorrhage or necrosis. Typical theco-mas are almost invariably unilateral;only 3% are bilateral. Luteinized theco-mas associated with sclerosing peritoni-tis are usually bilateral.
H i s t o p a t h o l o g yTypical thecomas are characterized bycells with uniform, bland, oval to spindle
shaped nuclei with abundant, pale, vac-uolated, lipid-rich cytoplasm. Individualcells are invested by reticulin. Mitosesa re absent or rare. Rare l y, the nucleimay be large or bizarre {3210}. Thef i b romatous component commonly con-tains hyaline plaques and may be calci-fied. Extensively calcified thecomastend to occur in young women {3194}.R a re l y, thecomas include a minor com-ponent of sex cord elements {3211}.Luteinized thecomas contain luteincells, individually or in nests, in a back-g round often more fibromatous than the-comatous. Oedema and microcyst for-mation may be striking.
I m m u n o p ro f i l eThecomas are immunoreactive forvimentin and alpha-inhibin {482,562,1 4 9 9 , 1 8 1 6 , 2 1 8 1 , 2 2 1 1 } .
Somatic geneticsTrisomy and tetrasomy 12 have beendemonstrated in tumours in the theco-m a - f i b roma group by karyotypic analy-sis and fluorescence in situ hybridiza-tion {1635,1653,2221,2635,2862}. Thisc h romosomal abnormality is not, howev-e r, specific to tumours in this gro u psince it has also been found in somebenign and borderline epithelialtumours, as well as in occasional granu-losa cell tumours {2209,2221}.
Prognosis and predictive factorsR a re l y, a typical or luteinized thecomawith nuclear atypia and mitotic activitymay metastasize {1819,3074,3252},although most cases re p o rted as "malig-nant thecomas" are probably fibro s a rc o-mas or diffuse granulosa cell tumours.Patients with luteinized thecomas asso-ciated with sclerosing peritonitis mayexperience small bowel obstruction,and several have died of complicationsrelated to peritoneal lesions, but therehas been no re c u r rence or metastasis ofthe ovarian lesion {520}.
Fibroma and cellular fibroma
D e f i n i t i o nF i b romas are stromal tumours com-posed of spindle, oval or round cellsp roducing collagen. In cellular fibro m a sthe cells are closely packed, collagen is scanty, and the mitotic rate isi n c re a s e d .
E p i d e m i o l o g yF i b romas account for 4% of all ovariantumours. They are most common in mid-dle age (mean 48 years) {709}; less than10% occur before age 30, and theyoccur only occasionally in childre n{ 3 2 8 } .Fig. 2.68 Cellular fibroma. The tumour is cellular but shows no cytological atypia and has a low mitotic rate.
B CAFig. 2.67 Fibroma. A The sectioned surface shows a white fibrous tumour. B The neoplasm is composed of spindle-shaped cells with abundant collagen. C Oedemais striking in this fibroma associated with Meigs syndrome.
Tumours of the ovary and peritoneum150
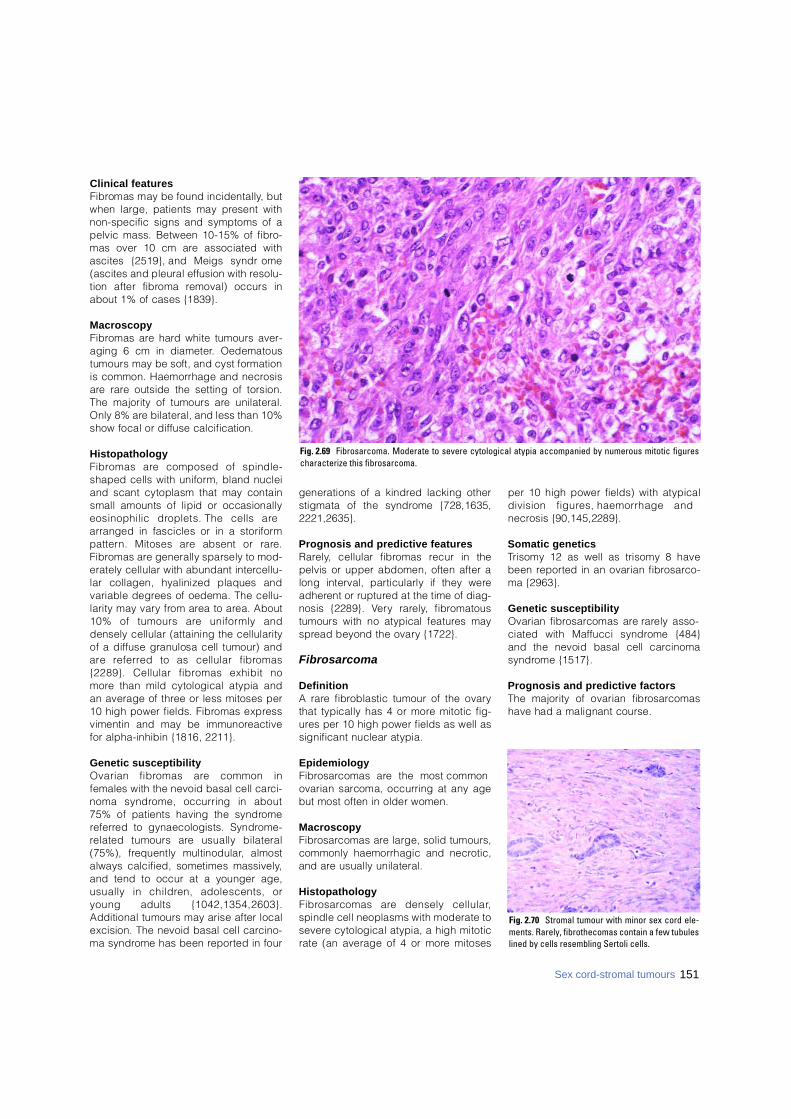
Clinical featuresF i b romas may be found incidentally, butwhen large, patients may present withnon-specific signs and symptoms of apelvic mass. Between 10-15% of fibro-mas over 10 cm are associated withascites {2519}, and Meigs syndro m e(ascites and pleural effusion with re s o l u-tion after fibroma removal) occurs inabout 1% of cases {1839}.
M a c r o s c o p yF i b romas are hard white tumours aver-aging 6 cm in diameter. Oedematoustumours may be soft, and cyst form a t i o nis common. Haemorrhage and necro s i sa re rare outside the setting of torsion.The majority of tumours are unilateral.Only 8% are bilateral, and less than 10%show focal or diffuse calcification.
H i s t o p a t h o l o g yF i b romas are composed of spindle-shaped cells with uniform, bland nucleiand scant cytoplasm that may containsmall amounts of lipid or occasionallyeosinophilic droplets. The cells arearranged in fascicles or in a storiformp a t t e rn. Mitoses are absent or rare .F i b romas are generally sparsely to mod-erately cellular with abundant interc e l l u-lar collagen, hyalinized plaques andvariable degrees of oedema. The cellu-larity may vary from area to area. About10% of tumours are uniformly anddensely cellular (attaining the cellularityof a diffuse granulosa cell tumour) anda re re f e r red to as cellular fibro m a s{2289}. Cellular fibromas exhibit nom o re than mild cytological atypia andan average of three or less mitoses per10 high power fields. Fibromas expre s svimentin and may be immunore a c t i v efor alpha-inhibin {1816, 2211}.
Genetic susceptibilityOvarian fibromas are common infemales with the nevoid basal cell carc i-noma syndrome, occurring in about75% of patients having the syndro m ere f e r red to gynaecologists. Syndro m e -related tumours are usually bilateral(75%), frequently multinodular, almostalways calcified, sometimes massively,and tend to occur at a younger age,usually in children, adolescents, oryoung adults {1042,1354,2603}.Additional tumours may arise after localexcision. The nevoid basal cell carc i n o-ma syndrome has been re p o rted in four
generations of a kindred lacking otherstigmata of the syndrome {728,1635,2 2 2 1 , 2 6 3 5 } .
Prognosis and predictive featuresR a re l y, cellular fibromas recur in thepelvis or upper abdomen, often after along interval, particularly if they werea d h e rent or ruptured at the time of diag-nosis {2289}. Ve ry rare l y, fibro m a t o u stumours with no atypical features mays p read beyond the ovary {1722}.
F i b r o s a r c o m a
D e f i n i t i o nA rare fibroblastic tumour of the ovarythat typically has 4 or more mitotic fig-u res per 10 high power fields as well assignificant nuclear atypia.
E p i d e m i o l o g yF i b ro s a rcomas are the most commonovarian sarcoma, occurring at any agebut most often in older women.
M a c r o s c o p yF i b ro s a rcomas are large, solid tumours,commonly haemorrhagic and necro t i c ,and are usually unilateral.
H i s t o p a t h o l o g yF i b ro s a rcomas are densely cellular,spindle cell neoplasms with moderate tos e v e re cytological atypia, a high mitoticrate (an average of 4 or more mitoses
per 10 high power fields) with atypicaldivision figures, haemorrhage andn e c rosis {90,145,2289}.
Somatic geneticsTrisomy 12 as well as trisomy 8 havebeen re p o rted in an ovarian fibro s a rc o-ma {2963}.
Genetic susceptibilityOvarian fibro s a rcomas are rarely asso-ciated with Maffucci syndrome {484}and the nevoid basal cell carc i n o m as y n d rome {1517}.
Prognosis and predictive factorsThe majority of ovarian fibro s a rc o m a shave had a malignant course.
Fig. 2.69 Fibrosarcoma. Moderate to severe cytological atypia accompanied by numerous mitotic figurescharacterize this fibrosarcoma.
151Sex cord-stromal tumours
Fig. 2.70 Stromal tumour with minor sex cord ele-ments. Rarely, fibrothecomas contain a few tubuleslined by cells resembling Sertoli cells.
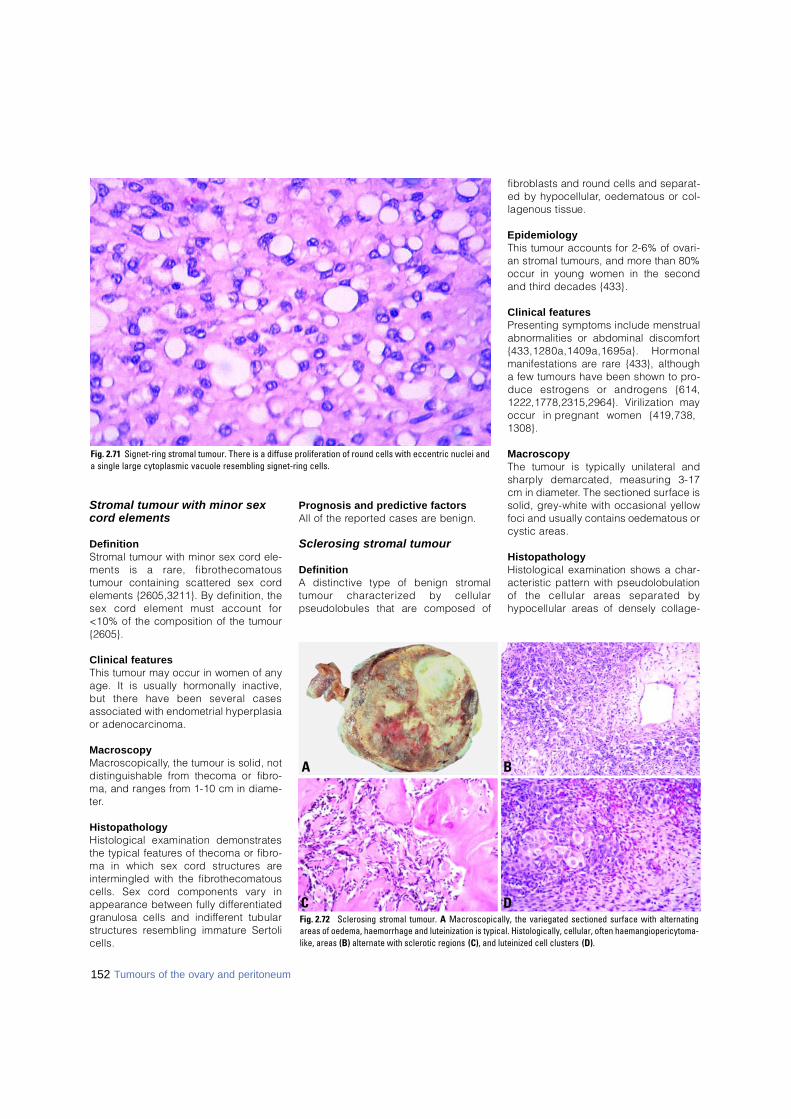
Stromal tumour with minor sexcord elements
D e f i n i t i o nS t romal tumour with minor sex cord ele-ments is a rare, fibro t h e c o m a t o u stumour containing scattered sex cordelements {2605,3211}. By definition, thesex cord element must account for<10% of the composition of the tumour{ 2 6 0 5 } .
Clinical featuresThis tumour may occur in women of anyage. It is usually hormonally inactive,but there have been several casesassociated with endometrial hyperplasiaor adenocarcinoma.
M a c r o s c o p yM a c ro s c o p i c a l l y, the tumour is solid, notdistinguishable from thecoma or fibro-ma, and ranges from 1-10 cm in diame-t e r.
H i s t o p a t h o l o g yHistological examination demonstratesthe typical features of thecoma or fibro-ma in which sex cord structures arei n t e rmingled with the fibro t h e c o m a t o u scells. Sex cord components vary inappearance between fully diff e re n t i a t e dgranulosa cells and indiff e rent tubulars t r u c t u res resembling immature Sert o l ic e l l s .
Prognosis and predictive factorsAll of the re p o rted cases are benign.
Sclerosing stromal tumour
D e f i n i t i o nA distinctive type of benign stro m a ltumour characterized by cellularpseudolobules that are composed of
f i b roblasts and round cells and separat-ed by hypocellular, oedematous or col-lagenous tissue.
E p i d e m i o l o g yThis tumour accounts for 2-6% of ovari-an stromal tumours, and more than 80%occur in young women in the secondand third decades {433}.
Clinical featuresP resenting symptoms include menstruala b n o rmalities or abdominal discomfort{433,1280a,1409a,1695a}. Horm o n a lmanifestations are rare {433}, althougha few tumours have been shown to pro-duce estrogens or androgens {614,1222,1778,2315,2964}. Virilization mayoccur in pregnant women {419,738,1 3 0 8 } .
M a c r o s c o p yThe tumour is typically unilateral andsharply demarcated, measuring 3-17cm in diameter. The sectioned surface issolid, grey-white with occasional yellowfoci and usually contains oedematous orcystic areas.
H i s t o p a t h o l o g yHistological examination shows a char-acteristic pattern with pseudolobulationof the cellular areas separated byhypocellular areas of densely collage-
Fig. 2.71 Signet-ring stromal tumour. There is a diffuse proliferation of round cells with eccentric nuclei anda single large cytoplasmic vacuole resembling signet-ring cells.
BA
DCFig. 2.72 Sclerosing stromal tumour. A Macroscopically, the variegated sectioned surface with alternatingareas of oedema, haemorrhage and luteinization is typical. Histologically, cellular, often haemangiopericytoma-like, areas (B) alternate with sclerotic regions (C), and luteinized cell clusters (D).
152 Tumours of the ovary and peritoneum
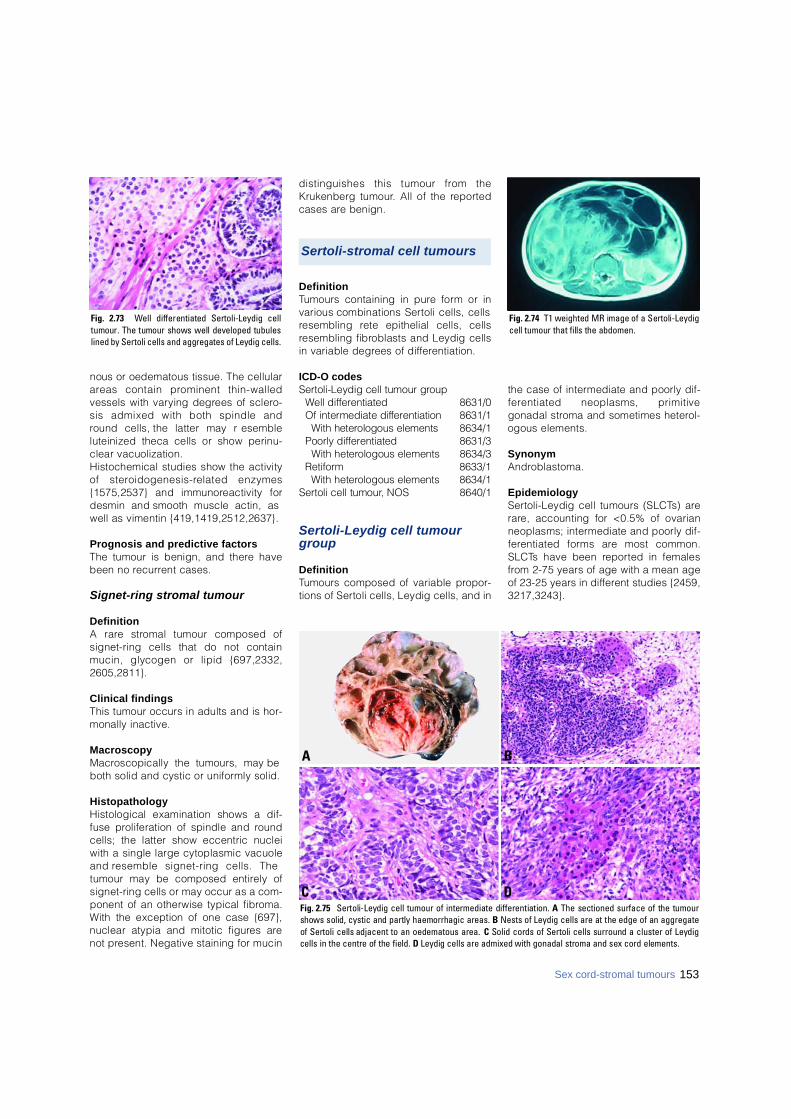
nous or oedematous tissue. The cellulara reas contain prominent thin-walledvessels with varying degrees of sclero-sis admixed with both spindle andround cells, the latter may re s e m b l eluteinized theca cells or show perinu-clear vacuolization.Histochemical studies show the activityof stero i d o g e n e s i s - related enzymes{1575,2537} and immunoreactivity fordesmin and smooth muscle actin, aswell as vimentin {419,1419,2512,2637}.
Prognosis and predictive factorsThe tumour is benign, and there havebeen no re c u r rent cases.
Signet-ring stromal tumour
D e f i n i t i o nA rare stromal tumour composed ofsignet-ring cells that do not containmucin, glycogen or lipid {697,2332,2 6 0 5 , 2 8 1 1 } .
Clinical findingsThis tumour occurs in adults and is hor-monally inactive.
M a c r o s c o p yM a c roscopically the tumours, may beboth solid and cystic or uniformly solid.
H i s t o p a t h o l o g yHistological examination shows a dif-fuse proliferation of spindle and ro u n dcells; the latter show eccentric nucleiwith a single large cytoplasmic vacuoleand resemble signet-ring cells. Thetumour may be composed entirely ofsignet-ring cells or may occur as a com-ponent of an otherwise typical fibro m a .With the exception of one case {697},nuclear atypia and mitotic figures arenot present. Negative staining for mucin
distinguishes this tumour from theKrukenberg tumour. All of the re p o rt e dcases are benign.
D e f i n i t i o nTumours containing in pure form or invarious combinations Sertoli cells, cellsresembling rete epithelial cells, cellsresembling fibroblasts and Leydig cellsin variable degrees of diff e re n t i a t i o n .
ICD-O codesS e rtoli-Leydig cell tumour gro u p
Well diff e re n t i a t e d 8 6 3 1 / 0Of intermediate diff e re n t i a t i o n 8631/1
With heterologous elements 8 6 3 4 / 1Poorly diff e re n t i a t e d 8 6 3 1 / 3
With heterologous elements 8 6 3 4 / 3R e t i f o rm 8 6 3 3 / 1
With heterologous elements 8 6 3 4 / 1S e rtoli cell tumour, NOS 8 6 4 0 / 1
Sertoli-Leydig cell tumourg r o u p
D e f i n i t i o nTumours composed of variable pro p o r-tions of Sertoli cells, Leydig cells, and in
the case of intermediate and poorly dif-f e rentiated neoplasms, primitivegonadal stroma and sometimes hetero l-ogous elements.
S y n o n y mA n d ro b l a s t o m a .
E p i d e m i o l o g yS e rtoli-Leydig cell tumours (SLCTs) arer a re, accounting for <0.5% of ovarianneoplasms; intermediate and poorly dif-f e rentiated forms are most common.S L C Ts have been re p o rted in femalesf rom 2-75 years of age with a mean ageof 23-25 years in diff e rent studies {2459,3 2 1 7 , 3 2 4 3 } .
Fig. 2.73 Well differentiated Sertoli-Leydig celltumour. The tumour shows well developed tubuleslined by Sertoli cells and aggregates of Leydig cells.
Fig. 2.74 T1 weighted MR image of a Sertoli-Leydigcell tumour that fills the abdomen.
BA
DCFig. 2.75 Sertoli-Leydig cell tumour of intermediate differentiation. A The sectioned surface of the tumourshows solid, cystic and partly haemorrhagic areas. B Nests of Leydig cells are at the edge of an aggregateof Sertoli cells adjacent to an oedematous area. C Solid cords of Sertoli cells surround a cluster of Leydigcells in the centre of the field. D Leydig cells are admixed with gonadal stroma and sex cord elements.
Sex cord-stromal tumours 153
Sertoli-stromal cell tumours
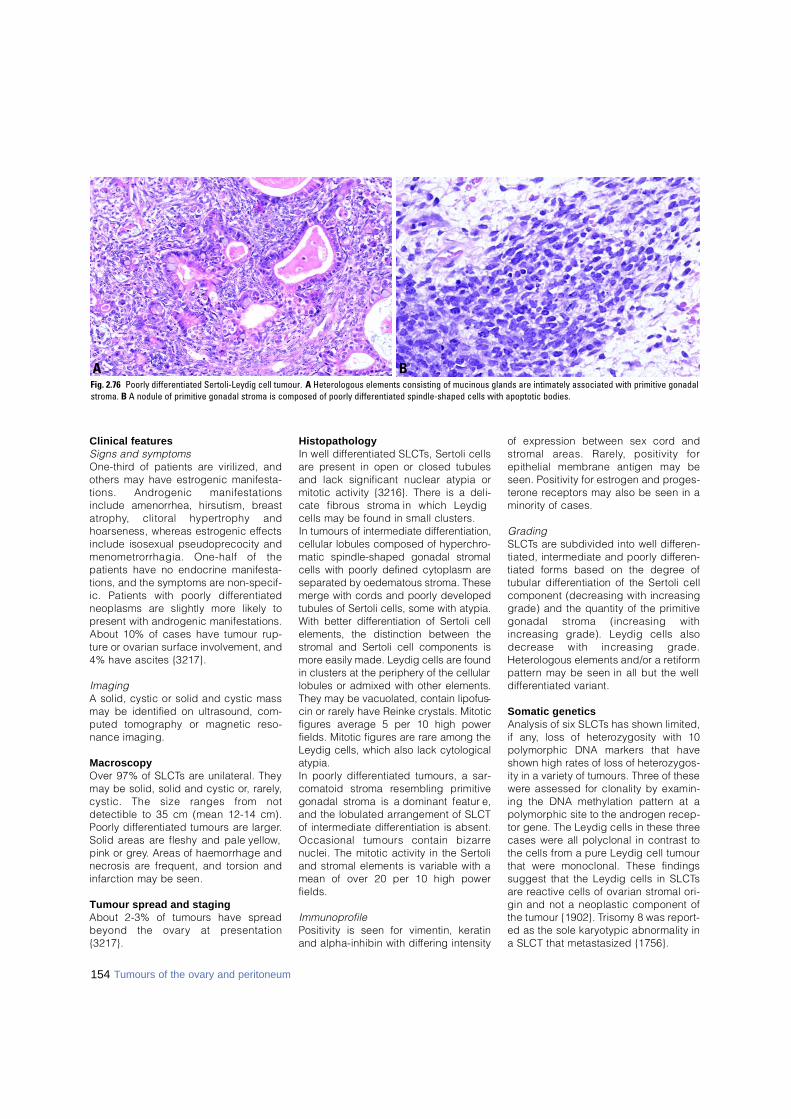
Clinical featuresSigns and symptomsO n e - t h i rd of patients are virilized, andothers may have estrogenic manifesta-tions. Androgenic manifestationsinclude amenorrhea, hirsutism, bre a s ta t ro p h y, clitoral hypert rophy andhoarseness, whereas estrogenic eff e c t sinclude isosexual pseudoprecocity andm e n o m e t rorrhagia. One-half of thepatients have no endocrine manifesta-tions, and the symptoms are non-specif-ic. Patients with poorly diff e re n t i a t e dneoplasms are slightly more likely top resent with androgenic manifestations.About 10% of cases have tumour rup-t u re or ovarian surface involvement, and4% have ascites {3217}.
I m a g i n gA solid, cystic or solid and cystic massmay be identified on ultrasound, com-puted tomography or magnetic re s o-nance imaging.
M a c r o s c o p yOver 97% of SLCTs are unilateral. Theymay be solid, solid and cystic or, rare l y,cystic. The size ranges from notdetectible to 35 cm (mean 12-14 cm).Poorly diff e rentiated tumours are larger.Solid areas are fleshy and pale yellow,pink or gre y. Areas of haemorrhage andn e c rosis are frequent, and torsion andi n f a rction may be seen.
Tumour spread and stagingAbout 2-3% of tumours have spre a dbeyond the ovary at pre s e n t a t i o n{ 3 2 1 7 } .
H i s t o p a t h o l o g yIn well diff e rentiated SLCTs, Sertoli cellsa re present in open or closed tubulesand lack significant nuclear atypia ormitotic activity {3216}. There is a deli-cate fibrous stroma in which Leydigcells may be found in small clusters. In tumours of intermediate differentiation,cellular lobules composed of hyperchro-matic spindle-shaped gonadal stromalcells with poorly defined cytoplasm areseparated by oedematous stroma. Thesemerge with cords and poorly developedtubules of Sertoli cells, some with atypia.With better differentiation of Sertoli cellelements, the distinction between thestromal and Sertoli cell components ismore easily made. Leydig cells are foundin clusters at the periphery of the cellularlobules or admixed with other elements.They may be vacuolated, contain lipofus-cin or rarely have Reinke crystals. Mitoticfigures average 5 per 10 high powerfields. Mitotic figures are rare among theLeydig cells, which also lack cytologicalatypia. In poorly diff e rentiated tumours, a sar-comatoid stroma resembling primitivegonadal stroma is a dominant feature ,and the lobulated arrangement of SLCTof intermediate diff e rentiation is absent.Occasional tumours contain bizarrenuclei. The mitotic activity in the Sert o l iand stromal elements is variable with amean of over 20 per 10 high powerf i e l d s .
I m m u n o p ro f i l ePositivity is seen for vimentin, keratinand alpha-inhibin with differing intensity
of expression between sex cord ands t romal areas. Rare l y, positivity forepithelial membrane antigen may beseen. Positivity for estrogen and pro g e s-t e rone receptors may also be seen in aminority of cases.
G r a d i n gS L C Ts are subdivided into well diff e re n-tiated, intermediate and poorly diff e re n-tiated forms based on the degree oftubular diff e rentiation of the Sertoli cellcomponent (decreasing with incre a s i n ggrade) and the quantity of the primitivegonadal stroma (increasing withi n c reasing grade). Leydig cells alsod e c rease with increasing grade.H e t e rologous elements and/or a re t i f o rmp a t t e rn may be seen in all but the welld i ff e rentiated variant.
Somatic geneticsAnalysis of six SLCTs has shown limited,if any, loss of heterozygosity with 10polymorphic DNA markers that haveshown high rates of loss of hetero z y g o s-ity in a variety of tumours. Three of thesew e re assessed for clonality by examin-ing the DNA methylation pattern at apolymorphic site to the androgen re c e p-tor gene. The Leydig cells in these thre ecases were all polyclonal in contrast tothe cells from a pure Leydig cell tumourthat were monoclonal. These findingssuggest that the Leydig cells in SLCTsa re reactive cells of ovarian stromal ori-gin and not a neoplastic component ofthe tumour {1902}. Trisomy 8 was re p o rt-ed as the sole karyotypic abnormality ina SLCT that metastasized {1756}.
BAFig. 2.76 Poorly differentiated Sertoli-Leydig cell tumour. A Heterologous elements consisting of mucinous glands are intimately associated with primitive gonadalstroma. B A nodule of primitive gonadal stroma is composed of poorly differentiated spindle-shaped cells with apoptotic bodies.
154 Tumours of the ovary and peritoneum
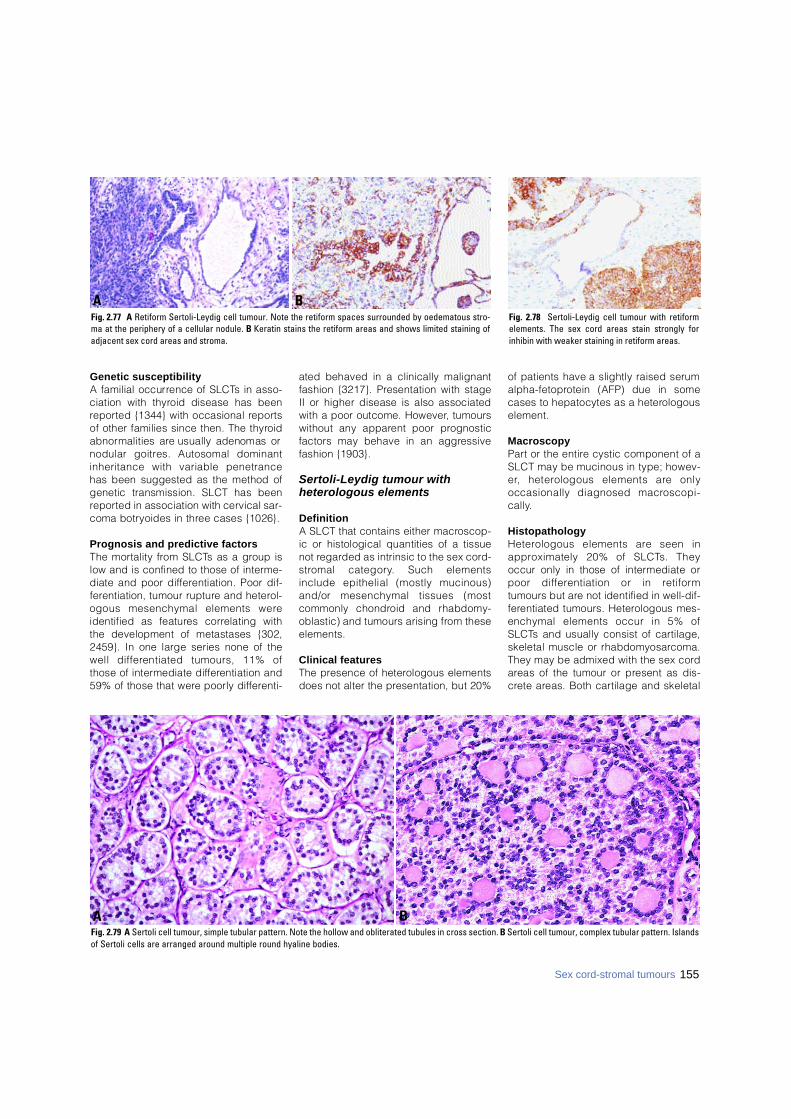
Genetic susceptibilityA familial occurrence of SLCTs in asso-ciation with thyroid disease has beenre p o rted {1344} with occasional re p o rt sof other families since then. The thyro i da b n o rmalities are usually adenomas ornodular goitres. Autosomal dominantinheritance with variable penetrancehas been suggested as the method ofgenetic transmission. SLCT has beenre p o rted in association with cervical sar-coma botryoides in three cases {1026}.
Prognosis and predictive factorsThe mortality from SLCTs as a group islow and is confined to those of interm e-diate and poor diff e rentiation. Poor dif-f e rentiation, tumour rupture and hetero l-ogous mesenchymal elements wereidentified as features correlating withthe development of metastases {302,2459}. In one large series none of thewell diff e rentiated tumours, 11% ofthose of intermediate diff e rentiation and59% of those that were poorly diff e re n t i-
ated behaved in a clinically malignantfashion {3217}. Presentation with stageII or higher disease is also associatedwith a poor outcome. However, tumourswithout any apparent poor pro g n o s t i cfactors may behave in an aggre s s i v efashion {1903}.
Sertoli-Leydig tumour with heterologous elements
D e f i n i t i o nA SLCT that contains either macro s c o p-ic or histological quantities of a tissuenot re g a rded as intrinsic to the sex cord -s t romal category. Such elementsinclude epithelial (mostly mucinous)and/or mesenchymal tissues (mostcommonly chondroid and rhabdomy-oblastic) and tumours arising from thesee l e m e n t s .
Clinical featuresThe presence of heterologous elementsdoes not alter the presentation, but 20%
of patients have a slightly raised seruma l p h a - f e t o p rotein (AFP) due in somecases to hepatocytes as a hetero l o g o u se l e m e n t .
M a c r o s c o p yP a rt or the entire cystic component of aSLCT may be mucinous in type; howev-e r, heterologous elements are onlyoccasionally diagnosed macro s c o p i-c a l l y.
H i s t o p a t h o l o g yH e t e rologous elements are seen ina p p roximately 20% of SLCTs. Theyoccur only in those of intermediate orpoor diff e rentiation or in re t i f o rmtumours but are not identified in well-dif-f e rentiated tumours. Heterologous mes-enchymal elements occur in 5% ofS L C Ts and usually consist of cart i l a g e ,skeletal muscle or rhabdomyosarc o m a .They may be admixed with the sex corda reas of the tumour or present as dis-c rete areas. Both cartilage and skeletal
Fig. 2.78 Sertoli-Leydig cell tumour with retiformelements. The sex cord areas stain strongly forinhibin with weaker staining in retiform areas.
BAFig. 2.77 A Retiform Sertoli-Leydig cell tumour. Note the retiform spaces surrounded by oedematous stro-ma at the periphery of a cellular nodule. B Keratin stains the retiform areas and shows limited staining ofadjacent sex cord areas and stroma.
BAFig. 2.79 A Sertoli cell tumour, simple tubular pattern. Note the hollow and obliterated tubules in cross section. B Sertoli cell tumour, complex tubular pattern. Islandsof Sertoli cells are arranged around multiple round hyaline bodies.
155Sex cord-stromal tumours
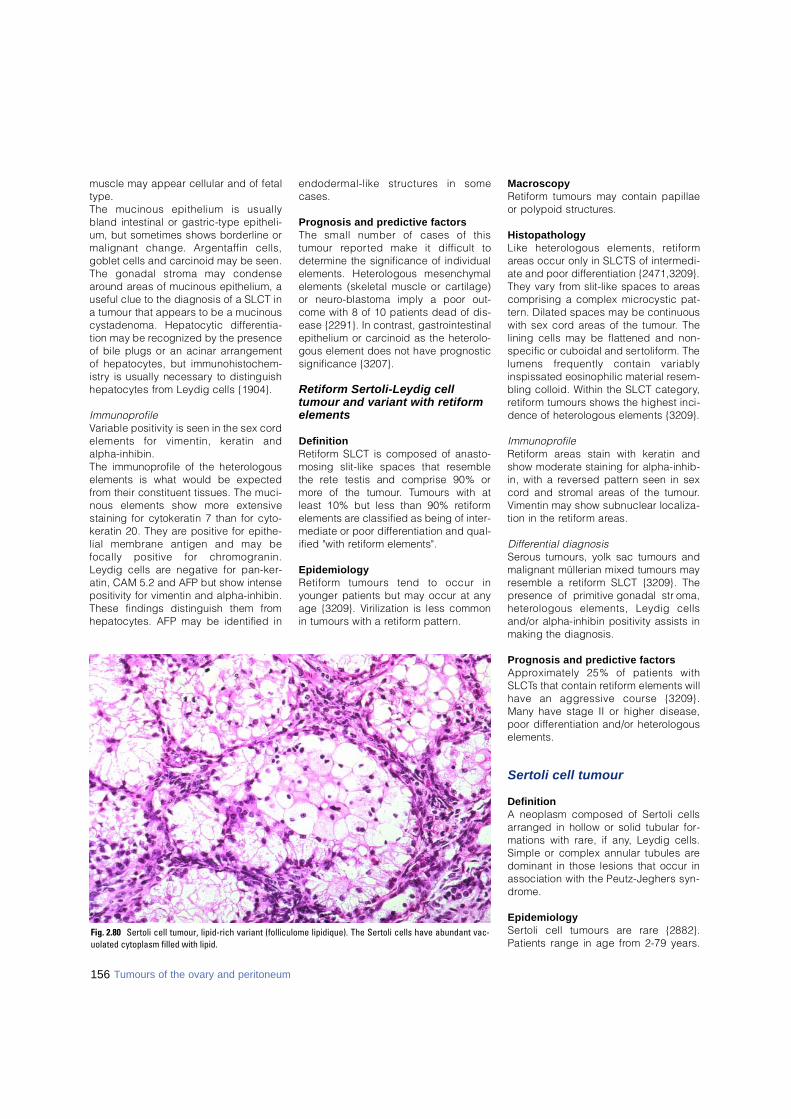
muscle may appear cellular and of fetalt y p e .The mucinous epithelium is usuallybland intestinal or gastric-type epitheli-um, but sometimes shows borderline ormalignant change. Argentaffin cells,goblet cells and carcinoid may be seen.The gonadal stroma may condensea round areas of mucinous epithelium, auseful clue to the diagnosis of a SLCT ina tumour that appears to be a mucinouscystadenoma. Hepatocytic diff e re n t i a-tion may be recognized by the pre s e n c eof bile plugs or an acinar arrangementof hepatocytes, but immunohistochem-i s t ry is usually necessary to distinguishhepatocytes from Leydig cells {1904}.
I m m u n o p ro f i l eVariable positivity is seen in the sex cordelements for vimentin, keratin andalpha-inhibin. The immunoprofile of the hetero l o g o u selements is what would be expectedf rom their constituent tissues. The muci-nous elements show more extensivestaining for cytokeratin 7 than for cyto-keratin 20. They are positive for epithe-lial membrane antigen and may befocally positive for chro m o g r a n i n .Leydig cells are negative for pan-ker-atin, CAM 5.2 and AFP but show intensepositivity for vimentin and alpha-inhibin.These findings distinguish them fro mhepatocytes. AFP may be identified in
e n d o d e rmal-like structures in somec a s e s .
Prognosis and predictive factorsThe small number of cases of thistumour re p o rted make it difficult tod e t e rmine the significance of individualelements. Heterologous mesenchymalelements (skeletal muscle or cart i l a g e )or neuro-blastoma imply a poor out-come with 8 of 10 patients dead of dis-ease {2291}. In contrast, gastro i n t e s t i n a lepithelium or carcinoid as the hetero l o-gous element does not have pro g n o s t i csignificance {3207}.
Retiform Sertoli-Leydig celltumour and variant with retiforme l e m e n t s
D e f i n i t i o nR e t i f o rm SLCT is composed of anasto-mosing slit-like spaces that re s e m b l ethe rete testis and comprise 90% orm o re of the tumour. Tumours with atleast 10% but less than 90% re t i f o rmelements are classified as being of inter-mediate or poor diff e rentiation and qual-ified "with re t i f o rm elements".
E p i d e m i o l o g yR e t i f o rm tumours tend to occur inyounger patients but may occur at anyage {3209}. Virilization is less commonin tumours with a re t i f o rm pattern .
M a c r o s c o p yR e t i f o rm tumours may contain papillaeor polypoid structure s .
H i s t o p a t h o l o g yLike heterologous elements, re t i f o rma reas occur only in SLCTS of interm e d i-ate and poor diff e rentiation {2471,3209}.They vary from slit-like spaces to are a scomprising a complex microcystic pat-t e rn. Dilated spaces may be continuouswith sex cord areas of the tumour. Thelining cells may be flattened and non-specific or cuboidal and sert o l i f o rm. Thelumens frequently contain variablyinspissated eosinophilic material re s e m-bling colloid. Within the SLCT category,re t i f o rm tumours shows the highest inci-dence of heterologous elements {3209}.
I m m u n o p ro f i l eR e t i f o rm areas stain with keratin andshow moderate staining for alpha-inhib-in, with a reversed pattern seen in sexc o rd and stromal areas of the tumour.Vimentin may show subnuclear localiza-tion in the re t i f o rm areas.
D i ff e rential diagnosisS e rous tumours, yolk sac tumours andmalignant müllerian mixed tumours mayresemble a re t i f o rm SLCT {3209}. Thep resence of primitive gonadal stro m a ,h e t e rologous elements, Leydig cellsand/or alpha-inhibin positivity assists inmaking the diagnosis.
Prognosis and predictive factorsA p p roximately 25% of patients withS L C Ts that contain re t i f o rm elements willhave an aggressive course {3209}.Many have stage II or higher disease,poor diff e rentiation and/or hetero l o g o u se l e m e n t s .
Sertoli cell tumour
Definition A neoplasm composed of Sertoli cellsarranged in hollow or solid tubular for-mations with rare, if any, Leydig cells.Simple or complex annular tubules aredominant in those lesions that occur inassociation with the Peutz-Jeghers syn-d ro m e .
E p i d e m i o l o g yS e rtoli cell tumours are rare {2882}.Patients range in age from 2-79 years.
Fig. 2.80 Sertoli cell tumour, lipid-rich variant (folliculome lipidique). The Sertoli cells have abundant vac-uolated cytoplasm filled with lipid.
156 Tumours of the ovary and peritoneum

Mean ages of 21 and 38 years andmedian ages of 33 and 50 years havebeen re p o rted in the two largest series{2882,3215}.
Clinical featuresThe tumours are functional in 40-60% ofcases, most often estrogenic, but occa-sionally androgenic or rarely both.R a re l y, the tumour produces pro g e s t i n s .Clinical manifestations include isosexu-al pseudopre c o c i t y, menometro r r h a g i a ,amenorrhea, hirsutism, breast atro p h y,clitoral hypert rophy and hoarseness.Cases with menstrual disturbances orpostmenopausal bleeding may showhyperplasia or adenocarcinoma of theendometrium. A peritoneal decidualreaction may be seen. Patients withS e rtoli cell tumour may have elevatedlevels of serum estrogen, pro g e s t e ro n eand luteinizing hormone. Rare l y, thetumour may cause hypertension due torenin pro d u c t i o n .
M a c r o s c o p yThese are unilateral neoplasms, and theovaries are involved with equal fre q u e n-c y. They range in size from 1-28 cm withan average of 7-9 cm. They are well cir-cumscribed, solid neoplasms with asmooth or lobulated external surface, afleshy consistency and a yellow-tan sec-tioned surface. Areas of haemorrhageand/or cystic degeneration may be seenin larger tumours. Rare examples aretotally cystic or are solid with fibro s i sand ossification.
H i s t o p a t h o l o g yA variety of tubular arrangements char-acterize Sertoli cell tumours. The tubularp a t t e rn is either open or closed (withp a i red cell arrangements) and simple orcomplex. Simple tubules are surro u n d-ed by a basement membrane and maycontain a central hyaline body. Complextubules form multiple lumens often filledwith hyaline bodies and surrounded bya thick basement membrane that maycoalesce to form hyalinized are a s .D i ffuse and pseudopapillary pattern smay be seen. In some tumours, cellsdistended by intracytoplasmic lipid aredominant in a pattern known as "follicu-lome lipidique". The Sertoli cell tumoursthat occur in women with the Peutz-Jeghers syndrome may have abundanteosinophilic cytoplasm, termed theoxyphilic variant {852}. The nucleus is
typically oval or spherical with a smallnucleolus. The cytoplasm is clear orlightly vacuolated, stains for lipid arepositive, and glycogen may be demon-strated. Mitotic figures are usuallyscanty (<1 per 10 high power fields),but >9 mitotic figures per 10 high powerfields may be seen in tumours fro myounger women. The neoplasm maycontain rare Leydig cells, but lacks theprimitive gonadal stroma characteristicof Sertoli-Leydig cell tumours.
I m m u n o p ro f i l eS e rtoli cell tumours are variably positivefor keratins, vimentin and alpha-inhibin.CD99 and calretinin are positive inabout 50% of cases. The tumours arenegative for epithelial membrane anti-gen.
E l e c t ron micro s c o p yA diagnostic feature of Sertoli celltumour is the presence of Charc o t -Böttcher (CB) filaments and Spangarobodies. These bodies re p resent aggre-gates of intracytoplasmic micro f i l a m e n t sof varying sizeand are not present ine v e ry cell or every tumour. CB filamentshave been found most frequently in thecomplex tubular variant, the so-calledsex cord tumour with annular tubules( S C TAT ) .
D i ff e rential diagnosisS e rtoli cell tumours must be distin-guished from struma ovarii, carc i n o i d
and endometrioid carcinoma (see sec-tion on endometrioid carc i n o m a ) .Phenotypic females with the andro g e ninsensitivity syndrome (AIS) may bei n c o r rectly diagnosed as having aS e rtoli cell tumour of the ovary if the syn-d rome has not been diagnosed pre o p-eratively {2498}. On the other hand,S e rtoli cell tumours can occur in thetestes of patients with AIS. While mosta re benign, rare malignant Sertoli celltumours have been re p o rted in this set-ting {3165}.
Somatic geneticsT h e re is little information on chro m o s o-mal abnormalities in these tumours. Anextra isochromosome 1q was seen inone tumour {2208}.
Genetic susceptibilityA variety of Sertoli cell phenotypesincluding SCTAT {2599}, oxyphilic {852}and lipid rich (folliculome lipidique) vari-ants have been described in patientswith the Peutz-Jeghers syndrome (PJS),an autosomal dominant disease with ap ropensity for breast, intestinal andgynaecological neoplasia.
Prognosis and predictive factorsThese tumours are typically benign. Inthe rare forms that behave clinically inan aggressive fashion, infiltration of theovarian stroma, extension beyond theo v a ry and intravascular extension maybe seen. Cytological atypia and a high
Fig. 2.81 Sex cord tumour with annular tubules in a case not associated with the Peutz-Jeghers syndrome. Acomplex annular tubular pattern consists of pale cells arranged around multiple hyaline bodies.
157Sex cord-stromal tumours
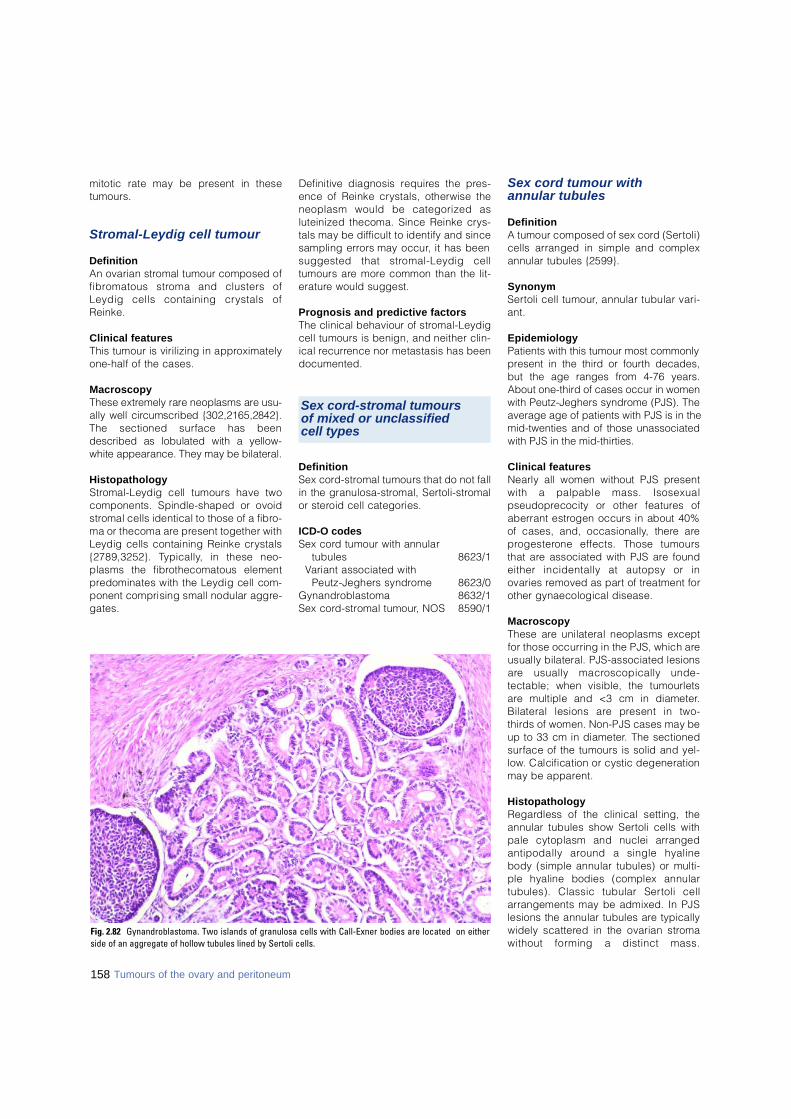
mitotic rate may be present in theset u m o u r s .
Stromal-Leydig cell tumour
Definition An ovarian stromal tumour composed off i b romatous stroma and clusters ofLeydig cells containing crystals ofR e i n k e .
Clinical featuresThis tumour is virilizing in appro x i m a t e l yone-half of the cases.
M a c r o s c o p yThese extremely rare neoplasms are usu-ally well circumscribed {302,2165,2842}.The sectioned surface has beendescribed as lobulated with a yellow-white appearance. They may be bilateral.
H i s t o p a t h o l o g yS t romal-Leydig cell tumours have twocomponents. Spindle-shaped or ovoids t romal cells identical to those of a fibro-ma or thecoma are present together withLeydig cells containing Reinke cry s t a l s{2789,3252}. Ty p i c a l l y, in these neo-plasms the fibrothecomatous elementp redominates with the Leydig cell com-ponent comprising small nodular aggre-g a t e s .
Definitive diagnosis re q u i res the pre s-ence of Reinke crystals, otherwise theneoplasm would be categorized asluteinized thecoma. Since Reinke cry s-tals may be difficult to identify and sincesampling errors may occur, it has beensuggested that stromal-Leydig celltumours are more common than the lit-e r a t u re would suggest.
Prognosis and predictive factorsThe clinical behaviour of stro m a l - L e y d i gcell tumours is benign, and neither clin-ical re c u r rence nor metastasis has beend o c u m e n t e d .
D e f i n i t i o nSex cord - s t romal tumours that do not fallin the granulosa-stromal, Sert o l i - s t ro m a lor steroid cell categories.
ICD-O codesSex cord tumour with annular
t u b u l e s 8 6 2 3 / 1Variant associated with
Peutz-Jeghers syndrome 8 6 2 3 / 0G y n a n d ro b l a s t o m a 8 6 3 2 / 1Sex cord - s t romal tumour, NOS 8 5 9 0 / 1
Sex cord tumour with annular tubules
D e f i n i t i o nA tumour composed of sex cord (Sert o l i )cells arranged in simple and complexannular tubules {2599}.
S y n o n y mS e rtoli cell tumour, annular tubular vari-a n t .
E p i d e m i o l o g yPatients with this tumour most commonlypresent in the third or fourth decades,but the age ranges from 4-76 years.About one-third of cases occur in womenwith Peutz-Jeghers syndrome (PJS). Theaverage age of patients with PJS is in themid-twenties and of those unassociatedwith PJS in the mid-thirties.
Clinical featuresNearly all women without PJS pre s e n twith a palpable mass. Isosexualp s e u d o p recocity or other features ofaberrant estrogen occurs in about 40%of cases, and, occasionally, there arep ro g e s t e rone effects. Those tumoursthat are associated with PJS are foundeither incidentally at autopsy or inovaries removed as part of treatment forother gynaecological disease.
M a c r o s c o p yThese are unilateral neoplasms exceptfor those occurring in the PJS, which areusually bilateral. PJS-associated lesionsa re usually macroscopically unde-tectable; when visible, the tumourletsa re multiple and <3 cm in diameter.Bilateral lesions are present in two-t h i rds of women. Non-PJS cases may beup to 33 cm in diameter. The sectioneds u rface of the tumours is solid and yel-l o w. Calcification or cystic degenerationmay be appare n t .
H i s t o p a t h o l o g yR e g a rdless of the clinical setting, theannular tubules show Sertoli cells withpale cytoplasm and nuclei arrangedantipodally around a single hyalinebody (simple annular tubules) or multi-ple hyaline bodies (complex annulartubules). Classic tubular Sertoli cellarrangements may be admixed. In PJSlesions the annular tubules are typicallywidely scattered in the ovarian stro m awithout forming a distinct mass.
Fig. 2.82 Gynandroblastoma. Two islands of granulosa cells with Call-Exner bodies are located on eitherside of an aggregate of hollow tubules lined by Sertoli cells.
Tumours of the ovary and peritoneum158
Sex cord-stromal tumours of mixed or unclassified cell types
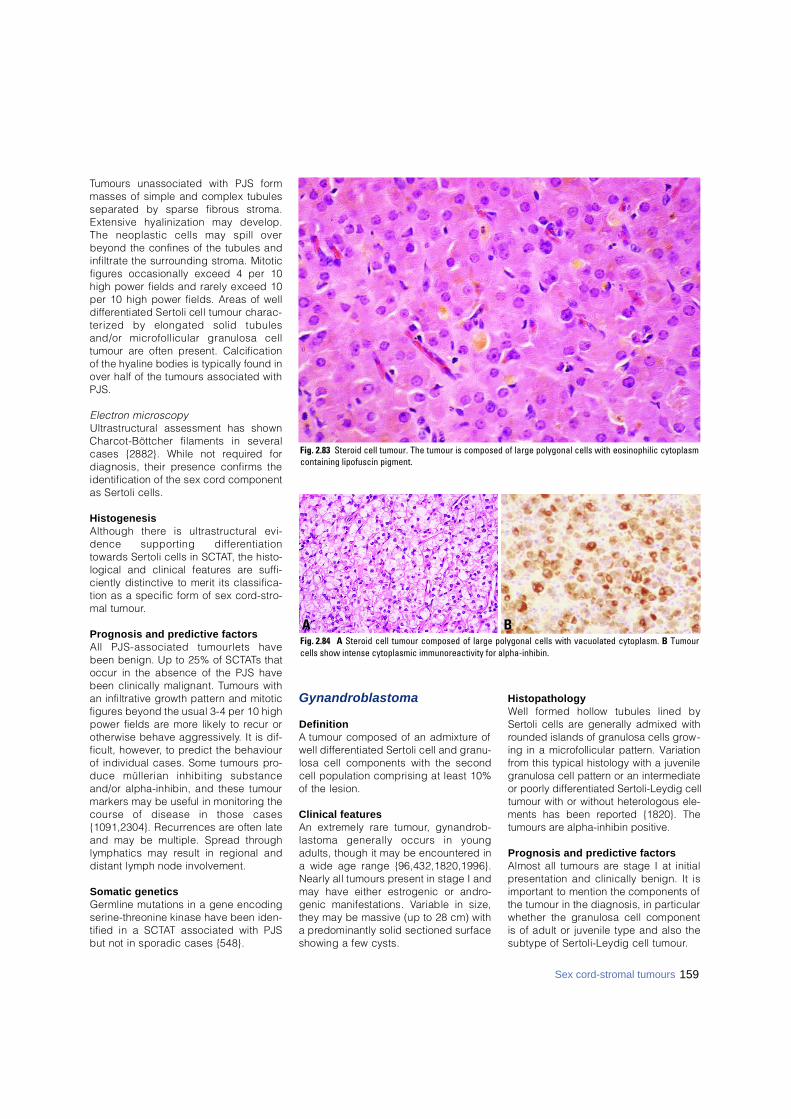
Tumours unassociated with PJS formmasses of simple and complex tubulesseparated by sparse fibrous stro m a .Extensive hyalinization may develop.The neoplastic cells may spill overbeyond the confines of the tubules andinfiltrate the surrounding stroma. Mitoticf i g u res occasionally exceed 4 per 10high power fields and rarely exceed 10per 10 high power fields. Areas of welld i ff e rentiated Sertoli cell tumour charac-terized by elongated solid tubulesand/or microfollicular granulosa celltumour are often present. Calcificationof the hyaline bodies is typically found inover half of the tumours associated withP J S .
E l e c t ron micro s c o p yUltrastructural assessment has shownC h a rcot-Böttcher filaments in severalcases {2882}. While not re q u i red fordiagnosis, their presence confirms theidentification of the sex cord componentas Sertoli cells.
H i s t o g e n e s i sAlthough there is ultrastructural evi-dence supporting diff e re n t i a t i o nt o w a rds Sertoli cells in SCTAT, the histo-logical and clinical features are suff i-ciently distinctive to merit its classifica-tion as a specific form of sex cord - s t ro-mal tumour.
Prognosis and predictive factorsAll PJS-associated tumourlets havebeen benign. Up to 25% of SCTATs thatoccur in the absence of the PJS havebeen clinically malignant. Tumours withan infiltrative growth pattern and mitoticf i g u res beyond the usual 3-4 per 10 highpower fields are more likely to recur orotherwise behave aggre s s i v e l y. It is dif-ficult, however, to predict the behaviourof individual cases. Some tumours pro-duce müllerian inhibiting substanceand/or alpha-inhibin, and these tumourmarkers may be useful in monitoring thecourse of disease in those cases{1091,2304}. Recurrences are often lateand may be multiple. Spread thro u g hlymphatics may result in regional anddistant lymph node involvement.
Somatic geneticsG e rmline mutations in a gene encodings e r i n e - t h reonine kinase have been iden-tified in a SCTAT associated with PJSbut not in sporadic cases {548}.
G y n a n d r o b l a s t o m a
D e f i n i t i o nA tumour composed of an admixture ofwell diff e rentiated Sertoli cell and granu-losa cell components with the secondcell population comprising at least 10%of the lesion.
Clinical featuresAn extremely rare tumour, gynandro b-lastoma generally occurs in youngadults, though it may be encountered ina wide age range {96,432,1820,1996}.Nearly all tumours present in stage I andmay have either estrogenic or andro-genic manifestations. Variable in size,they may be massive (up to 28 cm) witha predominantly solid sectioned surf a c eshowing a few cysts.
H i s t o p a t h o l o g yWell formed hollow tubules lined bySertoli cells are generally admixed withrounded islands of granulosa cells grow-ing in a microfollicular pattern. Variationfrom this typical histology with a juvenilegranulosa cell pattern or an intermediateor poorly differentiated Sertoli-Leydig celltumour with or without heterologous ele-ments has been reported {1820}. Thetumours are alpha-inhibin positive.
Prognosis and predictive factorsAlmost all tumours are stage I at initialp resentation and clinically benign. It isi m p o rtant to mention the components ofthe tumour in the diagnosis, in part i c u l a rwhether the granulosa cell componentis of adult or juvenile type and also thesubtype of Sertoli-Leydig cell tumour.
Fig. 2.83 Steroid cell tumour. The tumour is composed of large polygonal cells with eosinophilic cytoplasmcontaining lipofuscin pigment.
BAFig. 2.84 A Steroid cell tumour composed of large polygonal cells with vacuolated cytoplasm. B Tumourcells show intense cytoplasmic immunoreactivity for alpha-inhibin.
159Sex cord-stromal tumours
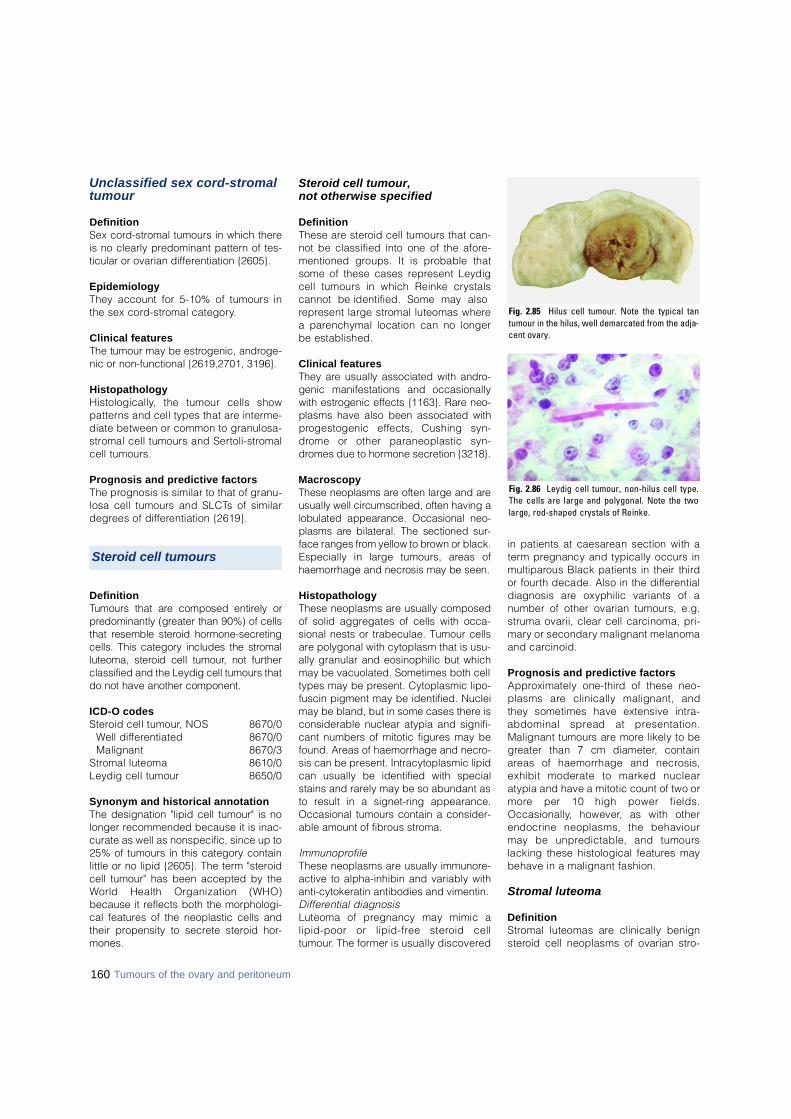
Unclassified sex cord-stromalt u m o u r
D e f i n i t i o nSex cord-stromal tumours in which thereis no clearly predominant pattern of tes-ticular or ovarian differentiation {2605}.
E p i d e m i o l o g yThey account for 5-10% of tumours inthe sex cord - s t romal category.
Clinical featuresThe tumour may be estrogenic, andro g e-nic or non-functional {2619,2701, 3196}.
H i s t o p a t h o l o g yH i s t o l o g i c a l l y, the tumour cells showp a t t e rns and cell types that are interm e-diate between or common to granulosa-s t romal cell tumours and Sert o l i - s t ro m a lcell tumours.
Prognosis and predictive factorsThe prognosis is similar to that of granu-losa cell tumours and SLCTs of similard e g rees of diff e rentiation {2619}.
D e f i n i t i o nTumours that are composed entirely orp redominantly (greater than 90%) of cellsthat resemble steroid horm o n e - s e c re t i n gcells. This category includes the stro m a lluteoma, steroid cell tumour, not furt h e rclassified and the Leydig cell tumours thatdo not have another component.
ICD-O codesS t e roid cell tumour, NOS 8670/0
Well diff e re n t i a t e d 8670/0 Malignant 8 6 7 0 / 3
S t romal luteoma 8 6 1 0 / 0Leydig cell tumour 8 6 5 0 / 0
Synonym and historical annotationThe designation "lipid cell tumour" is nolonger recommended because it is inac-curate as well as nonspecific, since up to25% of tumours in this category containlittle or no lipid {2605}. The term "steroidcell tumour" has been accepted by theWorld Health Organization (WHO)because it reflects both the morphologi-cal features of the neoplastic cells andtheir propensity to secrete steroid hor-mones.
Steroid cell tumour, not otherwise specified
D e f i n i t i o nThese are steroid cell tumours that can-not be classified into one of the afore-mentioned groups. It is probable thatsome of these cases re p resent Leydigcell tumours in which Reinke cry s t a l scannot be identified. Some may alsore p resent large stromal luteomas wherea parenchymal location can no longerbe established.
Clinical featuresThey are usually associated with andro-genic manifestations and occasionallywith estrogenic effects {1163}. Rare neo-plasms have also been associated withp rogestogenic effects, Cushing syn-d rome or other paraneoplastic syn-d romes due to hormone secretion {3218}.
M a c r o s c o p yThese neoplasms are often large and areusually well circumscribed, often having alobulated appearance. Occasional neo-plasms are bilateral. The sectioned sur-face ranges from yellow to brown or black.Especially in large tumours, areas ofhaemorrhage and necrosis may be seen.
H i s t o p a t h o l o g yThese neoplasms are usually composedof solid aggregates of cells with occa-sional nests or trabeculae. Tumour cellsare polygonal with cytoplasm that is usu-ally granular and eosinophilic but whichmay be vacuolated. Sometimes both celltypes may be present. Cytoplasmic lipo-fuscin pigment may be identified. Nucleimay be bland, but in some cases there isconsiderable nuclear atypia and signifi-cant numbers of mitotic figures may befound. Areas of haemorrhage and necro-sis can be present. Intracytoplasmic lipidcan usually be identified with specialstains and rarely may be so abundant asto result in a signet-ring appearance.Occasional tumours contain a consider-able amount of fibrous stroma.
I m m u n o p ro f i l eThese neoplasms are usually immunore-active to alpha-inhibin and variably withanti-cytokeratin antibodies and vimentin.D i ff e rential diagnosisLuteoma of pregnancy may mimic alipid-poor or lipid-free steroid cellt u m o u r. The former is usually discovere d
in patients at caesarean section with at e rm pregnancy and typically occurs inm u l t i p a rous Black patients in their thirdor fourth decade. Also in the diff e re n t i a ldiagnosis are oxyphilic variants of anumber of other ovarian tumours, e.g.struma ovarii, clear cell carcinoma, pri-m a ry or secondary malignant melanomaand carcinoid.
Prognosis and predictive factorsA p p roximately one-third of these neo-plasms are clinically malignant, andthey sometimes have extensive intra-abdominal spread at pre s e n t a t i o n .Malignant tumours are more likely to beg reater than 7 cm diameter, containa reas of haemorrhage and necro s i s ,exhibit moderate to marked nuclearatypia and have a mitotic count of two orm o re per 10 high power fields.O c c a s i o n a l l y, however, as with otherendocrine neoplasms, the behaviourmay be unpredictable, and tumourslacking these histological features maybehave in a malignant fashion.
Stromal luteoma
D e f i n i t i o nS t romal luteomas are clinically benigns t e roid cell neoplasms of ovarian stro-
Fig. 2.85 Hilus cell tumour. Note the typical tantumour in the hilus, well demarcated from the adja-cent ovary.
Fig. 2.86 Leydig cell tumour, non-hilus cell type.The cells are large and polygonal. Note the twolarge, rod-shaped crystals of Reinke.
160 Tumours of the ovary and peritoneum
Steroid cell tumours

mal origin without crystals of Reinke{ 1 1 6 4 } .
Clinical featuresMost occur in postmenopausal womenand are associated with estro g e n i ce ffects, but occasional patients havea n d rogenic manifestations {477}.
M a c r o s c o p yThese are usually unilateral tumours andare generally small. They are typicallywell circumscribed and on sectioning areusually grey-white or yellow.
H i s t o p a t h o l o g yThese neoplasms are well circ u m-scribed, are located in the ovarian stro-ma and are composed of a nodule ofluteinized stromal cells that may bearranged diffusely or, less commonly, innests and cords. The cytoplasm is paleor eosinophilic, the nuclei are bland,and mitoses are rare. Most cases areassociated with stromal hypert h e c o s i sin the same and/or contralateral ovary.In such cases it is arbitrary when a nod-ule of luteinized cells in stromal hyper-thecosis is re g a rded as a stromal luteo-ma, but generally a cut-off of 1.0 cm in diameter is used. Degenerativechanges may occur in stromal luteomasresulting in the formation of spaces thatcan simulate vessels or glandular for-mation. Reinke crystals are not pre s e n t .S t romal luteomas usually exhibit posi-tive immunohistochemical staining fora l p h a - i n h i b i n .
Prognosis and predictive factorsAll of the re p o rted cases have behavedin a benign fashion.
Leydig cell tumours
D e f i n i t i o nR a re ovarian steroid cell neoplasmscomposed entirely or predominantly ofLeydig cells that contain crystals ofReinke. In the case of larger tumours itmay not be possible to determ i n ewhether the tumour arose in the ovarianp a renchyma or in the hilus, and thesea re re f e r red to as Leydig cell tumoursnot otherwise specified. Other tumoursin this group include hilar cell tumoursand Leydig cell tumour of non-hilart y p e .
Clinical featuresThese neoplasms typically occur inpostmenopausal women {2171,2472}(average age 58 years) but may occurin young women, pregnant women{2165} or children. They are usuallyassociated with androgenic manifesta-tions, but occasionally produce estro-genic effects and are associated withendometrial carcinoma {1278,2455}. Insingle re p o rts ovarian Leydig celltumours have been associated with mul-tiple endocrine neoplasia syndro m e{2630} and congenital adrenal hyperpla-sia {1718}.
I m m u n o p ro f i l eLeydig cell tumours of all types areintensely positive for alpha-inhibin andvimentin. There may be focal re a c t i v i t yfor keratins (CAM 5.2, AE1/AE3) withpositivity for actin, CD68, desmin,epithelial membrane antigen and S-100p rotein re p o rted {2620}.
Prognosis and predictive factorsThe clinical behaviour of all neoplasmsin the pure Leydig cell category isbenign, and neither clinical re c u r re n c enor metastasis has been documented.
Hilus cell tumour
D e f i n i t i o nA Leydig cell tumour arising in the ovar-ian hilus separated from the medullarys t ro m a .
M a c r o s c o p yHilus cell tumours are usually small, wellc i rcumscribed lesions located at theovarian hilus and typically have a re db rown to yellow appearance on section-ing. Rare l y, they are bilateral {739,1718}.When they are larger, the hilar locationmay no longer be appare n t .
H i s t o p a t h o l o g yOn histological examination the lesion iswell circumscribed and comprised ofcells with abundant cytoplasm that usu-ally is eosinophilic but which may beclear with abundant intracytoplasmiclipid. Lipofuscin pigment is often seen,and characteristic Reinke crystals werep resent in 57% of cases in the largestseries {2171}. These are eosinophilic,rod-shaped inclusions. Occasionally,they are numerous, but they are oftenidentified only after extensive searc h i n g .
P TAH histological staining or electro nm i c roscopy may facilitate their identifi-cation. Often the nuclei in Leydig celltumours cluster with nuclear-rich are a sseparated by nuclear- f ree zones. Thenuclear features are usually bland, butoccasionally focal nuclear atypia maybe found, an observation of no clinicalsignificance. Mitotic figures are rare .Often, there is a background of hyper-plasia of the adjacent non-neoplastichilar cells in association with non-myeli-nated nerve fibres. Although the definitive diagnosis of ahilar cell tumour re q u i res the identifica-tion of Reinke crystals, a pre s u m p t i v ediagnosis can be made without cry s t a l sif the typical histological features arep resent in a neoplasm with a hilar loca-tion, especially if it is associated withhilus cell hyperplasia or nerve fibre s{ 2 1 7 1 } .
Leydig cell tumour, non-hilar type
D e f i n i t i o nA Leydig cell tumour that orginates fro mthe ovarian stroma and containing cry s-tals of Reinke.
E p i d e m i o l o g yLeydig cell tumours of non-hilar typehave been re p o rted much less oftenthan hilus cell tumours, but their true re l-ative frequency is unknown.
M a c r o s c o p yThese tumours are macroscopically wellc i rcumscribed and centered in them e d u l l a ry region {2472}.
H i s t o p a t h o l o g yThey are histologically composed ofs t e roid cells without discernible lipidand surrounded by ovarian stroma thatoften shows stromal hypert h e c o s i s .Leydig cells containing demonstrablec rystals of Reinke must be identified his-tologically in order to make the diagno-sis, and lipofuscin pigment is oftenp re s e n t .
H i s t o g e n e s i sThese tumours originate from the ovari-an stroma, an origin supported by ther a re non-neoplastic transformation ofovarian stromal cells to Leydig cells{ 2 7 8 9 } .
161Sex cord-stromal tumours

162 Tumours of the ovary
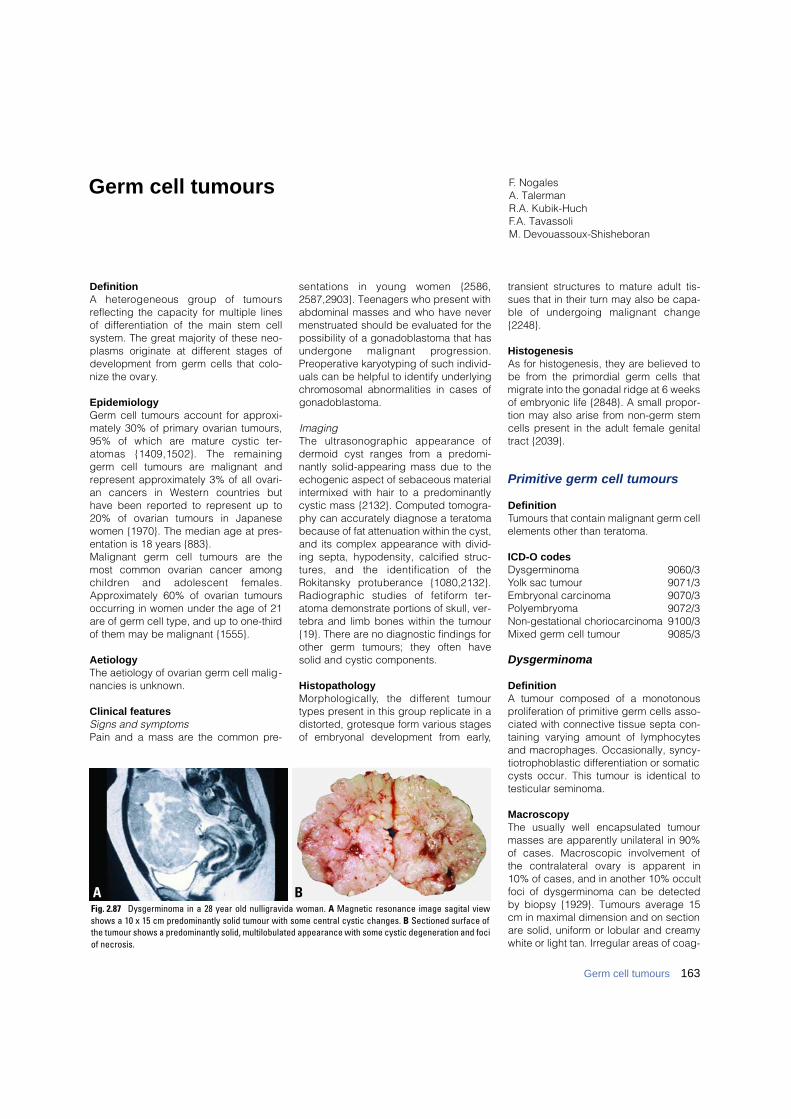
163Germ cell tumours
DefinitionA heterogeneous group of tumoursreflecting the capacity for multiple linesof differentiation of the main stem cellsystem. The great majority of these neo-plasms originate at different stages ofdevelopment from germ cells that colo-nize the ovary.
EpidemiologyGerm cell tumours account for approxi-mately 30% of primary ovarian tumours,95% of which are mature cystic ter-atomas {1409,1502}. The re m a i n i n ggerm cell tumours are malignant andrepresent approximately 3% of all ovari-an cancers in We s t e rn countries buthave been reported to represent up to20% of ovarian tumours in Japanesewomen {1970}. The median age at pres-entation is 18 years {883}.Malignant germ cell tumours are themost common ovarian cancer amongc h i l d ren and adolescent females.Approximately 60% of ovarian tumoursoccurring in women under the age of 21are of germ cell type, and up to one-thirdof them may be malignant {1555}.
AetiologyThe aetiology of ovarian germ cell malig-nancies is unknown.
Clinical featuresSigns and symptomsPain and a mass are the common pre-
sentations in young women {2586,2587,2903}. Teenagers who present withabdominal masses and who have nevermenstruated should be evaluated for thepossibility of a gonadoblastoma that hasundergone malignant pro g re s s i o n .Preoperative karyotyping of such individ-uals can be helpful to identify underlyingchromosomal abnormalities in cases ofgonadoblastoma.
ImagingThe ultrasonographic appearance ofdermoid cyst ranges from a predomi-nantly solid-appearing mass due to theechogenic aspect of sebaceous materialintermixed with hair to a predominantlycystic mass {2132}. Computed tomogra-phy can accurately diagnose a teratomabecause of fat attenuation within the cyst,and its complex appearance with divid-ing septa, hypodensity, calcified struc-t u res, and the identification of theRokitansky protuberance {1080,2132}.Radiographic studies of fetiform ter-atoma demonstrate portions of skull, ver-tebra and limb bones within the tumour{19}. There are no diagnostic findings forother germ tumours; they often havesolid and cystic components.
HistopathologyM o r p h o l o g i c a l l y, the diff e rent tumourtypes present in this group replicate in adistorted, grotesque form various stagesof embryonal development from early,
transient structures to mature adult tis-sues that in their turn may also be capa-ble of undergoing malignant change{2248}.
HistogenesisAs for histogenesis, they are believed tobe from the primordial germ cells thatmigrate into the gonadal ridge at 6 weeksof embryonic life {2848}. A small propor-tion may also arise from non-germ stemcells present in the adult female genitaltract {2039}.
Primitive germ cell tumours
DefinitionTumours that contain malignant germ cellelements other than teratoma.
ICD-O codesDysgerminoma 9060/3Yolk sac tumour 9071/3Embryonal carcinoma 9070/3 Polyembryoma 9072/3Non-gestational choriocarc i n o m a 9100/3Mixed germ cell tumour 9085/3
Dysgerminoma
DefinitionA tumour composed of a monotonousproliferation of primitive germ cells asso-ciated with connective tissue septa con-taining varying amount of lymphocytesand macrophages. Occasionally, syncy-tiotrophoblastic differentiation or somaticcysts occur. This tumour is identical totesticular seminoma.
MacroscopyThe usually well encapsulated tumourmasses are apparently unilateral in 90%of cases. Macroscopic involvement ofthe contralateral ovary is apparent in10% of cases, and in another 10% occultfoci of dysgerminoma can be detectedby biopsy {1929}. Tumours average 15cm in maximal dimension and on sectionare solid, uniform or lobular and creamywhite or light tan. Irregular areas of coag-
F. NogalesA. TalermanR.A. Kubik-HuchF.A. TavassoliM. Devouassoux-Shisheboran
Germ cell tumours
BAFig. 2.87 Dysgerminoma in a 28 year old nulligravida woman. A Magnetic resonance image sagital viewshows a 10 x 15 cm predominantly solid tumour with some central cystic changes. B Sectioned surface ofthe tumour shows a predominantly solid, multilobulated appearance with some cystic degeneration and fociof necrosis.
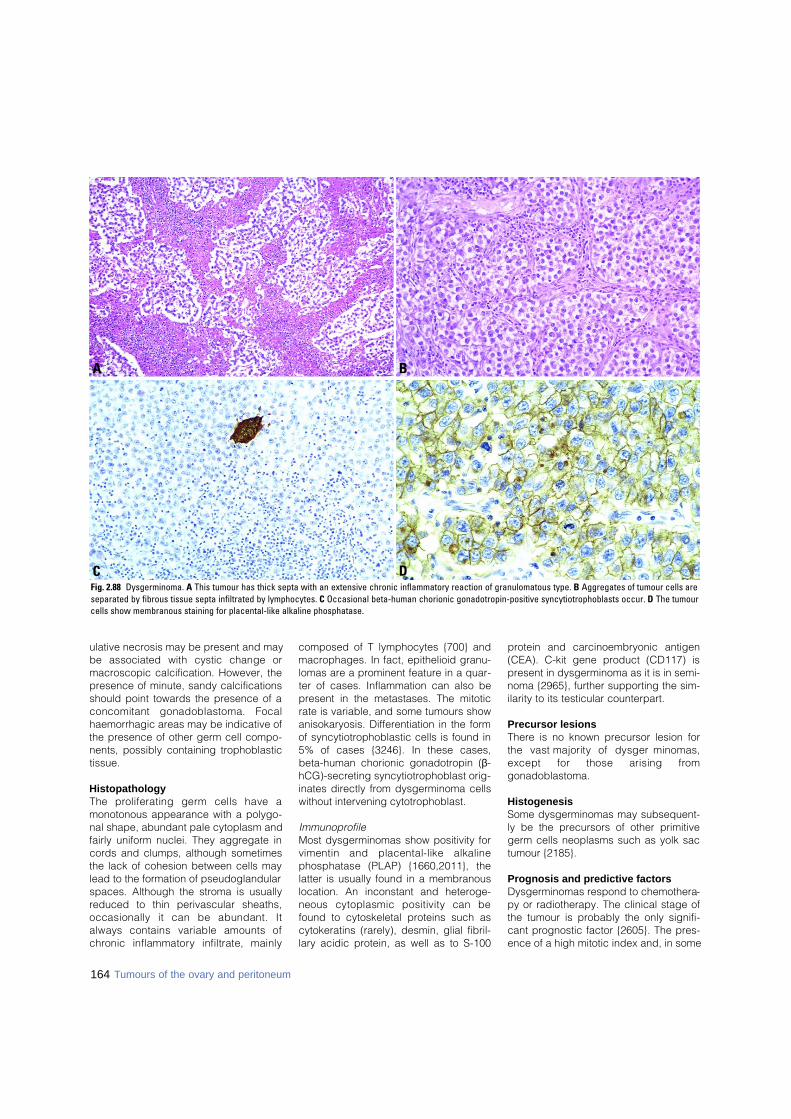
ulative necrosis may be present and maybe associated with cystic change ormacroscopic calcification. However, thepresence of minute, sandy calcificationsshould point towards the presence of aconcomitant gonadoblastoma. Focalhaemorrhagic areas may be indicative ofthe presence of other germ cell compo-nents, possibly containing trophoblastictissue.
HistopathologyThe proliferating germ cells have amonotonous appearance with a polygo-nal shape, abundant pale cytoplasm andfairly uniform nuclei. They aggregate incords and clumps, although sometimesthe lack of cohesion between cells maylead to the formation of pseudoglandularspaces. Although the stroma is usuallyreduced to thin perivascular sheaths,occasionally it can be abundant. Italways contains variable amounts ofc h ronic inflammatory infiltrate, mainly
composed of T lymphocytes {700} andmacrophages. In fact, epithelioid granu-lomas are a prominent feature in a quar-ter of cases. Inflammation can also bepresent in the metastases. The mitoticrate is variable, and some tumours showanisokaryosis. Differentiation in the formof syncytiotrophoblastic cells is found in5% of cases {3246}. In these cases,beta-human chorionic gonadotropin (β-hCG)-secreting syncytiotrophoblast orig-inates directly from dysgerminoma cellswithout intervening cytotrophoblast.
ImmunoprofileMost dysgerminomas show positivity forvimentin and placental-like alkalinephosphatase (PLAP) {1660,2011}, thelatter is usually found in a membranouslocation. An inconstant and heteroge-neous cytoplasmic positivity can befound to cytoskeletal proteins such ascytokeratins (rarely), desmin, glial fibril-lary acidic protein, as well as to S-100
protein and carcinoembryonic antigen(CEA). C-kit gene product (CD117) ispresent in dysgerminoma as it is in semi-noma {2965}, further supporting the sim-ilarity to its testicular counterpart.
Precursor lesionsThere is no known precursor lesion forthe vast majority of dysgerm i n o m a s ,except for those arising fro mgonadoblastoma.
HistogenesisSome dysgerminomas may subsequent-ly be the precursors of other primitivegerm cells neoplasms such as yolk sactumour {2185}.
Prognosis and predictive factorsDysgerminomas respond to chemothera-py or radiotherapy. The clinical stage ofthe tumour is probably the only signifi-cant prognostic factor {2605}. The pres-ence of a high mitotic index and, in some
164 Tumours of the ovary and peritoneum
DC
BA
Fig. 2.88 Dysgerminoma. A This tumour has thick septa with an extensive chronic inflammatory reaction of granulomatous type. B Aggregates of tumour cells areseparated by fibrous tissue septa infiltrated by lymphocytes. C Occasional beta-human chorionic gonadotropin-positive syncytiotrophoblasts occur. D The tumourcells show membranous staining for placental-like alkaline phosphatase.

cases, anisokaryosis has no prognosticimplication The behaviour of dysgermi-noma with trophoblastic differentiation isidentical to the usual type, but with theadvantage of having β-hCG as a serummarker.
Yolk sac tumour
DefinitionYolk sac tumours are morphologicallyh e t e rogeneous, primitive teratoid neo-plasms differentiating into multiple endo-dermal structures, ranging from the prim-itive gut to its derivatives of extraembryo-nal (secondary yolk sac vesicle) andembryonal somatic type, e.g. intestine,liver {2035}. These neoplasms havemany epithelial patterns and are typical-ly immunoreactive for alpha-fetoprotein.
Synonym and historical annotationSince the secondary yolk sac componentrepresents only one of its many lines ofdifferentiation, the current nomenclatureis clearly restrictive. Perhaps the term“endodermal primitive tumours” wouldbe more accurate in defining all the pos-sible lines of differentiation, both epithe-lial and mesenchymal, that occur inthese neoplasms.The term “endodermal sinus tumour”,although still in use, is misleading, sincethe endodermal sinus is neither a struc-ture present in human embryogenesis{1463} nor is it a constant feature of theseneoplasms, as it only occurs in a minori-ty of cases {1537}.
MacroscopyThese tumours are usually well encapsu-lated with an average diameter of 15 cm{1537}. The sectioned tumour surface issoft and grey-yellow with frequent areas
of necrosis, haemorrhage and liquefac-tion. Cysts can be found in the peripheryf o rming a honeycomb appearance{2043}; rare l y, they can be unicystic{522}. A relatively frequent finding is thepresence of a benign cystic teratoma inthe contralateral ovary {3033}.
HistopathologyAlthough a marked histological hetero-geneity due to numerous patterns of dif-ferentiation coexisting in the same neo-plasm may occur, almost invariably char-acteristic areas are present that allow forthe correct diagnosis.The characteristic reticular patternformed by a loose, basophilic, myxoidstroma harbouring a meshwork of micro-cystic, labyrinthine spaces lined by clearor flattened epithelial cells with variousdegrees of atypia and cytoplasmic PAS-positive, diastase-resistant hyaline glob-ules permits tumour identification.Irregular but constant amounts of hya-line, amorphous basement membranematerial are found in relation to theepithelial cells. Both hyaline globulesand the coarse aggregates of basementmembrane material {2032,2979} aregood histological indicators for tumouridentity. Less frequently, in 13-20% ofcases, papillary fibrovascular projectionslined by epithelium (Schiller-Duval bod-ies) are found that bear a resemblance tothe structures of the choriovitelline pla-centa of the rat, a fact that permitted theestablishment of the teratoid, endoder-mal identity of these tumours {2896}.
Histological variantsLess common histological variantsinclude the polyvesicular vitelline tumour,solid yolk sac tumour, parietal yolk sac
t u m o u r, glandular types of yolk sactumour and hepatoid yolk sac tumour.In the polyvesicular vitelline tumour cys-tic, organoid change of the epithelialspaces occurs that consists of multipledilatations lined by mesothelial-like cellsthat coexist with a columnar, PAS-posi-tive epithelium {2043}. The solid yolk sac tumour shows areas ofsolid epithelial sheets of cells with a char-acteristic abundant clear cytoplasm andnumerous hyaline globules. These areasmay resemble anaplastic changes ofd y s g e rminoma or even clear celltumours {1537} but have the distinctiveimmunophenotype of a yolk sac tumour.Although exceptionally rare, parietal-typeyolk sac tumours that are AFP-negativehave been described {598,620}. Theya re analogous to the experimentalmurine tumour of the same name andcan be identified by the massive deposi -tion of amorphous extracellular base-ment membrane, a material similar to theReichert membrane of the murine pari-etal yolk sac.D i ff e rentiation into organized somaticendodermal derivatives such as endo-dermal type gland-like structures resem-bling early lung and intestine as well asliver tissue can occur in a focal fashion inas many as a third of tumours {1968,2515,2979}. In rare instances these dif-ferentiated tissues may become the pre-dominant elements in the tumour.Extensive differentiation of endodermaltype glands characterizes the glandularvariants of yolk sac tumours, which mayadopt different morphological subtypes.F rom an embryological viewpoint themore immature type is represented byn u m e rous dilated angular glands orpapillae lined by an eosinophilic colum-
165Germ cell tumours
Table 2.05 Morphological patterns of yolk sac tumours with their equivalent types of tissue differentiation.
Somatic endodermPrimitive intestine and lung (?)
Early liver
Glandular
Hepatic
Extraembryonal endoderm
Primitive endoderm and secondary yolk sac
Allantois
Murine-type (?) parietal yolk sac
ReticularSolidEndodermal sinus
Polyvesicular
Parietal
Site differentiated Tissue differentiated Histological pattern
Fig. 2.89 Yolk sac tumour. Sectioned surface is pre-dominately solid and fleshy with areas of haemor-rhage, necrosis and cyst formation.
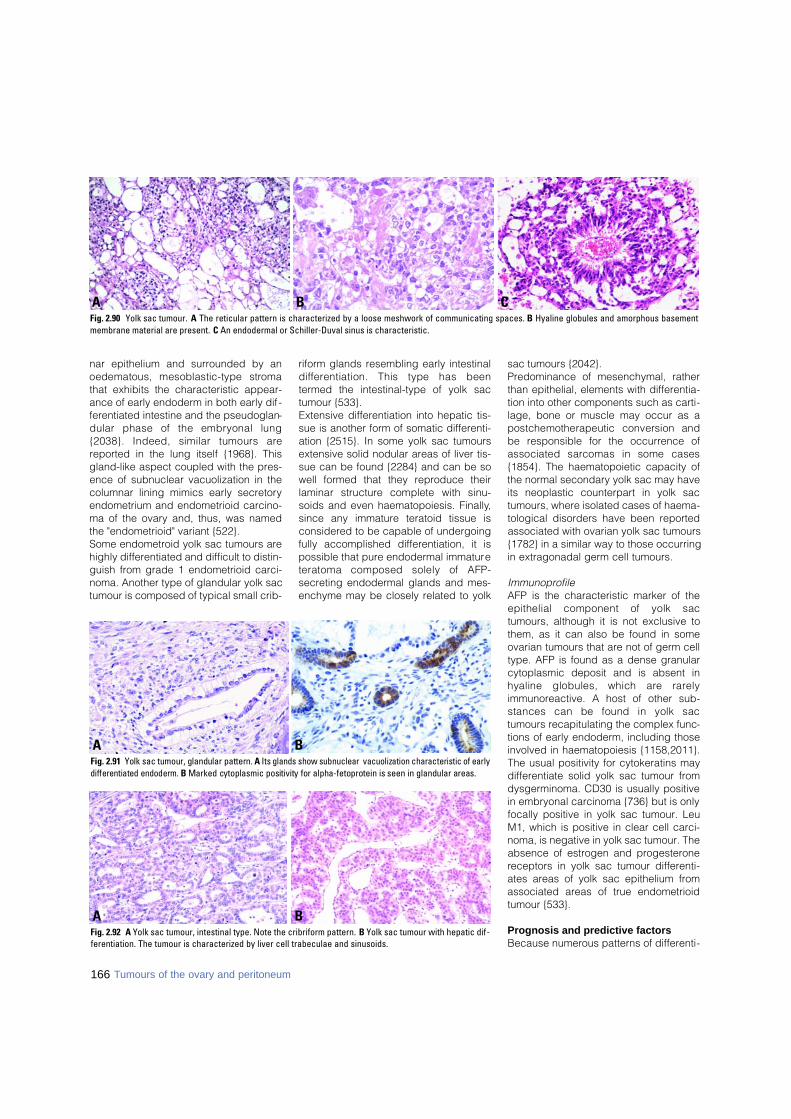
166 Tumours of the ovary and peritoneum
nar epithelium and surrounded by anoedematous, mesoblastic-type stro m athat exhibits the characteristic appear-ance of early endoderm in both early dif -ferentiated intestine and the pseudoglan-dular phase of the embryonal lung{2038}. Indeed, similar tumours arereported in the lung itself {1968}. Thisgland-like aspect coupled with the pres-ence of subnuclear vacuolization in thecolumnar lining mimics early secretoryendometrium and endometrioid carcino-ma of the ovary and, thus, was namedthe "endometrioid" variant {522}. Some endometroid yolk sac tumours arehighly differentiated and difficult to distin-guish from grade 1 endometrioid carci-noma. Another type of glandular yolk sactumour is composed of typical small crib-
riform glands resembling early intestinald i ff e rentiation. This type has beentermed the intestinal-type of yolk sactumour {533}. Extensive differentiation into hepatic tis-sue is another form of somatic differenti-ation {2515}. In some yolk sac tumoursextensive solid nodular areas of liver tis-sue can be found {2284} and can be sowell formed that they reproduce theirlaminar structure complete with sinu-soids and even haematopoiesis. Finally,since any immature teratoid tissue isconsidered to be capable of undergoingfully accomplished differentiation, it ispossible that pure endodermal immatureteratoma composed solely of AFP-secreting endodermal glands and mes-enchyme may be closely related to yolk
sac tumours {2042}.Predominance of mesenchymal, ratherthan epithelial, elements with differentia-tion into other components such as carti-lage, bone or muscle may occur as apostchemotherapeutic conversion andbe responsible for the occurrence ofassociated sarcomas in some cases{1854}. The haematopoietic capacity ofthe normal secondary yolk sac may haveits neoplastic counterpart in yolk sactumours, where isolated cases of haema-tological disorders have been reportedassociated with ovarian yolk sac tumours{1782} in a similar way to those occurringin extragonadal germ cell tumours.
ImmunoprofileAFP is the characteristic marker of theepithelial component of yolk sactumours, although it is not exclusive tothem, as it can also be found in someovarian tumours that are not of germ celltype. AFP is found as a dense granularcytoplasmic deposit and is absent inhyaline globules, which are rare l yimmunoreactive. A host of other sub-stances can be found in yolk sactumours recapitulating the complex func-tions of early endoderm, including thoseinvolved in haematopoiesis {1158,2011}.The usual positivity for cytokeratins maydifferentiate solid yolk sac tumour fromdysgerminoma. CD30 is usually positivein embryonal carcinoma {736} but is onlyfocally positive in yolk sac tumour. LeuM1, which is positive in clear cell carci-noma, is negative in yolk sac tumour. Theabsence of estrogen and progesteronereceptors in yolk sac tumour differenti-ates areas of yolk sac epithelium fromassociated areas of true endometrioidtumour {533}.
Prognosis and predictive factorsBecause numerous patterns of differenti-
B CAFig. 2.90 Yolk sac tumour. A The reticular pattern is characterized by a loose meshwork of communicating spaces. B Hyaline globules and amorphous basementmembrane material are present. C An endodermal or Schiller-Duval sinus is characteristic.
BAFig. 2.91 Yolk sac tumour, glandular pattern. A Its glands show subnuclear vacuolization characteristic of earlydifferentiated endoderm. B Marked cytoplasmic positivity for alpha-fetoprotein is seen in glandular areas.
BAFig. 2.92 A Yolk sac tumour, intestinal type. Note the cribriform pattern. B Yolk sac tumour with hepatic dif-ferentiation. The tumour is characterized by liver cell trabeculae and sinusoids.
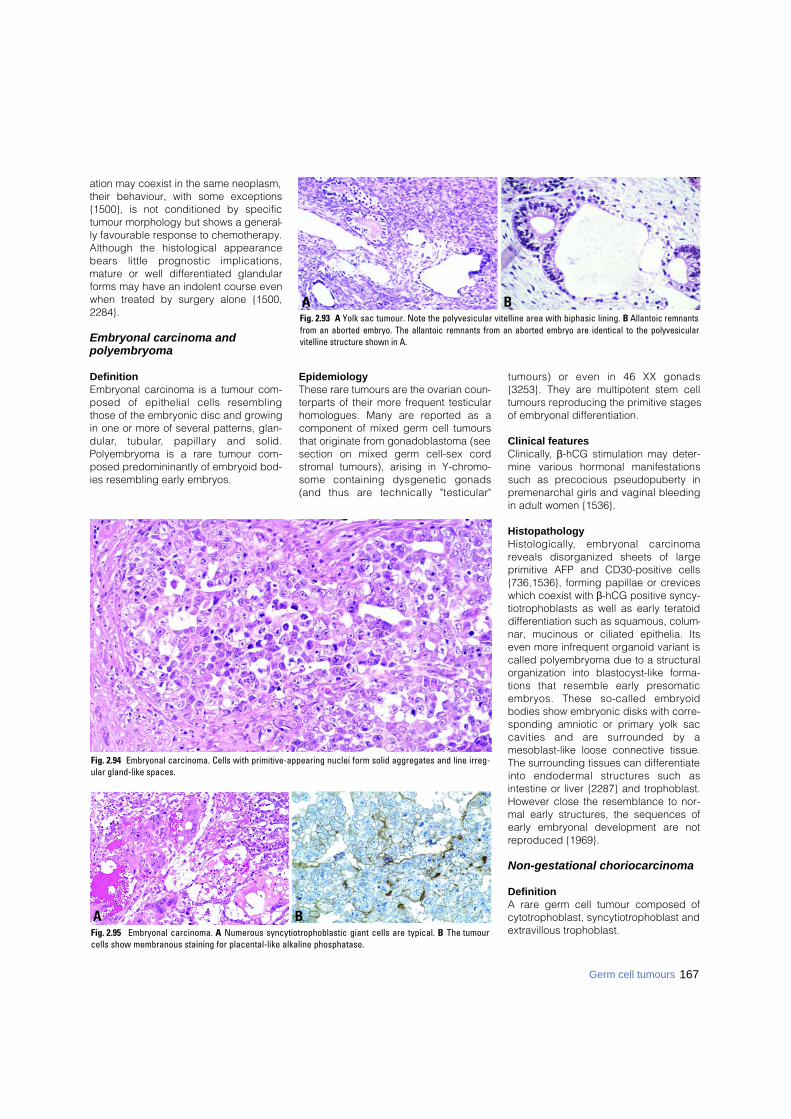
ation may coexist in the same neoplasm,their behaviour, with some exceptions{1500}, is not conditioned by specifictumour morphology but shows a general-ly favourable response to chemotherapy.Although the histological appearancebears little prognostic implications,mature or well differentiated glandularforms may have an indolent course evenwhen treated by surgery alone {1500,2284}.
Embryonal carcinoma and polyembryoma
DefinitionEmbryonal carcinoma is a tumour com-posed of epithelial cells re s e m b l i n gthose of the embryonic disc and growingin one or more of several patterns, glan-d u l a r, tubular, papillary and solid.Polyembryoma is a rare tumour com-posed predomininantly of embryoid bod-ies resembling early embryos.
EpidemiologyThese rare tumours are the ovarian coun-terparts of their more frequent testicularhomologues. Many are reported as acomponent of mixed germ cell tumoursthat originate from gonadoblastoma (seesection on mixed germ cell-sex cordstromal tumours), arising in Y-chromo-some containing dysgenetic gonads(and thus are technically "testicular"
tumours) or even in 46 XX gonads{3253}. They are multipotent stem celltumours reproducing the primitive stagesof embryonal differentiation.
Clinical featuresClinically, β-hCG stimulation may deter-mine various hormonal manifestationssuch as precocious pseudopuberty inpremenarchal girls and vaginal bleedingin adult women {1536}.
HistopathologyH i s t o l o g i c a l l y, embryonal carc i n o m areveals disorganized sheets of largeprimitive AFP and CD30-positive cells{736,1536}, forming papillae or creviceswhich coexist with β-hCG positive syncy-tiotrophoblasts as well as early teratoiddifferentiation such as squamous, colum-nar, mucinous or ciliated epithelia. Itseven more infrequent organoid variant iscalled polyembryoma due to a structuralorganization into blastocyst-like forma-tions that resemble early pre s o m a t i ce m b ryos. These so-called embry o i dbodies show embryonic disks with corre-sponding amniotic or primary yolk saccavities and are surrounded by amesoblast-like loose connective tissue.The surrounding tissues can differentiateinto endodermal structures such asintestine or liver {2287} and trophoblast.However close the resemblance to nor-mal early structures, the sequences ofearly embryonal development are notreproduced {1969}.
Non-gestational choriocarcinoma
DefinitionA rare germ cell tumour composed ofcytotrophoblast, syncytiotrophoblast andextravillous trophoblast.
BAFig. 2.93 A Yolk sac tumour. Note the polyvesicular vitelline area with biphasic lining. B Allantoic remnantsfrom an aborted embryo. The allantoic remnants from an aborted embryo are identical to the polyvesicularvitelline structure shown in A.
Fig. 2.94 Embryonal carcinoma. Cells with primitive-appearing nuclei form solid aggregates and line irreg-ular gland-like spaces.
BAFig. 2.95 Embryonal carcinoma. A Numerous syncytiotrophoblastic giant cells are typical. B The tumourcells show membranous staining for placental-like alkaline phosphatase.
167Germ cell tumours

Clinical featuresClinically, hormonal manifestations suchas precocious pseudopuberty and vagi-nal bleeding are present in children andyoung adults.
MacroscopyMacroscopically, tumours are large andhaemorrhagic, and large luteinized nod-ules or cysts due to β-hCG stimulationmay appear in the uninvolved ovarian tis-sue.
HistopathologyMorphologically identical to gestationalchoriocarcinoma, primary non-gestation -al choriocarcinoma is rare in pure form,differentiates as an admixture of cytotro-phoblast, syncytiotrophoblast andextravillous trophoblast and is usuallyfound associated with other germ cellcomponents {2704}. Histologically, thereare fenestrated or plexiform sheets or
pseudopapillae of cytotrophoblast andextravillous trophoblast admixed withnumerous syncytiotrophoblasts. Tumourcan be found in blood-filled spaces andsinusoids. Vascular invasion is frequent.The immunophenotype is characteristicfor each type of proliferating trophoblas-tic cell {1759} and includes cytokeratins,human placental lactogen and, aboveall, β-hCG.
Differential diagnosisWhen found in a pure form in childbear-ing age, gestational choriocarc i n o m a ,either primary in the ovary {3024} ormetastatic {718} must be excluded. Thismay be accomplished by identifyingp a t e rnal sequences by DNA analysis{1698,2655}.
Prognosis and predictive factorsThe distinction from gestational chorio-carcinoma is important since non-gesta-tional choriocarcinoma has a lessfavourable prognosis and requires moreaggressive chemotherapeutic treatmentregimens.
Mixed germ cell tumours
DefinitionMixed germ cell tumours are composedof at least two different germ cell ele-ments of which at least one is primitive.
Clinical featuresThe value of tumour markers such as β-hCG and AFP in the diagnosis and fol-low-up of patients with mixed germ celltumours containing elements of chorio-
carcinoma or yolk sac tumour has beenproven over the years {2850}. Elevatedserum levels of these markers shouldprompt a search for different compo-nents with extensive sampling of thetumour.
HistopathologyHistologically, the most common combi-nation of neoplastic germ cell elementsfound in ovarian mixed germ celltumours is dysgerminoma and yolk sactumour {2850}. Additional neoplasticgerm cell elements, including immatureor mature teratoma, embryonal carcino-ma, polyembryoma and/or choriocarci-noma, may also be present. All compo-nents of a mixed germ cell tumour andtheir approximate proportions should bementioned in the diagnosis.Most ovarian embryonal carcinomas arereally malignant mixed germ celltumours, usually admixed with yolk sactumour and showing a large or predomi-nant component of embryonal carcinoma{2850}. Although polyembryoma mayhave been the predominant malignantgerm cell element within the tumour, acareful review of all the published casesof ovarian polyembryoma shows thatother germ cell elements were also pres-ent {2850}. Also, ovarian choriocarcino-ma of germ cell origin is in the majority ofcases combined with other neoplasticgerm cell elements. Immunohistochemi-cal demonstration of β-hCG and AFP is auseful diagnostic modality in this groupof tumours, as is the demonstration ofPLAP in a component of dysgerminoma
Prognosis and predictive factorsAll elements in a malignant mixed germcell tumour are capable of widespreadmetastatic dissemination. The metas-tases may be composed of a single neo-plastic germ cell element or of variouselements. Although these tumours are highlyresponsive to platinum-based chemo-therapy, the therapeutic regimens shouldbe based primarily on the most malig-nant elements of the tumour {2850}.
Biphasic or triphasic teratomas
DefinitionTumours composed of derivatives of twoor three primary germ layers (ectoderm,mesoderm, endoderm).
Fig. 2.97 Ovarian choriocarcinoma. A plexiform pattern is present with syncytiotrophoblasts covering clus-ters of smaller cytotrophoblasts.
Fig. 2.96 Embryoid body in polyembryoma. Note theblastocyst-like formation consisting of an embry-onic disc that is continuous with a primitive yolksac cavity exhibiting alpha-fetoproten secretion inits distal portion.
168 Tumours of the ovary and peritoneum
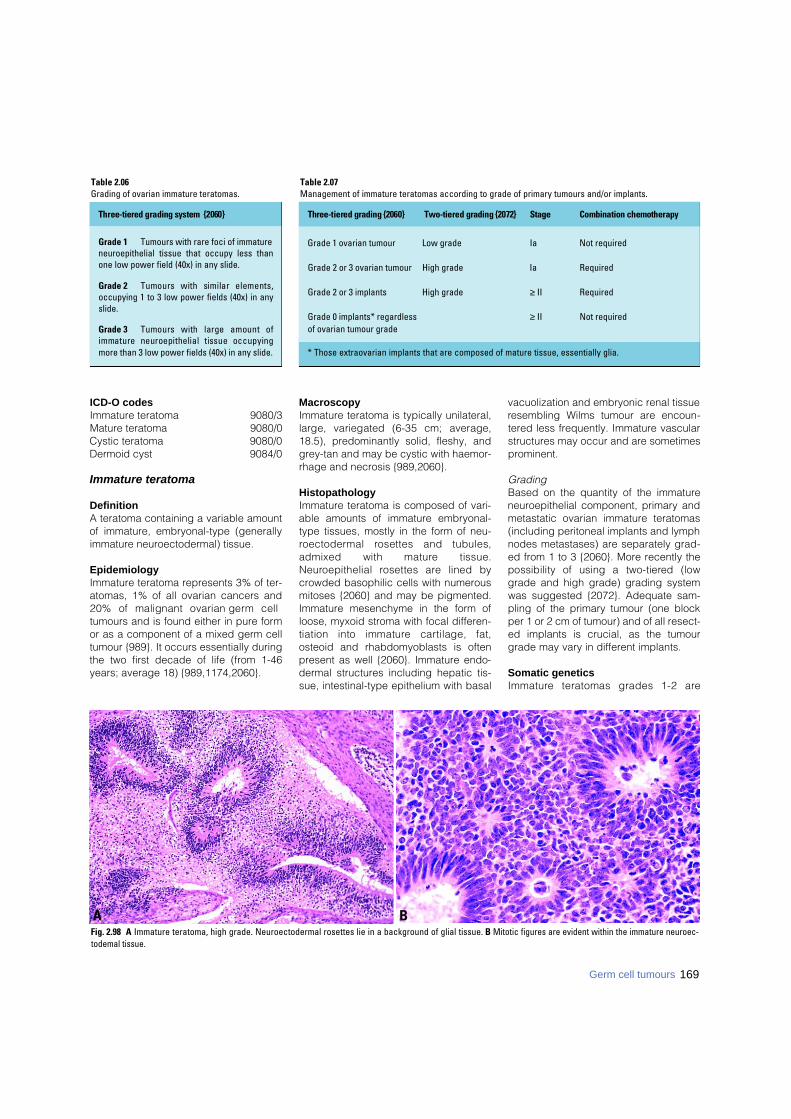
ICD-O codesImmature teratoma 9080/3Mature teratoma 9080/0Cystic teratoma 9080/0Dermoid cyst 9084/0
Immature teratoma
DefinitionA teratoma containing a variable amountof immature, embryonal-type (generallyimmature neuroectodermal) tissue.
EpidemiologyImmature teratoma represents 3% of ter-atomas, 1% of all ovarian cancers and20% of malignant ovarian germ celltumours and is found either in pure formor as a component of a mixed germ celltumour {989}. It occurs essentially duringthe two first decade of life (from 1-46years; average 18) {989,1174,2060}.
MacroscopyImmature teratoma is typically unilateral,large, variegated (6-35 cm; average,18.5), predominantly solid, fleshy, andgrey-tan and may be cystic with haemor-rhage and necrosis {989,2060}.
HistopathologyImmature teratoma is composed of vari-able amounts of immature embryonal-type tissues, mostly in the form of neu-ro e c t o d e rmal rosettes and tubules,admixed with mature tissue.N e u roepithelial rosettes are lined bycrowded basophilic cells with numerousmitoses {2060} and may be pigmented.Immature mesenchyme in the form ofloose, myxoid stroma with focal differen-tiation into immature cartilage, fat,osteoid and rhabdomyoblasts is oftenpresent as well {2060}. Immature endo-dermal structures including hepatic tis-sue, intestinal-type epithelium with basal
vacuolization and embryonic renal tissueresembling Wilms tumour are encoun-tered less frequently. Immature vascularstructures may occur and are sometimesprominent.
Grading Based on the quantity of the immatureneuroepithelial component, primary andmetastatic ovarian immature teratomas(including peritoneal implants and lymphnodes metastases) are separately grad-ed from 1 to 3 {2060}. More recently thepossibility of using a two-tiered (lowgrade and high grade) grading systemwas suggested {2072}. Adequate sam-pling of the primary tumour (one blockper 1 or 2 cm of tumour) and of all resect-ed implants is crucial, as the tumourgrade may vary in different implants.
Somatic geneticsI m m a t u re teratomas grades 1-2 are
169Germ cell tumours
Table 2.07Management of immature teratomas according to grade of primary tumours and/or implants.
BAFig. 2.98 A Immature teratoma, high grade. Neuroectodermal rosettes lie in a background of glial tissue. B Mitotic figures are evident within the immature neuroec-todemal tissue.
Three-tiered grading system {2060}
Grade 1 Tumours with rare foci of immatureneuroepithelial tissue that occupy less thanone low power field (40x) in any slide.
Grade 2 Tumours with similar elements,occupying 1 to 3 low power fields (40x) in anyslide.
Grade 3 Tumours with large amount ofimmature neuroepithelial tissue occupyingmore than 3 low power fields (40x) in any slide.
Three-tiered grading {2060} Two-tiered grading {2072} S t a g e Combination chemotherapy
Grade 1 ovarian tumour Low grade Ia Not required
Grade 2 or 3 ovarian tumour High grade Ia Required
Grade 2 or 3 implants High grade ≥ II Required
Grade 0 implants* regardless ≥ II Not requiredof ovarian tumour grade
* Those extraovarian implants that are composed of mature tissue, essentially glia.
Table 2.06Grading of ovarian immature teratomas.

diploid in 90% of cases, whereas most(66%) of grade 3 tumours are aneuploid{165,2684}. Similarly, karyotypic abnor-malities are most often seen in grade 3tumours {165}. Immature teratomas showfewer DNA copy number changesdetected by comparative genomichybridization than other ovarian germcell tumours and do not usually exhibit again of 12p or i(12p) {1518,2378}.
Prognosis and predictive factorsThe stage and grade of the primarytumour and the grade of its metastasesare important predictive factors. Prior tothe chemotherapy era, the overall sur-vival rate of patients with grade 1, 2 and3 neoplasms was 82%, 63% and 30%,respectively {2060}.The use of cisplatin-based combinationchemotherapy has dramaticallyimproved the survival rate of patients; 90-100% of those receiving this regimenremain disease-free {989}.The tumour grade is a crucial feature thatdetermines behaviour and type of thera-py. Patients with grade 1 tumours that arestage IA and those with mature (grade 0)implants do not re q u i re adjuvantchemotherapy. Those with grade 2 or 3tumours, including stage IA, as well asthose with immature implants re q u i recombination chemotherapy. The man-agement of patients with grade 1implants/metastases is not well estab-lished.A recent re p o rt from the PediatricOncology Group concludes that surgeryalone is curative in children and adoles-cents with immature teratoma of anygrade, reserving chemotherapy for
cases with relapse {600}. Also, in imma-ture teratomas occurring in childhood,the presence of histological foci of yolksac tumour rather than the grade of theimmature component, per se, is the onlypredictor of recurrence {1174}.
Mature teratoma
DefinitionA cystic or, more rarely, a solid tumourcomposed exclusively of mature, adult-type tissues. A cyst lined by mature tis-sue resembling the epidermis with itsappendages is clinically designated as"dermoid cyst". Homunculus or fetiformteratoma is a rare type of mature, solidteratoma containing highly organizedstructures resembling a malformed fetus("homunculus" = little man).
EpidemiologyAgeAlthough most mature cystic teratomasoccur during the reproductive years, theyhave a wide age distribution, from 2-80years (mean, 32), and 5% occur in post-menopausal women {564}. Mature solidteratoma occurs mainly in the first twodecades of life {199,2922}.
IncidenceM a t u re cystic teratoma accounts for 27-44% of all ovarian tumours and up to58% of the benign tumours {1502}. Inaddition to their pure form, derm o i dcysts are found macroscopically within25% of immature teratomas and in theo v a ry contralateral to a malignant prim-itrive germ cell tumour in 10-15% of thecases.
Clinical featuresSigns and symptoms Most mature cystic teratomas presentwith a mass, but at least 25% (up to 60%in some series) are discovered inciden-tally {546}. Symptoms such as a pelvicmass or pain are more common when themature teratoma is solid {199,2922}. The following complications have beend e s c r i b e d :(1) Torsion of the pedicle occurs in 10-16% of the cases, is responsible for acuteabdominal pain and may be complicatedby infarction, perforation or intra-abdomi-nal haemorrhage.(2) Tumour rupture occurs in 1% of casesand can be spontaneous or traumatic.The spillage of the cyst contents into theperitoneum produces chemical peritonitiswith granulomatous nodules mimickingt u b e rculosis or carcinomatosis. Rupture ofm a t u re teratoma containing neuro g l i a lelements is thought to be responsible forgliomatosis peritonei characterized byperitoneal “implants” composed of matureglial tissue and does not affect the pro g-nosis {2389}. However, a recent molecularstudy has demonstrated that these glialimplants were heterozygous, whereas theassociated mature ovarian teratomasw e re homozygous at the same micro s a t e l-lite loci. This finding suggests that glialimplants may arise from metaplasia ofpluripotent müllerian stem cells ratherthan from implantation of the associatedovarian teratomas {845}. Similarly, peri-toneal melanosis characterized by pig-mentation of the peritoneum has beenre p o rted in cases of dermoid cysts.(3) Infection of the tumour occurs in 1% ofc a s e s .
Fig. 2.101 Fetiform teratoma (homunculus). Limbbuds are apparent, and there is abundant hair overthe cephalic portion.
Fig. 2.100 Mature cystic teratoma with dark hair.The Rokitansky protuberance is composed of fattytissue, bone, and teeth protuding into the lumen.
Fig. 2.99 Mature cystic teratoma. T1-weighted pre-contrast magnetic resonance image. A fat-fluidlevel is seen (arrow).
170 Tumours of the ovary and peritoneum

(4) Haemolytic anaemia has been report-ed in rare cases {1020}.
MacroscopyDermoid cyst is an ovoid, occasionallybilateral (8-15% of cases), cystic mass of0.5-40 cm (average 15 cm) with asmooth external surface and is filled withsebaceous material and hair. A nodulecomposed of fat tissue with teeth or boneprotrudes into the cyst and is termed aRokitansky protuberance. Mature solid teratoma is a large, solidmass with multiple cysts of varying size,a soft, cerebroid appearance and smallfoci of haemorrhage.
HistopathologyM a t u re teratomas are composed ofadult-type tissue derived from two orthree embryonic layers. Benign tumourssuch as struma ovarii, carcinoid, corti-c o t roph cell adenoma, pro l a c t i n o m a ,naevus and glomus tumour may arisewithin a typical dermoid cyst {143,1389,2162,2682}.
HistogenesisThe presence of Barr bodies (nuclearsex chromatin) and a 46 XX karyotype isconsistent with origin through partheno-genetic development. Selective tissuemicrodissection and genetic analysis ofmature ovarian teratomas demonstrateda genotypic difference between homozy-gous teratomatous tissues and heterozy-
gous host tissue in support of their originf rom a post-meiotic germ cell {1667,3032}. Lymphoid aggregates associatedwith squamous or glandular epitheliumwithin teratomas are heterozygous andderived from host tissue, whereas welldifferentiated thymic tissue is homozy-gous, suggesting capability for lymphoiddifferentiation {3032}. Although multiple teratomas in the sameovary originate independently from differ-ent progenitor germ cells, they mayappear histologically similar indicatingthe role of possible local and environ-mental factors in phenotypic differentia-tion of ovarian germ cell tumours {683}.
Prognosis and predictive factorsDermoid cysts with histological foci (upto 21 mm2) of immature neuroepithelialtissue have an excellent pro g n o s i s{3174}. Recurrence in the form of a der-moïd cyst (3% of cases) or immature ter-atoma (2-2.6% of cases) in the residualipsilateral ovary is most frequent whenthe initial cysts are bilateral or multipleand have ruptured {104,3174}.
Monodermal teratomas and somatic-type tumours associated with dermoid cysts
DefinitionTeratomas composed exclusively or pre-dominantly of a single type of tissue
derived from one embryonic layer (ecto-d e rm or endoderm) and adult-typetumours derived from a dermoid cyst.
ICD-O codesStruma ovarii 9090/0Carcinoid 8240/3Mucinous carcinoid 8243/3Strumal carcinoid 9091/1Ependymoma 9391/3 Primitive neuro e c t o d e rmal tumour 9473/3Glioblastoma multiforme 9440/3Teratoma with malignant
transformation 9084/3Malignant melanoma 8720/3Melanocytic naevus 8720/0Sebaceous adenoma 8410/0Sebaceous carcinoma 8410/3Retinal anlage tumour 9363/0
Struma ovarii
DefinitionA mature teratoma composed eitherexclusively or predominantly of thyroidtissue. Struma ovarii may harbourchanges histologically identical to thyroidadenoma, carcinoma (malignant strumaovarii) or both. Those admixed with a car-cinoid (strumal carcinoid) are classifiedseparately.
EpidemiologyStruma ovarii, the most common type ofm o n o d e rmal teratoma, accounts for2.7% of all ovarian teratomas {3146} with
Fig. 2.102 A Mature cystic teratoma. Adult-type tissues such as intestine tend to have an organoid arrange-ment with two layers of smooth muscle beneath glandular mucosa. B Note the pigmented retinal epitheli-um and associated mature glial tissue.
BAFig. 2.103 Mature teratoma. Note the cerebellarstructures adjacent to adipose and fibrous connec-tive tissue.
171Germ cell tumours
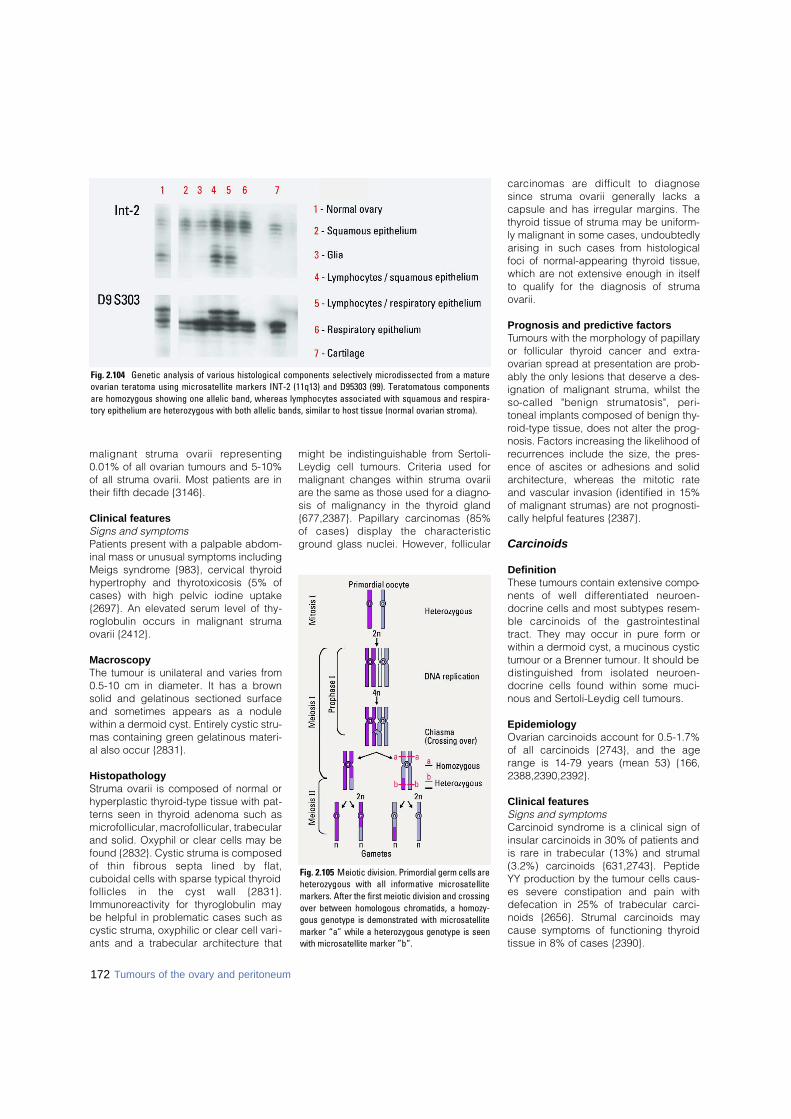
172 Tumours of the ovary and peritoneum
malignant struma ovarii re p re s e n t i n g0.01% of all ovarian tumours and 5-10%of all struma ovarii. Most patients are intheir fifth decade {3146}.
Clinical featuresSigns and symptoms Patients present with a palpable abdom-inal mass or unusual symptoms includingMeigs syndrome {983}, cervical thyroidhypertrophy and thyrotoxicosis (5% ofcases) with high pelvic iodine uptake{2697}. An elevated serum level of thy-roglobulin occurs in malignant strumaovarii {2412}.
MacroscopyThe tumour is unilateral and varies from0.5-10 cm in diameter. It has a brownsolid and gelatinous sectioned surfaceand sometimes appears as a nodulewithin a dermoid cyst. Entirely cystic stru-mas containing green gelatinous materi-al also occur {2831}.
HistopathologyStruma ovarii is composed of normal orhyperplastic thyroid-type tissue with pat-terns seen in thyroid adenoma such asmicrofollicular, macrofollicular, trabecularand solid. Oxyphil or clear cells may befound {2832}. Cystic struma is composedof thin fibrous septa lined by flat,cuboidal cells with sparse typical thyroidfollicles in the cyst wall {2831}.Immunoreactivity for thyroglobulin maybe helpful in problematic cases such ascystic struma, oxyphilic or clear cell vari-ants and a trabecular architecture that
might be indistinguishable from Sertoli-Leydig cell tumours. Criteria used formalignant changes within struma ovariiare the same as those used for a diagno-sis of malignancy in the thyroid gland{677,2387}. Papillary carcinomas (85%of cases) display the characteristicground glass nuclei. However, follicular
c a rcinomas are difficult to diagnosesince struma ovarii generally lacks acapsule and has irregular margins. Thethyroid tissue of struma may be uniform-ly malignant in some cases, undoubtedlyarising in such cases from histologicalfoci of normal-appearing thyroid tissue,which are not extensive enough in itselfto qualify for the diagnosis of strumaovarii.
Prognosis and predictive factorsTumours with the morphology of papillaryor follicular thyroid cancer and extra-ovarian spread at presentation are prob-ably the only lesions that deserve a des-ignation of malignant struma, whilst theso-called "benign strumatosis", peri-toneal implants composed of benign thy-roid-type tissue, does not alter the prog-nosis. Factors increasing the likelihood ofrecurrences include the size, the pres-ence of ascites or adhesions and solida rc h i t e c t u re, whereas the mitotic rateand vascular invasion (identified in 15%of malignant strumas) are not prognosti-cally helpful features {2387}.
Carcinoids
DefinitionThese tumours contain extensive compo-nents of well diff e rentiated neuro e n-docrine cells and most subtypes resem-ble carcinoids of the gastro i n t e s t i n a ltract. They may occur in pure form orwithin a dermoid cyst, a mucinous cystictumour or a Brenner tumour. It should bedistinguished from isolated neuro e n-docrine cells found within some muci-nous and Sertoli-Leydig cell tumours.
EpidemiologyOvarian carcinoids account for 0.5-1.7%of all carcinoids {2743}, and the agerange is 14-79 years (mean 53) {166,2388,2390,2392}.
Clinical featuresSigns and symptomsCarcinoid syndrome is a clinical sign ofinsular carcinoids in 30% of patients andis rare in trabecular (13%) and strumal(3.2%) carcinoids {631,2743}. PeptideYY production by the tumour cells caus-es severe constipation and pain withdefecation in 25% of trabecular carci-noids {2656}. Strumal carcinoids maycause symptoms of functioning thyroidtissue in 8% of cases {2390}.
Fig. 2.105 Meiotic division. Primordial germ cells areheterozygous with all informative microsatellitemarkers. After the first meiotic division and crossingover between homologous chromatids, a homozy-gous genotype is demonstrated with microsatellitemarker “a” while a heterozygous genotype is seenwith microsatellite marker ”b”.
Fig. 2.104 Genetic analysis of various histological components selectively microdissected from a matureovarian teratoma using microsatellite markers INT-2 (11q13) and D95303 (99). Teratomatous componentsare homozygous showing one allelic band, whereas lymphocytes associated with squamous and respira-tory epithelium are heterozygous with both allelic bands, similar to host tissue (normal ovarian stroma).
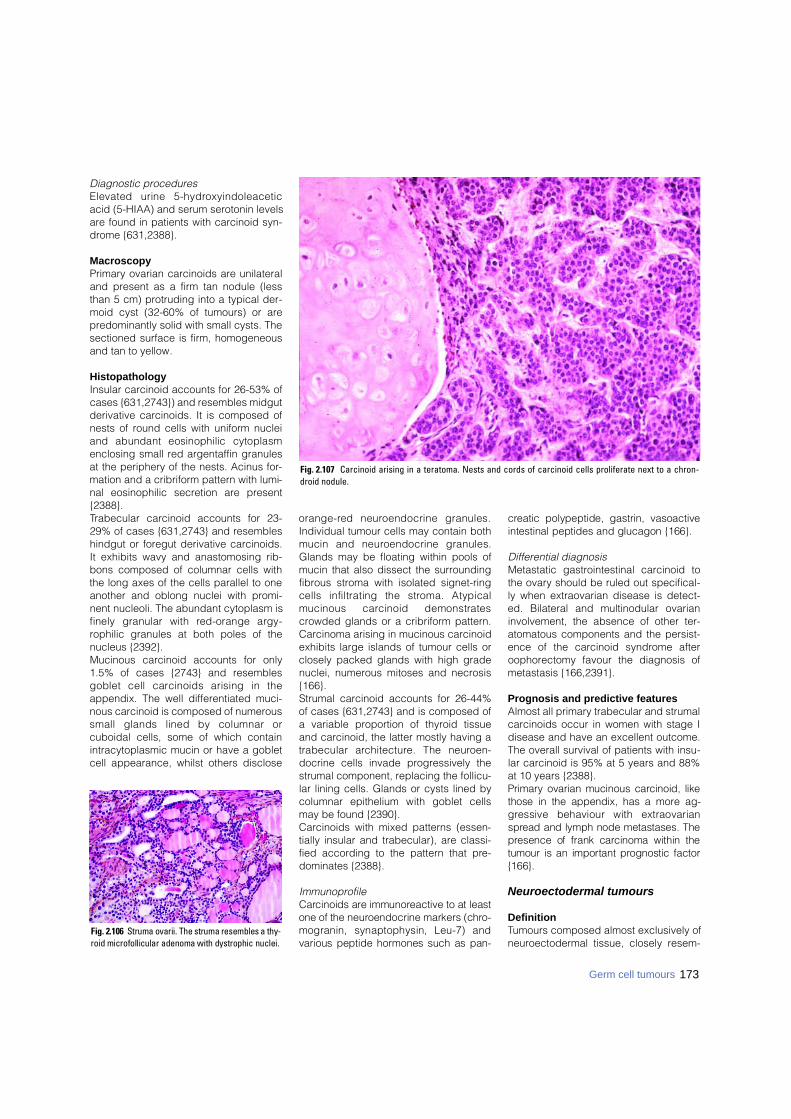
173Germ cell tumours
Diagnostic procedures Elevated urine 5-hydro x y i n d o l e a c e t i cacid (5-HIAA) and serum serotonin levelsare found in patients with carcinoid syn-drome {631,2388}.
MacroscopyPrimary ovarian carcinoids are unilateraland present as a firm tan nodule (lessthan 5 cm) protruding into a typical der-moid cyst (32-60% of tumours) or arepredominantly solid with small cysts. Thesectioned surface is firm, homogeneousand tan to yellow.
HistopathologyInsular carcinoid accounts for 26-53% ofcases {631,2743}) and resembles midgutderivative carcinoids. It is composed ofnests of round cells with uniform nucleiand abundant eosinophilic cytoplasmenclosing small red argentaffin granulesat the periphery of the nests. Acinus for-mation and a cribriform pattern with lumi-nal eosinophilic secretion are present{2388}.Trabecular carcinoid accounts for 23-29% of cases {631,2743} and resembleshindgut or foregut derivative carcinoids.It exhibits wavy and anastomosing rib-bons composed of columnar cells withthe long axes of the cells parallel to oneanother and oblong nuclei with promi-nent nucleoli. The abundant cytoplasm isfinely granular with red-orange argy-rophilic granules at both poles of thenucleus {2392}. Mucinous carcinoid accounts for only1.5% of cases {2743} and resemblesgoblet cell carcinoids arising in theappendix. The well differentiated muci-nous carcinoid is composed of numeroussmall glands lined by columnar orcuboidal cells, some of which containintracytoplasmic mucin or have a gobletcell appearance, whilst others disclose
o r a n g e - red neuroendocrine granules.Individual tumour cells may contain bothmucin and neuroendocrine granules.Glands may be floating within pools ofmucin that also dissect the surroundingfibrous stroma with isolated signet-ringcells infiltrating the stroma. Atypicalmucinous carcinoid demonstratescrowded glands or a cribriform pattern.Carcinoma arising in mucinous carcinoidexhibits large islands of tumour cells orclosely packed glands with high gradenuclei, numerous mitoses and necrosis{166}.Strumal carcinoid accounts for 26-44%of cases {631,2743} and is composed ofa variable proportion of thyroid tissueand carcinoid, the latter mostly having atrabecular arc h i t e c t u re. The neuro e n-docrine cells invade progressively thestrumal component, replacing the follicu-lar lining cells. Glands or cysts lined bycolumnar epithelium with goblet cellsmay be found {2390}. Carcinoids with mixed patterns (essen-tially insular and trabecular), are classi-fied according to the pattern that pre-dominates {2388}.
ImmunoprofileC a rcinoids are immunoreactive to at leastone of the neuroendocrine markers (chro-mogranin, synaptophysin, Leu-7) andvarious peptide hormones such as pan-
c reatic polypeptide, gastrin, vasoactiveintestinal peptides and glucagon {166}.
Differential diagnosisMetastatic gastrointestinal carcinoid tothe ovary should be ruled out specifical-ly when extraovarian disease is detect-ed. Bilateral and multinodular ovarianinvolvement, the absence of other ter-atomatous components and the persist-ence of the carcinoid syndrome afteroophorectomy favour the diagnosis ofmetastasis {166,2391}.
Prognosis and predictive featuresAlmost all primary trabecular and strumalcarcinoids occur in women with stage Idisease and have an excellent outcome.The overall survival of patients with insu-lar carcinoid is 95% at 5 years and 88%at 10 years {2388}. P r i m a ry ovarian mucinous carcinoid, likethose in the appendix, has a more ag-g ressive behaviour with extraovarians p read and lymph node metastases. Thep resence of frank carcinoma within thetumour is an important prognostic factor{166}.
Neuroectodermal tumours
DefinitionTumours composed almost exclusively ofneuroectodermal tissue, closely resem-
Fig. 2.106 Struma ovarii. The struma resembles a thy-roid microfollicular adenoma with dystrophic nuclei.
Fig. 2.107 Carcinoid arising in a teratoma. Nests and cords of carcinoid cells proliferate next to a chron-droid nodule.

174 Tumours of the ovary and peritoneum
bling neoplasms of the nervous systemwith a similar spectrum of differentiation.
EpidemiologyLess than 40 cases are re p o rted inpatients 6-69 years old (average 28),{1077,1418,1476}.
Clinical featuresThe tumours usually present as a pelvicmass.
MacroscopyTumours are unilateral and 4-20 cm indiameter, averaging 14 cm {1476}. Thesectioned surface varies from solid withfriable, gray-pink tissue to cystic withpapillary excrescences in their inner orouter surface {1077}.
Tumour spread and stagingThe majority of patients have stage II orIII disease at laparotomy usually in theform of peritoneal implants {1476}.
HistopathologyThese tumours are morphologically iden-tical to their nervous system counter-parts. They may be divided into threecategories as follows:(1) Well diff e rentiated forms such asependymoma.(2) Poorly differentiated tumours such asprimitive neurectodermal tumour (PNET),and medulloepithelioma. (3) Anaplastic forms such as glioblas-toma multiforme.Whilst ependymomas are not found inassociation with teratoma, other neuroec-todermal tumours in the ovary may beassociated with elements of mature orimmature teratoma {2605}. Cases previ-ously re p o rted as neuroblastoma ormedulloblastoma would now most likelybe classifed as PNETs since the mor-
phology of all three tumours is similarwith the term medulloblastoma beingreserved for cerebellar and neuroblas-toma for adrenal neoplasms {1474}.Medulloepithelioma, on the other hand,has a distinctive appearance character-ized by papillary, tubular or trabeculararrangements of neoplasiic neuroepithe-lium mimicking the embryonic neuraltube {1474}. Ependymomas and anaplastic tumoursa re immunoreactive for glial fibrillaryacidic protein. The characteristicimmunoprofile of PNETs, vimentin andMIC2 protein (CD99) positive and GFAP,cytokeratin, desmin. chromogranin, andinhibin negative, help to distinguishthese tumours from small cell carcinomaand juvenile granulosa cell tumour.
Somatic genetics Reverse transcription-polymerase chainreaction in a case of ovarian PNET led tothe detection of EWS/FLI1 chimeric tran-script, originating from the characteristict(11;22)(q24;q12) translocation of thePNET/Ewing tumour family {1418}.
Prognosis and predictive factorsMost patients with ovarian ependymo-mas survive despite multiple re c u r-rences, whereas patients with PNET andanaplastic tumours have a poor outcome{1476}.
Carcinomas
DefinitionA dermoid cyst in which a secondarycarcinoma develops.
EpidemiologyMalignancy arising within a mature cysticteratoma is a rare complication (1-2% ofcases), mostly re p o rted in post-
menopausal women (mean 51-62 years){1214,1429,2164}.
Clinical features The tumour may present as a dermoidcyst or as an advanced ovarian cancerdepending on tumour stage {2605}. Thetumour may show adherence to sur-rounding pelvic structures {1214,1429,2164}.
MacroscopyOn macroscopic examination cauliflowerexophytic growth, infiltrative grey-whiteplaques or thickenings of the cyst wallwith necrosis and haemorrhage may beseen {1214,1429,2164}.
HistopathologyThe malignancy may be detectable onlyafter histological examination, thus der-moid cysts in postmenopausal womenmust be adequately sampled. Any com-ponent of a mature teratoma may under-go malignant transform a t i o n .Carcinomas are the most common malig-nancy, with squamous cell carcinomasaccounting for 80% of cases and 51% ofall primary ovarian squamous cell carci-nomas {1214,2255}. Adenocarcinoma isthe second most common lmalignancyarising in dermoid cysts {1456}.A d e n o c a rcinoma of intestinal type{2970}, Paget disease, adenosquamousc a rcinoma, transitional cell carc i n o m a{1456}, undifferentiated carcinoma, smallcell carcinoma, basal cell carcinoma andc a rc i n o s a rcoma {123} have beendescribed {2605}. The malignant compo-nent invades other parts of the dermoidcyst and its wall.
Somatic geneticsSelective tissue microdissection andgenetic analyses of malignant tumours
B CAFig. 2.108 Strumal carcinoid. A Sectioned surface of the ovarian tumour shows a spongy brown area reflecting the strumal component and a solid yellow regionreflecting the carcinoid component. B The strumal and carcinoid tumour patterns are located side by side, with the struma on the right. C Immunoreactivity for cytok-eratin 7 is present in the strumal elements but not in the carcinoid trabeculae.
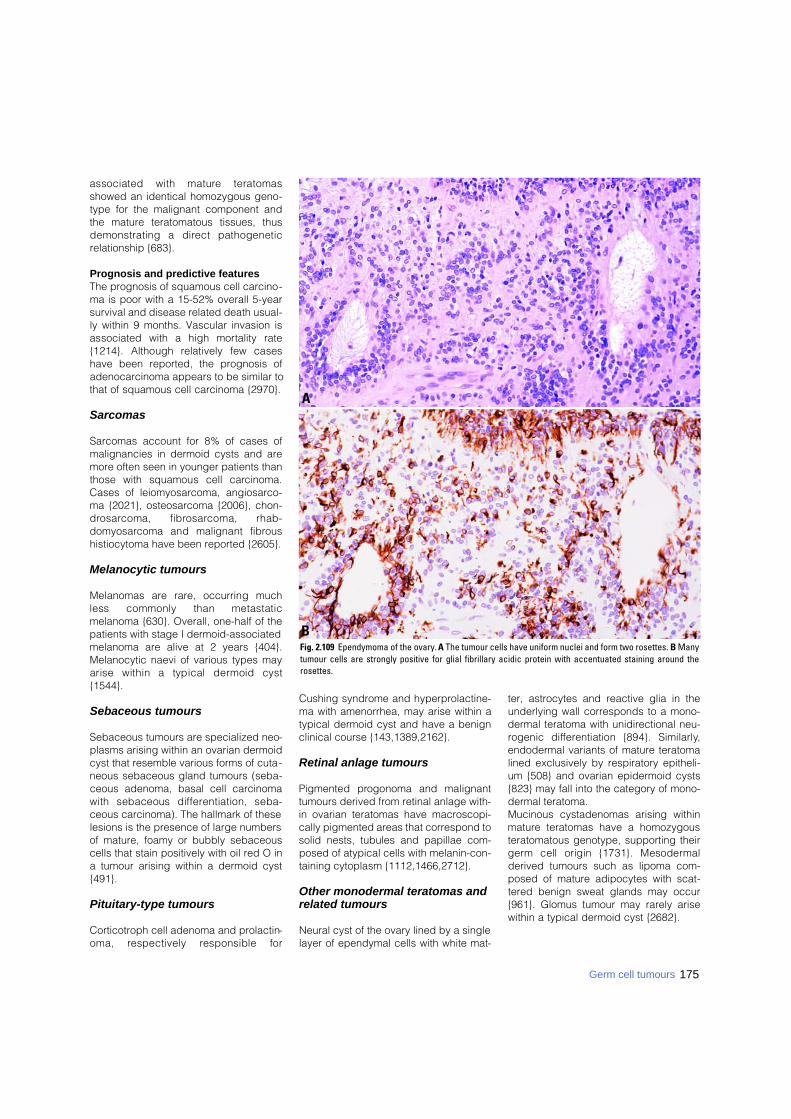
associated with mature teratomasshowed an identical homozygous geno-type for the malignant component andthe mature teratomatous tissues, thusdemonstrating a direct pathogeneticrelationship {683}.
Prognosis and predictive featuresThe prognosis of squamous cell carcino-ma is poor with a 15-52% overall 5-yearsurvival and disease related death usual-ly within 9 months. Vascular invasion isassociated with a high mortality rate{1214}. Although relatively few caseshave been reported, the prognosis ofadenocarcinoma appears to be similar tothat of squamous cell carcinoma {2970}.
Sarcomas
Sarcomas account for 8% of cases ofmalignancies in dermoid cysts and aremore often seen in younger patients thanthose with squamous cell carc i n o m a .Cases of leiomyosarcoma, angiosarco-ma {2021}, osteosarcoma {2006}, chon-d ro s a rcoma, fibro s a rcoma, rhab-d o m y o s a rcoma and malignant fibro u shistiocytoma have been reported {2605}.
Melanocytic tumours
Melanomas are rare, occurring muchless commonly than metastaticmelanoma {630}. Overall, one-half of thepatients with stage I dermoid-associatedmelanoma are alive at 2 years {404}.Melanocytic naevi of various types mayarise within a typical dermoid cyst{1544}.
Sebaceous tumours
Sebaceous tumours are specialized neo-plasms arising within an ovarian dermoidcyst that resemble various forms of cuta-neous sebaceous gland tumours (seba-ceous adenoma, basal cell carcinomawith sebaceous diff e rentiation, seba-ceous carcinoma). The hallmark of theselesions is the presence of large numbersof mature, foamy or bubbly sebaceouscells that stain positively with oil red O ina tumour arising within a dermoid cyst{491}.
Pituitary-type tumours
Corticotroph cell adenoma and prolactin-oma, respectively responsible for
Cushing syndrome and hyperprolactine-ma with amenorrhea, may arise within atypical dermoid cyst and have a benignclinical course {143,1389,2162}.
Retinal anlage tumours
Pigmented progonoma and malignanttumours derived from retinal anlage with-in ovarian teratomas have macroscopi-cally pigmented areas that correspond tosolid nests, tubules and papillae com-posed of atypical cells with melanin-con-taining cytoplasm {1112,1466,2712}.
Other monodermal teratomas and related tumours
Neural cyst of the ovary lined by a singlelayer of ependymal cells with white mat-
ter, astrocytes and reactive glia in theunderlying wall corresponds to a mono-dermal teratoma with unidirectional neu-rogenic diff e rentiation {894}. Similarly,endodermal variants of mature teratomalined exclusively by respiratory epitheli-um {508} and ovarian epidermoid cysts{823} may fall into the category of mono-dermal teratoma. Mucinous cystadenomas arising withinmature teratomas have a homozygousteratomatous genotype, supporting theirg e rm cell origin {1731}. Mesoderm a lderived tumours such as lipoma com-posed of mature adipocytes with scat-tered benign sweat glands may occur{961}. Glomus tumour may rarely arisewithin a typical dermoid cyst {2682}.
175Germ cell tumours
Fig. 2.109 Ependymoma of the ovary. A The tumour cells have uniform nuclei and form two rosettes. B Manytumour cells are strongly positive for glial fibrillary acidic protein with accentuated staining around therosettes.
A
B
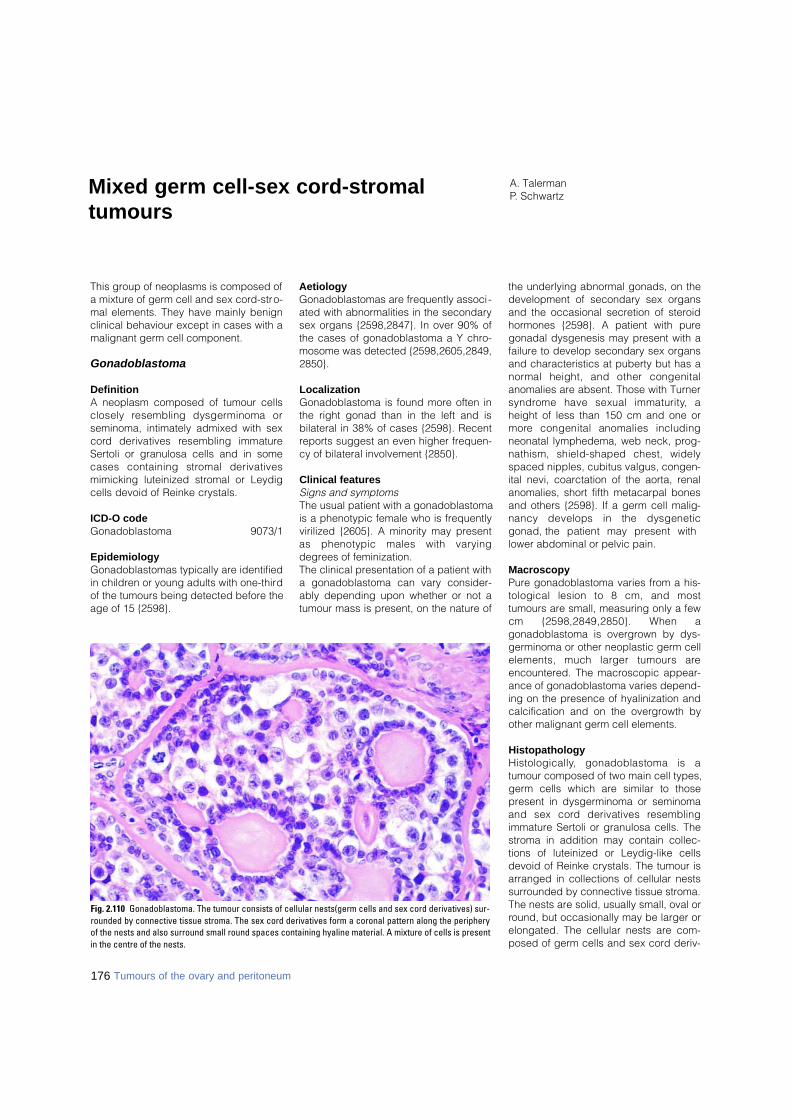
176 Tumours of the ovary and peritoneum
This group of neoplasms is composed ofa mixture of germ cell and sex cord-stro-mal elements. They have mainly benignclinical behaviour except in cases with amalignant germ cell component.
Gonadoblastoma
DefinitionA neoplasm composed of tumour cellsclosely resembling dysgerminoma orseminoma, intimately admixed with sexc o rd derivatives resembling immatureSertoli or granulosa cells and in somecases containing stromal derivativesmimicking luteinized stromal or Leydigcells devoid of Reinke crystals.
ICD-O codeGonadoblastoma 9073/1
EpidemiologyGonadoblastomas typically are identifiedin children or young adults with one-thirdof the tumours being detected before theage of 15 {2598}.
AetiologyGonadoblastomas are frequently associ-ated with abnormalities in the secondarysex organs {2598,2847}. In over 90% ofthe cases of gonadoblastoma a Y chro-mosome was detected {2598,2605,2849,2850}.
LocalizationGonadoblastoma is found more often inthe right gonad than in the left and isbilateral in 38% of cases {2598}. Recentreports suggest an even higher frequen-cy of bilateral involvement {2850}.
Clinical featuresSigns and symptoms The usual patient with a gonadoblastomais a phenotypic female who is frequentlyvirilized {2605}. A minority may presentas phenotypic males with vary i n gdegrees of feminization. The clinical presentation of a patient witha gonadoblastoma can vary consider-ably depending upon whether or not atumour mass is present, on the nature of
the underlying abnormal gonads, on thedevelopment of secondary sex organsand the occasional secretion of steroidhormones {2598}. A patient with puregonadal dysgenesis may present with afailure to develop secondary sex organsand characteristics at puberty but has an o rmal height, and other congenitalanomalies are absent. Those with Turners y n d rome have sexual immaturity, aheight of less than 150 cm and one orm o re congenital anomalies includingneonatal lymphedema, web neck, prog-nathism, shield-shaped chest, widelyspaced nipples, cubitus valgus, congen-ital nevi, coarctation of the aorta, renalanomalies, short fifth metacarpal bonesand others {2598}. If a germ cell malig-nancy develops in the dysgeneticgonad, the patient may present withlower abdominal or pelvic pain.
MacroscopyPure gonadoblastoma varies from a his-tological lesion to 8 cm, and mosttumours are small, measuring only a fewcm {2598,2849,2850}. When agonadoblastoma is overgrown by dys-germinoma or other neoplastic germ cellelements, much larger tumours areencountered. The macroscopic appear-ance of gonadoblastoma varies depend-ing on the presence of hyalinization andcalcification and on the overgrowth byother malignant germ cell elements.
HistopathologyH i s t o l o g i c a l l y, gonadoblastoma is atumour composed of two main cell types,germ cells which are similar to thosepresent in dysgerminoma or seminomaand sex cord derivatives re s e m b l i n gimmature Sertoli or granulosa cells. Thestroma in addition may contain collec-tions of luteinized or Leydig-like cellsdevoid of Reinke crystals. The tumour isarranged in collections of cellular nestssurrounded by connective tissue stroma.The nests are solid, usually small, oval orround, but occasionally may be larger orelongated. The cellular nests are com-posed of germ cells and sex cord deriv-
A. TalermanP. SchwartzMixed germ cell-sex cord-stromal
tumours
Fig. 2.110 Gonadoblastoma. The tumour consists of cellular nests(germ cells and sex cord derivatives) sur-rounded by connective tissue stroma. The sex cord derivatives form a coronal pattern along the peripheryof the nests and also surround small round spaces containing hyaline material. A mixture of cells is presentin the centre of the nests.

177Mixed germ cell-sex cord-stromal tumours
atives intimately admixed. The germ cellsare large and round with clear or slightlygranular cytoplasm and large, ro u n d ,vesicular nuclei, often with pro m i n e n tnucleoli, and show mitotic activity, whichmay be brisk. Their histological and ultra-structural appearance and histochemicalreactions are similar to the germ cells ofdysgerminoma or seminoma. The imma-ture Sertoli or granulosa cells are smallerand epithelial-like. These cells are roundor oval and contain dark, oval or slightlyelongated carrot-shaped nuclei. They donot show mitotic activity {2598,2849,2850}. The sex cord derivatives arearranged within the cell nests in threetypical patterns as follows:(1) Forming a coronal pattern along theperiphery of the nests.(2) Surrounding individual or collectionsof germ cells.(3) Surrounding small round spaces con-taining amorphous, hyaline, eosinophilic,PAS-positive material resembling Call-Exner bodies.The connective tissue stroma surround-ing the cellular nests may be scant orabundant and cellular, resembling ovari-an stroma, or dense and hyalinized. Itmay contain luteinized or Leydig-likecells devoid of Reinke crystals {2598,2849,2850}.Three processes, hyalinization, calcifica-tion and overgrowth by a malignant germcell element, usually dysgerm i n o m a ,may alter the basic histological appear-ance of gonadoblastoma. The hyaliniza-tion occurs by coalescence of the hya-line bodies and bands of hyaline materi-al around the nests with replacement ofthe cellular contents. Calcification origi-nates in the hyaline Call-Exner-like bod-ies and is seen histologically in morethan 80% of cases {2598}. It tends toreplace the hyalinized nests form i n grounded, calcified concretions. Coa-lescence of such concretions may leadto the calcification of the whole lesion,and the presence of smooth, rounded,calcified bodies may be the only evi-dence that gonadoblastoma has beenpresent. The term "burned-out gonado-blastoma" has been applied to suchlesions {2598,2849,2850}. Gonadoblas-toma is overgrown by dysgerminoma inapproximately 50% of cases, and in anadditional 10% another malignant germcell element is present {2598,2846,2849,2850}. Gonadoblastoma has neverbeen observed in metastatic lesions or
outside the gonads {2598,2849,2850}. In most cases the gonad of origin is inde-terminate because it is overgrown by thetumour. When the nature of the gonadcan be identified, it is usually a streak ora testis. The contralateral gonad, whenidentifiable, may be either a streak or atestis, and the latter is more likely to har-bour a gonadoblastoma {2598,2849,2850}. Occasionally, gonadoblastomamay be found in otherwise norm a lovaries {2077,2598,2849,2850}.
Tumour spread and stagingAt the time of operation gonadoblas-tomas typically are bilateral, although attimes they may be not macroscopicallydetectible in the gonad. Those that areovergrown by dysgerminoma or othermalignant germ cell tumour may bemuch larger. If a malignant germ celltumour develops, the potential formetastatic disease exists. Dysgerm i-nomas typically spread by the lymphaticroute, less frequently by peritoneal dis-semination. There f o re, it is extre m e l yi m p o rtant not only to remove bothgonads but to perform surgical staging ifat the time of operative consultation amalignant germ cell tumour is identified.The typical staging for a dysgerminomaor other malignant germ cell tumourincludes pelvic and para-aortic lymphnode sampling as well as peritonealwashings if no ascites is present {2586}.
The operation should include omentecto-my, and multiple peritoneal samplingsare required. For patients with spread ofa malignant germ cell tumour other thand y s g e rminoma, aggressive cytore d u c-tion surgery is appropriate {2586}.
Precursor lesionsGonadoblastoma is almost invariablyassociated with an underlying gonadaldisorder. When the disorder is identifi-able, it is usually pure or mixed gonadaldysgenesis with a Y chromosome beingdetected in over 90% of the cases {2598,2605}.
Prognosis and predictive factorsClinical criteriaPatients having gonadoblastoma withoutdysgerminoma or other germ cell tumourare treated by surgical excision of thegonads without additional therapy.However, if dysgerminoma and/or anoth-er malignant germ cell element is pres-ent, surgical staging and postoperativecombination chemotherapy, the mostpopular current regimen beingbleomycin, etoposide and cisplatin(BEP), are re q u i red. Other re g i m e n sinclude etoposide and carboplatin{2586}. Dysgerminoma is exquisitelysensitive to chemotherapy, as it was pre-viously shown to be exquisitely respon-sive to radiation therapy.
Fig. 2.111 Dysgerminoma with “burnt out” gonadoblastoma. The typical pattern of a dysgerminoma consistsof aggegates of primitive germ cells separated by fibrous septa infiltrated by lymphocytes. The presence of“burnt out” gonadoblastoma is indicated by smooth, rounded, calcified bodies.

178 Tumours of the ovary and peritoneum
Histopathological criteriaPure gonadoblastoma may show exten-sive involvement of the gonad but doesnot behave as a malignant lesion {2598,2849,2850}. More frequently, its germcell component gives rise to a malignantgerm cell neoplasm capable of invasionand metastases. Gonadoblastoma maysometimes undergo ablation by aprocess of marked hyalinization and cal-cification. In such cases the lesionbecomes innocuous, but great care mustbe taken to exclude the presence ofviable elements, especially of germ celllineage. D y s g e rminoma arising withingonadoblastoma tends to metastasizeless frequently and at a later stage thandysgerminoma arising de novo {2598,2849,2850}. There is no satisfactoryexplanation for this phenomenon. Thepatients can be treated similarly topatients with pure dysgerminoma with avery high likelihood of complete cure.
Mixed germ cell-sex cord-stromaltumour
DefinitionA neoplasm composed of intimatelyadmixed germ cells and sex cord deriv-atives that has a different histologicalappearance from gonadoblastoma.Mixed germ cell-sex cord-stromal tumouralso differs from gonadoblastoma by itsoccurrence in anatomically, phenotypi-cally and genetically normal females{2844,2845,2847}.
EpidemiologyMixed germ cell-sex cord - s t ro m a ltumours usually occur in infants or chil-dren under the age of 10, but have beenoccasionally reported in postmenarchalwomen {1556,2844,2852}.
AetiologyPatients with mixed germ cell-sex cord-s t romal tumour have normal gonadaldevelopment and a normal XX kary-otype. The tumour is not associated withgonadal dysgenesis, and its aetiology isunknown {1556,2844,2852,3270}.
Clinical featuresPatients with a mixed germ cell-sex cord-stromal tumour generally present withlower abdominal pain. In almost a fourthof the cases patients have isosexualpseudoprecocity and may have vaginalbleeding and bilateral breast develop-ment {1556,2852,3270}. Physical exami-nation routinely reveals a large mass inthe adnexal area or in the lowerabdomen.
MacroscopyThis tumour, unlike gonadoblastoma,tends to be relatively large, measuring7.5-18 cm and weighing 100-1,050grams. Except for two reported cases,mixed germ cell-sex cord-stromal tumouris unilateral {1321,2849,2850}. Thetumour is usually round or oval and issurrounded by a smooth, grey or grey-yellow capsule. In most cases it is solid,but in some cases it may be partly cystic.The sectioned surface is grey-pink or yel-low to pale brown. There is no evidenceof calcification. In all cases the fallopiantube, the uterus and the external geni-talia are normal
Tumour spread and stagingSince mixed germ cell-sex cord-stromaltumours are less aggressive thangonadoblastoma and uncommonly bilat-eral, the routine evaluation of patientswith a mixed germ cell-sex cord-stromaltumour can be less extensive. Althoughthe tumours are often of considerable
size, metastases have occurred in onlytwo cases {124,1556}. If intraoperativeconsultation is inconclusive, it is appro-priate to limit the operation to removal ofthe involved gonad and to await the finalpathology results before performing anydefinitive surgery that might impair futurefertility.
HistopathologyMixed germ cell-sex cord-stromal tumouris composed of germ cells and sex cordderivatives resembling immature Sertolior granulosa cells intimately admixedwith each other. The tumour cells formfour distinctive histological patterns asfollows:(1). A cord-like or trabecular patterncomposed of long, narro w, ramifyingc o rds or trabeculae that in placesexpand to form wider columns and larg-er round cellular aggregates surroundedby connective tissue stroma that variesfrom dense and hyalinized to loose andoedematous.(2). A tubular pattern composed of solidtubules surrounded by fine connectivetissue septa and containing peripherallylocated smaller epithelial-like sex cordderivatives surrounding large, ro u n dgerm cells with clear or slightly granularcytoplasm and large vesicular nucleicontaining prominent nucleoli.(3). A haphazard pattern consisting ofscattered collections of germ cells sur-rounded by sex cord derivatives, whichmay be very abundant.(4). A mixed pattern showing an admix-ture of the three above mentioned pat-terns without any predominance.The germ cells show mitotic activity anda close similarity to those of dysgermino-ma, but in some cases they are better dif-ferentiated showing smaller nuclei andless marked mitotic activity. Unlike the
B CAFig. 2.112 Mixed germ cell-sex cord-stromal tumour. A The sectioned surface shows a lobulated, pale yellow tumour. B The tumour is composed of an admixtureof smaller sex cord cells and larger germ cells with clear cytoplasm forming cords and trabeculae surrounded by loose oedematous connective tissue. C Small car-rot-shaped sex cord cells are admixed with large pale germ cells in a haphazard fashion. .
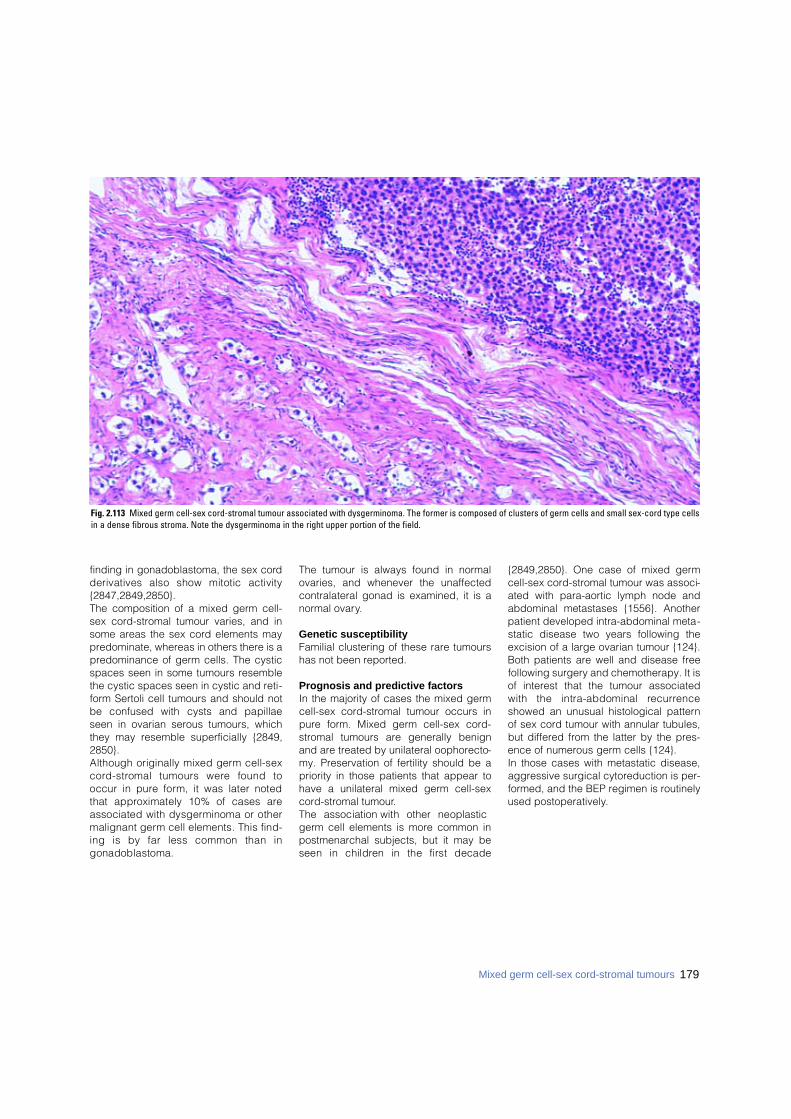
179Mixed germ cell-sex cord-stromal tumours
finding in gonadoblastoma, the sex cordderivatives also show mitotic activity{2847,2849,2850}. The composition of a mixed germ cell-sex cord-stromal tumour varies, and insome areas the sex cord elements maypredominate, whereas in others there is apredominance of germ cells. The cysticspaces seen in some tumours resemblethe cystic spaces seen in cystic and reti-form Sertoli cell tumours and should notbe confused with cysts and papillaeseen in ovarian serous tumours, whichthey may resemble superficially {2849,2850}. Although originally mixed germ cell-sexc o rd - s t romal tumours were found tooccur in pure form, it was later notedthat approximately 10% of cases areassociated with dysgerminoma or othermalignant germ cell elements. This find-ing is by far less common than ingonadoblastoma.
The tumour is always found in normalovaries, and whenever the unaffectedcontralateral gonad is examined, it is anormal ovary.
Genetic susceptibilityFamilial clustering of these rare tumourshas not been reported.
Prognosis and predictive factorsIn the majority of cases the mixed germcell-sex cord-stromal tumour occurs inpure form. Mixed germ cell-sex cord-stromal tumours are generally benignand are treated by unilateral oophorecto-my. Preservation of fertility should be apriority in those patients that appear tohave a unilateral mixed germ cell-sexcord-stromal tumour.The association with other neoplasticgerm cell elements is more common inpostmenarchal subjects, but it may beseen in children in the first decade
{2849,2850}. One case of mixed germcell-sex cord-stromal tumour was associ-ated with para-aortic lymph node andabdominal metastases {1556}. Anotherpatient developed intra-abdominal meta-static disease two years following theexcision of a large ovarian tumour {124}.Both patients are well and disease freefollowing surgery and chemotherapy. It isof interest that the tumour associatedwith the intra-abdominal re c u r re n c eshowed an unusual histological patternof sex cord tumour with annular tubules,but differed from the latter by the pres-ence of numerous germ cells {124}. In those cases with metastatic disease,aggressive surgical cytoreduction is per-formed, and the BEP regimen is routinelyused postoperatively.
Fig. 2.113 Mixed germ cell-sex cord-stromal tumour associated with dysgerminoma. The former is composed of clusters of germ cells and small sex-cord type cellsin a dense fibrous stroma. Note the dysgerminoma in the right upper portion of the field.
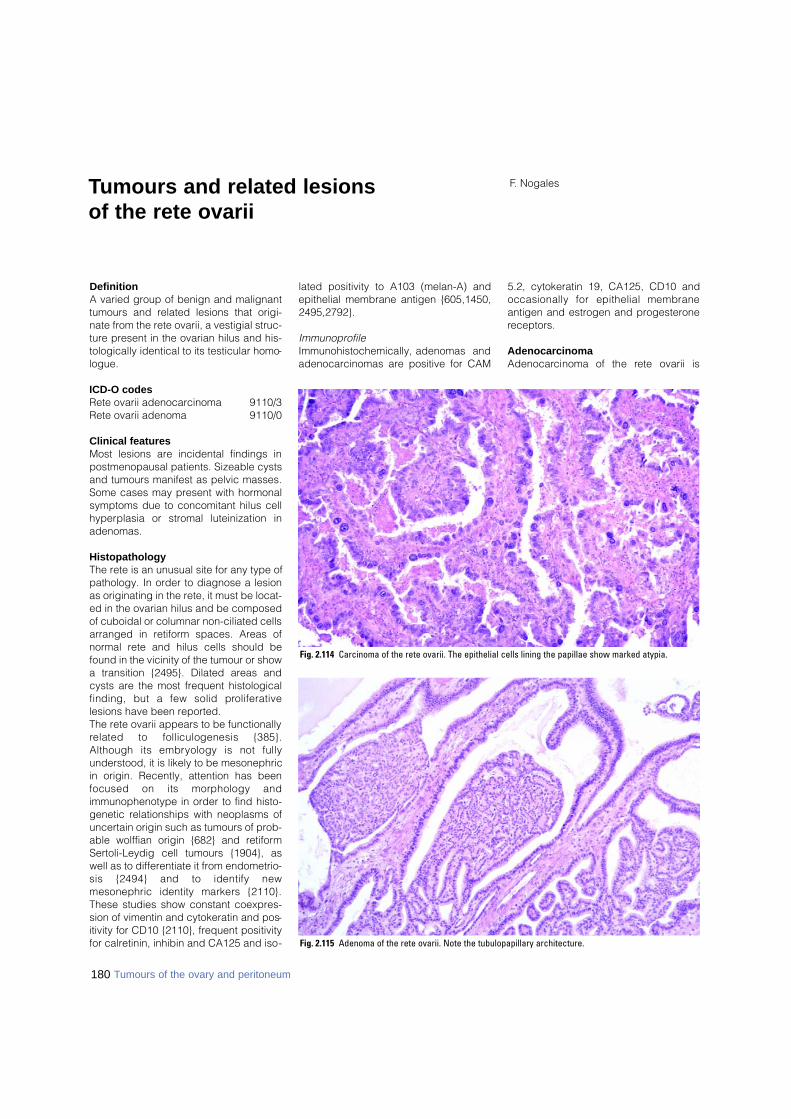
Definition A varied group of benign and malignanttumours and related lesions that origi-nate from the rete ovarii, a vestigial struc-ture present in the ovarian hilus and his-tologically identical to its testicular homo-logue.
ICD-O codesRete ovarii adenocarcinoma 9110/3Rete ovarii adenoma 9110/0
Clinical features Most lesions are incidental findings inpostmenopausal patients. Sizeable cystsand tumours manifest as pelvic masses.Some cases may present with hormonalsymptoms due to concomitant hilus cellhyperplasia or stromal luteinization inadenomas.
HistopathologyThe rete is an unusual site for any type ofpathology. In order to diagnose a lesionas originating in the rete, it must be locat-ed in the ovarian hilus and be composedof cuboidal or columnar non-ciliated cellsarranged in retiform spaces. Areas ofnormal rete and hilus cells should befound in the vicinity of the tumour or showa transition {2495}. Dilated areas andcysts are the most frequent histologicalfinding, but a few solid pro l i f e r a t i v elesions have been reported.The rete ovarii appears to be functionallyrelated to folliculogenesis {385}.Although its embryology is not fullyunderstood, it is likely to be mesonephricin origin. Recently, attention has beenfocused on its morphology andimmunophenotype in order to find histo-genetic relationships with neoplasms ofuncertain origin such as tumours of prob-able wolffian origin {682} and retiformSertoli-Leydig cell tumours {1904}, aswell as to differentiate it from endometrio-sis {2494} and to identify newmesonephric identity markers {2110}.These studies show constant coexpres-sion of vimentin and cytokeratin and pos-itivity for CD10 {2110}, frequent positivityfor calretinin, inhibin and CA125 and iso-
lated positivity to A103 (melan-A) andepithelial membrane antigen {605,1450,2495,2792}.
ImmunoprofileImmunohistochemically, adenomas andadenocarcinomas are positive for CAM
5.2, cytokeratin 19, CA125, CD10 andoccasionally for epithelial membraneantigen and estrogen and progesteronereceptors.
AdenocarcinomaA d e n o c a rcinoma of the rete ovarii is
F. NogalesTumours and related lesions of the rete ovarii
Fig. 2.114 Carcinoma of the rete ovarii. The epithelial cells lining the papillae show marked atypia.
180 Tumours of the ovary and peritoneum
Fig. 2.115 Adenoma of the rete ovarii. Note the tubulopapillary architecture.
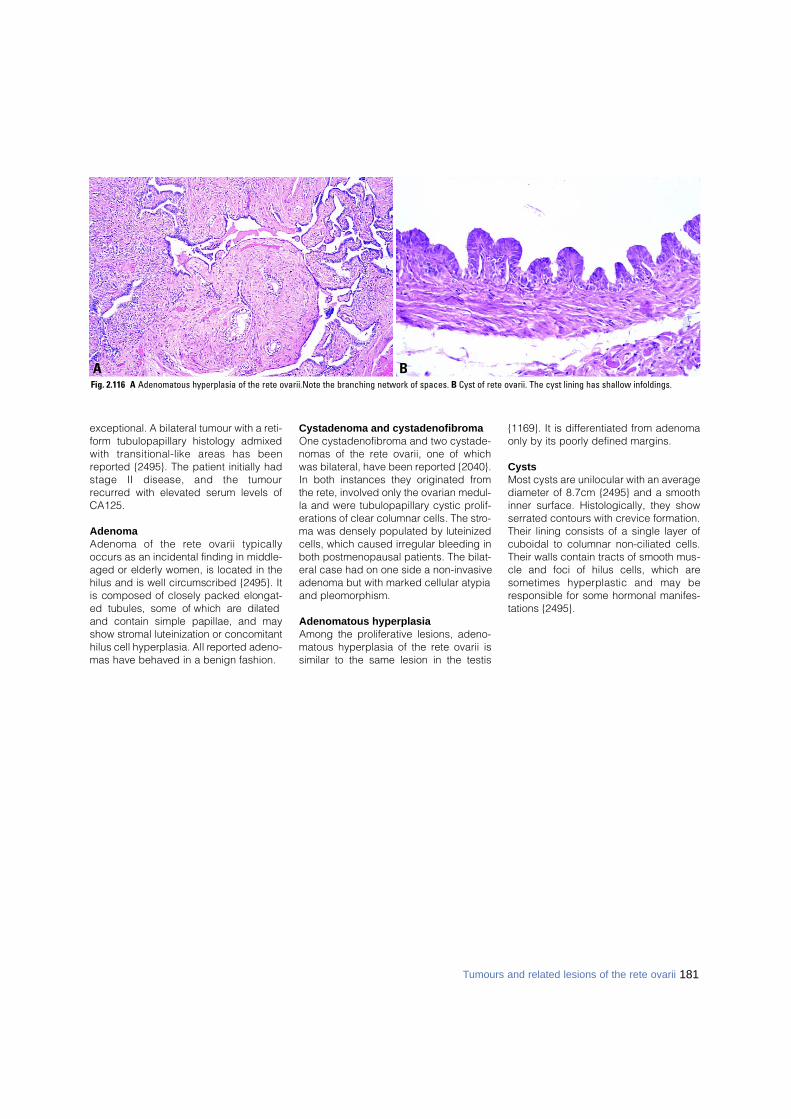
181Tumours and related lesions of the rete ovarii
exceptional. A bilateral tumour with a reti-form tubulopapillary histology admixedwith transitional-like areas has beenreported {2495}. The patient initially hadstage II disease, and the tumourrecurred with elevated serum levels ofCA125.
AdenomaAdenoma of the rete ovarii typicallyoccurs as an incidental finding in middle-aged or elderly women, is located in thehilus and is well circumscribed {2495}. Itis composed of closely packed elongat-ed tubules, some of which are dilatedand contain simple papillae, and mayshow stromal luteinization or concomitanthilus cell hyperplasia. All re p o rted adeno-mas have behaved in a benign fashion.
Cystadenoma and cystadenofibromaOne cystadenofibroma and two cystade-nomas of the rete ovarii, one of whichwas bilateral, have been reported {2040}.In both instances they originated fromthe rete, involved only the ovarian medul-la and were tubulopapillary cystic prolif-erations of clear columnar cells. The stro-ma was densely populated by luteinizedcells, which caused irregular bleeding inboth postmenopausal patients. The bilat-eral case had on one side a non-invasiveadenoma but with marked cellular atypiaand pleomorphism.
Adenomatous hyperplasiaAmong the proliferative lesions, adeno-matous hyperplasia of the rete ovarii issimilar to the same lesion in the testis
{1169}. It is differentiated from adenomaonly by its poorly defined margins.
CystsMost cysts are unilocular with an averagediameter of 8.7cm {2495} and a smoothinner surface. Histologically, they showserrated contours with crevice formation.Their lining consists of a single layer ofcuboidal to columnar non-ciliated cells.Their walls contain tracts of smooth mus-cle and foci of hilus cells, which aresometimes hyperplastic and may beresponsible for some hormonal manifes-tations {2495}.
BAFig. 2.116 A Adenomatous hyperplasia of the rete ovarii.Note the branching network of spaces. B Cyst of rete ovarii. The cyst lining has shallow infoldings.
D e f i n i t i o nA group of benign and malignant ovariantumours of diverse or uncertain origin.
ICD-O codes Small cell carcinoma,
hypercalcaemic type 8041/3Small cell carcinoma,
pulmonary type 8041/3Large cell neuroendocrine
carcinoma 8013/3Adenoid cystic carcinoma 8200/3Basal cell tumour 8090/1Hepatoid carcinoma 8576/3Malignant mesothelioma 9050/3Gestational choriocarcinoma 9100/3Hydatidiform mole 9100/0Ovarian wolffian tumour 9110/1Wilms tumour 8960/3Paraganglioma 8693/1Myxoma 8840/0
Small cell carcinoma, hypercalcaemic type
D e f i n i t i o nAn undiff e rentiated carcinoma that is usu-ally associated with paraendocrine hyper-calcaemia and is composed primarily ofsmall cells.
Clinical featuresThis neoplasm typically occurs in youngwomen and is associated with paraen-docrine hypercalcaemia in appro x i m a t e l yt w o - t h i rds of patients {3204}. Most of thepatients presented with abdominalswelling or pain related to their tumour;h o w e v e r, one patient had a neck explo-ration for presumed parathyroid diseasewith negative results before the ovariantumour was discovered {3204}.
M a c r o s c o p yThe tumours are usually large and pre-dominantly solid, pale white to gray mass-es. Necrosis, haemorrhage and cysticdegeneration are common.
Tumour spread and staging In approximately 50% of the patients the
tumour has spread beyond the ovary atthe time of initial laporatomy.
Histopathology On histological examination the tumourstypically grow diff u s e l y, but they may formsmall islands, trabeculae or cords. Theyf requently form follicle-like spaces thatalmost always contain eosinophilic fluid,and nuclei show easily discernible nucle-oli. Foci of either benign or malignantmucinous epithelium are present in 10-15% of the cases. Ty p i c a l l y, the cells ofthe tumour contain scant cytoplasm, butin approximately one-half of cases a com-ponent of large cells with abundanteosinophilic cytoplasm and nuclei con-taining prominent nucleoli is present.
I m m u n o p ro f i l eSmall cell carcinomas generally stain forepithelial membrane antigen but not forinhibin {2376}. Variable staining of theneoplastic cells for vimentin, cytokeratin
and epithelial membrane antigen isobserved {46}.
Cytometric studies Flow cytometric studies of paraff i n -embedded tissue has demonstrated thatthe neoplastic cells are diploid {755}.
Electron microscopyE l e c t ron microscopic examination hasshown an epithelial appearance to theneoplasm consisting of small desmo-somes and, in some cases, tight junctions{695}. Dilated granular endoplasmic re t i c-ulum containing amorphous material ischaracteristically present within the cyto-plasm {695,696}. Few or no neuro s e c re t o-ry granules have been identified.
D i ff e rential diagnosisBecause of the young age of the patientsand the presence of follicle-like spaces inthe neoplasm, the diff e rential diagnosisincludes juvenile granulosa cell tumour.
182 Tumours of the ovary and peritoneum
L.M. RothA. TsuburaM. DietelH. Senzaki
Miscellaneous tumours and tumour-likeconditions of the ovary
Table 2.08Comparison of small cell carcinoma of the hypercalcaemic type with juvenile granulosa cell tumour.
Small cell carcinoma, hypercalcaemic type Juvenile granulosa cell tumour
Stage I in 50% of cases Stage I in greater than 97% of cases
Highly malignant Usually non-aggressive
Hypercalcaemia in two-thirds of cases Hypercalcaemia absent
Never estrogenic Usually estrogenic
Scant or non-specific stroma Fibrothecomatous stroma common
Follicles often contain mucicarminophilic Follicles rarely contain mucicarminophilic basophilic secretion basophilic secretion
Nuclei hyperchromatic Rounded euchromatic nuclei,
Prominent nucleoli Indistinct nucleoli
Mitoses frequent Mitoses variable
Usually epithelial membrane antigen positive Epithelial membrane antigen negative
Alpha-inhibin negative Alpha-inhibin positive
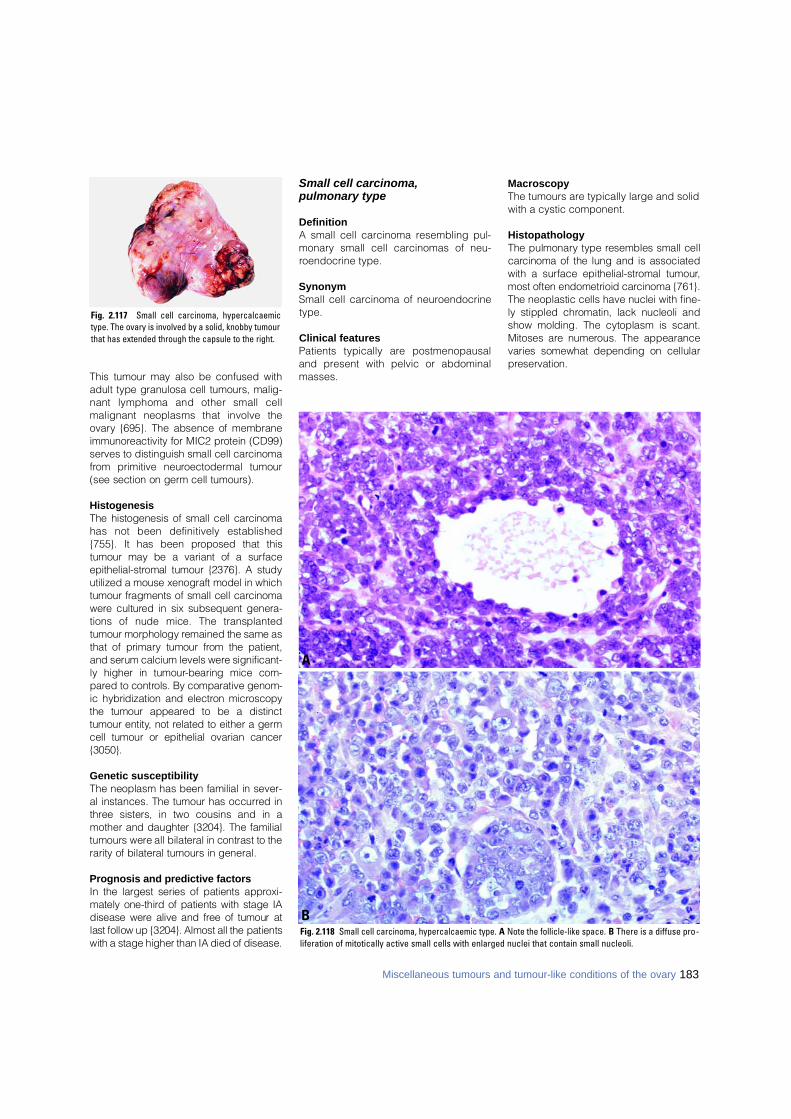
This tumour may also be confused withadult type granulosa cell tumours, malig-nant lymphoma and other small cellmalignant neoplasms that involve theo v a ry {695}. The absence of membranei m m u n o reactivity for MIC2 protein (CD99)serves to distinguish small cell carc i n o m af rom primitive neuro e c t o d e rmal tumour(see section on germ cell tumours).
H i s t o g e n e s i sThe histogenesis of small cell carc i n o m ahas not been definitively established{755}. It has been proposed that thistumour may be a variant of a surf a c ee p i t h e l i a l - s t romal tumour {2376}. A studyutilized a mouse xenograft model in whichtumour fragments of small cell carc i n o m aw e re cultured in six subsequent genera-tions of nude mice. The transplantedtumour morphology remained the same asthat of primary tumour from the patient,and serum calcium levels were significant-ly higher in tumour-bearing mice com-p a red to controls. By comparative genom-ic hybridization and electron micro s c o p ythe tumour appeared to be a distincttumour entity, not related to either a germcell tumour or epithelial ovarian cancer{3050}.
Genetic susceptibilityThe neoplasm has been familial in sever-al instances. The tumour has occurred int h ree sisters, in two cousins and in amother and daughter {3204}. The familialtumours were all bilateral in contrast to therarity of bilateral tumours in general.
Prognosis and predictive factorsIn the largest series of patients appro x i-mately one-third of patients with stage IAdisease were alive and free of tumour atlast follow up {3204}. Almost all the patientswith a stage higher than IA died of disease.
Small cell carcinoma, pulmonary type
DefinitionA small cell carcinoma resembling pul-monary small cell carcinomas of neu-roendocrine type.
SynonymSmall cell carcinoma of neuroendocrinetype.
Clinical features Patients typically are postmenopausaland present with pelvic or abdominalmasses.
MacroscopyThe tumours are typically large and solidwith a cystic component.
HistopathologyThe pulmonary type resembles small cellc a rcinoma of the lung and is associatedwith a surface epithelial-stromal tumour,most often endometrioid carcinoma {761}.The neoplastic cells have nuclei with fine-ly stippled chromatin, lack nucleoli andshow molding. The cytoplasm is scant.Mitoses are numerous. The appearancevaries somewhat depending on cellularp reservation.
Fig. 2.117 Small cell carcinoma, hypercalcaemictype. The ovary is involved by a solid, knobby tumourthat has extended through the capsule to the right.
Fig. 2.118 Small cell carcinoma, hypercalcaemic type. A Note the follicle-like space. B There is a diffuse pro-liferation of mitotically active small cells with enlarged nuclei that contain small nucleoli.
A
B
183Miscellaneous tumours and tumour-like conditions of the ovary
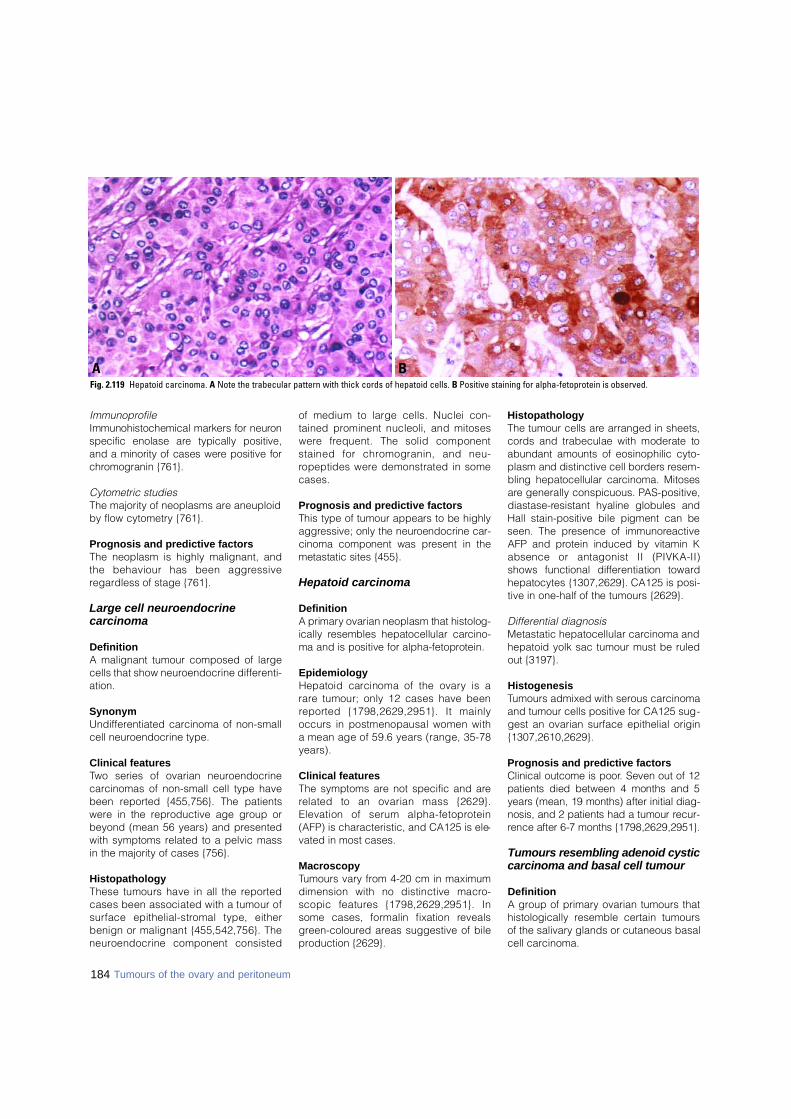
184 Tumours of the ovary and peritoneum
ImmunoprofileImmunohistochemical markers for neuro nspecific enolase are typically positive,and a minority of cases were positive forc h romogranin {761}.
Cytometric studiesThe majority of neoplasms are aneuploidby flow cytometry {761}.
Prognosis and predictive factorsThe neoplasm is highly malignant, andthe behaviour has been aggre s s i v eregardless of stage {761}.
Large cell neuroendocrine carcinoma
DefinitionA malignant tumour composed of largecells that show neuroendocrine differenti-ation.
SynonymUndifferentiated carcinoma of non-smallcell neuroendocrine type.
Clinical featuresTwo series of ovarian neuroendocrinecarcinomas of non-small cell type havebeen reported {455,756}. The patientswere in the reproductive age group orbeyond (mean 56 years) and presentedwith symptoms related to a pelvic massin the majority of cases {756}.
Histopathology These tumours have in all the re p o rt e dcases been associated with a tumour ofs u rface epithelial-stromal type, eitherbenign or malignant {455,542,756}. Then e u roendocrine component consisted
of medium to large cells. Nuclei con-tained prominent nucleoli, and mitosesw e re frequent. The solid componentstained for chromogranin, and neu-ropeptides were demonstrated in somecases.
Prognosis and predictive factors This type of tumour appears to be highlya g g ressive; only the neuroendocrine car-cinoma component was present in themetastatic sites {455}.
Hepatoid carcinoma
DefinitionA primary ovarian neoplasm that histolog-ically resembles hepatocellular carc i n o-ma and is positive for alpha-fetoprotein.
EpidemiologyHepatoid carcinoma of the ovary is ar a re tumour; only 12 cases have beenre p o rted {1798,2629,2951}. It mainlyoccurs in postmenopausal women witha mean age of 59.6 years (range, 35-78years).
Clinical features The symptoms are not specific and arerelated to an ovarian mass {2629}.Elevation of serum alpha-fetopro t e i n(AFP) is characteristic, and CA125 is ele-vated in most cases.
MacroscopyTumours vary from 4-20 cm in maximumdimension with no distinctive macro-scopic features {1798,2629,2951}. Insome cases, formalin fixation re v e a l sgreen-coloured areas suggestive of bileproduction {2629}.
HistopathologyThe tumour cells are arranged in sheets,c o rds and trabeculae with moderate toabundant amounts of eosinophilic cyto-plasm and distinctive cell borders re s e m-bling hepatocellular carcinoma. Mitosesa re generally conspicuous. PA S - p o s i t i v e ,d i a s t a s e - resistant hyaline globules andHall stain-positive bile pigment can beseen. The presence of immunore a c t i v eAFP and protein induced by vitamin Kabsence or antagonist II (PIVKA-II)shows functional diff e rentiation towardhepatocytes {1307,2629}. CA125 is posi-tive in one-half of the tumours {2629}.
Differential diagnosisMetastatic hepatocellular carcinoma andhepatoid yolk sac tumour must be ruledout {3197}.
HistogenesisTumours admixed with serous carcinomaand tumour cells positive for CA125 sug-gest an ovarian surface epithelial origin{1307,2610,2629}.
Prognosis and predictive factorsClinical outcome is poor. Seven out of 12patients died between 4 months and 5years (mean, 19 months) after initial diag-nosis, and 2 patients had a tumour re c u r-rence after 6-7 months {1798,2629,2 9 5 1 } .
Tumours resembling adenoid cysticcarcinoma and basal cell tumour
DefinitionA group of primary ovarian tumours thathistologically resemble certain tumoursof the salivary glands or cutaneous basalcell carcinoma.
BAFig. 2.119 Hepatoid carcinoma. A Note the trabecular pattern with thick cords of hepatoid cells. B Positive staining for alpha-fetoprotein is observed.
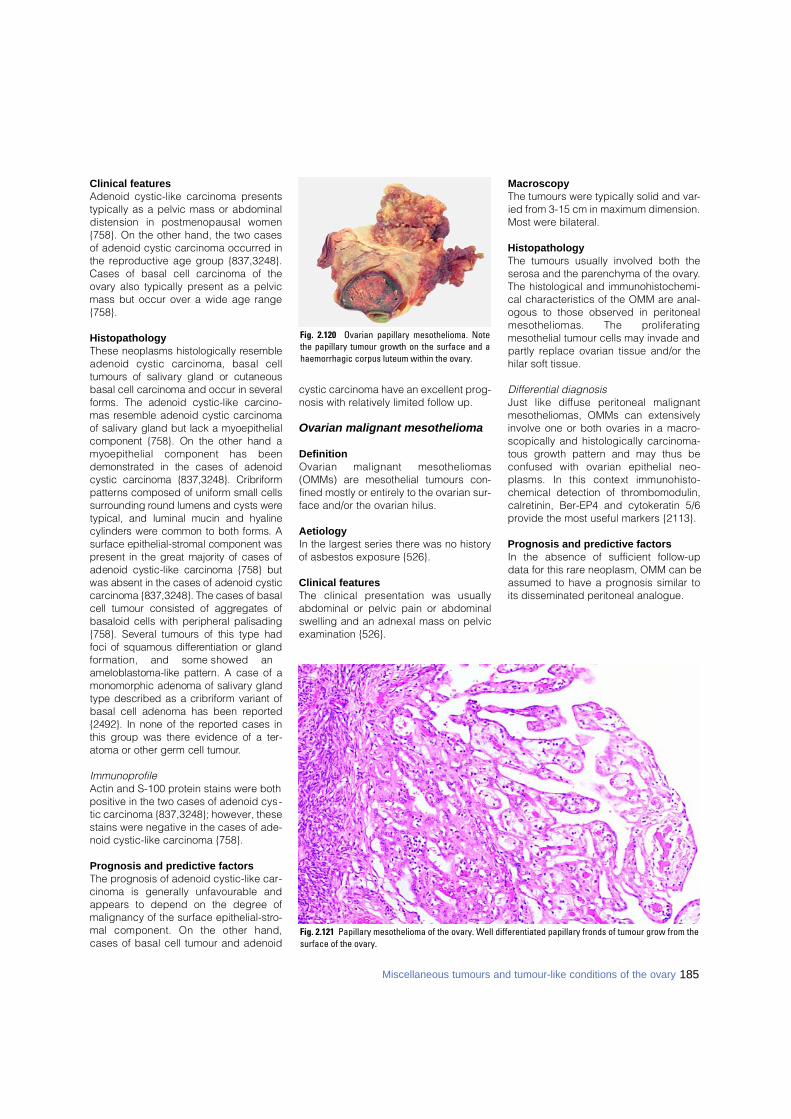
Clinical featuresAdenoid cystic-like carcinoma presentstypically as a pelvic mass or abdominaldistension in postmenopausal women{758}. On the other hand, the two casesof adenoid cystic carcinoma occurred inthe reproductive age group {837,3248}.Cases of basal cell carcinoma of theovary also typically present as a pelvicmass but occur over a wide age range{758}.
HistopathologyThese neoplasms histologically re s e m b l eadenoid cystic carcinoma, basal celltumours of salivary gland or cutaneousbasal cell carcinoma and occur in severalf o rms. The adenoid cystic-like carc i n o-mas resemble adenoid cystic carc i n o m aof salivary gland but lack a myoepithelialcomponent {758}. On the other hand amyoepithelial component has beendemonstrated in the cases of adenoidcystic carcinoma {837,3248}. Cribriformp a t t e rns composed of uniform small cellss u r rounding round lumens and cysts weretypical, and luminal mucin and hyalinecylinders were common to both forms. As u rface epithelial-stromal component wasp resent in the great majority of cases ofadenoid cystic-like carcinoma {758} butwas absent in the cases of adenoid cysticc a rcinoma {837,3248}. The cases of basalcell tumour consisted of aggregates ofbasaloid cells with peripheral palisading{758}. Several tumours of this type hadfoci of squamous diff e rentiation or glandf o rmation, and some showed anameloblastoma-like pattern. A case of amonomorphic adenoma of salivary glandtype described as a cribriform variant ofbasal cell adenoma has been re p o rt e d{2492}. In none of the re p o rted cases inthis group was there evidence of a ter-atoma or other germ cell tumour.
ImmunoprofileActin and S-100 protein stains were bothpositive in the two cases of adenoid cys-tic carcinoma {837,3248}; however, thesestains were negative in the cases of ade-noid cystic-like carcinoma {758}.
Prognosis and predictive factorsThe prognosis of adenoid cystic-like car-cinoma is generally unfavourable andappears to depend on the degree ofmalignancy of the surface epithelial-stro-mal component. On the other hand,cases of basal cell tumour and adenoid
cystic carcinoma have an excellent prog-nosis with relatively limited follow up.
Ovarian malignant mesothelioma
DefinitionOvarian malignant mesotheliomas(OMMs) are mesothelial tumours con-fined mostly or entirely to the ovarian sur-face and/or the ovarian hilus.
AetiologyIn the largest series there was no historyof asbestos exposure {526}.
Clinical featuresThe clinical presentation was usuallyabdominal or pelvic pain or abdominalswelling and an adnexal mass on pelvicexamination {526}.
MacroscopyThe tumours were typically solid and var-ied from 3-15 cm in maximum dimension.Most were bilateral.
Histopathology The tumours usually involved both theserosa and the parenchyma of the ovary.The histological and immunohistochemi-cal characteristics of the OMM are anal-ogous to those observed in peritonealmesotheliomas. The pro l i f e r a t i n gmesothelial tumour cells may invade andpartly replace ovarian tissue and/or thehilar soft tissue.
Differential diagnosisJust like diffuse peritoneal malignantmesotheliomas, OMMs can extensivelyinvolve one or both ovaries in a macro-scopically and histologically carcinoma-tous growth pattern and may thus beconfused with ovarian epithelial neo-plasms. In this context immunohisto-chemical detection of thrombomodulin,calretinin, Ber-EP4 and cytokeratin 5/6provide the most useful markers {2113}.
Prognosis and predictive factorsIn the absence of sufficient follow-updata for this rare neoplasm, OMM can beassumed to have a prognosis similar toits disseminated peritoneal analogue.
Fig. 2.120 Ovarian papillary mesothelioma. Notethe papillary tumour growth on the surface and ahaemorrhagic corpus luteum within the ovary.
Fig. 2.121 Papillary mesothelioma of the ovary. Well differentiated papillary fronds of tumour grow from thesurface of the ovary.
185Miscellaneous tumours and tumour-like conditions of the ovary
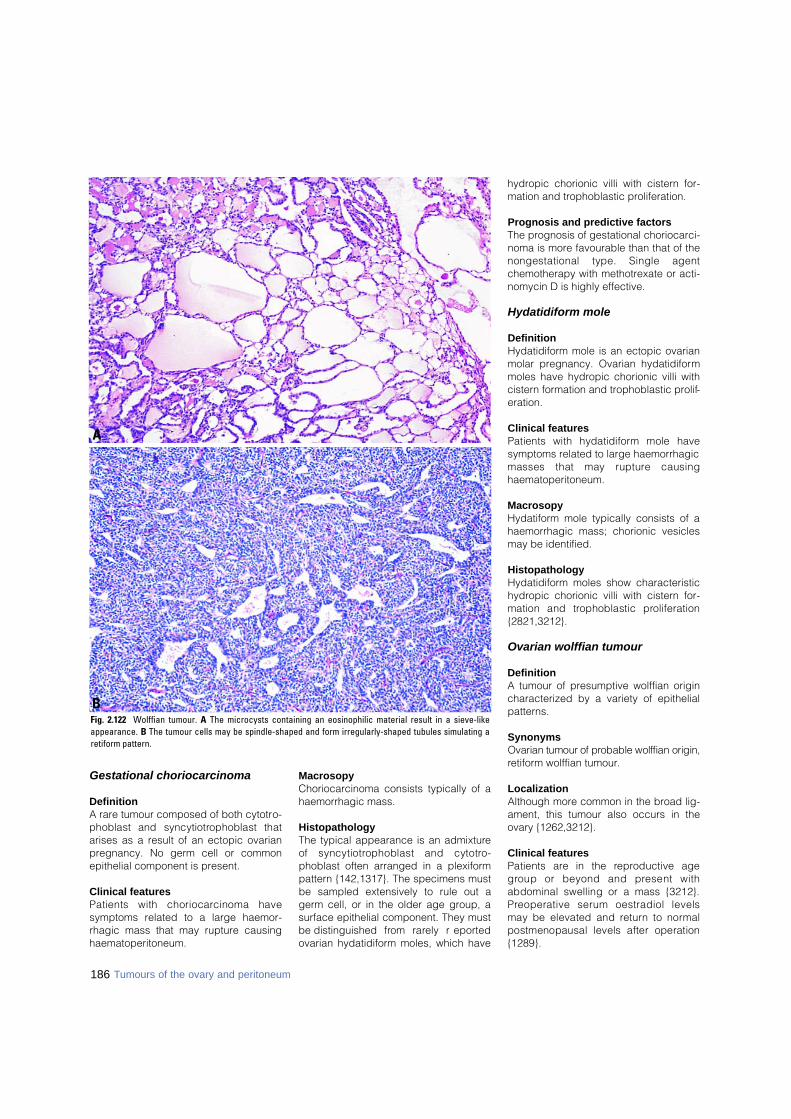
Gestational choriocarcinoma
DefinitionA rare tumour composed of both cytotro-phoblast and syncytiotrophoblast thatarises as a result of an ectopic ovarianpregnancy. No germ cell or commonepithelial component is present.
Clinical featuresPatients with choriocarcinoma havesymptoms related to a large haemor-rhagic mass that may rupture causinghaematoperitoneum.
MacrosopyChoriocarcinoma consists typically of ahaemorrhagic mass.
HistopathologyThe typical appearance is an admixtureof syncytiotrophoblast and cytotro-phoblast often arranged in a plexiformpattern {142,1317}. The specimens mustbe sampled extensively to rule out agerm cell, or in the older age group, asurface epithelial component. They mustbe distinguished from rarely re p o rt e dovarian hydatidiform moles, which have
hydropic chorionic villi with cistern for-mation and trophoblastic proliferation.
Prognosis and predictive factorsThe prognosis of gestational choriocarci-noma is more favourable than that of thenongestational type. Single agentchemotherapy with methotrexate or acti-nomycin D is highly effective.
Hydatidiform mole
DefinitionHydatidiform mole is an ectopic ovarianmolar pregnancy. Ovarian hydatidiformmoles have hydropic chorionic villi withcistern formation and trophoblastic prolif-eration.
Clinical featuresPatients with hydatidiform mole havesymptoms related to large haemorrhagicmasses that may rupture causinghaematoperitoneum.
MacrosopyHydatiform mole typically consists of ahaemorrhagic mass; chorionic vesiclesmay be identified.
HistopathologyHydatidiform moles show characteristichydropic chorionic villi with cistern for-mation and trophoblastic pro l i f e r a t i o n{2821,3212}.
Ovarian wolffian tumour
DefinitionA tumour of presumptive wolffian origincharacterized by a variety of epithelialpatterns.
SynonymsOvarian tumour of probable wolffian origin,retiform wolffian tumour.
LocalizationAlthough more common in the broad lig-ament, this tumour also occurs in theovary {1262,3212}.
Clinical featuresPatients are in the re p roductive ageg roup or beyond and present withabdominal swelling or a mass {3212}.P reoperative serum oestradiol levelsmay be elevated and re t u rn to norm a lpostmenopausal levels after operation{1289}.
186 Tumours of the ovary and peritoneum
Fig. 2.122 Wolffian tumour. A The microcysts containing an eosinophilic material result in a sieve-likeappearance. B The tumour cells may be spindle-shaped and form irregularly-shaped tubules simulating aretiform pattern.
A
B

HistopathologyThis epithelial tumour may show diffuse,solid tubular, hollow tubular and sieve-like patterns, and combinations of thevarious patterns may occur. Cases havebeen reported associated with endome-trial hyperplasia {1262,1289}.
Immunoprofile The neoplasms are positive for CAM5.2,cytokeratins 7 and 19 and vimentin buta re negative for cytokeratin 20,34betaE12, B72.3, carc i n o e m b ry o n i cantigen, and epithelial membrane antigen{2321,2878,2926}. The neoplastic cellsoften express CD10 {2110} and often areweakly positive for alpha-inhibin {1499}.
HistogenesisCases have been reported arising withinthe rete ovarii {662,2878}. An immunohis-tochemical study based on a compari-son with mesonephric remnants andparamesonephric structures supportedbut did not prove a mesonephric origin ofthese neoplasms {2926}.
Prognosis and predictive factorsThese tumours typically are not aggres-sive; however, a significant minority ofpatients have had an aggressive course{3212}. The malignant cases sometimes,but not always, show nuclear atypia andincreased mitotic activity.
Wilms tumour
DefinitionA primary ovarian neoplasm that has thetypical features of a Wilms tumour of thekidney.
EpidemiologySeveral cases of pure Wilms tumour of theo v a ry have been re p o rted {1303,2506}.
Clinical featuresThe tumour occurs in patients in the re p ro-ductive age group and beyond and pre s-ents as a rapidly growing adnexal mass.
HistopathologyThey have the typical appearance of aWilms tumour including small tubules,glomeruloid structures and blastema. Noteratomatous elements were identified.
Prognosis and predictive factorsTwo of the patients were living and well10 months and 7 years postoperatively.
Paraganglioma
DefinitionA unique neuroendocrine neoplasm,usually encapsulated and benign, arisingin specialized neural crest cells associat-ed with autonomic ganglia (paraganglia).
SynonymPhaeochromocytoma.
Clinical featuresA single case of a paraganglioma of theovary in a fifteen year old girl with hyper-tension has been reported {832}. In addi-tion two unpublished cases have beendescribed {2605}.
HistopathologyThe tumours consist of polygonal epithe-lioid cells arranged in nests separated bya fibrovascular stroma.
ImmunoprofileThe tumour is positive for chromogranin.In addition, stains for S-100 protein canidentify sustentacular cells {2605}.
BiochemistryEpinephrine and norepinephrine wereextracted from the tumour {832}.
Myxoma
DefinitionA benign mesenchymal tumour com-posed of cells with bland nuclear fea-t u res producing abundant basophilicintercellular ground substance.
Clinical featuresPatients with ovarian myxomas present inthe reproductive age group typically withan asymptomatic unilateral adnexalmass {757}.
MacrosocopyThe tumours are large, averaging 11 cmin diameter. The sectioned surface issoft, often with cystic degeneration.
HistopathologyMyxoma is a sharply demarcated tumourcomposed of spindle and stellate-shapedcells within an abundant, well vascular-ized myxoid background. Small foci ofnon-myxoid fibrous tissue or smooth mus-cle may be present. Lipoblasts are notidentified. Mitoses are rare. The interc e l-lular material stains with alcian blue and
colloidal iron. Staining is prevented byp re t reatment with hyaluronidase indicat-ing that the material is hyaluronic acid.
ImmunoprofileImmunohistochemical stains show thatthe tumours are positive for vimentin andsmooth muscle actin but negative formost other common immunohistochemi-cal markers {567}.
Electron microscopyUltrastructural features of thin filamentscondensed into dense bodies also supportthe presence of myofibroblasts {567}.
HistogenesisBased on an immunohistochemical com-parison with myxoid areas of ovarian stro-mal tumours, myxomas were considere dto be a variant of the thecoma-fibro m ag roup {3254}.
Prognosis and predictive factorsThe tumour is practically always benignalthough one case diagnosed originallyas myxoma had a late recurrence after19 years {2901}. In that case the originaltumour showed occasional mitotic fig-ures (less than 1 per ten high powerfields), slight atypia and occasional vac-uolated cells. The recurrent neoplasm,but not the original, was aneuploid byDNA-flow cytometry {2901}.
Malignant soft tissue tumours notspecific to the ovary
Pure soft tissue sarcomas of somatictype rarely occur as primary tumours ofthe ovary. They typically present as arapidly enlarging adnexal mass. Theirhistological appearance is similar to softtissue tumours in other locations. Amongthe reported cases of pure sarcomas are
Fig. 2.123 Luteoma of pregnancy. The sectionedsurface shows a nodular brown tumour.
187Miscellaneous tumours and tumour-like conditions of the ovary
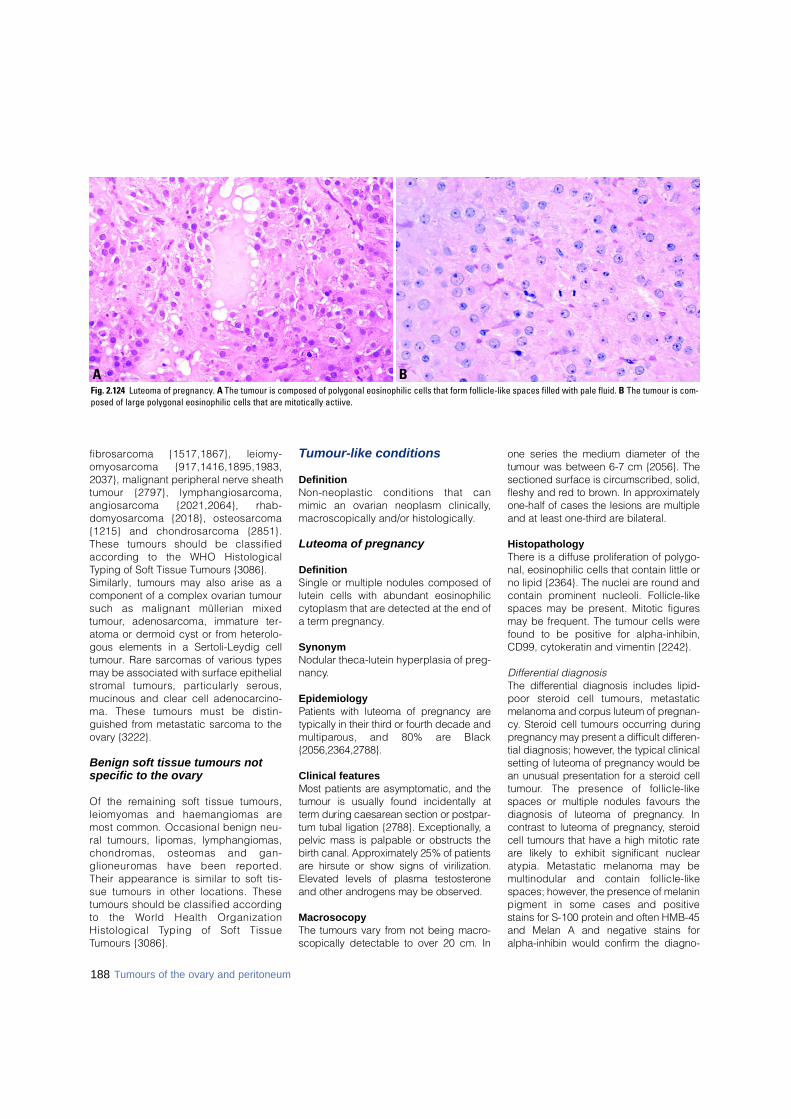
f i b ro s a rcoma {1517,1867}, leiomy-o m y o s a rcoma {917,1416,1895,1983,2037}, malignant peripheral nerve sheathtumour {2797}, lymphangiosarc o m a ,a n g i o s a rcoma {2021,2064}, rhab-d o m y o s a rcoma {2018}, osteosarc o m a{1215} and chondro s a rcoma {2851}.These tumours should be classifieda c c o rding to the WHO HistologicalTyping of Soft Tissue Tumours {3086}.Similarly, tumours may also arise as acomponent of a complex ovarian tumoursuch as malignant müllerian mixedt u m o u r, adenosarcoma, immature ter-atoma or dermoid cyst or from heterolo-gous elements in a Sertoli-Leydig celltumour. Rare sarcomas of various typesmay be associated with surface epithelials t romal tumours, particularly sero u s ,mucinous and clear cell adenocarcino-ma. These tumours must be distin-guished from metastatic sarcoma to theovary {3222}.
Benign soft tissue tumours notspecific to the ovary
Of the remaining soft tissue tumours,leiomyomas and haemangiomas aremost common. Occasional benign neu-ral tumours, lipomas, lymphangiomas,c h o n d romas, osteomas and gan-g l i o n e u romas have been re p o rt e d .Their appearance is similar to soft tis-sue tumours in other locations. Thesetumours should be classified accord i n gto the World Health OrganizationHistological Typing of Soft TissueTumours {3086}.
Tumour-like conditions
DefinitionNon-neoplastic conditions that canmimic an ovarian neoplasm clinically,macroscopically and/or histologically.
Luteoma of pregnancy
DefinitionSingle or multiple nodules composed oflutein cells with abundant eosinophiliccytoplasm that are detected at the end ofa term pregnancy.
SynonymNodular theca-lutein hyperplasia of preg-nancy.
EpidemiologyPatients with luteoma of pregnancy aretypically in their third or fourth decade andm u l t i p a rous, and 80% are Black{ 2 0 5 6 , 2 3 6 4 , 2 7 8 8 } .
Clinical featuresMost patients are asymptomatic, and thetumour is usually found incidentally att e rm during caesarean section or postpar-tum tubal ligation {2788}. Exceptionally, apelvic mass is palpable or obstructs theb i rth canal. Approximately 25% of patientsa re hirsute or show signs of virilization.Elevated levels of plasma testostero n eand other androgens may be observed.
MacrosocopyThe tumours vary from not being macro-scopically detectable to over 20 cm. In
one series the medium diameter of thetumour was between 6-7 cm {2056}. Thesectioned surface is circumscribed, solid,fleshy and red to brown. In appro x i m a t e l yone-half of cases the lesions are multipleand at least one-third are bilateral.
HistopathologyThere is a diffuse proliferation of polygo-nal, eosinophilic cells that contain little orno lipid {2364}. The nuclei are round andcontain prominent nucleoli. Follicle-likespaces may be present. Mitotic figuresmay be frequent. The tumour cells werefound to be positive for alpha-inhibin,CD99, cytokeratin and vimentin {2242}.
Differential diagnosisThe diff e rential diagnosis includes lipid-poor steroid cell tumours, metastaticmelanoma and corpus luteum of pre g n a n-c y. Steroid cell tumours occurring duringp regnancy may present a difficult diff e re n-tial diagnosis; however, the typical clinicalsetting of luteoma of pregnancy would bean unusual presentation for a steroid cellt u m o u r. The presence of follicle-likespaces or multiple nodules favours thediagnosis of luteoma of pre g n a n c y. Incontrast to luteoma of pre g n a n c y, stero i dcell tumours that have a high mitotic ratea re likely to exhibit significant nuclearatypia. Metastatic melanoma may bemultinodular and contain follicle-likespaces; however, the presence of melaninpigment in some cases and positivestains for S-100 protein and often HMB-45and Melan A and negative stains foralpha-inhibin would confirm the diagno-
BAFig. 2.124 Luteoma of pregnancy. A The tumour is composed of polygonal eosinophilic cells that form follicle-like spaces filled with pale fluid. B The tumour is com-posed of large polygonal eosinophilic cells that are mitotically actiive.
188 Tumours of the ovary and peritoneum
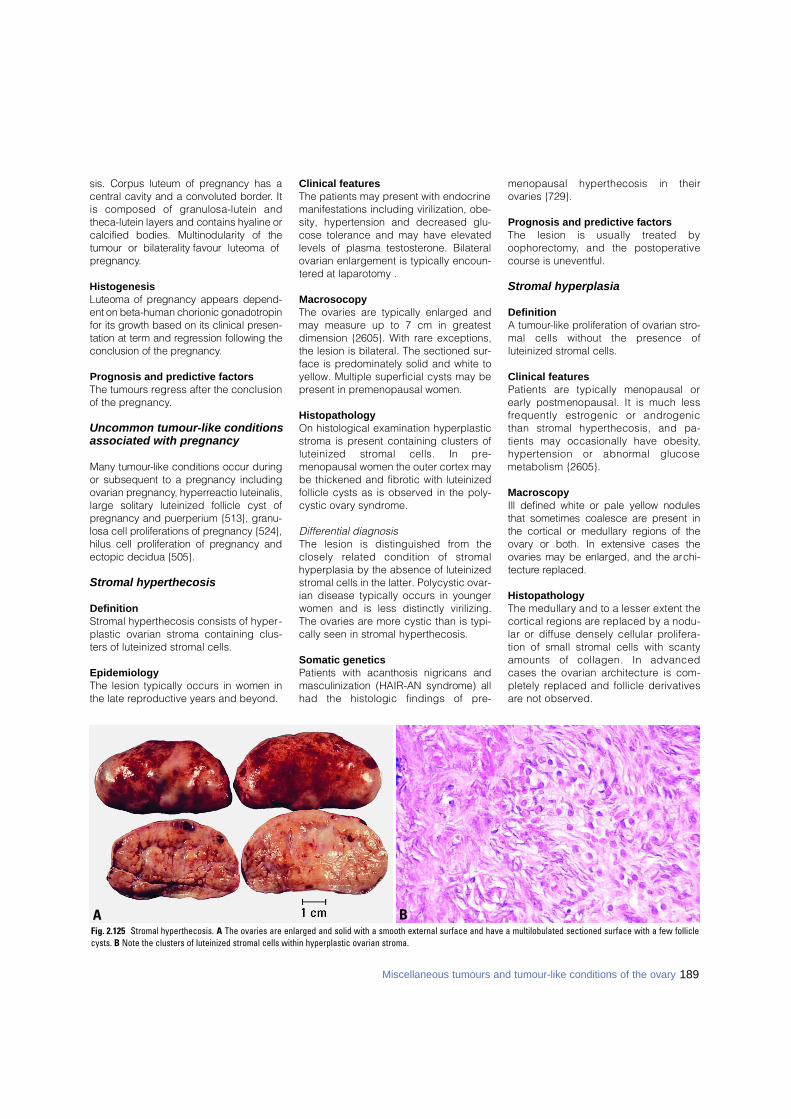
sis. Corpus luteum of pregnancy has acentral cavity and a convoluted bord e r. Itis composed of granulosa-lutein andtheca-lutein layers and contains hyaline orcalcified bodies. Multinodularity of thetumour or bilaterality favour luteoma ofp re g n a n c y.
HistogenesisLuteoma of pregnancy appears depend-ent on beta-human chorionic gonadotro p i nfor its growth based on its clinical pre s e n-tation at term and re g ression following theconclusion of the pre g n a n c y.
Prognosis and predictive factorsThe tumours regress after the conclusionof the pregnancy.
Uncommon tumour-like conditions associated with pregnancy
Many tumour-like conditions occur duringor subsequent to a pregnancy includingovarian pre g n a n c y, hyperreactio luteinalis,large solitary luteinized follicle cyst ofp regnancy and puerperium {513}, granu-losa cell proliferations of pregnancy {524},hilus cell proliferation of pregnancy andectopic decidua {505}.
Stromal hyperthecosis
DefinitionStromal hyperthecosis consists of hyper-plastic ovarian stroma containing clus-ters of luteinized stromal cells.
EpidemiologyThe lesion typically occurs in women inthe late reproductive years and beyond.
Clinical featuresThe patients may present with endocrinemanifestations including virilization, obe-sity, hypertension and decreased glu-cose tolerance and may have elevatedlevels of plasma testosterone. Bilateralovarian enlargement is typically encoun-tered at laparotomy .
MacrosocopyThe ovaries are typically enlarged andmay measure up to 7 cm in greatestdimension {2605}. With rare exceptions,the lesion is bilateral. The sectioned sur-face is predominately solid and white toyellow. Multiple superficial cysts may bepresent in premenopausal women.
HistopathologyOn histological examination hyperplasticstroma is present containing clusters ofluteinized stromal cells. In pre-menopausal women the outer cortex maybe thickened and fibrotic with luteinizedfollicle cysts as is observed in the poly-cystic ovary syndrome.
Differential diagnosisThe lesion is distinguished from theclosely related condition of stro m a lhyperplasia by the absence of luteinizedstromal cells in the latter. Polycystic ovar-ian disease typically occurs in youngerwomen and is less distinctly virilizing.The ovaries are more cystic than is typi-cally seen in stromal hyperthecosis.
Somatic geneticsPatients with acanthosis nigricans andmasculinization (HAIR-AN syndrome) allhad the histologic findings of pre-
menopausal hyperthecosis in theirovaries {729}.
Prognosis and predictive factorsThe lesion is usually treated byo o p h o re c t o m y, and the postoperativecourse is uneventful.
Stromal hyperplasia
DefinitionA tumour-like proliferation of ovarian stro-mal cells without the presence ofluteinized stromal cells.
Clinical featuresPatients are typically menopausal orearly postmenopausal. It is much lessf requently estrogenic or andro g e n i cthan stromal hyperthecosis, and pa-tients may occasionally have obesity,h y p e rtension or abnormal glucosemetabolism {2605}.
MacroscopyIll defined white or pale yellow nodulesthat sometimes coalesce are present inthe cortical or medullary regions of theo v a ry or both. In extensive cases theovaries may be enlarged, and the arc h i-t e c t u re re p l a c e d .
HistopathologyThe medullary and to a lesser extent thec o rtical regions are replaced by a nodu-lar or diffuse densely cellular pro l i f e r a-tion of small stromal cells with scantyamounts of collagen. In advancedcases the ovarian arc h i t e c t u re is com-pletely replaced and follicle derivativesa re not observed.
BAFig. 2.125 Stromal hyperthecosis. A The ovaries are enlarged and solid with a smooth external surface and have a multilobulated sectioned surface with a few folliclecysts. B Note the clusters of luteinized stromal cells within hyperplastic ovarian stroma.
189Miscellaneous tumours and tumour-like conditions of the ovary
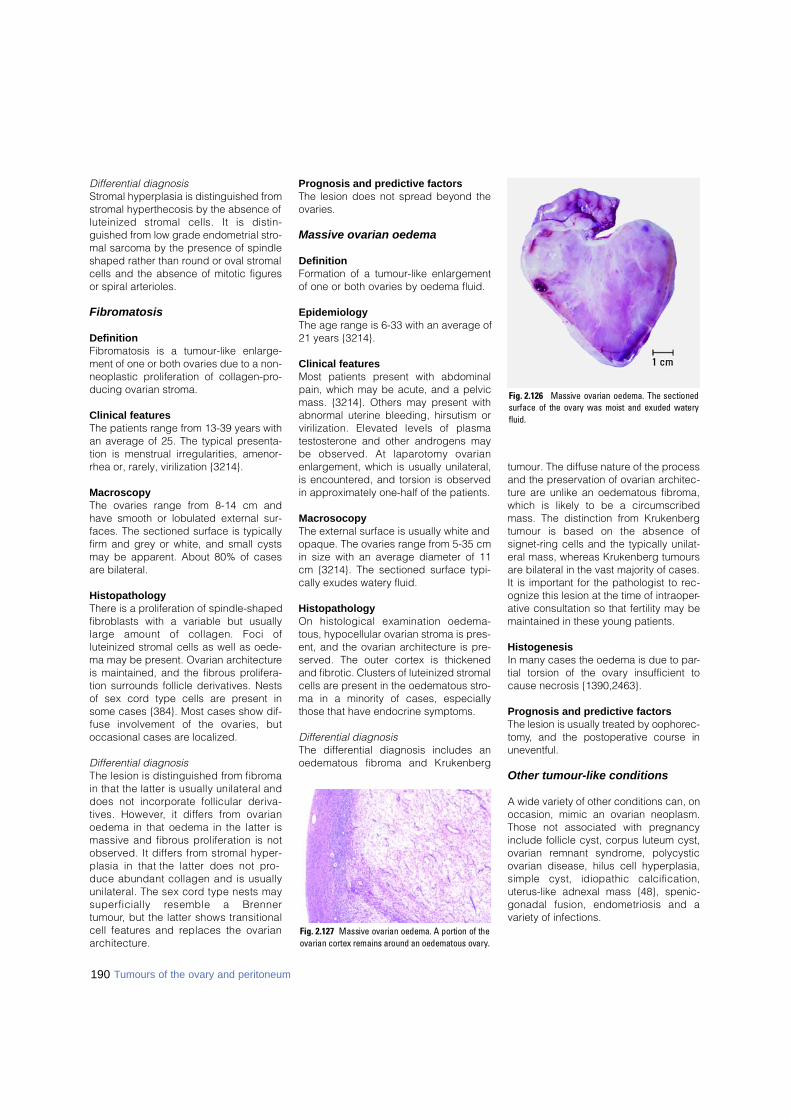
190 Tumours of the ovary and peritoneum
Differential diagnosisStromal hyperplasia is distinguished fromstromal hyperthecosis by the absence ofluteinized stromal cells. It is distin-guished from low grade endometrial stro-mal sarcoma by the presence of spindleshaped rather than round or oval stromalcells and the absence of mitotic figuresor spiral arterioles.
Fibromatosis
DefinitionFibromatosis is a tumour-like enlarge-ment of one or both ovaries due to a non-neoplastic proliferation of collagen-pro-ducing ovarian stroma.
Clinical featuresThe patients range from 13-39 years withan average of 25. The typical presenta-tion is menstrual irregularities, amenor-rhea or, rarely, virilization {3214}.
MacroscopyThe ovaries range from 8-14 cm andhave smooth or lobulated external sur-faces. The sectioned surface is typicallyfirm and grey or white, and small cystsmay be apparent. About 80% of casesare bilateral.
HistopathologyThere is a proliferation of spindle-shapedfibroblasts with a variable but usuallylarge amount of collagen. Foci ofluteinized stromal cells as well as oede-ma may be present. Ovarian architectureis maintained, and the fibrous prolifera-tion surrounds follicle derivatives. Nestsof sex cord type cells are present insome cases {384}. Most cases show dif-fuse involvement of the ovaries, butoccasional cases are localized.
Differential diagnosisThe lesion is distinguished from fibro m ain that the latter is usually unilateral anddoes not incorporate follicular deriva-tives. However, it differs from ovarianoedema in that oedema in the latter ismassive and fibrous proliferation is notobserved. It differs from stromal hyper-plasia in that the latter does not pro-duce abundant collagen and is usuallyunilateral. The sex cord type nests mays u p e rficially resemble a Bre n n e rt u m o u r, but the latter shows transitionalcell features and replaces the ovariana rc h i t e c t u re .
Prognosis and predictive factorsThe lesion does not spread beyond theo v a r i e s .
Massive ovarian oedema
DefinitionFormation of a tumour-like enlargementof one or both ovaries by oedema fluid.
EpidemiologyThe age range is 6-33 with an average of21 years {3214}.
Clinical featuresMost patients present with abdominalpain, which may be acute, and a pelvicmass. {3214}. Others may present withabnormal uterine bleeding, hirsutism orvirilization. Elevated levels of plasmatestosterone and other androgens maybe observed. At laparotomy ovarianenlargement, which is usually unilateral,is encountered, and torsion is observedin approximately one-half of the patients.
MacrosocopyThe external surface is usually white andopaque. The ovaries range from 5-35 cmin size with an average diameter of 11cm {3214}. The sectioned surface typi-cally exudes watery fluid.
HistopathologyOn histological examination oedema-tous, hypocellular ovarian stroma is pres-ent, and the ovarian architecture is pre-served. The outer cortex is thickenedand fibrotic. Clusters of luteinized stromalcells are present in the oedematous stro-ma in a minority of cases, especiallythose that have endocrine symptoms.
Differential diagnosisThe differential diagnosis includes anoedematous fibroma and Krukenberg
tumour. The diffuse nature of the processand the preservation of ovarian architec-ture are unlike an oedematous fibroma,which is likely to be a circumscribedmass. The distinction from Krukenbergtumour is based on the absence ofsignet-ring cells and the typically unilat-eral mass, whereas Krukenberg tumoursare bilateral in the vast majority of cases.It is important for the pathologist to rec-ognize this lesion at the time of intraoper-ative consultation so that fertility may bemaintained in these young patients.
HistogenesisIn many cases the oedema is due to par-tial torsion of the ovary insufficient tocause necrosis {1390,2463}.
Prognosis and predictive factorsThe lesion is usually treated by oophore c-t o m y, and the postoperative course inu n e v e n t f u l .
Other tumour-like conditions
A wide variety of other conditions can, onoccasion, mimic an ovarian neoplasm.Those not associated with pregnancyinclude follicle cyst, corpus luteum cyst,ovarian remnant syndrome, polycysticovarian disease, hilus cell hyperplasia,simple cyst, idiopathic calcification,uterus-like adnexal mass {48}, spenic-gonadal fusion, endometriosis and avariety of infections.
Fig. 2.126 Massive ovarian oedema. The sectionedsurface of the ovary was moist and exuded wateryf l u i d .
Fig. 2.127 Massive ovarian oedema. A portion of theovarian cortex remains around an oedematous ovary.
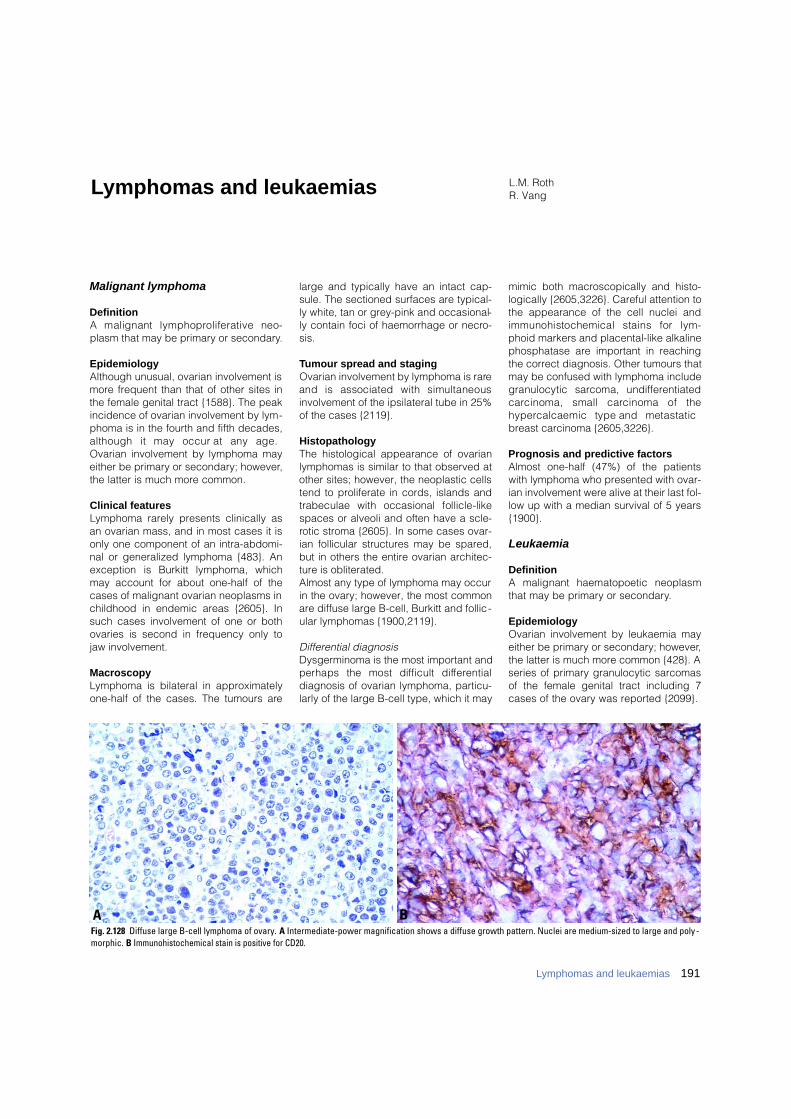
Malignant lymphoma
DefinitionA malignant lymphoproliferative neo-plasm that may be primary or secondary.
EpidemiologyAlthough unusual, ovarian involvement ismore frequent than that of other sites inthe female genital tract {1588}. The peakincidence of ovarian involvement by lym-phoma is in the fourth and fifth decades,although it may occur at any age.Ovarian involvement by lymphoma mayeither be primary or secondary; however,the latter is much more common.
Clinical featuresLymphoma rarely presents clinically asan ovarian mass, and in most cases it isonly one component of an intra-abdomi-nal or generalized lymphoma {483}. Anexception is Burkitt lymphoma, whichmay account for about one-half of thecases of malignant ovarian neoplasms inchildhood in endemic areas {2605}. Insuch cases involvement of one or bothovaries is second in frequency only tojaw involvement.
MacroscopyLymphoma is bilateral in approximatelyone-half of the cases. The tumours are
large and typically have an intact cap-sule. The sectioned surfaces are typical-ly white, tan or grey-pink and occasional-ly contain foci of haemorrhage or necro-sis.
Tumour spread and stagingOvarian involvement by lymphoma is rareand is associated with simultaneousinvolvement of the ipsilateral tube in 25%of the cases {2119}.
HistopathologyThe histological appearance of ovarianlymphomas is similar to that observed atother sites; however, the neoplastic cellstend to proliferate in cords, islands andtrabeculae with occasional follicle-likespaces or alveoli and often have a scle-rotic stroma {2605}. In some cases ovar-ian follicular structures may be spared,but in others the entire ovarian architec-ture is obliterated. Almost any type of lymphoma may occurin the ovary; however, the most commonare diffuse large B-cell, Burkitt and follic-ular lymphomas {1900,2119}.
Differential diagnosisDysgerminoma is the most important andperhaps the most difficult diff e re n t i a ldiagnosis of ovarian lymphoma, particu-larly of the large B-cell type, which it may
mimic both macroscopically and histo-logically {2605,3226}. Careful attention tothe appearance of the cell nuclei andimmunohistochemical stains for lym-phoid markers and placental-like alkalinephosphatase are important in reachingthe correct diagnosis. Other tumours thatmay be confused with lymphoma includegranulocytic sarcoma, undiff e re n t i a t e dc a rcinoma, small carcinoma of theh y p e rcalcaemic type and metastaticbreast carcinoma {2605,3226}.
Prognosis and predictive factorsAlmost one-half (47%) of the patientswith lymphoma who presented with ovar-ian involvement were alive at their last fol-low up with a median survival of 5 years{1900}.
Leukaemia
DefinitionA malignant haematopoetic neoplasmthat may be primary or secondary.
EpidemiologyOvarian involvement by leukaemia mayeither be primary or secondary; however,the latter is much more common {428}. Aseries of primary granulocytic sarcomasof the female genital tract including 7cases of the ovary was reported {2099}.
L.M. RothR. VangLymphomas and leukaemias
BAFig. 2.128 Diffuse large B-cell lymphoma of ovary. A Intermediate-power magnification shows a diffuse growth pattern. Nuclei are medium-sized to large and poly-morphic. B Immunohistochemical stain is positive for CD20.
191Lymphomas and leukaemias

Clinical featuresRarely, a patient presents with an ovariangranulocytic sarcoma with or withouthaematological evidence of acutemyeloid leukaemia {2099}. Cases ofacute lymphoblastic leukaemia, mostly inchildren and teenagers, are known torecur in the ovaries during haematologi-cal remission.
MacroscopyThe ovarian tumours are usually largeand may be either unilateral or bilateral.They are typically solid, soft, and white,yellow or red-brown; occasionally, theymay be green, and such tumours havebeen designated as a "chloroma" {2605}.
HistopathologyGranulocytic sarcomas have a predomi-nantly diffuse growth pattern, but some-times a cord-like or pseudoacinararrangement of the tumour cells is pres-ent focally {2099]. They are usually com-posed of cells with finely dispersednuclear chromatin and abundant cyto-
plasm that may be deeply eosinophilic.The identification of eosinophilic myelo-cytes is helpful in establishing the diag-nosis; however, they are not always pres-ent.
Differential diagnosisThe most important differential diagnosisis malignant lymphoma. Histochemicalstains for chloracetate esterase orimmunohistochemical stains for myelo-proxidase, CD68 and CD43 will establishthe diagnosis in almost all cases {2099}.
Plasmacytoma
DefinitionA clonal proliferation of plasma cells thatis cytologically and immunophenotypi-cally identical to plasma cell myelomabut manifests a localized growth pattern.
HistopathologyThe tumour cells may be mature orimmature. The mature type has eccentricnuclei with clumped chromatin, low
nuclear to cytoplasmic ratios, abundantcytoplasm and a prominent perinuclearhof. The immature form is pleomorphicwith frequent multinucleated cells.
Clinical findingsOvarian plasmacytoma is a rare tumourthat may present clinically with a unilater-al adnexal mass. The 7 reported patientswere 12-63 years old {782}.
MacroscopyThe tumours were large, and the sec-tioned surface was white, pale yellow orgrey.
Prognosis and predictive factorsOne patient developed multiple myeloma2 years after removal of the tumour.
BAFig. 2.129 Precursor T-cell lymphoblastic lymphoma of ovary. A High power magnification shows small to medium-sized cells with scant cytoplasm, round nucleiand fine chromatin. B Immunohistochemical stain is positive for CD99.
192 Tumours of the ovary and peritoneum

DefinitionMalignant tumours that metastasize tothe ovary from extraovarian primary neo-plasms. Tumours that extend to the ovarydirectly from adjacent organs or tissuesa re also included in this category.However, most ovarian carcinomas asso-ciated with uterine cancers of similar his-tological type are independent primaryneoplasms. General features of ovarianmetastasis include: bilaterality, smallmultinodular surface tumours, extensiveextraovarian spread, unusual patterns ofdissemination, unusual histological fea-tures, blood vessel and lymphatic inva-sion and a desmoplastic reaction.
SynonymMetastatic tumours.The term Krukenberg tumour refers to ametastatic mucinous/signet-ring celladenocarcinoma of the ovaries whichtypically originates from primary tumoursof the G.I. tract, most often colon andstomach.
EpidemiologyMetastatic tumours to the ovary are com-mon and occur in approximately 30% ofwomen dying of cancer. Approximately6-7% of all adnexal masses found duringphysical examination are actuallymetastatic ovarian tumours, frequentlyunsuspected by gynaecologists {1587,2605,2980}. The metastasis often mas-querades as a primary ovarian tumour
and may even be the initial manifestationof the patient's cancer. Pathologists alsotend to mistake metastatic tumours forprimary ovarian neoplasms even afterhistological examination. Carcinomas ofthe colon, stomach, breast andendometrium as well as lymphomas andleukaemias account for the vast majorityof cases {3226}. Ovarian metastases areassociated with breast cancer in 32-38%of cases, with colorectal cancer in 28-35% of cases and with tumours of thegenital tract (endometrium, uterinecervix, vagina, vulva) in 16% of cases. Inrecent years attention has been drawn tomucinous tumours of the appendix, pan-creas and biliary tract that often spreadto the ovary and closely simulate ovarianmucinous borderline tumours or carcino-mas {590,1848,2406,3199,3200}.
AetiologyThe routes of tumour spread to the ovaryare variable. Lymphatic and haematoge-nous metastasis to the ovaries is themost common form of dissemination{1587,2605,2980}. Direct extension isalso a common manner of spread fromadjacent tumours of the fallopian tube,uterus and colorectum {3226}. Transtubalspread provides an explanation for somes u rface ovarian implants from uterinecancers. Neoplasms may also reach theovary by the transperitoneal route fromabdominal organs, such as the appendix{3199}. Embolic spread often produces
multiple nodules within the substance ofthe ovary and commonly is accompaniedby prominent intravascular nests oftumour in the ovarian hilum, mesovariumand mesosalpinx.
Clinical featuresSigns and symptomsOvarian metastases can be discoveredin patients during follow-up after treat-ment of a primary tumour, seredipitouslydiagnosed during a surgical procedurefor treatment of an abdominal tumour orfortuitously found at autopsy. The circum-stances leading to the discovery of thesemetastatic lesions depends on the site ofthe primary tumour {951,1802}. Ovarianmetastasis was detected before thebreast cancer in only 1.5% of cases
J. PratP. MoriceSecondary tumours of the ovary
B CAFig. 2.130 Metastatic colonic adenocarcinoma of the ovaries. A The ovaries are replaced by bilateral, multinodular metastases. Note the additional leiomyomas ofthe corpus uteri (centre). B This tumour shows a garland-like glandular pattern with focal segmental necrosis of glands and luminal necrotic debris. C Immunohistochemical stain for carcinoembryonic antigen is strongly positive.
Table 2.09Metastatic tumours to the ovary.
193Secondary tumours of the ovary
Clues to the diagnosis
1 - Bilaterality (mucinous and endometrioid-like)
2 - Small, superficial, multinodular tumours
3 - Vascular invasion
4 - Desmoplastic reaction
5 - Extensive, unusual extraovarian spread
6 - Unusual clinical history
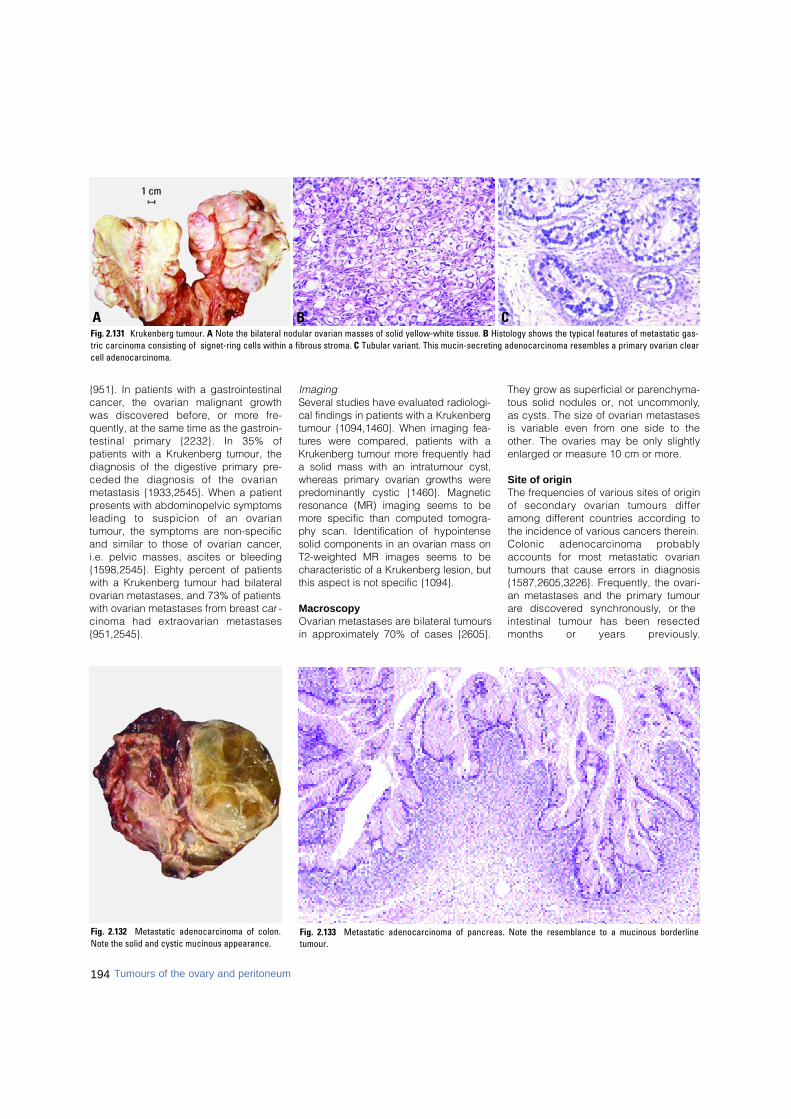
{951}. In patients with a gastrointestinalc a n c e r, the ovarian malignant gro w t hwas discovered before, or more fre-quently, at the same time as the gastroin-testinal primary {2232}. In 35% ofpatients with a Krukenberg tumour, thediagnosis of the digestive primary pre-ceded the diagnosis of the ovarianmetastasis {1933,2545}. When a patientpresents with abdominopelvic symptomsleading to suspicion of an ovariantumour, the symptoms are non-specificand similar to those of ovarian cancer,i.e. pelvic masses, ascites or bleeding{1598,2545}. Eighty percent of patientswith a Krukenberg tumour had bilateralovarian metastases, and 73% of patientswith ovarian metastases from breast car-cinoma had extraovarian metastases{951,2545}.
ImagingSeveral studies have evaluated radiologi-cal findings in patients with a Krukenbergtumour {1094,1460}. When imaging fea-t u res were compared, patients with aKrukenberg tumour more frequently hada solid mass with an intratumour cyst,w h e reas primary ovarian growths werep redominantly cystic {1460}. Magneticresonance (MR) imaging seems to bem o re specific than computed tomogra-phy scan. Identification of hypointensesolid components in an ovarian mass onT2-weighted MR images seems to becharacteristic of a Krukenberg lesion, butthis aspect is not specific {1094}.
MacroscopyOvarian metastases are bilateral tumoursin approximately 70% of cases {2605}.
They grow as superficial or parenchyma-tous solid nodules or, not uncommonly,as cysts. The size of ovarian metastasesis variable even from one side to theother. The ovaries may be only slightlyenlarged or measure 10 cm or more.
Site of originThe frequencies of various sites of originof secondary ovarian tumours diff e ramong different countries according tothe incidence of various cancers therein.Colonic adenocarcinoma pro b a b l yaccounts for most metastatic ovariantumours that cause errors in diagnosis{1587,2605,3226}. Frequently, the ovari-an metastases and the primary tumoura re discovered synchro n o u s l y, or theintestinal tumour has been re s e c t e dmonths or years pre v i o u s l y.
Fig. 2.132 Metastatic adenocarcinoma of colon.Note the solid and cystic mucinous appearance.
B CAFig. 2.131 Krukenberg tumour. A Note the bilateral nodular ovarian masses of solid yellow-white tissue. B Histology shows the typical features of metastatic gas-tric carcinoma consisting of signet-ring cells within a fibrous stroma. C Tubular variant. This mucin-secreting adenocarcinoma resembles a primary ovarian clearcell adenocarcinoma.
194 Tumours of the ovary and peritoneum
Fig. 2.133 Metastatic adenocarcinoma of pancreas. Note the resemblance to a mucinous borderlinetumour.
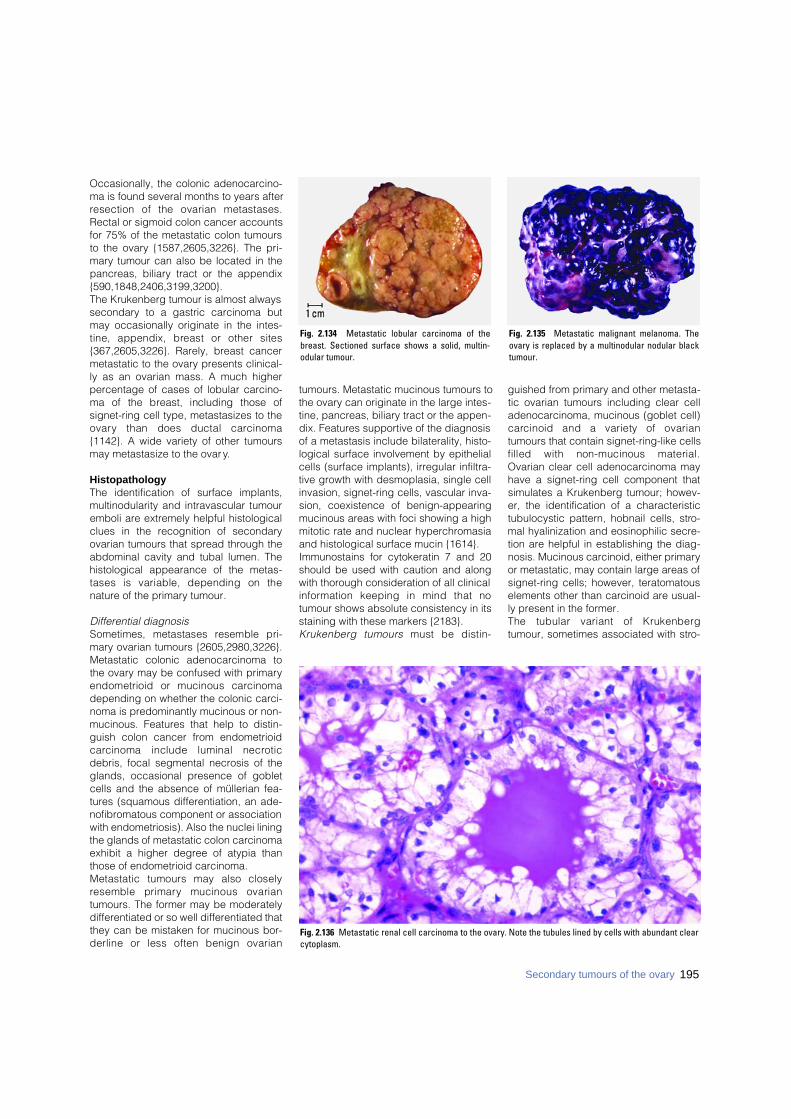
Occasionally, the colonic adenocarcino-ma is found several months to years afterresection of the ovarian metastases.Rectal or sigmoid colon cancer accountsfor 75% of the metastatic colon tumoursto the ovary {1587,2605,3226}. The pri-mary tumour can also be located in thepancreas, biliary tract or the appendix{590,1848,2406,3199,3200}.The Krukenberg tumour is almost alwayssecondary to a gastric carcinoma butmay occasionally originate in the intes-tine, appendix, breast or other sites{367,2605,3226}. Rarely, breast cancermetastatic to the ovary presents clinical-ly as an ovarian mass. A much higherpercentage of cases of lobular carcino-ma of the breast, including those ofsignet-ring cell type, metastasizes to theo v a ry than does ductal carc i n o m a{1142}. A wide variety of other tumoursmay metastasize to the ovary.
HistopathologyThe identification of surface implants,multinodularity and intravascular tumouremboli are extremely helpful histologicalclues in the recognition of secondaryovarian tumours that spread through theabdominal cavity and tubal lumen. Thehistological appearance of the metas-tases is variable, depending on thenature of the primary tumour.
Differential diagnosisSometimes, metastases resemble pri-mary ovarian tumours {2605,2980,3226}.Metastatic colonic adenocarcinoma tothe ovary may be confused with primaryendometrioid or mucinous carc i n o m adepending on whether the colonic carci-noma is predominantly mucinous or non-mucinous. Features that help to distin-guish colon cancer from endometrioidc a rcinoma include luminal necro t i cdebris, focal segmental necrosis of theglands, occasional presence of gobletcells and the absence of müllerian fea-tures (squamous differentiation, an ade-nofibromatous component or associationwith endometriosis). Also the nuclei liningthe glands of metastatic colon carcinomaexhibit a higher degree of atypia thanthose of endometrioid carcinoma.Metastatic tumours may also closelyresemble primary mucinous ovariantumours. The former may be moderatelydifferentiated or so well differentiated thatthey can be mistaken for mucinous bor-derline or less often benign ovarian
tumours. Metastatic mucinous tumours tothe ovary can originate in the large intes-tine, pancreas, biliary tract or the appen-dix. Features supportive of the diagnosisof a metastasis include bilaterality, histo-logical surface involvement by epithelialcells (surface implants), irregular infiltra-tive growth with desmoplasia, single cellinvasion, signet-ring cells, vascular inva-sion, coexistence of benign-appearingmucinous areas with foci showing a highmitotic rate and nuclear hyperchromasiaand histological surface mucin {1614}.Immunostains for cytokeratin 7 and 20should be used with caution and alongwith thorough consideration of all clinicali n f o rmation keeping in mind that notumour shows absolute consistency in itsstaining with these markers {2183}.Krukenberg tumours must be distin-
guished from primary and other metasta-tic ovarian tumours including clear celladenocarcinoma, mucinous (goblet cell)c a rcinoid and a variety of ovariantumours that contain signet-ring-like cellsfilled with non-mucinous material.Ovarian clear cell adenocarcinoma mayhave a signet-ring cell component thatsimulates a Krukenberg tumour; howev-er, the identification of a characteristictubulocystic pattern, hobnail cells, stro-mal hyalinization and eosinophilic secre-tion are helpful in establishing the diag-nosis. Mucinous carcinoid, either primaryor metastatic, may contain large areas ofsignet-ring cells; however, teratomatouselements other than carcinoid are usual-ly present in the former.The tubular variant of Krukenbergtumour, sometimes associated with stro-
Fig. 2.134 Metastatic lobular carcinoma of thebreast. Sectioned surface shows a solid, multin-odular tumour.
Fig. 2.135 Metastatic malignant melanoma. Theovary is replaced by a multinodular nodular blacktumour.
Fig. 2.136 Metastatic renal cell carcinoma to the ovary. Note the tubules lined by cells with abundant clearcytoplasm.
195Secondary tumours of the ovary

mal luteinization, can be confused with aSertoli-Leydig cell tumour. Positive muci -carmine and PAS-stains with diastasedigestion are of great value in establish-ing the diagnosis of a Krukenbergtumour. Occasional Krukenberg tumoursmay closely resemble fibromas onmacroscopic examination and may con-tain relatively few signet-ring cells.Bilaterality and positive mucin stainsfacilitate the differential diagnosis.Distinction between a transitional cellcarcinoma of the urinary tract metastaticto the ovary and a primary transitionalcell carcinoma may be diff i c u l t{2100,3220}. Clinical information may benecessary to resolve the issue.Renal cell carcinoma rarely metastasizesto the ovaries; however, when it does, itmust be distinguished from a primaryclear cell carcinoma. The metastatictumour usually shows a sinusoidal vas-cular pattern, a homogenous clear cellp a t t e rn without hobnail cells, theabsence of hyalinized papillae and theabsence of mucin {3226}.A metastatic carcinoid can be confused
with a primary carcinoid, granulosa cellt u m o u r, Sertoli-Leydig cell tumour,B renner tumour, adenofibroma orendometrioid carcinoma {2605,3226}.Bilaterality and extraovarian extensionare important features of metastatic car-cinoid.In the ovary, metastatic malignantmelanoma may be confused with primarymalignant melanoma; the latter is unilat-eral and usually associated with a der-moid cyst. When a melanoma is com-posed predominantly of large cells, itmay resemble steroid cell lesions suchas steroid cell tumour or luteoma of preg-nancy; when it is composed predomi-nantly of small cells it may be confusedwith a variety of other tumours character-ized by small cells {3223}. Positive stainsfor melanin, S-100 protein, melan A,and/or HMB-45 should establish thediagnosis of melanoma.Sarcomas may metastasize to the ovaryfrom the uterus or extragenital sites andmay occasionally be discovered beforethe primary tumour {3222}. Metastasticlow grade endometrial stromal sarcoma
(ESS) may simulate a primary ovariansex cord-stromal tumour. Features help-ful in their distinction include the pres-ence of extraovarian disease, bilateralityand the characteristic content of spiralarterioles in metastatic low grade ESS.Metastatic epitheliolid leiomyosarc o m amay have an appearance that simulatesthe solid tubular pattern of a Sertoli celltumour.Although lymphoma and leukaemia caninvolve the ovaries simulating various pri-mary tumours, they rarely present clini-cally as an ovarian mass. In countriesw h e re Burkitt lymphoma is endemic,however, it accounts for approximatelyhalf the cases of malignant ovariantumours in childhood. Dysgerminoma isone of the most common and difficult dif-ferential diagnoses. The appearance ofthe cell nuclei is very import a n t .I m m u n o h i s t o c h e m i s t ry for lymphoidmarkers and placental alkaline phos-phatase are helpful. Carcinoid, granu-losa cell tumour or small cell carcinomacan also resemble lymphoma. In patientswith acute myeloid leukaemia, ovarianinvolvement in the form of granulocyticsarcoma ("chloroma") may rarely consti-tute the initial clinical presentation of thedisease. Histological examinationreveals a diffuse growth pattern with aprominent "single file" arrangement of thetumour cells. Myeloid differentiation canbe demonstrated by the chloroacetateesterase stain. Immunoperoxidase stainsfor lysozyme, CD68, and LCA are alsohelpful.Recognition of the secondary nature ofan ovarian tumour depends on a com-plete clinical history, a careful operativesearch for a primary extraovarian tumour,and accurate evaluation of the macro-scopic and histological features of theovarian tumour. In rare cases the primarytumour is not found until several yearsafter resection of the ovarian metastases{2605,3226}.
Prognosis and predictive factorsOvarian metastases often represent alate disseminated stage of the disease inwhich other haematogenous metastasesare also found. The prognosis is, there-fore, poor.
B
FT
CFig. 2.137 Burkitt-like lymphoma. A T2 weighted sagital computed tomography scan from an 8-year old girlshows a large pelvic mass. B Sagital section of the ovarian tumour shows a homogeneous, pale surface.Notice the enlargement of the fallopian tube (FT). C A starry-sky pattern is apparent (B5 fixation).
A
196 Tumours of the ovary and peritoneum
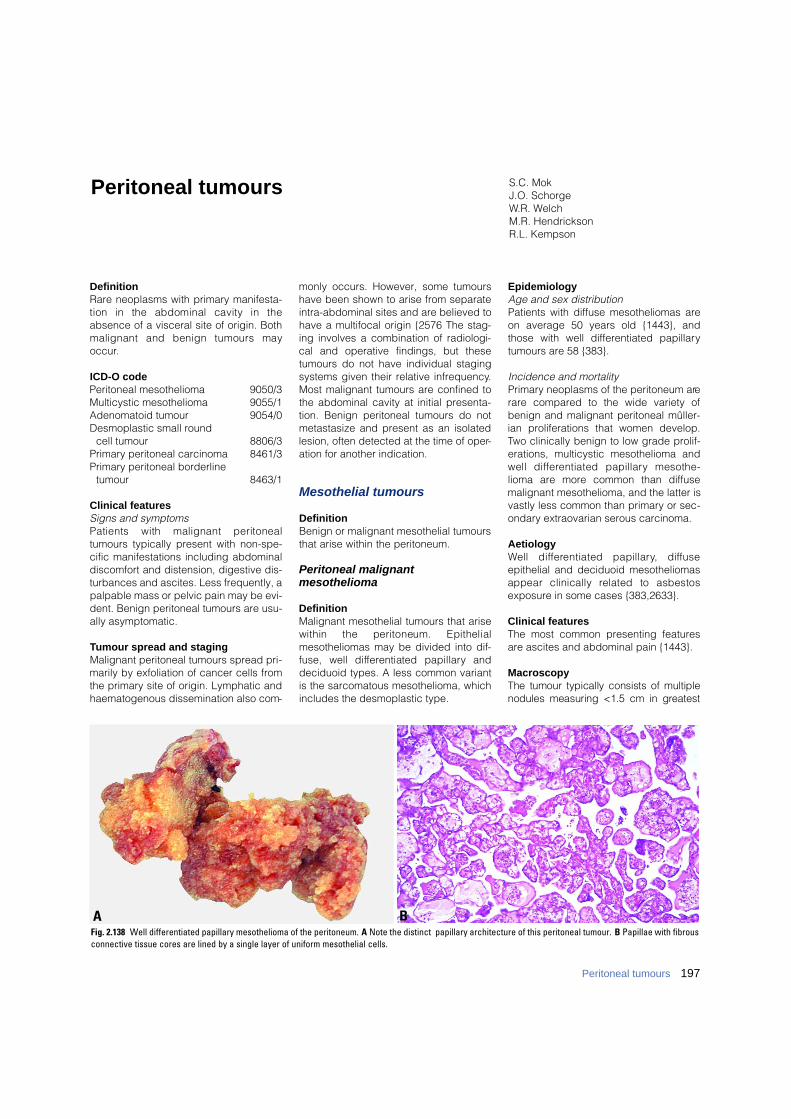
Definition Rare neoplasms with primary manifesta-tion in the abdominal cavity in theabsence of a visceral site of origin. Bothmalignant and benign tumours mayoccur.
ICD-O codePeritoneal mesothelioma 9050/3Multicystic mesothelioma 9055/1Adenomatoid tumour 9054/0Desmoplastic small round
cell tumour 8806/3Primary peritoneal carcinoma 8461/3Primary peritoneal borderline
tumour 8463/1
Clinical featuresSigns and symptomsPatients with malignant peritonealtumours typically present with non-spe-cific manifestations including abdominaldiscomfort and distension, digestive dis-turbances and ascites. Less frequently, apalpable mass or pelvic pain may be evi-dent. Benign peritoneal tumours are usu-ally asymptomatic.
Tumour spread and stagingMalignant peritoneal tumours spread pri-marily by exfoliation of cancer cells fromthe primary site of origin. Lymphatic andhaematogenous dissemination also com-
monly occurs. However, some tumourshave been shown to arise from separateintra-abdominal sites and are believed tohave a multifocal origin {2576 The stag-ing involves a combination of radiologi-cal and operative findings, but thesetumours do not have individual stagingsystems given their relative infrequency.Most malignant tumours are confined tothe abdominal cavity at initial presenta-tion. Benign peritoneal tumours do notmetastasize and present as an isolatedlesion, often detected at the time of oper-ation for another indication.
Mesothelial tumours
DefinitionBenign or malignant mesothelial tumoursthat arise within the peritoneum.
Peritoneal malignant mesothelioma
DefinitionMalignant mesothelial tumours that arisewithin the peritoneum. Epithelialmesotheliomas may be divided into dif-fuse, well diff e rentiated papillary anddeciduoid types. A less common variantis the sarcomatous mesothelioma, whichincludes the desmoplastic type.
EpidemiologyAge and sex distributionPatients with diffuse mesotheliomas areon average 50 years old {1443}, andthose with well differentiated papillarytumours are 58 {383}.
Incidence and mortalityPrimary neoplasms of the peritoneum arerare compared to the wide variety ofbenign and malignant peritoneal mûller-ian proliferations that women develop.Two clinically benign to low grade prolif-erations, multicystic mesothelioma andwell diff e rentiated papillary mesothe-lioma are more common than diffusemalignant mesothelioma, and the latter isvastly less common than primary or sec-ondary extraovarian serous carcinoma.
AetiologyWell diff e rentiated papillary, diff u s eepithelial and deciduoid mesotheliomasappear clinically related to asbestosexposure in some cases {383,2633}.
Clinical featuresThe most common presenting featuresare ascites and abdominal pain {1443}.
MacroscopyThe tumour typically consists of multiplenodules measuring <1.5 cm in gre a t e s t
Peritoneal tumours S.C. MokJ.O. SchorgeW.R. WelchM.R. HendricksonR.L. Kempson
BAFig. 2.138 Well differentiated papillary mesothelioma of the peritoneum. A Note the distinct papillary architecture of this peritoneal tumour. B Papillae with fibrousconnective tissue cores are lined by a single layer of uniform mesothelial cells.
197Peritoneal tumours
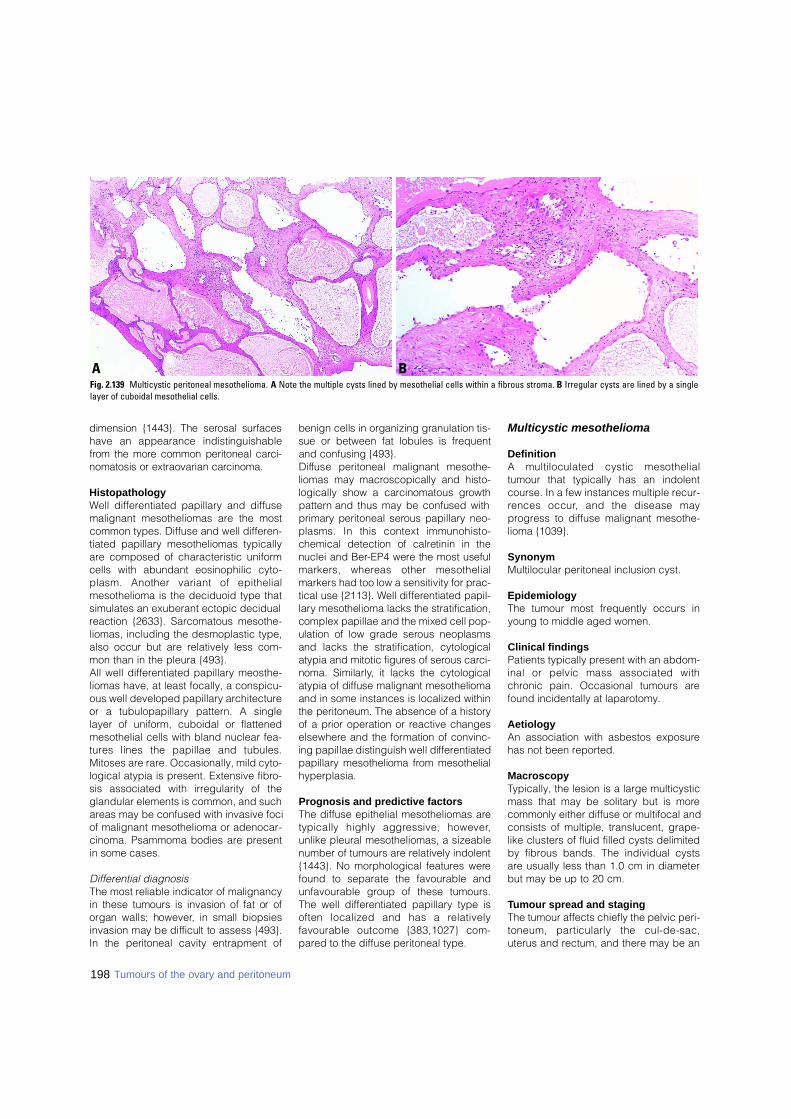
198 Tumours of the ovary and peritoneum
dimension {1443}. The serosal surf a c e shave an appearance indistinguishablef rom the more common peritoneal carc i-nomatosis or extraovarian carc i n o m a .
Histopathology Well differentiated papillary and diffusemalignant mesotheliomas are the mostcommon types. Diffuse and well differen-tiated papillary mesotheliomas typicallyare composed of characteristic uniformcells with abundant eosinophilic cyto-plasm. Another variant of epithelialmesothelioma is the deciduoid type thatsimulates an exuberant ectopic decidualreaction {2633}. Sarcomatous mesothe-liomas, including the desmoplastic type,also occur but are relatively less com-mon than in the pleura {493}. All well differentiated papillary meosthe-liomas have, at least focally, a conspicu-ous well developed papillary architectureor a tubulopapillary pattern. A singlelayer of uniform, cuboidal or flattenedmesothelial cells with bland nuclear fea-t u res lines the papillae and tubules.Mitoses are rare. Occasionally, mild cyto-logical atypia is present. Extensive fibro-sis associated with irregularity of theglandular elements is common, and suchareas may be confused with invasive fociof malignant mesothelioma or adenocar-cinoma. Psammoma bodies are presentin some cases.
Differential diagnosisThe most reliable indicator of malignancyin these tumours is invasion of fat or oforgan walls; however, in small biopsiesinvasion may be difficult to assess {493}.In the peritoneal cavity entrapment of
benign cells in organizing granulation tis-sue or between fat lobules is fre q u e n tand confusing {493}.D i ffuse peritoneal malignant mesothe-liomas may macroscopically and histo-logically show a carcinomatous gro w t hp a t t e rn and thus may be confused withp r i m a ry peritoneal serous papillary neo-plasms. In this context immunohisto-chemical detection of calretinin in thenuclei and Ber-EP4 were the most usefulmarkers, whereas other mesothelialmarkers had too low a sensitivity for prac-tical use {2113}. Well diff e rentiated papil-l a ry mesothelioma lacks the stratification,complex papillae and the mixed cell pop-ulation of low grade serous neoplasmsand lacks the stratification, cytologicalatypia and mitotic figures of serous carc i-noma. Similarly, it lacks the cytologicalatypia of diffuse malignant mesotheliomaand in some instances is localized withinthe peritoneum. The absence of a historyof a prior operation or reactive changese l s e w h e re and the formation of convinc-ing papillae distinguish well diff e re n t i a t e dp a p i l l a ry mesothelioma from mesothelialh y p e r p l a s i a .
Prognosis and predictive factorsThe diffuse epithelial mesotheliomas aretypically highly aggressive; however,unlike pleural mesotheliomas, a sizeablenumber of tumours are relatively indolent{1443}. No morphological features werefound to separate the favourable andunfavourable group of these tumours.The well differentiated papillary type isoften localized and has a re l a t i v e l yfavourable outcome {383,1027} com-pared to the diffuse peritoneal type.
Multicystic mesothelioma
DefinitionA multiloculated cystic mesothelialtumour that typically has an indolentcourse. In a few instances multiple recur-rences occur, and the disease mayprogress to diffuse malignant mesothe-lioma {1039}.
SynonymMultilocular peritoneal inclusion cyst.
EpidemiologyThe tumour most frequently occurs inyoung to middle aged women.
Clinical findingsPatients typically present with an abdom-inal or pelvic mass associated withchronic pain. Occasional tumours arefound incidentally at laparotomy.
AetiologyAn association with asbestos exposurehas not been reported.
MacroscopyTypically, the lesion is a large multicysticmass that may be solitary but is morecommonly either diffuse or multifocal andconsists of multiple, translucent, grape-like clusters of fluid filled cysts delimitedby fibrous bands. The individual cystsare usually less than 1.0 cm in diameterbut may be up to 20 cm.
Tumour spread and stagingThe tumour affects chiefly the pelvic peri-toneum, particularly the cul-de-sac,uterus and rectum, and there may be an
BAFig. 2.139 Multicystic peritoneal mesothelioma. A Note the multiple cysts lined by mesothelial cells within a fibrous stroma. B Irregular cysts are lined by a singlelayer of cuboidal mesothelial cells.
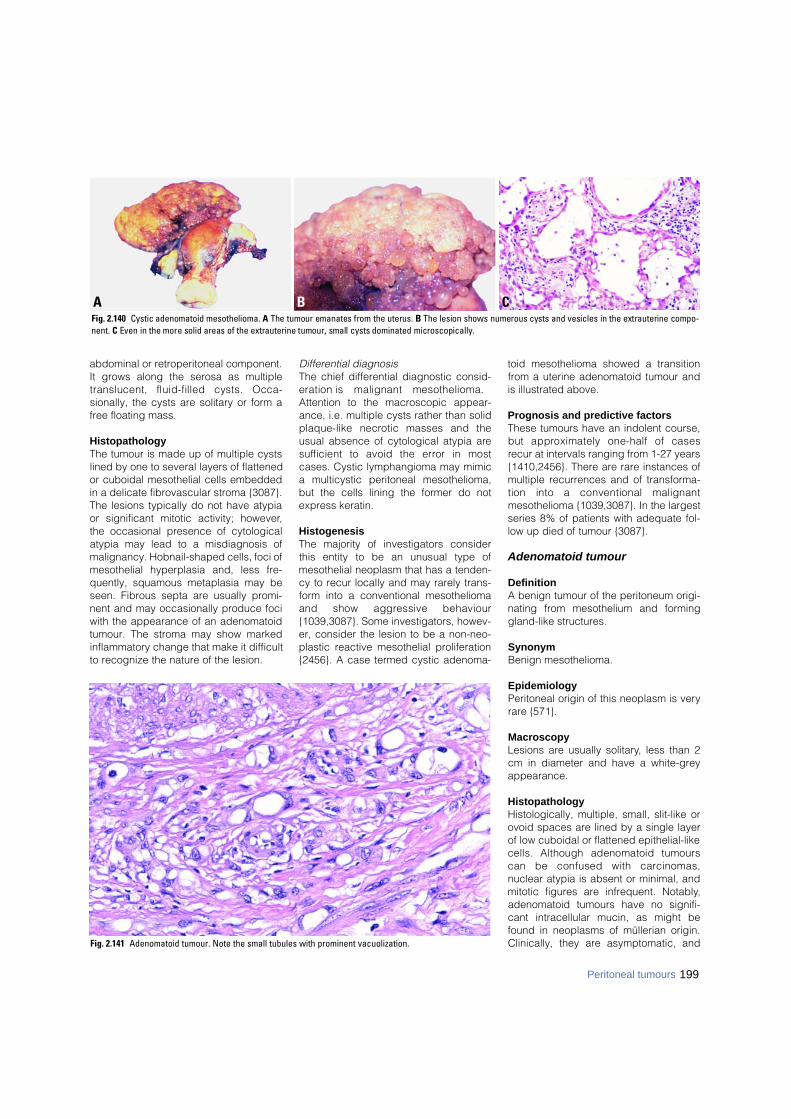
abdominal or retroperitoneal component.It grows along the serosa as multipletranslucent, fluid-filled cysts. Occa-sionally, the cysts are solitary or form afree floating mass.
HistopathologyThe tumour is made up of multiple cystslined by one to several layers of flattenedor cuboidal mesothelial cells embeddedin a delicate fibrovascular stroma {3087}.The lesions typically do not have atypiaor significant mitotic activity; however,the occasional presence of cytologicalatypia may lead to a misdiagnosis ofmalignancy. Hobnail-shaped cells, foci ofmesothelial hyperplasia and, less fre-quently, squamous metaplasia may beseen. Fibrous septa are usually promi-nent and may occasionally produce fociwith the appearance of an adenomatoidtumour. The stroma may show markedinflammatory change that make it difficultto recognize the nature of the lesion.
Differential diagnosisThe chief differential diagnostic consid-eration is malignant mesothelioma.Attention to the macroscopic appear-ance, i.e. multiple cysts rather than solidplaque-like necrotic masses and theusual absence of cytological atypia ares u fficient to avoid the error in mostcases. Cystic lymphangioma may mimica multicystic peritoneal mesothelioma,but the cells lining the former do notexpress keratin.
HistogenesisThe majority of investigators considerthis entity to be an unusual type ofmesothelial neoplasm that has a tenden-cy to recur locally and may rarely trans-form into a conventional mesotheliomaand show aggressive behaviour{1039,3087}. Some investigators, howev-er, consider the lesion to be a non-neo-plastic reactive mesothelial proliferation{2456}. A case termed cystic adenoma-
toid mesothelioma showed a transitionfrom a uterine adenomatoid tumour andis illustrated above.
Prognosis and predictive factorsThese tumours have an indolent course,but approximately one-half of casesrecur at intervals ranging from 1-27 years{1410,2456}. There are rare instances ofmultiple recurrences and of transforma-tion into a conventional malignantmesothelioma {1039,3087}. In the largestseries 8% of patients with adequate fol-low up died of tumour {3087}.
Adenomatoid tumour
DefinitionA benign tumour of the peritoneum origi-nating from mesothelium and forminggland-like structures.
SynonymBenign mesothelioma.
EpidemiologyPeritoneal origin of this neoplasm is veryrare {571}.
MacroscopyLesions are usually solitary, less than 2cm in diameter and have a white-greyappearance.
HistopathologyHistologically, multiple, small, slit-like orovoid spaces are lined by a single layerof low cuboidal or flattened epithelial-likecells. Although adenomatoid tumourscan be confused with carc i n o m a s ,nuclear atypia is absent or minimal, andmitotic figures are infrequent. Notably,adenomatoid tumours have no signifi-cant intracellular mucin, as might befound in neoplasms of müllerian origin.Clinically, they are asymptomatic, andFig. 2.141 Adenomatoid tumour. Note the small tubules with prominent vacuolization.
B CAFig. 2.140 Cystic adenomatoid mesothelioma. A The tumour emanates from the uterus. B The lesion shows numerous cysts and vesicles in the extrauterine compo-n e n t . C Even in the more solid areas of the extrauterine tumour, small cysts dominated microscopically.
199Peritoneal tumours
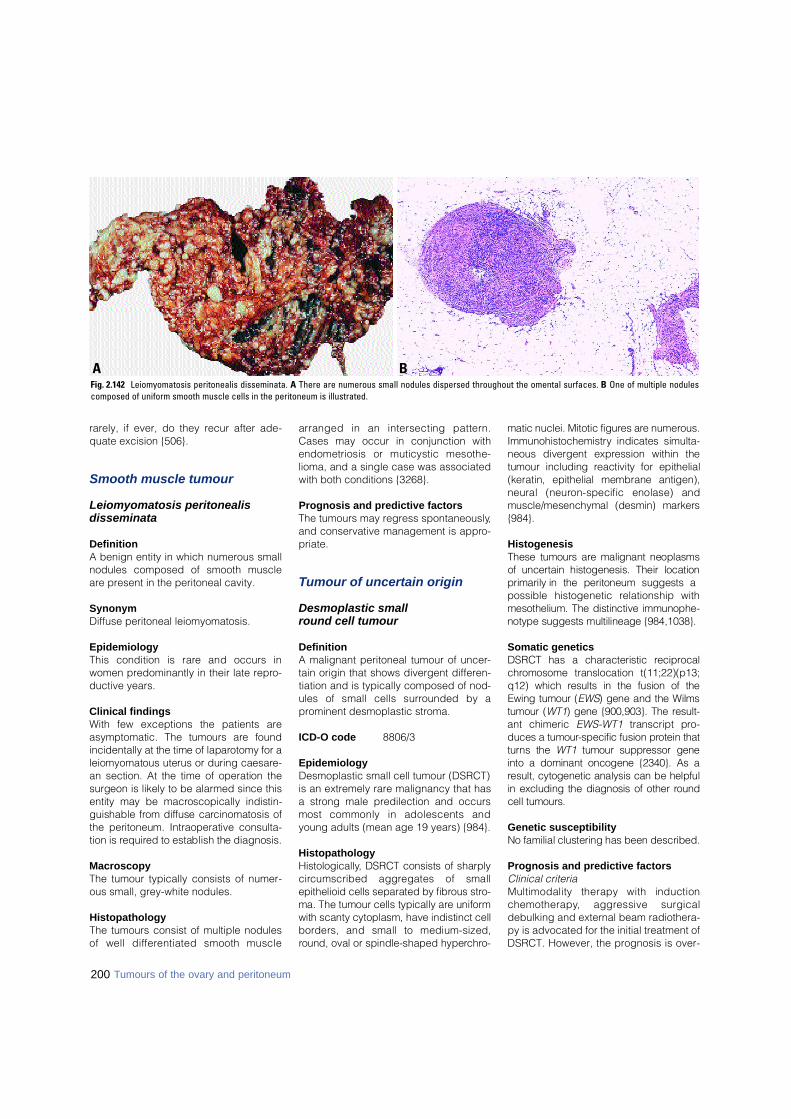
rarely, if ever, do they recur after ade-quate excision {506}.
Smooth muscle tumour
Leiomyomatosis peritonealis disseminata
DefinitionA benign entity in which numerous smallnodules composed of smooth muscleare present in the peritoneal cavity.
SynonymDiffuse peritoneal leiomyomatosis.
EpidemiologyThis condition is rare and occurs inwomen predominantly in their late repro-ductive years.
Clinical findingsWith few exceptions the patients areasymptomatic. The tumours are foundincidentally at the time of laparotomy for aleiomyomatous uterus or during caesare-an section. At the time of operation thesurgeon is likely to be alarmed since thisentity may be macroscopically indistin-guishable from diffuse carcinomatosis ofthe peritoneum. Intraoperative consulta-tion is re q u i red to establish the diagnosis.
MacroscopyThe tumour typically consists of numer-ous small, grey-white nodules.
HistopathologyThe tumours consist of multiple nodulesof well diff e rentiated smooth muscle
arranged in an intersecting pattern .Cases may occur in conjunction withendometriosis or muticystic mesothe-lioma, and a single case was associatedwith both conditions {3268}.
Prognosis and predictive factorsThe tumours may regress spontaneously,and conservative management is appro-priate.
Tumour of uncertain origin
Desmoplastic small round cell tumour
DefinitionA malignant peritoneal tumour of uncer-tain origin that shows divergent differen-tiation and is typically composed of nod-ules of small cells surrounded by aprominent desmoplastic stroma.
ICD-O code 8806/3
EpidemiologyDesmoplastic small cell tumour (DSRCT)is an extremely rare malignancy that hasa strong male predilection and occursmost commonly in adolescents andyoung adults (mean age 19 years) {984}.
HistopathologyH i s t o l o g i c a l l y, DSRCT consists of sharplyc i rcumscribed aggregates of smallepithelioid cells separated by fibrous stro-ma. The tumour cells typically are uniformwith scanty cytoplasm, have indistinct cellb o rders, and small to medium-sized,round, oval or spindle-shaped hyperc h ro-
matic nuclei. Mitotic figures are numero u s .I m m u n o h i s t o c h e m i s t ry indicates simulta-neous divergent expression within thetumour including reactivity for epithelial(keratin, epithelial membrane antigen),neural (neuron-specific enolase) andmuscle/mesenchymal (desmin) markers{ 9 8 4 } .
HistogenesisThese tumours are malignant neoplasmsof uncertain histogenesis. Their locationprimarily in the peritoneum suggests apossible histogenetic relationship withmesothelium. The distinctive immunophe-notype suggests multilineage {984,1038}.
Somatic genetics DSRCT has a characteristic re c i p ro c a lc h romosome translocation t(11;22)(p13;q12) which results in the fusion of theEwing tumour (E W S) gene and the Wilmstumour (W T 1) gene {900,903}. The re s u l t-ant chimeric E W S - W T 1 transcript pro-duces a tumour-specific fusion protein thatt u rns the W T 1 tumour suppressor geneinto a dominant oncogene {2340}. As aresult, cytogenetic analysis can be helpfulin excluding the diagnosis of other ro u n dcell tumours.
Genetic susceptibilityNo familial clustering has been described.
Prognosis and predictive factorsClinical criteriaMultimodality therapy with inductionc h e m o t h e r a p y, aggressive surgicaldebulking and external beam radiothera-py is advocated for the initial treatment ofDSRCT. However, the prognosis is over-
200 Tumours of the ovary and peritoneum
BAFig. 2.142 Leiomyomatosis peritonealis disseminata. A There are numerous small nodules dispersed throughout the omental surfaces. B One of multiple nodulescomposed of uniform smooth muscle cells in the peritoneum is illustrated.
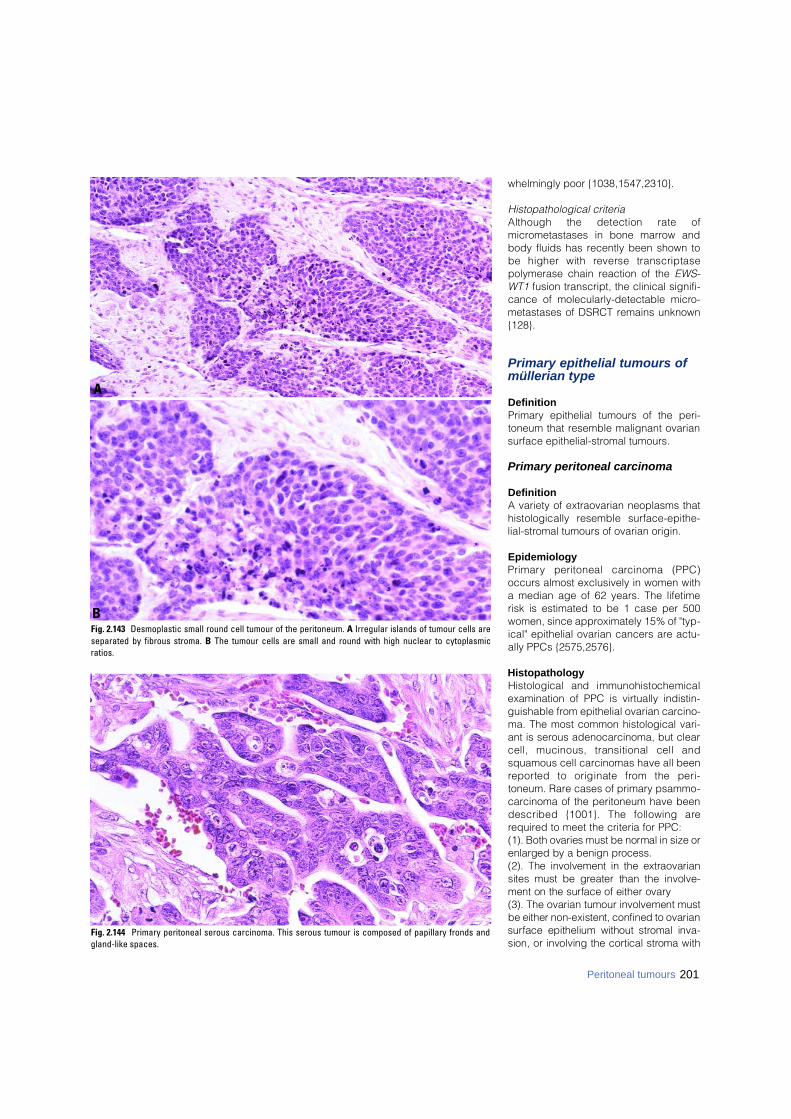
whelmingly poor {1038,1547,2310}.
Histopathological criteriaAlthough the detection rate ofmicrometastases in bone marrow andbody fluids has recently been shown tobe higher with reverse transcriptasepolymerase chain reaction of the EWS-WT1 fusion transcript, the clinical signifi-cance of molecularly-detectable micro-metastases of DSRCT remains unknown{128}.
Primary epithelial tumours of müllerian type
DefinitionPrimary epithelial tumours of the peri-toneum that resemble malignant ovariansurface epithelial-stromal tumours.
Primary peritoneal carcinoma
DefinitionA variety of extraovarian neoplasms thathistologically resemble surf a c e - e p i t h e-lial-stromal tumours of ovarian origin.
EpidemiologyP r i m a ry peritoneal carcinoma (PPC)occurs almost exclusively in women witha median age of 62 years. The lifetimerisk is estimated to be 1 case per 500women, since approximately 15% of "typ-ical" epithelial ovarian cancers are actu-ally PPCs {2575,2576}.
HistopathologyHistological and immunohistochemicalexamination of PPC is virtually indistin-guishable from epithelial ovarian carcino-ma. The most common histological vari-ant is serous adenocarcinoma, but clearcell, mucinous, transitional cell andsquamous cell carcinomas have all beenre p o rted to originate from the peri-toneum. Rare cases of primary psammo-carcinoma of the peritoneum have beendescribed {1001}. The following arerequired to meet the criteria for PPC:(1). Both ovaries must be normal in size orenlarged by a benign pro c e s s .(2). The involvement in the extraovariansites must be greater than the involve-ment on the surface of either ovary(3). The ovarian tumour involvement mustbe either non-existent, confined to ovarians u rface epithelium without stromal inva-sion, or involving the cortical stroma with
Fig. 2.144 Primary peritoneal serous carcinoma. This serous tumour is composed of papillary fronds andgland-like spaces.
Fig. 2.143 Desmoplastic small round cell tumour of the peritoneum. A Irregular islands of tumour cells areseparated by fibrous stroma. B The tumour cells are small and round with high nuclear to cytoplasmicratios.
B
A
201Peritoneal tumours
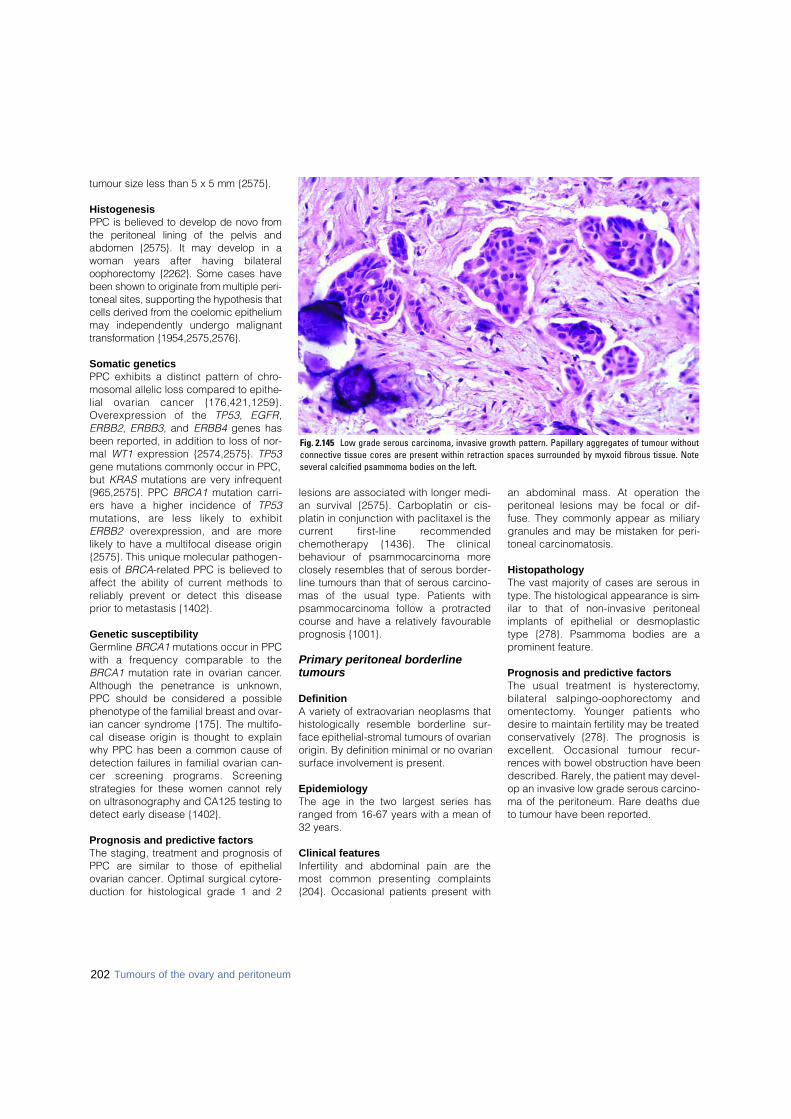
tumour size less than 5 x 5 mm {2575}.
HistogenesisPPC is believed to develop de novo fro mthe peritoneal lining of the pelvis andabdomen {2575}. It may develop in awoman years after having bilateralo o p h o rectomy {2262}. Some cases havebeen shown to originate from multiple peri-toneal sites, supporting the hypothesis thatcells derived from the coelomic epitheliummay independently undergo malignantt r a n s f o rmation {1954,2575,2576}.
Somatic geneticsPPC exhibits a distinct pattern of chro-mosomal allelic loss compared to epithe-lial ovarian cancer {176,421,1259}.O v e re x p ression of the T P 5 3, E G F R,ERBB2, ERBB3, and ERBB4 genes hasbeen reported, in addition to loss of nor-mal WT1 expression {2574,2575}. TP53gene mutations commonly occur in PPC,but KRAS mutations are very infrequent{965,2575}. PPC BRCA1 mutation carri-ers have a higher incidence of TP53mutations, are less likely to exhibitERBB2 overexpression, and are morelikely to have a multifocal disease origin{2575}. This unique molecular pathogen-esis of BRCA-related PPC is believed toaffect the ability of current methods toreliably prevent or detect this diseaseprior to metastasis {1402}.
Genetic susceptibilityG e rmline B R C A 1 mutations occur in PPCwith a frequency comparable to theB R C A 1 mutation rate in ovarian cancer.Although the penetrance is unknown,PPC should be considered a possiblephenotype of the familial breast and ovar-ian cancer syndrome {175}. The multifo-cal disease origin is thought to explainwhy PPC has been a common cause ofdetection failures in familial ovarian can-cer screening programs. Scre e n i n gstrategies for these women cannot re l yon ultrasonography and CA125 testing todetect early disease {1402}.
Prognosis and predictive factorsThe staging, treatment and prognosis ofPPC are similar to those of epithelialovarian cancer. Optimal surgical cytore-duction for histological grade 1 and 2
lesions are associated with longer medi-an survival {2575}. Carboplatin or cis-platin in conjunction with paclitaxel is thec u r rent first-line re c o m m e n d e dchemotherapy {1436}. The clinicalbehaviour of psammocarcinoma moreclosely resembles that of serous border-line tumours than that of serous carcino-mas of the usual type. Patients withpsammocarcinoma follow a protractedcourse and have a relatively favourableprognosis {1001}.
Primary peritoneal borderlinetumours
DefinitionA variety of extraovarian neoplasms thathistologically resemble borderline sur-face epithelial-stromal tumours of ovarianorigin. By definition minimal or no ovariansurface involvement is present.
EpidemiologyThe age in the two largest series hasranged from 16-67 years with a mean of32 years.
Clinical featuresInfertility and abdominal pain are themost common presenting complaints{204}. Occasional patients present with
an abdominal mass. At operation theperitoneal lesions may be focal or dif-fuse. They commonly appear as miliarygranules and may be mistaken for peri-toneal carcinomatosis.
HistopathologyThe vast majority of cases are serous intype. The histological appearance is sim-ilar to that of non-invasive peritonealimplants of epithelial or desmoplastictype {278}. Psammoma bodies are aprominent feature.
Prognosis and predictive factorsThe usual treatment is hystere c t o m y,bilateral salpingo-oophorectomy ando m e n t e c t o m y. Younger patients whodesire to maintain fertility may be treatedconservatively {278}. The prognosis isexcellent. Occasional tumour re c u r-rences with bowel obstruction have beendescribed. Rarely, the patient may devel-op an invasive low grade serous carcino-ma of the peritoneum. Rare deaths dueto tumour have been reported.
Fig. 2.145 Low grade serous carcinoma, invasive growth pattern. Papillary aggregates of tumour withoutconnective tissue cores are present within retraction spaces surrounded by myxoid fibrous tissue. Noteseveral calcified psammoma bodies on the left.
202 Tumours of the ovary and peritoneum
CHAPTER 3
Tumours of the FallopianTube and Uterine Ligaments
Tumours of the fallopian tube are much less common than thecorresponding ovarian neoplasms; however, histologically thesame surface epithelial-stromal tumour subtypes are recog-nized. Sex cord-stromal and germ cell tumours are rare.H y d a t i d i f o rm moles and gestational choriocarcinoma areuncommon complications of tubal ectopic pregnancy. Thewolffian adnexal tumour is also infrequent and typically occursin the leaves of the broad ligament.
The risk factors appear similar to those of the ovary. Fallopiantube carcinomas are a component of the hereditary breast-ovarian cancer syndrome caused by BRCA1 and BRCA2germline mutations.
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
204 Tumours of the fallopian tube and uterine ligaments
Epithelial tumoursMalignant
Serous adenocarcinoma 8 4 4 1 / 31
Mucinous adenocarcinoma 8480/3Endometrioid adenocarcinoma 8380/3Clear cell adenocarcinoma 8310/3Transitional cell carcinoma 8120/3Squamous cell carcinoma 8070/3Undifferentiated carcinoma 8020/3Others
Borderline tumour (of low malignant potential)Serous borderline tumour 8442/1Mucinous borderline tumour 8472/1Endometrioid borderline tumour 8380/1Others
Carcinoma in situ (specify type)Benign tumours
Papilloma (specify type)Cystadenoma (specify type)Adenofibroma (specify type)Cystadenofibroma (specify type)Metaplastic papillary tumourEndometrioid polypOthers
Tumour-like epithelial lesionsTubal epithelial hyperplasiaSalpingitis isthmica nodosaEndosalpingiosis
Mixed epithelial-mesenchymal tumoursMalignant müllerian mixed tumour 8950/3(carcinosarcoma; metaplastic carcinoma)Adenosarcoma 8933/3
Soft tissue tumoursLeiomyosarcoma 8890/3Leiomyoma 8890/0Others
Mesothelial tumoursAdenomatoid tumour 9054/0
Germ cell tumoursTeratoma
Mature 9080/0Immature 9080/3
OthersTrophoblastic disease
Choriocarcinoma 9100/3Placental site trophoblastic tumour 9104/1Hydatidiform mole 9100/0Placental site noduleOthers
Lymphoid and haematopoetic tumoursMalignant lymphomaLeukaemia
Secondary tumours
WHO histological classification of tumours of the fallopian tube
Epithelial tumours of müllerian typeSerous adenocarcinoma 8460/3Endometrioid adenocarcinoma 8380/3Mucinous adenocarcinoma 8480/3Clear cell adenocarcinoma 8310/3Borderline tumour (of low malignant potential), (specify type)Adenoma and cystadenoma (specify type)
Miscellaneous tumoursWolffian adnexal tumour 9110/1Ependymona 9391/3
Papillary cystadenoma (with von-Hippel-Lindau disease) 8450/0Uterus-like massAdenosarcoma 8933/3Others
Mesenchymal tumoursMalignant Benign
Secondary tumours
WHO histological classification of tumours of the broad ligamentand other uterine ligaments

_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The regional lymph nodes are the hypogastric (obturator), common iliac, external iliac, lateral sacral, para-aortic, and inguinal nodes.
TNM and FIGO classification 1,2
T – Primary TumourTNM FIGOCategories StagesTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis 0 Carcinoma in situ (preinvasive carcinoma)T1 I Tumour confined to fallopian tube(s)T1a IA Tumour limited to one tube, without penetrating
the serosal surfaceT1b IB Tumour limited to both tubes, without penetrating
the serosal surfaceT1c IC Tumour limited to one or both tube(s) with extension
onto or through the tubal serosa, or with malignantcells in ascites or peritoneal washings
T2 II Tumour involves one or both fallopian tube(s) withpelvic extension
T2a IIA Extension and/or metastasis to uterus and/or ovariesT2b IIB Extension to other pelvic structuresT2c IIC Pelvic extension (2a or 2b) with malignant cells in
ascites or peritoneal washingsT3 and/or N1 III Tumour involves one or both fallopian tube(s) with
peritoneal implants outside the pelvis and/or positive regional lymph nodes
T3a IIIA Microscopic peritoneal metastasis outside the pelvisT3b IIIB Macroscopic peritoneal metastasis outside the
pelvis 2 cm or less in greatest dimensionT3c and/or N1 IIIC Peritoneal metastasis more than 2 cm in greatest
dimension and/or positive regional lymph nodes
M1 IV Distant metastasis (excludes peritoneal metastasis)Note: Liver capsule metastasis is T3/stage III, liver parenchymal metastasis,M1/stage IV. Pleural effusion must have positive cytology for M1/stage IV.
N – Regional Lymph Nodes 3
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage 0 Tis N0 M0Stage IA T1a N0 M0Stage IB T1b N0 M0Stage IC T1c N0 M0Stage IIA T2a N0 M0Stage IIB T2b N0 M0Stage IIC T2c N0 M0Stage IIIA T3a N0 M0Stage IIIB T3b N0 M0Stage IIIC T3c N0 M0
Any T N1 M0Stage IV Any T Any N M1
TNM and FIGO classification of carcinomas of the fallopian tube
205
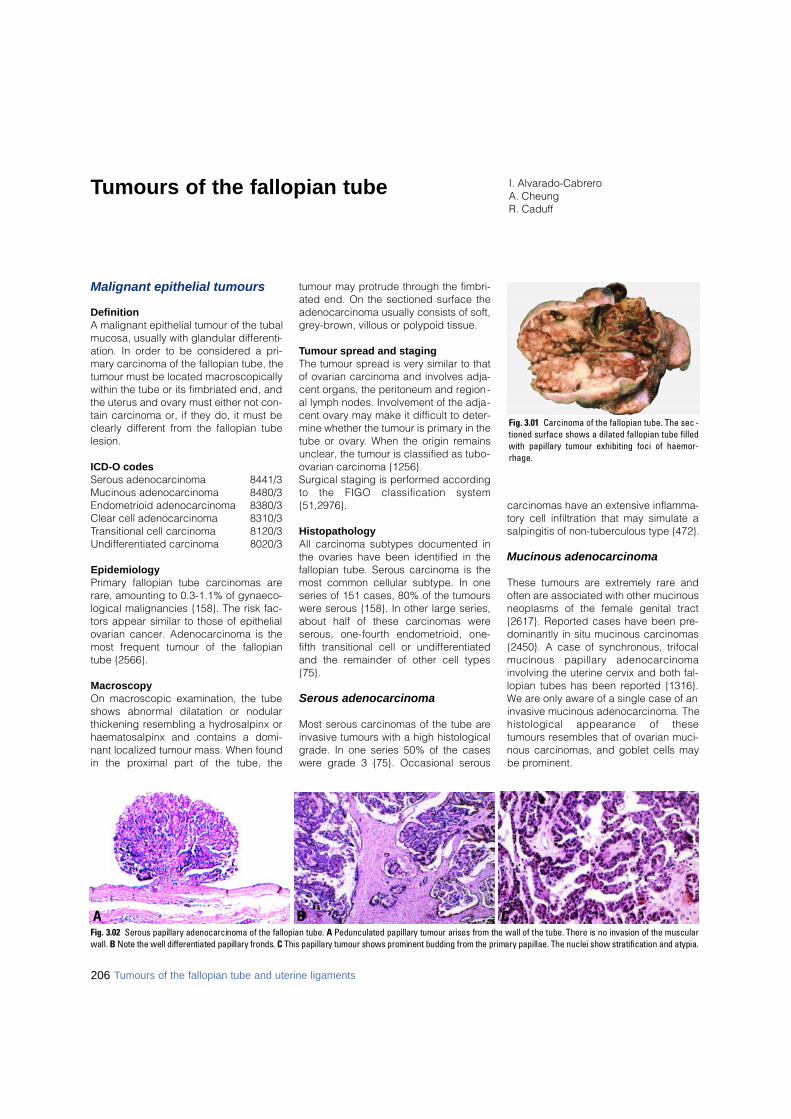
Tumours of the fallopian tube
Malignant epithelial tumours
DefinitionA malignant epithelial tumour of the tubalmucosa, usually with glandular differenti-ation. In order to be considered a pri-mary carcinoma of the fallopian tube, thetumour must be located macroscopicallywithin the tube or its fimbriated end, andthe uterus and ovary must either not con-tain carcinoma or, if they do, it must beclearly different from the fallopian tubelesion.
ICD-O codesSerous adenocarcinoma 8441/3Mucinous adenocarcinoma 8480/3Endometrioid adenocarcinoma 8380/3Clear cell adenocarcinoma 8310/3Transitional cell carcinoma 8120/3Undifferentiated carcinoma 8020/3
EpidemiologyPrimary fallopian tube carcinomas arerare, amounting to 0.3-1.1% of gynaeco-logical malignancies {158}. The risk fac-tors appear similar to those of epithelialovarian cancer. Adenocarcinoma is themost frequent tumour of the fallopiantube {2566}.
MacroscopyOn macroscopic examination, the tubeshows abnormal dilatation or nodularthickening resembling a hydrosalpinx orhaematosalpinx and contains a domi-nant localized tumour mass. When foundin the proximal part of the tube, the
tumour may protrude through the fimbri-ated end. On the sectioned surface theadenocarcinoma usually consists of soft,grey-brown, villous or polypoid tissue.
Tumour spread and stagingThe tumour spread is very similar to thatof ovarian carcinoma and involves adja-cent organs, the peritoneum and region-al lymph nodes. Involvement of the adja-cent ovary may make it difficult to deter-mine whether the tumour is primary in thetube or ovary. When the origin remainsunclear, the tumour is classified as tubo-ovarian carcinoma {1256}.Surgical staging is performed accordingto the FIGO classification system{51,2976}.
HistopathologyAll carcinoma subtypes documented inthe ovaries have been identified in thefallopian tube. Serous carcinoma is themost common cellular subtype. In oneseries of 151 cases, 80% of the tumourswere serous {158}. In other large series,about half of these carcinomas weres e rous, one-fourth endometrioid, one-fifth transitional cell or undifferentiatedand the remainder of other cell types{75}.
Serous adenocarcinoma
Most serous carcinomas of the tube areinvasive tumours with a high histologicalgrade. In one series 50% of the caseswere grade 3 {75}. Occasional serous
carcinomas have an extensive inflamma-tory cell infiltration that may simulate asalpingitis of non-tuberculous type {472}.
Mucinous adenocarcinoma
These tumours are extremely rare andoften are associated with other mucinousneoplasms of the female genital tract{2617}. Reported cases have been pre-dominantly in situ mucinous carcinomas{2450}. A case of synchronous, trifocalmucinous papillary adenocarc i n o m ainvolving the uterine cervix and both fal-lopian tubes has been reported {1316}.We are only aware of a single case of aninvasive mucinous adenocarcinoma. Thehistological appearance of thesetumours resembles that of ovarian muci-nous carcinomas, and goblet cells maybe prominent.
Fig. 3.01 Carcinoma of the fallopian tube. The sec -tioned surface shows a dilated fallopian tube filledwith papillary tumour exhibiting foci of haemor-rhage.
B CAFig. 3.02 Serous papillary adenocarcinoma of the fallopian tube. A Pedunculated papillary tumour arises from the wall of the tube. There is no invasion of the muscularwall. B Note the well differentiated papillary fronds. C This papillary tumour shows prominent budding from the primary papillae. The nuclei show stratification and atypia.
I. Alvarado-CabreroA. CheungR. Caduff
206 Tumours of the fallopian tube and uterine ligaments
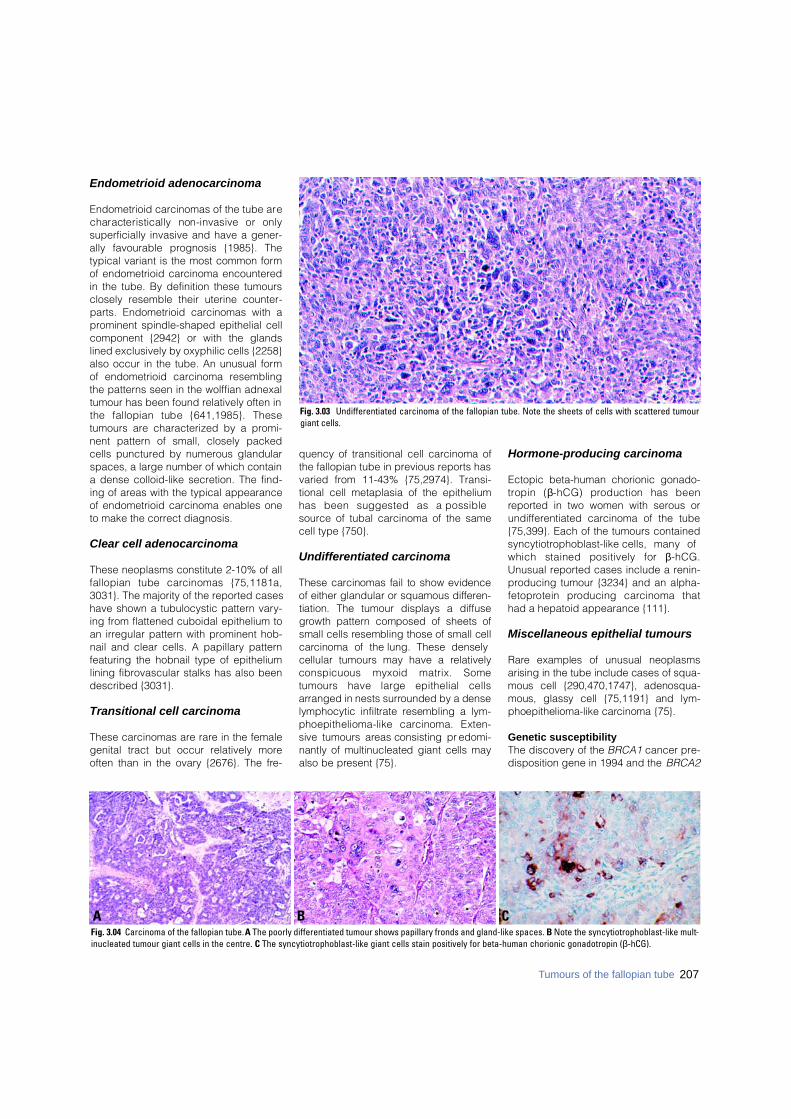
Endometrioid adenocarcinoma
Endometrioid carcinomas of the tube arecharacteristically non-invasive or onlysuperficially invasive and have a gener-ally favourable prognosis {1985}. Thetypical variant is the most common formof endometrioid carcinoma encounteredin the tube. By definition these tumoursclosely resemble their uterine counter-parts. Endometrioid carcinomas with aprominent spindle-shaped epithelial cellcomponent {2942} or with the glandslined exclusively by oxyphilic cells {2258}also occur in the tube. An unusual formof endometrioid carcinoma resemblingthe patterns seen in the wolffian adnexaltumour has been found relatively often inthe fallopian tube {641,1985}. Thesetumours are characterized by a promi-nent pattern of small, closely packedcells punctured by numerous glandularspaces, a large number of which containa dense colloid-like secretion. The find-ing of areas with the typical appearanceof endometrioid carcinoma enables oneto make the correct diagnosis.
Clear cell adenocarcinoma
These neoplasms constitute 2-10% of allfallopian tube carcinomas {75,1181a,3031}. The majority of the reported caseshave shown a tubulocystic pattern vary-ing from flattened cuboidal epithelium toan irregular pattern with prominent hob-nail and clear cells. A papillary patternfeaturing the hobnail type of epitheliumlining fibrovascular stalks has also beendescribed {3031}.
Transitional cell carcinoma
These carcinomas are rare in the femalegenital tract but occur relatively moreoften than in the ovary {2676}. The fre-
quency of transitional cell carcinoma ofthe fallopian tube in previous reports hasvaried from 11-43% {75,2974}. Transi-tional cell metaplasia of the epitheliumhas been suggested as a possiblesource of tubal carcinoma of the samecell type {750}.
Undifferentiated carcinoma
These carcinomas fail to show evidenceof either glandular or squamous diff e re n-tiation. The tumour displays a diff u s eg rowth pattern composed of sheets ofsmall cells resembling those of small cellc a rcinoma of the lung. These denselycellular tumours may have a re l a t i v e l yconspicuous myxoid matrix. Sometumours have large epithelial cellsarranged in nests surrounded by a denselymphocytic infiltrate resembling a lym-phoepithelioma-like carcinoma. Exten-sive tumours areas consisting pre d o m i-nantly of multinucleated giant cells mayalso be present {75}.
Hormone-producing carcinoma
Ectopic beta-human chorionic gonado-t ropin (β-hCG) production has beenreported in two women with serous orundifferentiated carcinoma of the tube{75,399}. Each of the tumours containeds y n c y t i o t rophoblast-like cells, many ofwhich stained positively for β- h C G .Unusual reported cases include a renin-producing tumour {3234} and an alpha-f e t o p rotein producing carcinoma thathad a hepatoid appearance {111}.
Miscellaneous epithelial tumours
R a re examples of unusual neoplasmsarising in the tube include cases of squa-mous cell {290,470,1747}, adenosqua-mous, glassy cell {75,1191} and lym-phoepithelioma-like carcinoma {75}.
Genetic susceptibilityThe discovery of the BRCA1 cancer pre-disposition gene in 1994 and the BRCA2
B CAFig. 3.04 Carcinoma of the fallopian tube. A The poorly differentiated tumour shows papillary fronds and gland-like spaces. B Note the syncytiotrophoblast-like mult-inucleated tumour giant cells in the centre. C The syncytiotrophoblast-like giant cells stain positively for beta-human chorionic gonadotropin (β-hCG).
Fig. 3.03 Undifferentiated carcinoma of the fallopian tube. Note the sheets of cells with scattered tumourgiant cells.
207Tumours of the fallopian tube

cancer predisposition gene in 1995 hasallowed the identification of a group ofwomen who are at a greatly increasedrisk of developing breast and ovariancancer {8,499}. Two previous series inwhich 5% and 11% respectively ofpatients with tubal cancer also hadbreast carcinoma suggest an associationbetween breast cancer and tubal carci-noma {75,2225}. Recently, several high-risk "breast-ovarian cancer families" withB R C A 1 mutations and fallopian tubecancer have been reported. Additionally,a family history of fallopian tube cancerwas found to be predictive of the pres-ence of a BRCA1 mutation in a panel of26 Canadian "breast-ovarian cancer fam-ilies" {2939}. A slightly increased risk of
ovarian cancer and of early-onset breastcancer was found in the first-degree rel-atives of the fallopian tube cancer cases{144}. Thus, fallopian tube carcinomashould be considered to be a clinicalcomponent of the hereditary breast-ovar-ian cancer syndrome and may be asso-ciated with BRCA1 and BRCA2 muta-tions. See Chapter 8.
Prognosis and predictive factorsThe surgical stage is an independentp rognostic factor {75,158} and is criticalfor determining whether adjuvant therapyis appropriate. Stage I carcinomas thatoccur in the tubal fimbriae appear to havea worse prognosis than stage I tubal car-cinomas that are nonfimbrial {74}.
Borderline epithelial tumours
Borderline epithelial tumours of the fal-lopian tube are rare and include cases ofs e rous, mucinous and endometrioidtypes {74}. Borderline serous tumoursinvolve the tube, including its fimbriatedportion, and have histological featuressimilar to those of the ovary {74,1421,3257}. Mucinous tumours are sometimesassociated with mucinous metaplasia ofthe fallopian tube or the Peutz-Jegherss y n d rome {1806,2617}. Patients thathave multiple organ involvement orpseudomyxoma peritonei may have ametastatic lesion to the tube, and in allcases the appendix needs to be ruledout as a source.
BAFig. 3.05 Endometrioid carcinoma of the fallopian tube. A Closely packed tubules of endometrioid carcinoma are present adjacent to a focus of endometriosis com-posed of larger glands present on the left. B The tumour forms closely packed glands lined by pseudostratified epithelium.
Fig. 3.06 Lymphoepithelial-like carcinoma. The tumour is composed of paleepithelial cells with large vesicular nuclei and prominent nucleoli. Note the lym-phocytic infiltration.
Fig. 3.07 Serous borderline tumour. The tumour consists of papillae with connec-tive tissue cores lined by epithelium showing cellular stratification and tufting,resembling its ovarian counterpart.
208 Tumours of the fallopian tube and uterine ligaments
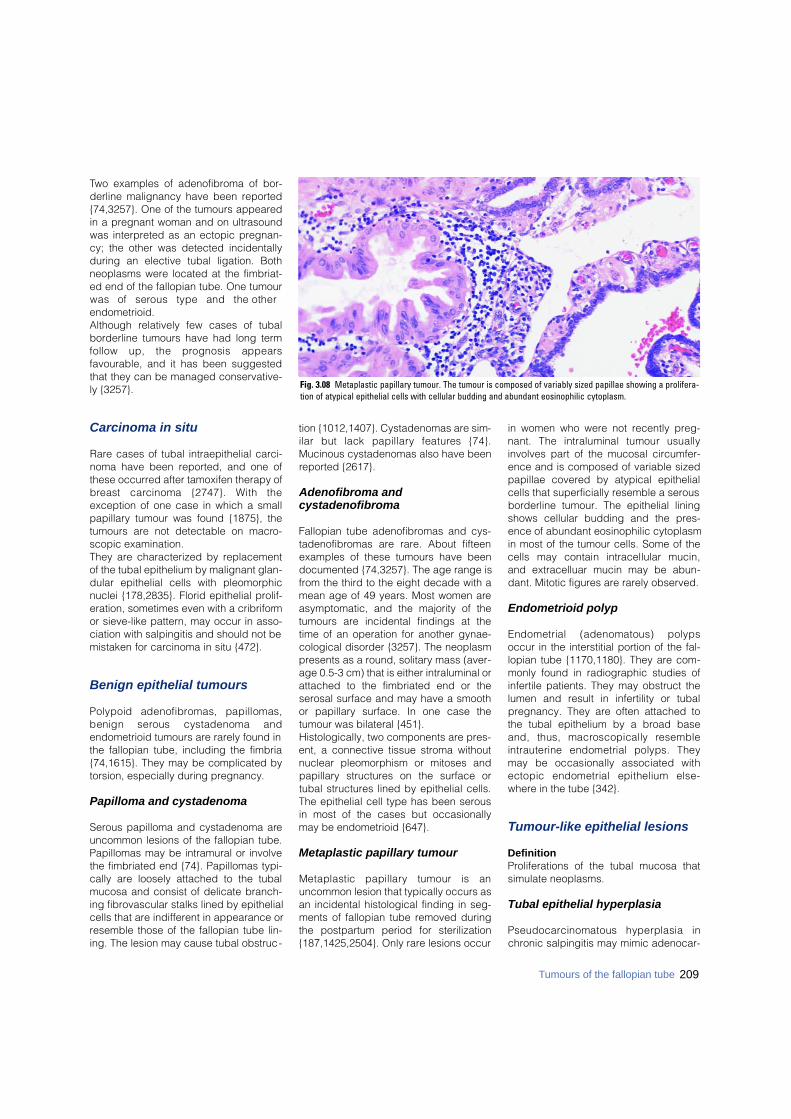
Two examples of adenofibroma of bor-derline malignancy have been reported{74,3257}. One of the tumours appearedin a pregnant woman and on ultrasoundwas interpreted as an ectopic pregnan-cy; the other was detected incidentallyduring an elective tubal ligation. Bothneoplasms were located at the fimbriat-ed end of the fallopian tube. One tumourwas of serous type and the otherendometrioid. Although relatively few cases of tubalborderline tumours have had long termfollow up, the prognosis appearsfavourable, and it has been suggestedthat they can be managed conservative-ly {3257}.
Carcinoma in situ
Rare cases of tubal intraepithelial carci-noma have been reported, and one ofthese occurred after tamoxifen therapy ofb reast carcinoma {2747}. With theexception of one case in which a smallpapillary tumour was found {1875}, thetumours are not detectable on macro-scopic examination. They are characterized by replacementof the tubal epithelium by malignant glan-dular epithelial cells with pleomorphicnuclei {178,2835}. Florid epithelial prolif-eration, sometimes even with a cribriformor sieve-like pattern, may occur in asso-ciation with salpingitis and should not bemistaken for carcinoma in situ {472}.
Benign epithelial tumours
Polypoid adenofibromas, papillomas,benign serous cystadenoma andendometrioid tumours are rarely found inthe fallopian tube, including the fimbria{74,1615}. They may be complicated bytorsion, especially during pregnancy.
Papilloma and cystadenoma
Serous papilloma and cystadenoma areuncommon lesions of the fallopian tube.Papillomas may be intramural or involvethe fimbriated end {74}. Papillomas typi-cally are loosely attached to the tubalmucosa and consist of delicate branch-ing fibrovascular stalks lined by epithelialcells that are indifferent in appearance orresemble those of the fallopian tube lin-ing. The lesion may cause tubal obstruc-
tion {1012,1407}. Cystadenomas are sim-ilar but lack papillary features {74}.Mucinous cystadenomas also have beenreported {2617}.
Adenofibroma and cystadenofibroma
Fallopian tube adenofibromas and cys-tadenofibromas are rare. About fifteenexamples of these tumours have beendocumented {74,3257}. The age range isfrom the third to the eight decade with amean age of 49 years. Most women areasymptomatic, and the majority of thetumours are incidental findings at thetime of an operation for another gynae-cological disorder {3257}. The neoplasmpresents as a round, solitary mass (aver-age 0.5-3 cm) that is either intraluminal orattached to the fimbriated end or theserosal surface and may have a smoothor papillary surface. In one case thetumour was bilateral {451}.Histologically, two components are pres-ent, a connective tissue stroma withoutnuclear pleomorphism or mitoses andpapillary structures on the surface ortubal structures lined by epithelial cells.The epithelial cell type has been serousin most of the cases but occasionallymay be endometrioid {647}.
Metaplastic papillary tumour
Metaplastic papillary tumour is anuncommon lesion that typically occurs asan incidental histological finding in seg-ments of fallopian tube removed duringthe postpartum period for sterilization{187,1425,2504}. Only rare lesions occur
in women who were not recently preg-nant. The intraluminal tumour usuallyinvolves part of the mucosal circumfer-ence and is composed of variable sizedpapillae covered by atypical epithelialcells that superficially resemble a serousborderline tumour. The epithelial liningshows cellular budding and the pres-ence of abundant eosinophilic cytoplasmin most of the tumour cells. Some of thecells may contain intracellular mucin,and extracelluar mucin may be abun-dant. Mitotic figures are rarely observed.
Endometrioid polyp
Endometrial (adenomatous) polypsoccur in the interstitial portion of the fal-lopian tube {1170,1180}. They are com-monly found in radiographic studies ofinfertile patients. They may obstruct thelumen and result in infertility or tubalpregnancy. They are often attached tothe tubal epithelium by a broad baseand, thus, macroscopically re s e m b l eintrauterine endometrial polyps. Theymay be occasionally associated withectopic endometrial epithelium else-where in the tube {342}.
Tumour-like epithelial lesions
DefinitionProliferations of the tubal mucosa thatsimulate neoplasms.
Tubal epithelial hyperplasia
P s e u d o c a rcinomatous hyperplasia inchronic salpingitis may mimic adenocar-
209Tumours of the fallopian tube
Fig. 3.08 Metaplastic papillary tumour. The tumour is composed of variably sized papillae showing a prolifera-tion of atypical epithelial cells with cellular budding and abundant eosinophilic cytoplasm.

cinoma histologically because of thepseudoglandular and cribriform perme-ation of the tubal wall by hyperplasticepithelium and the florid mesothelialhyperplasia {472}. The typically youngage of the patients, the presence ofmarked chronic inflammation, theabsence of a macroscopically detectedtumour or solid epithelial proliferation, themildness of the nuclear atypia and thepaucity of mitotic figures facilitate the dif-ferential diagnosis. Recently, atypical hyperplasia of the fal-lopian tube has been observed inpatients on tamoxifen therapy for breastcancer {2244}.
Salpingitis isthmica nodosa
Salpingitis isthmica nodosa is a manifes-tation of tubal diverticulosis and is asso-ciated with female infertility and ectopicpregnancy {1064}. These nodules in theisthmus are composed of hypertrophicmyosalpinx and glandular spaces linedby tubal epithelium.
Endosalpingiosis
Endosalpingiosis is the benign transfor-mation of the mesothelium into tubalepithelium with ciliated and secretorycells. Psammoma bodies and atypicalchanges may be found {2919}.Endosalpingiosis is distinguished fromendometriosis by the absence ofendometrial stroma since tubal typeepithelium can also occur occasionally inendometriosis. Endosalpingiosis occursin the peritoneum and may involve theserosal surfaces of the uterus and itsadnexa. Endosalpingiosis may either present aspelvic pain or may be discovered as an
incidental finding {659,1591}. Rare l y,endosalpingiosis can present clinicallyas a cystic mass and can be confusedwith a neoplasm on macroscopic exami-nation {518a}.
Mixed epithelial and mesenchymal tumours
DefinitionNeoplasms composed of an admixture ofneoplastic epithelial and mesenchymalelements. Each of these componentsmay be either benign or malignant.
ICD-O codesMalignant müllerian mixed tumour 8 9 5 0 / 3Adenosarcoma 8933/3
Malignant müllerian mixed tumour
As a group, these malignancies areuncommon. The fallopian tube is theleast common site for malignant müller-ian mixed tumours in the female genitalsystem, accounting for less than 4% ofthe reported cases {1124}. Patients arealmost always postmenopausal (meanage, 57 years) and usually present withabdominal pain, atypical genital bleed-ing or abdominal distension {1124,1284}.The histological appearance of thesetumours resembles that of ovarian malig-nant müllerian mixed tumour. The prog-nosis is poor {1124,1284,3079}.
AdenosarcomaThis tumour is exceedingly uncommon.Only one well documented case thatarose in the fimbriated end of the tubeand recurred on the pelvic wall has beenreported {1036}. Another example of atubal tumour of this type was character-ized by marked adenoacanthotic atypiaof its epithelial component {2605}.
Gestational trophoblastic disease
DefinitionA heterogeneous group of gestationaland neoplastic conditions arising fromtrophoblast, including molar gestationsand trophoblastic tumours.
ICD-O codesChoriocarcinoma 9100/3Placental site trophoblastic tumour 9 1 0 4 / 1H y d a t i d i f o rm mole 9 1 0 0 / 0
Choriocarcinoma
Tubal choriocarcinomas account forapproximately 4% of all choriocarcino-mas {660}. Most of the cases are discov-ered by chance during an ectopic preg-nancy, but about 40% present with anenlarging adnexal mass {2078}.Histological examination shows typicalfeatures of gestational choriocarcinoma.In the older literature before the advent ofm o d e rn chemotherapy, choriocarc i n o-mas associated with ectopic pregnancyw e re frequently very aggressive, and75% showed metastases at the time ofdiagnosis. The response to modernchemotherapy generally has beenencouraging {1717,1953}.
Placental site trophoblastictumour
This neoplasm is composed predomi-nantly of intermediate trophoblast. It isgenerally benign but occasionally maybe highly malignant {1540}. To date, onlyone case of tubal placental site tro-phoblastic tumour has been reported{2810}.
Hydatidiform mole
Approximately thirty tubal hydatidiformmoles have been reported {1999}; how-ever, only four valid examples of thislesion were accepted in 1981 {2078}.Those authors concluded that theremaining "moles" were actually ectopicpregnancies with villous hydrops. Thistumour usually occurs as an isolatedgrowth, but it may be associated with anintrauterine pregnancy {1048}. The histo-logical appearance may be that of acomplete, partial or invasive mole with clear
210 Tumours of the fallopian tube and uterine ligaments
Fig. 3.09 Prominent mucosal hyperplasia. A glandu-lar proliferation producing a cribriform pattern simu-lates a neoplastic process within the plicae of thefallopian tube.
Fig. 3.10 Malignant müllerian mixed tumour of fal-lopian tube. The fallopian tube is distended and dis-torted by a multinodular tumour mass that hasextended through the serosa.
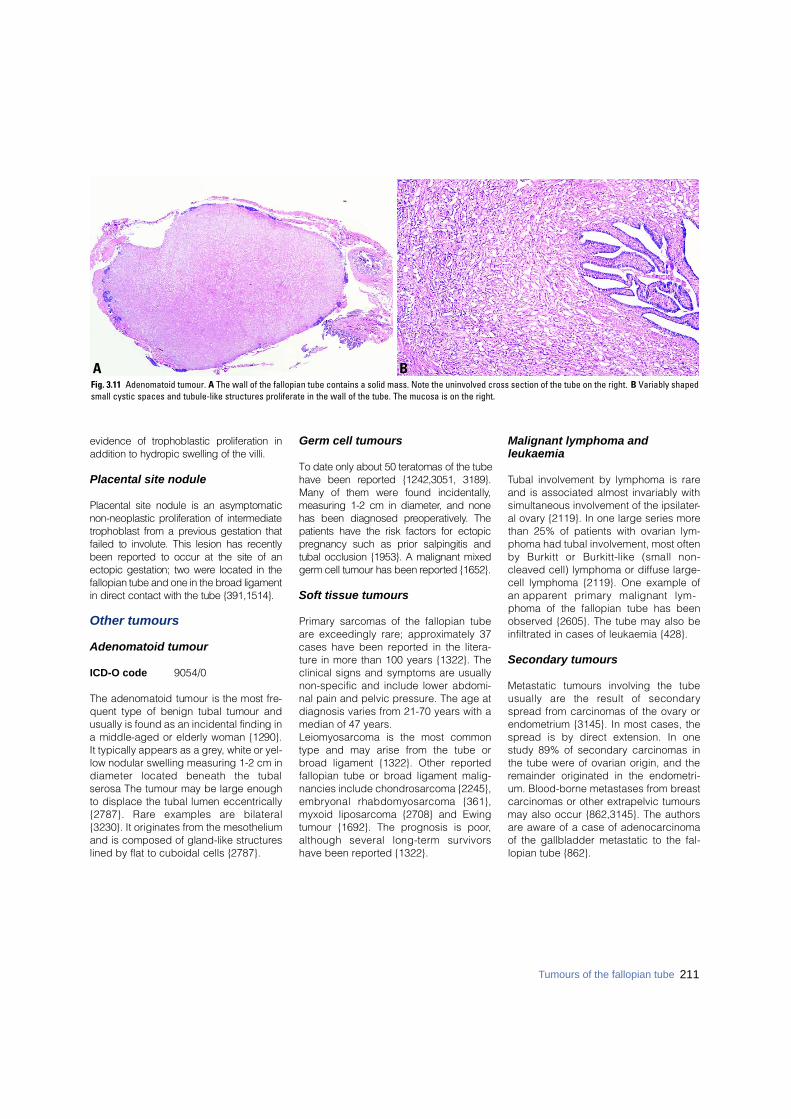
evidence of trophoblastic proliferation inaddition to hydropic swelling of the villi.
Placental site nodule
Placental site nodule is an asymptomaticnon-neoplastic proliferation of interm e d i a t et rophoblast from a previous gestation thatfailed to involute. This lesion has re c e n t l ybeen re p o rted to occur at the site of anectopic gestation; two were located in thefallopian tube and one in the broad ligamentin direct contact with the tube {391,1514}.
Other tumours
Adenomatoid tumour
ICD-O code 9054/0
The adenomatoid tumour is the most fre-quent type of benign tubal tumour andusually is found as an incidental finding ina middle-aged or elderly woman {1290}.It typically appears as a gre y, white or yel-low nodular swelling measuring 1-2 cm indiameter located beneath the tubals e rosa The tumour may be large enoughto displace the tubal lumen eccentrically{2787}. Rare examples are bilateral{3230}. It originates from the mesotheliumand is composed of gland-like structure slined by flat to cuboidal cells {2787}.
Germ cell tumours
To date only about 50 teratomas of the tubehave been re p o rted {1242,3051, 3189}.Many of them were found incidentally,measuring 1-2 cm in diameter, and nonehas been diagnosed pre o p e r a t i v e l y. Thepatients have the risk factors for ectopicp regnancy such as prior salpingitis andtubal occlusion {1953}. A malignant mixedg e rm cell tumour has been re p o rted {1652}.
Soft tissue tumours
Primary sarcomas of the fallopian tubeare exceedingly rare; approximately 37cases have been reported in the litera-ture in more than 100 years {1322}. Theclinical signs and symptoms are usuallynon-specific and include lower abdomi-nal pain and pelvic pressure. The age atdiagnosis varies from 21-70 years with amedian of 47 years. Leiomyosarcoma is the most commontype and may arise from the tube orbroad ligament {1322}. Other reportedfallopian tube or broad ligament malig-nancies include chondrosarcoma {2245},e m b ryonal rhabdomyosarcoma {361},myxoid liposarcoma {2708} and Ewingtumour {1692}. The prognosis is poor,although several long-term survivorshave been reported {1322}.
Malignant lymphoma andleukaemia
Tubal involvement by lymphoma is rareand is associated almost invariably withsimultaneous involvement of the ipsilater-al ovary {2119}. In one large series morethan 25% of patients with ovarian lym-phoma had tubal involvement, most oftenby Burkitt or Burkitt-like (small non-cleaved cell) lymphoma or diffuse large-cell lymphoma {2119}. One example ofan apparent primary malignant lym-phoma of the fallopian tube has beenobserved {2605}. The tube may also beinfiltrated in cases of leukaemia {428}.
Secondary tumours
Metastatic tumours involving the tubeusually are the result of secondaryspread from carcinomas of the ovary orendometrium {3145}. In most cases, thespread is by direct extension. In onestudy 89% of secondary carcinomas inthe tube were of ovarian origin, and theremainder originated in the endometri-um. Blood-borne metastases from breastcarcinomas or other extrapelvic tumoursmay also occur {862,3145}. The authorsare aware of a case of adenocarcinomaof the gallbladder metastatic to the fal-lopian tube {862}.
BAFig. 3.11 Adenomatoid tumour. A The wall of the fallopian tube contains a solid mass. Note the uninvolved cross section of the tube on the right. B Variably shapedsmall cystic spaces and tubule-like structures proliferate in the wall of the tube. The mucosa is on the right.
211Tumours of the fallopian tube
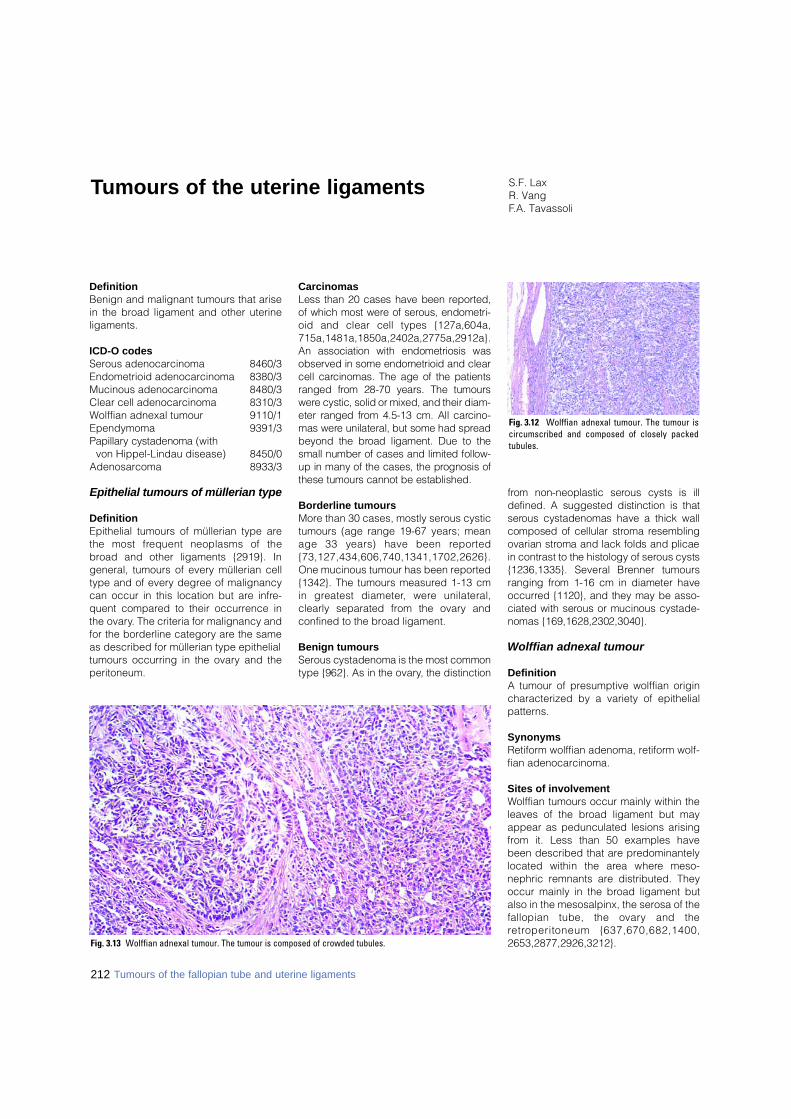
DefinitionBenign and malignant tumours that arisein the broad ligament and other uterineligaments.
ICD-O codesSerous adenocarcinoma 8460/3Endometrioid adenocarcinoma 8380/3Mucinous adenocarcinoma 8480/3Clear cell adenocarcinoma 8310/3Wolffian adnexal tumour 9110/1Ependymoma 9391/3P a p i l l a ry cystadenoma (with
von Hippel-Lindau disease) 8450/0Adenosarcoma 8933/3
Epithelial tumours of müllerian type
DefinitionEpithelial tumours of müllerian type arethe most frequent neoplasms of thebroad and other ligaments {2919}. Ingeneral, tumours of every müllerian celltype and of every degree of malignancycan occur in this location but are infre-quent compared to their occurrence inthe ovary. The criteria for malignancy andfor the borderline category are the sameas described for müllerian type epithelialtumours occurring in the ovary and theperitoneum.
CarcinomasLess than 20 cases have been re p o rt e d ,of which most were of serous, endometri-oid and clear cell types {127a,604a,7 1 5 a , 1 4 8 1 a , 1 8 5 0 a , 2 4 0 2 a , 2 7 7 5 a , 2 9 1 2 a } .An association with endometriosis wasobserved in some endometrioid and clearcell carcinomas. The age of the patientsranged from 28-70 years. The tumoursw e re cystic, solid or mixed, and their diam-eter ranged from 4.5-13 cm. All carc i n o-mas were unilateral, but some had spre a dbeyond the broad ligament. Due to thesmall number of cases and limited follow-up in many of the cases, the prognosis ofthese tumours cannot be established.
Borderline tumoursMore than 30 cases, mostly serous cystictumours (age range 19-67 years; meanage 33 years) have been re p o rt e d{ 7 3 , 1 2 7 , 4 3 4 , 6 0 6 , 7 4 0 , 1 3 4 1 , 1 7 0 2 , 2 6 2 6 } .One mucinous tumour has been reported{1342}. The tumours measured 1-13 cmin greatest diameter, were unilateral,clearly separated from the ovary andconfined to the broad ligament.
Benign tumoursS e rous cystadenoma is the most commontype {962}. As in the ovary, the distinction
f rom non-neoplastic serous cysts is illdefined. A suggested distinction is thats e rous cystadenomas have a thick wallcomposed of cellular stroma re s e m b l i n govarian stroma and lack folds and plicaein contrast to the histology of serous cysts{1236,1335}. Several Brenner tumoursranging from 1-16 cm in diameter haveo c c u r red {1120}, and they may be asso-ciated with serous or mucinous cystade-nomas {169,1628,2302,3040}.
Wolffian adnexal tumour
DefinitionA tumour of presumptive wolffian origincharacterized by a variety of epithelialpatterns.
SynonymsRetiform wolffian adenoma, retiform wolf-fian adenocarcinoma.
Sites of involvementWolffian tumours occur mainly within theleaves of the broad ligament but mayappear as pedunculated lesions arisingfrom it. Less than 50 examples havebeen described that are predominantelylocated within the area where meso-nephric remnants are distributed. Theyoccur mainly in the broad ligament butalso in the mesosalpinx, the serosa of thefallopian tube, the ovary and there t roperitoneum {637,670,682,1400,2653,2877,2926,3212}.
S.F. LaxR. VangF.A. Tavassoli
Tumours of the uterine ligaments
Fig. 3.12 Wolffian adnexal tumour. The tumour iscircumscribed and composed of closely packedtubules.
Fig. 3.13 Wolffian adnexal tumour. The tumour is composed of crowded tubules.
212 Tumours of the fallopian tube and uterine ligaments

Clinical featuresPatients range in age from 15-81 years,and most present with a unilateral adnex-al mass. Ultrasound studies may showan ill defined mass {637}.
MacroscopyThese predominantly solid tumoursrange from 0.5-18 cm in diameter. Thesectioned surface may contain variablysized cysts and is yellow-tan to grey-white {2877}. The tumour is firm to rub-bery and occasionally may have areas ofhaemorrhage and necrosis.
Tumour spread and stagingTumour implants may be present at thetime of diagnosis and indicate anaggressive tumour {637,2653}.
HistopathologyThe tumour shows a variable admixtureof diffuse, solid and sieve-like cysticareas, with the solid pattern dominatingin the majority of cases. The diffuse, solidareas show a compact proliferation ofovoid to spindle-shaped cells reflectingclosed tubules bound by a basementmembrane and separated by variableamounts of fibrous stroma or none at all.The round to ovoid nuclei may showindentations. The hollow tubules have aretiform or sertoliform appearance. Whenthe closed tubules dominate, the lesionresembles a mesenchymal tumour; aPAS or reticulin stain helps unmask thetubular pattern. The cells lining thetubules are cuboidal to low columnarwith a minimal amount of eosinophilic
cytoplasm and round to spindle-shaped,uniform nuclei. Sieve-like areas displayclusters of variably sized cysts lined byattenuated cells. Most cases do not showatypia or mitotic figures.
ImmunoprofileThe tumour cells are positive for mostcytokeratins and vimentin and are oftenpositive for calretinin (91%), inhibin(68%) and CD10 {2110}. They are usual -ly negative for epithelial membrane anti-gen, estrogen receptor (ER) and proges-terone receptor (PR) and are negative forcytokeratin 20, 34betaE12 and glu-tathione S-transferase {682,2926}.
CytometryThe ploidy of a metastatic tumour wasassessed and found to be diploid {2653}.
Electron microscopyAt the ultrastructural level, the tubulesare surrounded by basal lamina andlined by cells with complex interdigita-tions, desmosomes and/or tight junctionsand a few microvilli along the luminal bor-der; no cilia are identifiable {670}. Thecytoplasmic organelles are not distinc-tive and include lysosomes, a smallamount of smooth endoplasmic reticulumand a few lipid droplets.
Differential diagnosisThe main tumours in the differential diag-nosis are Sertoli cell tumour, Sert o l i -Leydig cell tumour, and well differentiat-ed endometrioid carcinoma. The pres-ence of a sieve-like pattern and the
absence of Leydig cells help distinguishwolffian tumours from all these lesions.The absence of immunoreactivity witheither ER or PR also would distinguishwolffian tumours from well differentiatedendometrioid carcinomas; the latter areinvariably positive for ER and PR; howev-e r, positive immunostaining does notexclude the possibility of a wolff i a ntumour {682}.
Prognosis and predictive factorsThe tumour stage as well as cytologicalatypia and frequent mitotic figures arei m p o rtant predictors of aggre s s i v ebehaviour. Careful follow-up of all womenwith wolffian adnexal tumours is prudent{637,2653}.Most wolffian adnexal tumours arebenign and adequately treated by unilat-eral salpingo-oophorectomy. About 10%either recur or metastasize. Recurrencesand metastases to the lungs and liverhave been reported within 1 year or aslate as 8 years after diagnosis{637,2653}. The metastatic tumour oftenhas more atypia compared to the pri-mary. Some aggressive tumours havehad no significant atypia or mitotic activ-ity in either the primary or the metastaticlesion {2653}.
Ependymoma
DefinitionTumours closely resembling neoplasmsof the central nervous system that showependymal differentiation.
BAFig. 3.14 Wolffian adnexal tumour. A The pattern of closely packed tubules simulates a Sertoli cell tumour. B Reticulin stain accentuates the tubular pattern.
213Tumours of the uterine ligaments
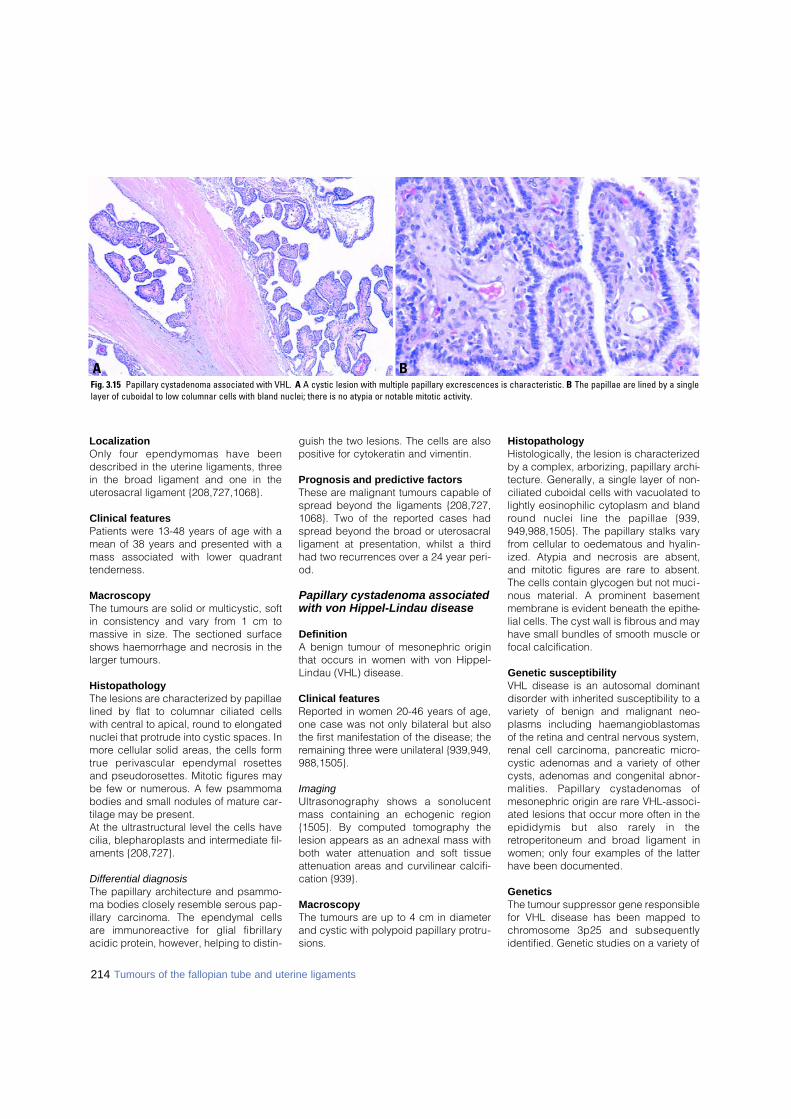
LocalizationOnly four ependymomas have beendescribed in the uterine ligaments, threein the broad ligament and one in theuterosacral ligament {208,727,1068}.
Clinical featuresPatients were 13-48 years of age with amean of 38 years and presented with amass associated with lower quadranttenderness.
MacroscopyThe tumours are solid or multicystic, softin consistency and vary from 1 cm tomassive in size. The sectioned surfaceshows haemorrhage and necrosis in thelarger tumours.
HistopathologyThe lesions are characterized by papillaelined by flat to columnar ciliated cellswith central to apical, round to elongatednuclei that protrude into cystic spaces. Inmore cellular solid areas, the cells formtrue perivascular ependymal ro s e t t e sand pseudorosettes. Mitotic figures maybe few or numerous. A few psammomabodies and small nodules of mature car-tilage may be present. At the ultrastructural level the cells havecilia, blepharoplasts and intermediate fil-aments {208,727}.
Differential diagnosisThe papillary architecture and psammo-ma bodies closely resemble serous pap-illary carcinoma. The ependymal cellsa re immunoreactive for glial fibrillaryacidic protein, however, helping to distin-
guish the two lesions. The cells are alsopositive for cytokeratin and vimentin.
Prognosis and predictive factorsThese are malignant tumours capable ofspread beyond the ligaments {208,727,1068}. Two of the reported cases hadspread beyond the broad or uterosacralligament at presentation, whilst a thirdhad two recurrences over a 24 year peri-od.
Papillary cystadenoma associatedwith von Hippel-Lindau disease
DefinitionA benign tumour of mesonephric originthat occurs in women with von Hippel-Lindau (VHL) disease.
Clinical featuresReported in women 20-46 years of age,one case was not only bilateral but alsothe first manifestation of the disease; theremaining three were unilateral {939,949,988,1505}.
ImagingUltrasonography shows a sonolucentmass containing an echogenic region{1505}. By computed tomography thelesion appears as an adnexal mass withboth water attenuation and soft tissueattenuation areas and curvilinear calcifi-cation {939}.
MacroscopyThe tumours are up to 4 cm in diameterand cystic with polypoid papillary protru-sions.
HistopathologyHistologically, the lesion is characterizedby a complex, arborizing, papillary archi-tecture. Generally, a single layer of non-ciliated cuboidal cells with vacuolated tolightly eosinophilic cytoplasm and blandround nuclei line the papillae {939,949,988,1505}. The papillary stalks varyfrom cellular to oedematous and hyalin-ized. Atypia and necrosis are absent,and mitotic figures are rare to absent.The cells contain glycogen but not muci-nous material. A prominent basementmembrane is evident beneath the epithe-lial cells. The cyst wall is fibrous and mayhave small bundles of smooth muscle orfocal calcification.
Genetic susceptibilityVHL disease is an autosomal dominantdisorder with inherited susceptibility to avariety of benign and malignant neo-plasms including haemangioblastomasof the retina and central nervous system,renal cell carcinoma, pancreatic micro-cystic adenomas and a variety of othercysts, adenomas and congenital abnor-malities. Papillary cystadenomas ofmesonephric origin are rare VHL-associ-ated lesions that occur more often in theepididymis but also rarely in theretroperitoneum and broad ligament inwomen; only four examples of the latterhave been documented.
GeneticsThe tumour suppressor gene responsiblefor VHL disease has been mapped toc h romosome 3p25 and subsequentlyidentified. Genetic studies on a variety of
214 Tumours of the fallopian tube and uterine ligaments
BAFig. 3.15 Papillary cystadenoma associated with VHL. A A cystic lesion with multiple papillary excrescences is characteristic. B The papillae are lined by a singlelayer of cuboidal to low columnar cells with bland nuclei; there is no atypia or notable mitotic activity.

215Tumours of the uterine ligaments
tumours from patients with VHL diseasehave demonstrated loss of heterozygosi -ty at chromosome 3p within the VHLgene region. Two papillary cystadeno-mas (one from broad ligament, the otherretroperitoneal) were studied by poly-merase chain reaction and single-strandc o n f o rmation polymorphism with fourpolymorphic markers spanning the VHLgene locus (D3S1038, D3S1110,D3S2452, 104/105) {2640}. Both tumoursshowed loss of heterozygosity at one ormore of the markers providing evidencethat somatic loss of the VHL gene isresponsible for the genesis of these pap-illary cystadenomas {2640}.
Prognosis and predictive featuresAll lesions reported so far have beenbenign.
Uterus-like mass
DefinitionA tumour-like lesion composed ofendometrial tissue and smooth muscle,histologically resembling the uterus.
Clinical featuresPatients present with a pelvic mass. Mostarise within the ovary, but extraovarian
cases have been described. Casesreported in the uterosacral and broad lig-aments have occurred in women under50 years of age {48}.
Macroscopy The lesions form a cystic mass.
HistopathologyThe inner lining consists of benignendometrial glands and endometrial stro-ma with an arrangement re s e m b l i n gendometrium. The outer layer of the cystwall consists of thickened smooth mus-cle bundles appearing similar tomyometrium.
ImmunoprofileLesions may express ER and PR in theendometrial and myometrial compo-nents.
Differential diagnosis"Endomyometriosis" is likely the sameentity as uterine-like mass. "Endometrio-sis with smooth muscle metaplasia" ishistologically related to uterus-like mass,if not the same. Adenomyoma is distin-guished from uterus-like mass by lackingthe uterus-like organization. A uterus-likemass lacks the classic features ofendometrioid carcinoma and extrauter-ine adenosarcoma.
GeneticsA deletion on the short arm of chromo-some 2 has been identified.
Prognosis and predictive factorsBenign behaviour would be expected.
Adenosarcoma
A single case of a high grade adenosar-coma arising from the round ligamentwas reported {1396}.
Mesenchymal tumours
Mesenchymal tumours originating fromthe broad and other ligaments are rare.Almost any kind of malignant or benignmesenchymal tumour may occur.
Malignant tumoursS a rcomas are extremely rare, the mostf requent being leiomyosarcoma, {465,689,1192,1608,1630,2210} for which thesame diagnostic criteria should beapplied as for its uterine counterpart .
A p p roximately 10 cases have beenre p o rted, and the prognosis is poor.Other sarcomas re p o rted includeendometrioid stromal sarcoma arising inendometriosis {2220}, embryonal rhab-d o m y o s a rcoma (occurring in childre nand having a poor prognosis) {991},alveolar rhabdomyosarcoma (in anadult) {558}, mixed mesenchymal sarc o-ma {2822}, myxoid liposarcoma {2708}and alveolar soft part sarcoma {2017}.
Benign tumoursThe most common tumours are leiomy-omas and lipomas {340,962}. It is oftend i fficult to determine the site of origin ofleiomyomas within the broad ligament. Ithas been suggested that leiomyomasbe designated as ligamentous only ifclearly separated from the myometrium.A leiomyoma of the broad ligament wasimitated by Dracunculosis {70}.Lipomas are usually small and locatedwithin the mesosalpinx {847} and maybe mixed with leiomyomas. Cases ofother mesenchymal tumours of theb road and round ligament have beenre p o rted including two benign mes-enchymomas {2069}, neuro f i b ro m a s ,schwannomas {246,1047,2910} and af i b roma with heterotopic bone form a t i o n{2899}. Massive ascites and bilateralpleural effusion has been described inassociation with broad ligament leiomy-oma and with paraovarian fibro m a(pseudo-Meigs syndrome) {357,364,9 9 2 } .
Miscellaneous tumours
A variety of miscellaneous tumours havebeen described. Many of them are ofovarian type, such as germ cell and sexc o rd - s t romal tumours. Although thequestion of origin from accessory ovari-an tissue may be raised, in most casesno pre-existing ovarian tissue is identi-fied. Mature teratomas, in particular der-moid cysts, occurred bilaterally withina c c e s s o ry ovaries of the broad ligament{941}. A dermoid cyst containing pitu-i t a ry tissue occurred in the utero s a c r a lligament {1179}. A yolk sac tumour wasfound in the broad ligament {1270}. Other re p o rted cases included granu-losa cell tumours, but some of thesew e re in fact wolffian adnexal tumours{962,1427,2347,2997}. Several bro a dligament tumours of the thecoma-fibro-ma group, some of which had estro-
Fig. 3.16 Uterus-like mass. The cystic mass resem-bles the uterus and is composed of a layer ofendometrium consisting of glands and stromaoverlying smooth muscle.
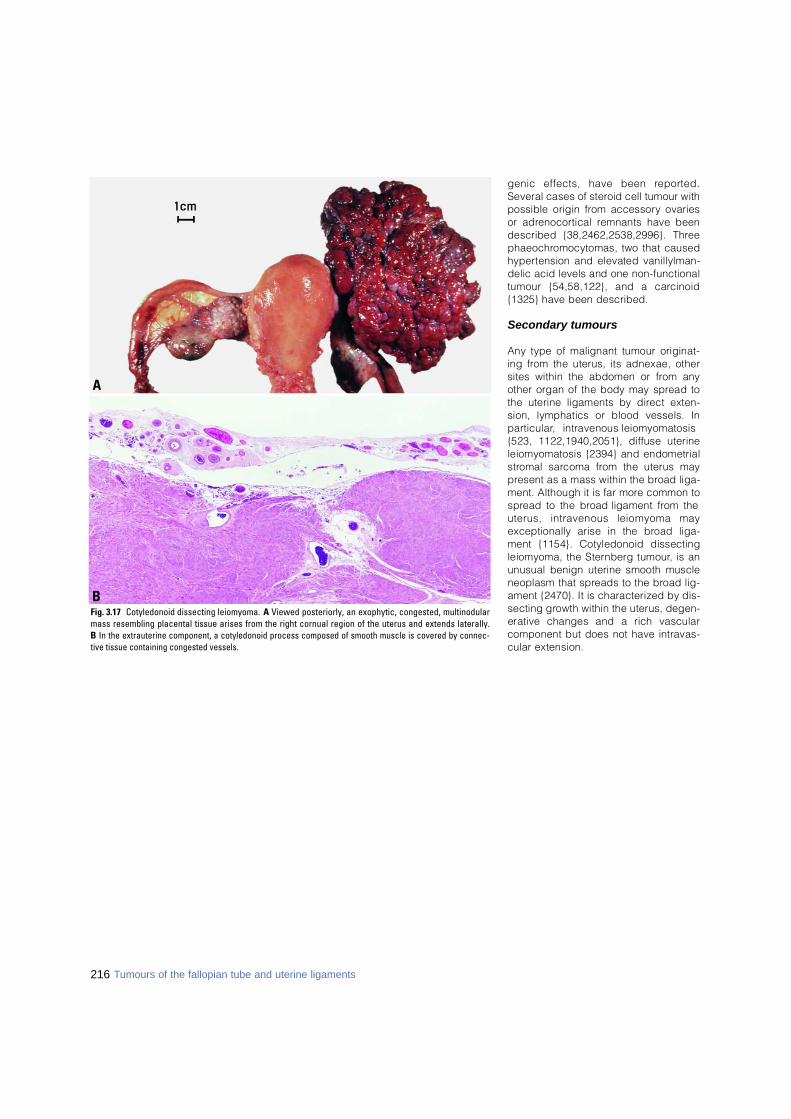
genic effects, have been re p o rt e d .Several cases of steroid cell tumour withpossible origin from accessory ovariesor adre n o c o rtical remnants have beendescribed {38,2462,2538,2996}. Thre ep h a e o c h romocytomas, two that causedh y p e rtension and elevated vanillylman-delic acid levels and one non-functionaltumour {54,58,122}, and a carc i n o i d{1325} have been described.
Secondary tumours
Any type of malignant tumour originat-ing from the uterus, its adnexae, othersites within the abdomen or from anyother organ of the body may spread tothe uterine ligaments by direct exten-sion, lymphatics or blood vessels. Inp a rt i c u l a r, intravenous leiomyomatosis{523, 1122,1940,2051}, diffuse uterineleiomyomatosis {2394} and endometrials t romal sarcoma from the uterus mayp resent as a mass within the broad liga-ment. Although it is far more common tos p read to the broad ligament from theuterus, intravenous leiomyoma mayexceptionally arise in the broad liga-ment {1154}. Cotyledonoid dissectingleiomyoma, the Sternberg tumour, is anunusual benign uterine smooth muscleneoplasm that spreads to the broad lig-ament {2470}. It is characterized by dis-secting growth within the uterus, degen-erative changes and a rich vascularcomponent but does not have intravas-cular extension.
216 Tumours of the fallopian tube and uterine ligaments
Fig. 3.17 Cotyledonoid dissecting leiomyoma. A Viewed posteriorly, an exophytic, congested, multinodularmass resembling placental tissue arises from the right cornual region of the uterus and extends laterally. B In the extrauterine component, a cotyledonoid process composed of smooth muscle is covered by connec-tive tissue containing congested vessels.
B
A
CHAPTER 4
Tumours of the Uterine Corpus
The uterine corpus represents the second most common sitefor malignancy of the female genital system. These neoplasmsare divided into epithelial, mesenchymal, mixed epithelial andmesenchymal tumours and trophoblastic tumours.
Endometrial carcinoma occurs predominantly in developedcountries and is frequently associated with obesity. Two majortypes are distinguished. Type I is estrogen-dependent anddevelops through the hyperplasia-carcinoma sequence. TypeII is not estrogen-dependent and develops independently ofendometrial hyperplasia. It occurs in older women and is moreaggressive.
Carcinosarcoma is still classified morphologically as a mixedepithelial and mesenchymal tumour, although it is consideredmonoclonal, with immunohistochemical and molecular studiesstrongly supporting its inclusion in the epithelial group. Itsprognosis is worse than that of other members of the epithelialcategory.
Gestational trophoblastic disease is approximately 10-foldmore common in the developing than in developed countries.Risk factors include a history of prior gestational trophoblasticdisease, a diet low in vitamin A and blood group A women mar-ried to group 0 men.
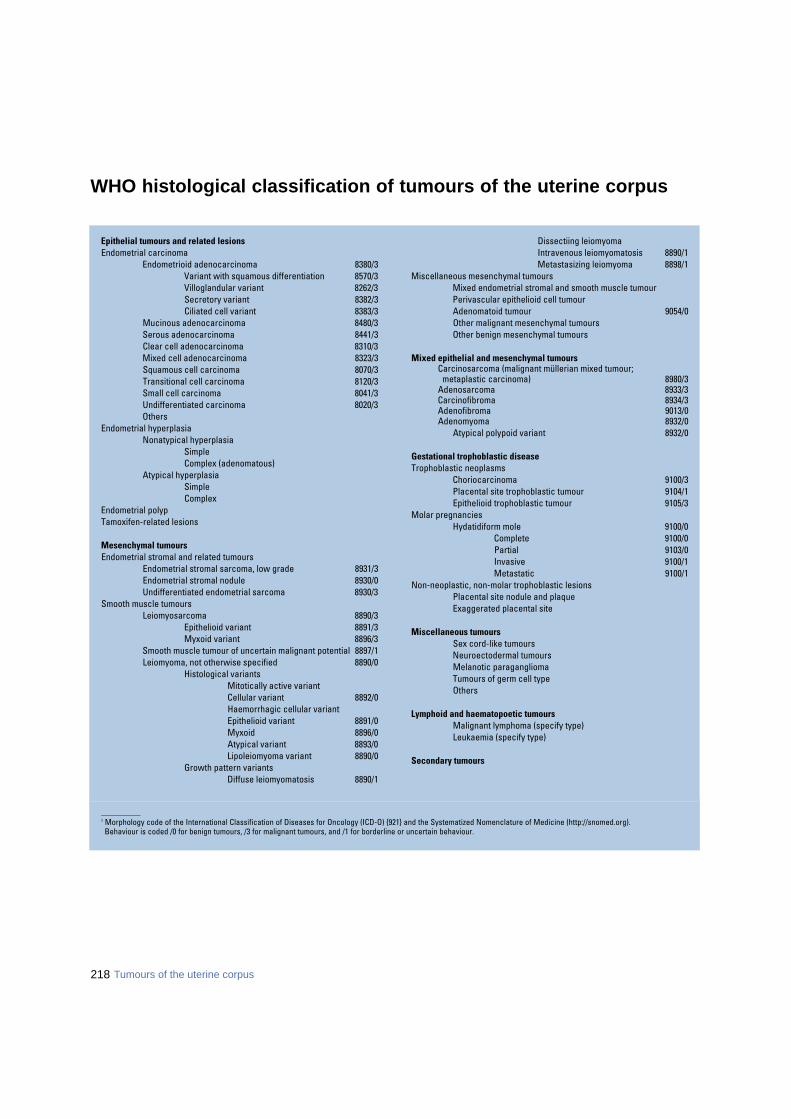
218 Tumours of the uterine corpus
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Epithelial tumours and related lesionsEndometrial carcinoma
Endometrioid adenocarcinoma 8380/3 Variant with squamous differentiation 8570/3Villoglandular variant 8262/3Secretory variant 8382/3Ciliated cell variant 8383/3
Mucinous adenocarcinoma 8480/3Serous adenocarcinoma 8441/3Clear cell adenocarcinoma 8310/3Mixed cell adenocarcinoma 8323/3Squamous cell carcinoma 8070/3Transitional cell carcinoma 8120/3Small cell carcinoma 8041/3Undifferentiated carcinoma 8020/3Others
Endometrial hyperplasiaNonatypical hyperplasia
SimpleComplex (adenomatous)
Atypical hyperplasiaSimpleComplex
Endometrial polypTamoxifen-related lesions
Mesenchymal tumours Endometrial stromal and related tumours
Endometrial stromal sarcoma, low grade 8931/3Endometrial stromal nodule 8930/0Undifferentiated endometrial sarcoma 8930/3
Smooth muscle tumoursLeiomyosarcoma 8890/3
Epithelioid variant 8891/3Myxoid variant 8896/3
Smooth muscle tumour of uncertain malignant potential 8897/1Leiomyoma, not otherwise specified 8890/0
Histological variantsMitotically active variantCellular variant 8892/0Haemorrhagic cellular variantEpithelioid variant 8891/0Myxoid 8896/0Atypical variant 8893/0Lipoleiomyoma variant 8890/0
Growth pattern variantsDiffuse leiomyomatosis 8890/1
Dissectiing leiomyomaIntravenous leiomyomatosis 8890/1Metastasizing leiomyoma 8898/1
Miscellaneous mesenchymal tumoursMixed endometrial stromal and smooth muscle tumourPerivascular epithelioid cell tumourAdenomatoid tumour 9054/0Other malignant mesenchymal tumoursOther benign mesenchymal tumours
Mixed epithelial and mesenchymal tumoursCarcinosarcoma (malignant müllerian mixed tumour;
metaplastic carcinoma) 8980/3Adenosarcoma 8933/3Carcinofibroma 8934/3Adenofibroma 9013/0Adenomyoma 8932/0
Atypical polypoid variant 8932/0
Gestational trophoblastic diseaseTrophoblastic neoplasms
Choriocarcinoma 9100/3Placental site trophoblastic tumour 9104/1Epithelioid trophoblastic tumour 9105/3
Molar pregnanciesHydatidiform mole 9100/0
Complete 9100/0Partial 9103/0Invasive 9100/1Metastatic 9100/1
Non-neoplastic, non-molar trophoblastic lesionsPlacental site nodule and plaqueExaggerated placental site
Miscellaneous tumoursSex cord-like tumoursNeuroectodermal tumoursMelanotic paragangliomaTumours of germ cell typeOthers
Lymphoid and haematopoetic tumoursMalignant lymphoma (specify type)Leukaemia (specify type)
Secondary tumours
WHO histological classification of tumours of the uterine corpus
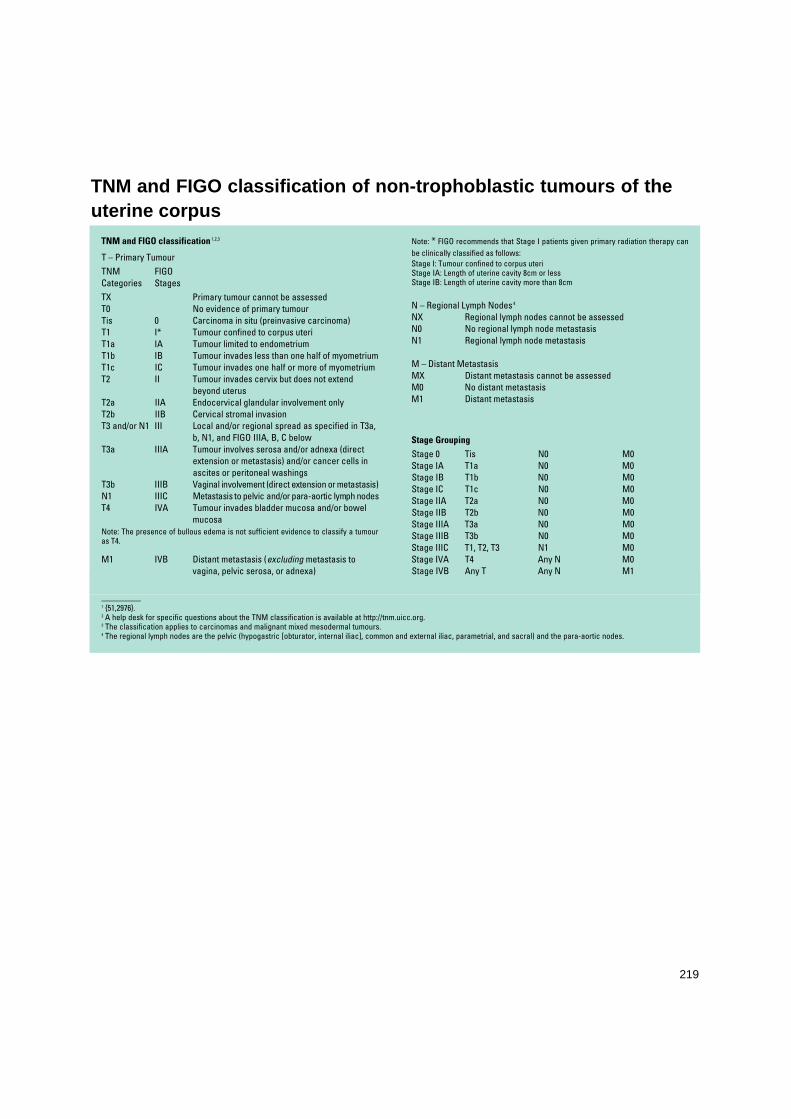
_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The classification applies to carcinomas and malignant mixed mesodermal tumours.4 The regional lymph nodes are the pelvic (hypogastric [obturator, internal iliac], common and external iliac, parametrial, and sacral) and the para-aortic nodes.
219
TNM and FIGO classification 1,2,3
T – Primary Tumour TNM FIGO Categories StagesTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis 0 Carcinoma in situ (preinvasive carcinoma)T1 I* Tumour confined to corpus uteriT1a IA Tumour limited to endometriumT1b IB Tumour invades less than one half of myometriumT1c IC Tumour invades one half or more of myometriumT2 II Tumour invades cervix but does not extend
beyond uterusT2a IIA Endocervical glandular involvement onlyT2b IIB Cervical stromal invasionT3 and/or N1 III Local and/or regional spread as specified in T3a,
b, N1, and FIGO IIIA, B, C belowT3a IIIA Tumour involves serosa and/or adnexa (direct
extension or metastasis) and/or cancer cells inascites or peritoneal washings
T3b IIIB Vaginal involvement (direct extension or metastasis)N1 IIIC Metastasis to pelvic and/or para-aortic lymph nodesT4 IVA Tumour invades bladder mucosa and/or bowel
mucosaNote: The presence of bullous edema is not sufficient evidence to classify a tumouras T4.
M1 IVB Distant metastasis (excluding metastasis to vagina, pelvic serosa, or adnexa)
Note: * FIGO recommends that Stage I patients given primary radiation therapy canbe clinically classified as follows:Stage I: Tumour confined to corpus uteriStage IA: Length of uterine cavity 8cm or lessStage IB: Length of uterine cavity more than 8cm
N – Regional Lymph Nodes 4
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage 0 Tis N0 M0Stage IA T1a N0 M0Stage IB T1b N0 M0Stage IC T1c N0 M0Stage IIA T2a N0 M0Stage IIB T2b N0 M0Stage IIIA T3a N0 M0Stage IIIB T3b N0 M0Stage IIIC T1, T2, T3 N1 M0Stage IVA T4 Any N M0Stage IVB Any T Any N M1
TNM and FIGO classification of non-trophoblastic tumours of theuterine corpus
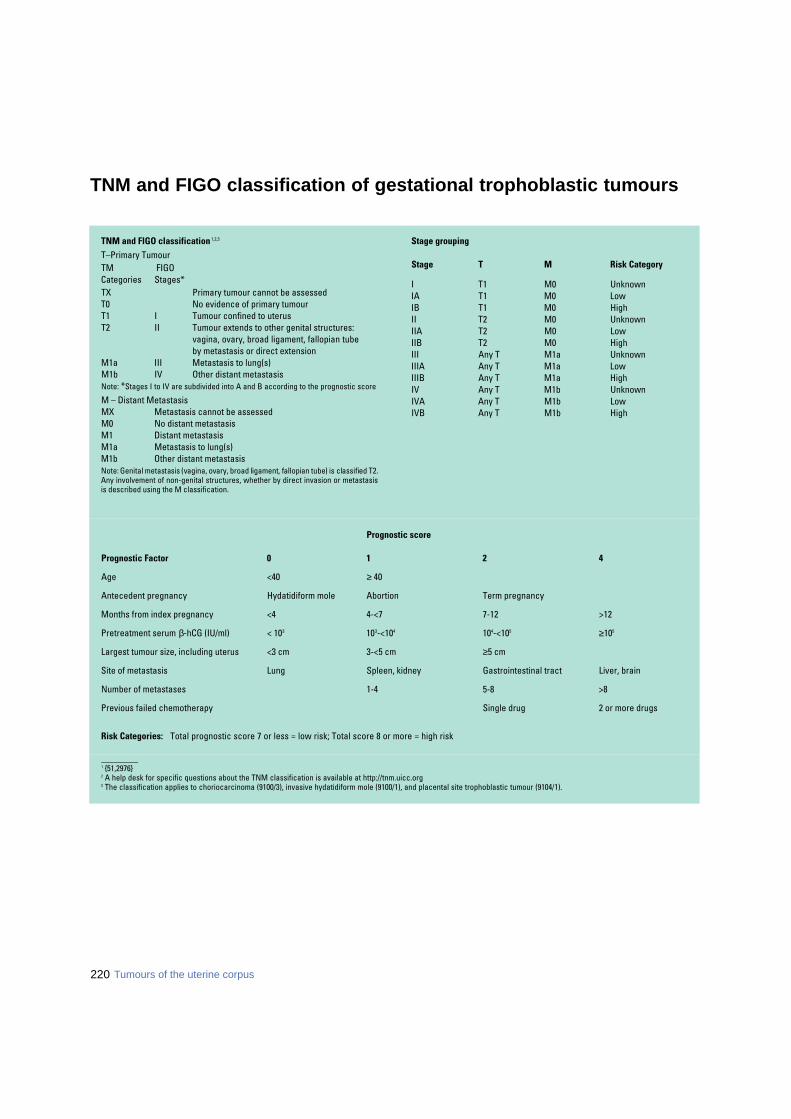
220 Tumours of the uterine corpus
_________1 {51,2976}2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org3 The classification applies to choriocarcinoma (9100/3), invasive hydatidiform mole (9100/1), and placental site trophoblastic tumour (9104/1).
TNM and FIGO classification of gestational trophoblastic tumours
Prognostic score
Prognostic Factor 0 1 2 4
Age <40 ≥ 40
Antecedent pregnancy Hydatidiform mole Abortion Term pregnancy
Months from index pregnancy <4 4-<7 7-12 >12
Pretreatment serum β-hCG (IU/ml) < 103 103-<104 104-<105 ≥105
Largest tumour size, including uterus <3 cm 3-<5 cm ≥5 cm
Site of metastasis Lung Spleen, kidney Gastrointestinal tract Liver, brain
Number of metastases 1-4 5-8 >8
Previous failed chemotherapy Single drug 2 or more drugs
Risk Categories: Total prognostic score 7 or less = low risk; Total score 8 or more = high risk
TNM and FIGO classification 1,2,3
T–Primary TumourTM FIGO Categories Stages*TX Primary tumour cannot be assessedT0 No evidence of primary tumourT1 I Tumour confined to uterusT2 II Tumour extends to other genital structures:
vagina, ovary, broad ligament, fallopian tube by metastasis or direct extension
M1a III Metastasis to lung(s)M1b IV Other distant metastasis Note: *Stages I to IV are subdivided into A and B according to the prognostic score
M – Distant MetastasisMX Metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasisM1a Metastasis to lung(s)M1b Other distant metastasis Note: Genital metastasis (vagina, ovary, broad ligament, fallopian tube) is classified T2. Any involvement of non-genital structures, whether by direct invasion or metastasisis described using the M classification.
Stage grouping
Stage T M Risk Category
I T1 M0 UnknownIA T1 M0 LowIB T1 M0 HighII T2 M0 UnknownIIA T2 M0 LowIIB T2 M0 HighIII Any T M1a UnknownIIIA Any T M1a LowIIIB Any T M1a HighIV Any T M1b UnknownIVA Any T M1b LowIVB Any T M1b High
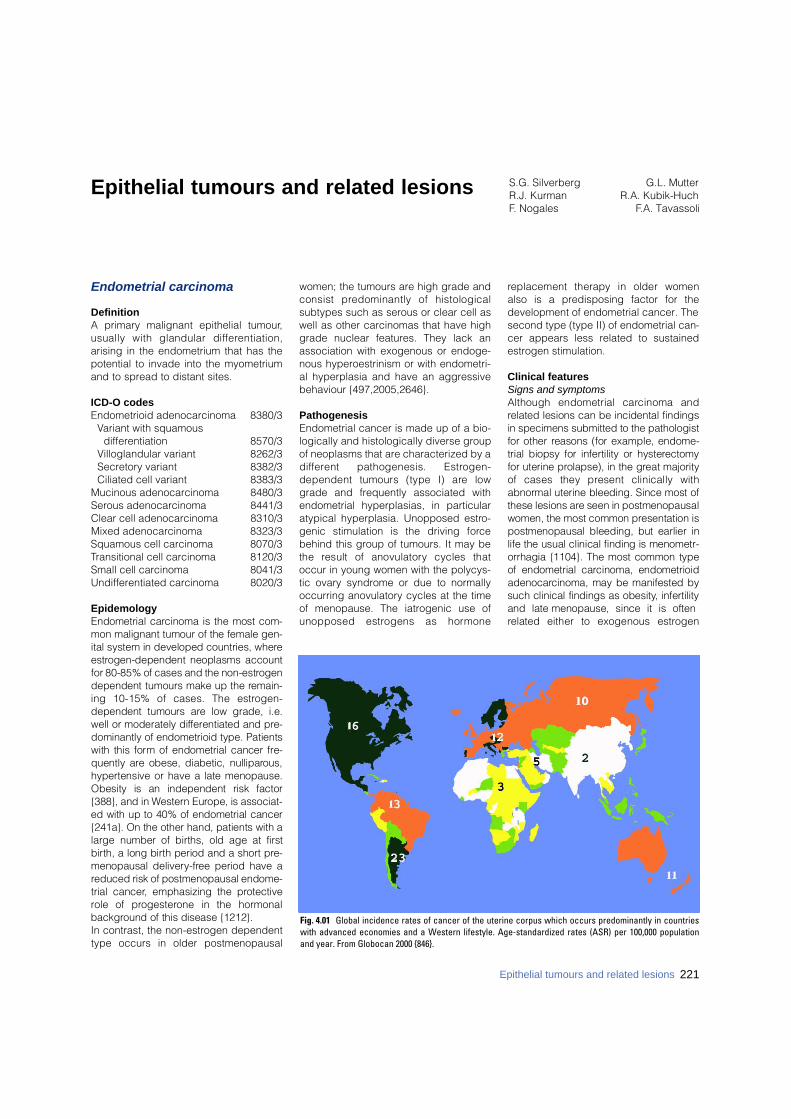
Epithelial tumours and related lesions S.G. Silverberg G.L. MutterR.J. Kurman R.A. Kubik-HuchF. Nogales F.A. Tavassoli
Endometrial carcinoma
DefinitionA primary malignant epithelial tumour,usually with glandular diff e re n t i a t i o n ,arising in the endometrium that has thepotential to invade into the myometriumand to spread to distant sites.
ICD-O codesEndometrioid adenocarcinoma 8380/3
Variant with squamous differentiation 8570/3
Villoglandular variant 8262/3Secretory variant 8382/3Ciliated cell variant 8383/3
Mucinous adenocarcinoma 8480/3Serous adenocarcinoma 8441/3Clear cell adenocarcinoma 8310/3Mixed adenocarcinoma 8323/3Squamous cell carcinoma 8070/3Transitional cell carcinoma 8120/3Small cell carcinoma 8041/3Undifferentiated carcinoma 8020/3
EpidemologyEndometrial carcinoma is the most com-mon malignant tumour of the female gen-ital system in developed countries, wheree s t rogen-dependent neoplasms accountfor 80-85% of cases and the non-estro g e ndependent tumours make up the re m a i n-ing 10-15% of cases. The estro g e n -dependent tumours are low grade, i.e.well or moderately diff e rentiated and pre-dominantly of endometrioid type. Patientswith this form of endometrial cancer fre-quently are obese, diabetic, nulliparo u s ,h y p e rtensive or have a late menopause.Obesity is an independent risk factor{388}, and in We s t e rn Europe, is associat-ed with up to 40% of endometrial cancer{241a}. On the other hand, patients with alarge number of births, old age at firstb i rth, a long birth period and a short pre-menopausal delivery - f ree period have areduced risk of postmenopausal endome-trial cancer, emphasizing the pro t e c t i v erole of pro g e s t e rone in the horm o n a lb a c k g round of this disease {1212}. In contrast, the non-estrogen dependenttype occurs in older postmenopausal
women; the tumours are high grade andconsist predominantly of histologicalsubtypes such as serous or clear cell aswell as other carcinomas that have highgrade nuclear features. They lack anassociation with exogenous or endoge-nous hyperoestrinism or with endometri-al hyperplasia and have an aggressivebehaviour {497,2005,2646}.
PathogenesisEndometrial cancer is made up of a bio-logically and histologically diverse groupof neoplasms that are characterized by ad i ff e rent pathogenesis. Estro g e n -dependent tumours (type I) are lowgrade and frequently associated withendometrial hyperplasias, in particularatypical hyperplasia. Unopposed estro-genic stimulation is the driving forc ebehind this group of tumours. It may bethe result of anovulatory cycles thatoccur in young women with the polycys-tic ovary syndrome or due to normallyoccurring anovulatory cycles at the timeof menopause. The iatrogenic use ofunopposed estrogens as horm o n e
replacement therapy in older womenalso is a predisposing factor for thedevelopment of endometrial cancer. Thesecond type (type II) of endometrial can-cer appears less related to sustainedestrogen stimulation.
Clinical features Signs and symptomsAlthough endometrial carcinoma andrelated lesions can be incidental findingsin specimens submitted to the pathologistfor other reasons (for example, endome-trial biopsy for infertility or hystere c t o m yfor uterine prolapse), in the great majorityof cases they present clinically witha b n o rmal uterine bleeding. Since most ofthese lesions are seen in postmenopausalwomen, the most common presentation ispostmenopausal bleeding, but earlier inlife the usual clinical finding is menometr-orrhagia {1104}. The most common typeof endometrial carcinoma, endometrioida d e n o c a rcinoma, may be manifested bysuch clinical findings as obesity, infert i l i t yand late menopause, since it is oftenrelated either to exogenous estro g e n
Fig. 4.01 Global incidence rates of cancer of the uterine corpus which occurs predominantly in countrieswith advanced economies and a Western lifestyle. Age-standardized rates (ASR) per 100,000 populationand year. From Globocan 2000 {846}.
Epithelial tumours and related lesions 221

administration or to endogenous hyper-oestrinism {2276,2648,2805}. Endometrialhyperplasia and atypical hyperplasiahave similar clinical associations.
ImagingTransvaginal ultrasound (US) is the imag-ing technique of choice for the assess-ment of the endometrium in symptomaticpatients, e.g. in cases of postmenopausalbleeding {133}. In postmenopausalwomen without hormonal replacement anendometrial thickness of 5 mm is re g a rd-ed as the upper normal limit {133,2650}.The presence of endometrial thickeningon ultrasound or cross sectional imagingis, however, a nonspecific finding. It maybe due to endometrial hyperplasia,polyps or carcinoma. The final diagnosisusually needs to be determined byendometrial sampling {133}.Whereas currently magnetic resonanceimaging (MRI) has no established role inscreening for endometrial pathology, it isregarded as the best imaging techniquefor preoperative staging of endometrialcarcinoma proven by endometrial sam-pling. MRI was shown to be superior tocomputed tomography (CT) in thisregard {1135}. It is especially useful forpatients with suspected advanced dis-ease, for those with associated uterinepathology, such as leiomyomas, and forthose with histological subtypes that sig-nify a worse prognosis {916,1136}.
MacroscopyEndometrial carcinoma usually arises inthe uterine corpus, but some cases origi-nate in the lower uterine segment, andrecent studies suggest that the latter may
have diff e rent clinical and histological fea-t u res {1323,3067}. Regardless of the his-tological type, the macroscopic appear-ance of endometrial carcinoma is general-ly that of a single dominant mass, usuallyoccurring in an enlarged uterus, althoughoccasionally the uterus is small or thetumour presents as a diffuse thickening ofmost of the endometrial surface, part i c u-larly in the serous type. Endometrial carc i-noma is seen more frequently on the pos-terior than on the anterior wall {2691}.The typical carcinoma is exophytic andhas a shaggy, frequently ulcerated sur-face beneath which a soft or firm whitetumour may extend shallowly or deeplyinto the underlying myometrium. Inadvanced cases the tumour may pene-trate the serosa or extend into the cervix.An estimate of the extent of tumour maybe requested preoperatively or operative-ly in order to determine the extent of thesurgical pro c e d u re to be perf o rmed {594}.In occasional cases no tumour may bevisible macro s c o p i c a l l y, with carc i n o m aidentified only at histological examination.
Tumour spread and stagingThe staging of uterine tumours is by theTNM/FIGO classification {51,2976}.
Endometrioid adenocarcinoma
DefinitionA primary endometrial adenocarcinomacontaining glands resembling those ofthe normal endometrium.
HistopathologyAll but a few rare endometrial carcino-mas are adenocarcinomas, and the most
common of these is the endometrioidtype {2691}. Endometrioid adenocarcino-ma represents a spectrum of histologicaldifferentiation from a very well differenti-ated carcinoma difficult to distinguishf rom atypical complex hyperplasia tominimally differentiated tumours that canbe confused not only with undifferentiat-ed carcinoma but with various sarcomasas well. A highly characteristic feature ofendometrioid adenocarcinoma is thepresence of at least some glandular orvilloglandular structures lined by simpleto pseudostratified columnar cells thathave their long axes arranged perpendi-cular to the basement membrane with atleast somewhat elongated nuclei that arealso polarized in the same direction. Asthe glandular differentiation decreasesand is replaced by solid nests andsheets of cells, the tumour is classified asless well differentiated (higher grade).Deep myometrial invasion and lymphnode metastases are both more frequentin higher grade carcinomas, and survivalrates are correspondingly lower {574,1359}. It should be noted that: (1). Only those cells which are consid-ered to be of glandular type are consid-ered in the grading schema, so that solidnests of cells showing squamous ormorular differentiation do not increasethe tumour grade.(2). Bizarre nuclear atypia should raise thegrade by one, e.g. from 1 to 2 or 2 to 3.(3). It should be emphasized that thepresence of bizarre nuclei occurring ineven a predominantly glandular tumourmay indicate serous or clear cell ratherthan endometrioid differentiation {2691}.The distinction of very well differentiated
BAFig. 4.02 Well differentiated endometrioid adenocarcinoma. A Invasion is indicated by back to back glands, complex folds and stromal disappearance. B The neo-plastic glands are lined by columnar cells with relatively uniform nuclei; note the altered stroma in the top of the field.
222 Tumours of the uterine corpus
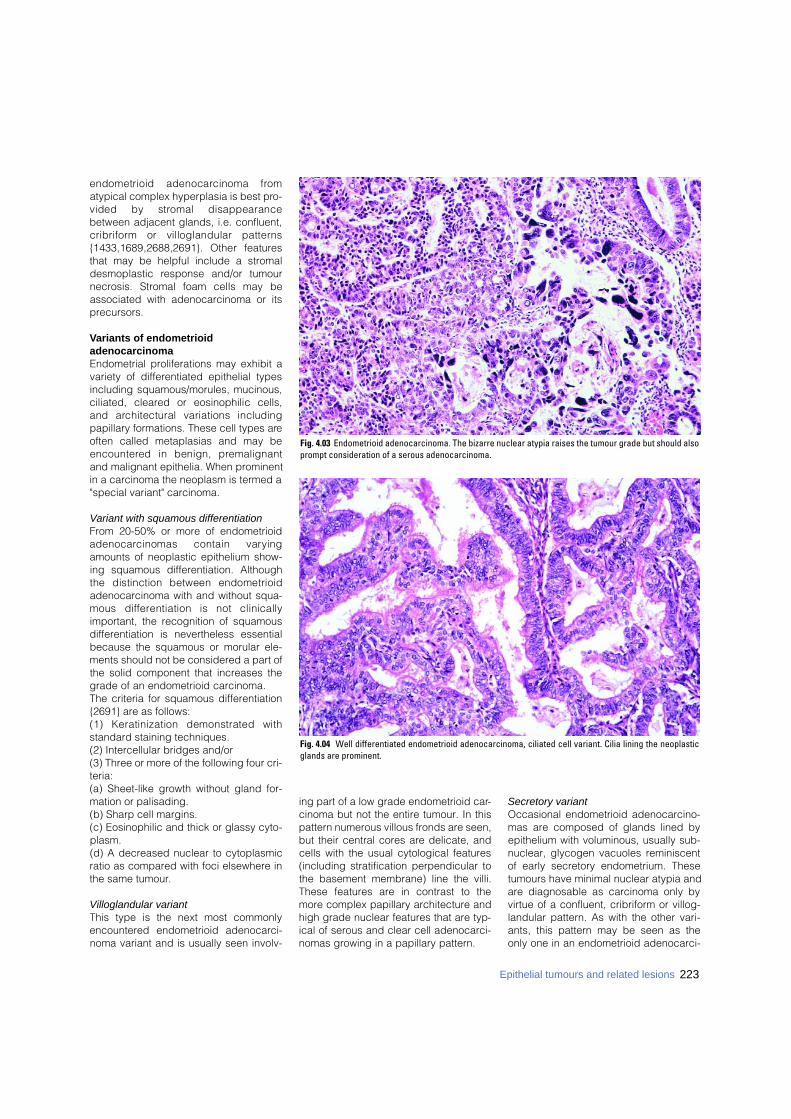
endometrioid adenocarcinoma fro matypical complex hyperplasia is best pro-vided by stromal disappearancebetween adjacent glands, i.e. confluent,c r i b r i f o rm or villoglandular pattern s{1433,1689,2688,2691}. Other feature sthat may be helpful include a stromaldesmoplastic response and/or tumourn e c rosis. Stromal foam cells may beassociated with adenocarcinoma or itsprecursors.
Variants of endometrioid adenocarcinomaEndometrial proliferations may exhibit avariety of differentiated epithelial typesincluding squamous/morules, mucinous,ciliated, cleared or eosinophilic cells,and architectural variations includingpapillary formations. These cell types areoften called metaplasias and may bee n c o u n t e red in benign, pre m a l i g n a n tand malignant epithelia. When prominentin a carcinoma the neoplasm is termed a"special variant" carcinoma.
Variant with squamous differentiationFrom 20-50% or more of endometrioida d e n o c a rcinomas contain vary i n gamounts of neoplastic epithelium show-ing squamous differentiation. Althoughthe distinction between endometrioidadenocarcinoma with and without squa-mous diff e rentiation is not clinicallyimportant, the recognition of squamousdifferentiation is nevertheless essentialbecause the squamous or morular ele-ments should not be considered a part ofthe solid component that increases thegrade of an endometrioid carcinoma. The criteria for squamous differentiation{2691} are as follows:(1) Keratinization demonstrated withstandard staining techniques.(2) Intercellular bridges and/or(3) Three or more of the following four cri-teria:(a) Sheet-like growth without gland for-mation or palisading.(b) Sharp cell margins.(c) Eosinophilic and thick or glassy cyto-plasm.(d) A decreased nuclear to cytoplasmicratio as compared with foci elsewhere inthe same tumour.
Villoglandular variantThis type is the next most commonlyencountered endometrioid adenocarci-noma variant and is usually seen involv-
ing part of a low grade endometrioid car-cinoma but not the entire tumour. In thispattern numerous villous fronds are seen,but their central cores are delicate, andcells with the usual cytological features(including stratification perpendicular tothe basement membrane) line the villi.These features are in contrast to themore complex papillary architecture andhigh grade nuclear features that are typ-ical of serous and clear cell adenocarci-nomas growing in a papillary pattern.
Secretory variantOccasional endometrioid adenocarcino-mas are composed of glands lined byepithelium with voluminous, usually sub-nuclear, glycogen vacuoles reminiscentof early secretory endometrium. Thesetumours have minimal nuclear atypia andare diagnosable as carcinoma only byvirtue of a confluent, cribriform or villog-landular pattern. As with the other vari-ants, this pattern may be seen as theonly one in an endometrioid adenocarci-
223Epithelial tumours and related lesions
Fig. 4.03 Endometrioid adenocarcinoma. The bizarre nuclear atypia raises the tumour grade but should alsoprompt consideration of a serous adenocarcinoma.
Fig. 4.04 Well differentiated endometrioid adenocarcinoma, ciliated cell variant. Cilia lining the neoplasticglands are prominent.
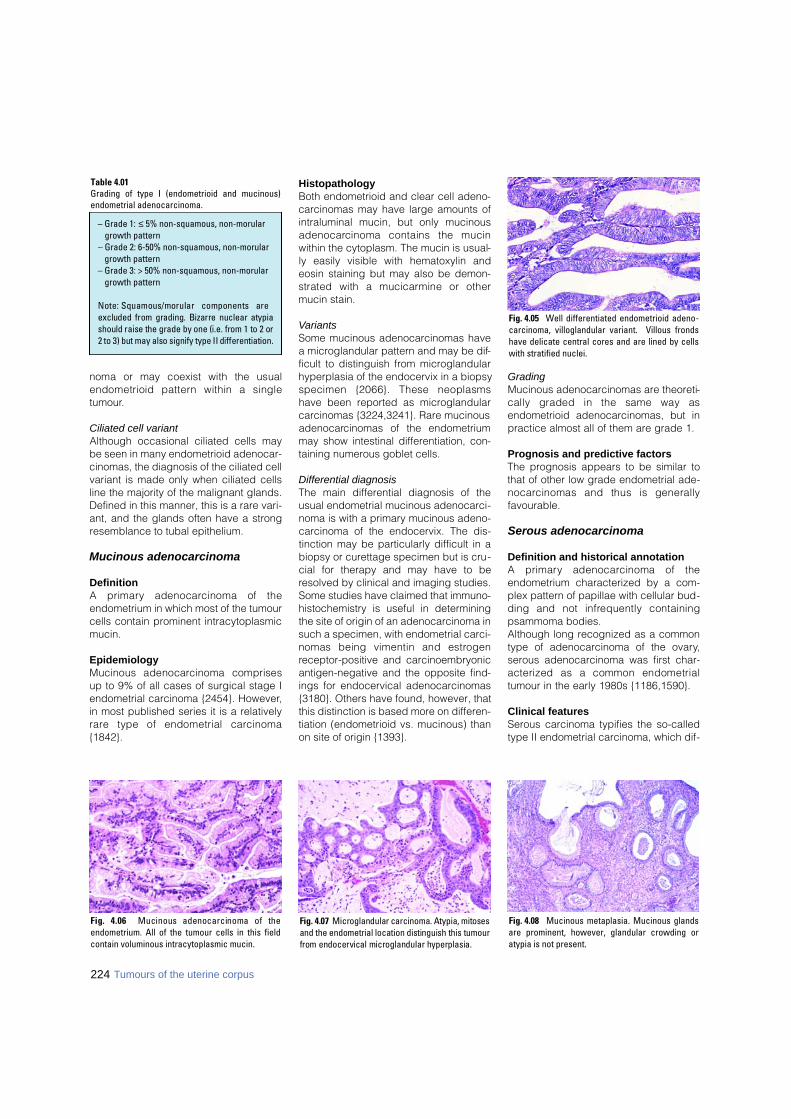
noma or may coexist with the usualendometrioid pattern within a singletumour.
Ciliated cell variantAlthough occasional ciliated cells maybe seen in many endometrioid adenocar-cinomas, the diagnosis of the ciliated cellvariant is made only when ciliated cellsline the majority of the malignant glands.Defined in this manner, this is a rare vari-ant, and the glands often have a strongresemblance to tubal epithelium.
Mucinous adenocarcinoma
DefinitionA primary adenocarcinoma of theendometrium in which most of the tumourcells contain prominent intracytoplasmicmucin.
EpidemiologyMucinous adenocarcinoma comprisesup to 9% of all cases of surgical stage Iendometrial carcinoma {2454}. However,in most published series it is a relativelyr a re type of endometrial carc i n o m a{1842}.
HistopathologyBoth endometrioid and clear cell adeno-carcinomas may have large amounts ofintraluminal mucin, but only mucinousa d e n o c a rcinoma contains the mucinwithin the cytoplasm. The mucin is usual-ly easily visible with hematoxylin andeosin staining but may also be demon-strated with a mucicarmine or othermucin stain.
VariantsSome mucinous adenocarcinomas havea microglandular pattern and may be dif-ficult to distinguish from microglandularhyperplasia of the endocervix in a biopsyspecimen {2066}. These neoplasmshave been reported as microglandularcarcinomas {3224,3241}. Rare mucinousa d e n o c a rcinomas of the endometriummay show intestinal differentiation, con-taining numerous goblet cells.
Differential diagnosisThe main differential diagnosis of theusual endometrial mucinous adenocarci-noma is with a primary mucinous adeno-carcinoma of the endocervix. The dis-tinction may be particularly difficult in abiopsy or curettage specimen but is cru-cial for therapy and may have to beresolved by clinical and imaging studies.Some studies have claimed that immuno-histochemistry is useful in determiningthe site of origin of an adenocarcinoma insuch a specimen, with endometrial carci-nomas being vimentin and estro g e nreceptor-positive and carcinoembryonicantigen-negative and the opposite find-ings for endocervical adenocarcinomas{3180}. Others have found, however, thatthis distinction is based more on differen-tiation (endometrioid vs. mucinous) thanon site of origin {1393}.
GradingMucinous adenocarcinomas are theoreti-cally graded in the same way asendometrioid adenocarcinomas, but inpractice almost all of them are grade 1.
Prognosis and predictive factorsThe prognosis appears to be similar tothat of other low grade endometrial ade-n o c a rcinomas and thus is generallyfavourable.
Serous adenocarcinoma
Definition and historical annotationA primary adenocarcinoma of theendometrium characterized by a com-plex pattern of papillae with cellular bud-ding and not infrequently containingpsammoma bodies.Although long recognized as a commontype of adenocarcinoma of the ovary,serous adenocarcinoma was first char-acterized as a common endometrialtumour in the early 1980s {1186,1590}.
Clinical featuresSerous carcinoma typifies the so-calledtype II endometrial carcinoma, which dif-
Fig. 4.06 Mucinous adenocarcinoma of theendometrium. All of the tumour cells in this fieldcontain voluminous intracytoplasmic mucin.
Fig. 4.07 Microglandular carcinoma. Atypia, mitosesand the endometrial location distinguish this tumourfrom endocervical microglandular hyperplasia.
Fig. 4.08 Mucinous metaplasia. Mucinous glandsare prominent, however, glandular crowding oratypia is not present.
Table 4.01Grading of type I (endometrioid and mucinous)endometrial adenocarcinoma.
– Grade 1: ≤ 5% non-squamous, non-morulargrowth pattern
– Grade 2: 6-50% non-squamous, non-morulargrowth pattern
– Grade 3: > 50% non-squamous, non-morulargrowth pattern
Note: Squamous/morular components areexcluded from grading. Bizarre nuclear atypiashould raise the grade by one (i.e. from 1 to 2 or2 to 3) but may also signify type II differentiation.
Fig. 4.05 Well differentiated endometrioid adeno-carcinoma, villoglandular variant. Villous frondshave delicate central cores and are lined by cellswith stratified nuclei.
224 Tumours of the uterine corpus
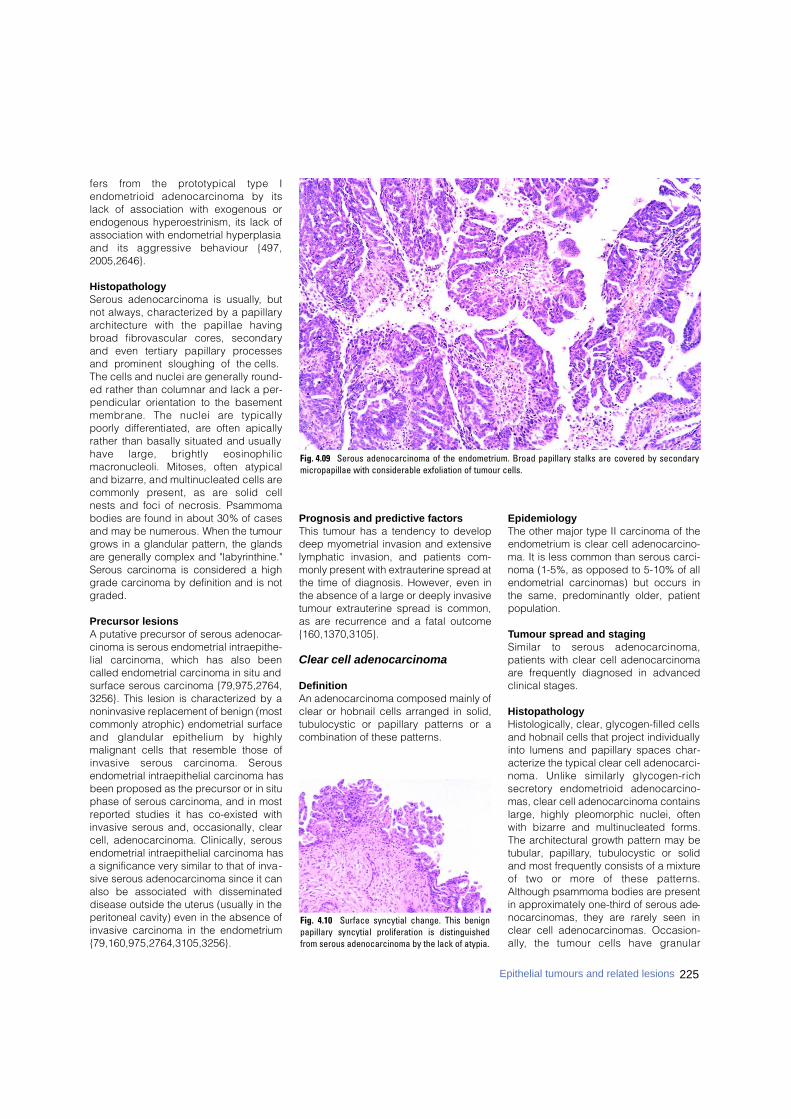
225Epithelial tumours and related lesions
fers from the prototypical type Iendometrioid adenocarcinoma by itslack of association with exogenous orendogenous hyperoestrinism, its lack ofassociation with endometrial hyperplasiaand its aggressive behaviour {497,2005,2646}.
HistopathologyS e rous adenocarcinoma is usually, butnot always, characterized by a papillarya rc h i t e c t u re with the papillae havingb road fibrovascular cores, secondaryand even tert i a ry papillary pro c e s s e sand prominent sloughing of the cells.The cells and nuclei are generally ro u n d-ed rather than columnar and lack a per-pendicular orientation to the basementmembrane. The nuclei are typicallypoorly diff e rentiated, are often apicallyrather than basally situated and usuallyhave large, brightly eosinophilicm a c ronucleoli. Mitoses, often atypicaland bizarre, and multinucleated cells arecommonly present, as are solid cellnests and foci of necrosis. Psammomabodies are found in about 30% of casesand may be numerous. When the tumourg rows in a glandular pattern, the glandsa re generally complex and "labyrinthine."S e rous carcinoma is considered a highgrade carcinoma by definition and is notgraded.
Precursor lesionsA putative precursor of serous adenocar-cinoma is serous endometrial intraepithe-lial carcinoma, which has also beencalled endometrial carcinoma in situ andsurface serous carcinoma {79,975,2764,3256}. This lesion is characterized by anoninvasive replacement of benign (mostcommonly atrophic) endometrial surfaceand glandular epithelium by highlymalignant cells that resemble those ofinvasive serous carcinoma. Sero u sendometrial intraepithelial carcinoma hasbeen proposed as the precursor or in situphase of serous carcinoma, and in mostreported studies it has co-existed withinvasive serous and, occasionally, clearcell, adenocarcinoma. Clinically, serousendometrial intraepithelial carcinoma hasa significance very similar to that of inva-sive serous adenocarcinoma since it canalso be associated with disseminateddisease outside the uterus (usually in theperitoneal cavity) even in the absence ofinvasive carcinoma in the endometrium{79,160,975,2764,3105,3256}.
Prognosis and predictive factorsThis tumour has a tendency to developdeep myometrial invasion and extensivelymphatic invasion, and patients com-monly present with extrauterine spread atthe time of diagnosis. However, even inthe absence of a large or deeply invasivetumour extrauterine spread is common,as are recurrence and a fatal outcome{160,1370,3105}.
Clear cell adenocarcinoma
DefinitionAn adenocarcinoma composed mainly ofclear or hobnail cells arranged in solid,tubulocystic or papillary patterns or acombination of these patterns.
EpidemiologyThe other major type II carcinoma of theendometrium is clear cell adenocarcino-ma. It is less common than serous carci-noma (1-5%, as opposed to 5-10% of allendometrial carcinomas) but occurs inthe same, predominantly older, patientpopulation.
Tumour spread and stagingSimilar to serous adenocarc i n o m a ,patients with clear cell adenocarcinomaare frequently diagnosed in advancedclinical stages.
HistopathologyHistologically, clear, glycogen-filled cellsand hobnail cells that project individuallyinto lumens and papillary spaces char-acterize the typical clear cell adenocarci-noma. Unlike similarly glycogen-richs e c re t o ry endometrioid adenocarc i n o-mas, clear cell adenocarcinoma containslarge, highly pleomorphic nuclei, oftenwith bizarre and multinucleated forms.The architectural growth pattern may betubular, papillary, tubulocystic or solidand most frequently consists of a mixtureof two or more of these pattern s .Although psammoma bodies are presentin approximately one-third of serous ade-nocarcinomas, they are rarely seen inclear cell adenocarcinomas. Occasion-a l l y, the tumour cells have granular
Fig. 4.10 Surface syncytial change. This benignpapillary syncytial proliferation is distinguishedfrom serous adenocarcinoma by the lack of atypia.
Fig. 4.09 Serous adenocarcinoma of the endometrium. Broad papillary stalks are covered by secondarymicropapillae with considerable exfoliation of tumour cells.
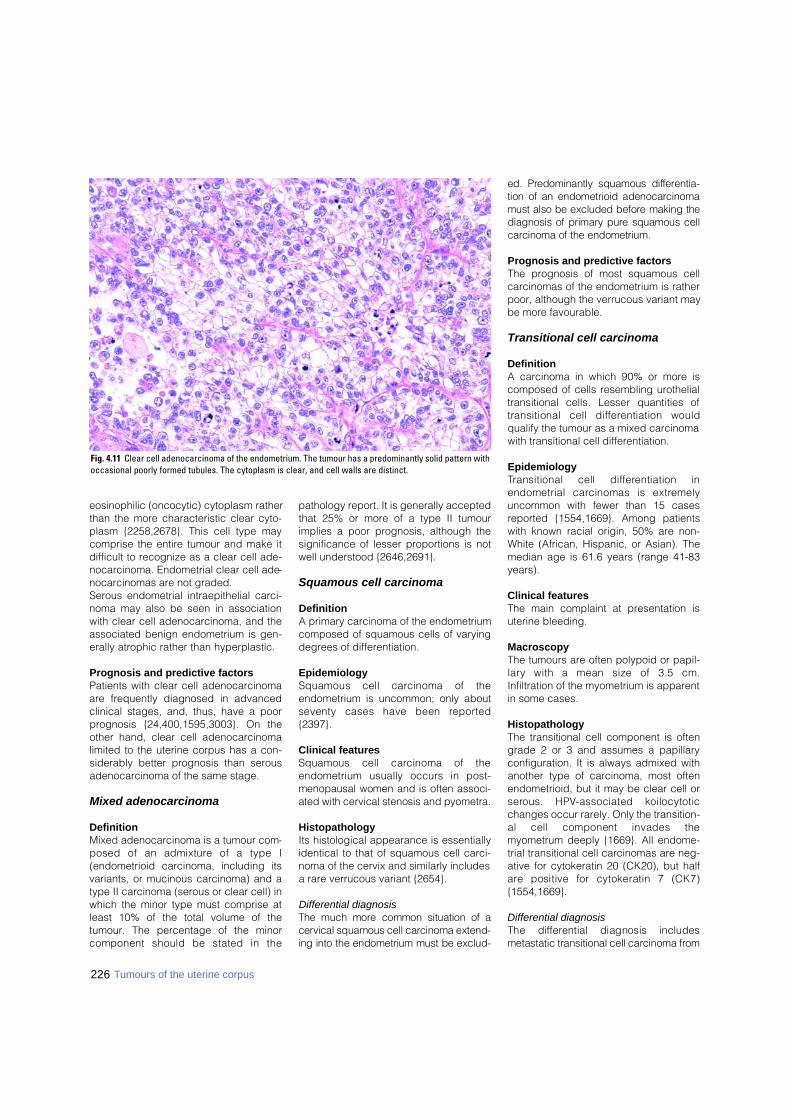
eosinophilic (oncocytic) cytoplasm ratherthan the more characteristic clear cyto-plasm {2258,2678}. This cell type maycomprise the entire tumour and make itdifficult to recognize as a clear cell ade-nocarcinoma. Endometrial clear cell ade-nocarcinomas are not graded.Serous endometrial intraepithelial carci-noma may also be seen in associationwith clear cell adenocarcinoma, and theassociated benign endometrium is gen-erally atrophic rather than hyperplastic.
Prognosis and predictive factorsPatients with clear cell adenocarcinomaare frequently diagnosed in advancedclinical stages, and, thus, have a poorp rognosis {24,400,1595,3003}. On theother hand, clear cell adenocarcinomalimited to the uterine corpus has a con-siderably better prognosis than serousadenocarcinoma of the same stage.
Mixed adenocarcinoma
DefinitionMixed adenocarcinoma is a tumour com-posed of an admixture of a type I(endometrioid carcinoma, including itsvariants, or mucinous carcinoma) and atype II carcinoma (serous or clear cell) inwhich the minor type must comprise atleast 10% of the total volume of thetumour. The percentage of the minorcomponent should be stated in the
pathology report. It is generally acceptedthat 25% or more of a type II tumourimplies a poor prognosis, although thesignificance of lesser proportions is notwell understood {2646,2691}.
Squamous cell carcinoma
DefinitionA primary carcinoma of the endometriumcomposed of squamous cells of varyingdegrees of differentiation.
EpidemiologySquamous cell carcinoma of theendometrium is uncommon; only aboutseventy cases have been re p o rt e d{2397}.
Clinical featuresSquamous cell carcinoma of theendometrium usually occurs in post-menopausal women and is often associ-ated with cervical stenosis and pyometra.
HistopathologyIts histological appearance is essentiallyidentical to that of squamous cell carci-noma of the cervix and similarly includesa rare verrucous variant {2654}.
Differential diagnosisThe much more common situation of acervical squamous cell carcinoma extend-ing into the endometrium must be exclud-
ed. Predominantly squamous diff e re n t i a-tion of an endometrioid adenocarc i n o m amust also be excluded before making thediagnosis of primary pure squamous cellc a rcinoma of the endometrium.
Prognosis and predictive factorsThe prognosis of most squamous cellcarcinomas of the endometrium is ratherpoor, although the verrucous variant maybe more favourable.
Transitional cell carcinoma
DefinitionA carcinoma in which 90% or more iscomposed of cells resembling urothelialtransitional cells. Lesser quantities oftransitional cell diff e rentiation wouldqualify the tumour as a mixed carcinomawith transitional cell differentiation.
EpidemiologyTransitional cell diff e rentiation inendometrial carcinomas is extre m e l yuncommon with fewer than 15 casesreported {1554,1669}. Among patientswith known racial origin, 50% are non-White (African, Hispanic, or Asian). Themedian age is 61.6 years (range 41-83years).
Clinical featuresThe main complaint at presentation isuterine bleeding.
MacroscopyThe tumours are often polypoid or papil-l a ry with a mean size of 3.5 cm.Infiltration of the myometrium is apparentin some cases.
HistopathologyThe transitional cell component is oftengrade 2 or 3 and assumes a papillaryconfiguration. It is always admixed withanother type of carcinoma, most oftenendometrioid, but it may be clear cell ors e rous. HPV-associated koilocytoticchanges occur rarely. Only the transition-al cell component invades themyometrum deeply {1669}. All endome-trial transitional cell carcinomas are neg-ative for cytokeratin 20 (CK20), but halfa re positive for cytokeratin 7 (CK7){1554,1669}.
Differential diagnosisThe diff e rential diagnosis includesmetastatic transitional cell carcinoma fro m
226 Tumours of the uterine corpus
Fig. 4.11 Clear cell adenocarcinoma of the endometrium. The tumour has a predominantly solid pattern withoccasional poorly formed tubules. The cytoplasm is clear, and cell walls are distinct.
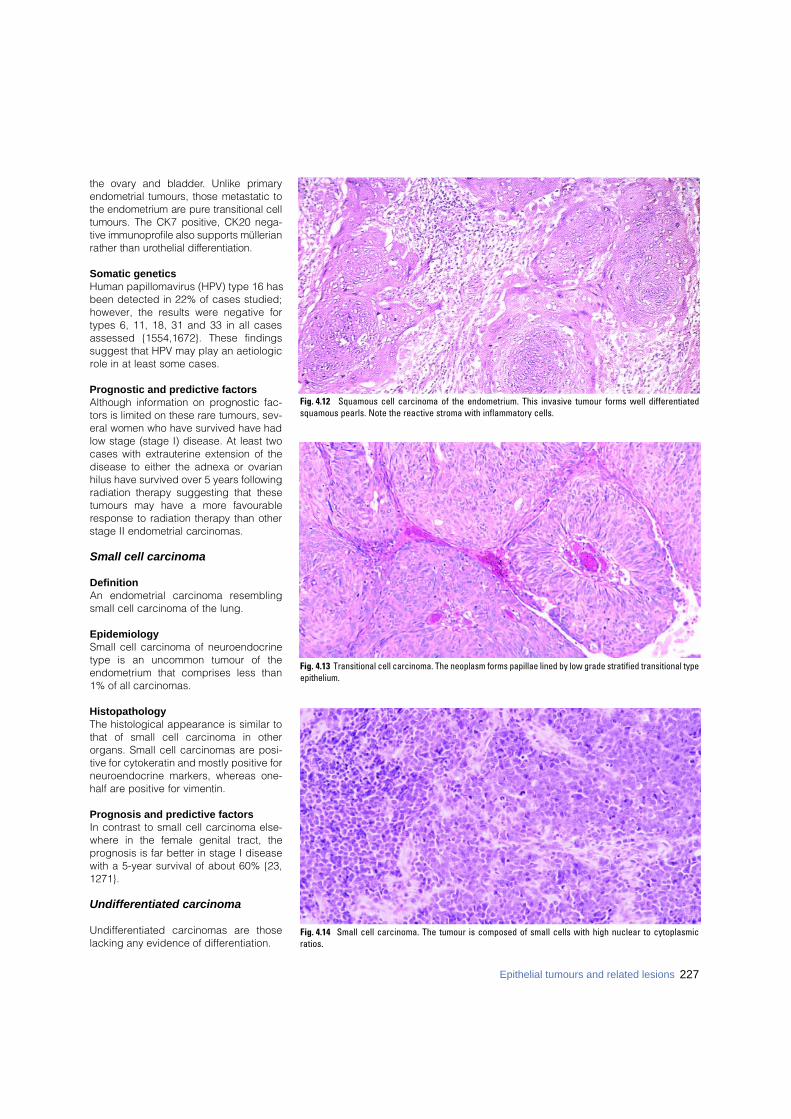
the ovary and bladder. Unlike primaryendometrial tumours, those metastatic tothe endometrium are pure transitional celltumours. The CK7 positive, CK20 nega-tive immunoprofile also supports müllerianrather than urothelial diff e re n t i a t i o n .
Somatic geneticsHuman papillomavirus (HPV) type 16 hasbeen detected in 22% of cases studied;however, the results were negative fortypes 6, 11, 18, 31 and 33 in all casesassessed {1554,1672}. These findingssuggest that HPV may play an aetiologicrole in at least some cases.
Prognostic and predictive factorsAlthough information on prognostic fac-tors is limited on these rare tumours, sev-eral women who have survived have hadlow stage (stage I) disease. At least twocases with extrauterine extension of thedisease to either the adnexa or ovarianhilus have survived over 5 years followingradiation therapy suggesting that thesetumours may have a more favourableresponse to radiation therapy than otherstage II endometrial carc i n o m a s .
Small cell carcinoma
DefinitionAn endometrial carcinoma resemblingsmall cell carcinoma of the lung.
EpidemiologySmall cell carcinoma of neuroendocrinetype is an uncommon tumour of theendometrium that comprises less than1% of all carcinomas.
HistopathologyThe histological appearance is similar tothat of small cell carcinoma in otherorgans. Small cell carcinomas are posi-tive for cytokeratin and mostly positive forneuroendocrine markers, whereas one-half are positive for vimentin.
Prognosis and predictive factorsIn contrast to small cell carcinoma else-where in the female genital tract, theprognosis is far better in stage I diseasewith a 5-year survival of about 60% {23,1271}.
Undifferentiated carcinoma
Undifferentiated carcinomas are thoselacking any evidence of differentiation.
Fig. 4.12 Squamous cell carcinoma of the endometrium. This invasive tumour forms well differentiatedsquamous pearls. Note the reactive stroma with inflammatory cells.
Fig. 4.14 Small cell carcinoma. The tumour is composed of small cells with high nuclear to cytoplasmicratios.
Fig. 4.13 Transitional cell carcinoma. The neoplasm forms papillae lined by low grade stratified transitional typeepithelium.
227Epithelial tumours and related lesions
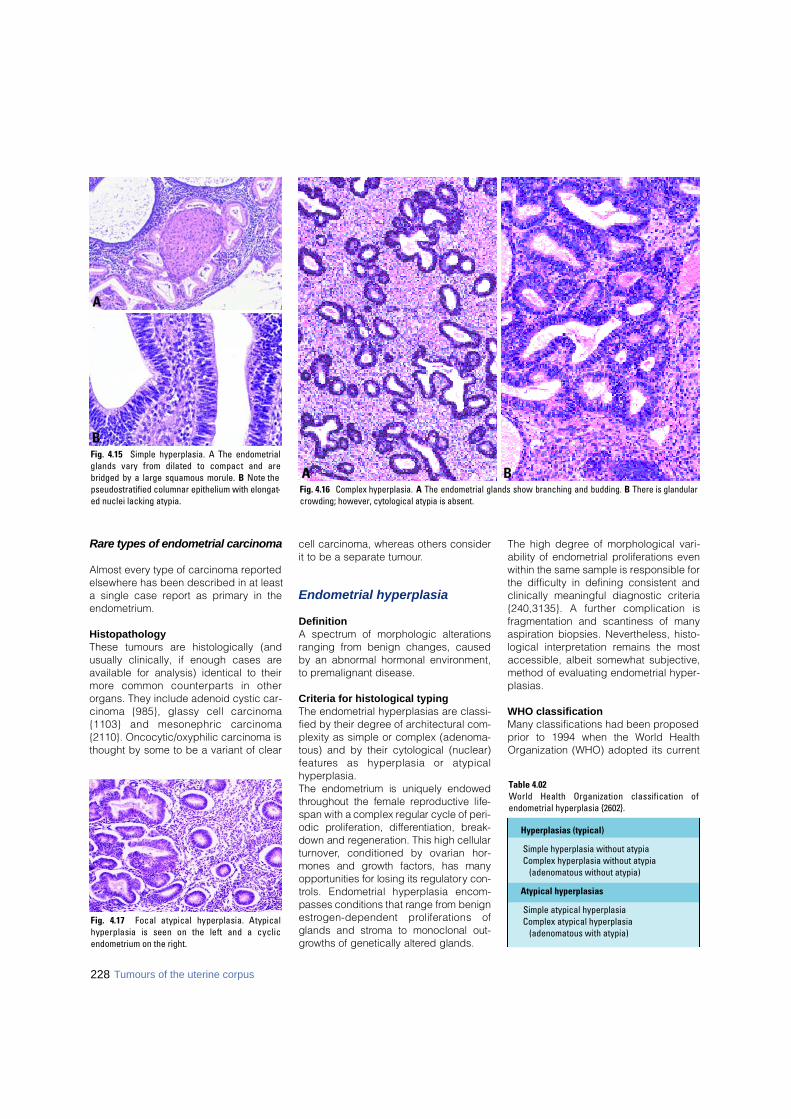
Rare types of endometrial carcinoma
Almost every type of carcinoma reportedelsewhere has been described in at leasta single case report as primary in theendometrium.
HistopathologyThese tumours are histologically (andusually clinically, if enough cases areavailable for analysis) identical to theirm o re common counterparts in otherorgans. They include adenoid cystic car-cinoma {985}, glassy cell carc i n o m a{1103} and mesonephric carc i n o m a{2110}. Oncocytic/oxyphilic carcinoma isthought by some to be a variant of clear
cell carcinoma, whereas others considerit to be a separate tumour.
Endometrial hyperplasia
DefinitionA spectrum of morphologic alterationsranging from benign changes, causedby an abnormal hormonal environment,to premalignant disease.
Criteria for histological typingThe endometrial hyperplasias are classi-fied by their degree of architectural com-plexity as simple or complex (adenoma-tous) and by their cytological (nuclear)f e a t u res as hyperplasia or atypicalhyperplasia.The endometrium is uniquely endowedt h roughout the female re p roductive life-span with a complex regular cycle of peri-odic proliferation, diff e rentiation, bre a k-down and regeneration. This high cellulart u rn o v e r, conditioned by ovarian hor-mones and growth factors, has manyo p p o rtunities for losing its re g u l a t o ry con-t rols. Endometrial hyperplasia encom-passes conditions that range from benigne s t rogen-dependent proliferations ofglands and stroma to monoclonal out-g rowths of genetically altered glands.
The high degree of morphological vari-ability of endometrial proliferations evenwithin the same sample is responsible forthe difficulty in defining consistent andclinically meaningful diagnostic criteria{240,3135}. A further complication isfragmentation and scantiness of manyaspiration biopsies. Nevertheless, histo-logical interpretation remains the mostaccessible, albeit somewhat subjective,method of evaluating endometrial hyper-plasias.
WHO classificationMany classifications had been proposedprior to 1994 when the World HealthOrganization (WHO) adopted its current
Table 4.02World Health Organization classification ofendometrial hyperplasia {2602}.
Fig. 4.17 Focal atypical hyperplasia. Atypicalhyperplasia is seen on the left and a cyclicendometrium on the right.
228 Tumours of the uterine corpus
Fig. 4.16 Complex hyperplasia. A The endometrial glands show branching and budding. B There is glandularcrowding; however, cytological atypia is absent.
BAFig. 4.15 Simple hyperplasia. A The endometrialglands vary from dilated to compact and arebridged by a large squamous morule. B Note thepseudostratified columnar epithelium with elongat-ed nuclei lacking atypia.
A
B
Hyperplasias (typical)
Simple hyperplasia without atypiaComplex hyperplasia without atypia
(adenomatous without atypia)
Atypical hyperplasias
Simple atypical hyperplasiaComplex atypical hyperplasia
(adenomatous with atypia)

schema {1535,2602}. Although this clas-sification has been widely applied, itsreproducibility is somewhat disappoint-ing {240,1433}, and molecular data withdirect implications for histological diag-nosis were unavailable at the time of the1994 classification {1956}. Nevertheless,it remains the best available classifica-tion and has been adopted in this newedition.Endometrial hyperplasias are assumedto evolve as a progressive spectrum ofendometrial glandular alterations dividedinto four separate categories by architec-ture and cytology. The vast majority ofendometrial hyperplasias mimic prolifer-ative endometria, but rare examplesdemonstrate secre t o ry features. Theentire spectrum of metaplastic changesmay be observed in hyperplasticendometria.
Hyperplasias without atypiaHyperplasias without atypia re p re s e n tthe exaggerated proliferative responseto an unopposed estrogenic stimulus;the endometrium responds in a diffusemanner with a balanced increase of bothglands and stroma. In simple hyperpla-sia the glands are tubular although fre-quently cystic or angular, and some evenshow minor epithelial budding. The liningis pseudostratified with cells displayingregular, elongated nuclei lacking atypia.In complex (adenomatous) hyperplasiathe glands display extensive complicat-ed architectural changes represented byi r regular epithelial budding into bothlumina and stroma and a typical cytologywith pseudostratified but uniform, elon-
gated and polarized glandular nuclei;squamous epithelial morules can bepresent. There is most often a shift in thegland to stroma ratio in favour of theglands.
Atypical hyperplasiasThe main feature which differentiates thiscategory from the previous one is theatypical cytology of the glandular liningas represented by loss of axial polarity,unusual nuclear shapes that are oftenrounded, irregularity in the nuclear mem-branes, prominent nucleoli and clearedor dense chromatin. Atypia occurs near-ly always focally.Simple atypical hyperplasia feature satypical glandular cytology superim-posed on the arc h i t e c t u re of simplehyperplasia. This pattern is extremelyunusual. The frequently found complexatypical (adenomatous with atypia)hyperplasia is a lesion characterized byan increased glandular complexity withi r regular outgrowths and cytologicalatypia. There may be associated foci ofnon-endometrioid differentiation such assquamous morules. Due to the expan-sion and crowding of glands, the inter-glandular stroma is diminished butremains present. Characteristic featuresof adenocarcinoma are absent.The assessment of cytological atypia isthe key problem in assigning individualcases to one of the four different WHOcategories. Definitions of cytologicalatypia are difficult to apply in theendometrium because nuclear cytologi-cal changes occur frequently in hormon-al imbalance, benign regeneration and
metaplasia {1619,2033}. Paradoxically,atypical hyperplasia may exhibit moreatypical features than adenocarcinoma{2688}, and some grade 1 invasiveendometrioid carcinomas have ane x t remely bland cytology. Perhaps, itwould be more appropriate to considercytological changes in the context ofoverall glandular architecture. Indeed,architectural focality of the lesion is soclosely linked with atypia that possiblythey are inseparable. In this way, atypiais best observed by comparison withadjoining normal glands.
Caveat: sampling problemsThe focal nature of atypical endometrialhyperplasias may allow young women tomaintain fertility, but has the disadvan-tage of possible underdiagnosis due toincomplete sampling. The problem isg reatest in scanty fragmented speci-mens, something commonly encoun-tered in routine office biopsies. Clearly,this situation is responsible for the falsenegative biopsies during follow up. Hysteroscopic direction may assist in tar-geting a macroscopically apparent local-ized lesion but is not a common practicein most settings.
Contemporary approach to endometrial hyperplasiaPoor reproducibility of the 1994 WHOhyperplasia schema {240,1433} has ledto a proposal to reduce the number ofdiagnostic classes {240}. New conceptsof pathogenesis have been incorporatedinto an integrated genetic, histomorpho-metric and clinical outcome model of
BAFig. 4.18 Complex atypical hyperplasia. A There is glandular crowding with eosinophilic cytoplasm and nuclear enlargement, loss of polarity and prominent nucle-oli. On the right is a residual, non-atypical cystic gland. B The glands are tortuous with epithelial tufts (reflecting abnormal polarity) protruding into the lumens andshow cytological atypia.
229Epithelial tumours and related lesions
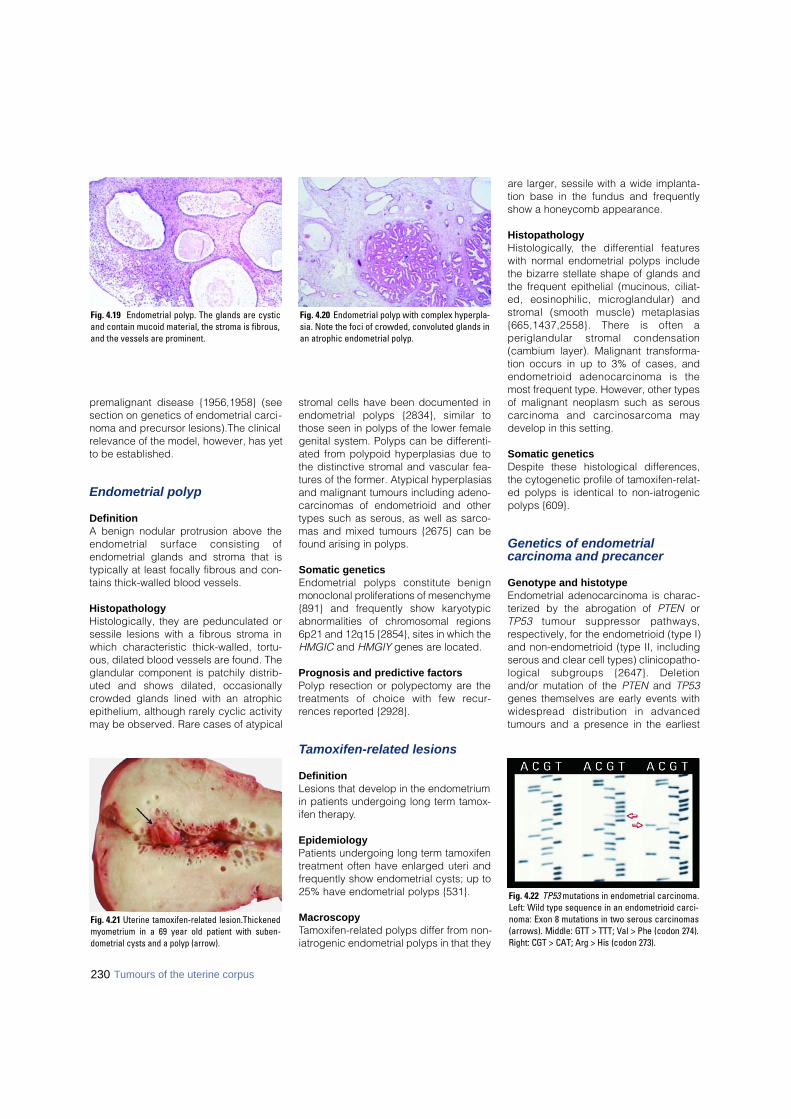
230 Tumours of the uterine corpus
premalignant disease {1956,1958} (seesection on genetics of endometrial carci-noma and precursor lesions).The clinicalrelevance of the model, however, has yetto be established.
Endometrial polyp
DefinitionA benign nodular protrusion above theendometrial surface consisting ofendometrial glands and stroma that istypically at least focally fibrous and con-tains thick-walled blood vessels.
HistopathologyHistologically, they are pedunculated orsessile lesions with a fibrous stroma inwhich characteristic thick-walled, tortu-ous, dilated blood vessels are found. Theglandular component is patchily distrib-uted and shows dilated, occasionallycrowded glands lined with an atrophicepithelium, although rarely cyclic activitymay be observed. Rare cases of atypical
stromal cells have been documented inendometrial polyps {2834}, similar tothose seen in polyps of the lower femalegenital system. Polyps can be differenti-ated from polypoid hyperplasias due tothe distinctive stromal and vascular fea-tures of the former. Atypical hyperplasiasand malignant tumours including adeno-carcinomas of endometrioid and othertypes such as serous, as well as sarco-mas and mixed tumours {2675} can befound arising in polyps.
Somatic geneticsEndometrial polyps constitute benignmonoclonal proliferations of mesenchyme{891} and frequently show kary o t y p i ca b n o rmalities of chromosomal re g i o n s6p21 and 12q15 {2854}, sites in which theH M G I C and H M G I Y genes are located.
Prognosis and predictive factorsPolyp resection or polypectomy are thet reatments of choice with few re c u r-rences reported {2928}.
Tamoxifen-related lesions
DefinitionLesions that develop in the endometriumin patients undergoing long term tamox-ifen therapy.
EpidemiologyPatients undergoing long term tamoxifentreatment often have enlarged uteri andfrequently show endometrial cysts; up to25% have endometrial polyps {531}.
MacroscopyTamoxifen-related polyps differ from non-iatrogenic endometrial polyps in that they
are larger, sessile with a wide implanta-tion base in the fundus and frequentlyshow a honeycomb appearance.
HistopathologyH i s t o l o g i c a l l y, the diff e rential feature swith normal endometrial polyps includethe bizarre stellate shape of glands andthe frequent epithelial (mucinous, ciliat-ed, eosinophilic, microglandular) ands t romal (smooth muscle) metaplasias{665,1437,2558}. There is often aperiglandular stromal condensation(cambium layer). Malignant transforma-tion occurs in up to 3% of cases, andendometrioid adenocarcinoma is themost frequent type. However, other typesof malignant neoplasm such as serousc a rcinoma and carc i n o s a rcoma maydevelop in this setting.
Somatic geneticsDespite these histological differences,the cytogenetic profile of tamoxifen-relat-ed polyps is identical to non-iatrogenicpolyps {609}.
Genetics of endometrial carcinoma and precancer
Genotype and histotypeEndometrial adenocarcinoma is charac-terized by the abrogation of PTEN orT P 5 3 tumour suppressor pathways,respectively, for the endometrioid (type I)and non-endometrioid (type II, includingserous and clear cell types) clinicopatho-logical subgroups {2647}. Deletionand/or mutation of the PTEN and TP53genes themselves are early events withw i d e s p read distribution in advancedtumours and a presence in the earliest
Fig. 4.22 TP53 mutations in endometrial carcinoma.Left: Wild type sequence in an endometrioid carci-noma: Exon 8 mutations in two serous carcinomas(arrows). Middle: GTT > TTT; Val > Phe (codon 274).R i g h t : CGT > CAT; Arg > His (codon 273).
Fig. 4.21 Uterine tamoxifen-related lesion.Thickenedmyometrium in a 69 year old patient with suben-dometrial cysts and a polyp (arrow).
Fig. 4.19 Endometrial polyp. The glands are cysticand contain mucoid material, the stroma is fibrous,and the vessels are prominent.
Fig. 4.20 Endometrial polyp with complex hyperpla-sia. Note the foci of crowded, convoluted glands inan atrophic endometrial polyp.
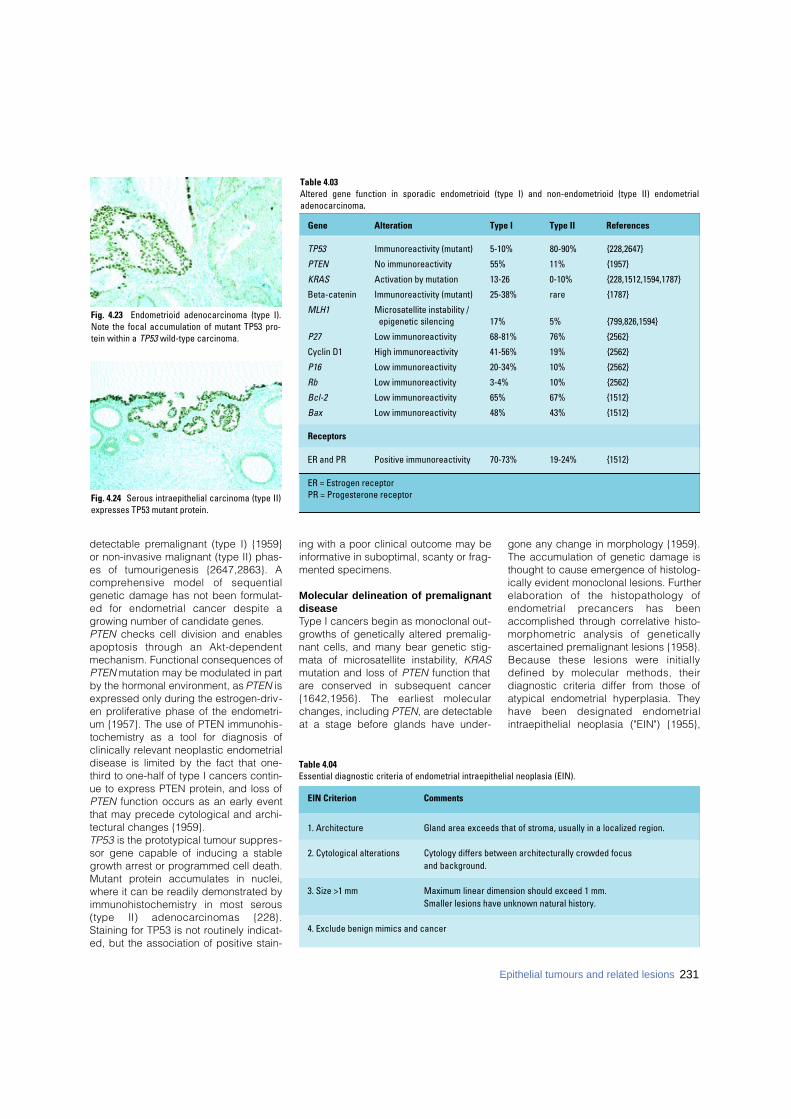
detectable premalignant (type I) {1959}or non-invasive malignant (type II) phas-es of tumourigenesis {2647,2863}. Ac o m p rehensive model of sequentialgenetic damage has not been formulat-ed for endometrial cancer despite agrowing number of candidate genes.PTEN checks cell division and enablesapoptosis through an Akt-dependentmechanism. Functional consequences ofPTEN mutation may be modulated in partby the hormonal environment, as PTEN isexpressed only during the estrogen-driv-en proliferative phase of the endometri-um {1957}. The use of PTEN immunohis-tochemistry as a tool for diagnosis ofclinically relevant neoplastic endometrialdisease is limited by the fact that one-third to one-half of type I cancers contin-ue to express PTEN protein, and loss ofPTEN function occurs as an early eventthat may precede cytological and archi-tectural changes {1959}. TP53 is the prototypical tumour suppres-sor gene capable of inducing a stablegrowth arrest or programmed cell death.Mutant protein accumulates in nuclei,where it can be readily demonstrated byi m m u n o h i s t o c h e m i s t ry in most sero u s(type II) adenocarcinomas {228}.Staining for TP53 is not routinely indicat-ed, but the association of positive stain-
ing with a poor clinical outcome may beinformative in suboptimal, scanty or frag-mented specimens.
Molecular delineation of premalignantdiseaseType I cancers begin as monoclonal out-growths of genetically altered premalig-nant cells, and many bear genetic stig-mata of microsatellite instability, KRASmutation and loss of PTEN function thata re conserved in subsequent cancer{1642,1956}. The earliest molecularchanges, including PTEN, are detectableat a stage before glands have under-
gone any change in morphology {1959}.The accumulation of genetic damage isthought to cause emergence of histolog-ically evident monoclonal lesions. Furtherelaboration of the histopathology ofendometrial precancers has beenaccomplished through correlative histo-morphometric analysis of geneticallyascertained premalignant lesions {1958}.Because these lesions were initiallydefined by molecular methods, theirdiagnostic criteria differ from those ofatypical endometrial hyperplasia. Theyhave been designated endometrialintraepithelial neoplasia ("EIN") {1955},
Fig. 4.23 Endometrioid adenocarcinoma (type I).Note the focal accumulation of mutant TP53 pro-tein within a TP53 wild-type carcinoma.
Fig. 4.24 Serous intraepithelial carcinoma (type II)expresses TP53 mutant protein.
Table 4.04Essential diagnostic criteria of endometrial intraepithelial neoplasia (EIN).
Table 4.03Altered gene function in sporadic endometrioid (type I) and non-endometrioid (type II) endometrial adenocarcinoma.
Gene Alteration Type I Type II References
TP53 Immunoreactivity (mutant) 5-10% 80-90% {228,2647}
PTEN No immunoreactivity 55% 11% {1957}
KRAS Activation by mutation 13-26 0-10% {228,1512,1594,1787}
Beta-catenin Immunoreactivity (mutant) 25-38% rare {1787}
MLH1 Microsatellite instability /epigenetic silencing 17% 5% {799,826,1594}
P27 Low immunoreactivity 68-81% 76% {2562}
Cyclin D1 High immunoreactivity 41-56% 19% {2562}
P16 Low immunoreactivity 20-34% 10% {2562}
Rb Low immunoreactivity 3-4% 10% {2562}
Bcl-2 Low immunoreactivity 65% 67% {1512}
Bax Low immunoreactivity 48% 43% {1512}
Receptors
ER and PR Positive immunoreactivity 70-73% 19-24% {1512}
ER = Estrogen receptor PR = Progesterone receptor
EIN Criterion Comments
1. Architecture Gland area exceeds that of stroma, usually in a localized region.
2. Cytological alterations Cytology differs between architecturally crowded focus and background.
3. Size >1 mm Maximum linear dimension should exceed 1 mm. Smaller lesions have unknown natural history.
4. Exclude benign mimics and cancer
231Epithelial tumours and related lesions

232 Tumours of the uterine corpus
and many examples with corre l a t i v egenotypes and morphometry can beseen online at www.endometrium.org.
Endometrial intraepithelial neoplasia (EIN)This lesion is defined as the histopatho-logical presentation of pre m a l i g n a n tendometrial disease as identified by inte-grated molecular genetic, histomorpho-metric and clinical outcome data. Tissuemorphometry (D-Score {153} predictiveof cancer outcome) and genetic studiesare cross validating in that these method-ologically independent techniques pro-vide concordant identification of EINlesions when applied to a common poolof study material {1958}. The EIN schemepartitions endometrial proliferations intodifferent therapeutic groups. Distinctivediagnostic categories include: (1) Benign architectural changes ofunopposed estrogens (endometrialhyperplasia).(2) EIN.(3) Well differentiated adenocarcinoma.
The histological changes produced byunopposed estrogens (non-atypicalhyperplasias) are quite unlike localizingEIN lesions. The latter originate focallyt h rough monoclonal outgrowth of amutant epithelial clone with altered cytol-ogy and arc h i t e c t u re. Computerizedmorphometric analysis, which quantifiesspecific architectural patterns associat-ed with increased clinical cancer risk{154}, objectively defined the morpholo-gy of monoclonal EIN lesions. Becauseof differing diagnostic criteria, only 79%of atypical endometrial hyperplasiastranslate to EIN, and approximately athird of all EIN diagnoses are garneredf rom non-atypical hyperplasia cate-gories.
Genetic susceptibilityThe overwhelming majority of endometri -al cancers are sporadic, but they mayrarely present as a manifestation of mul-
ticancer familial syndromes. Examplesinclude here d i t a ry nonpolyposis coloncancer (HNPCC), caused by mutation ofDNA mismatch repair genes that pro-duce constitutive microsatellite instability{799} and Cowden syndrome in patientswith germline PTEN inactivation {1957}.
Prognosis and predictive factorsIn addition to tumour type and, for type Iadenocarcinomas, tumour grade, otherhistological and non-histological deter-minations influence the prognosis ofendometrial carcinoma. The most impor-tant of these is the surgical stage, whichin 1988 replaced the clinical staging sys-tem that had been in use for many years{2642}. The extent of surgical stagingperformed is based in part on the med-ical condition of the patient and in part onthe preoperative or intraoperativeassessment of tumour risk factors suchas type and grade, depth of myometrialinvasion and extension to involve thecervix {2692,2714}.Myometrial invasion is thus an importantissue, both as a prognostic factor in itsown right and as a determinant of theextent of staging and of subsequent ther-apy in cases treated by hysterectomy.FIGO divides stage I tumours into IA (lim-ited to the endometrium), IB (invasion ofless than half of the myometrium), and IC(invasion of more than half of themyometrium), {51,2976}. Some oncolo-gists, however, make treatment decisionsbased on thirds (inner, mid, outer) ofmyometrial invasion or distance in mil-limetres (mm) from the serosal surface.Thus, the pathologist can best satisfy thed e s i res for all of this information byreporting the maximal depth of tumourinvasion from the endomyometrial junc-tion and the thickness of the myometriumat that point (e.g. 7 mm tumour invasioninto a 15 mm thick myometrium) {2686}.True myometrial invasion must be distin-guished from carcinomatous extension(not invasion) into pre-existing "tongues"
of endometrium penetrating themyometrium or into foci (sometimesdeep-seated) of adenomyosis {2652,2688}. It should also be noted thattumour extension to the uterine serosaraises the stage to IIIA. Vascular or lym-phatic space invasion is an unfavourableprognostic factor that should be reported{78}. Perivascular lymphocytic infiltratesmay be the first clue to vascular invasionand, thus, should prompt deeper levelswithin the suspect block and/or the sub-mission of more tissue sections for histo-logical examination.It is also important to evaluate cervicalinvolvement in the hysterectomy speci-men since extension to the cervix raisesthe stage to II. The distinction betweenstage IIA and IIB is based on whether theextension involves the endocervical sur-face and/or underlying glands only orinvades the cervical stroma. One shouldbe aware that an adenocarcinoma involv-ing glands only might be an entirely sep-arate adenocarcinoma in situ primary inthe endocervix.Non-histological factors may also play arole in determining the prognosis ofendometrial carcinoma. It is unclear atthe present time, however, what thecost/benefit ratio of performing addition-al studies might be since the prognosisand treatment are currently based on thecombination of tumour type, grade,where appropriate, and extent, as dis-cussed above. Nevertheless, patientswith carcinomas of intermediate progno-sis, such as stage I well differentiatedendometrioid adenocarcinoma with focaldeep myometrial invasion might benefitf rom additional information includingsuch factors as tumour ploidy{1349,1441}, hormone receptor status{575,1441}, tumour suppressor genes{1309,1449}, oncogenes {1205,1449},p roliferation markers {966,1449,2012}and morphometry {2751}. Which, if any,of these or other studies will prove to bemost useful is problematic at this time.
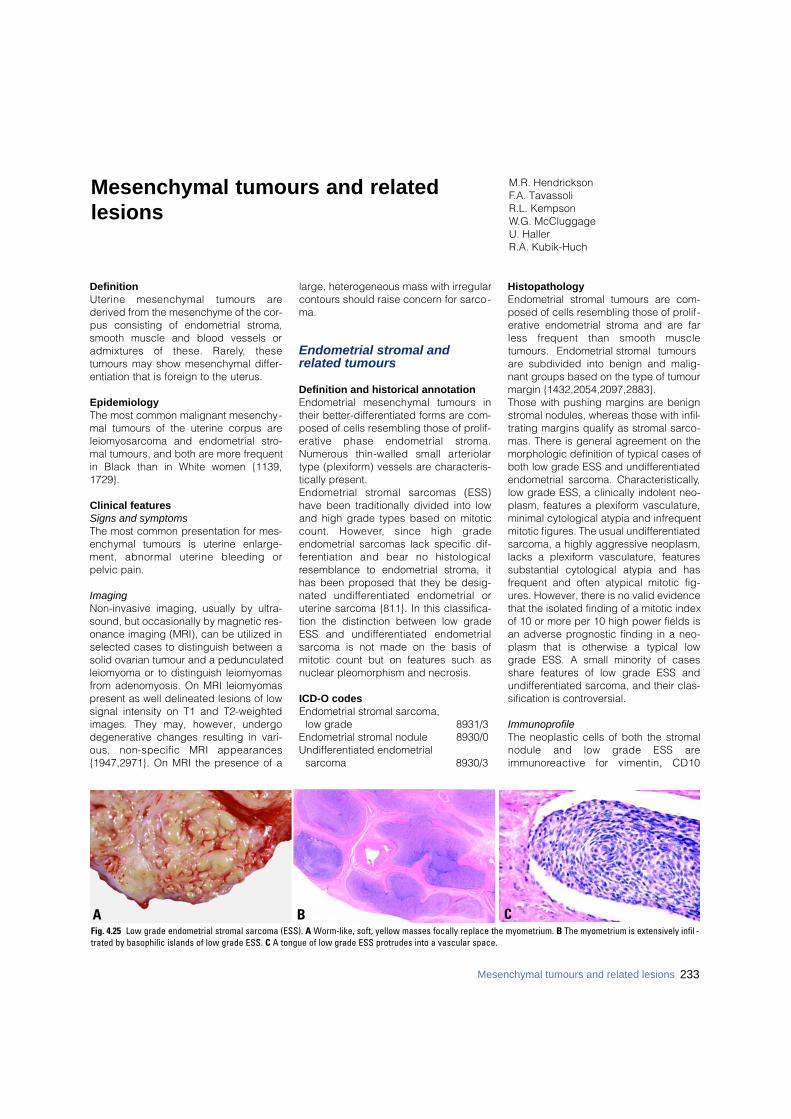
DefinitionUterine mesenchymal tumours arederived from the mesenchyme of the cor-pus consisting of endometrial stroma,smooth muscle and blood vessels ora d m i x t u res of these. Rare l y, thesetumours may show mesenchymal differ-entiation that is foreign to the uterus.
EpidemiologyThe most common malignant mesenchy-mal tumours of the uterine corpus areleiomyosarcoma and endometrial stro-mal tumours, and both are more frequentin Black than in White women {1139,1729}.
Clinical featuresSigns and symptomsThe most common presentation for mes-enchymal tumours is uterine enlarge-ment, abnormal uterine bleeding orpelvic pain.
ImagingNon-invasive imaging, usually by ultra-sound, but occasionally by magnetic res-onance imaging (MRI), can be utilized inselected cases to distinguish between asolid ovarian tumour and a pedunculatedleiomyoma or to distinguish leiomyomasfrom adenomyosis. On MRI leiomyomaspresent as well delineated lesions of lowsignal intensity on T1 and T2-weightedimages. They may, however, undergodegenerative changes resulting in vari-ous, non-specific MRI appearances{1947,2971}. On MRI the presence of a
large, heterogeneous mass with irregularcontours should raise concern for sarco-ma.
Endometrial stromal and related tumours
Definition and historical annotationEndometrial mesenchymal tumours intheir better-differentiated forms are com-posed of cells resembling those of prolif-erative phase endometrial stro m a .N u m e rous thin-walled small art e r i o l a rtype (plexiform) vessels are characteris-tically present. Endometrial stromal sarcomas (ESS)have been traditionally divided into lowand high grade types based on mitoticcount. However, since high gradeendometrial sarcomas lack specific dif-f e rentiation and bear no histologicalresemblance to endometrial stroma, ithas been proposed that they be desig-nated undiff e rentiated endometrial oruterine sarcoma {811}. In this classifica-tion the distinction between low gradeESS and undiff e rentiated endometrialsarcoma is not made on the basis ofmitotic count but on features such asnuclear pleomorphism and necrosis.
ICD-O codesEndometrial stromal sarcoma,
low grade 8931/3Endometrial stromal nodule 8930/0Undifferentiated endometrial
sarcoma 8930/3
HistopathologyEndometrial stromal tumours are com-posed of cells resembling those of prolif-erative endometrial stroma and are farless frequent than smooth muscletumours. Endometrial stromal tumoursare subdivided into benign and malig-nant groups based on the type of tumourmargin {1432,2054,2097,2883}. Those with pushing margins are benignstromal nodules, whereas those with infil-trating margins qualify as stromal sarco-mas. There is general agreement on themorphologic definition of typical cases ofboth low grade ESS and undifferentiatedendometrial sarcoma. Characteristically,low grade ESS, a clinically indolent neo-plasm, features a plexiform vasculature,minimal cytological atypia and infrequentmitotic figures. The usual undifferentiatedsarcoma, a highly aggressive neoplasm,lacks a plexiform vasculature, featuressubstantial cytological atypia and hasfrequent and often atypical mitotic fig-ures. However, there is no valid evidencethat the isolated finding of a mitotic indexof 10 or more per 10 high power fields isan adverse prognostic finding in a neo-plasm that is otherwise a typical lowgrade ESS. A small minority of casesshare features of low grade ESS andundifferentiated sarcoma, and their clas-sification is controversial.
Immunoprofile The neoplastic cells of both the stromalnodule and low grade ESS arei m m u n o reactive for vimentin, CD10
M.R. HendricksonF.A. TavassoliR.L. KempsonW.G. McCluggageU. HallerR.A. Kubik-Huch
Mesenchymal tumours and relatedlesions
BAFig. 4.25 Low grade endometrial stromal sarcoma (ESS). A Worm-like, soft, yellow masses focally replace the myometrium. B The myometrium is extensively infil -trated by basophilic islands of low grade ESS. C A tongue of low grade ESS protrudes into a vascular space.
C
233Mesenchymal tumours and related lesions
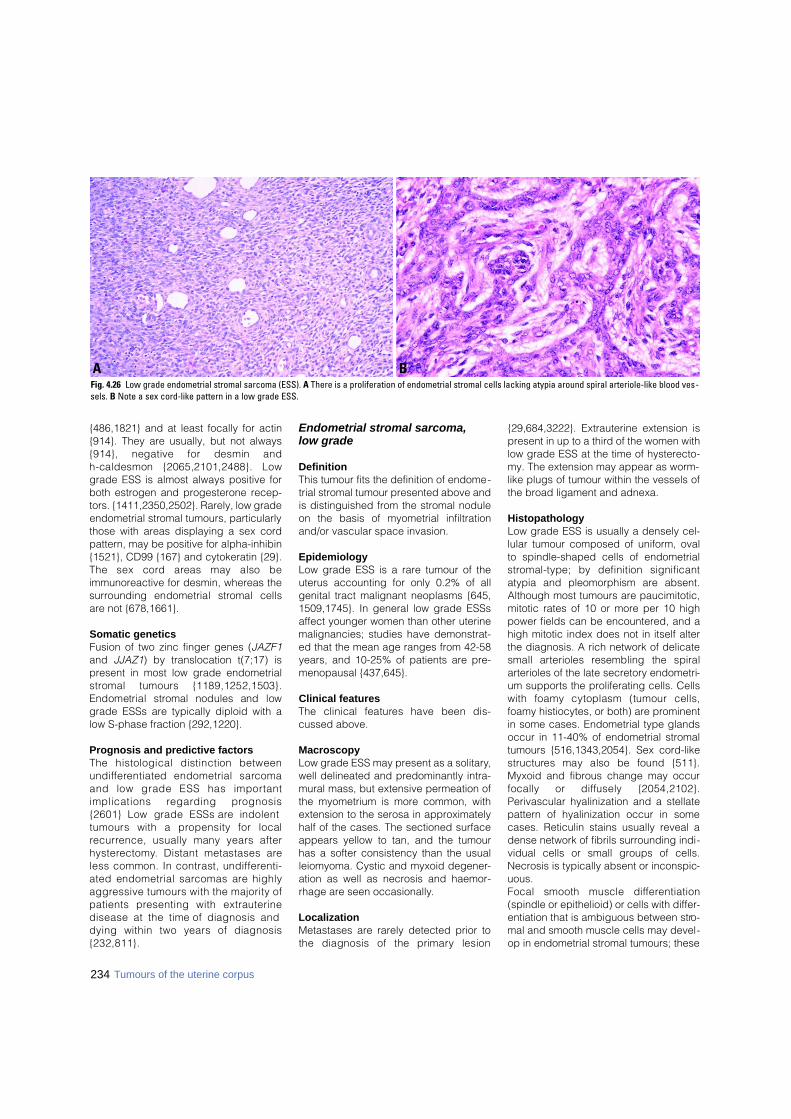
234 Tumours of the uterine corpus
{486,1821} and at least focally for actin{914}. They are usually, but not always{914}, negative for desmin and h-caldesmon {2065,2101,2488}. Lowgrade ESS is almost always positive forboth estrogen and progesterone recep-tors. {1411,2350,2502}. Rarely, low gradeendometrial stromal tumours, particularlythose with areas displaying a sex cordpattern, may be positive for alpha-inhibin{1521}, CD99 {167} and cytokeratin {29}.The sex cord areas may also beimmunoreactive for desmin, whereas thes u r rounding endometrial stromal cellsare not {678,1661}.
Somatic genetics Fusion of two zinc finger genes (JAZF1and JJAZ1) by translocation t(7;17) ispresent in most low grade endometrials t romal tumours {1189,1252,1503}.Endometrial stromal nodules and lowgrade ESSs are typically diploid with alow S-phase fraction {292,1220}.
Prognosis and predictive factorsThe histological distinction betweenu n d i ff e rentiated endometrial sarc o m aand low grade ESS has import a n timplications re g a rding pro g n o s i s{2601} Low grade ESSs are indolenttumours with a propensity for localre c u r rence, usually many years afterh y s t e re c t o m y. Distant metastases areless common. In contrast, undiff e re n t i-ated endometrial sarcomas are highlya g g ressive tumours with the majority ofpatients presenting with extrauterinedisease at the time of diagnosis anddying within two years of diagnosis{ 2 3 2 , 8 1 1 } .
Endometrial stromal sarcoma, low grade
DefinitionThis tumour fits the definition of endome-trial stromal tumour presented above andis distinguished from the stromal noduleon the basis of myometrial infiltrationand/or vascular space invasion.
EpidemiologyLow grade ESS is a rare tumour of theuterus accounting for only 0.2% of allgenital tract malignant neoplasms {645,1509,1745}. In general low grade ESSsaffect younger women than other uterinemalignancies; studies have demonstrat-ed that the mean age ranges from 42-58years, and 10-25% of patients are pre-menopausal {437,645}.
Clinical featuresThe clinical features have been dis-cussed above.
MacroscopyLow grade ESS may present as a solitary,well delineated and predominantly intra-mural mass, but extensive permeation ofthe myometrium is more common, withextension to the serosa in approximatelyhalf of the cases. The sectioned surfaceappears yellow to tan, and the tumourhas a softer consistency than the usualleiomyoma. Cystic and myxoid degener-ation as well as necrosis and haemor-rhage are seen occasionally.
LocalizationMetastases are rarely detected prior tothe diagnosis of the primary lesion
{29,684,3222}. Extrauterine extension ispresent in up to a third of the women withlow grade ESS at the time of hysterecto-my. The extension may appear as worm-like plugs of tumour within the vessels ofthe broad ligament and adnexa.
HistopathologyLow grade ESS is usually a densely cel-lular tumour composed of uniform, ovalto spindle-shaped cells of endometrials t romal-type; by definition significantatypia and pleomorphism are absent.Although most tumours are paucimitotic,mitotic rates of 10 or more per 10 highpower fields can be encountered, and ahigh mitotic index does not in itself alterthe diagnosis. A rich network of delicatesmall arterioles resembling the spiralarterioles of the late secretory endometri-um supports the proliferating cells. Cellswith foamy cytoplasm (tumour cells,foamy histiocytes, or both) are prominentin some cases. Endometrial type glandsoccur in 11-40% of endometrial stromaltumours {516,1343,2054}. Sex cord-likes t r u c t u res may also be found {511}.Myxoid and fibrous change may occurfocally or diffusely {2054,2102}.Perivascular hyalinization and a stellatepattern of hyalinization occur in somecases. Reticulin stains usually reveal adense network of fibrils surrounding indi-vidual cells or small groups of cells.Necrosis is typically absent or inconspic-uous. Focal smooth muscle diff e re n t i a t i o n(spindle or epithelioid) or cells with differ-entiation that is ambiguous between stro-mal and smooth muscle cells may devel-op in endometrial stromal tumours; these
BAFig. 4.26 Low grade endometrial stromal sarcoma (ESS). A There is a proliferation of endometrial stromal cells lacking atypia around spiral arteriole-like blood ves-sels. B Note a sex cord-like pattern in a low grade ESS.
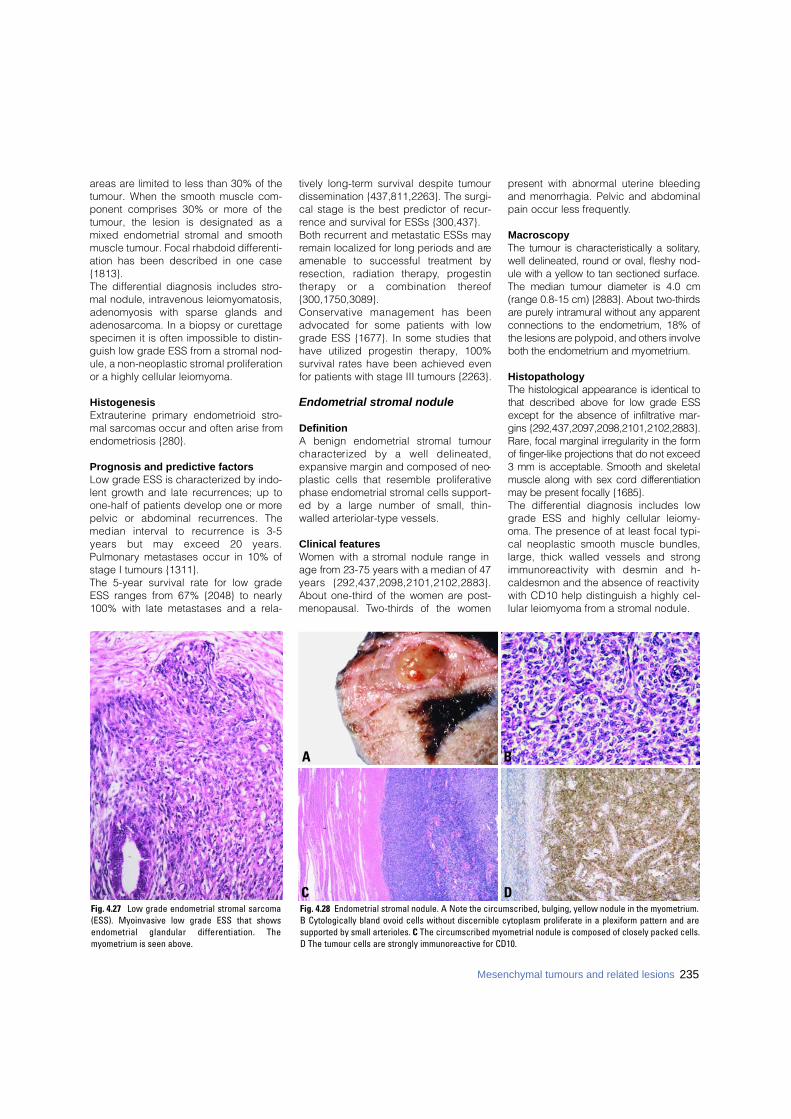
areas are limited to less than 30% of thetumour. When the smooth muscle com-ponent comprises 30% or more of thetumour, the lesion is designated as amixed endometrial stromal and smoothmuscle tumour. Focal rhabdoid differenti-ation has been described in one case{1813}. The differential diagnosis includes stro-mal nodule, intravenous leiomyomatosis,adenomyosis with sparse glands andadenosarcoma. In a biopsy or curettagespecimen it is often impossible to distin-guish low grade ESS from a stromal nod-ule, a non-neoplastic stromal proliferationor a highly cellular leiomyoma.
HistogenesisExtrauterine primary endometrioid stro-mal sarcomas occur and often arise fromendometriosis {280}.
Prognosis and predictive factors Low grade ESS is characterized by indo-lent growth and late recurrences; up toone-half of patients develop one or morepelvic or abdominal recurrences. Themedian interval to re c u r rence is 3-5years but may exceed 20 years.Pulmonary metastases occur in 10% ofstage I tumours {1311}. The 5-year survival rate for low gradeESS ranges from 67% {2048} to nearly100% with late metastases and a rela-
tively long-term survival despite tumourdissemination {437,811,2263}. The surgi-cal stage is the best predictor of recur-rence and survival for ESSs {300,437}. Both recurrent and metastatic ESSs mayremain localized for long periods and areamenable to successful treatment byresection, radiation therapy, pro g e s t i ntherapy or a combination there o f{300,1750,3089}. Conservative management has beenadvocated for some patients with lowgrade ESS {1677}. In some studies thathave utilized progestin therapy, 100%survival rates have been achieved evenfor patients with stage III tumours {2263}.
Endometrial stromal nodule
DefinitionA benign endometrial stromal tumourcharacterized by a well delineated,expansive margin and composed of neo-plastic cells that resemble proliferativephase endometrial stromal cells support-ed by a large number of small, thin-walled arteriolar-type vessels.
Clinical featuresWomen with a stromal nodule range inage from 23-75 years with a median of 47years {292,437,2098,2101,2102,2883}.About one-third of the women are post-menopausal. Tw o - t h i rds of the women
p resent with abnormal uterine bleedingand menorrhagia. Pelvic and abdominalpain occur less fre q u e n t l y.
MacroscopyThe tumour is characteristically a solitary,well delineated, round or oval, fleshy nod-ule with a yellow to tan sectioned surf a c e .The median tumour diameter is 4.0 cm(range 0.8-15 cm) {2883}. About two-third sa re purely intramural without any appare n tconnections to the endometrium, 18% ofthe lesions are polypoid, and others involveboth the endometrium and myometrium.
HistopathologyThe histological appearance is identical tothat described above for low grade ESSexcept for the absence of infiltrative mar-gins {292,437,2097,2098,2101,2102,2883}.R a re, focal marginal irregularity in the formof finger-like projections that do not exceed3 mm is acceptable. Smooth and skeletalmuscle along with sex cord diff e re n t i a t i o nmay be present focally {1685}. The differential diagnosis includes lowgrade ESS and highly cellular leiomy-oma. The presence of at least focal typi-cal neoplastic smooth muscle bundles,large, thick walled vessels and strongi m m u n o reactivity with desmin and h-caldesmon and the absence of reactivitywith CD10 help distinguish a highly cel-lular leiomyoma from a stromal nodule.
235Mesenchymal tumours and related lesions
Fig. 4.27 Low grade endometrial stromal sarcoma(ESS). Myoinvasive low grade ESS that showsendometrial glandular differentiation. Themyometrium is seen above.
BA
DCFig. 4.28 Endometrial stromal nodule. A Note the circumscribed, bulging, yellow nodule in the myometrium. B Cytologically bland ovoid cells without discernible cytoplasm proliferate in a plexiform pattern and aresupported by small arterioles. C The circumscribed myometrial nodule is composed of closely packed cells. D The tumour cells are strongly immunoreactive for CD10.
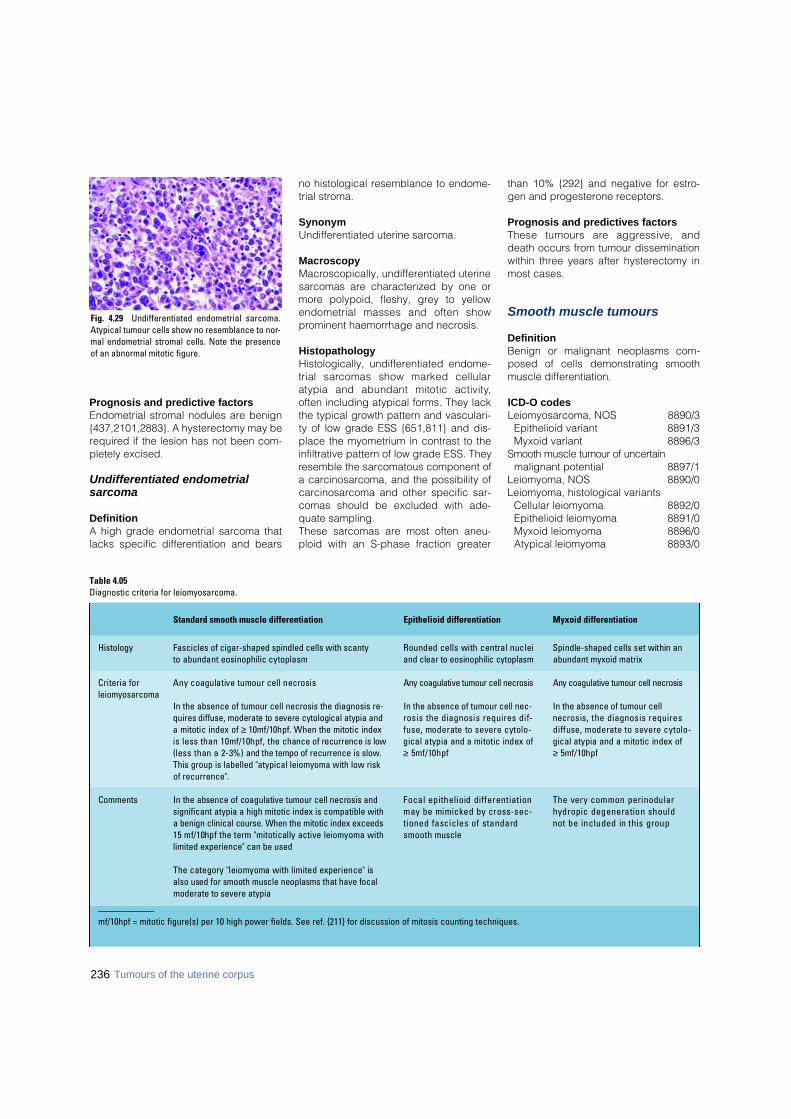
Prognosis and predictive factors Endometrial stromal nodules are benign{437,2101,2883}. A hysterectomy may berequired if the lesion has not been com-pletely excised.
Undifferentiated endometrial sarcoma
DefinitionA high grade endometrial sarcoma thatlacks specific differentiation and bears
no histological resemblance to endome-trial stroma.
SynonymUndifferentiated uterine sarcoma.
MacroscopyMacroscopically, undifferentiated uterinesarcomas are characterized by one ormore polypoid, fleshy, grey to yellowendometrial masses and often showprominent haemorrhage and necrosis.
HistopathologyHistologically, undifferentiated endome-trial sarcomas show marked cellularatypia and abundant mitotic activity,often including atypical forms. They lackthe typical growth pattern and vasculari-ty of low grade ESS {651,811} and dis-place the myometrium in contrast to theinfiltrative pattern of low grade ESS. Theyresemble the sarcomatous component ofa carcinosarcoma, and the possibility ofcarcinosarcoma and other specific sar-comas should be excluded with ade-quate sampling. These sarcomas are most often aneu-ploid with an S-phase fraction greater
than 10% {292} and negative for estro-gen and progesterone receptors.
Prognosis and predictives factorsThese tumours are aggressive, anddeath occurs from tumour disseminationwithin three years after hysterectomy inmost cases.
Smooth muscle tumours
DefinitionBenign or malignant neoplasms com-posed of cells demonstrating smoothmuscle differentiation.
ICD-O codesLeiomyosarcoma, NOS 8890/3
Epithelioid variant 8891/3Myxoid variant 8896/3
Smooth muscle tumour of uncert a i nmalignant potential 8897/1
Leiomyoma, NOS 8890/0Leiomyoma, histological variants
Cellular leiomyoma 8892/0Epithelioid leiomyoma 8891/0Myxoid leiomyoma 8896/0Atypical leiomyoma 8893/0
Table 4.05Diagnostic criteria for leiomyosarcoma.
Standard smooth muscle differentiation Epithelioid differentiation Myxoid differentiation
Histology Fascicles of cigar-shaped spindled cells with scanty Rounded cells with central nuclei Spindle-shaped cells set within anto abundant eosinophilic cytoplasm and clear to eosinophilic cytoplasm abundant myxoid matrix
Criteria for Any coagulative tumour cell necrosis Any coagulative tumour cell necrosis Any coagulative tumour cell necrosisl e i o m y o s a r c o m a
In the absence of tumour cell necrosis the diagnosis re- In the absence of tumour cell nec- In the absence of tumour cell quires diffuse, moderate to severe cytological atypia and rosis the diagnosis requires dif- necrosis, the diagnosis requires a mitotic index of ≥ 10mf/10hpf. When the mitotic index fuse, moderate to severe cytolo- d i ffuse, moderate to severe cytolo-is less than 10mf/10hpf, the chance of recurrence is low gical atypia and a mitotic index of gical atypia and a mitotic index of(less than a 2-3%) and the tempo of recurrence is slow. ≥ 5mf/10hpf ≥ 5mf/10hpfThis group is labelled "atypical leiomyoma with low risk of recurrence".
Comments In the absence of coagulative tumour cell necrosis and Focal epithelioid differentiation The very common perinodular significant atypia a high mitotic index is compatible with may be mimicked by cross-sec- hydropic degeneration shoulda benign clinical course. When the mitotic index exceeds tioned fascicles of standard not be included in this group15 mf/10hpf the term "mitotically active leiomyoma with s m o o t h musclelimited experience" can be used
The category "leiomyoma with limited experience" is also used for smooth muscle neoplasms that have focal moderate to severe atypia
____________mf/10hpf = mitotic figure(s) per 10 high power fields. See ref. {211} for discussion of mitosis counting techniques.
Fig. 4.29 Undifferentiated endometrial sarcoma.Atypical tumour cells show no resemblance to nor-mal endometrial stromal cells. Note the presenceof an abnormal mitotic figure.
236 Tumours of the uterine corpus
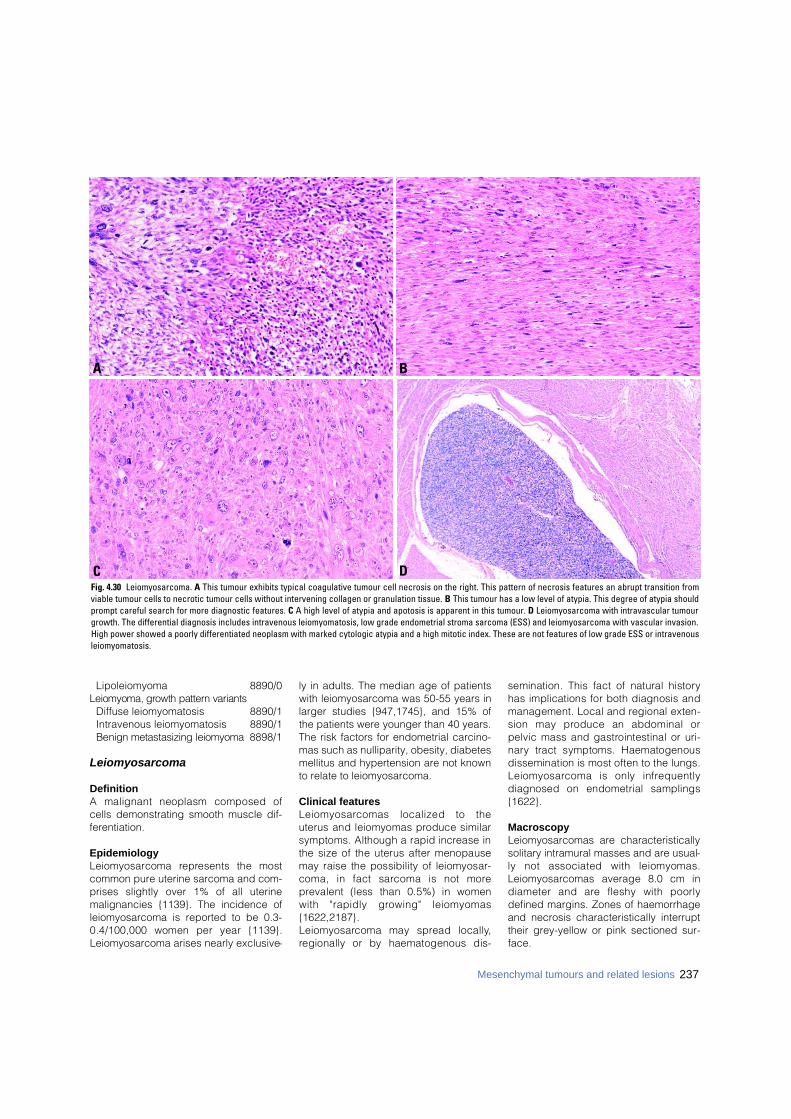
Lipoleiomyoma 8890/0Leiomyoma, growth pattern variants
Diffuse leiomyomatosis 8890/1Intravenous leiomyomatosis 8890/1Benign metastasizing leiomyoma 8898/1
Leiomyosarcoma
DefinitionA malignant neoplasm composed ofcells demonstrating smooth muscle dif-ferentiation.
EpidemiologyL e i o m y o s a rcoma re p resents the mostcommon pure uterine sarcoma and com-prises slightly over 1% of all uterinemalignancies {1139}. The incidence ofleiomyosarcoma is reported to be 0.3-0.4/100,000 women per year {1139}.Leiomyosarcoma arises nearly exclusive-
ly in adults. The median age of patientswith leiomyosarcoma was 50-55 years inlarger studies {947,1745}, and 15% ofthe patients were younger than 40 years.The risk factors for endometrial carcino-mas such as nulliparity, obesity, diabetesmellitus and hypertension are not knownto relate to leiomyosarcoma.
Clinical featuresL e i o m y o s a rcomas localized to theuterus and leiomyomas produce similarsymptoms. Although a rapid increase inthe size of the uterus after menopausemay raise the possibility of leiomyosar-coma, in fact sarcoma is not morep revalent (less than 0.5%) in womenwith "rapidly growing" leiomyomas{1622,2187}. L e i o m y o s a rcoma may spread locally,regionally or by haematogenous dis-
semination. This fact of natural historyhas implications for both diagnosis andmanagement. Local and regional exten-sion may produce an abdominal orpelvic mass and gastrointestinal or uri-n a ry tract symptoms. Haematogenousdissemination is most often to the lungs.L e i o m y o s a rcoma is only infre q u e n t l ydiagnosed on endometrial samplings{1622}.
MacroscopyLeiomyosarcomas are characteristicallysolitary intramural masses and are usual-ly not associated with leiomyomas.L e i o m y o s a rcomas average 8.0 cm indiameter and are fleshy with poorlydefined margins. Zones of haemorrhageand necrosis characteristically interrupttheir grey-yellow or pink sectioned sur-face.
237Mesenchymal tumours and related lesions
DC
BA
Fig. 4.30 Leiomyosarcoma. A This tumour exhibits typical coagulative tumour cell necrosis on the right. This pattern of necrosis features an abrupt transition fromviable tumour cells to necrotic tumour cells without intervening collagen or granulation tissue. B This tumour has a low level of atypia. This degree of atypia shouldprompt careful search for more diagnostic features. C A high level of atypia and apotosis is apparent in this tumour. D Leiomyosarcoma with intravascular tumourgrowth. The differential diagnosis includes intravenous leiomyomatosis, low grade endometrial stroma sarcoma (ESS) and leiomyosarcoma with vascular invasion.High power showed a poorly differentiated neoplasm with marked cytologic atypia and a high mitotic index. These are not features of low grade ESS or intravenousleiomyomatosis.
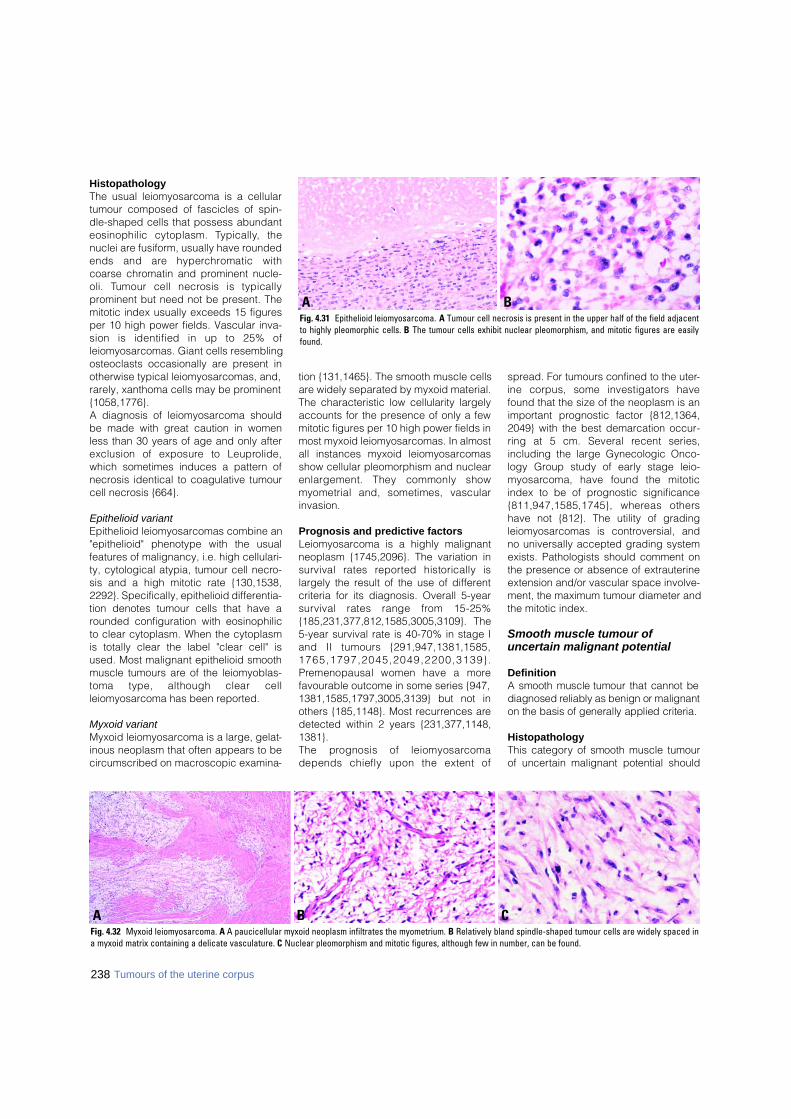
HistopathologyThe usual leiomyosarcoma is a cellulartumour composed of fascicles of spin-dle-shaped cells that possess abundanteosinophilic cytoplasm. Ty p i c a l l y, thenuclei are fusiform, usually have roundedends and are hyperc h romatic withcoarse chromatin and prominent nucle-oli. Tumour cell necrosis is typicallyprominent but need not be present. Themitotic index usually exceeds 15 figuresper 10 high power fields. Vascular inva-sion is identified in up to 25% ofleiomyosarcomas. Giant cells resemblingosteoclasts occasionally are present inotherwise typical leiomyosarcomas, and,rarely, xanthoma cells may be prominent{1058,1776}.A diagnosis of leiomyosarcoma shouldbe made with great caution in womenless than 30 years of age and only afterexclusion of exposure to Leupro l i d e ,which sometimes induces a pattern ofnecrosis identical to coagulative tumourcell necrosis {664}.
Epithelioid variantEpithelioid leiomyosarcomas combine an"epithelioid" phenotype with the usualfeatures of malignancy, i.e. high cellulari-ty, cytological atypia, tumour cell necro-sis and a high mitotic rate {130,1538,2292}. Specifically, epithelioid differentia-tion denotes tumour cells that have arounded configuration with eosinophilicto clear cytoplasm. When the cytoplasmis totally clear the label "clear cell" isused. Most malignant epithelioid smoothmuscle tumours are of the leiomyoblas-toma type, although clear cellleiomyosarcoma has been reported.
Myxoid variantMyxoid leiomyosarcoma is a large, gelat-inous neoplasm that often appears to becircumscribed on macroscopic examina-
tion {131,1465}. The smooth muscle cellsare widely separated by myxoid material.The characteristic low cellularity largelyaccounts for the presence of only a fewmitotic figures per 10 high power fields inmost myxoid leiomyosarcomas. In almostall instances myxoid leiomyosarcomasshow cellular pleomorphism and nuclearenlargement. They commonly showmyometrial and, sometimes, vascularinvasion.
Prognosis and predictive factorsLeiomyosarcoma is a highly malignantneoplasm {1745,2096}. The variation insurvival rates re p o rted historically islargely the result of the use of differentcriteria for its diagnosis. Overall 5-yearsurvival rates range from 15-25%{185,231,377,812,1585,3005,3109}. The5-year survival rate is 40-70% in stage Iand II tumours {291,947,1381,1585,1 7 6 5 , 1 7 9 7 , 2 0 4 5 , 2 0 4 9 , 2 2 0 0 , 3 1 3 9 } .P remenopausal women have a morefavourable outcome in some series {947,1381,1585,1797,3005,3139} but not inothers {185,1148}. Most recurrences aredetected within 2 years {231,377,1148,1381}.The prognosis of leiomyosarc o m adepends chiefly upon the extent of
spread. For tumours confined to the uter-ine corpus, some investigators havefound that the size of the neoplasm is animportant prognostic factor {812,1364,2049} with the best demarcation occur-ring at 5 cm. Several recent series,including the large Gynecologic Onco-logy Group study of early stage leio-m y o s a rcoma, have found the mitoticindex to be of prognostic significance{811,947,1585,1745}, whereas othershave not {812}. The utility of gradingleiomyosarcomas is controversial, andno universally accepted grading systemexists. Pathologists should comment onthe presence or absence of extrauterineextension and/or vascular space involve-ment, the maximum tumour diameter andthe mitotic index.
Smooth muscle tumour of uncertain malignant potential
DefinitionA smooth muscle tumour that cannot bediagnosed reliably as benign or malignanton the basis of generally applied criteria.
HistopathologyThis category of smooth muscle tumourof uncertain malignant potential should
238 Tumours of the uterine corpus
B CAFig. 4.32 Myxoid leiomyosarcoma. A A paucicellular myxoid neoplasm infiltrates the myometrium. B Relatively bland spindle-shaped tumour cells are widely spaced ina myxoid matrix containing a delicate vasculature. C Nuclear pleomorphism and mitotic figures, although few in number, can be found.
BAFig. 4.31 Epithelioid leiomyosarcoma. A Tumour cell necrosis is present in the upper half of the field adjacentto highly pleomorphic cells. B The tumour cells exhibit nuclear pleomorphism, and mitotic figures are easilyfound.

be used sparingly and is reserved forsmooth muscle neoplasms whoseappearance is ambiguous for some re a-son, and the relevant diagnostic possibil-ities differ in their clinical implications{211}. Examples include cases in whichthe subtype of smooth muscle diff e re n t i a-tion is in doubt, i.e. standard smoothmuscle, epithelioid or myxoid, and appli-cation of the competing classificationrules would lead to diff e rent clinical pre-dictions. On other occasions the assess-ment of a diagnostic feature, e.g. the typeof necrosis or the interpretation of mitoticf i g u res, is ambiguous, and the compet-ing alternative interpretations would leadto diff e rent clinical pre d i c t i o n s .
Leiomyoma
DefinitionA benign neoplasm composed of smoothmuscle cells with a variable amount offibrous stroma.
MacroscopyLeiomyomas are typically multiple,spherical and firm. The sectioned sur-face is white to tan and has a whorledtrabecular texture. Leiomyomas bulgeabove the surrounding myometrium fromwhich they are easily shelled out.Submucosal leiomyomas distort theoverlying endometrium, and, as theyenlarge, they may bulge into theendometrial cavity and produce bleed-ing. Rare examples become pedunculat-ed and prolapse through the cervix.Intramural leiomyomas are the mostcommon. Subserosal leiomyomas canbecome pedunculated, and on torsionwith necrosis of the pedicle the leiomy-oma may lose its connection with theuterus. Ve ry rare l y, some becomeattached to another pelvic structure (par-asitic leiomyoma). The appearance of aleiomyoma often is altered by degenera-tive changes. Submucosal leiomyomasfrequently are ulcerated and haemor-rhagic. Haemorrhage and necrosis areobserved in some leiomyomas, particu-larly in large ones in women who arepregnant or who are undergoing high-dose progestin therapy. Dark red areasre p resent haemorrhage and sharplydemarcated yellow areas reflect necro-sis. The damaged smooth muscle isreplaced eventually by firm white ortranslucent collagenous tissue. Cysticdegeneration also occurs, and some
leiomyomas become extensively calci-fied.
HistopathologyMost leiomyomas are composed of easi-ly recognized smooth muscle featuringwhorled, anastomosing fascicles of uni-f o rm, fusiform cells. Characteristically,the spindle-shaped cells have indistinctb o rders and abundant, often fibrillar,eosinophilic cytoplasm. Sometimes, par-ticularly in cellular leiomyomas, the cyto-plasm is sparse, and the fasciculararrangement of the cells may be muted.
Nuclei are elongated with blunt ortapered ends and have finely dispersedchromatin and small nucleoli. Mitotic fig-ures usually are infrequent.Most leiomyomas are more cellular thanthe surrounding myometrium. Leiomy-omas lacking increased cellularity areidentified by their nodular circumscrip-tion and by the disorderly arrangement ofthe smooth muscle fascicles within them,out of alignment with the surroundingmyometrium.Degenerative changes are common inleiomyomas. Hyaline fibrosis, oedemaand, on occasion, marked hydro p i cchange can be present {525}.Haemorrhage, necrosis, oedema, myx-oid change, hypercellular foci and cellu-lar hypertrophy occur in leiomyomas inwomen who are pregnant or taking prog-estins. Not infre q u e n t l y, there isincreased mitotic activity near the areasof necrosis. On the other hand, the coagulativetumour cell necrosis common inleiomyosarcoma is not associated veryoften with acute inflammation and haem-orrhage. Progestational agents are asso-ciated with a slight increase in mitoticactivity, but not to the level observed in aleiomyosarcoma. In addition, the mitoticfigures seen in conjunction with inflam-matory necrosis have a normal histologi-
Table 4.06Definition of terms used in the diagnosis of uterine smooth muscle neoplasms.
Term Definition or comment
Necrosis Death of a portion of tissue
Coagulative tumour Abrupt transition from viable tumour to necrotic tumour, ghost outlinescell necrosis of cells usual, haemorrhage and inflammation uncommon.
Hyaline necrosis Intervening zone of collagen or granulation tissue between nonviable andviable tumour, haemorrhage common, cellular outlines often not visible.
Atypia Assessed at scanning power
Diffuse vs. focal Cells diffusely present in most fields examined vs. scattered widely spaced aggregates of cells
None to mild
Moderate to severe Pleomorphic type: Nuclear pleomorphism appreciated at scanning powerUniform type: Cells lack pleomorphism but exhibit uniform but markednuclear chromatin abnormalities
Mitotic index Expressed in mitotic figures per 10 high power fields in the mitotically most active areas
Only unequivocal mitotic figures are counted {211}
Fig. 4.33 MRI showing an enlarged uterus withmultiple leiomyomas.
239Mesenchymal tumours and related lesions
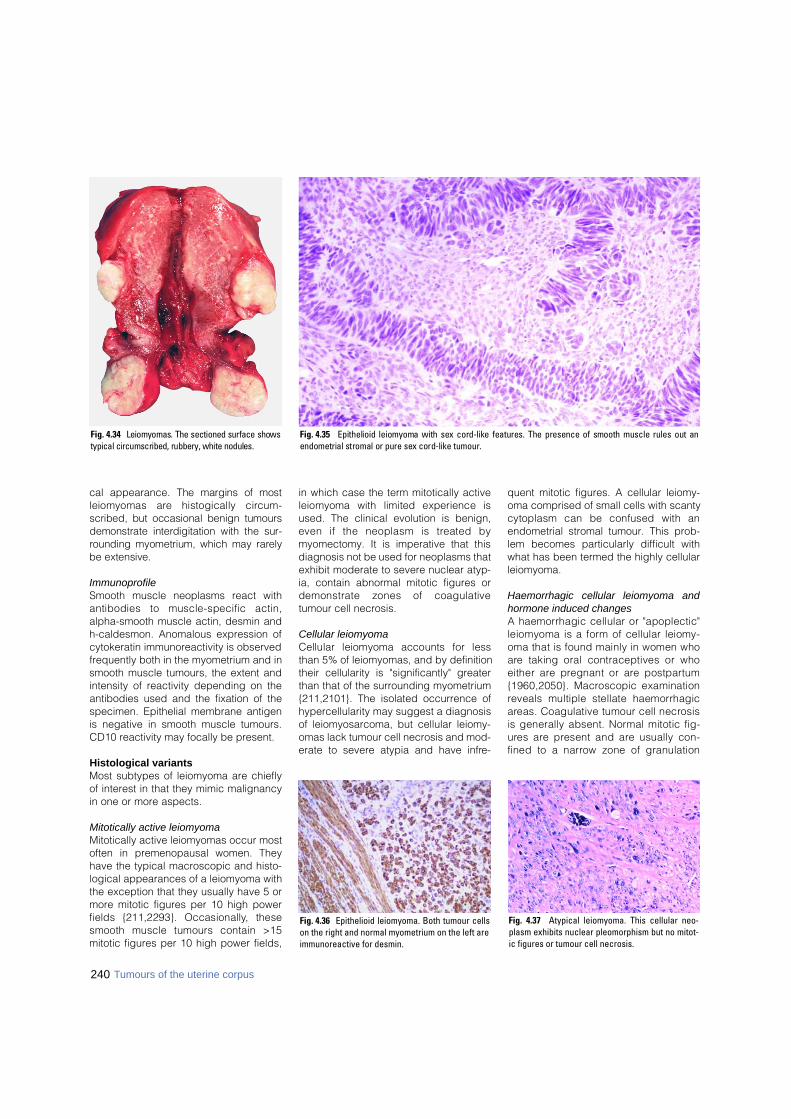
cal appearance. The margins of mostleiomyomas are histogically circ u m-scribed, but occasional benign tumoursdemonstrate interdigitation with the sur-rounding myometrium, which may rare l ybe extensive.
ImmunoprofileSmooth muscle neoplasms react withantibodies to muscle-specific actin,alpha-smooth muscle actin, desmin andh-caldesmon. Anomalous expression ofcytokeratin immunoreactivity is observedfrequently both in the myometrium and insmooth muscle tumours, the extent andintensity of reactivity depending on theantibodies used and the fixation of thespecimen. Epithelial membrane antigenis negative in smooth muscle tumours.CD10 reactivity may focally be present.
Histological variantsMost subtypes of leiomyoma are chieflyof interest in that they mimic malignancyin one or more aspects.
Mitotically active leiomyomaMitotically active leiomyomas occur mostoften in premenopausal women. Theyhave the typical macroscopic and histo-logical appearances of a leiomyoma withthe exception that they usually have 5 ormore mitotic figures per 10 high powerfields {211,2293}. Occasionally, thesesmooth muscle tumours contain >15mitotic figures per 10 high power fields,
in which case the term mitotically activeleiomyoma with limited experience isused. The clinical evolution is benign,even if the neoplasm is treated bymyomectomy. It is imperative that thisdiagnosis not be used for neoplasms thatexhibit moderate to severe nuclear atyp-ia, contain abnormal mitotic figures ordemonstrate zones of coagulativetumour cell necrosis.
Cellular leiomyoma Cellular leiomyoma accounts for lessthan 5% of leiomyomas, and by definitiontheir cellularity is "significantly" greaterthan that of the surrounding myometrium{211,2101}. The isolated occurrence ofhypercellularity may suggest a diagnosisof leiomyosarcoma, but cellular leiomy-omas lack tumour cell necrosis and mod-erate to severe atypia and have infre-
quent mitotic figures. A cellular leiomy-oma comprised of small cells with scantycytoplasm can be confused with anendometrial stromal tumour. This prob-lem becomes particularly difficult withwhat has been termed the highly cellularleiomyoma.
Haemorrhagic cellular leiomyoma andhormone induced changesA haemorrhagic cellular or "apoplectic"leiomyoma is a form of cellular leiomy-oma that is found mainly in women whoa re taking oral contraceptives or whoeither are pregnant or are postpart u m{1960,2050}. Macroscopic examinationreveals multiple stellate haemorrhagica reas. Coagulative tumour cell necro s i sis generally absent. Normal mitotic fig-u res are present and are usually con-fined to a narrow zone of granulation
240 Tumours of the uterine corpus
Fig. 4.34 Leiomyomas. The sectioned surface showstypical circumscribed, rubbery, white nodules.
Fig. 4.36 Epithelioid leiomyoma. Both tumour cellson the right and normal myometrium on the left areimmunoreactive for desmin.
Fig. 4.37 Atypical leiomyoma. This cellular neo-plasm exhibits nuclear pleomorphism but no mitot-ic figures or tumour cell necrosis.
Fig. 4.35 Epithelioid leiomyoma with sex cord-like features. The presence of smooth muscle rules out anendometrial stromal or pure sex cord-like tumour.

tissue in relation to areas of haemor-r h a g e .
Epithelioid leiomyoma Epithelioid leiomyomas are composed ofepithelial-like cells {130,1538,2292}.They are yellow or grey and may containvisible areas of haemorrhage and necro-sis. They tend to be softer than the usualleiomyoma, and most are solitary.Histologically, the epithelioid cells areround or polygonal, they are arranged inclusters or cords, and their nuclei areround, relatively large and centrally posi-tioned. There are three basic subtypes ofepithelioid leiomyoma: leiomyoblastoma,clear cell leiomyoma and plexiformleiomyoma. Mixtures of the various pat-terns are common, hence the designa-tion "epithelioid" for all of them. Small tumours without cytological atypia,tumour cell necrosis or an elevated mitoticindex can be safely re g a rded as benign.P l e x i f o rm tumourlets invariably are benign.Epithelioid leiomyomas with circ u m-scribed margins, extensive hyalinizationand a predominance of clear cells gener-ally are benign. The behaviour of epithe-lioid leiomyomas with two or more of thefollowing features is not well established:(1). Large size (greater than 6 cm).(2). Moderate mitotic activity (2-4 mitoticfigures per 10 high power fields), (3) Moderate to severe cytological atypia(4) Necrosis Such tumours should be classified in theuncertain malignant potential category,and careful follow-up is warranted.Neoplasms with 5 or more mitotic figuresper 10 high power fields metastasize withsufficient frequency that all should beregarded as epithelioid leiomyosarcoma.
Myxoid leiomyoma Myxoid leiomyomas are benign smoothmuscle tumours in which myxoid materi-
al separates the tumour cells {131,1465}.They are soft and translucent.H i s t o l o g i c a l l y, abundant amorphousmyxoid material is present between thesmooth muscle cells. The margins of amyxoid leiomyoma are circumscribed,and neither cytological atypia nor mitoticfigures are present.
Atypical leiomyoma (pleomorphic, bizarreor symplastic leiomyoma)When unassociated with either coagula-tive tumour cell necrosis or a mitoticindex in excess of 10 mitotic figures per10 high power fields, cytological atypia,even when severe, is an unreliable crite-rion for identifying clinically malignantuterine smooth muscle tumours. Theseatypical cells have enlarged hyperchro-matic nuclei with prominent chromatinclumping (often smudged). Large cyto-plasmic pseudonuclear inclusions oftenare present. The atypical cells may bedistributed throughout the leiomyoma(diffuse) or they may be present focally(possibly, multifocally). When the atypiais at most multifocal and the neoplasmhas been completely sampled, suchtumours are designated "atypical leiomy-oma with minimal, if any, re c u r re n c e
potential." Such lesions have behavedbenignly except for a single reportedcase.
Lipoleiomyoma S c a t t e red adipocytes in an otherwisetypical leiomyoma are a relatively com-mon finding; a leiomyoma that contains astriking number of these cells is called alipoleiomyoma {2357,2671}.
Growth pattern variantsGrowth pattern variants may produceunusual clinical, macroscopic and/or his-tological features.
Diffuse leiomyomatosis D i ffuse leiomyomatosis is an unusualcondition in which numerous smallsmooth muscle nodules produce sym-metrical, sometimes substantial, enlarge-ment of the uterus {518}. The hyperplas-tic smooth muscle nodules range fro mhistological to 3 cm in size, but most areless than 1 cm in diameter. They are com-posed of uniform, bland, spindle-shapedsmooth muscle cells and are less circ u m-scribed than leiomyomas. The clinicalcourse may be complicated by haemor-rhage, but the condition is benign.
Dissecting leiomyoma Dissecting leiomyoma refers to a benignsmooth muscle proliferation with a bordermarked by the dissection of compressivetongues of smooth muscle into the sur-rounding myometrium and, occasionally,into the broad ligament and pelvis{2469}. This pattern of infiltration mayalso be seen in intravenous leiomy-omatosis. When oedema and congestiona re prominent, a uterine dissectingleiomyoma with extrauterine extensionmay resemble placental tissue; hencethe name cotyledonoid dissectingleiomyoma {2470}.
B CAFig. 4.38 Leiomyoma with perinodular hydropic degeneration. A Sectioned surface shows a lobulated neoplasm. B Nodules of smooth muscle are delimited by oede-matous bands of collagen in which are suspended large calibre vessels. C The tumour is composed of uniform spindle-shaped smooth muscle cells.
Fig. 4.39 Intravenous leiomyomatosis with atypical(symplastic and epithelioid) features. Note thetumour plugs in myometrial vessels at the lower leftand mid-right.
241Mesenchymal tumours and related lesions

Intravenous leiomyomatosisIntravenous leiomyomatosis is a very raresmooth muscle tumour featuring nodularmasses and cords of histologicallybenign smooth muscle growing withinvenous channels outside the confines ofa leiomyoma {1928,2051}. Intravenousleiomyomatosis should be distinguishedfrom the common vascular intrusion with-in the confines of a leiomyoma.M a c ro s c o p i c a l l y, Intravenous leiomy-omatosis consists of a complex, coiled ornodular myometrial growth often withconvoluted, worm-like extensions into theuterine veins in the broad ligament or intoother pelvic veins. On occasion, thegrowth extends into the vena cava, andsometimes it extends into the right heart.H i s t o l o g i c a l l y, tumour is found withinvenous channels that are lined byendothelium. The histological appear-ance is highly variable, even within thesame tumour. The cellular composition ofsome examples of intravenous leiomy-omatosis is similar to a leiomyoma, butmost contain prominent zones of fibrosisor hyalinization. Smooth muscle cellsmay be inconspicuous and difficult toidentify. Any variant smooth muscle his-tology, i.e. cellular, atypical, epithelioid orlipoleiomyomatous, may be encounteredin intravenous leiomyomatosis.
Benign metastasizing leiomyomaBenign metastasizing leiomyoma is an ill-defined clinicopathological conditionwhich features "metastatic" histologicallybenign smooth muscle tumour depositsin the lung, lymph nodes or abdomenthat appear to be derived from a benignuterine leiomyoma {798,2923}. Reportsof this condition often are difficult to eval-uate. Almost all cases of benign metas-tasizing leiomyoma occur in women whohave a history of pelvic surgery. The pri -mary neoplasm, typically removed years
b e f o re the extrauterine deposits aredetected, often has been inadequatelystudied. Most examples of "benignmetastasizing leiomyoma," however,appear to be either a primary benignsmooth muscle lesion of the lung in awoman with a history of uterine leiomy-oma or pulmonary metastases from a his-tologically non-informative smooth mus-cle neoplasm of the uterus. The findingsof a recent cytogenetic study were mostconsistent with a monoclonal origin ofboth uterine and pulmonary tumours andthe interpretation that the pulmonarytumours were metastatic {2923}. The hor-mone dependence of this proliferation issuggested by the finding of estrogen andp ro g e s t e rone receptors in metastaticdeposits and the regression of tumourduring pregnancy, after the menopauseand after oophorectomy.
Somatic geneticsUterine leiomyomas often have chromo-somal abnormalities detectable by cyto-genetic analysis, most frequently involv-ing the H M G I C (12q15) and H M G I Y(6p21) genes {2204a}.
Miscellaneous mesenchymalt u m o u r s
DefinitionA diverse group of mesenchymaltumours of the uterus that do not showpredominantly smooth muscle or stromaldifferentiation.
Mixed endometrial stromal andsmooth muscle tumour
Definition and historical annotationThese neoplasms, previously designateds t romomyoma, are composed of anadmixture of endometrial stromal and
smooth muscle elements {1448,2098,2550,2860}. Small areas of smooth mus-cle differentiation are commonly seen inotherwise typical endometrial stro m a lneoplasms and vice versa, but a mini-mum of 30% of the minor component isrecommended for the designation ofmixed endometrial stromal-smooth mus-cle neoplasm {2098}.
MacroscopyThese neoplasms may have a predomi-nant intramural, submucosal or sub-s e rosal location. Some have beendescribed as well circumscribed, where-as others have been multinodular or havehad infiltrating margins. Some neo-plasms contain areas with a whorledappearance admixed with tan foci thata re softer than typical leiomyomas{2098}.
HistopathologyA population of small cells with round toovoid nuclei and inconspicuous cyto-plasm characterizes the endometrials t romal component. Numerous smallarterioles are a characteristic feature.The endometrial stromal component usu-ally exhibits minimal cytological atypia,and the mitotic rate is variable. Areasexhibiting sex cord-like diff e re n t i a t i o nand perivascular hyalinization may bepresent in the endometrial stromal com-ponent {2098}. A case has beendescribed with an associated glandularcomponent consisting of benignendometrial glands surrounded byendometrial stroma {1812}.The smooth muscle component is usual-ly benign in appearance and is oftenarranged in nodules with a prominentcentral area of hyalinization creating astarburst appearance. However, in somecases the smooth muscle componentmay exhibit any one or a combination of
B CAFig. 4.40 Perivascular epithelioid cell tumour. A Low power image shows a "tongue-like" growth pattern, similar to low grade endometrial stromal sarcoma. B Highpower image shows epithelioid cells with clear to pale granular cytoplasm without significant atypia or mitotic figures. C HMB-45 stain is positive.
242 Tumours of the uterine corpus
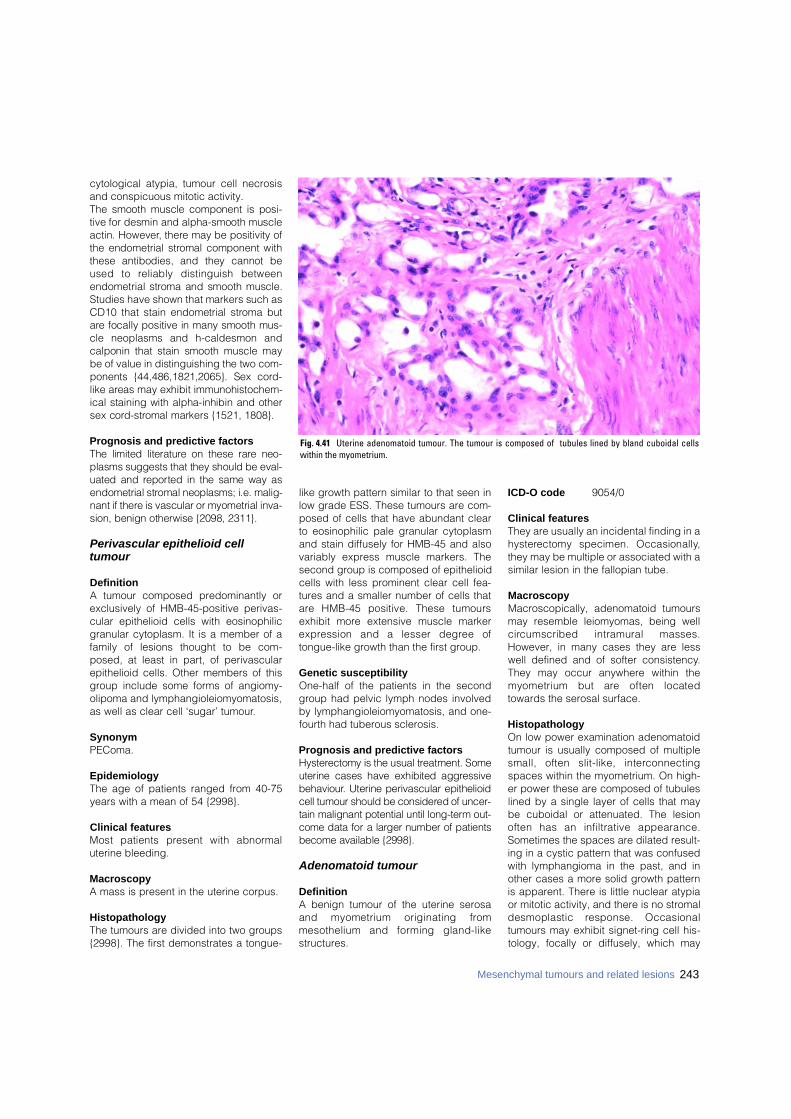
cytological atypia, tumour cell necrosisand conspicuous mitotic activity.The smooth muscle component is posi-tive for desmin and alpha-smooth muscleactin. However, there may be positivity ofthe endometrial stromal component withthese antibodies, and they cannot beused to reliably distinguish betweenendometrial stroma and smooth muscle.Studies have shown that markers such asCD10 that stain endometrial stroma buta re focally positive in many smooth mus-cle neoplasms and h-caldesmon andcalponin that stain smooth muscle maybe of value in distinguishing the two com-ponents {44,486,1821,2065}. Sex cord -like areas may exhibit immunohistochem-ical staining with alpha-inhibin and othersex cord - s t romal markers {1521, 1808}.
Prognosis and predictive factorsThe limited literature on these rare neo-plasms suggests that they should be eval-uated and re p o rted in the same way asendometrial stromal neoplasms; i.e. malig-nant if there is vascular or myometrial inva-sion, benign otherwise {2098, 2311}.
Perivascular epithelioid celltumour
DefinitionA tumour composed predominantly orexclusively of HMB-45-positive perivas-cular epithelioid cells with eosinophilicgranular cytoplasm. It is a member of afamily of lesions thought to be com-posed, at least in part, of perivascularepithelioid cells. Other members of thisgroup include some forms of angiomy-olipoma and lymphangioleiomyomatosis,as well as clear cell ‘sugar’ tumour.
SynonymPEComa.
EpidemiologyThe age of patients ranged from 40-75years with a mean of 54 {2998}.
Clinical featuresMost patients present with abnorm a luterine bleeding.
MacroscopyA mass is present in the uterine corpus.
HistopathologyThe tumours are divided into two groups{2998}. The first demonstrates a tongue-
like growth pattern similar to that seen inlow grade ESS. These tumours are com-posed of cells that have abundant clearto eosinophilic pale granular cytoplasmand stain diffusely for HMB-45 and alsovariably express muscle markers. Thesecond group is composed of epithelioidcells with less prominent clear cell fea-tures and a smaller number of cells thata re HMB-45 positive. These tumoursexhibit more extensive muscle markere x p ression and a lesser degree oftongue-like growth than the first group.
Genetic susceptibilityOne-half of the patients in the secondgroup had pelvic lymph nodes involvedby lymphangioleiomyomatosis, and one-fourth had tuberous sclerosis.
Prognosis and predictive factorsH y s t e rectomy is the usual treatment. Someuterine cases have exhibited aggre s s i v eb e h a v i o u r. Uterine perivascular epithelioidcell tumour should be considered of uncer-tain malignant potential until long-term out-come data for a larger number of patientsbecome available {2998}.
Adenomatoid tumour
DefinitionA benign tumour of the uterine serosaand myometrium originating fro mmesothelium and forming gland-likestructures.
ICD-O code 9054/0
Clinical featuresThey are usually an incidental finding in ah y s t e rectomy specimen. Occasionally,they may be multiple or associated with asimilar lesion in the fallopian tube.
MacroscopyMacroscopically, adenomatoid tumoursmay resemble leiomyomas, being wellc i rcumscribed intramural masses.However, in many cases they are lesswell defined and of softer consistency.They may occur anywhere within themyometrium but are often locatedtowards the serosal surface.
HistopathologyOn low power examination adenomatoidtumour is usually composed of multiplesmall, often slit-like, interc o n n e c t i n gspaces within the myometrium. On high-er power these are composed of tubuleslined by a single layer of cells that maybe cuboidal or attenuated. The lesionoften has an infiltrative appearance.Sometimes the spaces are dilated result-ing in a cystic pattern that was confusedwith lymphangioma in the past, and inother cases a more solid growth patternis apparent. There is little nuclear atypiaor mitotic activity, and there is no stromaldesmoplastic response. Occasionaltumours may exhibit signet-ring cell his-tology, focally or diffusely, which may
243Mesenchymal tumours and related lesions
Fig. 4.41 Uterine adenomatoid tumour. The tumour is composed of tubules lined by bland cuboidal cellswithin the myometrium.

cause obvious diagnostic pro b l e m s .Sometimes a papillary pattern may bea p p a rent. Ultrastructural examinationshows the long slender microvilli charac-teristic of mesothelial cells.
ImmunoprofileImmunohistochemical positivity with anti-cytokeratin antibodies and anti-mesothe-lial antibodies, such as HBME1 and cal-retinin, is usual. This finding may be use-ful in the distinction between adenoma-toid tumour and lymphangioma. There isno reactivity with Ber-EP4, helping toexclude a carcinoma in those cases thathave signet-ring cell morphology {211,2101,2123}.
Histogenesis The histogenesis has been debated inthe past, but immunohistochemical andultrastructural studies have shown theseneoplasms to be of mesothelial origin.When located within the uterus {654,2041,2311,2768,2924}, they are proba-bly derived from the serosal mesotheli-um.
Prognosis and predictive factorsAdenomatoid tumours are invariablybenign with no risk of recurrence ormetastasis.
Rare mesenchymal tumours
DefinitionA variety of mesenchymal tumours, bothmalignant and benign, occurring withinthe uterus that are not endometrial stro-mal, smooth muscle or mesothelial in
type. These are rare and are identicalhistologically to their counterparts arisingin more usual sites.
Malignant tumours In cases of malignancy the neoplasmshould be extensively sampled in orderto exclude sarcomatous overgrowth in aMMMT or an adenosarcoma. The mostcommon of these neoplasms to arise inthe uterus is rhabdomyosarcoma {716,1149,1814,2112}. The latter is usually ofembryonal type in young females and ofpleomorphic type in the middle aged orelderly. Occasional cases of uterine alve-olar rhabdomyosarcoma have also beendescribed {475}. Occasional re s i d u a lentrapped benign endometrial glandsmay be present, especially towards thesurface of these neoplasms. That findingshould not be taken as evidence of ana d e n o s a rcoma. Other malignant mes-enchymal neoplasms described in theuterus include malignant fibrous histiocy-toma {1404}, angiosarcoma (includingthe epithelioid variant) {2551,2853},liposarcoma {180}, osteosarcoma {784,1137,1844}, c h o n d ro s a rc o m a { 1 4 8 9 } ,alveolar soft part sarcoma {2319}, Ewingt u m o u r, malignant peripheral nervesheath tumour, malignant pigmentedn e u ro e c t o d e rmal tumour of infancy{2580} and peripheral primitive neuroec-t o d e rmal tumour {638,1894,2017}. Ingeneral, these are all bulky neoplasms,frequently high stage at presentation,and the histology is similar to their coun-terparts elsewhere. Immunohistochemi-cal studies may assist in establishing adefinitive diagnosis.
H a e m a n g i o p e r i c y t o m a has also beendescribed in the uterus, but it is likely thatmost of the reported cases representvascular endometrial stromal neoplasms{2693}. Malignant rhabdoid tumours have alsobeen described {948,1255}. Since a rhab-doid component may rarely be found in anotherwise typical endometrial stromal neo-plasm {1813}, it is possible that somerhabdoid tumours re p resent an unusualhistological variant of an endometrial stro-mal or some other neoplasm. As with othere x t r a renal rhabdoid tumours, the uterineneoplasm may re p resent a peculiar histo-logical growth pattern that may be found ina variety of neoplasms; there f o re, exten-sive sampling should be undertaken toexclude a diagnosis of rhabdoid diff e re n t i-ation in another more common neoplasm.Only when other elements are not identi-fied should a diagnosis of uterine malig-nant rhabdoid tumour be considere d .
Benign tumours Benign tumours include lipoma, haeman-gioma, lymphangioma and rhabdomy-oma {466,686}. Occasional uterine myx-omas have been described in Carneys y n d rome {2654}. Before diagnosingthese entities, a lipoleiomyoma should beexcluded in the case of lipoma, a vascu-lar leiomyoma in the case of haeman-gioma, an adenomatoid tumour in thecase of lymphangioma and a myxoidsmooth muscle neoplasm in the case ofmyxoma. A single case of postoperativespindle cell nodule of the endometriumthat occurred following a uterine curet-tage has been described {504}.
244 Tumours of the uterine corpus
DefinitionTumours of the uterine corpus composedof an epithelial and a mesenchymal com-ponent.
ICD-O codesCarcinosarcoma 8980/3Adenosarcoma 8933/3Carcinofibroma 8934/3Adenofibroma 9013/0Adenomyoma 8932/0
Atypical polypoid variant 8932/0
Carcinosarcoma
DefinitionA neoplasm composed of an admixtureof malignant epithelial and mesenchymalcomponents.
SynonymsMalignant müllerian mixed tumour, malig-nant mesodermal mixed tumour, meta-plastic carcinoma. These tumours are still classified as"mixed" by convention, although there isincreasing evidence that they are mono-clonal and should be considered subsetsof endometrial carcinoma.
EpidemiologyCarcinosarcoma is the most commonneoplasm of this group {703}.Carcinosarcomas usually occur in elder-ly postmenopausal women, althoughoccasional cases may occur in youngerwomen and rarely even in young girls.The median age of patients presenting
with carcinosarcoma is 65 years, higherthan that of patients with leiomyosarcoma{813,1745}. Less than 5% of patients areyounger than 50 years.
AetiologyAn occasional case is secondary to priorpelvic irradiation. In recent years anassociation between long term tamoxifentherapy and the development of uterinec a rc i n o s a rcoma has been suggested{813,1811,2947}.
Clinical featuresSigns and symptomsVaginal bleeding is the most frequentpresenting symptom of patients with car-cinosarcoma, followed by an abdominalmass and pelvic pain {703}.Carcinosarcomas may be polypoid andmay prolapse through the cervix to pres-ent as an upper vaginal mass. The mostimportant diagnostic method is uterinecurettage, but in 25% of cases the diag-nosis is made following hysterectomy{2965}.
ImagingMagnetic resonance imaging (MRI) ofwomen with a typical carcinosarcomausually shows an enlarged uterus with awidened endometrial cavity and evi-dence of deep myometrial invasion.Whereas a carcinosarcoma cannot bedistinguished from endometrial carcino-ma by means of MRI, the presence of alarge tumour with extensive myometrialinvasion as well as the presence of ovar-
ian or intraperitoneal metastases shouldraise suspicion {1060,2838}.
MacroscopyAt the time of presentation uterine carci-nosarcomas are usually polypoid, bulky,necrotic and haemorrhagic neoplasmsthat fill the endometrial cavity and deeplyinvade the myometrium, often extendingbeyond the uterus. If cartilage or boneforms a significant portion of the neo-plasm, the neoplasm may have a hardc o n s i s t e n c y. Occasionally, these neo-plasms may arise within a benignendometrial polyp.
Tumour spread and stagingIntra-abdominal and re t ro p e r i t o n e a lnodal metastases are frequent {1745}.
HistopathologyThe malignant epithelial element is usual-ly glandular, although rarely it may benon-glandular, most commonly consist-ing of squamous or undifferentiated car-cinoma. The glandular component maybe either endometrioid or non-endometri-oid, such as serous or clear cell in type.The sarcomatous elements may be eitherhomologous or heterologous. In homolo-gous neoplasms the mesenchymal com-ponent usually consists of undifferentiat-ed sarcoma, leiomyosarcoma orendometrial stromal sarcoma and is usu-ally, although not always, high grade.H e t e rologous mesenchymal elementsmost commonly consist of malignant car-tilage or malignant skeletal muscle in the
W.G. McCluggageU. HallerR.J. KurmanR.A. Kubik-Huch
Mixed epithelial and mesenchymaltumours
Table 4.07Nomenclature of mixed epithelial and mesenchymal tumours defined by phenotypes of epithelial and mes-enchymal components.
Benign epithelium Malignant epithelium
Benign mesenchyme Adenofibroma Carcinofibroma
Adenomyoma (including atypical)
Malignant mesenchyme Adenosarcoma Carcinosarcoma Fig. 4.42 Carcinosarcoma. Sagittal section of the uterusshows a solid, polypoid tumour within the fundus.
245Mixed epithelial and mesenchymal tumours
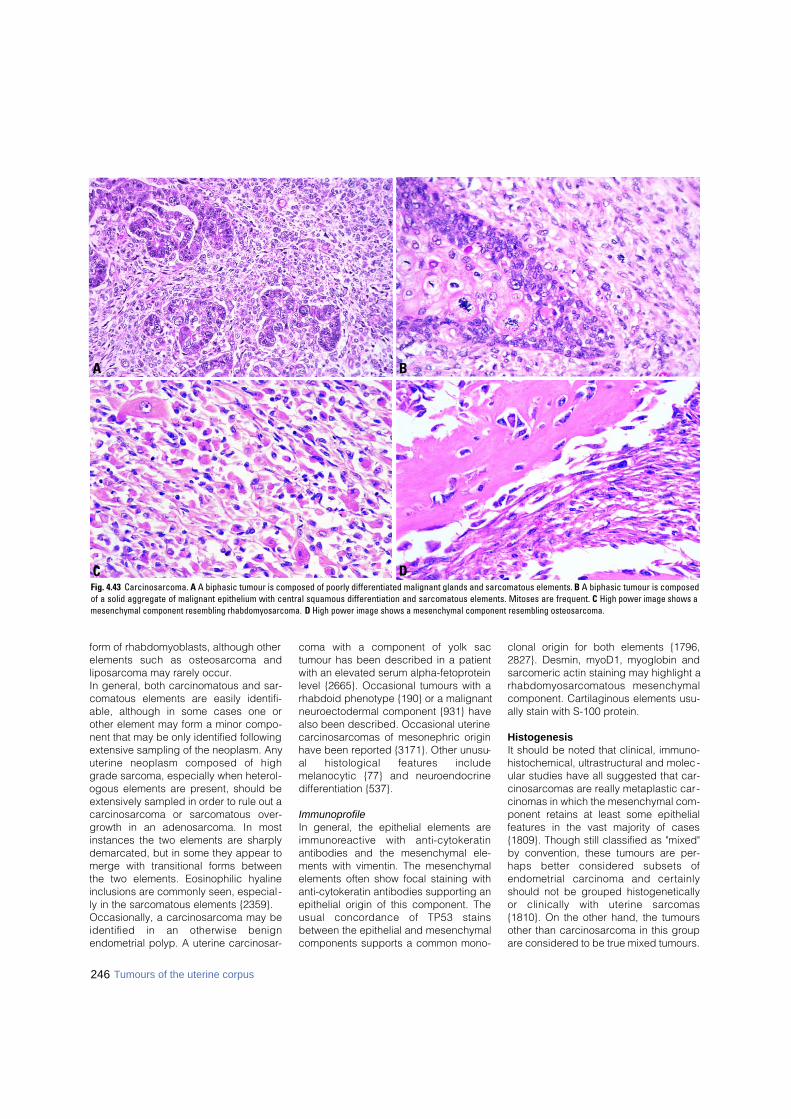
246 Tumours of the uterine corpus
form of rhabdomyoblasts, although otherelements such as osteosarcoma andliposarcoma may rarely occur.In general, both carcinomatous and sar-comatous elements are easily identifi-able, although in some cases one orother element may form a minor compo-nent that may be only identified followingextensive sampling of the neoplasm. Anyuterine neoplasm composed of highgrade sarcoma, especially when heterol-ogous elements are present, should beextensively sampled in order to rule out ac a rc i n o s a rcoma or sarcomatous over-growth in an adenosarcoma. In mostinstances the two elements are sharplydemarcated, but in some they appear tomerge with transitional forms betweenthe two elements. Eosinophilic hyalineinclusions are commonly seen, especial -ly in the sarcomatous elements {2359}. Occasionally, a carcinosarcoma may beidentified in an otherwise benignendometrial polyp. A uterine carcinosar-
coma with a component of yolk sactumour has been described in a patientwith an elevated serum alpha-fetoproteinlevel {2665}. Occasional tumours with arhabdoid phenotype {190} or a malignantneuroectodermal component {931} havealso been described. Occasional uterinecarcinosarcomas of mesonephric originhave been reported {3171}. Other unusu-al histological features includemelanocytic {77} and neuro e n d o c r i n edifferentiation {537}.
ImmunoprofileIn general, the epithelial elements arei m m u n o reactive with anti-cytokeratinantibodies and the mesenchymal ele-ments with vimentin. The mesenchymalelements often show focal staining withanti-cytokeratin antibodies supporting anepithelial origin of this component. Theusual concordance of TP53 stainsbetween the epithelial and mesenchymalcomponents supports a common mono-
clonal origin for both elements {1796,2827}. Desmin, myoD1, myoglobin andsarcomeric actin staining may highlight ar h a b d o m y o s a rcomatous mesenchymalcomponent. Cartilaginous elements usu-ally stain with S-100 protein.
HistogenesisIt should be noted that clinical, immuno-histochemical, ultrastructural and molec-ular studies have all suggested that car-cinosarcomas are really metaplastic car-cinomas in which the mesenchymal com-ponent retains at least some epithelialfeatures in the vast majority of cases{1809}. Though still classified as "mixed"by convention, these tumours are per-haps better considered subsets ofendometrial carcinoma and cert a i n l yshould not be grouped histogeneticallyor clinically with uterine sarc o m a s{1810}. On the other hand, the tumoursother than carcinosarcoma in this groupare considered to be true mixed tumours.
DC
BA
Fig. 4.43 Carcinosarcoma. A A biphasic tumour is composed of poorly differentiated malignant glands and sarcomatous elements. B A biphasic tumour is composedof a solid aggregate of malignant epithelium with central squamous differentiation and sarcomatous elements. Mitoses are frequent. C High power image shows amesenchymal component resembling rhabdomyosarcoma. D High power image shows a mesenchymal component resembling osteosarcoma.
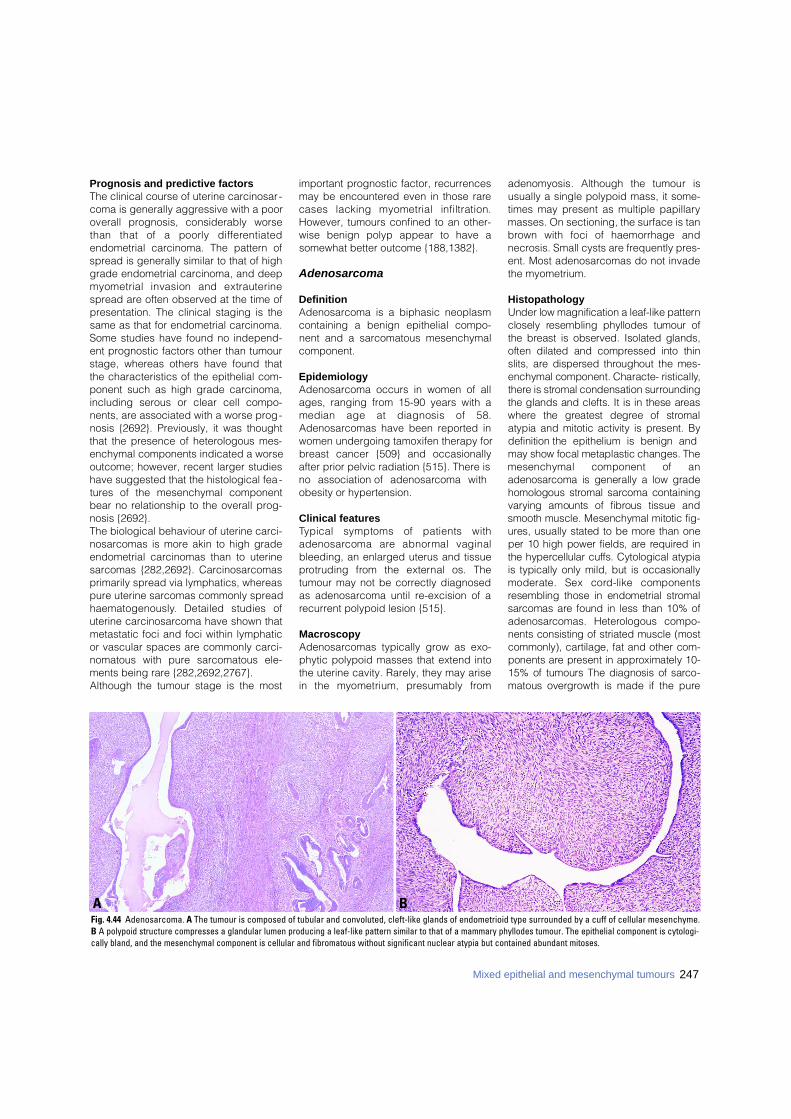
Prognosis and predictive factorsThe clinical course of uterine carcinosar-coma is generally aggressive with a pooroverall prognosis, considerably worsethan that of a poorly diff e re n t i a t e dendometrial carcinoma. The pattern ofspread is generally similar to that of highgrade endometrial carcinoma, and deepmyometrial invasion and extrauterinespread are often observed at the time ofpresentation. The clinical staging is thesame as that for endometrial carcinoma.Some studies have found no independ-ent prognostic factors other than tumourstage, whereas others have found thatthe characteristics of the epithelial com-ponent such as high grade carcinoma,including serous or clear cell compo-nents, are associated with a worse prog-nosis {2692}. Previously, it was thoughtthat the presence of heterologous mes-enchymal components indicated a worseoutcome; however, recent larger studieshave suggested that the histological fea-tures of the mesenchymal componentbear no relationship to the overall prog-nosis {2692}. The biological behaviour of uterine carci-nosarcomas is more akin to high gradeendometrial carcinomas than to uterinesarcomas {282,2692}. Carcinosarcomasprimarily spread via lymphatics, whereaspure uterine sarcomas commonly spreadh a e m a t o g e n o u s l y. Detailed studies ofuterine carcinosarcoma have shown thatmetastatic foci and foci within lymphaticor vascular spaces are commonly carci-nomatous with pure sarcomatous ele-ments being rare {282,2692,2767}.Although the tumour stage is the most
important prognostic factor, recurrencesmay be encountered even in those rarecases lacking myometrial infiltration.However, tumours confined to an other-wise benign polyp appear to have asomewhat better outcome {188,1382}.
Adenosarcoma
DefinitionAdenosarcoma is a biphasic neoplasmcontaining a benign epithelial compo-nent and a sarcomatous mesenchymalcomponent.
EpidemiologyAdenosarcoma occurs in women of allages, ranging from 15-90 years with amedian age at diagnosis of 58.Adenosarcomas have been reported inwomen undergoing tamoxifen therapy forbreast cancer {509} and occasionallyafter prior pelvic radiation {515}. There isno association of adenosarcoma withobesity or hypertension.
Clinical featuresTypical symptoms of patients witha d e n o s a rcoma are abnormal vaginalbleeding, an enlarged uterus and tissuep rotruding from the external os. Thetumour may not be correctly diagnosedas adenosarcoma until re-excision of arecurrent polypoid lesion {515}.
MacroscopyAdenosarcomas typically grow as exo-phytic polypoid masses that extend intothe uterine cavity. Rarely, they may arisein the myometrium, presumably fro m
adenomyosis. Although the tumour isusually a single polypoid mass, it some-times may present as multiple papillarymasses. On sectioning, the surface is tanb rown with foci of haemorrhage andnecrosis. Small cysts are frequently pres-ent. Most adenosarcomas do not invadethe myometrium.
HistopathologyUnder low magnification a leaf-like patternclosely resembling phyllodes tumour ofthe breast is observed. Isolated glands,often dilated and compressed into thinslits, are dispersed throughout the mes-enchymal component. Characte- ristically,t h e re is stromal condensation surro u n d i n gthe glands and clefts. It is in these are a sw h e re the greatest degree of stro m a latypia and mitotic activity is present. Bydefinition the epithelium is benign andmay show focal metaplastic changes. Themesenchymal component of ana d e n o s a rcoma is generally a low gradehomologous stromal sarcoma containingv a rying amounts of fibrous tissue andsmooth muscle. Mesenchymal mitotic fig-u res, usually stated to be more than oneper 10 high power fields, are re q u i red inthe hypercellular cuffs. Cytological atypiais typically only mild, but is occasionallymoderate. Sex cord-like componentsresembling those in endometrial stro m a ls a rcomas are found in less than 10% ofa d e n o s a rcomas. Heterologous compo-nents consisting of striated muscle (mostcommonly), cartilage, fat and other com-ponents are present in approximately 10-15% of tumours The diagnosis of sarc o-matous overgrowth is made if the pure
BAFig. 4.44 Adenosarcoma. A The tumour is composed of tubular and convoluted, cleft-like glands of endometrioid type surrounded by a cuff of cellular mesenchyme.B A polypoid structure compresses a glandular lumen producing a leaf-like pattern similar to that of a mammary phyllodes tumour. The epithelial component is cytologi-cally bland, and the mesenchymal component is cellular and fibromatous without significant nuclear atypia but contained abundant mitoses.
247Mixed epithelial and mesenchymal tumours

248 Tumours of the uterine corpus
sarcomatous component, usually of highgrade, occupies 25% or more of the totaltumour volume.
ImmunoprofileAs might be expected, the epithelialcomponent reacts with a broad spectrumof antibodies to cytokeratins. The mes-enchymal component usually re a c t sfocally with antibodies to CD10. Variabledegrees of staining for smooth musclemarkers, desmin and caldesmon, canalso be observed.
Differential diagnosisThe differential diagnosis includes ade-nofibroma and in children sarcoma botry-oides (embryonal rhabdomyosarcoma).
Prognosis and predictive factorsA d e n o s a rcoma is considered a lowgrade neoplasm but recurs in approxi-mately 25-40% of cases, typically in thepelvis or vagina, and distant metastasishas been reported in 5% of cases {515}.The metastases almost always are com-posed of a sarcomatous element only,but rarely epithelium has been reported.Factors in the primary tumour that arep redictive of a poor outcome areextrauterine spread, deep myometrialinvasion into the outer half of themyometrium and sarcomatous over-growth. Vascular invasion is usually notidentified but, if present, is a poor riskfactor. Rhabdomyosarcomatous differen-tiation was an adverse prognostic factorin one series {1388}. There appears to beno correlation between the pro g n o s i sand the level of mitotic activity. Long-t e rm follow-up is necessary becausere c u r rences may manifest after manyyears. Most tumour deaths occur morethan five years after the diagnosis.
Carcinofibroma
DefinitionA neoplasm composed of an admixtureof a malignant epithelial element and abenign mesenchymal component.
EpidemiologyThese are extremely uncommon neo-plasms with few cases reported in the lit-erature {1286,2228,2916}.
HistopathologyIn one case the epithelial component wasclear cell in type {2228}. The mesenchy-
mal component is usually fibro u s ,although occasional cases with a hetero l-ogous mesenchymal component havebeen described and have been designat-ed as carcinomesenchymoma {459}.
Prognosis and predictive factorsThe behaviour is not well establishedsince so few cases have been reportedbut would be expected to depend on thestage, depth of myometrial invasion andhistological subtype of the epithelialcomponent.
Adenofibroma
DefinitionA biphasic uterine neoplasm composedof benign epithelial and mesenchymalcomponents.
EpidemiologyUterine adenofibroma is an uncommonneoplasm, much less frequent thanadenosarcoma, which occurs most oftenin postmenopausal patients but also inyounger women. {3245}. Occasionalcases have been associated with tamox-ifen therapy {1258}.
MacroscopyAdenofibromas usually present as poly-poid lesions, commonly have a fibrousconsistency on sectioning, and some-times contain dilated cystic spaces.
HistopathologyAdenofibromas have a papillary or club-like growth pattern. They are composedof benign epithelial and mesenchymalcomponents, the epithelial componentforming a lining on the underlying mes-enchymal core. Cleft-like spaces areoften present. The epithelial componentmay be endometrioid or ciliated in typebut often is non-descript cuboidal orcolumnar. Rarely, there are foci of squa-mous metaplasia. The mesenchyme isusually of a non-specific fibro b l a s t i ctype, although rarely it may containendometrial stromal or smooth musclecomponents. Stromal atypia, mitoticactivity and periglandular cuffing areabsent or inconspicuous. Rare l y, adi-pose tissue or skeletal muscle compo-nents are present, and such lesions havebeen designated lipoadenofibroma oradenomyofibroma {1239,2711}.
Differential diagnosisIf there is a stromal mitotic count of >1mitosis per 10 high power fields, markedstromal hypercellularity with periglandu-lar cuffing and/or more than mild stromalatypia, a diagnosis of low gradeadenosarcoma should be made.
Prognosis and predictive factorsA d e n o f i b romas are benign lesions,although they may recur following"polypectomy" {2625}. Occasional
Fig. 4.45 Atypical polypoid adenomyoma. This polypoid lesion shows a biphasic epithelial and stromal pro-liferation. The glandular component consists of endometrioid glands with a variable degree of complexity,whereas the mesenchymal component is myofibromatous and cytologically bland.

249Mixed epithelial and mesenchymal tumours
tumours may superficially invade themyometrium, but metastases have notbeen reported. Invasion of myometrialveins has also been described {514}.Occasional cases have been focallyinvolved by adenocarcinoma, but theassociation is probably incidental {1873}.
Adenomyoma including atypicalpolypoid adenomyoma
DefinitionA lesion composed of benign epithelial(usually endometrial glands) and mes-enchymal components in which the mes-enchymal component is fibromyomatousAtypical polypoid adenomyoma is a vari-ant of adenomyoma in which the glandu-lar component exhibits arc h i t e c t u r a lcomplexity with or without cytologicalatypia.
EpidemiologyAdenomyoma may occur at any age,whereas atypical polypoid adenomyomacharacteristically occurs in pre-menopausal women {1690,1801,3228}.
MacroscopyAdenomyomas and atypical polypoidadenomyomas usually are polypoid sub-mucosal lesions but may rarely be intra-mural or subserosal {1002}. They have af i rm sectioned surface. Atypical poly-poid adenomyoma usually involves thelower uterine segment or upper endo-c e r v i x .
HistopathologyAdenomyoma is composed of an admix-t u re of benign endometrial glands (theremay be minor foci of tubal, mucinous orsquamous epithelium) with minimal cyto-logical atypia and architectural complexi-ty embedded in a benign fibro m y o m a t o u smesenchyme. Often endometrial types t roma surrounds the endometrial glandu-lar component, and the former is in turns u r rounded by smooth muscle {1002}.
Atypical polypoid adenomyomaIn atypical polypoid adenomyoma theglands characteristically show markeda rchitectural complexity; there is noendometrial type stroma around the dis-t o rted glands. There is often also cytolog-ical atypia that varies from mild to marked.Foci may be present that arc h i t e c t u r a l l yresemble well diff e rentiated adenocarc i-noma, and such tumours have been des-ignated "atypical polypoid adenomyomaof low malignant potential" {1690}.Extensive squamous or morular metapla-sia of the glandular elements, with or with-out central necrosis, is a common finding.The mesenchymal component is com-posed of swirling and interlacing fasciclesof benign smooth muscle.
Differential diagnosisIt should be noted that many simpleendometrial polyps contain a minor com-ponent of smooth muscle within the stro-ma; however, this finding alone is nots u fficient for the diagnosis of adenomy-oma. The designation adenomyoma has
also been used for a localized adeno-myosis that forms a discrete mass, butsuch usage is confusing and not re c o m-mended. D i ff e rentiation from a well diff e re n t i a t e dendometrioid adenocarcinoma invadingthe myometrium may be difficult, espe-cially on a curettage or biopsy specimen.H o w e v e r, the usual lack of pro n o u n c e dcellular atypia and the absence of a stro-mal desmoplastic response would beagainst a diagnosis of adenocarc i n o m a .Additional features against a diagnosis ofc a rcinoma are the usual youth of thepatient and the presence of norm a lendometrial fragments in the sample.
Genetic susceptibilityAtypical polypoid adenomyomas mayoccur in women with Tu rner syndro m e{ 5 1 7 } .
Prognosis and predictive factorsAdenomyoma is generally cured by sim-ple polypectomy, but if associated withmyometrial adenomyosis, symptoms maypersist. Atypical polypoid adenomyomamay re c u r, especially following incom-plete removal. In addition, superf i c i a lmyometrial infiltration is often identified inh y s t e rectomy specimens, a finding thatmay be more common in those cases withmarked glandular architectural complexi-ty {1690}. A small number of cases areassociated with an underlying endometri-oid adenocarcinoma with a transition zonebetween the two components {1882,2 8 1 3 } .
250 Tumours of the uterine corpus
DefinitionA heterogeneous group of gestationaland neoplastic conditions arising fromtrophoblast, including molar gestationsand trophoblastic tumours.
EpidemiologyGestational trophoblastic disease (GTD)varies widely among various populationswith figures as high as 1 in 120 pregnan-cies in some areas of Asia and SouthAmerica compared to 0.6-1.1 per 1000 inthe United States {1162}. The incidenceof hydatidiform moles is greater inwomen older than 40 years {161} and isalso increased in those younger than 20years. Patients who have had prior GTDare more at risk of having a second GTDafter subsequent pregnancies. Other riskfactors include: a diet low in vitamin A,lower socioeconomic status and bloodgroup A women married to group 0 men{161,162,244,363}.
AetiologyHydatiform moles arise from abnormalconceptions. Partial moles result fromdiandric triploidy, whereas completemoles result from diandry (fertilization ofan empty ovum). Up to 50% of chorio-carcinomas and 15% of placental sitet rophoblastic tumours follow completemoles.
Clinical featuresSigns and symptomsA complete molar pregnancy usuallyp resents with first trimester bleeding, auterus larger than expected for gestation-al age and the absence of fetal parts onultrasound in association with a markedlyelevated beta-human chorionicg o n a d o t ropin (β-hCG) level {568}. Othersigns include hyperemesis, toxaemia dur-ing the first or second trimester, thecalutein cysts and hypert h y roidism. Patientswith partial molar gestations usually pre s-ent as spontaneous abortions, sometimeswith increased β-hCG levels. GTD shouldalways be considered when a patient hascontinued vaginal bleeding followingd e l i v e ry or abortion.
ImagingA characteristic pattern of multiple vesi-cles (snowstorm pattern) is commonlyseen with complete molar pregnancy.The diagnosis of partial molar pregnancyby ultrasonography is more difficult.
Tumour spread and stagingC h o r i o c a rcinoma spreads haematoge-nously and may involve the lung (57-80%), vagina (30%), pelvis (20%), brain(17%), and liver (10%) {168,243}. Sinceβ-hCG titres accurately reflect the clinicaldisease, histological verification is notrequired for diagnosis. Staging shouldbe based on history, clinical examinationand appropriate laboratory and radiolog-ical studies.Metastatic GTD is also categorized bythe WHO scoring system as low, medi-um, and high risk {51,2976}. The individ-ual scores for each prognostic factor areadded together to obtain a total score. Atotal prognostic score less than or equalto 4 is considered low risk, a total scoreof 5-7 is considered middle risk, and atotal score of 8 or greater is consideredhigh risk. (See TNM and FIGO classifica-tion of gestational trophoblastic tumoursat the beginning of the chapter).
Somatic geneticsOverexpression of TP53 protein may beassociated with more aggressive behav-iour in gestational trophoblastic disease
since it is more commonly observed incomplete moles and choriocarc i n o m a{937,1616,2307}, but TP53 mutations areuncommon {471}. Overexpression of thep21 gene has also been detected incomplete moles and choriocarc i n o m a{469}. No correlation between p21 andTP53 expression has been detected ingestational trophoblastic disease.Both complete mole and choriocarcino-ma exhibit overe x p ression of severalgrowth factors including c-Myc, epider-mal growth factors receptor (EGFR),c-erbB-2, Rb, mdm2, and bcl-2 as com-pared to normal placenta and partialmole {938,2966}. Expression of c-fmsprotein does not differ between normalplacenta and gestational trophoblasticdiseases {938}. In one study stro n gimmunostaining of c-erbB-3 and epider-mal growth factor receptor in extravilloustrophoblast of complete mole was signif-icantly correlated with the developmentof persistent gestational tro p h o b l a s t i ctumour {2966}. The molecular pathogen-esis of gestational trophoblastic diseasesmay involve these and potentially othergrowth-regulatory factors.
Prognosis and predictive factorsMajor adverse prognostic variables forGTD are:
(1) Age >39(2) Prior term pregnancy(3) Interval from antecedent
pregnancy of >12 months(4) β-hCG >105 IU/litre(5) Tumour mass >5cm(6) Disease in liver and brain (7) Failure of 2 or more prior
chemotherapiesThe above factors are included in aprognostic score (see the TNM and FIGOclassification of gestational trophoblastictumours at the beginning of the chapter).The patients are separated into low riskand high risk groups for different treat-ments {1123,3111}.The prognosis of patients with low riskdisease is very close to 100% survival,whilst patients with high risk diseasehave a survival of 85-95%, depending onthe number of patients with ultra highriskdisease in the patient population.
D.R. GenestR.S. BerkowitzR.A. FisherE.S. NewlandsM. Fehr
Gestational trophoblastic disease
Table 4.08The U.S. National Institutes of Health staging classi-fication for gestational trophoblastic disease (GTD).
I Benign GTDA. Complete hydatidiform moleB. Partial hydatidiform mole
II Malignant GTDA. Non-metastatic GTDB. Metastatic GTD
1. Good prognosis: absence of any risk factor
2. Poor prognosis: presence of any risk factor
a. Duration of GTD >4monthsb. Pre-therapy serum
β-hCG>40,000 mIU/mLc. Brain or liver metastasisd. GTD after term gestatione. Failed prior chemotherapy
for GTD
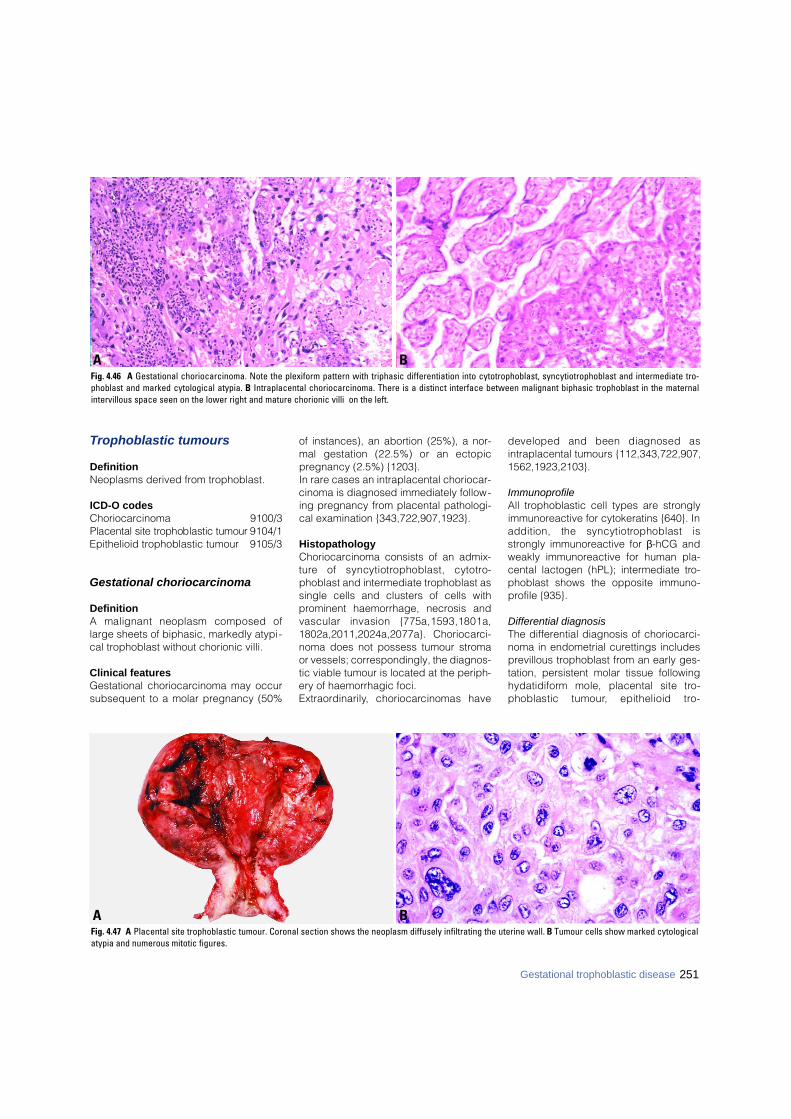
Trophoblastic tumours
DefinitionNeoplasms derived from trophoblast.
ICD-O codesChoriocarcinoma 9100/3Placental site trophoblastic tumour 9104/1Epithelioid trophoblastic tumour 9105/3
Gestational choriocarcinoma
DefinitionA malignant neoplasm composed oflarge sheets of biphasic, markedly atypi-cal trophoblast without chorionic villi.
Clinical featuresGestational choriocarcinoma may occursubsequent to a molar pregnancy (50%
of instances), an abortion (25%), a nor-mal gestation (22.5%) or an ectopicpregnancy (2.5%) {1203}. In rare cases an intraplacental choriocar-cinoma is diagnosed immediately follow-ing pregnancy from placental pathologi-cal examination {343,722,907,1923}.
HistopathologyChoriocarcinoma consists of an admix-t u re of syncytiotrophoblast, cytotro-phoblast and intermediate trophoblast assingle cells and clusters of cells withprominent haemorrhage, necrosis andvascular invasion {775a,1593,1801a,1802a,2011,2024a,2077a}. Choriocarc i -noma does not possess tumour stromaor vessels; correspondingly, the diagnos-tic viable tumour is located at the periph-ery of haemorrhagic foci.E x t r a o rd i n a r i l y, choriocarcinomas have
developed and been diagnosed asintraplacental tumours {112,343,722,907,1562,1923,2103}.
ImmunoprofileAll trophoblastic cell types are stronglyimmunoreactive for cytokeratins {640}. Inaddition, the syncytiotrophoblast isstrongly immunoreactive for β-hCG andweakly immunoreactive for human pla-cental lactogen (hPL); intermediate tro-phoblast shows the opposite immuno-profile {935}.
Differential diagnosisThe differential diagnosis of choriocarci-noma in endometrial curettings includesprevillous trophoblast from an early ges-tation, persistent molar tissue followingh y d a t i d i f o rm mole, placental site tro-phoblastic tumour, epithelioid tro-
BAFig. 4.46 A Gestational choriocarcinoma. Note the plexiform pattern with triphasic differentiation into cytotrophoblast, syncytiotrophoblast and intermediate tro-phoblast and marked cytological atypia. B Intraplacental choriocarcinoma. There is a distinct interface between malignant biphasic trophoblast in the maternalintervillous space seen on the lower right and mature chorionic villi on the left.
BAFig. 4.47 A Placental site trophoblastic tumour. Coronal section shows the neoplasm diffusely infiltrating the uterine wall. B Tumour cells show marked cytologicalatypia and numerous mitotic figures.
251Gestational trophoblastic disease

252 Tumours of the uterine corpus
phoblastic tumour and undifferentiatedcarcinoma.
Somatic geneticsRecent studies using cDNA microarrayanalysis have demonstrated decreasedexpression of heat shock protein-27 inchoriocarcinoma, a finding which hasbeen associated with chemotherapyresponsiveness in other cancers {3014}.
Placental site trophoblastictumour
DefinitionA monophasic neoplasm composed ofi n t e rmediate trophoblast and cytotro-phoblast without a significant componentof syncytiotrophoblast.
HistopathologyThe tumour cells are medium to largesized and mononuclear or multinucleat-ed with mild to marked nuclear atypia,prominent nucleoli, eosinophilic to clearcytoplasm, scattered mitoses and occa-sional intranuclear inclusions {746,747,8 4 2 , 8 6 1 , 9 3 3 , 1 0 1 8 , 1 0 1 9 , 1 1 7 7 , 1 2 3 7 ,1 5 1 1 , 1 5 4 0 , 1 5 4 3 , 1 5 8 9 , 2 9 6 7 , 3 2 0 2 , 3 2 2 7 } .They permeate the myometrium and ves-sels in a manner reminiscent of theimplantation site trophoblast.
Differential diagnosisThe differential diagnosis of placentalsite trophoblastic tumour includes pla-cental site nodule, exaggerated implan-tation site, epithelioid leiomyosarcoma,epithelioid trophoblastic tumour andpoorly diff e rentiated carc i n o m a .Extensive sampling and immunohisto-
chemistry for keratin, β-hCG and hPL arehelpful in distinguishing among theabove lesions {2658,2659}.
Somatic geneticsA Y- c h romosomal locus and/or new(paternal) alleles not present in adjacentnormal uterine tissue was demonstratedin all cases of placental site trophoblastictumour studied confirming the placentalorigin of these neoplasms {2747}.
Prognosis and predictive factorsPlacental site trophoblastic tumours arerare, and their biological behaviour isvariable. The major prognostic variable isa long interval from the last knownantecedent pregnancy. All patient deathsfrom placental site trophoblastic tumourin the Charing Cross series occurredwhen the interval from the last knownpregnancy was greater than 4 years. Anelevated mitotic index predicts a pooroutcome {842}.
Epithelioid trophoblastic tumour
DefinitionA tumour composed of a monomorphicpopulation of intermediate trophoblasticcells closely resembling those of thechorion laeve (membranous chorion).
HistopathologyThe epithelioid trophoblastic tumour is arelatively uncommon, recently describedneoplasm that differs from the placentalsite trophoblastic tumour in that thetumour cells of the epithelioid tro-phoblastic tumour are smaller and lesspleomorphic and grow in a nodular as
opposed to a diffusely infiltrative pattern.Because they are frequently found in thecervix, they may be confused with hyalin-izing squamous cell carc i n o m a s .Epithelioid trophoblastic tumours arefocally immunoreactive for placental-likealkaline phosphatase (PLAP) and hPLbut strongly and diffusely immunoreac-tive for E-cadherin and epidermal growthfactor receptor {2658}.
Somatic geneticsA Y- c h romosomal locus and/or new( p a t e rnal) alleles not present in adjacentn o rmal uterine tissue was demonstratedin all cases of epithelioid tro p h o b l a s t i ctumour studied confirming the placentalorigin of this neoplasm {2747}.
Prognosis and predictive factorsBased on available data, the behaviour ofepithelioid trophoblastic tumour re s e m b l e sthat of placental site trophoblastic tumour.
Hydatidiform mole
DefinitionAn abnormal placenta with villoushydrops and variable degrees of tro-phoblastic proliferation.
ICD-O codesHydatidiform mole, NOS 9100/0
Complete 9100/0Partial 9103/0Invasive 9100/1
Complete hydatidiform mole
DefinitionA hydatidiform mole involving most of the
BAFig. 4.48 Epithelioid trophoblastic tumour. A Neoplastic aggregates are better defined than in placental site trophoblastic tumour and may resemble carcinoma.B Groups of tumour cells, occasionally with clear cytoplasm, are separated by a hyaline stroma.
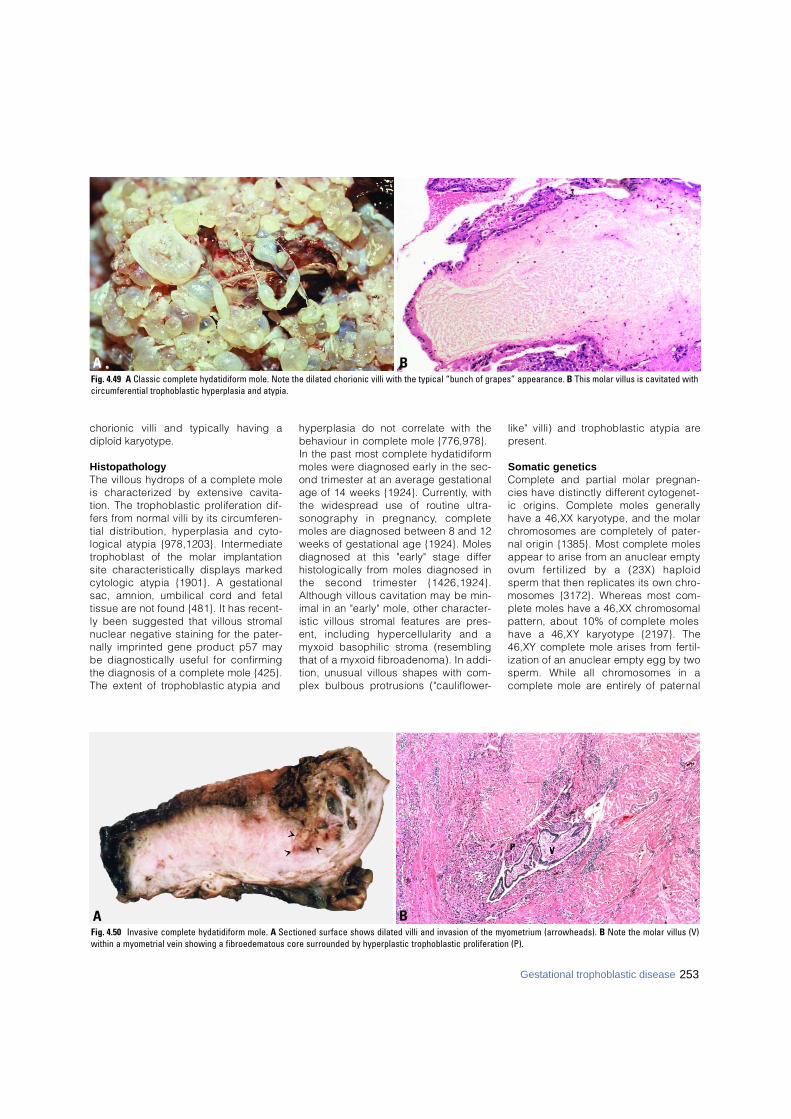
253Gestational trophoblastic disease
chorionic villi and typically having adiploid karyotype.
HistopathologyThe villous hydrops of a complete moleis characterized by extensive cavita-tion. The trophoblastic proliferation dif-fers from normal villi by its circ u m f e re n-tial distribution, hyperplasia and cyto-logical atypia {978,1203}. Interm e d i a t et rophoblast of the molar implantationsite characteristically displays markedcytologic atypia {1901}. A gestationalsac, amnion, umbilical cord and fetaltissue are not found {481}. It has re c e n t-ly been suggested that villous stro m a lnuclear negative staining for the pater-nally imprinted gene product p57 maybe diagnostically useful for confirm i n gthe diagnosis of a complete mole {425}.The extent of trophoblastic atypia and
hyperplasia do not correlate with thebehaviour in complete mole {776,978}.In the past most complete hydatidiformmoles were diagnosed early in the sec-ond trimester at an average gestationalage of 14 weeks {1924}. Curre n t l y, withthe widespread use of routine ultra-sonography in pre g n a n c y, completemoles are diagnosed between 8 and 12weeks of gestational age {1924}. Molesdiagnosed at this "early" stage diff e rhistologically from moles diagnosed inthe second trimester {1426,1924}.Although villous cavitation may be min-imal in an "early" mole, other character-istic villous stromal features are pre s-ent, including hypercellularity and amyxoid basophilic stroma (re s e m b l i n gthat of a myxoid fibroadenoma). In addi-tion, unusual villous shapes with com-plex bulbous protrusions ("cauliflower-
like" villi) and trophoblastic atypia arep re s e n t .
Somatic geneticsComplete and partial molar pre g n a n-cies have distinctly diff e rent cytogenet-ic origins. Complete moles generallyhave a 46,XX karyotype, and the molarc h romosomes are completely of pater-nal origin {1385}. Most complete molesappear to arise from an anuclear emptyovum fertilized by a (23X) haploids p e rm that then replicates its own chro-mosomes {3172}. Whereas most com-plete moles have a 46,XX chro m o s o m a lp a t t e rn, about 10% of complete moleshave a 46,XY karyotype {2197}. The46,XY complete mole arises from fert i l-ization of an anuclear empty egg by twos p e rm. While all chromosomes in acomplete mole are entirely of patern a l
BAFig. 4.50 Invasive complete hydatidiform mole. A Sectioned surface shows dilated villi and invasion of the myometrium (arrowheads). B Note the molar villus (V)within a myometrial vein showing a fibroedematous core surrounded by hyperplastic trophoblastic proliferation (P).
BAFig. 4.49 A Classic complete hydatidiform mole. Note the dilated chorionic villi with the typical “bunch of grapes” appearance. B This molar villus is cavitated withcircumferential trophoblastic hyperplasia and atypia.
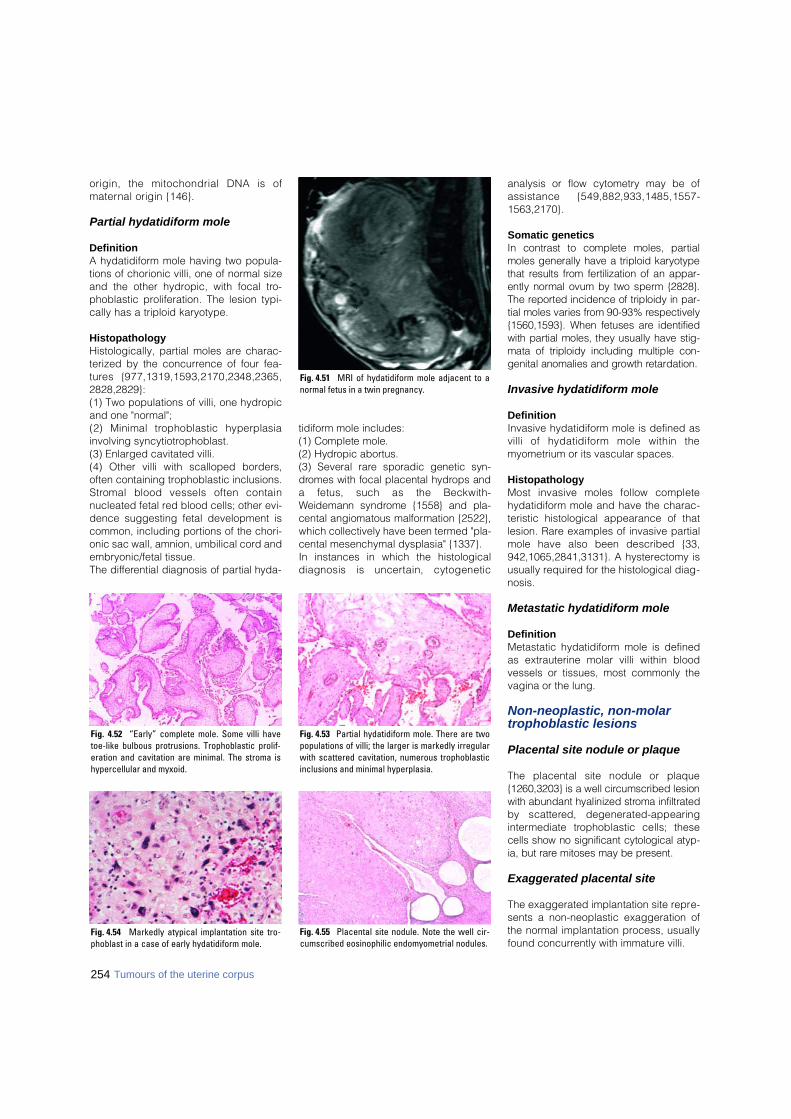
254 Tumours of the uterine corpus
origin, the mitochondrial DNA is ofm a t e rnal origin {146}.
Partial hydatidiform mole
DefinitionA hydatidiform mole having two popula-tions of chorionic villi, one of normal sizeand the other hydropic, with focal tro-phoblastic proliferation. The lesion typi-cally has a triploid karyotype.
HistopathologyHistologically, partial moles are charac-terized by the concurrence of four fea-t u res {977,1319,1593,2170,2348,2365,2828,2829}: (1) Two populations of villi, one hydropicand one "normal"; (2) Minimal trophoblastic hyperplasiainvolving syncytiotrophoblast.(3) Enlarged cavitated villi.(4) Other villi with scalloped borders,often containing trophoblastic inclusions.S t romal blood vessels often containnucleated fetal red blood cells; other evi-dence suggesting fetal development iscommon, including portions of the chori-onic sac wall, amnion, umbilical cord andembryonic/fetal tissue. The diff e rential diagnosis of partial hyda-
t i d i f o rm mole includes:(1) Complete mole.(2) Hydropic abort u s .(3) Several rare sporadic genetic syn-d romes with focal placental hydrops anda fetus, such as the Beckwith-Weidemann syndrome {1558} and pla-cental angiomatous malformation {2522},which collectively have been termed "pla-cental mesenchymal dysplasia" {1337}.In instances in which the histologicaldiagnosis is uncertain, cytogenetic
analysis or flow cytometry may be ofassistance {549,882,933,1485,1557-1563,2170}.
Somatic geneticsIn contrast to complete moles, part i a lmoles generally have a triploid kary o t y p ethat results from fertilization of an appar-ently normal ovum by two sperm {2828}.The re p o rted incidence of triploidy in par-tial moles varies from 90-93% re s p e c t i v e l y{1560,1593}. When fetuses are identifiedwith partial moles, they usually have stig-mata of triploidy including multiple con-genital anomalies and growth re t a rd a t i o n .
Invasive hydatidiform mole
DefinitionInvasive hydatidiform mole is defined asvilli of hydatidiform mole within themyometrium or its vascular spaces.
HistopathologyMost invasive moles follow completehydatidiform mole and have the charac-teristic histological appearance of thatlesion. Rare examples of invasive partialmole have also been described {33,942,1065,2841,3131}. A hysterectomy isusually required for the histological diag-nosis.
Metastatic hydatidiform mole
DefinitionMetastatic hydatidiform mole is definedas extrauterine molar villi within bloodvessels or tissues, most commonly thevagina or the lung.
Non-neoplastic, non-molar trophoblastic lesions
Placental site nodule or plaque
The placental site nodule or plaque{1260,3203} is a well circumscribed lesionwith abundant hyalinized stroma infiltratedby scattered, degenerated-appearingi n t e rmediate trophoblastic cells; thesecells show no significant cytological atyp-ia, but rare mitoses may be present.
Exaggerated placental site
The exaggerated implantation site repre-sents a non-neoplastic exaggeration ofthe normal implantation process, usuallyfound concurrently with immature villi.
Fig. 4.52 “Early” complete mole. Some villi havetoe-like bulbous protrusions. Trophoblastic prolif-eration and cavitation are minimal. The stroma ishypercellular and myxoid.
Fig. 4.53 Partial hydatidiform mole. There are twopopulations of villi; the larger is markedly irregularwith scattered cavitation, numerous trophoblasticinclusions and minimal hyperplasia.
Fig. 4.55 Placental site nodule. Note the well cir-cumscribed eosinophilic endomyometrial nodules.
Fig. 4.54 Markedly atypical implantation site tro-phoblast in a case of early hydatidiform mole.
Fig. 4.51 MRI of hydatidiform mole adjacent to anormal fetus in a twin pregnancy.
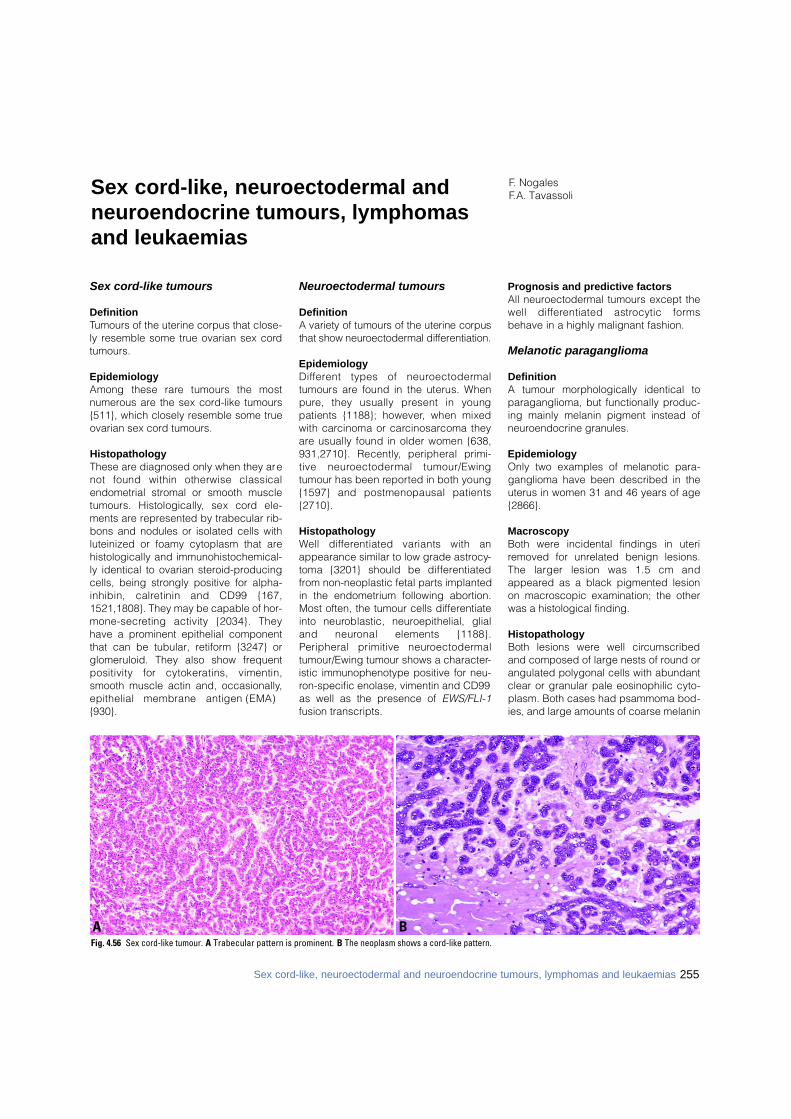
Sex cord-like tumours
DefinitionTumours of the uterine corpus that close-ly resemble some true ovarian sex cordtumours.
EpidemiologyAmong these rare tumours the mostnumerous are the sex cord-like tumours{511}, which closely resemble some trueovarian sex cord tumours.
HistopathologyThese are diagnosed only when they arenot found within otherwise classicalendometrial stromal or smooth muscletumours. Histologically, sex cord ele-ments are represented by trabecular rib-bons and nodules or isolated cells withluteinized or foamy cytoplasm that arehistologically and immunohistochemical-ly identical to ovarian steroid-producingcells, being strongly positive for alpha-inhibin, calretinin and CD99 {167,1521,1808}. They may be capable of hor-m o n e - s e c reting activity {2034}. Theyhave a prominent epithelial componentthat can be tubular, retiform {3247} orglomeruloid. They also show frequentpositivity for cytokeratins, vimentin,smooth muscle actin and, occasionally,epithelial membrane antigen (EMA){930}.
Neuroectodermal tumours
DefinitionA variety of tumours of the uterine corpusthat show neuro e c t o d e rmal diff e re n t i a t i o n .
EpidemiologyD i ff e rent types of neuro e c t o d e rm a ltumours are found in the uterus. Whenp u re, they usually present in youngpatients {1188}; however, when mixedwith carcinoma or carc i n o s a rcoma theya re usually found in older women {638,931,2710}. Recently, peripheral primi-tive neuro e c t o d e rmal tumour/Ewingtumour has been re p o rted in both young{1597} and postmenopausal patients{ 2 7 1 0 } .
HistopathologyWell diff e rentiated variants with anappearance similar to low grade astrocy-toma {3201} should be diff e re n t i a t e dfrom non-neoplastic fetal parts implantedin the endometrium following abortion.Most often, the tumour cells differentiateinto neuroblastic, neuroepithelial, glialand neuronal elements {1188}.Peripheral primitive neuro e c t o d e rm a ltumour/Ewing tumour shows a character-istic immunophenotype positive for neu-ron-specific enolase, vimentin and CD99as well as the presence of EWS/FLI-1fusion transcripts.
Prognosis and predictive factorsAll neuroectodermal tumours except thewell diff e rentiated astrocytic form sbehave in a highly malignant fashion.
Melanotic paraganglioma
DefinitionA tumour morphologically identical toparaganglioma, but functionally produc-ing mainly melanin pigment instead ofneuroendocrine granules.
EpidemiologyOnly two examples of melanotic para-ganglioma have been described in theuterus in women 31 and 46 years of age{2866}.
MacroscopyBoth were incidental findings in uteriremoved for unrelated benign lesions.The larger lesion was 1.5 cm andappeared as a black pigmented lesionon macroscopic examination; the otherwas a histological finding.
HistopathologyBoth lesions were well circ u m s c r i b e dand composed of large nests of round orangulated polygonal cells with abundantclear or granular pale eosinophilic cyto-plasm. Both cases had psammoma bod-ies, and large amounts of coarse melanin
F. NogalesF.A. TavassoliSex cord-like, neuroectodermal and
neuroendocrine tumours, lymphomasand leukaemias
BAFig. 4.56 Sex cord-like tumour. A Trabecular pattern is prominent. B The neoplasm shows a cord-like pattern.
255Sex cord-like, neuroectodermal and neuroendocrine tumours, lymphomas and leukaemias
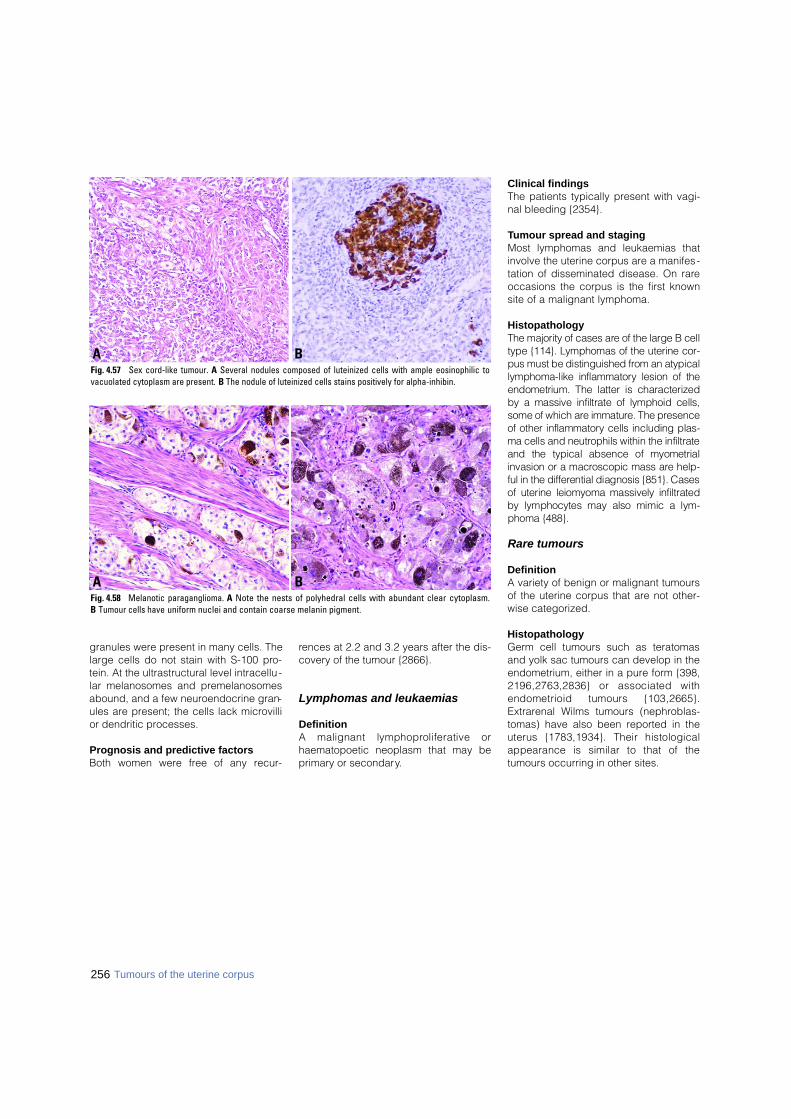
256 Tumours of the uterine corpus
granules were present in many cells. Thelarge cells do not stain with S-100 pro-tein. At the ultrastructural level intracellu -lar melanosomes and premelanosomesabound, and a few neuroendocrine gran-ules are present; the cells lack microvillior dendritic processes.
Prognosis and predictive factorsBoth women were free of any recur-
rences at 2.2 and 3.2 years after the dis-covery of the tumour {2866}.
Lymphomas and leukaemias
DefinitionA malignant lymphoproliferative orhaematopoetic neoplasm that may beprimary or secondary.
Clinical findingsThe patients typically present with vagi-nal bleeding {2354}.
Tumour spread and stagingMost lymphomas and leukaemias thatinvolve the uterine corpus are a manifes-tation of disseminated disease. On rareoccasions the corpus is the first knownsite of a malignant lymphoma.
HistopathologyThe majority of cases are of the large B celltype {114}. Lymphomas of the uterine cor-pus must be distinguished from an atypicallymphoma-like inflammatory lesion of theendometrium. The latter is characterizedby a massive infiltrate of lymphoid cells,some of which are immature. The pre s e n c eof other inflammatory cells including plas-ma cells and neutrophils within the infiltrateand the typical absence of myometrialinvasion or a macroscopic mass are help-ful in the diff e rential diagnosis {851}. Casesof uterine leiomyoma massively infiltratedby lymphocytes may also mimic a lym-phoma {488}.
Rare tumours
DefinitionA variety of benign or malignant tumoursof the uterine corpus that are not other-wise categorized.
HistopathologyGerm cell tumours such as teratomasand yolk sac tumours can develop in theendometrium, either in a pure form {398,2196,2763,2836} or associated withendometrioid tumours {103,2665}.Extrarenal Wilms tumours (nephroblas-tomas) have also been reported in theuterus {1783,1934}. Their histologicalappearance is similar to that of thetumours occurring in other sites.
BAFig. 4.57 Sex cord-like tumour. A Several nodules composed of luteinized cells with ample eosinophilic to vacuolated cytoplasm are present. B The nodule of luteinized cells stains positively for alpha-inhibin.
BAFig. 4.58 Melanotic paraganglioma. A Note the nests of polyhedral cells with abundant clear cytoplasm. B Tumour cells have uniform nuclei and contain coarse melanin pigment.
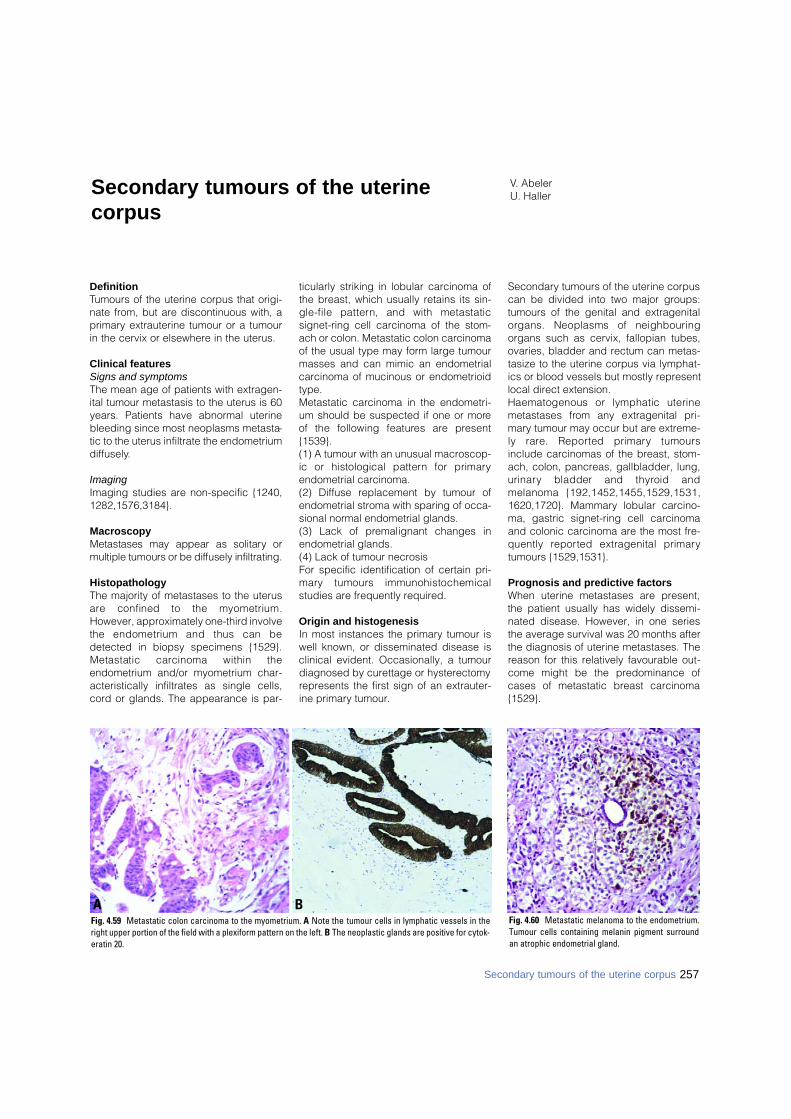
DefinitionTumours of the uterine corpus that origi-nate from, but are discontinuous with, aprimary extrauterine tumour or a tumourin the cervix or elsewhere in the uterus.
Clinical features Signs and symptomsThe mean age of patients with extragen-ital tumour metastasis to the uterus is 60years. Patients have abnormal uterinebleeding since most neoplasms metasta-tic to the uterus infiltrate the endometriumdiffusely.
ImagingImaging studies are non-specific {1240,1282,1576,3184}.
MacroscopyMetastases may appear as solitary ormultiple tumours or be diffusely infiltrating.
HistopathologyThe majority of metastases to the uterusa re confined to the myometrium.However, approximately one-third involvethe endometrium and thus can bedetected in biopsy specimens {1529}.Metastatic carcinoma within theendometrium and/or myometrium char-acteristically infiltrates as single cells,cord or glands. The appearance is par-
ticularly striking in lobular carcinoma ofthe breast, which usually retains its sin-gle-file pattern, and with metastaticsignet-ring cell carcinoma of the stom-ach or colon. Metastatic colon carcinomaof the usual type may form large tumourmasses and can mimic an endometrialcarcinoma of mucinous or endometrioidtype.Metastatic carcinoma in the endometri-um should be suspected if one or moreof the following features are pre s e n t{1539}. (1) A tumour with an unusual macroscop-ic or histological pattern for primaryendometrial carcinoma.(2) Diffuse replacement by tumour ofendometrial stroma with sparing of occa-sional normal endometrial glands.(3) Lack of premalignant changes inendometrial glands.(4) Lack of tumour necrosis For specific identification of certain pri-m a ry tumours immunohistochemicalstudies are frequently required.
Origin and histogenesisIn most instances the primary tumour iswell known, or disseminated disease isclinical evident. Occasionally, a tumourdiagnosed by curettage or hysterectomyrepresents the first sign of an extrauter-ine primary tumour.
Secondary tumours of the uterine corpuscan be divided into two major groups:tumours of the genital and extragenitalorgans. Neoplasms of neighbouringorgans such as cervix, fallopian tubes,ovaries, bladder and rectum can metas-tasize to the uterine corpus via lymphat-ics or blood vessels but mostly representlocal direct extension.Haematogenous or lymphatic uterinemetastases from any extragenital pri-mary tumour may occur but are extreme-ly rare. Reported primary tumoursinclude carcinomas of the breast, stom-ach, colon, pancreas, gallbladder, lung,u r i n a ry bladder and thyroid andmelanoma {192,1452,1455,1529,1531,1620,1720}. Mammary lobular carcino-ma, gastric signet-ring cell carcinomaand colonic carcinoma are the most fre-quently re p o rted extragenital primarytumours {1529,1531}.
Prognosis and predictive factorsWhen uterine metastases are present,the patient usually has widely dissemi-nated disease. However, in one seriesthe average survival was 20 months afterthe diagnosis of uterine metastases. Thereason for this relatively favourable out-come might be the predominance ofcases of metastatic breast carcinoma{1529}.
V. AbelerU. HallerSecondary tumours of the uterine
corpus
Fig. 4.60 Metastatic melanoma to the endometrium.Tumour cells containing melanin pigment surroundan atrophic endometrial gland.
BAFig. 4.59 Metastatic colon carcinoma to the myometrium. A Note the tumour cells in lymphatic vessels in theright upper portion of the field with a plexiform pattern on the left. B The neoplastic glands are positive for cytok-eratin 20.
257Secondary tumours of the uterine corpus
CHAPTER 5
Tumours of the Uterine Cervix
Cervical carcinoma is the second most common cancer inwomen worldwide. Chronic infection with human papilloma-virus (HPV) is a necessary event in the evolution of cervical carcinomas. The incidence of cervical cancer, which is pre-dominantly of the squamous cell type, has markedly declinedin many developed countries, mainly due to cytological screen-ing programmes. Today, more than 80% of women dying fromcervical cancer live in developing countries. It is anticipatedthat preventive HPV vaccination will become available in thenear future.
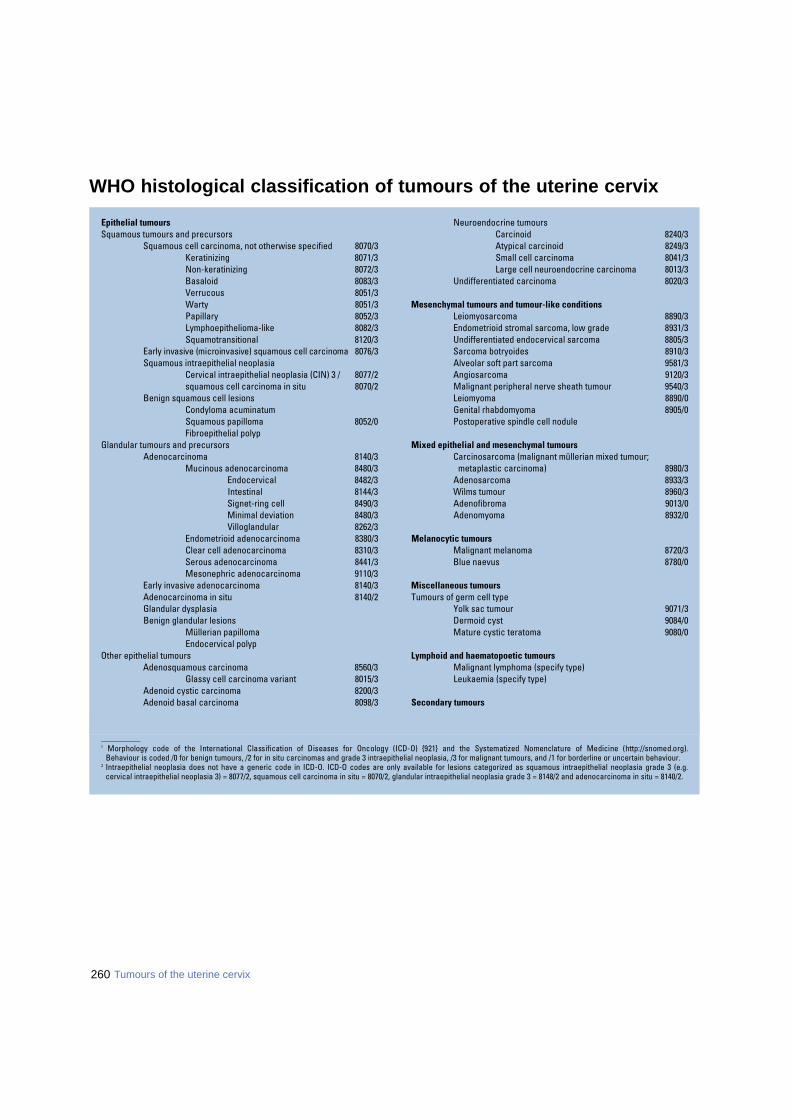
260 Tumours of the uterine cervix
WHO histological classification of tumours of the uterine cervix
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /2 for in situ carcinomas and grade 3 intraepithelial neoplasia, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.2 Intraepithelial neoplasia does not have a generic code in ICD-O. ICD-O codes are only available for lesions categorized as squamous intraepithelial neoplasia grade 3 (e.g.
cervical intraepithelial neoplasia 3) = 8077/2, squamous cell carcinoma in situ = 8070/2, glandular intraepithelial neoplasia grade 3 = 8148/2 and adenocarcinoma in situ = 8140/2.
Epithelial tumoursSquamous tumours and precursors
Squamous cell carcinoma, not otherwise specified 8070/3Keratinizing 8071/3Non-keratinizing 8072/3Basaloid 8083/3Verrucous 8051/3Warty 8051/3Papillary 8052/3Lymphoepithelioma-like 8082/3Squamotransitional 8120/3
Early invasive (microinvasive) squamous cell carcinoma 8076/3Squamous intraepithelial neoplasia
Cervical intraepithelial neoplasia (CIN) 3 / 8077/2squamous cell carcinoma in situ 8070/2
Benign squamous cell lesionsCondyloma acuminatumSquamous papilloma 8052/0Fibroepithelial polyp
Glandular tumours and precursorsAdenocarcinoma 8140/3
Mucinous adenocarcinoma 8480/3Endocervical 8482/3Intestinal 8144/3Signet-ring cell 8490/3Minimal deviation 8480/3Villoglandular 8262/3
Endometrioid adenocarcinoma 8380/3Clear cell adenocarcinoma 8310/3Serous adenocarcinoma 8441/3Mesonephric adenocarcinoma 9110/3
Early invasive adenocarcinoma 8140/3Adenocarcinoma in situ 8140/2Glandular dysplasiaBenign glandular lesions
Müllerian papillomaEndocervical polyp
Other epithelial tumoursAdenosquamous carcinoma 8560/3
Glassy cell carcinoma variant 8015/3Adenoid cystic carcinoma 8200/3Adenoid basal carcinoma 8098/3
Neuroendocrine tumoursCarcinoid 8240/3Atypical carcinoid 8249/3Small cell carcinoma 8041/3Large cell neuroendocrine carcinoma 8013/3
Undifferentiated carcinoma 8020/3
Mesenchymal tumours and tumour-like conditionsLeiomyosarcoma 8890/3Endometrioid stromal sarcoma, low grade 8931/3Undifferentiated endocervical sarcoma 8805/3Sarcoma botryoides 8910/3Alveolar soft part sarcoma 9581/3Angiosarcoma 9120/3Malignant peripheral nerve sheath tumour 9540/3Leiomyoma 8890/0Genital rhabdomyoma 8905/0Postoperative spindle cell nodule
Mixed epithelial and mesenchymal tumoursCarcinosarcoma (malignant müllerian mixed tumour;
metaplastic carcinoma) 8980/3Adenosarcoma 8933/3Wilms tumour 8960/3Adenofibroma 9013/0Adenomyoma 8932/0
Melanocytic tumoursMalignant melanoma 8720/3Blue naevus 8780/0
Miscellaneous tumoursTumours of germ cell type
Yolk sac tumour 9071/3Dermoid cyst 9084/0Mature cystic teratoma 9080/0
Lymphoid and haematopoetic tumoursMalignant lymphoma (specify type)Leukaemia (specify type)
Secondary tumours

_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The regional lymph nodes are the paracervical, parametrial, hypogastric (internal iliac, obturator), common and external iliac, presacral, and lateral sacral nodes.
TNM classification1,2
T – Primary Tumour
TNM FIGO Categories Stages
TX Primary tumour cannot be assessedT0 No evidence of primary tumourTis 0 Carcinoma in situ (preinvasive carcinoma)T1 I Cervical carcinoma confined to uterus (extension
to corpus should be disregarded)T1a IA Invasive carcinoma diagnosed only by microscopy.
All macroscopically visible lesions - even withsuperficial invasion - are T1b/Stage IB
T1a1 IA1 Stromal invasion no greater than 3.0 mm in depthand 7.0 mm or less in horizontal spread
T1a2 IA2 Stromal invasion more than 3.0 mm and not morethan 5.0 mm with a horizontal spread 7.0 mm or less
Note: The depth of invasion should not be more than 5 mm taken from the base of theepithelium, either surface or glandular, from which it originates. The depth of invasionis defined as the measurement of the tumour from the epithelial-stromal junction ofthe adjacent most superficial epithelial papilla to the deepest point of invasion.Vascular space involvement, venous or lymphatic, does not affect classification.
T1b IB Clinically visible lesion confined to the cervix ormicroscopic lesion greater than T1a2/IA2
T1b1 IB1 Clinically visible lesion 4.0 cm or less in greatestdimension
T1b2 IB2 Clinically visible lesion more than 4 cm in greatestdimension
T2 II Tumour invades beyond uterus but not to pelvic wallor to lower third of the vagina
T2a IIA Without parametrial invasionT2b IIB With parametrial invasionT3 III Tumour extends to pelvic wall, involves lower
third ofvagina, or causes hydronephrosis ornon-functioning kidney
T 3 a IIIA Tumour involves lower third of vagina, no extensionto pelvic wall
T3b IIIB Tumour extends to pelvic wall or causeshydronephrosis or non-functioning kidney
T4 IVA Tumour invades mucosa of bladder or rectum orextends beyond true pelvis
Note: The presence of bullous oedema is not sufficient to classify a tumour as T4.
M1 IVB Distant metastasis
N – Regional Lymph Nodes 3
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasis
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping
Stage 0 Tis N0 M0Stage IA T1a N0 M0Stage IA1 T1a1 N0 M0Stage IA2 T1a2 N0 M0Stage IB T1b N0 M0Stage IB1 T1b1 N0 M0Stage IB2 T1b2 N0 M0Stage IIA T2a N0 M0Stage IIB T2b N0 M0Stage IIIA T3a N0 M0Stage IIIB T1, T2, T3a N1 M0
T3b Any N M0Stage IVA T4 Any N M0Stage IVB Any T Any N M1
TNM and FIGO classification of carcinomas of the uterine cervix
261

Epithelial tumours M. Wells J.M. NeslandA.G. Östör A.K. GoodmanC.P. Crum R. SankaranarayananS. Franceschi A.G. HanselaarM. Tommasino J. Albores-Saavedra
This section covers the entire spectrum ofinvasive squamous and glandular carc i-nomas and their intraepithelial pre c u r s o rlesions that originate for the most partf rom the transformation zone of the cervix.In addition, benign epithelial tumours aredescribed which are not considered pre-cursors of invasive cancer.
EpidemiologyIn 1990 cervical cancer comprised 10%of cancers in women for a total of appro x-imately 470,000 cancer cases world-wide{846}, re p resenting the third most com-mon cancer in females and the most com-mon cancer in Sub-Saharan Africa,Central America, South Central Asia andMelanesia. Approximately 230,000women die annually from cervical cancer,and over 190,000 of those are from devel-oping countries. Zimbabwe and Indiastand out not only for their high incidencebut also for an unfavourable incidence tom o rtality ratio. Some relatively high-inci-dence countries can also be found inE a s t e rn and Central Europe {1638}. The incidence of cervical cancer hasbeen declining in the last three or fourdecades in most developed countriespredominantly due to the introduction ofcervical screening programmes. Otherreasons include a decrease in parity{1943} and improved living conditions{226}. In women under 45 years of age,however, mortality rates are levelling offor increasing in several countries {226}.Stable or, in some instances, upwardmortality trends in high-risk populationsin Latin America {2395} and EasternEurope {1638} are especially disturbing.Finally, adenocarcinoma of the cervix,which accounts for 10-15% of all cervicalcancers, has shown an increased inci-dence in the last three decades {3028}.
Aetiology Sexually transmitted virus, human papil-lomavirus (HPV), is the major aetiologicalfactor, as shown by:(1) the identification of HPV DNA in mostcervical cancer biopsy specimensworldwide {3044};
(2) relative risks (RRs) for cervical squa-mous cell and adenocarcinoma ofgreater than 70 for several high-risk HPVtypes in case-control studies {1199,1293};(3) RRs of approximately 10 for womenwith HPV infection in cohort studies{3143}. Several host and environmental factorscontribute, however, to enhance the pro b-ability of HPV persistence and pro g re s-sion to cervical neoplasia. Immune impair-ment, whether due to immunosuppre s s i v et reatments {274} or human immunodefi-ciency (HIV) infection {913, 920}, incre a s-es the risk of cervical intraepithelial neo-plasia (CIN) and invasive cancer of thecervix 5 to 10-fold. Among HPV-DNA pos-itive women long-term use of oral contra-ceptives {1911}, high parity {1943}, tobac-co smoking {3164} and certain sexuallytransmitted infections, such as Chlamydiatrachomatis {2733}, are associated with aRR between 2 and 4.
HPV-induced carcinogenesisThe products of two early genes, E6 andE7, have been shown to play a major role
in HPV-mediated cervical carcinogene-sis This has been established by threedifferent lines of evidence:(1) The first indication came from theanalysis of HPV-infected cells, whichshowed that viral DNA is randomly inte-grated in the genome of the majority ofcervical carcinomas. Integration leads todisruption of several viral genes withp reservation of only the E 6 and E 7genes, which are actively transcribed. (2) The discovery that E6 and E7 pro t e i n sa re able to induce cellular transform a t i o nin vitro confirmed their oncogenic ro l e .I m m o rtalized rodent fibroblasts can befully transformed by expression of HPV 16E6 or E7 protein. These rodent cellsa c q u i re the ability to grow in an anchor-age-independent manner and are tumori-genic when injected in nude mice. In addi-tion, HPV 16 E6 and E7 are able to immor-talize primary human keratinocytes, thenatural host cell of the virus. In agre e m e n twith the in vitro assays, transgenic micec o - e x p ressing both viral genes exhibit epi-d e rmal hyperplasia and various tumours. (3) Finally, biochemical studies haveclarified the mechanism of action of E6
Fig. 5.01 Global burden of cervical cancer. Age-standardized incidence rates (ASR) per 100,000 populationand year. From Globocan 2000 {846}.
262 Tumours of the uterine cervix
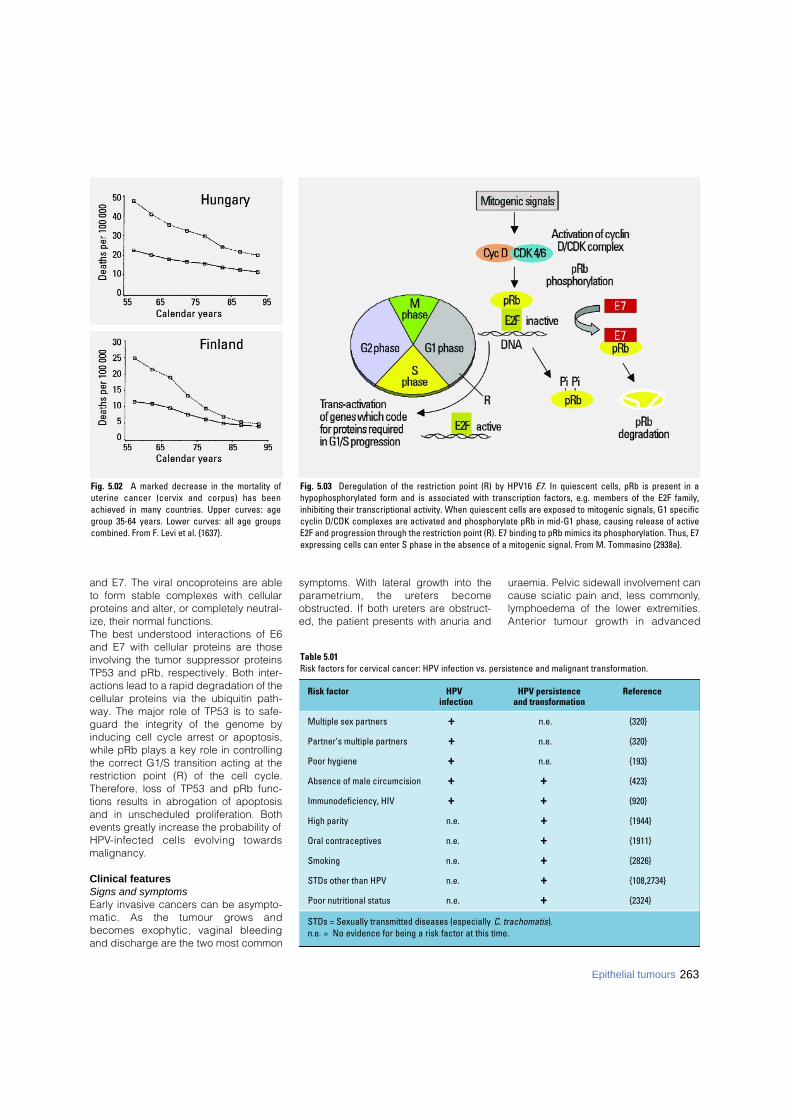
and E7. The viral oncoproteins are ableto form stable complexes with cellularproteins and alter, or completely neutral-ize, their normal functions.The best understood interactions of E6and E7 with cellular proteins are thoseinvolving the tumor suppressor proteinsTP53 and pRb, respectively. Both inter-actions lead to a rapid degradation of thecellular proteins via the ubiquitin path-way. The major role of TP53 is to safe-guard the integrity of the genome byinducing cell cycle arrest or apoptosis,while pRb plays a key role in controllingthe correct G1/S transition acting at therestriction point (R) of the cell cycle.Therefore, loss of TP53 and pRb func-tions results in abrogation of apoptosisand in unscheduled proliferation. Bothevents greatly increase the probability ofH P V-infected cells evolving toward smalignancy.
Clinical featuresSigns and symptoms Early invasive cancers can be asympto-matic. As the tumour grows andbecomes exophytic, vaginal bleedingand discharge are the two most common
symptoms. With lateral growth into theparametrium, the ureters becomeobstructed. If both ureters are obstruct-ed, the patient presents with anuria and
uraemia. Pelvic sidewall involvement cancause sciatic pain and, less commonly,lymphoedema of the lower extremities.Anterior tumour growth in advanced
Fig. 5.03 Deregulation of the restriction point (R) by HPV16 E7. In quiescent cells, pRb is present in ahypophosphorylated form and is associated with transcription factors, e.g. members of the E2F family,inhibiting their transcriptional activity. When quiescent cells are exposed to mitogenic signals, G1 specificcyclin D/CDK complexes are activated and phosphorylate pRb in mid-G1 phase, causing release of activeE2F and progression through the restriction point (R). E7 binding to pRb mimics its phosphorylation. Thus, E7expressing cells can enter S phase in the absence of a mitogenic signal. From M. Tommasino {2938a}.
Fig. 5.02 A marked decrease in the mortality ofuterine cancer (cervix and corpus) has beenachieved in many countries. Upper curves: agegroup 35-64 years. Lower curves: all age groupscombined. From F. Levi et al. {1637}.
263Epithelial tumours
Table 5.01Risk factors for cervical cancer: HPV infection vs. persistence and malignant transformation.
Risk factor HPV HPV persistence Referenceinfection and transformation
Multiple sex partners + n.e. {320}
Partner’s multiple partners + n.e. {320}
Poor hygiene + n.e. {193}
Absence of male circumcision + + {423}
Immunodeficiency, HIV + + {920}
High parity n.e. + {1944}
Oral contraceptives n.e. + {1911}
Smoking n.e. + {2826}
STDs other than HPV n.e. + {108,2734}
Poor nutritional status n.e. + {2324}
STDs = Sexually transmitted diseases (especially C. trachomatis).n.e. = No evidence for being a risk factor at this time.
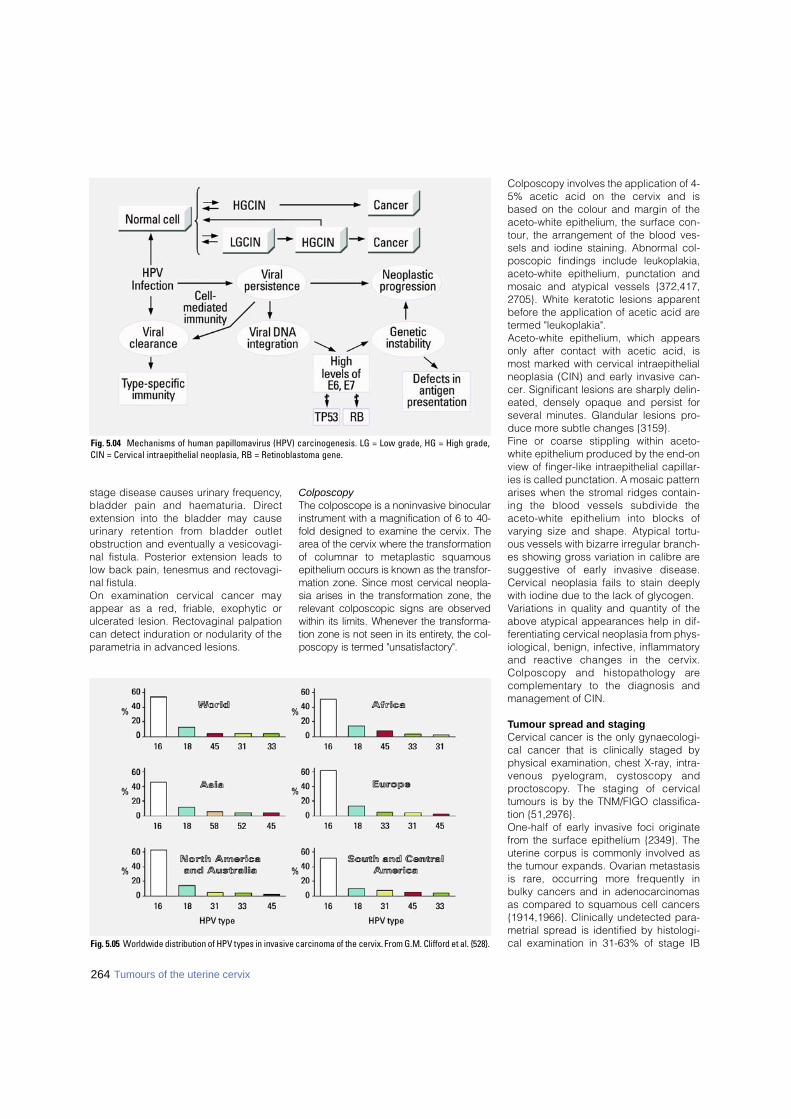
stage disease causes urinary frequency,bladder pain and haematuria. Dire c textension into the bladder may causeu r i n a ry retention from bladder outletobstruction and eventually a vesicovagi-nal fistula. Posterior extension leads tolow back pain, tenesmus and rectovagi-nal fistula.On examination cervical cancer mayappear as a red, friable, exophytic orulcerated lesion. Rectovaginal palpationcan detect induration or nodularity of theparametria in advanced lesions.
Colposcopy The colposcope is a noninvasive binocularinstrument with a magnification of 6 to 40-fold designed to examine the cervix. Thea rea of the cervix where the transform a t i o nof columnar to metaplastic squamousepithelium occurs is known as the transfor-mation zone. Since most cervical neopla-sia arises in the transformation zone, therelevant colposcopic signs are observedwithin its limits. Whenever the transform a-tion zone is not seen in its entire t y, the col-poscopy is termed "unsatisfactory".
Colposcopy involves the application of 4-5% acetic acid on the cervix and isbased on the colour and margin of theaceto-white epithelium, the surface con-tour, the arrangement of the blood ves-sels and iodine staining. Abnormal col-poscopic findings include leukoplakia,aceto-white epithelium, punctation andmosaic and atypical vessels {372,417,2705}. White keratotic lesions apparentbefore the application of acetic acid aretermed "leukoplakia".Aceto-white epithelium, which appearsonly after contact with acetic acid, ismost marked with cervical intraepithelialneoplasia (CIN) and early invasive can-cer. Significant lesions are sharply delin-eated, densely opaque and persist forseveral minutes. Glandular lesions pro-duce more subtle changes {3159}.Fine or coarse stippling within aceto-white epithelium produced by the end-onview of finger-like intraepithelial capillar-ies is called punctation. A mosaic patternarises when the stromal ridges contain-ing the blood vessels subdivide theaceto-white epithelium into blocks ofvarying size and shape. Atypical tortu-ous vessels with bizarre irregular branch-es showing gross variation in calibre aresuggestive of early invasive disease.Cervical neoplasia fails to stain deeplywith iodine due to the lack of glycogen.Variations in quality and quantity of theabove atypical appearances help in dif-ferentiating cervical neoplasia from phys-iological, benign, infective, inflammatoryand reactive changes in the cervix.Colposcopy and histopathology arec o m p l e m e n t a ry to the diagnosis andmanagement of CIN.
Tumour spread and stagingCervical cancer is the only gynaecologi-cal cancer that is clinically staged byphysical examination, chest X-ray, intra-venous pyelogram, cystoscopy andp ro c t o s c o p y. The staging of cervicaltumours is by the TNM/FIGO classifica-tion {51,2976}.One-half of early invasive foci originatefrom the surface epithelium {2349}. Theuterine corpus is commonly involved asthe tumour expands. Ovarian metastasisis rare, occurring more frequently inbulky cancers and in adenocarcinomasas compared to squamous cell cancers{1914,1966}. Clinically undetected para-metrial spread is identified by histologi-cal examination in 31-63% of stage IBFig. 5.05 Worldwide distribution of HPV types in invasive carcinoma of the cervix. From G.M. Clifford et al. {528}.
Fig. 5.04 Mechanisms of human papillomavirus (HPV) carcinogenesis. LG = Low grade, HG = High grade,CIN = Cervical intraepithelial neoplasia, RB = Retinoblastoma gene.
264 Tumours of the uterine cervix
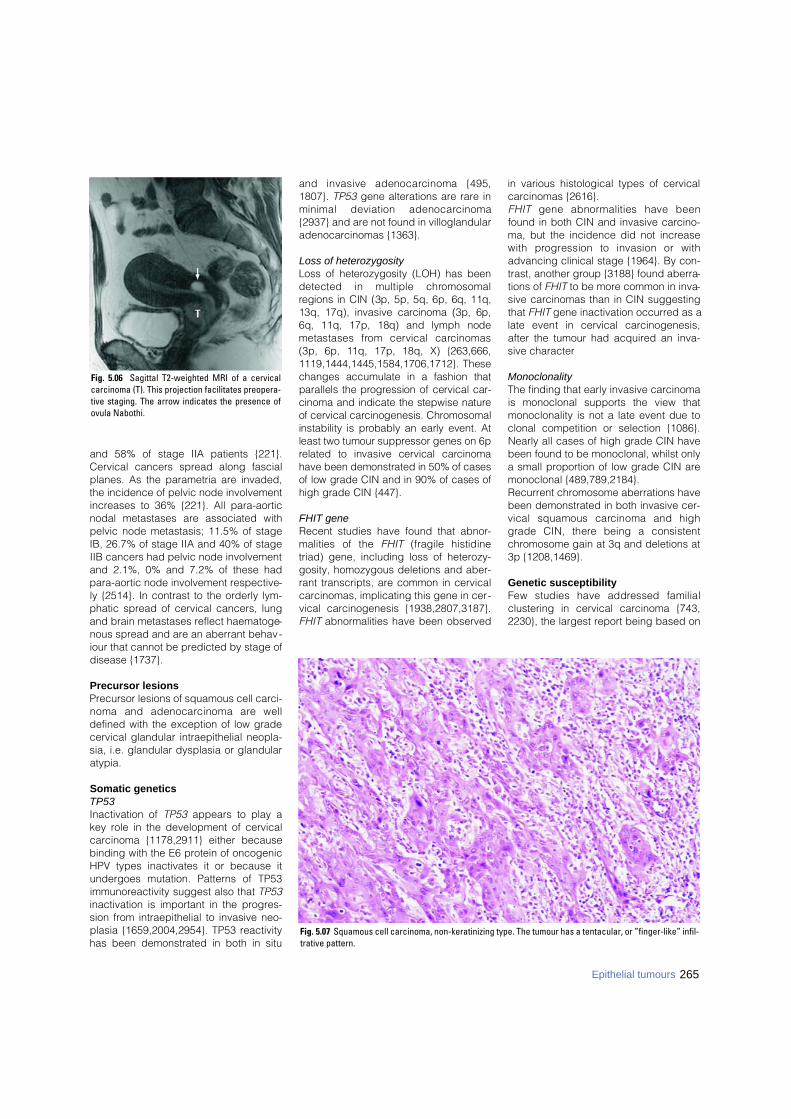
and 58% of stage IIA patients {221}.Cervical cancers spread along fascialplanes. As the parametria are invaded,the incidence of pelvic node involvementincreases to 36% {221}. All para-aorticnodal metastases are associated withpelvic node metastasis; 11.5% of stageIB, 26.7% of stage IIA and 40% of stageIIB cancers had pelvic node involvementand 2.1%, 0% and 7.2% of these hadpara-aortic node involvement respective-ly {2514}. In contrast to the orderly lym-phatic spread of cervical cancers, lungand brain metastases reflect haematoge-nous spread and are an aberrant behav-iour that cannot be predicted by stage ofdisease {1737}.
Precursor lesionsPrecursor lesions of squamous cell carci-noma and adenocarcinoma are welldefined with the exception of low gradecervical glandular intraepithelial neopla-sia, i.e. glandular dysplasia or glandularatypia.
Somatic geneticsTP53Inactivation of TP53 appears to play akey role in the development of cervicalcarcinoma {1178,2911} either becausebinding with the E6 protein of oncogenicHPV types inactivates it or because itundergoes mutation. Patterns of TP53immunoreactivity suggest also that TP53inactivation is important in the progres-sion from intraepithelial to invasive neo-plasia {1659,2004,2954}. TP53 reactivityhas been demonstrated in both in situ
and invasive adenocarcinoma {495,1807}. TP53 gene alterations are rare inminimal deviation adenocarc i n o m a{2937} and are not found in villoglandularadenocarcinomas {1363}.
Loss of heterozygosityLoss of heterozygosity (LOH) has beendetected in multiple chro m o s o m a lregions in CIN (3p, 5p, 5q, 6p, 6q, 11q,13q, 17q), invasive carcinoma (3p, 6p,6q, 11q, 17p, 18q) and lymph nodemetastases from cervical carc i n o m a s(3p, 6p, 11q, 17p, 18q, X) {263,666,1119,1444,1445,1584,1706,1712}. Thesechanges accumulate in a fashion thatparallels the pro g ression of cervical car-cinoma and indicate the stepwise natureof cervical carcinogenesis. Chro m o s o m a linstability is probably an early event. Atleast two tumour suppressor genes on 6prelated to invasive cervical carc i n o m ahave been demonstrated in 50% of casesof low grade CIN and in 90% of cases ofhigh grade CIN {447}.
FHIT geneRecent studies have found that abnor-malities of the F H I T (fragile histidinetriad) gene, including loss of heterozy-gosity, homozygous deletions and aber-rant transcripts, are common in cervicalcarcinomas, implicating this gene in cer-vical carcinogenesis {1938,2807,3187}.FHIT abnormalities have been observed
in various histological types of cervicalcarcinomas {2616}.F H I T gene abnormalities have beenfound in both CIN and invasive carcino-ma, but the incidence did not increasewith pro g ression to invasion or withadvancing clinical stage {1964}. By con-trast, another group {3188} found aberra-tions of FHIT to be more common in inva-sive carcinomas than in CIN suggestingthat FHIT gene inactivation occurred as alate event in cervical carc i n o g e n e s i s ,after the tumour had acquired an inva-sive character
MonoclonalityThe finding that early invasive carcinomais monoclonal supports the view thatmonoclonality is not a late event due toclonal competition or selection {1086}.Nearly all cases of high grade CIN havebeen found to be monoclonal, whilst onlya small proportion of low grade CIN aremonoclonal {489,789,2184}. Recurrent chromosome aberrations havebeen demonstrated in both invasive cer-vical squamous carcinoma and highgrade CIN, there being a consistentchromosome gain at 3q and deletions at3p {1208,1469}.
Genetic susceptibilityFew studies have addressed familialclustering in cervical carcinoma {743,2230}, the largest report being based on
265Epithelial tumours
Fig. 5.07 Squamous cell carcinoma, non-keratinizing type. The tumour has a tentacular, or ”finger-like” infil-trative pattern.
Fig. 5.06 Sagittal T2-weighted MRI of a cervicalcarcinoma (T). This projection facilitates preopera-tive staging. The arrow indicates the presence ofovula Nabothi.

266 Tumours of the uterine cervix
the Swedish Family-Cancer Database{1184}. The relative risk when the motheror a daughter was affected by cervicalcancer was 2. An aggregation of tobac-co-related cancers and cancers linkedwith HPV and immunosuppression wasfound in such families. Thus, familial pre-disposition for cervical cancer is likely toimply genes which modulate immuneresponse, e.g. human leukocyte antigen(HLA) haplotypes {2524} and/or sharedsexual or lifestyle factors in family mem-bers.
Prognosis and predictive factorsClinical criteriaThe clinical factors that influence prog-nosis in invasive cervical cancer are age,stage of disease, volume, lymphaticspread and vascular invasion {370,663,673,818,970,1506,2525,2672,2782}. In alarge series of cervical cancer patientstreated by radiation therapy, the frequen-cy of distant metastases (most frequentlyto the lung, abdominal cavity, liver andg a s t rointestinal tract) was shown toincrease with increasing stage of diseasefrom 3% in stage IA to 75% in stage IVA{818}. Radiotherapy and surgery produce similarresults for early invasive cancer (stages IBand IIA). More advanced lesions (IIB to IV)a re treated with a combination of extern a lradiotherapy and intracavitary radiation.Randomized phase III trials have shown asignificant overall and disease free sur-vival advantage for cisplatin-based thera-py given concurrently with radiotherapy{1063, 2908}. A significant benefit ofchemoradiation on both local (odds ratio0.61) and distant re c u r rence (odds ratio0.57) has been observed. The absolutebenefit with combined therapy on overallsurvival was 16%. Based on this evidence,c o n c u r rent chemotherapy with radiothera-
py is emerging as the new standard ofc a re for advanced cervical cancer.
Histopathological criteriaAmong histopathological variablesbased on histological findings and notincluded in the staging system for cervi-cal cancer {1532}, the grading oftumours does not seem to be a strongpredictive factor {3233}. In non-squa-mous cell carcinomas the only histologi-cal type of cervical cancer of prognosticsignificance is small cell carcinoma {68}.There is some evidence that women witha d e n o c a rcinoma and adenosquamouscarcinoma have a poorer prognosis thanthose with squamous cell carc i n o m aafter adjustment for stage {2314}.
Genetic predictive factors T P 5 3 . The prognostic value of TP53immunoreactivity in cervical carcinoma iscontroversial. Some have found no asso-ciation between p53 overexpression orthe presence of mutant p53 protein andclinical outcome {1267,2251}, whilst oth-ers have reported that TP53 expressionidentifies a subset of cervical carcino-mas with a poor prognosis {2969}.c-erbB. Frequent amplification of c-erbB-2 has been documented in cervical car-cinoma {2634}, and c-erbB-2 immunos-taining has been found to be significant-ly associated with poor survival and wasconsidered to be a marker of high riskdisease {1998}. Additionally, c-erbB-2immunostaining was found to be animportant prognostic factor for predictingtumour recurrence in cervical carcino-mas treated by radiotherapy {1967,2026}. On the other hand, overexpres-sion of c-erbB-3 oncoprotein in squa-mous, adenosquamous and adenocarci-nomas of the cervix showed no associa-tion with clinical outcome {1267}
c - m y c . c - m y c amplification has beendemonstrated in CIN and invasive cervi-cal carcinoma {110,666,2004} suggest-ing that it is important in early cervicalcarcinogenesis. Moreover, c-myc over-expression correlates with high risk HPV-positive neoplasia and with cellular prolif-eration {666}. It has been claimed that anincreased level of c-myc transcripts isstrongly indicative of a poor prognosis inearly stage cervical carcinoma {1314}but not in late stage disease {2823}.
DefinitionPrimary squamous epithelial tumours ofthe uterine cervix, either benign or malig-nant.
ICD-O codes Squamous cell carcinoma 8070/3
Keratinizing 8071/3Non-keratinizing 8072/3Basaloid 8083/3Verrucous 8051/3Warty 8051/3Papillary 8052/3Lymphoepithelioma-like 8082/3Squamotransitional cell 8120/3
Microinvasive squamous 8076/3cell carcinoma
Cervical intraepithelial neoplasia 3 8077/2squamous cell carcinoma in situ 8070/2Squamous papilloma 8 0 5 2 / 0
Squamous cell carcinoma
DefinitionAn invasive carcinoma composed ofsquamous cells of varying degrees of dif-ferentiation.
MacroscopyMacroscopically, squamous cell carcino-ma may be either predominantly exo-phytic, in which case it grows out fromthe surface, often as a papillary or poly-poid excrescence, or else it may bemainly endophytic, such that it infiltratesinto the surrounding structures withoutmuch surface growth.
Fig. 5.09 Non-keratinizing squamous cell carcinoma.There is a syncytium with anisokaryosis, irregulardistributed coarsely chromatin and nucleoli.
Fig. 5.08 Keratinizing squamous cell carcinoma.Note the partly spindle-shaped cells witheosinophilic cytoplasm and hyperchromatic nuclei.
Squamous tumours and precursors

267Epithelial tumours
HistopathologyThere have been few recent develop-ments in the histological diagnosis offrankly invasive squamous cell carcino-ma of the cervix {362,1201}. They vary intheir pattern of growth, cell type anddegree of differentiation. Most carcino-mas infiltrate as networks of anastomos-ing bands with intervening stroma andappear as irregular islands, sometimesrounded, but more usually angular andspiked. Often, particularly in smalltumours, CIN may be found on the sur-face and at the edge of the invasivetumour, and, occasionally, difficulty maybe encountered in distinguishingbetween invasive islands and CIN involv-ing crypts. Similarly, invasion cannot beexcluded when neoplastic squamousepithelium shows features of CIN 2 or 3but underlying stroma is not present.A number of histological grading sys-tems have been proposed that dependupon the type and degree of differentia-tion of the predominant cell {2794}. Asimpler classification is a modification ofthe four grades of Broders {350} andsubdivides the tumours into well differen-tiated (keratinizing), moderately differen-tiated and poorly differentiated types.Approximately 60% are moderately dif-ferentiated, and the remaining tumoursare evenly distributed between the welland poorly differentiated groups. A simple two-tiered classification is rec-ommended, keratinizing and non-kera-tinizing, to avoid nosological confusionwith small cell carcinoma, a term thatshould be reserved for tumours of neu-roendocrine type.The cervical stroma separating theislands of invasive carcinoma is usuallyinfiltrated by a variety of cell types, main-ly lymphocytes and plasma cells. Amarkedly eosinophilic stromal response{262} or a foreign body type giant cellreaction is occasionally seen.A variety of histological types of squa-mous cell carcinoma have beendescribed.
Keratinizing These tumours contain keratin pearlscomposed of circular whorls of squa-mous cells with central nests of keratin.Intercellular bridges, keratohyaline gran-ules and cytoplasmic keratinization areusually observed. The nuclei are usuallylarge and hyperchromatic with coarsechromatin. Mitotic figures are not fre-
quent and are usually seen in the less-well differentiated cells at the peripheryof the invasive masses. In cytological preparations the cells usu-ally have bizarre shapes with mostlyeosinophilic cytoplasm and large, irregu-l a r, hyperc h romatic nuclei. Necro t i cdebris is present.
Non-keratinizingThese tumours are composed of gener-ally recognizable polygonal squamouscells that may have individual cell kera-tinization and intercellular bridges, butkeratin pearls are absent. Cellular andnuclear pleomorphism is more obviousthan in the well differentiated tumours,and mitotic figures are usually numerous. In cytological preparations the cells aresolitary or arranged in syncytia and showanisokaryosis. The nuclei are relativelylarge with unevenly distributed, coarselygranular chromatin and may have irregu-lar nucleoli
BasaloidBasaloid squamous cell carcinoma iscomposed of nests of immature, basaltype squamous cells with scanty cyto-plasm that resemble closely the cells ofsquamous carcinoma in situ of thecervix. Some keratinization may be evi-dent in the centres of the nests, but ker-atin pearls are rarely present. In the vulvathis tumour has been associated withHPV infections, predominantly type 16{1541,2936}.This underrecognized variant of squa-mous cell carcinoma is an aggressivetumour with basaloid features {1057}.This tumour along with adenoid cysticcarcinoma is at one end of the spectrumof basaloid tumours of the cervix. At theopposite end are low grade lesions suchas adenoid basal carcinoma. To avoidconfusion in the diagnosis of a cervicaltumour with basaloid features, the term"basaloid carcinoma" should be avoided{1057}.
Verrucous Verrucous carcinoma is a highly diff e re n-tiated squamous cell carcinoma that hasa hyperkeratotic, undulating, warty sur-face and invades the underlying stro m ain the form of bulbous pegs with a push-ing bord e r. The tumour cells have abun-dant cytoplasm, and their nuclei showminimal atypia. Features of HPV infectiona re not evident. Verrucous carc i n o m a s
have a tendency to recur locally afterexcision but do not metastasize. Theya re distinguished from condyloma bytheir broad papillae that lack fibro v a s c u-lar cores and the absence of koilocyto-sis. Verrucous carcinoma is distin-guished from the more common types ofsquamous cell carcinoma in that itshows no more than minimal nucleara t y p i a .
Warty This lesion is defined as a squamous cellcarcinoma with a warty surface and cel-lular features of HPV infection {720,1541,2936}. High risk HPV-DNA is typi-cally detected {2936}. It is also referredto as condylomatous squamous cell car-cinoma.
PapillaryThis is a tumour in which thin or bro a dpapillae with connective tissue stro m aa re covered by epithelium showing thef e a t u res of CIN. Whilst a superf i c i a lbiopsy may not reveal evidence of inva-sion, the underlying tumour is usually atypical squamous cell carc i n o m a{345,2333}. Such tumours are positivefor HPV type 16. Papillary squamouscell carcinoma differs from warty squa-mous carcinoma by the inconspicuouskeratinization and lack of cellular fea-t u res of HPV infection and from transi-tional cell carcinoma by its squamouscell diff e rentiation {345}.
Lymphoepithelioma-likeH i s t o l o g i c a l l y, lymphoepithelioma-likec a rcinoma is strikingly similar to then a s o p h a ryngeal tumour of the samename. It is composed of poorly definedislands of undiff e rentiated cells in abackground intensely infiltrated by lym-
Fig. 5.10 Schematic representation of the FIGO definition of stage 1A carcinoma of the cervix. A: Depth of invasion no greater than 5 mm; B: Horizontal spread 7 mm or less.
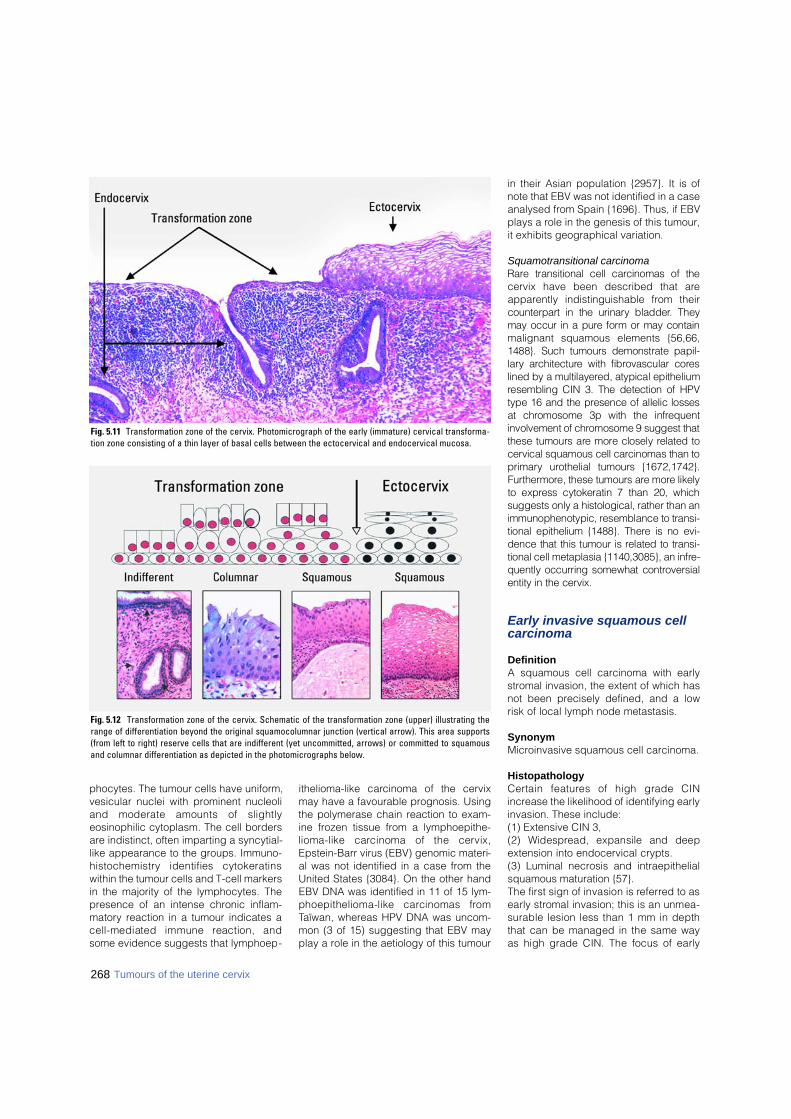
268 Tumours of the uterine cervix
phocytes. The tumour cells have uniform,vesicular nuclei with prominent nucleoliand moderate amounts of slightlyeosinophilic cytoplasm. The cell bordersare indistinct, often imparting a syncytial-like appearance to the groups. Immuno-h i s t o c h e m i s t ry identifies cytokeratinswithin the tumour cells and T-cell markersin the majority of the lymphocytes. Thepresence of an intense chronic inflam-matory reaction in a tumour indicates acell-mediated immune reaction, andsome evidence suggests that lymphoep-
ithelioma-like carcinoma of the cervixmay have a favourable prognosis. Usingthe polymerase chain reaction to exam-ine frozen tissue from a lymphoepithe-lioma-like carcinoma of the cervix,Epstein-Barr virus (EBV) genomic materi-al was not identified in a case from theUnited States {3084}. On the other handEBV DNA was identified in 11 of 15 lym-phoepithelioma-like carcinomas from Taïwan, whereas HPV DNA was uncom-mon (3 of 15) suggesting that EBV mayplay a role in the aetiology of this tumour
in their Asian population {2957}. It is ofnote that EBV was not identified in a caseanalysed from Spain {1696}. Thus, if EBVplays a role in the genesis of this tumour,it exhibits geographical variation.
Squamotransitional carcinomaR a re transitional cell carcinomas of thecervix have been described that areapparently indistinguishable from theirc o u n t e r p a rt in the urinary bladder. Theymay occur in a pure form or may containmalignant squamous elements {56,66,1488}. Such tumours demonstrate papil-l a ry arc h i t e c t u re with fibrovascular core slined by a multilayered, atypical epitheliumresembling CIN 3. The detection of HPVtype 16 and the presence of allelic lossesat chromosome 3p with the infre q u e n tinvolvement of chromosome 9 suggest thatthese tumours are more closely related tocervical squamous cell carcinomas than top r i m a ry urothelial tumours {1672,1742}.F u rt h e rm o re, these tumours are more likelyto express cytokeratin 7 than 20, whichsuggests only a histological, rather than animmunophenotypic, resemblance to transi-tional epithelium {1488}. There is no evi-dence that this tumour is related to transi-tional cell metaplasia {1140,3085}, an infre-quently occurring somewhat contro v e r s i a lentity in the cervix.
Early invasive squamous cellcarcinoma
DefinitionA squamous cell carcinoma with earlystromal invasion, the extent of which hasnot been precisely defined, and a lowrisk of local lymph node metastasis.
SynonymMicroinvasive squamous cell carcinoma.
HistopathologyC e rtain features of high grade CINincrease the likelihood of identifying earlyinvasion. These include: (1) Extensive CIN 3, (2) Widespread, expansile and deepextension into endocervical crypts. (3) Luminal necrosis and intraepithelialsquamous maturation {57}. The first sign of invasion is re f e r red to asearly stromal invasion; this is an unmea-surable lesion less than 1 mm in depththat can be managed in the same wayas high grade CIN. The focus of early
Fig. 5.11 Transformation zone of the cervix. Photomicrograph of the early (immature) cervical transforma-tion zone consisting of a thin layer of basal cells between the ectocervical and endocervical mucosa.
Fig. 5.12 Transformation zone of the cervix. Schematic of the transformation zone (upper) illustrating therange of differentiation beyond the original squamocolumnar junction (vertical arrow). This area supports(from left to right) reserve cells that are indifferent (yet uncommitted, arrows) or committed to squamousand columnar differentiation as depicted in the photomicrographs below.

269Epithelial tumours
s t romal invasion often appears to bebetter diff e rentiated than the overlyingCIN. Early stromal invasion is encom-passed in the term microinvasive carc i-noma. The criteria for the diagnosis of microin-vasive carcinoma were historically basedon the depth of invasion, and theascribed upper limit has varied in the lit-erature from 3 to 5 mm. Microinvasivecarcinoma now equates most closely toFIGO stage IA, the definition of whichincludes both the depth and horizontaldimension of the tumour. The currentFIGO staging is controversial because itdoes not recognize early stromal inva-sion as a separate entity {371}. Whethermicroinvasive carcinoma should includeFIGO Stage IA2 because there is a sig-nificantly increased risk of local lymphnode metastasis between 3 and 5 mmdepth of invasion has also been ques-tioned. Pooled data indicate that a maxi-mum depth of invasion of 3 mm or less isassociated with a risk of lymph nodemetastasis of <1% and a risk of an inva-sive recurrence of 0.9%. On the otherhand, invasion of 3.1-5.0 mm is associat-ed with an overall risk of lymph nodemetastases of 2% and a recurrence rateof 4% {2138}. Microinvasive squamouscell carcinoma is usually associated withstromal oedema and a stromal desmo-plastic and lymphocytic response, fea-tures that aid in its distinction from cryptinvolvement by CIN. Immunohistochemi-cal stains for CD31 and CD34 may aid inthe recognition of lymphatic vascularspace involvement.Preclinical invasive carcinomas of thecervix with dimensions greater thanthose acceptable as stage IA carcinomashould be designated by the histopathol-ogist simply as stage IB carcinomas.
" F i n g e r-like" or "confluent" patterns ofstromal invasion are of questionable clin-ical significance and probably are areflection of a greater depth of stromalinvasion.
Cervical intraepithelial neoplasia
DefinitionThe spectrum of CIN representing theprecursor lesions of cervical squamouscell carcinoma {2368}.
SynonymsD y s p l a s i a / c a rcinoma-in-situ, squamousintraepithelial lesion.
EpidemiologyThe risk of CIN is closely linked to thenumber of sexual partners and to HPVexposure. It is highest in early reproduc-tive life {1160}. HPV is detected in asmany as 39% of adolescents in a singles c reening visit {2451}, and 20% ofwomen under age 19 in a sexually trans-mitted disease clinic developed CIN 2 or3 {1513}. The strong associationbetween HPV 16 and high grade CINcoupled with follow-up studies suggeststhat infections by this virus induce a highgrade lesion over a relatively short periodof time {586,1513,1699}. The risk of CINdrops substantially in the fourth and fifthdecades, coinciding with a sharp reduc-tion in frequency of HPV attributed to thedevelopment of immunity to HPV and
elimination of the virus from the genitaltract in most women. Other factors influ-encing risk include immunological, suchas HIV infection, and other host factors,including coincident cervical infectionsand HLA status.
AetiologyAt puberty there is a change in theanatomical relationships of the lower partof the cervix composed of squamousepithelium, an original squamocolumnarjunction and endocervical columnarepithelium. There is eversion of the colum-nar epithelium, which undergoes squa-mous metaplasia through a sequence ofreserve cell hyperplasia, immature squa-mous metaplasia and mature squamousmetaplasia with the formation of a newsquamocolumnar junction. These histolog-ical changes are entirely physiological.H o w e v e r, it is this epithelium of the cervicalt r a n s f o rmation zone that is part i c u l a r l ysusceptible to oncogenic stimuli. In the last 25 years “flat” and exophyticcondylomata of the cervix and CIN havebeen linked by an association with HPVs,many of them weakly or strongly associ-ated with cancer (intermediate and highrisk HPVs) {586,737,1014,1841,2305}.Although some HPVs are not associatedwith cervical cancer (low risk HPVs), themajority are associated with high riskHPVs {1699}. High risk HPV infection mayp resent histologically as CIN 1, althoughc e rtain infections, such as HPV type 16,
Table 5.02Classification of HPV-associated intraepithelial lesions of the cervix.
Exophytic condyloma Low risk LGSIL
Flat condyloma Low and high risk LGSIL
CIN 2 High risk High grade CIN Moderate dysplasia HGSIL
Term HPV risk category Comparison of classification systems
Two-tiered CIN Dysplasia/CIS SIL
Squamous papilloma Low risk LGSIL
CIN 3 High risk High grade CIN Severe dysplasia/CIS HGSIL
CIN 1 Low and high risk Low grade CIN Mild dysplasia LGSIL
CIN = Cervical intraepithelial neoplasia LG = Low grade SIL = Squamous intraepithelial lesion HG = High grade CIS = Carcinoma in situ
Fig. 5.13 Early squamous cell carcinoma of thecervix. Early stromal invasion is indicated by a budof more mature squamous cells extending from afocus of in situ carcinoma.
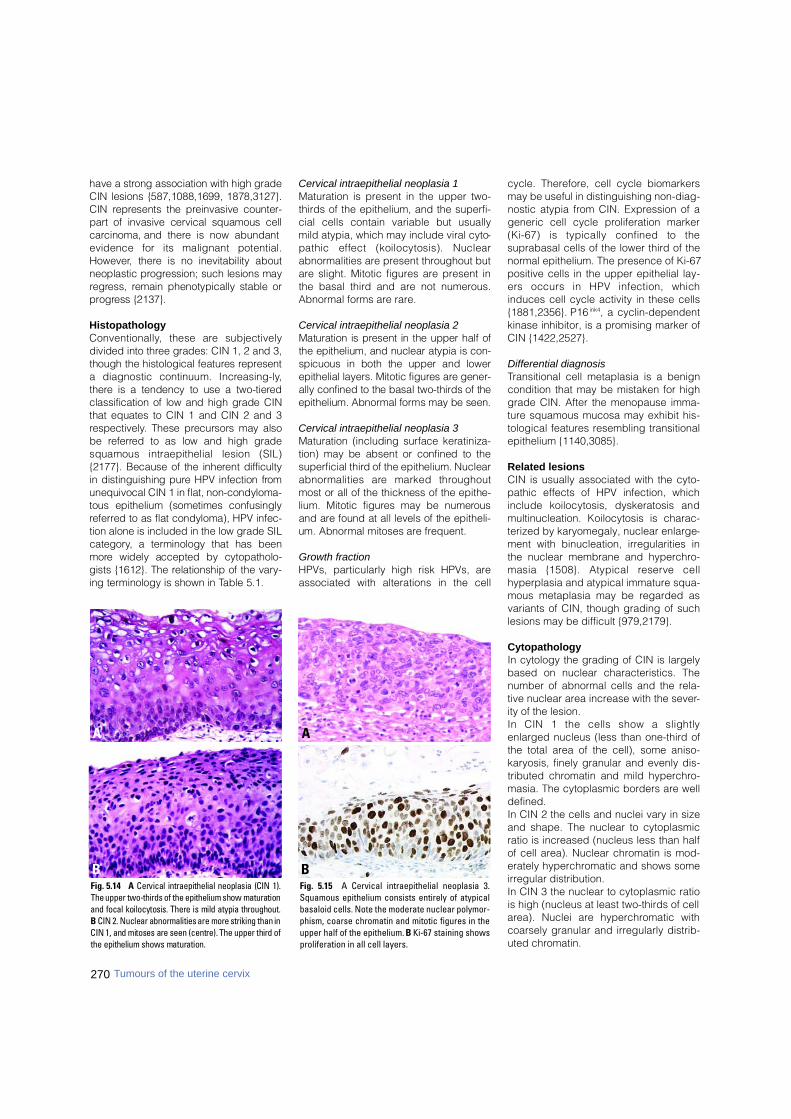
270 Tumours of the uterine cervix
have a strong association with high gradeCIN lesions {587,1088,1699, 1878,3127}.CIN re p resents the preinvasive counter-p a rt of invasive cervical squamous cellc a rcinoma, and there is now abundantevidence for its malignant potential.H o w e v e r, there is no inevitability aboutneoplastic pro g ression; such lesions mayre g ress, remain phenotypically stable orp ro g ress {2137}.
Histopathology C o n v e n t i o n a l l y, these are subjectivelydivided into three grades: CIN 1, 2 and 3,though the histological features re p re s e n ta diagnostic continuum. Incre a s i n g - l y,t h e re is a tendency to use a two-tiere dclassification of low and high grade CINthat equates to CIN 1 and CIN 2 and 3re s p e c t i v e l y. These precursors may alsobe re f e r red to as low and high gradesquamous intraepithelial lesion (SIL){2177}. Because of the inherent diff i c u l t yin distinguishing pure HPV infection fro munequivocal CIN 1 in flat, non-condyloma-tous epithelium (sometimes confusinglyre f e r red to as flat condyloma), HPV infec-tion alone is included in the low grade SILc a t e g o ry, a terminology that has beenm o re widely accepted by cytopatholo-gists {1612}. The relationship of the vary-ing terminology is shown in Table 5.1.
Cervical intraepithelial neoplasia 1 Maturation is present in the upper two-thirds of the epithelium, and the superfi-cial cells contain variable but usuallymild atypia, which may include viral cyto-pathic effect (koilocytosis). Nuclearabnormalities are present throughout butare slight. Mitotic figures are present inthe basal third and are not numerous.Abnormal forms are rare.
Cervical intraepithelial neoplasia 2 Maturation is present in the upper half ofthe epithelium, and nuclear atypia is con-spicuous in both the upper and lowerepithelial layers. Mitotic figures are gener-ally confined to the basal two-thirds of theepithelium. Abnormal forms may be seen.
Cervical intraepithelial neoplasia 3 Maturation (including surface keratiniza-tion) may be absent or confined to thes u p e rficial third of the epithelium. Nucleara b n o rmalities are marked thro u g h o u tmost or all of the thickness of the epithe-lium. Mitotic figures may be numero u sand are found at all levels of the epitheli-um. Abnormal mitoses are fre q u e n t .
Growth fractionHPVs, particularly high risk HPVs, areassociated with alterations in the cell
cycle. Therefore, cell cycle biomarkersmay be useful in distinguishing non-diag-nostic atypia from CIN. Expression of ageneric cell cycle proliferation marker(Ki-67) is typically confined to thesuprabasal cells of the lower third of thenormal epithelium. The presence of Ki-67positive cells in the upper epithelial lay-ers occurs in HPV infection, whichinduces cell cycle activity in these cells{1881,2356}. P16 ink4, a cyclin-dependentkinase inhibitor, is a promising marker ofCIN {1422,2527}.
Differential diagnosisTransitional cell metaplasia is a benigncondition that may be mistaken for highgrade CIN. After the menopause imma-ture squamous mucosa may exhibit his-tological features resembling transitionalepithelium {1140,3085}.
Related lesionsCIN is usually associated with the cyto-pathic effects of HPV infection, whichinclude koilocytosis, dyskeratosis andmultinucleation. Koilocytosis is charac-terized by karyomegaly, nuclear enlarge-ment with binucleation, irregularities inthe nuclear membrane and hyperchro-masia {1508}. Atypical reserve cellhyperplasia and atypical immature squa-mous metaplasia may be regarded asvariants of CIN, though grading of suchlesions may be difficult {979,2179}.
CytopathologyIn cytology the grading of CIN is largelybased on nuclear characteristics. Thenumber of abnormal cells and the rela-tive nuclear area increase with the sever-ity of the lesion. In CIN 1 the cells show a slightlyenlarged nucleus (less than one-third ofthe total area of the cell), some aniso-karyosis, finely granular and evenly dis-tributed chromatin and mild hyperchro-masia. The cytoplasmic borders are welldefined.In CIN 2 the cells and nuclei vary in sizeand shape. The nuclear to cytoplasmicratio is increased (nucleus less than halfof cell area). Nuclear chromatin is mod-erately hyperchromatic and shows someirregular distribution.In CIN 3 the nuclear to cytoplasmic ratiois high (nucleus at least two-thirds of cellarea). Nuclei are hyperchromatic withcoarsely granular and irregularly distrib-uted chromatin.
Fig. 5.15 A Cervical intraepithelial neoplasia 3.Squamous epithelium consists entirely of atypicalbasaloid cells. Note the moderate nuclear polymor-phism, coarse chromatin and mitotic figures in theupper half of the epithelium. B Ki-67 staining showsproliferation in all cell layers.
A
BFig. 5.14 A Cervical intraepithelial neoplasia (CIN 1).The upper two-thirds of the epithelium show maturationand focal koilocytosis. There is mild atypia throughout.B CIN 2. Nuclear abnormalities are more striking than inCIN 1, and mitoses are seen (centre). The upper third ofthe epithelium shows maturation.
A
B
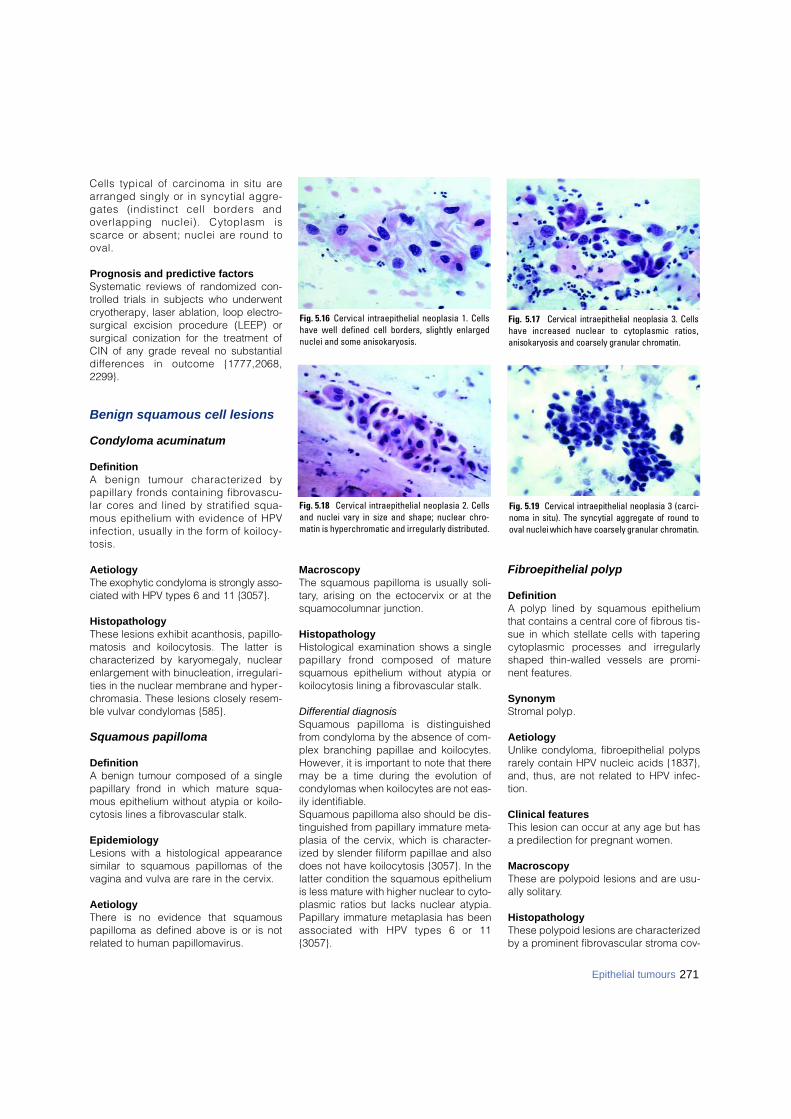
271Epithelial tumours
Cells typical of carcinoma in situ arearranged singly or in syncytial aggre-gates (indistinct cell borders andoverlapping nuclei). Cytoplasm iss c a rce or absent; nuclei are round too v a l .
Prognosis and predictive factorsSystematic reviews of randomized con-trolled trials in subjects who underwentcryotherapy, laser ablation, loop electro-surgical excision procedure (LEEP) orsurgical conization for the treatment ofCIN of any grade reveal no substantiald i ff e rences in outcome {1777,2068,2299}.
Benign squamous cell lesions
Condyloma acuminatum
DefinitionA benign tumour characterized byp a p i l l a ry fronds containing fibro v a s c u-lar cores and lined by stratified squa-mous epithelium with evidence of HPVinfection, usually in the form of koilocy-t o s i s .
AetiologyThe exophytic condyloma is strongly asso-ciated with HPV types 6 and 11 {3057}.
HistopathologyThese lesions exhibit acanthosis, papillo-matosis and koilocytosis. The latter ischaracterized by karyomegaly, nuclearenlargement with binucleation, irregulari-ties in the nuclear membrane and hyper-chromasia. These lesions closely resem-ble vulvar condylomas {585}.
Squamous papilloma
DefinitionA benign tumour composed of a singlepapillary frond in which mature squa-mous epithelium without atypia or koilo-cytosis lines a fibrovascular stalk.
EpidemiologyLesions with a histological appearancesimilar to squamous papillomas of thevagina and vulva are rare in the cervix.
AetiologyThere is no evidence that squamouspapilloma as defined above is or is notrelated to human papillomavirus.
MacroscopyThe squamous papilloma is usually soli-tary, arising on the ectocervix or at thesquamocolumnar junction.
HistopathologyHistological examination shows a singlep a p i l l a ry frond composed of maturesquamous epithelium without atypia orkoilocytosis lining a fibrovascular stalk.
Differential diagnosisSquamous papilloma is distinguishedfrom condyloma by the absence of com-plex branching papillae and koilocytes.However, it is important to note that theremay be a time during the evolution ofcondylomas when koilocytes are not eas-ily identifiable. Squamous papilloma also should be dis-tinguished from papillary immature meta-plasia of the cervix, which is character-ized by slender filiform papillae and alsodoes not have koilocytosis {3057}. In thelatter condition the squamous epitheliumis less mature with higher nuclear to cyto-plasmic ratios but lacks nuclear atypia.Papillary immature metaplasia has beenassociated with HPV types 6 or 11{3057}.
Fibroepithelial polyp
DefinitionA polyp lined by squamous epitheliumthat contains a central core of fibrous tis-sue in which stellate cells with taperingcytoplasmic processes and irregularlyshaped thin-walled vessels are promi-nent features.
SynonymStromal polyp.
AetiologyUnlike condyloma, fibroepithelial polypsrarely contain HPV nucleic acids {1837},and, thus, are not related to HPV infec-tion.
Clinical featuresThis lesion can occur at any age but hasa predilection for pregnant women.
MacroscopyThese are polypoid lesions and are usu-ally solitary.
HistopathologyThese polypoid lesions are characterizedby a prominent fibrovascular stroma cov-
Fig. 5.16 Cervical intraepithelial neoplasia 1. Cellshave well defined cell borders, slightly enlargednuclei and some anisokaryosis.
Fig. 5.18 Cervical intraepithelial neoplasia 2. Cellsand nuclei vary in size and shape; nuclear chro-matin is hyperchromatic and irregularly distributed.
Fig. 5.17 Cervical intraepithelial neoplasia 3. Cellshave increased nuclear to cytoplasmic ratios,anisokaryosis and coarsely granular chromatin.
Fig. 5.19 Cervical intraepithelial neoplasia 3 (carci-noma in situ). The syncytial aggregate of round tooval nuclei which have coarsely granular chromatin.

e red by squamous epithelium {380}.Unlike squamous papilloma, they do notshow acanthosis or a papillary architec-ture. Bizarre stromal cells, marked hyper-cellularity and elevated mitotic countsincluding atypical forms have beendescribed that can lead to an erroneousdiagnosis of sarcoma {2067}.
ICD-O codesAdenocarcinoma, NOS 8140/3Mucinous adenocarcinoma 8480/3
Endocervical 8482/3Intestinal 8144/3Signet-ring cell 8490/3Minimal deviation 8480/3Villoglandular 8262/3
Endometrioid adenocarcinoma 8380/3Clear cell adenocarcinoma 8310/3Serous adenocarcinoma 8441/3 Mesonephric adenocarcinoma 9110/3Early invasive adenocarcinoma 8140/3Adenocarcinoma in situ 8140/2
Adenocarcinoma
DefinitionA carcinoma that shows glandular differ-entiation.
Clinical featuresAbout one-half of all adenocarc i n o m a sa re exophytic, polypoid or papillarymasses. Others are nodular with dif-fuse enlargement or ulceration of thecervix. Deep infiltration of the wall pro-duces a barrel-shaped cervix.A p p roximately 15% of patients have novisible lesion.
HistopathologyImmunohistochemistry may be useful todistinguish between benign and malig-nant conditions of the cervix, to discrimi-nate between the various subtypes andto separate primary endocervical fromp r i m a ry endometrial tumours. Thetumour that is estrogen receptor positive,vimentin positive and carcinoembryonicantigen negative is almost certainly ofendometrial origin, whilst an endocervi-cal source is very likely for the tumourthat is estrogen receptor negative,vimentin negative and carcinoembryonicantigen positive {424,1822}. A moderateto high Ki-67 proliferation index alsopoints towards endocervical neoplasia{495}. It is equally important to recognizethat none of these stains are needed inthe majority of cases, where the clinicalevidence and history are entirely ade-quate. Carcinoembryonic antigen is usu-ally negative in benign mimics, such asm i c roglandular hyperplasia {2780}. Incontrast to normal endocervical epitheli-um, some of the cells of a minimal devia-tion adenocarcinoma are reactive forserotonin and gastrointestinal tract-pan-creatic peptide hormones and uniformlylack immunoreactivity for estrogen andprogesterone receptors and CA125.
Mucinous adenocarcinoma
DefinitionAn adenocarcinoma in which at leastsome of the cells contain a moderate tolarge amount of intracytoplasmic mucin.
Endocervical The endocervical type accounts for 70%of cervical adenocarcinomas, and thetumour cells resemble those of the endo-cervix. Most tumours are well to moder-ately differentiated. The glandular ele-
ments are arranged in a complex pat-tern. Papillae may project into the glandlumens and from the surface. At times acribriform arrangement is observed. Am i c roglandular pattern re s e m b l i n gmicroglandular hyperplasia of the cervix{3224} and a microcystic variant arerarely seen {2856}. The stroma may bedesmoplastic. The cells are typicallystratified with basal nuclei and abundantpale granular cytoplasm that stains posi -tively for mucin. They show considerablenuclear atypia with variation in nuclearsize, coarsely clumped chromatin andprominent nucleoli. Mitoses are usuallynumerous. Large amounts of mucin maybe found in the stroma forming mucinlakes or pools in the so-called colloidcarcinoma {1646,2975}. In poorly differ-entiated tumours the cells contain lesscytoplasm but usually still form recogniz-able glandular structures. Co-existentCIN occurs in up to 40% of cases {1739},and adenocarcinoma in situ is also com-mon. Synchronous mucinous tumoursmay be found elsewhere in the femalegenital tract {1392,3219}.In cytological preparations the cells arearranged in crowded cell aggregateswith overlapping nuclei. Gland openings,rosettes, strips with palisading and pseu-dostratification and cell balls may beseen. The cytoplasm is vacuolated. Thenuclei are round, oval or "cigar" shapedand vary in size. The nuclear chromatin iscoarse and unevenly distributed withclearing, and nucleoli are present.
Intestinal variant These tumours resemble adenocarcino-ma of the large intestine. Intestinal-typechange may be found diffusely or onlyfocally within a mucinous tumour. Theyfrequently contain goblet cells and lesscommonly endocrine and Paneth cells.
B CAFig. 5.20 Adenocarcinoma. A A large, polypoid, exophytic tumour arises from the cervix with focal cystic change and necrosis. B A cribriform pattern along with otherfeatures may indicate an invasive, rather than an in situ, neoplastic glandular process. C Endocervical variant. Atypical cells with enlarged nuclei, coarsely granular clearedchromatin and nucleoli form a gland opening.
272 Tumours of the uterine cervix
Glandular tumours and precursors
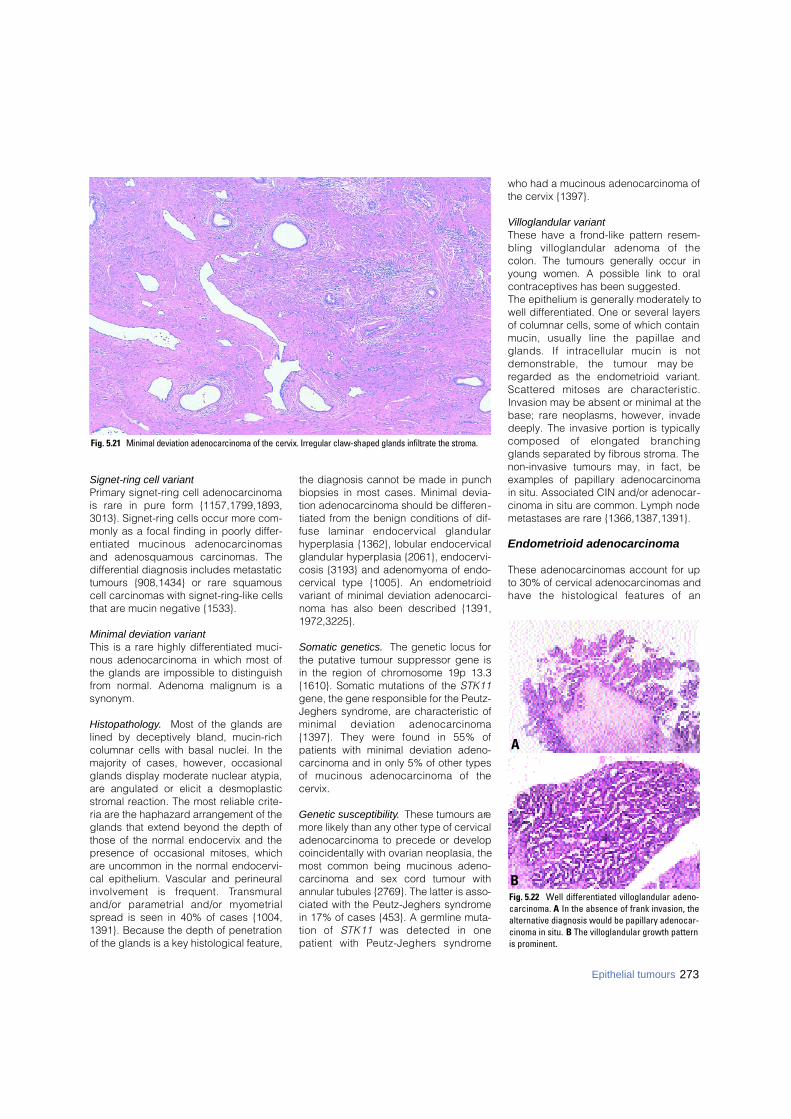
Signet-ring cell variant Primary signet-ring cell adenocarcinomais rare in pure form {1157,1799,1893,3013}. Signet-ring cells occur more com-monly as a focal finding in poorly differ-entiated mucinous adenocarc i n o m a sand adenosquamous carcinomas. Thedifferential diagnosis includes metastatictumours {908,1434} or rare squamouscell carcinomas with signet-ring-like cellsthat are mucin negative {1533}.
Minimal deviation variant This is a rare highly differentiated muci-nous adenocarcinoma in which most ofthe glands are impossible to distinguishfrom normal. Adenoma malignum is asynonym.
Histopathology. Most of the glands arelined by deceptively bland, mucin-richcolumnar cells with basal nuclei. In themajority of cases, however, occasionalglands display moderate nuclear atypia,are angulated or elicit a desmoplasticstromal reaction. The most reliable crite-ria are the haphazard arrangement of theglands that extend beyond the depth ofthose of the normal endocervix and thepresence of occasional mitoses, whichare uncommon in the normal endocervi-cal epithelium. Vascular and perineuralinvolvement is frequent. Tr a n s m u r a land/or parametrial and/or myometrialspread is seen in 40% of cases {1004,1391}. Because the depth of penetrationof the glands is a key histological feature,
the diagnosis cannot be made in punchbiopsies in most cases. Minimal devia-tion adenocarcinoma should be differen-tiated from the benign conditions of dif-fuse laminar endocervical glandularhyperplasia {1362}, lobular endocervicalglandular hyperplasia {2061}, endocervi-cosis {3193} and adenomyoma of endo-cervical type {1005}. An endometrioidvariant of minimal deviation adenocarci-noma has also been described {1391,1972,3225}.
Somatic genetics. The genetic locus forthe putative tumour suppressor gene isin the region of chromosome 19p 13.3{1610}. Somatic mutations of the STK11gene, the gene responsible for the Peutz-Jeghers syndrome, are characteristic ofminimal deviation adenocarc i n o m a{1397}. They were found in 55% ofpatients with minimal deviation adeno-carcinoma and in only 5% of other typesof mucinous adenocarcinoma of thecervix.
Genetic susceptibility. These tumours aremore likely than any other type of cervicaladenocarcinoma to precede or developcoincidentally with ovarian neoplasia, themost common being mucinous adeno-carcinoma and sex cord tumour withannular tubules {2769}. The latter is asso-ciated with the Peutz-Jeghers syndromein 17% of cases {453}. A germline muta-tion of STK11 was detected in onepatient with Peutz-Jeghers syndro m e
who had a mucinous adenocarcinoma ofthe cervix {1397}.
Villoglandular variant These have a frond-like pattern resem-bling villoglandular adenoma of thecolon. The tumours generally occur inyoung women. A possible link to oralcontraceptives has been suggested.The epithelium is generally moderately towell differentiated. One or several layersof columnar cells, some of which containmucin, usually line the papillae andglands. If intracellular mucin is notdemonstrable, the tumour may beregarded as the endometrioid variant.S c a t t e red mitoses are characteristic.Invasion may be absent or minimal at thebase; rare neoplasms, however, invadedeeply. The invasive portion is typicallycomposed of elongated branchingglands separated by fibrous stroma. Thenon-invasive tumours may, in fact, beexamples of papillary adenocarcinomain situ. Associated CIN and/or adenocar-cinoma in situ are common. Lymph nodemetastases are rare {1366,1387,1391}.
Endometrioid adenocarcinoma
These adenocarcinomas account for upto 30% of cervical adenocarcinomas andhave the histological features of an
Fig. 5.22 Well differentiated villoglandular adeno-carcinoma. A In the absence of frank invasion, thealternative diagnosis would be papillary adenocar-cinoma in situ. B The villoglandular growth patternis prominent.
A
B
Fig. 5.21 Minimal deviation adenocarcinoma of the cervix. Irregular claw-shaped glands infiltrate the stroma.
273Epithelial tumours
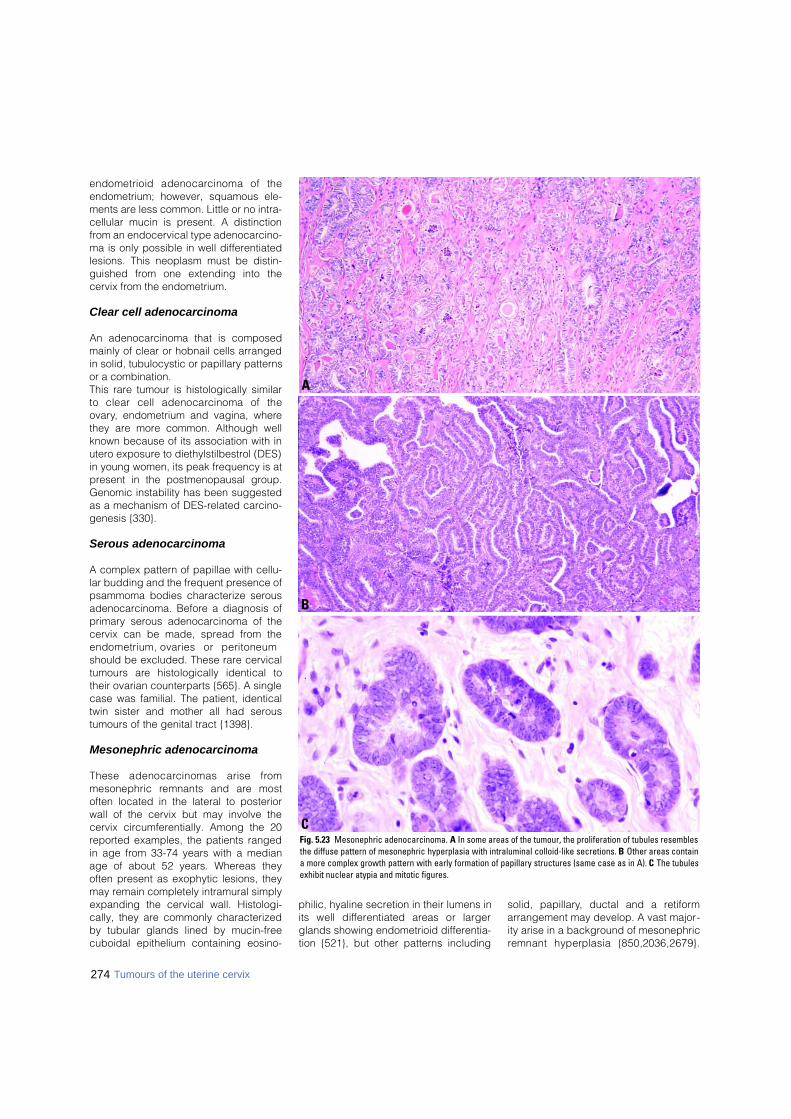
274 Tumours of the uterine cervix
endometrioid adenocarcinoma of theendometrium; however, squamous ele-ments are less common. Little or no intra-cellular mucin is present. A distinctionfrom an endocervical type adenocarcino-ma is only possible in well differentiatedlesions. This neoplasm must be distin-guished from one extending into thecervix from the endometrium.
Clear cell adenocarcinoma
An adenocarcinoma that is composedmainly of clear or hobnail cells arrangedin solid, tubulocystic or papillary patternsor a combination. This rare tumour is histologically similarto clear cell adenocarcinoma of theovary, endometrium and vagina, wherethey are more common. Although wellknown because of its association with inutero exposure to diethylstilbestrol (DES)in young women, its peak frequency is atpresent in the postmenopausal group.Genomic instability has been suggestedas a mechanism of DES-related carcino-genesis {330}.
Serous adenocarcinoma
A complex pattern of papillae with cellu-lar budding and the frequent presence ofpsammoma bodies characterize serousadenocarcinoma. Before a diagnosis ofprimary serous adenocarcinoma of thecervix can be made, spread from theendometrium, ovaries or peritoneumshould be excluded. These rare cervicaltumours are histologically identical totheir ovarian counterparts {565}. A singlecase was familial. The patient, identicaltwin sister and mother all had seroustumours of the genital tract {1398}.
Mesonephric adenocarcinoma
These adenocarcinomas arise fro mmesonephric remnants and are mostoften located in the lateral to posteriorwall of the cervix but may involve thecervix circumferentially. Among the 20reported examples, the patients rangedin age from 33-74 years with a medianage of about 52 years. Whereas theyoften present as exophytic lesions, theymay remain completely intramural simplyexpanding the cervical wall. Histologi-cally, they are commonly characterizedby tubular glands lined by mucin-freecuboidal epithelium containing eosino-
philic, hyaline secretion in their lumens inits well diff e rentiated areas or largerglands showing endometrioid differentia-tion {521}, but other patterns including
solid, papillary, ductal and a retiformarrangement may develop. A vast major-ity arise in a background of mesonephricremnant hyperplasia {850,2036,2679}.
Fig. 5.23 Mesonephric adenocarcinoma. A In some areas of the tumour, the proliferation of tubules resemblesthe diffuse pattern of mesonephric hyperplasia with intraluminal colloid-like secretions. B Other areas containa more complex growth pattern with early formation of papillary structures (same case as in A). C The tubulesexhibit nuclear atypia and mitotic figures.
C
B
A
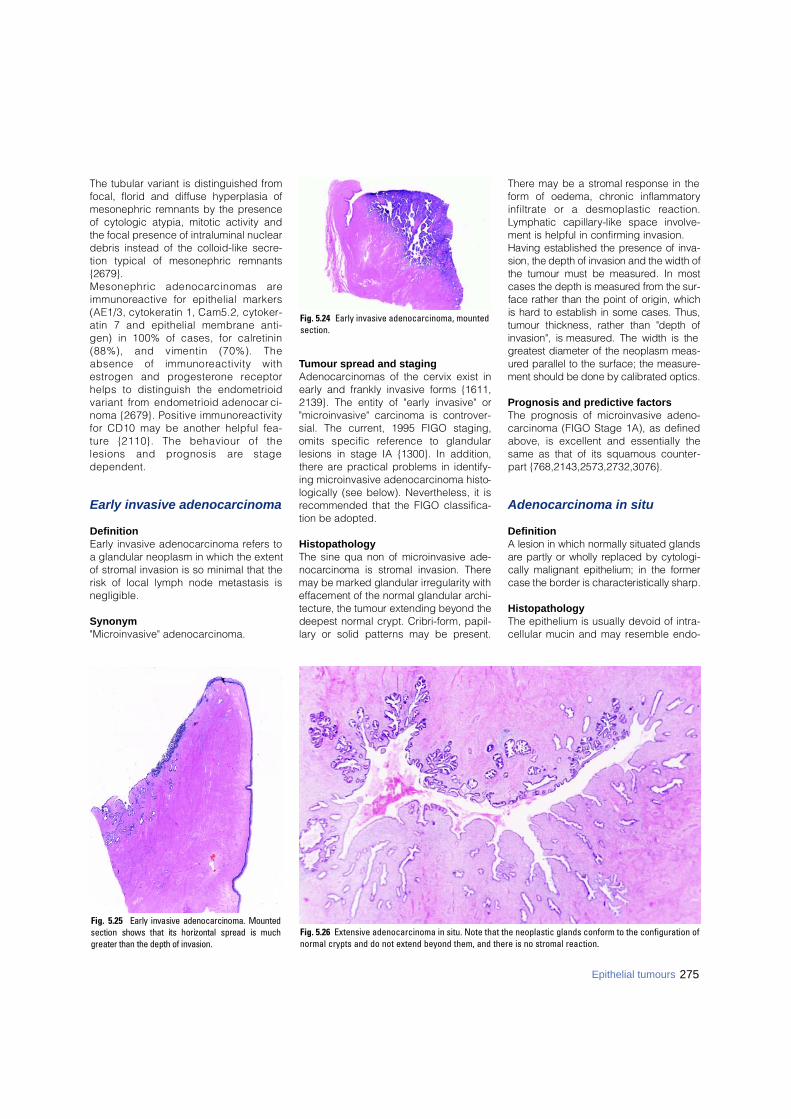
The tubular variant is distinguished fromfocal, florid and diffuse hyperplasia ofmesonephric remnants by the presenceof cytologic atypia, mitotic activity andthe focal presence of intraluminal nucleardebris instead of the colloid-like secre-tion typical of mesonephric re m n a n t s{2679}. Mesonephric adenocarcinomas arei m m u n o reactive for epithelial markers(AE1/3, cytokeratin 1, Cam5.2, cytoker-atin 7 and epithelial membrane anti-gen) in 100% of cases, for calre t i n i n(88%), and vimentin (70%). Theabsence of immunoreactivity withe s t rogen and pro g e s t e rone re c e p t o rhelps to distinguish the endometrioidvariant from endometrioid adenocarc i-noma {2679}. Positive immunore a c t i v i t yfor CD10 may be another helpful fea-t u re {2110}. The behaviour of thelesions and prognosis are staged e p e n d e n t .
Early invasive adenocarcinoma
DefinitionEarly invasive adenocarcinoma refers toa glandular neoplasm in which the extentof stromal invasion is so minimal that therisk of local lymph node metastasis isnegligible.
Synonym"Microinvasive" adenocarcinoma.
Tumour spread and stagingAdenocarcinomas of the cervix exist inearly and frankly invasive forms {1611,2139}. The entity of "early invasive" or"microinvasive" carcinoma is controver-sial. The current, 1995 FIGO staging,omits specific re f e rence to glandularlesions in stage IA {1300}. In addition,there are practical problems in identify-ing microinvasive adenocarcinoma histo-logically (see below). Nevertheless, it isrecommended that the FIGO classifica-tion be adopted.
HistopathologyThe sine qua non of microinvasive ade-n o c a rcinoma is stromal invasion. Theremay be marked glandular irregularity withe ffacement of the normal glandular arc h i-t e c t u re, the tumour extending beyond thedeepest normal crypt. Cribri-form, papil-l a ry or solid patterns may be pre s e n t .
T h e re may be a stromal response in thef o rm of oedema, chronic inflammatoryinfiltrate or a desmoplastic re a c t i o n .Lymphatic capillary-like space involve-ment is helpful in confirming invasion.Having established the presence of inva-sion, the depth of invasion and the width ofthe tumour must be measured. In mostcases the depth is measured from the sur-face rather than the point of origin, whichis hard to establish in some cases. Thus,tumour thickness, rather than "depth ofinvasion", is measured. The width is theg reatest diameter of the neoplasm meas-u red parallel to the surface; the measure-ment should be done by calibrated optics.
Prognosis and predictive factors The prognosis of microinvasive adeno-carcinoma (FIGO Stage 1A), as definedabove, is excellent and essentially thesame as that of its squamous counter-part {768,2143,2573,2732,3076}.
Adenocarcinoma in situ
DefinitionA lesion in which normally situated glandsa re partly or wholly replaced by cytologi-cally malignant epithelium; in the form e rcase the border is characteristically sharp.
HistopathologyThe epithelium is usually devoid of intra-cellular mucin and may resemble endo-
275Epithelial tumours
Fig. 5.26 Extensive adenocarcinoma in situ. Note that the neoplastic glands conform to the configuration ofnormal crypts and do not extend beyond them, and there is no stromal reaction.
Fig. 5.25 Early invasive adenocarcinoma. Mountedsection shows that its horizontal spread is muchgreater than the depth of invasion.
Fig. 5.24 Early invasive adenocarcinoma, mountedsection.

metrial epithelium. In some cases theglands are lined by intestinal epitheliumcontaining goblet, neuroendocrine andPaneth cells. The neoplastic glands con-form to the expected location of normalendocervical glands and do not extendbeyond the deepest normal crypt. A crib-riform pattern is common. The epitheliumis usually stratified with the long axes ofthe cells perpendicular to the base. Theelongated, pleomorphic and hyperchro-matic nuclei are basal in position. Mitoses are common and are disposed onthe luminal side {2142}. Apoptosis is pro m i-nent {279}. The neoplastic epithelium maya ffect the surface, where it is often singlel a y e red, but more commonly is found in thec rypts. These features help to explain thef requent failure of its colposcopic detec-tion. The cell types, in order of fre q u e n c y,a re endocervical, endometrioid and intes-tinal. A putative tubal variant has alsorecently been described {2559}. Althoughthe stroma may be intensely inflamed,t h e re is no desmoplastic reaction. Adeno-c a rcinoma in situ is associated with CIN inat least 50% of cases and is immunore a c-tive for carc i n o e m b ryonic antigen in 80%of cases.
Prognosis and predictive factorsEvidence supporting the pre c a n c e ro u spotential of adenocarcinoma in situincludes its occurrence 10-15 years earli-er than its invasive counterparts, its com-mon association with microinvasive orinvasive adenocarcinoma, its histologicalsimilarity to invasive adenocarc i n o m aand the frequent occurrence of high-riskHPV types. The transformation of adeno-c a rcinoma in situ into invasive adenocar-cinoma over time has also been docu-mented on rare occasions {1224,2076}. Although the treatment of adenocarcino-ma in situ is controversial, increasing evi-
dence is available that conservative ther-apy, such as conization only, is safe andeffective in selected cases {1870,2140}
Glandular dysplasia
DefinitionA glandular lesion characterized by sig-nificant nuclear abnormalities that arem o re striking than those in glandularatypia but fall short of the criteria for ade-n o c a rcinoma in situ.
HistopathologyThe nuclei are not cytologically malignant,and mitoses are less numerous than ina d e n o c a rcinoma in situ. Nuclear hyper-c h romasia and enlargement identify theinvolved glands, and pseudostratificationof cells is prominent. Cribriform and pap-i l l a ry formations are usually absent. The concept that glandular dysplasiaf o rms a biological spectrum of cervicalglandular intraepithelial neoplasia re m a i n su n p roven {420,1032,1534}. Glandular dysplasia must be distin-guished from glandular atypia. The latteris an atypical glandular epithelial alter-ation which does not fulfil the criteria forglandular dysplasia or adenocarcinomain situ and which may be associated withinflammation or irradiation.
Benign glandular lesions
Müllerian papilloma
DefinitionA rare, benign, papillary tumour com-posed of a complex arborizing fibro -vascular core covered by a mantle ofsingle or double-layered mucinousepithelium that may undergo squamousmetaplasia.
Clinical featuresMüllerian papilloma occurs almost exclu-sively in children typically between 2 and5 years of age (range 1-9 years), whopresent with bleeding, discharge or a fri-able, polypoid to papillary, unifocal ormultifocal mass, usually less than 2 cm ingreatest dimension.
HistopathologyThese tumours consist of multiple smallpolypoid projections composed of fibro u ss t roma and lined by simple epithelium.Occasional cells may have a hobnailappearance simulating clear cell adeno-c a rcinoma; however, no clear cells, atyp-ia or mitoses are present. The stroma isoften inflamed and rarely contains psam-moma bodies.
Prognosis and predictive factorsOccasional cases recur {2736}. (Seechapter on the vagina).
Endocervical polyp
DefinitionAn intraluminal protrusion composed ofbland endocervical glands and a fibro-vascular stroma.
EpidemiologyThese are very common lesions thatrarely are of concern clinically and areeasy to diagnose histologically.
Clinical featuresIn 75% of cases they are asympto-matic. The rest present with bleeding(especially post-coital) and/or dis-charge.
MacroscopyThe great majority are less than 1 cm andsingle {15}.
Fig. 5.28 High grade cervical glandular dysplasia.The histological features are not of sufficientseverity to be regarded as adenocarcinoma in situ.
Fig. 5.29 Glandular dysplasia involving endocervi-cal papillae.
Fig. 5.27 Adenocarcinoma in situ. High power mag-nification shows pseudostratified nuclei and amarked degree of apoptosis.
276 Tumours of the uterine cervix
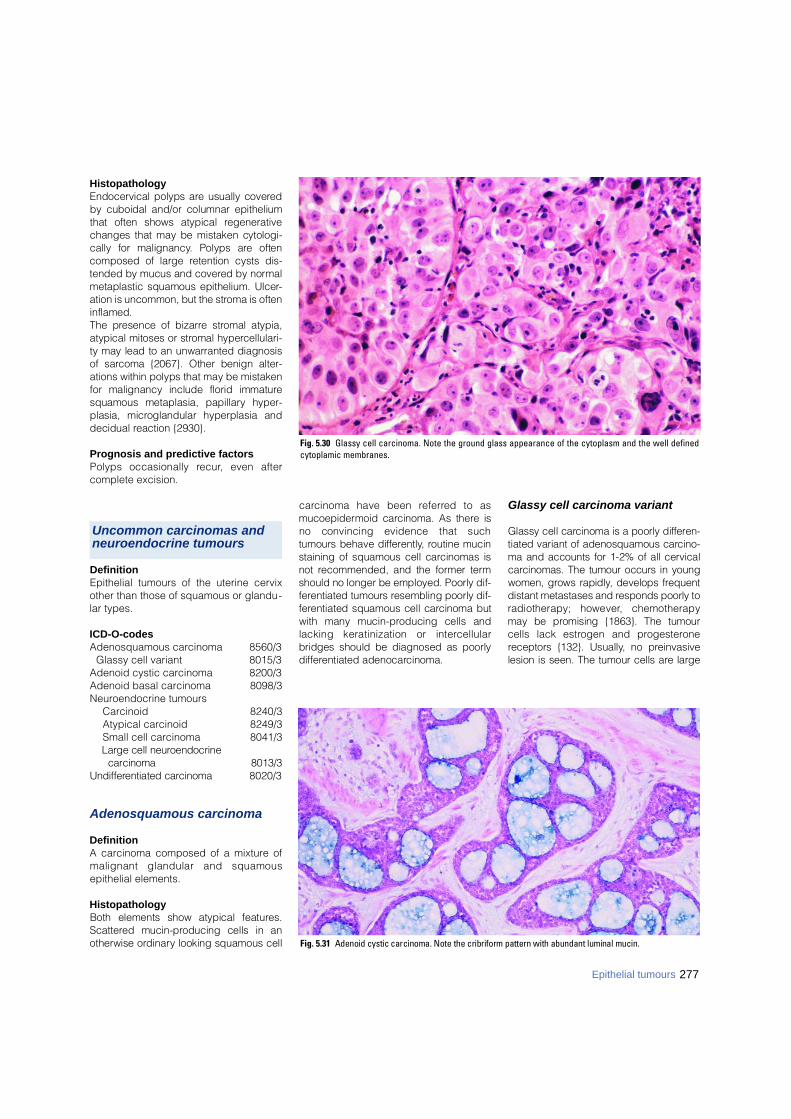
HistopathologyEndocervical polyps are usually covere dby cuboidal and/or columnar epitheliumthat often shows atypical re g e n e r a t i v echanges that may be mistaken cytologi-cally for malignancy. Polyps are oftencomposed of large retention cysts dis-tended by mucus and covered by norm a lmetaplastic squamous epithelium. Ulcer-ation is uncommon, but the stroma is ofteninflamed. The presence of bizarre stromal atypia,atypical mitoses or stromal hyperc e l l u l a r i-ty may lead to an unwarranted diagnosisof sarcoma {2067}. Other benign alter-ations within polyps that may be mistakenfor malignancy include florid immaturesquamous metaplasia, papillary hyper-plasia, microglandular hyperplasia anddecidual reaction {2930}.
Prognosis and predictive factorsPolyps occasionally re c u r, even aftercomplete excision.
DefinitionEpithelial tumours of the uterine cervixother than those of squamous or glandu-lar types.
ICD-O-codesAdenosquamous carcinoma 8560/3
Glassy cell variant 8015/3Adenoid cystic carcinoma 8200/3Adenoid basal carcinoma 8098/3Neuroendocrine tumours
Carcinoid 8240/3Atypical carcinoid 8249/3Small cell carcinoma 8041/3Large cell neuroendocrine
c a rc i n o m a 8 0 1 3 / 3U n d i ff e rentiated carc i n o m a 8020/3
Adenosquamous carcinoma
DefinitionA carcinoma composed of a mixture ofmalignant glandular and squamousepithelial elements.
HistopathologyBoth elements show atypical feature s .S c a t t e red mucin-producing cells in anotherwise ord i n a ry looking squamous cell
c a rcinoma have been re f e r red to asm u c o e p i d e rmoid carcinoma. As there isno convincing evidence that suchtumours behave diff e re n t l y, routine mucinstaining of squamous cell carcinomas isnot recommended, and the former termshould no longer be employed. Poorly dif-f e rentiated tumours resembling poorly dif-f e rentiated squamous cell carcinoma butwith many mucin-producing cells andlacking keratinization or interc e l l u l a rbridges should be diagnosed as poorlyd i ff e rentiated adenocarcinoma.
Glassy cell carcinoma variant
Glassy cell carcinoma is a poorly diff e re n-tiated variant of adenosquamous carc i n o-ma and accounts for 1-2% of all cervicalc a rcinomas. The tumour occurs in youngwomen, grows rapidly, develops fre q u e n tdistant metastases and responds poorly toradiotherapy; however, chemotherapymay be promising {1863}. The tumourcells lack estrogen and pro g e s t e ro n ereceptors {132}. Usually, no pre i n v a s i v elesion is seen. The tumour cells are large
Fig. 5.30 Glassy cell carcinoma. Note the ground glass appearance of the cytoplasm and the well definedcytoplamic membranes.
277Epithelial tumours
Fig. 5.31 Adenoid cystic carcinoma. Note the cribriform pattern with abundant luminal mucin.
Uncommon carcinomas and neuroendocrine tumours
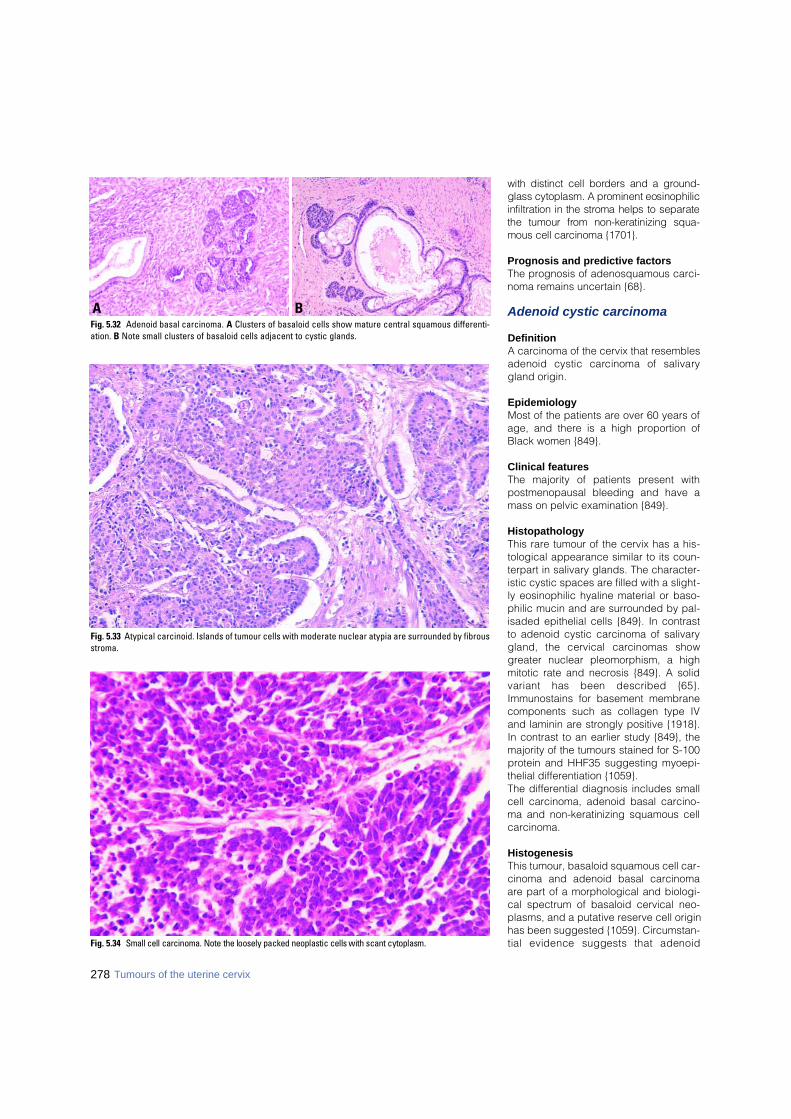
with distinct cell borders and a gro u n d -glass cytoplasm. A prominent eosinophilicinfiltration in the stroma helps to separatethe tumour from non-keratinizing squa-mous cell carcinoma {1701}.
Prognosis and predictive factorsThe prognosis of adenosquamous carci-noma remains uncertain {68}.
Adenoid cystic carcinoma
DefinitionA carcinoma of the cervix that resemblesadenoid cystic carcinoma of salivarygland origin.
EpidemiologyMost of the patients are over 60 years ofage, and there is a high proportion ofBlack women {849}.
Clinical featuresThe majority of patients present withpostmenopausal bleeding and have amass on pelvic examination {849}.
HistopathologyThis rare tumour of the cervix has a his-tological appearance similar to its coun-terpart in salivary glands. The character-istic cystic spaces are filled with a slight-ly eosinophilic hyaline material or baso-philic mucin and are surrounded by pal-isaded epithelial cells {849}. In contrastto adenoid cystic carcinoma of salivarygland, the cervical carcinomas showgreater nuclear pleomorphism, a highmitotic rate and necrosis {849}. A solidvariant has been described {65}.Immunostains for basement membranecomponents such as collagen type IVand laminin are strongly positive {1918}.In contrast to an earlier study {849}, themajority of the tumours stained for S-100protein and HHF35 suggesting myoepi-thelial differentiation {1059}.The differential diagnosis includes smallcell carcinoma, adenoid basal carcino-ma and non-keratinizing squamous cellcarcinoma.
HistogenesisThis tumour, basaloid squamous cell car-cinoma and adenoid basal carcinomaare part of a morphological and biologi-cal spectrum of basaloid cervical neo-plasms, and a putative reserve cell originhas been suggested {1059}. Circumstan-tial evidence suggests that adenoid
BAFig. 5.32 Adenoid basal carcinoma. A Clusters of basaloid cells show mature central squamous differenti-ation. B Note small clusters of basaloid cells adjacent to cystic glands.
Fig. 5.33 Atypical carcinoid. Islands of tumour cells with moderate nuclear atypia are surrounded by fibrousstroma.
278 Tumours of the uterine cervix
Fig. 5.34 Small cell carcinoma. Note the loosely packed neoplastic cells with scant cytoplasm.
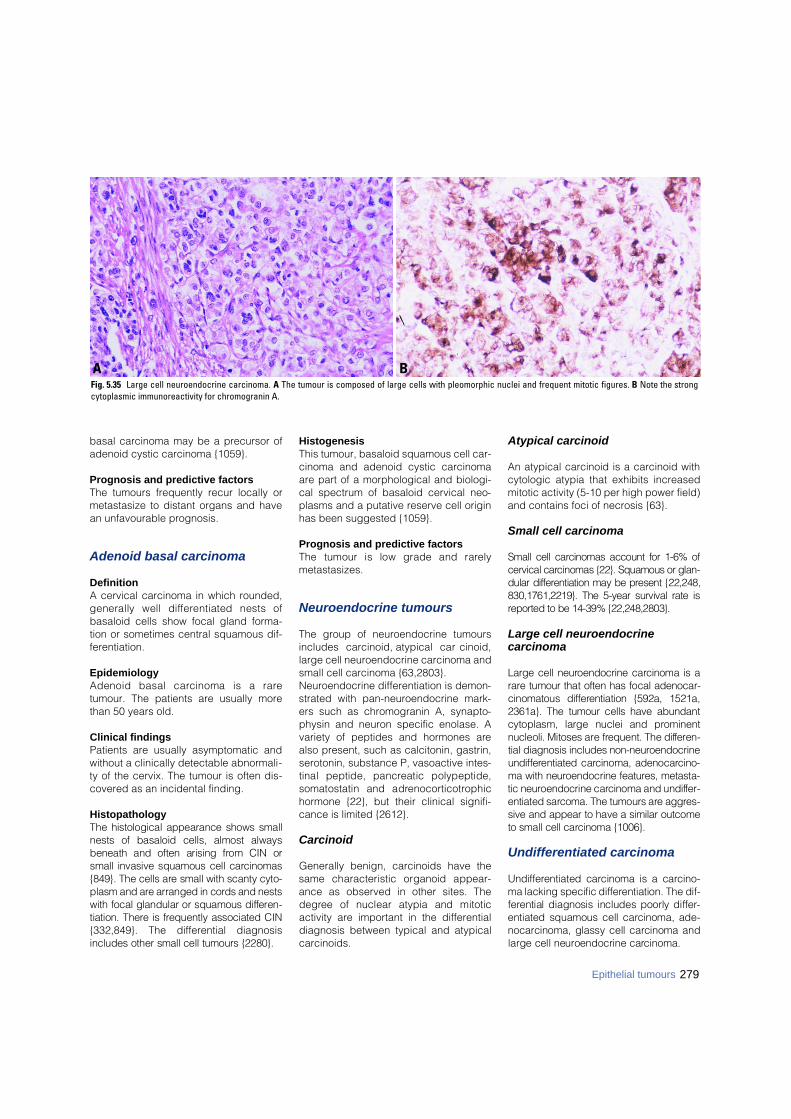
basal carcinoma may be a precursor ofadenoid cystic carcinoma {1059}.
Prognosis and predictive factors The tumours frequently recur locally ormetastasize to distant organs and havean unfavourable prognosis.
Adenoid basal carcinoma
DefinitionA cervical carcinoma in which rounded,generally well diff e rentiated nests ofbasaloid cells show focal gland forma-tion or sometimes central squamous dif-ferentiation.
EpidemiologyAdenoid basal carcinoma is a raretumour. The patients are usually morethan 50 years old.
Clinical findingsPatients are usually asymptomatic andwithout a clinically detectable abnormali-ty of the cervix. The tumour is often dis-covered as an incidental finding.
HistopathologyThe histological appearance shows smallnests of basaloid cells, almost alwaysbeneath and often arising from CIN orsmall invasive squamous cell carc i n o m a s{849}. The cells are small with scanty cyto-plasm and are arranged in cords and nestswith focal glandular or squamous diff e re n-tiation. There is frequently associated CIN{332,849}. The differential diagnosisincludes other small cell tumours {2280}.
HistogenesisThis tumour, basaloid squamous cell car-cinoma and adenoid cystic carcinomaare part of a morphological and biologi-cal spectrum of basaloid cervical neo-plasms and a putative reserve cell originhas been suggested {1059}.
Prognosis and predictive factorsThe tumour is low grade and rare l ymetastasizes.
Neuroendocrine tumours
The group of neuroendocrine tumoursincludes carcinoid, atypical carc i n o i d ,large cell neuroendocrine carcinoma andsmall cell carcinoma {63,2803}.Neuroendocrine differentiation is demon-strated with pan-neuroendocrine mark-ers such as chromogranin A, synapto-physin and neuron specific enolase. Avariety of peptides and hormones arealso present, such as calcitonin, gastrin,serotonin, substance P, vasoactive intes-tinal peptide, pancreatic polypeptide,somatostatin and adre n o c o rt i c o t ro p h i chormone {22}, but their clinical signifi-cance is limited {2612}.
Carcinoid
Generally benign, carcinoids have thesame characteristic organoid appear-ance as observed in other sites. Thed e g ree of nuclear atypia and mitoticactivity are important in the differentialdiagnosis between typical and atypicalcarcinoids.
Atypical carcinoid
An atypical carcinoid is a carcinoid withcytologic atypia that exhibits increasedmitotic activity (5-10 per high power field)and contains foci of necrosis {63}.
Small cell carcinoma
Small cell carcinomas account for 1-6% ofcervical carcinomas {22}. Squamous or glan-dular diff e rentiation may be present {22,248,830,1761,2219}. The 5-year survival rate isre p o rted to be 14-39% {22,248,2803}.
Large cell neuroendocrine carcinoma
Large cell neuroendocrine carcinoma is ar a re tumour that often has focal adenocar-cinomatous diff e rentiation {592a, 1521a,2361a}. The tumour cells have abundantcytoplasm, large nuclei and pro m i n e n tnucleoli. Mitoses are frequent. The diff e re n-tial diagnosis includes non-neuro e n d o c r i n eu n d i ff e rentiated carcinoma, adenocarc i n o-ma with neuroendocrine features, metasta-tic neuroendocrine carcinoma and undiff e r-entiated sarcoma. The tumours are aggre s-sive and appear to have a similar outcometo small cell carcinoma {1006}.
Undifferentiated carcinoma
U n d i ff e rentiated carcinoma is a carc i n o-ma lacking specific diff e rentiation. The dif-f e rential diagnosis includes poorly diff e r-entiated squamous cell carcinoma, ade-n o c a rcinoma, glassy cell carcinoma andlarge cell neuroendocrine carc i n o m a .
279Epithelial tumours
BAFig. 5.35 Large cell neuroendocrine carcinoma. A The tumour is composed of large cells with pleomorphic nuclei and frequent mitotic figures. B Note the strongcytoplasmic immunoreactivity for chromogranin A.
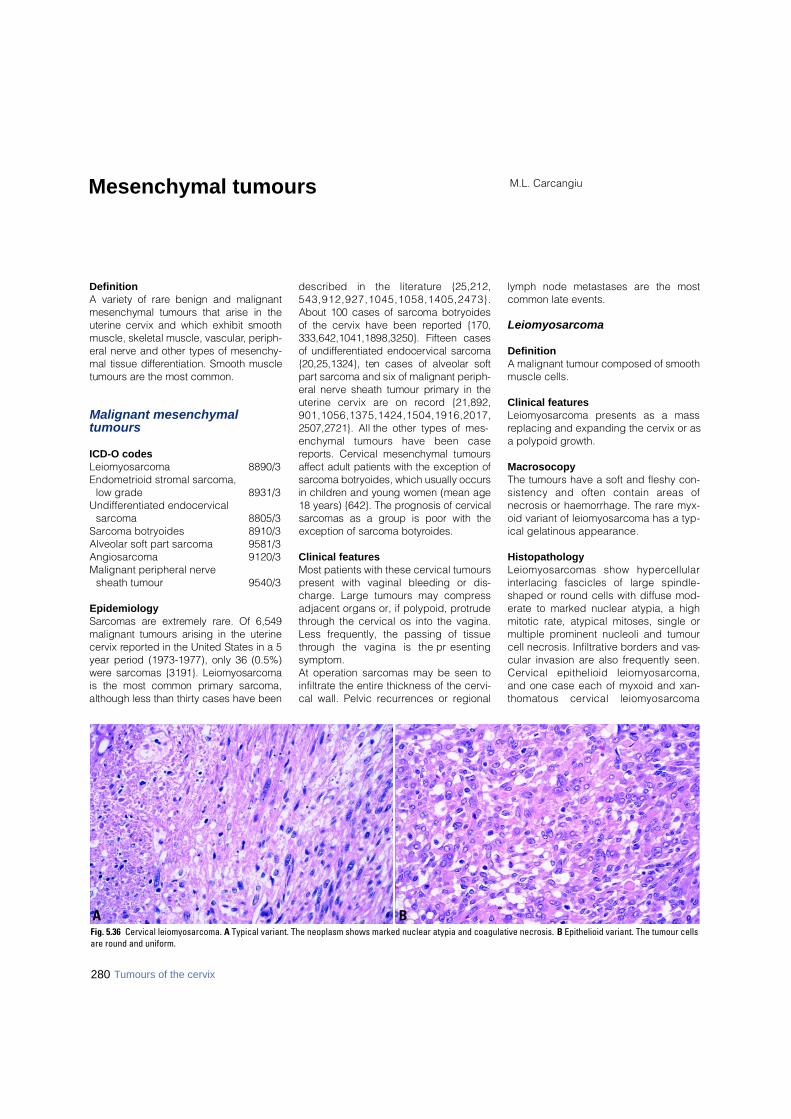
DefinitionA variety of rare benign and malignantmesenchymal tumours that arise in theuterine cervix and which exhibit smoothmuscle, skeletal muscle, vascular, periph-eral nerve and other types of mesenchy-mal tissue diff e rentiation. Smooth muscletumours are the most common.
Malignant mesenchymal tumours
ICD-O codesLeiomyosarcoma 8890/3Endometrioid stromal sarcoma,
low grade 8931/3Undifferentiated endocervical
sarcoma 8805/3Sarcoma botryoides 8910/3Alveolar soft part sarcoma 9581/3Angiosarcoma 9120/3Malignant peripheral nerve
sheath tumour 9540/3
EpidemiologyS a rcomas are extremely rare. Of 6,549malignant tumours arising in the uterinecervix re p o rted in the United States in a 5year period (1973-1977), only 36 (0.5%)w e re sarcomas {3191}. Leiomyosarc o m ais the most common primary sarc o m a ,although less than thirty cases have been
described in the literature {25,212,5 4 3 , 9 1 2 , 9 2 7 , 1 0 4 5 , 1 0 5 8 , 1 4 0 5 , 2 4 7 3 } .About 100 cases of sarcoma botry o i d e sof the cervix have been re p o rted {170,333,642,1041,1898,3250}. Fifteen casesof undiff e rentiated endocervical sarc o m a{20,25,1324}, ten cases of alveolar softp a rt sarcoma and six of malignant periph-eral nerve sheath tumour primary in theuterine cervix are on re c o rd {21,892,9 0 1 , 1 0 5 6 , 1 3 7 5 , 1 4 2 4 , 1 5 0 4 , 1 9 1 6 , 2 0 1 7 ,2507,2721}. All the other types of mes-enchymal tumours have been casere p o rts. Cervical mesenchymal tumoursa ffect adult patients with the exception ofs a rcoma botryoides, which usually occursin children and young women (mean age18 years) {642}. The prognosis of cervicals a rcomas as a group is poor with theexception of sarcoma botyro i d e s .
Clinical featuresMost patients with these cervical tumourspresent with vaginal bleeding or dis-charge. Large tumours may compressadjacent organs or, if polypoid, protrudethrough the cervical os into the vagina.Less frequently, the passing of tissuet h rough the vagina is the pre s e n t i n gsymptom.At operation sarcomas may be seen toinfiltrate the entire thickness of the cervi-cal wall. Pelvic recurrences or regional
lymph node metastases are the mostcommon late events.
Leiomyosarcoma
DefinitionA malignant tumour composed of smoothmuscle cells.
Clinical featuresLeiomyosarcoma presents as a massreplacing and expanding the cervix or asa polypoid growth.
MacrosocopyThe tumours have a soft and fleshy con-sistency and often contain areas ofnecrosis or haemorrhage. The rare myx-oid variant of leiomyosarcoma has a typ-ical gelatinous appearance.
HistopathologyL e i o m y o s a rcomas show hyperc e l l u l a rinterlacing fascicles of large spindle-shaped or round cells with diffuse mod-erate to marked nuclear atypia, a highmitotic rate, atypical mitoses, single ormultiple prominent nucleoli and tumourcell necrosis. Infiltrative borders and vas-cular invasion are also frequently seen.Cervical epithelioid leiomyosarc o m a ,and one case each of myxoid and xan-thomatous cervical leiomyosarc o m a
M.L. CarcangiuMesenchymal tumours
BAFig. 5.36 Cervical leiomyosarcoma. A Typical variant. The neoplasm shows marked nuclear atypia and coagulative necrosis. B Epithelioid variant. The tumour cellsare round and uniform.
280 Tumours of the cervix

have been reported {543,912,927,1045,1058}.
Differential diagnosisThe criteria used in the distinction fromleiomyoma are the same as those forsmooth muscle tumours of the uterinecorpus. At least two of three features(marked nuclear atypia, a mitotic ratehigher than 10 mitoses per 10 highpower fields and tumour necrosis) arerequired for the diagnosis of leiomyosar-coma {211}. For epithelioid leiomyosar-coma a mitotic count higher than 5mitoses per 10 high power fields is con-sidered diagnostic of malignancy. A lowmitotic count is typical of the myxoid vari-ant {912}. Antibodies to smooth muscleactin and/or desmin may be used todemonstrate smooth muscle differentia-tion in these tumours. L e i o m y o s a rcoma should be diff e re n t i a t-ed from postoperative spindle cell nod-ule {1420}. The latter is mitoticallyactive and may infiltrate the underlyingtissue. The distinction from leiomyosar-coma or other malignant spindle celltumour depends to a large extent on theh i s t o ry of a recent operation at thesame site.
Endometrioid stromal sarcoma,low grade
DefinitionA sarcoma arising outside of the funduscomposed of cells resembling endome-trial stromal cells.
EpidemiologyVery rarely, tumours with the features oflow grade endometrial stromal sarcomaarise in the cervix {295,437}.
HistopathologyThis tumour may arise from cervicalendometriosis and must be distin-guished from stromal endometriosis andp r i m a ry endometrial stromal sarc o m athat has invaded the cervix. The termundifferentiated endocervical sarcoma ispreferred for high grade lesions.
Undifferentiated endocervical sarcoma
DefinitionAn endocervical sarcoma lackingendometrial stromal or other specific dif-ferentiation {20,1324}.
HistopathologyTumours described in the literature asu n d i ff e rentiated endocervical sarc o m aare characterized by a polypoid or infil-trative cervical growth similar to thatexhibited by malignant peripheral nervesheath tumours arising in the uterinecervix {25,1424}.The tumour is composed of spindle orstellate-shaped cells with scanty cyto-plasm, ill defined cell borders and ovalh y p e rc h romatic nuclei arranged in asheet-like, fasciculated or storiform pat-tern {25}. The prominent vascular patterntypical of endometrioid stromal sarcomais not a characteristic of these tumours,and the stromal proliferation tends toencircle the endocervical glands creat-ing a focal resemblance to adenosarco-ma. Nuclear atypia and markedlyincreased mitotic activity are seen in allcases, as well as areas of haemorrhage,necrosis and myxoid degeneration.
Sarcoma botryoides
DefinitionA tumour composed of cells with small,round, oval or spindle-shaped nuclei,some of which show evidence of differ-entiation towards skeletal muscle cells.
SynonymEmbryonal rhabdomyosarcoma.
MacroscopyEmbryonal rhabdomyosarcoma usuallygrows in a polypoid fashion. The grape-like type of growth classically exhibitedby vaginal sarcoma botryoides is onlyrarely seen in cervical tumours. The poly-poid masses have a glistening translu-cent surface and a soft consistency andmay be pedunculated or sessile. Theirsize ranges from 2-10 cm {642}. The sec-tioned surface of the tumour appearssmooth and myxoid with small haemor-rhagic areas.
HistopathologyThe histological features are described inthe section on the vagina. Islands ofmature neoplastic cartilage are more fre-quently seen in cervical than in vaginaltumours {642}.
Somatic geneticsIn one case of sarcoma botryoides chro-mosomal analysis has demonstrated dele-tion of the short arm of chromosome 1,
and trisomies 13 and 18 {2156}, and inanother a point mutation in exon 6 of T P 5 3was found, but no K R A S point mutations atcodons 12,13 and 61 were detected{ 2 6 2 7 } .
Genetic susceptibilityAn association between ovarian Sertoli-Leydig tumour and cervical sarc o m abotryoides has been described {1026}
Prognosis and predictive factorsThe use of neoadjuvant chemotherapyallows a more conservative approach forthese neoplasms {170,1041,3250}.
Alveolar soft part sarcoma
DefinitionA sarcoma characterized by solid andalveolar groups of large epithelial-like cellswith granular, eosinophilic cytoplasm.
281Mesenchymal tumours
Fig. 5.37 Cervical sarcoma botyroides. A T h esubepithelial cambium layer is prominent. B Notethe focus of neoplastic cartilage. C Tumour cellswith eosinophilic cytoplasm exhibit myoblastic dif-ferentiation.
B
A
C
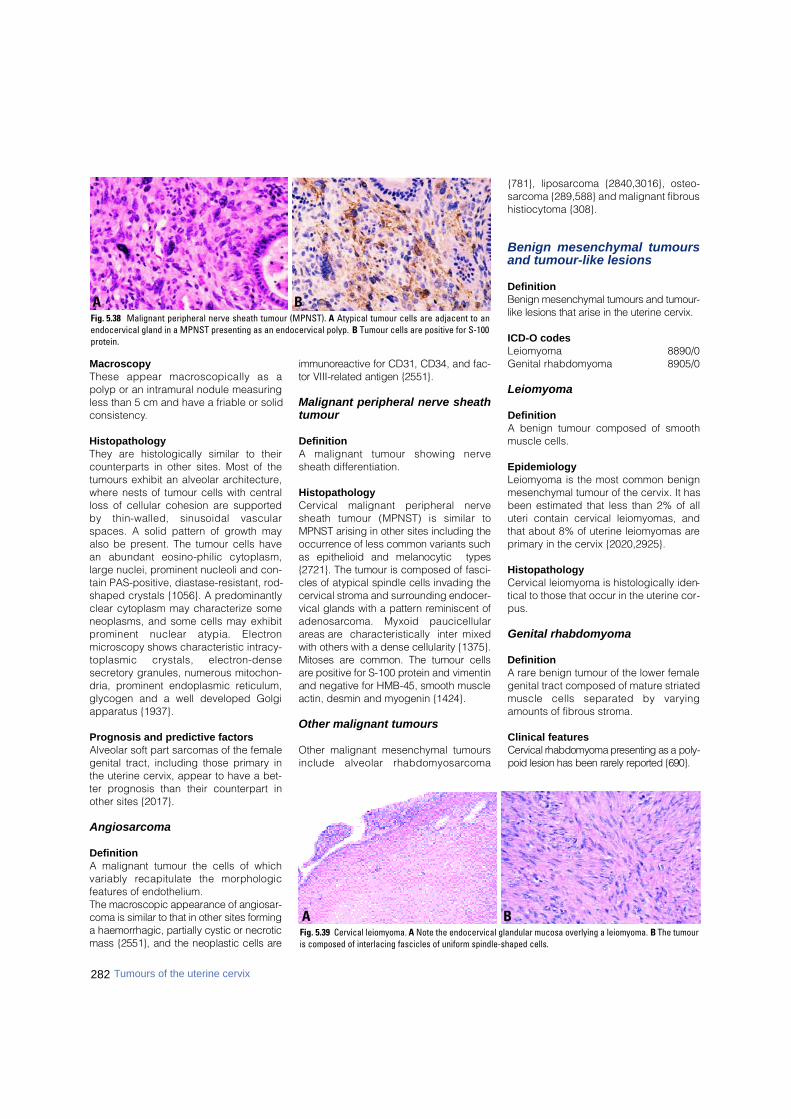
282 Tumours of the uterine cervix
MacroscopyThese appear macroscopically as apolyp or an intramural nodule measuringless than 5 cm and have a friable or solidconsistency.
HistopathologyThey are histologically similar to theircounterparts in other sites. Most of thetumours exhibit an alveolar architecture,where nests of tumour cells with centralloss of cellular cohesion are supportedby thin-walled, sinusoidal vascularspaces. A solid pattern of growth mayalso be present. The tumour cells havean abundant eosino-philic cytoplasm,large nuclei, prominent nucleoli and con-tain PAS-positive, diastase-resistant, rod-shaped crystals {1056}. A predominantlyclear cytoplasm may characterize someneoplasms, and some cells may exhibitp rominent nuclear atypia. Electro nmicroscopy shows characteristic intracy-toplasmic crystals, electro n - d e n s esecretory granules, numerous mitochon-dria, prominent endoplasmic reticulum,glycogen and a well developed Golgiapparatus {1937}.
Prognosis and predictive factorsAlveolar soft part sarcomas of the femalegenital tract, including those primary inthe uterine cervix, appear to have a bet-ter prognosis than their counterpart inother sites {2017}.
Angiosarcoma
DefinitionA malignant tumour the cells of whichvariably recapitulate the morphologicfeatures of endothelium.The macroscopic appearance of angiosar-coma is similar to that in other sites form i n ga haemorrhagic, partially cystic or necro t i cmass {2551}, and the neoplastic cells are
i m m u n o reactive for CD31, CD34, and fac-tor VIII-related antigen {2551}.
Malignant peripheral nerve sheathtumour
DefinitionA malignant tumour showing nervesheath differentiation.
HistopathologyCervical malignant peripheral nervesheath tumour (MPNST) is similar toMPNST arising in other sites including theo c c u r rence of less common variants suchas epithelioid and melanocytic types{2721}. The tumour is composed of fasci-cles of atypical spindle cells invading thecervical stroma and surrounding endocer-vical glands with a pattern reminiscent ofa d e n o s a rcoma. Myxoid paucicellulara reas are characteristically interm i x e dwith others with a dense cellularity {1375}.Mitoses are common. The tumour cellsa re positive for S-100 protein and vimentinand negative for HMB-45, smooth muscleactin, desmin and myogenin {1424}.
Other malignant tumours
Other malignant mesenchymal tumoursinclude alveolar rhabdomyosarc o m a
{781}, liposarcoma {2840,3016}, osteo-sarcoma {289,588} and malignant fibroushistiocytoma {308}.
Benign mesenchymal tumoursand tumour-like lesions
DefinitionBenign mesenchymal tumours and tumour-like lesions that arise in the uterine cervix.
ICD-O codesLeiomyoma 8890/0Genital rhabdomyoma 8905/0
Leiomyoma
DefinitionA benign tumour composed of smoothmuscle cells.
EpidemiologyLeiomyoma is the most common benignmesenchymal tumour of the cervix. It hasbeen estimated that less than 2% of alluteri contain cervical leiomyomas, andthat about 8% of uterine leiomyomas areprimary in the cervix {2020,2925}.
HistopathologyCervical leiomyoma is histologically iden-tical to those that occur in the uterine cor-pus.
Genital rhabdomyoma
DefinitionA rare benign tumour of the lower femalegenital tract composed of mature striatedmuscle cells separated by vary i n gamounts of fibrous stroma.
Clinical featuresCervical rhabdomyoma presenting as a poly-poid lesion has been rarely re p o rted {690}.
BAFig. 5.39 Cervical leiomyoma. A Note the endocervical glandular mucosa overlying a leiomyoma. B The tumouris composed of interlacing fascicles of uniform spindle-shaped cells.
BAFig. 5.38 Malignant peripheral nerve sheath tumour (MPNST). A Atypical tumour cells are adjacent to anendocervical gland in a MPNST presenting as an endocervical polyp. B Tumour cells are positive for S-100protein.
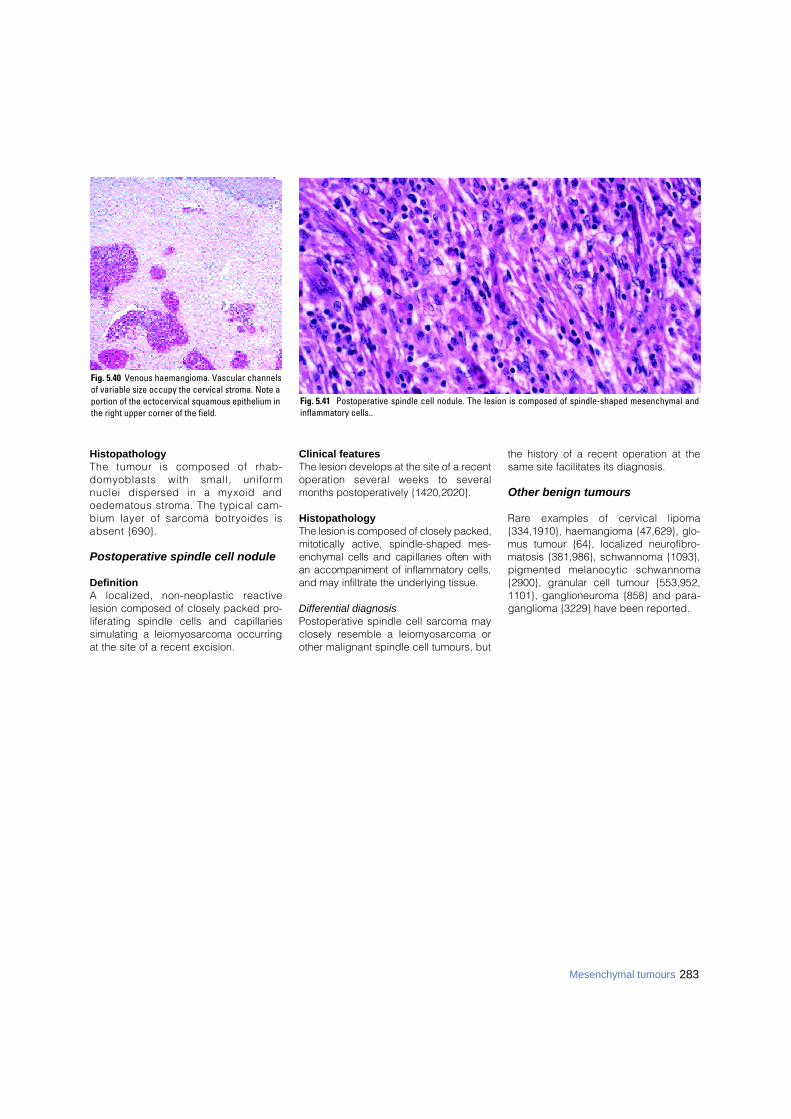
283Mesenchymal tumours
HistopathologyThe tumour is composed of rhab-domyoblasts with small, uniformnuclei dispersed in a myxoid andoedematous stroma. The typical cam-bium layer of sarcoma botryoides isabsent {690}.
Postoperative spindle cell nodule
DefinitionA localized, non-neoplastic re a c t i v elesion composed of closely packed pro-liferating spindle cells and capillariessimulating a leiomyosarcoma occurringat the site of a recent excision.
Clinical featuresThe lesion develops at the site of a recentoperation several weeks to severalmonths postoperatively {1420,2020}.
HistopathologyThe lesion is composed of closely packed,mitotically active, spindle-shaped mes-enchymal cells and capillaries often withan accompaniment of inflammatory cells,and may infiltrate the underlying tissue.
Differential diagnosisPostoperative spindle cell sarcoma mayclosely resemble a leiomyosarcoma orother malignant spindle cell tumours, but
the history of a recent operation at thesame site facilitates its diagnosis.
Other benign tumours
R a re examples of cervical lipoma{334,1910}, haemangioma {47,629}, glo-mus tumour {64}, localized neurofibro-matosis {381,986}, schwannoma {1093},pigmented melanocytic schwannoma{2900}, granular cell tumour {553,952,1101}, ganglioneuroma {858} and para-ganglioma {3229} have been reported.
Fig. 5.41 Postoperative spindle cell nodule. The lesion is composed of spindle-shaped mesenchymal andinflammatory cells..
Fig. 5.40 Venous haemangioma. Vascular channelsof variable size occupy the cervical stroma. Note aportion of the ectocervical squamous epithelium inthe right upper corner of the field.
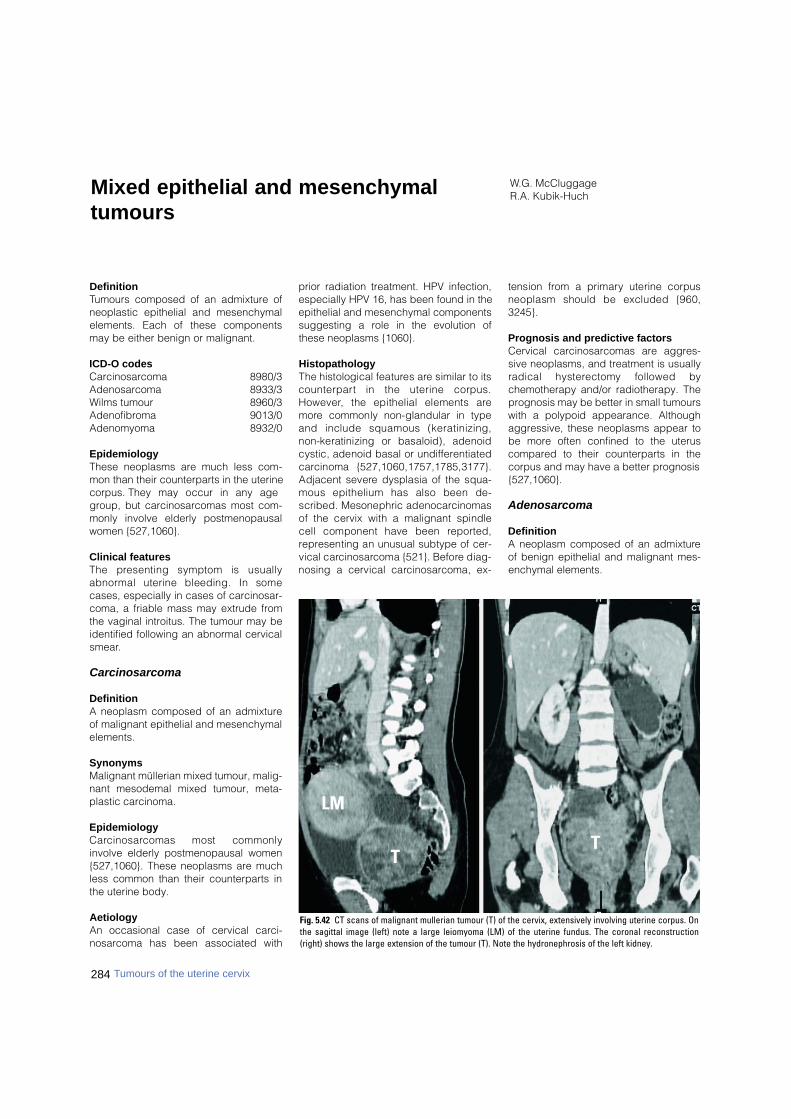
DefinitionTumours composed of an admixture ofneoplastic epithelial and mesenchymalelements. Each of these componentsmay be either benign or malignant.
ICD-O codesCarcinosarcoma 8980/3Adenosarcoma 8933/3Wilms tumour 8960/3Adenofibroma 9013/0Adenomyoma 8932/0
EpidemiologyThese neoplasms are much less com-mon than their counterparts in the uterinecorpus. They may occur in any agegroup, but carcinosarcomas most com-monly involve elderly postmenopausalwomen {527,1060}.
Clinical featuresThe presenting symptom is usuallya b n o rmal uterine bleeding. In somecases, especially in cases of carcinosar-coma, a friable mass may extrude fromthe vaginal introitus. The tumour may beidentified following an abnormal cervicalsmear.
Carcinosarcoma
DefinitionA neoplasm composed of an admixtureof malignant epithelial and mesenchymalelements.
SynonymsMalignant müllerian mixed tumour, malig-nant mesodemal mixed tumour, meta-plastic carcinoma.
EpidemiologyC a rc i n o s a rcomas most commonlyinvolve elderly postmenopausal women{527,1060}. These neoplasms are muchless common than their counterparts inthe uterine body.
AetiologyAn occasional case of cervical carci-nosarcoma has been associated with
prior radiation treatment. HPV infection,especially HPV 16, has been found in theepithelial and mesenchymal componentssuggesting a role in the evolution ofthese neoplasms {1060}.
HistopathologyThe histological features are similar to itsc o u n t e r p a rt in the uterine corpus.H o w e v e r, the epithelial elements arem o re commonly non-glandular in typeand include squamous (keratinizing,non-keratinizing or basaloid), adenoidcystic, adenoid basal or undiff e re n t i a t e dc a rcinoma {527,1060,1757,1785,3177}.Adjacent severe dysplasia of the squa-mous epithelium has also been de-scribed. Mesonephric adenocarc i n o m a sof the cervix with a malignant spindlecell component have been re p o rt e d ,re p resenting an unusual subtype of cer-vical carc i n o s a rcoma {521}. Before diag-nosing a cervical carc i n o s a rcoma, ex-
tension from a primary uterine corpusneoplasm should be excluded {960,3245}.
Prognosis and predictive factorsCervical carcinosarcomas are aggres-sive neoplasms, and treatment is usuallyradical hysterectomy followed bychemotherapy and/or radiotherapy. Theprognosis may be better in small tumourswith a polypoid appearance. Althoughaggressive, these neoplasms appear tobe more often confined to the uteruscompared to their counterparts in thecorpus and may have a better prognosis{527,1060}.
Adenosarcoma
DefinitionA neoplasm composed of an admixtureof benign epithelial and malignant mes-enchymal elements.
W.G. McCluggageR.A. Kubik-HuchMixed epithelial and mesenchymal
tumours
284 Tumours of the uterine cervix
Fig. 5.42 CT scans of malignant mullerian tumour (T) of the cervix, extensively involving uterine corpus. Onthe sagittal image (left) note a large leiomyoma (LM) of the uterine fundus. The coronal reconstruction(right) shows the large extension of the tumour (T). Note the hydronephrosis of the left kidney.
TT
LM
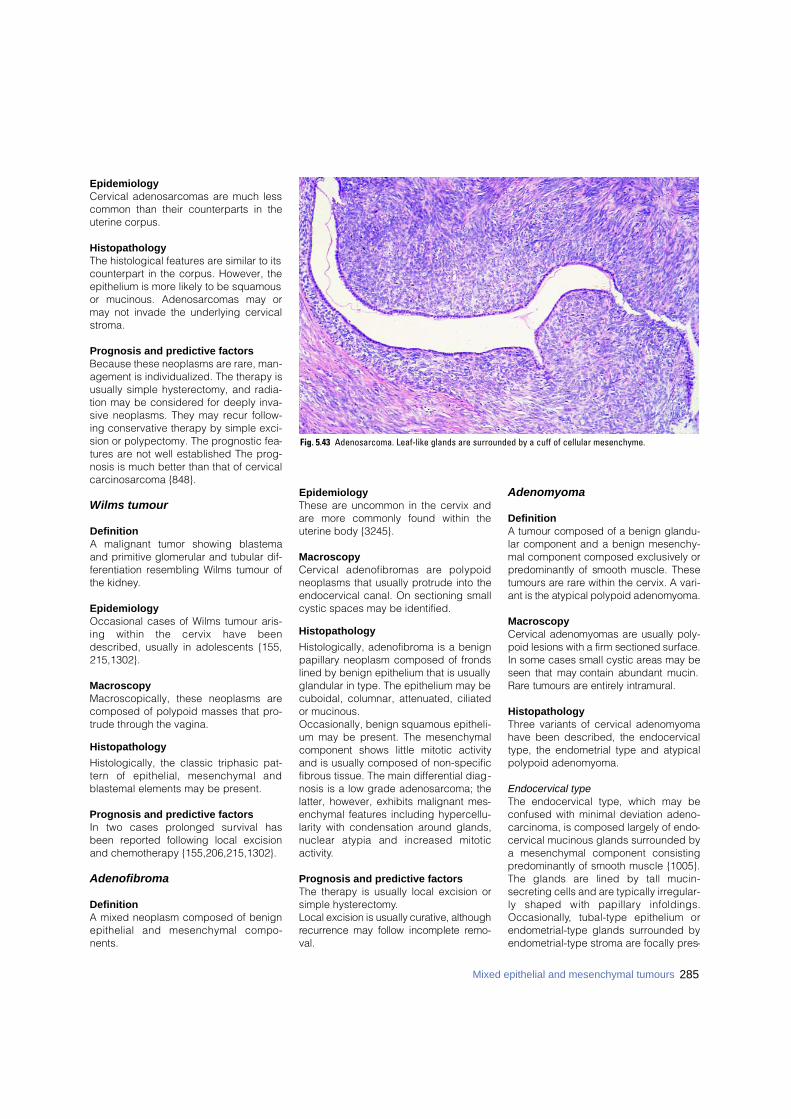
EpidemiologyCervical adenosarcomas are much lesscommon than their counterparts in theuterine corpus.
HistopathologyThe histological features are similar to itscounterpart in the corpus. However, theepithelium is more likely to be squamousor mucinous. Adenosarcomas may ormay not invade the underlying cervicalstroma.
Prognosis and predictive factorsBecause these neoplasms are rare, man-agement is individualized. The therapy isusually simple hysterectomy, and radia-tion may be considered for deeply inva-sive neoplasms. They may recur follow-ing conservative therapy by simple exci-sion or polypectomy. The prognostic fea-tures are not well established The prog-nosis is much better than that of cervicalcarcinosarcoma {848}.
Wilms tumour
DefinitionA malignant tumor showing blastemaand primitive glomerular and tubular dif-ferentiation resembling Wilms tumour ofthe kidney.
EpidemiologyOccasional cases of Wilms tumour aris-ing within the cervix have beendescribed, usually in adolescents {155,215,1302}.
MacroscopyMacroscopically, these neoplasms arecomposed of polypoid masses that pro-trude through the vagina.
Histopathology
Histologically, the classic triphasic pat-t e rn of epithelial, mesenchymal andblastemal elements may be present.
Prognosis and predictive factorsIn two cases prolonged survival hasbeen reported following local excisionand chemotherapy {155,206,215,1302}.
Adenofibroma
DefinitionA mixed neoplasm composed of benignepithelial and mesenchymal compo-nents.
EpidemiologyThese are uncommon in the cervix andare more commonly found within theuterine body {3245}.
Macroscopy Cervical adenofibromas are polypoidneoplasms that usually protrude into theendocervical canal. On sectioning smallcystic spaces may be identified.
Histopathology
Histologically, adenofibroma is a benignpapillary neoplasm composed of frondslined by benign epithelium that is usuallyglandular in type. The epithelium may becuboidal, columnar, attenuated, ciliatedor mucinous. Occasionally, benign squamous epitheli-um may be present. The mesenchymalcomponent shows little mitotic activityand is usually composed of non-specificfibrous tissue. The main differential diag-nosis is a low grade adenosarcoma; thelatter, however, exhibits malignant mes-enchymal features including hypercellu-larity with condensation around glands,nuclear atypia and increased mitoticactivity.
Prognosis and predictive factorsThe therapy is usually local excision orsimple hysterectomy.Local excision is usually curative, althoughre c u r rence may follow incomplete re m o -v a l .
Adenomyoma
DefinitionA tumour composed of a benign glandu-lar component and a benign mesenchy-mal component composed exclusively orp redominantly of smooth muscle. Thesetumours are rare within the cervix. A vari-ant is the atypical polypoid adenomyoma.
MacroscopyCervical adenomyomas are usually poly-poid lesions with a firm sectioned surf a c e .In some cases small cystic areas may beseen that may contain abundant mucin.R a re tumours are entirely intramural.
HistopathologyThree variants of cervical adenomyomahave been described, the endocervicaltype, the endometrial type and atypicalpolypoid adenomyoma.
Endocervical typeThe endocervical type, which may beconfused with minimal deviation adeno-carcinoma, is composed largely of endo-cervical mucinous glands surrounded bya mesenchymal component consistingpredominantly of smooth muscle {1005}.The glands are lined by tall mucin-secreting cells and are typically irregular-ly shaped with papillary infoldings.O c c a s i o n a l l y, tubal-type epithelium orendometrial-type glands surrounded byendometrial-type stroma are focally pres-
285Mixed epithelial and mesenchymal tumours
Fig. 5.43 Adenosarcoma. Leaf-like glands are surrounded by a cuff of cellular mesenchyme.
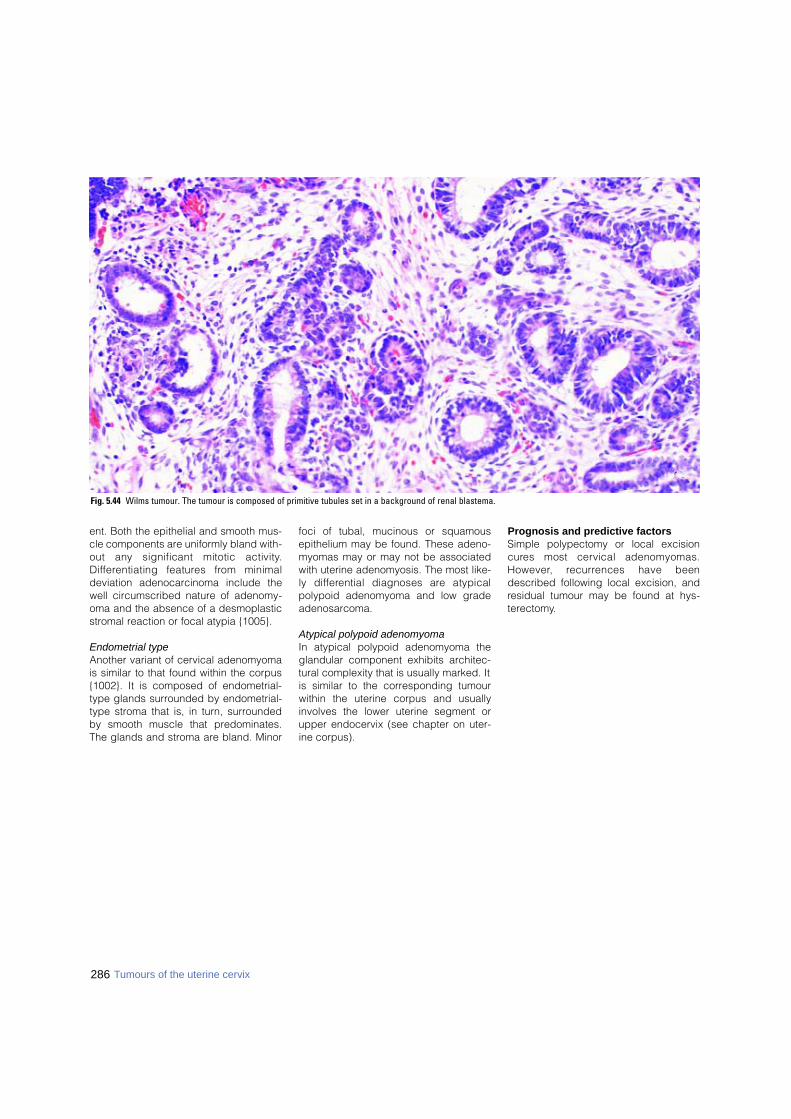
286 Tumours of the uterine cervix
ent. Both the epithelial and smooth mus-cle components are uniformly bland with-out any significant mitotic activity.D i ff e rentiating features from minimaldeviation adenocarcinoma include thewell circumscribed nature of adenomy-oma and the absence of a desmoplasticstromal reaction or focal atypia {1005}.
Endometrial typeAnother variant of cervical adenomyomais similar to that found within the corpus{1002}. It is composed of endometrial-type glands surrounded by endometrial-type stroma that is, in turn, surroundedby smooth muscle that predominates.The glands and stroma are bland. Minor
foci of tubal, mucinous or squamousepithelium may be found. These adeno-myomas may or may not be associatedwith uterine adenomyosis. The most like-ly diff e rential diagnoses are atypicalpolypoid adenomyoma and low gradeadenosarcoma.
Atypical polypoid adenomyomaIn atypical polypoid adenomyoma theglandular component exhibits architec-tural complexity that is usually marked. Itis similar to the corresponding tumourwithin the uterine corpus and usuallyinvolves the lower uterine segment orupper endocervix (see chapter on uter-ine corpus).
Prognosis and predictive factorsSimple polypectomy or local excisionc u res most cervical adenomyomas.H o w e v e r, re c u r rences have beendescribed following local excision, andresidual tumour may be found at hys-terectomy.
Fig. 5.44 Wilms tumour. The tumour is composed of primitive tubules set in a background of renal blastema.
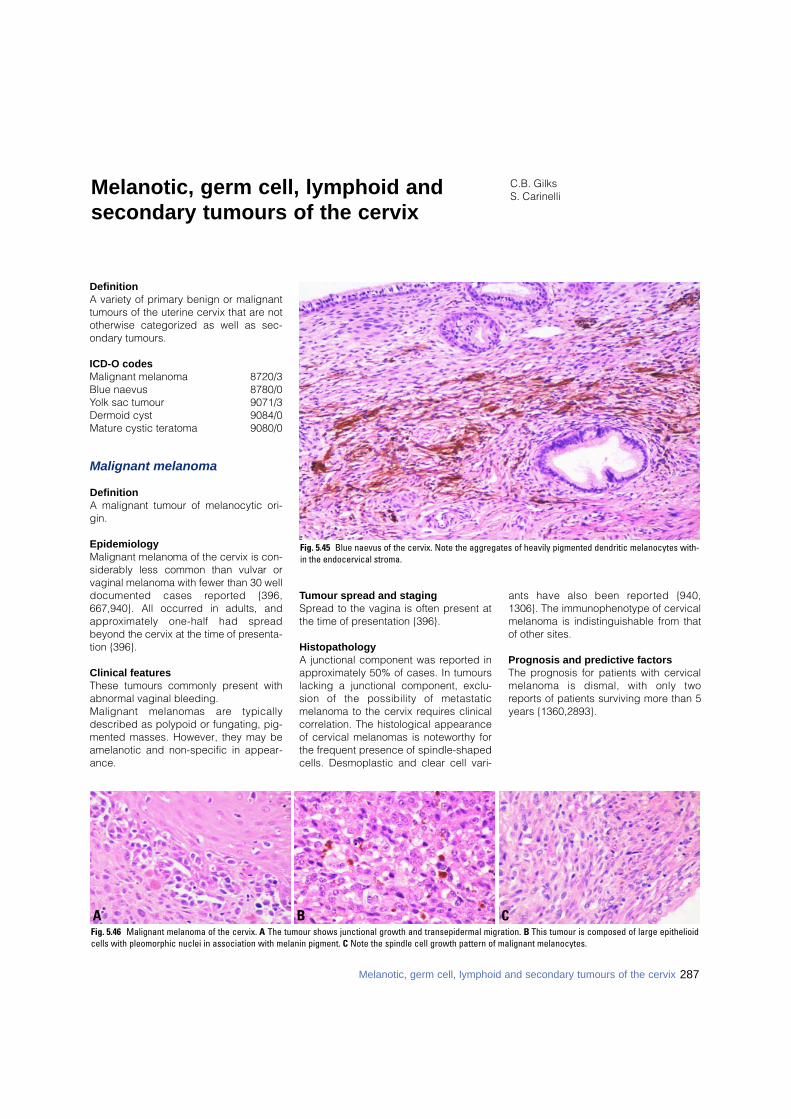
DefinitionA variety of primary benign or malignanttumours of the uterine cervix that are nototherwise categorized as well as sec-ondary tumours.
ICD-O codesMalignant melanoma 8720/3Blue naevus 8780/0Yolk sac tumour 9071/3Dermoid cyst 9084/0Mature cystic teratoma 9080/0
Malignant melanoma
DefinitionA malignant tumour of melanocytic ori-gin.
EpidemiologyMalignant melanoma of the cervix is con-siderably less common than vulvar orvaginal melanoma with fewer than 30 welldocumented cases re p o rted {396,667,940}. All occurred in adults, anda p p roximately one-half had spre a dbeyond the cervix at the time of pre s e n t a-tion {396}.
Clinical featuresThese tumours commonly present withabnormal vaginal bleeding. Malignant melanomas are typicallydescribed as polypoid or fungating, pig-mented masses. However, they may beamelanotic and non-specific in appear-ance.
Tumour spread and stagingSpread to the vagina is often present atthe time of presentation {396}.
HistopathologyA junctional component was reported inapproximately 50% of cases. In tumourslacking a junctional component, exclu-sion of the possibility of metastaticmelanoma to the cervix requires clinicalcorrelation. The histological appearanceof cervical melanomas is noteworthy forthe frequent presence of spindle-shapedcells. Desmoplastic and clear cell vari-
ants have also been re p o rted {940,1306}. The immunophenotype of cervicalmelanoma is indistinguishable from thatof other sites.
Prognosis and predictive factorsThe prognosis for patients with cervicalmelanoma is dismal, with only tworeports of patients surviving more than 5years {1360,2893}.
C.B. GilksS. CarinelliMelanotic, germ cell, lymphoid and
secondary tumours of the cervix
Fig. 5.45 Blue naevus of the cervix. Note the aggregates of heavily pigmented dendritic melanocytes with-in the endocervical stroma.
B CAFig. 5.46 Malignant melanoma of the cervix. A The tumour shows junctional growth and transepidermal migration. B This tumour is composed of large epithelioidcells with pleomorphic nuclei in association with melanin pigment. C Note the spindle cell growth pattern of malignant melanocytes.
287Melanotic, germ cell, lymphoid and secondary tumours of the cervix
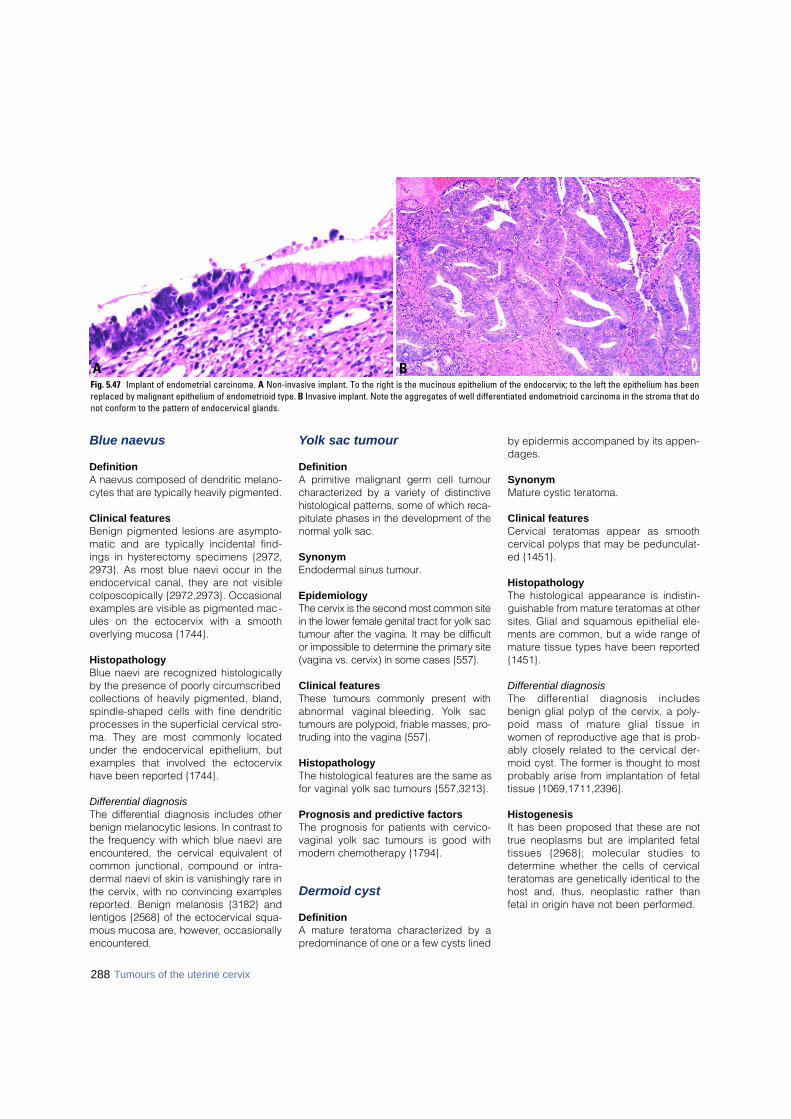
Blue naevus
DefinitionA naevus composed of dendritic melano-cytes that are typically heavily pigmented.
Clinical featuresBenign pigmented lesions are asympto-matic and are typically incidental find-ings in hysterectomy specimens {2972,2973}. As most blue naevi occur in theendocervical canal, they are not visiblecolposcopically {2972,2973}. Occasionalexamples are visible as pigmented mac-ules on the ectocervix with a smoothoverlying mucosa {1744}.
HistopathologyBlue naevi are recognized histologicallyby the presence of poorly circumscribedcollections of heavily pigmented, bland,spindle-shaped cells with fine dendriticprocesses in the superficial cervical stro-ma. They are most commonly locatedunder the endocervical epithelium, butexamples that involved the ectocervixhave been reported {1744}.
Differential diagnosisThe diff e rential diagnosis includes otherbenign melanocytic lesions. In contrast tothe frequency with which blue naevi aree n c o u n t e red, the cervical equivalent ofcommon junctional, compound or intra-d e rmal naevi of skin is vanishingly rare inthe cervix, with no convincing examplesre p o rted. Benign melanosis {3182} andlentigos {2568} of the ectocervical squa-mous mucosa are, however, occasionallye n c o u n t e re d .
Yolk sac tumour
DefinitionA primitive malignant germ cell tumourcharacterized by a variety of distinctivehistological patterns, some of which re c a-pitulate phases in the development of then o rmal yolk sac.
SynonymEndodermal sinus tumour.
EpidemiologyThe cervix is the second most common sitein the lower female genital tract for yolk sactumour after the vagina. It may be diff i c u l tor impossible to determine the primary site(vagina vs. cervix) in some cases {557}.
Clinical featuresThese tumours commonly present witha b n o rmal vaginal bleeding. Yolk sactumours are polypoid, friable masses, pro-truding into the vagina {557}.
HistopathologyThe histological features are the same asfor vaginal yolk sac tumours {557,3213}.
Prognosis and predictive factorsThe prognosis for patients with cervico-vaginal yolk sac tumours is good withmodern chemotherapy {1794}.
Dermoid cyst
DefinitionA mature teratoma characterized by apredominance of one or a few cysts lined
by epidermis accompaned by its appen-dages.
SynonymMature cystic teratoma.
Clinical featuresCervical teratomas appear as smoothcervical polyps that may be pedunculat-ed {1451}.
HistopathologyThe histological appearance is indistin-guishable from mature teratomas at othersites. Glial and squamous epithelial ele-ments are common, but a wide range ofmature tissue types have been reported{1451}.
Differential diagnosisThe diff e rential diagnosis includesbenign glial polyp of the cervix, a poly-poid mass of mature glial tissue inwomen of reproductive age that is prob-ably closely related to the cervical der-moid cyst. The former is thought to mostprobably arise from implantation of fetaltissue {1069,1711,2396}.
HistogenesisIt has been proposed that these are nottrue neoplasms but are implanted fetaltissues {2968}; molecular studies todetermine whether the cells of cervicalteratomas are genetically identical to thehost and, thus, neoplastic rather thanfetal in origin have not been performed.
BAFig. 5.47 Implant of endometrial carcinoma. A Non-invasive implant. To the right is the mucinous epithelium of the endocervix; to the left the epithelium has beenreplaced by malignant epithelium of endometrioid type. B Invasive implant. Note the aggregates of well differentiated endometrioid carcinoma in the stroma that donot conform to the pattern of endocervical glands.
288 Tumours of the uterine cervix
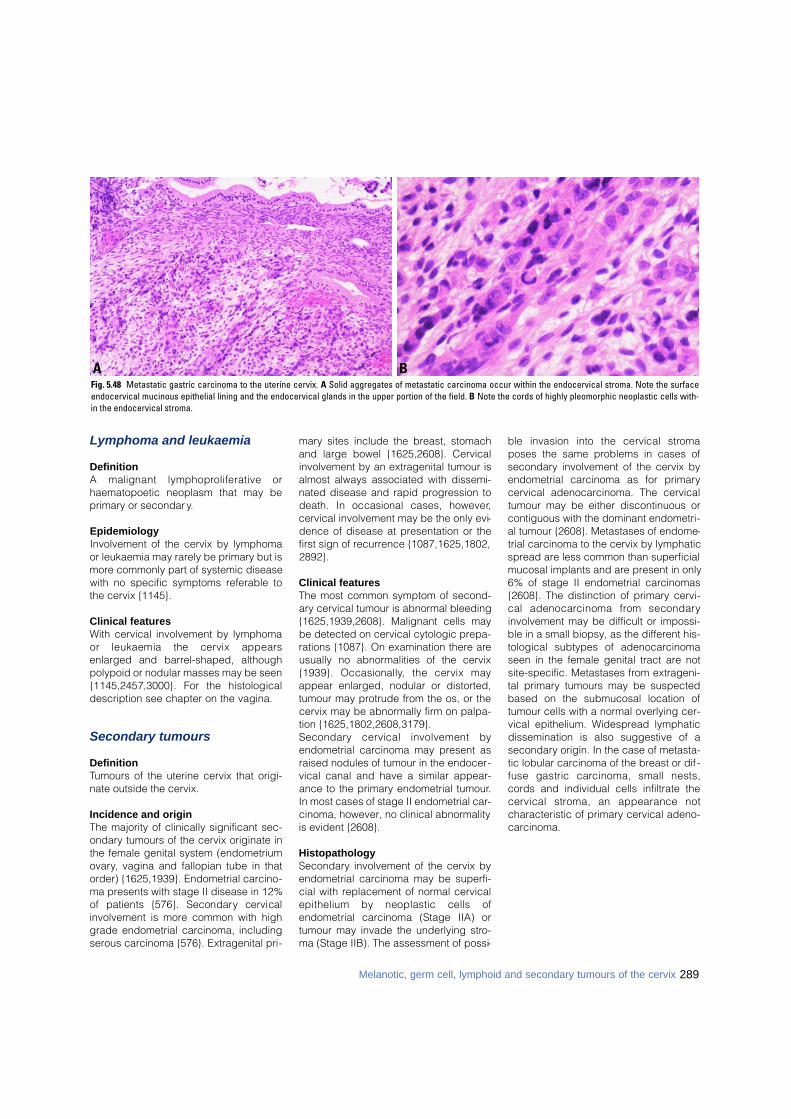
289Melanotic, germ cell, lymphoid and secondary tumours of the cervix
Lymphoma and leukaemia
DefinitionA malignant lymphoproliferative orhaematopoetic neoplasm that may beprimary or secondary.
EpidemiologyInvolvement of the cervix by lymphomaor leukaemia may rarely be primary but ismore commonly part of systemic diseasewith no specific symptoms referable tothe cervix {1145}.
Clinical featuresWith cervical involvement by lymphomaor leukaemia the cervix appearsenlarged and barrel-shaped, althoughpolypoid or nodular masses may be seen{1145,2457,3000}. For the histologicaldescription see chapter on the vagina.
Secondary tumours
Definition Tumours of the uterine cervix that origi-nate outside the cervix.
Incidence and originThe majority of clinically significant sec-ondary tumours of the cervix originate inthe female genital system (endometriumovary, vagina and fallopian tube in thatorder) {1625,1939}. Endometrial carcino-ma presents with stage II disease in 12%of patients {576}. Secondary cervicalinvolvement is more common with highgrade endometrial carcinoma, includingserous carcinoma {576}. Extragenital pri-
mary sites include the breast, stomachand large bowel {1625,2608}. Cervicalinvolvement by an extragenital tumour isalmost always associated with dissemi-nated disease and rapid progression todeath. In occasional cases, however,cervical involvement may be the only evi-dence of disease at presentation or thefirst sign of recurrence {1087,1625,1802,2892}.
Clinical featuresThe most common symptom of second-ary cervical tumour is abnormal bleeding{1625,1939,2608}. Malignant cells maybe detected on cervical cytologic prepa-rations {1087}. On examination there areusually no abnormalities of the cervix{1939}. Occasionally, the cervix mayappear enlarged, nodular or distorted,tumour may protrude from the os, or thecervix may be abnormally firm on palpa-tion {1625,1802,2608,3179}.S e c o n d a ry cervical involvement byendometrial carcinoma may present asraised nodules of tumour in the endocer-vical canal and have a similar appear-ance to the primary endometrial tumour.In most cases of stage II endometrial car-cinoma, however, no clinical abnormalityis evident {2608}.
HistopathologySecondary involvement of the cervix byendometrial carcinoma may be superfi-cial with replacement of normal cervicalepithelium by neoplastic cells ofendometrial carcinoma (Stage IIA) ortumour may invade the underlying stro-ma (Stage IIB). The assessment of possi-
ble invasion into the cervical stro m aposes the same problems in cases ofsecondary involvement of the cervix byendometrial carcinoma as for primarycervical adenocarcinoma. The cervicaltumour may be either discontinuous orcontiguous with the dominant endometri-al tumour {2608}. Metastases of endome-trial carcinoma to the cervix by lymphaticspread are less common than superficialmucosal implants and are present in only6% of stage II endometrial carcinomas{2608}. The distinction of primary cervi-cal adenocarcinoma from secondaryinvolvement may be difficult or impossi-ble in a small biopsy, as the different his-tological subtypes of adenocarcinomaseen in the female genital tract are notsite-specific. Metastases from extrageni-tal primary tumours may be suspectedbased on the submucosal location oftumour cells with a normal overlying cer-vical epithelium. Widespread lymphaticdissemination is also suggestive of asecondary origin. In the case of metasta-tic lobular carcinoma of the breast or dif -fuse gastric carcinoma, small nests,cords and individual cells infiltrate thecervical stroma, an appearance notcharacteristic of primary cervical adeno-carcinoma.
BAFig. 5.48 Metastatic gastric carcinoma to the uterine cervix. A Solid aggregates of metastatic carcinoma occur within the endocervical stroma. Note the surfaceendocervical mucinous epithelial lining and the endocervical glands in the upper portion of the field. B Note the cords of highly pleomorphic neoplastic cells with-in the endocervical stroma.
CHAPTER 6
Tumours of the Vagina
Although the incidence rate of vaginal intraepithelial neoplasiais increasing, that of squamous cell carcinoma is decreasing,reflecting earlier detection and more successful treatment.Human papillomavirus infection is a risk factor for both vaginalintraepithelial neoplasia and squamous cell carcinoma.
In past decades, clear cell adenocarcinoma occurred in youngwomen, about two-thirds of whom had been exposed transpla-centally to diethylstilbestrol. At that time, it was the the mostimportant glandular lesion of the vagina and the second mostcommon epithelial malignancy. The precursor lesion appearsto be atypical adenosis.
The most important non-epithelial tumours are malignantmelanoma and sarcoma botyoides.
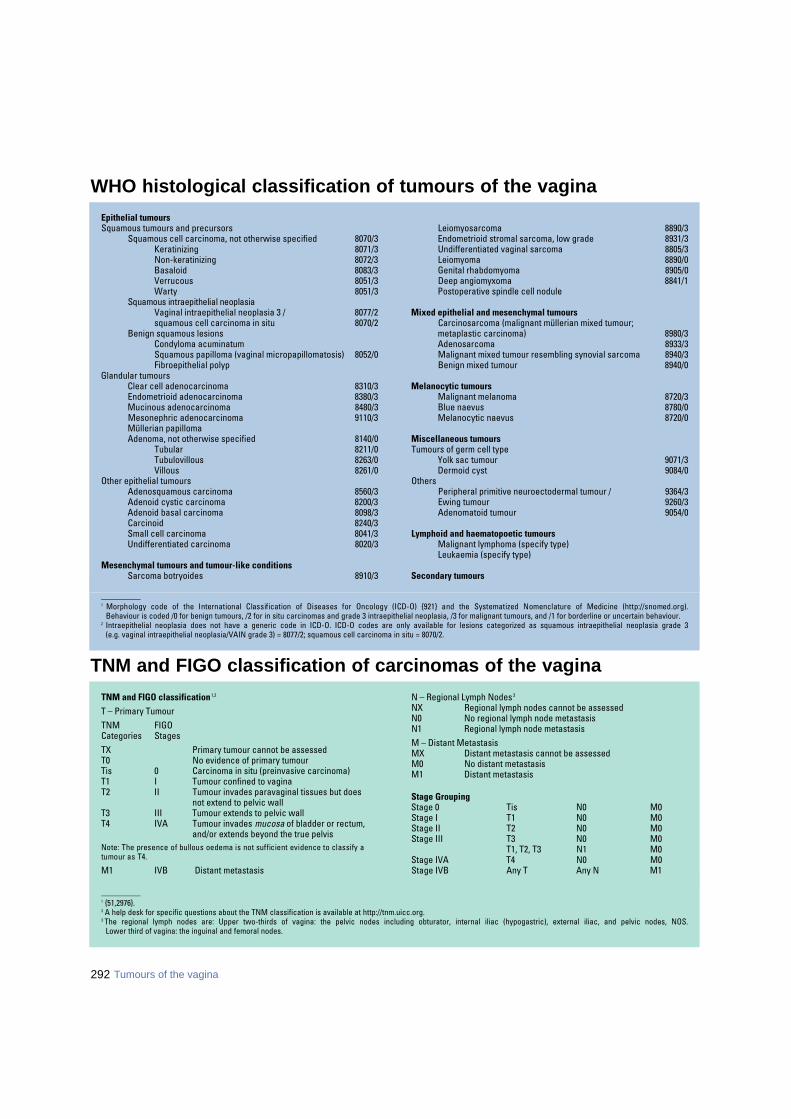
292 Tumours of the vagina
WHO histological classification of tumours of the vagina
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /2 for in situ carcinomas and grade 3 intraepithelial neoplasia, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.2 Intraepithelial neoplasia does not have a generic code in ICD-O. ICD-O codes are only available for lesions categorized as squamous intraepithelial neoplasia grade 3
(e.g. vaginal intraepithelial neoplasia/VAIN grade 3) = 8077/2; squamous cell carcinoma in situ = 8070/2.
Epithelial tumoursSquamous tumours and precursors
Squamous cell carcinoma, not otherwise specified 8070/3Keratinizing 8071/3Non-keratinizing 8072/3Basaloid 8083/3Verrucous 8051/3Warty 8051/3
Squamous intraepithelial neoplasiaVaginal intraepithelial neoplasia 3 / 8077/2squamous cell carcinoma in situ 8070/2
Benign squamous lesionsCondyloma acuminatumSquamous papilloma (vaginal micropapillomatosis) 8052/0Fibroepithelial polyp
Glandular tumoursClear cell adenocarcinoma 8310/3Endometrioid adenocarcinoma 8380/3Mucinous adenocarcinoma 8480/3Mesonephric adenocarcinoma 9110/3Müllerian papillomaAdenoma, not otherwise specified 8140/0
Tubular 8211/0Tubulovillous 8263/0Villous 8261/0
Other epithelial tumoursAdenosquamous carcinoma 8560/3Adenoid cystic carcinoma 8200/3Adenoid basal carcinoma 8098/3Carcinoid 8240/3Small cell carcinoma 8041/3Undifferentiated carcinoma 8020/3
Mesenchymal tumours and tumour-like conditionsSarcoma botryoides 8910/3
Leiomyosarcoma 8890/3Endometrioid stromal sarcoma, low grade 8931/3Undifferentiated vaginal sarcoma 8805/3Leiomyoma 8890/0Genital rhabdomyoma 8905/0Deep angiomyxoma 8841/1Postoperative spindle cell nodule
Mixed epithelial and mesenchymal tumoursCarcinosarcoma (malignant müllerian mixed tumour; metaplastic carcinoma) 8980/3Adenosarcoma 8933/3Malignant mixed tumour resembling synovial sarcoma 8940/3Benign mixed tumour 8940/0
Melanocytic tumoursMalignant melanoma 8720/3Blue naevus 8780/0Melanocytic naevus 8720/0
Miscellaneous tumoursTumours of germ cell type
Yolk sac tumour 9071/3Dermoid cyst 9084/0
OthersPeripheral primitive neuroectodermal tumour / 9364/3Ewing tumour 9260/3Adenomatoid tumour 9054/0
Lymphoid and haematopoetic tumoursMalignant lymphoma (specify type)Leukaemia (specify type)
Secondary tumours
_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org.3 The regional lymph nodes are: Upper two-thirds of vagina: the pelvic nodes including obturator, internal iliac (hypogastric), external iliac, and pelvic nodes, NOS.
Lower third of vagina: the inguinal and femoral nodes.
TNM and FIGO classification 1,2
T – Primary Tumour TNM FIGO Categories StagesTX Primary tumour cannot be assessedT0 No evidence of primary tumourTis 0 Carcinoma in situ (preinvasive carcinoma)T1 I Tumour confined to vaginaT2 II Tumour invades paravaginal tissues but does
not extend to pelvic wallT3 III Tumour extends to pelvic wallT4 IVA Tumour invades mucosa of bladder or rectum,
and/or extends beyond the true pelvisNote: The presence of bullous oedema is not sufficient evidence to classify a tumour as T4.
M1 IVB Distant metastasis
N – Regional Lymph Nodes 3
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Regional lymph node metastasisM – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Stage Grouping Stage 0 Tis N0 M0Stage I T1 N0 M0Stage II T2 N0 M0Stage III T3 N0 M0
T1, T2, T3 N1 M0Stage IVA T4 N0 M0Stage IVB Any T Any N M1
TNM and FIGO classification of carcinomas of the vagina

Squamous tumours
DefinitionPrimary squamous epithelial tumours ofthe vagina are the most frequent neo-plasms at this site. They occur in all agegroups but preferentially in the elderly.Vaginal intraepithelial neoplasia (VAIN) isconsidered a typical, though not obliga-tory, precursor lesion of squamous cellcarcinoma.
ICD-O codesSquamous cell carcinoma 8070/3Vaginal intraepithelial neoplasia
(VAIN), grade 3 8077/2Squamous cell carcinoma in situ 8070/2
Squamous papilloma 8052/0
Squamous cell carcinoma
DefinitionAn invasive carcinoma composed ofsquamous cells of varying degrees ofd i ff e rentiation. According to theI n t e rnational Federation of Gynaecologyand Obstetrics (FIGO), a tumour of thevagina involving the uterine cervix or thevulva should be classified as a primarycervical or vulvar cancer, re s p e c t i v e l y.A d d i t i o n a l l y, before the diagnosis of ap r i m a ry vaginal carcinoma can beestablished, a 5-10 year disease fre e
interval is re q u i red to rule out re c u r re n tdisease in those patients with a priorp reinvasive or invasive cervical or vulvarneoplasm.
EpidemiologySquamous cell carcinoma comprises upto 85% of vaginal carcinomas andaccounts for 1-2% of all malignanttumours of the female genital tract {634,1193}. The mean age of patients is about60 years.
AetiologyIn squamous cell carcinoma persistentinfection with high-risk human papillo-mavirus (HPV) is probably a major aetio-logical factor. The same risk factors areobserved as for vaginal intraepithelialneoplasia (VAIN), i.e. previous preinva-sive or invasive disease of the lower gen-ital tract, immunosuppression and priorpelvic irradiation {303}. The developmentof VAIN and eventual progression to inva-sive disease is most likely, though theprogression rate is unknown {347}.Prior pelvic irradiation is a predisposingfactor for vaginal squamous carcinoma{303,748,3075}. Simultaneous or priorp reinvasive or invasive disease else-w h e re in the lower genital tract isobserved in up to 30% of cases{220,2227,2480}.
Clinical featuresSigns and symptomsThe commonest symptom is a bloodyvaginal discharge. Nearly 75% ofpatients present with painless bleeding,u r i n a ry tract symptoms or postcoitalbleeding; however, the patient may becompletely asymptomatic. Pelvic painand dysuria usually signify advanceddisease {2499}. Most cases occur in theupper third of the vagina and are locatedon the posterior wall {2265}.
Imaging Magnetic resonance imaging (MRI) ofthe pelvis can be used to image vaginaltumours as well as to assess whetherpelvic or inguinal lymphadenopathy ispresent. The MRI appearance, however,is not specific, and inflammatorychanges and congestion of the vaginamay mimic vaginal carcinoma {439}.
Exfoliative cytologyOccasionally, cancer cells of vaginal ori-gin may be observed in cervical smears.
MacroscopyTumours may be exophytic, ulcerative orannular and constricting. The lesionsvary in size from being undetectable togreater than 10 cm. They may be poly-poid, sessile, indurated, ulcerated or fun-
E.S. Andersen A.G. HanselaarJ. Paavonen C. BergeronM. Murnaghan S.P. DobbsA.G. Östör
Epithelial tumours
BAFig. 6.01 Squamous cell carcinoma. A Keratinizing type. Carcinoma arises from the surface epithelium and forms several keratin pearls. B Non-keratinizing type. The neo-plasm forms prominent squamous pearls with little keratinization.
293Epithelial tumours

gating and may be found anywhere with-in the vagina. Squamous cell carcinoma,the commonest vaginal carcinoma, isulcerative in half of cases, exophytic in athird and annular and constricting in theremainder.
Tumour spread and stagingSquamous cell carcinoma spreads pre-dominantly laterally to the paravaginaland parametrial tissues when located inthe lower and upper vagina, respectively.Tumours also invade lymphatics, metas-tasizing to regional lymph nodes andeventually distant sites including the
lungs, liver and brain. The staging ofvaginal tumours is by the TNM/FIGOclassification {51,2976}. Appro x i m a t e l y25% of patients present with stage I dis-ease, one-third with stage II disease and40% with stage III or IV disease {220,748,1245,1524,2301,2480}.
HistopathologyVaginal squamous cell carcinoma hasthe same histological characteristics assuch tumours in other sites. Most casesare moderately differentiated and non-keratinizing {2301}. Rarely, the tumourshave spindle-cell features {2778}. Wartycarcinoma is another variant of vaginalsquamous cell carcinoma {2339}. Thetumour is papillary with hyperkeratoticepithelium. Nuclear enlargement andkoilocytosis with hyperchromasia, wrin-kling of the nuclear membrane and mult-inucleation are typical changes {1541,2936}. Verrucous carcinoma has a papil-lary growth pattern with pushing bordersand bulbous pegs of acanthotic epitheli-um with little or no atypia and surfacematuration in the form of parakeratosisand hyperkeratosis. For a more detaileddiscussion of the subypes of squamouscell carcinoma see chapter 5 or 7.
Prognosis and predictive factorsRadiation is the preferred treatment formost cases of vaginal carcinoma {1524,2217,2981}. In Stage I disease located inthe upper part of the vagina, a radicalhysterectomy, pelvic lymphadenectomyand partial vaginectomy may be consid-ered {55,171}. Otherwise, radiation thera-py given as intracavitary therapy, intersti-tial implants and/or extern a lpelvic/inguinal radiation, often in combi-nation, is the most frequently adoptedmodality {1524,2217}. In tumours of the
middle or lower third of the vagina theexternal radiation field should include theinguinal and femoral lymph nodes. The clinical stage is the most significantp rognostic factor {220,748,1245,1524,2301,2480}. Recurrences are typicallylocal and usually happen within 2 yearsof treatment. The five-year survival ratesare 70% for stage I, 45% for stage II,30% for stage III and 15% for stage IV.The overall 5-year survival is about 42%{220,748,1245,1524,2301,2480}.Tumour localization, grade or keratiniza-tion or patient age has not been demon-strated to have prognostic significance.
Vaginal intraepithelial neoplasia
DefinitionA premalignant lesion of the vaginalsquamous epithelium that can developprimarily in the vagina or as an extensionfrom the cervix. VAIN is often a manifes-tation of the so-called lower genital tractneoplastic syndrome. Histologically,VAIN is defined in the same way as cer-vical intraepithelial neoplasia (CIN).
SynonymsDysplasia/carcinoma in situ, squamousintraepithelial lesion.
EpidemiologyVAIN is much less common than CIN,though its true incidence is unknown.T h e re is some evidence that the inci-dence of VAIN has increased in re c e n tdecades, particularly among young andi m m u n o s u p p ressed women. The meanage for patients with VAIN is appro x i m a t e-ly 50 years. The majority of VAIN casesoccur in women who have had a priorh y s t e rectomy or who have a history ofcervical or vulvar neoplasia {1626, 2403}.
Table 6.01Terminology of premalignant vaginal squamous epithelial lesions.
Fig. 6.02 Vaginal intraepithelial neoplasia, grade 2.Nuclear features of intraepithelial neoplasia are evi-dent in the lower two-thirds of the squamous epithe-lium with overlying parakeratosis.
Classification Synonyms
Vaginal intraepithelial Mild dysplasia Low grade VAINneoplasia, grade 1
Vaginal intraepithelial Moderate dysplasia High grade VAINneoplasia, grade 2
Vaginal intraepithelial Severe dysplasia High grade VAINneoplasia, grade 3 and carcinoma in situ
VAIN = vaginal intraepithelial neoplasia
Fig. 6.03 Vaginal intraepithelial neoplasia, grade3.The upper portion of the epithelium is covered byhyperkeratosis. The remaining cells are character-ized by nuclear enlargement and pleomorphism.
294 Tumours of the vagina
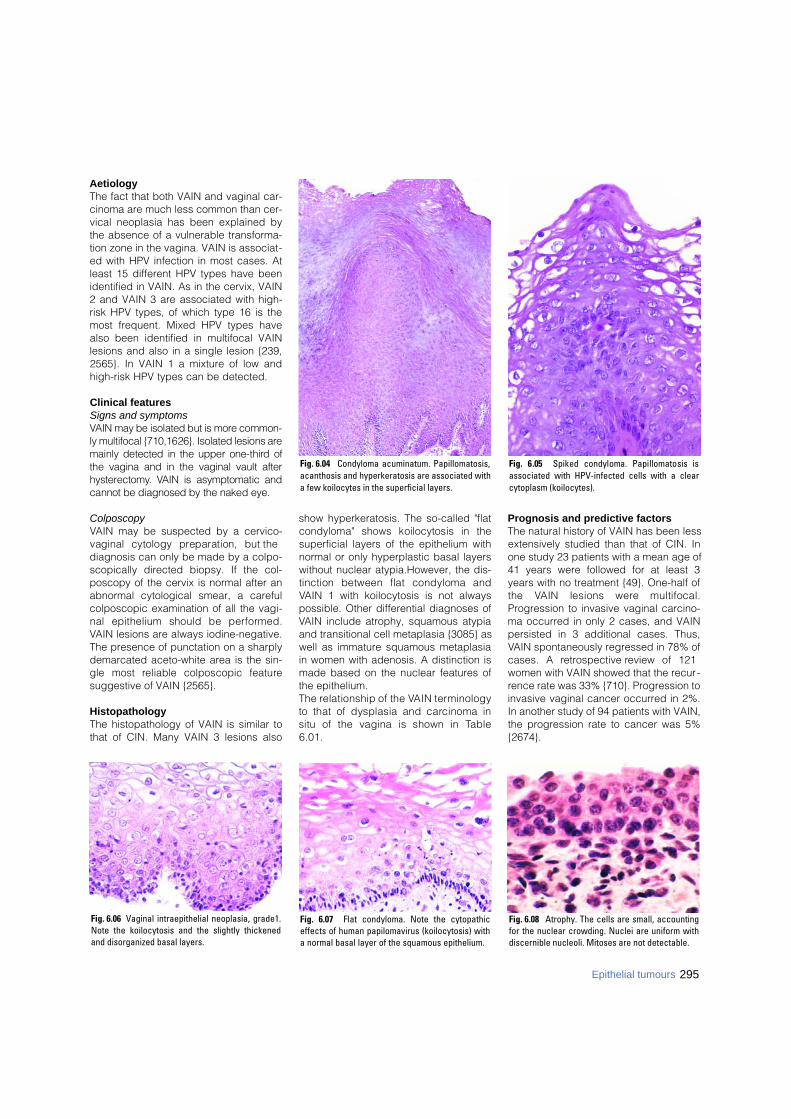
AetiologyThe fact that both VAIN and vaginal car-cinoma are much less common than cer-vical neoplasia has been explained bythe absence of a vulnerable transforma-tion zone in the vagina. VAIN is associat-ed with HPV infection in most cases. Atleast 15 different HPV types have beenidentified in VAIN. As in the cervix, VAIN2 and VAIN 3 are associated with high-risk HPV types, of which type 16 is themost frequent. Mixed HPV types havealso been identified in multifocal VAINlesions and also in a single lesion {239,2565}. In VAIN 1 a mixture of low andhigh-risk HPV types can be detected.
Clinical featuresSigns and symptomsVAIN may be isolated but is more common-ly multifocal {710,1626}. Isolated lesions aremainly detected in the upper one-third ofthe vagina and in the vaginal vault afterh y s t e re c t o m y. VAIN is asymptomatic andcannot be diagnosed by the naked eye.
ColposcopyVAIN may be suspected by a cervico-vaginal cytology preparation, but thediagnosis can only be made by a colpo-scopically directed biopsy. If the col-poscopy of the cervix is normal after anabnormal cytological smear, a carefulcolposcopic examination of all the vagi-nal epithelium should be perf o rm e d .VAIN lesions are always iodine-negative.The presence of punctation on a sharplydemarcated aceto-white area is the sin-gle most reliable colposcopic featuresuggestive of VAIN {2565}.
HistopathologyThe histopathology of VAIN is similar tothat of CIN. Many VAIN 3 lesions also
show hyperkeratosis. The so-called "flatcondyloma" shows koilocytosis in thesuperficial layers of the epithelium withnormal or only hyperplastic basal layerswithout nuclear atypia.However, the dis-tinction between flat condyloma andVAIN 1 with koilocytosis is not alwayspossible. Other differential diagnoses ofVAIN include atrophy, squamous atypiaand transitional cell metaplasia {3085} aswell as immature squamous metaplasiain women with adenosis. A distinction ismade based on the nuclear features ofthe epithelium. The relationship of the VAIN term i n o l o g yto that of dysplasia and carcinoma insitu of the vagina is shown in Ta b l e6 . 0 1 .
Prognosis and predictive factorsThe natural history of VAIN has been lessextensively studied than that of CIN. Inone study 23 patients with a mean age of41 years were followed for at least 3years with no treatment {49}. One-half ofthe VAIN lesions were multifocal.Progression to invasive vaginal carcino-ma occurred in only 2 cases, and VAINpersisted in 3 additional cases. Thus,VAIN spontaneously regressed in 78% ofcases. A re t rospective review of 121women with VAIN showed that the recur-rence rate was 33% {710}. Progression toinvasive vaginal cancer occurred in 2%.In another study of 94 patients with VAIN,the progression rate to cancer was 5%{2674}.
Fig. 6.06 Vaginal intraepithelial neoplasia, grade1.Note the koilocytosis and the slightly thickenedand disorganized basal layers.
Fig. 6.04 Condyloma acuminatum. Papillomatosis,acanthosis and hyperkeratosis are associated witha few koilocytes in the superficial layers.
Fig. 6.05 Spiked condyloma. Papillomatosis isassociated with HPV-infected cells with a clearcytoplasm (koilocytes).
Fig. 6.07 Flat condyloma. Note the cytopathiceffects of human papilomavirus (koilocytosis) witha normal basal layer of the squamous epithelium.
Fig. 6.08 Atrophy. The cells are small, accountingfor the nuclear crowding. Nuclei are uniform withdiscernible nucleoli. Mitoses are not detectable.
295Epithelial tumours
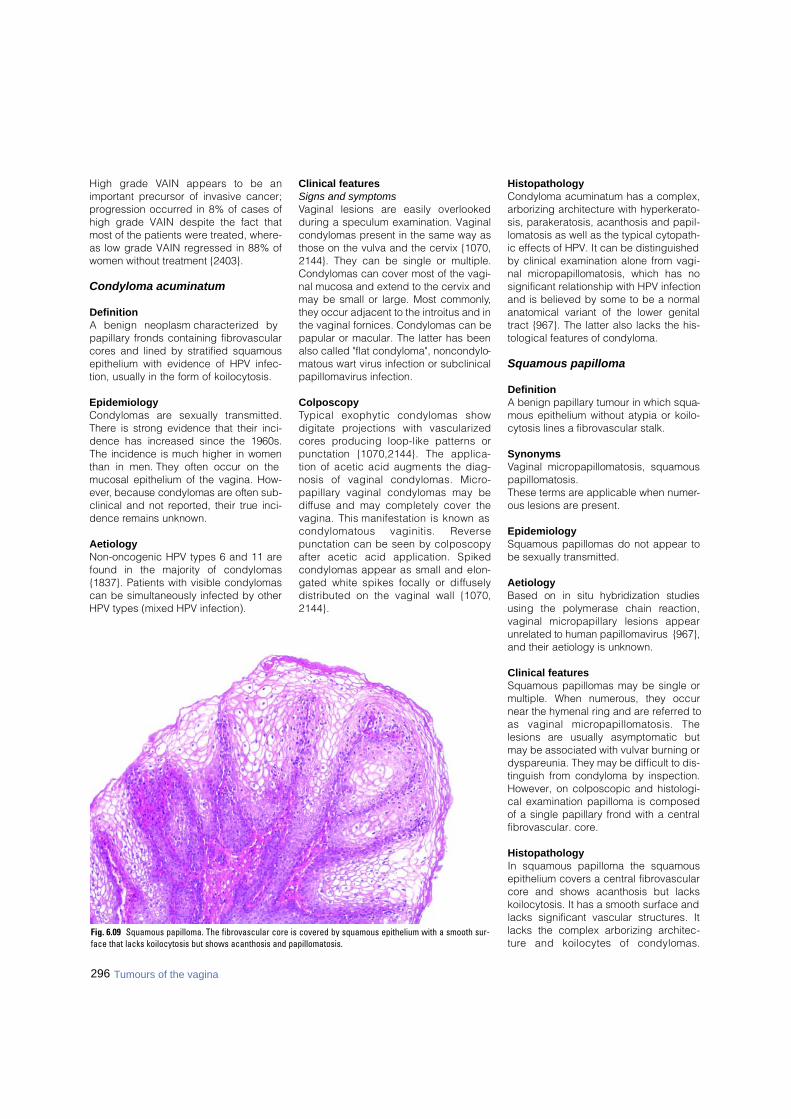
296 Tumours of the vagina
High grade VAIN appears to be animportant precursor of invasive cancer;progression occurred in 8% of cases ofhigh grade VAIN despite the fact thatmost of the patients were treated, where-as low grade VAIN regressed in 88% ofwomen without treatment {2403}.
Condyloma acuminatum
DefinitionA benign neoplasm characterized bypapillary fronds containing fibrovascularcores and lined by stratified squamousepithelium with evidence of HPV infec-tion, usually in the form of koilocytosis.
EpidemiologyCondylomas are sexually transmitted.T h e re is strong evidence that their inci-dence has increased since the 1960s.The incidence is much higher in womenthan in men. They often occur on themucosal epithelium of the vagina. How-e v e r, because condylomas are often sub-clinical and not re p o rted, their true inci-dence remains unknown.
AetiologyNon-oncogenic HPV types 6 and 11 arefound in the majority of condylomas{1837}. Patients with visible condylomascan be simultaneously infected by otherHPV types (mixed HPV infection).
Clinical featuresSigns and symptomsVaginal lesions are easily overlookedduring a speculum examination. Vaginalcondylomas present in the same way asthose on the vulva and the cervix {1070,2144}. They can be single or multiple.Condylomas can cover most of the vagi-nal mucosa and extend to the cervix andmay be small or large. Most commonly,they occur adjacent to the introitus and inthe vaginal fornices. Condylomas can bepapular or macular. The latter has beenalso called "flat condyloma", noncondylo-matous wart virus infection or subclinicalpapillomavirus infection.
ColposcopyTypical exophytic condylomas showdigitate projections with vascularizedc o res producing loop-like patterns orpunctation {1070,2144}. The applica-tion of acetic acid augments the diag-nosis of vaginal condylomas. Micro -p a p i l l a ry vaginal condylomas may bed i ffuse and may completely cover thevagina. This manifestation is known ascondylomatous vaginitis. Reversepunctation can be seen by colposcopyafter acetic acid application. Spikedcondylomas appear as small and elon-gated white spikes focally or diff u s e l ydistributed on the vaginal wall {1070,2 1 4 4 } .
Histopathology Condyloma acuminatum has a complex,arborizing architecture with hyperkerato-sis, parakeratosis, acanthosis and papil-lomatosis as well as the typical cytopath-ic effects of HPV. It can be distinguishedby clinical examination alone from vagi-nal micropapillomatosis, which has nosignificant relationship with HPV infectionand is believed by some to be a normalanatomical variant of the lower genitaltract {967}. The latter also lacks the his-tological features of condyloma.
Squamous papilloma
DefinitionA benign papillary tumour in which squa-mous epithelium without atypia or koilo-cytosis lines a fibrovascular stalk.
SynonymsVaginal micropapillomatosis, squamouspapillomatosis.These terms are applicable when numer-ous lesions are present.
EpidemiologySquamous papillomas do not appear tobe sexually transmitted.
AetiologyBased on in situ hybridization studiesusing the polymerase chain re a c t i o n ,vaginal micro p a p i l l a ry lesions appearu n related to human papillomavirus {967},and their aetiology is unknown.
Clinical features Squamous papillomas may be single ormultiple. When numerous, they occurnear the hymenal ring and are referred toas vaginal micropapillomatosis. Thelesions are usually asymptomatic butmay be associated with vulvar burning ordyspareunia. They may be difficult to dis-tinguish from condyloma by inspection.However, on colposcopic and histologi-cal examination papilloma is composedof a single papillary frond with a centralfibrovascular. core.
HistopathologyIn squamous papilloma the squamousepithelium covers a central fibrovascularcore and shows acanthosis but lackskoilocytosis. It has a smooth surface andlacks significant vascular structures. Itlacks the complex arborizing architec-t u re and koilocytes of condylomas.
Fig. 6.09 Squamous papilloma. The fibrovascular core is covered by squamous epithelium with a smooth sur-face that lacks koilocytosis but shows acanthosis and papillomatosis.

297Epithelial tumours
However, it is important to note that theremay be a time during the evolution ofcondylomas when koilocytes are not eas-ily identifiable.
Fibroepithelial polyp
DefinitionA polyp lined by squamous epitheliumthat contains a central core of fibrous tis-sue in which stellate cells with taperingcytoplasmic processes and irregularlyshaped thin-walled vessels are promi-nent features.
SynonymStromal polyp.
Clinical featuresThis lesion can occur at any age but hasa predilection for pregnant women.
MacroscopyThese are polypoid lesions, usually solitary.
HistopathologyThese polypoid lesions are characterizedby a prominent fibrovascular stroma cov-e red by squamous epithelium {380}.They lack epithelial acanthosis and pap-illary architecture. Bizarre stromal cells,marked hypercellularity and elevatedmitotic counts including atypical formshave been described that can lead to anerroneous diagnosis of sarcoma botry-oides, but a cambium layer and rhab-domyoblasts are absent, and mitoticactivity is typically low {2067}.
Glandular tumours and theirprecursors
ICD-O codesAdenocarcinoma, NOS 8140/3
Clear cell adenocarcinoma 8310/3Endometrioid adenocarcinoma 8380/3
Mucinous adenocarcinoma 8480/3 Mesonephric adenocarcinoma 9110/3
Adenoma, NOS 8140/0Tubular 8211/0Tubulovillous 8263/0Villous 8261/0
Clear cell adenocarcinoma
DefinitionAn invasive neoplasm with an epithelialcomponent that contains one or more celltypes, most commonly clear cells andhobnail cells, but flat and/or eosinophiliccells may, on occasion, pre d o m i n a t e .
EpidemiologyThe occurrence of cases of vaginal clearcell adenocarcinoma associated with inu t e ro exposure to diethylstilbestrol (DES)was responsible for an increase in inci-dence of adenocarcinoma in youngwomen from the 1970s {1194}. In the early1970s the peak incidence of clear cella d e n o c a rcinoma was around 19 years,the youngest patient being 8 years. Withthe ageing of the DES-exposed cohort ,the peak incidence has been shiftingt o w a rds an older age group.
Aetiology
DES was prescribed for threatened orrepeated abortions from the 1940s to theearly 1970s. Millions of women wereexposed in utero to this and related drugs
in several countries, including the UnitedStates, France and the Netherlands{2946}. DES is a teratogen and causes avariety of congenital abnormalities of thelower genital tract in about 30% of thefemale offspring {1883}. The absolute riskof clear cell adenocarcinoma of the vagi-na or cervix is estimated at 1:1000{1843}. About two-thirds of the cases ofclear cell adenocarcinoma occurring inindividuals under the age of 40 are linkedto transplacental DES exposure. DESinhibits the development of uro g e n i t a lsinus-derived squamous epithelium thatis destined to become vaginal epitheliumand normally grows up to the junction ofthe ectocervix and endocervix, re p l a c i n gthe pre-existing müllerian-derived colum-nar epithelium. The embryonic müllerianepithelium that is not replaced persistsand develops into adenosis. Adenosis isfound immediately adjacent to the tumourin over 90% of cases and is thought to bethe precursor of clear cell adenocarc i n o-ma. The rarity of clear cell adenocarc i n o-ma in the exposed population suggeststhat DES is an incomplete carcinogen orthat susceptibility factors are necessaryfor it to produce neoplastic transform a-tion. Genetic factors and hormonal dis-ruption by environmental toxins are impli-cated. A maternal history of prior sponta-neous abortion increases the risk of clearcell adenocarcinoma {2161}. Endoge-nous estrogens probably also play a ro l e ,
Fig. 6.11 Fibroepithelial polyp. A This polypoid lesion is composed of stroma and covered by squamousepthelium. B The stroma contains scattered bizarre multinucleated giant cells.
A B
Fig. 6.10 Fibroepithelial polyp.A multilobulated poly-poid lesion arises from the vaginal wall.

since most cases of clear cell adenocar-cinoma are first detected around the timeof pubert y.
LocalizationWhilst any part of the vagina may beinvolved, clear cell adenocarcinoma mostoften arises from its upper part. A primaryvaginal clear cell adenocarcinoma mayalso involve the cervix. According to FIGOcriteria about two-thirds of clear cell ade-n o c a rcinomas after DES exposure areclassified as tumours of the vagina ando n e - t h i rd of the cervix {1131}. In non-DESexposed young women and post-menopausal women this ratio is re v e r s e d.
Clinical featuresVaginal bleeding, discharge and dys-p a reunia are the most common symp-toms, but women may be asymptomatic.A b n o rmal cytologic findings may lead to
detection, but care must be taken tosample the vagina as well as the cervixsince cervical smears are re l a t i v e l yinsensitive for the detection of clear cella d e n o c a rcinoma {1132}.Clear cell adenocarcinomas typicallya re polypoid, nodular, or papillary butmay also be flat or ulcerated. Someclear cell adenocarcinomas are con-fined to the superficial stroma andmay remain undetected for a long time{1131,2386}. Such small tumours maybe invisible on macroscopic or even col-poscopic examination and are onlydetected by palpation or when tumourcells are shed through the mucosa anddetected by exfoliative cytology. Largetumours may be up to 10 cm in diameter.
HistopathologyClear cell adenocarcinoma of the vaginahas an appearance similar to those aris-
ing in the cervix, endometrium and ovary.Clear cell adenocarcinomas may showseveral growth patterns; the most com-mon pattern is tubulocystic, but it alsomay be solid or mixed. A papillary growthpattern is seldom predominant. The maincell types are clear cells and hobnailcells. The appearance of the clear cellsis due to the presence of abundant intra-cytoplasmic glycogen. Hobnail cells arecharacterized by inconspicuous cyto-plasm and a bulbous nucleus that pro-trudes into glandular lumens. The tumourcells may also be flat with bland nucleiand scant cytoplasm in cystic areas orhave granular eosinophilic cytoplasmwithout glycogen. The nuclei vary con-siderably in appearance. They may besignificantly enlarged with multiple irreg-ular nucleoli in clear and hobnail cells, orthey may have fine chromatin and incon-spicuous nucleoli in flat cells. The num-
BAFig. 6.13 Clear cell adenocarcinoma. A Note the neoplastic tubules lined by hobnail cells on the right and adenosis of the tuboendometrial type on the left. B Cytologicalpreparation shows hobnail cells with anisonucleosis, unevenly distributed chromatin, nucleoli and vacuolated cytoplasm.
BAFig. 6.12 Adenosis of the vagina. A By colposcopy red granular areas of adenosis are apparent. B Colposcopy after iodine application. The areas of adenosis do notstain.
298 Tumours of the vagina

ber of mitoses varies but is usually lessthan 10 per 10 high power fields.Psammoma and intracellular hyalinebodies may occasionally be encoun-tered.
Cytopathology In cytological preparations the malignantcells may occur singly or in clusters andresemble large endocervical or endome-trial cells. Typically, the nuclei are largewith one or more prominent nucleoli.Nuclei may be bizarre. The bland cyto-logical features of tumours that show onlymild nuclear atypia may, however, ham-per cytological detection.
Prognosis and predictive factorsClear cell adenocarcinoma may be treat-ed by radical hysterectomy, vaginectomyand lymphadenectomy or by externalbeam or local radiotherapy. The tumourspreads primarily by local invasion andlymphatic metastases and has a recur-rence rate of 25%. The incidence oflymph node disease increases dramati-cally with tumour invasion beyond 3 mmin depth. Lymph node metastases occurin 16% of patients with stage I diseaseand 50% of those with stage II disease.Haematogenous metastasis to distantorgans occurs mainly to the lungs. The 5-year survival of patients with tumours ofall stages is approximately 80% and isclose to 100% for patients with stage Itumours. Most recurrences occur within 3years. Long disease-free intervals ofmore than 20 years have been observed.Factors associated with a favourableprognosis are: low stage, small tumoursize, a tubulocystic pattern, low mitoticactivity and mild nuclear atypia.
Adenosis
DefinitionAdenosis is the presence of glandularepithelium in the vagina and is thought tobe the result of the persistence of embry-onic müllerian epithelium.
EpidemiologyAdenosis has been reported to occur inapproximately 30% of women after inu t e ro exposure to DES. Congenitaladenosis may be present in up to 8% ofunexposed women. Adenosis has beendescribed after laser vaporization orintravaginal application of 5-fluorouracil{730}.
LocalizationThe most frequent site of involvement isthe anterior upper third of the vagina.
Clinical featuresSigns and symptomsAdenosis is usually asymptomatic. Somewomen present with a mucous dis-charge, bleeding or dyspare u n i a . .Adenosis may spontaneously regress atthe surface and be replaced by meta-plastic squamous epithelium, particularlywith increasing age. Because of the riskof development of clear cell adenocarci-noma within the vaginal wall, palpation,colposcopic examination and cytologicalsmears are necessary to monitor patientswith adenosis.
ColposcopyAreas of adenosis and associated squa-mous metaplasia may be visible colpo-scopically and by iodine staining {2046}.Adenosis may be occult or may presentas cysts or as a diffusely red granulararea.
CytologyCytology can be helpful in the diagnosticevaluation of DES-exposed women (seebelow). It may serve a dual purpose, as ameans for detection of adenocarcinomaor as a follow-up procedure after treat-ment of the lesion.
Adenosis can be detected on cytologicalexamination by the finding of columnar ormetaplastic squamous cells in scrapesof the middle and upper third of the vagi-na. However, similar findings may occurin non-DES-exposed women as a resultof contamination of the vaginal specimenby columnar or metaplastic squamouscells from the cervix.
HistopathologyAdenosis is characterized by the pres-ence in the vagina of columnar epitheli-um resembling mucinous epithelium ofthe endocervix (mucinous type) and/orthe endometrium or the fallopian tube(tuboendometrial type). Adenosis maybe found on the surface or deeper in thestroma. Mixtures of the various types ofadenosis may be encountere d .Squamous metaplasia may occur as aresult of healing.
Atypical adenosis
DefinitionAtypical adenosis is the presence ofatypical glandular epithelium in the vagi-na. It is reported to be a precursor lesionof clear cell adenocarcinoma.
HistopathologyAtypical adenosis occurs in the tuboen-dometrial type of adenosis and is a fre-
299Epithelial tumours
Fig. 6.15 Submucosal atypical adenosis of the vagi-na. Note the nuclear enlargement and atypia in theglands.
Fig. 6.14 Adenosis of the vagina. A Note the tubo-endometrioid type glands. B On the surface withinadenosis is a focus of squamous metaplasia .
A
B
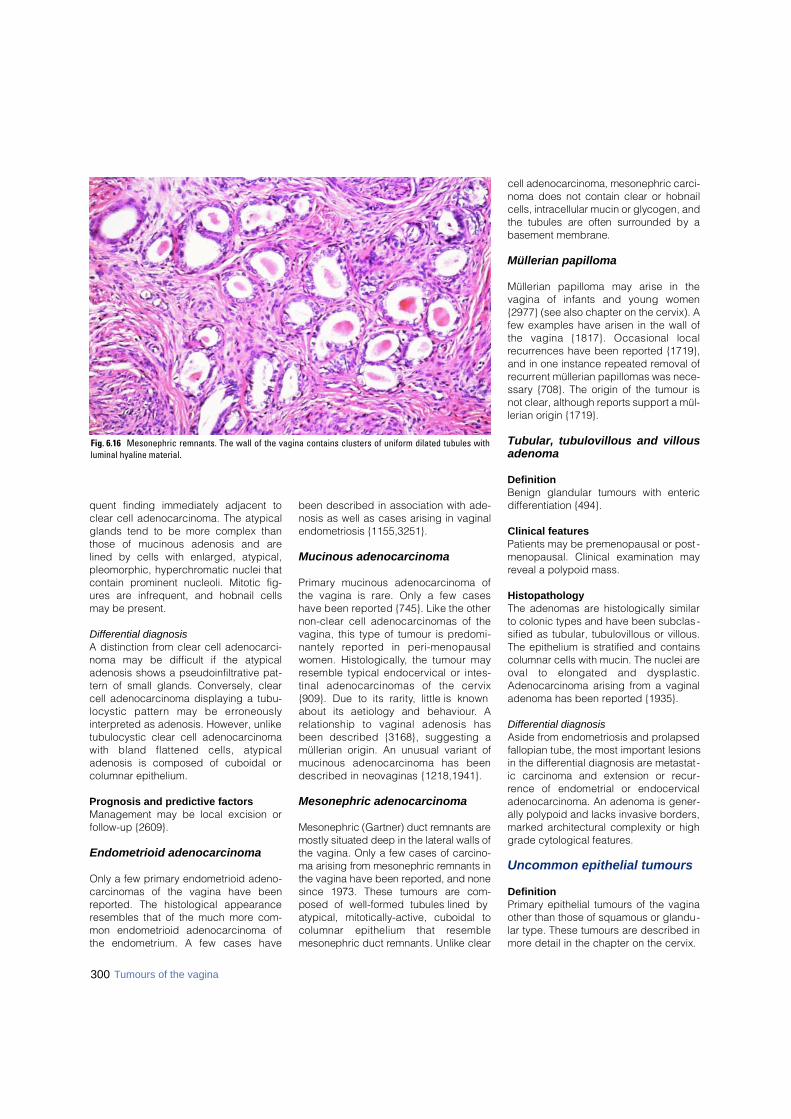
300 Tumours of the vagina
quent finding immediately adjacent toclear cell adenocarcinoma. The atypicalglands tend to be more complex thanthose of mucinous adenosis and arelined by cells with enlarged, atypical,pleomorphic, hyperchromatic nuclei thatcontain prominent nucleoli. Mitotic fig-ures are infrequent, and hobnail cellsmay be present.
Differential diagnosisA distinction from clear cell adenocarci-noma may be difficult if the atypicaladenosis shows a pseudoinfiltrative pat-tern of small glands. Conversely, clearcell adenocarcinoma displaying a tubu-locystic pattern may be erro n e o u s l yinterpreted as adenosis. However, unliketubulocystic clear cell adenocarcinomawith bland flattened cells, atypicaladenosis is composed of cuboidal orcolumnar epithelium.
Prognosis and predictive factors Management may be local excision orfollow-up {2609}.
Endometrioid adenocarcinoma
Only a few primary endometrioid adeno-carcinomas of the vagina have beenreported. The histological appearanceresembles that of the much more com-mon endometrioid adenocarcinoma ofthe endometrium. A few cases have
been described in association with ade-nosis as well as cases arising in vaginalendometriosis {1155,3251}.
Mucinous adenocarcinoma
P r i m a ry mucinous adenocarcinoma ofthe vagina is rare. Only a few caseshave been re p o rted {745}. Like the othernon-clear cell adenocarcinomas of thevagina, this type of tumour is pre d o m i-nantely re p o rted in peri-menopausalwomen. Histologically, the tumour mayresemble typical endocervical or intes-tinal adenocarcinomas of the cervix{909}. Due to its rarity, little is knownabout its aetiology and behaviour. Arelationship to vaginal adenosis hasbeen described {3168}, suggesting amüllerian origin. An unusual variant ofmucinous adenocarcinoma has beendescribed in neovaginas {1218,1941}.
Mesonephric adenocarcinoma
Mesonephric (Gartner) duct remnants aremostly situated deep in the lateral walls ofthe vagina. Only a few cases of carc i n o-ma arising from mesonephric remnants inthe vagina have been re p o rted, and nonesince 1973. These tumours are com-posed of well-formed tubules lined byatypical, mitotically-active, cuboidal tocolumnar epithelium that re s e m b l emesonephric duct remnants. Unlike clear
cell adenocarcinoma, mesonephric carc i-noma does not contain clear or hobnailcells, intracellular mucin or glycogen, andthe tubules are often surrounded by abasement membrane.
Müllerian papilloma
Müllerian papilloma may arise in thevagina of infants and young women{2977} (see also chapter on the cervix). Afew examples have arisen in the wall ofthe vagina {1817}. Occasional localrecurrences have been reported {1719},and in one instance repeated removal ofrecurrent müllerian papillomas was nece-ssary {708}. The origin of the tumour isnot clear, although reports support a mül-lerian origin {1719}.
Tubular, tubulovillous and villousadenoma
DefinitionBenign glandular tumours with entericdifferentiation {494}.
Clinical featuresPatients may be premenopausal or post -menopausal. Clinical examination mayreveal a polypoid mass.
HistopathologyThe adenomas are histologically similarto colonic types and have been subclas-sified as tubular, tubulovillous or villous.The epithelium is stratified and containscolumnar cells with mucin. The nuclei areoval to elongated and dysplastic.Adenocarcinoma arising from a vaginaladenoma has been reported {1935}.
Differential diagnosisAside from endometriosis and prolapsedfallopian tube, the most important lesionsin the differential diagnosis are metastat-ic carcinoma and extension or recur-rence of endometrial or endocervicaladenocarcinoma. An adenoma is gener-ally polypoid and lacks invasive borders,marked architectural complexity or highgrade cytological features.
Uncommon epithelial tumours
DefinitionPrimary epithelial tumours of the vaginaother than those of squamous or glandu-lar type. These tumours are described inmore detail in the chapter on the cervix.
Fig. 6.16 Mesonephric remnants. The wall of the vagina contains clusters of uniform dilated tubules withluminal hyaline material.

ICD-O codesAdenosquamous carcinoma 8560/3Adenoid cystic carcinoma 8200/3Adenoid basal carcinoma 8098/3Carcinoid 8240/3Small cell carcinoma 8041/3Undifferentiated carcinoma 8020/3
Adenosquamous carcinoma
A carcinoma composed of a mixture ofmalignant glandular and squamousepithelial elements {2360}.
Adenoid cystic carcinoma
An adenocarcinoma which re s e m b l e sadenoid cystic carcinoma of salivarygland origin but usually lacks the myoep-ithelial cell component of the latter{2781}.
Adenoid basal carcinoma
A carcinoma with rounded, generally welld i ff e rentiated nests of basaloid cellsshowing focal gland formation; centralsquamous differentiation may be presentas well {1906,1986}.
Carcinoid
A tumour resembling carcinoids of thegastrointestinal tract and lung {936}.
Small cell carcinoma
A carcinoma of neuroendocrine type thatresembles small cell carcinomas of thelung {1371,1869,1877,2281}.
Undifferentiated carcinoma
A carcinoma that is not of the small celltype and lacks evidence of glandular,squamous, neuroendocrine or othertypes of differentiation.
301Epithelial tumours
302 Tumours of the vagina
Vaginal sarcomas
DefinitionMalignant mesenchymal tumours thatarise in the vagina.
ICD-O codesSarcoma botryoides 8910/3Leiomyosarcoma 8890/3Endometrioid stromal sarcoma,
low grade 8931/3Undifferentiated vaginal sarcoma 8805/3
EpidemiologySarcomas are rare and comprise <2% ofall malignant vaginal neoplasms {633}.
AetiologyThere are virtually no clues to the patho-genesis of this group of tumours.
Clinical featuresSigns and symptomsMalignant tumours usually present withbleeding and/or discharge and a massand are usually readily detected by clini -cal examination. Occasional cases aredetected by an abnormal cytologicalexamination. Some sarcomas, however,are asymptomatic, and the diagnosis is,therefore, delayed.
ImagingThe extent of tumour spread may bedetermined by transvaginal ultrasound.
Tumour spread and stagingVaginal sarcomas spread by dire c textension and by metastasis; the latteroccurs both by lymphatic and haema-togenous routes. The tumour initiallygrows into the vaginal wall and soft tissueof the pelvis, bladder or rectum. Thestaging of vaginal sarcomas in adults uti-lizes the TNM/FIGO classification{51,2976}.
Sarcoma botryoides
DefinitionA malignant mesenchymal tumour com-posed of small, round or oval to spindle-
shaped cells, some of which show evi-dence of striated muscle differentiation.
SynonymEmbryonal rhabdomyosarcoma.
EpidemiologySarcoma botryoides (Greek bothryos:grapes) is the most common vaginal sar-coma and occurs almost exclusively inc h i l d ren and infants <5 years of age (mean1.8 years) {633}, although occasionalcases are encountered in young adults oreven postmenopausal women. At least twocases of sarcoma botryoides have beendescribed in pregnancy {2709}.
Clinical featuresThese tumours present typically as avaginal mass that on clinical and macro-scopic examination appears soft, oede-matous and nodular, papillary, polypoidor grape-like, often protruding throughthe introitus.
MacroscopyThe tumours vary from 0.2-12 cm in max-imum dimension and may be covered byan intact mucosa or be ulcerated andbleeding. The sectioned surface dis-plays grey to red areas of myxomatouschange and haemorrhage.
Tumour spread and stagingIn children the Intergroup Rhabdo-myosarcoma Study group clinical classi-
fication is used, which is based on thecombined features of extent of disease,resectability and histological evaluationof margins of excision {99}.
HistopathologyThe neoplasm is composed of cells withround to oval or spindle-shaped nucleiand eosinophilic cytoplasm that may showd i ff e rentiation towards striated musclecells. Ty p i c a l l y, there is a dense cambiumlayer composed of closely packed cellswith small hyperc h romatic nuclei immedi-ately subjacent to the squamous epitheli-um that may be invaded. The nuclei havean open chromatin pattern and inconspic-uous nucleoli. The central portion of thepolypoid mass is typically hypocellular,oedematous or myxomatous. The mitoticrate is high. Rhabdo-myoblasts (strapcells), which may be sparse, may befound in any of the patterns. Their re c o g n i-tion may be facilitated by immunohisto-chemical staining with antibodies dire c t e dagainst actin, desmin or myoglobin.Although the first two antibodies are moresensitive than myoglobin, they are notspecific for skeletal muscle diff e re n t i a t i o n .Ultrastructural examination may re v e a lcharacteristic features of rhabdomyoblas-tic diff e rentiation, such as thick and thin fil-aments with Z-band material.
Differential diagnosisThe distinction from a benign fibroepithe-lial polyp with bizarre nuclei is important.
A.G. ÖstörMesenchymal tumours
Table 6.02Clinical classification of vaginal sarcoma botyroides / rhabdomyosarcoma {99}.
IIIa Biopsy only
IV Metastatic disease
IIIb Partial surgical excision (gross disease present)
IIb Excision, lymph nodes positive
IIa Excision, margin positive
I Complete surgical resection
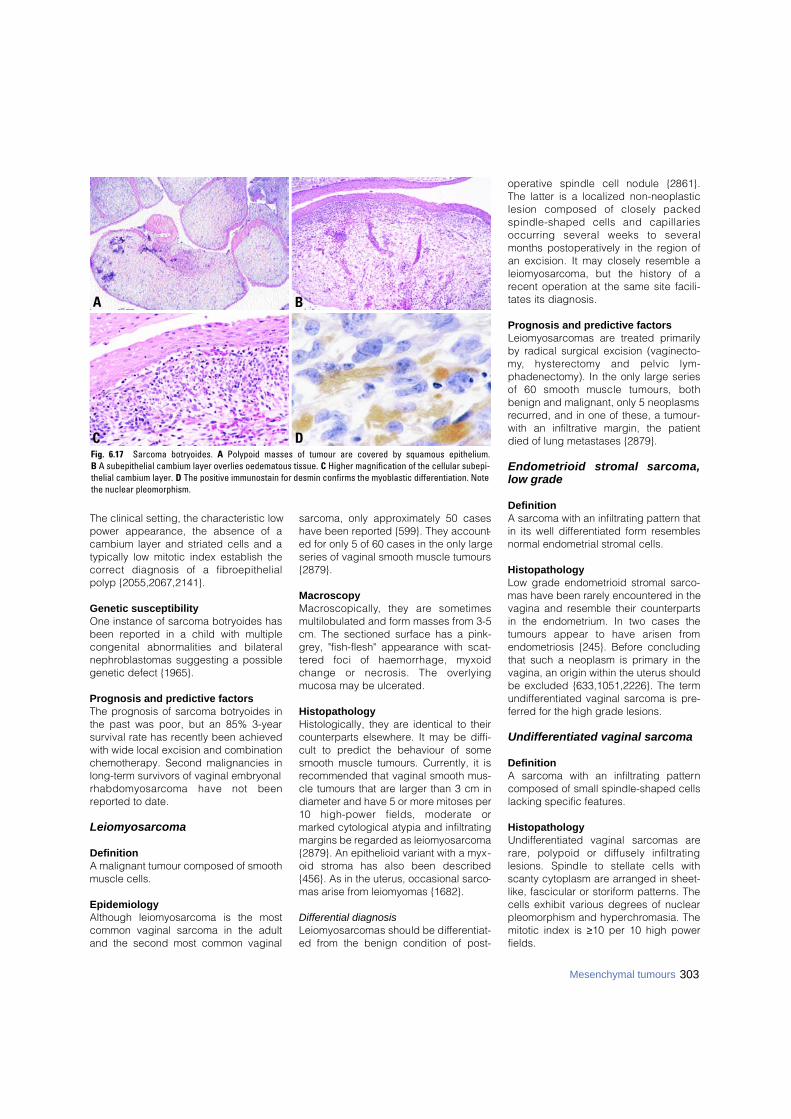
303Mesenchymal tumours
The clinical setting, the characteristic lowpower appearance, the absence of acambium layer and striated cells and atypically low mitotic index establish thec o r rect diagnosis of a fibro e p i t h e l i a lpolyp {2055,2067,2141}.
Genetic susceptibilityOne instance of sarcoma botryoides hasbeen reported in a child with multiplecongenital abnormalities and bilateralnephroblastomas suggesting a possiblegenetic defect {1965}.
Prognosis and predictive factorsThe prognosis of sarcoma botryoides inthe past was poor, but an 85% 3-yearsurvival rate has recently been achievedwith wide local excision and combinationchemotherapy. Second malignancies inlong-term survivors of vaginal embryonalr h a b d o m y o s a rcoma have not beenreported to date.
Leiomyosarcoma
DefinitionA malignant tumour composed of smoothmuscle cells.
EpidemiologyAlthough leiomyosarcoma is the mostcommon vaginal sarcoma in the adultand the second most common vaginal
sarcoma, only approximately 50 caseshave been reported {599}. They account-ed for only 5 of 60 cases in the only largeseries of vaginal smooth muscle tumours{2879}.
MacroscopyM a c ro s c o p i c a l l y, they are sometimesmultilobulated and form masses from 3-5cm. The sectioned surface has a pink-grey, "fish-flesh" appearance with scat-t e red foci of haemorrhage, myxoidchange or necrosis. The overlyingmucosa may be ulcerated.
HistopathologyHistologically, they are identical to theircounterparts elsewhere. It may be diffi-cult to predict the behaviour of somesmooth muscle tumours. Currently, it isrecommended that vaginal smooth mus-cle tumours that are larger than 3 cm indiameter and have 5 or more mitoses per10 high-power fields, moderate ormarked cytological atypia and infiltratingmargins be regarded as leiomyosarcoma{2879}. An epithelioid variant with a myx-oid stroma has also been described{456}. As in the uterus, occasional sarco-mas arise from leiomyomas {1682}.
Differential diagnosisL e i o m y o s a rcomas should be diff e re n t i a t-ed from the benign condition of post-
operative spindle cell nodule {2861}.The latter is a localized non-neoplasticlesion composed of closely packedspindle-shaped cells and capillariesoccurring several weeks to severalmonths postoperatively in the region ofan excision. It may closely resemble al e i o m y o s a rcoma, but the history of arecent operation at the same site facili-tates its diagnosis.
Prognosis and predictive factorsLeiomyosarcomas are treated primarilyby radical surgical excision (vaginecto-m y, hysterectomy and pelvic lym-phadenectomy). In the only large seriesof 60 smooth muscle tumours, bothbenign and malignant, only 5 neoplasmsrecurred, and in one of these, a tumour-with an infiltrative margin, the patientdied of lung metastases {2879}.
Endometrioid stromal sarcoma,low grade
DefinitionA sarcoma with an infiltrating pattern thatin its well differentiated form resemblesnormal endometrial stromal cells.
HistopathologyLow grade endometrioid stromal sarco-mas have been rarely encountered in thevagina and resemble their counterpartsin the endometrium. In two cases thetumours appear to have arisen fro mendometriosis {245}. Before concludingthat such a neoplasm is primary in thevagina, an origin within the uterus shouldbe excluded {633,1051,2226}. The termundifferentiated vaginal sarcoma is pre-ferred for the high grade lesions.
Undifferentiated vaginal sarcoma
DefinitionA sarcoma with an infiltrating patterncomposed of small spindle-shaped cellslacking specific features.
HistopathologyU n d i ff e rentiated vaginal sarcomas arer a re, polypoid or diffusely infiltratinglesions. Spindle to stellate cells withscanty cytoplasm are arranged in sheet-like, fascicular or storiform patterns. Thecells exhibit various degrees of nuclearpleomorphism and hyperchromasia. Themitotic index is ≥10 per 10 high powerfields.
BA
DCFig. 6.17 Sarcoma botryoides. A Polypoid masses of tumour are covered by squamous epithelium. B A subepithelial cambium layer overlies oedematous tissue. C Higher magnification of the cellular subepi-thelial cambium layer. D The positive immunostain for desmin confirms the myoblastic differentiation. Notethe nuclear pleomorphism.
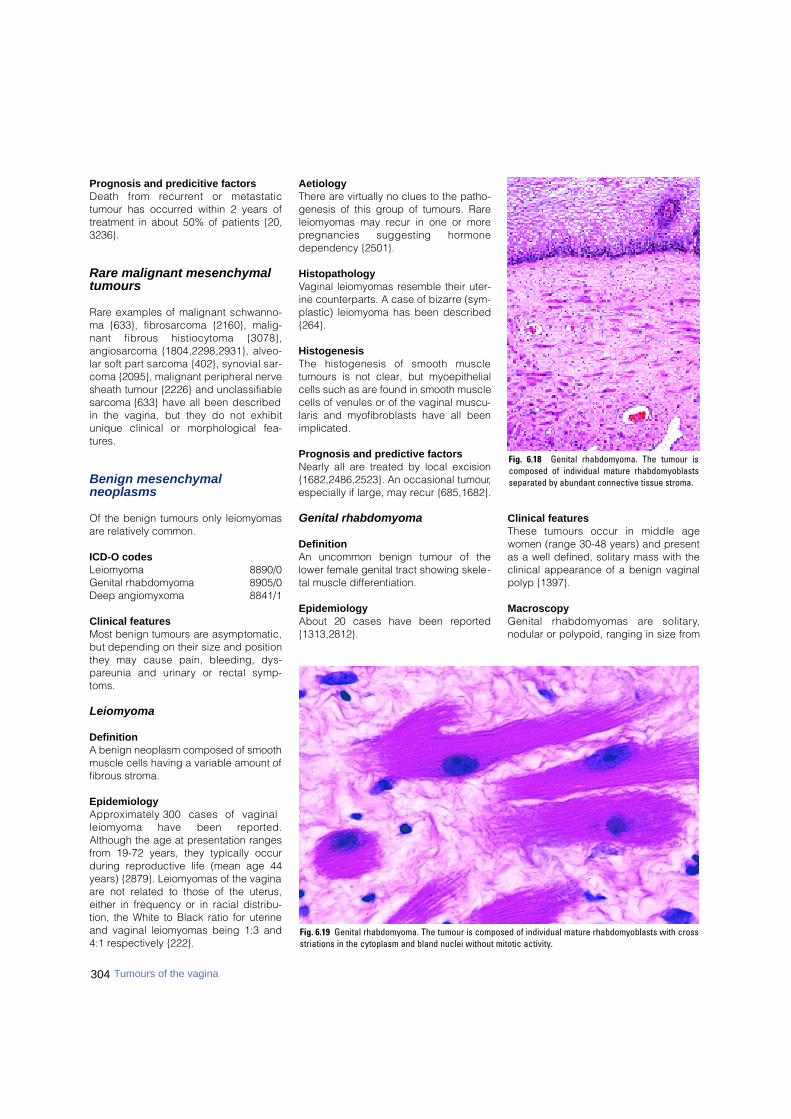
304 Tumours of the vagina
Prognosis and predicitive factorsDeath from re c u r rent or metastatictumour has occurred within 2 years oftreatment in about 50% of patients {20,3236}.
Rare malignant mesenchymaltumours
R a re examples of malignant schwanno-ma {633}, fibro s a rcoma {2160}, malig-nant fibrous histiocytoma {3078},a n g i o s a rcoma {1804,2298,2931}, alveo-lar soft part sarcoma {402}, synovial sar-coma {2095}, malignant peripheral nervesheath tumour {2226} and unclassifiables a rcoma {633} have all been describedin the vagina, but they do not exhibitunique clinical or morphological fea-t u re s .
Benign mesenchymal neoplasms
Of the benign tumours only leiomyomasare relatively common.
ICD-O codesLeiomyoma 8890/0Genital rhabdomyoma 8905/0Deep angiomyxoma 8841/1
Clinical features Most benign tumours are asymptomatic,but depending on their size and positionthey may cause pain, bleeding, dys-p a reunia and urinary or rectal symp-t o m s .
Leiomyoma
DefinitionA benign neoplasm composed of smoothmuscle cells having a variable amount offibrous stroma.
EpidemiologyA p p roximately 300 cases of vaginalleiomyoma have been re p o rt e d .Although the age at presentation rangesfrom 19-72 years, they typically occurduring reproductive life (mean age 44years) {2879}. Leiomyomas of the vaginaare not related to those of the uterus,either in frequency or in racial distribu-tion, the White to Black ratio for uterineand vaginal leiomyomas being 1:3 and4:1 respectively {222}.
AetiologyThere are virtually no clues to the patho-genesis of this group of tumours. Rareleiomyomas may recur in one or morep regnancies suggesting horm o n edependency {2501}.
HistopathologyVaginal leiomyomas resemble their uter-ine counterparts. A case of bizarre (sym-plastic) leiomyoma has been described{264}.
HistogenesisThe histogenesis of smooth muscletumours is not clear, but myoepithelialcells such as are found in smooth musclecells of venules or of the vaginal muscu-laris and myofibroblasts have all beenimplicated.
Prognosis and predictive factorsNearly all are treated by local excision{1682,2486,2523}. An occasional tumour,especially if large, may recur {685,1682}.
Genital rhabdomyoma
DefinitionAn uncommon benign tumour of thelower female genital tract showing skele-tal muscle differentiation.
EpidemiologyAbout 20 cases have been re p o rt e d{1313,2812}.
Clinical features These tumours occur in middle agewomen (range 30-48 years) and presentas a well defined, solitary mass with theclinical appearance of a benign vaginalpolyp {1397}.
MacroscopyGenital rhabdomyomas are solitary,nodular or polypoid, ranging in size from
Fig. 6.18 Genital rhabdomyoma. The tumour iscomposed of individual mature rhabdomyoblastsseparated by abundant connective tissue stroma.
Fig. 6.19 Genital rhabdomyoma. The tumour is composed of individual mature rhabdomyoblasts with crossstriations in the cytoplasm and bland nuclei without mitotic activity.

1-11 cm. They may arise anywhere in thevagina, and some protrude into thelumen. The overlying mucosa is usuallyintact since the tumour arises in the wall.The texture is rubbery and the sectionedsurface is grey and glassy.
HistopathologyThey are composed of mature, blandrhabdomyoblasts that are oval or strap-shaped with obvious cross striations in thecytoplasm. Mitotic activity and nuclearpleomorphism are absent. Abundant con-nective tissue stroma surrounds individualmuscle cells. Rhabdo-myoma should notbe confused with sarcoma botryoides.
Prognosis and predictive factorsNo recurrences have been reported aftercomplete local excision.
Deep angiomyxoma
DefinitionA locally infiltrative tumour with apredilection for the pelvic and perinealregions and a tendency for local recur-rence composed of fibroblasts, myofi-broblasts and numerous, characteristi-cally thick-walled, blood vessels embed-ded in an abundant myxoid matrix.
SynonymAggressive angiomyxoma.
Clinical featuresMost patients present with a large, slow-ly growing, painless mass in the pelviper-ineal region that may give rise to pres-sure effects on the adjacent urogenital or
anorectal tracts. Imaging studies oftenshow the mass to be substantially largerthan clinically suspected.
MacroscopyMacroscopically, the tumour is lobulatedbut poorly circumscribed due to finger-like extensions into the surrounding tis-sue. The neoplasm is grey-pink or red-tan and rubbery or gelatinous.
Tumour spread and stagingDeep angiomyxoma is a locally infiltrativebut non-metastasizing neoplasm thatoccurs for the most part during the re p ro-ductive years. At least two cases havebeen reported within the vagina, anuncommon site for this neoplasm {81, 496}.
HistopathologyThe tumour is of low to moderate cellu-larity and is composed of small, uniform,spindle-shaped to stellate cells withpoorly defined, pale eosinophilic cyto-plasm and bland, often vesicular nuclei.An abundant myxoid matrix contains avariable number of rounded, medium-sized to large vessels that possess thick-ened focally hyalinized walls. A charac-teristic feature is the presence of looselyorganized islands of myoid cells aroundthe larger nerve segments and vessels{3086}. The neoplasm is positive fordesmin in almost all cases, where a sstains for S-100 protein are consistentlynegative {1431,2082}.
Prognosis and predictive factorsThe treatment for this locally aggressivebut non-metastasizing neoplasm is pri-
marily surgical with close attention tomargins. Approximately 30% of tumoursrecur locally.
Postoperative spindle cell nodule
DefinitionA non-neoplastic localized lesion com-posed of closely packed pro l i f e r a t i n gspindle cells and capillaries simulating aleiomyosarcoma.
Clinical featuresThe lesion develops at the site of a recentoperation several weeks to severalmonths postoperatively {2861}.
HistopathologyThe lesion is composed of closelypacked, mitotically active, spindle-shaped mesenchymal cells and capillar-ies often with an accompaniment ofinflammatory cells.
Differential diagnosisThe history of a recent operation at thesame site serves to distinguish this lesionf rom leiomyosarcoma. Postoperativespindle cell nodule may closely resemblea leiomyosarcoma or other spindle cellsarcoma, but the history of a recentoperation at the same site facilitates itsdiagnosis.
305Mesenchymal tumours
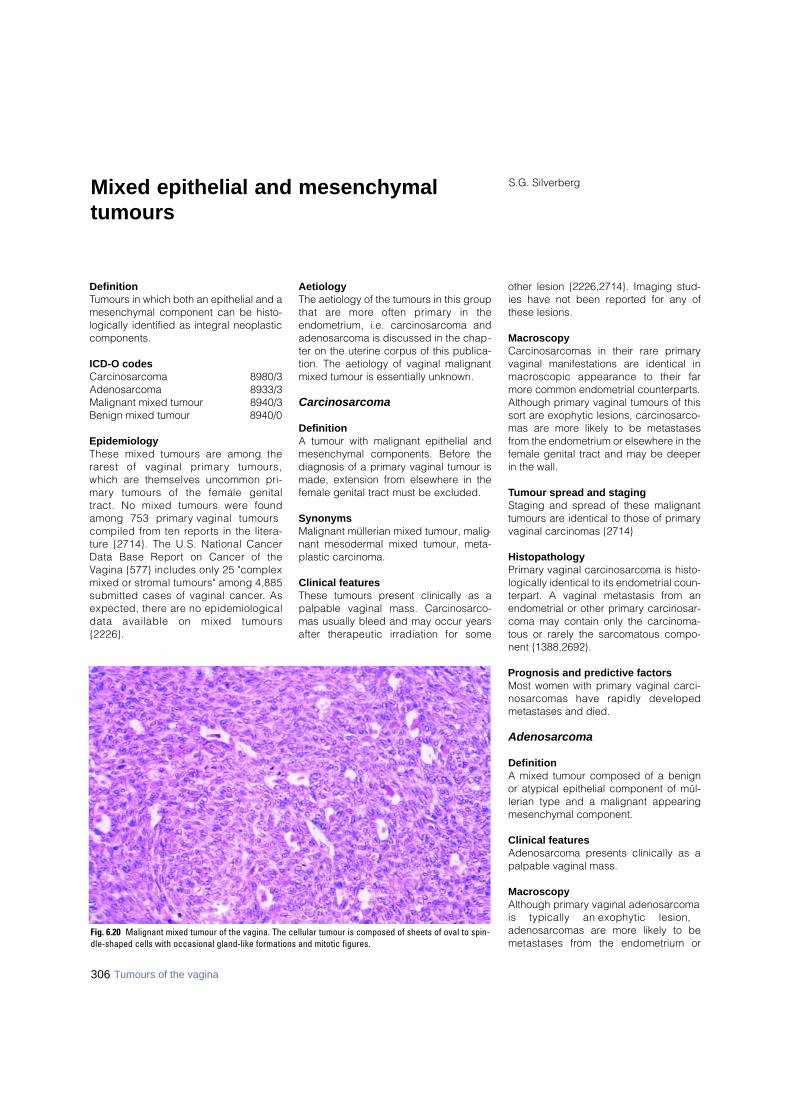
DefinitionTumours in which both an epithelial and amesenchymal component can be histo-logically identified as integral neoplasticcomponents.
ICD-O codes Carcinosarcoma 8980/3Adenosarcoma 8933/3Malignant mixed tumour 8940/3Benign mixed tumour 8940/0
EpidemiologyThese mixed tumours are among ther a rest of vaginal primary tumours,which are themselves uncommon pri-m a ry tumours of the female genitaltract. No mixed tumours were foundamong 753 primary vaginal tumourscompiled from ten re p o rts in the litera-t u re {2714}. The U.S. National CancerData Base Report on Cancer of theVagina {577} includes only 25 "complexmixed or stromal tumours" among 4,885submitted cases of vaginal cancer. Asexpected, there are no epidemiologicaldata available on mixed tumours{ 2 2 2 6 } .
AetiologyThe aetiology of the tumours in this groupthat are more often primary in theendometrium, i.e. carcinosarcoma andadenosarcoma is discussed in the chap-ter on the uterine corpus of this publica-tion. The aetiology of vaginal malignantmixed tumour is essentially unknown.
Carcinosarcoma
DefinitionA tumour with malignant epithelial andmesenchymal components. Before thediagnosis of a primary vaginal tumour ismade, extension from elsewhere in thefemale genital tract must be excluded.
SynonymsMalignant müllerian mixed tumour, malig-nant mesodermal mixed tumour, meta-plastic carcinoma.
Clinical featuresThese tumours present clinically as apalpable vaginal mass. Carc i n o s a rc o -mas usually bleed and may occur yearsafter therapeutic irradiation for some
other lesion {2226,2714}. Imaging stud-ies have not been reported for any ofthese lesions.
MacroscopyCarcinosarcomas in their rare primaryvaginal manifestations are identical inm a c roscopic appearance to their farmore common endometrial counterparts.Although primary vaginal tumours of thissort are exophytic lesions, carcinosarco-mas are more likely to be metastasesfrom the endometrium or elsewhere in thefemale genital tract and may be deeperin the wall.
Tumour spread and stagingStaging and spread of these malignanttumours are identical to those of primaryvaginal carcinomas {2714}
HistopathologyPrimary vaginal carcinosarcoma is histo-logically identical to its endometrial coun-terpart. A vaginal metastasis from anendometrial or other primary carcinosar-coma may contain only the carcinoma-tous or rarely the sarcomatous compo-nent {1388,2692}.
Prognosis and predictive factorsMost women with primary vaginal carci-n o s a rcomas have rapidly developedmetastases and died.
Adenosarcoma
DefinitionA mixed tumour composed of a benignor atypical epithelial component of mül-lerian type and a malignant appearingmesenchymal component.
Clinical featuresAdenosarcoma presents clinically as apalpable vaginal mass.
MacroscopyAlthough primary vaginal adenosarcomais typically an exophytic lesion,adenosarcomas are more likely to bemetastases from the endometrium or
S.G. SilverbergMixed epithelial and mesenchymaltumours
Fig. 6.20 Malignant mixed tumour of the vagina. The cellular tumour is composed of sheets of oval to spin-dle-shaped cells with occasional gland-like formations and mitotic figures.
306 Tumours of the vagina
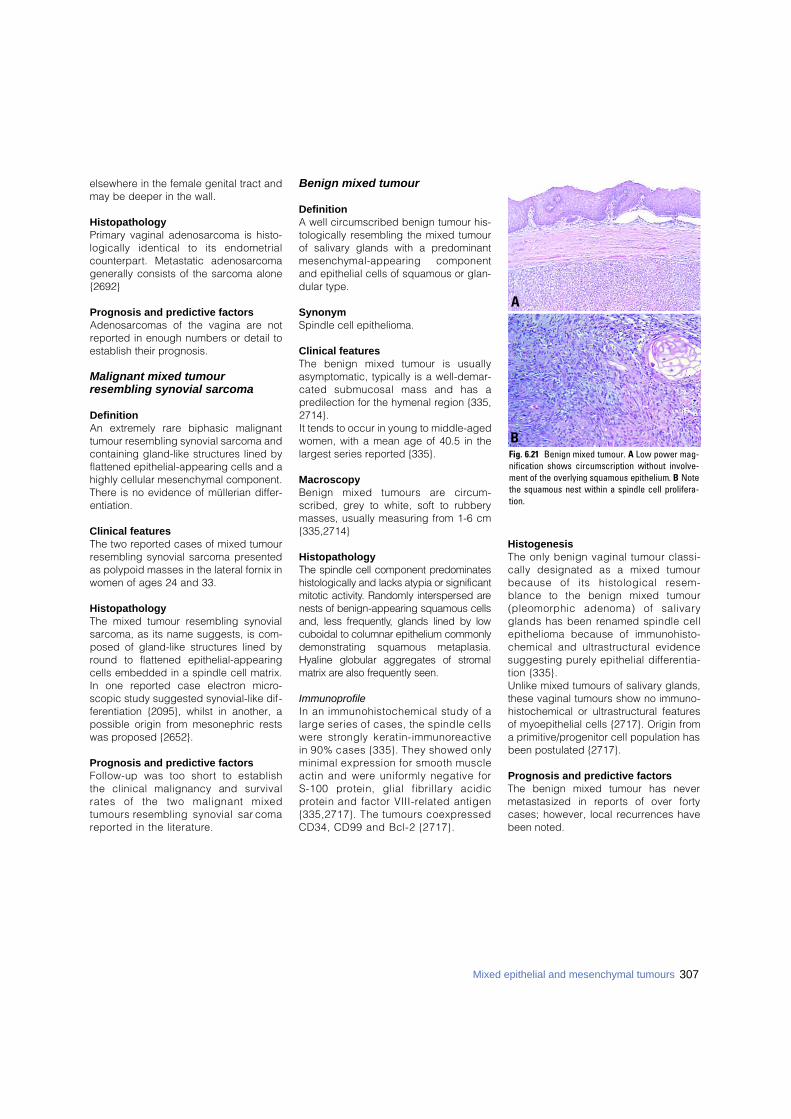
307Mixed epithelial and mesenchymal tumours
elsewhere in the female genital tract andmay be deeper in the wall.
HistopathologyPrimary vaginal adenosarcoma is histo-logically identical to its endometrialc o u n t e r p a rt. Metastatic adenosarc o m agenerally consists of the sarcoma alone{2692}
Prognosis and predictive factorsAdenosarcomas of the vagina are notreported in enough numbers or detail toestablish their prognosis.
Malignant mixed tumour resembling synovial sarcoma
DefinitionAn extremely rare biphasic malignanttumour resembling synovial sarcoma andcontaining gland-like structures lined byflattened epithelial-appearing cells and ahighly cellular mesenchymal component.There is no evidence of müllerian differ-entiation.
Clinical featuresThe two reported cases of mixed tumourresembling synovial sarcoma presentedas polypoid masses in the lateral fornix inwomen of ages 24 and 33.
HistopathologyThe mixed tumour resembling synovialsarcoma, as its name suggests, is com-posed of gland-like structures lined byround to flattened epithelial-appearingcells embedded in a spindle cell matrix.In one reported case electron micro-scopic study suggested synovial-like dif-ferentiation {2095}, whilst in another, apossible origin from mesonephric restswas proposed {2652}.
Prognosis and predictive factorsFollow-up was too short to establishthe clinical malignancy and survivalrates of the two malignant mixedtumours resembling synovial sarc o m are p o rted in the literature .
Benign mixed tumour
DefinitionA well circumscribed benign tumour his-tologically resembling the mixed tumourof salivary glands with a predominantmesenchymal-appearing componentand epithelial cells of squamous or glan-dular type.
SynonymSpindle cell epithelioma.
Clinical featuresThe benign mixed tumour is usuallyasymptomatic, typically is a well-demar-cated submucosal mass and has apredilection for the hymenal region {335,2714}.It tends to occur in young to middle-agedwomen, with a mean age of 40.5 in thelargest series reported {335}.
MacroscopyBenign mixed tumours are circ u m-scribed, grey to white, soft to rubberymasses, usually measuring from 1-6 cm{335,2714}
HistopathologyThe spindle cell component pre d o m i n a t e shistologically and lacks atypia or significantmitotic activity. Randomly interspersed arenests of benign-appearing squamous cellsand, less fre q u e n t l y, glands lined by lowcuboidal to columnar epithelium commonlydemonstrating squamous metaplasia.Hyaline globular aggregates of stro m a lmatrix are also frequently seen.
ImmunoprofileIn an immunohistochemical study of alarge series of cases, the spindle cellsw e re strongly keratin-immunore a c t i v ein 90% cases {335}. They showed onlyminimal expression for smooth muscleactin and were uniformly negative for S-100 protein, glial fibrillary acidicp rotein and factor VIII-related antigen{335,2717}. The tumours coexpre s s e dCD34, CD99 and Bcl-2 {2717}.
HistogenesisThe only benign vaginal tumour classi-cally designated as a mixed tumourbecause of its histological re s e m-blance to the benign mixed tumour(pleomorphic adenoma) of salivaryglands has been renamed spindle cellepithelioma because of immunohisto-chemical and ultrastructural evidencesuggesting purely epithelial diff e re n t i a-tion {335}. Unlike mixed tumours of salivary glands,these vaginal tumours show no immuno-histochemical or ultrastructural featuresof myoepithelial cells {2717}. Origin froma primitive/progenitor cell population hasbeen postulated {2717}.
Prognosis and predictive factorsThe benign mixed tumour has nevermetastasized in re p o rts of over fort ycases; however, local recurrences havebeen noted.
Fig. 6.21 Benign mixed tumour. A Low power mag-nification shows circumscription without involve-ment of the overlying squamous epithelium. B N o t ethe squamous nest within a spindle cell prolifera-t i o n .
A
B
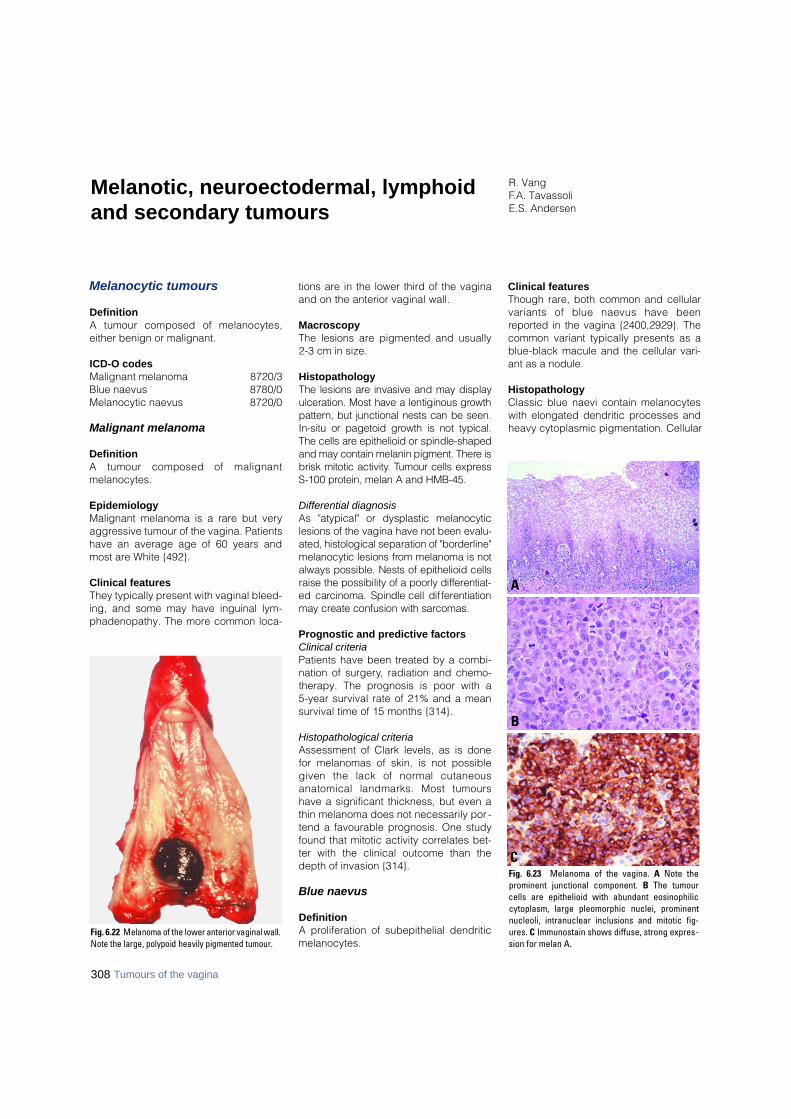
Melanocytic tumours
DefinitionA tumour composed of melanocytes,either benign or malignant.
ICD-O codesMalignant melanoma 8720/3Blue naevus 8780/0Melanocytic naevus 8720/0
Malignant melanoma
DefinitionA tumour composed of malignantmelanocytes.
EpidemiologyMalignant melanoma is a rare but veryaggressive tumour of the vagina. Patientshave an average age of 60 years andmost are White {492}.
Clinical featuresThey typically present with vaginal bleed-ing, and some may have inguinal lym-phadenopathy. The more common loca-
tions are in the lower third of the vaginaand on the anterior vaginal wall.
MacroscopyThe lesions are pigmented and usually 2-3 cm in size.
HistopathologyThe lesions are invasive and may displayulceration. Most have a lentiginous gro w t hp a t t e rn, but junctional nests can be seen.In-situ or pagetoid growth is not typical.The cells are epithelioid or spindle-shapedand may contain melanin pigment. There isbrisk mitotic activity. Tumour cells expre s sS-100 protein, melan A and HMB-45.
Differential diagnosisAs "atypical" or dysplastic melanocyticlesions of the vagina have not been evalu-ated, histological separation of "bord e r l i n e "melanocytic lesions from melanoma is notalways possible. Nests of epithelioid cellsraise the possibility of a poorly diff e re n t i a t-ed carcinoma. Spindle cell diff e re n t i a t i o nmay create confusion with sarc o m a s .
Prognostic and predictive factorsClinical criteriaPatients have been treated by a combi-nation of surgery, radiation and chemo-therapy. The prognosis is poor with a 5-year survival rate of 21% and a meansurvival time of 15 months {314}.
Histopathological criteriaAssessment of Clark levels, as is donefor melanomas of skin, is not possiblegiven the lack of normal cutaneousanatomical landmarks. Most tumourshave a significant thickness, but even athin melanoma does not necessarily por -tend a favourable prognosis. One studyfound that mitotic activity correlates bet-ter with the clinical outcome than thedepth of invasion {314}.
Blue naevus
DefinitionA proliferation of subepithelial dendriticmelanocytes.
Clinical featuresThough rare, both common and cellularvariants of blue naevus have beenreported in the vagina {2400,2929}. Thecommon variant typically presents as ablue-black macule and the cellular vari-ant as a nodule.
HistopathologyClassic blue naevi contain melanocyteswith elongated dendritic processes andheavy cytoplasmic pigmentation. Cellular
R. VangF.A. TavassoliE.S. Andersen
Melanotic, neuroectodermal, lymphoidand secondary tumours
Fig. 6.22 Melanoma of the lower anterior vaginal wall.Note the large, polypoid heavily pigmented tumour.
Fig. 6.23 Melanoma of the vagina. A Note theprominent junctional component. B The tumourcells are epithelioid with abundant eosinophiliccytoplasm, large pleomorphic nuclei, prominentnucleoli, intranuclear inclusions and mitotic fig-ures. C Immunostain shows diffuse, strong expres-sion for melan A.
B
A
C
308 Tumours of the vagina
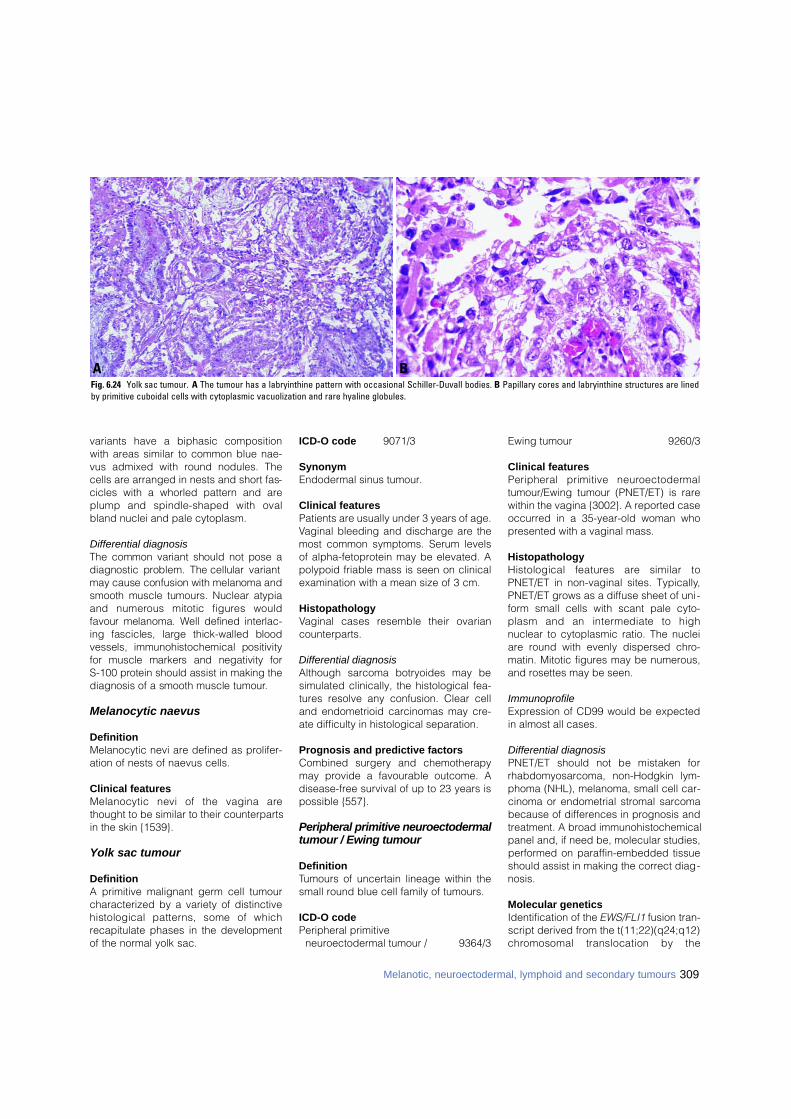
variants have a biphasic compositionwith areas similar to common blue nae-vus admixed with round nodules. Thecells are arranged in nests and short fas-cicles with a whorled pattern and areplump and spindle-shaped with ovalbland nuclei and pale cytoplasm.
Differential diagnosisThe common variant should not pose adiagnostic problem. The cellular variantmay cause confusion with melanoma andsmooth muscle tumours. Nuclear atypiaand numerous mitotic figures wouldfavour melanoma. Well defined interlac-ing fascicles, large thick-walled bloodvessels, immunohistochemical positivityfor muscle markers and negativity for S-100 protein should assist in making thediagnosis of a smooth muscle tumour.
Melanocytic naevus
DefinitionMelanocytic nevi are defined as prolifer-ation of nests of naevus cells.
Clinical featuresMelanocytic nevi of the vagina arethought to be similar to their counterpartsin the skin {1539}.
Yolk sac tumour
DefinitionA primitive malignant germ cell tumourcharacterized by a variety of distinctivehistological patterns, some of whichrecapitulate phases in the developmentof the normal yolk sac.
ICD-O code 9071/3
SynonymEndodermal sinus tumour.
Clinical featuresPatients are usually under 3 years of age.Vaginal bleeding and discharge are themost common symptoms. Serum levelsof alpha-fetoprotein may be elevated. Apolypoid friable mass is seen on clinicalexamination with a mean size of 3 cm.
HistopathologyVaginal cases resemble their ovariancounterparts.
Differential diagnosisAlthough sarcoma botryoides may besimulated clinically, the histological fea-tures resolve any confusion. Clear celland endometrioid carcinomas may cre-ate difficulty in histological separation.
Prognosis and predictive factorsCombined surgery and chemotherapymay provide a favourable outcome. Adisease-free survival of up to 23 years ispossible {557}.
Peripheral primitive neuroectodermaltumour / Ewing tumour
DefinitionTumours of uncertain lineage within thesmall round blue cell family of tumours.
ICD-O codePeripheral primitive
neuroectodermal tumour / 9364/3
Ewing tumour 9260/3
Clinical featuresPeripheral primitive neuro e c t o d e rm a ltumour/Ewing tumour (PNET/ET) is rarewithin the vagina {3002}. A reported caseoccurred in a 35-year-old woman whopresented with a vaginal mass.
HistopathologyHistological features are similar toPNET/ET in non-vaginal sites. Typically,PNET/ET grows as a diffuse sheet of uni-form small cells with scant pale cyto-plasm and an intermediate to highnuclear to cytoplasmic ratio. The nucleiare round with evenly dispersed chro-matin. Mitotic figures may be numerous,and rosettes may be seen.
ImmunoprofileExpression of CD99 would be expectedin almost all cases.
Differential diagnosisPNET/ET should not be mistaken forrhabdomyosarcoma, non-Hodgkin lym-phoma (NHL), melanoma, small cell car-cinoma or endometrial stromal sarcomabecause of differences in prognosis andtreatment. A broad immunohistochemicalpanel and, if need be, molecular studies,performed on paraffin-embedded tissueshould assist in making the correct diag-nosis.
Molecular geneticsIdentification of the EWS/FLI1 fusion tran-script derived from the t(11;22)(q24;q12)c h romosomal translocation by the
BAFig. 6.24 Yolk sac tumour. A The tumour has a labryinthine pattern with occasional Schiller-Duvall bodies. B Papillary cores and labryinthine structures are linedby primitive cuboidal cells with cytoplasmic vacuolization and rare hyaline globules.
309Melanotic, neuroectodermal, lymphoid and secondary tumours
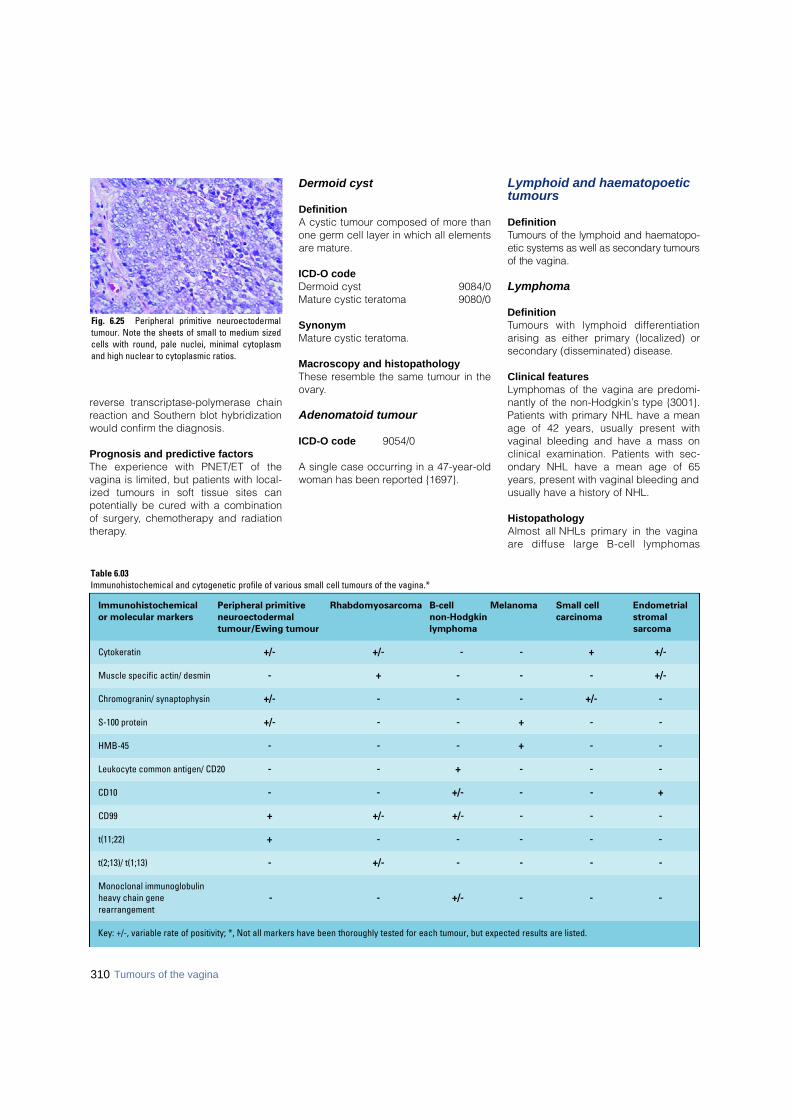
310 Tumours of the vagina
reverse transcriptase-polymerase chainreaction and Southern blot hybridizationwould confirm the diagnosis.
Prognosis and predictive factorsThe experience with PNET/ET of thevagina is limited, but patients with local-ized tumours in soft tissue sites canpotentially be cured with a combinationof surgery, chemotherapy and radiationtherapy.
Dermoid cyst
DefinitionA cystic tumour composed of more thanone germ cell layer in which all elementsare mature.
ICD-O codeDermoid cyst 9084/0Mature cystic teratoma 9080/0
SynonymMature cystic teratoma.
Macroscopy and histopathologyThese resemble the same tumour in theovary.
Adenomatoid tumour
ICD-O code 9054/0
A single case occurring in a 47-year-oldwoman has been reported {1697}.
Lymphoid and haematopoetictumours
DefinitionTumours of the lymphoid and haematopo-etic systems as well as secondary tumoursof the vagina.
Lymphoma
DefinitionTumours with lymphoid diff e re n t i a t i o narising as either primary (localized) orsecondary (disseminated) disease.
Clinical featuresLymphomas of the vagina are predomi-nantly of the non-Hodgkin’s type {3001}.Patients with primary NHL have a meanage of 42 years, usually present withvaginal bleeding and have a mass onclinical examination. Patients with sec-ondary NHL have a mean age of 65years, present with vaginal bleeding andusually have a history of NHL.
HistopathologyAlmost all NHLs primary in the vaginaa re diffuse large B-cell lymphomas
Table 6.03Immunohistochemical and cytogenetic profile of various small cell tumours of the vagina.*
Immunohistochemical Peripheral primitive Rhabdomyosarcoma B-cell Melanoma Small cell Endometrialor molecular markers neuroectodermal non-Hodgkin carcinoma stromal
tumour/Ewing tumour lymphoma sarcoma
Cytokeratin +/- +/- - - + +/-
Muscle specific actin/ desmin - + - - - +/-
Chromogranin/ synaptophysin +/- - - - +/- -
S-100 protein +/- - - + - -
HMB-45 - - - + - -
Leukocyte common antigen/ CD20 - - + - - -
CD10 - - +/- - - +
CD99 + +/- +/- - - -
t(11;22) + - - - - -
t(2;13)/ t(1;13) - +/- - - - -
Monoclonal immunoglobulin heavy chain gene - - +/- - - -rearrangement
Key: +/-, variable rate of positivity; *, Not all markers have been thoroughly tested for each tumour, but expected results are listed.
Fig. 6.25 Peripheral primitive neuroectodermaltumour. Note the sheets of small to medium sizedcells with round, pale nuclei, minimal cytoplasmand high nuclear to cytoplasmic ratios.

311Melanotic, neuroectodermal, lymphoid and secondary tumours
g rowing in sheets. Some may have scle-rosis. The neoplastic cells are large withround nuclei, vesicular chromatin andnucleoli. Secondary cases are usuallyd i ffuse large B-cell lymphomas and arehistologically similar to the primarycases.
ImmunoprofileAlmost all NHLs of the vagina (primary orsecondary) are of B-cell lineage and typ-ically express CD20.
Differential diagnosisThe main lesions in the differential diag-nosis of NHL include granulocytic sarco-ma and other haematological malignan-cies, carcinoma, melanoma and smallround blue cell tumours such as rhab-domyosarcoma. Knowledge of the age,previous history of NHL or leukaemia,and the immunoprofile (keratin, CD20,CD3, CD43, myeloperoxidase, S-100protein, desmin and other muscle mark-ers) should help establish the correctdiagnosis.
Somatic geneticsSouthern blot analysis and polymerasechain reaction (PCR) can demonstratemonoclonal immunoglobulin heavy chaingene rearrangements in vaginal NHL. In-situ hybridization has not confirmed thepresence of human papillomavirus DNAor Epstein-Barr virus (EBV) RNA {2999};however, EBV DNA has been found byPCR {2718}.
Prognosis and predictive factorsVaginal NHL is usually treated bychemotherapy and radiation. The deter-mination of the Ann Arbor stage is prog-nostically important for vaginal NHL.Patients with low stage tumours (stagesIE and IIE) have a longer disease-freesurvival than those with high-stage dis-ease have (stages IIIE and IV).
Leukaemia
DefinitionA malignant haematopoetic neoplasmthat may be primary or secondary.
SynonymGranulocytic sarcoma.
EpidemiologyVaginal involvement by leukaemia mayeither be primary or secondary; however,the latter is much more common {428}.
Clinical featuresLeukaemia of the vagina is rare but isusually of the myeloid type (granulocyticsarcoma or "chloroma") {2099}. Patientsa re elderly, have a mass on clinicalexamination and may have other evi-dence of acute myeloid leukaemia.
HistopathologyA series of primary granulocytic sarco-mas of the female genital tract including3 cases of the vagina was re p o rt e d{2099}. Granulocytic sarcomas are usu-ally composed of cells with finely dis-persed nuclear chromatin and abundantcytoplasm that may be deeply eosino-philic. The identification of eosinophilicmyelocytes is helpful in establishing thediagnosis; however, they are not alwayspresent. The tumours are positive forchloroacetate esterase.
ImmunoprofileGranulocytic sarcomas express lyso-zyme, myeloperoxidase, CD43 andCD68. Staining for CD45 may be seen,but the tumour cells are negative forCD20 and CD3.
Differential diagnosisThe most important differential diagnosisis malignant lymphoma. Enzyme histo-chemical stains for chloracetate esterase
or immunohistochemical stains formyeloproxidase, CD68 and CD43 willestablish the diagnosis in almost allcases {2099}.
Prognosis and predictive factorsGranulocytic sarcoma of the vaginaappears to behave in an aggre s s i v efashion. Although experience is limited,the few reported granulocytic sarcomasof the vagina have also been treated withchemotherapy or radiation.
Secondary tumours
Definition Tumours of the vagina that originate out-side the vagina.
Incidence and originMetastatic tumours are more fre q u e n tthan primary malignant tumours of thevagina. Tumours may spread by dire c textension, most commonly from the cervixor vulva, vascular and lymphatic dissemi-nation or by implantation. Metastatic ade-n o c a rcinomas originate from the endo-metrium, colon, rectum and, more rare l y,the breast. Transitional cell carc i n o m ametastatic from the urethra and the blad-der and renal cell carcinomas have beenre p o rted. In the past vaginal metastasesw e re re p o rted in up to 50% of cases ofuterine choriocarc i n o m a .
Clinical featuresThe primary tumour is often clinically evi-dent or has previously been treated. Themost significant symptom is abnormalvaginal bleeding. Vaginal cytology mayaid detection. A biopsy is contraindicat-ed in metastatic trophoblastic diseasedue to the risk of excessive bleeding.
CHAPTER 7
Tumours of the Vulva
Squamous cell carcinoma of the vulva occurs predominantly inthe older age group. Although the incidence rate of vulvarintraepithelial neoplasia is increasing, that of squamous cellcarcinoma of the vulva is declining, reflecting earlier detectionand more successful treatment. In addition to human papillo-mavirus infection, cigarette smoking is a putative risk factor forvulvar squamous cell carcinoma. There are three known pre-cursor lesions: vulvar intraepithelial neoplasia, lichen sclerosisand chronic granulomatous disease.
Other important epithelial malignancies of the vulva are Pagetdisease and Bartholin gland carcinoma. They are much lesscommon than squamous lesions, and the risk factors are large-ly unknown.
Prominent non-epithelial tumours are malignant melanoma andsarcoma botyoides.
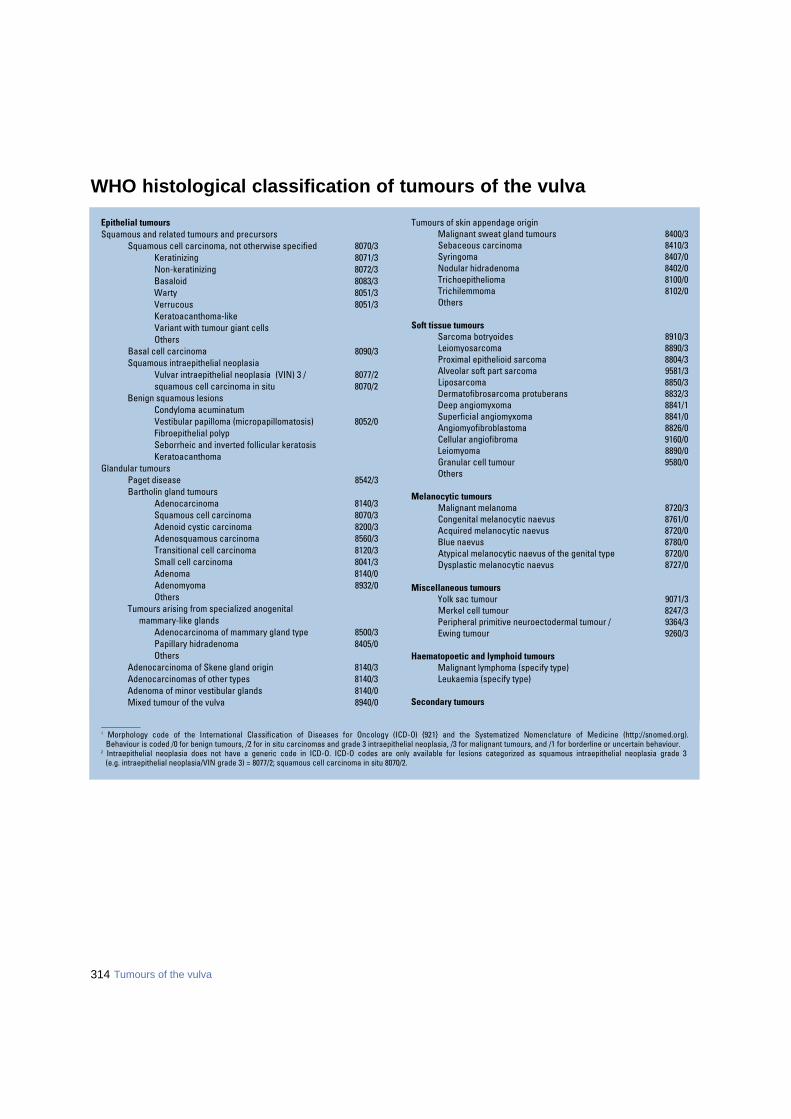
WHO histological classification of tumours of the vulva
_ _ _ _ _ _ _ _ _ _1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {921} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /2 for in situ carcinomas and grade 3 intraepithelial neoplasia, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.2 Intraepithelial neoplasia does not have a generic code in ICD-O. ICD-O codes are only available for lesions categorized as squamous intraepithelial neoplasia grade 3
(e.g. intraepithelial neoplasia/VIN grade 3) = 8077/2; squamous cell carcinoma in situ 8070/2.
Epithelial tumoursSquamous and related tumours and precursors
Squamous cell carcinoma, not otherwise specified 8070/3Keratinizing 8071/3Non-keratinizing 8072/3Basaloid 8083/3Warty 8051/3Verrucous 8051/3Keratoacanthoma-like Variant with tumour giant cellsOthers
Basal cell carcinoma 8090/3Squamous intraepithelial neoplasia
Vulvar intraepithelial neoplasia (VIN) 3 / 8077/2squamous cell carcinoma in situ 8070/2
Benign squamous lesions Condyloma acuminatumVestibular papilloma (micropapillomatosis) 8052/0Fibroepithelial polypSeborrheic and inverted follicular keratosis Keratoacanthoma
Glandular tumoursPaget disease 8542/3Bartholin gland tumours
Adenocarcinoma 8140/3Squamous cell carcinoma 8070/3Adenoid cystic carcinoma 8200/3Adenosquamous carcinoma 8560/3Transitional cell carcinoma 8120/3Small cell carcinoma 8041/3Adenoma 8140/0 Adenomyoma 8932/0Others
Tumours arising from specialized anogenital mammary-like glands
Adenocarcinoma of mammary gland type 8500/3Papillary hidradenoma 8405/0Others
Adenocarcinoma of Skene gland origin 8140/3Adenocarcinomas of other types 8140/3Adenoma of minor vestibular glands 8140/0Mixed tumour of the vulva 8940/0
Tumours of skin appendage originMalignant sweat gland tumours 8400/3Sebaceous carcinoma 8410/3Syringoma 8407/0Nodular hidradenoma 8402/0Trichoepithelioma 8100/0Trichilemmoma 8102/0Others
Soft tissue tumoursSarcoma botryoides 8910/3Leiomyosarcoma 8890/3Proximal epithelioid sarcoma 8804/3Alveolar soft part sarcoma 9581/3Liposarcoma 8850/3Dermatofibrosarcoma protuberans 8832/3Deep angiomyxoma 8841/1Superficial angiomyxoma 8841/0Angiomyofibroblastoma 8826/0Cellular angiofibroma 9160/0Leiomyoma 8890/0Granular cell tumour 9580/0Others
Melanocytic tumoursMalignant melanoma 8720/3Congenital melanocytic naevus 8761/0Acquired melanocytic naevus 8720/0Blue naevus 8780/0Atypical melanocytic naevus of the genital type 8720/0Dysplastic melanocytic naevus 8727/0
Miscellaneous tumoursYolk sac tumour 9071/3Merkel cell tumour 8247/3Peripheral primitive neuroectodermal tumour / 9364/3Ewing tumour 9260/3
Haematopoetic and lymphoid tumoursMalignant lymphoma (specify type)Leukaemia (specify type)
Secondary tumours
314 Tumours of the vulva
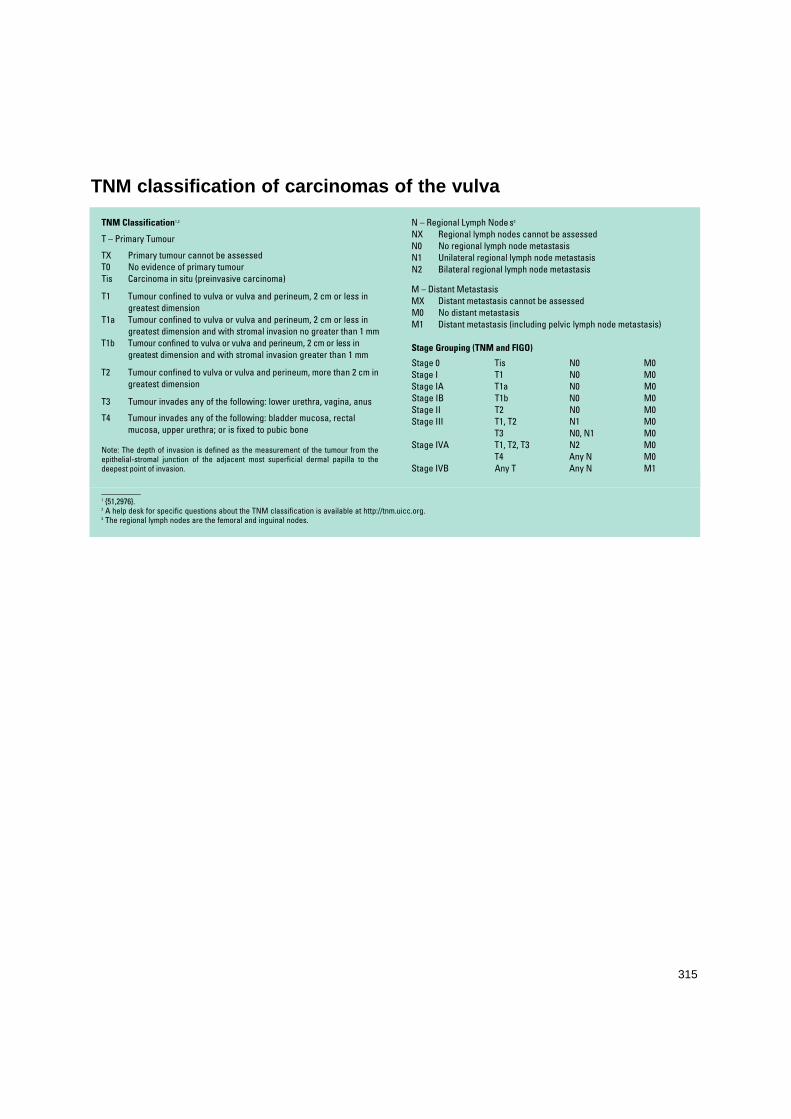
315
_ _ _ _ _ _ _ _ _ _1 {51,2976}.2 A help desk for specific questions about the TNM classification is available at http://tnm.uicc.org. 3 The regional lymph nodes are the femoral and inguinal nodes.
TNM Classification1,2
T – Primary Tumour
TX Primary tumour cannot be assessedT0 No evidence of primary tumourTis Carcinoma in situ (preinvasive carcinoma)
T1 Tumour confined to vulva or vulva and perineum, 2 cm or less in greatest dimension
T1a Tumour confined to vulva or vulva and perineum, 2 cm or less in greatest dimension and with stromal invasion no greater than 1 mm
T1b Tumour confined to vulva or vulva and perineum, 2 cm or less in greatest dimension and with stromal invasion greater than 1 mm
T2 Tumour confined to vulva or vulva and perineum, more than 2 cm ingreatest dimension
T3 Tumour invades any of the following: lower urethra, vagina, anus
T4 Tumour invades any of the following: bladder mucosa, rectalmucosa, upper urethra; or is fixed to pubic bone
Note: The depth of invasion is defined as the measurement of the tumour from theepithelial-stromal junction of the adjacent most superficial dermal papilla to thedeepest point of invasion.
N – Regional Lymph Node s3
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Unilateral regional lymph node metastasisN2 Bilateral regional lymph node metastasis
M – Distant MetastasisMX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis (including pelvic lymph node metastasis)
Stage Grouping (TNM and FIGO)
Stage 0 Tis N0 M0Stage I T1 N0 M0Stage IA T1a N0 M0Stage IB T1b N0 M0Stage II T2 N0 M0Stage III T1, T2 N1 M0
T3 N0, N1 M0Stage IVA T1, T2, T3 N2 M0
T4 Any N M0Stage IVB Any T Any N M1
TNM classification of carcinomas of the vulva
316 Tumours of the vulva
Squamous tumours
DefinitionMalignant or benign epithelial tumourscomposed primarily of squamous cells.
ICD-O codesSquamous cell carcinoma 8070/3
Keratinizing 8071/3Non-keratinizing 8072/3Basaloid 8083/3Warty 8051/3Verrucous 8051/3
Basal cell carcinoma 8090/3Vulvar intraepithelial
neoplasia (VIN), grade 3 / 8077/2squamous cell carcinoma in situ 8070/2Vestibular papilloma 8052/0
Squamous cell carcinoma
DefinitionAn invasive carcinoma composed ofsquamous cells of varying degrees of dif-ferentiation.
EpidemiologySquamous cell carcinoma is the mostcommon malignant tumour of the vulva. Primary squamous cell carcinoma of thevulva occurs more frequently in the olderage group; the reported incidence ratesare 1:100,000 in younger women and 20in 100,000 in the elderly {2804}.
AetiologyIn addition to human papillomavirus(HPV), cigarette smoking is a risk factorfor vulvar carcinoma {611}. However, thespecific aetiology of most vulvar epithe-lial tumours is unknown. The carcinomasassociated with HPV include warty andbasaloid carcinomas with the correspon-ding intraepithelial precursor lesions{584,1106,1541,2180,2936}. Ve r r u c o u scarcinoma is associated with HPV, usual-ly of type 6 or 11. In some cases there isno recognized precursor lesion. Squa-mous cell hyperplasia per se is appar-ently not a precursor of vulvar squamouscell carcinoma {1461}.There are currently four recognized pre-cursor of vulvar carcinoma (See table7.1). Vulvar intraepithelial neoplasia (VIN)of the simpex (differentiated) type is usu-ally associated with lichen sclerosus. Thelatter is also considered to be a precur-sor of keratinizing squamous cell carci-noma and is not HPV associated {3175}.In the retrospective evaluation of vulvec-tomy specimens from women with vulvarsquamous cell carcinoma, the frequencyof identifying associated lichen sclerosusranges from 15-40%, the higher ratebeing observed in deeply invasive carci-nomas {403,1621,3240}. The lifetime riskof squamous cell carcinoma arising invulvar lichen sclerosus is unknown butmay exceed 6% {403,1621,1824,2369,2606}. The squamous cell carcinomasassociated with lichen sclerosus involv-ing the vulva are usually of the keratiniz-ing type.
LocalizationVulvar squamous cell carcinoma is usu-ally solitary and is found most commonlyon the labia minora or majora; the clitorisis the primary site in approximately 10%of cases.
Clinical featuresSigns and symptomsSquamous cell carcinoma may presentas an ulcer, nodule, macule or peduncu-lated mass. Symptoms may be similar tothose seen with VIN, although in moreadvanced cases discharge, bleeding,
pain, odour or self-palpation of a massmay bring the patient to the physician.
Imaging Imaging studies are generally not appli-cable for the detection of vulvar tumours.When the regional lymph nodes are clin-ically suspicious, imaging studies,including computed tomography or mag-netic resonance, are employed, whereavailable, to evaluate pelvic and para-aortic lymph nodes. Dye and technetium-99m labelled colloid have been used todetect inguino-femoral sentinel lymphnodes {646}.
ColposcopyColposcopic examination employing top-ically applied 3% acetic acid to enhancevisualization of lesions and photographicrecording of vulvar lesions may be ofvalue in clinical management and follow-up {3124}
Exfoliative and aspiration cytologyAlthough exfoliative cytology has beenapplied to the evaluation of primarytumours of the vulva, this practice is notcommonly used, and directed biopsy ofidentified lesions is the most effectivemethod of primary diagnosis. Fine needle aspiration cytology is ofvalue in assessing suspicious lymphnodes or subcutaneous nodules {1283}.
MacroscopyMost vulvar squamous carcinomas aresolitary. The tumours may be nodular,verruciform or ulcerated with raised firmedges.
Tumour spread and stagingThe staging of vulvar tumours is by theTNM/FIGO classification {51,2976}.Superficially invasive vulvar carcinoma,stage 1A as defined by FIGO, is a singlefocus of squamous cell carcinoma hav-ing a diameter of 2 cm or less and adepth of invasion of 1 mm or less. Thedefinition includes cases that have capil-lary-like space involvement by tumour.The term "microinvasive carcinoma" isnot recommended.
E.J. WilkinsonM.R. TeixeiraEpithelial tumours
Table 7.01Currently recognized precursors of vulvar squamous cell carcinoma.
(1) Vulvar intraepithelial neoplasia (VIN)and associated human papillomavirus(HPV) infection.
(2) The simplex (differentiated) type ofVIN not associated with HPV infection{1621,3175}.
(3) Lichen sclerosus {1621} with associatedsquamous cell hyperplasia {403}.
(4) Chronic granulomatous vulvar diseasesuch as granuloma inguinale {2628}.

317Epithelial tumours
HistopathologySquamous cell carcinoma is an invasiveneoplasm composed of squamous cellsof varying degrees of diff e re n t i a t i o n .Several morphological variants havebeen described:
KeratinizingKeratinizing squamous cell carcinomacontains keratin pearls.
Non-keratinizingNon-keratinizing squamous cell carcino-ma does not form appreciable keratin; itmay contain small numbers of individual-ly keratinized cells but lacks keratinpearls. Rarely, the tumour is composedpredominantly of spindle-shaped cells{2529}. In some cases the carcinomamay have a sarcoma-like stroma {2778}.
BasaloidBasaloid squamous cell carcinoma iscomposed of nests of immature, basaltype squamous cells with scanty cyto-plasm that resemble closely the cells ofsquamous carcinoma in situ of the cervix.Some keratinization may be evident in thec e n t res of the nests, but keratin pearlsa re rarely present. This tumour may beassociated with HPV infections, pre d o m i-nantly type 16 {1541, 2936}.
Warty Warty (condylomatous) squamous cellcarcinoma has a warty surface and cel-lular features of HPV infection {720,1541,2936}.
VerrucousVerrucous carcinoma is a highly differen-tiated squamous cell carcinoma that hasa hyperkeratinized, undulating, wart ysurface and invades the underlying stro-ma in the form of bulbous pegs with apushing border.Verrucous carcinoma accounts for 1-2%of all vulvar carcinomas and has little orno metastatic potential. The cellular fea-tures include minimal nuclear atypia andabundant eosinophilic cytoplasm. Mitoticfigures are rare and, when present, aretypical. There is usually a pro m i n e n tchronic inflammatory cell infiltrate in thestroma. HPV, especially type 6, has beenidentified in a number of cases. Giantcondyloma (Buschke-Lowenstein tu-mour) is considered by some to be syno-nymous with verrucous carcinoma {100,348,1336,1501}.
Keratoacanthoma-likeThese tumours, often referred to as kera-toacanthoma, may arise on the hair-bear-ing skin of the vulva. They are rapidly
g rowing but are usually self-limited.Histologically, they consist of a centralcrater filled with a glassy squamousepithelial proliferation in which horn ymasses of keratin are pushed upward,while tongues of squamous epitheliuminvade the dermis. Metastasis of so-called keratoacanthoma has beendescribed {1227}. Complete excisionwith a clear histological margin is the rec-ommended treatment.
Variant with tumour giant cellsSquamous cell carcinoma with a promi-nent tumour giant cell component is ahighly aggressive neoplasm that can beconfused with malignant melanoma{3122}.
Tumour measurementsIt is recommended that the following fea-tures should be included in the patholo-gy report {2601,3119}:(1) Depth of invasion (mm).(2) Tumour thickness.(3) Method of measurement of depth ofinvasion and thickness of the tumour.(4) Presence or absence of vascularspace involvement by tumour.(5) Diameter of the tumour, including theclinically measured diameter, if available. In the event that invasion is equivocal
Fig. 7.01 Squamous cell carcinoma, keratinizingtype. Keratin pearls are prominent. Invasion is con-fluent with a desmoplastic stromal response.
Fig. 7.02 Squamous cell carcinoma, basaloid type. Irregular aggregates of poorly differentiated squamouscells without keratinization infiltrate the stroma in the form of interconnecting columns. The tumour is com-posed of poorly differentiated basaloid type cells.

even with additional sectioning, it is rec-ommended that invasion should not bediagnosed {3119}.The following criteria apply to the measure-ment of vulvar squamous cell carcinoma: (1) Thickness: measurement from thesurface, or the granular layer if kera-tinized, to the deepest point of invasion.(2) Depth of invasion: measurement fromthe epithelial-stromal junction of the adja-cent most superficial dermal papillae tothe deepest point of invasion.The preferred measurement is the depthof invasion, as defined above.
Somatic geneticsCytogenetic data exist on 11 squamouscell carcinomas of the vulva {2897,3156}.The most common karyotypic changesare loss of 3p, 8p, 22q, Xp, 10q and 18qand gain of 3q and 11q21. There is aninverse correlation between histologicaldifferentiation and karyotypic complexity.F u rt h e rm o re, a comparative genomichybridization study of 10 cases revealedlosses of 4p, 3p, and 5q and gains of 3qand 8p {1338}. Loss of 10q and 18qseems to be particularly associated witha poor prognosis in squamous cell carci-noma {2897,3156}. On the other hand,the only cytogenetically analysed squa-mous cell carcinoma in situ of the vulva(VIN 3) had a rearrangement of 11p asthe sole anomaly {2818}. TP53 mutation or HPV can independent-ly lead to cell cycle disruption relevant tovulvar squamous cell carc i n o g e n e s i s .Besides mutational inactivation, T P 5 3can be inactivated through binding ofHPV protein E6. PTEN is another genethat is frequently mutated in carcinomasof the vulva {1234}. Both TP53 and PTENmutations have also been detected inVIN, indicating that they are early eventsin vulvar carcinogenesis {1234,1866}.High frequencies of allelic imbalancehave been detected at 1q, 2q, 3p, 5q,8p, 8q, 10p, 10q, 11p, 11q, 15q, 17p,18q, 21q and 22q, most of these irre-spective of HPV status {2256}. This find-ing suggests that despite a diff e re n tpathogenesis both HPV-positive andHPV-negative vulvar squamous cell car-cinomas share several genetic changesduring their progression.
Prognosis and predictive factorsRisk factors for re c u r rence includeadvanced stage, tumour diameter >2.5 cm,m u l t i f o c a l i t y, capillary-like space involve-
ment, associated VIN 2 or VIN 3 andinvolved margins of resection {1235,2004}.The extent of lymph node involvement andmode of treatment may also influence sur-vival {721}. Patients whose tumours have a"spray" or finger-like pattern of invasionhave a poorer survival than those with a"pushing" pattern {1235}.For patients with stage 1A carcinoma, thetherapy is usually local excision with at leasta 1-cm margin of normal tissue {3, 1428}.Inguinofemoral lymph node dissection isusually unnecessary {247,373,374,1105,1428}. The risk of re c u r rence in stage 1Acases is very low, with 5 and 10-year re c u r-re n c e - f ree tumour specific survivals of100% and 94.7%, respectively {1732}. Latere c u r rence or "re o c c u r rence" of a secondsquamous carcinoma in another site withinthe vulva is rare but can occur, and there-f o re long-term follow-up is warranted.
For tumours greater than stage 1A partialor total deep vulvectomy with ipsilateralor bilateral inguino-femoral lymph noderesection may be required. If superficiallymph nodes contain tumour, radiothera-py to the deep pelvic nodes or chemora-diation may be necessary {360,373,1749,2783}.
Basal cell carcinoma
DefinitionAn infiltrating tumour composed predom-inantly of cells resembling the basal cellsof the epidermis.
Clinical featuresThis tumour presents as a slow gro w-ing, locally invasive, but rarely metasta-sizing lesion in the vulva {218,833,1872,2 2 6 0 } .
BAFig. 7.03 Verrucous carcinoma. A The characteristic exophytic and endophytic growth pattern is evident inthe sectioned surface of the tumour on the right side of the field. B The tumour is composed of well differ-entiated squamous epithelium with an undulating surface, minimal cytological atypia and a pushing border.
318 Tumours of the vulva
Fig. 7.04 Basal cell carcinoma. Aggregates of uniform basaloid cells with peripherial palisading arise fromthe basal layer of the overlying squamous epithelium and infiltrate the stroma.
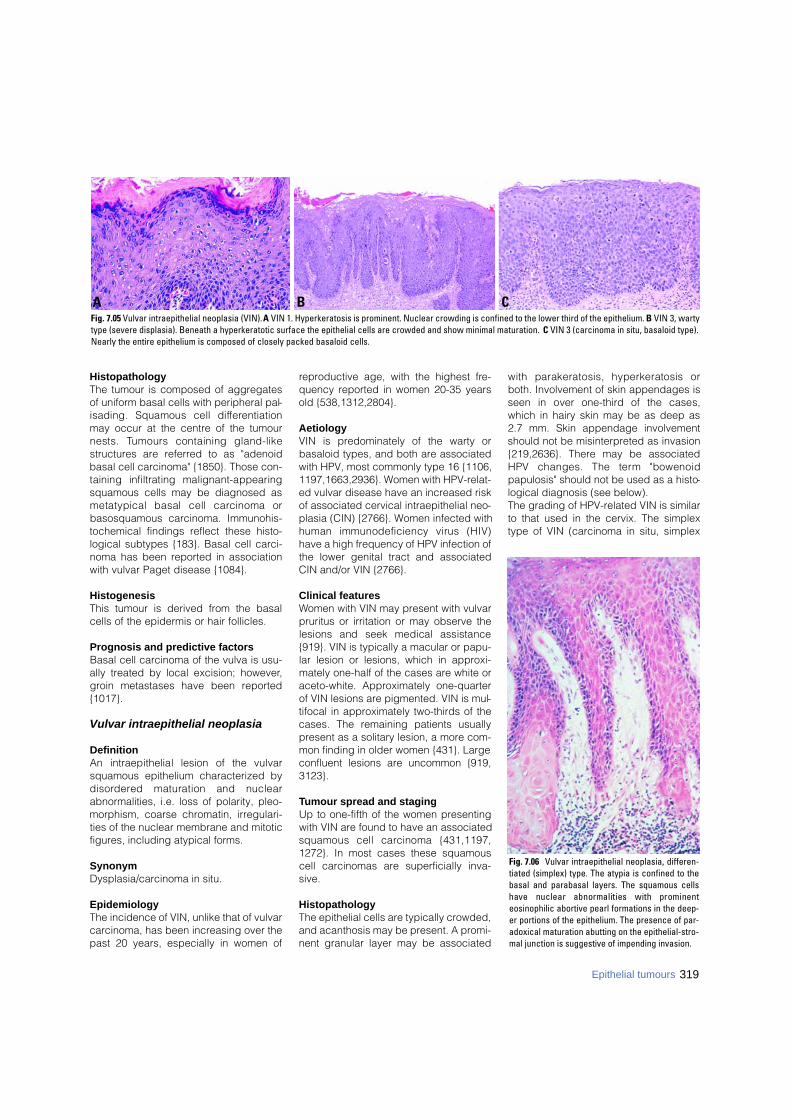
319Epithelial tumours
HistopathologyThe tumour is composed of aggregatesof uniform basal cells with peripheral pal-isading. Squamous cell diff e re n t i a t i o nmay occur at the centre of the tumournests. Tumours containing gland-likestructures are referred to as "adenoidbasal cell carcinoma" {1850}. Those con-taining infiltrating malignant-appearingsquamous cells may be diagnosed asmetatypical basal cell carcinoma orbasosquamous carcinoma. Immunohis-tochemical findings reflect these histo-logical subtypes {183}. Basal cell carci-noma has been reported in associationwith vulvar Paget disease {1084}.
HistogenesisThis tumour is derived from the basalcells of the epidermis or hair follicles.
Prognosis and predictive factorsBasal cell carcinoma of the vulva is usu-ally treated by local excision; however,groin metastases have been reported{1017}.
Vulvar intraepithelial neoplasia
DefinitionAn intraepithelial lesion of the vulvarsquamous epithelium characterized byd i s o rd e red maturation and nuclearabnormalities, i.e. loss of polarity, pleo-morphism, coarse chromatin, irregulari-ties of the nuclear membrane and mitoticfigures, including atypical forms.
SynonymDysplasia/carcinoma in situ.
EpidemiologyThe incidence of VIN, unlike that of vulvarcarcinoma, has been increasing over thepast 20 years, especially in women of
reproductive age, with the highest fre-quency reported in women 20-35 yearsold {538,1312,2804}.
AetiologyVIN is predominately of the warty orbasaloid types, and both are associatedwith HPV, most commonly type 16 {1106,1197,1663,2936}. Women with HPV-relat-ed vulvar disease have an increased riskof associated cervical intraepithelial neo-plasia (CIN) {2766}. Women infected withhuman immunodeficiency virus (HIV)have a high frequency of HPV infection ofthe lower genital tract and associatedCIN and/or VIN {2766}.
Clinical featuresWomen with VIN may present with vulvarpruritus or irritation or may observe thelesions and seek medical assistance{919}. VIN is typically a macular or papu-lar lesion or lesions, which in approxi-mately one-half of the cases are white oraceto-white. Approximately one-quarterof VIN lesions are pigmented. VIN is mul-tifocal in approximately two-thirds of thecases. The remaining patients usuallypresent as a solitary lesion, a more com-mon finding in older women {431}. Largeconfluent lesions are uncommon {919,3123}.
Tumour spread and stagingUp to one-fifth of the women presentingwith VIN are found to have an associatedsquamous cell carcinoma {431,1197,1272}. In most cases these squamouscell carcinomas are superficially inva-sive.
Histopathology The epithelial cells are typically crowded,and acanthosis may be present. A promi-nent granular layer may be associated
with parakeratosis, hyperkeratosis orboth. Involvement of skin appendages isseen in over one-third of the cases,which in hairy skin may be as deep as2.7 mm. Skin appendage involvementshould not be misinterpreted as invasion{219,2636}. There may be associatedHPV changes. The term "bowenoidpapulosis" should not be used as a histo-logical diagnosis (see below). The grading of HPV-related VIN is similarto that used in the cervix. The simplextype of VIN (carcinoma in situ, simplex
Fig. 7.06 Vulvar intraepithelial neoplasia, differen-tiated (simplex) type. The atypia is confined to thebasal and parabasal layers. The squamous cellshave nuclear abnormalities with prominenteosinophilic abortive pearl formations in the deep-er portions of the epithelium. The presence of par-adoxical maturation abutting on the epithelial-stro-mal junction is suggestive of impending invasion.
B CAFig. 7.05 Vulvar intraepithelial neoplasia (VIN). A VIN 1. Hyperkeratosis is prominent. Nuclear crowding is confined to the lower third of the epithelium. B VIN 3, wartytype (severe displasia). Beneath a hyperkeratotic surface the epithelial cells are crowded and show minimal maturation. C VIN 3 (carcinoma in situ, basaloid type).Nearly the entire epithelium is composed of closely packed basaloid cells.

type) is a highly diff e rentiated lesionresembling well differentiated squamouscell carcinoma in which the atypia ismost prominent in or confined to thebasal and parabasal layers of the epithe-lium, where the cells have abundantcytoplasm and form pearls and thenuclei are relatively uniform in size andcontain coarse chromatin and prominentnucleoli {3175}.
Somatic geneticsThe only cytogenetically analysed caseof VIN 3 (squamous cell carcinoma insitu) of the vulva had a rearrangement of11p as the sole anomaly {2818}. Genomic deletions have been demon-strated in the simplex (diff e re n t i a t e d )form of VIN and its subsequent squa-mous carcinoma unrelated to HPV infec-tion {1663}. These also express TP53{1824,3175}.
Prognosis and predictive factors VIN is usually treated by local excision.Laser or other ablative procedure mayalso have a role {1197,1369,3124}.Spontaneous regression of VIN 2 and 3in younger women with papular pigment-ed lesions is recognized, and suchlesions are re f e r red to clinically as
bowenoid papulosis by some investiga-tors {1369}. The recurrence of VIN is wellrecognized, especially in women who areheavy cigarette smokers or positive forHIV.
Condyloma acuminatum
DefinitionA benign neoplasm characterized bypapillary fronds containing fibrovascularcores and lined by stratified squamousepithelium with evidence of HPV infec-tion, usually in the form of koilocytosis.
Tumour spread and stagingCo-infection of the vulva and cervix iswell recognized {1528}. Vulvar carcino-ma in young women has been associat-ed with genital condyloma {2945}.
Histopathology The lesions are typically multiple andpapillomatous or papular. The epitheliumis acanthotic with parabasal hyperplasiaand koilocytosis in the upper portion.Hyperkeratosis and parakeratosis areusual, and binucleated and multinucleat-ed keratinocytes are often present. Therete ridges are elongated and thickened.A chronic inflammatory infiltrate is usual-
ly present within the underlying connec-tive tissue.HPV infection in the vulvar epithelium isexpressed in three broad categories: (1) Fully expressed, with morphologicalfeatures of HPV infection, as seen incondyloma acuminatum(2) Minimally expressed, with only mildmorphological changes, e.g. koilocytosis (3) Latent, in which no characteristicmorphological changes are seen,although HPV can be detected with theuse of molecular techniques {1013}.
Vestibular papilloma
DefinitionA benign papillary tumour with a squa-mous epithelial mucosal surface thatoverlies a delicate fibrovascular stalk.
SynonymsM i c ropapillomatosis labialis, vestibularmicropapillomatosis.These terms are applicable when numer-ous lesions are present.
Clinical featuresThe lesions may be solitary but frequent -ly are multiple, often occurring in clustersnear the hymenal ring, resulting in a con-dition referred to as vestibular papillo-matosis or micropapillomatosis orm i c ropapillomatosis labialis {238,644,980,1930,2277}. They are less than 6 mmin height. Unlike condylomas, they do nottypically respond to podophyllin and/orinterferon {2277}.
HistopathologyThese lesions have papillary architectureand a smooth surface without acanthosisor koilocytotic atypia. They lack the com-plex arborizing architecture of condylo-ma.
AetiologyThe great majority of studies of vestibularm i c ropapillomatosis as defined abovehave demonstrated no relationship ofthese lesions to HPV {238,644,1856,2118,2277}.
Fibroepithelial polyp
DefinitionA polypoid lesion covered by squamousepithelium and containing a central coreof fibrous tissue in which stellate cellswith tapering cytoplasmic processes and
Fig. 7.08 Vestibular papilloma. Smooth surfacedsquamous epithelium without acanthosis orkoilocytotic atypia lines a delicate fibrovasculars t a l k .
Fig. 7.07 Condyloma acuminatum. Papillary frondswith fibrovascular cores are lined by squamousepithelium with hyperkeratosis, acanthosis andkoilocytosis.
320 Tumours of the vulva
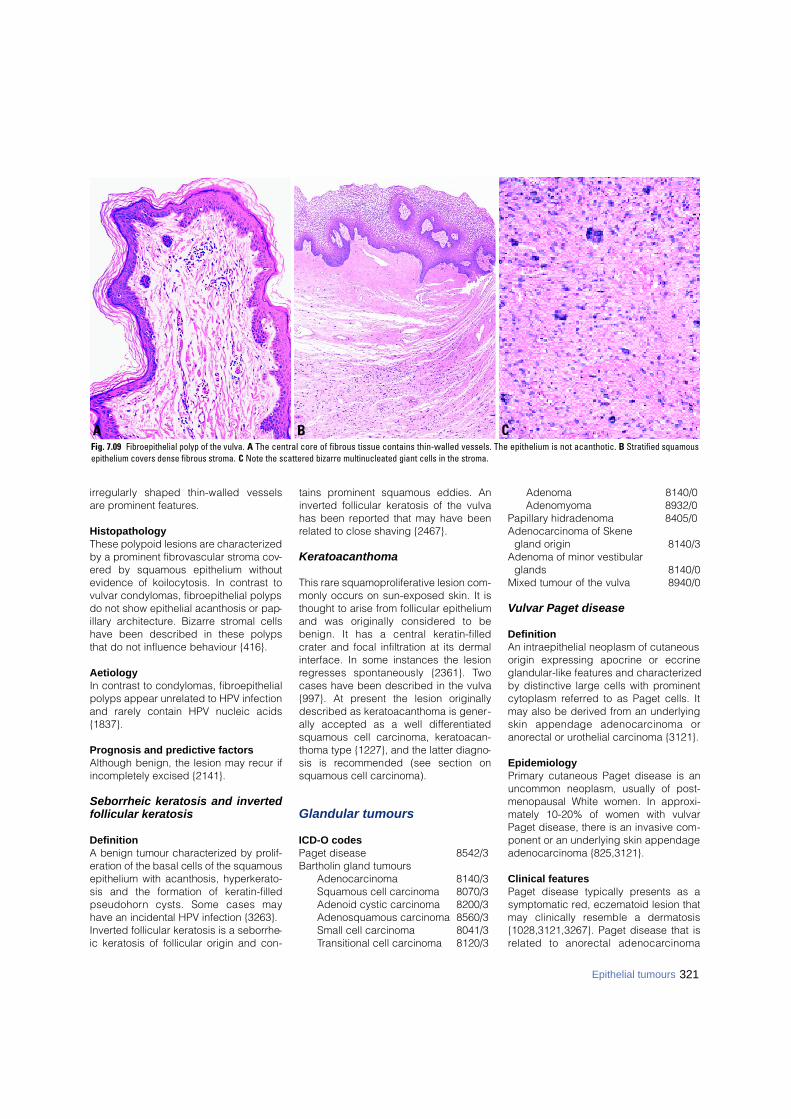
321Epithelial tumours
i r regularly shaped thin-walled vesselsare prominent features.
HistopathologyThese polypoid lesions are characterizedby a prominent fibrovascular stroma cov-ered by squamous epithelium withoutevidence of koilocytosis. In contrast tovulvar condylomas, fibroepithelial polypsdo not show epithelial acanthosis or pap-illary architecture. Bizarre stromal cellshave been described in these polypsthat do not influence behaviour {416}.
AetiologyIn contrast to condylomas, fibroepithelialpolyps appear unrelated to HPV infectionand rarely contain HPV nucleic acids{1837}.
Prognosis and predictive factorsAlthough benign, the lesion may recur ifincompletely excised {2141}.
Seborrheic keratosis and invertedfollicular keratosis
DefinitionA benign tumour characterized by pro l i f-eration of the basal cells of the squamousepithelium with acanthosis, hyperkerato-sis and the formation of keratin-filledp s e u d o h o rn cysts. Some cases mayhave an incidental HPV infection {3263}.Inverted follicular keratosis is a seborrhe-ic keratosis of follicular origin and con-
tains prominent squamous eddies. Aninverted follicular keratosis of the vulvahas been reported that may have beenrelated to close shaving {2467}.
Keratoacanthoma
This rare squamoproliferative lesion com-monly occurs on sun-exposed skin. It isthought to arise from follicular epitheliumand was originally considered to bebenign. It has a central keratin-filledcrater and focal infiltration at its dermalinterface. In some instances the lesionre g resses spontaneously {2361}. Tw ocases have been described in the vulva{997}. At present the lesion originallydescribed as keratoacanthoma is gener-ally accepted as a well differentiatedsquamous cell carcinoma, keratoacan-thoma type {1227}, and the latter diagno-sis is recommended (see section onsquamous cell carcinoma).
Glandular tumours
ICD-O codesPaget disease 8542/3Bartholin gland tumours
Adenocarcinoma 8140/3Squamous cell carcinoma 8070/3Adenoid cystic carcinoma 8200/3Adenosquamous carcinoma 8560/3Small cell carcinoma 8041/3Transitional cell carcinoma 8120/3
Adenoma 8140/0Adenomyoma 8932/0
Papillary hidradenoma 8405/0Adenocarcinoma of Skene
gland origin 8140/3Adenoma of minor vestibular
glands 8140/0Mixed tumour of the vulva 8940/0
Vulvar Paget disease
DefinitionAn intraepithelial neoplasm of cutaneousorigin expressing apocrine or eccrineglandular-like features and characterizedby distinctive large cells with prominentcytoplasm referred to as Paget cells. Itmay also be derived from an underlyingskin appendage adenocarcinoma oranorectal or urothelial carcinoma {3121}.
EpidemiologyPrimary cutaneous Paget disease is anuncommon neoplasm, usually of post-menopausal White women. In approxi-mately 10-20% of women with vulvarPaget disease, there is an invasive com-ponent or an underlying skin appendageadenocarcinoma {825,3121}.
Clinical featuresPaget disease typically presents as asymptomatic red, eczematoid lesion thatmay clinically resemble a derm a t o s i s{1028,3121,3267}. Paget disease that isrelated to anorectal adenocarc i n o m a
Fig. 7.09 Fibroepithelial polyp of the vulva. A The central core of fibrous tissue contains thin-walled vessels. The epithelium is not acanthotic. B Stratified squamousepithelium covers dense fibrous stroma. C Note the scattered bizarre multinucleated giant cells in the stroma.
B CA
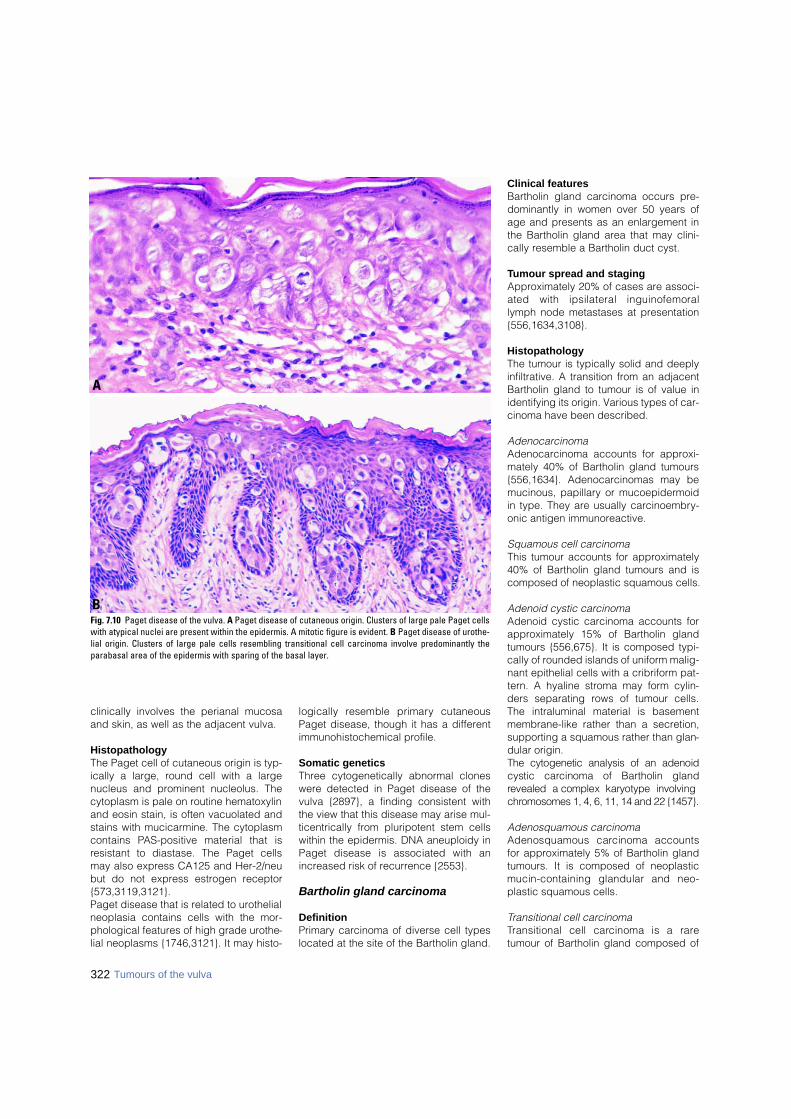
clinically involves the perianal mucosaand skin, as well as the adjacent vulva.
HistopathologyThe Paget cell of cutaneous origin is typ-ically a large, round cell with a largenucleus and prominent nucleolus. Thecytoplasm is pale on routine hematoxylinand eosin stain, is often vacuolated andstains with mucicarmine. The cytoplasmcontains PAS-positive material that isresistant to diastase. The Paget cellsmay also express CA125 and Her-2/neubut do not express estrogen receptor{573,3119,3121}.Paget disease that is related to urothelialneoplasia contains cells with the mor-phological features of high grade urothe-lial neoplasms {1746,3121}. It may histo-
logically resemble primary cutaneousPaget disease, though it has a differentimmunohistochemical profile.
Somatic geneticsThree cytogenetically abnormal cloneswere detected in Paget disease of thevulva {2897}, a finding consistent withthe view that this disease may arise mul-ticentrically from pluripotent stem cellswithin the epidermis. DNA aneuploidy inPaget disease is associated with anincreased risk of recurrence {2553}.
Bartholin gland carcinoma
DefinitionPrimary carcinoma of diverse cell typeslocated at the site of the Bartholin gland.
Clinical featuresBartholin gland carcinoma occurs pre-dominantly in women over 50 years ofage and presents as an enlargement inthe Bartholin gland area that may clini-cally resemble a Bartholin duct cyst.
Tumour spread and stagingApproximately 20% of cases are associ-ated with ipsilateral inguinofemorallymph node metastases at presentation{556,1634,3108}.
HistopathologyThe tumour is typically solid and deeplyinfiltrative. A transition from an adjacentBartholin gland to tumour is of value inidentifying its origin. Various types of car-cinoma have been described.
Adenocarcinoma Adenocarcinoma accounts for approxi-mately 40% of Bartholin gland tumours{556,1634}. Adenocarcinomas may bemucinous, papillary or mucoepidermoidin type. They are usually carcinoembry-onic antigen immunoreactive.
Squamous cell carcinoma This tumour accounts for approximately40% of Bartholin gland tumours and iscomposed of neoplastic squamous cells.
Adenoid cystic carcinoma Adenoid cystic carcinoma accounts forapproximately 15% of Bartholin glandtumours {556,675}. It is composed typi-cally of rounded islands of uniform malig-nant epithelial cells with a cribriform pat-tern. A hyaline stroma may form cylin-ders separating rows of tumour cells.The intraluminal material is basementmembrane-like rather than a secretion,supporting a squamous rather than glan-dular origin. The cytogenetic analysis of an adenoidcystic carcinoma of Bartholin glandrevealed a complex karyotype involvingc h romosomes 1, 4, 6, 11, 14 and 22 {1457}.
Adenosquamous carcinoma Adenosquamous carcinoma accountsfor approximately 5% of Bartholin glandtumours. It is composed of neoplasticmucin-containing glandular and neo-plastic squamous cells.
Transitional cell carcinomaTransitional cell carcinoma is a raretumour of Bartholin gland composed of
322 Tumours of the vulva
Fig. 7.10 Paget disease of the vulva. A Paget disease of cutaneous origin. Clusters of large pale Paget cellswith atypical nuclei are present within the epidermis. A mitotic figure is evident. B Paget disease of urothe-lial origin. Clusters of large pale cells resembling transitional cell carcinoma involve predominantly theparabasal area of the epidermis with sparing of the basal layer.
B
A

neoplastic urothelial-type cells, occa-sionally with a minor component of glan-dular or squamous cells.
Small cell carcinoma This rare highly malignant neoplasm iscomposed of small neuroendocrine cellswith scant cytoplasm and numero u smitotic figures {1361}.
Benign neoplasms of Bartholingland
Adenoma and adenomyomaB a rtholin gland adenoma is a rarebenign tumour of Bartholin gland charac-terized by small clustered closelypacked glands and tubules lined bycolumnar to cuboidal epithelium with col-loid-like secretion arranged in a lobularpattern and contiguous with identifiableB a rtholin gland elements. Bart h o l i ngland adenoma has been reported inassociation with adenoid cystic carcino-ma {1487}. Bartholin gland nodularhyperplasia can be distinguished fromadenoma by the preservation of the nor-
mal duct-acinar relationships present inhyperplasia. Bartholin gland adenomy-oma has a fibromuscular stromal elementthat is immunoreactive for smooth mus-cle actin and desmin as well as a lobularglandular architecture with glands linedby columnar mucin-secreting epithelialcells adjacent to tubules {1487}.
Tumours arising from specializedanogenital mammary-like glands
DefinitionMalignant and benign tumours, usually ofglandular type and resembling neo-plasms of the breast, may arise in spe-cialized anogenital mammary - l i k eglands. These glands and the tumoursthat arise from them are usually identifiedin or adjacent to the intralabial sulcus.Adenocarcinoma with morphological fea-t u res of breast carcinoma has beenre p o rted as a primary vulvar tumour{687}. Such tumours are curre n t l ythought to arise from the specializedanogenital glands and not from ectopicbreast tissue {2991,2992}. The papillary
hidradenoma is an example of a benignneoplasm {2991,2992}. Intraductal ade-nocarcinoma of mammary-type within ahidradenoma has been reported {2212}.
Papillary hidradenomaDefinitionA benign tumour composed of epithelials e c re t o ry cells and underlying myoep-ithelial cells lining complex branchingpapillae with delicate fibrovascular stalks.
EpidemiologyThis tumour is rare in the vulva but is themost common benign glandular neo-plasm at this site.
Clinical featuresIt usually presents as an asymptomaticmass within or adjacent to the intralabialsulcus and may cause bleeding resem-bling carcinoma if the gland prolapsesand/or ulcerates.
HistopathologyThe tumour is distinctly circumscribedand composed of complex papillae and
Table 7.02 Immunohistochemical findings of Paget disease.
Fig. 7.11 Paget disease of the vulva. Note the red,eczematous appearance.
Type of Paget disease CK-7 CK 20 GCDFP-15 CEA UP-III
Primary skin neoplasm + - + + -
Related to anorectal carcinoma + + - + -
Related to urothelial carcinoma + (+) - - +
______Abbreviations for antibodies used as follows:CK = cytokeratin; CEA = carcinoembryonic antigen; GCDFP-15 = gross cystic disease fluid protein-15; UP-III = uroplakin III {2088,3121}.
B CAFig. 7.12 Bartholin gland neoplasms. A Squamous cell carcinoma. Aggregates of neoplastic squamous cells infiltrate Bartholin gland seen on the left. B Adenoidcystic carcinoma. Note the cribriform pattern with the lumens containing basophilic mucin. C Bartholin gland adenoma. A nodule is composed of clustered glandslined by mucinous epithelium.
323Epithelial tumours

324 Tumours of the vulva
glandular elements surrounded byfibrous tissue. Relatively uniform colum-nar epithelial secretory cells with under-lying myoepithelial cells cover the glandsand papillary stalks.
Adenocarcinoma of Skene glandorigin
An adenocarcinoma of Skene gland withassociated metastasis has been re p o rt-ed {2726}. Skene gland is the femalehomologue of the male prostate, and thetumour expresses prostate antigens byi m m u n o h i s t o c h e m i s t ry {2726}. A carc i-noma of Skene duct origin was associ-ated with systemic coagulopathy{ 2 8 9 5 } .
Adenocarcinomas of other types
These tumours may arise fro mendometriosis or ectopic cloacal tissue{307,3126,3237}.
Adenoma of minor vestibularglands
Adenoma of minor vestibular glands isa rare benign tumour composed ofclusters of small glands lined by mucin-s e c reting columnar epithelial cellsarranged in a lobular pattern withoutintervening Bartholin duct elements. Itis usually an incidental finding measur-ing 1-2 mm in diameter, although oneexample was as large as 10 mm.Nodular hyperplasia of the minorvestibular glands may also occur{ 1 4 1 , 2 2 9 5 }
Mixed tumour of the vulva
DefinitionA benign epithelial tumour composed ofepithelial cells arranged in tubules ornests mixed with a fibrous stromal com-ponent that may include chondro i d ,osseous and myxoid elements.
SynonymsPleomorphic adenoma, chondro i dsyringoma.
Clinical featuresMixed tumour of the vulva usually pres-ents as a subcutaneous nodule involvingthe labum majus and/or the Bartholingland area.
HistopathologyThe histological features are similar tothose of mixed tumours of salivaryglands. The tumour with its stromal-likeelements is believed to arise fro mpluripotential myoepithelial cells that arepresent in Bartholin gland, sweat glandsand the specialized anogenital (mam-mary-like) glands of the vulva {2410}.
Prognosis and predictive factorsAlthough these tumours are consideredbenign, insufficient cases of vulvar mixedtumours have been reported to deter-mine their natural history at this site. Thetumour may recur locally. A carcinomaarising in a mixed tumour has beendescribed {2117}. Complete local exci-sion with free margins is the recommend-ed therapy for the primary tumour as wellas for local recurrences.
Tumours of skin appendage origin
DefinitionBenign or malignant tumours differentiat-ing towards hair follicles or sweat orsebaceous glands.
ICD-O codesMalignant sweat gland tumour 8400/3Sebaceous carcinoma 8410/3Syringoma 8407/0Nodular hidradenoma 8402/0Trichoepithelioma 8100/0Trichilemmoma 8102/0
Malignant sweat gland tumours
Vulvar malignant sweat gland tumoursinclude eccrine adenocarcinoma, poro-carcinoma, clear cell hidradenocarcino-ma, and apocrine adenocarcinoma, thelast of which may be associated withPaget disease {3112}.
Sebaceous carcinoma
Vulvar sebaceous carcinoma resemblesits cutaneous counterpart. It is a malig-nant tumour composed of cords andnests of basaloid appearing neoplasticglandular elements with cellular featuresof sebaceous epithelium. The tumourmay be associated with neoplastic seba-ceous cells present in pagetoid nestswithin the parabasal component of theoverlying epithelium and in larger clus-ters near the epithelial surface {405,795}.Sebaceous carcinoma of the vulva maybe associated with VIN {1318}.
BAFig. 7.13 Papillary hidradenoma of the vulva. A Note the circumscribed tumour composed of complex branching papillae. B The epithelial lining is composed of adouble layer of cells, an inner layer of secretory cells and an outer layer of myoepithelial cells.
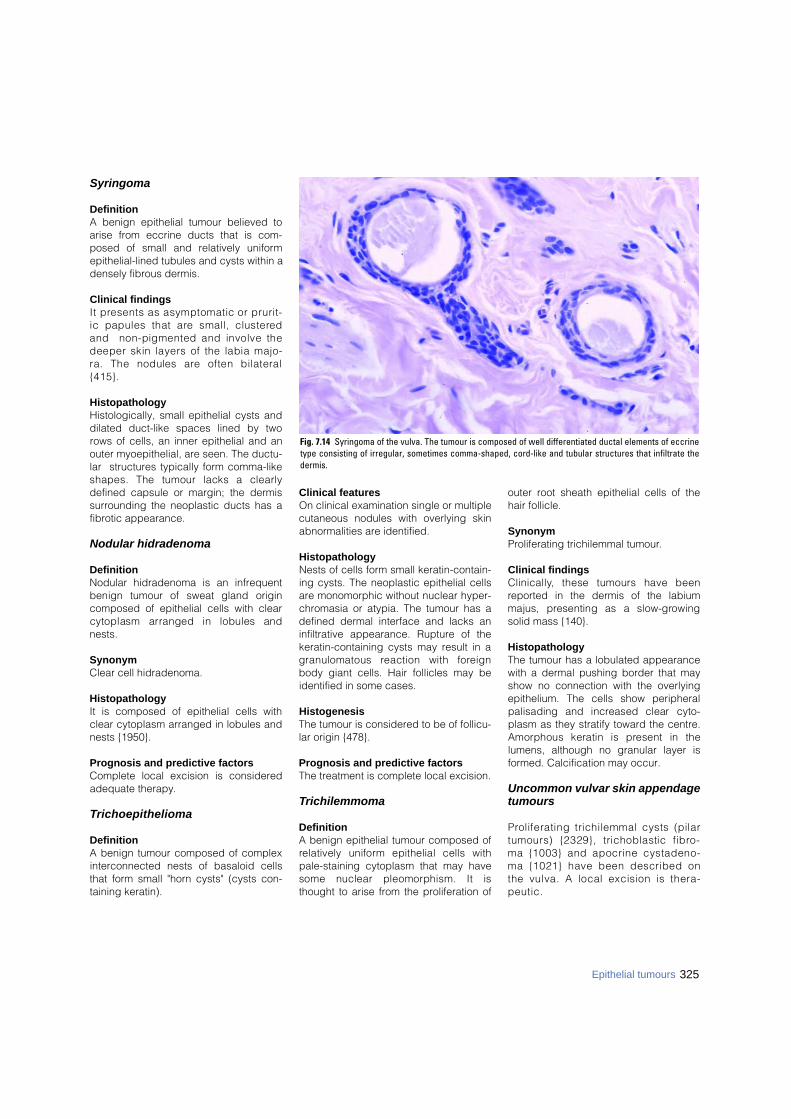
325Epithelial tumours
Syringoma
DefinitionA benign epithelial tumour believed toarise from eccrine ducts that is com-posed of small and relatively uniformepithelial-lined tubules and cysts within adensely fibrous dermis.
Clinical findingsIt presents as asymptomatic or prurit-ic papules that are small, clustere dand non-pigmented and involve thedeeper skin layers of the labia majo-ra. The nodules are often bilateral{ 4 1 5 } .
HistopathologyHistologically, small epithelial cysts anddilated duct-like spaces lined by tworows of cells, an inner epithelial and anouter myoepithelial, are seen. The ductu-lar structures typically form comma-likeshapes. The tumour lacks a clearlydefined capsule or margin; the dermissurrounding the neoplastic ducts has afibrotic appearance.
Nodular hidradenoma
DefinitionNodular hidradenoma is an infrequentbenign tumour of sweat gland origincomposed of epithelial cells with clearcytoplasm arranged in lobules andnests.
SynonymClear cell hidradenoma.
HistopathologyIt is composed of epithelial cells withclear cytoplasm arranged in lobules andnests {1950}.
Prognosis and predictive factorsComplete local excision is consideredadequate therapy.
Tr i c h o e p i t h e l i o m a
Definition A benign tumour composed of complexinterconnected nests of basaloid cellsthat form small "horn cysts" (cysts con-taining keratin).
Clinical featuresOn clinical examination single or multiplecutaneous nodules with overlying skinabnormalities are identified.
HistopathologyNests of cells form small keratin-contain-ing cysts. The neoplastic epithelial cellsare monomorphic without nuclear hyper-chromasia or atypia. The tumour has adefined dermal interface and lacks aninfiltrative appearance. Rupture of thekeratin-containing cysts may result in agranulomatous reaction with fore i g nbody giant cells. Hair follicles may beidentified in some cases.
HistogenesisThe tumour is considered to be of follicu-lar origin {478}.
Prognosis and predictive factorsThe treatment is complete local excision.
Trichilemmoma
Definition A benign epithelial tumour composed ofrelatively uniform epithelial cells withpale-staining cytoplasm that may havesome nuclear pleomorphism. It isthought to arise from the proliferation of
outer root sheath epithelial cells of thehair follicle.
Synonym Proliferating trichilemmal tumour.
Clinical findingsC l i n i c a l l y, these tumours have beenreported in the dermis of the labiummajus, presenting as a slow-gro w i n gsolid mass {140}.
HistopathologyThe tumour has a lobulated appearancewith a dermal pushing border that mayshow no connection with the overlyingepithelium. The cells show peripheralpalisading and increased clear cyto-plasm as they stratify toward the centre.Amorphous keratin is present in thelumens, although no granular layer isformed. Calcification may occur.
Uncommon vulvar skin appendagetumours
P roliferating trichilemmal cysts (pilartumours) {2329}, trichoblastic fibro-ma {1003} and apocrine cystadeno-ma {1021} have been described onthe vulva. A local excision is thera-p e u t i c .
Fig. 7.14 Syringoma of the vulva. The tumour is composed of well differentiated ductal elements of eccrinetype consisting of irregular, sometimes comma-shaped, cord-like and tubular structures that infiltrate thedermis.
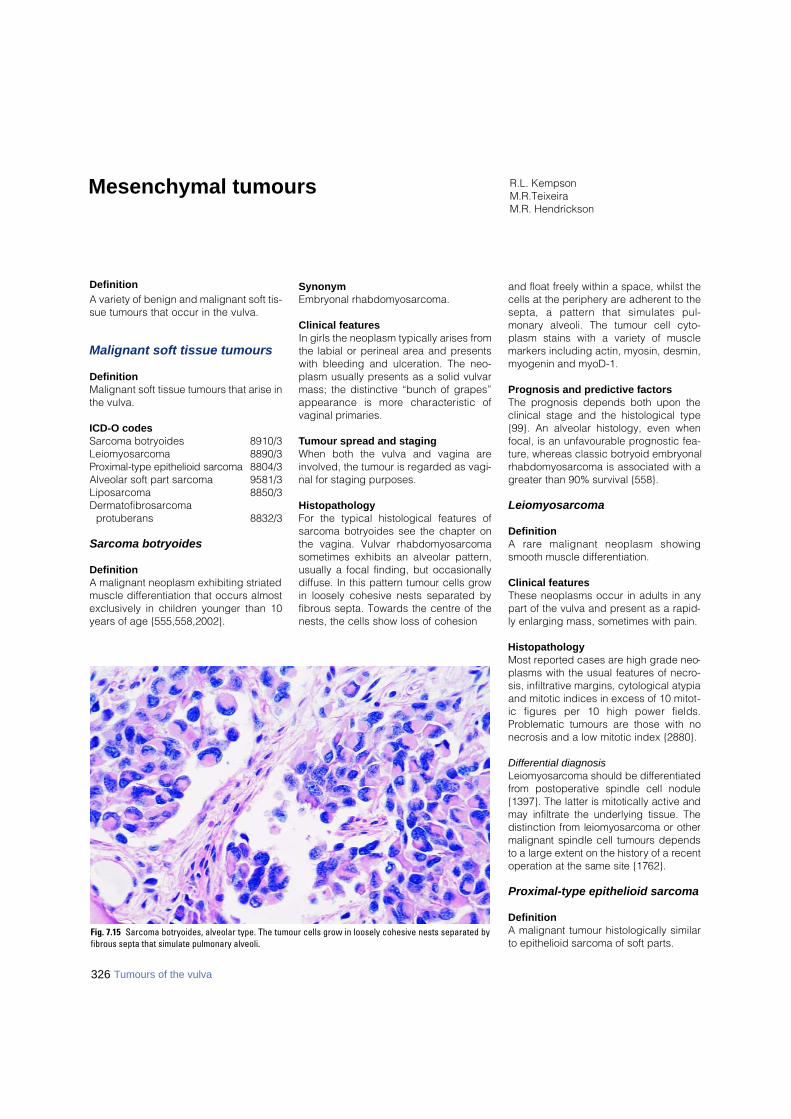
DefinitionA variety of benign and malignant soft tis-sue tumours that occur in the vulva.
Malignant soft tissue tumours
DefinitionMalignant soft tissue tumours that arise inthe vulva.
ICD-O codesSarcoma botryoides 8910/3Leiomyosarcoma 8890/3P roximal-type epithelioid sarc o m a 8804/3Alveolar soft part sarcoma 9581/3Liposarcoma 8850/3Dermatofibrosarcoma
protuberans 8832/3
Sarcoma botryoides
DefinitionA malignant neoplasm exhibiting striatedmuscle differentiation that occurs almostexclusively in children younger than 10years of age {555,558,2002}.
SynonymEmbryonal rhabdomyosarcoma.
Clinical featuresIn girls the neoplasm typically arises fromthe labial or perineal area and presentswith bleeding and ulceration. The neo-plasm usually presents as a solid vulvarmass; the distinctive “bunch of grapes”appearance is more characteristic ofvaginal primaries.
Tumour spread and stagingWhen both the vulva and vagina areinvolved, the tumour is regarded as vagi-nal for staging purposes.
HistopathologyFor the typical histological features ofsarcoma botryoides see the chapter onthe vagina. Vulvar rhabdomyosarcomasometimes exhibits an alveolar pattern,usually a focal finding, but occasionallydiffuse. In this pattern tumour cells growin loosely cohesive nests separated byfibrous septa. Towards the centre of thenests, the cells show loss of cohesion
and float freely within a space, whilst thecells at the periphery are adherent to thesepta, a pattern that simulates pul-monary alveoli. The tumour cell cyto-plasm stains with a variety of musclemarkers including actin, myosin, desmin,myogenin and myoD-1.
Prognosis and predictive factorsThe prognosis depends both upon theclinical stage and the histological type{99}. An alveolar histology, even whenfocal, is an unfavourable prognostic fea-ture, whereas classic botryoid embryonalrhabdomyosarcoma is associated with agreater than 90% survival {558}.
Leiomyosarcoma
DefinitionA rare malignant neoplasm showingsmooth muscle differentiation.
Clinical featuresThese neoplasms occur in adults in anypart of the vulva and present as a rapid-ly enlarging mass, sometimes with pain.
HistopathologyMost reported cases are high grade neo-plasms with the usual features of necro-sis, infiltrative margins, cytological atypiaand mitotic indices in excess of 10 mitot-ic figures per 10 high power fields.Problematic tumours are those with nonecrosis and a low mitotic index {2880}.
Differential diagnosisL e i o m y o s a rcoma should be diff e re n t i a t e df rom postoperative spindle cell nodule{1397}. The latter is mitotically active andmay infiltrate the underlying tissue. Thedistinction from leiomyosarcoma or othermalignant spindle cell tumours dependsto a large extent on the history of a re c e n toperation at the same site {1762}.
Proximal-type epithelioid sarcoma
DefinitionA malignant tumour histologically similarto epithelioid sarcoma of soft parts.
R.L. KempsonM.R.Teixeira M.R. Hendrickson
Mesenchymal tumours
Fig. 7.15 Sarcoma botryoides, alveolar type. The tumour cells grow in loosely cohesive nests separated byfibrous septa that simulate pulmonary alveoli.
326 Tumours of the vulva
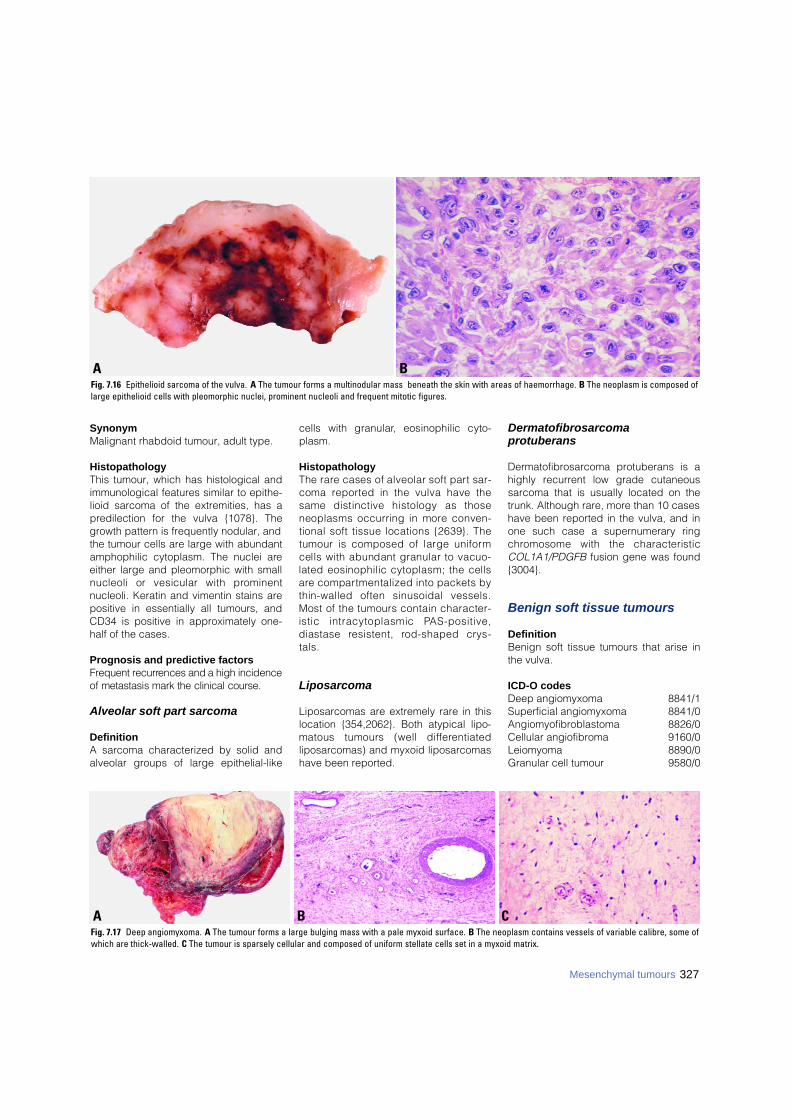
327Mesenchymal tumours
SynonymMalignant rhabdoid tumour, adult type.
HistopathologyThis tumour, which has histological andimmunological features similar to epithe-lioid sarcoma of the extremities, has apredilection for the vulva {1078}. Thegrowth pattern is frequently nodular, andthe tumour cells are large with abundantamphophilic cytoplasm. The nuclei areeither large and pleomorphic with smallnucleoli or vesicular with pro m i n e n tnucleoli. Keratin and vimentin stains arepositive in essentially all tumours, andCD34 is positive in approximately one-half of the cases.
Prognosis and predictive factorsF requent re c u r rences and a high incidenceof metastasis mark the clinical course.
Alveolar soft part sarcoma
DefinitionA sarcoma characterized by solid andalveolar groups of large epithelial-like
cells with granular, eosinophilic cyto-plasm.
HistopathologyThe rare cases of alveolar soft part sar-coma re p o rted in the vulva have thesame distinctive histology as thoseneoplasms occurring in more conven-tional soft tissue locations {2639}. Thetumour is composed of large uniformcells with abundant granular to vacuo-lated eosinophilic cytoplasm; the cellsa re compartmentalized into packets bythin-walled often sinusoidal vessels.Most of the tumours contain character-istic intracytoplasmic PA S - p o s i t i v e ,diastase resistent, rod-shaped cry s-t a l s .
Liposarcoma
Liposarcomas are extremely rare in thislocation {354,2062}. Both atypical lipo-matous tumours (well diff e re n t i a t e dliposarcomas) and myxoid liposarcomashave been reported.
Dermatofibrosarcoma protuberans
Dermatofibrosarcoma protuberans is ahighly recurrent low grade cutaneoussarcoma that is usually located on thetrunk. Although rare, more than 10 caseshave been reported in the vulva, and inone such case a supernumerary ringc h romosome with the characteristicCOL1A1/PDGFB fusion gene was found{3004}.
Benign soft tissue tumours
DefinitionBenign soft tissue tumours that arise inthe vulva.
ICD-O codesDeep angiomyxoma 8841/1Superficial angiomyxoma 8841/0Angiomyofibroblastoma 8826/0Cellular angiofibroma 9160/0Leiomyoma 8890/0Granular cell tumour 9580/0
B CAFig. 7.17 Deep angiomyxoma. A The tumour forms a large bulging mass with a pale myxoid surface. B The neoplasm contains vessels of variable calibre, some ofwhich are thick-walled. C The tumour is sparsely cellular and composed of uniform stellate cells set in a myxoid matrix.
BAFig. 7.16 Epithelioid sarcoma of the vulva. A The tumour forms a multinodular mass beneath the skin with areas of haemorrhage. B The neoplasm is composed oflarge epithelioid cells with pleomorphic nuclei, prominent nucleoli and frequent mitotic figures.
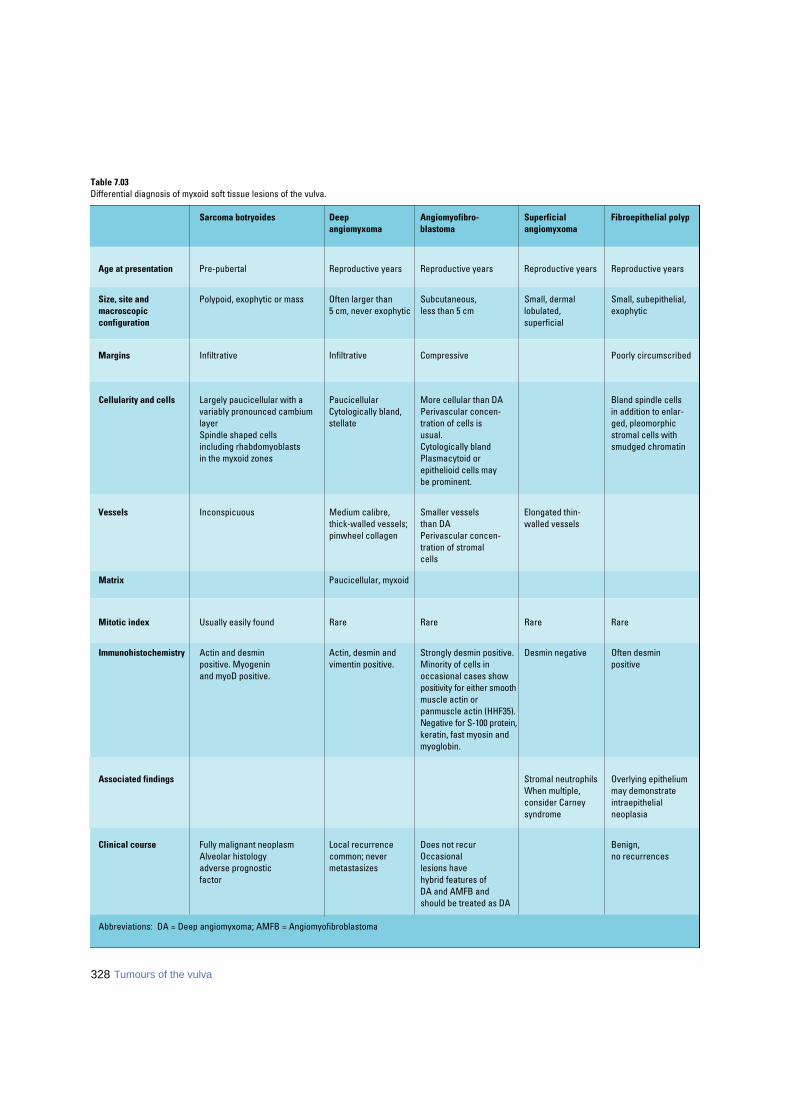
328 Tumours of the vulva
Table 7.03Differential diagnosis of myxoid soft tissue lesions of the vulva.
Abbreviations: DA = Deep angiomyxoma; AMFB = Angiomyofibroblastoma
Sarcoma botryoides Deep Angiomyofibro- Superficial Fibroepithelial polypangiomyxoma blastoma angiomyxoma
Age at presentation Pre-pubertal Reproductive years Reproductive years Reproductive years Reproductive years
Size, site and Polypoid, exophytic or mass Often larger than Subcutaneous, Small, dermal Small, subepithelial,macroscopic 5 cm, never exophytic less than 5 cm lobulated, exophyticconfiguration superficial
Margins Infiltrative Infiltrative Compressive Poorly circumscribed
Cellularity and cells Largely paucicellular with a Paucicellular More cellular than DA Bland spindle cellsvariably pronounced cambium Cytologically bland, Perivascular concen- in addition to enlar-layer stellate tration of cells is ged, pleomorphicSpindle shaped cells usual. stromal cells with including rhabdomyoblasts Cytologically bland smudged chromatinin the myxoid zones Plasmacytoid or
epithelioid cells maybe prominent.
Vessels Inconspicuous Medium calibre, Smaller vessels Elongated thin-thick-walled vessels; than DA walled vesselspinwheel collagen Perivascular concen-
tration of stromalcells
Matrix Paucicellular, myxoid
Mitotic index Usually easily found Rare Rare Rare Rare
Immunohistochemistry Actin and desmin Actin, desmin and Strongly desmin positive. Desmin negative Often desmin positive. Myogenin vimentin positive. Minority of cells in positiveand myoD positive. occasional cases show
positivity for either smooth muscle actin or panmuscle actin (HHF35).Negative for S-100 protein,keratin, fast myosin and myoglobin.
Associated findings Stromal neutrophils Overlying epitheliumWhen multiple, may demonstrateconsider Carney intraepithelial syndrome neoplasia
Clinical course Fully malignant neoplasm Local recurrence Does not recur Benign, Alveolar histology common; never Occasional no recurrencesadverse prognostic metastasizes lesions have factor hybrid features of
DA and AMFB andshould be treated as DA
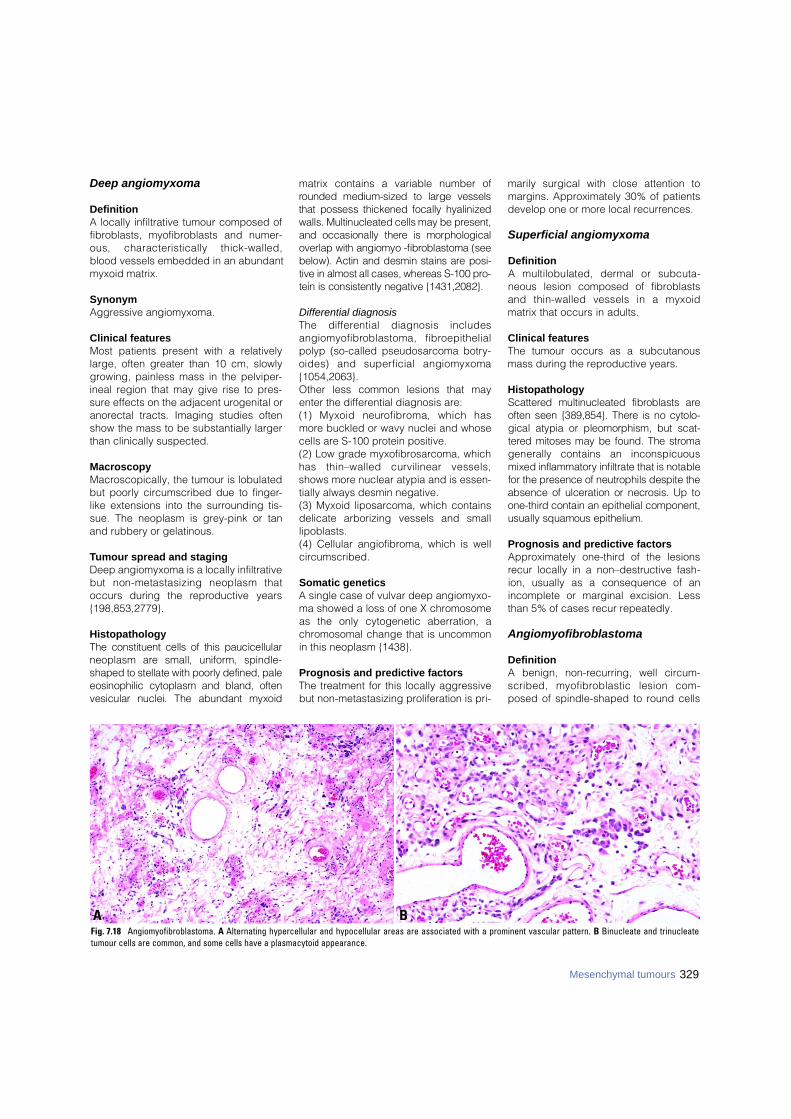
329Mesenchymal tumours
Deep angiomyxoma
DefinitionA locally infiltrative tumour composed offibroblasts, myofibroblasts and numer-ous, characteristically thick-walled,blood vessels embedded in an abundantmyxoid matrix.
SynonymAggressive angiomyxoma.
Clinical featuresMost patients present with a relativelylarge, often greater than 10 cm, slowlygrowing, painless mass in the pelviper-ineal region that may give rise to pres-sure effects on the adjacent urogenital oranorectal tracts. Imaging studies oftenshow the mass to be substantially largerthan clinically suspected.
MacroscopyMacroscopically, the tumour is lobulatedbut poorly circumscribed due to finger-like extensions into the surrounding tis-sue. The neoplasm is grey-pink or tanand rubbery or gelatinous.
Tumour spread and stagingDeep angiomyxoma is a locally infiltrativebut non-metastasizing neoplasm thatoccurs during the re p roductive years{198,853,2779}.
HistopathologyThe constituent cells of this paucicellularneoplasm are small, uniform, spindle-shaped to stellate with poorly defined, paleeosinophilic cytoplasm and bland, oftenvesicular nuclei. The abundant myxoid
matrix contains a variable number ofrounded medium-sized to large vesselsthat possess thickened focally hyalinizedwalls. Multinucleated cells may be pre s e n t ,and occasionally there is morphologicaloverlap with angiomyo -fibroblastoma (seebelow). Actin and desmin stains are posi-tive in almost all cases, whereas S-100 pro-tein is consistently negative {1431,2082}.
Differential diagnosisThe diff e rential diagnosis includesa n g i o m y o f i b roblastoma, fibro e p i t h e l i a lpolyp (so-called pseudosarcoma botry-oides) and superficial angiomyxoma{1054,2063}.Other less common lesions that mayenter the differential diagnosis are:(1) Myxoid neuro f i b roma, which hasmore buckled or wavy nuclei and whosecells are S-100 protein positive.(2) Low grade myxofibrosarcoma, whichhas thin–walled curvilinear vessels,shows more nuclear atypia and is essen-tially always desmin negative.(3) Myxoid liposarcoma, which containsdelicate arborizing vessels and smalllipoblasts.(4) Cellular angiofibroma, which is wellcircumscribed.
Somatic geneticsA single case of vulvar deep angiomyxo-ma showed a loss of one X chromosomeas the only cytogenetic aberration, achromosomal change that is uncommonin this neoplasm {1438}.
Prognosis and predictive factorsThe treatment for this locally aggressivebut non-metastasizing proliferation is pri-
marily surgical with close attention tomargins. Approximately 30% of patientsdevelop one or more local recurrences.
Superficial angiomyxoma
DefinitionA multilobulated, dermal or subcuta-neous lesion composed of fibroblastsand thin-walled vessels in a myxoidmatrix that occurs in adults.
Clinical featuresThe tumour occurs as a subcutanousmass during the reproductive years.
HistopathologyS c a t t e red multinucleated fibroblasts areoften seen {389,854}. There is no cytolo-gical atypia or pleomorphism, but scat-t e red mitoses may be found. The stro m agenerally contains an inconspicuousmixed inflammatory infiltrate that is notablefor the presence of neutrophils despite theabsence of ulceration or necrosis. Up too n e - t h i rd contain an epithelial component,usually squamous epithelium.
Prognosis and predictive factorsApproximately one-third of the lesionsrecur locally in a non–destructive fash-ion, usually as a consequence of anincomplete or marginal excision. Lessthan 5% of cases recur repeatedly.
Angiomyofibroblastoma
DefinitionA benign, non-recurring, well circ u m-scribed, myofibroblastic lesion com-posed of spindle-shaped to round cells
BAFig. 7.18 Angiomyofibroblastoma. A Alternating hypercellular and hypocellular areas are associated with a prominent vascular pattern. B Binucleate and trinucleatetumour cells are common, and some cells have a plasmacytoid appearance.

330 Tumours of the vulva
that tend to concentrate around vessels{890,1054,2019,2082}.
Clinical featuresA n g i o m y o f i b roblastoma occurs in thereproductive years and usually presentsas a slowly growing, painless, well cir-cumscribed, subcutaneous mass meas-uring less than 5 cm in maximum diame-ter.
MacroscopyM a c ro s c o p i c a l l y, a narrow fibro u spseudocapsule delimits these tumours.
HistopathologyAt low power angiomyofibro b l a s t o m ashows alternating hypercellular andhypocellular areas associated with aprominent vascular pattern throughout.Binucleate or multinucleate tumour cellsa re common, and some cells havedenser, more hyaline cytoplasm, impart-ing a plasmacytoid appearance. Mitosesare very infrequent. The constituent cellsare desmin positive. The major differen-tial diagnostic considerations are deepangiomyxoma and fibroepithelial polyp.
Cellular angiofibroma
DefinitionA recently described distinctive benignmesenchymal tumour composed ofbland spindle-shaped cells admixed withnumerous hyalinized blood vessels.
Clinical featuresThe tumour typically presents as a cir-cumscribed solid rubbery vulvar mass inmiddle-aged women.
HistopathologyCellular angiofibroma is usually a well cir-cumscribed cellular lesion that is com-posed of bland spindle-shaped cellsinterspersed with medium to small bloodvessels, which typically have thickhyalinized walls {597,1818,2063}. Matureadipocytes, especially around theperiphery of the lesion, are a characteris-tic feature.Cellular angiofibroma is vimentin-positiveand desmin-negative, an immunoprofilethat differentiates this tumour from deepangiomyxoma and angiomyofibro b l a s-toma.
Prognosis and predictive factorsA local recurrence following excision hasbeen described in a single case {1818}.
LeiomyomaThese benign neoplasms do not diff e rm a c roscopically or histologically fro mleiomyomas encountered elsewhere in thefemale genital tract and are treated bysimple excision. Problematic smooth mus-cle neoplasms are those that are gre a t e rthan 7.0 cm in greatest dimension, haveinfiltrative margins and a mitotic index inexcess of 5 per 10 high power fields{2880} (see section on leiomyosarc o m a ) .
Granular cell tumour
DefinitionA tumour composed of cells with uniformcentral nuclei and abundant granular,slightly basophilic cytoplasm.
HistopathologyThese have the same appearance as inother more common sites. A proliferation ofcells with small uniform nuclei and abun-dant, granular, slightly basophilic cyto-plasm diffusely involves the superficial con-nective tissue {2554}. The tumour cells areu n i f o rmly S-100 protein positive. Of part i c u-lar importance in the vulva is the tendencyfor the overlying squamous epithelium toundergo pseudoepitheliomatous hyperpla-sia and simulate a well diff e rentiated squa-mous carcinoma {3138}. Malignant vari-eties are rare and show high cellularity,nuclear pleomorphism, tumour cell necro-sis and frequent mitotic figures {824}.
Other benign tumours and tumour-like conditionsOther benign tumours and tumour-likeconditions that occur in the vulva includelipoma, haemangioma, angiokeratoma,pyogenic granuloma (lobular capillaryhaemangioma), lymphangioma, neurofi-b roma, schwannoma, glomus tumour,rhabdomyoma and post-operative spin-dle cell nodule {1762}. The histologicalfeatures are similar to their appearancein more common sites.
Fig. 7.19 Granular cell tumour of the vulva. The neoplasm is composed of cells with abundant granular cyto-plasm and small uniform nuclei between pegs of proliferative squamous epithelium.
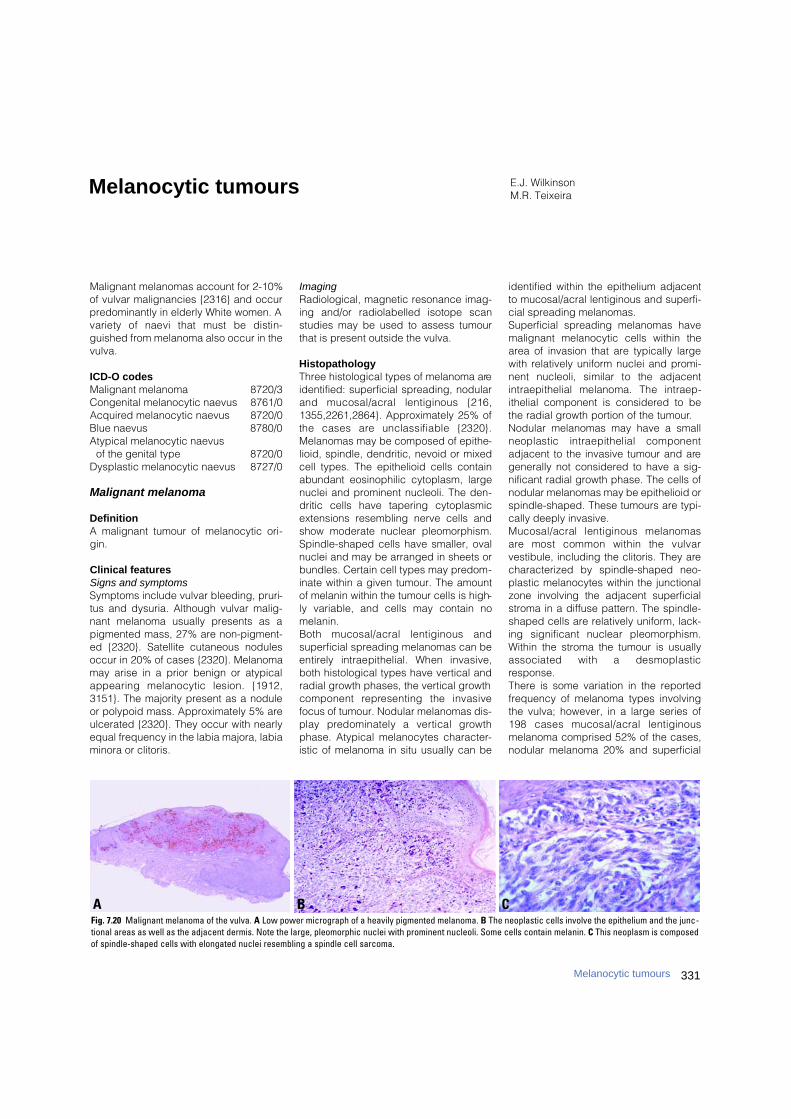
331Melanocytic tumours
Malignant melanomas account for 2-10%of vulvar malignancies {2316} and occurpredominantly in elderly White women. Avariety of naevi that must be distin-guished from melanoma also occur in thevulva.
ICD-O codesMalignant melanoma 8720/3Congenital melanocytic naevus 8761/0Acquired melanocytic naevus 8720/0Blue naevus 8780/0Atypical melanocytic naevus
of the genital type 8720/0Dysplastic melanocytic naevus 8727/0
Malignant melanoma
DefinitionA malignant tumour of melanocytic ori-gin.
Clinical featuresSigns and symptomsSymptoms include vulvar bleeding, pruri-tus and dysuria. Although vulvar malig-nant melanoma usually presents as apigmented mass, 27% are non-pigment-ed {2320}. Satellite cutaneous nodulesoccur in 20% of cases {2320}. Melanomamay arise in a prior benign or atypicalappearing melanocytic lesion. {1912,3151}. The majority present as a noduleor polypoid mass. Approximately 5% areulcerated {2320}. They occur with nearlyequal frequency in the labia majora, labiaminora or clitoris.
ImagingRadiological, magnetic resonance imag-ing and/or radiolabelled isotope scanstudies may be used to assess tumourthat is present outside the vulva.
HistopathologyThree histological types of melanoma areidentified: superficial spreading, nodularand mucosal/acral lentiginous {216,1355,2261,2864}. Approximately 25% ofthe cases are unclassifiable {2320}.Melanomas may be composed of epithe-lioid, spindle, dendritic, nevoid or mixedcell types. The epithelioid cells containabundant eosinophilic cytoplasm, largenuclei and prominent nucleoli. The den-dritic cells have tapering cytoplasmicextensions resembling nerve cells andshow moderate nuclear pleomorphism.Spindle-shaped cells have smaller, ovalnuclei and may be arranged in sheets orbundles. Certain cell types may predom-inate within a given tumour. The amountof melanin within the tumour cells is high-ly variable, and cells may contain nomelanin. Both mucosal/acral lentiginous andsuperficial spreading melanomas can bee n t i rely intraepithelial. When invasive,both histological types have vertical andradial growth phases, the vertical growthcomponent re p resenting the invasivefocus of tumour. Nodular melanomas dis-play predominately a vertical gro w t hphase. Atypical melanocytes character-istic of melanoma in situ usually can be
identified within the epithelium adjacentto mucosal/acral lentiginous and superfi-cial spreading melanomas. Superficial spreading melanomas havemalignant melanocytic cells within thearea of invasion that are typically largewith relatively uniform nuclei and promi-nent nucleoli, similar to the adjacentintraepithelial melanoma. The intraep-ithelial component is considered to bethe radial growth portion of the tumour.Nodular melanomas may have a smallneoplastic intraepithelial componentadjacent to the invasive tumour and aregenerally not considered to have a sig-nificant radial growth phase. The cells ofnodular melanomas may be epithelioid orspindle-shaped. These tumours are typi-cally deeply invasive.Mucosal/acral lentiginous melanomasa re most common within the vulvarvestibule, including the clitoris. They arecharacterized by spindle-shaped neo-plastic melanocytes within the junctionalzone involving the adjacent superficialstroma in a diffuse pattern. The spindle-shaped cells are relatively uniform, lack-ing significant nuclear pleomorphism.Within the stroma the tumour is usuallyassociated with a desmoplasticresponse. There is some variation in the reportedfrequency of melanoma types involvingthe vulva; however, in a large series of198 cases mucosal/acral lentiginousmelanoma comprised 52% of the cases,nodular melanoma 20% and superficial
E.J. WilkinsonM.R. TeixeiraMelanocytic tumours
B CAFig. 7.20 Malignant melanoma of the vulva. A Low power micrograph of a heavily pigmented melanoma. B The neoplastic cells involve the epithelium and the junc-tional areas as well as the adjacent dermis. Note the large, pleomorphic nuclei with prominent nucleoli. Some cells contain melanin. C This neoplasm is composedof spindle-shaped cells with elongated nuclei resembling a spindle cell sarcoma.
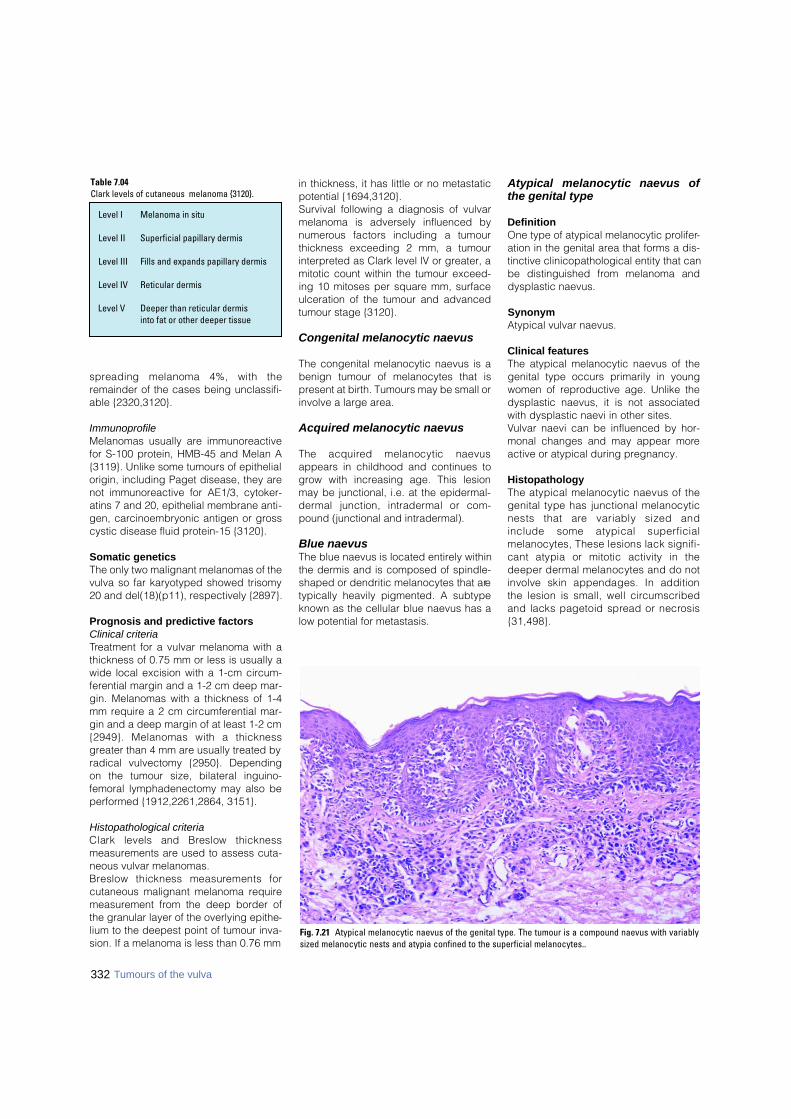
332 Tumours of the vulva
s p reading melanoma 4%, with theremainder of the cases being unclassifi-able {2320,3120}.
ImmunoprofileMelanomas usually are immunoreactivefor S-100 protein, HMB-45 and Melan A{3119}. Unlike some tumours of epithelialorigin, including Paget disease, they arenot immunoreactive for AE1/3, cytoker-atins 7 and 20, epithelial membrane anti-gen, carcinoembryonic antigen or grosscystic disease fluid protein-15 {3120}.
Somatic geneticsThe only two malignant melanomas of thevulva so far karyotyped showed trisomy20 and del(18)(p11), respectively {2897}.
Prognosis and predictive factorsClinical criteriaTreatment for a vulvar melanoma with athickness of 0.75 mm or less is usually awide local excision with a 1-cm circum-ferential margin and a 1-2 cm deep mar-gin. Melanomas with a thickness of 1-4mm require a 2 cm circumferential mar-gin and a deep margin of at least 1-2 cm{2949}. Melanomas with a thicknessgreater than 4 mm are usually treated byradical vulvectomy {2950}. Dependingon the tumour size, bilateral inguino-femoral lymphadenectomy may also beperformed {1912,2261,2864, 3151}.
Histopathological criteriaClark levels and Breslow thicknessmeasurements are used to assess cuta-neous vulvar melanomas. B reslow thickness measurements forcutaneous malignant melanoma requiremeasurement from the deep border ofthe granular layer of the overlying epithe-lium to the deepest point of tumour inva-sion. If a melanoma is less than 0.76 mm
in thickness, it has little or no metastaticpotential {1694,3120}.Survival following a diagnosis of vulvarmelanoma is adversely influenced byn u m e rous factors including a tumourthickness exceeding 2 mm, a tumourinterpreted as Clark level lV or greater, amitotic count within the tumour exceed-ing 10 mitoses per square mm, surfaceulceration of the tumour and advancedtumour stage {3120}.
Congenital melanocytic naevus
The congenital melanocytic naevus is abenign tumour of melanocytes that ispresent at birth. Tumours may be small orinvolve a large area.
Acquired melanocytic naevus
The acquired melanocytic naevusappears in childhood and continues togrow with increasing age. This lesionmay be junctional, i.e. at the epidermal-d e rmal junction, intradermal or com-pound (junctional and intradermal).
Blue naevusThe blue naevus is located entirely withinthe dermis and is composed of spindle-shaped or dendritic melanocytes that aretypically heavily pigmented. A subtypeknown as the cellular blue naevus has alow potential for metastasis.
Atypical melanocytic naevus ofthe genital type
DefinitionOne type of atypical melanocytic prolifer-ation in the genital area that forms a dis-tinctive clinicopathological entity that canbe distinguished from melanoma anddysplastic naevus.
SynonymAtypical vulvar naevus.
Clinical featuresThe atypical melanocytic naevus of thegenital type occurs primarily in youngwomen of reproductive age. Unlike thedysplastic naevus, it is not associatedwith dysplastic naevi in other sites. Vulvar naevi can be influenced by hor-monal changes and may appear moreactive or atypical during pregnancy.
HistopathologyThe atypical melanocytic naevus of thegenital type has junctional melanocyticnests that are variably sized andinclude some atypical superf i c i a lmelanocytes, These lesions lack signifi-cant atypia or mitotic activity in thedeeper dermal melanocytes and do notinvolve skin appendages. In additionthe lesion is small, well circ u m s c r i b e dand lacks pagetoid spread or necro s i s{ 3 1 , 4 9 8 } .
Table 7.04Clark levels of cutaneous melanoma {3120}.
Level I Melanoma in situ
Level II Superficial papillary dermis
Level III Fills and expands papillary dermis
Level IV Reticular dermis
Level V Deeper than reticular dermis into fat or other deeper tissue
Fig. 7.21 Atypical melanocytic naevus of the genital type. The tumour is a compound naevus with variablysized melanocytic nests and atypia confined to the superficial melanocytes..
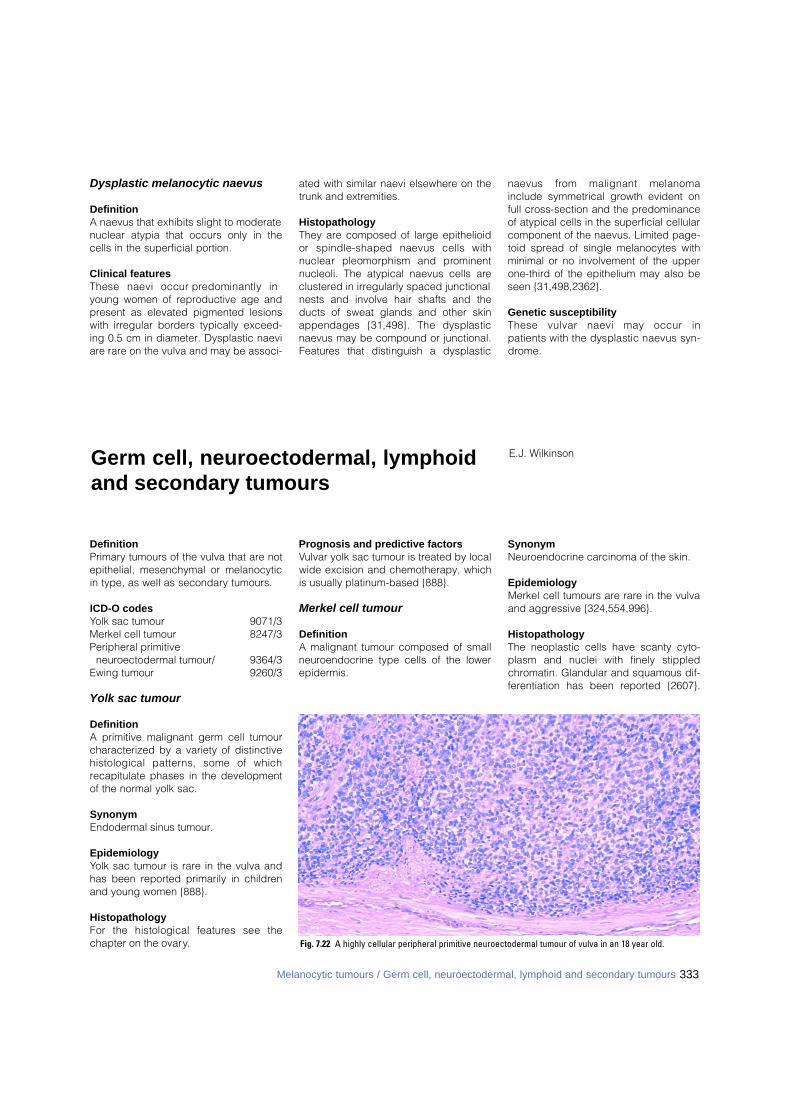
DefinitionPrimary tumours of the vulva that are notepithelial, mesenchymal or melanocyticin type, as well as secondary tumours.
ICD-O codesYolk sac tumour 9071/3Merkel cell tumour 8247/3Peripheral primitive
neuroectodermal tumour/ 9364/3Ewing tumour 9260/3
Yolk sac tumour
DefinitionA primitive malignant germ cell tumourcharacterized by a variety of distinctivehistological patterns, some of whichrecapitulate phases in the developmentof the normal yolk sac.
SynonymEndodermal sinus tumour.
EpidemiologyYolk sac tumour is rare in the vulva andhas been reported primarily in childrenand young women {888}.
HistopathologyFor the histological features see thechapter on the ovary.
Prognosis and predictive factorsVulvar yolk sac tumour is treated by localwide excision and chemotherapy, whichis usually platinum-based {888}.
Merkel cell tumour
DefinitionA malignant tumour composed of smallneuroendocrine type cells of the lowerepidermis.
SynonymNeuroendocrine carcinoma of the skin.
EpidemiologyMerkel cell tumours are rare in the vulvaand aggressive {324,554,996}.
HistopathologyThe neoplastic cells have scanty cyto-plasm and nuclei with finely stippledchromatin. Glandular and squamous dif-ferentiation has been reported {2607}.
E.J. WilkinsonGerm cell, neuroectodermal, lymphoidand secondary tumours
Dysplastic melanocytic naevus
DefinitionA naevus that exhibits slight to moderatenuclear atypia that occurs only in thecells in the superficial portion.
Clinical featuresThese naevi occur predominantly inyoung women of reproductive age andpresent as elevated pigmented lesionswith irregular borders typically exceed-ing 0.5 cm in diameter. Dysplastic naeviare rare on the vulva and may be associ-
ated with similar naevi elsewhere on thetrunk and extremities.
HistopathologyThey are composed of large epithelioidor spindle-shaped naevus cells withnuclear pleomorphism and pro m i n e n tnucleoli. The atypical naevus cells areclustered in irregularly spaced junctionalnests and involve hair shafts and theducts of sweat glands and other skinappendages {31,498}. The dysplasticnaevus may be compound or junctional.F e a t u res that distinguish a dysplastic
naevus from malignant melanomainclude symmetrical growth evident onfull cross-section and the predominanceof atypical cells in the superficial cellularcomponent of the naevus. Limited page-toid spread of single melanocytes withminimal or no involvement of the upperone-third of the epithelium may also beseen {31,498,2362}.
Genetic susceptibilityThese vulvar naevi may occur inpatients with the dysplastic naevus syn-d ro m e .
Fig. 7.22 A highly cellular peripheral primitive neuroectodermal tumour of vulva in an 18 year old.
333Melanocytic tumours / Germ cell, neuroectodermal, lymphoid and secondary tumours
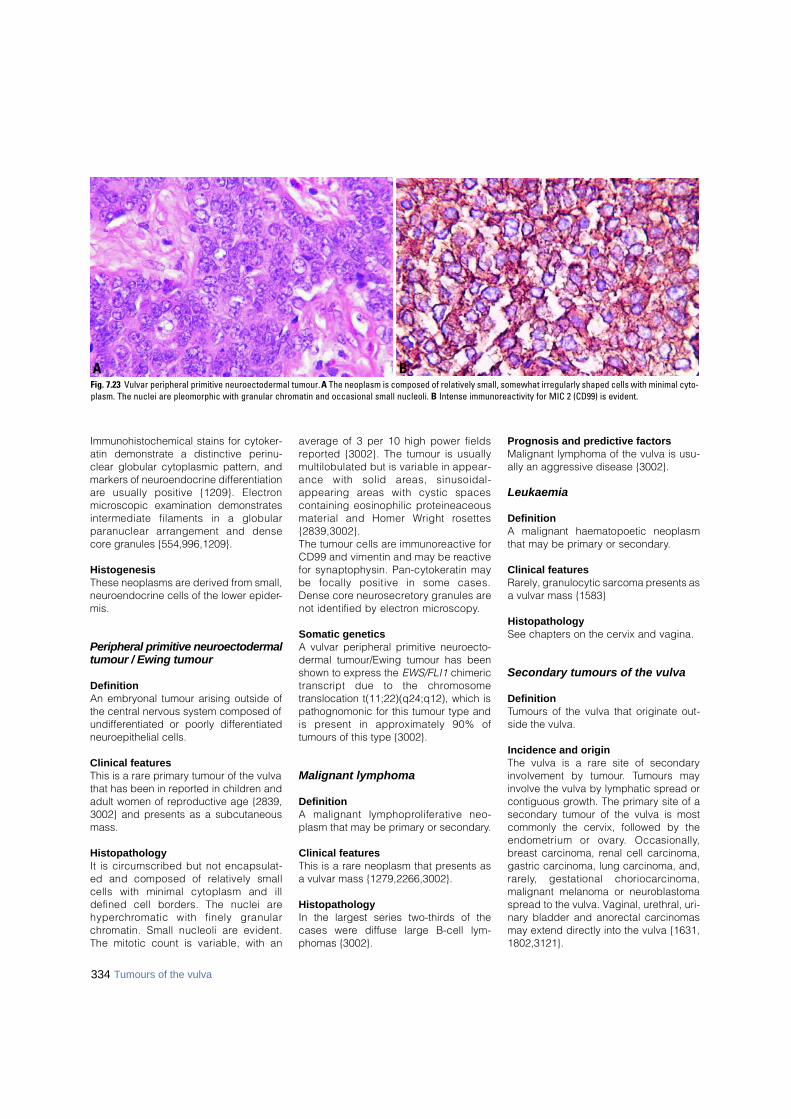
334 Tumours of the vulva
Immunohistochemical stains for cytoker-atin demonstrate a distinctive perinu-clear globular cytoplasmic pattern, andmarkers of neuroendocrine differentiationa re usually positive {1209}. Electro nmicroscopic examination demonstratesi n t e rmediate filaments in a globularparanuclear arrangement and densecore granules {554,996,1209}.
HistogenesisThese neoplasms are derived from small,neuroendocrine cells of the lower epider-mis.
Peripheral primitive neuroectodermaltumour / Ewing tumour
DefinitionAn embryonal tumour arising outside ofthe central nervous system composed ofundifferentiated or poorly differentiatedneuroepithelial cells.
Clinical featuresThis is a rare primary tumour of the vulvathat has been in reported in children andadult women of reproductive age {2839,3002} and presents as a subcutaneousmass.
HistopathologyIt is circumscribed but not encapsulat-ed and composed of relatively smallcells with minimal cytoplasm and illdefined cell borders. The nuclei areh y p e rc h romatic with finely granularc h romatin. Small nucleoli are evident.The mitotic count is variable, with an
average of 3 per 10 high power fieldsre p o rted {3002}. The tumour is usuallymultilobulated but is variable in appear-ance with solid areas, sinusoidal-appearing areas with cystic spacescontaining eosinophilic pro t e i n e a c e o u smaterial and Homer Wright ro s e t t e s{ 2 8 3 9 , 3 0 0 2 } .The tumour cells are immunoreactive forCD99 and vimentin and may be re a c t i v efor synaptophysin. Pan-cytokeratin maybe focally positive in some cases.Dense core neuro s e c re t o ry granules arenot identified by electron micro s c o p y.
Somatic geneticsA vulvar peripheral primitive neuroecto-dermal tumour/Ewing tumour has beenshown to express the EWS/FLI1 chimerictranscript due to the chro m o s o m etranslocation t(11;22)(q24;q12), which ispathognomonic for this tumour type andis present in approximately 90% oftumours of this type {3002}.
Malignant lymphoma
DefinitionA malignant lymphoproliferative neo-plasm that may be primary or secondary.
Clinical featuresThis is a rare neoplasm that presents asa vulvar mass {1279,2266,3002}.
HistopathologyIn the largest series two-thirds of thecases were diffuse large B-cell lym-phomas {3002}.
Prognosis and predictive factorsMalignant lymphoma of the vulva is usu-ally an aggressive disease {3002}.
Leukaemia
DefinitionA malignant haematopoetic neoplasmthat may be primary or secondary.
Clinical featuresRarely, granulocytic sarcoma presents asa vulvar mass {1583}
HistopathologySee chapters on the cervix and vagina.
Secondary tumours of the vulva
DefinitionTumours of the vulva that originate out-side the vulva.
Incidence and originThe vulva is a rare site of secondaryinvolvement by tumour. Tumours mayinvolve the vulva by lymphatic spread orcontiguous growth. The primary site of asecondary tumour of the vulva is mostcommonly the cervix, followed by theendometrium or ovary. Occasionally,breast carcinoma, renal cell carcinoma,gastric carcinoma, lung carcinoma, and,r a re l y, gestational choriocarc i n o m a ,malignant melanoma or neuroblastomaspread to the vulva. Vaginal, urethral, uri-nary bladder and anorectal carcinomasmay extend directly into the vulva {1631,1802,3121}.
BAFig. 7.23 Vulvar peripheral primitive neuroectodermal tumour. A The neoplasm is composed of relatively small, somewhat irregularly shaped cells with minimal cyto-plasm. The nuclei are pleomorphic with granular chromatin and occasional small nucleoli. B Intense immunoreactivity for MIC 2 (CD99) is evident.
CHAPTER 8
Inherited Tumour Syndromes
Inherited cancer susceptibility is now recognized as a signifi-cant risk for cancer of the breast and female genitals organs.For many inherited tumour syndromes, the underlying germlinemutations have been identified. This allows genetic testing andcounseling of at risk family members and to estimate the asso -ciated disease burden. The genetic basis involves mutationalinactivation of tumour supressor and DNA repair genes. Suchgermline mutations follow a mendelian inheritance pattern andusually confer substantial cancer risks, with breast and ovaryas most frequent target organs. Additional familial aggrega-tions have been observed but the responsible genes have notyet been identified and may involve multigenic traits.

336 Inherited tumour syndromes
Evidence of familial aggregation ofb reast, ovarian, and other tumours of thefemale genital organs derived from anec-dotal observation of large families andf rom systematic analyses of cancer inci-dence in relatives of cancer cases.Although there are a number of potentialm e a s u res of familial aggregation, themost commonly used is the familial re l a-tive risk (FRR) or standardized incidencerate (SlR). This is defined as the ratio ofthe incidence of disease among re l a t i v e sof an individual with disease compare dwith the incidence in the population as awhole. The FRR is most often estimatedt h rough comparison of family history databetween cases and controls, with theresulting odds ratio used as an estimatorof the familial risk. Using genealogicalre s o u rces linked to cancer registries hasa number of advantages; the number ofcases is usually large compared to case-c o n t rol studies and, more import a n t l y, allcancers found among relatives are con-f i rmed in the cancer re g i s t ry.
Breast cancerEvidence that women with a positive fam-ily history of breast cancer are ati n c reased risk for developing the diseasehas been accumulating for over 50 years;v i rtually every study has found signifi-cantly elevated relative risks to female re l-atives of breast cancer patients. Moststudies have found relative risks between2 and 3 for first-degree relatives of bre a s tcancer patients selected without re g a rdto age at diagnosis or laterality. A re c e n treview of 74 published studies {2238} cal-culated familial relative risks of 2.1 (95%CI 2.0, 2.2) for breast cancer in any firstd e g ree relative, 2.3 for a sister aff e c t e d ,and 2.0 for an affected mother, and a re l-ative risk of 3.6 if an individual had both amother and sister affected. For individu-als with a first degree relative diagnosedwith breast cancer under age 50, the re l-ative risk to develop breast cancer beforeage 50 was 3.3 (CI 2.8, 3.9). In a population-based study of familialcancer using the Utah PopulationDatabase, Goldgar et al. {1029} studied
the incidence of breast and other can-cers among 49 202 first-degree relativesof 5559 breast cancer probands diag-nosed before age 80. This study estimat-ed a relative risk of 1.8 in first degree rel-atives of these breast cancer probands.When restricted to early-onset cancer(diagnosed before age 50), the relativerisk of breast cancer among first-degreerelatives increased to 2.6 and the risk forearly-onset breast cancer among theserelatives was 3.7 (95% CI. 2.8–4.6). TheSwedish family cancer database {715}contains >9.6 million individuals, withdata on nearly 700,000 invasive cancersand consists of individuals born inSweden after 1934 and their parents.Analyzing cancers diagnosed betweenthe years 1958 to 1996, the standardizedincidence ratio for breast cancer was1.85 (95% CI 1.74–1.96) for having anaffected mother, 1.98 (1.79–2.18) for hav-ing an affected sister, and 2.4 (1.72–3.23) if both mother and sister werea ffected. Other studies found largerfamilial effects among relatives of youngbilateral probands compared with youngprobands with unilateral breast cancer{700,1246,2129}. The issue of relationship of histology tofamilial breast cancer is less clear {375,500,1724,2441,2989}. Some studiesfound that lobular carcinoma is moreoften associated with a positive familyh i s t o ry {791} while others {1566}observed that cases with tubular carci-noma were more frequently associatedwith a positive family history. Multi-centricity was also found to be positivelyassociated with family history {1564}.Occurrence of breast cancer in a maleconveys a two to three fold increased riskof breast cancer in female re l a t i v e s{94,2449}.
Ovarian cancerIn a population-based case-control studyof families of 493 ovarian cancer casesand 2465 controls, Schildkraut andThompson {2557} reported an odds ratiofor ovarian cancer in first degree rela-tives of 3.6 (95% CI 1.8–7.1). A compre-
hensive study of first-degree relatives of883 ovarian cancer probands from theUtah Population Database estimated arelative risk of 2.1 (1.0–3.4) for ovariancancer in the relatives {1029}. Analysis ofthe Swedish family cancer database{715} found a standardized incidenceratio for ovarian cancer of 2.81 (95% CI2.21–3.51) for having an affected mother,1.94 (0.99–3.41) for having an affectedsister, and 25.5 (6.6–66.0) if both motherand sister were affected. A meta-analysisof all case-control and cohort studiespublished before 1998 estimates the riskto first degree relatives at 3.1, with a95%CI of 2.6-3.7 {2801}.
Endometrial cancerGruber and Thompson {1071} in a studyof first-degree relatives of 455 cases ofp r i m a ry epithelial carcinoma of theendometrium and 3216 controls, reportan odds ratio (OR) of 2.8 (CI 1.9 – 4.2) forhaving one or more relatives affectedwith endometrial cancer. In a similar sizestudy (726 cases and 2123 controls)Parrazini et al. {2173} found a smallereffect, with an OR of 1.5 (CI 1.0–2.3). Thismay partly be explained by the fact thatin the former study, cases were restrictedto ages 20-54, while in the latter, themedian age at diagnosis was 61. ADanish case-control study of 237 casesof endometrial cancer diagnosed underage 50 and 538 population contro l sreported an OR for family history of 2.1(1.1–3.8). In contrast to most other sites,the two registry/geneaology based stud-ies of endometrial cancer produced con-flicting results, with the Utah study find-ing a FRR of 1.32 and the Swedish fami-ly cancer database reporting a SIR of2.85. The reason for this discrepancy isunclear, but may to some extent reflectdifferences in the age distribution of thetwo populations.
Cervical cancerIn the Utah Population Database {1029},a FRR to first degree relatives of 999 cer-vical cancer cases of 1.74 was obtained(95% CI 1.03-2.53) while in the Swedish
D. GoldgarM.R. StrattonFamilial aggregation of cancers of the
breast and female genital organs
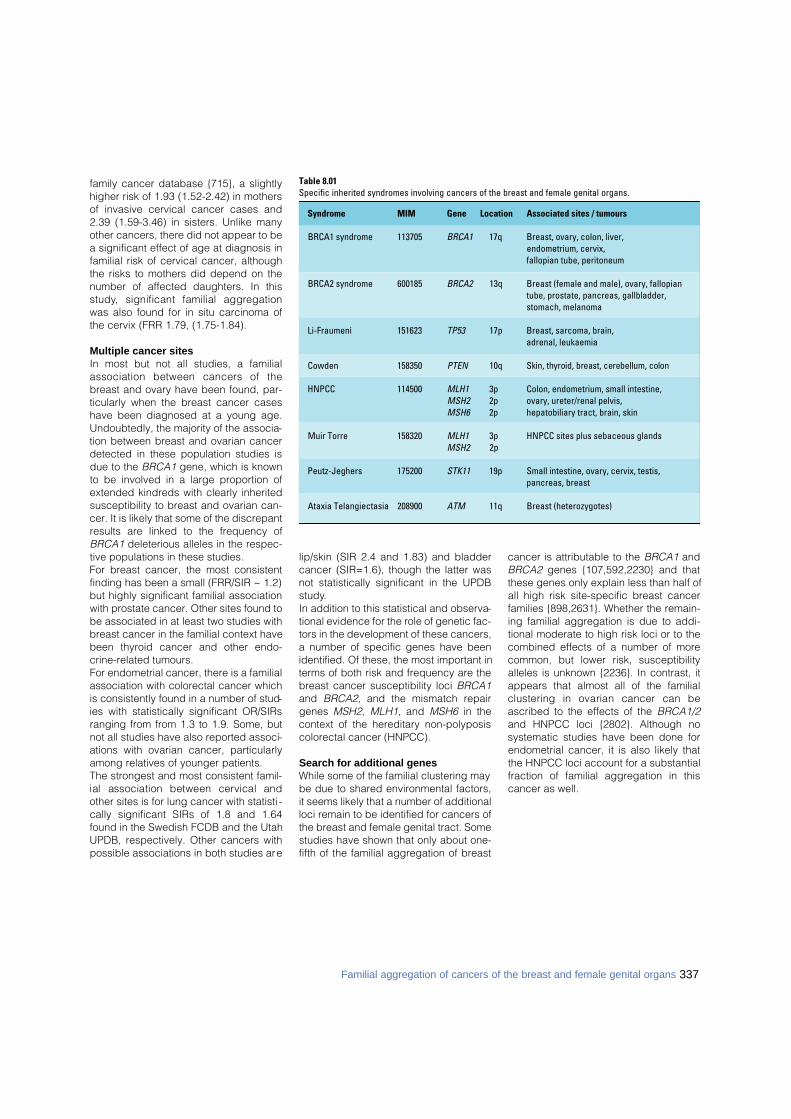
337Familial aggregation of cancers of the breast and female genital organs
family cancer database {715}, a slightlyhigher risk of 1.93 (1.52-2.42) in mothersof invasive cervical cancer cases and2.39 (1.59-3.46) in sisters. Unlike manyother cancers, there did not appear to bea significant effect of age at diagnosis infamilial risk of cervical cancer, althoughthe risks to mothers did depend on thenumber of affected daughters. In thiss t u d y, significant familial aggre g a t i o nwas also found for in situ carcinoma ofthe cervix (FRR 1.79, (1.75-1.84).
Multiple cancer sitesIn most but not all studies, a familialassociation between cancers of thebreast and ovary have been found, par-ticularly when the breast cancer caseshave been diagnosed at a young age.Undoubtedly, the majority of the associa-tion between breast and ovarian cancerdetected in these population studies isdue to the BRCA1 gene, which is knownto be involved in a large proportion ofextended kindreds with clearly inheritedsusceptibility to breast and ovarian can-cer. It is likely that some of the discrepantresults are linked to the frequency ofBRCA1 deleterious alleles in the respec-tive populations in these studies.For breast cancer, the most consistentfinding has been a small (FRR/SIR ~ 1.2)but highly significant familial associationwith prostate cancer. Other sites found tobe associated in at least two studies withbreast cancer in the familial context havebeen thyroid cancer and other endo-crine-related tumours.For endometrial cancer, there is a familialassociation with colorectal cancer whichis consistently found in a number of stud-ies with statistically significant OR/SIRsranging from from 1.3 to 1.9. Some, butnot all studies have also reported associ-ations with ovarian cancer, particularlyamong relatives of younger patients. The strongest and most consistent famil-ial association between cervical andother sites is for lung cancer with statisti -cally significant SIRs of 1.8 and 1.64found in the Swedish FCDB and the UtahUPDB, respectively. Other cancers withpossible associations in both studies are
lip/skin (SIR 2.4 and 1.83) and bladdercancer (SIR=1.6), though the latter wasnot statistically significant in the UPDBstudy.In addition to this statistical and observa-tional evidence for the role of genetic fac-tors in the development of these cancers,a number of specific genes have beenidentified. Of these, the most important interms of both risk and frequency are thebreast cancer susceptibility loci BRCA1and BRCA2, and the mismatch repairgenes MSH2, MLH1, and MSH6 in thecontext of the hereditary non-polyposiscolorectal cancer (HNPCC).
Search for additional genesWhile some of the familial clustering maybe due to shared environmental factors,it seems likely that a number of additionalloci remain to be identified for cancers ofthe breast and female genital tract. Somestudies have shown that only about one-fifth of the familial aggregation of breast
cancer is attributable to the BRCA1 andBRCA2 genes {107,592,2230} and thatthese genes only explain less than half ofall high risk site-specific breast cancerfamilies {898,2631}. Whether the remain-ing familial aggregation is due to addi-tional moderate to high risk loci or to thecombined effects of a number of morecommon, but lower risk, susceptibilityalleles is unknown {2236}. In contrast, itappears that almost all of the familialclustering in ovarian cancer can beascribed to the effects of the BRCA1/2and HNPCC loci {2802}. Although nosystematic studies have been done forendometrial cancer, it is also likely thatthe HNPCC loci account for a substantialfraction of familial aggregation in thiscancer as well.
Table 8.01Specific inherited syndromes involving cancers of the breast and female genital organs.
Syndrome MIM Gene Location Associated sites / tumours
BRCA1 syndrome 113705 BRCA1 17q Breast, ovary, colon, liver,endometrium, cervix,fallopian tube, peritoneum
BRCA2 syndrome 600185 BRCA2 13q Breast (female and male), ovary, fallopian tube, prostate, pancreas, gallbladder, stomach, melanoma
Li-Fraumeni 151623 TP53 17p Breast, sarcoma, brain,adrenal, leukaemia
Cowden 158350 PTEN 10q Skin, thyroid, breast, cerebellum, colon
HNPCC 114500 MLH1 3p Colon, endometrium, small intestine,MSH2 2p ovary, ureter/renal pelvis,MSH6 2p hepatobiliary tract, brain, skin
Muir Torre 158320 MLH1 3p HNPCC sites plus sebaceous glandsMSH2 2p
Peutz-Jeghers 175200 STK11 19p Small intestine, ovary, cervix, testis,pancreas, breast
Ataxia Telangiectasia 208900 ATM 11q Breast (heterozygotes)
338 Inherited tumour syndromes
DefinitionInherited tumour syndrome with autoso-mal dominant trait and markedlyi n c reased susceptibility to breast andovarian tumours, due to germline muta-tions in the B R C A 1 gene. Additional organsites include colon, liver, endometrium,cervix, fallopian tube, and peritoneum.
MIM No. 113705 {1835}
SynonymsBreast cancer 1, early onset breast ova-rian cancer syndrome.
IncidenceThe prevalence of BRCA1 mutations inmost Caucasian populations is estimatedto be 1 in 883 {897}. However, in certainpopulations, this is higher, e.g. 1% inAshkenazi Jews {3065}. Using recombi-nation techniques, B R C A 1 m u t a t i o n shave been dated to the early Romantimes {1997}. De novo mutations are rare.
Diagnostic criteriaA definitive diagnosis is only possible bygenetic testing. BRCA1 mutations arecommon in certain populations and infamilies with numerous early onset breastcancer cases (≥4 cases of breast cancerat <60 years) or in those with ovariancancer at any age in addition to earlyonset breast cancer. The chance of amutation in either BRCA1 or BRCA2 islower (<30%) when only two or threebreast cancer cases are present in af a m i l y. The main diff e rence betweenBRCA1 and BRCA2 is the increased riskof male breast cancer in BRCA2. TheAmerican Society of Clinical Oncology(ASCO) guidelines suggest offering test-ing at a probability of mutation of >10%but many other countries will only offertesting to those with a chance >30%because of the need to concentrateresources.
Breast tumoursPenetranceAnalyses of worldwide data submitted tothe Breast Cancer Linkage Consortium
(BCLC) have provided general estimatesof penetrance {8}. Estimates for specificpopulations have shown that theAshkenazim have a lower than averagelifetime breast cancer penetrance ofabout 50-60% {3065}. Population basedstudies in UK breast cancer patients alsorevealed a lower penetrance and indi-cate that the presence of a mutation with-in a familial breast cancer cluster doesconfer a higher penetrance {2230}. Thismay be due to an association with othergenes or epidemiological factors that arepresent in the family. There are alsoreports of variable penetrance depend-ent on the position of the mutation withinthe BRCA1 gene {2914}.
Clinical features Breast cancer in BRCA1 mutation carri-ers occurs more often at a younger age,typically before age 40 {1687}. It tends top ro g ress directly to invasive diseasewithout a precancerous DCIS component{8,1574}. Accordingly, there appears tobe a lower chance of early detection bymammographic screening and a higherproportion of invasive cancers {1025}.There is an almost linear increase in thelifetime risk of contralateral breast cancerfrom the age of 35 years, reaching a levelof 64% by the age of 80 {742}.
PathologyCertain morphological types of breastcancer, including medullary carcinoma,tubular carcinoma, lobular carcinoma insitu, and invasive lobular carc i n o m a ,
have been reported more commonly inpatients with a positive family history ofb reast cancer {191,1566,1684,1724,2441}. Patients with BRCA1 germline mutationshave an excess of medullary or atypicalmedullary carcinoma compared to con-trols {8,764,1767}. Tumours in BRCA1mutation carriers are generally of a high-er grade than their sporadic counterparts{8,764,1767}. Ductal carcinoma in situ(DCIS) adjacent to invasive cancer isobserved less frequently while the fre-quency of lobular neoplasia in situ is sim-ilar in both groups {8}. However, in a mul-tifactorial analysis of the BCLC database,the only features significantly associatedwith BRCA1 were total mitotic count, con-tinuous pushing margins, and lympho-cytic infiltrate. All other features, includ-ing the diagnosis of medullary and atyp-ical medullary carcinoma, were not foundto be significant {1572}.B R C A 1-associated tumours are morelikely to be estrogen (ER) and proges-t e rone receptor (PgR) negative {766,1352,1574,2121}. Data on ERBB2 arelimited but BRCA1-linked tumours aremore likely to be negative than controls{1352,1574}. B R C A 1-linked tumoursshow a higher frequency of TP53 muta-tions and p53 expression than sporadicb reast cancer {580,581,765,1574}.BRCA1-associated tumours show verylow expression of Cyclin D1 in both theinvasive and in situ components {2122}.The absence of Cyclin D1 in thesetumours could be an additional evidence
BRCA1 syndrome
Table 8.02Probability of BRCA1/2 mutation in women with breast/ovarian cancer.
Chance of mutation Clinical criteria
<10% Single breast cancer / ovarian cancer case at <40 years in non Ashkenazim10-30% 2-3 female breast cancers <60 years (no ovarian / male breast cancer)
30% One female breast cancer <60 and one ovarian cancerFemale breast cancer <40 in Ashkenazi
>60% Four cases of female breast cancer at <60 years≥2 cases female breast cancer <60 and ovarian cancer any age ≥2 cases female breast cancer <60 and male breast cancer any age
__________________From R.A. Eeles {749}.
D. Goldgar R.H.M. VerheijenR. Eeles C. SzaboD. Easton A.N. MonteiroS.R. Lakhani P. DevileeS.Piver S. NarodJ.M. Piek E.H. Meijers-HeijboerP.J. van Diest N. Sodha
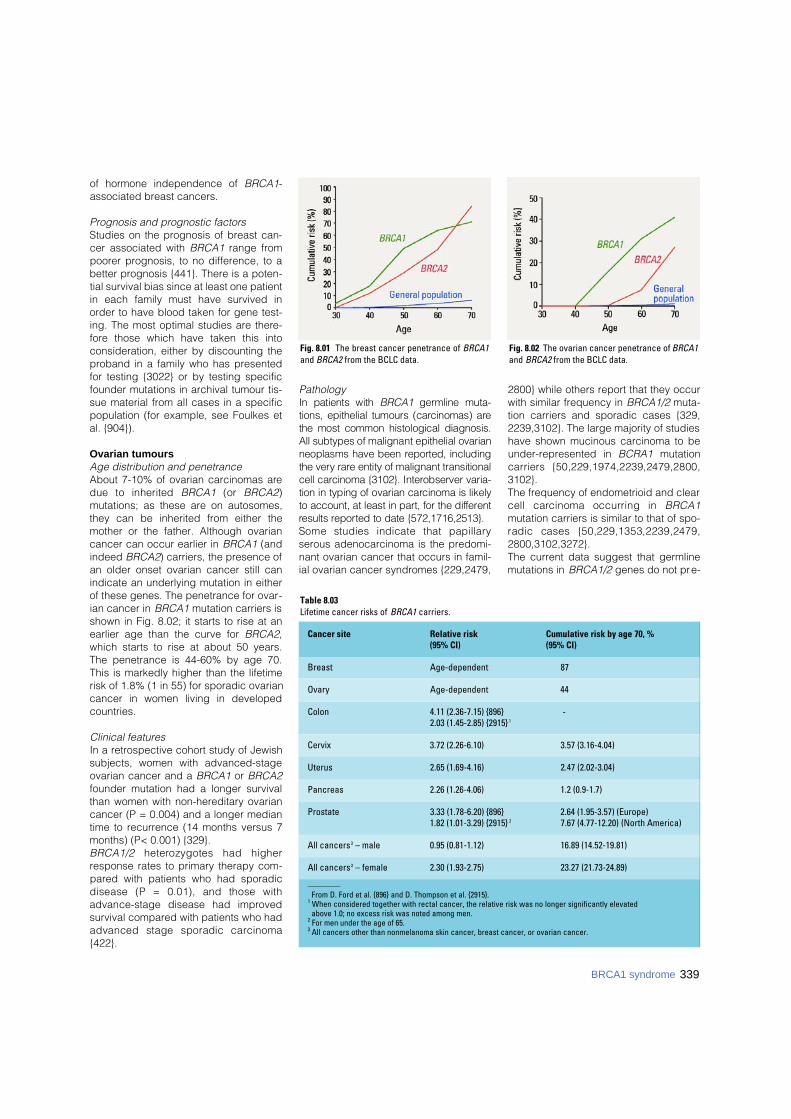
of hormone independence of BRCA1-associated breast cancers.
Prognosis and prognostic factorsStudies on the prognosis of breast can-cer associated with BRCA1 range frompoorer prognosis, to no difference, to abetter prognosis {441}. There is a poten-tial survival bias since at least one patientin each family must have survived inorder to have blood taken for gene test-ing. The most optimal studies are there-fore those which have taken this intoconsideration, either by discounting theproband in a family who has presentedfor testing {3022} or by testing specificfounder mutations in archival tumour tis-sue material from all cases in a specificpopulation (for example, see Foulkes etal. {904}).
Ovarian tumoursAge distribution and penetranceAbout 7-10% of ovarian carcinomas aredue to inherited B R C A 1 (or B R C A 2)mutations; as these are on autosomes,they can be inherited from either themother or the father. Although ovariancancer can occur earlier in BRCA1 (andindeed BRCA2) carriers, the presence ofan older onset ovarian cancer still canindicate an underlying mutation in eitherof these genes. The penetrance for ovar-ian cancer in BRCA1 mutation carriers isshown in Fig. 8.02; it starts to rise at anearlier age than the curve for BRCA2,which starts to rise at about 50 years.The penetrance is 44-60% by age 70.This is markedly higher than the lifetimerisk of 1.8% (1 in 55) for sporadic ovariancancer in women living in developedcountries.
Clinical featuresIn a retrospective cohort study of Jewishsubjects, women with advanced-stageovarian cancer and a BRCA1 or BRCA2founder mutation had a longer survivalthan women with non-hereditary ovariancancer (P = 0.004) and a longer mediantime to recurrence (14 months versus 7months) (P< 0.001) {329}.B R C A 1 / 2 h e t e rozygotes had higherresponse rates to primary therapy com-pared with patients who had sporadicdisease (P = 0.01), and those withadvance-stage disease had impro v e dsurvival compared with patients who hadadvanced stage sporadic carc i n o m a{422}.
PathologyIn patients with B R C A 1 g e rmline muta-tions, epithelial tumours (carcinomas) arethe most common histological diagnosis.All subtypes of malignant epithelial ovarianneoplasms have been re p o rted, includingthe very rare entity of malignant transitionalcell carcinoma {3102}. Interobserver varia-tion in typing of ovarian carcinoma is likelyto account, at least in part, for the diff e re n tresults re p o rted to date {572,1716,2513}.Some studies indicate that papillaryserous adenocarcinoma is the predomi-nant ovarian cancer that occurs in famil-ial ovarian cancer syndromes {229,2479,
2800} while others report that they occurwith similar frequency in BRCA1/2 muta-tion carriers and sporadic cases {329,2239,3102}. The large majority of studieshave shown mucinous carcinoma to beunder-represented in BCRA1 mutationcarriers {50,229,1974,2239,2479,2800,3102}.The frequency of endometrioid and clearcell carcinoma occurring in B R C A 1mutation carriers is similar to that of spo-radic cases {50,229,1353,2239,2479,2800,3102,3272}.The current data suggest that germlinemutations in BRCA1/2 genes do not pre-
Fig. 8.02 The ovarian cancer penetrance of BRCA1and BRCA2 from the BCLC data.
Fig. 8.01 The breast cancer penetrance of BRCA1and BRCA2 from the BCLC data.
Table 8.03Lifetime cancer risks of BRCA1 carriers.
Cancer site Relative risk Cumulative risk by age 70, %(95% CI) (95% CI)
Breast Age-dependent 87
Ovary Age-dependent 44
Colon 4.11 (2.36-7.15) {896} -2.03 (1.45-2.85) {2915} 1
Cervix 3.72 (2.26-6.10) 3.57 (3.16-4.04)
Uterus 2.65 (1.69-4.16) 2.47 (2.02-3.04)
Pancreas 2.26 (1.26-4.06) 1.2 (0.9-1.7)
Prostate 3.33 (1.78-6.20) {896} 2.64 (1.95-3.57) (Europe)1.82 (1.01-3.29) {2915} 2 7.67 (4.77-12.20) (North America)
All cancers3 – male 0.95 (0.81-1.12) 16.89 (14.52-19.81)
All cancers3 – female 2.30 (1.93-2.75) 23.27 (21.73-24.89)
________From D. Ford et al. {896} and D. Thompson et al. {2915}.
1 When considered together with rectal cancer, the relative risk was no longer significantly elevatedabove 1.0; no excess risk was noted among men.
2 For men under the age of 65.3 All cancers other than nonmelanoma skin cancer, breast cancer, or ovarian cancer.
339BRCA1 syndrome
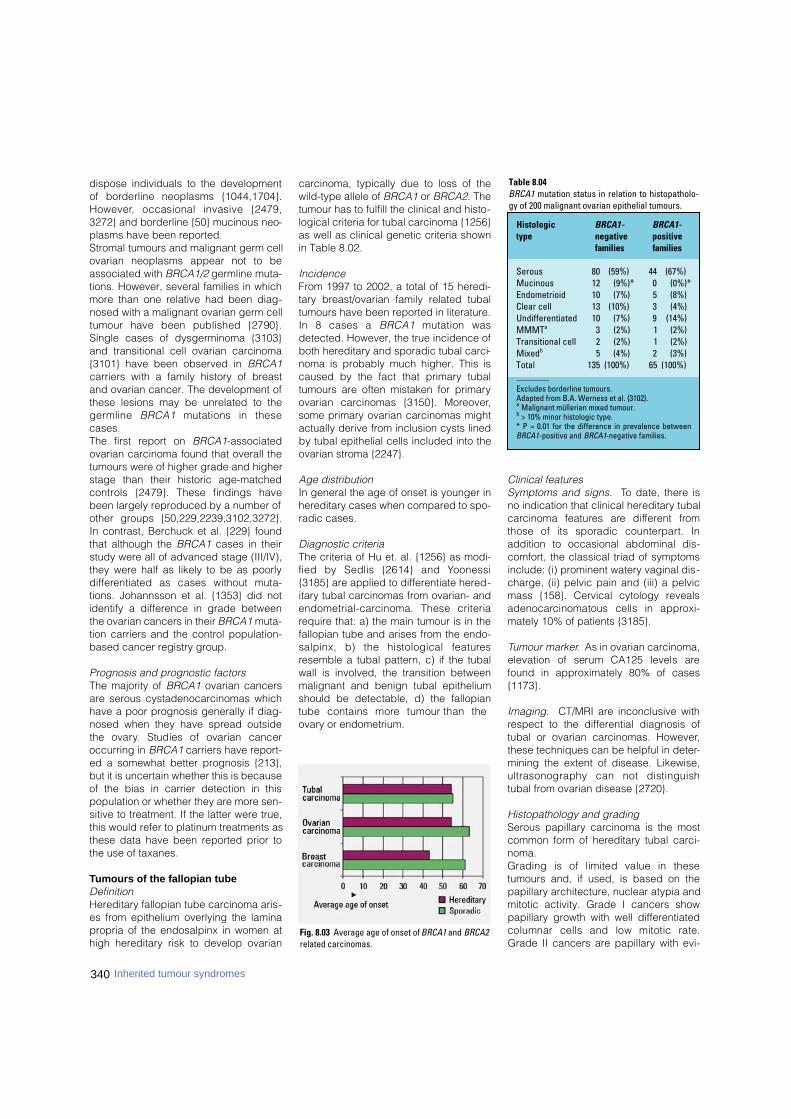
340 Inherited tumour syndromes
dispose individuals to the developmentof borderline neoplasms {1044,1704}.H o w e v e r, occasional invasive {2479,3272} and borderline {50} mucinous neo-plasms have been reported. Stromal tumours and malignant germ cellovarian neoplasms appear not to beassociated with BRCA1/2 germline muta-tions. However, several families in whichmore than one relative had been diag-nosed with a malignant ovarian germ celltumour have been published {2790}.Single cases of dysgerminoma {3103}and transitional cell ovarian carcinoma{3101} have been observed in BRCA1carriers with a family history of breastand ovarian cancer. The development ofthese lesions may be unrelated to theg e rmline B R C A 1 mutations in thesecases. The first report on BRCA1-associatedovarian carcinoma found that overall thetumours were of higher grade and higherstage than their historic age-matchedc o n t rols {2479}. These findings havebeen largely reproduced by a number ofother groups {50,229,2239,3102,3272}.In contrast, Berchuck et al. {229} foundthat although the BRCA1 cases in theirstudy were all of advanced stage (III/IV),they were half as likely to be as poorlyd i ff e rentiated as cases without muta-tions. Johannsson et al. {1353} did notidentify a difference in grade betweenthe ovarian cancers in their BRCA1 muta-tion carriers and the control population-based cancer registry group.
Prognosis and prognostic factorsThe majority of BRCA1 ovarian cancersare serous cystadenocarcinomas whichhave a poor prognosis generally if diag-nosed when they have spread outsidethe ovary. Studies of ovarian canceroccurring in BRCA1 carriers have report-ed a somewhat better prognosis {213},but it is uncertain whether this is becauseof the bias in carrier detection in thispopulation or whether they are more sen-sitive to treatment. If the latter were true,this would refer to platinum treatments asthese data have been reported prior tothe use of taxanes.
Tumours of the fallopian tubeDefinitionHereditary fallopian tube carcinoma aris-es from epithelium overlying the laminapropria of the endosalpinx in women athigh hereditary risk to develop ovarian
carcinoma, typically due to loss of thewild-type allele of BRCA1 or BRCA2. Thetumour has to fulfill the clinical and histo-logical criteria for tubal carcinoma {1256}as well as clinical genetic criteria shownin Table 8.02.
IncidenceFrom 1997 to 2002, a total of 15 heredi-tary breast/ovarian family related tubaltumours have been reported in literature.In 8 cases a B R C A 1 mutation wasdetected. However, the true incidence ofboth hereditary and sporadic tubal carci-noma is probably much higher. This iscaused by the fact that primary tubaltumours are often mistaken for primaryovarian carcinomas {3150}. More o v e r,some primary ovarian carcinomas mightactually derive from inclusion cysts linedby tubal epithelial cells included into theovarian stroma {2247}.
Age distributionIn general the age of onset is younger inhereditary cases when compared to spo-radic cases.
Diagnostic criteriaThe criteria of Hu et. al. {1256} as modi-fied by Sedlis {2614} and Yo o n e s s i{3185} are applied to differentiate hered-itary tubal carcinomas from ovarian- ande n d o m e t r i a l - c a rcinoma. These criteriarequire that: a) the main tumour is in thefallopian tube and arises from the endo-salpinx, b) the histological feature sresemble a tubal pattern, c) if the tubalwall is involved, the transition betweenmalignant and benign tubal epitheliumshould be detectable, d) the fallopiantube contains more tumour than theovary or endometrium.
Clinical featuresSymptoms and signs. To date, there isno indication that clinical hereditary tubalc a rcinoma features are diff e rent fro mthose of its sporadic counterpart. Inaddition to occasional abdominal dis-comfort, the classical triad of symptomsinclude: (i) prominent watery vaginal dis-charge, (ii) pelvic pain and (iii) a pelvicmass {158}. Cervical cytology revealsa d e n o c a rcinomatous cells in appro x i-mately 10% of patients {3185}.
Tumour marker. As in ovarian carcinoma,elevation of serum CA125 levels arefound in approximately 80% of cases{1173}.
Imaging. CT/MRI are inconclusive withrespect to the differential diagnosis oftubal or ovarian carcinomas. However,these techniques can be helpful in deter-mining the extent of disease. Likewise,ultrasonography can not distinguishtubal from ovarian disease {2720}.
Histopathology and gradingSerous papillary carcinoma is the mostcommon form of hereditary tubal carci-noma. Grading is of limited value in thesetumours and, if used, is based on thepapillary architecture, nuclear atypia andmitotic activity. Grade I cancers showpapillary growth with well differentiatedcolumnar cells and low mitotic rate.Grade II cancers are papillary with evi-
Table 8.04BRCA1 mutation status in relation to histopatholo-gy of 200 malignant ovarian epithelial tumours.
Histologic BRCA1- BRCA1-type negative positive
f a m i l i e s f a m i l i e s
Serous 80 (59%) 44 (67%)Mucinous 12 (9%)* 0 (0%)*Endometrioid 10 (7%) 5 (8%)Clear cell 13 (10%) 3 (4%)Undifferentiated 10 (7%) 9 (14%)MMMTa 3 (2%) 1 (2%) Transitional cell 2 (2%) 1 (2%)Mixedb 5 (4%) 2 (3%)Total 135 (100%) 65 (100%) ________Excludes borderline tumours. Adapted from B.A. Werness et al. {3102}.a Malignant müllerian mixed tumour.b > 10% minor histologic type. * P = 0.01 for the difference in prevalence betweenBRCA1-positive and BRCA1-negative families.
Fig. 8.03 Average age of onset of BRCA1 and BRCA2related carcinomas.

341BRCA1 syndrome
dent gland formation with intermediatelydifferentiated cells with moderate mitoticactivity. Grade III shows solid growth withloss of papillae and a medullary/glandu-lar pattern. The cells are poorly differen-tiated and the mitotic activity is high.
Immunohistochemistry. Being predomi-nantly of serous papillary type, hereditarytubal carcinomas are positive for cytok-eratins 7 and 8, MUC1, CEA, OVTL3,OV632, CA125, and negative or showingonly low expression for cytokeratin 20,CEA and vimentin. Also, p53 is oftenexpressed, and cyclins E and A and Ki67show a varying number of proliferatingcells, whereas staining for ERBB2 andcyclin D1 is usually negative. Steroidreceptor content varies. In the rare clearcell cancers, p21 is highly expressed.
Seeding and metastasisHereditary tubal carcinomas presumablyspread like their sporadic counterparts.Empirical data are available to date pointto a mode of spread similar to ovariancancer.
PrognosisThe five-year survival rate of 30% in spo-radic cases varies with stage {158,3185},but not with grade. The survival rate ofhereditary tubal carcinomas has yet tobe established since only small numbersof patients have been reported and mostpatients have still not completed their 5-year follow-up.
Other tumoursB R C A 1 p redominantly predisposes tofemale breast cancer and ovarian can-cer. Unlike BRCA2, it is not thought topredispose to male breast cancer. A fewfamilies with male breast cancer and aBRCA1 mutation have been described,but these may be within the numbersexpected by chance. A study of causesof mortality by Ford et al. {896} reportedan increased risk of colon cancer andprostate cancer. However, a reanalysis{2914} has shown a small pancreaticcancer excess, as is seen in BRCA2 car-riers and an excess of prostate cancerrisk only at age <60 years. The excess ofcolonic cancer was counteracted by adeficit of rectal cancer. See Table 8.03 fordetails on risk estimates.
GeneticsChromosomal location and gene structureThe BRCA1 gene is located on chromo-some 17q21 {1109}. The 24 exons of theBRCA1 gene (22 coding exons; alterna-tive 5’UTR exons, 1a & 1b) span an 81-kb chromosomal region, that has anunusually high density of Alu repetitiveDNA (41.5%) {1864,2735}. A part i a lpseudogene (BRCA1Ψ) consisting of atandem duplication of exons 1a, 1b and2 lies 44.5kb upstream of B R C A 1{356,2303}. Exon 11 of BRCA1 (3.4 kb)encodes 61% of the 1863 amino acidprotein. The amino-terminal RING fingerdomain and the carboxy-terminal BRCTrepeats {316} of BRCA1 are highly con-served among vertebrates {2825}, whilethe rest of the protein bears little homolo-gy to other known genes.
Gene expressionSeveral alternatively spliced transcriptshave been described for the BRCA1gene, the most prevalent of these lead toin-frame deletions of exon 11 (BRCA1-∆11). Both full length and ∆11 transcriptsa re ubiquitously expressed. The 100-and 97-kDa ∆11 protein isoforms lack thenuclear localization signal and are cyto-plasmic {1864,2904}. However, the full-length 220-kDa protein is predominantly
observed in the nucleus. Its expressionand phosphorylation is cell-cycledependent, commencing in G1 andreaching maximal levels by early S-phase. BRCA1 colocalizes with theBRCA2 and Rad51 proteins in discretefoci during S-phase. DNA damage leadsto hyperphosphorylation of BRCA1, dis-persal of the BRCA1/BRCA2/Rad51nuclear foci, and their relocalization toPCNA-containing DNA replication struc-tures. In meiotic cells, BRCA1, BRCA2and Rad51 colocalize on the axial ele-ments of developing synaptonemal com-plexes {450,2594,2596}. A large proteincomplex consisting of other tumour sup-pressor and DNA repair proteins, knownas BASC (BRCA1-associated genomesurveillance complex) has been identi-fied. Among these, partial colocalizationof BRCA1 with Rad50, MRE11 and BLMin nuclear foci analogous to thoseobserved with BRCA2 and Rad51 hasbeen demonstrated {3054}. In addition toits interactions with BRCA2, Rad51, andBASC, the BRCA1 protein has beenshown to form complexes with a numberof other proteins involved in diverse cel-lular functions, including DNA re p a i r,transcription, chromatin remodeling, andprotein ubiquination (reviewed in {3018}). During mouse embryonic development,B rc a 1 exhibits a dynamic expre s s i o n
BA
DCFig. 8.04 A Normal endosalpinx, stained for bcl-2, which is a differentiation marker of serous tubal cells. B Tubal cell-lined inclusion cyst in the ovary stained for bcl-2. C Dysplastic lesion in a fallopian tube of aBRCA1 mutation carrier, stained for p53. D Serous adenocarcinoma of the fallopian tube stained for bcl-2(note: not all serous carcinomas are bcl-positive).
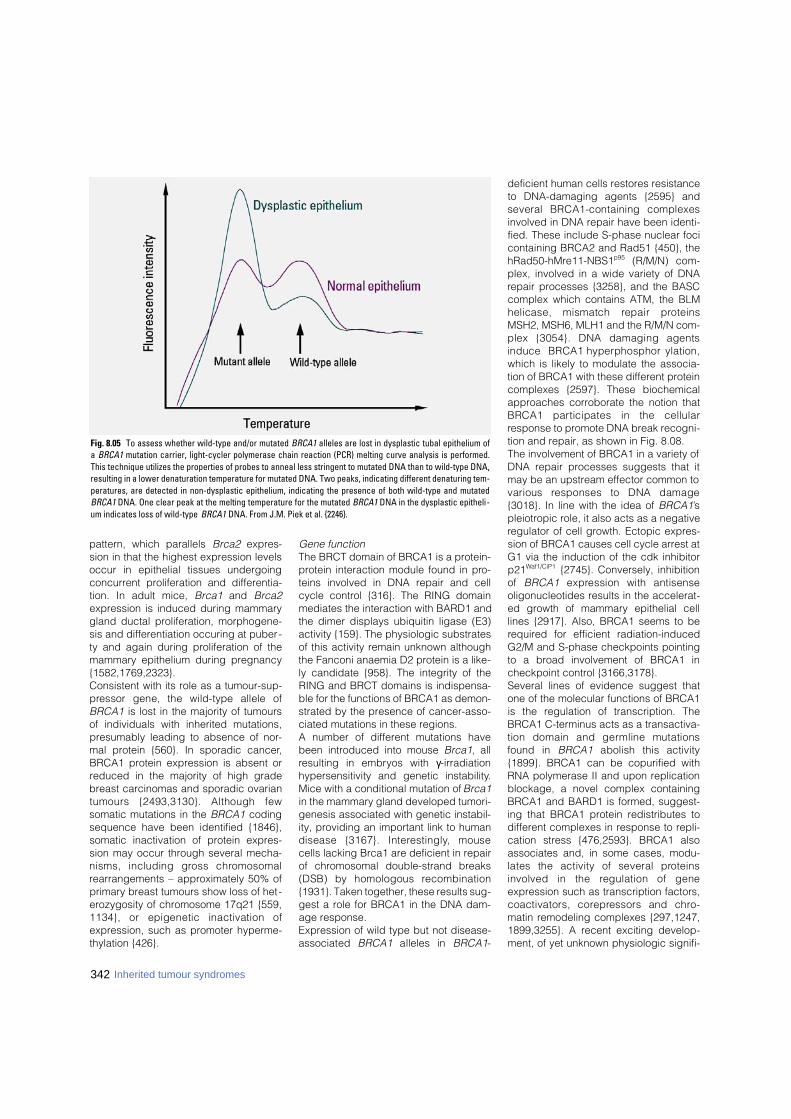
342 Inherited tumour syndromes
pattern, which parallels Brca2 expres-sion in that the highest expression levelsoccur in epithelial tissues undergoingconcurrent proliferation and differentia-tion. In adult mice, Brca1 and Brca2expression is induced during mammarygland ductal proliferation, morphogene-sis and differentiation occuring at puber-ty and again during proliferation of themammary epithelium during pregnancy{1582,1769,2323}.Consistent with its role as a tumour-sup-p ressor gene, the wild-type allele ofBRCA1 is lost in the majority of tumoursof individuals with inherited mutations,presumably leading to absence of nor-mal protein {560}. In sporadic cancer,BRCA1 protein expression is absent orreduced in the majority of high gradebreast carcinomas and sporadic ovariantumours {2493,3130}. Although fewsomatic mutations in the BRCA1 codingsequence have been identified {1846},somatic inactivation of protein expres-sion may occur through several mecha-nisms, including gross chro m o s o m a lrearrangements – approximately 50% ofprimary breast tumours show loss of het-erozygosity of chromosome 17q21 {559,1134}, or epigenetic inactivation ofexpression, such as promoter hyperme-thylation {426}.
Gene functionThe BRCT domain of BRCA1 is a protein-protein interaction module found in pro-teins involved in DNA repair and cellcycle control {316}. The RING domainmediates the interaction with BARD1 andthe dimer displays ubiquitin ligase (E3)activity {159}. The physiologic substratesof this activity remain unknown althoughthe Fanconi anaemia D2 protein is a like-ly candidate {958}. The integrity of theRING and BRCT domains is indispensa-ble for the functions of BRCA1 as demon-strated by the presence of cancer-asso-ciated mutations in these regions.A number of different mutations havebeen introduced into mouse Brca1, allresulting in embryos with γ- i r r a d i a t i o nhypersensitivity and genetic instability.Mice with a conditional mutation of Brca1in the mammary gland developed tumori-genesis associated with genetic instabil-ity, providing an important link to humandisease {3167}. Intere s t i n g l y, mousecells lacking Brca1 are deficient in repairof chromosomal double-strand breaks(DSB) by homologous re c o m b i n a t i o n{1931}. Taken together, these results sug-gest a role for BRCA1 in the DNA dam-age response.Expression of wild type but not disease-associated B R C A 1 alleles in B R C A 1-
deficient human cells restores resistanceto DNA-damaging agents {2595} andseveral BRCA1-containing complexesinvolved in DNA repair have been identi-fied. These include S-phase nuclear focicontaining BRCA2 and Rad51 {450}, theh R a d 5 0 - h M re 1 1 - N B S 1p 9 5 (R/M/N) com-plex, involved in a wide variety of DNArepair processes {3258}, and the BASCcomplex which contains ATM, the BLMhelicase, mismatch repair pro t e i n sMSH2, MSH6, MLH1 and the R/M/N com-plex {3054}. DNA damaging agentsinduce BRCA1 hyperphosphory l a t i o n ,which is likely to modulate the associa-tion of BRCA1 with these different proteincomplexes {2597}. These biochemicalapproaches corroborate the notion thatBRCA1 participates in the cellularresponse to promote DNA break recogni-tion and repair, as shown in Fig. 8.08. The involvement of BRCA1 in a variety ofDNA repair processes suggests that itmay be an upstream effector common tovarious responses to DNA damage{3018}. In line with the idea of BRCA1’spleiotropic role, it also acts as a negativeregulator of cell growth. Ectopic expres-sion of BRCA1 causes cell cycle arrest atG1 via the induction of the cdk inhibitorp21Waf1/CiP1 {2745}. Conversely, inhibitionof B R C A 1 e x p ression with antisenseoligonucleotides results in the accelerat-ed growth of mammary epithelial celllines {2917}. Also, BRCA1 seems to berequired for efficient radiation-inducedG2/M and S-phase checkpoints pointingto a broad involvement of BRCA1 incheckpoint control {3166,3178}.Several lines of evidence suggest thatone of the molecular functions of BRCA1is the regulation of transcription. TheBRCA1 C-terminus acts as a transactiva-tion domain and germline mutationsfound in B R C A 1 abolish this activity{1899}. BRCA1 can be copurified withRNA polymerase II and upon replicationblockage, a novel complex containingBRCA1 and BARD1 is formed, suggest-ing that BRCA1 protein redistributes todifferent complexes in response to repli-cation stress {476,2593}. BRCA1 alsoassociates and, in some cases, modu-lates the activity of several pro t e i n sinvolved in the regulation of geneexpression such as transcription factors,coactivators, core p ressors and chro-matin remodeling complexes {297,1247,1899,3255}. A recent exciting develop-ment, of yet unknown physiologic signifi-
Fig. 8.05 To assess whether wild-type and/or mutated BRCA1 alleles are lost in dysplastic tubal epithelium ofa BRCA1 mutation carrier, light-cycler polymerase chain reaction (PCR) melting curve analysis is performed.This technique utilizes the properties of probes to anneal less stringent to mutated DNA than to wild-type DNA,resulting in a lower denaturation temperature for mutated DNA. Two peaks, indicating different denaturing tem-peratures, are detected in non-dysplastic epithelium, indicating the presence of both wild-type and mutatedBRCA1 DNA. One clear peak at the melting temperature for the mutated BRCA1 DNA in the dysplastic epitheli-um indicates loss of wild-type BRCA1 DNA. From J.M. Piek et al. {2246}.

cance, was the discovery of direct DNAbinding by BRCA1 in vitro which may beimportant for its function in transcriptionand DNA repair {2198}.Putative BRCA1 transcriptional targetgenes identified so far play a role insome aspect of the DNA damageresponse. BRCA1 induces the transacti-vation of p21WAF1/CiP1 in p53-dependentand independent manners, insuring apotent cell cycle arrest, reinforcing theconnection between cell cycle check-point control and transcription regulation{2130,2745}. Experiments using cDNAarrays identified the DNA-damage-responsive gene GADD45 as a major tar-get of BRCA1-mediated transcription{1138,1727}. These results, coupled withstudies showing that disruption of p53partially rescues embryonic lethality inBrca1-/- mouse, link the p53 pathway andBRCA1 function {1108,1710}. Import -antly, the majority of tumours derivedf rom B R C A 1-linked patients or fro mBrca1-/- mice present mutations in p53{581,3167}.
Mutation spectrumGermline mutations in BRCA1 have beendetected in 15-20% of clinic-basedbreast cancer families, and in 40-50% ofb reast-ovarian cancer families {2657,3023}. Mutations occur throughout thee n t i re coding region, and hence themutation spectrum has taught us rela-tively little about the gene’s function. Themajority of the mutations are predicted tolead to a prematurely truncated proteinwhen translated. In conjunction with theobserved loss of the wildtype allele intumours arising in mutation carriers{560}, this indicates that inactivation ofthe gene is an important step in tumori-genesis. Despite the strong variability inmutations detected in families, foundereffects have led to some mutations beingvery prevalent in certain populations ofdefined geographical or ethnic back-ground. An example is the 185delAGmutation, which is present in approxi-mately 1% of all individuals of AshkenaziJewish descent {1151}. As a result, muta-tion spectra may vary according to eth-nic background of the sampled popula-tion {2824}. In some populations, specif-ic large interstitial deletions or insertions,which are difficult to detect by conven-tional PCR-based mutation scanningtechnologies, have been observed to beparticularly frequent. They may comprise
between 10 and 20% of the total muta-tion spectrum {944,1229}.In recent years, an increasing numberof missense changes are being detect-ed in B R C A 1, of which the clinical sig-nificance is uncertain. These alre a d ycomprise up to 40% of all knownsequence changes in B R C A 1. TheB reast Cancer Information Core (BIC)maintains a website providing a centralre p o s i t o ry for information re g a rd i n gmutations and polymorphisms{ h t t p : / / re s e a rc h . n h g r i . n i h . g o v / b i c / } .
Genotype-phenotype correlationsInitially, the breast and ovarian cancercancer risks conferred by mutations inB R C A 1 w e re estimated from B R C A 1-linked, multiple-case families (see Figs.8.01 and 8.02) {896,898}. More recently,estimates from specific populations havecome up with lower estimates{106,3065}. This could point to 1) theexistence of mutation-specific risks(because different populations have dif-ferent mutation spectra, the overall can-cer risks would differ), 2) the existence ofgenetic variants in other genes, particu-larly prevalent in certain populations,which might modify the BRCA1-relatedcancer risks, 3) population-specific dif-ferences in environmental risk modifiers.
BRCA1 mutation positionOne report observed a significant corre-lation between the location of the muta-tion in the gene and the ratio of breast toovarian cancer incidence within eachfamily {974}, suggesting a transition inrisk such that mutations in the 3' third ofthe gene were associated with a lowerproportion of ovarian cancer. It wasn’tclear, however, whether this was due tohigher breast cancer risks, or lower ovar-ian cancer risks. A much larger study of
356 BRCA1-linked families {2914} foundthe breast cancer risk associated withmutations in the central region to be sig-nificantly lower than for other mutations(relative risk, 0.71), and the ovarian can-cer risk associated with mutations 3' tonucleotide 4191 to be significantlyreduced relative to the rest of the gene(relative risk, 0.81). Recent work sug-gests that the risk to ovarian cancermight also be influenced by genetic vari-ation in the wildtype BRCA1 copy inBRCA1 carriers {1009}.
Genetic risk modifiersOne study showed that the risk for ovari-an cancer was 2.11 times greater forBRCA1 carriers harbouring one or tworare HRAS1 alleles, compared to carrierswith only common alleles (P = 0.015).Susceptibility to breast cancer did notappear to be affected by the presence ofrare HRAS1 alleles {2240}. Likewise, alength-variation of the polyglutaminerepeats in the estrogen receptor co-acti-vator NCOA3 and the androgen receptorinfluences breast cancer risk in carriersof BRCA1 and BRCA2 {2342,2345}. Thevariant pro g e s t e rone receptor allelenamed PROGINS was associated withan odds ratio of 2.4 for ovarian canceramong 214 BRCA1/2 carriers with nopast exposure to oral contraceptives,c o m p a red to women without ovariancancer and with no PROGINS allele{2487}. These results support the hypothesis thatpathways involving endocrine signallingmay have a substantial effect onB R C A 1 / 2-associated cancer risk.Genetic variation in the genes constitut-ing the DNA repair pathways might alsobe involved. A C/G polymorphism in the5' untranslated region of RAD51 wasfound to modify both breast and ovarian
Fig. 8.06 Functional domains in BRCA1. The RING domain contains a C3HC4 motif that interacts with otherproteins. NLS = nuclear localization signal. BRCT = BRCA1-related C-terminal. The proportion encoded byexon 11 is indicated.
343BRCA1 syndrome
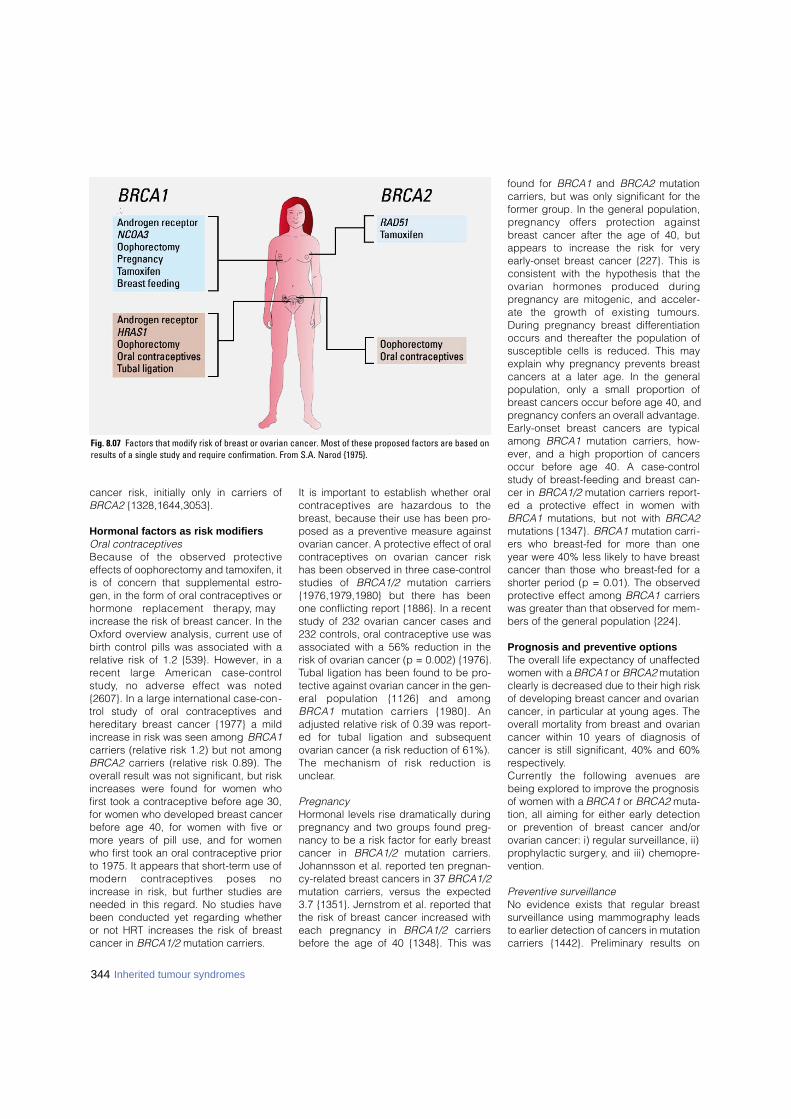
cancer risk, initially only in carriers ofBRCA2 {1328,1644,3053}.
Hormonal factors as risk modifiersOral contraceptivesBecause of the observed pro t e c t i v eeffects of oophorectomy and tamoxifen, itis of concern that supplemental estro-gen, in the form of oral contraceptives orh o rmone replacement therapy, mayincrease the risk of breast cancer. In theOxford overview analysis, current use ofbirth control pills was associated with arelative risk of 1.2 {539}. However, in arecent large American case-contro ls t u d y, no adverse effect was noted{2607}. In a large international case-con-t rol study of oral contraceptives andhereditary breast cancer {1977} a mildincrease in risk was seen among BRCA1carriers (relative risk 1.2) but not amongBRCA2 carriers (relative risk 0.89). Theoverall result was not significant, but riskincreases were found for women whofirst took a contraceptive before age 30,for women who developed breast cancerbefore age 40, for women with five ormore years of pill use, and for womenwho first took an oral contraceptive priorto 1975. It appears that short-term use ofm o d e rn contraceptives poses noincrease in risk, but further studies areneeded in this regard. No studies havebeen conducted yet regarding whetheror not HRT increases the risk of breastcancer in BRCA1/2 mutation carriers.
It is important to establish whether oralcontraceptives are hazardous to thebreast, because their use has been pro-posed as a preventive measure againstovarian cancer. A protective effect of oralcontraceptives on ovarian cancer riskhas been observed in three case-controlstudies of BRCA1/2 mutation carriers{1976,1979,1980} but there has beenone conflicting report {1886}. In a recentstudy of 232 ovarian cancer cases and232 controls, oral contraceptive use wasassociated with a 56% reduction in therisk of ovarian cancer (p = 0.002) {1976}.Tubal ligation has been found to be pro-tective against ovarian cancer in the gen-eral population {1126} and amongB R C A 1 mutation carriers {1980}. Anadjusted relative risk of 0.39 was report-ed for tubal ligation and subsequentovarian cancer (a risk reduction of 61%).The mechanism of risk reduction isunclear.
PregnancyHormonal levels rise dramatically duringpregnancy and two groups found preg-nancy to be a risk factor for early breastcancer in BRCA1/2 mutation carriers.Johannsson et al. reported ten pregnan-cy-related breast cancers in 37 BRCA1/2mutation carriers, versus the expected3.7 {1351}. Jernstrom et al. reported thatthe risk of breast cancer increased witheach pregnancy in BRCA1/2 c a r r i e r sbefore the age of 40 {1348}. This was
found for BRCA1 and BRCA2 mutationcarriers, but was only significant for theformer group. In the general population,p regnancy offers protection againstbreast cancer after the age of 40, butappears to increase the risk for veryearly-onset breast cancer {227}. This isconsistent with the hypothesis that theovarian hormones produced duringpregnancy are mitogenic, and acceler-ate the growth of existing tumours.During pregnancy breast differentiationoccurs and thereafter the population ofsusceptible cells is reduced. This mayexplain why pregnancy prevents breastcancers at a later age. In the generalpopulation, only a small proportion ofbreast cancers occur before age 40, andpregnancy confers an overall advantage.Early-onset breast cancers are typicalamong BRCA1 mutation carriers, how-ever, and a high proportion of cancersoccur before age 40. A case-contro lstudy of breast-feeding and breast can-cer in BRCA1/2 mutation carriers report-ed a protective effect in women withBRCA1 mutations, but not with BRCA2mutations {1347}. BRCA1 mutation carri-ers who breast-fed for more than oneyear were 40% less likely to have breastcancer than those who breast-fed for ashorter period (p = 0.01). The observedprotective effect among BRCA1 carrierswas greater than that observed for mem-bers of the general population {224}.
Prognosis and preventive optionsThe overall life expectancy of unaffectedwomen with a BRCA1 or BRCA2 mutationclearly is decreased due to their high riskof developing breast cancer and ovariancancer, in particular at young ages. Theoverall mortality from breast and ovariancancer within 10 years of diagnosis ofcancer is still significant, 40% and 60%respectively.C u r rently the following avenues arebeing explored to improve the prognosisof women with a BRCA1 or BRCA2 muta-tion, all aiming for either early detectionor prevention of breast cancer and/orovarian cancer: i) regular surveillance, ii)prophylactic surgery, and iii) chemopre-vention.
Preventive surveillanceNo evidence exists that regular breastsurveillance using mammography leadsto earlier detection of cancers in mutationcarriers {1442}. Preliminary results on
344 Inherited tumour syndromes
Fig. 8.07 Factors that modify risk of breast or ovarian cancer. Most of these proposed factors are based onresults of a single study and require confirmation. From S.A. Narod {1975}.
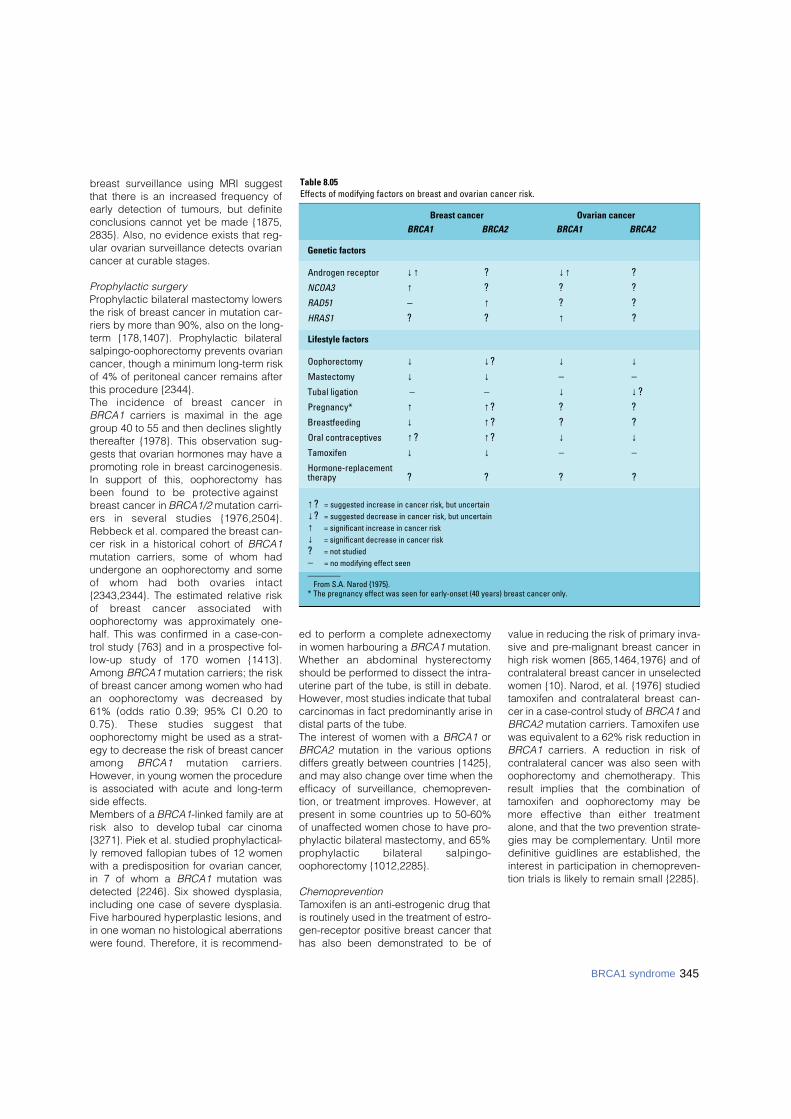
breast surveillance using MRI suggestthat there is an increased frequency ofearly detection of tumours, but definiteconclusions cannot yet be made {1875,2835}. Also, no evidence exists that reg-ular ovarian surveillance detects ovariancancer at curable stages.
Prophylactic surgeryProphylactic bilateral mastectomy lowersthe risk of breast cancer in mutation car-riers by more than 90%, also on the long-term {178,1407}. Prophylactic bilateralsalpingo-oophorectomy prevents ovariancancer, though a minimum long-term riskof 4% of peritoneal cancer remains afterthis procedure {2344}. The incidence of breast cancer inBRCA1 carriers is maximal in the agegroup 40 to 55 and then declines slightlythereafter {1978}. This observation sug-gests that ovarian hormones may have apromoting role in breast carcinogenesis.In support of this, oophorectomy hasbeen found to be protective againstbreast cancer in BRCA1/2 mutation carri-ers in several studies {1976,2504}.Rebbeck et al. compared the breast can-cer risk in a historical cohort of BRCA1mutation carriers, some of whom hadundergone an oophorectomy and someof whom had both ovaries intact{2343,2344}. The estimated relative riskof breast cancer associated withoophorectomy was approximately one-half. This was confirmed in a case-con-trol study {763} and in a prospective fol-low-up study of 170 women {1413}.Among BRCA1 mutation carriers; the riskof breast cancer among women who hadan oophorectomy was decreased by61% (odds ratio 0.39; 95% CI 0.20 to0.75). These studies suggest thatoophorectomy might be used as a strat-egy to decrease the risk of breast canceramong B R C A 1 mutation carriers.However, in young women the procedureis associated with acute and long-termside effects. Members of a BRCA1-linked family are atrisk also to develop tubal carc i n o m a{3271}. Piek et al. studied prophylactical-ly removed fallopian tubes of 12 womenwith a predisposition for ovarian cancer,in 7 of whom a BRCA1 mutation wasdetected {2246}. Six showed dysplasia,including one case of severe dysplasia.Five harboured hyperplastic lesions, andin one woman no histological aberrationswere found. Therefore, it is recommend-
ed to perform a complete adnexectomyin women harbouring a BRCA1 mutation.Whether an abdominal hystere c t o m yshould be performed to dissect the intra-uterine part of the tube, is still in debate.However, most studies indicate that tubalcarcinomas in fact predominantly arise indistal parts of the tube.The interest of women with a BRCA1 orBRCA2 mutation in the various optionsdiffers greatly between countries {1425},and may also change over time when theefficacy of surveillance, chemopreven-tion, or treatment improves. However, atpresent in some countries up to 50-60%of unaffected women chose to have pro-phylactic bilateral mastectomy, and 65%p rophylactic bilateral salpingo-oophorectomy {1012,2285}.
ChemopreventionTamoxifen is an anti-estrogenic drug thatis routinely used in the treatment of estro-gen-receptor positive breast cancer thathas also been demonstrated to be of
value in reducing the risk of primary inva-sive and pre-malignant breast cancer inhigh risk women {865,1464,1976} and ofcontralateral breast cancer in unselectedwomen {10}. Narod, et al. {1976} studiedtamoxifen and contralateral breast can-cer in a case-control study of BRCA1 andBRCA2 mutation carriers. Tamoxifen usewas equivalent to a 62% risk reduction inBRCA1 carriers. A reduction in risk ofcontralateral cancer was also seen withoophorectomy and chemotherapy. Thisresult implies that the combination oftamoxifen and oophorectomy may bem o re effective than either tre a t m e n talone, and that the two prevention strate-gies may be complementary. Until moredefinitive guidlines are established, theinterest in participation in chemopreven-tion trials is likely to remain small {2285}.
Table 8.05Effects of modifying factors on breast and ovarian cancer risk.
Breast cancer Ovarian cancer
BRCA1 BRCA2 BRCA1 BRCA2
Genetic factors
Androgen receptor ↓↑ ? ↓↑ ?NCOA3 ↑ ? ? ?RAD51 – ↑ ? ?HRAS1 ? ? ↑ ?
Lifestyle factors
Oophorectomy ↓ ↓? ↓ ↓Mastectomy ↓ ↓ – –Tubal ligation – – ↓ ↓?Pregnancy* ↑ ↑? ? ?Breastfeeding ↓ ↑? ? ?Oral contraceptives ↑? ↑? ↓ ↓Tamoxifen ↓ ↓ – –Hormone-replacementtherapy ? ? ? ?
↑? = suggested increase in cancer risk, but uncertain ↓? = suggested decrease in cancer risk, but uncertain ↑ = significant increase in cancer risk ↓ = significant decrease in cancer risk ? = not studied – = no modifying effect seen________
From S.A. Narod {1975}.* The pregnancy effect was seen for early-onset (40 years) breast cancer only.
345BRCA1 syndrome
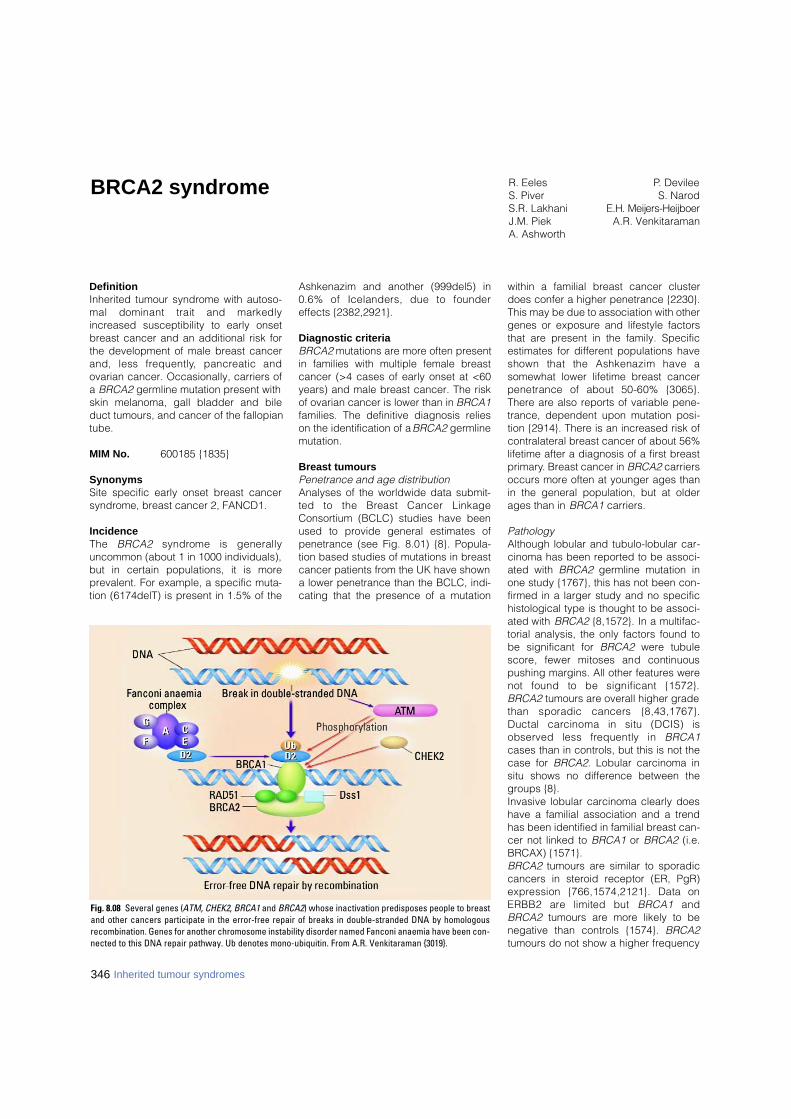
DefinitionInherited tumour syndrome with autoso-mal dominant trait and markedlyincreased susceptibility to early onsetbreast cancer and an additional risk forthe development of male breast cancerand, less fre q u e n t l y, pancreatic andovarian cancer. Occasionally, carriers ofa BRCA2 germline mutation present withskin melanoma, gall bladder and bileduct tumours, and cancer of the fallopiantube.
MIM No. 600185 {1835}
SynonymsSite specific early onset breast cancersyndrome, breast cancer 2, FANCD1.
IncidenceThe B R C A 2 s y n d rome is generallyuncommon (about 1 in 1000 individuals),but in certain populations, it is moreprevalent. For example, a specific muta-tion (6174delT) is present in 1.5% of the
Ashkenazim and another (999del5) in0.6% of Icelanders, due to foundereffects {2382,2921}.
Diagnostic criteriaBRCA2 mutations are more often presentin families with multiple female breastcancer (>4 cases of early onset at <60years) and male breast cancer. The riskof ovarian cancer is lower than in BRCA1families. The definitive diagnosis relieson the identification of a BRCA2 germlinemutation.
Breast tumoursPenetrance and age distributionAnalyses of the worldwide data submit-ted to the Breast Cancer LinkageConsortium (BCLC) studies have beenused to provide general estimates ofpenetrance (see Fig. 8.01) {8}. Popula-tion based studies of mutations in breastcancer patients from the UK have showna lower penetrance than the BCLC, indi-cating that the presence of a mutation
within a familial breast cancer clusterdoes confer a higher penetrance {2230}.This may be due to association with othergenes or exposure and lifestyle factorsthat are present in the family. Specificestimates for different populations haveshown that the Ashkenazim have asomewhat lower lifetime breast cancerpenetrance of about 50-60% {3065}.There are also reports of variable pene-trance, dependent upon mutation posi-tion {2914}. There is an increased risk ofcontralateral breast cancer of about 56%lifetime after a diagnosis of a first breastprimary. Breast cancer in BRCA2 carriersoccurs more often at younger ages thanin the general population, but at olderages than in BRCA1 carriers.
PathologyAlthough lobular and tubulo-lobular car-cinoma has been reported to be associ-ated with BRCA2 germline mutation inone study {1767}, this has not been con-firmed in a larger study and no specifichistological type is thought to be associ-ated with BRCA2 {8,1572}. In a multifac-torial analysis, the only factors found tobe significant for BRCA2 were tubules c o re, fewer mitoses and continuouspushing margins. All other features werenot found to be significant {1572}.BRCA2 tumours are overall higher gradethan sporadic cancers {8,43,1767}.Ductal carcinoma in situ (DCIS) isobserved less frequently in B R C A 1cases than in controls, but this is not thecase for BRCA2. Lobular carcinoma insitu shows no difference between thegroups {8}.Invasive lobular carcinoma clearly doeshave a familial association and a trendhas been identified in familial breast can-cer not linked to BRCA1 or BRCA2 (i.e.BRCAX) {1571}. BRCA2 tumours are similar to sporadiccancers in steroid receptor (ER, PgR)e x p ression {766,1574,2121}. Data onERBB2 are limited but B R C A 1 a n dBRCA2 tumours are more likely to benegative than controls {1574}. BRCA2tumours do not show a higher frequency
BRCA2 syndrome R. EelesS. PiverS.R. LakhaniJ.M. PiekA. Ashworth
P. DevileeS. Narod
E.H. Meijers-HeijboerA.R. Venkitaraman
Fig. 8.08 Several genes (ATM, CHEK2, BRCA1 and BRCA2) whose inactivation predisposes people to breastand other cancers participate in the error-free repair of breaks in double-stranded DNA by homologousrecombination. Genes for another chromosome instability disorder named Fanconi anaemia have been con-nected to this DNA repair pathway. Ub denotes mono-ubiquitin. From A.R. Venkitaraman {3019}.
346 Inherited tumour syndromes

of TP53 mutation and p53 expressionc o m p a red to sporadic breast cancer{580,581,1574}.
Prognosis and prognostic factorsSince the breast cancers associated withBRCA2 mutations are more often estro-gen receptor positive and are associatedwith DCIS, they would be expected tohave a better prognosis. The most sys-tematic study to investigate pro g n o s i shas analysed the survival of Ashkenaziwomen with breast cancer who havemutations as tested from paraff i n - s t o re dtissue. This is possible because theyhave a single 6174delT founder mutation.T h e re was no diff e rence in survivalbetween carriers and non-carriers {441}.
Risk modifiers and preventionThe preventive effect of oophorectomyand tamoxifen, mastectomy, and the pos-sible hazard associated with oral contra-ceptives are similar in both BRCA syn-dromes have been dealt with in the pre-ceding section on BRCA1.
Ovarian tumoursPenetrance and age distributionAbout 7-10% of ovarian carcinomas aredue to inherited BRCA1 or BRCA2 muta-tions; as these are on autosomes, theycan be inherited from either the mother orthe father. Although ovarian cancer canoccur earlier in B R C A 1 and indeedBRCA2 carriers, the presence of an olderonset ovarian cancer still can indicate anunderlying mutation in either of thesegenes. The penetrance of ovarian cancerin BRCA2 carriers is shown in Fig. 8.02;the risk of developing ovarian cancer byage 70 in BRCA2 families is approxi-mately 27% {898}. It should be noted thatthe penetrance curve starts to rise laterthan for BRCA1 which could have impli-cations for the timing of prophylacticoophorectomy.
PathologyCompared with the information on thepathology of BRCA1-associated ovariancancers, little is re p o rted on B R C A 2m u t a t i o n - related ovarian tumours. Thepaucity of information is accounted forby the low incidence of this diseasec o m p a red with that of B R C A 1- l i n k e dcases {329,973}. Some recent studiesindicate that the histological phenotypeof these ovarian neoplasms is similar tothat of BRCA1-associated carcinomas
and are predominantly of papillaryserous type {329,2239,3272}. A singlecase of an ovarian malignant mixed mül-lerian tumour (carc i n o s a rcoma), hasbeen reported as occurring in a BCRA2mutation carrier {2748}.The data on grade are similar to those ofBRCA1 ovarian cancers with an associa-tion with higher grade but limited num-bers in study and interobserver variation{329,2239,2479,3102,3272} in the scor-ing of grade should be taken intoaccount when considering the evidenceThere are no data to support a role ofB R C A 2 in borderline ovarian lesions{1044,1704} nor are there germ cell orsex cord stromal tumours.
Prevention by oral contraceptivesAlthough it has been long known that oralcontraceptives can decrease the risk ofdeveloping ovarian cancer in the generalpopulation {2}, recently there is evidencethat this may also be true for hereditaryovarian cancer {1976,1979,1980}. Seethe preceding section on BRCA1 syn-drome for further details.
Prognosis and prognostic factorsIn a retrospective cohort study, womenwith BRCA1 or BRCA2 founder mutationadvanced-stage ovarian cancer had alonger survival compared with womenwith non-hereditary ovarian cancer (P =0.004) and a longer median time torecurrence (14 months versus 7 months)(P< 0.001) {329}.Studies of ovarian cancer occurring inBRCA2 carriers have reported a betterp rognosis {329}, but it is uncert a i nwhether this is because of the bias incarrier detection in this population orwhether they are more sensitive to treat-ment. If the latter is true, this would beplatinum treatments as these data areprior to the use of taxanes.
Tumours of the fallopian tubeHereditary fallopian tube carcinoma aris-es from epithelium overlying the laminapropria of the endosalpinx in women athigh hereditary risk to develop ovariancarcinoma. Loss of the wild-type breastcancer 1 or 2 gene (BRCA1/2) allele ismost likely pivotal in carcinogenesis ofthese tumours. To be unequivocally iden-tified, the tumour has to fulfill the clinicaland histological criteria for tubal carcino-ma {1256} as well as clinical genetic cri-teria.
Incidence F rom 1997 to 2002, a total of 15 here d i t a ryb reast/ovarian family related tubaltumours have been re p o rted in literature .In 4 cases, a B R C A 2 mutation was detec-ted. However, the true incidence of here d i-t a ry tubal carcinoma is probably muchh i g h e r, as is suggested for its sporadicc o u n t e r p a rt. This is caused by the fact thatp r i m a ry tubal tumours are often mistakenfor primary ovarian carcinomas {3150}.M o re o v e r, some primary ovarian carc i n o-mas might actually derive from inclusioncysts lined by tubal epithelial cells inclu-ded into the ovarian stroma {2247}.
Age distributionIn general the age of onset is younger inhereditary cases when compared to spo-radic cases.
Diagnostic criteriaThe criteria of Hu et. al. {1256} as modi-fied by Sedlis {2614} and Yo o n e s s i{3185} are applied to differentiate hered-itary tubal carcinomas from ovarian andendometrial carcinoma. These criteriarequire that: (i) the main tumour is in thefallopian tube and arises from the endo-salpinx, (ii) the histological feature sresemble a tubal pattern, (iii) if the tubalwall is involved, the transition betweenmalignant and benign tubal epitheliumshould be detectable, (iv) the fallopiantube contains more tumour than theovary or endometrium.
Clinical features
Symptoms and signs. To date, there isno indication that clinical hereditary tubalc a rcinoma features are diff e rent fro mthose of its sporadic counterpart ;abdominal discomfort is more or lesscommon, but an atypical complaint. Theclassical but rare triad of symptomsinclude: (i) prominent watery vaginal dis -charge, (ii) pelvic pain and (iii) pelvicmass {158}. It has been reported thatapproximately 10% of patients will havea d e n o c a rcinomatous cells in cervicalcytology {3185}.
Tumour markers. As in ovarian carcino-ma elevation of serum CA125 levels canbe found in approximately 80% of cases{1173}.
Imaging. CT / MRI are inconclusive withrespect to the differential diagnosis of
347BRCA2 syndrome

348 Inherited tumour syndromes
tubal or ovarian carcinomas. However,these techniques can be helpful in deter-mining the extent of disease. Likewise,ultrasonography can not distinguishtubal from ovarian disease {2720}.
Pathology
Histopathology and grading. S e ro u spapillary carcinoma is the most commonf o rm of here d i t a ry tubal carc i n o m a .Grading is of limited value in thesetumours and, if used, is based on thepapillary architecture, nuclear atypia andmitotic activity. Grade I cancers showpapillary growth with well differentiatedcolumnar cells and low mitotic rate.Grade II cancers are papillary with evi-dent gland formation with intermediatelydifferentiated cells with moderate mitoticactivity. Grade III shows solid growth withloss of papillae and a medullary/glandu-lar pattern. The cells are poorly differen-tiated and the mitotic activity is high.
Immunoprofile. Being predominantly ofserous papillary type, hereditary tubalcarcinomas are positive for cytokeratins7 and 8, MUC1, CEA, OVTL3, OV632,CA125, and negative or showing only lowexpression for cytokeratin 20, CEA andvimentin. Also, p53 is often expressed,and cyclins E and A and Ki67 show av a rying number of proliferating cells,w h e reas staining for HER-2/neu andcyclin D1 is usually negative. Steroidreceptor content varies. In the rare clearcell cancers, p21 is highly expressed.
Seeding and metastasisHereditary tubal carcinomas presumablyspread like their sporadic counterparts.However, only empirical data are avail-able to date, pointing to a mode ofspread similar to ovarian cancer.
SurvivalThe five-year survival rate of 30% in spo-radic cases varies with stage {158,3185},but not with grade. The survival rate ofhereditary tubal carcinomas has yet tobe established since only small numbersof patients have been reported and mostpatients have still not completed their 5-year follow-up.
Prophylactic interventionsIn one study, 30 women with either a doc-umented deleterious BRCA1 or BRCA2mutation or a suggestive family history
underwent prophylactic oophore c t o m y{1617}. Five of these (17%) were found tohave clinically occult malignancy, 3 ofwhich involved a primary fallopian tubemalignancy. Three of the five were knownBRCA1 mutation carriers, one had a doc-umented BRCA2 mutation. Therefore, it isrecommended to perform a completeadnexectomy in women carrying aBRCA1 or a BRCA2 mutation. Whetheran abdominal hysterectomy should bep e rf o rmed to dissect the intra-uterinep a rt of the tube, is still in debate.However, most studies indicate that tubalcarcinomas in fact predominantly arise indistal parts of the tube.
Other tumoursBRCA2 confers an increased risk of ovar-ian cancer, but not as high as that forBRCA1. Statistically significant increasesin risk were observed for a number ofother tumour types, including prostate,pancreatic and stomach cancer. The riskfor prostate cancer is probably not suffi-ciently high to cause an appreciablefraction of early-onset prostate cancercases. The risk for male breast cancer,although the hallmark of BRCA2 muta-tions, is based on only four observedcases and hence is very imprecise.
GeneticsChromosomal location and genestructureB R C A 2 is located on chro m o s o m e13q12.3. It consists of 27 exons, of whichexon 11 is remarkably large (4.9 kb). Theopen reading frame is 10,254 basepairs,encoding a protein of 3,418 aminoacidsthat has no significant similarity to anyknown protein. Exon 11 encodes a struc-tural motif consisting of eight ‘BRC’repeats, through which BRCA2 controlsthe function of RAD51, a recombinaseenzyme, in pathways for DNA repair byhomologous recombination.
Gene expression A wide range of human tissues expressBRCA2 mRNA, in a pattern very similar tothat of BRCA1, but the highest levelswere observed in breast and thymus,with slightly lower levels in lung, ovary,and spleen {2891}. In normal cells,BRCA2 is a nuclear protein, preferential-ly expressed during the late-G1/early-Sphase of the cell cycle {258,480,3012}. Inmice, Brca1 and Brca2 are coordinatelyupregulated during ductal proliferation,morphogenesis and diff e rentiation ofbreast epithelial cells occurring at puber-ty, pregnancy and lactation {1582,1769,
Table 8.06Cancer risks of BRCA2 carriers.
Cancer site Relative risk Cumulative Risk By Age 70, %or type (95% CI) (95% CI)
Breast (female) Age-dependent 84 (43 – 95)
Breast (male) 150 6.3 (1.4 – 25.6)
Ovary Age-dependent 27 (0 – 47)
Gall bladder and bile ducts 4.97 (1.50 – 16.5) -
Prostate 4.65 (3.48 – 6.22) 7.5 (5.7 – 9.3)
Prostate before age 65 7.33 (4.66 – 11.52) -
Pancreas1 3.51 (1.87 – 6.58) Males: 2.1 (1.2 – 3.0))Females: 1.5 (0.9 – 2.1)
Stomach1 2.59 (1.46 - 4.61) -
Malignant melanoma 1 2.58 (1.28 – 5.17) -
All cancers2 2.45 (2.15 – 2.78) -________
From D. Ford et al. 1998 {898}, D.F. Easton et al. 1997 {744} and the Breast Cancer Linkage Consortium 1999 {11}.1 Relative risks were slightly higher for individuals aged 65 or under.2 All cancers other than nonmelanoma skin cancer, breast cancer, or ovarian cancer.

2323}. Both proteins co-exist with RAD51in subnuclear foci during S phase, whichredistribute following DNA damage{450,2193}.Exon 12 of the messenger is alternative-ly spliced, and there is some suggestionthat this splice variant is expressed athigher levels in about a third of sporadicbreast tumour when compared to normalepithelial cells {266}. In sporadic breasttumours, BRCA2 mRNA-expression washigher than that in normal surroundingtissues in 20% of the cases, and lower in11% {267}. In agreement with this, nohypermethylation of the BRCA2 promotorregion has been detected in breast andovarian cancer {541}.
Gene functionLoss, or mutational inactivation, of thesingle wild-type allele in heterozygouscarriers of mutations in the BRCA2 geneis a key step in tumourigenesis. Themechanism by which the encoded pro-tein contributes to disease progression isnot yet completely understood but isthought to be related, at least in part, tothe proposed role of BRCA2 in the repairof damaged DNA. B R C A 2 encodes a very large (3,418amino acids in humans) protein that isexpressed during S phase of the cellcycle when it is present in the cell nucle-us. Although the amino acid sequence ofthe BRCA2 protein presents few directclues as to its normal cellular role, somefunctional domains have been defined.The C-terminal region of BRCA2 containsa functional nuclear localization se-quence; many pathogenic truncatingmutations in human BRCA2 are proximalto this domain and would therefore bepredicted to encode cytoplasmic pro-teins. The central part of the proteinencoded by the large exon 11 containseight copies of a novel sequence (theBRC repeat) that has been shown to becapable of binding RAD51 pro t e i n .RAD51 is a key protein involved in dou-ble-strand DNA break repair and homol-ogous recombination and the interactionwith BRCA2 was the first evidence impli-cating the protein in these processes.BRCA2-deficient cells and tumours char-acteristically accumulate aberrations inc h romosome structure {3018}. Theselesions include breaks involving one ofthe two sister chromatids, as well as tri-radial and quadri-radial chromosomestypical of Bloom syndrome and Fanconi
anaemia. Thus, BRCA2 deficiency maybe similar in its pathogenesis to othergenetic diseases in which unstable chro-mosome structure is linked to cancerpredisposition.C h romatid-type breaks, tri-radial andquadri-radial chromosomes are thoughtto arise from defects in the repair of DNAdouble-strand breaks (DSBs) during theS phase of cell cycle. During S phase,DSB repair proceeds pre f e re n t i a l l ythrough mechanisms involving homolo-gous recombination. These mechanismsenable error-free repair of broken DNA,taking advantage of the availability of thereplicated sister chromatid as a sub-strate for recombination reactions. InBRCA2-deficient cells, DSB repair byhomologous recombination is defective.However, alternative – but error-prone -
mechanisms for DSB repair such as end-joining or strand-annealing are still pres-ent. The end result is that DSBs inBRCA2-deficient cells are mis-repaired,giving rise to mutations and chromoso-mal rearrangements including transloca-tions or deletions. The resulting geneticinstability is believed to potentiate theacquisition of mutations that transform anormal cell into a cancer cell. Thus,BRCA2 works as a tumour suppressorindirectly through its ‘caretaker’ role inprotecting chromosomal stability.BRCA2 is essential for homologousrecombination because it controls theintra-cellular transport and activity ofRAD51. In BRCA2-deficient cells, RAD51fails to efficiently enter the nucleus. Aftere x p o s u re of BRCA2-deficient cells to DNAdamaging agents, RAD51 fails to localize
Fig. 8.10 Aberrations in chromosome structure reminiscent of Bloom syndrome and Fanconi anaemia accu-mulate during the division of BRCA2-deficient cells in culture. Enlargements of characteristic aberrations areshown in the panels on the right hand-side (ctb, chromatid break, tr, tri-radial and qr, quadri-radial).Reproduced from K.J. Patel et al. {2193}.
349BRCA2 syndrome
Fig. 8.09 Functional domains in BRCA2. There are 8 BRC repeats in the central region of the protein whichinteract with RAD51. NLS = nuclear localization signal. The proportion encoded by exon 11 is indicated.

350 Inherited tumour syndromes
in typical nuclear foci that may re p re s e n tsites for DNA damage pro c e s s i n g .M o re o v e r, BRCA2 controls the assemblyof RAD51 into a nucleoprotein filamentthat coats DNA, a critical interm e d i a t es t r u c t u re in recombination re a c t i o n s .Unexpected and potentially inform a t i v einsight into the role of BRCA1/2 genes inDNA repair in humans in vivo has comef rom recent studies on Fanconi anaemia( FA), a complex disorder characterizedby congenital abnormalities, pro g re s s i v ebone marrow failure and cancer suscepti-b i l i t y. FA is a recessively inherited disor-der which can result from mutation in atleast 8 individual genes. It has re c e n t l ybeen suggested that one of the pre v i o u s-ly unidentified FA genes, FANCD1, is infact BRCA2 {1251}. The cellular conse-quences of homozygosity for B R C A 2mutation, including spontaneous chro m o-some instability and hypersensitivity toDNA cross-linking agents, are rather sim-ilar to those observed in cells derivedf rom FA patients. This is not the only linkbetween FA and breast cancer suscepti-bility genes. Another FA gene pro d u c t ,FANCD2, can interact and co-localizewith BRCA1 {958}. Thus it seems that thepathways disrupted in FA and breast can-cer susceptibility are intimately connect-ed. Only a small pro p o rtion of FA, which initself is rare, is caused by B R C A 2 m u t a-tion but the importance of this finding isthat it connects together two pre v i o u s l yd i ff e rent bodies of work on DNA re p a i r. A current simplified model on howBRCA2 and several other genes involvedin breast cancer predisposition act coor-dinately to repair DNA damage is indi-cated in Fig. 8.08. ATM and CHEK2 pro-tein kinases signal the presence of dou-ble-stranded DNA breaks and phospho-rylate (red arrows) a number of down-s t ream effector proteins, includingBRCA1. This induces their migration tosites where DNA is repaired. BRCA2 car-ries the DNA-recombination enzymeRAD51 to the same sites, guided thereby the DNA-binding structures formedbetween its C-terminal domain and Dss1protein. A complex of Fanconi anaemiaproteins – termed A, C, D2, E, F, and G –triggers the ubiquitination of the D2 pro-tein alone and its colocalization withBRCA1.Other roles for BRCA2 have been sug-gested in chromatin remodelling andgene transcription {1442}. Such func-tions – which remain very poorly charac-
terized – may help to explain why cancerpredisposition associated with BRCA2mutations should be specific to tissuessuch as the breast and ovary. However,notwithstanding these other potentialfunctions, it seems likely that loss ofBRCA2 function engenders genomicinstability leading to oncogene activationand tumour suppressor loss that culmi-nates in tumourigenic pro g ression. Amajor challenge for future work will be tounderstand how this basic pathogenicmechanism plays out in the complex tis-sue environments of the breast, ovary orp rostate, giving rise to site-specificepithelial malignancies.
Mutation spectrumG e rmline mutations in B R C A 2 have beendetected in 5-10% of clinic-based bre a s tcancer families, and in similar fre q u e n-cies of breast-ovarian cancer families{2657,3023}. Somatic mutations in spo-radic breast and ovarian tumours aree x t remely rare. Mutations occur thro u g h-out the entire coding region, and hencethe mutation spectrum did not pro v i d eimmediate clues to functional genedomains. The majority of the mutationsa re predicted to lead to a pre m a t u re l ytruncated protein when translated. Inconjunction with the observed loss of thewildtype allele in tumours arising in muta-tion carriers {560}, this indicates thei m p o rtance of gene inactivation fortumourigenesis to occur. Despite thes t rong variability in mutations detected infamilies, founder effects have led to somemutations being very prevalent in cert a i npopulations of defined geographical orethnic background. Examples are the999del5 mutation, which is present ina p p roximately 0.6% of all Icelandic indi-viduals {2920}, and the 6174delT muta-tion found in an equal pro p o rtion ofAshkenazi Jews {2083}. As a result, muta-tion spectra may vary according to ethnicb a c k g round of the sampled population{2824}. In recent years, an incre a s i n gnumber of missense changes are beingdetected in B R C A 2 of which the clinicalsignificance is uncertain in the absenceof a functional assay. These already com-prise up to 50% of all known sequencechanges in B R C A 2. Although many ofthem are expected to be rare neutralpolymorphisms, some might be associat-ed with elevated levels of breast cancerrisk. An example is the arginine for histi-dine substitution at codon 372 {1167}.
Many known deleterious B R C A 1 a n dB R C A 2 mutations affect splicing, andthese typically lie near intron/exon bound-aries. However, there are also potentiali n t e rnal exonic mutations that disruptfunctional exonic splicing enhancer (ESE)sequences, resulting in exon skipping. AT2722R mutation segregated with aff e c t-ed individuals in a family with breast can-cer and disrupted 3 potential ESE sites{816}. The mutation caused deleteriousp rotein truncation and suggested apotentially useful method for determ i n i n gthe clinical significance of a subset of themany unclassified variants of B R C A 1 a n dB R C A 2. As more functional and structur-al information on the BRCA1 and BRCA2p roteins accumulates, our understandingof genetic variation in these genes willi m p rove. The Breast Cancer Inform a t i o nC o re (BIC) maintains a website pro v i d i n ga central re p o s i t o ry for inform a t i o nre g a rding mutations and polymorphisms( h t t p : / / re s e a rc h . n h g r i . n i h . g o v / b i c / ) .
Genotype-phenotype correlationsEvidence is accumulating that the risksconferred by pathogenic BRCA2 muta-tions are dependent on the position ofthe mutation in the gene, genetic varia-tion in other genes, and environmental orlifestyle factors.
BRCA2 mutation positionTruncating mutations in families with thehighest risk of ovarian cancer relative tobreast cancer are clustered in a region ofapproximately 3.3 kb in exon 11 {972}.This region of B R C A 2, bounded bynucleotides 3035 and 6629, was dubbedthe 'ovarian cancer cluster region,' orOCCR. Notably, this region coincideswith the BRC repeats that are critical forthe functional interaction with the RAD51protein. A much larger study of 164 fam-ilies confirmed that OCCR mutations areassociated with a lower risk of breastcancer and with a higher risk of ovariancancer {2913}. The extent of risk modifi-cation is too moderate, however, to beused in genetic counseling.
Genetic risk-modifiersA length-variation of the polyglutaminerepeats in the estrogen receptor co-acti-vator NCOA3 influences breast cancerrisk in carriers of B R C A 1 and B R C A 2{2345}. Although it should be noted thatmost of the carriers in these studies areB R C A 1 carriers, and there was insuff i-
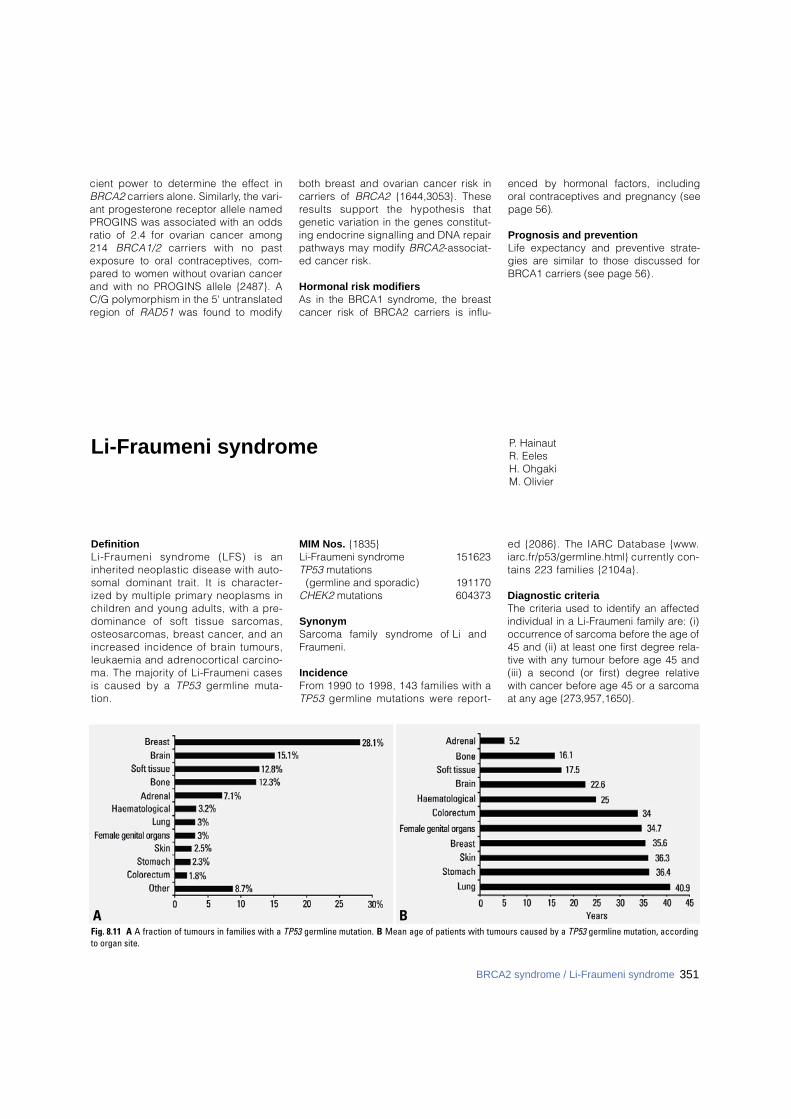
cient power to determine the effect inB R C A 2 carriers alone. Similarly, the vari-ant pro g e s t e rone receptor allele namedPROGINS was associated with an oddsratio of 2.4 for ovarian cancer among214 B R C A 1 / 2 carriers with no paste x p o s u re to oral contraceptives, com-p a red to women without ovarian cancerand with no PROGINS allele {2487}. AC/G polymorphism in the 5' untranslatedregion of R A D 5 1 was found to modify
both breast and ovarian cancer risk incarriers of B R C A 2 {1644,3053}. Theseresults support the hypothesis thatgenetic variation in the genes constitut-ing endocrine signalling and DNA re p a i rpathways may modify B R C A 2- a s s o c i a t-ed cancer risk.
Hormonal risk modifiersAs in the BRCA1 syndrome, the breastcancer risk of BRCA2 carriers is influ-
enced by hormonal factors, includingoral contraceptives and pregnancy (seepage 56).
Prognosis and preventionLife expectancy and preventive strate-gies are similar to those discussed forBRCA1 carriers (see page 56) .
Li-Fraumeni syndrome P. HainautR. EelesH. OhgakiM. Olivier
DefinitionLi-Fraumeni syndrome (LFS) is aninherited neoplastic disease with auto-somal dominant trait. It is character-ized by multiple primary neoplasms inc h i l d ren and young adults, with a pre-dominance of soft tissue sarc o m a s ,o s t e o s a rcomas, breast cancer, and ani n c reased incidence of brain tumours,leukaemia and adre n o c o rtical carc i n o-ma. The majority of Li-Fraumeni casesis caused by a T P 5 3 g e rmline muta-t i o n .
MIM Nos. {1835}Li-Fraumeni syndrome 151623TP53 mutations
(germline and sporadic) 191170CHEK2 mutations 604373
SynonymS a rcoma family syndrome of Li andFraumeni.
IncidenceF rom 1990 to 1998, 143 families with aT P 5 3 g e rmline mutations were re p o rt-
ed {2086}. The IARC Database { w w w.i a rc . f r / p 5 3 / g e rmline.html} c u r rently con-tains 223 families {2104a}.
Diagnostic criteriaThe criteria used to identify an affectedindividual in a Li-Fraumeni family are: (i)occurrence of sarcoma before the age of45 and (ii) at least one first degree rela-tive with any tumour before age 45 and(iii) a second (or first) degree relativewith cancer before age 45 or a sarcomaat any age {273,957,1650}.
BAFig. 8.11 A A fraction of tumours in families with a TP53 germline mutation. B Mean age of patients with tumours caused by a TP53 germline mutation, accordingto organ site.
351BRCA2 syndrome / Li-Fraumeni syndrome
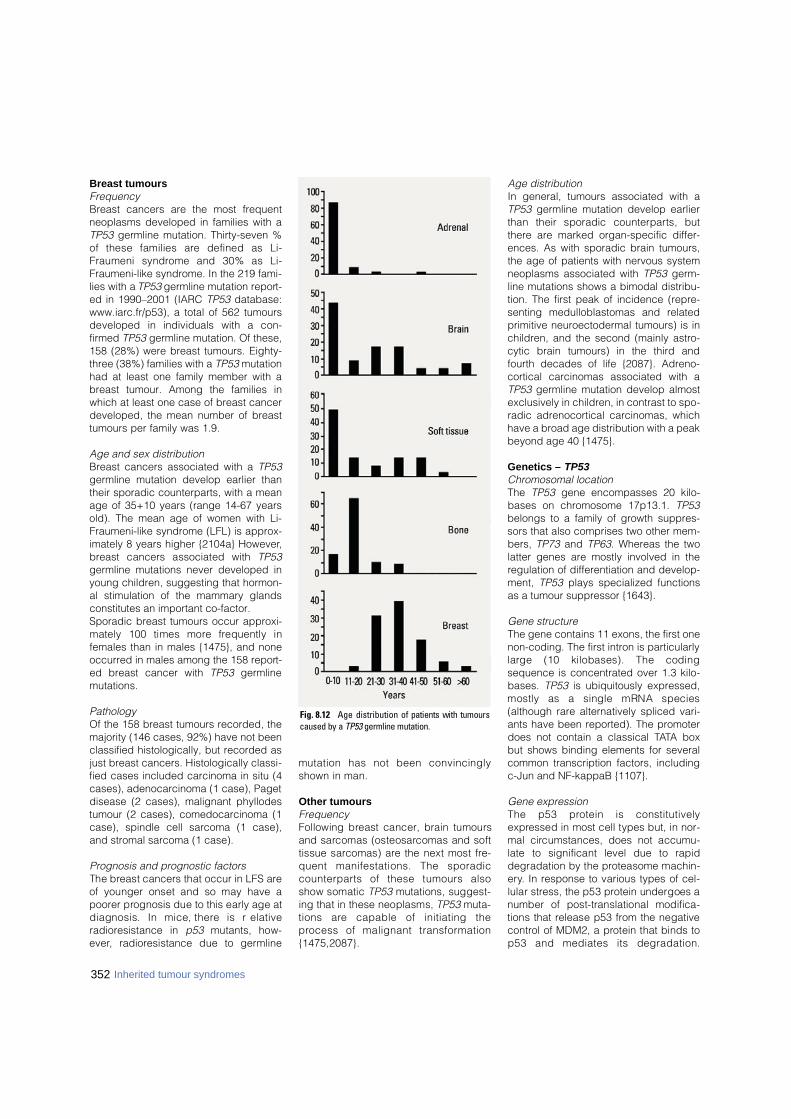
Breast tumoursFrequency Breast cancers are the most frequentneoplasms developed in families with aTP53 germline mutation. Thirty-seven %of these families are defined as Li-Fraumeni syndrome and 30% as Li-Fraumeni-like syndrome. In the 219 fami-lies with a TP53 germline mutation report-ed in 1990–2001 (IARC TP53 database:www.iarc.fr/p53), a total of 562 tumoursdeveloped in individuals with a con-firmed TP53 germline mutation. Of these,158 (28%) were breast tumours. Eighty-three (38%) families with a TP53 mutationhad at least one family member with abreast tumour. Among the families inwhich at least one case of breast cancerdeveloped, the mean number of breasttumours per family was 1.9.
Age and sex distributionBreast cancers associated with a TP53germline mutation develop earlier thantheir sporadic counterparts, with a meanage of 35+10 years (range 14-67 yearsold). The mean age of women with Li-Fraumeni-like syndrome (LFL) is approx-imately 8 years higher {2104a} However,b reast cancers associated with T P 5 3germline mutations never developed inyoung children, suggesting that hormon-al stimulation of the mammary glandsconstitutes an important co-factor.Sporadic breast tumours occur approxi-mately 100 times more frequently infemales than in males {1475}, and noneoccurred in males among the 158 report-ed breast cancer with TP53 germlinemutations.
PathologyOf the 158 breast tumours recorded, themajority (146 cases, 92%) have not beenclassified histologically, but recorded asjust breast cancers. Histologically classi-fied cases included carcinoma in situ (4cases), adenocarcinoma (1 case), Pagetdisease (2 cases), malignant phyllodestumour (2 cases), comedocarcinoma (1case), spindle cell sarcoma (1 case),and stromal sarcoma (1 case).
Prognosis and prognostic factorsThe breast cancers that occur in LFS areof younger onset and so may have ap o o rer prognosis due to this early age atdiagnosis. In mice, there is re l a t i v er a d i o resistance in p 5 3 mutants, how-e v e r, radioresistance due to germ l i n e
mutation has not been convincinglyshown in man.
Other tumoursFrequencyFollowing breast cancer, brain tumoursand sarcomas (osteosarcomas and softtissue sarcomas) are the next most fre-quent manifestations. The sporadicc o u n t e r p a rts of these tumours alsoshow somatic T P 5 3 mutations, suggest-ing that in these neoplasms, T P 5 3 m u t a-tions are capable of initiating thep rocess of malignant transform a t i o n{ 1 4 7 5 , 2 0 8 7 } .
Age distributionIn general, tumours associated with aTP53 germline mutation develop earlierthan their sporadic counterparts, butthere are marked organ-specific differ-ences. As with sporadic brain tumours,the age of patients with nervous systemneoplasms associated with TP53 germ-line mutations shows a bimodal distribu-tion. The first peak of incidence (repre-senting medulloblastomas and relatedprimitive neuroectodermal tumours) is inchildren, and the second (mainly astro-cytic brain tumours) in the third andfourth decades of life {2087}. Adreno-cortical carcinomas associated with aTP53 germline mutation develop almostexclusively in children, in contrast to spo-radic adrenocortical carcinomas, whichhave a broad age distribution with a peakbeyond age 40 {1475}.
Genetics – TP53Chromosomal locationThe TP53 gene encompasses 20 kilo-bases on chromosome 17p13.1. TP53belongs to a family of growth suppres-sors that also comprises two other mem-bers, TP73 and TP63. Whereas the twolatter genes are mostly involved in theregulation of differentiation and develop-ment, TP53 plays specialized functionsas a tumour suppressor {1643}.
Gene structureThe gene contains 11 exons, the first onenon-coding. The first intron is particularlylarge (10 kilobases). The codingsequence is concentrated over 1.3 kilo-bases. TP53 is ubiquitously expressed,mostly as a single mRNA species(although rare alternatively spliced vari-ants have been reported). The promoterdoes not contain a classical TATA boxbut shows binding elements for severalcommon transcription factors, includingc-Jun and NF-kappaB {1107}.
Gene expressionThe p53 protein is constitutivelye x p ressed in most cell types but, in nor-mal circumstances, does not accumu-late to significant level due to rapiddegradation by the proteasome machin-e ry. In response to various types of cel-lular stress, the p53 protein undergoes anumber of post-translational modifica-tions that release p53 from the negativec o n t rol of MDM2, a protein that binds top53 and mediates its degradation.
352 Inherited tumour syndromes
Fig. 8.12 Age distribution of patients with tumourscaused by a T P 5 3 germline mutation.

353Li-Fraumeni syndrome
These modifications result in the intranu-clear accumulation of p53 and in its acti-vation as a transcription factors. Tw omajor signaling pathways can triggerT P 5 3 activation. The first, and best char-acterized, is the pathway of response toDNA damage, including large kinases ofthe phosphoinositol-3 kinase family suchas AT M (ataxia telangiectasia mutated)and the cell-cycle re g u l a t o ry kinaseC H E K 2. Both of these kinases phospho-rylate p53 in the extreme N-term i n u s(serines 15, 20 and 37), within the re g i o nthat binds to MDM2. The second is acti-vated in response to the constitutivestimulation of gro w t h - p romoting signal-ing cascades. The central regulator inthis pathway is p14ARF, the altern a t i v ep roduct of the locus encoding thecyclin-kinase inhibitor p 1 6 / C D K N 2 a.p14ARF expression is activated by E2Ftranscription factors, and binds toMDM2, thus neutralizing its capacity toinduce p53 degradation. This pathwaymay be part of a normal feedback con-t rol loop in which p53 is activated as acell-cycle brake in cells exposed toh y p e r p roliferative stimuli {2267}.
Gene functionAfter accumulation, the p53 protein actsas a transcriptional regulator for a panelof genes that differ according to thenature of the stimulus, its intensity andthe cell type considered. Broadly speak-ing, the genes controlled by p53 fall intot h ree main categories, including cell-cycle regulatory genes (WAF1, GADD45,14-3-3S, CYCLING), pro - a p o p t o t i cgenes (FAS/APO1/CD95, KILLER/DR5,AIF1, PUMA, BAX) and genes involved inDNA repair (O6MGMT, MLH2). The p53protein also binds to compoments of thetranscription, replication and re p a i rmachineries and may exert additionalcontrols on DNA stability through themodulation of these mechanisms.Collectively, the p53 target genes medi-ate two type of cellular responses: cell-cycle arrest, followed by DNA repair incells exposed to light forms of genotoxicstress, and apoptosis, in cells exposedto levels of damage that cannot be effi-ciently repaired. Both responses con-tribute to the transient or permanent sup-pression of cells that contain damaged,potentially oncogenic DNA. In themouse, inactivation of Tp53 by homolo-gous recombination does not preventnormal growth but results in a strong pre-
disposition to early, multiple cancers,illustrating the crucial role of this gene asa tumour suppressor {714}.
Mutation spectrumThe T P 5 3 gene is frequently mutated inmost forms of sporadic cancers, withp revalences that range from a few per-cents in cervical cancers and in malignantmelanomas to over 50% in invasive carc i-nomas of the aero-digestive tract. Over75% of the mutations are single base sub-stitutions (missense or nonsense), cluster-ing in exons 5 to 8 that encode the DNA-binding domain of the protein. Codons175, 245, 248, 273 and 282 are majormutation hotspots in almost all types ofcancers. To g e t h e r, these codons containover 25% of all known T P 5 3 m u t a t i o n s .Other codons are mutation hotspots inonly specific tumour types, such as codon249 in hepatocellular carcinoma andcodon 157 in bronchial cancer. Mutationp a t t e rns can differ significantly betweenbetween diff e rent types cancers orbetween geographic areas for the samecancer type (as for example hepatocellu-lar carcinoma). These observations haveled to the concept that mutation pattern smay reveal clues on the cellular or envi-ronmental mechanisms that have causedthe mutations {1107}. In sporadic bre a s tcancers, T P 5 3 is mutated in about 25% ofthe cases. However, several studies havere p o rted accumulation of the p53 pro t e i nwithout mutation in up to 30-40% of inva-
sive ductal carcinoma in situ. The mutationp a t t e rn is similar to that of many other can-cers and does not provide information onpossible mutagenic events. There is limit-ed evidence that the mutation pre v a l e n c eis higher in BRCA1 mutation carriers. G e rmline T P 5 3 mutations have beenidentified in 223 families. Of these fami-lies, 83 match the strict LFS criteria, 67c o r respond to the extended, LFL defini-tion, 37 have a family history of cancerthat does not fit within LFS or LFL defini-tions and 36 have germline mutationswithout documented familial history ofcancer (IARC TP53 mutation database,w w w. i a rc.fr/p53). The codon distributionof germline T P 5 3 mutations show thesame mutational hotspots as somaticmutations {1475}. The distribution ofinherited mutations that predisposes tob reast cancer are scattered along exons5 to 8 with relative "hotspots" at codons245, 248 and 273, which are also com-monly mutated in somatic breast cancer.In contrast, a total of 16 breast cancershave been detected in 5 families with ag e rmline mutation at codon 133, a posi-tion which is not a common mutationhotspot in somatic breast cancer. Itremains to be established whether thismutant has particular functional pro p e r-ties that predispose to breast cancer.
Genotype-phenotype correlationsBrain tumours appear to be associatedwith missense TP53 mutations in the
Fig. 8.13 The p53 signaling pathway. In normal cells the p53 protein is kept in a latent state by MDM2.Oncogenic and genotoxic stresses release p53 from the negative control of MDM2, resulting in p53 accu-mulation and activation. Active p53 acts as transcription factor for genes involved cell cycle control, DNArepair and apoptosis, thus exerting a broad range of antiproliferative effects.
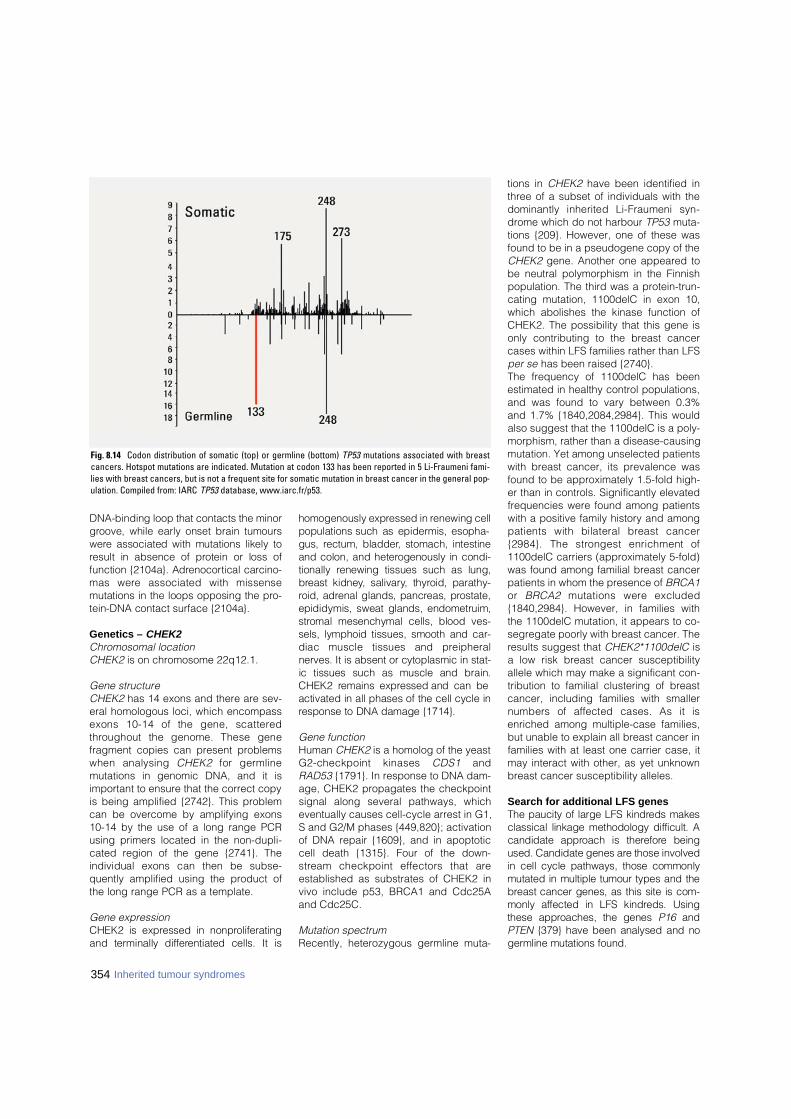
354 Inherited tumour syndromes
DNA-binding loop that contacts the minorg roove, while early onset brain tumoursw e re associated with mutations likely toresult in absence of protein or loss offunction {2104a}. Adre n o c o rtical carc i n o-mas were associated with missensemutations in the loops opposing the pro-tein-DNA contact surface {2104a}.
Genetics – CHEK2Chromosomal locationCHEK2 is on chromosome 22q12.1.
Gene structureCHEK2 has 14 exons and there are sev-eral homologous loci, which encompassexons 10-14 of the gene, scattere dt h roughout the genome. These genefragment copies can present problemswhen analysing C H E K 2 for germ l i n emutations in genomic DNA, and it isimportant to ensure that the correct copyis being amplified {2742}. This problemcan be overcome by amplifying exons10-14 by the use of a long range PCRusing primers located in the non-dupli-cated region of the gene {2741}. Theindividual exons can then be subse-quently amplified using the product ofthe long range PCR as a template.
Gene expressionCHEK2 is expressed in nonpro l i f e r a t i n gand terminally diff e rentiated cells. It is
homogenously expressed in renewing cellpopulations such as epidermis, esopha-gus, rectum, bladder, stomach, intestineand colon, and heterogenously in condi-tionally renewing tissues such as lung,b reast kidney, salivary, thyroid, parathy-roid, adrenal glands, pancreas, pro s t a t e ,epididymis, sweat glands, endometruim,s t romal mesenchymal cells, blood ves-sels, lymphoid tissues, smooth and car-diac muscle tissues and pre i p h e r a lnerves. It is absent or cytoplasmic in stat-ic tissues such as muscle and brain.CHEK2 remains expressed and can beactivated in all phases of the cell cycle inresponse to DNA damage {1714}.
Gene functionHuman CHEK2 is a homolog of the yeastG2-checkpoint kinases C D S 1 a n dRAD53 {1791}. In response to DNA dam-age, CHEK2 propagates the checkpointsignal along several pathways, whicheventually causes cell-cycle arrest in G1,S and G2/M phases {449,820}; activationof DNA repair {1609}, and in apoptoticcell death {1315}. Four of the down-s t ream checkpoint effectors that areestablished as substrates of CHEK2 invivo include p53, BRCA1 and Cdc25Aand Cdc25C.
Mutation spectrumRecently, heterozygous germline muta-
tions in CHEK2 have been identified inthree of a subset of individuals with thedominantly inherited Li-Fraumeni syn-drome which do not harbour TP53 muta-tions {209}. However, one of these wasfound to be in a pseudogene copy of theCHEK2 gene. Another one appeared tobe neutral polymorphism in the Finnishpopulation. The third was a protein-trun-cating mutation, 1100delC in exon 10,which abolishes the kinase function ofCHEK2. The possibility that this gene isonly contributing to the breast cancercases within LFS families rather than LFSper se has been raised {2740}. The frequency of 1100delC has beenestimated in healthy control populations,and was found to vary between 0.3%and 1.7% {1840,2084,2984}. This wouldalso suggest that the 1100delC is a poly-morphism, rather than a disease-causingmutation. Yet among unselected patientswith breast cancer, its prevalence wasfound to be approximately 1.5-fold high-er than in controls. Significantly elevatedfrequencies were found among patientswith a positive family history and amongpatients with bilateral breast cancer{2984}. The strongest enrichment of1100delC carriers (approximately 5-fold)was found among familial breast cancerpatients in whom the presence of BRCA1or B R C A 2 mutations were excluded{1840,2984}. However, in families withthe 1100delC mutation, it appears to co-segregate poorly with breast cancer. Theresults suggest that CHEK2*1100delC isa low risk breast cancer susceptibilityallele which may make a significant con-tribution to familial clustering of breastcancer, including families with smallernumbers of affected cases. As it isenriched among multiple-case families,but unable to explain all breast cancer infamilies with at least one carrier case, itmay interact with other, as yet unknownbreast cancer susceptibility alleles.
Search for additional LFS genesThe paucity of large LFS kindreds makesclassical linkage methodology difficult. Acandidate approach is there f o re beingused. Candidate genes are those involvedin cell cycle pathways, those commonlymutated in multiple tumour types and theb reast cancer genes, as this site is com-monly affected in LFS kindreds. Usingthese approaches, the genes P 1 6 a n dP T E N {379} have been analysed and nog e rmline mutations found.
Fig. 8.14 Codon distribution of somatic (top) or germline (bottom) TP53 mutations associated with breastcancers. Hotspot mutations are indicated. Mutation at codon 133 has been reported in 5 Li-Fraumeni fami-lies with breast cancers, but is not a frequent site for somatic mutation in breast cancer in the general pop-ulation. Compiled from: IARC TP53 database, www.iarc.fr/p53.
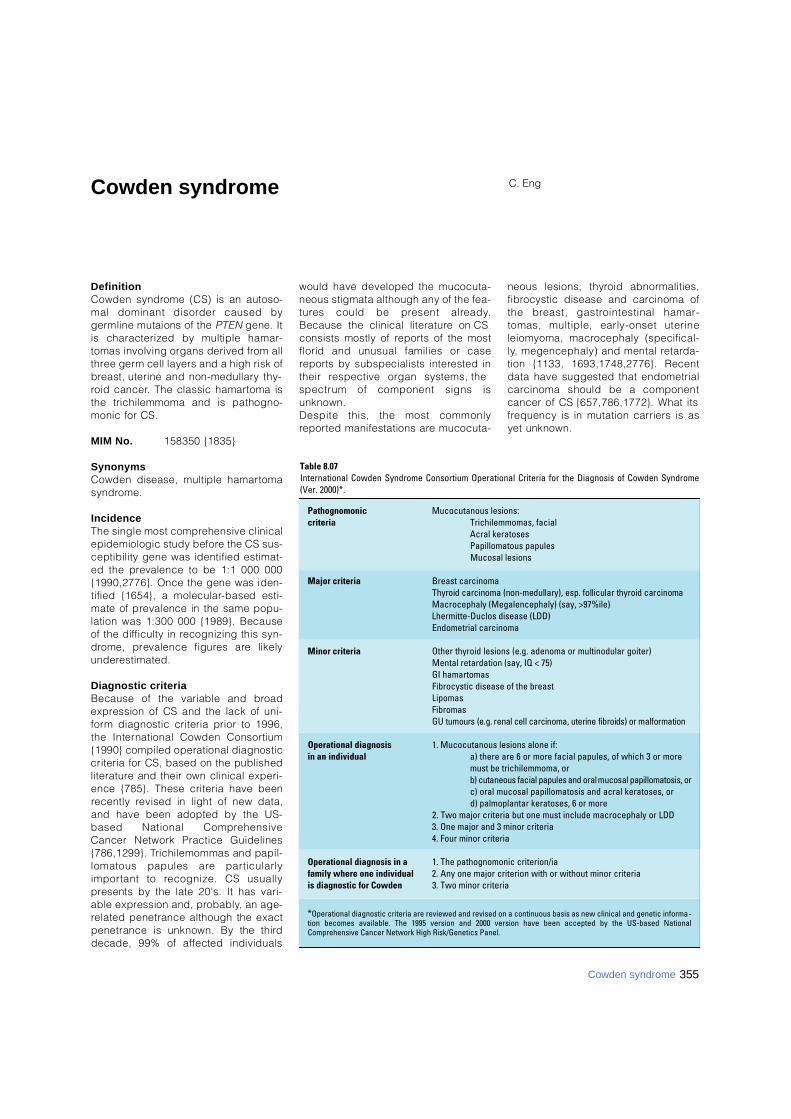
355Cowden syndrome
Cowden syndrome C. Eng
D e f i n i t i o nCowden syndrome (CS) is an autoso-mal dominant disorder caused byg e rmline mutaions of the P T E N gene. Itis characterized by multiple hamar-tomas involving organs derived from allt h ree germ cell layers and a high risk ofb reast, uterine and non-medullary thy-roid cancer. The classic hamartoma isthe trichilemmoma and is pathogno-monic for CS.
MIM No. 158350 {1835}
S y n o n y m sCowden disease, multiple hamart o m as y n d ro m e .
I n c i d e n c eThe single most comprehensive clinicalepidemiologic study before the CS sus-ceptibility gene was identified estimat-ed the prevalence to be 1:1 000 000{1990,2776}. Once the gene was iden-tified {1654}, a molecular-based esti-mate of prevalence in the same popu-lation was 1:300 000 {1989}. Becauseof the difficulty in recognizing this syn-d rome, prevalence figures are likelyu n d e re s t i m a t e d .
Diagnostic criteriaBecause of the variable and bro a de x p ression of CS and the lack of uni-f o rm diagnostic criteria prior to 1996,the International Cowden Consort i u m{1990} compiled operational diagnosticcriteria for CS, based on the publishedl i t e r a t u re and their own clinical experi-ence {785}. These criteria have beenrecently revised in light of new data,and have been adopted by the US-based National Compre h e n s i v eCancer Network Practice Guidelines{786,1299}. Trichilemommas and papil-lomatous papules are part i c u l a r l yi m p o rtant to recognize. CS usuallyp resents by the late 20's. It has vari-able expression and, pro b a b l y, an age-related penetrance although the exactpenetrance is unknown. By the thirddecade, 99% of affected individuals
would have developed the mucocuta-neous stigmata although any of the fea-t u res could be present alre a d y.Because the clinical literature on CSconsists mostly of re p o rts of the mostflorid and unusual families or casere p o rts by subspecialists interested intheir respective organ systems, thespectrum of component signs isunknown. Despite this, the most commonlyre p o rted manifestations are mucocuta-
neous lesions, thyroid abnorm a l i t i e s ,f i b rocystic disease and carcinoma ofthe breast, gastrointestinal hamar-tomas, multiple, early-onset uterineleiomyoma, macrocephaly (specifical-l y, megencephaly) and mental re t a rd a-tion {1133, 1693,1748,2776}. Recentdata have suggested that endometrialc a rcinoma should be a componentcancer of CS {657,786,1772}. What itsf requency is in mutation carriers is asyet unknown.
Table 8.07International Cowden Syndrome Consortium Operational Criteria for the Diagnosis of Cowden Syndrome(Ver. 2000)*.
Pathognomonic Mucocutanous lesions:criteria Trichilemmomas, facial
Acral keratosesPapillomatous papulesMucosal lesions
Major criteria Breast carcinomaThyroid carcinoma (non-medullary), esp. follicular thyroid carcinomaMacrocephaly (Megalencephaly) (say, >97%ile)Lhermitte-Duclos disease (LDD)Endometrial carcinoma
Minor criteria Other thyroid lesions (e.g. adenoma or multinodular goiter)Mental retardation (say, IQ < 75)GI hamartomasFibrocystic disease of the breastLipomasFibromasGU tumours (e.g. renal cell carcinoma, uterine fibroids) or malformation
Operational diagnosis 1. Mucocutanous lesions alone if:in an individual a) there are 6 or more facial papules, of which 3 or more
must be trichilemmoma, orb) cutaneous facial papules and oral mucosal papillomatosis, orc) oral mucosal papillomatosis and acral keratoses, ord) palmoplantar keratoses, 6 or more
2. Two major criteria but one must include macrocephaly or LDD3. One major and 3 minor criteria4. Four minor criteria
Operational diagnosis in a 1. The pathognomonic criterion/iafamily where one individual 2. Any one major criterion with or without minor criteriais diagnostic for Cowden 3. Two minor criteria
*Operational diagnostic criteria are reviewed and revised on a continuous basis as new clinical and genetic informa-tion becomes available. The 1995 version and 2000 version have been accepted by the US-based NationalComprehensive Cancer Network High Risk/Genetics Panel.

Breast tumoursAge distribution and penetranceInvasive carcinomas of the breast havebeen diagnosed as early as the age of14 years and as late as in the 60’s{1693}. However, the majority of CS-related breast cancers occur after theage of 30-35 years {786,788}. A singlepopulation-based clinical study, with-out the benefit of genetic analysis, sug-gested that benign breast disease canoccur in two-thirds of affected womenwhile CS females have a 25-50% life-time risk of developing invasive bre a s tcancer {786,2776}. Male breast cancercan occur in CS as well but the fre-quency is unknown {817,1771}.
Clinical featuresIt is believed that the clinical pre s e n t a-tion of breast cancer in CS is no diff e r-ent from that of the general population.H o w e v e r, no formal data is curre n t l ya v a i l a b l e .
P a t h o l o g yLike other inherited cancer syndro m e s ,multifocality and bilateral involvementis the rule. With re g a rd to the individualcancers, even of the breast and thy-roid, as of mid 1997, there has yet to bea systematic study published. Thereexists, however, one study which hasattempted to look at benign and malig-nant breast pathology in CS patients.Although these are pre l i m i n a ry studies,without true matched controls, it is, todate, the only study that examinesb reast pathology in a series of CScases. Breast histopathology from 59cases belonging to 19 CS women wassystematically analysed {2578}. Thirt y -five specimens had some form ofmalignant pathology. Of these, 31(90%) had ductal adenocarc i n o m a ,one tubular carcinoma and one lobularc a rcinoma-in-situ. Sixteen of the 31had both invasive and in situ (DCIS)components of ductal carcinoma while12 had DCIS only and two only invasivea d e n o c a rcinoma. Intere s t i n g l y, it wasnoted that 19 of these carc i n o m a sa p p e a red to have arisen in the midst ofdensely fibrotic hamartomatous tissue.Benign breast disease is more commonthan malignant, with the form e rbelieved to occur in 75% of aff e c t e dfemales. Fibrocystic disease of theb reast, breast hamartomas, andf i b roadenomas are commonly seen.
Uterine tumoursAge distribution and penetranceSince endometrial carcinomas haveonly recently been suggested to be aminor component of CS {786}, it isunknown what the true frequency isamong mutation carriers or what theage distribution is. Anecdotal casessuggest that the frequency could be 6-10% in affected women.Benign tumours of the uterus are com-mon in CS. Uterine leiomyomas arebelieved to occur in almost half ofa ffected women {1693}. They are usu-ally multi-focal and occur at a youngage, even in the 20’s. Other benignuterine pathologies such as polyps andhyperplasias have been found in CSpatients but are of unknown fre q u e n c y.
Clinical featuresT h e re have been no systematic studiesof uterine tumours in CS. Clinical obser-vation and anecdotal re p o rts suggestthat the leiomyomas can become quitesymptomatic, presenting with bleedingand pain. It is unclear if the clinicalp resentation of the endometrial carc i n o-mas is diff e rent from that of sporadicc a s e s .
P a t h o l o g yT h e re have been no systematic studiesof uterine tumours in CS although it isbelieved that the histopathology is nod i ff e rent from that of typical sporadicc a s e s .
Prognosis and prognostic factorsWhether the prognosis differs from spo-radic cases is unknown.
Thyroid tumoursAge of distribution and penetranceA p a rt from breast cancer, the othermajor component cancer in CS is non-m e d u l l a ry thyroid cancer. Nonmedullaryt h y roid carcinomas occur at a fre q u e n c yof 3-10% of affected individuals, re g a rd-less of sex, in non-systematic clinicalseries {1693,2776}. It is unclear, howev-e r, whether the age of onset is earlierthan that of sporadic cases.Benign thyroid disease occurs ina p p roximately 70% of affected individu-als. Component features include multin-odular goitre and follicular adenomas.These benign tumours can occur at anyage and can even manifest in teen-a g e r s .
Clinical featuresMany of the benign tumours in CS indi-viduals remain asymptomatic. However,the most common presenting sign orsymptom would be a neck mass. Likemany inherited syndromes, CS thyro i dlesions can be multifocal and bilobar.
P a t h o l o g yNo systematic studies have been per-f o rmed to examine the thyroid in CS.H o w e v e r, clinical observations and clin-ical re p o rts suggest that the histology ofthe nonmedullary thyroid carcinoma isp redominantly of the follicular type {786,2 7 7 6 } .
Other tumoursDysplastic gangliocytoma of the cere-bellum (Lhermitte-Duclos disease) is themajor manifestation in the central nerv-ous system. Peripheral lesions includeverrucous skin changes, cobblestone-like papules, fibromas of the oralmucosa, multiple facial trichilemmomasand hamartomatous polyps of the colon.
G e n e t i c sChromosomal location and mode oft r a n s m i s s i o nCS is an autosomal dominant disord e r,with age related penetrance and vari-able expression {787}. The CS suscepti-bility gene, P T E N, resides on 10q23.3{1651, 1654,1990}.
Gene structureP T E N / M M A C 1 / T E P 1 is comprised of 9exons spanning 120-150 kb of genomicdistance {1649,1651,1654,2777}. It isbelieved that intron 1 occupies much ofthis (approximately 100 kb). P T E Nencodes a transcript of 1.2 kb.
Gene expressionP T E N is expressed almost ubiquitouslyin the adult human. In normal humane m b ryonic and foetal development,PTEN protein is expressed ubiquitouslyas well, although levels might changet h roughout development {1008}. P T E Nis very highly expressed in the develop-ing central nervous system as well asneural crest and its derivatives, e.g.enteric ganglia {1008}.
Gene functionPTEN encodes a dual specificity lipidand protein phosphatase [reviewed in{3043}]. It is the major 3-phosphatase
356 Inherited tumour syndromes

acting in the phosphoinositol-3-kinase(PI3K)/Akt apoptotic pathway {1730,2774}. To date, virtually all naturallyoccurring missense mutations testeda b rogate both lipid and protein phos-phatase activity, and one mutant,G129E, affects only lipid phosphataseactivity [reviewed in {3043}]. Over-e x p ression of PTEN results, for the mostp a rt, in phosphatase-dependent cellcycle arrest at G1 and/or apoptosis,depending on cell type [reviewed in{3043}]. There is also growing evidencethat PTEN can mediate growth arre s tindependent of the PI3K/Akt pathwayand perhaps independent of the lipidphosphatase activity {3096-3098}[ reviewed in {3042}].Murine models null for Pten result inearly embryonic death {688,2268,2817}.Hemizygous knock-out of Pten result invarious neoplasias, and the spectra ared i ff e rent depending on the part i c u l a rmodel. While the neoplasias are re m i n i s-cent of the component tumours found inthe human syndrome, none of the thre emodels are similar to CS.
Mutation spectrumAs with most other tumour suppre s s o rgenes, the mutations found in P T E N a res c a t t e red throughout all 9 exons. Theycomprise loss-of-function mutationsincluding missense, nonsense,frameshift and splice site mutations{309, 1771}. Approximately 30-40% ofg e rmline P T E N mutations are found inexon 5, although exon 5 re p resents 20%of the coding sequence. Furt h e r,a p p roximately 65% of all mutations can
be found in one of exons 5, 7 or 8 {309,1 7 7 1 } .Although P T E N is the major susceptibli-ty gene for CS, one CS family, withoutP T E N mutations, was found to have ag e rmline mutation in B M P R 1 A, which isone of the susceptibility genes for juve-nile polyposis syndrome {1250,3262}.Whether B M P R 1 A is a minor CS sus-ceptiblity gene or whether this familywith CS features actually has occultjuvenile polyposis is as yet unknown.
Genotype-phenotype correlationsA p p roximately 70-80% of CS cases, asstrictly defined by the Consortium cri-tieria, have a germline P T E N m u t a t i o n{1654,1771}. If the diagnostic criteriaa re relaxed, then mutation fre q u e n c i e sd rop to 10-50% {1723,1991,2959}. Af o rmal study which ascertained 64 unre-lated CS-like cases revealed a mutationf requency of 2% if the criteria are notmet, even if the diagnosis is made shortof one criterion {1772}.A single re s e a rch centre study involving37 unrelated CS families, ascert a i n e da c c o rding to the strict diagnostic criteriaof the Consortium, revealed a mutationf requency of 80% {1771}. Exploratorygenotype-phenotype analyses re v e a l e dthat the presence of a germline mutationwas associated with a familial risk ofdeveloping malignant breast disease{1771}. Furt h e r, missense mutationsand/or mutations 5’ of the phosphatasec o re motif seem to be associated with as u r rogate for disease severity (multi-organ involvement). One other smallstudy comprising 13 families, with 8
P T E N mutation positive, could not findany genotype-phenotype associations{1989}. However, it should be noted thatthis small sample size is not suitable forstatistical analyses and no conclusionsshould be drawn.P reviously thought to be clinically dis-tinct, Bannayan-Riley-Ruvalcaba syn-d rome (BRR, MIM 153480), which ischaracterized by macro c e p h a l y, lipo-matosis, haemangiomatosis and speck-led penis, is likely allelic to CS {1773}.A p p roximately 60% of BRR families andisolated cases combined carry ag e rmline P T E N mutation {1774}. Intere s -t i n g l y, there were 11 cases classified astrue CS-BRR overlap families in thisc o h o rt, and 10 of the 11 had a PTENmutation. The overlapping mutationspectrum, the existence of true overlapfamilies and the genotype-phenotypeassociations which suggest that thep resence of germline P T E N mutation isassociated with cancer strongly suggestthat CS and BRR are allelic and arealong a single spectrum at the molecu-lar level. The aggregate term of PTENh a m a rtoma tumour syndrome (PHTS)has been suggested {1774}.R e c e n t l y, the clinical spectrum of PHTShas expanded to include subsets ofP roteus syndrome and Pro t e u s - l i k e(non-CS, non-BRR) syndromes {3260}.G e rmline P T E N mutations in one case ofm a c rocephaly and autism and hydro-cephaly associated with VATER associa-tion have been re p o rted {625,2341}.
357Cowden syndrome
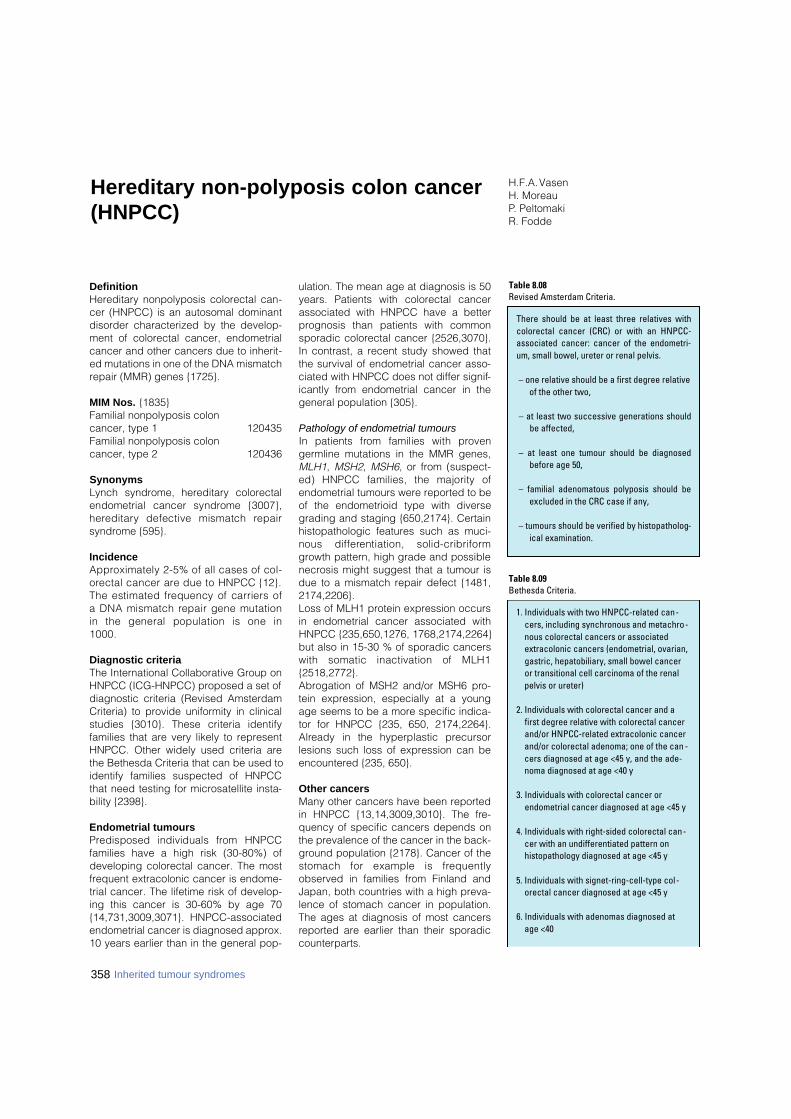
DefinitionHereditary nonpolyposis colorectal can-cer (HNPCC) is an autosomal dominantdisorder characterized by the develop-ment of colorectal cancer, endometrialcancer and other cancers due to inherit-ed mutations in one of the DNA mismatchrepair (MMR) genes {1725}.
MIM Nos. {1835}Familial nonpolyposis colon cancer, type 1 120435Familial nonpolyposis colon cancer, type 2 120436
SynonymsLynch syndrome, hereditary colorectalendometrial cancer syndrome {3007},h e re d i t a ry defective mismatch re p a i rsyndrome {595}.
IncidenceA p p roximately 2-5% of all cases of col-o rectal cancer are due to HNPCC {12}.The estimated frequency of carriers ofa DNA mismatch repair gene mutationin the general population is one in1000.
Diagnostic criteriaThe International Collaborative Group onHNPCC (ICG-HNPCC) proposed a set ofdiagnostic criteria (Revised AmsterdamCriteria) to provide uniformity in clinicalstudies {3010}. These criteria identifyfamilies that are very likely to representHNPCC. Other widely used criteria arethe Bethesda Criteria that can be used toidentify families suspected of HNPCCthat need testing for microsatellite insta-bility {2398}.
Endometrial tumoursP redisposed individuals from HNPCCfamilies have a high risk (30-80%) ofdeveloping colorectal cancer. The mostfrequent extracolonic cancer is endome-trial cancer. The lifetime risk of develop-ing this cancer is 30-60% by age 70 {14,731,3009,3071}. HNPCC-associatedendometrial cancer is diagnosed approx.10 years earlier than in the general pop-
ulation. The mean age at diagnosis is 50years. Patients with colorectal cancerassociated with HNPCC have a betterprognosis than patients with commonsporadic colorectal cancer {2526,3070}.In contrast, a recent study showed thatthe survival of endometrial cancer asso-ciated with HNPCC does not differ signif-icantly from endometrial cancer in thegeneral population {305}.
Pathology of endometrial tumoursIn patients from families with pro v e ngermline mutations in the MMR genes,MLH1, MSH2, MSH6, or from (suspect-ed) HNPCC families, the majority ofendometrial tumours were reported to beof the endometrioid type with diversegrading and staging {650,2174}. Certainhistopathologic features such as muci-nous diff e rentiation, solid-cribriformgrowth pattern, high grade and possiblenecrosis might suggest that a tumour isdue to a mismatch repair defect {1481,2174,2206}. Loss of MLH1 protein expression occursin endometrial cancer associated withHNPCC {235,650,1276, 1768,2174,2264}but also in 15-30 % of sporadic cancerswith somatic inactivation of MLH1{2518,2772}. Abrogation of MSH2 and/or MSH6 pro-tein expression, especially at a youngage seems to be a more specific indica-tor for HNPCC {235, 650, 2174,2264}.A l ready in the hyperplastic pre c u r s o rlesions such loss of expression can beencountered {235, 650}.
Other cancersMany other cancers have been reportedin HNPCC {13,14,3009,3010}. The fre-quency of specific cancers depends onthe prevalence of the cancer in the back-ground population {2178}. Cancer of thestomach for example is fre q u e n t l yobserved in families from Finland andJapan, both countries with a high preva-lence of stomach cancer in population.The ages at diagnosis of most cancersreported are earlier than their sporadiccounterparts.
358 Inherited tumour syndromes
H.F.A. VasenH. Moreau P. PeltomakiR. Fodde
Hereditary non-polyposis colon cancer(HNPCC)
1. Individuals with two HNPCC-related can-cers, including synchronous and metachro-nous colorectal cancers or associatedextracolonic cancers (endometrial, ovarian,gastric, hepatobiliary, small bowel canceror transitional cell carcinoma of the renalpelvis or ureter)
2. Individuals with colorectal cancer and afirst degree relative with colorectal cancerand/or HNPCC-related extracolonic cancerand/or colorectal adenoma; one of the can -cers diagnosed at age <45 y, and the ade-noma diagnosed at age <40 y
3. Individuals with colorectal cancer orendometrial cancer diagnosed at age <45 y
4. Individuals with right-sided colorectal can-cer with an undifferentiated pattern onhistopathology diagnosed at age <45 y
5. Individuals with signet-ring-cell-type col-orectal cancer diagnosed at age <45 y
6. Individuals with adenomas diagnosed atage <40
Table 8.09Bethesda Criteria.
There should be at least three relatives withcolorectal cancer (CRC) or with an HNPCC-associated cancer: cancer of the endometri-um, small bowel, ureter or renal pelvis.
– one relative should be a first degree relativeof the other two,
– at least two successive generations shouldbe affected,
– at least one tumour should be diagnosedbefore age 50,
– familial adenomatous polyposis should beexcluded in the CRC case if any,
– tumours should be verified by histopatholog-ical examination.
Table 8.08Revised Amsterdam Criteria.
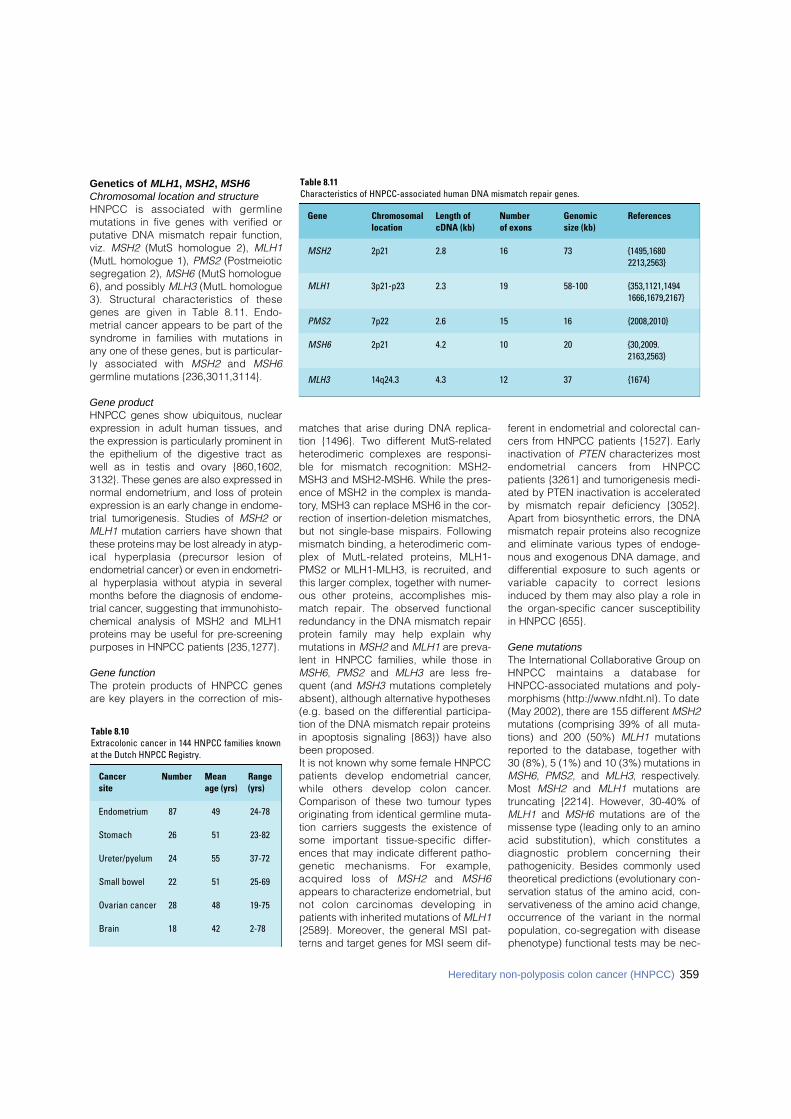
Genetics of MLH1, MSH2, MSH6Chromosomal location and structure HNPCC is associated with germ l i n emutations in five genes with verified orputative DNA mismatch repair function,viz. MSH2 (MutS homologue 2), MLH1(MutL homologue 1), PMS2 (Postmeioticsegregation 2), MSH6 (MutS homologue6), and possibly MLH3 (MutL homologue3). Structural characteristics of thesegenes are given in Table 8.11. Endo-metrial cancer appears to be part of thesyndrome in families with mutations inany one of these genes, but is particular-ly associated with M S H 2 and M S H 6germline mutations {236,3011,3114}.
Gene productHNPCC genes show ubiquitous, nucleare x p ression in adult human tissues, andthe expression is particularly prominent inthe epithelium of the digestive tract aswell as in testis and ovary {860,1602,3132}. These genes are also expressed inn o rmal endometrium, and loss of pro t e i ne x p ression is an early change in endome-trial tumorigenesis. Studies of M S H 2 o rM L H 1 mutation carriers have shown thatthese proteins may be lost already in atyp-ical hyperplasia (precursor lesion ofendometrial cancer) or even in endometri-al hyperplasia without atypia in severalmonths before the diagnosis of endome-trial cancer, suggesting that immunohisto-chemical analysis of MSH2 and MLH1p roteins may be useful for pre - s c re e n i n gpurposes in HNPCC patients {235,1277}.
Gene functionThe protein products of HNPCC genesare key players in the correction of mis-
matches that arise during DNA replica-tion {1496}. Two different MutS-relatedheterodimeric complexes are responsi-ble for mismatch recognition: MSH2-MSH3 and MSH2-MSH6. While the pres-ence of MSH2 in the complex is manda-tory, MSH3 can replace MSH6 in the cor-rection of insertion-deletion mismatches,but not single-base mispairs. Followingmismatch binding, a heterodimeric com-plex of MutL-related proteins, MLH1-PMS2 or MLH1-MLH3, is recruited, andthis larger complex, together with numer-ous other proteins, accomplishes mis-match repair. The observed functionalredundancy in the DNA mismatch repairp rotein family may help explain whymutations in MSH2 and MLH1 are preva-lent in HNPCC families, while those inMSH6, PMS2 and MLH3 are less fre-quent (and MSH3 mutations completelyabsent), although alternative hypotheses(e.g. based on the differential participa-tion of the DNA mismatch repair proteinsin apoptosis signaling {863}) have alsobeen proposed.It is not known why some female HNPCCpatients develop endometrial cancer,while others develop colon cancer.Comparison of these two tumour typesoriginating from identical germline muta-tion carriers suggests the existence ofsome important tissue-specific diff e r-ences that may indicate different patho-genetic mechanisms. For example,a c q u i red loss of M S H 2 and M S H 6appears to characterize endometrial, butnot colon carcinomas developing inpatients with inherited mutations of MLH1{2589}. Moreover, the general MSI pat-terns and target genes for MSI seem dif-
ferent in endometrial and colorectal can-cers from HNPCC patients {1527}. Earlyinactivation of PTEN characterizes mostendometrial cancers from HNPCCpatients {3261} and tumorigenesis medi-ated by PTEN inactivation is acceleratedby mismatch repair deficiency {3052}.Apart from biosynthetic errors, the DNAmismatch repair proteins also recognizeand eliminate various types of endoge-nous and exogenous DNA damage, anddifferential exposure to such agents orvariable capacity to correct lesionsinduced by them may also play a role inthe organ-specific cancer susceptibilityin HNPCC {655}.
Gene mutationsThe International Collaborative Group onHNPCC maintains a database forHNPCC-associated mutations and poly-morphisms (http://www.nfdht.nl). To date(May 2002), there are 155 different MSH2mutations (comprising 39% of all muta-tions) and 200 (50%) MLH1 mutationsreported to the database, together with30 (8%), 5 (1%) and 10 (3%) mutations inMSH6, PMS2, and MLH3, respectively.Most MSH2 and MLH1 mutations aretruncating {2214}. However, 30-40% ofMLH1 and MSH6 mutations are of themissense type (leading only to an aminoacid substitution), which constitutes adiagnostic problem concerning theirpathogenicity. Besides commonly usedtheoretical predictions (evolutionary con-servation status of the amino acid, con-servativeness of the amino acid change,occurrence of the variant in the normalpopulation, co-segregation with diseasephenotype) functional tests may be nec-
359Hereditary non-polyposis colon cancer (HNPCC)
Table 8.10Extracolonic cancer in 144 HNPCC families knownat the Dutch HNPCC Registry.
Cancer Number Mean Range site age (yrs) (yrs)
Endometrium 87 49 24-78
Stomach 26 51 23-82
Ureter/pyelum 24 55 37-72
Small bowel 22 51 25-69
Ovarian cancer 28 48 19-75
Brain 18 42 2-78
Table 8.11Characteristics of HNPCC-associated human DNA mismatch repair genes.
Gene Chromosomal Length of Number Genomic Referenceslocation cDNA (kb) of exons size (kb)
MSH2 2p21 2.8 16 73 {1495,16802213,2563}
MLH1 3p21-p23 2.3 19 58-100 {353,1121,14941666,1679,2167}
PMS2 7p22 2.6 15 16 {2008,2010}
MSH6 2p21 4.2 10 20 {30,2009. 2163,2563}
MLH3 14q24.3 4.3 12 37 {1674}

essary in the evaluation of the patho-genicity of missense changes.
Microsatellite instability Microsatellite instability (MSI) is the hall-mark of tumours that arise in carriers ofM L H 1, M S H 2, of M S H 6 m u t a t i o n s .Overall, MSI is detected in approximate-ly 15% of all colorectal cancers. It ismeasured as alterations in the length ofsimple repetitive genomic sequences,usually dinucleotide repeats, or mononu-cleotide runs. As these repeats have atendency to form mismatches duringDNA replication, a mismatch re p a i rdefect is expected to increase theirmutation frequency. Because the defini-tion of instability applied has been vari-able, in 1998 an international workingg roup recommended the use of fivemarkers to assess MSI {306}. Tumoursa re characterized as having high-fre-quency MSI (MSI-H) if two or more of thefive markers show instability (i.e. haveinsertion/deletion mutations), or as hav-ing low-frequency MSI (MSI-L) if only oneof the five markers shows instability. Thedistinction between microsatellite stable(MSS) and low frequency MSI (MSI-L)can only be accomplished if a greaternumber of markers is utilized. MSI analy-sis, in conjunction with immunohisto-chemistry, can greatly improve the effica-cy of the molecular screening for HNPCC{650,2516}.In one study, all 12 endometrial carcino-mas from carriers of MLH1 and MSH2g e rmline mutations demonstrated anMSI-high phenotype involving all types ofrepeat markers, while this was found inonly 4 out of 11 (36%) endometrial carci -nomas from M S H 6 mutation carriers{650}. In another study, MSI-patterns inendometrial cancers differed from thosein colorectal cancers, even though thepatients had identical pre d i s p o s i n gmutations in the MMR genes MLH1 orMSH2 {1527}. In endometrial cancers,the pattern was more heterogeneous andinvolved a lower proportion of unstablemarkers per tumour and shorter allelicshifts for BAT markers. These resultsmight point to gene-specific and/ororgan-specific differences that may beimportant determinants of the HNPCCtumour spectrum.
Mutation spectrum Hereditary non polyposis colorectal can-cer (HNPCC) is caused by germ l i n e
mutations in one of 5 DNA mismatchrepair genes (MMR): MSH2 {864}, MLH1{353}, PMS1 {2010}, PMS2 {2010}, andMSH6 (formerly GTBP) {53,1884}. Othergenes like E X O 1 {3161}, M L H 3{1674,3162} and TGFbRII {1705} havebeen re p o rted to possibly causeHNPCC-like syndromes, although nodefinitive evidence has been deliveredyet, both in terms of pathogenicity and/orcosegregation with the disease of thealleged germline mutations in affectedfamilies. To date, more than 300 different predis-posing mutations have been identified,most in MSH2 and MLH1 and in familiescomplying with the clinical Amsterdamcriteria (AMS+) {2214}. Many HNPCCfamilies, however, do not fully complywith these criteria, and in most of thesecases the disease-causing mutations areyet unknown. Mutations in MSH6 havebeen found in atypical HNPCC families(see below).In general, MMR mutations are scatteredalong the coding sequence of MSH2 andMLH1 and predict either the truncation ofthe corresponding protein products, or asubtler amino acid substitutions. Thesemutations appear evenly distributedthroughout the coding regions of themain MMR genes, with some clusteringin MSH2 exon 12 {2214} and MLH1 exon16 {3115}. While most of the MSH2 muta-tions consist of frameshift or nonsensechanges, MLH1 is mainly affected byframeshift or missense alterations. Mostof the mutations found to date areunique, with a few common recurringones {2214}. Genomic deletions havealso been found at both loci {442,2070,3116}. MSH2 deletions appear to be avery frequent cause of HNPCC, con-tributing for up to a quarter of the familiesselected by Amsterdam criteria {3116}.MLH1 deletions are less frequent than inM S H 2 {1793,2070}. Southern analysisand/or other PCR-based methods todetect larger rearrangements at thegenomic level {443} should be routinelyemployed when approaching the muta-tion analyses of these major mismatchrepair genes.
Genotype-phenotype correlationsThe combination of clinical (number andtype of tumours, age of onset, clinicalcourse of the disease, etc.) and genetic(different mismatch repair genes, trun-cating and missense mutations) hetero-
geneity in HNPCC represents an idealopportunity to attempt the establishmentof genotype-phenotype corre l a t i o n s .Unfortunately, and notwithstanding thelarge number of mutations and clinicaldata collected to date, no clear-cut cor-relations have been observed betweenspecific MMR gene mutations and theirclinical outcome. For example, the iden-tification of identical mutations both inHNPCC and in Muir-Torre or Turcot syn-drome does not support the existence ofconsistent genotype-phenotype correla-tions {179,1115,1494}. The most reliable correlation found todate is the association between clear-cutpathogenic mutations at MSH2, MLH1and MSH6, and the resulting spectrum ofc o l o rectal and extracolonic tumours.HNPCC kindreds due to MSH2 or MLH1germline mutations are characterized byhigh penetrance and early onset of col-o rectal and endometrial cancer. Thediagnostic criteria, Amsterdam I and II,established by the Intern a t i o n a lCollaborative Group on HNPCC {3008,3010} well serve the purpose of selectingfamilies with a high likelihood to carryMSH2 and MLH1 mutations {3117}. Inaddition to the fulfillment of the above cri-teria, other factors represent valid pre-dictors of the presence of germ l i n eMSH2 and MLH1 mutations in HNPCCfamilies. These include 1. young age atdiagnosis of colorectal cancer, and 2. theoccurrence of at least one patient with anextra-colonic cancer, such as those ofthe endometrium, small intestine, brain,and stomach, within an AMS+ HNPCCk i n d red. The frequency of mutationsidentified in these families increased toabout 70% {3117}. Moreover, the occur-rence of at least one patient with multiplesynchronous or metachronous colorectalcancers, and the combined occurrenceof colorectal cancer with endometrialcancer in one patient are very good pre-dictors of M S H 2 or M L H 1 m u t a t i o n s{3117}.The first reports on MSH6 germline muta-tions already indicated that the clinicalphenotype differed from the "classical"HNPCC caused by MSH2 and MLH1mutations {53,1884}. More re c e n t l y,M S H 6 g e rmline mutations have beendemonstrated in a considerable numberof the atypical HNPCC families, i.e. notcomplying with the Amsterdam criteria(ACI and II) {1497,3039,3114,3160}. Ingeneral, the penetrance of colore c t a l
360 Inherited tumour syndromes

cancer seemed to be reduced whileendometrial cancer seems to represent am o re important clinical manifestationamong female MSH6 mutation carriers.Also, the mean age of onset of colorectaland endometrial cancer appeared to bedelayed in families with MSH6 germlinemutations {3011,3039,3114}. Notably,
MSI analysis of tumours from M S H 6mutation carriers suggests a reducedpenetrance of the MSI-H phenotype andpreferential instability at mononucleotiderepeats {650,1497,3114,3160}.An additional MSH6-associated clinicalphenotype is the papillary transitionalcell carcinoma of the ureter and renal
pelvis, observed in approx. 10% of thecarriers from an extended MSH6 kindred{3039}. Notably, the lifetime cumulativerisk of this tumour type in MLH1 or MSH2mutation carriers is only 2.6% {2673}.
361Hereditary non-polyposis colon cancer (HNPCC)
DefinitionAtaxia telangiectasia syndrome (A-T) is arare, progressive neurological disorderthat manifests at the toddler stage. Thedisease is characterized by cerebellardegeneration (ataxia), dilated blood ves-sels in the eyes and skin (telangiectasia),immunodeficiency, chromosomal insta-b i l i t y, increased sensitivity to ionizingradiation and a predisposition to cancer,in particular leukaemias and lymphomas.Germline mutations in the ATM gene(ataxia telangiectasia mutated), homozy-gous or compound heterozygous, arethe cause of this autosomal recessivedisorder. Heterozygous carriers are phe-notypically unaffected but exhibit anincreased risk to develop breast cancerand often display a variety of age relateddisorders which may result in reducedlife expectancy {2808}.
MIM No. 208900 {1835}
Synonyms Louis-Bar Syndrome, A-T complementa-tion group A (ATA), group C (ATC), groupD (ATD) and group E (ATE). The differentcomplementation groups are all linked tothe ATM gene.
Incidence The rare A-T disease occurs in both gen-ders and world wide among all races. Thedisease has an estimated incidence of oneper 40,000 to one per 300,000 live birt h s .
A p p roximately 0.2-1% of the general pop-ulation has been estimated to be hetero z y-gous carriers of a type of germline muta-tion in the AT M gene that in homozygousstate causes the A-T syndro m e .
Tumours in A-T patients Individuals with A-T have a 50 to 150 foldexcess risk of cancer, with approximate-ly 70% being lymphomas and T cellleukaemias. In younger patients, anacute lymphoblastic leukaemia is mostoften of T-cell origin, although the pre-Bcommon ALL of childhood has also beenseen in A-T patients. When leukaemiadevelops in older A-T patients it is usual-ly an aggressive T-cell leukaemia (T-PLL,T cell prolymphocytic leukaemia).Lymphomas are usually B cell types. Awide range of solid tumours makes upthe remainder of the tumours seen in A-Tpatients and includes cancers of thebreast, stomach, ovary and melanoma. The presence of missense mutations inA-T patients has been associated with amilder clinical phenotype and alteredcancer predisposition. In two British A-Tfamilies a T>G tranversion at base pair7271 was found to be associated with amilder clinical phenotype, lowerradiosensitivity but an increased risk ofbreast cancer. This increased risk wasobserved in both the homozygote andheterozygotes carriers of this modifica-tion (RR 12.7 p=0.0025) {2775}. Thissequence alteration has subsequently
been found in multiple-case breast can-cer families. The expression and activityanalyses of the ATM protein in heterozy-gous cell lines carrying this sequencechange indicated that this mutation wasdominant negative {462}.
Breast cancer in ATM heterozygotes Heterozygous carriers of ATM mutationshave a higher mortality rate and an earli -er age at death from cancer andischemic heart disease than non-carriers{2808}. A-T heterozygotes have beenreported to have a 3 to 8 fold increasedrisk of breast cancer. The associationbetween ATM heterozygosity and breastcancer risk was initially found amongblood relatives of A-T patients {2820},and in almost every study of A-T relativessince an increased breast cancer riskhas been detected {318,741,981,1291,1334,2105,2257,2819}. Paradoxically, inthe years following the cloning of theATM gene {2546}, several studies inves-tigating large breast cancer cohort sfailed to find an increased incidence ofATM mutations of the type found in A-Tpatients, and a controversy aro s eregarding the role of ATM in breast can -cer susceptibility {194,281,884}.However, a number of recent studies,analysing the frequency of all type ofAT M mutations, did confirm pre v i o u sfindings of an elevated breast cancerrisk in ATM mutation carriers {129,351,462,2592,2775}.
A. Broeks L.J. van’t Veer A.L. Borresen-DaleJ. Hall
Ataxia telangiectasia syndrome

Age distribution and penetranceMost of the studies finding an incre a s e drisk of breast cancer in A-T relatives pointto an early onset of the disease. The pen-etrance has been difficult to estimatesince most of the studies are small, andd i ff e rent mutations may have diff e re n te ffects. In several studies of A-T re l a t i v e s ,the elevated risk is restricted to obligatecarriers (mothers), and is not increased inother relatives according to their pro b a-bility of being a mutation carrier. This maypoint to an interaction with enviro n m e n t a land/or other genetic factors contributingto the elevated breast cancer risk.
Clinical and pathological features No typical clinical or pathological fea-tures are so far known for ATM heterozy-gous breast cancer patients, other thanearly age at onset (before age 50) andfrequent bilateral occurrence {351}.
Response to therapy and prognosisATM heterozygotes with breast cancerdo not seem to exhibit acute radiationsensitivity as A-T patients do, and exces-sive toxicity has not been observed afterradiotherapy {115,2331,3088}. It hashowever been speculated whether ATMh e t e rozygous breast cancer patientshave an increased risk of developing asecond breast cancer after radiationtreatment, and large multi-center studiesare ongoing to answer this question.There are only few studies evaluating theprognosis of A-T carriers with breastcancer, pointing to a long-term survival.This may be due to their tumours beingmore susceptible to cell killing by ioniz-ing radiation than tumour cells in non-carriers {2809}.
ATM expression in breast cancerNormal breast tissue shows a distinctpattern of ATM expression, the proteinbeing found in the nucleus of the ductalepithelial cells and to a lesser extent inthe surrounding myoepithelial cells.D e c reased ATM expression is oftenobserved in breast carcinomas {102,1384} and ATM mRNA levels have alsobeen found to be lower in invasive breastcarcinomas than in normal tissues orbenign lesions {3041}.Significant loss of heterozygosity in spo-radic breast tumours across chro m o-some 11q22-23 where the ATM gene islocated has been reported {1118,1439,1553,1754,2375}.
GeneticsChromosomal locationThe ATM gene is located on human chro-mosome 11q22-23.
Gene structureThe ATM gene has 66 exons scanning150 kilobase of genomic DNA and isexpressed in a wide range of tissues asan approximately 12-kilobase messen-ger RNA encoding a 350 kD serine/thre-onine protein kinase. The initiation codonfalls within exon 4. The last exon is 3.8kband contains the stop codon and a 3’-untranslated region of about 3600nucleotides {2983}.
Gene expressionThe major 13 kb AT M transcript isobserved in every tissue tested to date.N o rt h e rn blots and RT-PCR pro d u c t sfrom various tissues failed to discloseany evidence of alternative forms withinthe coding region. However the first fourexons, which fall within the 5’-untranslat-ed region (UTR), undergo extensivea l t e rnative splicing. Diff e rential poly-adenylation results in 3’UTRs of varyinglengths. These structural features sug-gest that ATM expression might be sub-ject to complex post-transcriptional regu-lation {2547}.
Gene functionThe ATM protein plays a central role insensing and signalling the presence ofDNA double-strand breaks (DSBs)f o rmed in cells as a result of normal DNAmetabolism (e.g. meiotic or V(D)J re c o m-bination) or damage caused by extern a lagents. The kinase domain in the car-b o x y - t e rminal region of the protein con-tains the signature motifs of phos-
phatidylinositol 3-kinases. AT M ’s kinaseactivity is itself enhanced in response toDNA double-strand breaks resulting in ap h o s p h o rylation cascade activatingmany proteins each of which in turna ffects a specific signalling pathway.These substrates include the pro t e i np roducts of a number of well character-ized tumour- s u p p ressor genes includingT P 5 3, B R C A 1 and C H E K 2 which playi m p o rtant roles in triggering cell cyclea r rest, DNA repair or apoptosis (re v i e w e din Shiloh et al. {2660}). Additional DSB-induced responses that are ATM depend-ent include the activation of transcriptionfactors such as AP-1, p73 and NFKB, anddeacetylation of chromatin pro t e i n s( reviewed in Barzilai et al. {189}).
Mutation spectrum in A-T patientsSince the AT M gene was cloned {2546}m o re than 300 diff e rent A-T disease-causing mutations have been re p o rt e d .The profile of these has revealed thatmost are unique and uniformly distributedalong the length of the gene, no muta-tional hotspots have been detected. Themajority of A-T patients are compoundh e t e rozygotes having two diff e rent AT Mmutations and patients homozygous forthe same AT M mutation are rare. The pre-dominate type of mutation found in theAT M gene in A-T patients results in a trun-cated and unstable ATM protein. Some A-T patients have a milder phenotype (vari-ant A-T) that may be related to the pre s-ence of missense mutations or mutationsp roducing an ATM protein retaining somen o rmal function {1825,2592}.
Genotype-phenotype correlationsGatti et al. {971}, in distinguishingbetween truncating mutations where no
362 Inherited tumour syndromes
Table 8.12Proposed ATM genotype / phenotype relationships {971}.
Genotype Phenotype
ATM wt/wt Normal
ATM trun/trun Ataxia telangiectasia, High cancer risk
ATM trun/mis Ataxia telangiectasia, Variant A-T?, High cancer risk?
ATM mis/mis Ataxia telangiectasia? Variant A-T?, High cancer risk?
ATM trun/wt A-T relatives, Elevated breast cancer risk, Increased age related disorders?
ATM mis/wt Few A-T relatives, Moderate breast cancer risk? Increased age related disorders?

363Ataxia telangiectasia syndrome
ATM protein is detected and missensesubstitutions where mutant protein ofvariable stability is observed, have sug-gested that this mutant protein could pro-duce a dominant negative effect in het-erozygotes, resulting in an altered phe-notype and an increased breast cancersusceptibility. The expected phenotypesthat might arise from having two types ofA-T carriers in the general population areshown in Table 8.12. The genotype ATM trun/trun with two truncat-ing mutations causes the classical A-Tdisorder. The genotype ATMmis/mis with two
missense mutations is also found insome children with the classical form ofthe disease, in particular when these arelocated within the ATM kinase domain(for instance Belzen et al. {2987}, Angeleet al. {101}) but may also be associatedwith a variant A-T phenotype with someneurological features and cancer sus-ceptibility. Two types of ATM heterozy-gotes exist and the phenotypes differ, i.e.those with truncating mutations thatmake no protein and those with missensemutations that make reduced amount orp a rtly defective protein {115,462,971,
1825,2331,2592,2775,2809,3088}, andthese two groups may have differentb reast cancer risks. If this pro p o s e dmodel is correct it necessitates a re-analyses of the epidemiological datastratifying for the two types of heterozy-gotes. The literature to date suggeststhat germline ATM missense mutationsare more frequent than the 0.2-1% fre-quency of A-T causing mutations andhence contribute to a larger fraction ofbreast cancer patients {351,462,2592}.
365Contributors
Contributors
Dr Vera M. ABELER**Department of PathologyThe Norwegian Radium HospitalMontebello 0310 OsloNORWAYTel. +47 22 93 40 00 Fax. +47 22 93 54 [email protected]
Dr Jorge ALBORES-SAAVEDRADepartment of Pathology LSU Health Sciences Center1501 Kings Highway Shreveport, LA 71130U.S.ATel. +1 318 675 7732Fax. +1 318 675 [email protected]
Dr Isabel ALVARADO-CABREROVicente Suárez 42-201Colonia CondesaCP 06140MEXICO, DFTel. +52-56-27-69-00Fax. +52 [email protected]
Dr Erik Søgaard ANDERSENDepartment of Obstetrics andGynaecology, Aalborg HospitalHobrovejDK-9000 AalborgDENMARKTel. +45 9932 1218Fax. +45 9932 [email protected]
Dr Alan ASHWORTHThe Breakthrough Breast Cancer CentreThe Institute of Cancer Research237 Fulham RoadLondon SW3 6JBUNITED KINGDOMTel. +44 207 153 5333Fax. +44 207 153 [email protected]
Dr Jean-Pierre BELLOCQ*Service d'Anatomie Pathologique Hôpitaux Universitaires de StrasbourgAvenue Molière67098 Strasbourg FRANCETel. +33 3 88 12 70 53Fax. +33 3 88 12 70 52j e a n - p i e r r e . b e l l o c q @ c h r u - s t r a s b o u r g . f r
Dr Christine BERGERON**Laboratoire Pasteur-Cerba95066 Cergy Pontoise Cedex 9FRANCETel. +33 1 34 40 21 17Fax. +33 1 34 40 20 [email protected]
Dr Ross S. BERKOWITZBrigham and Women's Hospital Harvard Medical School, 75 Francis St.Boston, MA 02115U.S.ATel. +1 617 732 8843Fax. +1 617 738 [email protected]
Dr Werner BÖCKER*Gerhard Domagk Institute of PathologyUniversity of MünsterDomagkstrasse 17D-48129 MünsterGERMANYTel. +49 251 835 54 40/1Fax. +49 251 835 54 [email protected]
Dr Anne-Lise BØRRESEN-DALE Department of GeneticsInstitute for Cancer ResearchThe Norwegian Radium Hospital0310 OsloNORWAYTel. +47 22 93 44 19Fax. +47 22 93 44 [email protected]
Dr Annegien BROEKSDepartment of Molecular PathologyNetherlands Cancer InstitutePlesmanlaan 1211066 CX AmsterdamTHE NETHERLANDSTel. +31 20 5122754Fax. +31 20 [email protected]
Dr C. Hilary BUCKLEYDepartment of Gynecologic PathologySt Mary’s HospitalManchester M13 0JH UNITED KINGDOMTel. +44 161 445 7132Fax. +44 161 276 [email protected]
Dr Gianni BUSSOLATI*Istituto di Anatomia e Istologia PatologicaUniversity of TurinVia Santena 7 10126 TorinoITALYTel. +39 011 670 65 05Fax. +39 011 663 52 [email protected]
Dr Rosmarie CADUFFDepartment of PathologyUniversity Hospital USZSchmelzbergstr. 128091 ZürichSWITZERLANDTel. +41 1 255 25 05Fax. +41 1 255 44 [email protected]
Dr Maria-Luisa CARCANGIUDepartment of PathologyNational Cancer InstituteVia G. Venezian 120133 MilanoITALYTel. +39 02 239 02264Fax. +39 02 239 [email protected]
Dr Silvestro CARINELLIDepartment of PathologyIstituti Clinici di PerfezionamentoVia della Commenda 1220122 MilanoITALYTel. +39 02 5799 2415Fax. +39 02 5799 [email protected]
Dr Annie N. CHEUNGDepartment of PathologyQueen Mary HospitalThe University of Hong KongHong KongCHINATel. +852 2855 4876Fax. +852 2872 [email protected]
Dr Anne-Marie CLETON-JANSENDepartment of PathologyLeiden University Medical CentreP.O. Box 9600, L1-Q2300 RC LeidenTHE NETHERLANDSTel. +31 71 5266515Fax. +31 71 5248158 [email protected]
Dr Cees J. CORNELISSEDepartment of PathologyLeiden University Medical CenterAlbinusdreef 2 P.O. Box 96002300 RC LeidenTHE NETHERLANDSTel. +31 71 526 6624Fax. +31 71 524 [email protected]
Dr Christopher P. CRUMDepartment of PathologyBrigham and Women’s Hospital75 Francis StreetBoston MA 02115U.S.ATel. +1 617 732 75 30Fax. +1 617 264 51 [email protected]
Dr Bruno CUTULIDépartement de RadiothérapiePolyclinique de Courlancy38 rue de Courlancy51100 ReimsFRANCETel. +33 3 26 84 02 84 Fax. +33 3 26 84 70 [email protected]
Dr Peter DEVILEE*Departments of Human and ClinicalGenetics and PathologyLeiden University Medical Center2333 AL LeidenTHE NETHERLANDSTel. +31 71 527 6117Fax. +31 71 527 [email protected]
Dr Mojgan DEVOUASSOUX-SHISHEBORAN** Service d’Anatomie et Cytologie Hôpital de la Croix Rousse103, Grande rue de la Croix Rousse69317 Lyon FRANCETel. +33 4 72 07 18 78Fax. +33 4 72 07 18 [email protected]
Dr Manfred DIETEL**Institute of PathologyCharité University HospitalSchumanstrasse 20/2110117 BerlinGERMANYTel. +49 30 4505 36001Fax. +49 30 4505 [email protected]
Dr Stephen DOBBSDepartment of Gynaecological Oncology Belfast City HospitalLisburn RoadBelfast BT9 7ABUNITED KINGDOMTel. +44 28 90 26 38 94 Fax. +44 28 90 26 39 [email protected]
Dr Maria DRIJKONINGEN*Department of PathologyUniversity Hospital St. RafaelCatholic University Leuven3000 LeuvenBELGIUMTel. +32 16 33 66 41Fax. [email protected]
Dr Douglas EASTONCancer Research UKGenetic Epidemiology UnitUniversity of CambridgeCambridge CB1 8RNUNITED KINGDOMTel. +44 122 374 0160Fax. +44 122 374 [email protected]
* One asterisk indicates participation in theEditorial and Consensus Conference on theWHO classification of Tumours of theBreast during January 12-16 in Lyon,France. **Two asterisks indicate participa-tion in the conference on the WHO classifi-cation of Tumours of Female GenitalOrgans during March 16-20, 2002.
366 Contributors
Dr Rosalind EELESTranslational Cancer GeneticsInstitute of Cancer Research and RoyalMarsden NHS TrustSutton, Surrey SM2 5PT UNITED KINGDOMTel. +44 208 661 3642Fax. +44 208 770 [email protected]
Dr Ian O. ELLIS*Department of HistopathologyUniversity of NottinghamCity Hospital, Hucknall RoadNottingham NG5 1PB UNITED KINGDOMTel. +44 115 969 11 69 Ext. 46875Fax. +44 115 962 77 [email protected]
Dr Charis ENGDivision of Human GeneticsDepartment of Internal MedicineThe Ohio State UniversityColumbus, OH 43210U.S.A.Tel. +1 614 292 2347Fax. +1 614 688 [email protected]
Dr Vincenzo EUSEBI*M. Malphighi Department of Pathology Ospedale Bellaria, University of BolognaVia Altura 340139 BolognaITALYTel. +39 051 622 57 50/55 23Fax. +39 051 622 57 [email protected]
Dr Mathias FEHRDepartment of Obstetrics and GynecologyUniversity HospitalFrauenklinikstr. 108091 ZürichSWITZERLANDTel. +41 1 255 57 07Fax. +41 1 255 44 [email protected]
Dr Rosemary A. FISHERDepartment of Cancer MedicineImperial College LondonCharing Cross CampusLondon W6 8RFUNITED KINGDOMTel. +44 20 8846 1413Fax. +44 20 8748 [email protected]
Dr Riccardo FODDEJosephine Nefkens Institue Erasmus University Medical CenterP.O. Box 17383000 DR RotterdamTHE NETHERLANDSTel. +31 10 408 78 96Fax. +31 10 408 84 [email protected]
Dr Silvia FRANCESCHIUnit of Field and Intervention StudiesInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 84 02Fax. +33 4 72 73 83 [email protected]
Dr Shingo FUJIIDepartment of Gynecology and ObstetricsKyoto University Graduate School ofMedicineSakyoku, Kyoto 606-8507JAPANTel. +81 75 751 3267Fax. +81 75 751 [email protected]
Dr David R. GENEST**Dept. of PathologyBrigham and Women’s Hospital75 Francis StreetBoston, MA 02115U.S.ATel. +1 617 732 7542Fax. +1 617 630 [email protected]
Dr Deborah J. GERSELLDepartment of PathologySt. John’s Mercy Medical Center615 South New Ballas RoadSt Louis, MO 63141U.S.ATel. +1 314 569 6120Fax. +1 314 995 [email protected]
Dr Blake GILKSDepartment of Pathology and LaboratoryMedicine, Vancouver General Hospital University of British Columbia Vancouver V5M 1Z9CANADATel. +1 604 875 5555Fax. +1 604 875 [email protected]
Dr David E. GOLDGARUnit of Genetic EpidemiologyInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 7273 83 18Fax. +33 4 7273 83 [email protected]
Dr Annekathryn GOODMANGillette Center for Women’s CancerMassachusetts General Hospital100 Blossom StBoston, MA 02114U.S.ATel. +1 617 726 5997Fax. +1 617 523 [email protected]
Dr Pierre HAINAUTUnit of Molecular CarcinogenesisInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 32Fax. +33 4 72 73 83 [email protected]
Dr Janet HALLDNA Repair GroupInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 96Fax. +33 4 72 73 83 [email protected]
Dr Urs HALLERDepartement of Obstetrics and GynecologyUniversity HospitalFrauenklinikstr. 108091 ZürichSWITZERLANDTel. +41 1 255 5200Fax. +41 1 255 [email protected]
Dr Antonius G.J.M. HANSELAAR**Office of the Managing DirectorDutch Cancer SocietyP.O. Box 755081070 AM AmsterdamTHE NETHERLANDSTel. +31 20 57 00 510Fax. +31 20 67 50 [email protected]
Dr Steffen HAUPTMANNInstitute of PathologyMartin-Luther-University Halle-WittenbergMagdeburger Str. 1406112 Halle (Saale)GERMANYTel. +49-345-557-1880Fax. [email protected]
Dr Michael R. HENDRICKSON**Lab. of Surgical Pathology, H 2110Stanford University Medical Center300 Pasteur DriveStanford CA 94305-5243U.S.ATel. +1 650 498 64 60Fax. +1 650 725 69 02 [email protected]
Dr Sylvia H. HEYWANG-KöBRUNNERCenter for Breast Diagnosis andInterventionTechnical University MunichKlinikum Rechts der Isar81675 MunichGERMANYTel. +49 89 4140-0Fax. +49-89-4140-4831
Dr Heinz HÖFLER*Institute of PathologyTechnical University MunichIsmaninger Strasse 2281675 MunichGERMANYTel. +49 89 41 40 41 60Fax. +49 89 41 40 48 [email protected]
Dr Roland HOLLAND*National Breast Cancer Screening Centre Nÿmegen University HospitalGeert Grooteplein 18, Postbus 91016500 HB NÿmegenTHE NETHERLANDSTel. +31 24 361 6706Fax. +31 24 354 [email protected]
Dr Jocelyne JACQUEMIERDepartment of PathologyInstitut Paoli Calmettes232, Boulevard Sainte Marguerite13009 MarseilleFRANCETel. +33 4 91 22 34 57Fax. +33 4 91 22 35 [email protected]
Dr Rudolf KAAKS*Hormones and Cancer GroupInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 53Fax. +33 4 72 73 83 [email protected]
Dr Apollon I. KARSELADZE**Division of Human Tumour PathologyRussian Oncological CenterKashirskoye shosse, 24115 478 Moscow RUSSIATel. +7 095 324 96 44Fax. +7 095 323 57 [email protected]
Dr Richard L. KEMPSON**Department of PathologyStanford University Medical Center300 Pasteur Drive, Room L235Stanford, CA 94305-5324U.S.ATel. + 1 650 498 6460Fax. +1 650 725 [email protected]
Dr Takako KIYOKAWADepartment of PathologyJikei University School of Medecine3-25-8-Nishishinbashi Minato-kuTokyo 105-8461JAPANTel. +81 3 3433 1111 ex5372Fax. +81 3 5470 [email protected]
Dr Paul KLEIHUES* ** International Agency for Research onCancer (IARC)150, cours Albert Thomas69008 LyonFRANCETel. +33 4 72 73 81 77Fax. +33 4 72 73 85 [email protected]
Dr Ikuo KONISHI Department of Obstetrics and GynecologyShinshu University School of MedicineAsahiMatsumoto 390-8621JAPANTel. +81 263 37 2716Fax. +81 263 34 [email protected]
Dr Rahel KUBIK-HUCHInstitute of RadiologyCantonal Hospital5404 BadenSWITZERLANDTel. +41 56 486 38 03Fax. +41 56 483 38 [email protected]
Dr Robert J. KURMAN**Departements of Pathology andGynecology & ObstetricsThe Johns Hopkins HospitalBaltimore, MD 21231-2410U.S.ATel. +1 410 955 0471/2804Fax. +1 410 614 [email protected]
367
Dr Carlo LA VECCHIALaboratory of EpidemiologyIstituto "Mario Negri"Via Eritrea 62I-20157 MilanoITALYTel. +390 02 390 14527Fax. +39 02 332 [email protected]
Dr Sunil R. LAKHANI*The Breakthrough Toby Robins BreastCancer Research CentreChester Beatty LabsLondon SW3 6JBUNITED KINGDOMTel. +44 20 7153 5525Fax. +44 20 7153 [email protected]
Dr Janez LAMOVEC Department of PathologyInstitute of OncologyZaloska 21105 Ljubljana SLOVENIATel. +386 1 4322 099Fax. +386 1 4314 [email protected]
Dr Salvatore LANZAFAMEAnatomia PatologicaPoliclinoco Università di CataniaVia S. Sofia, 8795123 CataniaITALYTel. +39 095 310 241?Fax. +39 095 [email protected]
Dr Sigurd LAX**Department of PathologyGeneral Hospital Graz WestGoestinger Strasse 228020 GrazAUSTRIATel. +43 316 5466 4650Fax. +43 316 5466 [email protected]
Dr Kenneth R. LEEDepartment of PathologyBrigham and Women’s Hospital75 Francis StreetBoston MA 02115U.S.ATel. +1 617 278 0736Fax. +1 617 739 [email protected]
Dr Fabio LEVIUnité d’Epidémiologie du CancerInstitut Universitaire de Médecine Sociale et Préventive, CHUV-Falaises 11011 LausanneSWITZERLANDTel. +41 213 147 311Fax. +41 213 230 [email protected]
Dr Gaëtan MacGROGAN*Département de PathologieInstitut Bergonié229, Cours de l’Argonne33076 Bordeaux cedexFRANCETel. +33 5 56 33 33 23 Fax. +33 5 56 33 [email protected]
Dr Gaetano MAGRODipartimento G.F. INGRASSIAAnatomia PatologicaUniversità di Catania95123 CataniaITALYTel. +39 952 56025Fax. +39 [email protected]
Dr Kien T. MAILaboratory Medicine, Room 1131053 Carling Ave.Ottawa, Ontario K1Y 4E9CANADATel. +1 613 761 43 44Fax. +1613 761 48 [email protected]
Dr W. Glenn McCLUGGAGE**Department of PathologyRoyal Group of Hospitals TrustGrosvenor RoadBelfast BT12 6BL UNITED KINGDOMTel. +44 28 9063 2563Fax. +44 28 9023 [email protected]
Dr Hanne MEIJERS-HEIJBOERDepartment of Clinical GeneticsErasmus Medical Center RotterdamWestzeedijk 1123016 AH RotterdamTHE NETHERLANDSTel. +31 10 4636919Fax. +31 10 [email protected]
Dr Rosemary R. MILLIS*Hedley Atkins / Cancer Research UKBreast Pathology LaboratoryGuy’s HospitalLondon SE1 9RTUNITED KINGDOMTel. +44 207 955 4539Fax. +44 207 955 [email protected]
Dr Farid MOINFAR*Department of PathologyUniversity of GrazAuenbruggerplatz 258036 GrazAUSTRIATel. +43 316 380 4453Fax. +43 316 385 [email protected]
Dr Samuel C. MOKDepartment of Obstetrics, Gynecology &Reproductive BiologyBrigham and Women’s HospitalBoston, MA 02115U.S.ATel. +1 617 278 0196Fax. +1 617 975 [email protected]
Dr Alvaro N. MONTEIRODept. of Cell and Developmental BiologyWeill Medical College, Cornell University1300 York AvenueNew York, NY 10021U.S.ATel. +1 212 734 0567 / ext 225Fax. +1 212 472 [email protected]
Dr Eoghan E. MOONEY**Department of Pathology and LaboratoryMedicineNational Maternity HospitalDublin 2IRELANDTel. +353 1 63 735 31Fax. +353 1 67 65 [email protected]
Dr Philippe MORICEDépartement de ChirurgieInstitut Gustave Roussy39 rue Camille Desmoulins94805 VillejuifFRANCETel. +33 1 42 11 54 41Fax. +33 1 42 11 52 [email protected]
Dr Hans MORREAUDepartment of PathologyLeiden University Medical CentrePO Box 96002300 RC LeidenTHE NETHERLANDSTel. +33 71 52 66 625Fax. +33 71 52 48 [email protected]
Dr Kiyoshi MUKAIFirst Department of Pathology Tokyo Medical UniversityShinjuku 6-1-1, Shinjuku-ku160-8402 Tokyo JAPANTel. +81 3 3351 6141Fax. +81 3 3352 [email protected]
Dr Mary MURNAGHANRoyal Jubilee Maternity HospitalRoyal Hospitals TrustGrosvenor RoadBelfast BT12 6AAUNITED KINGDOMTel. +44 28 90 632150Fax. +44 28 90 [email protected]
Dr George L. MUTTER**Department of Pathology Brigham and Women’s HospitalHarvard Medical SchoolBoston, MA 02115U.S.ATel. +1 617 732 6096Fax. +1 617 738 6996 [email protected]
Dr Steven NARODThe Center for Research in Women’sHealth, University of Toronto790 Bay Street, 7th floorToronto, Ontario M5G 1N8CANADATel. +1 416 351 37 32Fax. +1 416 351 37 [email protected]
Dr Jahn M. NESLAND**Department of Pathology, University ClinicThe Norwegian Radium HospitalMontebello0310 OsloNORWAYTel. +47 22 93 5620Fax. +47 22 730 [email protected]
Dr Edward S. NEWLANDSMedical OncologyCharing Cross HospitalImperial College School of MedicineLondon W6 8RFUNITED KINGDOMTel. +44 208 8461419Fax. +44 208 [email protected]
Dr Bernt B. NIELSENInstitute of PathologyRanders HospitalSkovlyvej 18900 RandersDENMARKTel. +45 8910 2351Fax. +45 8642 [email protected]
Dr Francisco F. NOGALES**Department of PathologyGranada University Faculty of MedicineAvenida de Madrid, 1118071 GranadaSPAINTel. +34 9 58 243 508Fax. +34 9 58 243 [email protected]
Dr Hiroko OHGAKI* **Unit of Molecular PathologyInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 34Fax. +33 4 72 73 85 [email protected]
Dr Magali OLIVIERUnit of Molecular CarcinogenesisInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 86 69Fax. +33 4 72 73 83 [email protected]
Dr Andrew G. ÖSTÖR** (Deceased)Department of Pathology, Obstetrics andGynaecologyThe University of Melbourne48 Anderson Rd3123 Hawthorn East, Vic.AUSTRALIATel. +61 3 9822 1145Fax. +61 3 9882 0933
Dr Jorma PAAVONENDepartment of Obstetrics and GynecologyUniversity of HelsinkiHaartmaninkatu 200290 HelsinkiFINLANDTel. +358 9 4717 2807Fax. +358 9 4717 [email protected]
Dr Paivi PELTOMAKIBiomedicum Helsinki Department ofMedical Genetics, University of HelsinkiHaartmaninkatu 8, P. O. Box 6300014 HelsinkiFINLANDTel. +358 9 19125092Fax. +358 9 [email protected]
Contributors
368 Contributors
Dr Johannes L. PETERSE*Department of PathologyNetherlands Cancer InstitutePlesmanlaan 1211066 CXAmsterdamTHE NETHERLANDSTel. +31 20 512 27 50Fax +31 20 512 [email protected]
Dr Jurgen J.M. PIEKDepartment of Obstetrics and GynaecologyVU University Medical CenterP.O. Box 70571007 MB AmsterdamTHE NETHERLANDSTel. +31 20 444 2828 Fax. +31 20 444 [email protected]
Dr Paola PISANIUnit of Descriptive EpidemiologyInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 22 Fax. +33 4 72 73 86 [email protected]
Dr Steven PIVERDepartment of Gynecology and OncologySisters of Charity Hospital2157 Main StreetNew York, NY 14214U.S.A.Tel. +1 716-862 1000Fax. +1 716-862 1899 [email protected]
Dr Jaime PRAT**Department of PathologyHospital de la Sta Creu i Sant PauAutonomous University of Barcelona08025 BarcelonaSPAINTel. +34 93 291 90 23Fax. +34 93 291 93 [email protected]
Dr Klaus PRECHTEL*Pathologie StarnbergHöhenweg 18a82229 SeefeldGERMANYTel. +49 8152 7740Fax. +49 8152 [email protected]
Dr Dieter PRECHTELGemeinschaftspraxis PathologieAm Fuchsengraben 382319 StarnbergGERMANYTel. +49 8151/3612-0Fax. +49 8151/[email protected]
Dr Usha RAJUDepartment of PathologyHenry Ford Hospital2799 WG BlvdDetroit MI 48202U.S.ATel. +1 313 916 1917Fax. +1 313 916 [email protected]
Dr Juan ROSAI*Department of PathologyNational Cancer InstituteVia Venezian 120133 MilanITALYTel. +39 02 2390 2876Fax. +39 02 2390 [email protected]
Dr Lawrence M. ROTHDepartment of Pathology Indiana University School of Medicine550 North University Blvd., Room 3465Indianapolis, Indiana 46202-5280U.S.A.Tel. +1 317 274 5784Fax. +1 317 274 [email protected]
Dr Peter RUSSELLDepartment of Anatomical PathologyRoyal Prince Alfred HospitalCamperdown, NSW 2050AUSTRALIATel. +61 4 1822 2567Fax. +61 2 9515 [email protected]
Dr Joanne K.L. RUTGERSDepartment of PathologyLong Beach Memorial Medical Center2801 Atlantic Ave.Long Beach, CA 90801-1428U.S.ATel. +1 562 933 0726Fax. +1 562 933 [email protected]
Dr Rengaswamy SANKARANARAYANANUnit of Descriptive EpidemiologyInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 85 99Fax. +33 4 72 73 85 [email protected]
Dr Anna SAPINODepartment of Biomedical Sciences andOncology, University of TorinoVia Santena 710126 TorinoITALYTel. +39-011-6706510Fax. [email protected]
Dr Annie J. SASCO*Unit of Epidemiology for Cancer PreventionInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 84 12Fax. +33 4 72 73 83 [email protected]
Dr Xavier SASTRE-GARAU*Service de PathologieInstitut Curie26 rue d’Ulm75248 ParisFRANCETel. +33 1 44 32 42 54 / 50Fax. +33 1 44 32 40 [email protected]
Dr Stuart J. SCHNITT* Department of PathologyBeth Israel Deaconess Medical Center330 Brookline AvenueBoston, MA 02215U.S.ATel. +1 617 667 43 44Fax. +1 617 975 56 [email protected]
Dr John O. SCHORGEGynecologic OncologyUniv. of Texas Southwestern Medical Center 5323 Harry Hines Blvd, Room J7.124Dallas TX 75390-9032U.S.ATel. +1 214 648 3026Fax. +1 214 648 8404j o h n . s c h o r g e @ u t s o u t h w e s t e r n . e d u
Dr Peter E. SCHWARTZ**Department of Obstetrics and GynecologyYale University School of Medicine333 Cedar Street - FMB 316New Haven, CT 06520-8063U.S.ATel. +1 203 785 4014Fax. +1 203 785 [email protected]
Dr Robert E. SCULLY**Department of PathologyMassachusetts General Hospital55 Fruit Street, Warren 242Boston, MA 02114-2696U.S.ATel. +1 617 724 14 59Fax. +1 617 726 59 [email protected]
Dr Hideto SENZAKIDepartment of PathologyKansai Medical University10-15 Fumizonocho, Moriguchi,Osaka 570-8506JAPANTel. +81-6-6993-9432Fax. [email protected]
Dr Elvio G. SILVADept. of PathologyM.D. Anderson Cancer Center1515 Holcombe Blvd.Houston TX 77030U.S.ATel. +1 713 792 31 54Fax. +1 713 792 55 [email protected]
Dr Steven G. SILVERBERG**Department of PathologyUniversity of Maryland Medical System22 South Greene StreetBaltimore MD 21201U.S.ATel. +1 410 328 50 72Fax. +1 410 328 00 [email protected]
Dr Jorge SOARESDepartamento de Patologia MorfológicaInstituto Português de OncologiaRua Professor Lima Basto1099-023 LisboaPORTUGALTel. +351 21 7229825Fax. +351 21 [email protected]
Dr Leslie H. SOBIN* **Department of Hepatic andGastrointestinal PathologyArmed Forces Institute of PathologyWashington, DC 20306U.S.A.Tel. +1 202 782 2880Fax. +1 202 782 [email protected]
Ms Nayanta SODHA MScCancer Genetics LaboratoryInstitute of Cancer ResearchCotswold RoadSutton, Surrey SM2 5NG UNITED KINGDOMTel. +44 208 643 8901Fax. +44 208 770 [email protected]
Dr Mike R. STRATTONCancer Genome Project The Wellcome Trust Sanger InstituteHinxtonCambridge CB10 1SAUNITED KINGDOMTel. +44 1223 494757 Fax. +44 1223 [email protected]
Dr Csilla SZABOUnit of Genetic EpidemiologyInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 86 58Fax. +33 4 72 73 83 [email protected]
Dr László TABÁRMammography DepartmentCentral Hospital79182 FalunSWEDENTel. +46 23 49 2507Fax. +46 23 49 [email protected]
Dr Aleksander TALERMANDepartment of PathologyThomas Jefferson University132 South 10th StreetRoom 285Q / Main BuildingPhiladelphia, PA 19107-5244U.S.ATel. +1 215 955 2433Fax. +1 215 923 1969
Dr Colette TARANGER-CHARPINService d’Anatomie et CytologiePathologique, Hôpital NordBoulevard Dramard13916 MarseilleFRANCETel. +33 4 91 69 88 64Fax. +33 4 91 69 89 [email protected]
Dr Fattaneh A. TAVASSOLI* **Department of PathologyYale University School of Medicine310 Cedar Street, Room # LH 222New Haven, CT 06520U.S.ATel. +1 203 785 5439Fax. +1 203 785 [email protected]
369Contributors
Dr Manuel TEIXEIRADepartment of GeneticsPortuguese Oncology InstituteRua Dr. Antonio Bernardino Almeida4200-072 PortoPORTUGALTel. +351 22 550 20 11/50 78Fax. +351 22 502 64 [email protected]
Dr Massimo TOMMASINOUnit of Infection and CancerInternational Agency for Research onCancer (IARC)69008 LyonFRANCETel. +33 4 72 73 81 91Fax. +33 4 72 73 84 [email protected]
Dr Airo TSUBURASecond Department of PathologyKansai Medical University10-15 Fumizono, Moriguchi,Osaka 570-8506JAPANTel. +81 6 6993 9431Fax. +81 6 6992 [email protected]
Dr Paul J. VAN DIESTDepartment of Pathology Universitair Medisch Centrum UltrechtHeidelberglaan 1003508 GA UtrechtTHE NETHERLANDSTel. +31 30 250 6565Fax. +31 30 254 [email protected]
Dr Laura J. VAN’T VEERDepartment of Molecular PathologyNetherlands Cancer InstitutePlesmanlaan 1211066 CX AmsterdamTHE NETHERLANDSTel. +31 20 5122754Fax. +31 20 [email protected]
Dr Russell S. VANGDepartment of Gynecologic and BreastPathology, Building 54, Room 1072Armed Forces Institute of PathologyWashington, D.C. 20306-6000U.S.A.Tel. +1 202-782-1609Fax. +1 [email protected]
Dr Hans F.A. VASENNetherlands Foundation for the Detectionof Hereditary TumoursPoortgebouw Zuid, Rijnsburgerweg 102333 AA LeidenTHE NETHERLANDSTel. +31 71 5262687Fax. +31 71 [email protected]
Dr A.R. VENKITARAMANMRC Cancer Cell Unit Dept. of Oncology, Hills RoadUniversity of CambridgeCambridge CB2 2XZUNITED KINGDOMTel. +44 122 333 6901Fax. +44 122 376 [email protected]
Dr René H.M. VERHEIJENDivision of Gynaecologycal OncologyVU University Medical CenterP.O. Box 70571007 MB AmsterdamTHE NETHERLANDSTel. +31 20 444 4851Fax. +31 20 444 [email protected]
Dr William R. WELCHDepartment of PathologyBrigham and Women’s Hospital75 Francis StreetBoston MA 02115U.S.ATel. +1 617 732 4745Fax. +1 617 734 [email protected]
Dr Michael WELLS**Academic Unit of PathologyMedical SchoolBeech Hill RoadSheffield S10 2RX UNITED KINGDOMTel. +44 114 271 2397/2683Fax. +44 114 226 [email protected]
Dr Edward J. WILKINSONDepartment of PathologyUniversity of Florida College of Medicine1600 S.W. Archer Rd.Gainesville, FL 32610-0275U.S.ATel. +1 352 265 0238Fax. +1 352 265 [email protected]
Dr Andrew WOTHERSPOONDepartment of HistopathologyRoyal Marsden TrustFulham RoadLondon SW3 6JJUNITED KINGDOMTel. +44 207 352 73 48Fax. +44 207 352 73 48a n d r e w . w o t h e r s p o o n @ r m h . n t h a m e s . n h s . u k
370 Source of charts and photographs
Source of charts and photographs
1.
01.01 IARC, Lyon01.02 Dr. P. Pisani01.03 Dr. A. Sasco01.04 IARC, Lyon01.05 Dr. R. Kaaks01.06 Dr. R. Kaaks/
Dr. A. Sasco01.07 Dr. I.O. Ellis01.08A-01.10C Dr. L. Tabár01.11 Dr. R. Caduff01.12A,B Dr. S.J. Schnitt01.12C Dr. I.O. Ellis01.13 Dr. J. Jacquemier01.14A,B Dr. F.A. Tavassoli01.15-01.16A Dr. J.L. Peterse01.16B Dr. S.J. Schnitt01.17A,B Dr. F.A. Tavassoli01.18 Dr. X. Sastre-Garau01.19A,B Dr. L. Tabár01.20-01.21C Dr. X. Sastre-Garau01.22A,B Dr. F.A. Tavassoli01.23 Dr. L. Tabár01.24A-01.25 Dr. F.A. Tavassoli01.26 Dr. L. Tabár01.27 Dr. I.O. Ellis01.28 Dr. X. Sastre-Garau01.29A-C Dr. L. Tabár01.30 Dr. R. Caduff01.31A-01.32D Dr. F.A. Tavassoli01.33A Dr. S.J. Schnitt01.33B-01.34 Dr. G. Bussolati01.35A-C Dr. L. Tabár01.36A,B Dr. F.A. Tavassoli01.37-01.38C Dr. J.L. Peterse01.39-01.41 Dr. V. Eusebi01.42-01.43 Dr. F.A. Tavassoli01.44A Dr. Okcu
Institut für Pathologie,Karl-Franzens-Univer-sität, Graz, Austria
01.44B-01.47 Dr. F.A. Tavassoli01.48 Dr. U. Raju01.49A Dr. R. Caduff01.49B-01.51B Dr. F.A. Tavassoli01.52-01.55 Dr. V. Eusebi01.56 Dr. F.A. Tavassoli
01.57-01.61 Dr. V. Eusebi01.62A-01.64 Dr. F.A. Tavassoli01.65-01.068 Dr. P. Devilee01.69 Dr. A.L. Borresen-Dale01.70 Dr. F.A. Tavassoli01.71 Dr. S.J. Schnitt01.72 Dr. F.A. Tavassoli01.73 Dr. L.J. van’t Veer01.74A-01.75C Dr. F.A. Tavassoli01.76 Dr. W. Boecker01.77A-01.80B Dr. F.A. Tavassoli01.80C,D Dr. W. Boecker01.81-01.82 Dr. F.A. Tavassoli01.83 Dr. R. Heywang-
Koebrunner01.84 Dr. W. Boecker01.85A,B Dr. F.A. Tavassoli01.86A-D Dr. R. Heywang-
Koebrunner01.87A,B Dr. L. Tabár01.88A,B Dr. W. Boecker01.89A-01.90B Dr. F.A. Tavassoli01.90C-D Dr. W. Boecker01.90E-01.91 Dr. F.A. Tavassoli01.92-01.93 Dr. L. Tabár01.94A Dr. W. Boecker01.94B-01.97C Dr. F.A. Tavassoli01.98-01.99B Dr. G. MacGrogan01.100-01.101C Dr. U. Raju01.102A,B Dr. G. MacGrogan01.103A-C Dr. W. Boecker01.103D Dr. G. MacGrogan01.104 Dr. U. Raju01.105A-C Dr. L. Tabár01.106A Dr. M. Drijkoningen01.106B-D Dr. G. MacGrogan01.107 Dr. M. Drijkoningen01.108-01.109A Dr. B.B. Nielsen01.109B Dr. S.J. Schnitt01.109C Dr. M. Drijkoningen01.110A,B Dr. W. Boecker01.111 Dr. B.B. Nielsen01.112 Dr. F.A. Tavassoli01.113 Dr. B.B. Nielsen01.114-01.117 Dr. F.A. Tavassoli01.118 Dr. W. Boecker01.119 Dr. A.G.J.M. Hanselaar01.120 Dr. M. Drijkoningen01.121A-01.122B Dr. G. Bussolati01.123 Dr. F.A. Tavassoli01.124 Dr. G. Bussolati01.125A,B Dr. F.A. Tavassoli01.126A,B Dr. B.B. Nielsen01.127A-01.131B Dr. F.A. Tavassoli
01.132 Dr. J.L. Peterse01.133-01.136 Dr. F.A. Tavassoli01.137A-01.139 Dr. J.P. Bellocq01.140A-C Dr. V. Eusebi01.141-01.142 Dr. J.L. Peterse01.143-01.145B Dr. F.A. Tavassoli01.146A-01.152C Dr. J.P. Bellocq01.153A,B Dr. F.A. Tavassoli01.154 Dr. J.P. Bellocq01.155-01.157B Dr. V. Eusebi01.158A-C Dr. K.T. Mai01.159A-01.160 Dr. J. Lamovec01.161 Dr. E.S. Jaffe
NIH, National Cancer I n s t i t u t e, Bethesda MD, U.S.A
01.162 Dr. J. Lamovec01.163 Dr. J. Jacquemier01.164-01.166 Dr. K. Prechtel01.167 Dr. F.A. Tavassoli
2.
02.01 IARC02.02 Dr. R.A. Kubik-Huch02.03A Dr. J. Prat02.03B Dr. L. Roth02.04A Dr. F.A. Tavassoli02.04B Dr. S. Lax02.05 Dr. J. Prat02.06A.B Dr. M. Dietel02.07A Dr. F.A. Tavassoli02.07B Dr. S. Lax02.08 Dr. J. Prat02.09A Dr. F.A. Tavassoli02.09B Dr. M. Dietel02.10A,B Dr. J. Prat02.11 Dr. M. Dietel02.12 Dr. A.I. Karseladze02.13 Dr. M. Dietel02.14 Dr. R.H. Young
Dept. PathologyMassachusetts General HospitalBoston, U.S.A
02.15 Dr. K. Lee02.16A Dr. J. Prat02.16B Dr. K. Lee02.17 Dr. R.H. Young02.18-02.19 Dr. K. Lee02.20 Dr. J. Prat02.21A Dr. K. Lee02.21B Dr. J. Prat
02.22-02.24B Dr. K. Lee02.25 Dr. R.H. Young02.26 Dr. K. Lee02.27 Dr. J. Prat02.28A,B Dr. S. Lax02.29A,B Dr. J. Prat02.30A Dr. S. Lax02.30B-02.31A Dr. J. Prat02.31B Dr. L. Roth02.32-02.34 Dr. J. Prat02.35 Dr. C.H. Buckley02.36 Dr. F.A. Tavassoli02.37A Dr. S. Lax02.37B Dr. J. Prat02.38 Dr. S. Lax02.39A Dr. A.I. Karseladze02.39B Dr. L. Roth02.40 Dr. A.I. Karseladze02.41 Dr. J. Prat02.42 Dr. R. Vang02.43 Dr. V. Abeler02.44A,B Dr. J. Prat02.45 Dr. R.A. Kubik-Huch02.46 Dr. R. Vang02.47 Dr. J. Prat02.48A,B Dr. D.J. Gersell02.49 Dr. J. Prat02.50-02.53A Dr. D.J. Gersell02.53B Dr. J. Prat02.53C Dr. D.J. Gersell02.54A,B Dr. E.G. Silva02.55 Dr. R.A. Kubik-Huch02.56A-02.63B Dr. F.A. Tavassoli02.64A-02.65 Dr. D.J. Gersell02.66 Dr. F.A. Tavassoli02.67A-02.69 Dr. D.J. Gersell02.70 Dr. F.A. Tavassoli02.71 Dr. L. Roth02.72A-02.73 Dr. F.A. Tavassoli02.74-02.75A Dr. E. Mooney02.75B Dr. F.A. Tavassoli02.75C-02.78 Dr. E. Mooney02.79A-02.80 Dr. F.A. Tavassoli02.81 Dr. E. Mooney02.82 Dr. F.A. Tavassoli02.83-02.84A Dr. L. Roth02.84B Dr. S. Lax02.85 Dr. E. Mooney02.86 Dr. L. Roth02.87A,B Dr. P.E. Schwartz02.88A-02.97 Dr. F. Nogales02.98A,B Dr. F.A. Tavassoli02.99 Dr. R.A. Kubik-Huch
The copyright remains with the authors.Requests for permission to reproducefigures or charts should be directed tothe respective contributor. For addresssee Contributors List.
371Source of charts and photographs
02.100 Dr. A. Ostor02.101 Dr. F.A. Tavassoli02.102A,B Dr. M. Devouassoux-
Shisheboran02.103 Dr. S. Lax02.104-02.106 Dr. M. Devouassoux-
Shisheboran02.107-02.109B Dr. F.A. Tavassoli02.110-02.113 Dr. A. Talerman02.114-02.116B Dr. F. Nogales02.117-02.118B Dr. L. Roth02.119A,B Dr. H. Senzaki/
Dr. A. Tsubura02.120-02.121 Dr. L. Roth02.122A,B Dr. M. Devouassoux-
Shisheboran02.123-02.126 Dr. L. Roth02.127 Dr. F.A. Tavassoli02.128A-02.129B Dr. R. Vang02.130A-02.131A Dr. J. Prat02.131B Dr. L. Roth02.131C-02.134 Dr. J. Prat02.135 Dr. L. Roth02.136-02.137C Dr. J. Prat02.138A Dr. L. Roth02.138B Dr. F. Nogales02.139A,B Dr. L. Roth02.140A-C Dr. F.A. Tavassoli02.141 Dr. M.R. Hendrickson02.142A Dr. F.A. Tavassoli02.142B Dr. L. Roth02.143A-02.144 Dr. M.R. Hendrickson02.145 Dr. F.A. Tavassoli
3.
03.01 Dr. R. Caduff03.02A-03.04C Dr. I. Alvarado-Cabrero03.05A-03.06 Dr. L. Roth03.07 Dr. A. Cheung03.08 Dr. L. Roth03.09 Dr. A. Cheung03.10 Dr. L. Roth03.11A,B Dr. F.A. Tavassoli03.12-03.13 Dr. L. Roth03.14A Dr. M. Devouassoux-
Shisheboran03.14B Dr. L. Roth03.15A,B Dr. F.A. Tavassoli03.16 Dr. R. Vang03.17A,B Dr. L. Roth
4.
04.01 IARC04.02A,B Dr. F.A. Tavassoli04.03-04.04 Dr. S.G. Silverberg04.05 Dr. S. Lax04.06 Dr. F.A. Tavassoli04.07 Dr. S.G. Silverberg04.08 Dr. F. Nogales04.09-04.12 Dr. S.G. Silverberg04.13 Dr. F.A. Tavassoli04.14 Dr. S.G. Silverberg04.15A Dr. M. Márquez
Hospital Clinic Barcelona, Spain
04.15B Dr. F. Nogales04.16A Dr. E. Mendoza
Hospital Virgen del Rocio, Sevilla, Spain
04.16B-04.18A Dr. F. Nogales04.18B Dr. F.A. Tavassoli04.19-04.21 Dr. F. Nogales04.22 Dr. S. Lax04.23-04.24 Dr. G.L. Mutter04.25A-C Dr. M.R. Hendrickson04.26A Dr. S.G. Silverberg04.26B-04.28B Dr. M.R. Hendrickson04.28C,D Dr. F.A. Tavassoli04.29 Dr. S.G. Silverberg04.30A Dr. M.R. Hendrickson04.30B-C Dr. S.G. Silverberg04.30D-04.32B Dr. M.R. Hendrickson04.32C Dr. S.G. Silverberg04.33 Dr. R.A. Kubik-Huch04.34 Dr. M.R. Hendrickson04.35-04.36 Dr. S.G. Silverberg04.37-04.38C Dr. M.R. Hendrickson04.39 Dr. S.G. Silverberg04.40A-C Dr. R. Vang04.41 Dr. W.G. McCluggage04.42-04.43B Dr. F.A. Tavassoli04.43C,D Dr. R. Vang04.44A Dr. L. Roth04.44B-04.45 Dr. R. Vang04.46A,B Dr. D. Genest04.47A Dr. A. Ostor04.47B Dr. L. Roth04.48A Dr. D. Genest04.48B Dr. M. Wells04.49A Dr. A. Ostor04.49B Dr. D. Genest04.50A Dr. A. Ostor
04.50B Dr. D. Genest04.51 Dr. R.A. Kubik-Huch04.52-04.55 Dr. D. Genest04.56A-04.57B Dr. F. Nogales04.58A,B Dr. F.A. Tavassoli04.59A-04.60 Dr. V. Abeler
5.
05.01-05.02 IARC, Lyon05.03 Dr. M. Tommasino05.04 Dr. N. Muñoz, IARC, Lyon05.05 Dr. S. Franceschi05.06 Dr. R.A. Kubik-Huch05.07 Dr. E.J. Wilkinson05.08-05.09 Dr. A.G. Hanselaar05.10 Dr. A. Ostor05.11-05.12 Dr. C.P. Crum05.13 Dr. M. Wells05.14A,B Dr. C.P. Crum05.15A Dr. S. Lax05.15B-05.19 Dr. A.G.J.M. Hanselaar05.20A,B Dr. A. Ostor05.20C Dr. A.G.J.M. Hanselaar05.21 Dr. L. Roth05.22A,B Dr. A. Ostor05.23A-C Dr. R. Vang05.24-05.27 Dr. A. Ostor05.28 Dr. M. Wells05.29-05.30 Dr. A. Ostor05.31-05.32A Dr. J. Nesland05.32B Dr. C.P. Crum05.33-05.34 Dr. M. Wells05.35A,B Dr. T.P. Rollason
Dept. Histopathology,Birmingham Women'sHospital,Birmingham, UK
05.36A-05.41 Dr. M.L. Carcangiu05.42 Dr. R.A. Kubik-Huch05.43-05.44 Dr. F.A. Tavassoli05.45-05.48B Dr. B. Gilks
6.
06.01A,B Dr. E. Andersen06.02-06.09 Dr. J. Paavonen/
Dr. C. Bergeron06.10 Dr. F.A. Tavassoli06.11A Dr. R.L. Kempson06.11B Dr. L. Roth06.12A-06.15 Dr. A.G.J.M. Hanselaar
06.16 Dr. A. Ostor06.17A-06.19 Dr. R.L. Kempson06.20 Dr. L. Roth06.21A,B Dr. R. Vang06.22 Dr. F.A. Tavassoli06.23A-06.25 Dr. R. Vang
7.
07.01-07.02 Dr. E.J. Wilkinson07.03A Dr. F.A. Tavassoli07.03B-07.09A Dr. E.J. Wilkinson07.09B Dr. L. Roth07.09C Dr. R.L. Kempson07.10A,B Dr. E.J. Wilkinson07.11 Dr. L. Roth07.12A,B Dr. E.J. Wilkinson07.12C Dr. F.A. Tavassoli07.13A-07.14 Dr. E.J. Wilkinson07.15 Dr. R.L. Kempson07.16A-07.17C Dr. L. Roth07.18A-07.19 Dr. R.L. Kempson07.20A-07.22 Dr. E.J. Wilkinson07.23A,B Dr. M. Wells
8.08.01-08.02 Dr. D. Easton08.03-08.05 Dr. J. Piek08.06 Dr. P. Devilee08.07 Dr. S. Narod08.08 Dr. A.R. Venkitaraman
{4116}08.09 Dr. P. Devilee08.10 Dr. A.R. Venkitaraman08.11A-08.12 Dr. H. Ohgaki08.13-08.14 Dr. P. Hainaut

372 References
1 . Anon. (1982). The World HealthOrganization Histological Typing of BreastTumors-Second Edition. The World HealthOrganization. Am J Clin Pathol 78: 806-816. 2. Anon. (1987). The reduction in risk ofovarian cancer associated with oral-con-traceptive use. The Cancer and SteroidHormone Study of the Centers for DiseaseControl and the National Institute of ChildHealth and Human Development. N Engl JMed 316: 650-655. 3. Anon. (1990). Surgical-procedure termi-nology for the vulva and vagina. Report ofan International Society for the Study ofVulvar Disease Task Force. J Reprod Med35: 1033-1034. 4. Anon. (1992). Systemic treatment of earlybreast cancer by hormonal, cytotoxic, orimmune therapy. 133 randomised trialsinvolving 31,000 recurrences and 24,000deaths among 75,000 women. Early BreastCancer Trialists' Collaborative Group.Lancet 339: 1-15. 5. Anon. (1996). Clinical practice guidelinesfor the use of tumor markers in breast andcolorectal cancer. Adopted on May 17,1996 by the American Society of ClinicalOncology. J Clin Oncol 14: 2843-2877.
6. Anon. (1997). Consensus conference onthe classification of ductal carcinoma insitu. Hum Pathol 28: 1221-1225. 7. Anon. (1997). Consensus Conference on
the classification of ductal carcinoma insitu. The Consensus ConferenceCommittee. Cancer 80: 1798-1802.
8 . Anon. (1997). Pathology of familialbreast cancer: differences between breastcancers in carriers of BRCA1 or BRCA2mutations and sporadic cases. BreastCancer Linkage Consortium. Lancet 349:1505-1510. 9. Anon. (1998). 1997 update of recommen-
dations for the use of tumor markers inbreast and colorectal cancer. Adopted onNovember 7, 1997 by the American Societyof Clinical Oncology. J Clin Oncol 16: 793-795. 10. Anon. (1998). Tamoxifen for early breastcancer: an overview of the randomised tri-als. Early Breast Cancer Trialists'Collaborative Group. Lancet 351: 1451-1467. 11. Anon. (1999). Cancer risks in BRCA2mutation carriers. The Breast CancerLinkage Consortium. J Natl Cancer Inst 91:1310-1316.
1 2 . Aaltonen LA, Salovaara R, Kristo P, CanzianF, Hemminki A, Peltomaki P, Chadwick RB,Kaariainen H, Eskelinen M, Jarvinen H,Mecklin JP, de la CA (1998). Incidence ofhereditary nonpolyposis colorectal cancer andthe feasibility of molecular screening for thedisease. N Engl J Med 338: 1481-1487.
13. Aarnio M, Mecklin JP, Aaltonen LA,Nystrom-Lahti M, Jarvinen HJ (1995). Life-time risk of different cancers in hereditarynon-polyposis colorectal cancer (HNPCC)syndrome. Int J Cancer 64: 430-433.
1 4 . Aarnio M, Sankila R, Pukkala E,Salovaara R, Aaltonen LA, de la CA,Peltomaki P, Mecklin JP, Jarvinen HJ(1999). Cancer risk in mutation carriers ofDNA-mismatch-repair genes. Int J Cancer81: 214-218.
15. Aaro CA, Jacobson LJ, Soule EH (1963).Endocervical polyps. Obstet Gynecol 21:659-665.
16. Aas T, Borresen AL, Geisler S, Smith-Sorensen B, Johnsen H, Varhaug JE,Akslen LA, Lonning PE (1996). Specific P53mutations are associated with de novoresistance to doxorubicin in breast cancerpatients. Nat Med 2: 811-814.
1 7 . Abati AD, Kimmel M, Rosen PP (1990).Apocrine mammary carcinoma. A clinico-pathologic study of 72 cases. Am J ClinPathol 94: 371-377.
18. Abbondanzo SL, Seidman JD, LefkowitzM, Tavassoli FA, Krishnan J (1996). Primarydiffuse large B-cell lymphoma of thebreast. A clinicopathologic study of 31cases. Pathol Res Pract 192: 37-43.
19. Abbott TM, Hermann WJJr., Scully RE(1984). Ovarian fetiform teratoma(homunculus) in a 9-year-old girl. Int JGynecol Pathol 2: 392-402.
20. Abdul-Karim FW, Bazi TM, Sorensen K,Nasr MF (1987). Sarcoma of the uterinecervix: clinicopathologic findings in threecases. Gynecol Oncol 26: 103-111.
21. Abeler V, Nesland JM (1989). Alveolarsoft-part sarcoma in the uterine cervix.Arch Pathol Lab Med 113: 1179-1183.
2 2 . Abeler VM, Holm R, Nesland JM,Kjorstad KE (1994). Small cell carcinoma ofthe cervix. A clinicopathologic study of 26patients. Cancer 73: 672-677.
23. Abeler VM, Kjorstad KE, Nesland JM(1991). Undifferentiated carcinoma of theendometrium. A histopathologic and clini-cal study of 31 cases. Cancer 68: 98-105.
24. Abeler VM, Vergote IB, Kjorstad KE,Trope CG (1996). Clear cell carcinoma ofthe endometrium. Prognosis and metastat-ic pattern. Cancer 78: 1740-1747.
25. Abell MR, Ramirez JA (1973). Sarcomasand carcinosarcomas of the uterine cervix.Cancer 31: 1176-1192.
26. Abeln EC, Smit VT, Wessels JW, deLeeuw WJ, Cornelisse CJ, Fleuren GJ(1997). Molecular genetic evidence for theconversion hypothesis of the origin ofmalignant mixed mullerian tumours. JPathol 183: 424-431.
2 7 . Abner AL, Collins L, Peiro G, Recht A,Come S, Shulman LN, Silver B, Nixon A, HarrisJR, Schnitt SJ, Connolly JL (1998). Correlationof tumor size and axillary lymph node involve-ment with prognosis in patients with T1 breastc a r c i n o m a . Cancer 83: 2502-2508. 28. Aboumrad MH, Horn RC, Fine G (1963).Lipid-secreting mammary carcinoma.Cancer 16: 521-525. 29. Abrams J, Talcott J, Corson JM (1989).Pulmonary metastases in patients withlow-grade endometrial stromal sarcoma.Clinicopathologic findings with immuno-histochemical characterization. Am J SurgPathol 13: 133-140. 30. Acharya S, Wilson T, Gradia S, KaneMF, Guerrette S, Marsischky GT, KolodnerR, Fishel R (1996). hMSH2 forms specificmispair-binding complexes with hMSH3and hMSH6. Proc Natl Acad Sci USA 93:13629-13634. 3 1 . Ackerman AB, Mihara I (1985).Dysplasia, dysplastic melanocytes, dys-plastic nevi, the dysplastic nevus syn-drome, and the relation between dysplas-tic nevi and malignant melanomas. HumPathol 16: 87-91.32. Ackerman LV, Katzenstein AL (1977).The concept of minimal breast cancer andthe pathologist's role in the diagnosis of"early carcinoma". Cancer 39: 2755-2763. 33. Acosta-Sison H (1970). Chorioadenomadestruens. A report of 41 case. Am JObstet Gynecol 80: 176. 34. Acs G, Lawton TJ, Rebbeck TR, LiVolsiVA, Zhang PJ (2001). Differential expres-sion of E-cadherin in lobular and ductalneoplasms of the breast and its biologicand diagnostic implications. Am J ClinPathol 115: 85-98. 3 5 . Adami HO, Bergstrom R, Hansen J(1985). Age at first primary as a determi-nant of the incidence of bilateral breastcancer. Cumulative and relative risks in apopulation-based case-control study.Cancer 55: 643-647. 36. Adami HO, Signorello LB, TrichopoulosD (1998). Towards an understanding ofbreast cancer etiology. Semin Cancer Biol8: 255-262. 37. Adami HO, Sparen P, Bergstrom R,Holmberg L, Krusemo UB, Ponten J (1989).Increasing survival trend after cancerdiagnosis in Sweden: 1960-1984. J NatlCancer Inst 81: 1640-1647. 38. Adashi EY, Rosenshein NB, Parmley TH,Woodruff JD (1980). Histogenesis of thebroad ligament adrenal rest. Int JGynaecol Obstet 18: 102-104. 39. Adeniji KA, Adelusola KA, OdesanmiWO, Fadiran OA (1997). Histopathologicalanalysis of carcinoma of the male breast inIle-Ife, Nigeria. East Afr Med J 74: 455-457.
4 0 . Adeyinka A, Mertens F, Idvall I,Bondeson L, Ingvar C, Heim S, Mitelman F,Pandis N (1998). Cytogenetic findings ininvasive breast carcinomas with prognos-tically favourable histology: a less complexkaryotypic pattern? Int J Cancer 79: 361-364. 41. Adnane J, Gaudray P, Dionne CA,Crumley G, Jaye M, Schlessinger J, JeanteurP, Birnbaum D, Theillet C (1991). BEK andFLG, two receptors to members of the FGFfamily, are amplified in subsets of humanbreast cancers. Oncogene 6: 659-663. 4 2 . Agathanggelou A, Honorio S,Macartney DP, Martinez A, Dallol A, RaderJ, Fullwood P, Chauhan A, Walker R, ShawJA, Hosoe S, Lerman MI, Minna JD, MaherER, Latif F (2001). Methylation associatedinactivation of RASSF1A from region3p21.3 in lung, breast and ovarian tumours.Oncogene 20: 1509-1518. 4 3 . Agnarsson BA, Jonasson JG,Bjornsdottir IB, Barkardottir RB, EgilssonV, Sigurdsson H (1998). Inherited BRCA2mutation associated with high gradebreast cancer. Breast Cancer Res Treat 47:121-127. 44. Agoff SN, Grieco VS, Garcia R, GownAM (2001). Immunohistochemical distinc-tion of endometrial stromal sarcoma andcellular leiomyoma. Appl Immunohis-tochem Mol Morphol 9: 164-169. 45. Aguirre P, Scully RE, Wolfe HJ, DeLellisRA (1986). Argyrophil cells in Brennertumors: histochemical and immunohisto-chemical analysis. Int J Gynecol Pathol 5:223-234. 46. Aguirre P, Thor AD, Scully RE (1989).Ovarian small cell carcinoma. Histogeneticconsiderations based on immunohisto-chemical and other findings. Am J ClinPathol 92: 140-149. 47. Ahern JK, Allen NH (1978). Cervicalhemangioma: a case report and review ofthe literature. J Reprod Med 21: 228-231. 48. Ahmed AA, Swan RW, Owen A, KrausFT, Patrick F (1997). Uterus-like mass aris-ing in the broad ligament: a metaplasia ormullerian duct anomaly? Int J GynecolPathol 16: 279-281. 49. Aho M, Vesterinen E, Meyer B, PurolaE, Paavonen J (1991). Natural history ofvaginal intraepithelial neoplasia. Cancer68: 195-197. 50. Aida H, Takakuwa K, Nagata H, TsunekiI, Takano M, Tsuji S, Takahashi T, SonodaT, Hatae M, Takahashi K, Hasegawa K,Mizunuma H, Toyoda N, Kamata H, Torii Y,Saito N, Tanaka K, Yakushiji M, Araki T,Tanaka K (1998). Clinical features of ovari-an cancer in Japanese women with germ-line mutations of BRCA1. Clin Cancer Res4: 235-240. 5 1 . AJCC (2002). AJCC Cancer StagingManual. Sixth ed. Springer Verlag: NewYork.
References

373References
52. Akhtar M, Robinson C, Ashraf Ali M,Godwin JT (1983). Secretory carcinoma ofthe breast in adults. Cancer 51: 2245-2254. 53. Akiyama Y, Sato H, Yamada T, NagasakiH, Tsuchiya A, Abe R, Yuasa Y (1997).Germ-line mutation of the hMSH6/GTBPgene in an atypical hereditary nonpolypo-sis colorectal cancer kindred. Cancer Res57: 3920-3923. 54. Al Jafari MS, Panton HM, Gradwell E(1985). Phaeochromocytoma of the broadligament. Case report. Br J ObstetGynaecol 92: 649-651. 5 5 . Al Kurdi M, Monaghan JM (1981).Thirty-two years experience in manage-ment of primary tumours of the vagina. BrJ Obstet Gynaecol 88: 1145-1150. 56. Al Nafussi AI, Al Yusif R (1998). Papillarysquamotransitional cell carcinoma of theuterine cervix: an advanced stage diseasedespite superficial location: report of twocases and review of the literature. Eur JGynaecol Oncol 19: 455-457. 5 7 . Al Nafussi AI, Hughes DE (1994).Histological features of CIN3 and theirvalue in predicting invasive microinvasivesquamous carcinoma. J Clin Pathol 47:799-804. 5 8 . Alamowitch B, Mausset V, Ruiz A,Tissier F, Fourmestraux J, Bouillot JL,Bethoux JP (1999). [Non-secretingpheochromocytoma of the broad ligamentrevealed by appendicular peritonitis].Presse Med 28: 225-228. 59. Albain KS, Allred DC, Clark GM (1994).Breast cancer outcome and predictors ofoutcome: are there age differentials? JNatl Cancer Inst Monogr 35-42. 60. Albertson DG, Ylstra B, Segraves R,Collins C, Dairkee SH, Kowbel D, Kuo WL,Gray JW, Pinkel D (2000). Quantitativemapping of amplicon structure by arrayCGH identifies CYP24 as a candidate onco-gene. Nat Genet 25: 144-146. 6 1 . Albonico G, Querzoli P, Ferretti S,Rinaldi R, Nenci I (1996). Biological hetero-geneity of breast carcinoma in situ. Ann NY Acad Sci 784: 458-461. 6 2 . Albonico G, Querzoli P, Ferretti S,Rinaldi R, Nenci I (1998). Biological profileof in situ breast cancer investigated byimmunohistochemical technique. CancerDetect Prev 22: 313-318. 6 3 . Albores-Saavedra J, Gersell D, GilksCB, Henson DE, Lindberg G, Santiago H,Scully RE, Silva E, Sobin LH, Tavassoli FJ,Travis WD, Woodruff JM (1997).Terminology of endocrine tumors of theuterine cervix: results of a workshopsponsored by the College of AmericanPathologists and the National CancerI n s t i t u t e . Arch Pathol Lab Med 121: 34-39. 6 4 . Albores-Saavedra J, Gilcrease M(1999). Glomus tumor of the uterine cervix.Int J Gynecol Pathol 18: 69-72. 65. Albores-Saavedra J, Manivel C, MoraA, Vuitch F, Milchgrub S, Gould E (1992).The solid variant of adenoid cystic carci-noma of the cervix. Int J Gynecol Pathol11:2-10. 66. Albores-Saavedra J, Young RH (1995).Transitional cell neoplasms (carcinomasand inverted papillomas) of the uterinecervix. A report of five cases. Am J SurgPathol 19: 1138-1145. 67. Alderson MR, Hamlin I, Staunton MD(1971). The relative significance of prog-nostic factors in breast carcinoma. Br JCancer 25: 646-656.
68. Alfsen GC, Kristensen GB, Skovlund E,Pettersen EO, Abeler VM (2001). Histologicsubtype has minor importance for overallsurvival in patients with adenocarcinomaof the uterine cervix: a population-basedstudy of prognostic factors in 505 patientswith nonsquamous cell carcinomas of thecervix. Cancer 92: 2471-2483. 6 9 . Alizadeh AA, Ross DT, Perou CM, van deRijn M (2001). Towards a novel classifica-tion of human malignancies based on geneexpression patterns. J Pathol 195: 41-52. 7 0 . Allaire AD, Majmudar B (1993).Dracunculosis of the broad ligament. Acase of a "parasitic leiomyoma". Am J SurgPathol 17: 937-940. 71. Allred DC, Elledge RM (1999). Cautionconcerning micrometastatic breast carci-noma in sentinel lymph nodes. Cancer 86:905-907. 72. Allred DC, Mohsin SK, Fuqua SA (2001).Histological and biological evolution ofhuman premalignant breast disease.Endocr Relat Cancer 8: 47-61. 7 3 . Altaras MM, Jaffe R, Corduba M,Holtzinger M, Bahary C (1990). Primaryparaovarian cystadenocarcinoma: clinicaland management aspects and literaturereview. Gynecol Oncol 38: 268-272. 7 4 . Alvarado-Cabrero I, Navani SS, YoungRH, Scully RE (1997). Tumors of the fimbriatedend of the fallopian tube: a clinicopathologicanalysis of 20 cases, including nine carcino-m a s . Int J Gynecol Pathol 16: 189-196. 7 5 . Alvarado-Cabrero I, Young RH,Vamvakas EC, Scully RE (1999). Carcinomaof the fallopian tube: a clinicopathologicalstudy of 105 cases with observations onstaging and prognostic factors. GynecolOncol 72: 367-379. 7 6 . Alvarez-Fernandez E, Salinero-Paniagua E (1981). Vascular tumors of themammary gland. A histochemical andultrastructural study. Virchows Arch APathol Anat Histol 394: 31-47. 77. Amant F, Moerman P, Davel GH, De VosR, Vergote I, Lindeque BG, de Jonge E(2001). Uterine carcinosarcoma withmelanocytic differentiation. Int J GynecolPathol 20: 186-190. 7 8 . Ambros RA, Kurman RJ (1992).Combined assessment of vascular andmyometrial invasion as a model to predictprognosis in stage I endometrioid adeno-carcinoma of the uterine corpus. Cancer69: 1424-1431. 79. Ambros RA, Sherman ME, Zahn CM,Bitterman P, Kurman RJ (1995).Endometrial intraepithelial carcinoma: adistinctive lesion specifically associatedwith tumors displaying serous differentia-tion. Hum Pathol 26: 1260-1267. 80. American Joint Committee on Cancer(1997). AJCC Cancer Staging Manual. 5thed. Lippincott-Raven: Philadelphia.81. Amr SS, Elmallah KO (1995). Agressive
angiomyxoma of the vagina. Int JGynaecol Obstet 42: 207-210. 8 2 . Anan K, Mitsuyama S, Tamae K,Nishihara K, Iwashita T, Abe Y, Ihara T,Nakahara S, Katsumoto F, Toyoshima S(2001). Pathological features of mucinouscarcinoma of the breast are favourable forbreast-conserving therapy. Eur J SurgOncol 27: 459-463. 8 3 . Anand S, Penrhyn-Lowe S,Venkitaraman AR (2003). AURORA-A ampli-fication overrides the mitotic spindleassembly checkpoint, inducing resistanceto Taxol. Cancer Cell 3: 51-62.
8 4 . Anastassiades OT, Bouropoulou V,Kontogeorgos G, Tsakraklides EV (1979).Duct elastosis in infiltrating carcinoma ofthe breast. Pathol Res Pract 165: 411-421. 85. Anbazhagan R, Fujii H, Gabrielson E(1999). Microsatellite instability is uncom-mon in breast cancer. Clin Cancer Res 5:839-844. 86. Andersen JA (1974). Lobular carcinomain situ of the breast with ductal involve-ment. Frequency and possible influence onprognosis. Acta Pathol Microbiol Scand[A] 82: 655-662. 87. Andersen JA (1974).Lobular carcinoma in situ. A histologicstudy of 52 cases. Acta Pathol MicrobiolScand [A] 82: 735-741. 88. Andersen JA (1974). Lobular carcinomain situ. A long-term follow-up in 52 cases.Acta Pathol Microbiol Scand [A] 82: 519-533.89. Andersen JA, Vendelboe ML (1981).Cytoplasmic mucous globules in lobularcarcinoma in situ. Diagnosis and progno-sis. Am J Surg Pathol 5: 251-255. 9 0 . Anderson B, Turner DA, Benda J (1987).Ovarian sarcoma. Gynecol Oncol 26: 183-192. 9 1 . Anderson BO, Petrek JA, Byrd DR,Senie RT, Borgen PI (1996). Pregnancyinfluences breast cancer stage at diagno-sis in women 30 years of age and younger.Ann Surg Oncol 3: 204-211. 92. Anderson C, Ricci A Jr., Pedersen CA,Cartun RW (1991). Immunocytochemicalanalysis of estrogen and progesteronereceptors in benign stromal lesions of thebreast. Evidence for hormonal etiology inpseudoangiomatous hyperplasia of mam-mary stroma. Am J Surg Pathol 15: 145-149. 92a. Anderson DE (1971). Some character-istics of familial breast cancer. Cancer 28:1500-1504. 93. Anderson DE (1974). Genetic study ofbreast cancer: identification of a high riskgroup. Cancer 34: 1090-1097. 9 4 . Anderson DE, Badzioch MD (1992).Breast cancer risks in relatives of malebreast cancer patients. J Natl Cancer Inst84: 1114-1117. 9 5 . Anderson DE, Badzioch MD (1993).Familial effects of prostate and other can-cers on lifetime breast cancer risk. BreastCancer Res Treat 28: 107-113. 9 6 . Anderson MC, Rees DA (1975).Gynandroblastoma of the ovary. Br JObstet Gynaecol 82: 68-73. 9 7 . Anderson TJ, Lamb J, Donnan P,Alexander FE, Huggins A, Muir BB,Kirkpatrick AE, Chetty U, Hepburn W, SmithA, Prescott RJ, Forrest P. (1991).Comparative pathology of breast cancer ina randomised trial of screening. Br JCancer 64: 108-113. 98. Andrac-Meyer L, Solere K, Sappa P,Garcia S, Charpin C (2000). [Infiltratingsyringoadenoma of the nipple: a newcase]. Ann Pathol 20: 142-144. 99. Andrassy RJ, Wiener ES, Raney RB,Hays DM, Arndt CA, Lobe TE, Lawrence W,Anderson JR, Qualman SJ, Crist WM(1999). Progress in the surgical manage-ment of vaginal rhabdomyosarcoma: a 25-year review from the IntergroupRhabdomyosarcoma Study Group. JPediatr Surg 34: 731-734. 100. Andreasson B, Bock JE, Strom KV,Visfeldt J (1983). Verrucous carcinoma ofthe vulval region. Acta Obstet GynecolScand 62: 183-186.
1 0 1 . Angele S, Lauge A, Fernet M, MoullanN, Beauvais P, Couturier J, Stoppa-LyonnetD, Hall J (2003). Phenotypic cellular charac-terization of an ataxia telangiectasiapatient carrying a causal homozygous mis-sense mutation. Hum Mutat 21: 169-170. 1 0 2 . Angele S, Treilleux I, Taniere P,Martel-Planche G, Vuillaume M, Bailly C,Bremond A, Montesano R, Hall J (2000).Abnormal expression of the ATM and TP53genes in sporadic breast carcinomas. ClinCancer Res 6: 3536-3544. 103. Ansah-Boateng Y, Wells M, Poole DR(1985). Coexistent immature teratoma ofthe uterus and endometrial adenocarcino -ma complicated by gliomatosis peritonei.Gynecol Oncol 21: 106-110. 1 0 4 . Anteby EY, Ron M, Revel A,Shimonovitz S, Ariel I, Hurwitz A (1994).Germ cell tumors of the ovary arising afterdermoid cyst resection: a long-term fol-low-up study. Obstet Gynecol 83: 605-608. 1 0 5 . Anthony PP, James PD (1975).Adenoid cystic carcinoma of the breast:prevalence, diagnostic criteria, and histo-genesis. J Clin Pathol 28: 647-655. 106. Antoniou A, Pharoah PD, Narod S,Risch HA, Eyfjord JE, Hopper JL, Loman N,Olsson H, Johannsson O, Borg A, Pasini B,Radice P, Manoukian S, Eccles DM, TangN, Olah E, Anton-Culver H, Warner E,Lubinski J, Gronwald J, Gorski B, TuliniusH, Thorlacius S, Eerola H, Nevanlinna H,Syrjakoski K, Kallioniemi OP, Thompson D,Evans C, Peto J, Lalloo F, Evans DG, EastonDF (2003). Average risks of breast andovarian cancer associated with BRCA1 orBRCA2 mutations detected in case seriesunselected for family history: a combinedanalysis of 22 studies. Am J Hum Genet 72:1117-1130. 107. Antoniou AC, Pharoah PD, McMullanG, Day NE, Ponder BA, Easton D (2001).Evidence for further breast cancer sus-ceptibility genes in addition to BRCA1 andBRCA2 in a population-based study. GenetEpidemiol 21: 1-18. 108. Anttila T, Saikku P, Koskela P, BloiguA, Dillner J, Ikaheimo I, Jellum E, LehtinenM, Lenner P, Hakulinen T, Narvanen A,Pukkala E, Thoresen S, Youngman L,Paavonen J (2001). Serotypes of Chlamydiatrachomatis and risk for development ofcervical squamous cell carcinoma. JAMA285: 47-51. 109. Anzick SL, Kononen J, Walker RL,Azorsa DO, Tanner MM, Guan XY, SauterG, Kallioniemi OP, Trent JM, Meltzer PS(1997). AIB1, a steroid receptor coactivatoramplified in breast and ovarian cancer.Science 277: 965-968. 110. Aoyama C, Peters J, Senadheera S,Liu P, Shimada H (1998). Uterine cervicaldysplasia and cancer: identification of c-myc status by quantitative polymerasechain reaction. Diagn Mol Pathol 7: 324-330. 111. Aoyama T, Mizuno T, Andoh K, TakagiT, Mizuno T, Eimoto T (1996). alpha-Fetoprotein-producing (hepatoid) carcino-ma of the fallopian tube. Gynecol Oncol 63:261-266. 1 1 2 . Aozasa K, Ito H, Kohro T, Ha K,Nakamura M, Okada A (1981). Chorio-car-cinoma in infant and mother. Acta PatholJpn 31: 317-322. 1 1 3 . Aozasa K, Ohsawa M, Saeki K,Horiuchi K, Kawano K, Taguchi T (1992).Malignant lymphoma of the breast.Immunologic type and association withlymphocytic mastopathy. Am J Clin Pathol97: 699-704.

374 References
1 1 4 . Aozasa K, Saeki K, Ohsawa M,Horiuchi K, Mishima K, Tsujimoto M (1993).Malignant lymphoma of the uterus. Reportof seven cases with immunohistochemicalstudy. Cancer 72: 1959-1964. 115. Appleby JM, Barber JB, Levine E,Varley JM, Taylor AM, Stankovic T,Heighway J, Warren C, Scott D (1997).Absence of mutations in the ATM gene inbreast cancer patients with severeresponses to radiotherapy. Br J Cancer 76:1546-1549. 1 1 6 . Arbabi L, Warhol MJ (1982).Pleomorphic liposarcoma following radio-therapy for breast carcinoma. Cancer 49:878-880. 117. Arber DA, Simpson JF, Weiss LM,Rappaport H (1994). Non-Hodgkin's lym-phoma involving the breast. Am J SurgPathol 18: 288-295. 118. Arias-Stella J Jr., Rosen PP (1988).Hemangiopericytoma of the breast. ModPathol 1: 98-103. 119. Ariel IM, Kempner R (1989). The prog-nosis of patients who become pregnantafter mastectomy for breast cancer. IntSurg 74: 185-187. 1 2 0 . Ariyoshi K, Kawauchi S, Kaku T,Nakano H, Tsuneyoshi M (2000).Prognostic factors in ovarian carcinosar-coma: a clinicopathological and immuno-histochemical analysis of 23 cases.Histopathology 37: 427-436. 121. Armes JE, Egan AJ, Southey MC, DiteGS, McCredie MR, Giles GG, Hopper JL,Venter DJ (1998). The histologic pheno-types of breast carcinoma occurringbefore age 40 years in women with andwithout BRCA1 or BRCA2 germline muta-tions: a population-based study. Cancer 83:2335-2345. 122. Aron DC, Marks WM, Alper PR, KaramJH (1980). Pheochromocytoma of thebroad ligament. Localization by computer-ized tomography and ultrasonography.Arch Intern Med 140: 550-552. 1 2 3 . Arora DS, Haldane S (1996).Carcinosarcoma arising in a dermoid cystof the ovary. J Clin Pathol 49: 519-521. 124. Arroyo JG, Harris W, Laden SA (1998).Recurrent mixed germ cell-sex cord-stro-mal tumor of the ovary in an adult. Int JGynecol Pathol 17: 281-283. 1 2 5 . Asgeirsson KS, Jonasson JG,Tryggvadottir L, Olafsdottir K,Sigurgeirsdottir JR, Ingvarsson S,Ogmundsdottir HM (2000). Altered expres-sion of E-cadherin in breast cancer: pat-terns, mechanisms and clinical signifi-cance. Eur J Cancer 36: 1098-1106. 1 2 6 . Ashikari R, Huvos AG, Urban JA,Robbins GF (1973). Infiltrating lobular car-cinoma of the breast. Cancer 31: 110-116. 127. Aslani M, Ahn GH, Scully RE (1988).Serous papillary cystadenoma of border-line malignancy of broad ligament. A reportof 25 cases. Int J Gynecol Pathol 7: 131-138. 127a. Aslani M, Scully RE (1989). Primarycarcinoma of the broad ligament. Report offour cases and review of the literature.Cancer 64: 1540-1545. 128. Athale UH, Shurtleff SA, Jenkins JJ,Poquette CA, Tan M, Downing JR, PappoAS (2001). Use of reverse transcriptasepolymerase chain reaction for diagnosisand staging of alveolar rhabdomyosarco-ma, Ewing sarcoma family of tumors, anddesmoplastic small round cell tumor. Am JPediatr Hematol Oncol 23: 99-104.
129. Athma P, Rappaport R, Swift M (1996).Molecular genotyping shows that ataxia-telangiectasia heterozygotes are predis-posed to breast cancer. Cancer GenetCytogenet 92: 130-134. 1 3 0 . Atkins K, Bell S, Kempson R,Hendrickson M (2001). Epithelioid smoothmuscle tumors of the uterus. M o d e r nPathol 14: 132A. 1 3 1 . Atkins K, Bell S, Kempson R,Hendrickson M (2001). Myxoid smoothmuscle tumors of the uterus. M o d e r nPathol 14: 132A. 132. Atlas I, Gajewski W, Falkenberry S,Granai CO, Steinhoff MM (1998). Absenceof estrogen and progesterone receptors inglassy cell carcinoma of the cervix. ObstetGynecol 91: 136-138. 133. Atri M, Nazarnia S, Aldis AE, ReinholdC, Bret PM, Kintzen G (1994). TransvaginalUS appearance of endometrial abnormali-ties. Radiographics 14: 483-492. 134. Aubele M, Mattis A, Zitzelsberger H,Walch A, Kremer M, Welzl G, Hofler H,Werner M (2000). Extensive ductal carci-noma In situ with small foci of invasiveductal carcinoma: evidence of geneticresemblance by CGH. Int J Cancer 85: 82-86. 1 3 5 . Aubele M, Werner M (1999).Heterogeneity in breast cancer and theproblem of relevance of findings. Anal CellPathol 19: 53-58. 136. Aubele MM, Cummings MC, MattisAE, Zitzelsberger HF, Walch AK, Kremer M,Hofler H, Werner M (2000). Accumulationof chromosomal imbalances from intra-ductal proliferative lesions to adjacent insitu and invasive ductal breast cancer.Diagn Mol Pathol 9: 14-19. 137. Aure JC, Høeg K, Kolstad P (1971).Clinical and histologic studies of ovariancarcinoma. Long-term follow-up of 990cases. Obstet Gynecol 37: 1-9. 1 3 8 . Austin RM, Dupree WB (1986).Liposarcoma of the breast: a clinicopatho -logic study of 20 cases. Hum Pathol 17:906-913. 1 3 9 . Austin RM, Norris HJ (1987).Malignant Brenner tumor and transitionalcell carcinoma of the ovary: a comparison.Int J Gynecol Pathol 6: 29-39. 140. Avinoach I, Zirkin HJ, Glezerman M(1989). Proliferating trichilemmal tumor ofthe vulva. Case report and review of the lit-erature. Int J Gynecol Pathol 8: 163-168. 1 4 1 . Axe S, Parmley T, Woodruff JD,Hlopak B (1986). Adenomas in minorvestibular glands. Obstet Gynecol 68: 16-18. 142. Axe SR, Klein VR, Woodruff JD (1985).Choriocarcinoma of the ovary. O b s t e tGynecol 66: 111-114. 143. Axiotis CA, Lippes HA, Merino MJ,deLanerolle NC, Stewart AF, Kinder B(1987). Corticotroph cell pituitary adenomawithin an ovarian teratoma. A new causeof Cushing's syndrome. Am J Surg Pathol11: 218-224. 144. Aziz S, Kuperstein G, Rosen B, Cole D,Nedelcu R, McLaughlin J, Narod SA (2001).A genetic epidemiological study of carci-noma of the fallopian tube. Gynecol Oncol80: 341-345. 1 4 5 . Azoury RS, Woodruff JD (1971).Primary ovarian sarcomas. Report of 43cases from the Emil Novak Ovarian TumorRegistry. Obstet Gynecol 37: 920-941.
146. Azuma C, Saji F, Tokugawa Y, KimuraT, Nobunaga T, Takemura M, Kameda T,Tanizawa O (1991). Application of geneamplification by polymerase chain reac-tion to genetic analysis of molar mitochon-drial DNA: the detection of anuclear emptyovum as the cause of complete mole.Gynecol Oncol 40: 29-33. 1 4 7 . Azzopardi AG (1979). Problems inBreast Pathology. Classification of PrimaryBreast Carcinoma. AG Azzopardi (Ed.) WBSaunders: Philadelphia.148. Azzopardi JG (1979). Papilloma andpapillary carcinoma. In: Problems inBreast Pathology. JG Azzopardi (Ed.) WBSaunders: London, pp. 150-166.149. Azzopardi JG, Ahmed A, Millis RR(1979). Problems in Breast Pathology. AGAzzopardi (Ed.) WB Saunders:London/Philadelphia.1 5 0 . Azzopardi JG, Eusebi V (1977).Melanocyte colonization and pigmentationof breast carcinoma. Histopathology 1: 21-30. 151. Azzopardi JG, Salm R (1984). Ductaladenoma of the breast: a lesion which canmimic carcinoma. J Pathol 144: 15-23. 1 5 2 . Azzopardi JG, Smith, OD (1959).Salivary gland tumours and their mucins.J Pathol Bacteriol 77: 131-140. 1 5 3 . Baak JP, Nauta JJ, Wisse-Brekelmans EC, Bezemer PD (1988).Architectural and nuclear morphometricalfeatures together are more importantprognosticators in endometrial hyper-plasias than nuclear morphometrical fea-tures alone. J Pathol 154: 335-341. 154. Baak JP, Orbo A, van Diest PJ, JiwaM, de Bruin P, Broeckaert M, Snijders W,Boodt PJ, Fons G, Burger C, Verheijen RH,Houben PW, The HS, Kenemans P (2001).Prospective multicenter evaluation of themorphometric D-score for prediction of theoutcome of endometrial hyperplasias. AmJ Surg Pathol 25: 930-935. 155. Babin EA, Davis JR, Hatch KD, HallumAV III (2000). Wilms' tumor of the cervix: acase report and review of the literature.Gynecol Oncol 76: 107-111. 1 5 6 . Bacus SS, Zelnick CR, Chin DM,Yarden Y, Kaminsky DB, Bennington J,Wen D, Marcus JN, Page DL (1994).Medullary carcinoma is associated withexpression of intercellular adhesion mole-cule-1. Implication to its morphology andits clinical behavior. Am J Pathol 145: 1337-1348. 1 5 7 . Badve S, Sloane JP (1995).Pseudoangiomatous hyperplasia of malebreast. Histopathology 26: 463-466. 158. Baekelandt M, Jorunn NA, KristensenGB, Trope CG, Abeler VM (2000).Carcinoma of the fallopian tube. Cancer 89:2076-2084. 1 5 9 . Baer R, Ludwig T (2002). TheBRCA1/BARD1 heterodimer, a tumor sup-pressor complex with ubiquitin E3 ligaseactivity. Curr Opin Genet Dev 12: 86-91. 160. Baergen RN, Warren CD, Isacson C,Ellenson LH (2001). Early uterine serouscarcinoma: clonal origin of extrauterinedisease. Int J Gynecol Pathol 20: 214-219. 161. Bagshawe KD, Dent J, Webb J (1986).Hydatidiform mole in England and Wales1973-83. Lancet 2: 673-677. 162. Bagshawe KD, Rawlins G, Pike MC,Lawler SD (1971). ABO blood-groups in tro-phoblastic neoplasia. Lancet 1: 553-556.
163. Bague S, Rodriguez IM, Prat J (2002).Sarcoma-like mural nodules in mucinouscystic tumors of the ovary revisited: a clin-icopathologic analysis of 10 additionalcases. Am J Surg Pathol 26: 1467-1476. 164. Bailey MJ, Royce C, Sloane JP, FordHT, Powles TJ, Gazet JC (1980). Bilateralcarcinoma of the breast. Br J Surg 67: 514-516. 165. Baker BA, Frickey L, Yu IT, HawkinsEP, Cushing B, Perlman EJ (1998). DNAcontent of ovarian immature teratomasand malignant germ cell tumors. GynecolOncol 71: 14-18. 1 6 6 . Baker PM, Oliva E, Young RH,Talerman A, Scully RE (2001). Ovarianmucinous carcinoids including some witha carcinomatous component: a report of 17cases. Am J Surg Pathol 25: 557-568. 167. Baker RJ, Hildebrandt RH, Rouse RV,Hendrickson MR, Longacre TA (1999).Inhibin and CD99 (MIC2) expression inuterine stromal neoplasms with sex-cord-like elements. Hum Pathol 30: 671-679. 168. Bakri Y, Berkowitz RS, Goldstein DP,Subhi J, Senoussi M, von Sinner W,Jabbar FA (1994). Brain metastases of ges-tational trophoblastic tumor. J ReprodMed 39: 179-184. 1 6 9 . Balasa RW, Adcock LL, Prem KA,Dehner LP (1977). The Brenner tumor: aclinicopathologic review. Obstet Gynecol50: 120-128. 170. Balat O, Balat A, Verschraegen C,Tornos C, Edwards CL (1996). Sarcomabotryoides of the uterine endocervix: long-term results of conservative surgery. Eur JGynaecol Oncol 17: 335-337. 1 7 1 . Ball HG, Berman ML (1982).Management of primary vaginal carcino-ma. Gynecol Oncol 14: 154-163. 172. Ballance WA, Ro JY, el Naggar AK,Grignon DJ, Ayala AG, Romsdahl MG(1990). Pleomorphic adenoma (benignmixed tumor) of the breast. An immunohis-tochemical, flow cytometric, and ultra-structural study and review of the litera-ture. Am J Clin Pathol 93: 795-801. 173. Ballerini P, Recchione C, Cavalleri A,Moneta R, Saccozzi R, Secreto G (1990).Hormones in male breast cancer. Tumori76: 26-28. 174. Balzi D, Buiatti E, Geddes M, Khlat M,Masuyer E, Parkin DM (1993). Summary ofthe results by site. In: Cancer in ItalianMigrant Populations, IARC ScientificPublication No 123, International Agencyfor Research on Cancer: Lyon, pp. 193-292.175. Bandera CA, Muto MG, Schorge JO,Berkowitz RS, Rubin SC, Mok SC (1998).BRCA1 gene mutations in women withpapillary serous carcinoma of the peri-toneum. Obstet Gynecol 92: 596-600. 176. Bandera CA, Muto MG, Welch WR,Berkowitz RS, Mok SC (1998). Geneticimbalance on chromosome 17 in papillaryserous carcinoma of the peritoneum.Oncogene 16: 3455-3459. 177. Banik S, Bishop PW, Ormerod LP,O'Brien TE (1986). Sarcoidosis of thebreast. J Clin Pathol 39: 446-448. 178. Bannatyne P, Russell P (1981). Earlyadenocarcinoma of the fallopian tubes. Acase for multifocal tumorigenesis. DiagnGynecol Obstet 3: 49-60. 179. Bapat B, Xia L, Madlensky L, Mitri A,Tonin P, Narod SA, Gallinger S (1996). Thegenetic basis of Muir-Torre syndromeincludes the hMLH1 locus. Am J HumGenet 59: 736-739.

375References
180. Bapat K, Brustein S (1989). Uterinesarcoma with liposarcomatous differentia-tion: report of a case and review of the lit-erature. Int J Gynaecol Obstet 28: 71-75. 1 8 1 . Barlund M, Monni O, Kononen J,Cornelison R, Torhorst J, Sauter G,Kallioniemi OLLI, Kallioniemi A (2000).Multiple genes at 17q23 undergo amplifi-cation and overexpression in breast can-cer. Cancer Res 60: 5340-5344. 182. Baron JA (1984). Smoking and estro-gen-related disease. Am J Epidemiol 119:9-22. 183. Barrett TL, Smith KJ, Hodge JJ, ButlerR, Hall FW, Skelton HG (1997). Immunohis-tochemical nuclear staining for p53, PCNA,and Ki-67 in different histologic variants ofbasal cell carcinoma. J Am Acad Dermatol37: 430-437. 184. Barry TS, Schnitt SJ, Ellis I, Eusebi V,Gown AM (1999). Absence of myoepitheli-um in microglandular adenosis of thebreast confirmed with new myoepithelialmarkers. Lab Invest 79: 16A. 1 8 5 . Barter JF, Smith EB, Szpak CA,Hinshaw W, Clarke-Pearson DL, CreasmanWT (1985). Leiomyosarcoma of the uterus:clinicopathologic study of 21 cases.Gynecol Oncol 21: 220-227. 186. Barth RJ Jr. (1999). Histologic featurespredict local recurrence after breast con-serving therapy of phyllodes tumors.Breast Cancer Res Treat 57: 291-295. 186a. Barth A, Craig PH, Silverstein MJ(1997). Predictors of axillary lymph nodemetastases in patients with T1 breast car-cinoma. Cancer 79: 1918-1922. 187. Bartnik J, Powell WS, Moriber-Katz S,Amenta PS (1989). Metaplastic papillarytumor of the fallopian tube. Case report,immunohistochemical features, andreview of the literature. Arch Pathol LabMed 113: 545-547. 1 8 8 . Barwick KW, LiVolsi VA (1979).Heterologous mixed mullerian tumor con-fined to an endometrial polyp. O b s t e tGynecol 53: 512-514. 189. Barzilai A, Rotman G, Shiloh Y (2002).ATM deficiency and oxidative stress: anew dimension of defective response toDNA damage. DNA Repair (Amst) 1: 3-25. 190. Baschinsky DY, Niemann TH, EatonLA, Frankel WL (1999). Malignant mixedMullerian tumor with rhabdoid features: areport of two cases and a review of the lit-erature. Gynecol Oncol 73: 145-150. 1 9 1 . Bassler R, Katzer B (1992).Histopathology of myoepithelial (basocel-lular) hyperplasias in adenosis and epithe-liosis of the breast demonstrated by thereactivity of cytokeratins and S100 protein.An analysis of heterogenic cell prolifera-tions in 90 cases of benign and malignantbreast diseases. Virchows Arch A PatholAnat Histopathol 421: 435-442. 192. Bauer RD, McCoy CP, Roberts DK, FritzG (1984). Malignant melanoma metastaticto the endometrium. Obstet Gynecol 63:264-268. 193. Bayo S, Bosch FX, de Sanjose S,Munoz N, Combita AL, Coursaget P, DiazM, Dolo A, van den Brule AJ, Meijer CJ(2002). Risk factors of invasive cervicalcancer in Mali. Int J Epidemiol 31: 202-209. 194. Bebb DG, Yu Z, Chen J, Telatar M,Gelmon K, Phillips N, Gatti RA, GlickmanBW (1999). Absence of mutations in theATM gene in forty-seven cases of sporadicbreast cancer. Br J Cancer 80: 1979-1981.
195. Becker JL, Papenhausen PR, WidenRH (1997). Cytogenetic, morphologic andoncogene analysis of a cell line derivedfrom a heterologous mixed mullerian tumorof the ovary. In Vitro Cell Dev Biol Anim 33:325-331. 1 9 6 . Beckmann MW, Niederacher D,Schnurch HG, Gusterson BA, Bender HG(1997). Multistep carcinogenesis of breastcancer and tumour heterogeneity. J MolMed 75: 429-439. 197. Beerman H, Smit VT,Kluin PM, Bonsing BA, Hermans J,Cornelisse CJ (1991). Flow cytometricanalysis of DNA stemline heterogeneity inprimary and metastatic breast cancer.Cytometry 12: 147-154. 198. Begin LR, Clement PB, Kirk ME, JothyS, McCaughey WT, Ferenczy A (1985).Aggressive angiomyxoma of pelvic softparts: a clinicopathologic study of ninecases. Hum Pathol 16: 621-628. 1 9 9 . Beilby JO, Parkinson C (1975).Features of prognostic significance in solidovarian teratoma. Cancer 36: 2147-2154. 200. Bell DA (1991). Mucinous adenofibro-mas of the ovary. A report of 10 cases. AmJ Surg Pathol 15: 227-232. 201. Bell DA, Scully RE (1985). Atypical andborderline endometrioid adenofibromas ofthe ovary. A report of 27 cases. Am J SurgPathol 9: 205-214. 202. Bell DA, Scully RE (1985). Benign andborderline clear cell adenofibromas of theovary. Cancer 56: 2922-2931. 203. Bell DA, Scully RE (1990). Ovarianserous borderline tumors with stromalmicroinvasion: a report of 21 cases. HumPathol 21: 397-403. 204. Bell DA, Scully RE (1990). Serous bor-derline tumors of the peritoneum. Am JSurg Pathol 14: 230-239. 205. Bell DA, Scully RE (1994). Early denovo ovarian carcinoma. A study of four-teen cases. Cancer 73: 1859-1864. 206. Bell DA, Shimm DS, Gang DL (1985).Wilms' tumor of the endocervix. A r c hPathol Lab Med 109: 371-373. 207. Bell DA, Weinstock MA, Scully RE(1988). Peritoneal implants of ovarianserous borderline tumors. Histologic fea-tures and prognosis. Cancer 62: 2212-2222. 2 0 8 . Bell DA, Woodruff JM, Scully RE(1984). Ependymoma of the broad ligament.A report of two cases. Am J Surg Pathol 8:203-209. 209. Bell DW, Varley JM, Szydlo TE, KangDH, Wahrer DC, Shannon KE, LubratovichM, Verselis SJ, Isselbacher KJ, FraumeniJF, Birch JM, Li FP, Garber JE, Haber DA(1999). Heterozygous germ line hCHK2mutations in Li-Fraumeni syndrome.Science 286: 2528-2531. 210. Bell KA, Smith Sehdev AE, Kurman RJ(2001). Refined diagnostic criteria forimplants associated with ovarian atypicalproliferative serous tumors (borderline)and micropapillary serous carcinomas.Am J Surg Pathol 25: 419-432. 211. Bell SW, Kempson RL, HendricksonMR (1994). Problematic uterine smoothmuscle neoplasms. A clinicopathologicstudy of 213 cases. Am J Surg Pathol 18:535-558. 212. Ben David M, Dekel A, Gal R, Dicker D,Feldberg D, Goldman JA (1988). Prolapsedcervical leiomyosarcoma. Obstet GynecolSurv 43: 642-644.
2 1 3 . Ben David Y, Chetrit A, Hirsh-Yechezkel G, Friedman E, Beck BD, BellerU, Ben Baruch G, Fishman A, Levavi H,Lubin F, Menczer J, Piura B, Struewing JP,Modan B (2002). Effect of BRCA mutationson the length of survival in epithelial ovari -an tumors. J Clin Oncol 20: 463-466. 2 1 4 . Ben Ezra J, Sheibani K (1987).Antigenic phenotype of the lymphocyticcomponent of medullary carcinoma of thebreast. Cancer 59: 2037-2041. 2 1 5 . Benatar B, Wright C, Freinkel AL,Cooper K (1998). Primary extrarenal Wilms'tumor of the uterus presenting as a cervi-cal polyp. Int J Gynecol Pathol 17: 277-280. 2 1 6 . Benda JA, Platz CE, Anderson B(1986). Malignant melanoma of the vulva: aclinical-pathologic review of 16 cases. IntJ Gynecol Pathol 5: 202-216. 217. Benedet JL, Bender H, Jones H III,Ngan HY, Pecorelli S (2000). FIGO stagingclassifications and clinical practice guide-lines in the management of gynecologiccancers. FIGO Committee on GynecologicOncology. Int J Gynaecol Obstet 70: 209-262. 218. Benedet JL, Ehlen TG (2001). VulvarCancer In: Prognostic Factors in Cancer.MK Gospodarowicz, DE Henson, RV Hutter,B O'Sullivan, LH Oblin, CH Wittekink (Eds.)2nd ed. Willey- Liss: New York, pp. 489-500. 2 1 9 . Benedet JL, Miller DM, Ehlen TG,Bertrand MA (1997). Basal cell carcinomaof the vulva: clinical features and treat-ment results in 28 patients. Obstet Gynecol90: 765-768. 220. Benedet JL, Murphy KJ, Fairey RN,Boyes DA (1983). Primary invasive carcino-ma of the vagina. Obstet Gynecol 62: 715-719. 2 2 1 . Benedetti-Panici P, Maneschi F,D'Andrea G, Cutillo G, Rabitti C, Congiu M,Coronetta F, Capelli A (2000). Early cervicalcarcinoma: the natural history of lymphnode involvement redefined on the basis ofthorough parametrectomy and giant sec-tion study. Cancer 88: 2267-2274. 2 2 2 . Bennett HGJ, Ehrlich MM (1941).Myoma of the vagina. Am J ObstetGynecol 42: 314-320. 223. Bentz JS, Yassa N, Clayton F (1998).Pleomorphic lobular carcinoma of thebreast: clinicopathologic features of 12cases. Mod Pathol 11: 814-822. 224. Beral V (2002). Breast cancer andbreastfeeding: collaborative reanalysis ofindividual data from 47 epidemiologicalstudies in 30 countries, including 50302women with breast cancer and 96973women without the disease. Lancet 360:187-195. 225. Beral V, Banks E, Reeves G, Appleby P(1999). Use of HRT and the subsequent riskof cancer. J Epidemiol Biostat 4: 191-210. 226. Beral V, Hermon C, Munoz N, DevesaSS (1994). Cervical cancer. Cancer surv 19-20: 265-285. 227. Beral V, Reeves G (1993). Childbearing,oral contraceptive use, and breast cancer.Lancet 341: 1102. 228. Berchuck A, Boyd J (1995). Molecularbasis of endometrial cancer. Cancer 76:2034-2040. 229. Berchuck A, Heron KA, Carney ME,Lancaster JM, Fraser EG, Vinson VL,Deffenbaugh AM, Miron A, Marks JR,Futreal PA, Frank TS (1998). Frequency ofgermline and somatic BRCA1 mutations inovarian cancer. Clin Cancer Res 4: 2433-2437.
230. Berchuck A, Kohler MF, Marks JR,Wiseman R, Boyd J, Bast RC Jr. (1994). Thep53 tumor suppressor gene frequently isaltered in gynecologic cancers. Am JObstet Gynecol 170: 246-252. 231. Berchuck A, Rubin SC, Hoskins WJ,Saigo PE, Pierce VK, Lewis JL Jr. (1988).Treatment of uterine leiomyosarcoma.Obstet Gynecol 71: 845-850. 232. Berchuck A, Rubin SC, Hoskins WJ,Saigo PE, Pierce VK, Lewis JL Jr. (1990).Treatment of endometrial stromal tumors.Gynecol Oncol 36: 60-65. 233. Berean K, Tron VA, Churg A, ClementPB (1986). Mammary fibroadenoma withmultinucleated stromal giant cells. Am JSurg Pathol 10: 823-827. 234. Berek J, Adashi PA, Hillart PA (1996).Novak's Gynaecology. XII ed. Williams &Wilkins: Baltimore, Maryland.235. Berends MJ, Hollema H, Wu Y, Vander Sluis T, Mensink RG, ten Hoor KA,Sijmons RH, de Vries EG, Pras E, MouritsMJ, Hofstra RM, Buys CH, Kleibeuker JH,Der Zee AG (2001). MLH1 and MSH2 pro-tein expression as a pre-screening markerin hereditary and non-hereditary endome-trial hyperplasia and cancer. Int J Cancer92: 398-403. 236. Berends MJ, Wu Y, Sijmons RH,Mensink RG, Van Der Sluis T, Hordijk-HosJM, de Vries EG, Hollema H, Karrenbeld A,Buys CH, van der Zee AG, Hofstra RM,Kleibeuker JH (2002). Molecular and clini-cal characteristics of MSH6 variants: ananalysis of 25 index carriers of a germlinevariant. Am J Hum Genet 70: 26-37. 237. Berezowski K, Stastny JF, KornsteinMJ (1996). Cytokeratins 7 and 20 and carci-noembryonic antigen in ovarian andcolonic carcinoma. Mod Pathol 9: 426-429. 238. Bergeron C, Ferenczy A, Richart RM,Guralnick M (1990). Micropapillomatosislabialis appears unrelated to human papil-lomavirus. Obstet Gynecol 76: 281-286. 239. Bergeron C, Ferenczy A, Shah KV,Naghashfar Z (1987). Multicentric humanpapillomavirus infections of the femalegenital tract: correlation of viral types withabnormal mitotic figures, colposcopicpresentation, and location. Obstet Gynecol69: 736-742. 240. Bergeron C, Nogales FF, Masseroli M,Abeler V, Duvillard P, Muller-Holzner E,Pickartz H, Wells M (1999). A multicentricEuropean study testing the reproducibilityof the WHO classification of endometrialhyperplasia with a proposal of a simplifiedworking classification for biopsy andcurettage specimens. Am J Surg Pathol 23:1102-1108. 241. Bergh J, Norberg T, Sjogren S,Lindgren A, Holmberg L (1995). Completesequencing of the p53 gene provides prog-nostic information in breast cancerpatients, particularly in relation to adjuvantsystemic therapy and radiotherapy. NatMed 1: 1029-1034. 241a. Bergstrom A, Pisani P, Tenet V, WolkA, Adami HO (2001). Overweight as anavoidable cause of cancer in Europe. Int JCancer 91: 421-430. 242. Berkey CS, Frazier AL, Gardner JD,Colditz GA (1999). Adolescence and breastcarcinoma risk. Cancer 85: 2400-2409. 243. Berkowitz RS, Bernstein MR, LabordeO, Goldstein DP (1994). Subsequent preg-nancy experience in patients with gesta-tional trophoblastic disease. New EnglandTrophoblastic Disease Center, 1965-1992.J Reprod Med 39: 228-232.

376 References
244. Berkowitz RS, Cramer DW, BernsteinMR, Cassells S, Driscoll SG, Goldstein DP(1985). Risk factors for complete molarpregnancy from a case-control study. AmJ Obstet Gynecol 152: 1016-1020. 245. Berkowitz RS, Ehrmann RL, Knapp RC(1978). Endometrial stromal sarcoma aris-ing from vaginal endometriosis. O b s t e tGynecol 51: 34s-37s. 246. Berliant II (1970). [Neurofibroma of thebroad ligament of the uterus]. A k u s hGinekol (Mosk) 46: 70-71. 247. Berman ML, Soper JT, Creasman WT,Olt GT, Disaia PJ (1989). Conservative sur-gical management of superficially invasivestage I vulvar carcinoma. Gynecol Oncol35: 352-357. 248. Bermudez A, Vighi S, Garcia A, Sardi J(2001). Neuroendocrine cervical carcino-ma: a diagnostic and therapeutic chal-lenge. Gynecol Oncol 82: 32-39. 249. Berns EM, Foekens JA, Vossen R,Look MP, Devilee P, Henzen-Logmans SC,van Staveren IL, van Putten WL, InganasM, Meijer-van Gelder ME, Cornelisse C,Claassen CJ, Portengen H, Bakker B, KlijnJG (2000). Complete sequencing of TP53predicts poor response to systemic thera-py of advanced breast cancer. Cancer Res60: 2155-2162. 250. Berns EM, Klijn JG, van Putten WL,van Staveren IL, Portengen H, Foekens JA(1992). c-myc amplification is a betterprognostic factor than HER2/neu amplifi-cation in primary breast cancer. CancerRes 52: 1107-1113. 251. Berns EM, van Staveren IL, Look MP,Smid M, Klijn JG, Foekens JA (1998).Mutations in residues of TP53 that directlycontact DNA predict poor outcome inhuman primary breast cancer. Br J Cancer77: 1130-1136. 252. Bernstein JL, Thompson WD, Risch N,Holford TR (1992). Risk factors predictingthe incidence of second primary breastcancer among women diagnosed with afirst primary breast cancer. Am JEpidemiol 136: 925-936. 253. Bernstein JL, Thompson WD, Risch N,Holford TR (1992). The genetic epidemiolo -gy of second primary breast cancer. Am JEpidemiol 136: 937-948. 254. Bernstein L, Deapen D, Ross RK (1993).The descriptive epidemiology of malignantcystosarcoma phyllodes tumors of thebreast. Cancer 71: 3020-3024. 255. Bernstein L, Ross RK (1993).Endogenous hormones and breast cancerrisk. Epidemiol Rev 15: 48-65. 256. Berrino F, Capocaccia R, Esteve J,Gatta G, Hakulinen T, Micheli A, Sant M,Verdecchia A (1999). Survival of Cancerpatients in Europe: The EUROCARE-2Study. IARC Scientific Publication No 151.International Agency for Research onCancer: Lyon.257. Bertucci F, Nasser V, Granjeaud S,Eisinger F, Adelaide J, Tagett R, Loriod B,Giaconia A, Benziane A, Devilard E,Jacquemier J, Viens P, Nguyen C,Birnbaum D, Houlgatte R (2002). Geneexpression profiles of poor-prognosis pri-mary breast cancer correlate with sur-vival. Hum Mol Genet 11: 863-872. 258. Bertwistle D, Swift S, Marston NJ,Jackson LE, Crossland S, Crompton MR,Marshall CJ, Ashworth A (1997). Nuclearlocation and cell cycle regulation of theBRCA2 protein. Cancer Res 57 : 5485-5488. 259. Berx G, Becker KF, Hofler H, van Roy F(1998). Mutations of the human E-cadherin(CDH1) gene. Hum Mutat 12: 226-237.
260. Berx G, Cleton-Jansen AM, Nollet F,de Leeuw WJ, van de Vijvert M, CornelisseC, van Roy F (1995). E-cadherin is atumour/invasion suppressor gene mutatedin human lobular breast cancers. EMBO J14: 6107-6115. 261. Berx G, Cleton-Jansen AM, StrumaneK, de Leeuw WJ, Nollet F, van Roy F,Cornelisse C (1996). E-cadherin is inacti-vated in a majority of invasive human lobu-lar breast cancers by truncation mutationsthroughout its extracellular domain.Oncogene 13: 1919-1925. 262. Bethwaite PB, Holloway LJ, YeongML, Thornton A (1993). Effect of tumourassociated tissue eosinophilia on survivalof women with stage IB carcinoma of theuterine cervix. J Clin Pathol 46: 1016-1020. 263. Bethwaite PB, Koreth J, HerringtonCS, McGee JO (1995). Loss of heterozygos-ity occurs at the D11S29 locus on chromo-some 11q23 in invasive cervical carcino-ma. Br J Cancer 71: 814-818. 264. Biankin SA, O’Toole VE, Fung C,Russell P (2000). Bizarre leimyoma of thevagina: Report of a case. Int J GynecolPathol 19: 186-187. 265. Bieche I, Lidereau R (1995). Geneticalterations in breast cancer. G e n e sChromosomes Cancer 14: 227-251. 266. Bieche I, Lidereau R (1999). Increasedlevel of exon 12 alternatively splicedBRCA2 transcripts in tumor breast tissuecompared with normal tissue. Cancer Res59: 2546-2550. 267. Bieche I, Nogues C, Lidereau R (1999).Overexpression of BRCA2 gene in sporadicbreast tumours. Oncogene 18: 5232-5238. 268. Bienenstock J, Befus AD (1980).Mucosal immunology. Immunology 41: 249-270. 269. Biernat W, Jablkowski W (2000).Syringomatous adenoma of the nipple. PolJ Pathol 51: 201-202. 270. Bijker N, Peterse JL, Duchateau L,Robanus-Maandag EC, Bosch CA, Duval C,Pilotti S, Van de Vijver MJ (2001).Histological type and marker expression ofthe primary tumour compared with its localrecurrence after breast-conserving thera-py for ductal carcinoma in situ. Br JCancer 84: 539-544. 271. Bijker N, Rutgers EJ, Peterse JL,Fentiman IS, Julien JP, Duchateau L, vanDongen JA (2001). Variations in diagnosticand therapeutic procedures in a multicen-tre, randomized clinical trial (EORTC 10853)investigating breast-conserving treatmentfor DCIS. Eur J Surg Oncol 27: 135-140. 272. Bingham C, Roberts D, Hamilton TC(2001). The role of molecular biology inunderstanding ovarian cancer initiationand progression. Int J Gynecol Cancer 11Suppl 1: 7-11. 273. Birch JM, Hartley AL, Blair V, KelseyAM, Harris M, Teare MD, Jones PH (1990).Cancer in the families of children with softtissue sarcoma. Cancer 66: 2239-2248. 274. Birkeland SA, Storm HH, Lamm LU,Barlow L, Blohme I, Forsberg B, Eklund B,Fjeldborg O, Friedberg M, Frodin L, GlattreE, Halvorsen S, Holm NV, Jakobsen A,Jorgensen HE, Ladefoged J, Lindholm T,Lundgren G, Pukkala E. (1995). Cancer riskafter renal transplantation in the Nordiccountries, 1964-1986. Int J Cancer 60: 183-189. 275. Bisceglia M, Attino V, D'Addetta C,Murgo R, Fletcher CD (1996). [Early stageStewart-Treves syndrome: report of 2cases and review of the literature].Pathologica 88: 483-490.
276. Bisceglia M, Fusilli S, Zaffarano L,Fiorentino F, Tardio B (1995). [Inflammatorypseudotumor of the breast. Report of acase and review of the literature].Pathologica 87: 59-64. 277. Biscotti CV, Hart WR (1989). Juvenilegranulosa cell tumors of the ovary. ArchPathol Lab Med 113: 40-46. 278. Biscotti CV, Hart WR (1992). Peritonealserous micropapillomatosis of low malig-nant potential (serous borderline tumors ofthe peritoneum). A clinicopathologic studyof 17 cases. Am J Surg Pathol 16: 467-475. 279. Biscotti CV, Hart WR (1998). Apoptoticbodies: a consistent morphologic featureof endocervical adenocarcinoma in situ.Am J Surg Pathol 22: 434-439. 2 8 0 . Bishara M, Scapa E (1997). [Stromaluterine sarcoma arising from intestinalendometriosis after abdominal hysterecto-my and salpingo-oophorectomy]. H a r e f u a h133: 353-355. 281. Bishop DT, Hopper J (1997). AT-trib-utable risks? Nat Genet 15: 226. 2 8 2 . Bitterman P, Chun B, Kurman RJ(1990). The significance of epithelial differ-entiation in mixed mesodermal tumors ofthe uterus. A clinicopathologic andimmunohistochemical study. Am J SurgPathol 14: 317-328. 283. Bjorkholm E, Silfversward C (1980).Theca-cell tumors. Clinical features andprognosis. Acta Radiol Oncol 19: 241-244. 284. Bjorkholm E, Silfversward C (1981).Prognostic factors in granulosa-celltumors. Gynecol Oncol 11: 261-274. 285. Black CL, Morris DM, Goldman LI,McDonald JC (1983). The significance oflymph node involvement in patients withmedullary carcinoma of the breast. SurgGynecol Obstet 157: 497-499. 286. Black MM, Barclay TH, Hankey BF(1975). Prognosis in breast cancer utilizinghistologic characteristics of the primarytumor. Cancer 36: 2048-2055. 287. Blaker H, Graf M, Rieker RJ, Otto HF(1999). Comparison of losses of heterozy-gosity and replication errors in primarycolorectal carcinomas and correspondingliver metastases. J Pathol 188: 258-262. 288. Blamey RW (1998). Clinical aspects ofmalignant breast lesions In: SystemicPathology, CW Elston, IO Ellis (Eds.). 3rded. Churchill Livingstone: Edinburgh, pp.501-513. 289. Bloch T, Roth LM, Stehman FB, HullMT, Schwenk GR Jr. (1988). Osteosarcomaof the uterine cervix associated withhyperplastic and atypical mesonephricrests. Cancer 62: 1594-1600. 290. Block E (1947). Squamous cell carci-noma of the fallopian tube. Acta Radiol 28:49-68. 291. Blom R, Guerrieri C, Stal O, MalmstromH, Simonsen E (1998). Leiomyosarcoma ofthe uterus: A clinicopathologic, DNA flowcytometric, p53, and mdm-2 analysis of 49cases. Gynecol Oncol 68: 54-61. 292. Blom R, Malmstrom H, Guerrieri C(1999). Endometrial stromal sarcoma of theuterus: a clinicopathologic, DNA flow cyto-metric, p53, and mdm-2 analysis of 17cases. Int J Gynecol Cancer 9: 98-104. 293. Bloom HJ, Richardson WW (1957).Histological grading and prognosis inbreast cancer. Br J Cancer 11: 359-377. 294. Bloom HJ, Richardson WW, Field JR(1970). Host resistance and survival in car -cinoma of breast: a study of 104 cases ofmedullary carcinoma in a series of 1,411cases of breast cancer followed for 20years. Br Med J 3: 181-188.
295. Boardman CH, Webb MJ, Jefferies JA(2000). Low-grade endometrial stromal sar-coma of the ectocervix after therapy forbreast cancer. Gynecol Oncol 79: 120-123.296. Bobrow LG, Richards MA, HapperfieldLC, Diss TC, Isaacson PG, Lammie GA,Millis RR (1993). Breast lymphomas: a clin -icopathologic review. Hum Pathol 24: 274-278. 297. Bochar DA, Wang L, Beniya H, KinevA, Xue Y, Lane WS, Wang W, Kashanchi F,Shiekhattar R (2000). BRCA1 is associatedwith a human SWI/SNF-related complex:linking chromatin remodeling to breastcancer. Cell 102: 257-265. 298. Bodian CA, Perzin KH, Lattes R (1996).Lobular neoplasia. Long term risk of breastcancer and relation to other factors.Cancer 78: 1024-1034. 2 9 9 . Bodian CA, Perzin KH, Lattes R,Hoffmann P, Abernathy TG (1993).Prognostic significance of benign prolifer-ative breast disease. Cancer 71: 3896-3907. 300. Bodner K, Bodner-Adler B, ObermairA, Windbichler G, Petru E, Mayerhofer S,Czerwenka K, Leodolter S, Kainz C,Mayerhofer K (2001). Prognostic parame-ters in endometrial stromal sarcoma: aclinicopathologic study in 31 patients.Gynecol Oncol 81: 160-165. 301. Boecker W, Buerger H, Schmitz K, EllisIA, van Diest PJ, Sinn H-P, Geradts J,Diallo R, Poremba C, Herbst H (2001).Ductal epithelial proliferations of thebreast: a biological continuum? Compar-ative genomic hybridization an high-molecular-weight cytokeratin expressionpatterns. J Pathol 195: 415-421. 302. Bohm J, Roder-Weber M, Hofler H,Kolben M (1991). Bilateral stromal Leydigcell tumour of the ovary. Case report andliterature review. Pathol Res Pract 187:348-352. 303. Boice JD Jr., Engholm G, KleinermanRA, Blettner M, Stovall M, Lisco H,Moloney WC, Austin DF, Bosch A, CookfairDL, Krementz ET, Latourettte HB, MerrillJA, Peters LJ, Schultz MD, Strom HH,Bjorkholm E, Pettersson F, Bell CMJ,Coleman MP, Fraser P, Neal FE, Prior P,Choi NW, Hislop TG, Koch M, Kreiger N,Robb D, Robson D, Thomson DH,Lochmuller H, Vonfournier D, Frischkorn R,Kjorstad KE, Rimpela A, Pejovic MH, KirnVP, Stankusova H, Berrino F, Sigurdsson K,Hutchinson GB, Macmahon B (1988).Radiation dose and second cancer risk inpatients treated for cancer of the cervix.Radiat Res 116: 3-55. 304. Boice JD Jr., Preston D, Davis FG,Monson RR (1991). Frequent chest X-rayfluoroscopy and breast cancer incidenceamong tuberculosis patients inMassachusetts. Radiat Res 125: 214-222. 305. Boks D.E., Trujillo A.P., Voogd AC,Morreau H, Kenter GG, Vasen HF (2002).Survival analysis of endometrial carcino-ma asociated with hereditary nonpolyposiscolorectal cancer. Int J Cancer 102: 198-200. 306. Boland CR, Thibodeau SN, HamiltonSR, Sidransky D, Eshleman JR, Burt RW,Meltzer SJ, Rodriguez-Bigas MA, Fodde R,Ranzani GN, Srivastava S (1998). ANational Cancer Institute Workshop onMicrosatellite Instability for cancer detec-tion and familial predisposition: develop-ment of international criteria for the deter -mination of microsatellite instability incolorectal cancer. Cancer Res 58: 5248-5257.

377References
307. Bolis GB, Maccio T (2000). Clear celladenocarcinoma of the vulva arising inendometriosis. A case report. Eur JGynaecol Oncol 21: 416-417. 3 0 8 . Bonfiglio TA, Patten SF Jr.,Woodworth FE (1976). Fibroxanthosarcomaof the uterine cervix: cytopathologic andhistopathologic manifestations. Acta Cytol20: 501-504. 309. Bonneau D, Longy M (2000). Mutationsof the human PTEN gene. Hum Mutat 16:109-122. 3 1 0 . Bonnet M, Guinebretiere JM,Kremmer E, Grunewald V, Benhamou E,Contesso G, Joab I (1999). Detection ofEpstein-Barr virus in invasive breast can-cers. J Natl Cancer Inst 91: 1376-1381. 311. Bonnier P, Romain S, Dilhuydy JM,Bonichon F, Julien JP, Charpin C, LejeuneC, Martin PM, Piana L (1997). Influence ofpregnancy on the outcome of breast can-cer: a case-control study. SocieteFrancaise de Senologie et de PathologieMammaire Study Group. Int J Cancer 72:720-727. 312. Bonnier P, Romain S, Giacalone PL,Laffargue F, Martin PM, Piana L (1995).Clinical and biologic prognostic factors inbreast cancer diagnosed during post-menopausal hormone replacement thera-py. Obstet Gynecol 85: 11-17. 313. Bonsing BA, Corver WE, Fleuren GJ,Cleton-Jansen AM, Devilee P, CornelisseCJ (2000). Allelotype analysis of flow-sort-ed breast cancer cells demonstratesgenetically related diploid and aneuploidsubpopulations in primary tumors andlymph node metastases. Genes Chromo-somes Cancer 28: 173-183. 3 1 4 . Borazjani G, Prem KA, Okagaki T,Twiggs LB, Adcock LL (1990). Primarymalignant melanoma of the vagina: a clini -copathological analysis of 10 cases.Gynecol Oncol 37: 264-267. 315. Borgen PI, Senie RT, McKinnon WM,Rosen PP (1997). Carcinoma of the malebreast: analysis of prognosis comparedwith matched female patients. Ann SurgOncol 4: 385-388. 3 1 6 . Bork P, Hofmann K, Bucher P,Neuwald AF, Altschul SF, Koonin EV (1997).A superfamily of conserved domains inDNA damage-responsive cell cycle check-point proteins. FASEB J 11: 68-76. 317. Borresen AL, Andersen TI, Eyfjord JE,Cornelis RS, Thorlacius S, Borg A,Johansson U, Theillet C, Scherneck S,Hartman S, Cornelisse CJ, Hovig E, DevileeP (1995). TP53 mutations and breast cancerprognosis: particularly poor survival ratesfor cases with mutations in the zinc-bind-ing domains. Genes Chromosomes Cancer14: 71-75. 318. Borresen AL, Andersen TI, Tretli S,Heiberg A, Moller P (1990). Breast cancerand other cancers in Norwegian familieswith ataxia-telangiectasia. Genes Chromo-somes Cancer 2: 339-340. 319. Borst MJ, Ingold JA (1993). Metastaticpatterns of invasive lobular versus inva-sive ductal carcinoma of the breast.Surgery 114: 637-641. 320. Bosch FX, Lorincz A, Munoz N, MeijerCJ, Shah KV (2002). The causal relationbetween human papillomavirus and cervi-cal cancer. J Clin Pathol 55: 244-265. 321. Bose S, Derosa CM, Ozzello L (1999).Immunostaining of type IV collagen andsmooth muscle actin as an aid in the diag-nosis of breast lesions. Breast J 5: 194-201.
322. Bostwick DG, Tazelaar HD, Ballon SC,Hendrickson MR, Kempson RL (1986).Ovarian epithelial tumors of borderlinemalignancy. A clinical and pathologicstudy of 109 cases. Cancer 58: 2052-2065. 3 2 3 . Botta G, Fessia L, Ghiringhello B(1982). Juvenile milk protein secreting car-cinoma. Virchows Arch A Pathol AnatHistol 395: 145-152. 3 2 4 . Bottles K, Lacey CG, Goldberg J,Lanner-Cusin K, Hom J, Miller TR (1984).Merkel cell carcinoma of the vulva. ObstetGynecol 63: 61S-65S. 325. Boulat J, Mathoulin MP, Vacheret H,Andrac L, Habib MC, Pellissier JF, Piana L,Charpin C (1994). [Granular cell tumors ofthe breast]. Ann Pathol 14: 93-100. 326. Boussen H, Kochbati L, Besbes M,Dhiab T, Makhlouf R, Jerbi G, Gamoudi A,Benna F, Rahal K, Maalej M, Ben Ayed F(2000). [Male secondary breast cancerafter treatment for Hodgkin's disease.Case report and review of the literature].Cancer Radiother 4: 465-468. 327. Bouvet M, Ollila DW, Hunt KK, BabieraGV, Spitz FR, Giuliano AE, Strom EA, AmesFC, Ross MI, Singletary SE (1997). Role ofconservation therapy for invasive lobularcarcinoma of the breast. Ann Surg Oncol 4:650-654. 328. Bower JF, Erickson ER (1967). Bilateralovarian fibromas in a 5-year-old. Am JObstet Gynecol 99: 880-882. 3 2 9 . Boyd J, Sonoda Y, Federici MG,Bogomolniy F, Rhei E, Maresco DL, SaigoPE, Almadrones LA, Barakat RR, Brown CL,Chi DS, Curtin JP, Poynor EA, Hoskins WJ(2000). Clinicopathologic features of BRCA-linked and sporadic ovarian cancer. JAMA283: 2260-2265. 330. Boyd J, Takahashi H, Waggoner SE,Jones LA, Hajek RA, Wharton JT, Liu FS,Fujino T, Barrett JC, McLachlan JA (1996).Molecular genetic analysis of clear celladenocarcinomas of the vagina and cervixassociated and unassociated with diethyl -stilbestrol exposure in utero. Cancer 77:507-513. 3 3 1 . Boyer CV, Navin JJ (1965).Extraskeletal osteogenic sarcoma. A latecomplication of radiation therapy. Cancer18: 628-633. 332. Brainard JA, Hart WR (1998). Adenoidbasal epitheliomas of the uterine cervix: areevaluation of distinctive cervical basa-loid lesions currently classified as adenoidbasal carcinoma and adenoid basal hyper-plasia. Am J Surg Pathol 22: 965-975. 3 3 3 . Brand E, Berek JS, Nieberg RK,Hacker NF (1987). Rhabdomyosarcoma ofthe uterine cervix. Sarcoma botryoides.Cancer 60: 1552-1560. 3 3 4 . Brandfass RJ, Everts-Suarez EA(1955). Lipomatous tumors of the uterus: areview of the world's literature with a casereport of true lipoma. Am J Obstet Gynecol70: 359-367. 3 3 5 . Branton PA, Tavassoli FA (1993).Spindle cell epithelioma, the so-calledmixed tumor of the vagina. A clinicopatho -logic, immunohistochemical, and ultra-structural analysis of 28 cases. Am J SurgPathol 17: 509-515. 336. Bratthauer GL, Lininger RA, Man YG,Tavassoli FA (2002). Androgen and estro-gen receptor mRNA status in apocrine car-cinomas. Diagn Mol Pathol 11: 113-118.
337. Bratthauer GL, Moinfar F, StamatakosMD, Mezzetti TP, Shekitka KM, Man Y-G,Tavassoli FA (2002). Combined E-cadherinand high molecular weight cytokeratinimmunoprofile differentiates lobular, duc-tal and hybrid mammary intraepithelialneoplasia. Hum Pathol 33: 620-627. 338. Bratthauer GL, Tavassoli FA (2002).Lobular neoplasia: previously unexploredaspects assessed in 775 cases and theirclinical implications. Virchows Arch 440:134-138. 339. Braun S, Pantel K, Muller P, Janni W,Hepp F, Kentenich CR, Gastroph S,Wischnik A, Dimpfl T, Kindermann G,Riethmuller G, Schlimok G (2000).Cytokeratin-positive cells in the bone mar -row and survival of patients with stage I, II,or III breast cancer. N Engl J Med 342: 525-533. 3 4 0 . Breen JL, Neubecker RD (1962).Tumors of the round ligament. A review ofthe literature and a report of 25 cases.Obstet Gynecol 19: 771-780. 341. Brescia RJ, Dubin N, Demopoulos RI(1989). Endometrioid and clear cell carci-noma of the ovary. Factors affecting sur-vival. Int J Gynecol Pathol 8: 132-138. 3 4 2 . Bret AJ, Grepinet J (1967).[Endometrial polyps of the intramural por-tion of the Fallopian tube. Their relation tosterility and endometriosis]. Sem Hop 43:183-192. 3 4 3 . Brewer JI, Mazur MT (1981).Gestational choriocarcinoma. Its origin inthe placenta during seemingly normalpregnancy. Am J Surg Pathol 5: 267-277. 344. Briest S, Horn LC, Haupt R, SchneiderJP, Schneider U, Hockel M (1999).Metastasizing signet ring cell carcinomaof the stomach-mimicking bilateral inflam-matory breast cancer. Gynecol Oncol 74:491-494. 345. Brinck U, Jakob C, Bau O, Fuzesi L(2000). Papillary squamous cell carcinomaof the uterine cervix: report of three casesand a review of its classification. Int JGynecol Pathol 19: 231-235. 346. Brinkmann U (1998). CAS, the humanhomologue of the yeast chromosome-seg -regation gene CSE1, in proliferation, apop -tosis, and cancer. Am J Hum Genet 62: 509-513. 346 a. Brinton LA, Hoover R, Fraumeni JFJr. (1982). Interaction of familial and hor-monal risk factors for breast cancer. JNatl Cancer Inst 69: 817-822. 3 4 7 . Brinton LA, Nasca PC, Mallin K,Schairer C, Rosenthal J, Rothenberg R,Yordan E Jr., Richart RM (1990). Case-con -trol study of in situ and invasive carcinomaof the vagina. Gynecol Oncol 38: 49-54. 348. Brisigotti M, Moreno A, Murcia C,Matias-Guiu X, Prat J (1989). Verrucouscarcinoma of the vulva. A clinicopatholog -ic and immunohistochemical study of fivecases. Int J Gynecol Pathol 8: 1-7. 349. Brocca PP (1866). Traité des Tumeurs. 3 5 0 . Broders AC (2002). Squamous cellepithelioma of the skin. A study of 256cases. Ann Surg 73: 141-160. 351. Broeks A, Urbanus JH, Floore AN,Dahler EC, Klijn JG, Rutgers EJ, Devilee P,Russell NS, van Leeuwen FE, van't Veer LJ(2000). ATM-heterozygous germline muta-tions contribute to breast cancer-suscepti-bility. Am J Hum Genet 66: 494-500. 352. Brogi E, Harris NL (1999). Lymphomasof the breast: pathology and clinicalbehavior. Semin Oncol 26: 357-364.
353. Bronner CE, Baker SM, Morrison PT,Warren G, Smith LG, Lescoe MK, Kane M,Earabino C, Lipford J, Lindblom A,Tannergard P, Bollag AG, Godwin AR,Ward DC, Nordenskjold M, Fishel R,Kolodner R, Liskay RM. (1994). Mutation inthe DNA mismatch repair gene homologuehMLH1 is associated with hereditary non-polyposis colon cancer. Nature 368: 258-261. 3 5 4 . Brooks JJ, LiVolsi VA (1987).Liposarcoma presenting on the vulva. AmJ Obstet Gynecol 156: 73-75. 355. Brown H, Vlastos G, Newman LA,Benderly M, Singletary E, Sahin A (2000).Histopathological features of bilateral andunilateral breast carcinoma: a compara-tive study. Mod Pathol 13: 18A. 356. Brown MA, Xu CF, Nicolai H, GriffithsB, Chambers JA, Black D, Solomon E(1996). The 5' end of the BRCA1 gene lieswithin a duplicated region of human chro-mosome 17q21. Oncogene 12: 2507-2513. 357. Brown RS, Marley JL, Cassoni AM(1998). Pseudo-Meigs' syndrome due tobroad ligament leiomyoma: a mimic ofmetastatic ovarian carcinoma. Clin Oncol(R Coll Radiol ) 10: 198-201. 358. Brown VL, Proby CM, Barnes DM,Kelsell DP (2002). Lack of mutations withinST7 gene in tumour-derived cell lines andprimary epithelial tumours. Br J Cancer 87:208-211. 359. Brustein S, Filippa DA, Kimmel M,Lieberman PH, Rosen PP (1987). Malignantlymphoma of the breast. A study of 53patients. Ann Surg 205: 144-150. 360. Bryson SC, Colgan TJ, Vernon CP(1986). Invasive squamous cell carcinomaof the vulva: Delineation of high-risk grouprequiring adjuvant radiotherapy. J ReprodMed 31: 976-978. 361. Buchwalter CL, Jenison EL, Fromm M,Mehta VT, Hart WR (1997). Pure embryonalrhabdomyosarcoma of the fallopian tube.Gynecol Oncol 67: 95-101. 362. Buckley CH (2000). Tumours of thecervix - tumours of the female genital tract.In: Diagnostic Histopathology of Tumours,CDM Fletcher (Ed.) Churchill Livingstone:London. pp. 685-705.363. Buckley JD (1984). The epidemiologyof molar pregnancy and choriocarcinoma.Clin Obstet Gynecol 27: 153-159. 364. Buckshee K, Dhond AJ, Mittal S, BoseS (1990). Pseudo-Meigs' syndrome sec-ondary to broad ligament leiomyoma: acase report. Asia Oceania J ObstetGynaecol 16: 201-205. 365. Buerger H, Mommers EC, Littmann R,Simon R, Diallo R, Poremba C, Dockhorn-Dworniczak B, van Diest PJ, Boecker W(2001). Ductal invasive G2 and G3 carcino-mas of the breast are the end stages of atleast two different lines of genetic evolu-tion. J Pathol 194: 165-170. 3 6 6 . Buerger H, Otterbach F, Simon R,Poremba C, Diallo R, Decker T, Riethdorf L,Brinkschmidt C, Dockhorn-Dworniczak B,Boecker W (1999). Comparative genomichybridization of ductal carcinoma in situ ofthe breast-evidence of multiple geneticpathways. J Pathol 187: 396-402. 367. Bullón A, Arseneau J, Prat J, YoungRH, Scully RE (1981). Tubular Krukenbergtumor. A problem in histopathologic diag-nosis. Am J Surg Pathol 5: 225-232. 368. Bundred NJ (2001). Prognostic andpredictive factors in breast cancer.Cancer Treat Rev 27: 137-142.

378 References
369. Bur ME, Zimarowski MJ, Schnitt SJ,Baker S, Lew R (1992). Estrogen receptorimmunohistochemistry in carcinoma in situof the breast. Cancer 69: 1174-1181. 370. Burghardt E, Baltzer J, Tulusan AH,Haas J (1992). Results of surgical treat-ment of 1028 cervical cancers studied withvolumetry. Cancer 70: 648-655. 371. Burghardt E, Östör AG, Fox H (1997).The new FIGO definition of cervical cancerstage IA: a critique. Gynecol Oncol 65: 1-5. 372. Burghardt E, Pickel H, Girardi F (1998).Colposcopy-Cervical Pathology Textbookand Atlas. 3rd ed. Thieme: New York.373. Burke TW, Eifel PJ, McGuire P, et al.(2000). Vulva. In: Principles and Practice ofGynecologic Oncology. WJ Hoskins, CAPerez, RC Young (Eds.). 3rd ed. pp. 775-810.Williams & Wilkins: Philadelphia, 374. Burke TW, Stringer CA, GershensonDM, Edwards CL, Morris M, Wharton JT(1990). Radical wide excision and selectiveinguinal node dissection for squamous cellcarcinoma of the vulva. Gynecol Oncol 38:328-332. 375. Burki N, Buser M, Emmons LR, GencikA, Haner M, Torhorst JK, Weber W, MullerH (1990). Malignancies in families ofwomen with medullary, tubular and inva-sive ductal breast cancer. Eur J Cancer 26:295-303. 376. Burks RT, Sherman ME, Kurman RJ(1996). Micropapillary serous carcinoma ofthe ovary. A distinctive low-grade carcino-ma related to serous borderline tumors.Am J Surg Pathol 20: 1319-1330. 377. Burns B, Curry RH, Bell ME (1979).Morphologic features of prognostic signif -icance in uterine smooth muscle tumors: areview of eighty-four cases. Am J ObstetGynecol 135: 109-114. 378. Burrell HC, Sibbering DM, Wilson AR(1995). Case report: fibromatosis of thebreast in a male patient. Br J Radiol 68:1128-1129. 379. Burt EC, McGown G, Thorncroft M,James LA, Birch JM, Varley JM (1999).Exclusion of the genes CDKN2 and PTENas causative gene defects in Li-Fraumenisyndrome. Br J Cancer 80: 9-10. 380. Burt RL, Prichard RW, Kim BS (1976).Fibroepithelial polyp of the vagina. A reportof five cases. Obstet Gynecol 47: 52S-54S. 381. Busby JG (1952). Neurofibromatosis ofthe cervix. Am J Obstet Gynecol 63: 674-675. 382. Bussolati G, Gugliotta P, Sapino A,Eusebi V, Lloyd RV (1985). Chromogranin-reactive endocrine cells in argyrophiliccarcinomas ("carcinoids") and normal tis-sue of the breast. Am J Pathol 120: 186-192. 383. Butnor KJ, Sporn TA, Hammar SP,Roggli VL (2001). Well-differentiated papil-lary mesothelioma. Am J Surg Pathol 25:1304-1309. 3 8 4 . Byrne P, Vella EJ, Rollason T,Frampton J (1989). Ovarian fibromatosiswith minor sex cord elements. Case report.Br J Obstet Gynaecol 96: 245-248. 385. Byskov AG, Skakkebaek NE, StafangerG, Peters H (1977). Influence of ovariansurface epithelium and rete ovarii on folli-cle formation. J Anat 123: 77-86. 386. Calabresi E, De Giuli G, Becciolini A,Giannotti P, Lombardi G, Serio M (1976).Plasma estrogens and androgens in malebreast cancer. J Steroid Biochem 7: 605-609.
387. Calle EE, Murphy TK, Rodriguez C,Thun MJ, Heath CWJ (1998). Occupationand breast cancer mortality in a prospec-tive cohort of US women. Am J Epidemiol148: 191-197. 3 8 8 . Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ (2003). Overweight,obesity, and mortality from cancer in aprospectively studied cohort of U.S. adults.N Engl J Med 348: 1625-1638. 389. Calonje E, Guerin D, McCormick D,Fletcher CD (1999). Superficial angiomyxo -ma: clinicopathologic analysis of a seriesof distinctive but poorly recognized cuta-neous tumors with tendency for recur-rence. Am J Surg Pathol 23: 910-917. 390. Cameron CT, Adair FE (1965). The clin -ical features and diagnosis of the commonbreast tumours. Med J Aust 2: 651-654. 391. Campello TR, Fittipaldi H, O'Valle F,Carvia RE, Nogales FF (1998). Extrauterine(tubal) placental site nodule.Histopathology 32: 562-565. 392. Cancellieri A, Eusebi V, Mambelli V,Ricotti G, Gardini G, Pasquinelli G (1991).Well-differentiated angiosarcoma of theskin following radiotherapy. Report of twocases. Pathol Res Pract 187: 301-306. 393. Cangiarella J, Symmans WF, CohenJM, Goldenberg A, Shapiro RL, Waisman J(1998). Malignant melanoma metastatic tothe breast: a report of seven cases diag-nosed by fine-needle aspiration cytology.Cancer 84: 160-162. 394. Cannistra SA (1993). Cancer of theovary. N Engl J Med 329: 1550-1559. 395. Canola T, Kirkis EJ, Meckes PF, PittsSB (1994). Interdisciplinary groupapproach to occupational safety andhealth administration standard: reductionsin cost and duplication of effort. Am JInfect Control 22: 182-187. 396. Cantuaria G, Angioli R, Nahmias J,Estape R, Penalver M (1999). Primarymalignant melanoma of the uterine cervix:case report and review of the literature.Gynecol Oncol 75: 170-174. 397. Capella C, Usellini L, Papotti M, MacriL, Finzi G, Eusebi V, Bussolati G (1990).Ultrastructural features of neuroendocrinedifferentiated carcinomas of the breast.Ultrastruct Pathol 14: 321-334. 398. Cappello F, Barbato F, Tomasino RM(2000). Mature teratoma of the uterine cor-pus with thyroid differentiation. Pathol Int50: 546-548. 399. Carapeto R, Nogales FF Jr., Matilla A(1978). Ectopic pregnancy coexisting witha primary carcinoma of the Fallopian tube:a case report. Int J Gynaecol Obstet 16:263-264. 400. Carcangiu ML, Chambers JT (1995).Early pathologic stage clear cell carcino-ma and uterine papillary serous carcinomaof the endometrium: comparison of clinico-pathologic features and survival. Int JGynecol Pathol 14: 30-38. 4 0 1 . Cardenosa G, Eklund GW (1991).Benign papillary neoplasms of the breast:mammographic findings. Radiology 1 8 1 :751-755. 402. Carinelli SG, Giudici MN, Brioschi D,Cefis F (1990). Alveolar soft part sarcoma ofthe vagina. Tumori 76: 77-80.
403. Carlson JA, Ambros R, Malfetano J,Ross J, Grabowski R, Lamb P, Figge H,Mihm MC Jr. (1998). Vulvar lichen sclero-sus and squamous cell carcinoma: acohort, case control, and investigationalstudy with historical perspective; implica-tions for chronic inflammation and sclero-sis in the development of neoplasia. HumPathol 29: 932-948. 404. Carlson JA Jr., Wheeler JE (1993).Primary ovarian melanoma arising in a der-moid stage IIIc: long-term disease-freesurvival with aggressive surgery and plat-inum therapy. Gynecol Oncol 48: 397-401. 405. Carlson JW, McGlennen RC, Gomez R,Longbella C, Carter J, Carson LF (1996).Sebaceous carcinoma of the vulva: a casereport and review of the literature.Gynecol Oncol 60: 489-491. 4 0 6 . Carlson RW, Favret AM (1999).Multidisciplinary management of locallyadvanced breast cancer. Breast J 5: 303-307. 4 0 7 . Carney JA, Young WF Jr. (1992).Primary pigmented nodular adrenocorticaldisease and its associated conditions.Endocrinologist 2: 6-21. 408. Carpenter R, Gibbs N, Matthews J,Cooke T (1987). Importance of cellular DNAcontent in pre-malignant breast diseaseand pre-invasive carcinoma of the femalebreast. Br J Surg 74: 905-906. 409. Carstens PH, Greenberg RA, FrancisD, Lyon H (1985). Tubular carcinoma of thebreast. A long term follow-up. H i s t o -pathology 9: 271-280. 410. Carstens PH, Huvos AG, Foote FW Jr.,Ashikari R (1972). Tubular carcinoma of thebreast: a clinicopathologic study of 35cases. Am J Clin Pathol 58: 231-238. 411. Carter BA, Page DL, Schuyler P, ParlFF, Simpson JF, Jensen RA, Dupont WD(2001). No elevation in long-term breastcarcinoma risk for women with fibroade-nomas that contain atypical hyperplasia.Cancer 92: 30-36. 4 1 2 . Carter CL, Corle DK, Micozzi MS,Schatzkin A, Taylor PR (1988). A prospec-tive study of the development of breastcancer in 16,692 women with benignbreast disease. Am J Epidemiol 128: 467-477. 412a. Carter CL, Jones DY, Schatzkin A,Brinton LA (1989). A prospective study ofreproductive, familial and socioeconomicrisk factors for breast cancer usingNHANES I data. Public Health Rep 104: 45-50. 413. Carter D, Orr SL, Merino MJ (1983).Intracystic papillary carcinoma of thebreast. After mastectomy, radiotherapy orexcisional biopsy alone. Cancer 52: 14-19. 414. Carter D, Pipkin RD, Shepard RH,Elkins RC, Abbey H (1978). Relationship ofnecrosis and tumor border to lymph nodemetastases and 10-year survival in carci-noma of the breast. Am J Surg Pathol 2: 39-46. 415. Carter J, Elliott P (1990). Syringoma--an unusual cause of pruritus vulvae. AustNZ J Obstet Gynaecol 30: 382-383. 416. Carter J, Elliott P, Russell P (1992).Bilateral fibroepithelial polypi of labiumminus with atypical stromal cells.Pathology 24: 37-39. 417. Cartier R, Cartier I (1993). PracticalColposcopy. 3rd ed. Laboratoire Cartier:Paris.418. Casagrande JT, Hanisch R, Pike MC,Ross RK, Brown JB, Henderson BE (1988).A case-control study of male breast can-cer. Cancer Res 48: 1326-1330.
419. Cashell AW, Cohen ML (1991).Masculinizing sclerosing stromal tumor ofthe ovary during pregnancy. G y n e c o lOncol 43: 281-285. 420. Casper GR, Östör AG, Quinn MA (1997).A clinicopathologic study of glandular dys-plasia of the cervix. Gynecol Oncol 64: 166-170. 421. Cass I, Baldwin RL, Fasylova E, FieldsAL, Klinger HP, Runowicz CD, Karlan BY(2001). Allelotype of papillary serous peri-toneal carcinomas. Gynecol Oncol 82: 69-76. 422. Cass I, Baldwin RL, Varkey T, MoslehiR, Narod SA, Karlan BY (2003). Improvedsurvival in women with BRCA-associatedovarian carcinoma. Cancer 97: 2187-2195. 423. Castellsague X, Bosch FX, Munoz N,Meijer CJ, Shah KV, de Sanjose S, Eluf-Neto J, Ngelangel CA, Chichareon S, SmithJS, Herrero R, Moreno V, Franceschi S(2002). Male circumcision, penile humanpapillomavirus infection, and cervical can-cer in female partners. N Engl J Med 346:1105-1112. 424. Castrillon DH, Lee KR, Nucci MR(2002). Distinction between endometrialand endocervical adenocarcinoma: animmunohistochemical study. Int J GynecolPathol 21: 4-10. 425. Castrillon DH, Sun D, Weremowicz S,Fisher RA, Crum CP, Genest DR (2001).Discrimination of complete hydatidiformmole from its mimics by immunohisto-chemistry of the paternally imprinted geneproduct p57KIP2. Am J Surg Pathol 25:1225-1230. 426. Catteau A, Harris WH, Xu CF, SolomonE (1999). Methylation of the BRCA1 promot-er region in sporadic breast and ovariancancer: correlation with disease charac-teristics. Oncogene 18: 1957-1965. 427. Cavalli LR, Rogatto SR, Rainho CA, dosSantos MJ, Cavalli IJ, Grimaldi DM (1995).Cytogenetic report of a male breast can-cer. Cancer Genet Cytogenet 81: 66-71. 428. Cecalupo AJ, Frankel LS, Sullivan MP(1982). Pelvic and ovarian extramedullaryleukemic relapse in young girls: a report offour cases and review of the literature.Cancer 50: 587-593. 429. Cerhan JR, Kushi LH, Olson JE, RichSS, Zheng W, Folsom AR, Sellers TA (2000).Twinship and risk of postmenopausalbreast cancer. J Natl Cancer Inst 92: 261-265. 430. Chachlani N, Yue CT, Gerardo LT(1997). Granular cell tumor of the breast ina male. A case report. Acta Cytol 41: 1807-1810. 431. Chafe W, Richards A, Morgan L,Wilkinson E (1988). Unrecognized invasivecarcinoma in vulvar intraepithelial neopla -sia (VIN). Gynecol Oncol 31: 154-165. 432. Chalvardjian A, Derzko C (1982).Gynandroblastoma: its ultrastructure.Cancer 50: 710-721. 433. Chalvardjian A, Scully RE (1973).Sclerosing stromal tumors of the ovary.Cancer 31: 664-670. 434. Chandraratnam E, Leong AS (1983).Papillary serous cystadenoma of border-line malignancy arising in a parovarianparamesonephric cyst. Light microscopicand ultrastructural observations.Histopathology 7: 601-611. 435. Chang-Claude J, Eby N, Kiechle M,Bastert G, Becher H (2000). Breastfeedingand breast cancer risk by age 50 amongwomen in Germany. Cancer CausesControl 11: 687-695.

379References
436. Chang J, Sharpe JC, A'Hern RP, FisherC, Blake P, Shepherd J, Gore ME (1995).Carcinosarcoma of the ovary: incidence,prognosis, treatment and survival ofpatients. Ann Oncol 6: 755-758. 437. Chang KL, Crabtree GS, Lim-Tan SK,Kempson RL, Hendrickson MR (1990).Primary uterine endometrial stromal neo-plasms. A clinicopathologic study of 117cases. Am J Surg Pathol 14: 415-438. 438. Chang KL, Crabtree GS, Lim-Tan SK,Kempson RL, Hendrickson MR (1993).Primary extrauterine endometrial stromalneoplasms: a clinicopathologic study of 20cases and a review of the literature. Int JGynecol Pathol 12: 282-296. 439. Chang YC, Hricak H, Thurnher S, LaceyCG (1988). Vagina: evaluation with MRimaging. Part II. Neoplasms. Radiology 169:175-179. 4 4 0 . Chano T, Kontani K, Teramoto K,Okabe H, Ikegawa S (2002). Truncatingmutations of RB1CC1 in human breast can-cer. Nat Genet 31: 285-288. 441. Chappuis PO, Rosenblatt J, FoulkesWD (1999). The influence of familial andhereditary factors on the prognosis ofbreast cancer. Ann Oncol 10: 1163-1170. 442. Charbonnier F, Olschwang S, Wang Q,Boisson C, Martin C, Buisine MP, PuisieuxA, Frebourg T (2002). MSH2 in contrast toMLH1 and MSH6 is frequently inactivatedby exonic and promoter rearrangements inhereditary nonpolyposis colorectal can-cer. Cancer Res 62: 848-853. 4 4 3 . Charbonnier F, Raux G, Wang Q,Drouot N, Cordier F, Limacher JM, SaurinJC, Puisieux A, Olschwang S, Frebourg T(2000). Detection of exon deletions andduplications of the mismatch repair genesin hereditary nonpolyposis colorectal can-cer families using multiplex polymerasechain reaction of short fluorescent frag-ments. Cancer Res 60: 2760-2763. 4 4 4 . Charpin C, Bonnier P, Garcia S,Andrac L, Crebassa B, Dorel M, LavautMN, Allasia C (1999). E-cadherin and beta-catenin expression in breast medullarycarcinomas. Int J Oncol 15: 285-292. 445. Charpin C, Bonnier P, Khouzami A,Vacheret H, Andrac L, Lavaut MN, AllasiaC, Piana L (1992). Inflammatory breast car -cinoma: an immunohistochemical studyusing monoclonal anti-pHER-2/neu, pS2,cathepsin, ER and PR. Anticancer Res 12:591-597. 446. Charpin C, Mathoulin MP, Andrac L,Barberis J, Boulat J, Sarradour B, BonnierP, Piana L (1994). Reappraisal of breasthamartomas. A morphological study of 41cases. Pathol Res Pract 190: 362-371. 4 4 7 . Chatterjee A, Pulido HA, Koul S,Beleno N, Perilla A, Posso H, ManusukhaniM, Murty VV (2001). Mapping the sites ofputative tumor suppressor genes at 6p25and 6p21.3 in cervical carcinoma: occur-rence of allelic deletions in precancerouslesions. Cancer Res 61: 2119-2123. 448. Chaudary MA, Millis RR, Hoskins EO,Halder M, Bulbrook RD, Cuzick J, HaywardJL (1984). Bilateral primary breast cancer:a prospective study of disease incidence.Br J Surg 71: 711-714. 449. Chehab NH, Malikzay A, Appel M,Halazonetis TD (2000). Chk2/hCds1 func-tions as a DNA damage checkpoint in G(1)by stabilizing p53. Genes Dev 14: 278-288.
450. Chen J, Silver DP, Walpita D, CantorSB, Gazdar AF, Tomlinson G, Couch FJ,Weber BL, Ashley T, Livingston DM, ScullyR (1998). Stable interaction between theproducts of the BRCA1 and BRCA2 tumorsuppressor genes in mitotic and meioticcells. Mol Cell 2: 317-328. 451. Chen KT (1981). Bilateral papillary ade-nofibroma of the fallopian tube. Am J ClinPathol 75: 229-231. 452. Chen KT (1984). Bilateral malignantBrenner tumor of the ovary. J Surg Oncol26: 194-197. 453. Chen KT (1986). Female genital tracttumors in Peutz-Jeghers syndrome. HumPathol 17: 858-861. 454. Chen KT (1990). Pleomorphic adenomaof the breast. Am J Clin Pathol 93: 792-794. 455. Chen KT (2000). Composite Large-CellNeuroendocrine Carcinoma and SurfaceEpithelial-Stromal Neoplasm of the Ovary.Int J Surg Pathol 8: 169-174. 456. Chen KT, Hafez GR, Gilbert EF (1980).Myxoid variant of epithelioid smooth mus-cle tumor. Am J Clin Pathol 74: 350-353. 457. Chen KT, Kirkegaard DD, Bocian JJ(1980). Angiosarcoma of the breast.Cancer 46: 368-371. 458. Chen KT, Kuo TT, Hoffmann KD (1981).Leiomyosarcoma of the breast: a case oflong survival and late hepatic metastasis.Cancer 47: 1883-1886. 4 5 9 . Chen KT, Vergon JM (1981).Carcinomesenchymoma of the uterus. AmJ Clin Pathol 75: 746-748. 460. Chen T, Sahin A, Aldaz CM (1996).Deletion map of chromosome 16q in ductalcarcinoma in situ of the breast: refining aputative tumor suppressor gene region.Cancer Res 56: 5605-5609. 461. Chen YY,Schnitt SJ (1998). Prognostic factors forpatients with breast cancers 1cm andsmaller. Breast Cancer Res Treat 51: 209-225. 462. Chenevix-Trench G, Spurdle AB, GateiM, Kelly H, Marsh A, Chen X, Donn K,Cummings M, Nyholt D, Jenkins MA, ScottC, Pupo GM, Dork T, Bendix R, Kirk J,Tucker K, McCredie MR, Hopper JL,Sambrook J, Mann GJ, Khanna KK (2002).Dominant negative ATM mutations inbreast cancer families. J Natl Cancer Inst94: 205-215. 463. Cheng J, Saku T, Okabe H, FurthmayrH (1992). Basement membranes in adenoidcystic carcinoma. An immunohistochemi-cal study. Cancer 69: 2631-2640. 464. Cheng PC, Gosewehr JA, Kim TM,Velicescu M, Wan M, Zheng J, Felix JC,Cofer KF, Luo P, Biela BH, Godorov G,Dubeau L (1996). Potential role of the inac -tivated X chromosome in ovarian epithelialtumor development. J Natl Cancer Inst 88:510-518. 465. Cheng WF, Lin HH, Chen CK, ChangDY, Huang SC (1995). Leiomyosarcoma ofthe broad ligament: a case report and liter-ature review. Gynecol Oncol 56: 85-89. 466. Chestnut DH, Szpak CA, Fortier KJ,Hammond CB (1988). Uterine hemangiomaassociated with infertility. South Med J 81:926-928. 4 6 7 . Chetty R, Govender D (1997).Inflammatory pseudotumor of the breast.Pathology 29: 270-271. 468. Chetty R, Kalan MR (1992). Malignantgranular cell tumor of the breast. J SurgOncol 49: 135-137.
469. Cheung AN, Shen DH, Khoo US, WongLC, Ngan HY (1998). p21WAF1/CIP1 expres-sion in gestational trophoblastic disease:correlation with clinicopathologicalparameters, and Ki67 and p53 geneexpression. J Clin Pathol 51: 159-162. 470. Cheung AN, So KF, Ngan HY, Wong LC(1994). Primary squamous cell carcinomaof fallopian tube. Int J Gynecol Pathol 13:92-95. 471. Cheung AN, Srivastava G, Chung LP,Ngan HY, Man TK, Liu YT, Chen WZ, CollinsRJ, Wong LC, Ma HK (1994). Expression ofthe p53 gene in trophoblastic cells in hyda-tidiform moles and normal human placen-tas. J Reprod Med 39: 223-227. 4 7 2 . Cheung AN, Young RH, Scully RE(1994). Pseudocarcinomatous hyperplasiaof the fallopian tube associated with salp-ingitis. A report of 14 cases. Am J SurgPathol 18: 1125-1130. 473. Chevallier B, Asselain B, Kunlin A,Veyret C, Bastit P, Graic Y (1987).Inflammatory breast cancer.Determi-nation of prognostic factors by univariateand multivariate analysis. Cancer 60: 897-902. 4 7 4 . Chhieng C, Cranor M, Lesser ME,Rosen PP (1998). Metaplastic carcinoma ofthe breast with osteocartilaginous heterol-ogous elements. Am J Surg Pathol 22: 188-194. 475. Chiarle R, Godio L, Fusi D, Soldati T,Palestro G (1997). Pure alveolar rhab-domyosarcoma of the corpus uteri:description of a case with increasedserum level of CA-125. Gynecol Oncol 66:320-323. 4 7 6 . Chiba N, Parvin JD (2001).Redistribution of BRCA1 among four differ-ent protein complexes following replica-tion blockage. J Biol Chem 276: 38549-38554. 477. Chico A, Garcia JL, Matias-Guiu X,Webb SM, Rodriguez J, Prat J, Calaf J(1995). A gonadotrophin dependent stromalluteoma: a rare cause of post-menopausalvirilization. Clin Endocrinol (Oxf) 43: 645-649. 4 7 8 . Cho D, Woodruff JD (1988).Trichoepithelioma of the vulva. A report oftwo cases. J Reprod Med 33: 317-319. 479. Cho SB, Park CM, Park SW, Kim SH,Kim KA, Cha SH, Chung IJ, Kim YW, YoonYK, Kim JS (2001). Malignant mixed muller-ian tumor of the ovary: imaging findings.Eur Radiol 11: 1147-1150. 4 8 0 . Chodosh LA (1998). Expression ofBRCA1 and BRCA2 in normal and neoplas -tic cells. J Mammary Gland Biol Neoplasia3: 389-402. 481. Choi-Hong SR, Genest DR, Crum CP,Berkowitz R, Goldstein DP, Schofield DE(1995). Twin pregnancies with completehydatidiform mole and coexisting fetus:use of fluorescent in situ hybridization toevaluate placental X- and Y-chromosomalcontent. Hum Pathol 26: 1175-1180. 4 8 2 . Choi YL, Kim HS, Ahn G (2000).Immunoexpression of inhibin alpha sub-unit, inhibin/activin betaA subunit andCD99 in ovarian tumors. Arch Pathol LabMed 124: 563-569. 483. Chorlton I, Norris HJ, King FM (1974).Malignant reticuloendothelial diseaseinvolving the ovary as a primary manifesta-tion: a series of 19 lymphomas and 1 gran-ulocytic sarcoma. Cancer 34: 397-407. 4 8 4 . Christman JE, Ballon SC (1990).Ovarian fibrosarcoma associated withMaffucci's syndrome. Gynecol Oncol 37:290-291.
485. Chu KC, Tarone RE, Kessler LG, RiesLA, Hankey BF, Miller BA, Edwards BK(1996). Recent trends in U.S. breast cancerincidence, survival, and mortality rates. JNatl Cancer Inst 88: 1571-1579. 486. Chu PG, Arber DA, Weiss LM, ChangKL (2001). Utility of CD10 in distinguishingbetween endometrial stromal sarcoma anduterine smooth muscle tumors: animmunohistochemical comparison of 34cases. Mod Pathol 14: 465-471. 487. Chua CL, Thomas A, Ng BK (1988).Cystosarcoma phyllodes--Asian variations.Aust N Z J Surg 58: 301-305. 488. Chuang SS, Lin CN, Li CY, Wu CH(2001). Uterine leiomyoma with massivelymphocytic infiltration simulating malig-nant lymphoma. A case report withimmunohistochemical study showing thatthe infiltrating lymphocytes are cytotoxic Tcells. Pathol Res Pract 197: 135-138. 489. Chuaqui R, Silva M, Emmert-Buck M(2001). Allelic deletion mapping on chro-mosome 6q and X chromosome inactiva-tion clonality patterns in cervical intraep-ithelial neoplasia and invasive carcinoma.Gynecol Oncol 80: 364-371. 490. Chuaqui RF, Sanz-Ortega J, Vocke C,Linehan WM, Sanz-Esponera J, Zhuang Z,Emmert-Buck MR, Merino MJ (1995). Lossof heterozygosity on the short arm of chro-mosome 8 in male breast carcinomas.Cancer Res 55: 4995-4998. 491. Chumas JC, Scully RE (1991).Sebaceous tumors arising in ovarian der-moid cysts. Int J Gynecol Pathol 10: 356-363. 492. Chung AF, Casey MJ, Flannery JT,Woodruff JM, Lewis JL Jr. (1980).Malignant melanoma of the vagina--reportof 19 cases. Obstet Gynecol 55: 720-727. 493. Churg A, Colby TV, Cagle P, Corson J,Gibbs AR, Gilks B, Grimes M, Hammar S,Roggli V, Travis WD (2000). The separationof benign and malignant mesothelial prolif-erations. Am J Surg Pathol 24: 1183-1200. 494. Ciano PS, Antonioli DA, Critchlow J,Burke L, Goldman H (1987). Villous adeno-ma presenting as a vaginal polyp in a rec-tovaginal tract. Hum Pathol 18: 863-866. 495. Cina SJ, Richardson MS, Austin RM,Kurman RJ (1997). Immunohistochemicalstaining for Ki-67 antigen, carcinoembry-onic antigen, and p53 in the differentialdiagnosis of glandular lesions of thecervix. Mod Pathol 10: 176-180. 496. Cinel L, Taner D, Nabaei SM, Dogan M(2000). Aggressive angiomyxoma of thevagina. Report of a distinctive type gyne-cologic soft tissue neoplasm. Acta ObstetGynecol Scand 79: 232-233. 497. Cirisano FD Jr., Robboy SJ, Dodge RK,Bentley RC, Krigman HR, Synan IS, SoperJT, Clarke-Pearson DL (2000). The outcomeof stage I-II clinically and surgically stagedpapillary serous and clear cell endometrialcancers when compared with endometri-oid carcinoma. Gynecol Oncol 77: 55-65. 498. Clark WH Jr., Hood AF, Tucker MA,Jampel RM (1998). Atypical melanocyticnevi of the genital type with a discussion ofreciprocal parenchymal-stromal interac-tions in the biology of neoplasia. H u mPathol 29: S1-24. 499. Claus EB, Risch N, Thompson WD(1994). Autosomal dominant inheritance ofearly-onset breast cancer. Implications forrisk prediction. Cancer 73: 643-651. 500. Claus EB, Risch N, Thompson WD,Carter D (1993). Relationship betweenbreast histopathology and family history ofbreast cancer. Cancer 71: 147-153.

380 References
501. Claus EB, Risch NJ, Thompson WD(1990). Age at onset as an indicator offamilial risk of breast cancer. Am JEpidemiol 131: 961-972. 502. Clayton F (1986). Pure mucinous carci-nomas of breast: morphologic features andprognostic correlates. Hum Pathol 17: 34-38. 503. Clayton F, Bodian CA, Banogon P,Goetz H, Kancherla P, Lazarovic B. (1992).Reproducibility of diagnosis in noninvasivebreast disease. Lab Invest 66: 12A. 504. Clement PB (1988). Postoperativespindle-cell nodule of the endometrium.Arch Pathol Lab Med 112: 566-568. 505. Clement PB (1993). Tumor-like lesionsof the ovary associated with pregnancy.Int J Gynecol Pathol 12: 108-115. 506. Clement PB (1994). Diseases of theperitoneum (including endometriosis). In:Blaustein's Pathology of the FemaleGenital Tract, RJ Kurman (Ed.) 4th ed.Springer-Verlag: New York. pp. 647-703.507. Clement PB, Azzopardi JG (1983).Microglandular adenosis of the breast--alesion simulating tubular carcinoma.Histopathology 7: 169-180. 508. Clement PB, Dimmick JE (1979).Endodermal variant of mature cystic ter-atoma of the ovary: report of a case.Cancer 43: 383-385. 509. Clement PB, Oliva E, Young RH (1996).Mullerian adenosarcoma of the uterinecorpus associated with tamoxifen therapy:a report of six cases and a review oftamoxifen-associated endometrial lesions.Int J Gynecol Pathol 15: 222-229. 510. Clement PB, Scully RE (1974).Mullerian adenosarcoma of the uterus. Aclinicopathologic analysis of ten cases of adistinctive type of mullerian mixed tumor.Cancer 34: 1138-1149. 511. Clement PB, Scully RE (1976). Uterinetumors resembling ovarian sex-cordtumors. A clinicopathologic analysis offourteen cases. Am J Clin Pathol 66: 512-525. 512. Clement PB, Scully RE (1978).Extrauterine mesodermal (mullerian)adenosarcoma: a clinicopathologic analy-sis of five cases. Am J Clin Pathol 69: 276-283. 513. Clement PB, Scully RE (1980). Largesolitary luteinized follicle cyst of pregnan-cy and puerperium: A clinicopathologicalanalysis of eight cases. Am J Surg Pathol4: 431-438. 514. Clement PB, Scully RE (1990).Mullerian adenofibroma of the uterus withinvasion of myometrium and pelvic veins.Int J Gynecol Pathol 9: 363-371. 515. Clement PB, Scully RE (1990).Mullerian adenosarcoma of the uterus: aclinicopathologic analysis of 100 caseswith a review of the literature. Hum Pathol21: 363-381. 516. Clement PB, Scully RE (1992).Endometrial stromal sarcomas of theuterus with extensive endometrioid glan-dular differentiation: a report of threecases that caused problems in differentialdiagnosis. Int J Gynecol Pathol 11: 163-173. 517. Clement PB, Young RH (1987). Atypicalpolypoid adenomyoma of the uterus asso-ciated with Turner's syndrome. A report ofthree cases, including a review of "estro-gen-associated" endometrial neoplasmsand neoplasms associated with Turner'ssyndrome. Int J Gynecol Pathol 6: 104-113. 518. Clement PB, Young RH (1987). Diffuseleiomyomatosis of the uterus: a report offour cases. Int J Gynecol Pathol 6: 322-330.
518 a. Clement PB, Young RH (1999). Floridcystic endosalpingiosis with tumor-likemanifestations: a report of four casesincluding the first reported cases of trans-mural endosalpingiosis of the uterus. Am JSurg Pathol 23: 166-175. 519. Clement PB, Young RH, Azzopardi JG(1987). Collagenous spherulosis of thebreast. Am J Surg Pathol 11: 411-417. 520. Clement PB, Young RH, Hanna W,Scully RE (1994). Sclerosing peritonitisassociated with luteinized thecomas of theovary. A clinicopathological analysis of sixcases. Am J Surg Pathol 18: 1-13. 521. Clement PB, Young RH, Keh P, ÖstörAG, Scully RE (1995). Malignantmesonephric neoplasms of the uterinecervix. A report of eight cases, includingfour with a malignant spindle cell compo-nent. Am J Surg Pathol 19: 1158-1171. 522. Clement PB, Young RH, Scully RE(1987). Endometrioid-like variant of ovarianyolk sac tumor. A clinicopathologicalanalysis of eight cases. Am J Surg Pathol11: 767-778. 523. Clement PB, Young RH, Scully RE(1988). Intravenous leiomyomatosis of theuterus. A clinicopathological analysis of 16cases with unusual histologic features.Am J Surg Pathol 12: 932-945. 524. Clement PB, Young RH, Scully RE(1988). Ovarian granulosa cell prolifera-tions of pregnancy: a report of nine cases.Hum Pathol 19: 657-662. 525. Clement PB, Young RH, Scully RE(1992). Diffuse, perinodular, and other pat-terns of hydropic degeneration within andadjacent to uterine leiomyomas. Problemsin differential diagnosis. Am J Surg Pathol16: 26-32. 526. Clement PB, Young RH, Scully RE(1996). Malignant mesotheliomas present-ing as ovarian masses. A report of ninecases, including two primary ovarianmesotheliomas. Am J Surg Pathol 20: 1067-1080. 527. Clement PB, Zubovits JT, Young RH,Scully RE (1998). Malignant mullerianmixed tumors of the uterine cervix: a reportof nine cases of a neoplasm with morphol -ogy often different from its counterpart inthe corpus. Int J Gynecol Pathol 17: 211-222. 528. Clifford GM, Smith JS, Plummer M,Munoz N, Franceschi S (2003). Humanpapillomavirus types in invasive cervicalcancer worldwide: a meta-analysis. Br JCancer 88: 63-73. 529. Cobleigh MA, Vogel CL, Tripathy D,Robert NJ, Scholl S, Fehrenbacher L,Wolter JM, Paton V, Shak S, Lieberman G,Slamon DJ (1999). Multinational study ofthe efficacy and safety of humanized anti-HER2 monoclonal antibody in women whohave HER2-overexpressing metastaticbreast cancer that has progressed afterchemotherapy for metastatic disease. JClin Oncol 17: 2639-2648. 530. Cohen C, Guarner J, DeRose PB (1993).Mammary Paget's disease and associatedcarcinoma. An immunohistochemicalstudy. Arch Pathol Lab Med 117: 291-294. 531. Cohen I, Altaras MM, Shapira J,Tepper R, Rosen DJ, Cordoba M, Zalel Y,Figer A, Yigael D, Beyth Y (1996). Time-dependent effect of tamoxifen therapy onendometrial pathology in asymptomaticpostmenopausal breast cancer patients.Int J Gynecol Pathol 15: 152-157.
532. Cohen MA, Morris EA, Rosen PP,Dershaw DD, Liberman L, Abramson AF(1996). Pseudoangiomatous stromal hyper-plasia: mammographic, sonographic, andclinical patterns. Radiology 198: 117-120. 533. Cohen MB, Mulchahey KM, Molnar JJ(1986). Ovarian endodermal sinus tumorwith intestinal differentiation. Cancer 57:1580-1583. 534. Cohen PL, Brooks JJ (1991).Lymphomas of the breast. A clinicopatho-logic and immunohistochemical study ofprimary and secondary cases. Cancer 67:1359-1369. 535. Cohen PR, Kohn SR, Kurzrock R (1991).Association of sebaceous gland tumorsand internal malignancy: the Muir-Torresyndrome. Am J Med 90: 606-613. 536. Cohn-Cedermark G, Rutqvist LE,Rosendahl I, Silfversward C (1991).Prognostic factors in cystosarcoma phyl-lodes. A clinicopathologic study of 77patients. Cancer 68: 2017-2022. 537. Cokelaere K, Michielsen P, De Vos R,Sciot R (2001). Primary mesenteric malig-nant mixed mesodermal (mullerian) tumorwith neuroendocrine differentiation. ModPathol 14: 515-520. 538. Colgan TJ (1998). Vulvar intraepithelialneoplasia: a synopsis of recent develop-ments. J Lower Genital Tract Disease 2: 31-36. 539. Collaborative Group on HormonalFactors in Breast Cancer (1996). Breastcancer and hormonal contraceptives: col-laborative reanalysis of individual data on53 297 women with breast cancer and 100239 women without breast cancer from 54epidemiological studies. Lancet 347: 1713-1727. 540. Collaborative Group on HormonalFactors in Breast Cancer (1997). Breastcancer and hormone replacement therapy:collaborative reanalysis of data from 51epidemiological studies of 52,705 womenwith breast cancer and 108,411 womenwithout breast cancer. Lancet 350: 1047-1059. 541. Collins N, Wooster R, Stratton MR(1997). Absence of methylation of CpG din -ucleotides within the promoter of thebreast cancer susceptibility gene BRCA2in normal tissues and in breast and ovariancancers. Br J Cancer 76: 1150-1156. 542. Collins RJ, Cheung A, Ngan HY, WongLC, Chan SY, Ma HK (1991). Primary mixedneuroendocrine and mucinous carcinomaof the ovary. Arch Gynecol Obstet 248: 139-143. 543. Colombat M, Sevestre H, Gontier MF(2001). Epithelioid leiomyosarcoma of theuterine cervix. Report of a case. A n nPathol 21: 48-50. 544. Colome MI, Ro JY, Ayala AG, El-Nagger A, Siddiqui RT, Ordonez NG (1996).Adenoid cystic carcinoma of the breastmetastatic tio the kidney. J PatholBacteriol 4: 69-78. 545. Colpaert C, Vermeulen P, Jeuris W,van Beest P, Goovaerts G, Weyler J, VanDam P, Dirix L, Van Marck E (2001). Earlydistant relapse in "node-negative" breastcancer patients is not predicted by occultaxillary lymph node metastases, but by thefeatures of the primary tumour. J Pathol193: 442-449. 546. Comerci JT Jr., Licciardi F, Bergh PA,Gregori C, Breen JL (1994). Mature cysticteratoma: a clinicopathologic evaluation of517 cases and review of the literature.Obstet Gynecol 84: 22-28.
547. Conant EF, Dillon RL, Palazzo J, EhrlichSM, Feig SA (1994). Imaging findings inmucin-containing carcinomas of thebreast: correlation with pathologic fea-tures. AJR Am J Roentgenol 163: 821-824. 548. Connolly DC, Katabuchi H, Cliby WA,Cho KR (2000). Somatic mutations in theSTK11/LKB1 gene are uncommon in raregynecological tumor types associated withPeutz-Jegher's syndrome. Am J Pathol156: 339-345. 549. Conran RM, Hitchcock CL, Popek EJ,Norris HJ, Griffin JL, Geissel A, McCarthyWF (1993). Diagnostic considerations inmolar gestations. Hum Pathol 24: 41-48. 550. Contesso G, Mouriesse H, Friedman S,Genin J, Sarrazin D, Rouesse J (1987). Theimportance of histologic grade in long-term prognosis of breast cancer: a study of1,010 patients, uniformly treated at theInstitut Gustave-Roussy. J Clin Oncol 5:1378-1386. 551. Cook DL, Weaver DL (1995).Comparison of DNA content, S-phase frac-tion, and survival between medullary andductal carcinoma of the breast. Am J ClinPathol 104: 17-22. 552. Cooper HS, Patchefsky AS, Krall RA(1978). Tubular carcinoma of the breast.Cancer 42: 2334-2342. 553. Copas P, Dyer M, Hall DJ, Diddle AW(1981). Granular cell myoblastoma of theuterine cervix. Diagn Gynecol Obstet 3:251-254. 554. Copeland LJ, Cleary K, Sneige N,Edwards CL (1985). Neuroendocrine(Merkel cell) carcinoma of the vulva: acase report and review of the literature.Gynecol Oncol 22: 367-378. 555. Copeland LJ, Gershenson DM, SaulPB, Sneige N, Stringer CA, Edwards CL(1985). Sarcoma botryoides of the femalegenital tract. Obstet Gynecol 66: 262-266. 556. Copeland LJ, Sneige N, GershensonDM, Saul PB, Stringer CA, Seski JC (1986).Adenoid cystic carcinoma of Bartholingland. Obstet Gynecol 67: 115-120. 557. Copeland LJ, Sneige N, Ordonez NG,Hancock KC, Gershenson DM, Saul PB,Kavanagh JJ (1985). Endodermal sinustumor of the vagina and cervix. Cancer 55:2558-2565. 558. Copeland LJ, Sneige N, Stringer CA,Gershenson DM, Saul PB, Kavanagh JJ(1985). Alveolar rhabdomyosarcoma of thefemale genitalia. Cancer 56: 849-855. 559. Cornelis RS, Devilee P, van Vliet M,Kuipers-Dijkshoorn N, Kersenmaeker A,Bardoel A, Khan PM, Cornelisse CJ (1993).Allele loss patterns on chromosome 17q in109 breast carcinomas indicate at leasttwo distinct target regions. Oncogene 8:781-785. 560. Cornelis RS, Neuhausen SL,Johansson O, Arason A, Kelsell D, PonderBA, Tonin P, Hamann U, Lindblom A, LalleP, Longy M, Olah E, Scherneck S, BignonYJ, Sobol H, Changclaude J, Larsson C,Spurr N, Borg A, Barkardottir RB, Narod S,Devilee P. (1995). High allele loss rates at17q12-q21 in breast and ovarian tumorsfrom BRCAl-linked families. The BreastCancer Linkage Consortium. G e n e sChromosomes Cancer 13: 203-210.561. Costa A (1974). [A little known variantof pure adenoma of the breast: pure apoc -rine cell adenoma (with a classification ofbreast adenomas)]. Arch De Vecchi AnatPatol 60: 393-401.

381References
562. Costa MJ, Ames PF, Walls J, Roth LM(1997). Inhibin immunohistochemistryapplied to ovarian neoplasms: a novel,effective, diagnostic tool. Hum Pathol 28:1247-1254. 563. Costa MJ, DeRose PB, Roth LM,Brescia RJ, Zaloudek CJ, Cohen C (1994).Immunohistochemical phenotype of ovari-an granulosa cell tumors: absence ofepithelial membrane antigen has diagnos-tic value. Hum Pathol 25: 60-66. 564. Costa MJ, Hansen C, Dickerman A,Scudder SA (1998). Clinicopathologic sig-nificance of transitional cell carcinomapattern in nonlocalized ovarian epithelialtumors (stages 2-4). Am J Clin Pathol 109:173-180. 565. Costa MJ, McIlnay KR, Trelford J(1995). Cervical carcinoma with glandulardifferentiation: histological evaluation pre-dicts disease recurrence in clinical stage Ior II patients. Hum Pathol 26: 829-837. 566. Costa MJ, Silverberg SG (1989).Oncocytic carcinoma of the male breast.Arch Pathol Lab Med 113: 1396-1399. 567. Costa MJ, Thomas W, Majmudar B,Hewan-Lowe K (1992). Ovarian myxoma:ultrastructural and immunohistochemicalfindings. Ultrastruct Pathol 16: 429-438. 568. Coukos G, Makrigiannakis A, Chung J,Randall TC, Rubin SC, Benjamin I (1999).Complete hydatidiform mole. A diseasewith a changing profile. J Reprod Med 44:698-704. 569. Coyne J.D. (2001). Apocrine ductalcarcinoma in-situ with an unusual morpho-logical presentation. Histopathology 3 8 :277-280. 570. Cozen W, Bernstein L, Wang F, PressMF, Mack TM (1999). The risk of angiosar-coma following primary breast cancer. BrJ Cancer 81: 532-536. 571. Craig JR, Hart WR (1979). Extragenitaladenomatoid tumor: Evidence for themesothelial theory of origin. Cancer 43:1678-1681. 572. Cramer SF, Roth LM, Ulbright TM,Mazur MT, Nunez CA, Gersell DJ, Mills SE,Kraus FT (1987). Evaluation of the repro-ducibility of the World Health Organizationclassification of common ovarian cancers.With emphasis on methodology. A r c hPathol Lab Med 111: 819-829. 573. Crawford D, Nimmo M, Clement PB,Thomson T, Benedet JL, Miller D, Gilks CB(1999). Prognostic factors in Paget's dis-ease of the vulva: a study of 21 cases.Int JGynecol Pathol 18: 351-359. 5 7 4 . Creasman W, Ondicino F,Maisonneuve P, Benefet J, Shepherd J(1998). Carcinoma of the corpus uteri:Annual report on the results of treatment ingynaecological cancer. J EpidemiolBiostat 3: 46-47. 575. Creasman WT (1993). Prognostic sig-nificance of hormone receptors inendometrial cancer. Cancer 71: 1467-1470. 5 7 6 . Creasman WT, Odicino F,Maisonneuve P, Beller U, Benedet JL,Heintz AP, Ngan HY, Sideri M, Pecorelli S(2001). Carcinoma of the corpus uteri. JEpidemiol Biostat 6: 47-86. 577. Creasman WT, Phillips JL, Menck HR(1998). The National Cancer Data Basereport on cancer of the vagina. Cancer 83:1033-1040. 578. Crichlow RW, Galt SW (1990). Malebreast cancer. Surg Clin North Am 70:1165-1177.
579. Crissman JD, Visscher DW, Kubus J(1990). Image cytophotometric DNA analy -sis of atypical hyperplasias and intraductalcarcinomas of the breast. Arch Pathol LabMed 114: 1249-1253. 580. Crook T, Brooks LA, Crossland S, OsinP, Barker KT, Waller J, Philp E, Smith PD,Yulug I, Peto J, Parker G, Allday MJ,Crompton MR, Gusterson BA (1998). p53mutation with frequent novel condons butnot a mutator phenotype in B. Oncogene17: 1681-1689. 581. Crook T, Crossland S, Crompton MR,Osin P, Gusterson BA (1997). p53 mutationsin BRCA1-associated familial breast can-cer. Lancet 350: 638-639. 582. Crowe J, Hakes T, Rosen PP, RosenPP, Kinne DW, Robbins GF. (1985).Changing trends in the management ofinflammatory breast cancer: a clinical-pathological review of 69 patients. Am JClin Oncol 8: 21. 583. Crozier MA, Copeland LJ, Silva EG,Gershenson DM, Stringer CA (1989). Clearcell carcinoma of the ovary: a study of 59cases. Gynecol Oncol 35: 199-203. 584. Crum CP (1992). Carcinoma of thevulva: epidemiology and pathogenesis.Obstet Gynecol 79: 448-454. 585. Crum CP, Fu YS, Levine RU, RichartRM, Townsend DE, Fenoglio CM (1982).Intraepithelial squamous lesions of thevulva: biologic and histologic criteria forthe distinction of condylomas from vulvarintraepithelial neoplasia. Am J ObstetGynecol 144: 77-83. 586. Crum CP, Ikenberg H, Richart RM,Gissman L (1984). Human papillomavirustype 16 and early cervical neoplasia. NEngl J Med 310: 880-883. 587. Crum CP, Mitao M, Levine RU,Silverstein S (1985). Cervical papillo-maviruses segregate within morphologi-cally distinct precancerous lesions. J Virol54: 675-681.588. Crum CP, Rogers BH, Andersen W(1980). Osteosarcoma of the uterus: casereport and review of the literature.Gynecol Oncol 9: 256-268. 589. Cuatrecasas M, Erill N, Musulen E,Costa I, Matias-Guiu X, Prat J (1998). K-rasmutations in nonmucinous ovarian epithe-lial tumors: a molecular analysis and clini-copathologic study of 144 patients. Cancer82: 1088-1095. 590. Cuatrecasas M, Matias-Guiu X, Prat J(1996). Synchronous mucinous tumors ofthe appendix and the ovary associatedwith pseudomyxoma peritonei. A clinico-pathologic study of six cases with compar-ative analysis of c-Ki-ras mutations. Am JSurg Pathol 20: 739-746. 591. Cuatrecasas M, Villanueva A, Matias-Guiu X, Prat J (1997). K-ras mutations inmucinous ovarian tumors: a clinicopatho-logic and molecular study of 95 cases.Cancer 79: 1581-1586. 592. Cui J, Antoniou AC, Dite GS, SoutheyMC, Venter DJ, Easton DF, Giles GG,McCredie MR, Hopper JL (2001). AfterBRCA1 and BRCA2-what next?Multifactorial segregation analyses ofthree-generation, population-basedAustralian families affected by femalebreast cancer. Am J Hum Genet 68: 420-431. 592a. Cui S, Lespinasse P, Cracchiolo B,Sama J, Kreitzer MS, Heller DS (2001).Large cell neuroendocrine carcinoma ofthe cervix associated with adenocarcino-ma in situ: evidence of a common origin.Int J Gynecol Pathol 20: 311-312.
593. Cummings MC, Aubele M, Mattis A,Purdie D, Hutzler P, Hofler H, Werner M(2000). Increasing chromosome 1 copynumber parallels histological progressionin breast carcinogenesis. Br J Cancer 82:1204-1210. 594. Cunha TM, Felix A, Cabral I (2001).Preoperative assessment of deep myome-trial and cervical invasion in endometrialcarcinoma: comparison of magnetic reso-nance imaging and gross visual inspec-tion. Int J Gynecol Cancer 11: 130-136. 595. Cunningham JM, Kim CY, ChristensenER, Tester DJ, Parc Y, Burgart LJ, HallingKC, McDonnell SK, Schaid DJ, Walsh VC,Kubly V, Nelson H, Michels VV, ThibodeauSN (2001). The frequency of hereditarydefective mismatch repair in a prospectiveseries of unselected colorectal carcino-mas. Am J Hum Genet 69: 780-790. 596. Cuny M, Kramar A, Courjal F,Johannsdottir V, Iacopetta B, Fontaine H,Grenier J, Culine S, Theillet C (2000).Relating genotype and phenotype in breastcancer: an analysis of the prognostic sig-nificance of amplification at eight differentgenes or loci and of p53 mutations. CancerRes 60: 1077-1083. 597. Curry JL, Olejnik JL, Wojcik EM (2001).Cellular angiofibroma of the vulva withDNA ploidy analysis. Int J Gynecol Pathol20: 200-203. 598. Curtin JP, Rubin SC, Hoskins WJ,Hakes TB, Lewis JL Jr. (1989). Second-looklaparotomy in endodermal sinus tumor: areport of two patients with normal levels ofalpha-fetoprotein and residual tumor atreexploration. Obstet Gynecol 73: 893-895. 599. Curtin JP, Saigo P, Slucher B,Venkatraman ES, Mychalczak B, HoskinsWJ (1995). Soft-tissue sarcoma of the vagi-na and vulva: a clinicopathologic study.Obstet Gynecol 86: 269-272. 600. Cushing B, Giller R, Ablin A, Cohen L,Cullen J, Hawkins E, Heifetz SA, Krailo M,Lauer SJ, Marina N, Rao PV, Rescorla F,Vinocur CD, Weetman RM, Castleberry RP(1999). Surgical resection alone is effectivetreatment for ovarian immature teratomain children and adolescents: a report of thepediatric oncology group and the chil-dren's cancer group. Am J Obstet Gynecol181: 353-358. 601. Cutuli B, Borel C, Dhermain F, MagriniSM, Wasserman TH, Bogart JA, ProvencioM, de Lafontan B, de la RA, Cellai E, GraicY, Kerbrat P, Alzieu C, Teissier E, DilhuydyJM, Mignotte H, Velten M (2001). Breastcancer occurred after treatment forHodgkin's disease: analysis of 133 cases.Radiother Oncol 59: 247-255. 602. Cutuli B, Dilhuydy JM, de Lafontan B,Berlie J, Lacroze M, Lesaunier F, Graic Y,Tortochaux J, Resbeut M, Lesimple T,Gamelin E, Campana F, Reme-Saumon M,Moncho-Bernier V, Cuilliere JC, MarchalC, De Gislain G, N'Guyen TD, Teissier E,Velten M (1997). Ductal carcinoma in situof the male breast. Analysis of 31 cases.Eur J Cancer 33: 35-38. 603. Czernobilsky B (1967). Intracystic car-cinoma of the female breast. Surg GynecolObstet 124: 93-98. 604. Czernobilsky B, Gillespie JJ, Roth LM(1982). Adenosarcoma of the ovary. A light-and electron-microscopic study withreview of the literature. Diagn GynecolObstet 4: 25-36. 604a. Czernobilsky B, Lancet M (1972).Broad ligament adenocarcinoma ofMullerian origin. Obstet Gynecol 40: 238-242.
605. Czernobilsky B, Moll R, Levy R, FrankeWW (1985). Co-expression of cytokeratinand vimentin filaments in mesothelial,granulosa and rete ovarii cells of thehuman ovary. Eur J Cell Biol 37: 175-190. 606. d'Ablaing G III, Klatt EC, DiRocco G,Hibbard LT (1983). Broad ligament seroustumor of low malignant potential. Int JGynecol Pathol 2: 93-99. 607. D'Avanzo B, La Vecchia C (1995). Riskfactors for male breast cancer. Br JCancer 71: 1359-1362. 608. D'Orsi CJ, Feldhaus L, Sonnenfeld M(1983). Unusual lesions of the breast.Radiol Clin North Am 21: 67-80. 609. Dal Cin P, Timmerman D, Van denBerghe H, Wanschura S, Kazmierczak B,Vergote I, Deprest J, Neven P, Moerman P,Bullerdiek J, Van den Berghe H (1998).Genomic changes in endometrial polypsassociated with tamoxifen show no evi-dence for its action as an external carcino-gen. Cancer Res 58: 2278-2281. 610. Dalal P, Shousha S (1995). Keratin 19 inparaffin sections of medullary carcinomaand other benign and malignant breastlesions. Mod Pathol 8: 413-416. 611. Daling JR, Sherman KJ, Hislop TG,Maden C, Mandelson MT, Beckmann AM,Weiss NS (1992). Cigarette smoking andthe risk of anogenital cancer. Am JEpidemiol 135: 180-189. 612. Dalton LW, Page DL, Dupont WD(1994). Histologic grading of breast carci-noma. A reproducibility study. Cancer 73:2765-2770. 6 1 3 . Daly MB (1992). Ovarian Cancer.Hematology/oncology clinics of NorthAmerica. The epidemiology of ovariancancer. WB Saunders: Philadelphia.614. Damajanov I, Drobnjak P, Grizelj V,Longhino N (1975). Sclerosing stromaltumor of the ovary: A hormonal and ultra-structural analysis. Obstet Gynecol 45: 675-679. 615. Damiani S, Dina R, Eusebi V (1999).Eosinophilic and granular cell tumors ofthe breast. Semin Diagn Pathol 16: 117-125. 616. Damiani S, Eusebi V, Losi L, D'Adda T,Rosai J (1998). Oncocytic carcinoma(malignant oncocytoma) of the breast. AmJ Surg Pathol 22: 221-230. 617. Damiani S, Koerner FC, Dickersin GR,Cook MG, Eusebi V (1992). Granular celltumour of the breast. Virchows Arch APathol Anat Histopathol 420: 219-226. 618. Damiani S, Panarelli M (1996).Mammary adenohibernoma. H i s t o p a t h o l o g y28: 554-555. 619. Damiani S, Pasquinelli G, Lamovec J,Peterse JL, Eusebi V (2000). Acinic cell car-cinoma of the breast: an immunohisto-chemical and ultrastructural study.Virchows Arch 437: 74-81. 620. Damjanov I, Amenta PS, Zarghami F(1984). Transformation of an AFP-positiveyolk sac carcinoma into an AFP-negativeneoplasm. Evidence for in vivo cloning ofthe human parietal yolk sac carcinoma.Cancer 53: 1902-1907. 621. Dammann R, Li C, Yoon JH, Chin PL,Bates S, Pfeifer GP (2000). Epigenetic inac-tivation of a RAS association domain fami -ly protein from the lung tumour suppressorlocus 3p21.3. Nat Genet 25: 315-319. 622. Dammann R, Yang G, Pfeifer GP (2001).Hypermethylation of the cpG island of Rasassociation domain family 1A (RASSF1A), aputative tumor suppressor gene from the3p21.3 locus, occurs in a large percentageof human breast cancers. Cancer Res 61:3105-3109.

382 References
623. Daroca PJ Jr. (1987). Medullary carci-noma of the breast with granulomatousstroma. Hum Pathol 18: 761-763. 624. Daroca PJ Jr., Reed RJ, Love GL,Kraus SD (1985). Myoid hamartomas of thebreast. Hum Pathol 16: 212-219. 625. Dasouki M, Ishmael H, Eng C (2001).Macrocephaly, macrosomia and autisticbehavior due to a de novo PTEN germlinemutation. Am J Hum Genet 69S: 280. 626. Davies JD, Mera SL (1987). Elastosis inbreast carcinoma: II. Association of pro-tease inhibitors with immature elasticfibres. J Pathol 153: 317-324. 627. Davis BW, Gelber R, Goldhirsch A,Hartmann WH, Hollaway L, Russell I,Rudenstam CM (1985). Prognostic signifi-cance of peritumoral vessel invasion inclinical trials of adjuvant therapy for breastcancer with axillary lymph node metasta-sis. Hum Pathol 16: 1212-1218. 628. Davis DL, Bradlow HL, Wolff M,Woodruff T, Hoel DG, Anton-Culver H(1993). Medical hypothesis: xenoestrogensas preventable causes of breast cancer.Environ Health Perspect 101: 372-377. 629. Davis GD, Patton WS (1983). Capillaryhemangioma of the cervix and vagina:management with carbon dioxide laser.Obstet Gynecol 62: 95s-96s. 630. Davis GL (1996). Malignant melanomaarising in mature ovarian cystic teratoma(dermoid cyst). Report of two cases and lit-erature analysis. Int J Gynecol Pathol 15:356-362. 631. Davis KP, Hartmann LK, Keeney GL,Shapiro H (1996). Primary ovarian carci-noid tumors. Gynecol Oncol 61: 259-265. 632. Davis S, Mirick DK, Stevens RG (2001).Night shift work, light at night, and risk ofbreast cancer. J Natl Cancer Inst 93: 1557-1562. 633. Davos I, Abell MR (1976). Sarcomas ofthe vagina. Obstet Gynecol 47: 342-350. 634. Daw E (1971). Primary carcinoma ofthe vagina. J Obstet Gynaecol BrCommonw 78: 853-856. 635. Dawson PJ, Ferguson DJ, Karrison T(1982). The pathological findings of breastcancer in patients surviving 25 years afterradical mastectomy. Cancer 50: 2131-2138. 636. Dawson PJ, Schroer KR, Wolman SR(1996). ras and p53 genes in male breastcancer. Mod Pathol 9: 367-370. 637. Daya D (1994). Malignant femaleadnexal tumor of probable wolffian originwith review of the literature. Arch PatholLab Med 118: 310-312. 638. Daya D, Lukka H, Clement PB (1992).Primitive neuroectodermal tumors of theuterus: a report of four cases. Hum Pathol23: 1120-1129. 639. Daya D, Nazerali L, Frank GL (1992).Metastatic ovarian carcinoma of largeintestinal origin simulating primary ovariancarcinoma. A clinicopathologic study of 25cases. Am J Clin Pathol 97: 751-758. 640. Daya D, Sabet L (1991). The use ofcytokeratin as a sensitive and reliablemarker for trophoblastic tissue. Am J ClinPathol 95: 137-141. 641. Daya D, Young RH, Scully RE (1992).Endometrioid carcinoma of the fallopiantube resembling an adnexal tumor of prob-able wolffian origin: a report of six cases.Int J Gynecol Pathol 11: 122-130. 642. Daya DA, Scully RE (1988). Sarcomabotryoides of the uterine cervix in youngwomen: a clinicopathological study of 13cases. Gynecol Oncol 29: 290-304.
643. de Cremoux P, Salomon AV, Liva S,Dendale R, Bouchind'homme B, Martin E,Sastre-Garau X, Magdelenat H, FourquetA, Soussi T (1999). p53 mutation as a genet-ic trait of typical medullary breast carcino-ma. J Natl Cancer Inst 91: 641-643. 644. de Deus JM, Focchi J, Stavale JN, deLima GR (1995). Histologic and biomolecu-lar aspects of papillomatosis of the vulvarvestibule in relation to human papillo-mavirus. Obstet Gynecol 86: 758-763. 645. de Fusco PA, Gaffey TA, Malkasian GDJr., Long HJ, Cha SS (1989). Endometrialstromal sarcoma: review of Mayo Clinicexperience, 1945-1980. Gynecol Oncol 35:8-14. 646. de Hullu JA, Doting E, Piers DA,Hollema H, Aalders JG, Koops HS,Boonstra H, van der Zee AG (1998).Sentinel lymph node identification withtechnetium-99m-labeled nanocolloid insquamous cell cancer of the vulva. J NuclMed 39: 1381-1385. 647. de la Fuente AA (1982). Benign mixedMullerian tumour--adenofibroma of the fal-lopian tube. Histopathology 6: 661-666. 648. de la Rochefordiere A, Asselain B,Scholl S, Campana F, Ucla L, Vilcoq JR,Durand JC, Pouillart P, Fourquet A (1994).Simultaneous bilateral breast carcinomas:a retrospective review of 149 cases. Int JRadiat Oncol Biol Phys 30: 35-41. 6 4 9 . de Leeuw WJ, Berx G, Vos CB,Peterse JL, Van de Vijver MJ, Litvinov S,van Roy F, Cornelisse CJ, Cleton-JansenAM (1997). Simultaneous loss of E-cad-herin and catenins in invasive lobularbreast cancer and lobular carcinoma insitu. J Pathol 183: 404-411. 650. de Leeuw WJ, Dierssen J, Vasen HF,Wijnen JT, Kenter GG, Meijers-Heijboer H,Brocker-Vriends A, Stormorken A, MollerP, Menko F, Cornelisse CJ, Morreau H(2000). Prediction of a mismatch repairgene defect by microsatellite instabilityand immunohistochemical analysis inendometrial tumours from HNPCC patients.J Pathol 192: 328-335. 651. de Nictolis M, Curatola A, TommasoniS, Magiera G (1994). High-grade endome-trial stromal sarcoma: clinicopathologicand immunohistochemical study of a case.Pathologica 86: 217-221. 652. de Nictolis M, Montironi R,Tommasoni S, Carinelli S, Ojeda B, Matias-Guiu X, Prat J (1992). Serous borderlinetumors of the ovary. A clinicopathologic,immunohistochemical, and quantitativestudy of 44 cases. Cancer 70: 152-160. 653. de Nictolis M, Montironi R,Tommasoni S, Valli M, Pisani E, Fabris G,Prat J (1994). Benign, borderline, and well-differentiated malignant intestinal muci-nous tumors of the ovary: a clinicopatho-logic, histochemical, immunohisto-chemical, and nuclear quantitative studyof 57 cases. Int J Gynecol Pathol 13: 10-21. 654. de Rosa G, Boscaino A, TerraccianoLM, Giordano G (1992). Giant adenomatoidtumors of the uterus. Int J Gynecol Pathol11: 156-160. 655. de Wind N, Dekker M, van Rossum A,van der Valk M, te Riele H (1998). Mousemodels for hereditary nonpolyposis col-orectal cancer. Cancer Res 58: 248-255. 6 5 6 . de Mascarel I, MacGrogan G,Mathoulin-Pelissier S, Soubeyran I, PicotV, Coindre JM (2002). Breast ductal carci-noma in situ with microinvasion: a defini-tion supported by a long-term study of 1248serially sectioned ductal carcinomas.Cancer 94: 2134-2142.
657. de Vivo I, Gertig DM, Nagase S,Hankinson SE, O'Brien R, Speizer FE,Parsons R, Hunter DJ (2000). Novelgermline mutations in the PTEN tumoursuppressor gene found in women withmultiple cancers. J Med Genet 37: 336-341. 658. Deavers MT, Gershenson DM,Tortolero-Luna G, Malpica A, Lu KH, SilvaEG (2002). Micropapillary and cribriformpatterns in ovarian serous tumors of lowmalignant potential: a study of 99advanced stage cases. Am J Surg Pathol26: 1129-1141. 659. de Hoop TA, Mira J, Thomas MA(1997). Endosalpingiosis and chronic pelvicpain. J Reprod Med 42: 613-616. 660. Dekel A, van Iddekinge B, Isaacson C,Dicker D, Feldberg D, Goldman J (1986).Primary choriocarcinoma of the fallopiantube. Report of a case with survival andpostoperative delivery. Review of the liter -ature. Obstet Gynecol Surv 41: 142-148. 661. Del Giudice ME, Fantus IG, Ezzat S,McKeown-Eyssen G, Page D, Goodwin PJ(1998). Insulin and related factors in pre-menopausal breast cancer risk. B r e a s tCancer Res Treat 47: 111-120. 662. Delaloye JF, Ruzicka J, de Grandi P(1993). An ovarian tumor of probableWolffian origin. Acta Obstet GynecolScand 72: 314-316. 663. Delgado G, Bundy B, Zaino R, SevinBU, Creasman WT, Major F (1990).Prospective surgical-pathological study ofdisease-free interval in patients with stageIB squamous cell carcinoma of the cervix:a Gynecologic Oncology Group study.Gynecol Oncol 38: 352-357. 664. Deligdisch L, Hirschmann S, Altchek A(1997). Pathologic changes ingonadotropin releasing hormone agonistanalogue treated uterine leiomyomata.Fertil Steril 67: 837-841. 665. Deligdisch L, Kalir T, Cohen CJ, deLatour M, Le Bouedec G, Penault-Llorca F(2000). Endometrial histopathology in 700patients treated with tamoxifen for breastcancer. Gynecol Oncol 78: 181-186. 666. Dellas A, Schultheiss E, Holzgreve W,Oberholzer M, Torhorst J, Gudat F (1997).Investigation of the Bcl-2 and C-mycexpression in relationship to the Ki-67labelling index in cervical intraepithelialneoplasia. Int J Gynecol Pathol 16: 212-218. 667. de Matos P, Tyler D, Seigler HF (1998).Mucosal melanoma of the female geni-talia: a clinicopathologic study of forty-three cases at Duke University MedicalCenter. Surgery 124: 38-48. 668. de May RM, Kay S (1984). Granular celltumor of the breast. Pathol Annu 19 Pt 2:121-148. 669. Demers PA, Thomas DB, RosenblattKA, Jimenez LM, McTiernan A, StalsbergH, Stemhagen A, Thompson WD, CurnenMG, Satariano W, Austin DF, Isacson P,Greenberg RS, Key C, Kolonel LN, WestDW. (1991). Occupational exposure toelectromagnetic fields and breast cancerin men. Am J Epidemiol 134: 340-347. 670. Demopoulos RI, Sitelman A, Flotte T,Bigelow B (1980). Ultrastructural study of afemale adnexal tumor of probable wolffianorigin. Cancer 46: 2273-2280. 671. Deng G, Lu Y, Zlotnikov G, Thor AD,Smith HS (1996). Loss of heterozygosity innormal tissue adjacent to breast carcino-mas. Science 274: 2057-2059.
672. Denley H, Pinder SE, Tan PH, Sim CS,Brown R, Barker T, Gearty J, Elston CW,Ellis IO (2000). Metaplastic carcinoma ofthe breast arising within complex scleros-ing lesion: a report of five cases.Histopathology 36: 203-209. 673. Denton AS, Bond SJ, Matthews S,Bentzen SM, Maher EJ (2000). Nationalaudit of the management and outcome ofcarcinoma of the cervix treated with radio-therapy in 1993. Clin Oncol (R Coll Radiol)12: 347-353. 674. Department of Health (1998). Report onhealth and social subjects No. 48.Nutritional aspects of the development ofcancer. The Stationery Office: Norwich.675. DePasquale SE, McGuinness TB,Mangan CE, Husson M, Woodland MB(1996). Adenoid cystic carcinoma ofBartholin's gland: a review of the literatureand report of a patient. Gynecol Oncol 61:122-125. 676. DePriest PD, Banks ER, Powell DE, vanNagell JR Jr., Gallion HH, Puls LE, HunterJE, Kryscio RJ, Royalty MB (1992).Endometrioid carcinoma of the ovary andendometriosis: the association in post-menopausal women. Gynecol Oncol 47: 71-75. 677. Devaney K, Snyder R, Norris HJ,Tavassoli FA (1993). Proliferative and histo-logically malignant struma ovarii: a clinico-pathologic study of 54 cases. Int J GynecolPathol 12: 333-343. 678. Devaney K, Tavassoli FA (1991).Immunohistochemistry as a diagnostic aidin the interpretation of unusual mesenchy-mal tumors of the uterus. Mod Pathol 4:225-231. 679. Devilee P, Cleton-Jansen A,Cornelisse CJ (2001). Ever since Knudson.Trends Genet 17: 569-573. 680. Devilee P, Cornelisse CJ (1994).Somatic genetic changes in human breastcancer. Biochim Biophys Acta 1198: 113-130. 681. Devouassoux-Shisheboran M,Schammel MD, Man YG, Tavassoli FA(2000). Fibromatosis of the breast: age-cor-related morphofunctional features of 33cases. Arch Pathol Lab Med 124: 276-280. 682. Devouassoux-Shisheboran M, SilverSA, Tavassoli FA (1999). Wolffian adnexaltumor, so-called female adnexal tumor ofprobable Wolffian origin (FATWO):immunohistochemical evidence in supportof a Wolffian origin. Hum Pathol 30: 856-863. 683. Devouassoux-Shisheboran M,Vortmeyer AO, Silver SA, Zhuang Z,Tavassoli FA (2000). Teratomatous geno-type detected in malignancies of a non-germ cell phenotype. Lab Invest 80: 81-86. 684. Dgani R, Shoham Z, Czernobilsky B,Singer D, Shani A, Lancet M (1989).Endolymphatic stromal myosis (endometri-al low-grade stromal sarcoma) presentingwith hematuria: a diagnostic challenge.Gynecol Oncol 35: 263-266. 685. Dhaliwal LK, Das I, Gopalan S (1992).Recurrent leiomyoma of the vagina. Int JGynaecol Obstet 37: 281-283. 686. Dharkar DD, Kraft JR, Gangadharam D(1981). Uterine lipomas. Arch Pathol LabMed 105: 43-45. 687. Di Bonito L, Patriarca S, Falconieri G(1992). Aggressive "breast-like" adenocarci-noma of vulva. Pathol Res Pract 188: 211-214. 688. Di Cristofano A, Pesce B, Cordon-Cardo C, Pandolfi PP (1998). Pten is essen-tial for embryonic development and tumoursuppression. Nat Genet 19: 348-355.

383References
689. Di Domenico A, Stangl F, Bennington J(1982). Leiomyosarcoma of the broad liga-ment. Gynecol Oncol 13: 412-415. 690. DiSant'Agnese PA, Knowles DM (1980).Extracardiac rhabdomyoma: a clinico-pathologic study and review of the litera-ture. Cancer 46: 780-789. 691. Diab SG, Clark GM, Osborne CK, LibbyA, Allred DC, Elledge RM (1999). Tumorcharacteristics and clinical outcome oftubular and mucinous breast carcinomas.J Clin Oncol 17: 1442-1448. 692. Diaz NM, McDivitt RW, Wick MR(1991). Microglandular adenosis of thebreast. An immunohistochemical compari-son with tubular carcinoma. Arch PatholLab Med 115: 578-582. 693. Diaz NM, Palmer JO, McDivitt RW(1991). Carcinoma arising within fibroade-nomas of the breast. A clinicopathologicstudy of 105 patients. Am J Clin Pathol 95:614-622. 694. Dickersin GR, Maluf HM, Koerner FC(1997). Solid papillary carcinoma of breast:an ultrastructural study. Ultrastruct Pathol21: 153-161. 695. Dickersin GR, Scully RE (1993). Anupdate on the electron microscopy ofsmall cell carcinoma of the ovary withhypercalcemia. Ultrastruct Pathol 17: 411-422. 696. Dickersin GR, Scully RE (1998). Ovariansmall cell tumors: an electron microscopicreview. Ultrastruct Pathol 22: 199-226. 697. Dickersin GR, Young RH, Scully RE(1995). Signet-ring stromal and relatedtumors of the ovary. Ultrastruct Pathol 19:401-419. 698. Dickson JM, Mansel RE (2000). ABC ofBreast Diseases. Symptoms, Assessmentand Guidelines for Referral. 2nd ed. BMJBooks: London, pp. 1-5.699. DiCostanzo D, Rosen PP, Gareen I,Franklin S, Lesser M (1990). Prognosis ininfiltrating lobular carcinoma. An analysisof "classical" and variant tumors. Am JSurg Pathol 14: 12-23. 700. Dietl J, Horny HP, Ruck P, Kaiserling E(1993). Dysgerminoma of the ovary. Animmunohistochemical study of tumor-infil-trating lymphoreticular cells and tumorcells. Cancer 71: 2562-2568. 701. Dietrich CU, Pandis N, Teixeira MR,Bardi G, Gerdes AM, Andersen JA, Heim S(1995). Chromosome abnormalities inbenign hyperproliferative disorders ofepithelial and stromal breast tissue. Int JCancer 60: 49-53. 702. Dina R, Eusebi V (1997). Clear celltumors of the breast. Semin Diagn Pathol14: 175-182. 703. Dinh TV, Slavin RE, Bhagavan BS,Hannigan EV, Tiamson EM, Yandell RB(1989). Mixed mullerian tumors of theuterus: a clinicopathologic study. ObstetGynecol 74: 388-392. 704. Dixon AR, Ellis IO, Elston CW, BlameyRW (1991). A comparison of the clinicalmetastatic patterns of invasive lobular andductal carcinomas of the breast. Br JCancer 63: 634-635. 705. Dixon JM, Anderson TJ, Page DL, LeeD, Duffy SW (1982). Infiltrating lobular car-cinoma of the breast. Histopathology 6:149-161. 706. Dixon JM, Lumsden AB, Krajewski A,Elton RA, Anderson TJ (1987). Primary lym-phoma of the breast. Br J Surg 74: 214-216. 707. Dixon JM, Sainsbury JRC (1998).Handbook of Diseases of the Breast. 2nded. Churchill Livingstone: Edinburgh.
708. Dobbs SP, Shaw PA, Brown LJ,Ireland D (1998). Borderline malignantchange in recurrent mullerian papilloma ofthe vagina. J Clin Pathol 51: 875-877. 709. Dockerty MB, Masson JC (1944).Ovarian fibromas: a clinical and pathologi -cal study of two hundred-and eighty-threecases. Am J Obstet Gynecol 47: 741-752. 710. Dodge JA, Eltabbakh GH, Mount SL,Walker RP, Morgan A (2001). Clinical fea-tures and risk of recurrence amongpatients with vaginal intraepithelial neo-plasia. Gynecol Oncol 83: 363-369. 711. Domagala W, Harezga B, SzadowskaA, Markiewski M, Weber K, Osborn M(1993). Nuclear p53 protein accumulatespreferentially in medullary and high-gradeductal but rarely in lobular breast carcino -mas. Am J Pathol 142: 669-674. 712. Done SJ, Eskandarian S, Bull S,Redston M, Andrulis IL (2001). p53 mis-sense mutations in microdissected high-grade ductal carcinoma in situ of thebreast. J Natl Cancer Inst 93: 700-704. 713. Donegan WL, Redlich PN, Lang PJ,Gall MT (1998). Carcinoma of the breast inmales: a multiinstitutional survey. Cancer83: 498-509. 714. Donehower LA, Harvey M, Slagle BL,McArthur MJ, Montgomery CA Jr., ButelJS, Bradley A (1992). Mice deficient for p53are developmentally normal but suscepti-ble to spontaneous tumours. Nature 356:215-221. 715. Dong C, Hemminki K (2001).Modification of cancer risks in offspring bysibling and parental cancers from2,112,616 nuclear families. Int J Cancer 92:144-150. 715 a. Dong HJ, Li JG, Zeng JH, Huang SZ(1986). Papillary adenocarcinoma of thebroad ligament. Report of a case andreview of literature. Chin Med J (Engl) 99:431-432. 716. Donkers B, Kazzaz BA, Meijering JH(1972). Rhabdomyosarcoma of the corpusuteri. Report of two cases with review ofthe literature. Am J Obstet Gynecol 114:1025-1030. 717. Donnell RM, Rosen PP, Lieberman PH,Kaufman RJ, Kay S, Braun DW Jr., KinneDW (1981). Angiosarcoma and other vas-cular tumors of the breast. Am J SurgPathol 5: 629-642. 718. Dougherty CM, Cunningham C, MickalA (1978). Choriocarcinoma with metastasisin a postmenopausal woman. Am J ObstetGynecol 132: 700-701. 719. Douglas-Jones AG, Pace DP (1997).Pathology of R4 spiculated lesions in thebreast screening programme.Histopathology 30: 214-220. 720. Downey GO, Okagaki T, Ostrow RS,Clark BA, Twiggs LB, Faras AJ (1988).Condylomatous carcinoma of the vulvawith special reference to human papillo-mavirus DNA. Obstet Gynecol 72: 68-73. 721. Drew PA, al Abbadi MA, Orlando CA,Hendricks JB, Kubilis PS, Wilkinson EJ(1996). Prognostic factors in carcinoma ofthe vulva: a clinicopathologic and DNAflow cytometric study. Int J GynecolPathol 15: 235-241. 722. Driscoll SG (1963). Choriocarcinoma.An "incidental finding" within a term pla-centa. Obstet Gynecol 21: 96-101. 723. Droufakou S, Deshmane V, RoylanceR, Hanby A, Tomlinson I, Hart IR (2001).Multiple ways of silencing E-cadheringene expression in lobular carcinoma ofthe breast. Int J Cancer 92: 404-408.
724. Droulias CA, Sewell CW, McSweeneyMB, Powell RW (1976). Inflammatory carci-noma of the breast: A correlation of clini-cal, radiologic and pathogic findings. AnnSurg 184: 217-222. 725. du Toit RS, Locker AP, Ellis IO, ElstonCW, Nicholson RI, Blamey RW (1989).Invasive lobular carcinomas of the breast--the prognosis of histopathological sub-types. Br J Cancer 60: 605-609. 726. Dubeau L (1999). The cell of origin ofovarian epithelial tumors and the ovariansurface epithelium dogma: does theemperor have no clothes? Gynecol Oncol72: 437-442. 727. Duggan MA, Hugh J, Nation JG,Robertson DI, Stuart GC (1989).Ependymoma of the uterosacral ligament.Cancer 64: 2565-2571. 728. Dumont-Herskowitz RA, Safaii HS,Senior B (1978). Ovarian fibromata in foursuccessive generations. J Pediatr 93: 621-624. 729. Dunaif A, Hoffman AR, Scully RE, FlierJS, Longcope C, Levy LJ, Crowley WF Jr.(1985). Clinical, biochemical, and ovarianmorphologic features in women with acan-thosis nigricans and masculinization.Obstet Gynecol 66: 545-552. 7 3 0 . Dungar CF, Wilkinson EJ (1995).Vaginal columnar cell metaplasia. Anacquired adenosis associated with topical5-fluorouracil therapy. J Reprod Med 40:361-366. 731. Dunlop MG, Farrington SM, CarothersAD, Wyllie AH, Sharp L, Burn J, Liu B,Kinzler KW, Vogelstein B (1997). Cancerrisk associated with germline DNA mis-match repair gene mutations. Hum MolGenet 6: 105-110. 732. Dupont WD, Page DL (1985). Risk fac-tors for breast cancer in women with pro-liferative breast disease. N Engl J Med 312:146-151. 733. Dupont WD, Page DL (1987). Breastcancer risk associated with proliferativedisease, age at first birth, and a family his -tory of breast cancer. Am J Epidemiol 125:769-779. 734. Dupont WD, Page DL, Parl FF,Vnencak-Jones CL, Plummer WD Jr.,Rados MS, Schuyler PA (1994). Long-termrisk of breast cancer in women withfibroadenoma. N Engl J Med 331: 10-15. 735. Dupont WD, Parl FF, Hartmann WH,Brinton LA, Winfield AC, Worrell JA,Schuyler PA, Plummer WD (1993). Breastcancer risk associated with proliferativebreast disease and atypical hyperplasia.Cancer 71: 1258-1265. 7 3 6 . Durkop H, Foss HD, Eitelbach F,Anagnostopoulos I, Latza U, Pileri S, SteinH (2000). Expression of the CD30 antigen innon-lymphoid tissues and cells. J Pathol190: 613-618. 737. Durst M, Gissmann L, Ikenberg H, zurHausen H (1983). A papillomavirus DNAfrom a cervical carcinoma and its preva-lence in cancer biopsy samples from dif-ferent geographic regions. Proc Natl AcadSci USA 80: 3812-3815. 738. Duska LR, Flynn C, Goodman A (1998).Masculinizing sclerosing stromal celltumor in pregnancy: report of a case andreview of the literature. Eur J GynaecolOncol 19: 441-443. 739. Duun S (1994). Bilateral virilizing hilus(Leydig) cell tumors of the ovary. ActaObstet Gynecol Scand 73: 76-77. 740. Duvall E, Survis JA (1983). Borderlinetumour of the broad ligament. Case report.Br J Obstet Gynaecol 90: 372-375.
741. Easton DF (1994). Cancer risks in A-Theterozygotes. Int J Radiat Biol 66: S177-S182. 742. Easton DF, Ford D, Bishop DT (1995).Breast and ovarian cancer incidence inBRCA1-mutation carriers. Breast CancerLinkage Consortium. Am J Hum Genet 56:265-271. 743. Easton DF, Matthews FE, Ford D,Swerdlow AJ, Peto J (1996). Cancer mor-tality in relatives of women with ovariancancer: the OPCS Study. Office ofPopulation Censuses and Surveys. Int JCancer 65: 284-294. 744. Easton DF, Steele L, Fields P, OrmistonW, Averill D, Daly PA, McManus R,Neuhausen SL, Ford D, Wooster R,Cannon-Albright LA, Stratton MR, GoldgarDE (1997). Cancer risks in two large breastcancer families linked to BRCA2 on chro-mosome 13q12-13. Am J Hum Genet 61:120-128. 745. Ebrahim S, Daponte A, Smith TH,Tiltman A, Guidozzi F (2001). Primary muci-nous adenocarcinoma of the vagina.Gynecol Oncol 80: 89-92. 746. Eckstein RP, Paradinas FJ, BagshaweKD (1982). Placental site trophoblastictumour (trophoblastic pseudotumour): astudy of four cases requiring hysterectomyincluding one fatal case. Histopathology 6:211-226. 747. Eckstein RP, Russell P,Friedlander ML, Tattersall MH, Bradfield A(1985). Metastasizing placental site tro-phoblastic tumor: a case study. H u mPathol 16: 632-636. 748. Eddy GL, Marks RD Jr., Miller MC III,Underwood PB Jr. (1991). Primary invasivevaginal carcinoma. Am J Obstet Gynecol165: 292-296. 749. Eeles RA (1999). Screening for heredi -tary cancer and genetic testing, epito-mized by breast cancer. Eur J Cancer 35:1954-1962. 7 5 0 . Egan AJ, Russell P (1996). Transitional(urothelial) cell metaplasia of the fallopiantube mucosa: morphological assessment ofthree cases. Int J Gynecol Pathol 15: 72-76. 751. Egan RL (1976). Bilateral breast carci-nomas: Role of mammography. Cancer 38:931-938. 752. Eggers JW, Chesney TM (1984).Squamous cell carcinoma of the breast: aclinicopathologic analysis of eight casesand review of the literature.Hum Pathol 15:526-531. 753. Ehrlich CE, Roth LM (1971). TheBrenner tumor. A clinicopathologic studyof 57 cases. Cancer 27: 332-342. 754. Eichhorn JH, Bell DA, Young RH,Scully RE (1999). Ovarian serous borderlinetumors with micropapillary and cribriformpatterns: a study of 40 cases and compari-son with 44 cases without these patterns.Am J Surg Pathol 23: 397-409. 755. Eichhorn JH, Bell DA, Young RH,Swymer CM, Flotte TJ, Preffer RI, Scully RE(1992). DNA content and proliferativeactivity in ovarian small cell carcinomas ofthe hypercalcemic type. Implications fordiagnosis, prognosis, and histogenesis.Am J Clin Pathol 98: 579-586. 756. Eichhorn JH, Lawrence WD, YoungRH, Scully RE (1996). Ovarian neuroen-docrine carcinomas of non-small-cell typeassociated with surface epithelial adeno-carcinomas. A study of five cases andreview of the literature. Int J GynecolPathol 15: 303-314.

384 References
757. Eichhorn JH, Scully RE (1991). Ovarianmyxoma: clinicopathologic and immunocy-tologic analysis of five cases and a reviewof the literature. Int J Gynecol Pathol 10:156-169. 7 5 8 . Eichhorn JH, Scully RE (1995)."Adenoid cystic" and basaloid carcinomasof the ovary: evidence for a surface epithe-lial lineage. A report of 12 cases. ModPathol 8: 731-740. 7 5 9 . Eichhorn JH, Scully RE (1996).Endometrioid ciliated-cell tumors of theovary: a report of five cases. Int J GynecolPathol 15: 248-256. 760. Eichhorn JH, Young RH, Clement PB,Scully RE (2002). Mesodermal (mullerian)adenosarcoma of the ovary: a clinico-pathologic analysis of 40 cases and areview of the literature. Am J Surg Pathol26: 1243-1258. 761. Eichhorn JH, Young RH, Scully RE(1992). Primary ovarian small cell carcino-ma of pulmonary type. A clinicopathologic,immunohistologic, and flow cytometricanalysis of 11 cases. Am J Surg Pathol 16:926-938. 762. Eifel P, Hendrickson M, Ross J, BallonS, Martinez A, Kempson R (1982).Simultaneous presentation of carcinomainvolving the ovary and the uterine corpus.Cancer 50: 163-170. 7 6 3 . Eisen A, Rebbeck TR, Lynch HT,Lerman C, Ghadirian P, Dube MP (2000).Reduction in Breast Cancer Risk followingBilateral Prophylactic Oophorectomy inBRCA1 and BRCA2 Mutation Carriers. AmJ Hum Genet 67: 58. 764. Eisinger F, Jacquemier J, Charpin C,Stoppa-Lyonnet D, Bressac-de PailleretsB, Peyrat JP, Longy M, Guinebretiere JM,Sauvan R, Noguchi T, Birnbaum D, Sobol H(1998). Mutations at BRCA1: the medullarybreast carcinoma revisited. Cancer Res 58:1588-1592. 765. Eisinger F, Jacquemier J,Guinebretiere JM, Birnbaum D, Sobol H(1997). p53 involvement in BRCA1-associ-ated breast cancer. Lancet 350: 1101. 766. Eisinger F, Jacquemier J, Nogues C,Birnbaum D, Sobol H (1999). Steroid recep-tors in hereditary breast carcinomas asso-ciated with BRCA1 or BRCA2 mutations orunknown susceptibility genes. Cancer 85:2291-2295. 767. Eisner RF, Nieberg RK, Berek JS(1989). Synchronous primary neoplasms ofthe female reproductive tract. G y n e c o lOncol 33: 335-339. 768. Elliott P, Coppleson M, Russell P,Liouros P, Carter J, MacLeod C, Jones M(2000). Early invasive (FIGO stage IA) carci-noma of the cervix: a clinico-pathologicstudy of 476 cases. Int J Gynecol Cancer10: 42-52. 769. Ellis DL, Teitelbaum SL (1974).Inflammatory carcinoma of the breast. Apathologic definition. Cancer 33: 1045-1047. 770. Ellis IO, Elston CW, Goulding H, et al.(1998). Miscellaneous benign lesions. In:The Breast. CW Elston and IO Ellis (Ed.) 1sted. Churchill Livingstone: Edinburgh, p. 224.771. Ellis IO, Galea M, Broughton N, LockerA, Blamey RW, Elston CW (1992).Pathological prognostic factors in breastcancer. II. Histological type. Relationshipwith survival in a large study with long-term follow-up. Histopathology 20: 479-489.
772. Ellis IO, Galea MH, Locker A, RoebuckEJ, Elston CW, Blamey RW, Wilson ARM(1993). Early experience in breast cancerscreening: Emphasis on development ofprotocols for triple assessment. Breast 2:148-153. 773. Elsheikh A, Keramopoulos A, LazarisD, Ambela C, Louvrou N, Michalas S (2000).Breast tumors during adolescence. Eur JGynaecol Oncol 21: 408-410. 774. Elston C.W, Ellis I.O. (1998).Classification of malignant breast disease.In: The Breast. Systemic Pathology. CWElston and IO Ellis (Eds.) 3rd ed. ChurchillLivingstone: Edinburgh, pp. 239-247.775. Elston C.W, Ellis I.O. (1998).Fibroadenoma and related conditions. In:The Breast. CW Elston and IO Ellis (Ed.)Churchill Livingstone: Edinburgh. 775a. Elston CW, Bagshawe KD (1972). Thediagnosis of trophoblastic tumours fromuterine curettings. J Clin Pathol 25: 111-118. 776. Elston CW, Bagshawe KD (1972). Thevalue of histological grading in the man-agement of hydatidiform mole. J ObstetGynaecol Br Commonw 79: 717-724. 777. Elston CW, Ellis IO (1991). Pathologicalprognostic factors in breast cancer. I. Thevalue of histological grade in breast can-cer: experience from a large study withlong-term follow-up. Histopathology 1 9 :403-410. 778. Elston CW, Ellis IO (1998). Metastaseswithin the breast. In: The Breast. C WElston and IO Ellis (Eds.) ChurchillLivingstone: Edinburgh. 779. Elston CW, Ellis IO (1998). Systemicpathology 3E. In: The Breast. CW Elstonand IO Ellis (Eds.) Churchill Livingstone:Edinburgh. 780. Elston CW, Sloane JP, Amendoeira I,Apostolikas N, Bellocq JP, Bianchi S,Boecker W, Bussolati G, Coleman D,Connolly CE, Dervan P, Drijkoningen M,Eusebi V, Faverly D, Holland R, JacquemierJ, Lacerda M, Martinez-Penuela J, DeMiguel C, Mossi S, Munt C, Peterse JL,Rank F, Reiner A, Sylvan M, Wells CA,Zafrani B (2000). Causes of inconsistencyin diagnosing and classifying intraductalproliferations of the breast. EuropeanCommission Working Group on BreastScreening Pathology. Eur J Cancer 3 6 :1769-1772. 781. Emerich J, Senkus E, Konefka T (1996).Alveolar rhabdomyosarcoma of the uterinecervix. Gynecol Oncol 63: 398-403. 782. Emery JD, Kennedy AW, Tubbs RR,Castellani WJ, Hussein MA (1999).Plasmacytoma of the ovary: a case reportand literature review. Gynecol Oncol 73:151-154. 783. Emmert-Buck MR, Chuaqui R, ZhuangZ, Nogales F, Liotta LA, Merino MJ (1997).Molecular analysis of synchronous uterineand ovarian endometrioid tumors. Int JGynecol Pathol 16: 143-148. 784. Emoto M, Iwasaki H, KawarabayashiT, Egami D, Yoshitake H, Kikuchi M,Shirakawa K (1994). Primary osteosarcomaof the uterus: report of a case withimmunohistochemical analysis. G y n e c o lOncol 54: 385-388. 785. Eng C (1997). Cowden syndrome. JGenet Counsel 6: 181-191. 786. Eng C (2000). Will the real Cowdensyndrome please stand up: revised diag-nostic criteria. J Med Genet 37: 828-830.
787. Eng C, Parsons R (1998). Cowden syn-drome. In: The Genetic Basis of HumanCancer. B Vogelstein, K Kinzler (Eds.) NewYork: McGraw-Hill, pp. 519-526.788. Eng C, Parsons R (2001). Cowden syn-drome. In: Metabolic and Molecular Basesof Inherited Disease. C Scriver, ALBeaudet, WS Sly, D Valle (Eds.) 8th ed.McGraw-Hill: New York , pp. 979-988.789. Enomoto T, Haba T, Fujita M, HamadaT, Yoshino K, Nakashima R, Wada H,Kurachi H, Wakasa K, Sakurai M, MurataY, Shroyer KR (1997). Clonal analysis ofhigh-grade squamous intra-epitheliallesions of the uterine cervix. Int J Cancer73: 339-344. 790. Enzinger FM, Shiraki M (1967).Musculo-aponeurotic fibromatosis of theshoulder girdle (extra-abdominaldesmoid). Analysis of thirty cases followedup for ten or more years. Cancer 20: 1131-1140. 791. Erdreich LS, Asal NR, Hoge AF (1980).Morphologic types of breast cancer: age,bilaterality, and family history. South MedJ 73: 28-32. 792. Eriksson ET, Schimmelpenning H,Aspenblad U, Zetterberg A, Auer GU (1994).Immunohistochemical expression of themutant p53 protein and nuclear DNA con-tent during the transition from benign tomalignant breast disease. Hum Pathol 25:1228-1233. 7 9 3 . Erlandson RA, Rosen PP (1982).Infiltrating myoepithelioma of the breast.Am J Surg Pathol 6: 785-793. 794. Ernster VL, Barclay J, Kerlikowske K,Wilkie H, Ballard-Barbash R (2000).Mortality among women with ductal carci-noma in situ of the breast in the popula-tion-based surveillance, epidemiology andend results program. Arch Intern Med 160:953-958. 795. Escalonilla P, Grilli R, Canamero M,Soriano ML, Farina MC, Manzarbeitia F,Sainz R, Matsukura T, Requena L (1999).Sebaceous carcinoma of the vulva. Am JDermatopathol 21: 468-472. 796. Esche C, Kruse R, Lamberti C, Friedl W,Propping P, Lehmann P, Ruzicka T (1997).Muir-Torre syndrome: clinical features andmolecular genetic analysis. Br J Dermatol136: 913-917. 797. Essary LR, Kaarami M, Page DL, WickMR (1999). Immunohistology of variantadenosis & pseudoinvasive epithelial pro-liferations of the breast: helpful or not? LabInvest 79. 798. Esteban JM, Allen WM, Schaerf RH(1999). Benign metastasizing leiomyoma ofthe uterus: histologic and immunohisto-chemical characterization of primary andmetastatic lesions. Arch Pathol Lab Med123: 960-962. 799. Esteller M, Levine R, Baylin SB,Ellenson LH, Herman JG (1998). MLH1 pro-moter hypermethylation is associated withthe microsatellite instability phenotype insporadic endometrial carcinomas.Oncogene 17: 2413-2417. 800. Etzell JE, Devries S, Chew K, FlorendoC, Molinaro A, Ljung BM, Waldman FM(2001). Loss of chromosome 16q in lobularcarcinoma in situ. Hum Pathol 32: 292-296. 801. Eusebi V, Azzopardi JG (1980). Lobularendocrine neoplasia in fibroadenoma ofthe breast. Histopathology 4: 413-428. 802. Eusebi V, Betts CM, Haagensen DE,Gugliotta P, Bussolati G, Azzopardi JG(1984). Apocrine differentiation in lobularcarcinoma of the breast. Hum Pathol 15:134-140.
803. Eusebi V, Casadei GP, Bussolati G,Azzopardi JG (1986). Adenomyoepithe-lioma of the breast with a distinctive typeof apocrine adenosis. Histopathology 11:305-315. 804. Eusebi V, Damiani S, Losi L., Millis RR(1997). Apocrine differentiation in breastepithelium. Advances Anat Pathol 4: 139-155. 805. Eusebi V, Damiani S, Losi L, Millis RR(1997). Apocrine differentiation in breaste p i t h e l i u m . Advances in AnatomicPathology 4: 139-155. 806. Eusebi V, Foschini MP, Bussolati G,Rosen PP (1995). Myoblastomatoid (histio-cytoid) carcinoma of the breast. A type ofapocrine carcinoma. Am J Surg Pathol 19:553-562. 807. Eusebi V, Lamovec J, Cattani MG,Fedeli F, Millis RR (1986). Acantholytic vari-ant of squamous-cell carcinoma of thebreast. Am J Surg Pathol 10: 855-861. 808. Eusebi V, Magalhaes F, Azzopardi AG(1992). Pleomorphic lobular carcinoma ofthe breast: an aggressive tumour showingapocrine differentiation. Hum Pathol 23:655-662. 809. Eusebi V, Millis RR, Cattani MG,Bussolati G, Azzopardi JG (1986). Apocrinecarcinoma of the breast. A morphologicand immunocytochemical study. Am JPathol 123: 532-541. 810. Evans AJ, Pinder SE, Ellis IO, WilsonAR (2001). Screen detected ductal carcino-ma in situ (DCIS): overdiagnosis or an obli-gate precursor of invasive disease? J MedScreen 8: 149-151. 811. Evans HL (1982).Endometrial stromal sarcoma and poorlydifferentiated endometrial sarcoma.Cancer 50: 2170-2182. 812. Evans HL, Chawla SP, Simpson C, FinnKP (1988). Smooth muscle neoplasms ofthe uterus other than ordinary leiomyoma.A study of 46 cases, with emphasis ondiagnostic criteria and prognostic factors.Cancer 62: 2239-2247. 813. Evans MJ, Langlois NE, Kitchener HC,Miller ID (1995). Is there an associationbetween long-term tamoxifen treatmentand the development of carcinosarcoma(malignant mixed Mullerian tumor) of theuterus? Int J Gynecol Cancer 5: 310-313. 814. Ewertz M, Holmberg L, Karjalainen S,Tretli S, Adami HO (1989). Incidence ofmale breast cancer in Scandinavia, 1943-1982. Int J Cancer 43: 27-31. 815. Ewertz M, Holmberg L, Tretli S,Pedersen BV, Kristensen A (2001). Riskfactors for male breast cancer - a case-control study from Scandinavia. A c t aOncol 40: 467-471. 816. Fackenthal JD, Cartegni L, Krainer AR,Olopade OI (2002). BRCA2 T2722R is a dele-terious allele that causes exon skipping.Am J Hum Genet 71: 625-631. 817. Fackenthal JD, Marsh DJ, RichardsonAL, Cummings SA, Eng C, Robinson BG,Olopade OI (2001). Male breast cancer inCowden syndrome patients with germlinePTEN mutations. J Med Genet 38: 159-164. 818. Fagundes H, Perez CA, Grigsby PW,Lockett MA (1992). Distant metastasesafter irradiation alone in carcinoma of theuterine cervix. Int J Radiat Oncol Biol Phys24: 197-204. 819. Fairfield KM, Hankinson SE, RosnerBA, Hunter DJ, Colditz GA, Willett WC(2001). Risk of ovarian carcinoma and con-sumption of vitamins A, C, and E and spe-cific carotenoids: a prospective analysis.Cancer 92: 2318-2326.

385References
820. Falck J, Petrini JH, Williams BR, LukasJ, Bartek J (2002). The DNA damage-dependent intra-S phase checkpoint isregulated by parallel pathways. Nat Genet30: 290-294. 821. Falconieri G, Della LD, Zanconati F,Bittesini L (1997). Leiomyosarcoma of thefemale breast: report of two new casesand a review of the literature. Am J ClinPathol 108: 19-25. 822. Falkenberry SS, Steinhoff MM,Gordinier M, Rappoport S, Gajewski W,Granai CO (1996). Synchronous endometri-oid tumors of the ovary and endometrium.A clinicopathologic study of 22 cases. JReprod Med 41: 713-718. 823. Fan LD, Zang HY, Zhang XS (1996).Ovarian epidermoid cyst: report of eightcases. Int J Gynecol Pathol 15: 69-71. 824. Fanburg-Smith JC, Meis-KindblomJM, Fante R, Kindblom LG (1998).Malignant granular cell tumor of soft tis-sue: diagnostic criteria and clinicopatho-logic correlation. Am J Surg Pathol 22: 779-794. 825. Fanning J, Lambert HC, Hale TM,Morris PC, Schuerch C (1999). Paget's dis-ease of the vulva: prevalence of associat-ed vulvar adenocarcinoma, invasivePaget's disease, and recurrence after sur-gical excision. Am J Obstet Gynecol 180:24-27. 826. Faquin WC, Fitzgerald JT, Lin MC,Boynton KA, Muto MG, Mutter GL (2000).Sporadic microsatellite instability is spe-cific to neoplastic and preneoplasticendometrial tissues. Am J Clin Pathol 113:576-582. 827. Farshid G, Moinfar F, Meredith DJ,Peiterse S, Tavassoli FA (2001). Spindlecell ductal carcinoma in situ. An unusualvariant of ductal intra-epithelial neoplasiathat simulates ductal hyperplasia or amyoepithelial proliferation. Virchows Arch439: 70-77. 828. Fastenberg NA, Martin RG, Buzdar AU,Hortobagyi GN, Montague ED,Blumenschein GR, Jessup JM (1985).Management of inflammatory carcinomaof the breast. A combined modalityapproach. Am J Clin Oncol 8: 134-141. 829. Fathalla MF (1967). The occurrence ofgranulosa and theca tumours in clinicallynormal ovaries. A study of 25 cases. JObstet Gynaecol Br Commonw 74: 278-282. 830. Faul C, Kounelis S, Karasek K,Papadaki H, Greeenberger J, Jones MW(1996). Small cell carcinoma of the uterinecervix: Overespression of p53, Bcl2, andCD 44. Int J Gynecol Cancer 6: 369-375. 831. Faverly DR, Burgers L, Bult P, HollandR (1994). Three dimensional imaging ofmammary ductal carcinoma in situ: clinicalimplications. Semin Diagn Pathol 11: 193-198. 832. Fawcett FJ, Kimbell NK (1971).Phaeochromocytoma of the ovary. JObstet Gynaecol Br Commonw 78: 458-459. 833. Feakins RM, Lowe DG (1997). Basalcell carcinoma of the vulva: a clinicopatho-logic study of 45 cases. Int J GynecolPathol 16: 319-324. 834. Fechner RE (1972). Infiltrating lobularcarcinoma without lobular carcinoma insitu. Cancer 29: 1539-1545. 835. Fechner RE (1975). Histologic variantsof infiltrating lobular carcinoma of thebreast. Hum Pathol 6: 373-378. 836. Fechner RE, Mills SE (1990). BreastPathology Benign Proliferations, Atypias InSitu Carcinomas. ASCP Press - AmericanSociety of Clinical Pathologist: Chicago.
837. Feczko JD, Jentz DL, Roth LM (1996).Adenoid cystic ovarian carcinoma com-pared with other adenoid cystic carcino-mas of the female genital tract. M o dPathol 9: 413-417. 838. Feeley KM, Wells M (2001). Precursorlesions of ovarian epithelial malignancy.Histopathology 38: 87-95. 839. Fein DA, Fowble BL, Hanlon AL, HooksMA, Hoffman JP, Sigurdson ER, JardinesLA, Eisenberg BL (1997). Identification ofwomen with T1-T2 breast cancer at lowrisk of positive axillary nodes. J SurgOncol 65: 34-39. 840. Feinmesser M, Sulkes A, MorgensternS, Sulkes J, Stern S, Okon E (2000). HLA-DRand beta 2 microglobulin expression inmedullary and atypical medullary carcino-ma of the breast: histopathologically simi-lar but biologically distinct entities. J ClinPathol 53: 286-291. 841. Feldman LD, Hortobagyi GN, BuzdarAU, Ames FC, Blumenschein GR (1986).Pathological assessment of response toinduction chemotherapy in breast cancer.Cancer Res 46: 2578-2581. 842. Feltmate CM, Genest DR, Wise L,Bernstein MR, Goldstein DP, Berkowitz RS(2001). Placental site trophoblastic tumor:a 17-year experience at the New EnglandTrophoblastic Disease Center. G y n e c o lOncol 82: 415-419. 843. Fenoglio C, Lattes R (1974). Sclerosingpapillary proliferations in the femalebreast. A benign lesion often mistaken forcarcinoma. Cancer 33: 691-700. 844. Fentiman IS, Millis RR, Smith P, EllulJP, Lampejo O (1997). Mucoid breast carci-nomas: histology and prognosis. Br JCancer 75: 1061-1065. 845. Ferguson AW, Katabuchi H, RonnettBM, Cho KR (2001). Glial implants ingliomatosis peritonei arise from normal tis-sue, not from the associated teratoma. AmJ Pathol 159: 51-55. 846. Ferlay J, Bray F, Pisani P, Parkin DM(2001). Globocan 2000. Cancer Incidence,Mortality and Prevalence Worlwide.IARCPress: Lyon. 847. Fernandez FA, Val-Bernal F, Garijo-Ayensa F (1989). Mixed lipomas of theuterus and the broad ligament. Appl Pathol7: 70-71. 848. Feroze M, Aravindan KP, Thomas M(1997). Mullerian adenosarcoma of theuterine cervix. Indian J Cancer 34: 68-72. 849. Ferry JA, Scully RE (1988). "Adenoidcystic" carcinoma and adenoid basal car-cinoma of the uterine cervix. A study of 28cases. Am J Surg Pathol 12: 134-144. 850. Ferry JA, Scully RE (1990).Mesonephric remnants, hyperplasia, andneoplasia in the uterine cervix. A study of49 cases. Am J Surg Pathol 14: 1100-1111. 851. Ferry JA, Young RH (1991). Malignantlymphoma, pseudolymphoma, andhematopoietic disorders of the femalegenital tract. Pathol Annu 26 Pt 1: 227-263. 852. Ferry JA, Young RH, Engel G, Scully RE(1994). Oxyphilic Sertoli cell tumor of theovary: a report of three cases, two inpatients with the Peutz-Jeghers syndrome.Int J Gynecol Pathol 13: 259-266. 853. Fetsch JF, Laskin WB, Lefkowitz M,Kindblom LG, Meis-Kindblom JM (1996).Aggressive angiomyxoma: a clinicopatho-logic study of 29 female patients. Cancer78: 79-90.
854. Fetsch JF, Laskin WB, Tavassoli FA(1997). Superficial angiomyxoma (cuta-neous myxoma): a clinicopathologic studyof 17 cases arising in the genital region. IntJ Gynecol Pathol 16: 325-334. 855. Feyrter F, Hartmann G (1963). Uber diecarcinoide Wuchsform des Carcinomamammae, insbesondere das Carcinomasolidum (gelatinosum) mamma. Fradf ZPathol 73: 24-30. 856. Fiche M, Avet-Loiseau H, MaugardCM, Sagan C, Heymann MF, Leblanc M,Classe JM, Fumoleau P, Dravet F, Mahe M,Dutrillaux B (2000). Gene amplificationsdetected by fluorescence in situ hybridiza-tion in pure intraductal breast carcinomas:relation to morphology, cell proliferationand expression of breast cancer-relatedgenes. Int J Cancer 89: 403-410. 857. Fina F, Romain S, Ouafik L, Palmari J,Ben Ayed F, Benharkat S, Bonnier P,Spyratos F, Foekens JA, Rose C, BuissonM, Gerard H, Reymond MO, SeigneurinJM, Martin PM (2001). Frequency andgenome load of Epstein-Barr virus in 509breast cancers from different geographi-cal areas. Br J Cancer 84: 783-790. 858. Fingerland A (1938). Ganglioneuromaof the cervix uteri. J Pathol Bacteriol 47:631-634. 859. Fink D, Kubik-Huch RA, Wildermuth S(2001). Juvenile granulosa cell tumor.Abdom Imaging 26: 550-552. 860. Fink D, Nebel S, Aebi S, Zheng H, KimHK, Christen RD, Howell SB (1997).Expression of the DNA mismatch repairproteins hMLH1 and hPMS2 in normalhuman tissues. Br J Cancer 76: 890-893. 861. Finkler NJ, Berkowitz RS, Driscoll SG,Goldstein DP, Bernstein MR (1988). Clinicalexperience with placental site trophoblas -tic tumors at the New EnglandTrophoblastic Disease Center. O b s t e tGynecol 71: 854-857. 862. Finn WF, Javert CT (1949). Primary andmetastatic cancer of the fallopian tube.Cancer 2: 803-814. 863. Fishel R (2001). The selection for mis-match repair defects in hereditary non-polyposis colorectal cancer: revising themutator hypothesis. Cancer Res 61: 7369-7374. 8 6 4 . Fishel R, Lescoe MK, Rao MR,Copeland NG, Jenkins NA, Garber J, KaneM, Kolodner R (1993). The human mutatorgene homolog MSH2 and its associationwith hereditary nonpolyposis colon can-cer. Cell 75: 1027-1038. 865. Fisher B, Costantino JP, WickerhamDL, Redmond CK, Kavanah M, Cronin WM,Vogel V, Robidoux A, Dimitrov N, Atkins J,Daly M, Wieand S, Tan-Chiu E, Ford L,Wolmark N (1998). Tamoxifen for preven-tion of breast cancer: report of theNational Surgical Adjuvant Breast andBowel Project P-1 Study. J Natl CancerInst 90: 1371-1388. 8 6 6 . Fisher B, Dignam J, Wolmark N,Wickerham DL, Fisher ER, Mamounas E,Smith R, Begovic M, Dimitrov NV,Margolese RG, Kardinal CG, Kavanah MT,Fehrenbacher L, Oishi RH (1999).Tamoxifen in treatment of intraductalbreast cancer: National Surgical AdjuvantBreast and Bowel Project B-24 ran-domised controlled trial. Lancet 353: 1993-2000. 867. Fisher CJ, Hanby AM, Robinson L,Millis RR (1992). Mammary hamartoma--areview of 35 cases. Histopathology 20: 99-106.
868. Fisher ER, Anderson S, Redmond C,Fisher B (1993). Pathologic findings fromthe National Surgical Adjuvant BreastProject protocol B-06. 10-year pathologicand clinical prognostic discriminants.Cancer 71: 2507-2514. 8 6 9 . Fisher ER, Costantino J, Fisher B,Palekar AS, Paik SM, Suarez CM, WolmarkN (1996). Pathologic findings from theNational Surgical Adjuvant Breast Project(NSABP) Protocol B-17. Five-year observa-tions concerning lobular carcinoma in situ.Cancer 78: 1403-1416. 8 7 0 . Fisher ER, Costantino J, Fisher B,Palekar AS, Redmond C, Mamounas E(1995). Pathologic findings from theNational Surgical Adjuvant Breast Project(NSABP) Protocol B-17. Intraductal carci-noma (ductal carcinoma in situ). TheNational Surgical Adjuvant Breast andBowel Project Collaborating Investigators.Cancer 75: 1310-1319. 8 7 1 . Fisher ER, Costantino J, Fisher B,Redmond C (1993). Pathologic findingsfrom the National Surgical Adjuvant BreastProject (Protocol 4). Discriminants for 15-year survival. National Surgical AdjuvantBreast and Bowel Project Investigators.Cancer 71: 2141-2150. 8 7 2 . Fisher ER, Fisher B, Sass R,Wickerham L (1984). Pathologic findingsfrom the National Surgical Adjuvant BreastProject (Protocol No. 4). XI. Bilateral breastcancer. Cancer 54: 3002-3011. 8 7 3 . Fisher ER, Gregorio R, Kim WS,Redmond C (1977). Lipid in invasive cancerof the breast. Am J Clin Pathol 68: 558-561. 8 7 4 . Fisher ER, Gregorio RM, Fisher B,Redmond C, Vellios F, Sommers SC (1975).The pathology of invasive breast cancer. Asyllabus derived from findings of theNational Surgical Adjuvant Breast Project(protocol no. 4). Cancer 36: 1-85. 875. Fisher ER, Gregorio RM, Redmond C,Fisher B (1977). Tubulolobular invasivebreast cancer: a variant of lobular invasivecancer. Hum Pathol 8: 679-683. 876. Fisher ER, Kenny JP, Sass R, DimitrovNV, Siderits RH, Fisher B (1990). Medullarycancer of the breast revisited. B r e a s tCancer Res Treat 16: 215-229. 877. Fisher ER, Palekar AS, Gregorio RM,Redmond C, Fisher B (1978). Pathologicalfindings from the National SurgicalAdjuvant Breast Project (Protocol No 4) IV.Significance of tumour necrosis. H u mPathol 9: 523-530. 878. Fisher ER, Palekar AS, Gregorio RM,Paulson JD (1983). Mucoepidermoid andsquamous cell carcinomas of breast withreference to squamous metaplasia andgiant cell tumors. Am J Surg Pathol 7: 15-27. 879. Fisher ER, Palekar AS, Redmond C,Barton B, Fisher B (1980). Pathologic find-ings from the National Surgical AdjuvantBreast Project (protocol no. 4). VI. Invasivepapillary cancer. Am J Clin Pathol 73: 313-322. 880. Fisher ER, Tavares J, Bulatao IS, SassR, Fisher B (1985). Glycogen-rich, clear cellbreast cancer: with comments concerningother clear cell variants. Hum Pathol 16:1085-1090. 881. Fisher PE, Estabrook A, Cohen MB(1990). Fine needle aspiration biopsy ofintramammary neurilemoma. Acta Cytol 34:35-37.

386 References
882. Fisher RA, Lawler SD, Ormerod MG,Imrie PR, Povey S (1987). Flow cytometryused to distinguish between complete andpartial hydatidiform moles. Placenta 8: 249-256. 883. Fishman DA, Schwartz PE (1994).Current approaches to diagnosis andtreatment of ovarian germ cell malignan-cies. Curr Opin Obstet Gynecol 6: 98-104. 884. FitzGerald MG, Bean JM, Hegde SR,Unsal H, MacDonald DJ, Harkin DP,Finkelstein DM, Isselbacher KJ, Haber DA(1997). Heterozygous ATM mutations donot contribute to early onset of breast can-cer. Nat Genet 15: 307-310. 885. Fitzgibbons PL, Henson DE, Hutter RV(1998). Benign breast changes and the riskfor subsequent breast cancer: an updateof the 1985 consensus statement. CancerCommittee of the College of AmericanPathologists. Arch Pathol Lab Med 122:1053-1055. 886. Fitzgibbons PL, Page DL, Weaver D,Thor AD, Allred DC, Clark GM, Ruby SG,O'Malley F, Simpson JF, Connolly JL,Hayes DF, Edge SB, Lichter A, Schnitt SJ(2000). Prognostic factors in breast cancer.College of American PathologistsConsensus Statement 1999. Arch PatholLab Med 124: 966-978. 887. Flagiello D, Gerbault-Seureau M,Sastre-Garau X, Padoy E, Vielh P,Dutrillaux B (1998). Highly recurrentder(1;16)(q10;p10) and other 16q arm alter-ations in lobular breast cancer. G e n e sChromosomes Cancer 23: 300-306. 888. Flanagan CW, Parker JR, Mannel RS,Min KW, Kida M (1997). Primary endoder-mal sinus tumor of the vulva: a case reportand review of the literature. G y n e c o lOncol 66: 515-518. 889. Flemming P, Wellmann A, Maschek H,Lang H, Georgii A (1995). Monoclonal anti-bodies against inhibin represent key mark-ers of adult granulosa cell tumors of theovary even in their metastases. A report ofthree cases with late metastasis, beingpreviously misinterpreted as heman-giopericytoma. Am J Surg Pathol 19: 927-933. 890. Fletcher CD, Tsang WY, Fisher C, LeeKC, Chan JK (1992). Angiomyofibroblastomaof the vulva. A benign neoplasm distinctfrom aggressive angiomyxoma. Am J SurgPathol 16: 373-382. 891. Fletcher JA, Pinkus JL, Lage JM,Morton CC, Pinkus GS (1992). Clonal 6p21rearrangement is restricted to the mes-enchymal component of an endometrialpolyp. Genes Chromosomes Cancer 5: 260-263. 892. Flint A, Gikas PW, Roberts JA (1985).Alveolar soft part sarcoma of the uterinecervix. Gynecol Oncol 22: 263-267. 893. Flint A, Oberman HA (1984). Infarctionand squamous metaplasia of intraductalpapilloma: a benign breast lesion that maysimulate carcinoma. Hum Pathol 15: 764-767. 894. Fogt F, Vortmeyer AO, Ahn G, DeGirolami U, Hunt RB, Daly T, Loda M (1994).Neural cyst of the ovary with central nervoussystem microvasculature. Histopathology 2 4 :477-480. 895. Foote FW, Stewart FW (1946). A histo-logic classification of carcinoma of thebreast. Surgery 19: 74-99. 896. Ford D, Easton DF, Bishop DT, NarodSA, Goldgar DE (1994). Risks of cancer inBRCA1-mutation carriers. Breast CancerLinkage Consortium. Lancet 343: 692-695.
897. Ford D, Easton DF, Peto J (1995).Estimates of the gene frequency of BRCA1and its contribution to breast and ovariancancer incidence. Am J Hum Genet 57:1457-1462. 898. Ford D, Easton DF, Stratton M, NarodS, Goldgar D, Devilee P, Bishop DT, WeberB, Lenoir G, Chang-Claude J, Sobol H,Teare MD, Struewing J, Arason A,Scherneck S, Peto J, Rebbeck TR, Tonin P,Neuhausen S, Barkardottir R, Eyfjord J,Lynch H, Ponder BA, Gayther SA, Zelada-Hedman M, Birch JM, Lindblom A, Stoppa-Lyonnet D, Bignon Y, Borg A, Hamann U,Haites N, Scott RJ, Maugard CM, Vasen H(1998). Genetic heterogeneity and pene-trance analysis of the BRCA1 and BRCA2genes in breast cancer families. TheBreast Cancer Linkage Consortium. Am JHum Genet 62: 676-689. 899. Ford D, Easton DF, Stratton M, NarodS, Goldgar D, Devilee P, Bishop DT, WeberB, Lenoir G, Chang-Claude J, Sobol H,Teare MD, Struewing J, Arason A,Scherneck S, Peto J, Rebbeck TR, Tonin P,Neuhausen S, Barkardottir R, Eyfjord J,Lynch H, Ponder BA, Gayther SA, Zelada-Hedman M (1998). Genetic heterogeneityand penetrance analysis of the BRCA1 andBRCA2 genes in breast cancer families.The Breast Cancer Linkage Consortium.Am J Hum Genet 62: 676-689. 900. Foschini MP, Eusebi V (1998).Carcinomas of the breast showing myoep -ithelial cell differentiation. A review of theliterature. Virchows Arch 432: 303-310. 901. Foschini MP, Eusebi V, Tison V (1989).Alveolar soft part sarcoma of the cervixuteri. A case report. Pathol Res Pract 184:354-358. 902. Foschini MP, Marucci G, Eusebi V(2002). Low-grade mucoepidermoid carci-noma of salivary glands: characteristicimmunohistochemical profile and evi-dence of striated duct differentiation.Virchows Arch 440: 536-542. 903. Foschini MP, Pizzicannella G, PeterseJL, Eusebi V (1995). Adenomyoepitheliomaof the breast associated with low-gradeadenosquamous and sarcomatoid carci-nomas. Virchows Arch 427: 243-250. 904. Foulkes WD, Wong N, Brunet JS,Narod SA (1998). BRCA mutations and sur -vival in breast cancer. J Clin Oncol 16:3206-3208. 905. Fox H, Agrawal K, Langley FA (1972).The Brenner tumour of the ovary. A clini-copathological study of 54 cases. J ObstetGynaecol Br Commonw 79: 661-665. 906. Fox H, Agrawal K, Langley FA (1975). Aclinicopathologic study of 92 cases ofgranulosa cell tumor of the ovary with spe-cial reference to the factors influencingprognosis. Cancer 35: 231-241. 907. Fox H, Laurini RN (1988). Intraplacentalchoriocarcinoma: a report of two cases. JClin Pathol 41: 1085-1088. 908. Fox H, Sen DK (1967). A Krukenbergtumour of the uterine cervix. J ObstetGynaecol Br Commonw 74: 449-450. 909. Fox H, Wells M, Harris M, McWilliamLJ, Anderson GS (1988). Enteric tumours ofthe lower female genital tract: a report ofthree cases. Histopathology 12: 167-176. 910. Frable WJ, Kay S (1968). Carcinoma ofthe breast. Histologic and clinical featuresof apocrine tumors. Cancer 21: 756-763. 911. Fracchia AA, Robinson D, Legaspi A,Greenall MJ, Kinne DW, Groshen S (1985).Survival in bilateral breast cancer. Cancer55: 1414-1421.
912. Fraga M, Prieto O, Garcia-Caballero T,Beiras A, Forteza J (1994). Myxoidleiomyosarcoma of the uterine cervix.Histopathology 25: 381-384. 913. Franceschi S, Dal Maso L, Arniani S,Crosignani P, Vercelli M, Simonato L,Falcini F, Zanetti R, Barchielli A, SerrainoD, Rezza G (1998). Risk of cancer other thanKaposi's sarcoma and non-Hodgkin's lym-phoma in persons with AIDS in Italy.Cancer and AIDS Registry Linkage Study.Br J Cancer 78: 966-970. 9 1 4 . Franquemont DW, Frierson HF Jr.,Mills SE (1991). An immunohistochemicalstudy of normal endometrial stroma andendometrial stromal neoplasms. Evidencefor smooth muscle differentiation. Am JSurg Pathol 15: 861-870. 915. Fraser JL, Raza S, Chorny K, ConnollyJL, Schnitt SJ (1998). Columnar alterationwith prominent apical snouts and secre-tions: a spectrum of changes frequentlypresent in breast biopsies performed formicrocalcifications. Am J Surg Pathol 22:1521-1527. 916. Frei KA, Kinkel K (2001). Stagingendometrial cancer: role of magnetic reso-nance imaging. J Magn Reson Imaging 13:850-855. 917. Friedman HD, Mazur MT (1991).Primary ovarian leiomyosarcoma. Animmunohistochemical and ultrastructuralstudy. Arch Pathol Lab Med 115: 941-945. 918. Friedman LS, Gayther SA, Kurosaki T,Gordon D, Noble B, Casey G, Ponder BA,Anton-Culver H (1997). Mutation analysisof BRCA1 and BRCA2 in a male breast can-cer population. Am J Hum Genet 60: 313-319. 919. Friedrich EG Jr., Wilkinson EJ, Fu YS(1980). Carcinoma in situ of the vulva: acontinuing challenge. Am J ObstetGynecol 136: 830-843. 920. Frisch M, Biggar RJ, Goedert JJ(2000). Human papillomavirus-associatedcancers in patients with human immunod-eficiency virus infection and acquiredimmunodeficiency syndrome. J NatlCancer Inst 92: 1500-1510. 921. Fritz A, Percy C, Jack A,Shanmugaratnam K, Sobin LH, Parkin DM,Whelan S (2000). International Classifica-tion of Diseases for Oncology (ICD-O). 3rded. World Health Organization: Geneva.922. Frixen UH, Behrens J, Sachs M, EberleG, Voss B, Warda A, Lochner D, BirchmeierW (1991). E-cadherin-mediated cell-celladhesion prevents invasiveness of humancarcinoma cells. J Cell Biol 113: 173-185. 923. Fujii H, Matsumoto T, Yoshida M,Furugen Y, Takagaki T, Iwabuchi K, NakataY, Takagi Y, Moriya T, Ohtsuji N, Ohtsuji M,Hirose S, Shirai T (2002). Genetics of syn-chronous uterine and ovarian endometri-oid carcinoma: combined analyses of lossof heterozygosity, PTEN mutation, andmicrosatellite instability. Hum Pathol 33:421-428. 924. Fujii H, Szumel R, Marsh C, Zhou W,Gabrielson E (1996). Genetic progression,histological grade, and allelic loss in ductalcarcinoma in situ of the breast.Cancer Res56: 5260-5265. 925. Fujii H, Yoshida M, Gong ZX,Matsumoto T, Hamano Y, Fukunaga M,Hruban RH, Gabrielson E, Shirai T (2000).Frequent genetic heterogeneity in theclonal evolution of gynecological carci-nosarcoma and its influence on phenotyp-ic diversity. Cancer Res 60: 114-120.
926. Fujita M, Enomoto T, Wada H, InoueM, Okudaira Y, Shroyer KR (1996).Application of clonal analysis. Differentialdiagnosis for synchronous primary ovarianand endometrial cancers and metastaticcancer. Am J Clin Pathol 105: 350-359. 927. Fujiwaki R, Yoshida M, Iida K, OhnishiY, Ryuko K, Miyazaki K (1998). Epithelioidleiomyosarcoma of the uterine cervix.Acta Obstet Gynecol Scand 77: 246-248. 928. Fukunaga M (2001). Pseudoangio-matous hyperplasia of mammary stroma: acase of pure type after removal of fibroade-noma. APMIS 109: 113-116. 929. Fukunaga M, Ishihara A, Ushigome S(1998). Extrauterine low-grade endometrialstromal sarcoma: report of three cases.Pathol Int 48: 297-302. 930. Fukunaga M, Miyazawa Y, Ushigome S(1997). Endometrial low-grade stromal sar-coma with ovarian sex cord-like differenti-ation: report of two cases with an immuno-histochemical and flow cytometric study.Pathol Int 47: 412-415. 931. Fukunaga M, Nomura K, Endo Y,Ushigome S, Aizawa S (1996). Carcino-sar-coma of the uterus with extensive neu-roectodermal differentiation.Histopathology 29: 565-570. 932. Fukunaga M, Nomura K, Ishikawa E,Ushigome S (1997). Ovarian atypicalendometriosis: its close association withmalignant epithelial tumours. H i s t o -pathology 30: 249-255. 933. Fukunaga M, Ushigome S (1993).Malignant trophoblastic tumors: immuno-histochemical and flow cytometric com-parison of choriocarcinoma and placentalsite trophoblastic tumors. Hum Pathol 24:1098-1106. 934. Fukunaga M, Ushigome S (1997).Myofibroblastoma of the breast withdiverse differentiations. Arch Pathol LabMed 121: 599-603. 935. Fukunaga M, Ushigome S, FukunagaM, Sugishita M (1993). Application of flowcytometry in diagnosis of hydatidiformmoles. Mod Pathol 6: 353-359. 936. Fukushima M, Twiggs LB, Okagaki T(1986). Mixed intestinal adenocarcinoma-argentaffin carcinoma of the vagina.Gynecol Oncol 23: 387-394. 937. Fulop V, Mok SC, Genest DR, Gati I,Doszpod J, Berkowitz RS (1998). p53, p21,Rb and mdm2 oncoproteins. Expression innormal placenta, partial and completemole, and choriocarcinoma. J ReprodMed 43: 119-127. 9 3 8 . Fulop V, Mok SC, Genest DR, SzigetvariI, Cseh I, Berkowitz RS (1998). c-myc, c-erbB-2, c-fms and bcl-2 oncoproteins.Expression in normal placenta, partial andcomplete mole, and choriocarcinoma. JReprod Med 43: 101-110. 939. Funk KC, Heiken JP (1989). Papillarycystadenoma of the broad ligament in apatient with von Hippel-Lindau disease.AJR Am J Roentgenol 153: 527-528. 940. Furuya M, Shimizu M, Nishihara H, ItoT, Sakuragi N, Ishikura H, Yoshiki T (2001).Clear cell variant of malignant melanomaof the uterine cervix: a case report andreview of the literature. Gynecol Oncol 80:409-412. 941. Gabbay-Moore M, Ovadia Y, Neri A(1982). Accessory ovaries with bilateraldermoid cysts. Eur J Obstet GynecolReprod Biol 14: 171-173. 942. Gaber LW, Redline RW, Mostoufi-Zadeh M, Driscoll SG (1986). Invasive par-tial mole. Am J Clin Pathol 85: 722-724.

387References
943. Gad A, Azzopardi JG (1975). Lobularcarcinoma of the breast: a special variantof mucin-secreting carcinoma. J ClinPathol 28: 711-716. 944. Gad S, Caux-Moncoutier V, Pages-Berhouet S, Gauthier-Villars M, Coupier I,Pujol P, Frenay M, Gilbert B, Maugard C,Bignon YJ, Chevrier A, Rossi A, Fricker JP,Nguyen TD, Demange L, Aurias A,Bensimon A, Stoppa-Lyonnet D (2002).Significant contribution of large BRCA1gene rearrangements in 120 French breastand ovarian cancer families. Oncogene 21:6841-6847. 945. Gadaleanu V, Craciun C (1987).Malignant oncocytoma of the breast.Zentralbl Allg Pathol 133: 279-283. 946. Gadducci A, Ferdeghini M, Prontera C,Moretti L, Mariani G, Bianchi R, Fioretti P(1992). The concomitant determination ofdifferent tumor markers in patients withepithelial ovarian cancer and benign ovar-ian masses: relevance for differential diag-nosis. Gynecol Oncol 44: 147-154. 947. Gadducci A, Landoni F, Sartori E, ZolaP, Maggino T, Lissoni A, Bazzurini L, ArisioR, Romagnolo C, Cristofani R (1996).Uterine leiomyosarcoma: analysis of treat-ment failures and survival. Gynecol Oncol62: 25-32. 948. Gaertner EM, Farley JH, Taylor RR,Silver SA (1999). Collision of uterine rhab-doid tumor and endometrioid adenocarci-noma: a case report and review of the lit-erature. Int J Gynecol Pathol 18: 396-401. 949. Gaffey MJ, Mills SE, Boyd JC (1994).Aggressive papillary tumor of middleear/temporal bone and adnexal papillarycystadenoma. Manifestations of vonHippel-Lindau disease. Am J Surg Pathol18: 1254-1260. 950. Gaffey MJ, Mills SE, Frierson HF Jr.,Zarbo RJ, Boyd JC, Simpson JF, Weiss LM(1995). Medullary carcinoma of the breast:interobserver variability in histopathologicdiagnosis. Mod Pathol 8: 31-38. 951. Gagnon Y, Tetu B (1989). Ovarianmetastases of breast carcinoma. A clinico-pathologic study of 59 cases. Cancer 64:892-898. 952. Gal R, Dekel A, Ben David M, GoldmanJA, Kessler E (1988). Granular cellmyoblastoma of the cervix. Case report. BrJ Obstet Gynaecol 95: 720-722. 953. Galant C, Mazy S, Berliere M, Mazy G,Wallon J, Marbaix E (1997). Two schwan-nomas presenting as lumps in the samebreast. Diagn Cytopathol 16: 281-284. 954. Galea MH, Blamey RW, Elston CE, EllisIO (1992). The Nottingham PrognosticIndex in primary breast cancer. BreastCancer Res Treat 22: 207-219. 955. Gamallo C, Palacios J, Moreno G,Calvo dM, Suarez A, Armas A (1999). beta-catenin expression pattern in stage I and IIovarian carcinomas : relationship withbeta-catenin gene mutations, clinico-pathological features, and clinical out-come. Am J Pathol 155: 527-536. 956. Gamallo C, Palacios J, Suarez A,Pizarro A, Navarro P, Quintanilla M, Cano A(1993). Correlation of E-cadherin expres-sion with differentiation grade and histo-logical type in breast carcinoma. Am JPathol 142: 987-993. 957. Garber JE, Goldstein AM, Kantor AF,Dreyfus MG, Fraumeni JF Jr., Li FP (1991).Follow-up study of twenty-four familieswith Li-Fraumeni syndrome. Cancer Res51: 6094-6097.
958. Garcia-Higuera I, Taniguchi T,Ganesan S, Meyn MS, Timmers C, Hejna J,Grompe M, D'Andrea AD (2001).Interaction of the Fanconi anemia proteinsand BRCA1 in a common pathway. MolCell 7: 249-262. 959. Garcia A, Bussaglia E, Machin P,Matias-Guiu X, Prat J (2000). Loss of het-erozygosity on chromosome 17q in epithe-lial ovarian tumors: association with carci-nomas with serous differentiation. Int JGynecol Pathol 19: 152-157. 960. Garcia R, Troyas RG, Bercero EA(1995). Mullerian adenosarcoma of thecervix: differential diagnosis, histogenesisand review of the literature. Pathol Int 45:890-894. 961. Gardella C, Chumas JC, Pearl ML(1996). Ovarian lipoma of teratomatous ori -gin. Obstet Gynecol 87: 874-875. 962. Gardner GH, Greene RR, Peckham BM(1948). Normal and cystic structures of thebroad ligament. Am J Obstet Gynecol 55:917-939. 963. Garg PP, Kerlikowske K, Subak L,Grady D (1998). Hormone replacementtherapy and the risk of epithelial ovariancarcinoma: a meta-analysis. O b s t e tGynecol 92: 472-479. 964. Garrett AP, Lee KR, Colitti CR, MutoMG, Berkowitz RS, Mok SC (2001). k-rasmutation may be an early event in muci-nous ovarian tumorigenesis. Int J GynecolPathol 20: 244-251. 965. Garrett AP, Ng SW, Muto MG, WelchWR, Bell DA, Berkowitz RS, Mok SC (2000).ras gene activation and infrequent muta-tion in papillary serous carcinoma of theperitoneum. Gynecol Oncol 77: 105-111. 966. Garzetti GG, Ciavattini A, Goteri G,Stramazzoti D, Fabris G, Mannello B,Romanini C (1996). Proliferating cellnuclear antigen (PCNA) immunoreactivityin stage I endometrial cancer: A new prog-nostic factor. Int J Gynecol Cancer 6: 186-192. 967. Garzetti GG, Ciavattini A, Goteri G,Menzo S, de Nictolis M, Clementi M,Brugia M, Romanini C (1994). Vaginalmicropapillary lesions are not related tohuman papillomavirus infection: in situhybridization and polymerase chain reac-tion detection techniques. Gynecol ObstetInvest 38: 134-139. 968. Gatalica Z, Norris BA, Kovatich AJ(2000). Immunohistochemical localizationof prostate-specific antigen in ductalepithelium of male breast. Potential diag-nostic pitfall in patients with gynecomas-tia. Appl Immunohistochem MoleculMorphol 8: 158-161. 969. Gatchell FG, Dockerty MB, Clagett OT(1958). Intracystic carcinoma of the breast.Surg Gynecol Obstet 106: 347. 970. Gatta G, Lasota MB, Verdecchia A(1998). Survival of European women withgynaecological tumours, during the period1978-1989. Eur J Cancer 34: 2218-2225. 971. Gatti RA, Tward A, Concannon P(1999). Cancer risk in ATM heterozygotes:a model of phenotypic and mechanistic dif-ferences between missense and truncat-ing mutations. Mol Genet Metab 68: 419-423. 972. Gayther SA, Mangion J, Russell P,Seal S, Barfoot R, Ponder BA, Stratton MR,Easton D (1997). Variation of risks of breastand ovarian cancer associated with differ-ent germline mutations of the BRCA2 gene.Nat Genet 15: 103-105.
973. Gayther SA, Russell P, Harrington P,Antoniou AC, Easton DF, Ponder BA (1999).The contribution of germline BRCA1 andBRCA2 mutations to familial ovarian can-cer: no evidence for other ovarian cancer-susceptibility genes. Am J Hum Genet 65:1021-1029. 974. Gayther SA, Warren W, Mazoyer S,Russell PA, Harrington PA, Chiano M, SealS, Hamoudi R, van Rensburg EJ, DunningAM, Love R, Evans G, Easton D, Clayton D,Stratton MR, Ponder BAJ (1995). Germlinemutations of the BRCA1 gene in breast andovarian cancer families provide evidencefor a genotype-phenotype correlation. NatGenet 11: 428-433.975. Gehrig PA, Groben PA, Fowler WC Jr.,Walton LA, Van Le L (2001). Noninvasivepapillary serous carcinoma of theendometrium. Obstet Gynecol 97: 153-157. 976. Geisler S, Lonning PE, Aas T, JohnsenH, Fluge O, Haugen DF, Lillehaug JR,Akslen LA, Borresen-Dale AL (2001).Influence of TP53 gene alterations and c-erbB-2 expression on the response totreatment with doxorubicin in locallyadvanced breast cancer. Cancer Res 61:2505-2512. 977. Genest DR (2001). Partial hydatidiformmole: clinicopathological features, differ-ential diagnosis, ploidy and molecularstudies, and gold standards for diagnosis.Int J Gynecol Pathol 20: 315-322. 978. Genest DR, Laborde O, Berkowitz RS,Goldstein DP, Bernstein MR, Lage J (1991).A clinicopathologic study of 153 cases ofcomplete hydatidiform mole (1980-1990):histologic grade lacks prognostic signifi-cance. Obstet Gynecol 78: 402-409. 979. Geng L, Connolly DC, Isacson C, RonnettBM, Cho KR (1999). Atypical immature meta-plasia (AIM) of the cervix: is it related tohigh-grade squamous intraepithelial lesion(HSIL)? Hum Pathol 30: 345-351. 980. Gentile G, Formelli G, Pelusi G,Flamigni C (1997). Is vestibular micropapil-lomatosis associated with human papillo-mavirus infection? Eur J Gynaecol Oncol18: 523-525. 981. Geoffroy-Perez B, Janin N, Ossian K,Lauge A, Croquette MF, Griscelli C, DebreM, Bressac-de-Paillerets B, Aurias A,Stoppa-Lyonnet D, Andrieu N (2001).Cancer risk in heterozygotes for ataxia-telangiectasia. Int J Cancer 93: 288-293. 982. Georgiannos SN, Chin Aleong J,Goode AW, Sheaff M (2001). SecondaryNeoplasms of the Breast: A survey of the20th Century. Cancer 92: 2259-2266. 983. Geraads A, Tary P, Cloup N (1991).[Demons-Meigs syndrome caused byovarian goiter]. Rev Pneumol Clin 47: 194-196. 984. Gerald WL, Miller HK, Battifora H,Miettinen M, Silva EG, Rosai J (1991). Intra-abdominal desmoplastic small round-celltumor. Report of 19 cases of a distinctivetype of high-grade polyphenotypic malig-nancy affecting young individuals. Am JSurg Pathol 15: 499-513. 985. Gernow A, Ahrentsen OD (1989).Adenoid cystic carcinoma of theendometrium. Histopathology 15: 197-198. 986. Gersell DJ, Fulling KH (1989). Localizedneurofibromatosis of the female genitouri-nary tract. Am J Surg Pathol 13: 873-878. 987. Gersell DJ, Katzenstein AL (1981).Spindle cell carcinoma of the breast. Aclinocopathologic and ultrastructuralstudy. Hum Pathol 12: 550-561.
988. Gersell DJ, King TC (1988). Papillarycystadenoma of the mesosalpinx in vonHippel-Lindau disease. Am J Surg Pathol12: 145-149. 989. Gershenson DM, del Junco G, SilvaEG, Copeland LJ, Wharton JT, Rutledge FN(1986). Immature teratoma of the ovary.Obstet Gynecol 68: 624-629. 990. Ghadially FN (1985). D i a g n o s t i cElectron Microscopy of Tumors. Butter-worth & Company: London.991. Ghazali S (1973). Embryonic rhab-domyosarcoma of the urogenital tract. BrJ Surg 60: 124-128. 992. Giannacopoulos K, Giannacopoulou C,Matalliotakis I, Neonaki M, PapanicolaouN, Koumantakis E (1998). Pseudo-Meigs'syndrome caused by paraovarian fibroma.Eur J Gynaecol Oncol 19: 389-390. 993. Giannotti FO, Miiji LN, Vainchenker M,Gordan AN (2001). Breast cancer withchoriocarcinomatous and neuroendocrinefeatures. Sao Paulo Med J 119: 154-155. 994. Giardini R, Piccolo C, Rilke F (1992).Primary non-Hodgkin's lymphomas of thefemale breast. Cancer 69: 725-735. 995. Gibbons D, Leitch M, Coscia J,Lindberg G, Molberg K, Ashfaq R,Saboorian MH (2000). Fine NeedleAspiration Cytology and HistologicFindings of Granular Cell Tumor of theBreast: Review of 19 Cases withClinical/Radiologic Correlation. Breast J 6:27-30. 996. Gil-Moreno A, Garcia-Jimenez A,Gonzalez-Bosquet J, Esteller M, Castellvi-Vives J, Martinez Palones JM, Xercavins J(1997). Merkel cell carcinoma of the vulva.Gynecol Oncol 64: 526-532. 997. Gilbey S, Moore DH, Look KY, SuttonGP (1997). Vulvar keratoacanthoma. ObstetGynecol 89: 848-850. 998. Gilchrist KW, Gould VE, Hirschl S,Imbriglia JE, Patchefsky AS, Penner DW,Pickren J, Schwartz IS, Wheeler JE,Barnes JM, Mansour EG (1982).Interobserver variation in the identificationof breast carcinoma in intramammary lym-phatics. Hum Pathol 13: 170-172. 999. Gilchrist KW, Gray R, Fowble B,Tormey DC, Taylor SG (1993). Tumor necro-sis is a prognostic predictor for earlyrecurrence and death in lymph node-posi-tive breast cancer: a 10-year follow-upstudy of 728 Eastern Cooperative OncologyGroup patients. J Clin Oncol 11: 1929-1935. 1000. Gilks CB, Alkushi A, Yue JJ, Lanvin D,Ehlen TG, Miller DM (2003). Advanced-stage serous borderline tumors of theovary: a clinicopathological study of 49cases. Int J Gynecol Pathol 22: 29-36. 1001. Gilks CB, Bell DA, Scully RE (1990).Serous psammocarcinoma of the ovaryand peritoneum. Int J Gynecol Pathol 9:110-121. 1002. Gilks CB, Clement PB, Hart WR,Young RH (2000). Uterine adenomyomasexcluding atypical polypoid adenomyomasand adenomyomas of endocervical type: aclinicopathologic study of 30 cases of anunderemphasized lesion that may causediagnostic problems with brief considera-tion of adenomyomas of other female gen-ital tract sites. Int J Gynecol Pathol 19: 195-205. 1003. Gilks CB, Clement PB, Wood WS(1989). Trichoblastic fibroma. A clinico-pathologic study of three cases. Am JDermatopathol 11: 397-402.

388 References
1004. Gilks CB, Young RH, Aguirre P,DeLellis RA, Scully RE (1989). Adenomamalignum (minimal deviation adenocarci-noma) of the uterine cervix. A clinico-pathological and immunohistochemicalanalysis of 26 cases. Am J Surg Pathol 13:717-729. 1005. Gilks CB, Young RH, Clement PB, HartWR, Scully RE (1996). Adenomyomas of theuterine cervix of of endocervical type: areport of ten cases of a benign cervicaltumor that may be confused with adenomamalignum. Mod Pathol 9: 220-224. 1006. Gilks CB, Young RH, Gersell DJ,Clement PB (1997). Large cell neuroen-docrine carcinoma of the uterine cervix: aclinicopathologic study of 12 cases. Am JSurg Pathol 21: 905-914. 1007. Gillett CE, Lee AH, Millis RR, BarnesDM (1998). Cyclin D1 and associated pro-teins in mammary ductal carcinoma in situand atypical ductal hyperplasia. J Pathol184: 396-400. 1008. Gimm O, Attie-Bitach T, Lees JA,Vekemans M, Eng C (2000). Expression ofthe PTEN tumour suppressor protein dur-ing human development. Hum Mol Genet 9:1633-1639. 1009. Ginolhac SM, Gad S, Corbex M,Bressac-de-Paillerets B, Chompret A,Bignon YJ, Peyrat JP, Fournier J, Lasset C,Giraud S, Muller D, Fricker JP, Hardouin A,Berthet P, Maugard C, Nogues C, LidereauR, Longy M, Olschwang S, Toulas C,Guimbaud R, Yannoukakos D, Szabo C,Durocher F, Moisan AM, Simard J,Mazoyer S, Lynch HT, Goldgar D, Stoppa-Lyonnet D, Lenoir GM, Sinilnikova OM(2003). BRCA1 wild-type allele modifies riskof ovarian cancer in carriers of BRCA1germ-line mutations. Cancer EpidemiolBiomarkers Prev 12: 90-95. 1010. Giri DD, Dundas SA, Nottingham JF,Underwood JC (1989). Oestrogen recep-tors in benign epithelial lesions andintraduct carcinomas of the breast: animmunohistological study. Histopathology15: 575-584. 1011. Giroud F, Haroske G, Reith A, BockingA (1998). 1997 ESACP consensus report ondiagnostic DNA image cytometry. Part II:Specific recommendations for qualityassurance. European Society forAnalytical Cellular Pathology. Anal CellPathol 17: 201-208. 1012. Gisser SD (1986). Obstructing fallopi-an tube papilloma. Int J Gynecol Pathol 5:179-182. 1013. Gissmann L, deVilliers EM, zurHausen H (1982). Analysis of human genitalwarts (condylomata acuminata) and othergenital tumors for human papillomavirustype 6 DNA. Int J Cancer 29: 143-146. 1014. Gissmann L, Wolnik L, Ikenberg H,Koldovsky U, Schnurch HG, zur Hausen H(1983). Human papillomavirus types 6 and11 DNA sequences in genital and laryngealpapillomas and in some cervical cancers.Proc Natl Acad Sci USA 80: 560-563. 1015. Glaser SL, Ambinder RF, DiGiuseppeJA, Horn-Ross PL, Hsu JL (1998). Absenceof Epstein-Barr virus EBER-1 transcripts inan epidemiologically diverse group ofbreast cancers. Int J Cancer 75: 555-558. 1016. Glaubitz LC, Bowen JH, Cox EB,McCarty KS Jr. (1984). Elastosis in humanbreast cancer. Correlation with sex steroidreceptors and comparison with clinicaloutcome. Arch Pathol Lab Med 108: 27-30.
1017. Gleeson NC, Ruffolo EH, Hoffman MS,Cavanagh D (1994). Basal cell carcinomaof the vulva with groin node metastasis.Gynecol Oncol 53: 366-368. 1 0 1 8 . Gloor E, Dialdas J, Hurlimann J,Ribolzi J, Barrelet L (1983). Placental sitetrophoblastic tumor (trophoblastic pseudo-tumor) of the uterus with metastases andfatal outcome. Clinical and autopsy obser-vations of a case. Am J Surg Pathol 7: 483-486. 1019. Gloor E, Hurlimann J (1981).Trophoblastic pseudotumor of the uterus:clinicopathologic report with immunohis-tochemical and ultrastructural studies. AmJ Surg Pathol 5: 5-13. 1020. Glorieux I, Chabbert V, Rubie H,Baunin C, Gaspard MH, Guitard J, Duga I,Suc A, Puget C, Robert A (1998).[Autoimmune hemolytic anemia associat-ed with a mature ovarian teratoma]. ArchPediatr 5: 41-44. 1021. Glusac EJ, Hendrickson MS, SmollerBR (1994). Apocrine cystadenoma of thevulva. J Am Acad Dermatol 31: 498-499. 1022. Gobbi H, Simpson JF, Borowsky A,Jensen RA, Page DL (1999). Metaplasticbreast tumors with a dominant fibromato-sis-like phenotype have a high risk of localrecurrence. Cancer 85: 2170-2182. 1023. Gocht A, Bosmuller HC, Bassler R,Tavassoli FA, Moinfar F, Katenkamp D,Schirrmacher K, Luders P, Saeger W(1999). Breast tumors with myofibroblasticdifferentiation: clinico-pathological obser-vations in myofibroblastoma and myofi-brosarcoma. Pathol Res Pract 195: 1-10. 1 0 2 4 . Goff BA, Mandel L, Muntz HG,Melancon CH (2000). Ovarian carcinomadiagnosis. Cancer 89: 2068-2075. 1 0 2 5 . Goffin J, Chappuis PO, Wong N,Foulkes WD (2001). Re: Magnetic reso-nance imaging and mammography inwomen with a hereditary risk of breastcancer. J Natl Cancer Inst 93: 1754-1755. 1 0 2 6 . Golbang P, Khan A, Scurry J,MacIsaac I, Planner R (1997). Cervical sar-coma botryoides and ovarian Sertoli-Leydig cell tumor. Gynecol Oncol 67: 102-106. 1 0 2 7 . Goldblum J, Hart WR (1995).Localized and diffuse mesotheliomas ofthe genital tract and peritoneum in women.A clinicopathologic study of nineteen truemesothelial neoplasms, other than adeno-matoid tumors, multicystic mesotheliomas,and localized fibrous tumors. Am J SurgPathol 19: 1124-1137. 1 0 2 8 . Goldblum JR, Hart WR (1998).Perianal Paget's disease: a histologic andimmunohistochemical study of 11 caseswith and without associated rectal adeno -carcinoma. Am J Surg Pathol 22: 170-179. 1 0 2 9 . Goldgar DE, Easton DF, Cannon-Albright LA, Skolnick MH (1994).Systematic population-based assessmentof cancer risk in first-degree relatives ofcancer probands. J Natl Cancer Inst 86:1600-1608. 1030. Goldhirsch A, Glick JH, Gelber RD,Coates AS, Senn HJ (2001). Meeting high-lights: International Consensus Panel onthe Treatment of Primary Breast Cancer.Seventh International Conference onAdjuvant Therapy of Primary BreastCancer. J Clin Oncol 19: 3817-3827. 1031. Goldhirsch A, Glick JH, Gelber RD,Senn HJ (1998). Meeting highlights:International consensus panel on thetreatment of primary breast cancer. J NatlCancer Inst 90: 1601-1608.
1032. Goldstein NS, Ahmad E, Hussain M,Hankin RC, Perez-Reyes N (1998).Endocervical glandular atypia: does a pre -neoplastic lesion of adenocarcinoma insitu exist? Am J Clin Pathol 110: 200-209. 1033. Goldstein NS, Bassi D, Watts JC,Layfield LJ, Yaziji H, Gown AM (2001). E-cadherin reactivity of 95 noninvasive duc-tal and lobular lesions of the breast.Implications for the interpretation of prob-lematic lesions. Am J Clin Pathol 115: 534-542. 1034. Goldstein NS, O'Malley BA (1997).Cancerization of small ectatic ducts of thebreast by ductal carcinoma in situ cellswith apocrine snouts: a lesion associatedwith tubular carcinoma. Am J Clin Pathol107: 561-566. 1035. Gollamudi SV, Gelman RS, Peiro G,Schneider LJ, Schnitt SJ, Recht A, SilverBJ, Harris JR, Connolly JL (1997). Breast-conserving therapy for stage I-II synchro-nous bilateral breast carcinoma. Cancer79: 1362-1369. 1036. Gollard R, Kosty M, Bordin G, Wax A,Lacey C (1995). Two unusual presentationsof mullerian adenosarcoma: case reports,literature review, and treatment consider-ations. Gynecol Oncol 59: 412-422. 1037. Gong G, Devries S, Chew KL, Cha I,Ljung BM, Waldman FM (2001). Geneticchanges in paired atypical and usual duc-tal hyperplasia of the breast by compara-tive genomic hybridization. Clin CancerRes 7: 2410-2414. 1038. Gonzalez-Crussi F, Crawford SE, SunCC (1990). Intraabdominal desmoplasticsmall-cell tumors with divergent differenti-ation. Observations on three cases ofchildhood. Am J Surg Pathol 14: 633-642. 1039. Gonzalez-Moreno S, Yan H, AlcornKW, Sugarbaker PH (2002). Malignanttransformation of "benign" cystic mesothe-lioma of the peritoneum. J Surg Oncol 79:243-251. 1040. Goodman ZD, Taxy JB (1981).Fibroadenomas of the breast with promi-nent smooth muscle. Am J Surg Pathol 5:99-101. 1041. Gordon AN, Montag TW (1990).Sarcoma botryoides of the cervix: excisionfollowed by adjuvant chemotherapy forpreservation of reproductive function.Gynecol Oncol 36: 119-124. 1042. Gorlin RJ (1987). Nevoid basal-cellcarcinoma syndrome. Medicine (Baltimore)66: 98-113. 1043. Gorski GK, McMorrow LE, BlumsteinL, Faasse D, Donaldson MH (1992). Trisomy14 in two cases of granulosa cell tumor ofthe ovary. Cancer Genet Cytogenet 60: 202-205. 1044. Gotlieb WH, Friedman E, Bar-SadeRB, Kruglikova A, Hirsh-Yechezkel G,Modan B, Inbar M, Davidson B, KopolovicJ, Novikov I, Ben Baruch G (1998). Rates ofJewish ancestral mutations in BRCA1 andBRCA2 in borderline ovarian tumors. JNatl Cancer Inst 90: 995-1000. 1045. Gotoh T, Kikuchi Y, Takano M, Kita T,Ogata S, Aida S (2001). Epithelioidleiomyosarcoma of the uterine cervix.Gynecol Oncol 82: 400-405. 1046. Gottlieb C, Raju U, Greenwald KA(1990). Myoepithelial cells in the differen-tial diagnosis of complex benign andmalignant breast lesions: an immunohisto -chemical study. Mod Pathol 3: 135-140. 1047. Gould S (1967). Neurilemmoma withinthe broad ligament. A case report. J S CMed Assoc 63: 6-8.
1048. Govender NS, Goldstein DP (1977).Metastatic tubal mole and coexistingintrauterine pregnancy. Obstet Gynecol 49:67-69. 1049. Govoni E, Pileri S, Bazzocchi F, SeveriB, Martinelli G (1981). Postmastectomyangiosarcoma: ultrastructural study of acase. Tumori 67: 79-86. 1051. Goyert G, Budev H, Wright C, JonesA, Deppe G (1987). Vaginal mullerian stro-mal sarcoma. A case report. J ReprodMed 32: 129-130. 1052. Gradishar WJ (1996). Inflammatorybreast cancer: the evolution of multimodal-ity treatment strategies. Semin Surg Oncol12: 352-363. 1053. Graham MD, Yelland A, Peacock J,Beck N, Ford H, Gazet JC (1993). Bilateralcarcinoma of the breast. Eur J Surg Oncol19: 259-264. 1054. Granter SR, Nucci MR, Fletcher CD(1997). Aggressive angiomyxoma: reap-praisal of its relationship to angiomyofi-broblastoma in a series of 16 cases.Histopathology 30: 3-10. 1055. Gras E, Catasus L, Arguelles R,Moreno-Bueno G, Palacios J, Gamallo C,Matias-Guiu X, Prat J (2001). Microsatelliteinstability, MLH-1 promoter hypermethyla-tion, and frameshift mutations at codingmononucleotide repeat microsatellites inovarian tumors. Cancer 92: 2829-2836. 1056. Gray GF Jr., Glick AD, Kurtin PJ,Jones HW III (1986). Alveolar soft part sar-coma of the uterus. Hum Pathol 17: 297-300. 1057. Grayson W, Cooper K (2002). A reap-praisal of "Basaloid Carcinoma" of thecervix, and the differential diagnosis ofbasaloid cervical neoplasms. Adv AnatPathol 9: 290-300. 1058. Grayson W, Fourie J, Tiltman AJ(1998). Xanthomatous leiomyosarcoma ofthe uterine cervix. Int J Gynecol Pathol 17:89-90. 1059. Grayson W, Taylor LF, Cooper K(1999). Adenoid cystic and adenoid basalcarcinoma of the uterine cervix: compara-tive morphologic, mucin, and immunohisto-chemical profile of two rare neoplasms ofputative 'reserve cell' origin. Am J SurgPathol 23: 448-458. 1060. Grayson W, Taylor LF, Cooper K(2001). Carcinosarcoma of the uterinecervix: a report of eight cases withimmunohistochemical analysis and evalu-ation of human papillomavirus status. AmJ Surg Pathol 25: 338-347. 1061. Green DM (1990). Mucoid carcinomaof the breast with choriocarcinoma in itsmetastases. Histopathology 16: 504-506. 1062. Green I, McCormick B, Cranor M,Rosen PP (1997). A comparative study ofpure tubular and tubulolobular carcinomaof the breast. Am J Surg Pathol 21: 653-657. 1063. Green JA, Kirwan JM, Tierney JF,Symonds P, Fresco L, Collingwood M,Williams CJ (2001). Survival and recur-rence after concomitant chemotherapyand radiotherapy for cancer of the uterinecervix: a systematic review and meta-analysis. Lancet 358: 781-786. 1064. Green LK, Kott ML (1989).Histopathologic findings in ectopic tubalpregnancy. Int J Gynecol Pathol 8: 255-262. 1065. Greene JB, McCue SA (1978).Chorioadenoma destruens. Ann N Y AcadSci 80: 143. 1066. Greenlee RT, Hill-Harmon MB,Murray T, Thun M (2001). Cancer statistics,2001. CA Cancer J Clin 51: 15-36.

389References
1067. Grimes MM (1992). Cystosarcomaphyllodes of the breast: histologic fea-tures, flow cytometric analysis, and clini-cal correlations. Mod Pathol 5: 232-239. 1068. Grody WW, Nieberg RK, Bhuta S(1985). Ependymoma-like tumor of themesovarium. Arch Pathol Lab Med 109:291-293. 1069. Gronroos M, Meurman L, Kahra K(1983). Proliferating glia and other hetero-topic tissues in the uterus: fetal homo-grafts? Obstet Gynecol 61: 261-266. 1070. Gross GE, Barrasso R (1997). HumanPamilloma Virus Infection - A ClinicalAtlas. Berlin.1071. Gruber SB, Thompson WD (1996). Apopulation-based study of endometrialcancer and familial risk in younger women.Cancer and Steroid Hormone Study Group.Cancer Epidemiol Biomarkers Prev 5: 411-417. 1072. Gruvberger S, Ringner M, Chen Y,Panavally S, Saal LH, Borg A, Ferno M,Peterson C, Meltzer PS (2001). Estrogenreceptor status in breast cancer is associ-ated with remarkably distinct gene expres-sion patterns. Cancer Res 61: 5979-5984. 1073. Gudmundsson J, Barkardottir RB,Eiriksdottir G, Baldursson T, Arason A,Egilsson V, Ingvarsson S (1995). Loss ofheterozygosity at chromosome 11 in breastcancer: association of prognostic factorswith genetic alterations. Br J Cancer 72:696-701. 1074. Guerin M, Gabillot M, Mathieu MC,Travagli JP, Spielmann M, Andrieu N, RiouG (1989). Structure and expression of c-erbB-2 and EGF receptor genes in inflam-matory and non-inflammatory breast can-cer: prognostic significance. Int J Cancer43: 201-208. 1075. Guerrieri C, Franlund B, Boeryd B(1995). Expression of cytokeratin 7 in simul-taneous mucinous tumors of the ovary andappendix. Mod Pathol 8: 573-576. 1076. Guerrieri C, Hogberg T, Wingren S,Fristedt S, Simonsen E, Boeryd B (1994).Mucinous borderline and malignanttumors of the ovary. A clinicopathologicand DNA ploidy study of 92 cases. Cancer74: 2329-2340. 1077. Guerrieri C, Jarlsfelt I (1993).Ependymoma of the ovary. A case reportwith immunohistochemical, ultrastructural,and DNA cytometric findings, as well ashistogenetic considerations. Am J SurgPathol 17: 623-632. 1078. Guillou L, Wadden C, Coindre JM,Krausz T, Fletcher CD (1997). "Proximal-type" epithelioid sarcoma, a distinctiveaggressive neoplasm showing rhabdoidfeatures. Clinicopathologic, immunohisto-chemical, and ultrastructural study of aseries. Am J Surg Pathol 21: 130-146. 1079. Guinee VF, Olsson H, Moller T, HessKR, Taylor SH, Fahey T, Gladikov JV, vanden Blink JW, Bonichon F, Dische S, YatesJW, Cleaton FJ (1994). Effect of pregnancyon prognosis for young women with breastcancer. Lancet 343: 1587-1589. 1080. Guinet C, Ghossain MA, Buy JN,Malbec L, Hugol D, Truc JB, Vadrot D(1995). Mature cystic teratomas of theovary: CT and MR findings. Eur J Radiol 20:137-143. 1081. Gultekin SH, Cody HS III, Hoda SA(1996). Schwannoma of the breast. SouthMed J 89: 238-239. 1082. Gump FE (1990). Lobular carcinoma insitu. Pathology and treatment. Surg ClinNorth Am 70: 873-883.
1083. Gump FE, Sternschein MJ, Wolff M(1981). Fibromatosis of the breast. SurgGynecol Obstet 153: 57-60. 1084. Gunn RA, Gallager HS (1980). VulvarPaget's disease: a topographic study.Cancer 46: 590-594. 1085. Gunther K, Merkelbach-Bruse S,Amo-Takyi BK, Handt S, Schroder W,Tietze L (2001). Differences in geneticalterations between primary lobular andductal breast cancers detected by com-parative genomic hybridization. J Pathol193: 40-47. 1 0 8 6 . Guo Z, Thunberg U, Sallstrom J,Wilander E, Ponten J (1998). Clonalityanalysis of cervical cancer on microdis-sected archival materials by PCR-based X-chromosome inactivation approach. Int JOncol 12: 1327-1332. 1087. Gupta D, Balsara G (1999).Extrauterine malignancies. Role of Papsmears in diagnosis and management.Acta Cytol 43: 806-813. 1088. Gupta JW, Saito K, Saito A, Fu YS,Shah KV (1989). Human papillomavirusesand the pathogenesis of cervical neopla-sia. A study by in situ hybridization. Cancer64: 2104-2110. 1089. Gupta RK (1996). Aspiration cytodiag-nosis of a rare carcinoma of breast withbizarre malignant giant cells. D i a g nCytopathol 15: 66-69. 1090. Gupta SK, Douglas-Jones AG, JasaniB, Morgan JM, Pignatelli M, Mansel RE(1997). E-cadherin (E-cad) expression induct carcinoma in situ (DCIS) of the breast.Virchows Arch 430: 23-28. 1091. Gustafson ML, Lee MM, Scully RE,Moncure AC, Hirakawa T, Goodman A,Muntz HG, Donahoe PK, MacLaughlin DT,Fuller AF Jr. (1992). Mullerian inhibitingsubstance as a marker for ovarian sex-cord tumor. N Engl J Med 326: 466-471. 1092. Gustafsson A, Tartter PI, Brower ST,Lesnick G (1994). Prognosis of patientswith bilateral carcinoma of the breast. JAm Coll Surg 178: 111-116. 1093. Gwavava NJ, Traub AI (1980). Aneurilemmoma of the cervix. Br J ObstetGynaecol 87: 444-446. 1094. Ha HK, Baek SY, Kim SH, Kim HH,Chung EC, Yeon KM (1995). Krukenberg'stumor of the ovary: MR imaging features.AJR Am J Roentgenol 164: 1435-1439. 1095. Haagensen CD (1971). InflammatoryCarcinoma. In: Diseases of the Breast. CDHaagensen (Ed.) 2nd ed. WB Sauders:Philadelphia, pp. 576-584.1096. Haagensen CD (1986). Diseases ofthe Breast. 3rd ed. WB Saunders:Philadelphia.1097. Haagensen CD (1986). Multiple intra-ductal papilloma. In: Diseases of theBreast. 3rd ed. WB Saunders:Philadelphia, pp. 176-191.1098. Haagensen CD (1986). Solitary intra-ductal papilloma. In: Diseases of theB r e a s t . 3rd ed. WB Saunders:Philadelphia, pp. 136-175.1099. Haagensen CD, Lane N, Lattes R(1972). Neoplastic proliferation of theepithelium of the mammary lobules:adenosis, lobular neoplasia, and small cellcarcinoma. Surg Clin North Am 52: 497-524. 1100. Haagensen CD, Lane N, Lattes R,Bodian C (1978). Lobular neoplasia (so-called lobular carcinoma in situ) of thebreast. Cancer 42: 737-769. 1101. Haberal A, Turgut F, Ozbey B,Kucukali T, Sapmaz M (1995). Granular cellmyoblastoma of the cervix in a 14 year oldgirl. Cent Afr J Med 41: 298-300.
1102. Hachi H, Othmany A, Douayri A,Bouchikhi C, Tijami F, Laalou L, Chami M,Boughtab A, Jalil A, Benjelloun S, AhyoudF, Kettani F, Souadka A (2002). [Associationof ovarian juvenile granulosa cell tumorwith Maffucci's syndrome]. G y n e c o lObstet Fertil 30: 692-695. 1103. Hachisuga T, Sugimori H, Kaku T,Matsukuma K, Tsukamoto N, Nakano H(1990). Glassy cell carcinoma of theendometrium. Gynecol Oncol 36: 134-138. 1104. Hacker NF (2000). Uterine cancer. In:Practical Gynecologic Oncology. 3rd ed.Lippincott, William & Wilkins: Philadelphia,pp. 407-455.1105. Hacker NF, Berek JS, Lagasse LD,Nieberg RK, Leuchter RS (1984).Individualization of treatment for stage Isquamous cell vulvar carcinoma. ObstetGynecol 63: 155-162. 1106. Haefner HK, Tate JE, McLachlin CM,Crum CP (1995). Vulvar intraepithelial neo-plasia: age, morphological phenotype,papillomavirus DNA, and coexisting inva-sive carcinoma. Hum Pathol 26: 147-154. 1107. Hainaut P, Hollstein M (2000). p53 andhuman cancer: the first ten thousandmutations. Adv Cancer Res 77: 81-137. 1108. Hakem R, de la Pompa JL, Elia A,Potter J, Mak TW (1997). Partial rescue ofBrca1 (5-6) early embryonic lethality by p53or p21 null mutation. Nat Genet 16: 298-302. 1109. Hall JM, Lee MK, Newman B,Morrow JE, Anderson LA, Huey B, King MC(1990). Linkage of early-onset familialbreast cancer to chromosome 17q21.Science 250: 1684-1689. 1110. Hallgrimsson J, Scully RE (1972).Borderline and malignant Brenner tumoursof the ovary. A report of 15 cases. ActaPathol Microbiol Scand [A] 233: 56-66. 1111. Hamby LS, McGrath PC, Cibull ML,Schwartz RW (1991). Gastric carcinomametastatic to the breast. J Surg Oncol 48:117-121. 1112. Hameed K, Burslem MR (1970). Amelanotic ovarian neoplasm resemblingthe "retinal anlage" tumor. Cancer 25: 564-567. 1113. Hamele-Bena D, Cranor ML, SciottoC, Erlandson R, Rosen PP (1996).Uncommon presentation of mammarymyofibroblastoma. Mod Pathol 9: 786-790. 1114. Hamilton S, Aaltonen L (2000). WHOClassification of Tumours. Pathology andGenetics of Tumours of the DigestiveSystem. IARC Press: Lyon.1115. Hamilton SR, Liu B, Parsons RE,Papadopoulos N, Jen J, Powell SM, KrushAJ, Berk T, Cohen Z, Tetu B, Burger PC,Wood PA, Taqi F, Booker SV, Petersen GM,Offerhaus GJA, Tersmette AC, GiardielloFM, Volgelstein B, Kinzler KW. (1995). Themolecular basis of Turcot's syndrome. NEngl J Med 332: 839-847. 1116. Hamm B, Kubik-Huch RA, Fleige B(1999). MR imaging and CT of the femalepelvis: radiologic-pathologic correlation.Eur Radiol 9: 3-15. 1117. Hampl M, Hampl JA, Reiss G,Schackert G, Saeger HD, Schackert HK(1999). Loss of heterozygosity accumula-tion in primary breast carcinomas andadditionally in corresponding distantmetastases is associated with poor out-come. Clin Cancer Res 5: 1417-1425.
1118. Hampton GM, Mannermaa A,Winquist R, Alavaikko M, Blanco G,Taskinen PJ, Kiviniemi H, Newsham I,Cavenee WK, Evans GA (1994). Loss of het-erozygosity in sporadic human breast car-cinoma: a common region between 11q22and 11q23.3. Cancer Res 54: 4586-4589. 1119. Hampton GM, Penny LA, BaergenRN, Larson A, Brewer C, Liao S, Busby-Earle RM, Williams AW, Steel CM, Bird CC,Stanbridge EJ, Evans GA. (1994). Loss ofheterozygosity in cervical carcinoma: sub-chromosomal localization of a putativetumor-suppressor gene to chromosome11q22-q24. Proc Natl Acad Sci USA 91:6953-6957. 1120. Hampton HL, Huffman HT, Meeks GR(1992). Extraovarian Brenner tumor. ObstetGynecol 79: 844-846. 1121. Han HJ, Maruyama M, Baba S, ParkJG, Nakamura Y (1995). Genomic structureof human mismatch repair gene, hMLH1,and its mutation analysis in patients withhereditary non-polyposis colorectal can-cer (HNPCC). Hum Mol Genet 4: 237-242. 1122. Han HS, Park IA, Kim SH, Lee HP(1998). The clear cell variant of epithelioidintravenous leiomyomatosis of the uterus:report of a case. Pathol Int 48: 892-896. 1123. Hancock BW, Welch EM, GillespieAM, Newlands ES (2000). A retrospectivecomparison of current and proposed stag-ing and scoring systems for persistent ges-tational trophoblastic disease. Int JGynecol Cancer 10: 318-322. 1124. Hanjani P, Petersen RO, Bonnell SA(1980). Malignant mixed Mullerian tumor ofthe fallopian tube. Report of a case andreview of literature. Gynecol Oncol 9: 381-393. 1125. Hankins GR, De Souza AT, BentleyRC, Patel MR, Marks JR, Iglehart JD, JirtleRL (1996). M6P/IGF2 receptor: a candidatebreast tumor suppressor gene. Oncogene12: 2003-2009. 1126. Hankinson SE, Hunter DJ, Colditz GA,Willett WC, Stampfer MJ, Rosner B,Hennekens CH, Speizer FE (1993). Tubal lig-ation, hysterectomy, and risk of ovariancancer. A prospective study. JAMA 270:2813-2818. 1127. Hankinson SE, Willett WC, Colditz GA,Hunter DJ, Michaud DS, Deroo B, RosnerB, Speizer FE, Pollak M (1998). Circulatingconcentrations of insulin-like growth fac-tor-I and risk of breast cancer. Lancet 351:1393-1396. 1128. Hankinson SE, Willett WC, MansonJE, Colditz GA, Hunter DJ, Spiegelman D,Barbieri RL, Speizer FE (1998). Plasma sexsteroid hormone levels and risk of breastcancer in postmenopausal women. J NatlCancer Inst 90: 1292-1299. 1129. Hanna NN, O'Donnell K, Wolfe GR(1996). Alveolar soft part sarcoma metasta-tic to the breast. J Surg Oncol 61: 159-162. 1130. Hanna W, Kahn HJ (1985).Ultrastructural and immunohistochemicalcharacteristics of mucoepidermoid carci-noma of the breast. Hum Pathol 16: 941-946. 1131. Hanselaar A, van Loosbroek M,Schuurbiers O, Helmerhorst T, Bulten J,Bernhelm J (1997). Clear cell adenocarci-noma of the vagina and cervix. An updateof the central Netherlands registry show-ing twin age incidence peaks. Cancer 79:2229-2236.

390 References
1132. Hanselaar AG, Boss EA, MassugerLF, Bernheim JL (1999). Cytologic examina-tion to detect clear cell adenocarcinoma ofthe vagina or cervix. Gynecol Oncol 75:338-344. 1133. Hanssen AM, Fryns JP (1995).Cowden syndrome. J Med Genet 32: 117-119. 1134. Harada Y, Katagiri T, Ito I, Akiyama F,Sakamoto G, Kasumi F, Nakamura Y, Emi M(1994). Genetic studies of 457 breast can-cers. Clinicopathologic parameters com-pared with genetic alterations. Cancer 74:2281-2286. 1135. Hardesty LA, Sumkin JH, Hakim C,Johns C, Nath M (2001). The ability of heli-cal CT to preoperatively stage endometrialcarcinoma. Am J Roentgenol 176: 603-606. 1136. Hardesty LA, Sumkin JH, Nath ME,Edwards RP, Price FV, Chang TS, JohnsCM, Kelley JL (2000). Use of preoperativeMR imaging in the management ofendometrial carcinoma: cost analysis.Radiology 215: 45-49. 1137. Hardisson D, Simon RS, Burgos E(2001). Primary osteosarcoma of the uter-ine corpus: report of a case with immuno-histochemical and ultrastructural study.Gynecol Oncol 82: 181-186. 1138. Harkin DP, Bean JM, Miklos D, SongYH, Truong VB, Englert C, Christians FC,Ellisen LW, Maheswaran S, Oliner JD,Haber DA (1999). Induction of GADD45 andJNK/SAPK-dependent apoptosis followinginducible expression of BRCA1. Cell 97:575-586. 1139. Harlow BL, Weiss NS, Lofton S (1986).The epidemiology of sarcomas of theuterus. J Natl Cancer Inst 76: 399-402. 1140. Harnden P, Kennedy W, Andrew AC,Southgate J (1999). Immunophenotype oftransitional metaplasia of the uterinecervix. Int J Gynecol Pathol 18: 125-129. 1141. Haroske G, Giroud F, Reith A, BockingA (1998). 1997 ESACP consensus report ondiagnostic DNA image cytometry. Part I:basic considerations and recommenda-tions for preparation, measurement andinterpretation. European Society forAnalytical Cellular Pathology. Anal CellPathol 17: 189-200. 1142. Harris M, Howell A, Chrissohou M,Swindell RI, Hudson M, Sellwood RA(1984). A comparison of the metastatic pat-tern of infiltrating lobular carcinoma andinfiltrating duct carcinoma of the breast.Br J Cancer 50: 23-30. 1143. Harris M, Wells S, Vasudev KS (1978).Primary signet ring cell carcinoma of thebreast. Histopathology 2: 171-176. 1144. Harris NL, Jaffe ES, Diebold J,Flandrin G, Muller-Hermelink HK, VardimanJ, Lister TA, Bloomfield CD (2000). TheWorld Health Organization classification ofhematological malignancies report of theClinical Advisory Committee Meeting,Airlie House, Virginia, November 1997.Mod Pathol 13: 193-207. 1145. Harris NL, Scully RE (1984). Malignantlymphoma and granulocytic sarcoma ofthe uterus and vagina. A clinicopathologicanalysis of 27 cases. Cancer 53: 2530-2545. 1146. Harrison M, Magee HM, O'LoughlinJ, Gorey TF, Dervan PA (1995).Chromosome 1 aneusomy, identified byinterphase cytogenetics, in mammograph -ically detected ductal carcinoma in situ ofthe breast. J Pathol 175: 303-309. 1147. Hart WR (1977). Ovarian epithelialtumors of borderline malignancy (carcino-mas of low malignant potential). H u mPathol 8: 541-549.
1148. Hart WR, Billman JK Jr. (1978). Areassessment of uterine neoplasms origi-nally diagnosed as leiomyosarcomas.Cancer 41: 1902-1910. 1149. Hart WR, Craig JR (1978).Rhabdomyosarcomas of the uterus. Am JClin Pathol 70: 217-223. 1150. Hart WR, Norris HJ (1973). Borderlineand malignant mucinous tumors of theovary. Histologic criteria and clinicalbehavior. Cancer 31: 1031-1045. 1151. Hartge P, Struewing JP, WacholderS, Brody LC, Tucker MA (1999). The preva-lence of common BRCA1 and BRCA2 muta-tions among Ashkenazi Jews. Am J HumGenet 64: 963-970. 1152. Hartveit E (1990). Attenuated cells inbreast stroma: the missing lymphatic sys-tem of the breast. Histopathology 16: 533-543. 1153. Hasebe T, Mukai K, Tsuda H, Ochiai A(2000). New prognostic histological param-eter of invasive ductal carcinoma of thebreast: clinicopathological significance offibrotic focus. Pathol Int 50: 263-272. 1154. Hashiguchi J, Ito M, Kishikawa M,Sekine I, Kase Y (1994). Intravascularleiomyomatosis with uterine lipoleiomy-oma. Gynecol Oncol 52: 94-98. 1155. Haskel S, Chen SS, Spiegel G (1989).Vaginal endometrioid adenocarcinomaarising in vaginal endometriosis: a casereport and literature review. G y n e c o lOncol 34: 232-236. 1156. Hastrup N, Sehested M (1985). High-grade mucoepidermoid carcinoma of thebreast. Histopathology 9: 887-892. 1157. Haswani P, Arseneau J, Ferenczy A(1998). Primary signet cell carcinoma of theuterine cervix: a clinicopathologic study oftwo cases with review of the literature. IntJ Gynecol Cancer 8: 374-379. 1 1 5 8 . Hata JI, Ueyama Y, Tamaoki N,Akatsuka A, Yoshimura S, Shimuzu K,Morikawa Y, Furukawa T (1980). Humanyolk sac tumor serially transplanted innude mice: its morphologic and functionalproperties. Cancer 46: 2446-2455. 1159. Hauptmann S, Dietel M (2001).Serous tumors of low malignant potentialof the ovary-molecular pathology: part 2.Virchows Arch 438: 539-551. 1160. Hausen H. (2000). Papillomavirusescausing cancer: evasion from host-cellcontrol in early events in carcinogenesis.J Natl Cancer Inst 92: 690-698. 1161. Hawkins RE, Schofield JB, Fisher C,Wiltshaw E, McKinna JA (1992). The clini-cal and histologic criteria that predictmetastases from cystosarcoma phyllodes.Cancer 69: 141-147. 1162. Hayashi K, Bracken MB, Freeman DHJr., Hellenbrand K (1982). Hydatidiformmole in the United States (1970-1977): astatistical and theoretical analysis. Am JEpidemiol 115: 67-77. 1163. Hayes MC, Scully RE (1987). Ovariansteroid cell tumors (not otherwise speci-fied). A clinicopathological analysis of 63cases. Am J Surg Pathol 11: 835-845. 1164. Hayes MC, Scully RE (1987). Stromalluteoma of the ovary: a clinicopathologicalanalysis of 25 cases. Int J Gynecol Pathol6: 313-321. 1165. Hayes MM, Seidman JD, Ashton MA(1995). Glycogen-rich clear cell carcinomaof the breast. A clinicopathologic study of21 cases. Am J Surg Pathol 19: 904-911.
1166. Hays DM, Donaldson SS, Shimada H,Crist WM, Newton WA Jr., Andrassy RJ,Wiener E, Green J, Triche T, Maurer HM(1997). Primary and metastatic rhab-domyosarcoma in the breast: neoplasms ofadolescent females, a report from theIntergroup Rhabdomyosarcoma Study.Med Pediatr Oncol 29: 181-189. 1167. Healey CS, Dunning AM, Teare MD,Chase D, Parker L, Burn J, Chang-ClaudeJ, Mannermaa A, Kataja V, Huntsman DG,Pharoah PD, Luben RN, Easton DF, PonderBA (2000). A common variant in BRCA2 isassociated with both breast cancer riskand prenatal viability. Nat Genet 26: 362-364. 1168. Healey EA, Cook EF, Orav EJ, SchnittSJ, Connolly JL, Harris JR (1993).Contralateral breast cancer: clinical char-acteristics and impact on prognosis. J ClinOncol 11: 1545-1552. 1169. Heatley MK (2000). Adenomatoushyperplasia of the rete ovarii.Histopathology 36: 383-384. 1170. Heatley MK (2001). Polyp of the fal-lopian tube. Pathology 33: 538-539. 1171. Hedenfalk I, Duggan D, Chen Y,Radmacher M, Bittner M, Simon R, MeltzerP, Gusterson B, Esteller M, Kallioniemi OP,Wilfond B, Borg A, Trent J (2001). Gene-expression profiles in hereditary breastcancer. N Engl J Med 344: 539-548. 1172. Heffelfinger SC, Yassin R, Miller MA,Lower EE (2000). Cyclin D1, retinoblastoma,p53, and Her2/neu protein expression inpreinvasive breast pathologies: correlationwith vascularity. Pathobiology 68: 129-136. 1173. Hefler LA, Rosen AC, Graf AH,Lahousen M, Klein M, Leodolter S,Reinthaller A, Kainz C, Tempfer CB (2000).The clinical value of serum concentrationsof cancer antigen 125 in patients with pri-mary fallopian tube carcinoma: a multicen-ter study. Cancer 89: 1555-1560. 1 1 7 4 . Heifetz SA, Cushing B, Giller R,Shuster JJ, Stolar CJ, Vinocur CD,Hawkins EP (1998). Immature teratomas inchildren: pathologic considerations: areport from the combined PediatricOncology Group/Children's Cancer Group.Am J Surg Pathol 22: 1115-1124. 1175. Heim S, Teixeira MR, Dietrich CU,Pandis N (1997). Cytogenetic polyclonalityin tumors of the breast. Cancer GenetCytogenet 95: 16-19. 1176. Heimann R, Lan F, McBride R,Hellman S (2000). Separating favorablefrom unfavorable prognostic markers inbreast cancer: the role of E-cadherin.Cancer Res 60: 298-304. 1177. Heintz AP, Schaberg A, Engelsman E,van Hall EV (1985). Placental-site tro-phoblastic tumor: diagnosis, treatment,and biological behavior. Int J GynecolPathol 4: 75-82. 1178. Helland A, Karlsen F, Due EU, Holm R,Kristensen G, Borresen-Dale A (1998).Mutations in the TP53 gene and proteinexpression of p53, MDM 2 and p21/WAF-1in primary cervical carcinomas with no orlow human papillomavirus load. Br JCancer 78: 69-72. 1179. Heller DS, Keohane M, Bessim S,Jagirdar J, Deligdisch L (1989). Pituitary-containing benign cystic teratoma arisingfrom the uterosacral ligament. Arch PatholLab Med 113: 802-804. 1180. Heller DS, Rubinstein N, Dikman S,Deligdisch L, Moss R (1991). Adenomatouspolyp of the fallopian tube. A case report.J Reprod Med 36: 82-84.
1181. Hellman S, Harris JR (1987). Theappropriate breast cancer paradigm.Cancer Res 47: 339-342. 1181 a. Hellstrom AC, Hue J, Silfversward
C, Auer G (1994). DNA-ploidy and mutantp53 overexpression in primary fallopiantube cancer. Int J Gynecol Cancer 4: 408-413.1182. Hellstrom AC, Tegerstedt G,Silfversward C, Pettersson F (1999).Malignant mixed mullerian tumors of theovary: histopathologic and clinical reviewof 36 cases. Int J Gynecol Cancer 9: 312-316. 1183. Helzlsouer KJ, Alberg AJ, Bush TL,Longcope C, Gordon GB, Comstock GW(1994). A prospective study of endogenoushormones and breast cancer. C a n c e rDetect Prev 18: 79-85. 1184. Hemminki K, Dong C, Vaittinen P(1999). Familial risks in cervical cancer: isthere a hereditary component? Int JCancer 82: 775-781. 1185. Hemminki K, Vaittinen P (1999). Malebreast cancer: risk to daughters. Lancet353: 1186-1187. 1186. Hendrickson M, Ross J, Eifel P,Martinez A, Kempson R (1982). Uterinepapillary serous carcinoma: a highly malig-nant form of endometrial adenocarcinoma.Am J Surg Pathol 6: 93-108. 1187. Hendrickson MR, Kempson RL (1983).Ciliated carcinoma--a variant of endome-trial adenocarcinoma: a report of 10 cases.Int J Gynecol Pathol 2: 1-12. 1188. Hendrickson MR, Scheithauer BW(1986). Primitive neuroectodermal tumor ofthe endometrium: report of two cases, onewith electron microscopic observations.Int J Gynecol Pathol 5: 249-259. 1189. Hennig Y, Caselitz J, Bartnitzke S,Bullerdiek J (1997). A third case of a low-grade endometrial stromal sarcoma with at(7;17)(p14 approximately 21;q11.2 approxi -mately 21). Cancer Genet Cytogenet 98: 84-86. 1190. Henson DE, Ries L, Freedman LS,Carriaga M (1991). Relationship amongoutcome, stage of disease, and histologicgrade for 22,616 cases of breast cancer.The basis for a prognostic index. Cancer68: 2142-2149. 1191. Herbold DR, Axelrod JH, BobowskiSJ, Freel JH (1988). Glassy cell carcinomaof the fallopian tube. A case report. Int JGynecol Pathol 7: 384-390. 1192. Herbold DR, Fu YS, Silbert SW (1983).Leiomyosarcoma of the broad ligament. Acase report and literature review with fol-low-up. Am J Surg Pathol 7: 285-292. 1193. Herbst AL, Green TH Jr., Ulfelder H(1970). Primary carcinoma of the vagina.An analysis of 68 cases. Am J ObstetGynecol 106: 210-218. 1194. Herbst AL, Ulfelder H, Poskanzer DC(1971). Adenocarcinoma of the vagina.Association of maternal stilbestrol therapywith tumor appearance in young women.N Engl J Med 284: 878-881. 1195. Hermanek P, Hutter RV, Sobin LH,Wittekind C (1999). International UnionAgainst Cancer. Classification of isolatedtumor cells and micrometastasis. Cancer86: 2668-2673. 1 1 9 6 . Hernandez-Boussard TR-TPMRHP(2001). IARC p53 mutation database: a rela-tional database to compile and analyze p53mutations in human tumors and cell lines (R5version). WHO/IARC http://www.iarc.fr/P53.

391References
1197. Herod JJ, Shafi MI, Rollason TP,Jordan JA, Luesley DM (1996). Vulvarintraepithelial neoplasia with superficiallyinvasive carcinoma of the vulva. Br JObstet Gynaecol 103: 453-456. 1198. Herrera LJ, Lugo-Vicente H (1998).Primary embryonal rhabdomyosarcoma ofthe breast in an adolescent female: a casereport. J Pediatr Surg 33: 1582-1584. 1199. Herrero R, Munoz N (1999). Humanpapillomavirus and cancer. Cancer surv33: 75-98. 1200. Herrington CS, Tarin D, Buley I,Athanasou N (1994). Osteosarcomatousdifferentiation in carcinoma of the breast:a case of 'metaplastic' carcinoma withosteoclasts and osteoclast-like giant cells.Histopathology 24: 282-285. 1201. Herrington CS, Wells M (2002).Premalignant and malignant squamouslesions of the cervix. In: Haines and TaylorObstetrical and Gynaecological Pathology.H Fox, M Wells (Eds.) Fifth ed. ChurchillLivingstone: Edinburgh, pp. 297-338.1202. Hertel BF, Zaloudek C, Kempson RL(1976). Breast adenomas. Cancer 37: 2891-2905. 1203. Hertig AT, Mansell H (1956). Tumoursof the female sex organs. Part IHydatidiform mole and choriocarcinoma.In: Atlas of Tumour Pathology, AFIP (Ed.)AFIP: Washington,DC.1204. Hessler C, Schnyder P, Ozzello L(1978). Hamartoma of the breast: diagnos-tic observation of 16 cases. Radiology 126:95-98. 1205. Hetzel DJ, Wilson TO, Keeney GL,Roche PC, Cha SS, Podratz KC (1992). HER-2/neu expression: a major prognostic fac-tor in endometrial cancer. Gynecol Oncol47: 179-185. 1206. Heywang-Kobrunner SH, DershawDD, Schreer I (2000). Diagnostic BreastImaging. 2nd ed. Thieme: New York.1207. Hibberd AD, Horwood LJ, Wells JE(1983). Long term prognosis of women withbreast cancer in New Zealand: study ofsurvival to 30 years. Br Med J (Clin Res Ed)286: 1777-1779. 1208. Hidalgo A, Schewe C, Petersen S,Salcedo M, Gariglio P, Schluns K, Dietel M,Petersen I (2000). Human papilloma virusstatus and chromosomal imbalances inprimary cervical carcinomas and tumourcell lines. Eur J Cancer 36: 542-548. 1209. Hierro I, Blanes A, Matilla A, MunozS, Vicioso L, Nogales FF (2000). Merkel cell(neuroendocrine) carcinoma of the vulva.A case report with immunohistochemicaland ultrastructural findings and review ofthe literature. Pathol Res Pract 196: 503-509. 1210. Hill A, Yagmur Y, Tran KN, Bolton JS,Robson M, Borgen PI (1999). Localizedmale breast carcinoma and family history.An analysis of 142 patients. Cancer 86:821-825. 1211. Hill RP, Miller FN (1954). With casereport of carcinomatous transformation inan adenoma. Cancer 7: 318-324. 1212. Hinkula M, Pukkala E, Kyyronen P,Kauppila A (2002). Grand multiparity andincidence of endometrial cancer: a popu-lation-based study in Finland. Int J Cancer98: 912-915. 1213. Hiort O, Naber SP, Lehners A,Muletta-Feurer S, Sinnecker GH, Zollner A,Komminoth P (1996). The role of androgenreceptor gene mutations in male breastcarcinoma. J Clin Endocrinol Metab 81:3404-3407.
1214. Hirakawa T, Tsuneyoshi M, Enjoji M(1989). Squamous cell carcinoma arising inmature cystic teratoma of the ovary.Clinicopathologic and topographic analy-sis. Am J Surg Pathol 13: 397-405. 1215. Hirakawa T, Tsuneyoshi M, Enjoji M,Shigyo R (1988). Ovarian sarcoma with his-tologic features of telangiectatic osteosar-coma of the bone. Am J Surg Pathol 12:567-572. 1216. Hirano A, Emi M, Tsuneizumi M,Utada Y, Yoshimoto M, Kasumi F, AkiyamaF, Sakamoto G, Haga S, Kajiwara T,Nakamura Y (2001). Allelic losses of loci at3p25.1, 8p22, 13q12, 17p13.3, and 22q13 cor-relate with postoperative recurrence inbreast cancer. Clin Cancer Res 7: 876-882. 1217. Hirohashi S (1998). Inactivation of theE-cadherin-mediated cell adhesion systemin human cancers. Am J Pathol 153: 333-339. 1218. Hiroi H, Yasugi T, Matsumoto K, FujiiT, Watanabe T, Yoshikawa H, Taketani Y(2001). Mucinous adenocarcinoma arisingin a neovagina using the sigmoid colonthirty years after operation: a case report.J Surg Oncol 77: 61-64. 1219. Hislop TG, Elwood JM, Coldman AJ,Spinelli JJ, Worth AJ, Ellison LG (1984).Second primary cancers of the breast:incidence and risk factors. Br J Cancer 49:79-85. 1220. Hitchcock CL, Norris HJ (1992). Flowcytometric analysis of endometrial stromalsarcoma. Am J Clin Pathol 97: 267-271. 1221. Hittmair AP, Lininger RA, TavassoliFA (1998). Ductal carcinoma in situ (DCIS)in the male breast: a morphologic study of84 cases of pure DCIS and 30 cases ofDCIS associated with invasive carcinoma--a preliminary report. Cancer 83: 2139-2149. 1222. Ho YB, Robertson DI, Clement PB,Mincey EK (1982). Sclerosing stromaltumor of the ovary. Obstet Gynecol 60: 252-256. 1223. Hock YL, Mohamid W (1995). Myxoidneurofibroma of the male breast: fine nee-dle aspiration cytodiagnosis. C y t o p a t h o l o g y6: 44-47. 1224. Hocking GR, Hayman JA, Östör AG(1996). Adenocarcinoma in situ of the uter-ine cervix progressing to invasive adeno-carcinoma. Aust N Z J Obstet Gynaecol 36:218-220. 1225. Hoda SA, Cranor ML, Rosen PP(1992). Hemangiomas of the breast withatypical histological features. Furtheranalysis of histological subtypes confirm-ing their benign character. Am J SurgPathol 16: 553-560. 1226. Hoda SA, Prasad ML, Moore A, HodaRS, Giri D (1999). Microinvasive carcinomaof the breast: can it be diagnosed reliablyand is it clinically significant? H i s t o -pathology 35: 468-470. 1227. Hodak E, Jones RE, Ackerman AB(1993). Solitary keratoacanthoma is asquamous-cell carcinoma: three exampleswith metastases. Am J Dermatopathol 15:332-342. 1228. Hoerl HD, Hart WR (1998). Primaryovarian mucinous cystadenocarcinomas:a clinicopathologic study of 49 cases withlong-term follow-up. Am J Surg Pathol 22:1449-1462.
1229. Hogervorst FB, Nederlof PM, Gille JJ,McElgunn CJ, Grippeling M, Pruntel R,Regnerus R, van Welsem T, vanSpaendonk R, Menko FH, Kluijt I,Dommering C, Verhoef S, Schouten JP,van't Veer LJ, Pals G (2003). Large genom-ic deletions and duplications in the BRCA1gene identified by a novel quantitativemethod. Cancer Res 63: 1449-1453. 1230. Holland R, Faverly D (1997). Wholeorgan studies. In: Ductal Carcinoma in Situof the Breast. MJ Silverstein (Ed.) Williams& Wilkins: Baltimore. pp. 233-240.1230a. Holland R, Faverly D (1997). Thelocal distribution of ductal carcinoma insitu of the breast. In: Ductal Carcinoma inSitu of the Breast. MJ Silverstein (Ed.)Williams & Wilkins: Baltimore. pp. 233-240.1231. Holland R, Hendriks JH (1994).Microcalcifications associated with ductalcarcinoma in situ: mammographic-patho-logic correlation. Semin Diagn Pathol 11:181-192. 1232. Hollingsworth HC, Steinberg SM,Silverberg SG, Merino MJ (1996).Advanced stage transitional cell carcino-ma of the ovary. Hum Pathol 27: 1267-1272. 1233. Holmberg L, Adami HO, Ekbom A,Bergstrom R, Sandstrom A, Lindgren A(1988). Prognosis in bilateral breast can-cer. Effects of time interval between firstand second primary tumours. Br J Cancer58: 191-194. 1234. Holway AH, Rieger-Christ KM, MinerWR, Cain JW, Dugan JM, Pezza JA,Silverman ML, Shapter A, McLellan R,Summerhayes IC (2000). Somatic mutationof PTEN in vulvar cancer. Clin Cancer Res6: 3228-3235. 1235. Homesley HD, Bundy BN, Sedlis A,Yordan E, Berek JS, Jahshan A, Mortel R(1993). Prognostic factors for groin nodemetastasis in squamous cell carcinoma ofthe vulva (a Gynecologic Oncology Groupstudy). Gynecol Oncol 49: 279-283. 1236. Honore LH, Nickerson KG (1976).Papillary serous cystadenoma arising in aparamesonephric cyst of the parovarium.Am J Obstet Gynecol 125: 870-871. 1237. Hopkins M, Nunez C, Murphy JR,Wentz WB (1985). Malignant placental sitetrophoblastic tumor. Obstet Gynecol 66:95S-100S. 1238. Hopper JL, Carlin JB (1992). Familialaggregation of a disease consequent uponcorrelation between relatives in a risk fac-tor measured on a continuous scale. Am JEpidemiol 136: 1138-1147. 1239. Horie Y, Ikawa S, Kadowaki K,Minagawa Y, Kigawa J, Terakawa N(1995). Lipoadenofibroma of the uterinecorpus. Report of a new variant of adenofi-broma (benign mullerian mixed tumor).Arch Pathol Lab Med 119: 274-276. 1240. Horn LC, Einenkel J, Baier D (2000).Endometrial metastasis from breast can-cer in a patient receiving tamoxifen thera-py. Gynecol Obstet Invest 50: 136-138. 1241. Horn PL, Thompson WD (1988). Riskof contralateral breast cancer. A s s o-ciations with histologic, clinical, and thera-peutic factors. Cancer 62: 412-424. 1242. Horn T, Jao W, Keh PC (1983). Benigncystic teratoma of the fallopian tube. ArchPathol Lab Med 107: 48. 1243. Horne CH, Reid IN, Milne GD (1976).Prognostic significance of inappropriateproduction of pregnancy proteins bybreast cancers. Lancet 2: 279-282.
1244. Horsfall DJ, Tilley WD, Orell SR,Marshall VR, Cant EL (1986). Relationshipbetween ploidy and steroid hormonereceptors in primary invasive breast can-cer. Br J Cancer 53: 23-28. 1245. Houghton CR, Iversen T (1982).Squamous cell carcinoma of the vagina: aclinical study of the location of the tumor.Gynecol Oncol 13: 365-372. 1246. Houlston RS, McCarter E, Parbhoo S,Scurr JH, Slack J (1992). Family history andrisk of breast cancer. J Med Genet 29: 154-157. 1247. Houvras Y, Benezra M, Zhang H,Manfredi JJ, Weber BL, Licht JD (2000).BRCA1 physically and functionally inter-acts with ATF1. J Biol Chem 275: 36230-36237. 1248. Howarth CB, Caces JN, Pratt CB(1980). Breast metastases in children withrhabdomyosarcoma. Cancer 46: 2520-2524. 1249. Howat AJ, Armour A, Ellis IO (2000).Microinvasive lobular carcinoma of thebreast. Histopathology 37: 477-478. 1250. Howe JR, Bair JL, Sayed MG,Anderson ME, Mitros FA, Petersen GM,Velculescu VE, Traverso G, Vogelstein B(2001). Germline mutations of the geneencoding bone morphogenetic proteinreceptor 1A in juvenile polyposis. N a tGenet 28: 184-187. 1251. Howlett NG, Taniguchi T, Olson S,Cox B, Waisfisz Q, Die-Smulders C, PerskyN, Grompe M, Joenje H, Pals G, Ikeda H,Fox EA, D'Andrea AD (2002). Biallelic inac-tivation of BRCA2 in Fanconi anemia.Science 297: 606-609. 1252. Hrynchak M, Horsman D, Salski C,Berean K, Benedet JL (1994). Complexkaryotypic alterations in an endometrialstromal sarcoma. Cancer Genet Cytogenet77: 45-49. 1253. Hsing AW, McLaughlin JK, Cocco P,Co Chien HT, Fraumeni JFJr. (1998). Riskfactors for male breast cancer (UnitedStates). Cancer Causes Control 9: 269-275. 1254. Hsu SM, Raine L, Nayak RN (1981).Medullary carcinoma of breast: animmunohistochemical study of its lymphoidstroma. Cancer 48: 1368-1376. 1255. Hsueh S, Chang TC (1996). Malignantrhabdoid tumor of the uterine corpus.Gynecol Oncol 61: 142-146. 1256. Hu CY, Taymor ML, Hertig AT (1950).Primary carcinoma of the fallopian tube.Am J Obstet Gynecol 59: 58-60. 1257. Huang E, Cheng SH, Dressman H,Pittman J, Tsou MH, Horng CF, Bild A,Iversen ES, Liao M, Chen CM, West M,Nevins JR, Huang AT (2003). Gene expres-sion predictors of breast cancer out-comes. Lancet 361: 1590-1596. 1258. Huang KT, Chen CA, Cheng WF, WuCC, Jou HJ, Hsieh CY, Lin GJ, Hsieh FJ(1996). Sonographic characteristics ofadenofibroma of the endometrium follow-ing tamoxifen therapy for breast cancer:two case reports. Ultrasound ObstetGynecol 7: 363-366. 1259. Huang LW, Garrett AP, Schorge JO,Muto MG, Bell DA, Welch WR, BerkowitzRS, Mok SC (2000). Distinct allelic loss pat-terns in papillary serous carcinoma of theperitoneum. Am J Clin Pathol 114: 93-99. 1260. Huettner PC, Gersell DJ (1994).Placental site nodule: a clinicopathologicstudy of 38 cases. Int J Gynecol Pathol 1 3:191-198. 1261. Hugh JC, Jackson FI, Hanson J,Poppema S (1990). Primary breast lym-phoma. An immunohistologic study of 20new cases. Cancer 66: 2602-2611.

392 References
1262. Hughesdon PE (1982). Ovariantumours of Wolffian or allied nature: theirplace in ovarian oncology. J Clin Pathol 35:526-535. 1263. Hugues FC, Gourlot C, Le Jeunne C(2000). [Drug-induced gynecomastia]. AnnMed Interne (Paris) 151: 10-17. 1264. Hull MT, Warfel KA (1986). Glycogen-rich clear cell carcinomas of the breast. Aclinicopathologic and ultrastructuralstudy. Am J Surg Pathol 10: 553-559. 1265. Hull MT, Warfel KA (1987). Mucinousbreast carcinomas with abundant intracy-toplasmic mucin and neuroendocrine fea-tures: light microscopic, immunohisto-chemical, and ultrastructural study.Ultrastruct Pathol 11: 29-38. 1266. Humeniuk V, Forrest AP, Hawkins RA,Prescott R (1983). Elastosis and primarybreast cancer. Cancer 52: 1448-1452. 1267. Hunt CR, Hale RJ, Armstrong C,Rajkumar T, Gullick WJ, Buckley CH (1995).c-erbB-3 proto-oncogene expression inuterine cervical carcinoma. Int J GynecolCancer 5: 282-285. 1268. Hunt SJ, Santa Cruz DJ, Barr RJ(1990). Cellular angiolipoma. Am J SurgPathol 14: 75-81. 1269. Hunter CE Jr., Sawyers JL (1980).Intracystic papillary carcinoma of thebreast. South Med J 73: 1484-1486. 1270. Huntington RW Jr., Bullock WK(1970). Yolk sac tumors of extragonadal ori-gin. Cancer 25: 1368-1376. 1271. Huntsman DG, Clement PB, Gilks CB,Scully RE (1994). Small-cell carcinoma ofthe endometrium. A clinicopathologicalstudy of sixteen cases. Am J Surg Pathol18: 364-375. 1272. Husseinzadeh N, Recinto C (1999).Frequency of invasive cancer in surgicallyexcised vulvar lesions with intraepithelialneoplasia (VIN 3). Gynecol Oncol 73: 119-120. 1273. Huvos AG, Lucas JC Jr., Foote FW Jr.(1973). Metaplastic breast carcinoma. Rareform of mammary cancer. N Y State J Med73: 1078-1082. 1274. Iacocca MV, Maia DM (2001).Bilateral infiltrating lobular carcinoma ofthe breast with osteoclast-like giant cells.Breast J 7: 60-65. 1275. Ibrahim RE, Sciotto CG, Weidner N(1989). Pseudoangiomatous hyperplasia ofmammary stroma. Some observationsregarding its clinicopathologic spectrum.Cancer 63: 1154-1160. 1275a. Ichihara S, Aoyama H (1994).Intraductal carcinoma of the breast arising insclerosing adenosis. Pathol Int 44: 722-726. 1276. Ichikawa Y, Lemon SJ, Wang S,Franklin B, Watson P, Knezetic JA, BewtraC, Lynch HT (1999). Microsatellite instabili -ty and expression of MLH1 and MSH2 innormal and malignant endometrial andovarian epithelium in hereditary nonpoly-posis colorectal cancer family members.Cancer Genet Cytogenet 112: 2-8. 1277. Ichikawa Y, Tsunoda H, Takano K, OkiA, Yoshikawa H (2002). Microsatelliteinstability and immunohistochemicalanalysis of MLH1 and MSH2 in normalendometrium, endometrial hyperplasia andendometrial cancer from a hereditary non-polyposis colorectal cancer patient. Jpn JClin Oncol 32: 110-112.
1278. Ichinohasama R, Teshima S, Kishi K,Mukai K, Tsunematsu R, Ishii-Ohba H,Shimosato Y (1989). Leydig cell tumor of theovary associated with endometrial carci-noma and containing 17 beta-hydroxys-teroid dehydrogenase. Int J GynecolPathol 8: 64-71. 1279. Iczkowski KA, Han AC, Edelson MI,Rosenblum NG (2000). Primary, localizedvulvar B-cell lymphoma expressing CD44variant 6 but not cadherins. A case report.J Reprod Med 45: 853-856. 1280. Idvall I, Andersson C, Fallenius G,Ingvar C, Ringberg A, Strand C, AkermanM, Ferno M (2001). Histopathological andcell biological factors of ductal carcinomain situ before and after the introduction ofmammographic screening. Acta Oncol 40:653-659. 1280a. Ihara N, Togashi K, Todo G, Nakai A,Kojima N, Ishigaki T, Suginami N, KinoshitaM, Shintaku M (1999). Sclerosing stromaltumor of the ovary: MRI. J Comput AssistTomogr 23: 555-557. 1281. Ihekwaba FN (1994). Breast cancer inmen in black Africa: a report of 73 cases. JR Coll Surg Edinb 39: 344-347. 1282. Imachi M, Tsukamoto N, Amagase H,Shigematsu T, Amada S, Nakano H (1993).Metastatic adenocarcinoma to the uterinecervix from gastric cancer. A clinicopatho-logic analysis of 16 cases. Cancer 71: 3472-3477. 1283. Imachi M, Tsukamoto N, ShigematsuT, Nakano H (1992). Cytologic diagnosis ofprimary adenocarcinoma of Bartholin'sgland. A case report. Acta Cytol 36: 167-170. 1284. Imachi M, Tsukamoto N, ShigematsuT, Watanabe T, Uehira K, Amada S, UmezuT, Nakano H (1992). Malignant mixedMullerian tumor of the fallopian tube:report of two cases and review of litera-ture. Gynecol Oncol 47: 114-124. 1285. Imachi M, Tsukamoto N, ShimamotoT, Hirakawa T, Uehira K, Nakano H (1991).Clear cell carcinoma of the ovary: a clini-copathological analysis of 34 cases. Int JGynecol Cancer 1: 113-119. 1286. Imai H, Kitamura H, Nananura T,Watanabe M, Koyama T, Kitamura H(1999). Mullerian carcinofibroma of theuterus. A case report. Acta Cytol 43: 667-674. 1287. Inaji H, Koyama H (1991). [Tumormarkers. Personal experience--screeningof breast cancer by determining CEA innipple discharge]. Gan To Kagaku Ryoho18: 313-317. 1288. Innes KE, Byers TE (1999).Preeclampsia and breast cancer risk.Epidemiology 10: 722-732. 1289. Inoue H, Kikuchi Y, Hori T, Nabuchi K,Kobayashi M, Nagata I (1995). An ovariantumor of probable Wolffian origin with hor-monal function. Gynecol Oncol 59: 304-308. 1290. Inoue T, Nabeshima K, Shimao Y,Akiyama Y, Ohtsuka T, Koono M (2001).Tubal ectopic pregnancy associated withan adenomatoid tumor. Pathol Int 51: 211-214. 1291. Inskip HM, Kinlen LJ, Taylor AM,Woods CG, Arlett CF (1999). Risk of breastcancer and other cancers in heterozy-gotes for ataxia-telangiectasia. Br JCancer 79: 1304-1307. 1292. International Agency for Researchon Cancer (2002). IARC Handbooks ofCancer Prevention Vol. 6: Weight Controland Physical Activity. IARC Press: Lyon.
1293. International Agency for Researchon Cancer (1995). IARC Monographs on theEvaluation of the Carcinogenic Risks toHumans. Volume 64: Human papillo-maviruses. IARC Press: Lyon.1294. International Agency for Researchon Cancer (1999). Hormonal contracep-tives, progestogens only. In: IARCMonographs on the Evaluation ofCarcinogenic Risks to Humans Vol. 72Hormonal Contraception and Post-Menopausal Hormonal Therapy. I A R CPress: Lyon , pp. 339-397.1295. International Agency for Researchon Cancer (1999). IARC Monograph on theEvaluation of Carcinogenic Risk toHumans. Volume 72: Hormonal contracep-tion and post menopausal HormonalTherapy. IARC Press: Lyon.1296. International Agency for Researchon Cancer (1999). Oral contraceptives,combined. In: IARC Monographs on theEvaluation of Carcinogenic Risks toHumans Vol. 72 Hormonal Contraceptionand Post-Menopausal Hormonal Therapy.IARC Press: Lyon, pp. 49-338.1297. International Agency for Researchon Cancer (1999). Post-menopausaloestrogen-progestogen therapy. In: IARCMonographs on the Evaluation ofCarcinogenic Risks to Humans Vol. 72Hormonal Contraception and Post-Menopausal Hormonal Therapy. I A R CPress: Lyon, pp. 531-628.1298. International Agency for Researchon Cancer (1999). Post-menopausaloestrogen therapy. In: IARC Monographson the Evaluation of Carcinogenic Risks toHumans Vol. 72 Hormonal Contraceptionand Post-Menopausal Hormonal Therapy.IARC Press: Lyon, pp. 399-530.1299. International Cowden's SyndromeConsortium, Operational Criteria for theDiagnosis of CS, Daly M (1999). NCCNpractice guidelines: Genetics/familial high-risk cancer screening. Oncology 13: 161-186. 1 3 0 0 . International Federation ofGynecology and Obstretrics (1995).Modifications in the Staging for Stage IVulvar and Stage I Cervical Cancer.Reports of the FIGO Committee onGynaecologic Oncology. Int J GynaecolObstet 50: 215-216. 1301. Iqbal M, Davies MP, Shoker BS,Jarvis C, Sibson DR, Sloane JP (2001).Subgroups of non-atypical hyperplasia ofbreast defined by proliferation of oestro-gen receptor-positive cells. J Pathol 193:333-338. 1302. Iraniha S, Shen V, Kruppe CN,Downey EC (1999). Uterine cervicalextrarenal Wilms tumor managed withouthysterectomy. J Pediatr Hematol Oncol 21:548-550. 1303. Isaac MA, Vijayalakshmi S, MadhuCS, Bosincu L, Nogales FF (2000). Pure cys-tic nephroblastoma of the ovary with areview of extrarenal Wilms' tumors. HumPathol 31: 761-764. 1304. Isaacs C, Stearns V, Hayes DF (2001).New prognostic factors for breast cancerrecurrence. Semin Oncol 28: 53-67. 1305. Isaacson PG, Spencer J (1987).Malignant lymphoma of mucosa-associat-ed lymphoid tissue. Histopathology 11: 445-462. 1 3 0 6 . Ishikura H, Kojo T, Ichimura H,Yoshiki T (1998). Desmoplastic malignantmelanoma of the uterine cervix: a rare pri-mary malignancy in the uterus mimicking asarcoma. Histopathology 33: 93-94.
1307. Ishikura H, Scully RE (1987). Hepatoidcarcinoma of the ovary. A newly describedtumor. Cancer 60: 2775-2784. 1 3 0 8 . Ismail SM, Walker SM (1990).Bilateral virilizing sclerosing stromaltumours of the ovary in a pregnant womanwith Gorlin's syndrome: implications forpathogenesis of ovarian stromal neo-plasms. Histopathology 17: 159-163. 1309. Ito K, Watanabe K, Nasim S, SasanoH, Sato S, Yajima A, Silverberg SG, GarrettCT (1994). Prognostic significance of p53overexpression in endometrial cancer.Cancer Res 54: 4667-4670. 1310. Ito T, Saga S, Nagayoshi S, Imai M,Aoyama A, Yokoi T, Hoshino M (1986).Class distribution of immunoglobulin-con-taining plasma cells in the stroma ofmedullary carcinoma of breast. B r e a s tCancer Res Treat 7: 97-103. 1311. Itoh T, Mochizuki M, Kumazaki S,Ishihara T, Fukayama M (1997). Cystic pul-monary metastases of endometrial stromalsarcoma of the uterus, mimicking lym-phangiomyomatosis: a case report withimmunohistochemistry of HMB45. PatholInt 47: 725-729. 1312. Iversen T, Tretli S (1998). Intraepi-thelial and invasive squamous cell neopla-sia of the vulva: trends in incidence, recur-rence, and survival rate in Norway. ObstetGynecol 91: 969-972. 1313. Iversen UM (1996). Two cases ofbenign vaginal rhabdomyoma. Casereports. APMIS 104: 575-578. 1314. Iwasaka T, Yokoyama M, OhuchidaM, Matsuo N, Hara K, Fukuyama K,Hachisuga T, Fukuda K, Sugimori H (1992).Detection of human papillomavirusgenome and analysis of expression of c-myc and Ha-ras oncogenes in invasivecervical carcinomas. Gynecol Oncol 46:298-303. 1315. Jack MT, Woo RA, Hirao A, CheungA, Mak TW, Lee PW (2002). Chk2 is dispen-sable for p53-mediated G1 arrest but isrequired for a latent p53-mediated apop-totic response. Proc Natl Acad Sci USA .99:9825-9829. 1316. Jackson-York GL, Ramzy I (1992).Synchronous papillary mucinous adeno-carcinoma of the endocervix and fallopiantubes. Int J Gynecol Pathol 11: 63-67. 1317. Jacobs AJ, Newland JR, Green RK(1982). Pure choriocarcinoma of the ovary.Obstet Gynecol Surv 37: 603-609. 1318. Jacobs DM, Sandles LG, Leboit PE(1986). Sebaceous carcinoma arising fromBowen's disease of the vulva. A r c hDermatol 122: 1191-1193. 1319. Jacobs PA, Szulman AE, FunkhouserJ, Matsuura JS, Wilson CC (1982). Humantriploidy: relationship between parentalorigin of the additional haploid comple-ment and development of partial hydatidi-form mole. Ann Hum Genet 46: 223-231. 1320. Jacobs TW, Byrne C, Colditz G,Connolly JL, Schnitt SJ (1999). Radial scarsin benign breast-biopsy specimens and therisk of breast cancer. N Engl J Med 340:430-436. 1321. Jacobsen GK, Braendstrup O,Talerman A (1991). Bilateral mixed germcell sex-cord stroma tumour in a youngadult woman. Case report. APMIS Suppl23: 132-137. 1321a. Jacobsen O (1946). Heredity andBreast Cancer. London.1322. Jacoby AF, Fuller AF Jr., Thor AD,Muntz HG (1993). Primary leiomyosarcomaof the fallopian tube. Gynecol Oncol 51:404-407.

393References
1323. Jacques SM, Qureshi F, Ramirez NC,Malviya VK, Lawrence WD (1997). Tumorsof the uterine isthmus: clinicopathologicfeatures and immunohistochemical char-acterization of p53 expression and hor-mone receptors. Int J Gynecol Pathol 16:38-44. 1324. Jaffe R, Altaras M, Bernheim J, BenAderet N (1985). Endocervical stromal sar -coma--a case report. Gynecol Oncol 22:105-108. 1325. Jafri NH, Niemann TH, Nicklin JL,Copeland LJ (1998). A carcinoid tumor ofthe broad ligament. Obstet Gynecol 92: 708. 1326. Jain AN, Chin K, Borresen-Dale AL,Erikstein BK, Eynstein LP, Kaaresen R,Gray JW (2001). Quantitative analysis ofchromosomal CGH in human breast tumorsassociates copy number abnormalitieswith p53 status and patient survival. ProcNatl Acad Sci USA 98: 7952-7957. 1327. Jain S, Fisher C, Smith P, Millis RR,Rubens RD (1993). Patterns of metastaticbreast cancer in relation to histologicaltype. Eur J Cancer 29A: 2155-2157. 1328. Jakubowska A, Narod SA, GoldgarDE, Mierzejewski M, Masojc B, Nej K,Huzarska J, Byrski T, Gorski B, Lubinski J(2003). Breast Cancer Risk ReductionAssociated with the RAD51 Polymorphismamong Carriers of the BRCA1 5382insCMutation in Poland. Cancer EpidemiolBiomarkers Prev 12: 457-459. 1329. Jamal AA (2001). Pattern of breastdiseases in a teaching hospital in Jeddah,Saudi Arabia. Saudi Med J 22: 110-113. 1330. Jamal S, Mushtaq S, Malik IA, KhanAH, Mamoon N (1994). Malignant tumoursof the male breast - a review of 50 cases. JPak Med Assoc 44: 275-277. 1331. James BA, Cranor MI, Rosen PP(1993). Carcinoma of the breast arising inmicroglandular adenosis. Am J Clin Pathol100: 507-513. 1332. James K, Bridger J, Anthony PP(1988). Breast tumour of pregnancy ('lac-tating' adenoma). J Pathol 156: 37-44. 1333. James LA, Mitchell EL, Menasce L,Varley JM (1997). Comparative genomichybridisation of ductal carcinoma in situ ofthe breast: identification of regions of DNAamplification and deletion in common withinvasive breast carcinoma. Oncogene 14:1059-1065. 1334. Janin N, Andrieu N, Ossian K, LaugeA, Croquette MF, Griscelli C, Debre M,Bressac-de-Paillerets B, Aurias A, Stoppa-Lyonnet D (1999). Breast cancer risk inataxia telangiectasia (AT) heterozygotes:haplotype study in French AT families. Br JCancer 80: 1042-1045. 1335. Janvoski NA, Paramanandhan TL(1973). Ovarian Tumors. Tumors and tumor-like conditions of the ovaries, fallopiantubes and ligaments of the uterus. Majorproblems in obstetrics and gynecology.WB Sauders: Philadelphia.1336. Japaze H, Van Dinh T, Woodruff JD(1982). Verrucous carcinoma of the vulva:study of 24 cases. Obstet Gynecol 60: 462-466. 1337. Jauniaux E, Nicolaides KH, Hustin J(1997). Perinatal features associated withplacental mesenchymal dysplasia.Placenta 18: 701-706. 1338. Jee KJ, Kim YT, Kim KR, Kim HS, YanA, Knuutila S (2001). Loss in 3p and 4p andgain of 3q are concomitant aberrations insquamous cell carcinoma of the vulva.Mod Pathol 14: 377-381.
1339. Jensen ML, Kiaer H, Andersen J,Jensen V, Melsen F (1997). Prognosticcomparison of three classifications formedullary carcinomas of the breast.Histopathology 30: 523-532. 1340. Jensen ML, Kiaer H, Melsen F (1996).Medullary breast carcinoma vs. poorly dif -ferentiated ductal carcinoma: an immuno-histochemical study with keratin 19 andoestrogen receptor staining.Histopathology 29: 241-245. 1341. Jensen ML, Nielsen MN (1989).Broad ligament mucinous and serous cys-tadenomas of borderline malignancy. ActaObstet Gynecol Scand 68: 663-667. 1342. Jensen ML, Nielsen MN (1990).Broad ligament mucinous cystadenoma ofborderline malignancy. Histopathology 16:89-91. 1343. Jensen PA, Dockerty MB, SymmondsRE, Wilson RB (1966). Endometrioid sarco-ma ("stromal endometriosis"). Report of 15cases including 5 with metastases. Am JObstet Gynecol 95: 79-90. 1344. Jensen RD, Norris HJ, Fraumeni JFJr. (1974). Familial arrhenoblastoma andthyroid adenoma. Cancer 33: 218-223. 1345. Jensen V, Jensen ML, Kiaer H,Andersen J, Melsen F (1997). MIB-1expression in breast carcinomas withmedullary features. An immunohistologicalstudy including correlations with p53 andbcl-2. Virchows Arch 431: 125-130. 1346. Jeon HJ, Akagi T, Hoshida Y, HayashiK, Yoshino T, Tanaka T, Ito J, Kamei T,Kawabata K (1992). Primary non-Hodgkinmalignant lymphoma of the breast. Animmunohistochemical study of sevenpatients and literature review of 152patients with breast lymphoma in Japan.Cancer 70: 2451-2459. 1347. Jernstrom H (2001). Breast-feedingand the Risk of Breast Cancer in BRCA1and BRCA2 Carriers. Am J Hum Genet 69:9. 1348. Jernstrom H, Lerman C, Ghadirian P,Lynch HT, Weber B, Garber J, Daly M,Olopade OI, Foulkes WD, Warner E, BrunetJS, Narod SA (1999). Pregnancy and risk ofearly breast cancer in carriers of BRCA1and BRCA2. Lancet 354: 1846-1850. 1349. Jhala DN, Atkinson BF, Balsara GR,Hernandez E, Jhala NC (2001). Role of DNAploidy analysis in endometrial adenocarci -noma. Ann Diagn Pathol 5: 267-273. 1350. Jiao YF, Nakamura S, Oikawa T,Sugai T, Uesugi N (2001). Sebaceous glandmetaplasia in intraductal papilloma of thebreast. Virchows Arch 438: 505-508. 1351. Johannsson O, Loman N, Borg A,Olsson H (1998). Pregnancy-associatedbreast cancer in BRCA1 and BRCA2germline mutation carriers. Lancet 3 5 2 :1359-1360. 1352. Johannsson OT, Idvall I, Anderson C,Borg A, Barkardottir RB, Egilsson V, OlssonH (1997). Tumour biological features ofBRCA1-induced breast and ovarian can-cer. Eur J Cancer 33: 362-371. 1353. Johannsson OT, Ranstam J, Borg A,Olsson H (1998). Survival of BRCA1 breastand ovarian cancer patients: a population-based study from southern Sweden. J ClinOncol 16: 397-404. 1 3 5 4 . Johnson AD, Hebert AA, Esterly NB(1986). Nevoid basal cell carcinoma syn-drome: bilateral ovarian fibromas in a 3 1/2-year-old girl. J Am Acad Dermatol 14: 371-374. 1355. Johnson TL, Kumar NB, White CD,Morley GW (1986). Prognostic features ofvulvar melanoma: a clinicopathologicanalysis. Int J Gynecol Pathol 5: 110-118.
1356. Jones D.B. (1955). Florid papillomato-sis of the nipple ducts. Cancer 8: 315-319. 1357. Jones C, Damiani S, Wells D,Chaggar R, Lakhani SR, Eusebi V (2001).Molecular cytogenetic comparison ofapocrine hyperplasia and apocrine carci-noma of the breast. Am J Pathol 158: 207-214. 1358. Jones C, Merrett S, Thomas VA,Barker TH, Lakhani SR (2003). Comparativegenomic hybridization analysis of bilateralhyperplasia of usual type of the breast. JPathol 199: 152-156. 1359. Jones HW, III (1999). The importanceof grading in endometrial cancer. GynecolOncol 74: 1-2. 1360. Jones HW, III, Droegemueller W,Makowski EL (1971). A primary melanocar-cinoma of the cervix. Am J Obstet Gynecol111: 959-963. 1361. Jones MA, Mann EW, Caldwell CL,Tarraza HM, Dickersin GR, Young RH(1990). Small cell neuroendocrine carcino -ma of Bartholin's gland. Am J Clin Pathol94: 439-442. 1362. Jones MA, Young RH, Scully RE(1991). Diffuse laminar endocervical glan-dular hyperplasia. A benign lesion oftenconfused with adenoma malignum (mini-mal deviation adenocarcinoma). Am JSurg Pathol 15: 1123-1129. 1363. Jones MW, Kounelis S, Papadaki H,Bakker A, Swalsky PA, Woods J,Finkelstein SD (2000). Well-differentiatedvilloglandular adenocarcinoma of the uter-ine cervix: oncogene/tumor suppressorgene alterations and human papillo-mavirus genotyping. Int J Gynecol Pathol19: 110-117. 1 3 6 4 . Jones MW, Norris HJ (1995).Clinicopathologic study of 28 uterineleiomyosarcomas with metastasis. Int JGynecol Pathol 14: 243-249. 1365. Jones MW, Norris HJ, Snyder RC(1989). Infiltrating syringomatous adenomaof the nipple. A clinical and pathologicalstudy of 11 cases. Am J Surg Pathol 13:197-201. 1366. Jones MW, Silverberg SG, KurmanRJ (1993). Well-differentiated villoglandu-lar adenocarcinoma of the uterine cervix: aclinicopathological study of 24 cases. Int JGynecol Pathol 12: 1-7. 1367. Jones MW, Tavassoli FA (1995).Coexistence of nipple duct adenoma andbreast carcinoma: a clinicopathologicstudy of five cases and review of the liter-ature. Mod Pathol 8: 633-636. 1368. Jones PA, Laird PW (1999). Cancerepigenetics comes of age. Nat Genet 21:163-167. 1369. Jones RW, Rowan DM (1994). Vulvarintraepithelial neoplasia III: a clinical studyof the outcome in 113 cases with relationto the later development of invasive vulvarcarcinoma. Obstet Gynecol 84: 741-745. 1 3 7 0 . Jordan LB, Abdul-Kader M, alNafussi A (2001). Uterine serous papillarycarcinoma: histopathologic changes with-in the female genital tract. Int J GynecolCancer 11: 283-289. 1371. Joseph RE, Enghardt MH, DoeringDL, Brown BF, Shaffer DW, Raval HB(1992). Small cell neuroendocrine carcino -ma of the vagina. Cancer 70: 784-789. 1372. Joshi MG, Lee AK, Pedersen CA,Schnitt S, Camus MG, Hughes KS (1996).The role of immunocytochemical markersin the differential diagnosis of proliferativeand neoplastic lesions of the breast. ModPathol 9: 57-62.
1373. Jozefczyk MA, Rosen PP (1985).Vascular tumors of the breast. II.Perilobular hemangiomas and heman-giomas. Am J Surg Pathol 9: 491-503. 1374. Julien M, Trojani M, Coindre JM(1994). [Myofibroblastoma of the breast.Report of 8 cases]. Ann Pathol 14: 143-147. 1375. Junge J, Horn T, Bock J (1989).Primary malignant Schwannoma of theuterine cervix. Case report. Br J ObstetGynaecol 96: 111-116. 1376. Kaaks R (1996). Nutrition, hormones,and breast cancer: is insulin the missinglink? Cancer Causes Control 7: 605-625. 1377. Kaaks R, Lundin E, Manjer J, RinaldiS, Biessy C, Soderberg S, Lenner P, JanzonL, Riboli E, Berglund G, Hallmans G (2002).Prospective study of IGF-I, IGF-bindingproteins and breast cancer risk, in north-ern and southern Sweden. Cancer CausesControl 13: 307-316. 1378. Kachel G, Bornkamm GW, HermanekP, Kaduk B, Schricker KT (1980). [Burkittlymphoma of African type in Europe(author's transl)]. Dtsch Med Wochenschr105: 413-417. 1 3 7 9 . Kader HA, Jackson J, Mates D,Andersen S, Hayes M, Olivotto IA (2001).Tubular carcinoma of the breast: a popula-tion-based study of nodal metastases atpresentation and of patterns of relapse.Breast J 7: 8-13. 1380. Kaern J, Trope CG, Kristensen GB,Abeler VM, Pettersen EO (1993). DNAploidy; the most important prognostic fac-tor in patients with borderline tumors of theovary. Int J Gynecol Cancer 3: 349-358. 1381. Kahanpaa KV, Wahlstrom T, Grohn P,Heinonen E, Nieminen U, Widholm O(1986). Sarcomas of the uterus: a clinico-pathologic study of 119 patients. ObstetGynecol 67: 417-424. 1382. Kahner S, Ferenczy A, Richart RM(1975). Homologous mixed Mulleriantumors (carcinosarcomal) confined toendometrial polyps. Am J Obstet Gynecol121: 278-279. 1383. Kainu T, Juo SH, Desper R, SchafferAA, Gillanders E, Rozenblum E, Freas-LutzD, Weaver D, Stephan D, Bailey-Wilson J,Kallioniemi OP, Tirkkonen M, Syrjakoski K,Kuukasjarvi T, Koivisto P, Karhu R, Holli K,Arason A, Johannesdottir G, BergthorssonJT, Johannsdottir H, Egilsson V,Barkardottir RB, Johannsson O,Haraldsson K, Sandberg T, Holmberg E,Gronberg H, Olsson H, Borg A, VehmanenP, Eerola H, Heikkila P, Pyrhonen S,Nevanlinna H (2000). Somatic deletions inhereditary breast cancers implicate 13q21as a putative novel breast cancer suscep-tibility locus. Proc Natl Acad Sci USA 97:9603-9608. 1384. Kairouz R, Clarke RA, Marr PJ,Watters D, Lavin MF, Kearsley JH, Lee CS(1999). ATM protein synthesis patterns insporadic breast cancer. Mol Pathol 52:252-256. 1385. Kajii T, Ohama K (1977). Androgeneticorigin of hydatidiform mole. Nature 268:633-634. 1386. Kajiwara M, Toyoshima S, Yao T,Tanaka M, Tsuneyoshi M (1999). Apoptosisand cell proliferation in medullary carcino-ma of the breast: a comparative studybetween medullary and non-medullarycarcinoma using the TUNEL method andimmunohistochemistry. J Surg Oncol 70:209-216.

394 References
1387. Kaku T, Kamura T, Shigematsu T,Sakai K, Nakanami N, Uehira K, Amada S,Kobayashi H, Saito T, Nakano H (1997).Adenocarcinoma of the uterine cervix withpredominantly villogladular papillarygrowth pattern. Gynecol Oncol 64: 147-152. 1388. Kaku T, Silverberg SG, Major FJ,Miller A, Fetter B, Brady MF (1992).Adenosarcoma of the uterus: aGynecologic Oncology Group clinico-pathologic study of 31 cases. Int J GynecolPathol 11: 75-88. 1389. Kallenberg GA, Pesce CM, NormanB, Ratner RE, Silvergerg SG (1990). Ectopichyperprolactinemia resulting from an ovar-ian teratoma. JAMA 263: 2472-2474. 1390. Kalstone CE, Jaffe RB, Abell MR(1969). Massive edema of the ovary simu-lating fibroma. Obstet Gynecol 34: 564-571. 1391. Kaminski PF, Norris HJ (1983).Minimal deviation carcinoma (adenomamalignum) of the cervix. Int J GynecolPathol 2: 141-152. 1392. Kaminski PF, Norris HJ (1984).Coexistence of ovarian neoplasms andendocervical adenocarcinoma. O b s t e tGynecol 64: 553-556. 1393. Kamoi S, Iskander M, Akin MR,Silverberg SG (1998). Immunohistochemi-cal distinction between endometrial andendocervical adenocarcinomas: Site oforigin versus pathway of differentiation.Mod Pathol 11: 106 A. 1394. Kanai Y, Oda T, Tsuda H, Ochiai A,Hirohashi S (1994). Point mutation of the E-cadherin gene in invasive lobular carcino-ma of the breast. Jpn J Cancer Res 85:1035-1039. 1395. Kang Y, Siegel PM, Shu W, DrobnjakM, Kakonen SM, Cordon-Cardo C, GuiseTA, Massague J (2003). A multigenic pro-gram mediating breast cancer metastasisto bone. Cancer Cell 3: 537-549. 1396. Kao GF, Norris HJ (1978). Benign andlow grade variants of mixed mesodermaltumor (adenosarcoma) of the ovary andadnexal region. Cancer 42: 1314-1324. 1397. Kapadia SB, Norris HJ (1993).Rhabdomyoma of the vagina. Mod Pathol6: 75A. 1398. Kaplan EJ, Caputo TA, Shen PU,Sassoon RI, Soslow RA (1998). Familialpapillary serous carcinoma of the cervix,peritoneum, and ovary: a report of the firstcase. Gynecol Oncol 70: 289-294. 1399. Karayiannakis AJ, Bastounis EA,Chatzigianni EB, Makri GG, Alexiou D,Karamanakos P (1996). Immunohisto-chemical detection of oestrogen receptorsin ductal carcinoma in situ of the breast.Eur J Surg Oncol 22: 578-582. 1400. Kariminejad MH, Scully RE (1973).Female adnexal tumor of probableWolffian origin. A distinctive pathologicentity. Cancer 31: 671-677. 1401. Karl SR, Ballentine TVN, Hershey RZ(1985). Juvenile secretory carcinoma ofthe breast. J Ped Surg 20: 368-371. 1402. Karlan BY, Baldwin RL, Lopez-Luevanos E, Raffel LJ, Barbuto D, Narod S,Platt LD (1999). Peritoneal serous papillarycarcinoma, a phenotypic variant of familialovarian cancer: implications for ovariancancer screening. Am J Obstet Gynecol180: 917-928. 1403. Karseladze AI (2001). On the site oforigin of epithelial tumors of the ovary. EurJ Gynaecol Oncol 22: 110-115. 1404. Karseladze AI, Zakharova TI, NavarroS, Llombart-Bosch A (2000). Malignantfibrous histiocytoma of the uterus. Eur JGynaecol Oncol 21: 588-590.
1405. Kasamatsu T, Shiromizu K, TakahashiM, Kikuchi A, Uehara T (1998). Leiomyo-sarcoma of the uterine cervix. GynecolOncol 69: 169-171. 1406. Kasami M, Olson SJ, Simpson JF,Page DL (1998). Maintenance of polarityand a dual cell population in adenoid cys-tic carcinoma of the breast: an immunohis-tochemical study. Histopathology 32: 232-238. 1 4 0 7 . Kaspersen P, Buhl L, Moller BR(1988). Fallopian tube papilloma in a patientwith primary sterility. Acta Obstet GynecolScand 67: 93-94. 1408. Katabuchi H, Tashiro H, Cho KR,Kurman RJ, Hedrick EL (1998).Micropapillary serous carcinoma of theovary: an immunohistochemical and muta-tional analysis of p53. Int J Gynecol Pathol17: 54-60. 1409. Katsube Y, Berg JW, Silverberg SG(1982). Epidemiologic pathology of ovariantumors: a histopathologic review of pri-mary ovarian neoplasms diagnosed in theDenver Standard Metropolitan StatisticalArea, 1 July-31 December 1969 and 1 July-31 December 1979. Int J Gynecol Pathol 1:3-16. 1409 a. Katsube Y, Iwaoki Y, Silverberg SG,Fujiwara A (1988). Sclerosing stromaltumor of the ovary associated withendometrial adenocarcinoma: a casereport. Gynecol Oncol 29: 392-398. 1410. Katsube Y, Mukai K, Silverberg SG(1982). Cystic mesothelioma of the peri-toneum: a report of five cases and reviewof the literature. Cancer 50: 1615-1622. 1411. Katz L, Merino MJ, Sakamoto H,Schwartz PE (1987). Endometrial stromalsarcoma: a clinicopathologic study of 11cases with determination of estrogen andprogestin receptor levels in three tumors.Gynecol Oncol 26: 87-97. 1412. Katzenstein AL, Mazur MT, MorganTE, Kao MS (1978). Proliferative seroustumors of the ovary. Histologic featuresand prognosis. Am J Surg Pathol 2: 339-355. 1413. Kauff ND, Satagopan JM, RobsonME, Scheuer L, Hensley M, Hudis CA, EllisNA, Boyd J, Borgen PI, Barakat RR, NortonL, Castiel M, Nafa K, Offit K (2002). Risk-reducing salpingo-oophorectomy inwomen with a BRCA1 or BRCA2 mutation.N Engl J Med 346: 1609-1615. 1414. Kaufman MW, Marti JR, Gallager HS,Hoehn JL (1984). Carcinoma of the breastwith pseudosarcomatous metaplasia.Cancer 53: 1908-1917. 1415. Kaufman SL, Stout AP (1960).Hemangiopericytoma in children. Cancer13: 695-710. 1416. Kawai K, Horiguchi H, Sekido N,Akaza H, Koiso K (1996). Leiomyosarcomaof the ovarian vein: an unusual cause ofsevere abdominal and flank pain. Int J Urol3: 234-236. 1417. Kawamoto S, Urban BA, Fishman EK(1999). CT of epithelial ovarian tumors.Radiographics 19 Spec No: S85-102. 1418. Kawauchi S, Fukuda T, Miyamoto S,Yoshioka J, Shirahama S, Saito T,Tsukamoto N (1998). Peripheral primitiveneuroectodermal tumor of the ovary con-firmed by CD99 immunostaining, karyotyp-ic analysis, and RT-PCR for EWS/FLI-1chimeric mRNA. Am J Surg Pathol 2 2 :1417-1422.
1419. Kawauchi S, Tsuji T, Kaku T, KamuraT, Nakano H, Tsuneyoshi M (1998).Sclerosing stromal tumor of the ovary: aclinicopathologic, immunohistochemical,ultrastructural, and cytogenetic analysiswith special reference to its vasculature.Am J Surg Pathol 22: 83-92. 1420. Kay S, Schneider V (1985). Reactivespindle cell nodule of the endocervix simu-lating uterine sarcoma. Int J GynecolPathol 4: 255-257. 1421. Kayaalp E, Heller DS, Majmudar B(2000). Serous tumor of low malignantpotential of the fallopian tube. Int JGynecol Pathol 19: 398-400. 1422. Keating JT, Cviko A, Riethdorf S,Riethdorf L, Quade BJ, Sun D, Duensing S,Sheets EE, Munger K, Crum CP (2001). Ki-67, cyclin E, and p16INK4 are complimenta-ry surrogate biomarkers for human papillo-ma virus-related cervical neoplasia. Am JSurg Pathol 25: 884-891. 1423. Keatings L, Sinclair J, Wright C,Corbett IP, Watchorn C, Hennessy C,Angus B, Lennard T, Horne CH (1990). c-erbB-2 oncoprotein expression in mamma-ry and extramammary Paget's disease.Histopathology 17: 243-247. 1424. Keel SB, Clement PB, Prat J, YoungRH (1998). Malignant schwannoma of theuterine cervix: a study of three cases. Int JGynecol Pathol 17: 223-230. 1424a. Keelan PA, Myers JL, Wold LE,Katzmann JA, Gibney DJ (1992). Phyllodestumor: clinicopathologic review of 60patients and flow cytometric analysis in 30patients. Hum Pathol 23: 1048-1054. 1425. Keeney GL, Thrasher TV (1988).Metaplastic papillary tumor of the fallopiantube: a case report with ultrastructure. IntJ Gynecol Pathol 7: 86-92. 1426. Keep D, Zaragoza MV, Hassold T,Redline RW (1996). Very early completehydatidiform mole. Hum Pathol 27: 708-713. 1427. Keitoku M, Konishi I, Nanbu K,Yamamoto S, Mandai M, Kataoka N, OishiT, Mori T (1997). Extraovarian sex cord-stromal tumor: case report and review ofthe literature. Int J Gynecol Pathol 16: 180-185. 1428. Kelley JL, III, Burke TW, Tornos C,Morris M, Gershenson DM, Silva EG,Wharton JT (1992). Minimally invasive vul-var carcinoma: an indication for conserva-tive surgical therapy. Gynecol Oncol 44:240-244. 1429. Kelly RR, Scully RE (1961). Cancerdeveloping in dermoid cysts of the ovary. Areport of 8 cases, including a carcinoid anda leiomyosarcoma. Cancer 14: 989-1000. 1430. Kelsey JL, Gammon MD, John EM(1993). Reproductive factors and breastcancer. Epidemiol Rev 15: 36-47. 1431. Kempson RL, Fletcher CDM, EvansHL, Hendrikson MR, Sibley RK (2001).Tumours of the Soft Tissues. AFIP:Washington, DC.1432. Kempson RL, Hendrickson MR (2000).Smooth muscle, endometrial stromal, andmixed Mullerian tumors of the uterus. ModPathol 13: 328-342. 1433. Kendall BS, Ronnett BM, Isacson C,Cho KR, Hedrick L, Diener-West M,Kurman RJ (1998). Reproducibility of thediagnosis of endometrial hyperplasia,atypical hyperplasia, and well-differentiat-ed carcinoma. Am J Surg Pathol 22: 1012-1019. 1434. Kennebeck CH, Alagoz T (1998).Signet ring breast carcinoma metastaseslimited to the endometrium and cervix.Gynecol Oncol 71: 461-464.
1435. Kennedy AW, Biscotti CV, Hart WR,Webster KD (1989). Ovarian clear cell ade-nocarcinoma. Gynecol Oncol 32: 342-349. 1436. Kennedy AW, Markman M, WebsterKD, Kulp B, Peterson G, Rybicki LA,Belinson JL (1998). Experience with plat-inum-paclitaxel chemotherapy in the initialmanagement of papillary serous carcino-ma of the peritoneum. Gynecol Oncol 71:288-290. 1437. Kennedy MM, Baigrie CF, Manek S(1999). Tamoxifen and the endometrium:review of 102 cases and comparison withHRT-related and non-HRT-relatedendometrial pathology. Int J GynecolPathol 18: 130-137. 1438. Kenny-Moynihan MB, Hagen J,Richman B, McIntosh DG, Bridge JA(1996). Loss of an X chromosome inaggressive angiomyxoma of female softparts: a case report. Cancer GenetCytogenet 89: 61-64. 1439. Kerangueven F, Eisinger F, NoguchiT, Allione F, Wargniez V, Eng C, Padberg G,Theillet C, Jacquemier J, Longy M, SobolH, Birnbaum D (1997). Loss of heterozygos-ity in human breast carcinomas in the atax-ia telangiectasia, Cowden disease andBRCA1 gene regions. Oncogene 14: 339-347. 1439a. Kerlikowske K, Barclay J, Grady D,Sickles EA, Ernster V (1997). Comparison ofrisk factors for ductal carcinoma in situand invasive breast cancer. J Natl CancerInst 89: 76-82. 1440. Kermarec J, Plouvier S, Duplay H,Daniel R (1973). [Myoepithelial cell breasttumor. Ultrastructural study]. Arch AnatPathol (Paris) 21: 225-231. 1441. Kerner H, Sabo E, Friedman M, BeckD, Samare O, Lichtig C (1995). An immuno-histochemical study of estrogen and prog -esterone receptors in adenocarcinoma ofthe endometrium and in the adjacentmucosa. Int J Gynecol Cancer 5: 275-281. 1442. Kerr P, Ashworth A (2001). New com-plexities for BRCA1 and BRCA2. Curr Biol11: R668-R676. 1443. Kerrigan SA, Turnnir RT, Clement PB,Young RH, Churg A (2002). Diffuse malig-nant epithelial mesotheliomas of the peri-toneum in women: a clinicopathologicstudy of 25 patients. Cancer 94: 378-385. 1 4 4 4 . Kersemaekers AM, Hermans J,Fleuren GJ, Van de Vijver MJ (1998). Lossof heterozygosity for defined regions onchromosomes 3, 11 and 17 in carcinomasof the uterine cervix. Br J Cancer 77: 192-200. 1445. Kersemaekers AM, Van de Vijver MJ,Kenter GG, Fleuren GJ (1999). Geneticalterations during the progression of squa-mous cell carcinomas of the uterine cervix.Genes Chromosomes Cancer 26: 346-354. 1446. Key TJ (1999). Serum oestradiol andbreast cancer risk. Endocr Relat Cancer 6:175-180. 1447. Key TJ, Pike MC (1988). The role ofoestrogens and progestagens in the epi-demiology and prevention of breast can-cer. Eur J Cancer Clin Oncol 24: 29-43. 1448. Khalifa MA, Hansen CH, Moore JLJr., Rusnock EJ, Lage JM (1996).Endometrial stromal sarcoma with focalsmooth muscle differentiation: recurrenceafter 17 years: a follow-up report with dis-cussion of the nomenclature. Int JGynecol Pathol 15: 171-176.

395References
1449. Khalifa MA, Mannel RS, Haraway SD,Walker J, Min KW (1994). Expression ofEGFR, HER-2/neu, P53, and PCNA inendometrioid, serous papillary, and clearcell endometrial adenocarcinomas.Gynecol Oncol 53: 84-92. 1450. Khan MS, Dodson AR, Heatley MK(1999). Ki-67, oestrogen receptor, andprogesterone receptor proteins in thehuman rete ovarii and in endometriosis. JClin Pathol 52: 517-520. 1451. Khoor A, Fleming MV, Purcell CA,Seidman JD, Ashton AH, Weaver DL (1995).Mature teratoma of the uterine cervix withpulmonary differentiation. Arch Pathol LabMed 119: 848-850. 1452. Khoury S, Odeh M, Ophir E, Cohen H,Oettinger M (1997). Uterine metastasisfrom gastric cancer. Acta Obstet GynecolScand 76: 803. 1453. Khunamornpong S, Russell P,Dalrymple JC (1999). Proliferating (LMP)mucinous tumours of the ovaries withmicroinvasion: morphological assessmentof 13 cases. Int J Gynecol Pathol 18: 238-246. 1454. Kiaer H, Nielsen B, Paulsen S,Sorensen IM, Dyreborg U, Blichert-Toft M(1984). Adenomyoepithelial adenosis andlow-grade malignant adenomyoepithe-lioma of the breast. Virchows Arch APathol Anat Histopathol 405: 55-67. 1455. Kiaer W, Holm-Jensen S (1972).Metastases to the uterus. Five cases diag-nosed on the basis of curettings. ActaPathol Microbiol Scand [A] 80: 835-840. 1456. Kido A, Togashi K, Konishi I, KataokaML, Koyama T, Ueda H, Fujii S, Konishi J(1999). Dermoid cysts of the ovary withmalignant transformation: MR appear-ance. AJR Am J Roentgenol 172: 445-449. 1457. Kiechle-Schwarz M, Kommoss F,Schmidt J, Lukovic L, Walz L, Bauknecht T,Pfleiderer A (1992). Cytogenetic analysis ofan adenoid cystic carcinoma of theBartholin's gland. A rare, semimalignanttumor of the female genitourinary tract.Cancer Genet Cytogenet 61: 26-30. 1458. Kikkawa F, Kawai M, Tamakoshi K,Suganuma N, Nakashima N, Furuhashi Y,Kuzuya K, Hattori S, Arii Y, Tomoda Y(1996). Mucinous carcinoma of the ovary.Clinicopathologic analysis. Oncology 5 3 :303-307. 1459. Kim KR, Scully RE (1990). Peritonealkeratin granulomas with carcinomas ofendometrium and ovary and atypical poly-poid adenomyoma of endometrium. A clin -icopathological analysis of 22 cases. Am JSurg Pathol 14: 925-932. 1460. Kim SH, Kim WH, Park KJ, Lee JK,Kim JS (1996). CT and MR findings ofKrukenberg tumors: comparison with pri-mary ovarian tumors. J Comput AssistTomogr 20: 393-398. 1461. Kim YT, Thomas NF, Kessis TD,Wilkinson EJ, Hedrick L, Cho KR (1996). p53mutations and clonality in vulvar carcino-mas and squamous hyperplasias: evidencesuggesting that squamous hyperplasias donot serve as direct precursors of humanpapillomavirus-negative vulvar carcino-mas. Hum Pathol 27: 389-395. 1462. Kindblom LG, Stenman G, Angervall L(1991). Morphological and cytogeneticstudies of angiosarcoma in Stewart-Treves syndrome. Virchows Arch A PatholAnat Histopathol 419: 439-445. 1463. King BF, Enders AC (1993). T h eHuman Yolk Sac and Yolk Sac Tumours.Springer: Berlin.
1464. King MC, Wieand S, Hale K, Lee M,Walsh T, Owens K, Tait J, Ford L, Dunn BK,Costantino J, Wickerham L, Wolmark N,Fisher B (2001). Tamoxifen and breast can-cer incidence among women with inherit-ed mutations in BRCA1 and BRCA2:National Surgical Adjuvant Breast andBowel Project (NSABP-P1) Breast CancerPrevention Trial. JAMA 286: 2251-2256. 1465. King ME, Dickersin GR, Scully RE(1982). Myxoid leiomyosarcoma of theuterus. A report of six cases. Am J SurgPathol 6: 589-598. 1466. King ME, Micha JP, Allen SL,Mouradian JA, Chaganti RS (1985).Immature teratoma of the ovary with pre-dominant malignant retinal anlage compo -nent. A parthenogenically derived tumor.Am J Surg Pathol 9: 221-231. 1467. Kinne DW, Petrek JA, Osborne MP,Fracchia AA, DePalo AA, Rosen PP (1989).Breast carcinoma in situ. Arch Surg 124:33-36. 1468. Kinzler K, Vogelstein B (1998). TheGenetic Basis of Human Cancer. McGrawHill: Toronto.1469. Kirchhoff M, Rose H, Petersen BL,Maahr J, Gerdes T, Lundsteen C, BryndorfT, Kryger-Baggesen N, Christensen L,Engelholm SA, Philip J (1999). Comparativegenomic hybridization reveals a recurrentpattern of chromosomal aberrations insevere dysplasia/carcinoma in situ of thecervix and in advanced-stage cervical car-cinoma. Genes Chromosomes Cancer 24:144-150. 1470. Kister SJ, Sommers SC, HaagensenCD, Cooley E (1966). Reevaluation of bloodvessel invasion and lymphocytic infiltratesni breast carcinoma. Cancer 19: 1213-1216. 1471. Kitchen PR, Smith TH, HendersonMA, Goldhirsch A, Castiglione-Gertsch M,Coates AS, Gusterson B, Brown RW,Gelber RD, Collins JP (2001). Tubular carci-noma of the breast: prognosis andresponse to adjuvant systemic therapy.Aust N Z J Surg 71: 27-31. 1472. Klauber-DeMore N, Tan LK, LibermanL, Kaptain S, Fey J, Borgen P, Heerdt A,Montgomery L, Paglia M, Petrek JA, CodyHS, Van Zee KJ (2000). Sentinel lymphnode biopsy: is it indicated in patients withhigh-risk ductal carcinoma-in-situ andductal carcinoma-in-situ with microinva-sion? Ann Surg Oncol 7: 636-642. 1473. Kleer CG, Giordano TJ, Braun T,Oberman HA (2001). Pathologic, immuno-histochemical, and molecular features ofbenign and malignant phyllodes tumors ofthe breast. Mod Pathol 14: 185-190. 1474. Kleihues P, Cavenee WK (2000).WHO Classification of Tumours. Pathologyand Genetics of Tumours of the NervousSystem. IARC Press: Lyon, France.1475. Kleihues P, Schauble B, zur HausenA, Esteve J, Ohgaki H (1997). Tumors asso-ciated with p53 germline mutations: a syn-opsis of 91 families. Am J Pathol 150: 1-13. 1476. Kleinman GM, Young RH, Scully RE(1993). Primary neuroectodermal tumors ofthe ovary. A report of 25 cases. Am J SurgPathol 17: 764-778. 1 4 7 7 . Klemi PJ, Gronroos M (1979).Endometrioid carcinoma of the ovary. Aclinicopathologic, histochemical, andelectron microscopic study. O b s t e tGynecol 53: 572-579. 1478. Kliewer EV, Smith KR (1995). Breastcancer mortality among immigrants inAustralia and Canada. J Natl Cancer Inst87: 1154-1161.
1479. Kline RC, Wharton JT, Atkinson EN,Burke TW, Gershenson DM, Edwards CL(1990). Endometrioid carcinoma of theovary: retrospective review of 145 cases.Gynecol Oncol 39: 337-346. 1480. Ko SF, Wan YL, Ng SH, Lee TY, LinJW, Chen WJ, Kung FT, Tsai CC (1999).Adult ovarian granulosa cell tumors: spec-trum of sonographic and CT findings withpathologic correlation. AJR Am JRoentgenol 172: 1227-1233. 1481. Kobayashi K, Sagae S, Kudo R, SaitoH, Koi S, Nakamura Y (1995). Microsatelliteinstability in endometrial carcinomas: fre-quent replication errors in tumors of earlyonset and/or of poorly differentiated type.Genes Chromosomes Cancer 14: 128-132. 1481a. Kobayashi Y, Yamazaki K, ShinoharaM, Iwahashi K, Suzuki A, Fujii T, Sasaki H,Shiraishi S (1996). Undifferentiated carci-noma of the broad ligament in a 28-year-old woman--a case report and results ofimmunohistochemical and electron-micro-scopic studies. Gynecol Oncol 63: 382-387. 1482. Kocova L, Skalova A, Fakan F,Rousarova M (1998). Phyllodes tumour ofthe breast: immunohistochemical study of37 tumours using MIB1 antibody. PatholRes Pract 194: 97-104. 1483. Koenig C, Dadmanesh F, BratthauerGL, Tavassoli FA (2000). Carcinoma arisingin microglandular adenosis: an immunohis-tochemical analysis of 20 intraepithelialand invasive neoplasms. Int J Surg Pathol8: 303-315. 1485. Koenig C, Demopoulos RI, VamvakasEC, Mittal KR, Feiner HD, Espiritu EC (1993).Flow cytometric DNA ploidy and quantita-tive histopathology in partial moles. Int JGynecol Pathol 12: 235-240. 1486. Koenig C, Tavassoli FA (1998).Mucinous cystadenocarcinoma of thebreast. Am J Surg Pathol 22: 698-703. 1487. Koenig C, Tavassoli FA (1998).Nodular hyperplasia, adenoma, and ade-nomyoma of Bartholin's gland. Int JGynecol Pathol 17: 289-294. 1488. Koenig C, Turnicky RP, Kankam CF,Tavassoli FA (1997). Papillary squamotran -sitional cell carcinoma of the cervix: areport of 32 cases. Am J Surg Pathol 21:915-921. 1489. Kofinas AD, Suarez J, Calame RJ,Chipeco Z (1984). Chondrosarcoma of theuterus. Gynecol Oncol 19: 231-237. 1490. Kokal WA, Hill LR, Porudominsky D,Beatty JD, Kemeny MM, Riihimaki DU, TerzJJ (1985). Inflammatory breast carcinoma:a distinct entity? J Surg Oncol 30: 152-155. 1491. Kollias J, Ellis IO, Elston CW, BlameyRW (1999). Clinical and histological predic-tors of contralateral breast cancer. Eur JSurg Oncol 25: 584-589. 1492. Kollias J, Ellis IO, Elston CW, BlameyRW (2001). Prognostic significance of syn-chronous and metachronous bilateralbreast cancer. World J Surg 25: 1117-1124. 1 4 9 3 . Kollias J, Elston CW, Ellis IO,Robertson JF, Blamey RW (1997). Early-onset breast cancer--histopathologicaland prognostic considerations. Br JCancer 75: 1318-1323. 1494. Kolodner RD, Hall NR, Lipford J, KaneMF, Morrison PT, Finan PJ, Burn J,Chapman P, Earabino C, Merchant E,Bishop DT. (1995). Structure of the humanMLH1 locus and analysis of a large hered-itary nonpolyposis colorectal carcinomakindred for mlh1 mutations. Cancer Res 55:242-248.
1495. Kolodner RD, Hall NR, Lipford J, KaneMF, Rao MR, Morrison P, Wirth L, Finan PJ,Burn J, Chapman P (1994). Structure of thehuman MSH2 locus and analysis of twoMuir-Torre kindreds for msh2 mutations.Genomics 24: 516-526. 1496. Kolodner RD, Marsischky GT (1999).Eukaryotic DNA mismatch repair. C u r rOpin Genet Dev 9: 89-96. 1497. Kolodner RD, Tytell JD, Schmeits JL,Kane MF, Gupta RD, Weger J, Wahlberg S,Fox EA, Peel D, Ziogas A, Garber JE,Syngal S, Anton-Culver H, Li FP (1999).Germ-line msh6 mutations in colorectalcancer families. Cancer Res 59: 5068-5074. 1498. Komaki K, Sakamoto G, Sugano H,Morimoto T, Monden Y (1988). Mucinouscarcinoma of the breast in Japan. A prog-nostic analysis based on morphologic fea -tures. Cancer 61: 989-996. 1499. Kommoss F, Oliva E, Bhan AK, YoungRH, Scully RE (1998). Inhibin expression inovarian tumors and tumor-like lesions: animmunohistochemical study. Mod Pathol11: 656-664. 1500. Kommoss F, Schmidt M, Merz E,Knapstein PG, Young RH, Scully RE (1999).Ovarian endometrioid-like yolk sac tumortreated by surgery alone, with recurrenceat 12 years. Gynecol Oncol 72: 421-424. 1501. Kondi-Paphitis A, Deligeorgi-Politi H,Liapis A, Plemenou-Frangou M (1998).Human papilloma virus in verrucus carci-noma of the vulva: an immunopathologicalstudy of three cases. Eur J GynaecolOncol 19: 319-320. 1502. Koonings PP, Campbell K, Mishell DRJr., Grimes DA (1989). Relative frequencyof primary ovarian neoplasms: a 10-yearreview. Obstet Gynecol 74: 921-926. 1503. Koontz JI, Soreng AL, Nucci M, KuoFC, Pauwels P, Van den Berghe H, Cin PD,Fletcher JA, Sklar J (2001). Frequent fusionof the JAZF1 and JJAZ1 genes in endome -trial stromal tumors. Proc Natl Acad SciUSA 98: 6348-6353. 1504. Kopolovic J, Weiss DB, Dolberg L,Brezinsky A, Ne'eman Z, Anteby SO (1987).Alveolar soft-part sarcoma of the femalegenital tract. Case report with ultrastruc-tural findings. Arch Gynecol 240: 125-129. 1505. Korn WT, Schatzki SC, DiSciullo AJ,Scully RE (1990). Papillary cystadenoma ofthe broad ligament in von Hippel-Lindaudisease. Am J Obstet Gynecol 163: 596-598. 1506. Kosary CL (1994). FIGO stage, histol-ogy, histologic grade, age and race asprognostic factors in determining survivalfor cancers of the female gynecologicalsystem: an analysis of 1973-87 SEER casesof cancers of the endometrium, cervix,ovary, vulva, and vagina. Semin SurgOncol 10: 31-46. 1507. Koss LG, Brannan CD, Ashikari R(1970). Histologic and ultrastructural fea-tures of adenoid cystic carcinoma of thebreast. Cancer 26: 1271-1279. 1508. Koss LG, Durfee GR (1956). Unusualpatterns of squamous epithelium of theuterine cervix and pathological study ofkaoilocytotic atypia. Ann N Y Acad Sci 63:1245-1261. 1509. Koss LG, ShapiroR.H., Brunschwig A(1965). Endometrial stromal sarcoma. SurgGynecol Obstet 121: 531-537. 1510. Kotlan B, Gruel N, Zafrani B, Furedi G,Foldi J, Petranyi G, Fridman W, Teillaud J(1999). Immunoglobulin variable regionsusage by B-lymphocytes infiltrating ahuman breast medullary carcinoma.Immunology Letters 65: 143-151.

396 References
1511. Kotylo PK, Michael H, Davis TE,Sutton GP, Mark PR, Roth LM (1992). Flowcytometric DNA analysis of placental-sitetrophoblastic tumors. Int J Gynecol Pathol11: 245-252. 1512. Kounelis S, Kapranos N, Kouri E,Coppola D, Papadaki H, Jones MW (2000).Immunohistochemical profile of endome-trial adenocarcinoma: a study of 61 casesand review of the literature. Mod Pathol 13:379-388. 1513. Koutsky LA, Holmes KK, CritchlowCW, Stevens CE, Paavonen J, BeckmannAM, DeRouen TA, Galloway DA, Vernon D,Kiviat NB (1992). A cohort study of the riskof cervical intraepithelial neoplasia grade2 or 3 in relation to papillomavirus infec-tion. N Engl J Med 327: 1272-1278. 1514. Kouvidou C, Karayianni M, Liapi-Avgeri G, Toufexi H, Karaiossifidi H (2000).Old ectopic pregnancy remnants with mor-phological features of placental site nod-ule occurring in fallopian tube and broadligament. Pathol Res Pract 196: 329-332. 1515. Kovi J, Duong HD, Leffall LS Jr.(1981). High-grade mucoepidermoid carci-noma of the breast. Arch Pathol Lab Med105: 612-614. 1516. Koyama M, Kurotaki H, Yagihashi N,Aizawa S, Sugai M, Kamata Y, Oyama T,Yagihashi S (1997). Immunohistochemicalassessment of proliferative activity inmammary adenomyoepithelioma. Histopa-thology 31: 134-139. 1517. Kraemer BB, Silva EG, Sneige N(1984). Fibrosarcoma of ovary. A new com-ponent in the nevoid basal-cell carcinomasyndrome. Am J Surg Pathol 8: 231-236. 1518. Kraggerud SM, Szymanska J, AbelerVM, Kaern J, Eknaes M, Heim S, TeixeiraMR, Trope CG, Peltomaki P, Lothe RA(2000). DNA copy number changes inmalignant ovarian germ cell tumors.Cancer Res 60: 3025-3030. 1 5 1 9 . Krausz T, Jenkins D, Grontoft O,Pollock DJ, Azzopardi JG (1989). Secretorycarcinoma of the breast in adults: empha-sis on late recurrence and metastasis.Histopathology 14: 25-36. 1520. Krieger N, Hiatt RA (1992). Risk ofbreast cancer after benign breast dis-eases. Variation by histologic type, degreeof atypia, age at biopsy, and length of fol-low-up. Am J Epidemiol 135: 619-631. 1521. Krishnamurthy S, Jungbluth AA,Busam KJ, Rosai J (1998). Uterine tumorsresembling ovarian sex-cord tumors havean immunophenotype consistent with truesex-cord differentiation. Am J Surg Pathol22: 1078-1082. 1521 a. Krivak TC, McBroom JW, SundborgMJ, Crothers B, Parker MF (2001). Largecell neuroendocrine cervical carcinoma: areport of two cases and review of the liter-ature. Gynecol Oncol 82: 187-191. 1522. Kubik-Huch RA, Dorffler W, vonSchulthess GK, Marincek B, Kochli OR,Seifert B, Haller U, Steinert HC (2000).Value of (18F)-FDG positron emissiontomography, computed tomography, andmagnetic resonance imaging in diagnosingprimary and recurrent ovarian carcinoma.Eur Radiol 10: 761-767.
1523. Kucera E, Speiser P, Gnant M, SzaboL, Samonigg H, Hausmaninger H, MittlbockM, Fridrik M, Seifert M, Kubista E, Reiner A,Zeillinger R, Jakesz R (1999). Prognosticsignificance of mutations in the p53 gene,particularly in the zinc-binding domains, inlymph node- and steroid receptor positivebreast cancer patients. Austrian BreastCancer Study Group. Eur J Cancer 35: 398-405. 1524. Kucera H, Langer M, Smekal G,Weghaupt K (1985). Radiotherapy of pri-mary carcinoma of the vagina: manage-ment and results of different therapyschemes. Gynecol Oncol 21: 87-93. 1525. Kuijper A, Mommers EC, van der WallE, van Diest PJ (2001). Histopathology offibroadenoma of the breast. Am J ClinPathol 115: 736-742. 1526. Kuiper GG, Enmark E, Pelto-HuikkoM, Nilsson S, Gustafsson JA (1996).Cloning of a novel receptor expressed inrat prostate and ovary. Proc Natl Acad SciUSA 93: 5925-5930. 1527. Kuismanen SA, Moisio AL, SchweizerP, Truninger K, Salovaara R, Arola J,Butzow R, Jiricny J, Nystrom-Lahti M,Peltomaki P (2002). Endometrial and col-orectal tumors from patients with heredi-tary nonpolyposis colon cancer display dif-ferent patterns of microsatellite instability.Am J Pathol 160: 1953-1958. 1528. Kulski JK, Demeter T, Rakoczy P,Sterrett GF, Pixley EC (1989). Human papil-lomavirus coinfections of the vulva anduterine cervix. J Med Virol 27: 244-251. 1529. Kumar A, Schneider V (1983).Metastases to the uterus from extrapelvicprimary tumors. Int J Gynecol Pathol 2:134-140. 1530. Kumar L, Pokharel YH, Dawar R,Thulkar S (1999). Cervical cancer metasta -tic to the breast: a case report and reviewof the literature. Clin Oncol (R Coll Radiol )11: 414-416. 1531. Kumar NB, Hart WR (1982).Metastases to the uterine corpus fromextragenital cancers. A clinicopathologicstudy of 63 cases. Cancer 50: 2163-2169. 1532. Kupets R, Covens A (2001). Is theInternational Federation of Gynecologyand Obstetrics staging system for cervicalcarcinoma able to predict survival inpatients with cervical carcinoma?: anassessment of clinimetric properties.Cancer 92: 796-804. 1533. Kupryjanczyk J, Kujawa M (1992).Signet-ring cells in squamous cell carcino-ma of the cervix and in non-neoplasticectocervical epithelium. Int J GynecolCancer 2: 152-156. 1534. Kurian K, al Nafussi A (1999). Relationof cervical glandular intraepithelial neo-plasia to microinvasive and invasive ade-nocarcinoma of the uterine cervix: a studyof 121 cases. J Clin Pathol 52: 112-117. 1535. Kurman RJ, Kaminski PF, Norris HJ(1985). The behavior of endometrial hyper-plasia. A long-term study of "untreated"hyperplasia in 170 patients. Cancer 56: 403-412. 1536. Kurman RJ, Norris HJ (1976).Embryonal carcinoma of the ovary: a clini-copathologic entity distinct from endoder-mal sinus tumor resembling embryonalcarcinoma of the adult testis. Cancer 38:2420-2433. 1537. Kurman RJ, Norris HJ (1976).Endodermal sinus tumor of the ovary: aclinical and pathologic analysis of 71cases. Cancer 38: 2404-2419.
1538. Kurman RJ, Norris HJ (1976).Mesenchymal tumors of the uterus. VI.Epithelioid smooth muscle tumors includ-ing leiomyoblastoma and clear-cell leiomy-oma: a clinical and pathologic analysis of26 cases. Cancer 37: 1853-1865. 1539. Kurman RJ, Norris HJ, Wilkinson E(1992). Tumours of the cervix, vagina, andvulva. In: Atlas of Tumour Pathology, AFIP,ed., AFIP: Washington,DC .1540. Kurman RJ, Scully RE, Norris HJ(1976). Trophoblastic pseudotumor of theuterus: an exaggerated form of "syncytialendometritis" simulating a malignanttumor. Cancer 38: 1214-1226. 1541. Kurman RJ, Toki T, Schiffman MH(1993). Basaloid and warty carcinomas ofthe vulva. Distinctive types of squamouscell carcinoma frequently associated withhuman papillomaviruses. Am J SurgPathol 17: 133-145. 1542. Kurman RJ, Trimble CL (1993). Thebehavior of serous tumors of low malig-nant potential: are they ever malignant? IntJ Gynecol Pathol 12: 120-127. 1543. Kurman RJ, Young RH, Norris HJ,Main CS, Lawrence WD, Scully RE (1984).Immunocytochemical localization of pla-cental lactogen and chorionicgonadotropin in the normal placenta andtrophoblastic tumors, with emphasis onintermediate trophoblast and the placentalsite trophoblastic tumor. Int J GynecolPathol 3: 101-121. 1544. Kuroda N, Hirano K,Inui Y, Yamasaki Y, Toi M, Nakayama H,Hiroi M, Enzan H (2001). Compoundmelanocytic nevus arising in a mature cys-tic teratoma of the ovary. Pathol Int 51: 902-904. 1545. Kurose K, Hoshaw-Woodard S,Adeyinka A, Lemeshow S, Watson PH, EngC (2001). Genetic model of multi-stepbreast carcinogenesis involving theepithelium and stroma: clues to tumour-microenvironment interactions. Hum MolGenet 10: 1907-1913. 1546. Kurosumi M, Ishida T, Kurebayashi J,Kawai T, Joshita T, Honjo T, Izuo M (1988).Lipid-secreting mammary carcinoma: alight and electon microscopic investiga-tion. J Clin Electron Microscopy 21: 147-156. 1547. Kushner BH, LaQuaglia MP, WollnerN, Meyers PA, Lindsley KL, Ghavimi F,Merchant TE, Boulad F, Cheung NK,Bonilla MA, Crouch G, Kelleher JF Jr.,Steinherz PG, Gerald WL (1996).Desmoplastic small round-cell tumor: pro-longed progression-free survival withaggressive multimodality therapy. J ClinOncol 14: 1526-1531. 1548. Kuukasjarvi T, Tanner M, PennanenS, Karhu R, Kallioniemi OP, Isola J (1997).Genetic changes in intraductal breast can-cer detected by comparative genomichybridization. Am J Pathol 150: 1465-1471. 1549. Kuwabara H, Uda H (1997). Clear cellmammary malignant myoepithelioma withabundant glycogens. J Clin Pathol 50: 700-702. 1550. Kwiatkowska E, Teresiak M,Lamperska KM, Karczewska A,Breborowicz D, Stawicka M, Godlewski D,Krzyzosiak WJ, Mackiewicz A (2001).BRCA2 germline mutations in male breastcancer patients in the Polish population.Hum Mutat 17: 73. 1551. La Vecchia C, Levi F, Lucchini F(1992). Descriptive epidemiology of malebreast cancer in Europe. Int J Cancer 51:62-66.
1551 a. La Vecchia C, Parazzini F,Franceschi S, Decarli A (1985). Risk factorsfor benign breast disease and their relationwith breast cancer risk. Pooled informa-tion from epidemiologic studies. Tumori 71:167-178. 1552. Laake K, Launonen V, Niederacher D,Gudlaugsdottir S, Seitz S, Rio P,Champeme MH, Bieche I, Birnbaum D,White G, Sztan M, Sever N, Plummer S,Osorio A, Broeks A, Huusko P, Spurr N,Borg A, Cleton-Jansen AM, van't Veer L,Benitez J, Casey G, Peterlin B, Olah E,Varley J, Bignon YJ, Scherneck S,Sigurdardottir V, Lidereau R, Eyfjord J,Beckmann MW, Winqvist R, Skovlund E,Borresen-Dale AL. (1999). Loss of het-erozygosity at 11q23.1 and survival inbreast cancer: results of a large Europeanstudy. Breast Cancer Somatic GeneticsConsortium. Genes Chromosomes Cancer25: 212-221. 1553. Laake K, Odegard A, Andersen TI,Bukholm IK, Karesen R, Nesland JM,Ottestad L, Shiloh Y, Borresen-Dale AL(1997). Loss of heterozygosity at 11q23.1 inbreast carcinomas: indication for involve-ment of a gene distal and close to ATM.Genes Chromosomes Cancer 18: 175-180. 1554. Labonte S, Tetu B, Boucher D, LarueH (2001). Transitional cell carcinoma of theendometrium associated with a benignovarian Brenner tumor: a case report. HumPathol 32: 230-232. 1555. Lack EE, Goldstein DP (1984). Primaryovarian tumours in childhood and adoles-cence. Current Probl Obstet Gynecol 7: 9-36. 1556. Lacson AG, Gillis DA, Shawwa A(1988). Malignant mixed germ-cell-sexcord-stromal tumors of the ovary associat-ed with isosexual precocious puberty.Cancer 61: 2122-2133. 1557. Lage JM (1991). Placentomegaly withmassive hydrops of placental stem villi,diploid DNA content, and fetal omphaloce-les: possible association with Beckwith-Wiedemann syndrome. Hum Pathol 2 2 :591-597. 1558. Lage JM, Berkowitz RS, Rice LW,Goldstein DP, Bernstein MR, Weinberg DS(1991). Flow cytometric analysis of DNAcontent in partial hydatidiform moles withpersistent gestational trophoblastic tumor.Obstet Gynecol 77: 111-115. 1559. Lage JM, Driscoll SG, Yavner DL,Olivier AP, Mark SD, Weinberg DS (1988).Hydatidiform moles. Application of flowcytometry in diagnosis. Am J Clin Pathol89: 596-600. 1560. Lage JM, Mark SD, Roberts DJ,Goldstein DP, Bernstein MR, Berkowitz RS(1992). A flow cytometric study of 137 freshhydropic placentas: correlation betweentypes of hydatidiform moles and nuclearDNA ploidy. Obstet Gynecol 79: 403-410. 1561. Lage JM, Popek EJ (1993). The role ofDNA flow cytometry in evaluation of partialand complete hydatidiform moles andhydropic abortions. Semin Diagn Pathol 10:267-274. 1562. Lage JM, Roberts DJ (1993).Choriocarcinoma in a term placenta:pathologic diagnosis of tumor in an asymp-tomatic patient with metastatic disease.Int J Gynecol Pathol 12: 80-85. 1563. Lage JM, Weinberg DS, Yavner DL,Bieber FR (1989). The biology of tetraploidhydatidiform moles: histopathology, cyto-genetics, and flow cytometry. Hum Pathol20: 419-425.

397References
1564. Lagios MD (1977). Multicentricity ofbreast carcinoma demonstrated by routinecorrelated serial subgross and radiograph-ic examination. Cancer 40: 1726-1734. 1565. Lagios MD, Margolin FR, WestdahlPR, Rose MR (1989). Mammographicallydetected duct carcinoma in situ.Frequency of local recurrence followingtylectomy and prognostic effect of nucleargrade on local recurrence. Cancer 63: 618-624. 1566. Lagios MD, Rose MR, Margolin FR(1980). Tubular carcinoma of the breast:association with multicentricity, bilaterali-ty, and family history of mammary carcino-ma. Am J Clin Pathol 73: 25-30. 1567. Lakhani SR (1999). The transition fromhyperplasia to invasive carcinoma of thebreast. J Pathol 187: 272-278. 1568. Lakhani SR, Chaggar R, Davies S,Jones C, Collins N, Odel C, Stratton MR,O'Hare MJ (1999). Genetic alterations in'normal' luminal and myoepithelial cells ofthe breast. J Pathol 189: 496-503. 1569. Lakhani SR, Collins N, Sloane JP,Stratton MR (1995). Loss of heterozygosityin lobular carcinoma in situ of the breast.Jounal of Clinical Pathology:MolecularPathology 48: M74-M78. 1570. Lakhani SR, Collins N, Stratton MR,Sloane JP (1995). Atypical ductal hyperpla-sia of the breast: clonal proliferation withloss of heterozygosity on chromosomes16q and 17p. J Clin Pathol 48: 611-615. 1571. Lakhani SR, Gusterson BA,Jacquemier J, Sloane JP, Anderson TJ,Van de Vijver MJ, Venter D, Freeman A,Antoniou A, McGuffog L, Smyth E, SteelCM, Haites N, Scott RJ, Goldgar D,Neuhausen S, Daly PA, Ormiston W,McManus R, Scherneck S, Ponder BA,Futreal PA, Peto J, Stoppa-Lyonnet D,Bignon YJ, Stratton MR (2000). The pathol -ogy of familial breast cancer: histologicalfeatures of cancers in families not attribut-able to mutations in BRCA1 or BRCA2. ClinCancer Res 6: 782-789. 1572. Lakhani SR, Jacquemier J, SloaneJP, Gusterson BA, Anderson TJ, Van deVijver MJ, Farid LM, Venter D, Antoniou A,Storfer-Isser A, Smyth E, Steel CM, HaitesN, Scott RJ, Goldgar D, Neuhausen S, DalyPA, Ormiston W, McManus R, ScherneckS, Ponder BA, Ford D, Peto J, Stoppa-Lyonnet D, Bignon YJ, Struewing JP, SpurrNK, Bishop DT, Klijn JGM, Devilee P,Cornelisse CJ, Lasset C, Lenoir G,Barkardottir RB, Egilsson V, Hamann U,Chang-claude J, Sobol H, Weber B,Stratton MR, Easton DF. (1998).Multifactorial analysis of differencesbetween sporadic breast cancers andcancers involving BRCA1 and BRCA2mutations. J Natl Cancer Inst 90: 1138-1145. 1573. Lakhani SR, O'Hare MJ, MonaghanP, Winehouse J, Gazet JC, Sloane JP(1995). Malignant myoepithelioma (myoep -ithelial carcinoma) of the breast: a detailedcytokeratin study. J Clin Pathol 48: 164-167. 1574. Lakhani SR, Van de Vijver MJ,Jacquemier J, Anderson TJ, Osin PP,McGuffog L, Easton DF (2002). The pathol-ogy of familial breast cancer: predictivevalue of immunohistochemical markersestrogen receptor, progesterone receptor,HER-2, and p53 in patients with mutationsin BRCA1 and BRCA2. J Clin Oncol 20:2310-2318.
1575. Lam RM, Geittmann P (1988).Sclerosing stromal tumor of the ovary. Alight, electron microscopic and enzymehistochemical study. Int J Gynecol Pathol7: 280-290. 1576. Lambot MA, Eddafali B, Simon P, FaytI, Noel JC (2001). Metastasis from apocrinecarcinoma of the breast to an endometrialpolyp. Virchows Arch 438: 517-518. 1577. Lammie GA, Millis RR (1989). Ductaladenoma of the breast--a review of fifteencases. Hum Pathol 20: 903-908. 1578. Lamovec J, Bracko M (1991).Metastatic pattern of infiltrating lobularcarcinoma of the breast: an autopsy study.J Surg Oncol 48: 28-33. 1579. Lamovec J, Bracko M (1994).Secretory carcinoma of the breast: lightmicroscopical, immunohistochemical andflow cytometric study. Mod Pathol 7: 475-479. 1580. Lamovec J, Jancar J (1987). Primarymalignant lymphoma of the breast.Lymphoma of the mucosa-associated lym -phoid tissue. Cancer 60: 3033-3041. 1581. Lamovec J, Us-Krasovec M, Zidar A,Kljun A (1989). Adenoid cystic carcinomaof the breast: a histologic, cytologic, andimmunohistochemical study. Semin DiagnPathol 6: 153-164. 1582. Lane TF, Deng C, Elson A, Lyu MS,Kozak CA, Leder P (1995). Expression ofBrca1 is associated with terminal differen-tiation of ectodermally and mesodermallyderived tissues in mice. Genes Dev 9: 2712-2722. 1583. Laricchia R, Wierdis T, Loiudice L,Trisolini A, Riezzo A (1977). [Vulvar neo-plasms (myeloblastoma) as the first mani-festation of acute myeloblastic leukemia].Minerva Ginecol 29: 957-961. 1584. Larson AA, Liao SY, Stanbridge EJ,Cavenee WK, Hampton GM (1997). Geneticalterations accumulate during cervicaltumorigenesis and indicate a common ori-gin for multifocal lesions. Cancer Res 57:4171-4176. 1585. Larson B, Silfversward C, Nilsson B,Pettersson F (1990). Prognostic factors inuterine leiomyosarcoma. A clinical andhistopathological study of 143 cases. TheRadiumhemmet series 1936-1981. A c t aOncol 29: 185-191. 1586. Larson PS, de lasMA, Cupples LA, Huang K, Rosenberg CL(1998). Genetically abnormal clones in his-tologically normal breast tissue. Am JPathol 152: 1591-1598. 1587. Lash RH, Hart WR (1987). Intestinaladenocarcinomas metastatic to theovaries. A clinicopathologic evaluation of22 cases. Am J Surg Pathol 11: 114-121.1588. Lathrop JC (1967). Malignant pelviclymphomas. Obstet Gynecol 30: 137-145. 1589. Lathrop JC, Lauchlan S, Nayak R,Ambler M (1988). Clinical characteristics ofplacental site trophoblastic tumor (PSTT).Gynecol Oncol 31: 32-42. 1590. Lauchlan SC (1981). Tubal (serous)carcinoma of the endometrium. A r c hPathol Lab Med 105: 615-618. 1591. Laufer MR, Heerema AE, Parsons KE,Barbieri RL (1998). Endosalpingiosis: clini-cal presentation and follow-up. GynecolObstet Invest 46: 195-198. 1592. Lauria R, Perrone F, Carlomagno C,De Laurentiis M, Morabito A, Gallo C,Varriale E, Pettinato G, Panico L, PetrellaG, Bianco AR, Deplacido S. (1995). Theprognostic value of lymphatic and bloodvessel invasion in operable breast cancer.Cancer 76: 1772-1778.
1593. Lawler SD, Fisher RA, Dent J (1991). Aprospective genetic study of complete andpartial hydatidiform moles. Am J ObstetGynecol 164: 1270-1277. 1594. Lax SF, Kendall B, Tashiro H, SlebosRJ, Hedrick L (2000). The frequency of p53,K-ras mutations, and microsatellite insta-bility differs in uterine endometrioid andserous carcinoma: evidence of distinctmolecular genetic pathways. Cancer 88:814-824. 1595. Lax SF, Pizer ES, Ronnett BM,Kurman RJ (1998). Clear cell carcinoma ofthe endometrium is characterized by a dis-tinctive profile of p53, Ki-67, estrogen, andprogesterone receptor expression. H u mPathol 29: 551-558. 1596. Layfield LJ, Hart J, Neuwirth H,Bohman R, Trumbull WE, Giuliano AE(1989). Relation between DNA ploidy andthe clinical behavior of phyllodes tumors.Cancer 64: 1486-1489. 1597. Lazure T, Alsamad IA, Meuric S,Orbach D, Fabre M (2001). [Primary uterineand vulvar Ewing's sarcoma/peripheralneuroectodermal tumors in children: twounusual locations]. Ann Pathol 21: 263-266. 1598. Le Bouedec G, de Latour M, Levrel O,Dauplat J (1997). [Krukenberg tumors ofbreast origin. 10 cases]. Presse Med 26:454-457. 1599. Le Gal M, Ollivier L, Asselain B,Meunier M, Laurent M, Vielh P,Neuenschwander S (1992). Mammo-graphic features of 455 invasive lobularcarcinomas. Radiology 185: 705-708. 1600. Le Gal Y (1961). Adenoma of theBreast. Am Surg 27: 14-22. 1601. Le Doussal V, Tubiana-Hulin M,Friedman S, Hacene K, Spyratos F, BrunetM (1989). Prognostic value of histologicgrade nuclear components of Scarff-Bloom-Richardson (SBR). An improvedscore modification based on a multivariateanalysis of 1262 invasive ductal breast car-cinomas. Cancer 64: 1914-1921. 1602. Leach FS, Polyak K, Burrell M,Johnson KA, Hill D, Dunlop MG, Wyllie AH,Peltomaki P, de la CA, Hamilton SR, KinzlerKW, Vogelstein B (1996). Expression of thehuman mismatch repair gene hMSH2 innormal and neoplastic tissues. Cancer Res56: 235-240. 1603. Leake J, Woolas RP, Daniel J, OramDH, Brown CL (1994). Immunocytochemicaland serological expression of CA 125: aclinicopathological study of 40 malignantovarian epithelial tumours. Histopathology24: 57-64. 1604. Leal C, Costa I, Fonseca D, Lopes P,Bento MJ, Lopes C (1998). Intracystic(encysted) papillary carcinoma of thebreast: a clinical, pathological, andimmunohistochemical study. Hum Pathol29: 1097-1104. 1605. Leal C, Henrique R, Monteiro P, LopesC, Bento MJ, De Sousa CP, Lopes P, OlsonS, Silva MD, Page DL (2001). Apocrine duc-tal carcinoma in situ of the breast: histo-logic classification and expression of bio-logic markers. Hum Pathol 32: 487-493. 1606. Lee A.K.C., Loda M, Mackarem G,Bosari S., DeLellis R.A., Heatley G.J.,Hughes K. (1997). Lymph node negativeinvasive breast carcinoma 1 centimeter orless in size: clinicopathological featuresand outcome. Cancer 79: 761-771. 1607. Lee BJ, Tannenbaum E (1924).Inflammatory carcinoma of the breast: areport of twenty-eight cases from thebreast clinic of the Memorial Hospital.Surg Gynecol Obstet 39: 580-595.
1608. Lee JF, Yang YC, Lee YN, Wang KL,Lin YN (1991). Leiomyosarcoma of thebroad ligament--report of two cases.Zhonghua Yi Xue Za Zhi (Taipei) 48: 59-65. 1609. Lee JS, Collins KM, Brown AL, LeeCH, Chung JH (2000). hCds1-mediatedphosphorylation of BRCA1 regulates theDNA damage response. Nature 404: 201-204. 1610. Lee JY, Dong SM, Kim HS, Kim SY, NaEY, Shin MS, Lee SH, Park WS, Kim KM,Lee YS, Jang JJ, Yoo NJ (1998). A distinctregion of chromosome 19p13.3 associatedwith the sporadic form of adenomamalignum of the uterine cervix.Cancer Res58: 1140-1143. 1611. Lee KR, Flynn CE (2000). Early inva-sive adenocarcinoma of the cervix.Cancer 89: 1048-1055. 1612. Lee KR, Minter LJ, Crum CP (1997).Koilocytotic atypia in Papanicolaousmears. Reproducibility and biopsy corre-lations. Cancer 81: 10-15. 1613. Lee KR, Scully RE (2000). Mucinoustumors of the ovary: a clinicopathologicstudy of 196 borderline tumors (of intestin-al type) and carcinomas, including an eval-uation of 11 cases with 'pseudomyxomaperitonei'. Am J Surg Pathol 24: 1447-1464. 1614. Lee KR, Young RH (2003). The distinc-tion between primary and metastatic muci-nous carcinomas of the ovary: gross andhistologic findings in 50 cases. Am J SurgPathol 27: 281-292. 1615. Lee WL, Wang PH (2001). Torsion ofbenign serous cystadenoma of the fallopi-an tube: a challenge in differential diagno-sis of abdominal pain in women duringtheir childbearing years--a case report.Kaohsiung J Med Sci 17: 270-273. 1616. Lee YS (1995). p53 expression in ges -tational trophoblastic disease. Int JGynecol Pathol 14: 119-124. 1617. Leeper K, Garcia R, Swisher E, Goff B,Greer B, Paley P (2002). Pathologic findingsin prophylactic oophorectomy specimensin high-risk women. Gynecol Oncol 87: 52-56. 1618. Lefkowitz M, Lefkowitz W, WargotzES (1994). Intraductal (intracystic) papillarycarcinoma of the breast and its variants: aclinicopathological study of 77 cases. HumPathol 25: 802-809. 1619. Lehman MB, Hart WR (2001). Simpleand complex hyperplastic papillary prolif-erations of the endometrium: a clinico-pathologic study of nine cases of appar-ently localized papillary lesions withfibrovascular stromal cores and epithelialmetaplasia. Am J Surg Pathol 25: 1347-1354. 1620. Leiberman J, Chaim W, Cohen A,Czernobilsky B (1975). Primary carcinomaof stomach with uterine metastasis. Br JObstet Gynaecol 82: 917-921. 1621. Leibowitch M, Neill S, Pelisse M,Moyal-Baracco M (1990). The epithelialchanges associated with squamous cellcarcinoma of the vulva: a review of theclinical, histological and viral findings in 78women. Br J Obstet Gynaecol 97: 1135-1139. 1622. Leibsohn S, d'Ablaing G, Mishell DRJr., Schlaerth JB (1990). Leiomyosarcomain a series of hysterectomies performed forpresumed uterine leiomyomas. Am JObstet Gynecol 162: 968-974. 1623. Leitner SP, Swern AS, Weinberger D,Duncan LJ, Hutter RV (1995). Predictors ofrecurrence for patients with small (onecentimeter or less) localized breast cancer(T1a,b N0 M0). Cancer 76: 2266-2274.

398 References
1624. Lele SB, Piver MS, Barlow JJ,Tsukada Y (1978). Squamous cell carcino-ma arising in ovarian endometriosis.Gynecol Oncol 6: 290-293. 1625. Lemoine NR, Hall PA (1986). Epithelialtumors metastatic to the uterine cervix. Astudy of 33 cases and review of the litera-ture. Cancer 57: 2002-2005. 1626. Lenehan PM, Meffe F, Lickrish GM(1986). Vaginal intraepithelial neoplasia:biologic aspects and management. ObstetGynecol 68: 333-337. 1627. Lenfant-Pejovic MH, Mlika-CabanneN, Bouchardy C, Auquier A (1990). Risk fac-tors for male breast cancer: a Franco-Swiss case-control study. Int J Cancer 45:661-665. 1628. Leoncini L (1980). [Brenner tumor ofthe broad ligament]. Arch De Vecchi AnatPatol 64: 97-102. 1629. Leong AS, Williams JA (1985).Mucoepidermoid carcinoma of the breast:high grade variant. Pathology 17: 516-521. 1630. Leppien G (1987). Non-uterine gyne-cological sarcomas. Arch Gynecol Obstet241: 25-32. 1631. Lerner LB, Andrews SJ, Gonzalez JL,Heaney JA, Currie JL (1999). Vulvar metas-tases secondary to transitional cell carci-noma of the bladder. A case report. JReprod Med 44: 729-732. 1632. Lesser ML, Rosen PP, Kinne DW(1982). Multicentricity and bilaterality ininvasive breast carcinoma. Surgery 91:234-240. 1633. Lesueur GC, Brown RW, Bhathal PS(1983). Incidence of perilobular heman-gioma in the female breast. Arch PatholLab Med 107: 308-310. 1634. Leuchter RS, Hacker NF, Voet RL,Berek JS, Townsend DE, Lagasse LD(1982). Primary carcinoma of the Bartholingland: a report of 14 cases and review ofthe literature. Obstet Gynecol 60: 361-368. 1635. Leung WY, Schwartz PE, Ng HT,Yang-Feng TL (1990). Trisomy 12 in benignfibroma and granulosa cell tumor of theovary. Gynecol Oncol 38: 28-31. 1636. Levi F, La Vecchia C, Gulie C, Negri E(1993). Dietary factors and breast cancerrisk in Vaud, Switzerland. Nutr Cancer 19:327-335. 1637. Levi F, Lucchini F, Negri E, Boyle P, LaVecchia C (1999). Cancer mortality inEurope, 1990-1994, and an overview oftrends from 1955 to 1994. Eur J Cancer 35:1477-1516. 1638. Levi F, Lucchini F, Negri E, FranceschiS, La Vecchia C (2000). Cervical cancermortality in young women in Europe: pat-terns and trends. Eur J Cancer 36: 2266-2271. 1639. Levi F, Pasche C, Lucchini F, LaVecchia C (2001). Dietary intake of select-ed micronutrients and breast-cancer risk.Int J Cancer 91: 260-263. 1640. Levi F, Randimbison L, Te VC, LaVecchia C (1994). Incidence of breast can -cer in women with fibroadenoma. Int JCancer 57: 681-683. 1641. Levine PH, Steinhorn SC, Ries LG,Aron JL (1985). Inflammatory breast can-cer: the experience of the surveillance,epidemiology, and end results (SEER) pro-gram. J Natl Cancer Inst 74: 291-297. 1642. Levine RL, Cargile CB, Blazes MS,van Rees B, Kurman RJ, Ellenson LH (1998).PTEN mutations and microsatellite insta-bility in complex atypical hyperplasia, aprecursor lesion to uterine endometrioidcarcinoma. Cancer Res 58: 3254-3258.
1643. Levrero M, De Laurenzi V, CostanzoA, Gong J, Wang JY, Melino G (2000). Thep53/p63/p73 family of transcription factors:overlapping and distinct functions. J CellSci 113: 1661-1670. 1644. Levy-Lahad E, Lahad A, Eisenberg S,Dagan E, Paperna T, Kasinetz L, Catane R,Kaufman B, Beller U, Renbaum P,Gershoni-Baruch R (2001). A singlenucleotide polymorphism in the RAD51gene modifies cancer risk in BRCA2 butnot BRCA1 carriers. Proc Natl Acad SciUSA 98: 3232-3236. 1645. Lew WY (1993). Spindle cell lipoma ofthe breast: a case report and literaturereview. Diagn Cytopathol 9: 434-437. 1646. Lewis TL (1971). Colloid (mucussecreting) carcinoma of the cervix. JObstet Gynaecol Br Commonw 78: 1128-1132. 1647. Li CI, Anderson BO, Porter P, Holt SK,Daling JR, Moe RE (2000). Changing inci-dence rate of invasive lobular breast carci-noma among older women. Cancer 8 8 :2561-2569. 1648. Li CI, Weiss NS, Stanford JL, DalingJR (2000). Hormone replacement therapyin relation to risk of lobular and ductalbreast carcinoma in middle-aged women.Cancer 88: 2570-2577. 1649. Li DM, Sun H (1997). TEP1, encodedby a candidate tumor suppressor locus, isa novel protein tyrosine phosphatase regu-lated by transforming growth factor beta.Cancer Res 57: 2124-2129. 1650. Li FP, Fraumeni JF Jr., Mulvihill JJ,Blattner WA, Dreyfus MG, Tucker MA,Miller RW (1988). A cancer family syn-drome in twenty-four kindreds. Cancer Res48: 5358-5362. 1651. Li J, Yen C, Liaw D, Podsypanina K,Bose S, Wang SI, Puc J, Miliaresis C,Rodgers L, McCombie R, Bigner SH,Giovanella BC, Ittmann M, Tycko B,Hibshoosh H, Wigler MH, Parsons R (1997).PTEN, a putative protein tyrosine phos-phatase gene mutated in human brain,breast, and prostate cancer. Science 275:1943-1947. 1652. Li S, Zimmerman RL, LiVolsi VA (1999).Mixed malignant germ cell tumor of the fal-lopian tube. Int J Gynecol Pathol 18: 183-185. 1653. Liang SB, Sonobe H, Taguchi T,Takeuchi T, Furihata M, Yuri K, Ohtsuki Y(2001). Tetrasomy 12 in ovarian tumors ofthecoma-fibroma group: A fluorescence insitu hybridization analysis using paraffinsections. Pathol Int 51: 37-42. 1654. Liaw D, Marsh DJ, Li J, Dahia PL,Wang SI, Zheng Z, Bose S, Call KM, TsouHC, Peacocke M, Eng C, Parsons R (1997).Germline mutations of the PTEN gene inCowden disease, an inherited breast andthyroid cancer syndrome. Nat Genet 16:64-67. 1655. Liberman L (2000). Pathologic analy-sis of sentinel lymph nodes in breast carci-noma. Cancer 88: 971-977. 1656. Liberman L, Dershaw DD, KaufmanRJ, Rosen PP (1992). Angiosarcoma of thebreast. Radiology 183: 649-654. 1657. Liberman L, Giess CS, Dershaw DD,Louie DC, Deutch BM (1994). Non-Hodgkinlymphoma of the breast: imaging charac-teristics and correlation with histopatho-logic findings. Radiology 192: 157-160.
1658. Lichtenstein P, Holm NV, VerkasaloPK, Iliadou A, Kaprio J, Koskenvuo M,Pukkala E, Skytthe A, Hemminki K (2000).Environmental and heritable factors in thecausation of cancer--analyses of cohortsof twins from Sweden, Denmark, andFinland. N Engl J Med 343: 78-85. 1659. Lie AK, Skarsvag S, Skomedal H,Haugen OA, Holm R (1999). Expression ofp53, MDM2, and p21 proteins in high-gradecervical intraepithelial neoplasia and rela -tionship to human papillomavirus infection.Int J Gynecol Pathol 18: 5-11. 1660. Lifschitz-Mercer B, Walt H, Kushnir I,Jacob N, Diener PA, Moll R, Czernobilsky B(1995). Differentiation potential of ovariandysgerminoma: an immunohistochemicalstudy of 15 cases. Hum Pathol 26: 62-66. 1661. Lillemoe TJ, Perrone T, Norris HJ,Dehner LP (1991). Myogenous phenotypeof epithelial-like areas in endometrial stro-mal sarcomas. Arch Pathol Lab Med 115:215-219. 1662. Lim CL, Walker MJ, Mehta RR, DasGupta TK (1986). Estrogen and antiestro-gen binding sites in desmoid tumors. Eur JCancer Clin Oncol 22: 583-587. 1663. Lin MC, Mutter GL, Trivijisilp P,Boynton KA, Sun D, Crum CP (1998).Patterns of allelic loss (LOH) in vulvarsquamous carcinomas and adjacent non-invasive epithelia. Am J Pathol 152: 1313-1318. 1664. Lin WM, Forgacs E, Warshal DP, YehIT, Martin JS, Ashfaq R, Muller CY (1998).Loss of heterozygosity and mutationalanalysis of the PTEN/MMAC1 gene in syn -chronous endometrial and ovarian carci-nomas. Clin Cancer Res 4: 2577-2583. 1665. Lin Y, Govindan R, Hess JL (1997).Malignant hematopoietic breast tumors.Am J Clin Pathol 107: 177-186. 1666. Lindblom A, Tannergard P, WereliusB, Nordenskjold M (1993). Genetic map-ping of a second locus predisposing tohereditary non-polyposis colon cancer.Nat Genet 5: 279-282. 1667. Linder D, Power J (1970). Further evi -dence for post-meiotic origin of teratomasin the human female. Ann Hum Genet 34:21-30. 1668. Linell F, Ljungberg O, Andersson I(1980). Breast carcinoma. Aspects of earlystages, progression and related problems.Acta Pathol Microbiol Scand Suppl 1-233. 1669. Lininger RA, Ashfaq R, Albores-Saavedra J, Tavassoli FA (1997).Transitional cell carcinoma of theendometrium and endometrial carcinomawith transitional cell differentiation.Cancer 79: 1933-1943. 1670. Lininger RA, Fujii H, Man YG,Gabrielson E, Tavassoli FA (1998).Comparison of loss heterozygosity in pri-mary and recurrent ductal carcinoma insitu of the breast. Mod Pathol 11: 1151-1159. 1671. Lininger RA, Park WS, Man YG, PhamT, MacGrogan G, Zhuang Z, Tavassoli FA(1998). LOH at 16p13 is a novel chromoso-mal alteration detected in benign andmalignant microdissected papillary neo-plasms of the breast. Hum Pathol 29: 1113-1118. 1672. Lininger RA, Wistuba I, Gazdar A,Koenig C, Tavassoli FA, Albores-SaavedraJ (1998). Human papillomavirus type 16 isdetected in transitional cell carcinomasand squamotransitional cell carcinomas ofthe cervix and endometrium. Cancer 83:521-527.
1673. Lininger RA, Zhuang Z, Man Y, ParkWS, Emmert-Buck M, Tavassoli FA (1999).Loss of heterozygosity is detected at chro-mosomes 1p35-36 (NB), 3p25 (VHL), 16p13(TSC2/PKD1), and 17p13 (TP53) in microdis-sected apocrine carcinomas of the breast.Mod Pathol 12: 1083-1089. 1674. Lipkin SM, Wang V, Jacoby R,Banerjee-Basu S, Baxevanis AD, LynchHT, Elliott RM, Collins FS (2000). MLH3: aDNA mismatch repair gene associatedwith mammalian microsatellite instability.Nat Genet 24: 27-35. 1675. Lipper S, Wilson C, Copeland KC(1981). Pseudogynecomastia due to neu-rofibromatosis: a light microscopic andultrastructural study. Hum Pathol 12: 755-759. 1676. Lipworth L, Hsieh CC, Wide L, EkbomA, Yu SZ, Yu GP, Xu B, Hellerstein S,Carlstrom K, Trichopoulos D, Adami HO(1999). Maternal pregnancy hormone lev-els in an area with a high incidence(Boston, USA) and in an area with a lowincidence (Shanghai, China) of breast can-cer. Br J Cancer 79: 7-12. 1677. Lissoni A, Cormio G, Perego P,Gabriele A, Cantu MG, Bratina G (1997).Conservative management of endometrialstromal sarcoma en young women. Int JGynecol Cancer 7: 364-367. 1678. Little MP, Boice JDJ (1999).Comparison of breast cancer incidence inthe Massachusetts tuberculosis fluo-roscopy cohort and in the Japanese atom-ic bomb survivors. Radiat Res 151: 218-224. 1679. Liu B, Nicolaides NC, Markowitz S,Willson JK, Parsons RE, Jen J,Papadopolous N, Peltomaki P, de laChapelle A, Hamilton SR, Kinzler KW,Vogelstein B (1995). Mismatch repair genedefects in sporadic colorectal cancerswith microsatellite instability. Nat Genet 9:48-55. 1680. Liu B, Parsons RE, Hamilton SR,Petersen GM, Lynch HT, Watson P,Markowitz S, Willson JK, Green J, de laChapelle A, Kinzler KW, Vogelstein B(1994). hMSH2 mutations in hereditarynonpolyposis colorectal cancer kindreds.Cancer Res 54: 4590-4594. 1681. Liu FS, Kohler MF, Marks JR, Bast RCJr., Boyd J, Berchuck A (1994). Mutationand overexpression of the p53 tumor sup-pressor gene frequently occurs in uterineand ovarian sarcomas. Obstet Gynecol 83:118-124. 1682. Liu MM (1988). Fibromyoma of thevagina. Eur J Obstet Gynecol Reprod Biol29: 321-328. 1683. Liu WM, Chen CJ, Kan YY, Chao KC,Yuan CC, Ng HT (1989). Simultaneousendometrioid carcinoma of the uterinecorpus and ovary. Zhonghua Yi Xue Za Zhi(Taipei) 44: 38-44. 1684. LiVolsi VA, Kelsey JL, Fischer DB,Holford TR, Mostow ED, Goldenberg IS(1982). Effect of age at first childbirth onrisk of developing specific histologic sub-type of breast cancer. Cancer 49: 1937-1940. 1685. Lloreta J, Prat J (1992). Endometrialstromal nodule with smooth and skeletalmuscle components simulating stromalsarcoma. Int J Gynecol Pathol 11: 293-298. 1686. Lobaccaro JM, Lumbroso S, Belon C,Galtier-Dereure F, Bringer J, Lesimple T,Namer M, Cutuli BF, Pujol H, Sultan C(1993). Androgen receptor gene mutationin male breast cancer. Hum Mol Genet 2:1799-1802.

399References
1687. Loman N, Johannsson O,Kristoffersson U, Olsson H, Borg A (2001).Family history of breast and ovarian can-cers and BRCA1 and BRCA2 mutations in apopulation-based series of early-onsetbreast cancer. J Natl Cancer Inst 93: 1215-1223. 1688. London SJ, Connolly JL, Schnitt SJ,Colditz GA (1992). A prospective study ofbenign breast disease and the risk ofbreast cancer. JAMA 267: 941-944. 1689. Longacre TA, Chung MH, Jensen DN,Hendrickson MR (1995). Proposed criteriafor the diagnosis of well-differentiatedendometrial carcinoma. A diagnostic testfor myoinvasion. Am J Surg Pathol 19: 371-406. 1690. Longacre TA, Chung MH, Rouse RV,Hendrickson MR (1996). Atypical polypoidadenomyofibromas (atypical polypoid ade-nomyomas) of the uterus. A clinicopatho-logic study of 55 cases. Am J Surg Pathol20: 1-20. 1691. Longnecker MP (1994). Alcoholicbeverage consumption in relation to risk ofbreast cancer: meta-analysis and review.Cancer Causes Control 5: 73-82. 1692. Longway SR, Lind HM, Haghighi P(1986). Extraskeletal Ewing's sarcoma aris-ing in the broad ligament. Arch Pathol LabMed 110: 1058-1061. 1693. Longy M, Lacombe D (1996). Cowdendisease. Report of a family and review.Ann Genet 39: 35-42. 1694. Look KY, Roth LM, Sutton GP (1993).Vulvar melanoma reconsidered. Cancer 72:143-146. 1695. Loose JH, Patchefsky AS, HollanderIJ, Lavin LS, Cooper HS, Katz SM (1992).Adenomyoepithelioma of the breast. Aspectrum of biologic behavior. Am J SurgPathol 16: 868-876. 1 6 9 5 a . Lopes JM, Seruca R, Hall AP,Branco P, Castedo SM (1990). Cytogeneticstudy of a sclerosing stromal tumor of theovary. Cancer Genet Cytogenet 49: 103-106. 1696. Lopez-Rios F, Miguel PS, Bellas C,Ballestin C, Hernandez L (2000).Lymphoepithelioma-like carcinoma of theuterine cervix: a case report studied by insitu hybridization and polymerase chainreaction for Epstein-Barr virus. A r c hPathol Lab Med 124: 746-747. 1697. Lorenz G (1978). [Adenomatoid tumorof the ovary and vagina (author's transl)].Zentralbl Gynakol 100: 1412-1416. 1698. Lorigan PC, Grierson AJ, Goepel JR,Coleman RE, Goyns MH (1996). Gestationalchoriocarcinoma of the ovary diagnosedby analysis of tumour DNA. Cancer Lett104: 27-30. 1699. Lorincz AT, Reid R, Jenson AB,Greenberg MD, Lancaster W, Kurman RJ(1992). Human papillomavirus infection ofthe cervix: relative risk associations of 15common anogenital types. Obstet Gynecol79: 328-337. 1700. Losi L., Lorenzini R., Eusebi V,Bussolati G (1995). Apocrine differentiationin invasive carcinoma of the breast. ApplImmunohistochem 3: 91-98. 1701. Lotocki RJ, Krepart GV, ParaskevasM, Vadas G, Heywood M, Fung FK (1992).Glassy cell carcinoma of the cervix: abimodal treatment strategy. G y n e c o lOncol 44: 254-259. 1702. Loverro G, Cormio G, Renzulli G,Lepera A, Ricco R, Selvaggi L (1997).Serous papillary cystadenoma of border-line malignancy of the broad ligament. EurJ Obstet Gynecol Reprod Biol 74: 211-213.
1703. Loy TS, Calaluce RD, Keeney GL(1996). Cytokeratin immunostaining in dif-ferentiating primary ovarian carcinomafrom metastatic colonic adenocarcinoma.Mod Pathol 9: 1040-1044. 1704. Lu KH, Cramer DW, Muto MG, Li EY,Niloff J, Mok SC (1999). A population-based study of BRCA1 and BRCA2 muta-tions in Jewish women with epithelialovarian cancer. Obstet Gynecol 93: 34-37. 1705. Lu SL, Kawabata M, Imamura T,Akiyama Y, Nomizu T, Miyazono K, Yuasa Y(1998). HNPCC associated with germlinemutation in the TGF-beta type II receptorgene. Nat Genet 19: 17-18. 1706. Lu X, Nikaido T, Toki T, Zhai YL, KitaN, Konishi I, Fujii S (2000). Loss of het-erozygosity among tumor suppressorgenes in invasive and in situ carcinoma ofthe uterine cervix. Int J Gynecol Cancer 10:452-458. 1707. Lu YJ, Osin P, Lakhani SR, Di Palma S,Gusterson BA, Shipley JM (1998).Comparative genomic hybridization analy-sis of lobular carcinoma in situ and atypi-cal lobular hyperplasia and potential rolesfor gains and losses of genetic material inbreast neoplasia. Cancer Res 58: 4721-4727. 1708. Lucas FV, Perez-Mesa C (1978).Inflammatory carcinoma of the breast.Cancer 41: 1595-1605. 1709. Luchtrath H, Moll R (1989).Mucoepidermoid mammary carcinoma.Immunohistochemical and biochemicalanalyses of intermediate filaments.Virchows Arch A Pathol Anat Histopathol416: 105-113. 1710. Ludwig T, Chapman DL, PapaioannouVE, Efstratiadis A (1997). Targeted muta-tions of breast cancer susceptibility genehomologs in mice: lethal phenotypes ofBrca1, Brca2, Brca1/Brca2, Brca1/p53, andBrca2/p53 nullizygous embryos. G e n e sDev 11: 1226-1241. 1711. Luevano-Flores E, Sotelo J, Tena-Suck M (1985). Glial polyp (glioma) of theuterine cervix, report of a case withdemonstration of glial fibrillary acidic pro-tein. Gynecol Oncol 21: 385-390. 1712. Luft F, Gebert J, Schneider A,Melsheimer P, von Knebel DM (1999).Frequent allelic imbalance of tumor sup-pressor gene loci in cervical dysplasia. IntJ Gynecol Pathol 18: 374-380. 1713. Lui M, Dahlstrom JE, Bell S, JamesDT (2001). Apocrine adenoma of the breast:diagnosis on large core needle biopsy.Pathology 33: 149-152. 1714. Lukas C, Bartkova J, Latella L, FalckJ, Mailand N, Schroeder T, Sehested M,Lukas J, Bartek J (2001). DNA damage-activated kinase Chk2 is independent ofproliferation or differentiation yet corre-lates with tissue biology. Cancer Res 61:4990-4993. 1715. Luna-More S, Gonzalez B, Acedo C,Rodrigo I, Luna C (1994). Invasivemicropapillary carcinoma of the breast. Anew special type of invasive mammarycarcinoma. Pathol Res Pract 190: 668-674. 1716. Lund B, Thomsen HK, Olsen J (1991).Reproducibility of histopathological evalu-ation in epithelial ovarian carcinoma.Clinical implications. APMIS 99: 353-358. 1717. Lurain JR, Brewer JI, Torok EE,Halpern B (1982). Gestational trophoblasticdisease: treatment results at the BrewerTrophoblastic Disease Center. O b s t e tGynecol 60: 354-360.
1718. Luton JP, Clerc J, Paoli V, Bonnin A,Dumez Y, Vacher-Lavenu MC (1991).[Bilateral Leydig cell tumor of the ovary ina woman with congenital adrenal hyper-plasia. The first reported case]. PresseMed 20: 109-112. 1 7 1 9 . Luttges JE, Lubke M (1994).Recurrent benign Mullerian papilloma ofthe vagina. Immunohistological findingsand histogenesis. Arch Gynecol Obstet255: 157-160. 1720. Luxman D, Jossiphov J, Cohen JR,Wolf Y, David MP (1997). Uterine metasta-sis from vulvar malignant melanoma. Acase report. J Reprod Med 42: 244-246. 1721. Luzzi V, Holtschlag V, Watson MA(2001). Expression profiling of ductal carci-noma in situ by laser capture microdissec-tion and high-density oligonucleotidearrays. Am J Pathol 158: 2005-2010. 1722. Lyday RO (1952). Fibroma of the ovarywith abdominal implants. Am J Surg 84:737-738. 1723. Lynch ED, Ostermeyer EA, Lee MK,Arena JF, Ji H, Dann J, Swisshelm K,Suchard D, MacLeod PM, Kvinnsland S,Gjertsen BT, Heimdal K, Lubs H, Moller P,King MC (1997). Inherited mutations inPTEN that are associated with breast can -cer, cowden disease, and juvenile polypo-sis. Am J Hum Genet 61: 1254-1260. 1724. Lynch HT, Albano WA, Heieck JJ,Mulcahy GM, Lynch JF, Layton MA, DanesBS (1984). Genetics, biomarkers, and con-trol of breast cancer: a review. CancerGenet Cytogenet 13: 43-92. 1725. Lynch HT, de la Chapelle A (1999).Genetic susceptibility to non-polyposiscolorectal cancer. J Med Genet 36: 801-818. 1726. Mabuchi K, Bross DS, Kessler II(1985). Risk factors for male breast cancer.J Natl Cancer Inst 74: 371-375. 1727. MacLachlan TK, Somasundaram K,Sgagias M, Shifman Y, Muschel RJ, CowanKH, El Deiry WS (2000). BRCA1 effects onthe cell cycle and the DNA damageresponse are linked to altered geneexpression. J Biol Chem 275: 2777-2785. 1728. MacSweeney JE, King DM (1994).Computed tomography, diagnosis, stagingand follow-up of pure granulosa celltumour of the ovary. Clin Radiol 49: 241-245. 1729. Madison T, Schottenfeld D, Baker V(1998). Cancer of the corpus uteri in whiteand black women in Michigan, 1985-1994:an analysis of trends in incidence and mor-tality and their relation to histologic sub-type and stage. Cancer 83: 1546-1554. 1730. Maehama T, Dixon JE (1998). Thetumor suppressor, PTEN/MMAC1, dephos-phorylates the lipid second messenger,phosphatidylinositol 3,4,5-trisphosphate. JBiol Chem 273: 13375-13378. 1731. Magi-Galluzi C, O'Connor JT, NeffenF, Sun D, Quade BJ, Crum CP, Nucci MR(2001). Are mucinous cystadenomas of theovary derived from germ cells ? M o dPathol 14: 140 A. 1732. Magrina JF, Gonzalez-Bosquet J,Weaver AL, Gaffey TA, Leslie KO, WebbMJ, Podratz KC (2000). Squamous cell car -cinoma of the vulva stage IA: long-termresults. Gynecol Oncol 76: 24-27. 1733. Magro G, Bisceglia M, Michal M(2000). Expression of steroid hormonereceptors, their regulated proteins, andbcl-2 protein in myofibroblastoma of thebreast. Histopathology 36: 515-521.
1734. Magro G, Fraggetta F, Torrisi A,Emmanuele C, Lanzafame S (1999).Myofibroblastoma of the breast withhemangiopericytoma-like pattern andpleomorphic lipoma-like areas. Report of acase with diagnostic and histogeneticconsiderations. Pathol Res Pract 195: 257-262. 1735. Magro G, Michal M, Bisceglia M(2001). Benign spindle cell tumors of themammary stroma: diagnostic criteria, clas-sification, and histogenesis. Pathol ResPract 197: 453-466. 1736. Magro G, Michal M, Vasquez E,Bisceglia M (2000). Lipomatous myofibrob-lastoma: a potential diagnostic pitfall in thespectrum of the spindle cell lesions of thebreast. Virchows Arch 437: 540-544. 1737. Mahmoud-Ahmed AS, Suh JH,Barnett GH, Webster KD, Kennedy AW(2001). Tumor distribution and survival insix patients with brain metastases fromcervical carcinoma. Gynecol Oncol 8 1 :196-200. 1738. Mai KT, Yazdi HM, Bertrand MA,LeSaux N, Cathcart LL (1996). Bilateral pri-mary ovarian squamous cell carcinomaassociated with human papilloma virusinfection and vulvar and cervical intraep-ithelial neoplasia. A case report withreview of the literature. Am J Surg Pathol20: 767-772. 1739. Maier RC, Norris HJ (1980).Coexistence of cervical intraepithelial neo-plasia with primary adenocarcinoma of theendocervix. Obstet Gynecol 56: 361-364. 1740. Maier WP, Rosemond GP, GoldmanLI, Kaplan GF, Tyson RR (1977). A ten yearstudy of medullary carcinoma of thebreast. Surg Gynecol Obstet 144: 695-698. 1741. Maiorano E, Ricco R, Virgintino D, etal. (1994). Infiltrating myoepithelioma of thebreast. Appl Immunohistochem 2: 130-136. 1742. Maitra A, Wistuba II, Gibbons D,Gazdar AF, Albores-Saavedra J (1999).Allelic losses at chromosome 3p are seenin human papilloma virus 16 associatedtransitional cell carcinoma of the cervix.Gynecol Oncol 74: 361-368. 1743. Maitra A, Wistuba II, Washington C,Virmani AK, Ashfaq R, Milchgrub S, GazdarAF, Minna JD (2001). High-resolution chro-mosome 3p allelotyping of breast carcino-mas and precursor lesions demonstratesfrequent loss of heterozygosity and a dis-continuous pattern of allele loss. Am JPathol 159: 119-130. 1744. Majmudar B, Ross RJ, Gorelkin L(1979). Benign blue nevus of the uterinecervix. Am J Obstet Gynecol 134: 600-601. 1745. Major FJ, Blessing JA, Silverberg SG,Morrow CP, Creasman WT, Currie JL,Yordan E, Brady MF (1993). Prognostic fac-tors in early-stage uterine sarcoma. AGynecologic Oncology Group study.Cancer 71: 1702-1709. 1746. Malik SN, Wilkinson EJ (1999).Pseudo-Paget's disease of the vulva: acase report. J Lower Genital Tract Disease3: 201-203. 1747. Malinak LR, Miller GV, Armstrong JT(1966). Primary squamous cell carcinomaof the Fallopian tube. Am J Obstet Gynecol95: 1167-1168. 1748. Mallory SB (1995). Cowden syndrome(multiple hamartoma syndrome). DermatolClin 13: 27-31. 1749. Malmstrom H, Janson H, Simonsen E,Stenson S, Stendahl U (1990). Prognosticfactors in invasive squamous cell carcino-ma of the vulva treated with surgery andirradiation. Acta Oncol 29: 915-919.

400 References
1750. Maluf FC, Sabbatini P, Schwartz L,Xia J, Aghajanian C (2001). Endometrialstromal sarcoma: objective response toletrozole. Gynecol Oncol 82: 384-388. 1751. Maluf HM, Koerner FC (1994).Carcinomas of the breast with endocrinedifferentiation: a review. Virchows Arch425: 449-457. 1752. Maluf HM, Koerner FC (1995). Solidpapillary carcinoma of the breast. A formof intraductal carcinoma with endocrinedifferentiation frequently associated withmucinous carcinoma. Am J Surg Pathol 19:1237-1244. 1753. Mambo NC, Burke JS, Butler JJ(1977). Primary malignant lymphomas ofthe breast. Cancer 39: 2033-2040.1754. Man S, Ellis IO, Sibbering M, BlameyRW, Brook JD (1996). High levels of alleleloss at the FHIT and ATM genes in non-comedo ductal carcinoma in situ andgrade I tubular invasive breast cancers.Cancer Res 56: 5484-5489. 1755. Mandai M, Konishi I, Kuroda H,Komatsu T, Yamamoto S, Nanbu K,Matsushita K, Fukumoto M, Yamabe H,Mori T (1998). Heterogeneous distributionof K-ras-mutated epithelia in mucinousovarian tumors with special reference tohistopathology. Hum Pathol 29: 34-40. 1756. Manegold E, Tietze L, Gunther K,Fleischer A, Amo-Takyi BK, Schroder W,Handt S (2001). Trisomy 8 as sole karyotyp-ic aberration in an ovarian metastasizingSertoli-Leydig cell tumor. Hum Pathol 32:559-562. 1757. Manhoff DT, Schiffman R, Haupt HM(1995). Adenoid cystic carcinoma of theuterine cervix with malignant stroma. Anunusual variant of carcinosarcoma? Am JSurg Pathol 19: 229-233. 1758. Manini C, Pietribiasi F, Sapino A,Donadio S (1998). [Serous cystadenocarci-noma of the ovary with simultaneousbreast metastases. Description of a case].Pathologica 90: 152-155. 1759. Manivel JC, Niehans G, Wick MR,Dehner LP (1987). Intermediate trophoblastin germ cell neoplasms. Am J Surg Pathol11: 693-701. 1760. Manjer J, Malina J, Berglund G,Bondeson L, Garne JP, Janzon L (2001).Increased incidence of small and well-dif-ferentiated breast tumours in post-menopausal women following hormone-replacement therapy. Int J Cancer 9 2 :919-922. 1761. Mannion C, Park WS, Man YG,Zhuang Z, Albores-Saavedra J, TavassoliFA (1998). Endocrine tumors of the cervix:morphologic assessment, expression ofhuman papillomavirus, and evaluation forloss of heterozygosity on 1p, 3p, 11q, and17p. Cancer 83: 1391-1400. 1762. Manson CM, Hirsch PJ, Coyne JD(1995). Post-operative spindle cell noduleof the vulva. Histopathology 26: 571-574. 1763. Mansour EG, Ravdin PM, Dressler L(1994). Prognostic factors in early breastcarcinoma. Cancer 74: 381-400. 1764. Marchal C, Weber B, de Lafontan B,Resbeut M, Mignotte H, du Chatelard PP,Cutuli B, Reme-Saumon M, Broussier-Leroux A, Chaplain G, Lesaunier F,Dilhuydy JM, Lagrange JL (1999). Ninebreast angiosarcomas after conservativetreatment for breast carcinoma: a surveyfrom French comprehensive CancerCenters. Int J Radiat Oncol Biol Phys 44:113-119.
1765. Marchese MJ, Liskow AS, Crum CP,McCaffrey RM, Frick HC (1984). Uterinesarcomas: a clinicopathologic study, 1965-1981. Gynecol Oncol 18: 299-312. 1766. Marchetti A, Buttitta F, Pellegrini S,Campani D, Diella F, Cecchetti D, CallahanR, Bistocchi M (1993). p53 mutations andhistological type of invasive breast carci-noma. Cancer Res 53: 4665-4669. 1767. Marcus JN, Watson P, Page DL,Narod SA, Lenoir GM, Tonin P, Linder-Stephenson L, Salerno G, Conway TA,Lynch HT (1996). Hereditary breast cancer:pathobiology, prognosis, and BRCA1 andBRCA2 gene linkage. Cancer 77: 697-709. 1768. Marcus VA, Madlensky L, Gryfe R,Kim H, So K, Millar A, Temple LK, Hsieh E,Hiruki T, Narod S, Bapat BV, Gallinger S,Redston M (1999). Immunohistochemistryfor hMLH1 and hMSH2: a practical test forDNA mismatch repair-deficient tumors.Am J Surg Pathol 23: 1248-1255. 1769. Marquis ST, Rajan JV, Wynshaw-Boris A, Xu J, Yin GY, Abel KJ, Weber BL,Chodosh LA (1995). The developmentalpattern of Brca1 expression implies a rolein differentiation of the breast and othertissues. Nat Genet 11: 17-26. 1770. Marsden DE, Friedlander M, HackerNF (2000). Current management of epithe-lial ovarian carcinoma: a review. SeminSurg Oncol 19: 11-19. 1771. Marsh DJ, Coulon V, Lunetta KL,Rocca-Serra P, Dahia PL, Zheng Z, Liaw D,Caron S, Duboue B, Lin AY, Richardson AL,Bonnetblanc JM, Bressieux JM, Cabarrot-Moreau A, Chompret A, Demange L, EelesRA, Yahanda AM, Fearon ER, Fricker JP,Gorlin RJ, Hodgson SV, Huson S, LacombeD, Leprat F, Odent S, Toulouse C, OlopadeOI, Sobol H, Tishler S, Woods CG, RobinsonBG, Weber HC, Parsons R, Peacocke M,Longy M, Eng C. (1998). Mutation spectrumand genotype-phenotype analyses inCowden disease and Bannayan-Zonanasyndrome, two hamartoma syndromeswith germline PTEN mutation. Hum MolGenet 7: 507-515. 1772. Marsh DJ, Dahia PL, Caron S, KumJB, Frayling IM, Tomlinson IP, Hughes KS,Eeles RA, Hodgson SV, Murday VA,Houlston R, Eng C (1998). Germline PTENmutations in Cowden syndrome-like fami-lies. J Med Genet 35: 881-885. 1773. Marsh DJ, Dahia PL, Zheng Z, Liaw D,Parsons R, Gorlin RJ, Eng C (1997).Germline mutations in PTEN are present inBannayan-Zonana syndrome. Nat Genet16: 333-334. 1774. Marsh DJ, Kum JB, Lunetta KL,Bennett MJ, Gorlin RJ, Ahmed SF,Bodurtha J, Crowe C, Curtis MA, DasoukiM, Dunn T, Feit H, Geraghty MT, GrahamJM Jr., Hodgson SV, Hunter A, Korf BR,Manchester D, Miesfeldt S, Murday VA,Nathanson KL, Parisi M, Pober B, RomanoC, Tolmie JL, Trembath R, Winter RM,Zackai EH, Zori RT, Weng LP, Dahia PLM,Eng C (1999). PTEN mutation spectrum andgenotype-phenotype correlations inBannayan-Riley-Ruvalcaba syndrome sug-gest a single entity with Cowden syn-drome. Hum Mol Genet 8: 1461-1472. 1774a. Marsh WL, Jr., Lucas JG, Olsen J(1989). Chondrolipoma of the breast. ArchPathol Lab Med 113: 369-3711775. Marshall LM, Hunter DJ, Connolly JL,Schnitt SJ, Byrne C, London SJ, Colditz GA(1997). Risk of breast cancer associatedwith atypical hyperplasia of lobular andductal types. Cancer EpidemiolBiomarkers Prev 6: 297-301.
1776. Marshall RJ, Braye SG, Jones DB(1986). Leiomyosarcoma of the uterus withgiant cells resembling osteoclasts. Int JGynecol Pathol 5: 260-268. 1777. Martin-Hirsch PL, Paraskevaidis E,Kitchener H (2001). Surgery for cervicalintraepithelial neoplasia ( C o c h r a n eReview). The Cochrane Library.1778. Martinelli G, Govoni E, Pileri S,Grigioni FW, Doglioni C, Pelusi G (1983).Sclerosing stromal tumor of the ovary. Ahormonal, histochemical and ultrastructur-al study. Virchows Arch A Pathol AnatHistopathol 402: 155-161. 1779. Martinez A, Walker RA, Shaw JA,Dearing SJ, Maher ER, Latif F (2001).Chromosome 3p allele loss in early inva-sive breast cancer: detailed mapping andassociation with clinicopathological fea-tures. Mol Pathol 54: 300-306. 1780. Martinez V, Azzopardi JG (1979).Invasive lobular carcinoma of the breast:incidence and variants. Histopathology 3:467-488. 1781. Martino A, Zamparelli M, Santinelli A,Cobellis G, Rossi L, Amici G (2001). Unusualclinical presentation of a rare case of phyl-lodes tumor of the breast in an adolescentgirl. J Pediatr Surg 36: 941-943. 1782. Mascarello JT, Cajulis TR, BillmanGF, Spruce WE (1993). Ovarian germ celltumor evolving to myelodysplasia. GenesChromosomes Cancer 7: 227-230. 1783. Massarelli G, Bosincu L, Costanzi G,Onida GA (1999). Uterine Wilms' tumor. IntJ Gynecol Pathol 18: 402-403. 1784. Matanoski GM, Breysse PN, ElliottEA (1991). Electromagnetic field exposureand male breast cancer. Lancet 337: 737. 1785. Mathoulin-Portier MP, Penault-Llorca F, Labit-Bouvier C, Charafe E, MartinF, Hassoun J, Jacquemier J (1998).Malignant mullerian mixed tumor of theuterine cervix with adenoid cystic compo-nent. Int J Gynecol Pathol 17: 91-92. 1786. Matias-Guiu X, Bussaglia E, CatasusL, Lagarda H, Gras E, Machin P, Prat J(2000). Correspondence re: W.M. Lin et al.,loss of heterozygosity and mutationalanalysis of the PTEN/MMAC1 gene in syn -chronous endometrial and ovarian carci-nomas. Clin. Cancer Res., 4: 2577-2583,1998. Clin Cancer Res 6: 1598-1600. 1787. Matias-Guiu X, Catasus L, BussagliaE, Lagarda H, Garcia A, Pons C, Munoz J,Arguelles R, Machin P, Prat J (2001).Molecular pathology of endometrial hyper-plasia and carcinoma. Hum Pathol 32: 569-577. 1788. Matias-Guiu X, Lagarda H, CatasusLI, Bussaglia E, Gallardo A, Gras E, Prat J(2002). Clonality analysis in synchronous ormetachronous tumors of the female genitaltract. Int J Gynecol Pathol 21: 205-211. 1789. Matias-Guiu X, Pons C, Prat J (1998).Mullerian inhibiting substance, alpha-inhibin, and CD99 expression in sex cord-stromal tumors and endometrioid ovariancarcinomas resembling sex cord-stromaltumors. Hum Pathol 29: 840-845. 1790. Matias-Guiu X, Prat J (1990). Ovariantumors with functioning stroma. Animmunohistochemical study of 100 caseswith human chorionic gonadotropin mono-clonal and polyclonal antibodies. Cancer65: 2001-2005. 1791. Matsuoka S, Huang M, Elledge SJ(1998). Linkage of ATM to cell cycle regula-tion by the Chk2 protein kinase. Science282: 1893-1897.
1792. Mattia AR, Ferry JA, Harris NL (1993).Breast lymphoma. A B-cell spectrumincluding the low grade B-cell lymphomaof mucosa associated lymphoid tissue. AmJ Surg Pathol 17: 574-587. 1793. Mauillon JL, Michel P, Limacher JM,Latouche JB, Dechelotte P, Charbonnier F,Martin C, Moreau V, Metayer J, Paillot B,Frebourg T (1996). Identification of novelgermline hMLH1 mutations including a 22kb Alu-mediated deletion in patients withfamilial colorectal cancer. Cancer Res 56:5728-5733. 1794. Mauz-Korholz C, Harms D, CalaminusG, Gobel U (2000). Primary chemotherapyand conservative surgery for vaginal yolk-sac tumour. Maligne KeimzelltumorenStudy Group. Lancet 355: 625. 1795. Mawhinney RR, Powell MC,Worthington BS, Symonds EM (1988).Magnetic resonance imaging of benignovarian masses. Br J Radiol 61: 179-186. 1796. Mayall F, Rutty K, Campbell F,Goddard H (1994). p53 immunostainingsuggests that uterine carcinosarcomasare monoclonal. Histopathology 24: 211-214. 1797. Mayerhofer K, Obermair A,Windbichler G, Petru E, Kaider A, Hefler L,Czerwenka K, Leodolter S, Kainz C (1999).Leiomyosarcoma of the uterus: a clinico-pathologic multicenter study of 71 cases.Gynecol Oncol 74: 196-201. 1798. Maymon E, Piura B, Mazor M, BashiriA, Silberstein T, Yanai-Inbar I (1998).Primary hepatoid carcinoma of ovary inpregnancy. Am J Obstet Gynecol 179: 820-822. 1799. Mayorga M, Garcia-Valtuille A,Fernandez I, et al. (1997). Adenocarcinomaof the uterine cervix with massive signet-ring cell differentiation. Int J Surg Pathol 5:95-100. 1800. Mazoujian G, Pinkus GS, Davis S,Haagensen DE Jr. (1983). Immuno-histochemistry of a gross cystic diseasefluid protein (GCDFP-15) of the breast. Amarker of apocrine epithelium and breastcarcinomas with apocrine features. Am JPathol 110: 105-112. 1801. Mazur MT (1981). Atypical polypoidadenomyomas of the endometrium. Am JSurg Pathol 5: 473-482. 1801a. Mazur MT (1989). Metastatic gesta-tional choriocarcinoma. Unusual patholog-ic variant following therapy. Cancer 63:1370-1377. 1802. Mazur MT, Hsueh S, Gersell DJ(1984). Metastases to the female genitaltract. Analysis of 325 cases. Cancer 53:1978-1984. 1802a. Mazur MT, Lurain JR, Brewer JI(1982). Fatal gestational choriocarcinoma.Clinicopathologic study of patients treatedat a trophoblastic disease center. Cancer50: 1833-1846. 1803. Mazzella FM, Sieber SC, Braza F(1995). Ductal carcinoma of male breastwith prominent lipid-rich component.Pathology 27: 280-283. 1804. McAdam JA, Stewart F, Reid R (1998).Vaginal epithelioid angiosarcoma. J ClinPathol 51: 928-930. 1805. McBride CM, Hortobagyi GN (1985).Primary inflammatory carcinoma of thefemale breast: staging and treatment pos-sibilities. Surgery 98: 792-798. 1806. McCarthy JH, Aga R (1988). A fallopi-an tube lesion of borderline malignancyassociated with pseudo-myxoma peri-tonei. Histopathology 13: 223-225.

401References
1807. McCluggage G, McBride H, MaxwellP, Bharucha H (1997). Immunohistoche-mical detection of p53 and bcl-2 proteins inneoplastic and non-neoplastic endocervi-cal glandular lesions. Int J Gynecol Pathol16: 22-27. 1808. McCluggage WG (1999). Uterinetumours resembling ovarian sex cordtumours: immunohistochemical evidencefor true sex cord differentiation.Histopathology 34: 375-376. 1809. McCluggage WG (2002). Malignantbiphasic uterine tumours: carcinosarco-mas or metaplastic carcinomas (Reviewarticle). J Clin Pathol 55: 321-325. 1810. McCluggage WG (2002). Uterine car -cinosarcomas (malignant mixed Mulleriantumors) are metaplastic carcinomas. Int JGynecol Cancer 12: 687-690. 1811. McCluggage WG, Abdulkader M,Price JH, Kelehan P, Hamilton S, Beattie J,al Nafussi A (2000). Uterine carcinosarco-mas in patients receiving tamoxifen. Areport of 19 cases. Int J Gynecol Cancer10: 280-284. 1812. McCluggage WG, Cromie AJ, BrysonC, Traub AI (2001). Uterine endometrialstromal sarcoma with smooth muscle andglandular differentiation. J Clin Pathol 54:481-483. 1813. McCluggage WG, Date A, BharuchaH, Toner PG (1996). Endometrial stromalsarcoma with sex cord-like areas andfocal rhabdoid differentiation. H i s t o p a -thology 29: 369-374. 1814. McCluggage WG, Lioe TF,McClelland HR, Lamki H (2002).Rhabdomyosarcoma of the uterus: reportof two cases including one of the spindlecell variant. Int J Gynecol Cancer 12: 128-132. 1815. McCluggage WG, Maxwell P (2001).Immunohistochemical staining for calre-tinin is useful in the diagnosis of ovariansex cord-stromal tumours. Histopathology38: 403-408. 1816. McCluggage WG, Maxwell P, SloanJM (1997). Immunohistochemical stainingof ovarian granulosa cell tumors with mon-oclonal antibody against inhibin. H u mPathol 28: 1034-1038. 1817. McCluggage WG, Nirmala V,Radhakumari K (1999). Intramural mullerianpapilloma of the vagina. Int J GynecolPathol 18: 94-95. 1818. McCluggage WG, Perenyei M, IrwinST (2002). Recurrent cellular angiofibromaof the vulva. J Clin Pathol 55: 477-479. 1819. McCluggage WG, Sloan JM, BoyleDD, Toner PG (1998). Malignant fibrotheco-matous tumour of the ovary: diagnosticvalue of anti-inhibin immunostaining. J ClinPathol 51: 868-871. 1820. McCluggage WG, Sloan JM,Murnaghan M, White R (1996).Gynandroblastoma of ovary with juvenilegranulosa cell component and heterolo-gous intestinal type glands. Histopatholo-gy 29: 253-257. 1821. McCluggage WG, Sumathi VP,Maxwell P (2001). CD10 is a sensitive anddiagnostically useful immunohistochemi-cal marker of normal endometrial stromaand of endometrial stromal neoplasms.Histopathology 39: 273-278.
1822. McCluggage WG, Sumathi VP,McBride HA, Patterson A (2002). A panel ofimmunohistochemical stains, includingcarcinoembryonic antigen, vimentin, andestrogen receptor, aids in the distinctionbetween primary endometrial and endo-cervical adenocarcinomas. Int J GynecolPathol 21: 11-15. 1823. McCluskey LL, Dubeau L (1997).Biology of ovarian cancer. Curr Opin Oncol9: 465-470. 1824. McConnell DT, Miller ID, Parkin DE,Murray GI (1997). p53 protein expression ina population-based series of primary vul-val squamous cell carcinoma and immedi-ate adjacent field change. Gynecol Oncol67: 248-254. 1825. McConville CM, Stankovic T, ByrdPJ, McGuire GM, Yao QY, Lennox GG,Taylor MR (1996). Mutations associatedwith variant phenotypes in ataxia-telang-iectasia. Am J Hum Genet 59: 320-330. 1826. McCready DR, Hortobagyi GN, KauSW, Smith TL, Buzdar AU, Balch CM (1989).The prognostic significance of lymph nodemetastases after preoperative chemother-apy for locally advanced breast cancer.Arch Surg 124: 21-25. 1827. McCulloch GL, Evans AJ, Yeoman L,Wilson AR, Pinder SE, Ellis IO, Elston CW(1997). Radiological features of papillarycarcinoma of the breast. Clin Radiol 52:865-868. 1828. McCullough K, Froats ER, Falk HC(1946). Epidermoid carcinoma arising in anendometrial cyst of the ovary. Arch PatholLab Med 41: 335-337. 1829. McDivitt RW, Boyce W, Gersell D(1982). Tubular carcinoma of the breast.Clinical and pathological observationsconcerning 135 cases. Am J Surg Pathol 6:401-411. 1830. McDivitt RW, Stevens JA, Lee NC,Wingo PA, Rubin GL, Gersell D (1992).Histologic types of benign breast diseaseand the risk for breast cancer. The Cancerand Steroid Hormone Study Group. Cancer69: 1408-1414. 1831. McDivitt RW, Stewart FW (1966).Breast carcinoma in children. JAMA 195:388-390. 1832. McDivitt RW, Stewart FW, Berg JW(1968). Atlas of Tumour Pathology. 2 n dseries ed. Washington.1833. McGuire WL, Clark GM (1992).Prognostic factors and treatment deci-sions in axillary node-negative breast can-cer. N Engl J Med 326: 1756-1761. 1834. McKittrick JE, Doane WA, Failing RM(1969). Intracystic papillary carcinoma ofthe breast. Am Surg 35: 195-202. 1835. McKusick VA (1998). M e n d e l i a nInheritance in Man. Catalogs of HumanGenes and Genetic Disorders. 12th ed.John Hopkins University Press: Baltimore.1836. McLachlan SA, Erlichman C, Liu FF,Miller N, Pintilie M (1996). Male breastcancer: an 11 year review of 66 patients.Breast Cancer Res Treat 40: 225-230. 1837. McLachlin CM, Kozakewich H,Craighill M, O'Connell B, Crum CP (1994).Histologic correlates of vulvar humanpapillomavirus infection in children andyoung adults. Am J Surg Pathol 18: 728-735. 1838. Meier-Ruge W (1992). Epidemiologyof congenital innervation defects of thedistal colon. Virchows Arch A Pathol AnatHistopathol 420: 171-177. 1839. Meigs JV (1954). Fibroma of the ovarywith ascites and hydrothorax. Meigs' syn-drome. Am J Obstet Gynecol 67: 962-987.
1840. Meijers-Heijboer H, van denOuweland A, Klijn J, Wasielewski M, deSnoo A, Oldenburg R, Hollestelle A,Houben M, Crepin E, Veghel-Plandsoen M,Elstrodt F, van Duijn C, Bartels C, Meijers C,Schutte M, McGuffog L, Thompson D,Easton D, Sodha N, Seal S, Barfoot R,Mangion J, Chang-Claude J, Eccles D,Eeles R, Evans DG, Houlston R, Murday V,Narod S, Peretz T, Peto J, Phelan C, ZhangHX, Szabo C, Devilee P, Goldgar D, FutrealPA, Nathanson KL, Weber B, Rahman N,Stratton MR (2002). Low-penetrance sus-ceptibility to breast cancer due toCHEK2(*)1100delC in noncarriers of BRCA1or BRCA2 mutations. Nat Genet 31: 55-59. 1841. Meisels A, Fortin R (1976).Condylomatous lesions of the cervix andvagina. I. Cytologic patterns. Acta Cytol 20:505-509. 1842. Melhem MF, Tobon H (1987).Mucinous adenocarcinoma of theendometrium: a clinico-pathologicalreview of 18 cases. Int J Gynecol Pathol 6:347-355. 1843. Melnick S, Cole P, Anderson D,Herbst A (1987). Rates and risks of diethyl-stilbestrol-related clear-cell adenocarci-noma of the vagina and cervix. An update.N Engl J Med 316: 514-516. 1844. Mendez LE, Joy S, Angioli R, EstapeR, Penalver M (1999). Primary uterineangiosarcoma. Gynecol Oncol 75: 272-276. 1845. Mentzel T (2001). Myofibroblasticsarcomas: a brief review of sarcomasshowing a myofibroblastic line of differen-tiation and discussion of the differentialdiagnosis. Current Diagn Pathol 7: 17-24. 1846. Merajver SD, Pham TM, Caduff RF,Chen M, Poy EL, Cooney KA, Weber BL,Collins FS, Johnston C, Frank TS (1995).Somatic mutations in the BRCA1 gene insporadic ovarian tumours. Nat Genet 9:439-443. 1846 a. Merina MJ, Llombart-Bosch A,Menteagudo C (1990). Malignant changesassociated with sclerosing adenosis: amorphologic and immunohistocheicalanalysis of seven cases. Mod Pathol 3. 1847. Merino MJ, Carter D, Berman M(1983). Angiosarcoma of the breast. Am JSurg Pathol 7: 53-60. 1848. Merino MJ, Edmonds P, LiVolsi V(1985). Appendiceal carcinoma metastaticto the ovaries and mimicking primary ovar-ian tumors. Int J Gynecol Pathol 4: 110-120. 1849. Merino MJ, LiVolsi VA (1981). Signetring carcinoma of the female breast: a clin-icopathologic analysis of 24 cases. Cancer48: 1830-1837. 1850. Merino MJ, LiVolsi VA, Schwartz PE,Rudnicki J (1982). Adenoid basal cell carci-noma of the vulva. Int J Gynecol Pathol 1:299-306. 1850 a. Merrill JA (1959). Carcinoma of thebroad ligament. Obstet Gynecol 13: 472-476. 1851. Meyer AC, Dokerty MB, HarringtonSW (1948). Inflammatory carcinoma of thebreast. A correlation of clinical radiologicand pathological findings. Surg GynecolObstet 87: 417-424. 1852. Meyer JE, Lester SC, DiPrio PJ,Ferraro FA, Frenna TH, Denison CM (1995).Occult calcified fibroadenomas. B r e a s tdisease 8: 29-38. 1853. Meyer JS (1986). Cell kinetics of his-tologic variants of in situ breast carcino-ma. Breast Cancer Res Treat 7: 171-180.
1854. Michael H, Ulbright TM, BrodheckerCA (1989). The pluripotential nature of themesenchyme-like component of yolk sactumor. Arch Pathol Lab Med 113: 1115-1119. 1855. Michaels BM, Nunn CR, Roses DF(1994). Lobular carcinoma of the malebreast. Surgery 115: 402-405. 1856. Micheletti L, Preti M, Bogliatto F,Chieppa P (2000). [Vestibular papillomato-sis]. Minerva Ginecol 52: 87-91. 1857. Michels KB, Trichopoulos D, RobinsJM, Rosner BA, Manson JE, Hunter DJ,Colditz GA, Hankinson SE, Speizer FE,Willett WC (1996). Birthweight as a riskfactor for breast cancer. Lancet 348: 1542-1546. 1858. Middleton LP, Palacios DM, BryantBR, Krebs P, Otis CN, Merino MJ (2000).Pleomorphic lobular carcinoma: morpholo-gy, immunohistochemistry, and molecularanalysis. Am J Surg Pathol 24: 1650-1656. 1859. Middleton LP, Palacios DM, BryantBR, Krebs P, Otis CN, Merino MJ (2000).Pleomorphic lobular carcinoma: morpholo-gy, immunohistochemistry, and molecularanalysis. Am J Surg Pathol 24: 1650-1656. 1860. Mies C (1993). Recurrent secretorycarcinoma in residual mammary tissueafter mastectomy. Am J Surg Pathol 17:715-721. 1861. Mies C, Rosen PP (1987). Juvenilefibroadenoma with atypical epithelialhyperplasia. Am J Surg Pathol 11: 184-190. 1862. Miettinen M, Lehto VP, Virtanen I(1983). Postmastectomy angiosarcoma(Stewart-Treves syndrome). Light-micro-scopic, immunohistological, and ultra-structural characteristics of two cases.Am J Surg Pathol 7: 329-339. 1863. Mikami M, Ezawa S, Sakaiya N,Komuro Y, Tei C, Fukuchi T, Mukai M(2000). Response of glassy-cell carcinomaof the cervix to cisplatin, epirubicin, andmitomycin C. Lancet 355: 1159-1160. 1864. Miki Y, Swensen J, Shattuck-EidensD, Futreal PA, Harshman K, Tavtigian S, LiuQ, Cochran C, Bennett LM, Ding W, Bell R,Rosenthal J, Hussey C, Tran T, McClure M,Frye C, Hattier T, Phelps R, HaugenstranoA, Katcher H, Dayananth P, Ward J, ToninP, Narod S, Bristow PK, Norris FH,Helvering L, Morrison P, Rostek P, Lai M,Barrett JC, Lewis C, Neuhasen S,Cannonalbright L, Goldgar D, Wiseman R,Kamb A, Skolnick MH. (1994). A strongcandidate for the breast and ovarian can-cer susceptibility gene BRCA1. Science266: 66-71. 1865. Milanezi MF, Saggioro FP, Zanati SG,Bazan R, Schmitt FC (1998).Pseudoangiomatous hyperplasia of mam-mary stroma associated with gynaeco-mastia. J Clin Pathol 51: 204-206. 1866. Milde-Langosch K, Albrecht K, JoramS, Schlechte H, Giessing M, Loning T(1995). Presence and persistence of HPVinfection and p53 mutation in cancer of thecervix uteri and the vulva. Int J Cancer 63:639-645. 1867. Miles PA, Kiley KC, Mena H (1985).Giant fibrosarcoma of the ovary. Int JGynecol Pathol 4: 83-87. 1868. Miles PA, Norris HJ (1972).Proliferative and malignant Brennertumors of the ovary. Cancer 30: 174-186. 1 8 6 9 . Miliauskas JR, Leong AS (1992).Small cell (neuroendocrine) carcinoma ofthe vagina. Histopathology 21: 371-374.

402 References
1870. Miller B, Flax S, Dockter M,Photopulos G (1994). Nucleolar organizerregions in adenocarcinoma of the uterinecervix. Cancer 74: 3142-3145. 1871. Miller BE, Barron BA, Dockter ME,Delmore JE, Silva EG, Gershenson DM(2001). Parameters of differentiation andproliferation in adult granulosa cell tumorsof the ovary. Cancer Detect Prev 25: 48-54. 1872. Miller ES, Fairley JA, Neuburg M(1997). Vulvar basal cell carcinoma.Dermatol Surg 23: 207-209. 1873. Miller KN, McClure SP (1992).Papillary adenofibroma of the uterus.Report of a case involved by adenocarci-noma and review of the literature. Am JClin Pathol 97: 806-809. 1874. Miller WR, Telford J, Dixon JM,Shivas AA (1985). Androgen metabolismand apocrine differentiation in humanbreast cancer. Breast Cancer Res Treat 5:67-73. 1875. Minato H, Shimizu M, Hirokawa M,Fujiwara K, Kohno I, Manabe T (1998).Adenocarcinoma in situ of the fallopiantube. A case report. Acta Cytol 42: 1455-1457. 1876. Miremadi A, Pinder SE, Lee A, BellJA, Paish EC, Wencyk P, Elston CW,Nicholson RI, Blamey RW, Robertson JF,Ellis IO (2002). Neuroendocrine differentia-tion and prognosis in breast adenocarci-noma. Histopathology 40: 215-222. 1877. Mirhashemi R, Kratz A, Weir MM,Molpus KL, Goodman AK (1998). Vaginalsmall cell carcinoma mimicking aBartholin's gland abscess: a case report.Gynecol Oncol 68: 297-300. 1878. Mitao M, Nagai N, Levine RU,Silverstein SJ, Crum CP (1986). Humanpapillomavirus type 16 infection: a morpho-logical spectrum with evidence for lategene expression. Int J Gynecol Pathol 5:287-296. 1879. Mitelman F, Johansson B, Mertens F(2001). Mitelman Database of ChromosomeAberrations in Cancer. on-lineh t t p : / / c g a p . n c i . n i h . g o v / C h r o m o s o m e s / M i t elman. 1880. Mitnick JS, Vazquez MF, Harris MN,Schechter S, Roses DF (1990). Invasivepapillary carcinoma of the breast: mammo-graphic appearance. Radiology 177: 803-806. 1881. Mittal K, Mesia A, Demopoulos RI(1999). MIB-1 expression is useful in distin-guishing dysplasia from atrophy in elderlywomen. Int J Gynecol Pathol 18: 122-124. 1882. Mittal KR, Peng XC, Wallach RC,Demopoulos RI (1995). Coexistent atypicalpolypoid adenomyoma and endometrialadenocarcinoma. Hum Pathol 26: 574-576. 1883. Mittendorf R (1995). Teratogenupdate: carcinogenesis and teratogenesisassociated with exposure to diethylstilbe-strol (DES) in utero. Teratology 51: 435-445. 1884. Miyaki M, Konishi M, Tanaka K,Kikuchi-Yanoshita R, Muraoka M, YasunoM, Igari T, Koike M, Chiba M, Mori T (1997).Germline mutation of MSH6 as the causeof hereditary nonpolyposis colorectal can-cer. Nat Genet 17: 271-272. 1885. Miyoshi Y, Iwao K, Egawa C, NoguchiS (2001). Association of centrosomalkinase STK15/BTAK mRNA expressionwith chromosomal instability in humanbreast cancers. Int J Cancer 92: 370-373.
1886. Modan B, Hartge P, Hirsh-YechezkelG, Chetrit A, Lubin F, Beller U, Ben BaruchG, Fishman A, Menczer J, Ebbers SM,Tucker MA, Wacholder S, Struewing JP,Friedman E, Piura B (2001). Parity, oral con-traceptives, and the risk of ovarian canceramong carriers and noncarriers of aBRCA1 or BRCA2 mutation. N Engl J Med345: 235-240. 1 8 8 7 . Moffat CJ, Pinder SE, Dixon AR,Elston CW, Blamey RW, Ellis IO (1995).Phyllodes tumours of the breast: a clinico-pathological review of thirty-two cases.Histopathology 27: 205-218. 1888. Moffatt EJ, Kerns BJ, Madden JM,Layfield LJ (1997). Prognostic factors forfibromatoses: a correlation of proliferationindex, estrogen receptor, p53, retinoblas-toma, and src gene products and clinicalfeatures with outcome. J Surg Oncol 65:117-122. 1889. Moinfar F, Man YG, Arnould L,Bratthauer GL, Ratschek M, Tavassoli FA(2000). Concurrent and independent genet-ic alterations in the stromal and epithelialcells of mammary carcinoma: implicationsfor tumorigenesis. Cancer Res 60: 2562-2566. 1890. Moinfar F, Man YG, Lininger RA,Bodian C, Tavassoli FA (1999). Use of ker-atin 35betaE12 as an adjunct in the diagno-sis of mammary intraepithelial neoplasia-ductal type--benign and malignantintraductal proliferations. Am J SurgPathol 23: 1048-1058. 1891. Mok SC, Bell DA, Knapp RC,Fishbaugh PM, Welch WR, Muto MG,Berkowitz RS, Tsao SW (1993). Mutation ofK-ras protooncogene in human ovarianepithelial tumors of borderline malignancy.Cancer Res 53: 1489-1492. 1892. Moll R, Mitze M, Frixen UH,Birchmeier W (1993). Differential loss of E-cadherin expression in infiltrating ductaland lobular breast carcinomas. Am JPathol 143: 1731-1742. 1893. Moll UM, Chumas JC, Mann WJ,Patsner B (1990). Primary signet ring cellcarcinoma of the uterine cervix. N Y StateJ Med 90: 559-560. 1894. Molyneux AJ, Deen S, Sundaresan V(1992). Primitive neuroectodermal tumourof the uterus. Histopathology 21: 584-585. 1895. Monk BJ, Nieberg R, Berek JS (1993).Primary leiomyosarcoma of the ovary in aperimenarchal female. Gynecol Oncol 48:389-393. 1896. Monni O, Barlund M, Mousses S,Kononen J, Sauter G, Heiskanen M,Paavola P, Avela K, Chen Y, Bittner ML,Kallioniemi A (2001). Comprehensive copynumber and gene expression profiling ofthe 17q23 amplicon in human breast can-cer. Proc Natl Acad Sci USA 98: 5711-5716. 1897. Montag AG, Jenison EL, Griffiths CT,Welch WR, Lavin PT, Knapp RC (1989).Ovarian clear cell carcinoma. A clinico-pathologic analysis of 44 cases. Int JGynecol Pathol 8: 85-96. 1898. Montag TW, d'Ablaing G, SchlaerthJB, Gaddis O Jr., Morrow CP (1986).Embryonal rhabdomyosarcoma of the uter-ine corpus and cervix. Gynecol Oncol 25:171-194. 1899. Monteiro AN (2000). BRCA1: explor-ing the links to transcription. T r e n d sBiochem Sci 25: 469-474. 1900. Monterroso V, Jaffe ES, Merino MJ,Medeiros LJ (1993). Malignant lymphomasinvolving the ovary. A clinicopathologicanalysis of 39 cases. Am J Surg Pathol 17:154-170.
1901. Montes M, Roberts D, Berkowitz RS,Genest DR (1996). Prevalence and signifi-cance of implantation site trophoblasticatypia in hydatidiform moles and sponta-neous abortions. Am J Clin Pathol 105:411-416. 1902. Mooney EE, Man YG, Bratthauer GL,Tavassoli FA (1999). Evidence that Leydigcells in Sertoli-Leydig cell tumors have areactive rather than a neoplastic profile.Cancer 86: 2312-2319. 1903. Mooney EE, Nogales FF, Bergeron C,Tavassoli FA (2002). Retiform Sertoli-Leydig cell Tumours: Clinical,Morphological, and ImmunohistochemicalFindings. Histopathology 41: 110-117. 1904. Mooney EE, Nogales FF, Tavassoli FA(1999). Hepatocytic differentiation in reti-form Sertoli-Leydig cell tumors: distin-guishing a heterologous element fromLeydig cells. Hum Pathol 30: 611-617. 1905. Mooney EE, Tavassoli FA (1999).Papillary transitional cell carcinoma of thebreast: a report of five cases with distinc-tion from eccrine acrospiroma. M o dPathol 12: 287-294. 1906. Moore DH, Michael H, Furlin JJ, VonStein A (1998). Adenoid basal carcinoma ofthe vagina. Int J Gynecol Cancer 8: 261-263. 1907. Moore MP, Ihde JK, Crowe JP Jr.,Hakes TP, Kinne DW (1991). Inflammatorybreast cancer. Arch Surg 126: 304-306. 1908. Moore OS, Foote FW (1949). The rela-tively favorable prognosis of medullarycarcinoma of the breast. Cancer 2: 635-642. 1909. Moreno-Bueno G, Gamallo C, Perez-Gallego L, de Mora JC, Suarez A, PalaciosJ (2001). beta-Catenin expression pattern,beta-catenin gene mutations, andmicrosatellite instability in endometrioidovarian carcinomas and synchronousendometrial carcinomas. Diagn MolPathol 10: 116-122. 1910. Moreno-Rodriguez M, Perez-SiciliaM, Delinois R (1999). Lipoma of the endo-cervix. Histopathology 35: 483-484. 1911. Moreno V, Bosch FX, Munoz N,Meijer CJ, Shah KV, Walboomers JM,Herrero R, Franceschi S, InternationalAgency for Research on Cancer.Multicentric Cervical Cancer Study Group(2002). Effect of oral contraceptives on riskof cervical cancer in women with papillo-mavirus infection: the IARC multicentriccase-control study. Lancet 30: 1085-1092. 1912. Morgan LS, Joslyn P, Chafe W,Ferguson K (1988). A report on 18 cases ofprimary malignant melanoma of the vulva.Colposcopy and Gynecologic LaserSurgery 4 (3) and Laser Surg 4: 161-170. 1913. Morgan MB, Pitha JV (1998).Myofibroblastoma of the breast revisited:an etiologic association with androgens?Hum Pathol 29: 347-351. 1914. Morice P, Haie-Meder C, Pautier P,Lhomme C, Castaigne D (2001). Ovarianmetastasis on transposed ovary in patientstreated for squamous cell carcinoma of theuterine cervix: report of two cases and sur-gical implications. Gynecol Oncol 83: 605-607. 1915. Morikawa K, Hatabu H, Togashi K,Kataoka ML, Mori T, Konishi J (1997).Granulosa cell tumor of the ovary: MR find-ings. J Comput Assist Tomogr 21: 1001-1004. 1916. Morimitsu Y, Tanaka H, Iwanaga S,Kojiro M (1993). Alveolar soft part sarcomaof the uterine cervix. Acta Pathol Jpn 43:204-208.
1917. Morimoto T, Komaki K, Yamakawa T,Tanaka T, Oomine Y, Konishi Y, Mori T,Monden Y (1990). Cancer of the malebreast. J Surg Oncol 44: 180-184. 1918. Morimura Y, Honda T, Hoshi K,Yamada J, Nemoto K, Sato A (1995). A caseof uterine cervical adenoid cystic carcino-ma: immunohistochemical study for base-ment membrane material. Obstet Gynecol85: 903-905. 1 9 1 9 . Moross T, Lang AP, Mahoney L(1983). Tubular adenoma of breast. ArchPathol Lab Med 107: 84-86. 1920. Morrison JG, Gray GF Jr., Dao AH,Adkins RB Jr. (1987). Granular cell tumors.Am Surg 53: 156-160. 1921. Morrow M, Berger D, Thelmo W(1988). Diffuse cystic angiomatosis of thebreast. Cancer 62: 2392-2396. 1922. Moscovic EA, Azar HA (1967).Multiple granular cell tumors ("myoblas-tomas"). Case report with electron micro-scopic observations and review of the lit-erature. Cancer 20: 2032-2047. 1923. Mosher R, Genest DR (1997). Primaryintraplacental chorioacarcinoma: clinicaland pathological features of seven case(1967-1996) and discussion of the differen-tial diagnosis. J Surg Pathol 2: 83-97. 1924. Mosher R, Goldstein DP, Berkowitz R,Bernstein M, Genest DR (1998). Completehydatidiform mole. Comparison of clinico-pathologic features, current and past. JReprod Med 43: 21-27. 1925. Mosselman S, Polman J, Dijkema R(1996). ER beta: identification and charac-terization of a novel human estrogenreceptor. FEBS Lett 392: 49-53. 1926. Mossler JA, Barton TK, BrinkhousAD, McCarty KS, Moylan JA, McCarty KSJr. (1980). Apocrine differentiation inhuman mammary carcinoma. Cancer 46:2463-2471. 1927. Mostoufizadeh M, Scully RE (1980).Malignant tumors arising in endometriosis.Clin Obstet Gynecol 23: 951-963. 1928. Motoyama T, Watanabe H (1996).Extremely well differentiated squamouscell carcinoma of the breast. Report of acase with a comparative study of an epi-dermal cyst. Acta Cytol 40: 729-733. 1929. Mount PM, Norris HJ (1982). OverialTumouren. Springer: Berlin.1930. Moyal-Barracco M, Leibowitch M,Orth G (1990). Vestibular papillae of thevulva. Lack of evidence for human papillo-mavirus etiology. Arch Dermatol 126: 1594-1598. 1931. Moynahan ME, Chiu JW, Koller BH,Jasin M (1999). Brca1 controls homology-directed DNA repair. Mol Cell 4: 511-518. 1932. Mrad K, Driss M, Maalej M,Romdhane KB (2000). Bilateral cystosarco-ma phyllodes of the breast: a case reportof malignant form with contralateralbenign form. Ann Diagn Pathol 4: 370-372. 1933. Mrad K, Morice P, Fabre A, Pautier P,Lhomme C, Duvillard P, Sabourin JC (2000).Krukenberg tumor: a clinico-pathologicalstudy of 15 cases. Ann Pathol 20: 202-206. 1934. Muc RS, Grayson W, Grobbelaar JJ(2001). Adult extrarenal Wilms tumoroccurring in the uterus. Arch Pathol LabMed 125: 1081-1083. 1935. Mudhar HS, Smith JH, Tidy J (2001).Primary vaginal adenocarcinoma of intes-tinal type arising from an adenoma: casereport and review of the literature. Int JGynecol Pathol 20: 204-209. 1936. Mueller CB, Ames F (1978). Bilateralcarcinoma of the breast: frequency andmortality. Can J Surg 21: 459-465.

403References
1937. Mukai M, Torikata C, Iri H (1990).Alveolar soft part sarcoma: an electronmicroscopic study especially of uncrystal -lized granules using a tannic acid-contain-ing fixative. Ultrastruct Pathol 14: 41-50. 1938. Muller CY, O'Boyle JD, Fong KM,Wistuba II, Biesterveld E, Ahmadian M,Miller DS, Gazdar AF, Minna JD (1998).Abnormalities of fragile histidine triadgenomic and complementary DNAs in cer-vical cancer: association with humanpapillomavirus type. J Natl Cancer Inst 90:433-439. 1939. Mulvany NJ, Nirenberg A, Östör AG(1996). Non-primary cervical adenocarci-nomas. Pathology 28: 293-297. 1940. Mulvany NJ, Slavin JL, Östör AG,Fortune DW (1994). Intravenous leiomy-omatosis of the uterus: a clinicopathologicstudy of 22 cases. Int J Gynecol Pathol 13:1-9. 1941. Munkarah A, Malone JM Jr., BudevHD, Evans TN (1994). Mucinous adenocar-cinoma arising in a neovagina. GynecolOncol 52: 272-275. 1942. Munn KE, Walker RA, Varley JM(1995). Frequent alterations of chromo-some 1 in ductal carcinoma in situ of thebreast. Oncogene 10: 1653-1657. 1943. Munoz N, Franceschi S, Bosetti C,Moreno V, Herrero R, Shah KV, Smith J,Meijer CJ, for the IARC Multi-centreCervical Cancer Study Group (2001). Therole of parity and HPV in cervical cancer:The IARC multi-centric cas-control study.Lancet .1944. Munoz N, Franceschi S, Bosetti C,Moreno V, Herrero R, Smith JS, Shah KV,Meijer CJ, Bosch FX (2002). Role of parityand human papillomavirus in cervical can-cer: the IARC multicentric case-controlstudy. Lancet 359: 1093-1101. 1945. Murad TM, Contesso G, Mouriesse H(1981). Papillary tumors of large lactiferousducts. Cancer 48: 122-133. 1946. Murao T, Nakai M, Hamada E (1986).[Intravascular papillary endothelial hyper-plasia of the breast--report of a case withscanning electron microscopic observa-tions]. Gan No Rinsho 32: 1471-1474. 1947. Murase E, Siegelman ES, OutwaterEK, Perez-Jaffe LA, Tureck RW (1999).Uterine leiomyomas: histopathologic fea-tures, MR imaging findings, differentialdiagnosis, and treatment. Radiographics19: 1179-1197. 1948. Murayama Y, Yamamoto Y,Shimojima N, Takahara T, Kikuchi K, Iida S,Kondo Y (1999). T1 Breast CancerAssociated with Von Recklinghausen'sNeurofibromatosis. Breast Cancer 6: 227-230. 1949. Murphy DS, Hoare SF, Going JJ,Mallon EE, George WD, Kaye SB, Brown R,Black DM, Keith WN (1995).Characterization of extensive geneticalterations in ductal carcinoma in situ byfluorescence in situ hybridization andmolecular analysis. J Natl Cancer Inst 87:1694-1704. 1950. Murphy GF, Elder DE (1991). Non-melanocytic Tumors of the Skin. Atlas ofTumor Pathology, 3rd series, Fascicle 1AFIP: Washington,D.C.1951. Musgrave MA, Aronson KJ, Narod S,Hanna W, Miller AB, McCready DR (1998).Breast cancer and organochlorines: amarker for susceptibility? Surg Oncol 7: 1-4.
1952. Mussurakis S, Carleton PJ, TurnbullLW (1997). MR imaging of primary non-Hodgkin's breast lymphoma. A case report.Acta Radiol 38: 104-107. 1953. Muto MG, Lage JM, Berkowitz RS,Goldstein DP, Bernstein MR (1991).Gestational trophoblastic disease of thefallopian tube. J Reprod Med 36: 57-60. 1954. Muto MG, Welch WR, Mok SC,Bandera CA, Fishbaugh PM, Tsao SW, LauCC, Goodman HM, Knapp RC, Berkowitz RS(1995). Evidence for a multifocal origin ofpapillary serous carcinoma of the peri-toneum. Cancer Res 55: 490-492. 1955. Mutter GL (2000). Endometrialintraepithelial neoplasia (EIN): will it bringorder to chaos? The EndometrialCollaborative Group. Gynecol Oncol 7 6 :287-290. 1956. Mutter GL (2000). Histopathology ofgenetically defined endometrial precan-cers. Int J Gynecol Pathol 19: 301-309. 1957. Mutter GL (2001). Pten, a proteantumor suppressor. Am J Pathol 158: 1895-1898. 1958. Mutter GL, Baak JP, Crum CP, RichartRM, Ferenczy A, Faquin WC (2000).Endometrial precancer diagnosis byhistopathology, clonal analysis, and com-puterized morphometry. J Pathol 190: 462-469. 1959. Mutter GL, Ince TA, Baak JP, KustGA, Zhou XP, Eng C (2001). Molecular iden-tification of latent precancers in histologi-cally normal endometrium. Cancer Res 61:4311-4314. 1960. Myles JL, Hart WR (1985). Apoplecticleiomyomas of the uterus. A clinicopatho-logic study of five distinctive hemorrhagicleiomyomas associated with oral contra-ceptive usage. Am J Surg Pathol 9: 798-805. 1961. Naganawa S, Endo T, Aoyama H,Ichihara S (1996). MR lmaging of thePrimary Breast Lymphoma: A Case Report.Breast Cancer 3: 209-213. 1962. Nagasaki K, Maass N, Manabe T,Hanzawa H, Tsukada T, Kikuchi K,Yamaguchi K (1999). Identification of anovel gene, DAM1, amplified at chromo-some 1p13.3-21 region in human breastcancer cell lines. Cancer Lett 140: 219-226. 1963. Nagle RB, Bocker W, Davis JR, HeidHW, Kaufmann M, Lucas DO, Jarasch ED(1986). Characterization of breast carcino-mas by two monoclonal antibodies distin-guishing myoepithelial from luminal epithe-lial cells. J Histochem Cytochem 3 4 :869-881. 1964. Nakagawa S, Yoshikawa H, KimuraM, Kawana K, Matsumoto K, Onda T, KinoN, Yamada M, Yasugi T, Taketani Y (1999).A possible involvement of aberrant expres-sion of the FHIT gene in the carcinogene-sis of squamous cell carcinoma of the uter-ine cervix. Br J Cancer 79: 589-594. 1965. Nakamura Y, Nakashima T,Nakashima H, Hashimoto T (1981). Bilateralcystic nephroblastomas and botryoid sar-coma involving vagina and urinary bladderin a child with microcephaly, arhinen-cephaly, and bilateral cataracts. Cancer48: 1012-1015. 1966. Nakanishi T, Wakai K, Ishikawa H,Nawa A, Suzuki Y, Nakamura S, Kuzuya K(2001). A comparison of ovarian metastasisbetween squamous cell carcinoma andadenocarcinoma of the uterine cervix.Gynecol Oncol 82: 504-509.
1967. Nakano T, Oka K, Ishikawa A, MoritaS (1997). Correlation of cervical carcinomac-erb B-2 oncogene with cell proliferationparameters in patients treated with radia-tion therapy for cervical carcinoma.Cancer 79: 513-520. 1968. Nakashima N, Fukatsu T, NagasakaT, Sobue M, Takeuchi J (1987). The fre-quency and histology of hepatic tissue ingerm cell tumors. Am J Surg Pathol 11:682-692. 1969. Nakashima N, Murakami S, FukatsuT, Nagasaka T, Fukata S, Ohiwa N, Nara Y,Sobue M, Takeuchi J (1988).Characteristics of "embryoid body" inhuman gonadal germ cell tumors. HumPathol 19: 1144-1154. 1970. Nakashima N, Nagasaka T, Fukata S,Oiwa N, Nara Y, Fukatsu T, Takeuchi J(1990). Study of ovarian tumors treated atNagoya University Hospital, 1965-1988.Gynecol Oncol 37: 103-111. 1971. Nakashima N, Young RH, Scully RE(1984). Androgenic granulosa cell tumorsof the ovary. A clinicopathologic analysisof 17 cases and review of the literature.Arch Pathol Lab Med 108: 786-791. 1972. Nanbu K, Konishi I, Yamamoto S,Koshiyama M, Mandai M, Komatsu T, Li W,Tokushige M, Higuchi K, Mori T (1995).Minimal deviation adenocarcinoma ofendometrioid type may arise in the isth-mus: clinicopathological and immunohisto-chemical study of two cases. G y n e c o lOncol 58: 136-141. 1973. Naresh KN, Ahuja VK, Rao CR,Mukherjee G, Bhargava MK (1991).Squamous cell carcinoma arising inendometriosis of the ovary. J Clin Pathol44: 958-959. 1974. Narod S, Tonin P, Lynch H, Watson P,Feunteun J, Lenoir G (1994). Histology ofBRCA1-associated ovarian tumours.Lancet 343: 236. 1975. Narod SA (2002). Modifiers of risk ofhereditary breast and ovarian cancer. NatRev Cancer 2: 113-123. 1976. Narod SA, Brunet JS, Ghadirian P,Robson M, Heimdal K, Neuhausen SL,Stoppa-Lyonnet D, Lerman C, Pasini B, delos Rios P, Weber B, Lynch H (2000).Tamoxifen and risk of contralateral breastcancer in BRCA1 and BRCA2 mutation car-riers: a case-control study. HereditaryBreast Cancer Clinical Study Group.Lancet 356: 1876-1881. 1977. Narod SA, Dube MP, Klijn J, LubinskiJ, Lynch HT, Ghadirian P, Provencher D,Heimdal K, Moller P, Robson M, Offit K,Isaacs C, Weber B, Friedman E, Gershoni-Baruch R, Rennert G, Pasini B, Wagner T,Daly M, Garber JE, Neuhausen SL,Ainsworth P, Olsson H, Evans G, OsborneM, Couch F, Foulkes WD, Warner E, Kim-Sing C, Olopade O, Tung N, Saal HM,Weitzel J, Merajver S, Gauthier-Villars M,Jernstrom H, Sun P, Brunet JS (2002). Oralcontraceptives and the risk of breast can-cer in BRCA1 and BRCA2 mutations carri-ers. J Natl Cancer Inst 94: 1773-1779. 1978. Narod SA, Goldgar D, Cannon-Albright L, Weber B, Moslehi R, Ives E,Lenoir G, Lynch H (1995). Risk modifiers incarriers of BRCA1 mutations. Int J Cancer64: 394-398. 1979. Narod SA, Risch H, Moslehi R, DorumA, Neuhausen S, Olsson H, Provencher D,Radice P, Evans G, Bishop S, Brunet JS,Ponder BA (1998). Oral contraceptives andthe risk of hereditary ovarian cancer.Hereditary Ovarian Cancer Clinical StudyGroup. N Engl J Med 339: 424-428.
1980. Narod SA, Sun P, Ghadirian P, LynchH, Isaacs C, Garber J, Weber B, Karlan B,Fishman D, Rosen B, Tung N, NeuhausenSL (2001). Tubal ligation and risk of ovariancancer in carriers of BRCA1 or BRCA2mutations: a case-control study. Lancet357: 1467-1470. 1981. Nascimento AG, Karas M, Rosen PP,Caron AG (1979). Leiomyoma of the nipple.Am J Surg Pathol 3: 151-154. 1982. Nassar H, Wallis T, Andea A, Dey J,Adsay V, Visscher D (2001).Clinicopathologic analysis of invasivemicropapillary differentiation in breast car-cinoma. Mod Pathol 14: 836-841. 1983. Nasu M, Inoue J, Matsui M, MinouraS, Matsubara O (2000). Ovarianleiomyosarcoma: an autopsy case report.Pathol Int 50: 162-165. 1984. National Co-ordinating Group forBreast Screening Pathology (1995).Pathology Reporting. In: Breast ScreeningPathology, Breast Screening Pathology,2nd ed. ed. NHSBSP Publications.1 9 8 5 . Navani SS, Alvarado-Cabrero I,Young RH, Scully RE (1996). Endometrioidcarcinoma of the fallopian tube: a clinico-pathologic analysis of 26 cases. GynecolOncol 63: 371-378. 1986. Naves AE, Monti JA, Chichoni E(1980). Basal cell-like carcinoma in theupper third of the vagina. Am J ObstetGynecol 137: 136-137. 1987. Nayar R, Siriaunkgul S, Robbins KM,McGowan L, Ginzan S, Silverberg SG(1996). Microinvasion in low malignantpotential tumors of the ovary. Hum Pathol27: 521-527. 1988. Nayar R, Zhuang Z, Merino MJ,Silverberg SG (1997). Loss of heterozygosi-ty on chromosome 11q13 in lobular lesionsof the breast using tissue microdissectionand polymerase chain reaction. H u mPathol 28: 277-282. 1989. Nelen MR, Kremer H, Konings IB,Schoute F, van Essen AJ, Koch R, WoodsCG, Fryns JP, Hamel B, Hoefsloot LH,Peeters EA, Padberg GW (1999). NovelPTEN mutations in patients with Cowdendisease: absence of clear genotype-phe-notype correlations. Eur J Hum Genet 7:267-273. 1990. Nelen MR, Padberg GW, Peeters EA,Lin AY, van den Helm B, Frants RR, CoulonV, Goldstein AM, van Reen MM, Easton DF,Eeles RA, Hodgsen S, Mulvihill JJ, MurdayVA, Tucker MA, Mariman EC, Starink TM,Ponder BA, Ropers HH, Kremer H, LongyM, Eng C (1996). Localization of the genefor Cowden disease to chromosome10q22-23. Nat Genet 13: 114-116. 1991. Nelen MR, van Staveren WC, PeetersEA, Hassel MB, Gorlin RJ, Hamm H,Lindboe CF, Fryns JP, Sijmons RH, WoodsDG, Mariman EC, Padberg GW, Kremer H(1997). Germline mutations in thePTEN/MMAC1 gene in patients withCowden disease. Hum Mol Genet 6: 1383-1387. 1992. Nelson CL, Sellers TA, Rich SS, PotterJD, McGovern PG, Kushi LH (1993). Familialclustering of colon, breast, uterine, andovarian cancers as assessed by family his-tory. Genet Epidemiol 10: 235-244. 1993. Nemoto T, Castillo N, Tsukada Y, KoulA, Eckhert KH Jr., Bauer RL (1998). Lobularcarcinoma in situ with microinvasion. JSurg Oncol 67: 41-46. 1994. Nesland JM, Holm R, JohannessenJV (1985). Ultrastructural and immunohis-tochemical features of lobular carcinomaof the breast. J Pathol 145: 39-52.

404 References
1995. Nesland JM, Lunde S, Holm R,Johannessen JV (1987). Electronmicroscopy and immunostaining of thenormal breast and its benign lesions. Asearch for neuroendocrine cells. H i s t o lHistopathol 2: 73-77. 1 9 9 6 . Neubecker RD, Breen JL (1962).Gynandroblastoma. A report of five caseswith a discussion of the histogenesis ansclassification of ovarian tumours. Am JClin Pathol 38: 60-69. 1997. Neuhausen SL, Godwin AK,Gershoni-Baruch R, Schubert E, Garber J,Stoppa-Lyonnet D, Olah E, Csokay B,Serova O, Lalloo F, Osorio A, Stratton M,Offit K, Boyd J, Caligo MA, Scott RJ,Schofield A, Teugels E, Schwab M,Cannon-Albright L, Bishop T, Easton D,Benitez J, King MC, Ponder BAJ, Weber B,Devilee P, Borg A, Narod SA, Goldgar D.(1998). Haplotype and phenotype analysisof nine recurrent BRCA2 mutations in 111families: results of an international study.Am J Hum Genet 62: 1381-1388. 1998. Nevin J, Laing D, Kaye P, McCullochT, Barnard R, Silcocks P, Blackett T,Paterson M, Sharp F, Cruse P (1999). Thesignificance of Erb-b2 immunostaining incervical cancer. Gynecol Oncol 73: 354-358. 1999. Newcomer JR (1998). Ampullarytubal hydatidiform mole treated with linearsalpingotomy. A case report. J ReprodMed 43: 913-915. 2000. Newman PL, Fletcher CD (1991).Smooth muscle tumours of the externalgenitalia: clinicopathological analysis of aseries. Histopathology 18: 523-529. 2001. Newman W (1966). Lobular carcino-ma of the female breast. Report of 73cases. Ann Surg 164: 305-314. 2002. Newton WA Jr., Gehan EA, WebberBL, Marsden HB, van Unnik AJ, HamoudiAB, Tsokos MG, Shimada H, Harms D,Schmidt D, Ninfo V, Cavazzana AO,Gonzalezcrussi F, Parham DM, ReimanHM, Asmar L, Beltangady MS, Sachs NE,Triche TJ, Maurer HM. (1995).Classification of rhabdomyosarcomas andrelated sarcomas. Pathologic aspects andproposal for a new classification--anIntergroup Rhabdomyosarcoma Study.Cancer 76: 1073-1085.2003. Ng WK (2001). Fine needle aspirationcytology of invasive cribriform carcinomaof the breast with osteoclastlike giantcells: a case report. Acta Cytol 45: 593-598. 2004. Ngan HY, Liu SS, Yu H, Liu KL, CheungAN (1999). Proto-oncogenes and p53 pro-tein expression in normal cervical strati-fied squamous epithelium and cervicalintra-epithelial neoplasia. Eur J Cancer 35:1546-1550. 2005. Nguyen NP, Sallah S, Karlsson U, VosP, Ludin A, Semer D, Tait D, Salehpour M,Jendrasiak G, Robiou C (2001). Prognosisfor papillary serous carcinoma of theendometrium after surgical staging. Int JGynecol Cancer 11: 305-311. 2006. Ngwalle KE, Hirakawa T, TsuneyoshiM, Enjoji M (1990). Osteosarcoma arising ina benign dermoid cyst of the ovary.Gynecol Oncol 37: 143-147. 2007. Nichols GE, Mills SE, Ulbright TM,Czernobilsky B, Roth LM (1991). Spindlecell mural nodules in cystic ovarian muci-nous tumors. A clinicopathologic andimmunohistochemical study of five cases.Am J Surg Pathol 15: 1055-1062.
2008. Nicolaides NC, Carter KC, Shell BK,Papadopoulos N, Vogelstein B, Kinzler KW(1995). Genomic organization of the humanPMS2 gene family. Genomics 30: 195-206. 2009. Nicolaides NC, Palombo F, KinzlerKW, Vogelstein B, Jiricny J (1996).Molecular cloning of the N-terminus ofGTBP. Genomics 31: 395-397. 2010. Nicolaides NC, Papadopoulos N, LiuB, Wei YF, Carter KC, Ruben SM, Rosen CA,Haseltine WA, Fleischmann RD, FraserCM, Adams MD, Venter JC, Dunlop MG,Hamilton SR, Petersen GM, de la ChapelleA, Vogelstein B, Kinzler KW. (1994).Mutations of two PMS homologues inhereditary nonpolyposis colon cancer.Nature 371: 75-80. 2011. Niehans GA, Manivel JC, Copland GT,Scheithauer BW, Wick MR (1988).Immunohistochemistry of germ cell andtrophoblastic neoplasms. Cancer 62: 1113-1123. 2012. Nielsen AL, Nyholm HC, Engel P(1994). Expression of MIB-1 (paraffin ki-67)and AgNOR morphology in endometrialadenocarcinomas of endometrioid type.Int J Gynecol Pathol 13: 37-44. 2013. Nielsen BB (1981). Oncocytic breastpapilloma. Virchows Arch A Pathol Anat393: 345-351. 2014. Nielsen BB (1984). Leiomyosarcomaof the breast with late dissemination.Virchows Arch A Pathol Anat Histopathol403: 241-245. 2015. Nielsen BB (1987). Adenosis tumourof the breast--a clinicopathological inves-tigation of 27 cases. Histopathology 11:1259-1275. 2016. Nielsen BB, Holm-Nielsen P, KiaerHR (1993). Microglandular adenosis of thebreast concomitant with secretory carci-noma. Pathol Res Pract 189: 769. 2017. Nielsen GP, Oliva E, Young RH,Rosenberg AE, Dickersin GR, Scully RE(1995). Alveolar soft-part sarcoma of thefemale genital tract: a report of nine casesand review of the literature. Int J GynecolPathol 14: 283-292. 2018. Nielsen GP, Oliva E, Young RH,Rosenberg AE, Prat J, Scully RE (1998).Primary ovarian rhabdomyosarcoma: areport of 13 cases. Int J Gynecol Pathol 17:113-119. 2019. Nielsen GP, Rosenberg AE, YoungRH, Dickersin GR, Clement PB, Scully RE(1996). Angiomyofibroblastoma of the vulvaand vagina. Mod Pathol 9: 284-291. 2020. Nielsen GP, Young RH (2001).Mesenchymal tumors and tumor-likelesions of the female genital tract: a selec-tive review with emphasis on recentlydescribed entities. Int J Gynecol Pathol 20:105-127. 2021. Nielsen GP, Young RH, Prat J, ScullyRE (1997). Primary angiosarcoma of theovary: a report of seven cases and reviewof the literature. Int J Gynecol Pathol 16:378-382. 2022. Nielsen M, Andersen JA, HenriksenFW, Kristensen PB, Lorentzen M, Ravn V,Schiodt T, Thorborg JV, Ornvold K (1981).Metastases to the breast from extramam-mary carcinomas. Acta Pathol MicrobiolScand [A] 89: 251-256. 2023. Nielsen VT, Andreasen C (1987).Phyllodes tumour of the male breast.Histopathology 11: 761-762. 2024. Nirmul D, Pegoraro RJ, Jialal I,Naidoo C, Joubert SM (1983). The sex hor-mone profile of male patients with breastcancer. Br J Cancer 48: 423-427.
2024 a. Nishikawa Y, Kaseki S, Tomoda Y,Ishizuka T, Asai Y, Suzuki T, Ushijima H(1985). Histopathologic classification ofuterine choriocarcinoma. Cancer 55: 1044-1051. 2 0 2 5 . Nishimori H, Sasaki M, Hirata K,Zembutsu H, Yasoshima T, Fukui R,Kobayashi K (2000). Tubular adenoma ofthe breast in a 73-year-old woman. BreastCancer 7: 169-172. 2026. Nishioka T, West CM, Gupta N, WilksDP, Hendry JH, Davidson SE, Hunter RD(1999). Prognostic significance of c-erbB-2protein expression in carcinoma of thecervix treated with radiotherapy. J CancerRes Clin Oncol 125: 96-100. 2027. Nishizaki T, Chew K, Chu L, Isola J,Kallioniemi A, Weidner N, Waldman FM(1997). Genetic alterations in lobular breastcancer by comparative genomic hybridiza-tion. Int J Cancer 74: 513-517. 2028. Nishizaki T, Devries S, Chew K,Goodson WH, III, Ljung BM, Thor A,Waldman FM (1997). Genetic alterations inprimary breast cancers and their metas-tases: direct comparison using modifiedcomparative genomic hybridization. GenesChromosomes Cancer 19: 267-272. 2029. Nixon AJ, Neuberg D, Hayes DF,Gelman R, Connolly JL, Schnitt S, Abner A,Recht A, Vicini F, Harris JR (1994).Relationship of patient age to pathologicfeatures of the tumor and prognosis forpatients with stage I or II breast cancer. JClin Oncol 12: 888-894. 2 0 3 0 . Nixon AJ, Schnitt SJ, Gelman R,Gage I, Bornstein B, Hetelekidis S, Recht A,Silver B, Harris JR, Connolly JL (1996).Relationship of tumor grade to other patho-logic features and to treatment outcome ofpatients with early stage breast carcinomatreated with breast-conserving therapy.Cancer 78: 1426-1431. 2031. Nobukawa B, Fujii H, Hirai S,Kumasaka T, Shimizu H, Matsumoto T,Suda K, Futagawa S (1999). Breast carci-noma diverging to aberrant melanocyticdifferentiation: a case report withhistopathologic and loss of heterozygosityanalyses. Am J Surg Pathol 23: 1280-1287. 2032. Nogales-Fernandez F, Silverberg SG,Bloustein PA, Martinez-Hernandez A,Pierce GB (1977). Yolk sac carcinoma(endodermal sinus tumor): ultrastructureand histogenesis of gonadal and extrago-nadal tumors in comparison with normalhuman yolk sac. Cancer 39: 1462-1474. 2033. Nogales-Ortiz F, Puerta J, Nogales FFJr. (1978). The normal menstrual cycle.Chronology and mechanism of endometrialdesquamation. Obstet Gynecol 51: 259-264. 2 0 3 4 . Nogales FF, Isaac MA (2002).Functioning uterine sex cord tumour.Histopathology 41: 277-279. 2035. Nogales FF (1993). Embryologic cluesto human yolk sac tumors: a review. Int JGynecol Pathol 12: 101-107. 2036. Nogales FF (1995). Mesonephric(Wolffian) Tumours of the Female GenitalTract : is Mesonephric Histogenesis aMirage and a Trap ? Current Diagn Pathol2: 94-100. 2037. Nogales FF, Ayala A, Ruiz-Avila I,Sirvent JJ (1991). Myxoid leiomyosarcomaof the ovary: analysis of three cases. HumPathol 22: 1268-1273. 2038. Nogales FF, Beltran E, Pavcovich M(1993). Pathology of ovarian yolk sactumours. In: The Human Yolk Sac and YolkSac Tumours, FF Nogales (ed.), Springer-Verlag: Berlin , pp. 228-244.
2039. Nogales FF, Bergeron C, Carvia RE,Alvaro T, Fulwood HR (1996). Ovarianendometrioid tumors with yolk sac tumorcomponent, an unusual form of ovarianneoplasm. Analysis of six cases. Am JSurg Pathol 20: 1056-1066. 2040. Nogales FF, Carvia RE, Donne C,Campello TR, Vidal M, Martin A (1997).Adenomas of the rete ovarii. Hum Pathol28: 1428-1433. 2041. Nogales FF, Isaac MA, Hardisson D,Bosincu L, Palacios J, Ordi J, Mendoza E,Manzarbeitia F, Olivera H, O'Valle F,Krasevic M, Marquez M (2002).Adenomatoid tumors of the uterus: ananalysis of 60 cases. Int J Gynecol Pathol21: 34-40. 2042. Nogales FF, Ruiz A, I, Concha A, delMoral E (1993). Immature endodermal ter-atoma of the ovary: embryologic correla-tions and immunohistochemistry. H u mPathol 24: 364-370. 2043. Nogales FF Jr., Matilla A, NogalesOrtiz F, Galera-Davidson H (1978). Yolk sactumors with pure and mixed polyvesicularvitelline patterns. Hum Pathol 9: 553-566. 2044. Nogueira M, Andre S, Mendonca E(1998). Metaplastic carcinomas of thebreast--fine needle aspiration (FNA) cytol -ogy findings. Cytopathology 9: 291-300. 2045. Nola M, Babic D, Ilic J, Marusic M,Uzarevic B, Petrovecki M, Sabioncello A,Kovac D, Jukic S (1996). Prognostic param-eters for survival of patients with malig-nant mesenchymal tumors of the uterus.Cancer 78: 2543-2550. 2046. Noller KL (1993). Role of colposcopyin the examination of diethylstilbestrol-exposed women. Obstet Gynecol ClinNorth Am 20: 165-176. 2047. Nomura K, Aizawa S (2000).Noninvasive, microinvasive, and invasivemucinous carcinomas of the ovary: a clini-copathologic analysis of 40 cases. Cancer89: 1541-1546. 2048. Nordal RN, Kjorstad KE, Stenwig AE,Trope CG (1993). Leiomyosarcoma (LMS)and endometrial stromal sarcoma (ESS) ofthe uterus. A survey of patients treated inthe Norwegian Radium Hospital 1976-1985.Int J Gynecol Cancer 3: 110-115. 2049. Nordal RR, Kristensen GB, Kaern J,Stenwig AE, Pettersen EO, Trope CG (1995).The prognostic significance of stage,tumor size, cellular atypia and DNA ploidyin uterine leiomyosarcoma. Acta Oncol 34:797-802. 2050. Norris HJ, Hilliard GD, Irey NS (1988).Hemorrhagic cellular leiomyomas("apoplectic leiomyoma") of the uterusassociated with pregnancy and oral con-traceptives. Int J Gynecol Pathol 7: 212-224. 2051. Norris HJ, Parmley T (1975).Mesenchymal tumors of the uterus. V.Intravenous leiomyomatosis. A clinical andpathologic study of 14 cases. Cancer 36:2164-2178. 2 0 5 2 . Norris HJ, Robinowitz M (1971).Ovarian adenocarcinoma of mesonephrictype. Cancer 28: 1074-1081. 2053. Norris HJ, Taylor HB (1965).Prognosis of mucinous (gelatinous) carci-noma of the breast. Cancer 18: 879-885. 2054. Norris HJ, Taylor HB (1966).Mesenchymal tumors of the uterus. I. Aclinical and pathological study of 53endometrial stromal tumors. Cancer 1 9 :755-766. 2055. Norris HJ, Taylor HB (1966). Polyps ofthe vagina. A benign lesion resemblingsarcoma botryoides. Cancer 19: 227-232.

405References
2056. Norris HJ, Taylor HB (1967). Nodulartheca-lutein hyperplasia of pregnancy (so-called "pregnancy luteoma"). A clinical andpathologic study of 15 cases. Am J ClinPathol 47: 557-566. 2057. Norris HJ, Taylor HB (1967).Relationship of histologic features tobehavior of cystosarcoma phyllodes.Analysis of ninety-four cases. Cancer 20:2090-2099. 2058. Norris HJ, Taylor HB (1968).Prognosis of granulosa-theca tumors ofthe ovary. Cancer 21: 255-263. 2059. Norris HJ, Taylor HB (1969).Virilization associated with cystic granu-losa tumors. Obstet Gynecol 34: 629-635. 2060. Norris HJ, Zirkin HJ, Benson WL(1976). Immature (malignant) teratoma ofthe ovary: a clinical and pathologic studyof 58 cases. Cancer 37: 2359-2372. 2061. Nucci MR, Clement PB, Young RH(1999). Lobular endocervical glandularhyperplasia, not otherwise specified: aclinicopathologic analysis of thirteencases of a distinctive pseudoneoplasticlesion and comparison with fourteencases of adenoma malignum. Am J SurgPathol 23: 886-891. 2062. Nucci MR, Fletcher CD (1998).Liposarcoma (atypical lipomatous tumors)of the vulva: a clinicopathologic study ofsix cases. Int J Gynecol Pathol 17: 17-23. 2063. Nucci MR, Granter SR, Fletcher CD(1997). Cellular angiofibroma: a benignneoplasm distinct from angiomyofibroblas-toma and spindle cell lipoma. Am J SurgPathol 21: 636-644. 2064. Nucci MR, Krausz T, Lifschitz-MercerB, Chan JK, Fletcher CD (1998).Angiosarcoma of the ovary: clinicopatho-logic and immunohistochemical analysis offour cases with a broad morphologic spec-trum. Am J Surg Pathol 22: 620-630. 2065. Nucci MR, O'Connell JT, HuettnerPC, Cviko A, Sun D, Quade BJ (2001). h-Caldesmon expression effectively distin-guishes endometrial stromal tumors fromuterine smooth muscle tumors. Am J SurgPathol 25: 455-463. 2 0 6 6 . Nucci MR, Prasad CJ, Crum CP,Mutter GL (1999). Mucinous endometrialepithelial proliferations: a morphologicspectrum of changes with diverse clinicalsignificance. Mod Pathol 12: 1137-1142. 2067. Nucci MR, Young RH, Fletcher CD(2000). Cellular pseudosarcomatousfibroepithelial stromal polyps of the lowerfemale genital tract: an underrecognizedlesion often misdiagnosed as sarcoma. AmJ Surg Pathol 24: 231-240. 2068. Nuovo J, Melnikow J, Willan AR,Chan BK (2000). Treatment outcomes forsquamous intraepithelial lesions. Int JGynaecol Obstet 68: 25-33. 2069. Nuovo MA, Nuovo GJ, Smith D, LewisSH (1990). Benign mesenchymoma of theround ligament. A report of two cases withimmunohistochemistry. Am J Clin Pathol93: 421-424. 2070. Nystrom-Lahti M, Kristo P,Nicolaides NC, Chang SY, Aaltonen LA,Moisio AL, Jarvinen HJ, Mecklin JP,Kinzler KW, Vogelstein B, de la Chapelle A,Peltomaki P. (1995). Founding mutationsand Alu-mediated recombination in hered-itary colon cancer. Nat Med 1: 1203-1206. 2071. O'Connell P, Pekkel V, Fuqua SA,Osborne CK, Clark GM, Allred DC (1998).Analysis of loss of heterozygosity in 399premalignant breast lesions at 15 geneticloci. J Natl Cancer Inst 90: 697-703.
2072. O'Connor DM, Norris HJ (1994). Theinfluence of grade on the outcome of stageI ovarian immature (malignant) teratomasand the reproducibility of grading. Int JGynecol Pathol 13: 283-289. 2073. O'Connor IF, Shembekar MV,Shousha S (1998). Breast carcinoma devel-oping in patients on hormone replacementtherapy: a histological and immunohisto-logical study. J Clin Pathol 51: 935-938. 2074. O'Hara MF, Page DL (1985).Adenomas of the breast and ectopicbreast under lactational influences. HumPathol 16: 707-712. 2075. Obata K, Morland SJ, Watson RH,Hitchcock A, Chenevix-Trench G, ThomasEJ, Campbell IG (1998). FrequentPTEN/MMAC mutations in endometrioidbut not serous or mucinous epithelial ovar-ian tumors. Cancer Res 58: 2095-2097. 2076. Obata N, Sasaki A, Takeuchi S,Ishiguro Y (1987). Clinico-pathologic studyon the early diagnosis of cervical adeno-carcinoma. Nippon Sanka Fujinka GakkaiZasshi 39: 771-776. 2077. Obata NH, Nakashima N, Kawai M,Kikkawa F, Mamba S, Tomoda Y (1995).Gonadoblastoma with dysgerminoma inone ovary and gonadoblastoma with dys-germinoma and yolk sac tumor in the con-tralateral ovary in a girl with 46XX kary-otype. Gynecol Oncol 58: 124-128. 2077a. Ober WB, Edgcomb JH, Price EB Jr.(1971). The pathology of choriocarcinoma.Ann N Y Acad Sci 172: 299-426. 2078. Ober WB, Maier RC (1981).Gestational choriocarcinoma of the fallop -ian tube. Diagn Gynecol Obstet 3: 213-231. 2079. Oberman HA (1965). Cystosarcomaphyllodes. A clinicopathological study ofhypercellular periductal stromal neo-plasms of breast. Cancer 18: 697-710. 2080. Oberman HA (1980). Secretory carci -noma of the breast in adults. Am J SurgPathol 4: 465-470. 2081. Oberman HA, Fidler WJ Jr. (1979).Tubular carcinoma of the breast. Am JSurg Pathol 3: 387-395. 2082. Ockner DM, Sayadi H, Swanson PE,Ritter JH, Wick MR (1997). Genitalangiomyofibroblastoma. Comparison withaggressive angiomyxoma and other myx-oid neoplasms of skin and soft tissue. AmJ Clin Pathol 107: 36-44. 2083. Oddoux C, Struewing JP, Clayton CM,Neuhausen S, Brody LC, Kaback M, HaasB, Norton L, Borgen P, Jhanwar S, GoldgarD, Ostrer H, Offit K (1996). The carrier fre-quency of the BRCA2 6174delT mutationamong Ashkenazi Jewish individuals isapproximately 1%. Nat Genet 14: 188-190. 2 0 8 4 . Offit K, Pierce H, Kirchhoff T,Kolachana P, Rapaport B, Gregersen P,Johnson S, Yossepowitch O, Huang H,Satagopan J, Robson M, Scheuer L, NafaK, Ellis N (2003). Frequency ofCHEK2*1100delC in New York breast can-cer cases and controls. BMC Med Genet4: 1. 2085. Ogawa K, Johansson SL, Cohen SM(1999). Immunohistochemical analysis ofuroplakins, urothelial specific proteins, inovarian Brenner tumors, normal tissues,and benign and neoplastic lesions of thefemale genital tract. Am J Pathol 155: 1047-1050. 2086. Ohgaki H, Hernandez T, Kleihues P,Hainaut P (1999). p53 germline mutationsand the molecular basis of Li-Fraumenisyndrome. In: Molecular Biology in CancerMedicine, R Kurzrock, M Talpaz (eds.), 2nded. Martin Dunitz: London, pp. 477-492.
2087. Ohgaki H, Vital A, Kleihues P, HainautP (2000). Familial tumour syndromes involv-ing the nervous system. Li-Fraumeni syn-drome and TP53 germline mutations. In:WHO Classification of Tumours. Pathologyand Genetics of the Tumours of theNervous System., P Kleihues, WK Cavenee(eds.), 1st ed. IARC Press: Lyon, France,pp. 231-234.2088. Ohnishi T, Watanabe S (2000). Theuse of cytokeratins 7 and 20 in the diagno-sis of primary and secondary extramam-mary Paget's disease. Br J Dermatol 142:243-247. 2 0 8 9 . Ohtake T, Abe R, Kimijima I,Fukushima T, Tsuchiya A, Hoshi K, WakasaH (1995). Intraductal extension of primaryinvasive breast carcinoma treated bybreast-conservative surgery. Computergraphic three-dimensional reconstructionof the mammary duct-lobular systems.Cancer 76: 32-45. 2090. Ohuchi N (1999). Breast-conservingsurgery for invasive cancer: a principlebased on segmental anatomy. Tohoku JExp Med 188: 103-118. 2091. Ohuchi N, Abe R, Kasai M (1984).Possible cancerous change of intraductalpapillomas of the breast. A 3-D reconstruc-tion study of 25 cases. Cancer 54: 605-611. 2 0 9 2 . Ohuchi N, Abe R, Takahashi T,Tezuka F (1984). Origin and extension ofintraductal papillomas of the breast: athree-dimensional reconstruction study.Breast Cancer Res Treat 4: 117-128. 2093. Ohuchi N, Furuta A, Mori S (1994).Management of ductal carcinoma in situwith nipple discharge. Intraductal spread-ing of carcinoma is an unfavorable patho-logic factor for breast-conserving surgery.Cancer 74: 1294-1302. 2 0 9 4 . Oka H, Shiozaki H, Kobayashi K,Inoue M, Tahara H, Kobayashi T,Takatsuka Y, Matsuyoshi N, Hirano S,Takeichi M, Mori T (1993). Expression of E-cadherin cell adhesion molecules inhuman breast cancer and its relationshipto metastasis. Cancer Res 53: 1696-1701. 2095. Okagaki T, Ishida T, Hilgers RD (1976).A malignant tumor of the vagina resem-bling synovial sarcoma: a light and elec-tron microscopic study. Cancer 37: 2306-2320. 2096. Olah KS, Dunn JA, Gee H (1992).Leiomyosarcomas have a poorer progno-sis than mixed mesodermal tumours whenadjusting for known prognostic factors: theresult of a retrospective study of 423 casesof uterine sarcoma. Br J Obstet Gynaecol99: 590-594. 2097. Oliva E, Clement PB, Young RH (2000).Endometrial stromal tumors: an update ona group of tumors with a protean pheno-type. Adv Anat Pathol 7: 257-281. 2098. Oliva E, Clement PB, Young RH, ScullyRE (1998). Mixed endometrial stromal andsmooth muscle tumors of the uterus: a clin-icopathologic study of 15 cases. Am JSurg Pathol 22: 997-1005. 2099. Oliva E, Ferry JA, Young RH, Prat J,Srigley JR, Scully RE (1997). Granulocyticsarcoma of the female genital tract: a clin-icopathologic study of 11 cases. Am JSurg Pathol 21: 1156-1165. 2100. Oliva E, Musulen E, Prat J, Young RH(1995). Transitional cell carinoma of therenal pelvis with symptomatic ovarianmetastases. Int J Surg Pathol 2: 231-236.
2101. Oliva E, Young RH, Clement PB, BhanAK, Scully RE (1995). Cellular benign mes-enchymal tumors of the uterus. A compar-ative morphologic and immunohistochemi-cal analysis of 33 highly cellularleiomyomas and six endometrial stromalnodules, two frequently confused tumors.Am J Surg Pathol 19: 757-768. 2102. Oliva E, Young RH, Clement PB, ScullyRE (1999). Myxoid and fibrous endometrialstromal tumors of the uterus: a report of 10cases. Int J Gynecol Pathol 18: 310-319. 2103. Olive DL, Lurain JR, Brewer JI (1984).Choriocarcinoma associated with termgestation. Am J Obstet Gynecol 148: 711-716. 2104. Olivier M, Eeles R, Hollstein M, KhanMA, Harris CC, Hainaut P (2002). The IARCTP53 database: new online mutation analy-sis and recommendations to users. HumMutat 19: 607-614. 2104a. Olivier M, Goldgar DE, Sodha N,Ohgaki H, Kleihues P, Hainaut P, Eeles RA(2003). Li-Fraumeni and related syndromes:correlation between tumour type, familystructure and TP53 genotype. Cancer Res(in press).2105. Olsen JH, Hahnemann JM, Borresen-Dale AL, Brondum-Nielsen K,Hammarstrom L, Kleinerman R, KaariainenH, Lonnqvist T, Sankila R, Seersholm N,Tretli S, Yuen J, Boice JD Jr., Tucker M(2001). Cancer in patients with ataxia-telangiectasia and in their relatives in thenordic countries. J Natl Cancer Inst 93:121-127. 2106. Olson SH, Mignone L, Nakraseive C,Caputo TA, Barakat RR, Harlap S (2001).Symptoms of ovarian cancer. O b s t e tGynecol 98: 212-217. 2107. Olsson H, Alm P, Aspegren K,Gullberg B, Jonsson PE, Ranstam J (1990).Increased plasma prolactin levels in agroup of men with breast cancer--a pre-liminary study. Anticancer Res 10: 59-62. 2108. Olszewski W, Darzynkiewicz Z,Rosen PP, Schwartz MK, Melamed MR(1981). Flow cytometry of breast carcino-ma: I. Relation of DNA ploidy level to his-tology and estrogen receptor. Cancer 48:980-984. 2109. Orbo A, Stalsberg H, Kunde D (1990).Topographic criteria in the diagnosis oftumor emboli in intramammary lymphatics.Cancer 66: 972-977. 2 1 1 0 . Ordi J, Nogales FF, Palacin A,Marquez M, Pahisa J, Vanrell JA, CardesaA (2001). Mesonephric adenocarcinoma ofthe uterine corpus: CD10 expression asevidence of mesonephric differentiation.Am J Surg Pathol 25: 1540-1545. 2111. Ordi J, Schammel DP, Rasekh L,Tavassoli FA (1999). Sertoliform endometri-oid carcinomas of the ovary: a clinico-pathologic and immunohistochemicalstudy of 13 cases. Mod Pathol 12: 933-940. 2112. Ordi J, Stamatakos MD, Tavassoli FA(1997). Pure pleomorphic rhabdomyosar-comas of the uterus. Int J Gynecol Pathol16: 369-377. 2113. Ordonez NG (1998). Role of immuno-histochemistry in distinguishing epithelialperitoneal mesotheliomas from peritonealand ovarian serous carcinomas. Am JSurg Pathol 22: 1203-1214. 2114. Ordonez NG (1999). Granular celltumor: a review and update. Adv AnatPathol 6: 186-203. 2115. Ordonez NG (2000). Transitional cellcarcinomas of the ovary and bladder areimmunophenotypically different.Histopathology 36: 433-438.

406 References
2116. Ordonez NG, Mackay B (2000).Brenner tumor of the ovary: a comparativeimmunohistochemical and ultrastructuralstudy with transitional cell carcinoma ofthe bladder. Ultrastruct Pathol 24: 157-167. 2117. Ordonez NG, Manning JT, Luna MA(1981). Mixed tumor of the vulva: a report oftwo cases probably arising in Bartholin'sgland. Cancer 48: 181-186. 2118. Origoni M, Rossi M, Ferrari D, Lillo F,Ferrari AG (1999). Human papillomaviruswith co-existing vulvar vestibulitis syn-drome and vestibular papillomatosis. Int JGynaecol Obstet 64: 259-263. 2119. Osborne BM, Robboy SJ (1983).Lymphomas or leukemia presenting asovarian tumors. An analysis of 42 cases.Cancer 52: 1933-1943. 2120. Osborne CK (1998). Steroid hormonereceptors in breast cancer management.Breast Cancer Res Treat 51: 227-238. 2121. Osin P, Crook T, Powles T, Peto J,Gusterson B (1998). Hormone status of in-situ cancer in BRCA1 and BRCA2 mutationcarriers. Lancet 351: 1487. 2122. Osin P, Gusterson BA, Philp E, WallerJ, Bartek J, Peto J, Crook T (1998).Predicted anti-oestrogen resistance inBRCA-associated familial breast cancers.Eur J Cancer 34: 1683-1686. 2123. Otis CN (1996). Uterine adenomatoidtumors: immunohistochemical character-istics with emphasis on Ber-EP4immunoreactivity and distinction from ade-nocarcinoma. Int J Gynecol Pathol 15: 146-151. 2124. Otis CN, Powell JL, Barbuto D,Carcangiu ML (1992). Intermediate fila-mentous proteins in adult granulosa celltumors. An immunohistochemical study of25 cases. Am J Surg Pathol 16: 962-968. 2125. Ott G, Katzenberger T, Greiner A,Kalla J, Rosenwald A, Heinrich U, Ott MM,Muller-Hermelink HK (1997). The t(11;18)(q21;q21) chromosome translocation is afrequent and specific aberration in low-grade but not high-grade malignant non-Hodgkin's lymphomas of the mucosa-associated lymphoid tissue (MALT)- type.Cancer Res 57: 3944-3948. 2126. Otterbach F, Bankfalvi A, Bergner S,Decker T, Krech R, Boecker W (2000).Cytokeratin 5/6 immunohistochemistryassists the differential diagnosis of atypi-cal proliferations of the breast.Histopathology 37: 232-240. 2127. Ottesen GL, Graversen HP, Blichert-Toft M, Christensen IJ, Andersen JA(2000). Carcinoma in situ of the femalebreast. 10 year follow-up results of aprospective nationwide study. B r e a s tCancer Res Treat 62: 197-210. 2128. Ottesen GL, Graversen HP, Blichert-Toft M, Zedeler K, Andersen JA (1993).Lobular carcinoma in situ of the femalebreast. Short-term results of a prospectivenationwide study. The Danish BreastCancer Cooperative Group. Am J SurgPathol 17: 14-21. 2 1 2 9 . Ottman R, Pike MC, King MC,Casagrande JT, Henderson BE (1986).Familial breast cancer in a population-based series. Am J Epidemiol 123: 15-21. 2130. Ouchi T, Monteiro AN, August A,Aaronson SA, Hanafusa H (1998). BRCA1regulates p53-dependent gene expression.Proc Natl Acad Sci USA 95: 2302-2306. 2131. Outwater EK, Marchetto B, WagnerBJ (2000). Virilizing tumors of the ovary:imaging features. Ultrasound ObstetGynecol 15: 365-371.
2132. Outwater EK, Siegelman ES, Hunt JL(2001). Ovarian teratomas: tumor types andimaging characteristics. Radiographics 21:475-490. 2133. Oyama T, Kashiwabara K, YoshimotoK, Arnold A, Koerner F (1998). Frequentoverexpression of the cyclin D1 oncogenein invasive lobular carcinoma of the breast.Cancer Res 58: 2876-2880. 2134. Ozguroglu M, Ersavasti G, Ilvan S,Hatemi G, Demir G, Demirelli FH (1999).Bilateral inflammatory breast metastasesof epithelial ovarian cancer. Am J ClinOncol 22: 408-410. 2135. Ozguroglu M, Ozaras R, Tahan V,Demirkesen C, Demir G, Dogusoy G,Buyukunal E, Serdengecti S, Berkarda B(1999). Anorectal melanoma metastatic tothe breast. J Clin Gastroenterol 29: 197-199. 2136. Ozzello L, Gump FE (1985). The man-agement of patients with carcinomas infibroadenomatous tumors of the breast.Surg Gynecol Obstet 160: 99-104. 2137. Östör AG (1993). Natural history ofcervical intraepithelial neoplasia: a criticalreview. Int J Gynecol Pathol 12: 186-192. 2138. Östör AG (1995). Pandora's box orAriadne's thread? Definition and prognos-tic significance of microinvasion in theuterine cervix. Squamous lesions. PatholAnnu 30: 103-136. 2139. Östör AG (2000). Early invasive ade-nocarcinoma of the uterine cervix. Int JGynecol Pathol 19: 29-38. 2140. Östör AG, Duncan A, Quinn M, RomeR (2000). Adenocarcinoma in situ of theuterine cervix: an experience with 100cases. Gynecol Oncol 79: 207-210. 2141. Östör AG, Fortune DW, Riley CB(1988). Fibroepithelial polyps with atypicalstromal cells (pseudosarcoma botryoides)of vulva and vagina. A report of 13 cases.Int J Gynecol Pathol 7: 351-360. 2142. Östör AG, Pagano R, Davoren RA,Fortune DW, Chanen W, Rome R (1984).Adenocarcinoma in situ of the cervix. Int JGynecol Pathol 3: 179-190. 2143. Östör AG, Rome R, Quinn M (1997).Microinvasive adenocarcinoma of thecervix: a clinicopathologic study of 77women. Obstet Gynecol 89: 88-93. 2144. Paavonen J (1985). Colposcopic find-ings associated with human papillo-mavirus infection of the vagina and thecervix. Obstet Gynecol Surv 40: 185-189. 2145. Padberg BC, Stegner HE, vonSengbusch S, Arps H, Schroder S (1992).DNA-cytophotometry and immunocyto-chemistry in ovarian tumours of borderlinemalignancy and related peritoneal lesions.Virchows Arch A Pathol Anat Histopathol421: 497-503. 2146. Padmore RF, Lara JF, Ackerman DJ,Gales T, Sigurdson ER, Ehya H, Cooper HS,Patchefsky AS (1996). Primary combinedmalignant melanoma and ductal carcino-ma of the breast. A report of two cases.Cancer 78: 2515-2525. 2147. Page DL, Anderson TJ, Sakamoto G(1987). Infiltrating Carcinoma:MajorHistoligical Types. WB Saunders: London.2148. Page DL, Dixon JM, Anderson T, LeeD, Stwewart H (1993). Invasive cribriformcarcinoma of the breast. Histopathology 7:525-536. 2149. Page DL, Dupont WD (1990).Anatomic markers of human premalignan-cy and risk of breast cancer. Cancer 66:1326-1335.
2150. Page DL, Kidd TE Jr., Dupont WD,Simpson JF, Rogers LW (1991). Lobularneoplasia of the breast: higher risk for sub-sequent invasive cancer predicted bymore extensive disease. Hum Pathol 22:1232-1239. 2151. Page DL, Salhany KE, Jensen RA,Dupont WD (1996). Subsequent breast car-cinoma risk after biopsy with atypia in abreast papilloma. Cancer 78: 258-266. 2152. Palacios J, Benito N, Pizarro A,Suarez A, Espada J, Cano A, Gamallo C(1995). Anomalous expression of P-Cadherin in breast carcinoma. Correlationwith E-Cadherin expression and pathologi-cal features. Am J Pathol 146: 605-612. 2153. Palacios J, Gamallo C (1998).Mutations in the beta-catenin gene(CTNNB1) in endometrioid ovarian carci-nomas. Cancer Res 58: 1344-1347. 2154. Palangie T, Mosseri V, Mihura J,Campana F, Beuzeboc P, Dorval T, Garcia-Giralt E, Jouve M, Scholl S, Asselain B,Pouillart P. (1994). Prognostic factors ininflammatory breast cancer and therapeu -tic implications. Eur J Cancer 30A: 921-927. 2155. Palazzo J, Hyslop T (1998).Hyperplastic ductal and lobular lesionsand carcinoma in situ of the breast:Reproducibility of current diagnostic crite -ria among community and academic basedpathologists. Breast J 4: 230-237. 2156. Palazzo JP, Gibas Z, Dunton CJ,Talerman A (1993). Cytogenetic study ofbotryoid rhabdomyosarcoma of the uterinecervix. Virchows Arch A Pathol AnatHistopathol 422: 87-91. 2157. Palli D, Galli M, Bianchi S, BussolatiG, Di Palma S, Eusebi V, Gambacorta M,Rosselli DT (1996). Reproducibility of histo -logical diagnosis of breast lesions: resultsof a panel in Italy. Eur J Cancer 32A: 603-607. 2158. Palli D, Rosselli DT, Simoncini R,Bianchi S (1991). Benign breast diseaseand breast cancer: a case-control study ina cohort in Italy. Int J Cancer 47: 703-706. 2159. Pallis L, Wilking N, Cedermark B,Rutqvist LE, Skoog L (1992). Receptors forestrogen and progesterone in breast car-cinoma in situ. Anticancer Res 12: 2113-2115. 2160. Palmer JP, Biback SM (1954).Primary cancer of the vagina. Am J ObstetGynecol 67: 377-397. 2161. Palmer JR, Anderson D, Helmrich SP,Herbst AL (2000). Risk factors for diethyl-stilbestrol-associated clear cell adenocar-cinoma. Obstet Gynecol 95: 814-820. 2162. Palmer PE, Bogojavlensky S, BhanAK, Scully RE (1990). Prolactinoma in wallof ovarian dermoid cyst with hyperpro-lactinemia. Obstet Gynecol 75: 540-543. 2163. Palombo F, Gallinari P, Iaccarino I,Lettieri T, Hughes M, D'Arrigo A, Truong O,Hsuan JJ, Jiricny J (1995). GTBP, a 160-kilodalton protein essential for mismatch-binding activity in human cells. Science268: 1912-1914. 2164. Pantoja E, Rodriguez-Ibanez I,Axtmayer RW, Noy MA, Pelegrina I (1975).Complications of dermoid tumors of theovary. Obstet Gynecol 45: 89-94. 2165. Paoletti M, Pridjian G, Okagaki T,Talerman A (1987). A stromal Leydig celltumor of the ovary occurring in a pregnant15-year-old girl. Ultrastructural findings.Cancer 60: 2806-2810.
2166. Papadatos G, Rangan AM, PsarianosT, Ung O, Taylor R, Boyages J (2001).Probability of axillary node involvement inpatients with tubular carcinoma of thebreast. Br J Surg 88: 860-864. 2167. Papadopoulos N, Nicolaides NC, WeiYF, Ruben SM, Carter KC, Rosen CA,Haseltine WA, Fleischmann RD, FraserCM, Adams MD, Venter JC, Hamilton SR,Petersen GM, Watson P, Lynch HT,Peltomaki T, Mecklin JP, de la Chapelle A,Kinzler KW, Vogelstein B. (1994). Mutationof a mutL homolog in hereditary colon can-cer. Science 263: 1625-1629. 2168. Papchristou DN, Kinne DW, AshikariR, Fortner JG (1979). Melanoma of the nip-ple and aerola. Br J Surg (4) 66: 287-288. 2169. Papotti M, Macri L, Bussolati G,Reubi JC (1989). Correlative study onneuro-endocrine differentiation and pres-ence of somatostatin receptors in breastcarcinomas. Int J Cancer 43: 365-369. 2170. Paradinas FJ, Browne P, Fisher RA,Foskett M, Bagshawe KD, Newlands E(1996). A clinical, histopathological andflow cytometric study of 149 completemoles, 146 partial moles and 107 non-molarhydropic abortions. Histopathology 28: 101-110. 2171. Paraskevas M, Scully RE (1989). Hiluscell tumor of the ovary. A clinicopathologi-cal analysis of 12 Reinke crystal-positiveand nine crystal-negative cases. Int JGynecol Pathol 8: 299-310. 2172. Parazzini F, Franceschi S, La VecchiaC, Fasoli M (1991). The epidemiology ofovarian cancer. Gynecol Oncol 43: 9-23. 2173. Parazzini F, La Vecchia C, Moroni S,Chatenoud L, Ricci E (1994). Family historyand the risk of endometrial cancer. Int JCancer 59: 460-462. 2174. Parc YR, Halling KC, Burgart LJ,McDonnell SK, Schaid DJ, Thibodeau SN,Halling AC (2000). Microsatellite instabilityand hMLH1/hMSH2 expression in youngendometrial carcinoma patients: associa-tions with family history and histopatholo-gy. Int J Cancer 86: 60-66. 2175. Parham DM, Hagen N, Brown RA(1992). Simplified method of grading pri-mary carcinomas of the breast. J ClinPathol 45: 517-520. 2176. Park CC, Mitsumori M, Nixon A,Recht A, Connolly J, Gelman R, Silver B,Hetelekidis S, Abner A, Harris JR, SchnittSJ (2000). Outcome at 8 years after breast-conserving surgery and radiation therapyfor invasive breast cancer: influence ofmargin status and systemic therapy onlocal recurrence. J Clin Oncol 18: 1668-1675. 2177. Park J, Sun D, Genest DR, TrivijitsilpP, Suh I, Crum CP (1998). Coexistence oflow and high grade squamous intraepithe-lial lesions of the cervix: morphologic pro-gression or multiple papillomaviruses?Gynecol Oncol 70: 386-391. 2178. Park JG, Park YJ, Wijnen JT, VasenHF (1999). Gene-environment interaction inhereditary nonpolyposis colorectal cancerwith implications for diagnosis and genetictesting. Int J Cancer 82: 516-519. 2179. Park JJ, Genest DR, Sun D, Crum CP(1999). Atypical immature metaplastic-likeproliferations of the cervix: diagnosticreproducibility and viral (HPV) correlates.Hum Pathol 30: 1161-1165.

407References
2180. Park JS, Jones RW, McLean MR,Currie JL, Woodruff JD, Shah KV, KurmanRJ (1991). Possible etiologic heterogeneityof vulvar intraepithelial neoplasia. A corre-lation of pathologic characteristics withhuman papillomavirus detection by in situhybridization and polymerase chain reac-tion. Cancer 67: 1599-1607. 2181. Park SH, Kim I (1994). Histogeneticconsideration of ovarian sex cord-stromaltumors analyzed by expression pattern ofcytokeratins, vimentin, and laminin.Correlation studies with human gonads.Pathol Res Pract 190: 449-456. 2182. Park SK, Yoo KY, Lee SJ, Kim SU, AhnSH, Noh DY, Choe KJ, Strickland PT,Hirvonen A, Kang D (2000). Alcohol con-sumption, glutathione S-transferase M1and T1 genetic polymorphisms and breastcancer risk. Pharmacogenetics 10: 301-309. 2183. Park SY, Kim HS, Hong EK, Kim WH(2002). Expression of cytokeratins 7 and 20in primary carcinomas of the stomach andcolorectum and their value in the differen-tial diagnosis of metastatic carcinomas tothe ovary. Hum Pathol 33: 1078-1085. 2184. Park TW, Richart RM, Sun XW,Wright TC Jr. (1996). Association betweenhuman papillomavirus type and clonal sta-tus of cervical squamous intraepitheliallesions. J Natl Cancer Inst 88: 355-358. 2 1 8 5 . Parkash V, Carcangiu ML (1995).Transformation of ovarian dysgerminomato yolk sac tumor: evidence for a histoge-netic continuum. Mod Pathol 8: 881-887. 2186. Parker RG, Grimm P, Enstrom JE(1989). Contralateral breast cancers fol-lowing treatment for initial breast cancersin women. Am J Clin Oncol 12: 213-216. 2187. Parker WH, Fu YS, Berek JS (1994).Uterine sarcoma in patients operated onfor presumed leiomyoma and rapidly grow-ing leiomyoma. Obstet Gynecol 83: 414-418. 2188. Parkin DM, Bray F, Ferlay J, Pisani P(2001). Estimating the world cancer bur-den: Globocan 2000. Int J Cancer 94: 153-156. 2189. Parkin DM, Whelan SL, Ferlay J,Raymond L, Young J (1997). C a n c e rIncidence in Five Continents, Vol. VII (IARCScientific Publication N°143). Inter-national Agency for Research on Cancer:Lyon, France.2190. Parl FF, Richardson LD (1983). Thehistologic and biologic spectrum of tubularcarcinoma of the breast. Hum Pathol 14:694-698. 2191. Patchefsky AS, Frauenhoffer CM,Krall RA, Cooper HS (1979). Low-grademucoepidermoid carcinoma of the breast.Arch Pathol Lab Med 103: 196-198. 2192. Patchefsky AS, Shaber GS, SchwartzGF, Feig SA, Nerlinger RE (1977). Thepathology of breast cancer detected bymass population screening. Cancer 4 0 :1659-1670. 2193. Patel KJ, Yu VP, Lee H, Corcoran A,Thistlethwaite FC, Evans MJ, Colledge WH,Friedman LS, Ponder BA, Venkitaraman AR(1998). Involvement of Brca2 in DNA repair.Mol Cell 1: 347-357. 2194. Paterakos M, Watkin WG, EdgertonSM, Moore DH, Thor AD (1999). Invasivemicropapillary carcinoma of the breast: aprognostic study. Hum Pathol 30: 1459-1463. 2195. Patey DH, Scarff RW (1928). The posi-tion of histology in the prognosis of carci-noma of the breast. Lancet 1: 801-804.
2196. Patsner B (2001). Primary endoder-mal sinus tumor of the endometrium pre-senting as "recurrent" endometrial adeno-carcinoma. Gynecol Oncol 80: 93-95. 2197. Pattillo RA, Sasaki S, Katayama KP,Roesler M, Mattingly RF (1981). Genesis of46,XY hydatidiform mole. Am J ObstetGynecol 141: 104-105. 2198. Paull TT, Cortez D, Bowers B, ElledgeSJ, Gellert M (2001). From the Cover: DirectDNA binding by Brca1. Proc Natl Acad SciUSA 98: 6086-6091. 2199. Paulus DD (1990). Lymphoma of thebreast. Radiol Clin North Am 28: 833-840. 2200. Pautier P, Genestie C, Rey A, MoriceP, Roche B, Lhomme C, Haie-Meder C,Duvillard P (2000). Analysis of clinico-pathologic prognostic factors for 157 uter-ine sarcomas and evaluation of a gradingscore validated for soft tissue sarcoma.Cancer 88: 1425-1431. 2201. Pedersen L, Holck S, Schiodt T,Zedeler K, Mouridsen HT (1994). Medullarycarcinoma of the breast, prognostic impor-tance of characteristic histopathologicalfeatures evaluated in a multivariate Coxanalysis. Eur J Cancer 30A: 1792-1797. 2202. Pedersen L, Larsen JK, ChristensenIJ, Lykkesfeldt A, Holck S, Schiodt T (1994).DNA ploidy and S-phase fraction inmedullary carcinoma of the breast--a flowcytometric analysis using archival materi-al. Breast Cancer Res Treat 29: 297-306. 2203. Pedersen L, Zedeler K, Holck S,Schiodt T, Mouridsen HT (1991). Medullarycarcinoma of the breast, proposal for anew simplified histopathological definition.Based on prognostic observations andobservations on inter- and intraobservervariability of 11 histopathological charac-teristics in 131 breast carcinomas withmedullary features. Br J Cancer 63: 591-595. 2204. Pedersen L, Zedeler K, Holck S,Schiodt T, Mouridsen HT (1995). Medullarycarcinoma of the breast. Prevalence andprognostic importance of classical riskfactors in breast cancer. Eur J Cancer 31A:2289-2295. 2204a. Pedeutour F, Ligon AH, Morton CC(1999). [Genetics of uterine leiomyomata].Bull Cancer 86: 920-928. 2205. Peiro G, Bornstein BA, Connolly JL,Gelman R, Hetelekidis S, Nixon AJ, RechtA, Silver B, Harris JR, Schnitt SJ (2000).The influence of infiltrating lobular carci-noma on the outcome of patients treatedwith breast-conserving surgery and radia -tion therapy. Breast Cancer Res Treat 59:49-54. 2206. Peiro G, Diebold J, Lohse P,Ruebsamen H, Lohse P, Baretton GB, LohrsU (2002). Microsatellite instability, loss ofheterozygosity, and loss of hMLH1 andhMSH2 protein expression in endometrialcarcinoma. Hum Pathol 33: 347-354. 2207. Pejovic T, Burki N, Odunsi K, FiedlerP, Achong N, Schwartz PE, Ward DC(1999). Well-differentiated mucinous carci-noma of the ovary and a coexistingBrenner tumor both exhibit amplification of12q14-21 by comparative genomichybridization. Gynecol Oncol 74: 134-137. 2208. Pejovic T, Heim S, Alm P, Iosif S,Himmelmann A, Skjaerris J, Mitelman F(1993). Isochromosome 1q as the sole kary-otypic abnormality in a Sertoli cell tumor ofthe ovary. Cancer Genet Cytogenet 65: 79-80.
2209. Pejovic T, Heim S, Mandahl N,Elmfors B, Floderus UM, Furgyik S, Helm G,Willen H, Mitelman F (1990). Trisomy 12 is aconsistent chromosomal aberration inbenign ovarian tumors. G e n e sChromosomes Cancer 2: 48-52. 2210. Pekin T, Eren F, Pekin O (2000).Leiomyosarcoma of the broad ligament:case report and literature review. Eur JGynaecol Oncol 21: 318-319. 2211. Pelkey TJ, Frierson HF Jr., Mills SE,Stoler MH (1998). The diagnostic utility ofinhibin staining in ovarian neoplasms. Int JGynecol Pathol 17: 97-105. 2212. Pelosi G, Martignoni G, Bonetti F(1991). Intraductal carcinoma of mammary-type apocrine epithelium arising within apapillary hydradenoma of the vulva. Reportof a case and review of the literature.Arch Pathol Lab Med 115: 1249-1254. 2213. Peltomaki P, Aaltonen LA, Sistonen P,Pylkkanen L, Mecklin JP, Jarvinen H,Green JS, Jass JR, Weber JL, Leach FS,Petersen GM, Hamilton SR, de la ChapelleA, Vogelstein B. (1993). Genetic mapping ofa locus predisposing to human colorectalcancer. Science 260: 810-812. 2214. Peltomaki P, Vasen HF (1997).Mutations predisposing to hereditary non-polyposis colorectal cancer: database andresults of a collaborative study. TheInternational Collaborative Group onHereditary Nonpolyposis ColorectalCancer. Gastroenterology 113: 1146-1158. 2214a. Penrose LS, Mackenzie JH, KarnMN (1948). A genetical study of humanmammary cancer. Ann Euegenics 14: 234-266. 2215. Pensler JM, Silverman BL, SanghaviJ, Goolsby C, Speck G, Brizio-Molteni L,Molteni A (2000). Estrogen and proges-terone receptors in gynecomastia. PlastReconstr Surg 106: 1011-1013. 2216. Pereira H, Pinder SE, Sibbering DM,Galea MH, Elston CW, Blamey RW,Robertson JF, Ellis IO (1995). Pathologicalprognostic factors in breast cancer. IV:Should you be a typer or a grader? A com -parative study of two histological prognos-tic features in operable breast carcinoma.Histopathology 27: 219-226. 2217. Perez CA, Arneson AN, Dehner LP,Galakatos A (1974). Radiation therapy incarcinoma of the vagina. Obstet Gynecol44: 862-872. 2218. Perou CM, Sorlie T, Eisen MB, van deRijn M, Jeffrey SS, Rees CA, Pollack JR,Ross DT, Johnsen H, Akslen LA, Fluge O,Pergamenschikov A, Williams C, Zhu SX,Lonning PE, Borresen-Dale AL, Brown PO,Botstein D (2000). Molecular portraits ofhuman breast tumours. Nature 406: 747-752. 2219. Perrin L, Ward B (1995). Small cellcarcinoma of the cervix. Int J GynecolCancer 5: 200-203. 2 2 2 0 . Persaud V, Anderson MF (1977).Endometrial stromal sarcoma of the broadligament arising in an area of endometrio-sis in a paramesonephric cyst. Casereport. Br J Obstet Gynaecol 84: 149-152. 2221. Persons DL, Hartmann LC, Herath JF,Keeney GL, Jenkins RB (1994).Fluorescence in situ hybridization analysisof trisomy 12 in ovarian tumors. Am J ClinPathol 102: 775-779. 2222. Perzin KH, Lattes R (1972). Papillaryadenoma of the nipple (florid papillomato-sis, adenoma, adenomatosis). A clinico-pathologic study. Cancer 29: 996-1009.
2223. Peters GN, Wolff M (1983). Adenoidcystic carcinoma of the breast. Report of11 new cases: review of the literature anddiscussion of biological behavior. Cancer52: 680-686. 2224. Peters GN, Wolff M, Haagensen CD(1981). Tubular carcinoma of the breast.Clinical pathologic correlations based on100 cases. Ann Surg 193: 138-149. 2225. Peters WA, III, Andersen WA,Hopkins MP, Kumar NB, Morley GW (1988).Prognostic features of carcinoma of thefallopian tube. Obstet Gynecol 71: 757-762. 2226. Peters WA, III, Kumar NB, AndersenWA, Morley GW (1985). Primary sarcomaof the adult vagina: a clinicopathologicstudy. Obstet Gynecol 65: 699-704. 2227. Peters WA, III, Kumar NB, MorleyGW (1985). Carcinoma of the vagina.Factors influencing treatment outcome.Cancer 55: 892-897. 2228. Peters WM, Wells M, Bryce FC(1984). Mullerian clear cell carcinofibromaof the uterine corpus. Histopathology 8:1069-1078. 2229. Peterse JL (1993). Breast carcinomawith an unexpected inside out growth pat -tern, rotation of polarisation associatedwith angioinvasion. Pathol Res Pract 189:780. 2230. Peto J, Collins N, Barfoot R, Seal S,Warren W, Rahman N, Easton DF, Evans C,Deacon J, Stratton MR (1999). Prevalenceof BRCA1 and BRCA2 gene mutations inpatients with early-onset breast cancer. JNatl Cancer Inst 91: 943-949. 2231. Petridou E, Giokas G, Kuper H, MucciLA, Trichopoulos D (2000). Endocrine cor-relates of male breast cancer risk: a case-control study in Athens, Greece. Br JCancer 83: 1234-1237. 2232. Petru E, Pickel H, Heydarfadai M,Lahousen M, Haas J, Schaider H,Tamussino K (1992). Nongenital cancersmetastatic to the ovary. Gynecol Oncol 44:83-86. 2233. Petterson F (1991). Annual Report ofthe Treatment in Gynecological Cancer.International Federation of Gynecologyand Obstetrics: Stockholm.2234. Pettinato G, Insabato L, De Chiara A,Manco A, Petrella G (1989). High-grademucoepidermoid carcinoma of the breast.Fine needle aspiration cytology and clini-copathologic study of a case. Acta Cytol33: 195-200. 2235. Pettinato G, Manivel JC, Insabato L,De Chiara A, Petrella G (1988). Plasma cellgranuloma (inflammatory pseudotumor) ofthe breast. Am J Clin Pathol 90: 627-632. 2236. Pharoah PD, Antoniou A, Bobrow M,Zimmern RL, Easton DF, Ponder BA (2002).Polygenic susceptibility to breast cancerand implications for prevention. Nat Genet31: 33-36. 2237. Pharoah PD, Day NE, Caldas C (1999).Somatic mutations in the p53 gene andprognosis in breast cancer: a meta-analy-sis. Br J Cancer 80: 1968-1973. 2238. Pharoah PD, Day NE, Duffy S, EastonDF, Ponder BA (1997). Family history andthe risk of breast cancer: a systematicreview and meta-analysis. Int J Cancer 71:800-809. 2239. Pharoah PD, Easton DF, Stockton DL,Gayther S, Ponder BA (1999). Survival infamilial, BRCA1-associated, and BRCA2-associated epithelial ovarian cancer.United Kingdom Coordinating Committeefor Cancer Research (UKCCCR) FamilialOvarian Cancer Study Group. Cancer Res59: 868-871.

408 References
2240. Phelan CM, Rebbeck TR, Weber BL,Devilee P, Ruttledge MH, Lynch HT, LenoirGM, Stratton MR, Easton DF, Ponder BA,Cannon-Albright L, Larsson C, Goldgar DE,Narod SA (1996). Ovarian cancer risk inBRCA1 carriers is modified by the HRAS1variable number of tandem repeat (VNTR)locus. Nat Genet 12: 309-311. 2241. Phillipson J, Ostrzega N (1994). Fineneedle aspiration of invasive cribriformcarcinoma with benign osteoclast-likegiant cells of histiocytic origin. A casereport. Acta Cytol 38: 479-482. 2242. Piana S, Nogales FF, Corrado S,Cardinale L, Gusolfino D, Rivasi F (1999).Pregnancy luteoma with granulosa cellproliferation: an unusual hyperplasticlesion arising in pregnancy and mimickingan ovarian neoplasia. Pathol Res Pract 195:859-863. 2243. Picciocchi A, Masetti R, Terribile D,Ausili-Cefaro G, Antinori A, Marra A,Magistrelli P (1994). Inflammatory breastcarcinoma: contribution of surgery as partof a combined modality approach. Breastdisease 7: 143-149. 2244. Pickel H, Reich O, Tamussino K(1998). Bilateral atypical hyperplasia of thefallopian tube associated with tamoxifen: areport of two cases. Int J Gynecol Pathol17: 284-285. 2245. Pickel H, Thalhammer M (1971).[Chondrosarcoma of the Fallopian tube].Geburtshilfe Frauenheilkd 31: 1243-1248. 2246. Piek JM, van Diest PJ, Zweemer RP,Jansen JW, Poort-Keesom RJ, Menko FH,Gille JJ, Jongsma AP, Pals G, Kenemans P,Verheijen RH (2001). Dysplastic changes inprophylactically removed Fallopian tubesof women predisposed to developing ovar-ian cancer. J Pathol 195: 451-456. 2247. Piek JM, van Diest PJ, Zweemer RP,Kenemans P, Verheijen RH (2001). Tuballigation and risk of ovarian cancer. Lancet358: 844. 2248. Pierce GB (1974). Neoplasms, differ-entiations and mutations. Am J Pathol 77:103-118. 2 2 4 9 . Pietruszka M, Barnes L (1978).Cystosarcoma phyllodes: a clinicopatho-logic analysis of 42 cases. Cancer 41: 1974-1983. 2 2 5 0 . Pike AM, Oberman HA (1985).Juvenile (cellular) adenofibromas. A clini-copathologic study. Am J Surg Pathol 9:730-736. 2251. Pillai MR, Jayaprakash PG, Nair MK(1999). bcl-2 immunoreactivity but not p53accumulation associated with tumourresponse to radiotherapy in cervical carci-noma. J Cancer Res Clin Oncol 125: 55-60. 2252. Pina L, Apesteguia L, Cojo R, Cojo F,Arias-Camison I, Rezola R, De Miguel C(1997). Myofibroblastoma of male breast:report of three cases and review of the lit-erature. Eur Radiol 7: 931-934. 2253. Pinder SE, Ellis IO, Galea M, O'RoukeS, Blamey RW, Elston CW (1994).Pathological prognostic factors in breastcancer. III. Vascular invasion: relationshipwith recurrence and survival in a largestudy with long-term follow-up.Histopathology 24: 41-47. 2254. Pinder SE, Murray S, Ellis IO, Trihia H,Elston CW, Gelber RD, Goldhirsch A,Lindtner J, Cortes-Funes H, Simoncini E,Byrne MJ, Golouh R, Rudenstam CM,Castiglione-Gertsch M, Gusterson BA(1998). The importance of the histologicgrade of invasive breast carcinoma andresponse to chemotherapy. Cancer 8 3 :1529-1539.
2255. Pins MR, Young RH, Daly WJ, ScullyRE (1996). Primary squamous cell carcino-ma of the ovary. Report of 37 cases. Am JSurg Pathol 20: 823-833. 2256. Pinto AP, Lin MC, Sheets EE, MutoMG, Sun D, Crum CP (2000). Allelic imbal-ance in lichen sclerosus, hyperplasia, andintraepithelial neoplasia of the vulva.Gynecol Oncol 77: 171-176. 2257. Pippard EC, Hall AJ, Barker DJ,Bridges BA (1988). Cancer in homozygotesand heterozygotes of ataxia-telangiectasiaand xeroderma pigmentosum in Britain.Cancer Res 48: 2929-2932. 2258. Pitman MB, Young RH, Clement PB,Dickersin GR, Scully RE (1994).Endometrioid carcinoma of the ovary andendometrium, oxyphilic cell type: a reportof nine cases. Int J Gynecol Pathol 13: 290-301. 2259. Pitts WC, Rojas VA, Gaffey MJ, RouseRV, Esteban J, Frierson HF, Kempson RL,Weiss LM (1991). Carcinomas with meta-plasia and sarcomas of the breast. Am JClin Pathol 95: 623-632. 2260. Piura B, Rabinovich A, Dgani R (1999).Basal cell carcinoma of the vulva. J SurgOncol 70: 172-176. 2261. Piura B, Rabinovich A, Dgani R (1999).Malignant melanoma of the vulva: report ofsix cases and review of the literature. EurJ Gynaecol Oncol 20: 182-186. 2262. Piver MS, Jishi MF, Tsukada Y, NavaG (1993). Primary peritoneal carcinomaafter prophylactic oophorectomy inwomen with a family history of ovariancancer. A report of the Gilda RadnerFamilial Ovarian Cancer Registry. Cancer71: 2751-2755. 2263. Piver MS, Rutledge FN, Copeland L,Webster K, Blumenson L, Suh O (1984).Uterine endolymphatic stromal myosis: acollaborative study. Obstet Gynecol 6 4 :173-178. 2264. Planck M, Rambech E, Moslein G,Muller W, Olsson H, Nilbert M (2002). Highfrequency of microsatellite instability andloss of mismatch-repair protein expressionin patients with double primary tumors ofthe endometrium and colorectum. Cancer94: 2502-2510. 2265. Plentl AA, Frideman EA (1971).Lymphatic System of the Female Genitali -The Morphological Basis of OncologicDiagnosis and Therapy. WB Saunders:Philadelphia.2266. Plouffe L Jr., Tulandi T, Rosenberg A,Ferenczy A (1984). Non-Hodgkin's lym-phoma in Bartholin's gland: case reportand review of literature. Am J ObstetGynecol 148: 608-609. 2 2 6 7 . Pluquet O, Hainaut P (2001).Genotoxic and non-genotoxic pathways ofp53 induction. Cancer Lett 174: 1-15. 2268. Podsypanina K, Ellenson LH, NemesA, Gu J, Tamura M, Yamada KM, Cordon-Cardo C, Catoretti G, Fisher PE, Parsons R(1999). Mutation of Pten/Mmac1 in micecauses neoplasia in multiple organ sys-tems. Proc Natl Acad Sci USA 96: 1563-1568. 2269. Poen JC, Tran L, Juillard G, Selch MT,Giuliano A, Silverstein M, Fingerhut A,Lewinsky B, Parker RG (1992).Conservation therapy for invasive lobularcarcinoma of the breast. Cancer 69: 2789-2795. 2270. Polger MR, Denison CM, Lester S,Meyer JE (1996). Pseudoangiomatous stro-mal hyperplasia: mammographic andsonographic appearances. AJR Am JRoentgenol 166: 349-352.
2271. Polk P, Parker KM, Biggs PJ (1996).Soft tissue oncocytoma. Hum Pathol 27:206-208. 2272. Ponsky JL, Gliga L, Reynolds S (1984).Medullary carcinoma of the breast: anassociation with negative hormonal recep-tors. J Surg Oncol 25: 76-78. 2273. Pope TL Jr., Fechner RE, Wilhelm MC,Wanebo HJ, de Paredes ES (1988). Lobularcarcinoma in situ of the breast: mammo-graphic features. Radiology 168: 63-66. 2274. Porter PL, Garcia R, Moe R, CorwinDJ, Gown AM (1991). C-erbB-2 oncogeneprotein in in situ and invasive lobularbreast neoplasia. Cancer 68: 331-334. 2275. Pothuri B, Leitao M, Barakat R,Akram M, Bogomolny F, Olvera N, Lin O,Soslow R, Robson ME, Offit K, Boyd J(2001). Genetic analysis of ovarian carci-noma histogenesis. Gynecol Oncol 80: 277. 2276. Potischman N, Hoover RN, BrintonLA, Siiteri P, Dorgan JF, Swanson CA,Berman ML, Mortel R, Twiggs LB, BarrettRJ, Wilbanks GD, Persky V, Lurain JR(1996). Case-control study of endogenoussteroid hormones and endometrial cancer.J Natl Cancer Inst 88: 1127-1135. 2277. Potkul RK, Lancaster WD, KurmanRJ, Lewandowski G, Weck PK, Delgado G(1990). Vulvar condylomas and squamousvestibular micropapilloma. Differences inappearance and response to treatment. JReprod Med 35: 1019-1022. 2278. Powell CM, Cranor ML, Rosen PP(1994). Multinucleated stromal giant cellsin mammary fibroepithelial neoplasms. Astudy of 11 patients. Arch Pathol Lab Med118: 912-916. 2279. Powell CM, Cranor ML, Rosen PP(1995). Pseudoangiomatous stromal hyper-plasia (PASH). A mammary stromal tumorwith myofibroblastic differentiation. Am JSurg Pathol 19: 270-277. 2280. Powers CN, Stastny JF, Frable WJ(1996). Adenoid basal carcinoma of thecervix: a potential pitfall in cervicovaginalcytology. Diagn Cytopathol 14: 172-177. 2281. Prasad CJ, Ray JA, Kessler S (1992).Primary small cell carcinoma of the vaginaarising in a background of atypical adeno-sis. Cancer 70: 2484-2487. 2282. Prasad ML, Osborne MP, Giri DD,Hoda SA (2000). Microinvasive carcinoma(T1mic) of the breast: clinicopathologicprofile of 21 cases. Am J Surg Pathol 24:422-428. 2283. Prat J (2002). Clonality analysis insynchronous tumors of the female genitaltract. Hum Pathol 33: 383-385. 2 2 8 4 . Prat J, Bhan AK, Dickersin GR,Robboy SJ, Scully RE (1982). Hepatoid yolksac tumor of the ovary (endodermal sinustumor with hepatoid differentiation): a lightmicroscopic, ultrastructural and immuno-histochemical study of seven cases.Cancer 50: 2355-2368. 2285. Prat J, de Nictolis M (2002). Serousborderline tumors of the ovary: a long-termfollow-up study of 137 cases, including 18with a micropapillary pattern and 20 withmicroinvasion. Am J Surg Pathol 26: 1111-1128. 2286. Prat J, Matias-Guiu X, Barreto J(1991). Simultaneous carcinoma involvingthe endometrium and the ovary. A clinico-pathologic, immunohistochemical, andDNA flow cytometric study of 18 cases.Cancer 68: 2455-2459. 2 2 8 7 . Prat J, Matias-Guiu X, Scully RE(1989). Hepatic yolc sac differentiation inan ovarian polyembryoma. S u r g i c a lPathology 2: 147-150.
2287a. Prat J, Rodriguez IM, Ota S, Matias-Guiu X (2003). Endometrioid, clear cell, andmixed carcinomas of the ovary with andwithout endometriosis: a comparative clin-icopathological and molecular analysis of113 cases. Mod Pathol 207A. 2288. Prat J, Scully RE (1979). Sarcomas inovarian mucinous tumors: a report of twocases. Cancer 44: 1327-1331. 2289. Prat J, Scully RE (1981). Cellular fibro-mas and fibrosarcomas of the ovary: acomparative clinicopathologic analysis ofseventeen cases. Cancer 47: 2663-2670. 2290. Prat J, Young RH, Scully RE (1982).Ovarian mucinous tumors with foci ofanaplastic carcinoma. Cancer 50: 300-304. 2291. Prat J, Young RH, Scully RE (1982).Ovarian Sertoli-Leydig cell tumors withheterologous elements. II. Cartilage andskeletal muscle: a clinicopathologic analy-sis of twelve cases. Cancer 50: 2465-2475. 2292. Prayson RA, Goldblum JR, Hart WR(1997). Epithelioid smooth-muscle tumorsof the uterus: a clinicopathologic study of18 patients. Am J Surg Pathol 21: 383-391. 2293. Prayson RA, Hart WR (1992).Mitotically active leiomyomas of theuterus. Am J Clin Pathol 97: 14-20. 2294. Prayson RA, Hart WR, Petras RE(1994). Pseudomyxoma peritonei. A clinico-pathologic study of 19 cases with empha-sis on site of origin and nature of associat-ed ovarian tumors. Am J Surg Pathol 18:591-603. 2295. Prayson RA, Stoler MH, Hart WR(1995). Vulvar vestibulitis. A histopatholog -ic study of 36 cases, including humanpapillomavirus in situ hybridization analy-sis. Am J Surg Pathol 19: 154-160. 2296. Prechtel D, Werenskiold AK, PrechtelK, Keller G, Hofler H (1998). Frequent loss ofheterozygosity at chromosome 13q12-13with BRCA2 markers in sporadic malebreast cancer. Diagn Mol Pathol 7: 57-62. 2297. Prechtel K, Prechtel V (1997). [Breastcarcinoma in the man. Current results fromthe viewpoint of clinic and pathology].Pathologe 18: 45-52. 2298. Prempree T, Tang CK, Hatef A,Forster S (1983). Angiosarcoma of the vagi-na: a clinicopathologic report. A reap-praisal of the radiation treatment ofangiosarcomas of the female genital tract.Cancer 51: 618-622. 2299. Prendiville W, Cullimore J, Norman S(1989). Large loop excision of the transfor-mation zone (LLETZ). A new method ofmanagement for women with cervicalintraepithelial neoplasia. Br J ObstetGynaecol 96: 1054-1060. 2300. Press MF, Scully RE (1985).Endometrial "sarcomas" complicatingovarian thecoma, polycystic ovarian dis-ease and estrogen therapy. Gynecol Oncol21: 135-154. 2301. Pride GL, Schultz AE, Chuprevich TW,Buchler DA (1979). Primary invasive squa-mous carcinoma of the vagina. O b s t e tGynecol 53: 218-225. 2302. Pschera H, Wikstrom B (1991).Extraovarian Brenner tumor coexistingwith serous cystadenoma. Case report.Gynecol Obstet Invest 31: 185-187. 2303. Puget N, Gad S, Perrin-Vidoz L,Sinilnikova OM, Stoppa-Lyonnet D, LenoirGM, Mazoyer S (2002). Distinct BRCA1rearrangements involving the BRCA1pseudogene suggest the existence of arecombination hot spot. Am J Hum Genet70: 858-865.

409References
2304. Puls LE, Hamous J, Morrow MS,Schneyer A, MacLaughlin DT, CastracaneVD (1994). Recurrent ovarian sex cordtumor with annular tubules: tumor markerand chemotherapy experience. GynecolOncol 54: 396-401. 2305. Purola E, Savia E (1977). Cytology ofgynecologic condyloma acuminatum. ActaCytol 21: 26-31. 2306. Pysher TJ, Hitch DC, Krous HF (1981).Bilateral juvenile granulosa cell tumors ina 4-month-old dysmorphic infant. A clini-cal, histologic, and ultrastructural study.Am J Surg Pathol 5: 789-794. 2307. Qiao S, Nagasaka T, Harada T,Nakashima N (1998). p53, Bax and Bcl-2expression, and apoptosis in gestationaltrophoblast of complete hydatidiform mole.Placenta 19: 361-369. 2308. Qizilbash AH (1976). Cystosarcomaphyllodes with liposarcomatous stroma.Am J Clin Pathol 65: 321-327. 2309. Qizilbash AH, Patterson MC, OliveiraKF (1977). Adenoid cystic carcinoma of thebreast. Light and electron microscopy anda brief review of the literature. Arch PatholLab Med 101: 302-306. 2310. Quaglia MP, Brennan MF (2000). Theclinical approach to desmoplastic smallround cell tumor. Surg Oncol 9: 77-81. 2 3 1 1 . Quigley JC, Hart WR (1981).Adenomatoid tumors of the uterus. Am JClin Pathol 76: 627-635. 2312. Quincey C, Raitt N, Bell J, Ellis IO(1991). Intracytoplasmic lumina--a usefuldiagnostic feature of adenocarcinomas.Histopathology 19: 83-87. 2313. Quinn JM, McGee JO, Athanasou NA(1998). Human tumour-associatedmacrophages differentiate into osteoclas-tic bone-resorbing cells. J Pathol 184: 31-36. 2314. Quinn MA (1997). Adenocarcinoma ofthe cervix--are there arguments for a dif-ferent treatment policy? Curr Opin ObstetGynecol 9: 21-24. 2315. Quinn MA, Oster AO, Fortune D,Hudson B (1981). Sclerosing stromaltumour of the ovary case report withendocrine studies. Br J Obstet Gynaecol88: 555-558. 2316. Raber G, Mempel V, Jackisch C,Hundeiker M, Heinecke A, Kurzl R, GlaubitzM, Rompel R, Schneider HP (1996).Malignant melanoma of the vulva. Reportof 89 patients. Cancer 78: 2353-2358. 2317. Radford DM, Fair KL, Phillips NJ,Ritter JH, Steinbrueck T, Holt MS, Donis-Keller H (1995). Allelotyping of ductal carci-noma in situ of the breast: deletion of locion 8p, 13q, 16q, 17p and 17q. Cancer Res55: 3399-3405. 2318. Radhi JM (2000). Immunohistoche-mical analysis of pleomorphic lobular car-cinoma: higher expression of p53 andchromogranin and lower expression of ERand PgR. Histopathology 36: 156-160. 2319. Radig K, Buhtz P, Roessner A (1998).Alveolar soft part sarcoma of the uterinecorpus. Report of two cases and review ofthe literature. Pathol Res Pract 194: 59-63. 2320. Ragnarsson-Olding BK, Nilsson BR,Kanter-Lewensohn LR, Lagerlof B,Ringborg UK (1999). Malignant melanomaof the vulva in a nationwide, 25-year studyof 219 Swedish females: predictors of sur-vival. Cancer 86: 1285-1293. 2321. Rahilly MA, Williams AR, Krausz T, alNafussi A (1995). Female adnexal tumour ofprobable Wolffian origin: a clinicopatho-logical and immunohistochemical study ofthree cases. Histopathology 26: 69-74.
2322. Rajakariar R, Walker RA (1995).Pathological and biological features ofmammographically detected invasivebreast carcinomas. Br J Cancer 71: 150-154. 2323. Rajan JV, Marquis ST, Gardner HP,Chodosh LA (1997). Developmental expres-sion of Brca2 colocalizes with Brca1 and isassociated with proliferation and differen-tiation in multiple tissues. Dev Biol 184:385-401. 2324. Rajkumar T, Franceschi S, VaccarellaS, Gajalakshmi V, Sharmila A, Snijders PJ,Munoz N, Meijer CJ, Herrero R (2003). Roleof paan chewing and dietary habits in cer -vical carcinoma in Chennai, India. Br JCancer 88: 1388-1393. 2325. Raju U, Shah V, Perveen N, Linden M(2001). Evaluation of Breast Core NeedleBiopsies with CK 5/6, E-cadherin andCalponin. Mod Pathol 14: 34A. 2326. Raju U, Vertes D (1996). Breast papil -lomas with atypical ductal hyperplasia: aclinicopathologic study. Hum Pathol 2 7 :1231-1238. 2327. Raju UB, Lee MW, Zarbo RJ,Crissman JD (1989). Papillary neoplasia ofthe breast: immunohistochemicallydefined myoepithelial cells in the diagnosisof benign and malignant papillary breastneoplasms. Mod Pathol 2: 569-576. 2327 a. Ramachandra S, Machin L, AshleyS, Monaghan P, Gusterson BA (1990).Immunohistochemical distribution of c-erbB-2 in in situ breast carcinoma--adetailed morphological analysis. J Pathol161: 7-14. 2328. Ramaswamy S, Ross KN, Lander ES,Golub TR (2003). A molecular signature ofmetastasis in primary solid tumors. NatGenet 33: 49-54. 2329. Ramesh V, Iyengar B (1990).Proliferating trichilemmal cysts over thevulva. Cutis 45: 187-189. 2330. Ramos CV, Taylor HB (1974). Lipid-rich carcinoma of the breast. A clinico-pathologic analysis of 13 examples.Cancer 33: 812-819. 2331. Ramsay J, Birrell G, Lavin M (1998).Testing for mutations of the ataxia telang-iectasia gene in radiosensitive breast can-cer patients. Radiother Oncol 47: 125-128. 2332. Ramzy I (1976). Signet-ring stromaltumor of ovary. Histochemical, light, andelectron microscopic study. Cancer 3 8 :166-172. 2333. Randall ME, Kim JA, Mills SE, HahnSS, Constable WC (1986). Uncommon vari-ants of cervical carcinoma treated withradical irradiation. A clinicopathologicstudy of 66 cases. Cancer 57: 816-822. 2334. Rapin V, Contesso G, Mouriesse H,Bertin F, Lacombe MJ, Piekarski JD,Travagli JP, Gadenne C, Friedman S (1988).Medullary breast carcinoma. A reevalua-tion of 95 cases of breast cancer withinflammatory stroma. Cancer 61: 2503-2510. 2335. Rasbridge SA, Gillett CE, Millis RR(1993). Oestrogen and progesterone recep-tor expression in mammary fibromatosis. JClin Pathol 46: 349-351. 2336. Rasbridge SA, Gillett CE, SampsonSA, Walsh FS, Millis RR (1993). Epithelial(E-) and placental (P-) cadherin cell adhe-sion molecule expression in breast carci-noma. J Pathol 169: 245-250. 2336 a. Rasbridge SA, Millis RR (1995).Carcinoma in situ involving sclerosingadenosis: a mimic of invasive breast carci-noma. Histopathology 27: 269-273.
2337. Rasbridge SA, Millis RR, SampsonSA, Walsh FS (1992). Epithelial cadherinexpression in breast carcinomas. J Pathol167: 149. 2338. Rasmussen BB, Rose C, Thorpe SM,Andersen KW, Hou-Jensen K (1985).Argyrophilic cells in 202 human mucinousbreast carcinomas. Relation to histopatho-logic and clinical factors. Am J Clin Pathol84: 737-740. 2339. Rastkar G, Okagaki T, Twiggs LB,Clark BA (1982). Early invasive and in situwarty carcinoma of the vulva: clinical, his -tologic, and electron microscopic studywith particular reference to viral associa-tion. Am J Obstet Gynecol 143: 814-820. 2 3 4 0 . Rauscher FJ, III, Benjamin LE,Fredericks WJ, Morris JF (1994). Noveloncogenic mutations in the WT1 Wilms'tumor suppressor gene: a t(11;22) fuses theEwing's sarcoma gene, EWS1, to WT1 indesmoplastic small round cell tumor. ColdSpring Harb Symp Quant Biol 59: 137-146. 2341. Reardon W, Zhou XP, Eng C (2001). Anovel germline mutation of the PTEN genein a patient with macrocephaly, ventriculardilatation, and features of VATER associa-tion. J Med Genet 38: 820-823. 2342. Rebbeck TR, Kantoff PW, Krithivas K,Neuhausen S, Blackwood MA, Godwin AK,Daly MB, Narod SA, Garber JE, Lynch HT,Weber BL, Brown M (1999). Modification ofBRCA1-associated breast cancer risk bythe polymorphic androgen-receptor CAGrepeat. Am J Hum Genet 64: 1371-1377. 2343. Rebbeck TR, Levin AM, Eisen A,Snyder C, Watson P, Cannon-Albright L,Isaacs C, Olopade O, Garber JE, GodwinAK, Daly MB, Narod SA, Neuhausen SL,Lynch HT, Weber BL (1999). Breast cancerrisk after bilateral prophylactic oophorec-tomy in BRCA1 mutation carriers. J NatlCancer Inst 91: 1475-1479. 2344. Rebbeck TR, Lynch HT, NeuhausenSL, Narod SA, van't Veer L, Garber JE,Evans G, Isaacs C, Daly MB, Matloff E,Olopade OI, Weber BL (2002). Prophylacticoophorectomy in carriers of BRCA1 orBRCA2 mutations. N Engl J Med 346: 1616-1622. 2345. Rebbeck TR, Wang Y, Kantoff PW,Krithivas K, Neuhausen SL, Godwin AK,Daly MB, Narod SA, Brunet JS, Vesprini D,Garber JE, Lynch HT, Weber BL, Brown M(2001). Modification of BRCA1- andBRCA2-associated breast cancer risk byAIB1 genotype and reproductive history.Cancer Res 61: 5420-5424. 2346. Recht A, Rutgers EJ, Fentiman IS,Kurtz JM, Mansel RE, Sloane JP (1998).The fourth EORTC DCIS Consensus meet-ing (Chateau Marquette, Heemskerk, TheNetherlands, 23-24 January 1998)--confer -ence report. Eur J Cancer 34: 1664-1669. 2347. Reddy DB, Rao DB, Sarojini JS (1963).Extra-ovarian granulosa cell tumour. JIndian Med Assoc 41: 254-257. 2348. Redline RW, Hassold T, Zaragoza MV(1998). Prevalence of the partial molar phe-notype in triploidy of maternal and paternalorigin. Hum Pathol 29: 505-511. 2349. Reich O, Pickel H, Tamussino K,Winter R (2001). Microinvasive carcinomaof the cervix: site of first focus of invasion.Obstet Gynecol 97: 890-892. 2350. Reich O, Regauer S, Urdl W,Lahousen M, Winter R (2000). Expressionof oestrogen and progesterone receptorsin low-grade endometrial stromal sarco-mas. Br J Cancer 82: 1030-1034.
2351. Reiner A, Reiner G, Spona J,Schemper M, Holzner JH (1988).Histopathologic characterization of humanbreast cancer in correlation with estrogenreceptor status. A comparison of immuno-cytochemical and biochemical analysis.Cancer 61: 1149-1154. 2352. Reinfuss M, Stelmach A, Mitus J, RysJ, Duda K (1995). Typical medullary carci-noma of the breast: a clinical and patho-logical analysis of 52 cases. J Surg Oncol60: 89-94. 2353. Reitamo JJ, Scheinin TM, Hayry P(1986). The desmoid syndrome. Newaspects in the cause, pathogenesis andtreatment of the desmoid tumor. Am JSurg 151: 230-237. 2354. Renno SI, Moreland WS, PettenatiMJ, Beaty MW, Keung YK (2002). Primarymalignant lymphoma of uterine corpus:case report and review of the literature.Ann Hematol 81: 44-47. 2355. Report of an Advisory Group on Non-ionising Radiation (2001). ElectromagneticFields and the Risk of Cancer. Doc NRBP,Vol. 12(1): 3-179.2356. Resnick M, Lester S, Tate JE, SheetsEE, Sparks C, Crum CP (1996). Viral andhistopathologic correlates of MN andMIB-1 expression in cervical intraepithe-lial neoplasia. Hum Pathol 27: 234-239. 2357. Resta L, Maiorano E, Piscitelli D,Botticella MA (1994). Lipomatous tumors ofthe uterus. Clinico-pathological features of10 cases with immunocytochemical studyof histogenesis. Pathol Res Pract 190: 378-383. 2358. Revillion F, Bonneterre J, Peyrat J(1998). ERBB2 oncogene in human breastcancer and its clinical significance.European Journal of Cancer 34: 791-808. 2359. Reymundo C, Toro M, Morales C,Lopez-Beltran A, Nogales F, Nogales F Jr.(1993). Hyaline globules in uterine malig-nant mixed mullerian tumours. A diagnos-tic aid? Pathol Res Pract 189: 1063-1066. 2 3 6 0 . Rhatigan RM, Mojadidi Q (1973).Adenosquamous carcinomas of the vulvaand vagina. Am J Clin Pathol 60: 208-217. 2361. Rhatigan RM, Nuss RC (1985).Keratoacanthoma of the vulva. GynecolOncol 21: 118-123. 2361 a. Rhemtula H, Grayson W, vanIddekinge B, Tiltman A (2001). Large-cellneuroendocrine carcinoma of the uterinecervix--a clinicopathological study of fivecases. S Afr Med J 91: 525-528. 2362. Rhodes AR, Mihm MC Jr., WeinstockMA (1989). Dysplastic melanocytic nevi: areproducible histologic definition empha-sizing cellular morphology. Mod Pathol 2:306-319. 2363. Ribeiro GG, Phillips HV, Skinner LG(1980). Serum oestradiol-17 beta, testos-terone, luteinizing hormone and follicle-stimulating hormone in males with breastcancer. Br J Cancer 41: 474-477. 2364. Rice BF, Barclay DL, Sternberg WH(1969). Luteoma of pregnancy: steroido-genic and morphologic considerations.Am J Obstet Gynecol 104: 871-878. 2365. Rice LW, Berkowitz RS, Lage JM,Goldstein DP, Bernstein MR (1990).Persistent gestational trophoblastic tumorafter partial hydatidiform mole. GynecolOncol 36: 358-362. 2366. Richard F, Pacyna-Gengelbach M,Schluns K, Fleige B, Winzer KJ, Szymas J,Dietel M, Petersen I, Schwendel A (2000).Patterns of chromosomal imbalances ininvasive breast cancer. Int J Cancer 89:305-310.

410 References
2367. Richardson WW (1956). Medullarycarcinoma of the breast. A distinctivetumour type with a relatively good progno-sis following radical mastectomy. Br JCancer 10: 415-423. 2368. Richart RM (1973). Cervical intraep-ithelial neoplasia. Pathol Annu 8: 301-328. 2369. Ridley CM, Neill SM (1999). Non-infective cutaneous conditions of vulva inThe Vulva. 2nd ed. Malden, MA BlackwellScience: Oxford.2370. Ridolfi RL, Rosen PP, Port A, Kinne D,Mike V (1977). Medullary carcinoma of thebreast: a clinicopathologic study with 10year follow-up. Cancer 40: 1365-1385. 2371. Riedel I, Czernobilsky B, Lifschitz-Mercer B, Roth LM, Wu XR, Sun TT, Moll R(2001). Brenner tumors but not transitionalcell carcinomas of the ovary show urothe -lial differentiation: immunohistochemicalstaining of urothelial markers, includingcytokeratins and uroplakins. V i r c h o w sArch 438: 181-191. 2372. Rigaud C, Theobald S, Noel P,Badreddine J, Barlier C, Delobelle A,Gentile A, Jacquemier J, Maisongrosse V,Peffault de Latour M, Trojani M, Zafrani B(1993). Medullary carcinoma of the breast.A multicenter study of its diagnostic con-sistency. Arch Pathol Lab Med 117: 1005-1008. 2373. Riman T, Dickman PW, Nilsson S,Correia N, Nordlinder H, Magnusson CM,Weiderpass E, Persson IR (2002). Hormonereplacement therapy and the risk of inva-sive epithelial ovarian cancer in Swedishwomen. J Natl Cancer Inst 94: 497-504. 2374. Rimm DL, Sinard JH, Morrow JS(1995). Reduced alpha-catenin and E-cad-herin expression in breast cancer. LabInvest 72: 506-512. 2375. Rio PG, Pernin D, Bay JO, AlbuissonE, Kwiatkowski F, de Latour M, Bernard-Gallon DJ, Bignon YJ (1998). Loss of het-erozygosity of BRCA1, BRCA2 and ATMgenes in sporadic invasive ductal breastcarcinoma. Int J Oncol 13: 849-853. 2376. Riopel MA, Perlman EJ, Seidman JD,Kurman RJ, Sherman ME (1998). Inhibinand epithelial membrane antigen immuno-histochemistry assist in the diagnosis ofsex cord-stromal tumors and provide cluesto the histogenesis of hypercalcemic smallcell carcinomas. Int J Gynecol Pathol 17:46-53. 2377. Riopel MA, Ronnett BM, Kurman RJ(1999). Evaluation of diagnostic criteria andbehavior of ovarian intestinal-type muci-nous tumors: atypical proliferative (border-line) tumors and intraepithelial, microinva -sive, invasive, and metastatic carcinomas.Am J Surg Pathol 23: 617-635. 2378. Riopel MA, Spellerberg A, Griffin CA,Perlman EJ (1998). Genetic analysis ofovarian germ cell tumors by comparativegenomic hybridization. Cancer Res 5 8 :3105-3110. 2379. Rishi M, Howard LN, Bratthauer GL,Tavassoli FA (1997). Use of monoclonalantibody against human inhibin as a mark -er for sex cord-stromal tumors of theovary. Am J Surg Pathol 21: 583-589. 2380. Risinger JI, Berchuck A, Kohler MF,Boyd J (1994). Mutations of the E-cadheringene in human gynecologic cancers. NatGenet 7: 98-102. 2381. Ro JY, Silva EG, Gallager HS (1987).Adenoid cystic carcinoma of the breast.Hum Pathol 18: 1276-1281.
2382. Roa BB, Boyd AA, Volcik K, RichardsCS (1996). Ashkenazi Jewish populationfrequencies for common mutations inBRCA1 and BRCA2. Nat Genet 14: 185-187. 2383. Robbins GF, Berg JW (1964). Bilateralprimary breast cancers. A propective clin -ico-pathological study. Cancer 17: 1502-1527. 2384. Robbins GF, Shah J, Rosen P, Chu F,Taylor J (1974). Inflammatory carcinoma ofthe breast. Surg Clin North Am 54: 801-810. 2385. Robbins P, Pinder S, de Klerk N,Dawkins H, Harvey J, Sterrett G, Ellis I,Elston C (1995). Histological grading ofbreast carcinomas: a study of interobserv -er agreement. Hum Pathol 26: 873-879. 2386. Robboy SJ, Kaufman RH, Prat J,Welch WR, Gaffey T, Scully RE, Richart R,Fenoglio CM, Virata R, Tilley BC (1979).Pathologic findings in young womenenrolled in the National CooperativeDiethylstilbestrol Adenosis (DESAD) proj-ect. Obstet Gynecol 53: 309-317. 2387. Robboy SJ, Krigman HR, Donohue J,Scully RE (1995). Prognostic indices inmalignant struma ovarii: a clinicopatholog-ical analysis of 36 patients with 20-year fol-low up. Mod Pathol 8: 95A. 2 3 8 8 . Robboy SJ, Norris HJ, Scully RE(1975). Insular carcinoid primary in theovary. A clinicopathologic analysis of 48cases. Cancer 36: 404-418. 2389. Robboy SJ, Scully RE (1970). Ovarianteratoma with glial implants on the peri-toneum. An analysis of 12 cases. HumPathol 1: 643-653. 2390. Robboy SJ, Scully RE (1980). Strumalcarcinoid of the ovary: an analysis of 50cases of a distinctive tumor composed ofthyroid tissue and carcinoid. Cancer 46:2019-2034. 2391. Robboy SJ, Scully RE, Norris HJ(1974). Carcinoid metastatic to the ovary. Aclinocopathologic analysis of 35 cases.Cancer 33: 798-811. 2 3 9 2 . Robboy SJ, Scully RE, Norris HJ(1977). Primary trabecular carcinoid of theovary. Obstet Gynecol 49: 202-207. 2393. Robertson AJ, Brown RA, Cree IA,MacGillivray JB, Slidders W, Beck JS(1981). Prognostic value of measurementof elastosis in breast carcinoma. J ClinPathol 34: 738-743. 2394. Robles-Frias A, Severin CE, Robles-Frias MJ, Garrido JL (2001). Diffuse uterineleiomyomatosis with ovarian and parame-trial involvement. Obstet Gynecol 97: 834-835. 2395. Robles SC, White F, Peruga A (1996).Trends in cervical cancer mortality in theAmericas. Bull Pan Am Health Organ 30:290-301. 2396. Roca AN, Guajardo M, Estrada WJ(1980). Glial polyp of the cervix andendometrium. Report of a case and reviewof the literature. Am J Clin Pathol 73: 718-720. 2397. Rodolakis A, Papaspyrou I,Sotiropoulou M, Markaki S, Michalas S(2001). Primary squamous cell carcinomaof the endometrium. A report of 3 cases.Eur J Gynaecol Oncol 22: 143-146. 2398. Rodriguez-Bigas MA, Boland CR,Hamilton SR, Henson DE, Jass JR, KhanPM, Lynch H, Perucho M, Smyrk T, Sobin L,Srivastava S (1997). A National CancerInstitute Workshop on HereditaryNonpolyposis Colorectal CancerSyndrome: meeting highlights andBethesda guidelines. J Natl Cancer Inst 89:1758-1762.
2399. Rodriguez C, Patel AV, Calle EE,Jacob EJ, Thun MJ (2001). Estrogenreplacement therapy and ovarian cancermortality in a large prospective study of USwomen. JAMA 285: 1460-1465. 2400. Rodriguez HA, Ackerman LV (1968).Cellular blue nevus. Clinicopathologicstudy of forty-five cases. Cancer 21: 393-405. 2401. Rodriguez IM, Prat J (2002).Mucinous tumors of the ovary: a clinico-pathologic analysis of 75 borderline tumors(of intestinal type) and carcinomas. Am JSurg Pathol 26: 139-152. 2402. Rogers DA, Lobe TE, Rao BN, FlemingID, Schropp KP, Pratt AS, Pappo AS (1994).Breast malignancy in children. J PediatrSurg 29: 48-51. 2402a. Rojansky N, Ophir E, Sharony A,Spira H, Suprun H (1985). Broad ligamentadenocarcinoma--its origin and clinicalbehavior. A literature review and report ofa case. Obstet Gynecol Surv 40: 665-671. 2 4 0 3 . Rome RM, England PG (2000).Management of vaginal intraepithelialneoplasia: A series of 132 cases with long-term follow-up. Int J Gynecol Cancer 10:382-390. 2404. Roncaroli F, Lamovec J, Zidar A,Eusebi V (1996). Acinic cell-like carcinomaof the breast. Virchows Arch 429: 69-74. 2405. Roncaroli F, Riccioni L, Cerati M,Capella C, Calbucci F, Trevisan C, Eusebi V(1997). Oncocytic meningioma. Am J SurgPathol 21: 375-382. 2406. Ronnett BM, Kurman RJ, ShmooklerBM, Sugarbaker PH, Young RH (1997). Themorphologic spectrum of ovarian metas-tases of appendiceal adenocarcinomas: aclinicopathologic and immunohistochemi-cal analysis of tumors often misinterpretedas primary ovarian tumors or metastatictumors from other gastrointestinal sites.Am J Surg Pathol 21: 1144-1155. 2407. Ronnett BM, Kurman RJ, Zahn CM,Shmookler BM, Jablonski KA, Kass ME,Sugarbaker PH (1995). Pseudomyxomaperitonei in women: a clinicopathologicanalysis of 30 cases with emphasis on siteof origin, prognosis, and relationship toovarian mucinous tumors of low malignantpotential. Hum Pathol 26: 509-524. 2408. Ronnett BM, Shmookler BM, Diener-West M, Sugarbaker PH, Kurman RJ(1997). Immunohistochemical evidencesupporting the appendiceal origin ofpseudomyxoma peritonei in women. Int JGynecol Pathol 16: 1-9. 2409. Ronnett BM, Zahn CM, Kurman RJ,Kass ME, Sugarbaker PH, Shmookler BM(1995). Disseminated peritoneal adenomu-cinosis and peritoneal mucinous carcino-matosis. A clinicopathologic analysis of109 cases with emphasis on distinguishingpathologic features, site of origin, progno-sis, and relationship to "pseudomyxomaperitonei". Am J Surg Pathol 19: 1390-1408. 2410. Rorat E, Wallach RC (1984). Mixedtumors of the vulva: clinical outcome andpathology. Int J Gynecol Pathol 3: 323-328. 2411. Rosai J (1991). Borderline epitheliallesions of the breast. Am J Surg Pathol 15:209-221. 2412. Rose PG, Arafah B, Abdul-Karim FW(1998). Malignant struma ovarii: recur-rence and response to treatment moni-tored by thyroglobulin levels. G y n e c o lOncol 70: 425-427. 2413. Rosen PP (1983). Microglandularadenosis, a benign lesion simultating inva -sive mammary carcinoma. Am J SurgPathol 7: 137-144.
2414. Rosen PP (1983). Syringomatous ade-noma of the nipple. Am J Surg Pathol 7:739-745. 2415. Rosen PP (1983). Tumor emboli inintramammary lymphatics in breast carci-noma: pathologic criteria for diagnosis andclinical significance. Pathol Annu 18 Pt2:215-32.: 215-232. 2416. Rosen PP (1985). Vascular tumors ofthe breast. III. Angiomatosis. Am J SurgPathol 9: 652-658. 2417. Rosen PP (1986). Mucocele-liketumors of the breast. Am J Surg Pathol 10:464-469. 2418. Rosen PP (1987). Adenomyoepi-thelioma of the breast. Hum Pathol 18:1232-1237. 2419. Rosen PP (1989). Adenoid cystic car -cinoma of the breast. A morphologicallyheterogeneous neoplasm. Pathol Annu 24Pt 2: 237-254. 2420. Rosen PP (1997). Benign papillarytumors. In: Breast Pathology, PP Rosen(ed.), 1st ed. Lippincott-Raven:Philadelphia , pp. 67-104.2421. Rosen PP (1997). Carcinoma withmetaplasia. In: Rosen's Breast Pathology,PP Rosen (ed.), Lippincott-Raven:Philadelphia, pp. 375-395.2422. Rosen PP (1997). Glycogen-rich car-cinoma. In: Breast Pathology, PP Rosen(ed.), Lipincott-Raven, ed., Philadelphia/New York .2423. Rosen PP (1997). Mammary carcino-ma with osteoclast-like giant cells. In:Breast Pathology, PP Rosen (ed.),Lippincott-Raven, ed., Philadelphia/NewYork .2424. Rosen PP (1997). Metastases in thebreast from non-mammary malignant neo-plasms. In: Breast Pathology, PP Rosen(ed.), Lippincott-Raven, ed., Philadelphia/New York .2425. Rosen PP (1997). Rosen's BreastPathology. Lippincott-Raven: Philadelphia.2426. Rosen PP (1997). Rosen's BreastPathology. 2nd ed. Philadelphia.2427. Rosen PP (2001). Rosen's BreastPathology. Lippincott Williams and Wilkins:Philadelphia.2428. Rosen PP, Braun DW Jr., Lyngholm B,Urban JA, Kinne DW (1981). Lobular carci-noma in situ of the breast: preliminaryresults of treatment by ipsilateral mastec-tomy and contralateral breast biopsy.Cancer 47: 813-819. 2429. Rosen PP, Caicco JA (1986). Floridpapillomatosis of the nipple. A study of 51patients, including nine with mammarycarcinoma. Am J Surg Pathol 10: 87-101. 2430. Rosen PP, Cranor ML (1991).Secretory carcinoma of the breast. ArchPathol Lab Med 115: 141-144. 2431. Rosen PP, Ernsberger D (1987). Low-grade adenosquamous carcinoma. A vari-ant of metaplastic mammary carcinoma.Am J Surg Pathol 11: 351-358. 2432. Rosen PP, Ernsberger D (1989).Mammary fibromatosis. A benign spindle-cell tumor with significant risk for localrecurrence. Cancer 63: 1363-1369. 2433. Rosen PP, Groshen S, Kinne DW,Norton L (1993). Factors influencing prog-nosis in node-negative breast carcinoma:analysis of 767 T1N0M0/T2N0M0 patientswith long-term follow-up. J Clin Oncol 11:2090-2100.

411References
2 4 3 4 . Rosen PP, Groshen S, Saigo PE,Kinne DW, Hellman S (1989). Pathologicalprognostic factors in stage I (T1N0M0) andstage II (T1N1M0) breast carcinoma: astudy of 644 patients with median follow-up of 18 years. J Clin Oncol 7: 1239-1251. 2435. Rosen PP, Jozefczyk MA, Boram LH(1985). Vascular tumors of the breast. IV.The venous hemangioma. Am J SurgPathol 9: 659-665. 2436. Rosen PP, Kimmel M, Ernsberger D(1988). Mammary angiosarcoma. The prog-nostic significance of tumor differentiation.Cancer 62: 2145-2151. 2437. Rosen PP, Kinne DW, Lesser M,Hellman S (1986). Are prognostic factorsfor local control of breast cancer treatedby primary radiotherapy significant forpatients treated by mastectomy? Cancer57: 1415-1420. 2438. Rosen PP, Kosloff C, Lieberman PH,Adair F, Braun DW Jr. (1978). Lobular car-cinoma in situ of the breast. Detailedanalysis of 99 patients with average fol-low-up of 24 years. Am J Surg Pathol 2:225-251. 2439. Rosen PP, Lesser ML, Arroyo CD,Cranor M, Borgen P, Norton L (1995).Immunohistochemical detection ofHER2/neu in patients with axillary lymphnode negative breast carcinoma. A studyof epidemiologic risk factors, histologicfeatures, and prognosis. Cancer 75: 1320-1326. 2440. Rosen PP, Lesser ML, Arroyo CD,Cranor M, Borgen P, Norton L (1995). p53 innode-negative breast carcinoma: animmunohistochemical study of epidemio-logic risk factors, histologic features, andprognosis. J Clin Oncol 13: 821-830. 2441. Rosen PP, Lesser ML, Senie RT,Kinne DW (1982). Epidemiology of breastcarcinoma III: relationship of family historyto tumor type. Cancer 50: 171-179. 2442. Rosen PP, Oberman HA (1993). Atlasof Tumour Pathology. Tumour of theMammary Gland. Washington,D.C.2443. Rosen PP, Ridolfi RL (1977). The per-ilobular hemangioma. A benign microscop-ic vascular lesion of the breast. Am J ClinPathol 68: 21-23. 2444. Rosen PP, Saigo PE, Braun DW Jr.,Weathers E, Kinne DW (1981). Prognosis instage II (T1N1M0) breast cancer.Ann Surg194: 576-584. 2445. Rosen PP, Saigo PE, Braun DW Jr.,Weathers E, DePalo A (1981). Predictors ofrecurrence in stage I (T1N0M0) breast car-cinoma. Ann Surg 193: 15-25. 2446. Rosen PP, Senie R, Schottenfeld D,Ashikari R (1979). Noninvasive breast car-cinoma: frequency of unsuspected inva-sion and implications for treatment. AnnSurg 189: 377-382. 2447. Rosen PP, Wang T-Y (1980). Colloidcarcinoma of the breast. Analysis of 64patients with long term followup. Am J ClinPathol 73: 304. 2448. Rosenberg CR, Pasternack BS, ShoreRE, Koenig KL, Toniolo PG (1994).Premenopausal estradiol levels and therisk of breast cancer: a new method ofcontrolling for day of the menstrual cycle.Am J Epidemiol 140: 518-525. 2449. Rosenblatt KA, Thomas DB,McTiernan A, Austin MA, Stalsberg H,Stemhagen A, Thompson WD, Curnen MG,Satariano W, Austin DF, et al. (1991).Breast cancer in men: aspects of familialaggregation. J Natl Cancer Inst 83: 849-854.
2450. Rosenblatt KA, Weiss NS, SchwartzSM (1989). Incidence of malignant fallopi-an tube tumors. Gynecol Oncol 35: 236-239. 2451. Rosenfeld WD, Rose E, Vermund SH,Schreiber K, Burk RD (1992). Follow-upevaluation of cervicovaginal human papil-lomavirus infection in adolescents. JPediatr 121: 307-311. 2452. Roses DF, Bell DA, Flotte TJ, Taylor R,Ratech H, Dubin N (1982). Pathologic pre-dictors of recurrence in stage 1 (TINOMO)breast cancer. Am J Clin Pathol 78: 817-820. 2453. Rosner D, Lane WW, Penetrante R(1991). Ductal carcinoma in situ withmicroinvasion. A curable entity using sur-gery alone without need for adjuvant ther-apy. Cancer 67: 1498-1503. 2454. Ross JC, Eifel PJ, Cox RS, KempsonRL, Hendrickson MR (1983). Primary muci-nous adenocarcinoma of the endometrium.A clinicopathologic and histochemicalstudy. Am J Surg Pathol 7: 715-729. 2455. Ross LD (1984). Hilus cell tumour ofthe ovary with an associated endometrialcarcinoma, presenting with male patternbaldness and postmenopausal bleeding.Case report. Br J Obstet Gynaecol 91: 1266-1268. 2456. Ross MJ, Welch WR, Scully RE(1989). Multilocular peritoneal inclusioncysts (so-called cystic mesotheliomas).Cancer 64: 1336-1346. 2457. Rossi G, Bonacorsi G, Longo L, ArtusiT, Rivasi F (2001). Primary high-grademucosa-associated lymphoid tissue-typelymphoma of the cervix presenting as acommon endocervical polyp. Arch PatholLab Med 125: 537-540. 2458. Rossing MA, Daling JR, Weiss NS,Moore DE, Self SG (1994). Ovarian tumorsin a cohort of infertile women. N Engl JMed 331: 771-776. 2459. Roth LM, Anderson MC, Govan AD,Langley FA, Gowing NF, Woodcock AS(1981). Sertoli-Leydig cell tumors: a clinico-pathologic study of 34 cases. Cancer 48:187-197. 2460. Roth LM, Czernobilsky B (1985).Ovarian Brenner tumors. II. Malignant.Cancer 56: 592-601. 2461. Roth LM, Dallenbach-Hellweg G,Czernobilsky B (1985). Ovarian Brennertumors. I. Metaplastic, proliferating, and oflow malignant potential. Cancer 56: 582-591. 2462. Roth LM, Davis MM, Sutton GP(1996). Steroid cell tumor of the broad liga -ment arising in an accessory ovary. ArchPathol Lab Med 120: 405-409. 2463. Roth LM, Deaton RL, Sternberg WH(1979). Massive ovarian edema. A clinico-pathologic study of five cases includingultrastructural observations and review ofthe literature. Am J Surg Pathol 3: 11-21. 2464. Roth LM, Gersell DJ, Ulbright TM(1993). Ovarian Brenner tumors and transi -tional cell carcinoma: recent develop-ments. Int J Gynecol Pathol 12: 128-133. 2465. Roth LM, Gersell DJ, Ulbright TM(1996). Transitional cell carcinoma andother transitional cell tumors of the ovary.Anat Pathol 1: 179-191. 2466. Roth LM, Liban E, Czernobilsky B(1982). Ovarian endometrioid tumors mim-icking Sertoli and Sertoli-Leydig celltumors: Sertoliform variant of endometrioidcarcinoma. Cancer 50: 1322-1331.
2467. Roth LM, Look KY (2000). Inverted fol-licular keratosis of the vulvar skin: a lesionthat can be confused with squamous cellcarcinoma. Int J Gynecol Pathol 19: 369-373. 2468. Roth LM, Nicholas TR, Ehrlich CE(1979). Juvenile granulosa cell tumor: aclinicopathologic study of three cases withultrastructural observations. Cancer 4 4 :2194-2205. 2469. Roth LM, Reed RJ (1999). Dissectingleiomyomas of the uterus other thancotyledonoid dissecting leiomyomas: areport of eight cases. Am J Surg Pathol 23:1032-1039. 2470. Roth LM, Reed RJ, Sternberg WH(1996). Cotyledonoid dissecting leiomyomaof the uterus. The Sternberg tumor. Am JSurg Pathol 20: 1455-1461. 2471. Roth LM, Slayton RE, Brady LW,Blessing JA, Johnson G (1985). Retiformdifferentiation in ovarian Sertoli-Leydigcell tumors. A clinicopathologic study ofsix cases from a Gynecologic OncologyGroup study. Cancer 55: 1093-1098. 2472. Roth LM, Sternberg WH (1973).Ovarian stromal tumors containing Leydigcells. II. Pure Leydig cell tumor, non-hilartype. Cancer 32: 952-960. 2473. Rothbard MJ, Markham EH (1974).Leiomyosarcoma of the cervix: report of acase. Am J Obstet Gynecol 120: 853-854. 2474. Royar J, Becher H, Chang-Claude J(2001). Low-dose oral contraceptives: pro-tective effect on ovarian cancer risk. Int JCancer 95: 370-374. 2475. Roylance R, Gorman P, Hanby A,Tomlinson I (2002). Allelic imbalanceanalysis of chromosome 16q shows thatgrade I and grade III invasive ductal breastcancers follow different genetic pathways.J Pathol 196: 32-36. 2476. Roylance R, Gorman P, Harris W,Liebmann R, Barnes D, Hanby A, Sheer D(1999). Comparative genomic hybridizationof breast tumors stratified by histologicalgrade reveals new insights into the biolog-ical progression of breast cancer. CancerRes 59: 1433-1436. 2477. Rozan S, Vincent-Salomon A, ZafraniB, Validire P, de Cremoux P, Bernoux A,Nieruchalski M, Fourquet A, Clough K,Dieras V, Pouillart P, Sastre-Garau X(1998). No significant predictive value of c-erbB-2 or p53 expression regarding sensi-tivity to primary chemotherapy or radio-therapy in breast cancer. Int J Cancer 79:27-33. 2478. Rubens JR, Lewandrowski KB,Kopans DB, Koerner FC, Hall DA, McCarthyKA (1990). Medullary carcinoma of thebreast. Overdiagnosis of a prognosticallyfavorable neoplasm. Arch Surg 125: 601-604. 2479. Rubin SC, Benjamin I, Behbakht K,Takahashi H, Morgan MA, LiVolsi VA,Berchuck A, Muto MG, Garber JE, WeberBL, Lynch HT, Boyd J (1996). Clinical andpathological features of ovarian cancer inwomen with germ-line mutations ofBRCA1. N Engl J Med 335: 1413-1416. 2480. Rubin SC, Young J, Mikuta JJ (1985).Squamous carcinoma of the vagina: treat-ment, complications, and long-term follow-up. Gynecol Oncol 20: 346-353. 2481. Rubio IT, Korourian S, Brown H,Cowan C, Klimberg VS (1998). Carcinoidtumor metastatic to the breast. Arch Surg133: 1117-1119. 2482. Rudan I, Rudan N, Skoric T, SarcevicB (1996). Fibromatosis of male breast. ActaMed Croatica 50: 157-159.
2483. Rudas M, Neumayer R, Gnant MF,Mittelbock M, Jakesz R, Reiner A (1997).p53 protein expression, cell proliferationand steroid hormone receptors in ductaland lobular in situ carcinomas of thebreast. Eur J Cancer 33: 39-44. 2484. Rudas M, Schmidinger M, Wenzel C,Okamoto I, Budinsky A, Fazeny B, Marosi C(2000). Karyotypic findings in two cases ofmale breast cancer. Cancer GenetCytogenet 121: 190-193. 2485. Ruffolo EF, Koerner FC, Maluf HM(1997). Metaplastic carcinoma of thebreast with melanocytic differentiation.Mod Pathol 10: 592-596. 2486. Ruggieri AM, Brody JM, Curhan RP(1996). Vaginal leiomyoma. A case reportwith imaging findings. J Reprod Med 41:875-877. 2487. Runnebaum IB, Wang-Gohrke S,Vesprini D, Kreienberg R, Lynch H, MoslehiR, Ghadirian P, Weber B, Godwin AK, RischH, Garber J, Lerman C, Olopade OI, FoulkesWD, Karlan B, Warner E, Rosen B,Rebbeck T, Tonin P, Dube MP, Kieback DG,Narod SA (2001). Progesterone receptorvariant increases ovarian cancer risk inBRCA1 and BRCA2 mutation carriers whowere never exposed to oral contracep-tives. Pharmacogenetics 11: 635-638. 2488. Rush DS, Tan J, Baergen RN, SoslowRA (2001). h-Caldesmon, a novel smoothmuscle-specific antibody, distinguishesbetween cellular leiomyoma and endome-trial stromal sarcoma. Am J Surg Pathol 25:253-258. 2489. Russell P (1979). The pathologicalassessment of ovarian neoplasms. I:Introduction to the common 'epithelial'tumours and analysis of benign 'epithelial'tumours. Pathology 11: 5-26. 2490. Russell P (1979). The pathologicalassessment of ovarian neoplasms. II: Theproliferating 'epithelial' tumours.Pathology 11: 251-282. 2491. Russell P, Merkur H (1979).Proliferating ovarian "epithelial" tumours: aclinico-pathological analysis of 144 cases.Aust N Z J Obstet Gynaecol 19: 45-51. 2492. Russell P, Wills EJ, Watson G, Lee J,Geraghty T (1995). Monomorphic (basalcell) salivary adenoma of ovary: report of acase. Ultrastruct Pathol 19: 431-438. 2493. Russell PA, Pharoah PD, De Foy K,Ramus SJ, Symmonds I, Wilson A, Scott I,Ponder BA, Gayther SA (2000). Frequentloss of BRCA1 mRNA and protein expres-sion in sporadic ovarian cancers. Int JCancer 87: 317-321. 2494. Russo L, Woolmough E, Heatley MK(2000). Structural and cell surface antigenexpression in the rete ovarii andepoophoron differs from that in theFallopian tube and in endometriosis.Histopathology 37: 64-69. 2495. Rutgers JL, Scully RE (1988). Cysts(cystadenomas) and tumors of the reteovarii. Int J Gynecol Pathol 7: 330-342. 2496. Rutgers JL, Scully RE (1988). Ovarianmixed-epithelial papillary cystadenomas ofborderline malignancy of mullerian type. Aclinicopathologic analysis. Cancer 61: 546-554. 2497. Rutgers JL, Scully RE (1988). Ovarianmullerian mucinous papillary cystadeno-mas of borderline malignancy. A clinico-pathologic analysis. Cancer 61: 340-348. 2498. Rutgers JL, Scully RE (1991). Theandrogen insensitivity syndrome (testicu-lar feminization): a clinicopathologic studyof 43 cases. Int J Gynecol Pathol 10: 126-144.

412 References
2499. Rutledge F (1967). Cancer of the vagi-na. Am J Obstet Gynecol 97: 635-655. 2500. Rutqvist LE, Wallgren A (1983).Influence of age on outcome in breast car-cinoma. Acta Radiol Oncol 22: 289-294. 2501. Rywlin AM, Simmons RJ, RobinsonMJ (1969). Leiomyoma of vagina recurrentin pregnancy: a case with apparent hor-mone dependency. South Med J 62: 1449-1451. 2502. Sabini G, Chumas JC, Mann WJ(1992). Steroid hormone receptors inendometrial stromal sarcomas. A bio-chemical and immunohistochemical study.Am J Clin Pathol 97: 381-386. 2503. Safe SH (1997). Xenoestrogens andbreast cancer. N Engl J Med 337: 1303-1304. 2504. Saffos RO, Rhatigan RM, Scully RE(1980). Metaplastic papillary tumor of thefallopian tube--a distinctive lesion of preg -nancy. Am J Clin Pathol 74: 232-236. 2505. Sagebiel R.W. (1969). Ultrastructuralobservations on epidermal cells in Paget'sdisease of the breast. Am J Pathol 1: 49-64. 2506. Sahin A, Benda JA (1988). Primaryovarian Wilms' tumor. Cancer 61: 1460-1463. 2507. Sahin AA, Silva EG, Ordonez NG(1989). Alveolar soft part sarcoma of theuterine cervix. Mod Pathol 2: 676-680. 2508. Saigo PE, Rosen PP (1981). Mammarycarcinoma with "choriocarcinomatous"features. Am J Surg Pathol 5: 773-778. 2509. Sainsbury JR, Farndon JR, NeedhamGK, Malcolm AJ, Harris AL (1987).Epidermal-growth-factor receptor statusas predictor of early recurrence of anddeath from breast cancer. Lancet 1: 1398-1402. 2510. Saint Aubain SN, Larsimont D,Cluydts N, Heymans O, Verhest A (1997).Pseudoangiomatous hyperplasia of mam-mary stroma in an HIV patient. Gen DiagnPathol 143: 251-254. 2511. Sainz dlC, Eichhorn JH, Rice LW,Fuller AF Jr., Nikrui N, Goff BA (1996).Histologic transformation of benignendometriosis to early epithelial ovariancancer. Gynecol Oncol 60: 238-244. 2512. Saitoh A, Tsutsumi Y, Osamura RY,Watanabe K (1989). Sclerosing stromaltumor of the ovary. Immunohistochemicaland electron-microscopic demonstrationof smooth-muscle differentiation. A r c hPathol Lab Med 113: 372-376. 2513. Sakamoto A, Sasaki H, Furusato M,Suzuki M, Hirai Y, Tsugane S, FukushimaM, Terashima Y (1994). Observer disagree -ment in histological classification of ovari -an tumors in Japan. Gynecol Oncol 54: 54-58. 2514. Sakuragi N, Satoh C, Takeda N,Hareyama H, Takeda M, Yamamoto R,Fujimoto T, Oikawa M, Fujino T, Fujimoto S(1999). Incidence and distribution patternof pelvic and paraaortic lymph nodemetastasis in patients with Stages IB, IIA,and IIB cervical carcinoma treated withradical hysterectomy. Cancer 85: 1547-1554. 2515. Salazar H, Kanbour A, Tobon H,Gonzalez-Angulo A (1974). Endoderm cellderivatives in embryonal carcinoma of theovary: an electron microscopic study oftwo cases. Am J Pathol 74: 108 A.
2516. Salovaara R, Loukola A, Kristo P,Kaariainen H, Ahtola H, Eskelinen M,Harkonen N, Julkunen R, Kangas E, OjalaS, Tulikoura J, Valkamo E, Jarvinen H,Mecklin JP, Aaltonen LA, de la CA (2000).Population-based molecular detection ofhereditary nonpolyposis colorectal can-cer. J Clin Oncol 18: 2193-2200. 2517. Saltzstein SL (1974). Clinically occultinflammatory carcinoma of the breast.Cancer 34: 382-388. 2518. Salvesen HB, MacDonald N, Ryan A,Iversen OE, Jacobs IJ, Akslen LA, Das S(2000). Methylation of hMLH1 in a popula-tion-based series of endometrial carcino-mas. Clin Cancer Res 6: 3607-3613. 2519. Samanth KK, Black WC, III (1970).Benign ovarian stromal tumors associatedwith free peritoneal fluid. Am J ObstetGynecol 107: 538-545. 2520. Samuels TH, Miller NA, Manchul LA,DeFreitas G, Panzarella T (1996).Squamous cell carcinoma of the breast.Can Assoc Radiol J 47: 177-182. 2521. Sanchez AG, Villanueva AG, RedondoC (1986). Lobular carcinoma of the breast ina patient with Klinefelter's syndrome. Acase with bilateral, synchronous, histolog -ically different breast tumors. Cancer 57:1181-1183. 2522. Sander CM (1993). Angiomatous mal-formation of placental chorionic stem ves -sels and pseudo-partial molar placentas:report of five cases. Pediatr Pathol 13: 621-633. 2523. Sangwan K, Khosla AH, Hazra PC(1996). Leiomyoma of the vagina. Aust N ZJ Obstet Gynaecol 36: 494-495. 2524. Sanjeevi CB, Hjelmstrom P, HallmansG, Wiklund F, Lenner P, Angstrom T, DillnerJ, Lernmark A (1996). Different HLA-DR-DQhaplotypes are associated with cervicalintraepithelial neoplasia among humanpapillomavirus type-16 seropositive andseronegative Swedish women. Int JCancer 68: 409-414. 2525. Sankaranarayanan R, Black RJ,Parkin DM (1998). Cancer Survival inDeveloping Countries. IARC: Lyon.2526. Sankila R, Aaltonen LA, Jarvinen HJ,Mecklin JP (1996). Better survival rates inpatients with MLH1-associated hereditarycolorectal cancer. Gastroenterology 110:682-687. 2527. Sano T, Oyama T, Kashiwabara K,Fukuda T, Nakajima T (1998). Expressionstatus of p16 protein is associated withhuman papillomavirus oncogenic potentialin cervical and genital lesions. Am JPathol 153: 1741-1748. 2528. Santesson L, Kottmeier HL (1968).General classification of ovarian tumours.In: Ovarian Cancer, Gentil F, Junquiera AC,eds., Springer-Verlag: New York , pp. 1-8.2529. Santeusanio G, Schiaroli S, AnemonaL, Sesti F, Valli E, Piccione E, Spagnoli LG(1991). Carcinoma of the vulva with sarco-matoid features: a case report withimmunohistochemical study. G y n e c o lOncol 40: 160-163. 2530. Santini D, Gelli MC, Mazzoleni G,Ricci M, Severi B, Pasquinelli G, Pelusi G,Martinelli G (1989). Brenner tumor of theovary: a correlative histologic, histochemi-cal, immunohistochemical, and ultrastruc-tural investigation. Hum Pathol 20: 787-795. 2531. Santos MJ, Gonzalez SS, CarreteroAL (2000). Breast metastases from embry-onal rhabdomyosarcoma: apropos 2 casesand a review of the literature. Rev Clin Esp200: 21-25.
2532. Sanz-Ortega J, Chuaqui R, Zhuang Z,Sobel ME, Sanz-Esponera J, Liotta LA,Emmert-Buck MR, Merino MJ (1995). Lossof heterozygosity on chromosome 11q13 inmicrodissected human male breast carci-nomas. J Natl Cancer Inst 87: 1408-1410. 2 5 3 3 . Sapino A, Bussolati G (2002). Isdetection of endocrine cells in breast ade -nocarcinoma of diagnostic and clinicalsignificance? Histopathology 40: 211-214. 2534. Sapino A, Frigerio A, Peterse JL,Arisio R, Coluccia C, Bussolati G (2000).Mammographically detected in situ lobularcarcinomas of the breast. Virchows Arch436: 421-430. 2535. Sapino A, Righi L, Cassoni P, PapottiM, Gugliotta P, Bussolati G (2001).Expression of apocrine differentiationmarkers in neuroendocrine breast carci-nomas of aged women. Mod Pathol 14:768-776. 2536. Sapino A, Righi L, Cassoni P, PapottiM, Pietribiasi F, Bussolati G (2000).Expression of the neuroendocrine pheno-type in carcinomas of the breast. SeminDiagn Pathol 17: 127-137. 2536 a. Sartwell PE, Arthes FG, TonasciaJA (1978). Benign and malignant breasttumours: epidemiological similarities. Int JEpidemiol 7: 217-221. 2537. Sasano H, Mason JI, Sasaki E, YajimaA, Kimura N, Namiki T, Sasano N, NaguraH (1990). Immunohistochemical study of 3beta-hydroxysteroid dehydrogenase in sexcord-stromal tumors of the ovary. Int JGynecol Pathol 9: 352-362. 2538. Sasano H, Sato S, Yajima A, Akama J,Nagura H (1997). Adrenal rest tumor of thebroad ligament: case report with immuno-histochemical study of steroidogenicenzymes. Pathol Int 47: 493-496. 2539. Sasco AJ, Lowenfels AB, Pasker-deJong P (1993). Epidemiology of male breastcancer. A meta-analysis of publishedcase-control studies and discussion ofselected aetiological factors. Int J Cancer53: 538-549. 2540. Sashiyama H, Abe Y, Miyazawa Y,Nagashima T, Hasegawa M, Okuyama K,Kuwahara T, Takagi T (1999). Primary Non-Hodgkin's Lymphoma of the Male Breast:A Case Report. Breast Cancer 6: 55-58. 2541. Sastre-Garau X, Jouve M, AsselainB, Vincent-Salomon A, Beuzeboc P, DorvalT, Durand JC, Fourquet A, Pouillart P(1996). Infiltrating lobular carcinoma of thebreast. Clinicopathologic analysis of 975cases with reference to data on conserva-tive therapy and metastatic patterns.Cancer 77: 113-120. 2 5 4 2 . Satake T, Matsuyama M (1991).Endocrine cells in a normal breast andnon-cancerous breast lesion. Acta PatholJpn 41: 874-878. 2 5 4 3 . Sato N, Tsunoda H, Nishida M,Morishita Y, Takimoto Y, Kubo T, NoguchiM (2000). Loss of heterozygosity on 10q23.3and mutation of the tumor suppressor genePTEN in benign endometrial cyst of theovary: possible sequence progressionfrom benign endometrial cyst toendometrioid carcinoma and clear cellcarcinoma of the ovary. Cancer Res 60:7052-7056. 2544. Sau P, Solis J, Lupton GP, James WD(1989). Pigmented breast carcinoma. Aclinical and histopathologic simulator ofmalignant melanoma. Arch Dermatol 125:536-539.
2545. Savey L, Lasser P, Castaigne D,Michel G, Bognel C, Colau JC (1996).[Krukenberg tumors. Analysis of a series of28 cases]. J Chir (Paris) 133: 427-431. 2546. Savitsky K, Bar-Shira A, Gilad S,Rotman G, Ziv Y, Vanagaite L, Tagle DA,Smith S, Uziel T, Sfez S, Ashkenazi M,Pecker I, frydman M, Harnik R, PatanjaliSR, Simmons A, Clines GA, Sartiel A, GattiRA, Chessa L, Sanal O, Lavin MF, JaspersNGJ, Malcolm A, Taylor R, Arlett CF, Miki T,Weissman SM, Lovett M, Collins FS, ShilohH. (1995). A single ataxia telangiectasiagene with a product similar to PI-3 kinase.Science 268: 1749-1753. 2547. Savitsky K, Platzer M, Uziel T, Gilad S,Sartiel A, Rosenthal A, Elroy-Stein O,Shiloh Y, Rotman G (1997). Ataxia-telang-iectasia: structural diversity of untranslat-ed sequences suggests complex post-transcriptional regulation of ATM geneexpression. Nucleic Acids Res 25: 1678-1684. 2 5 4 8 . Scarff RW, Torloni H (1968).International Histological Classification ofTumours, n°2. Histological Typing ofBreast Tumours. World HealthOrganization: Geneva.2549. Scatarige JC, Hsiu JG, de la TR,Cramer MS, Siddiky MA, Jaffe AH (1987).Acoustic shadowing in benign granularcell tumor (myoblastoma) of the breast. JUltrasound Med 6: 545-547. 2550. Schammel DP, Silver SA, TavassoliFA (1999). Combined endometrial stro-mal/smooth muscle neoplasms of theuterus: clinicopathologic study of 38cases. Mod Pathol 12: 124A. 2551. Schammel DP, Tavassoli FA (1998).Uterine angiosarcomas: a morphologicand immunohistochemical study of fourcases. Am J Surg Pathol 22: 246-250. 2552. Scheidbach H, Dworak O,Schmucker B, Hohenberger W (2000).Lobular carcinoma of the breast in an 85-year-old man. Eur J Surg Oncol 26: 319-321. 2553. Scheistroen M, Trope C, Kaern J,Pettersen EO, Alfsen GC, Nesland JM(1997). DNA ploidy and expression of p53and C-erbB-2 in extramammary Paget'sdisease of the vulva. Gynecol Oncol 64: 88-92. 2554. Scheithauer B, Woodruff JM (1999).Tumours of the Peripheral NervousSystem. AFIP: Washington, DC.2555. Schell SR, Montague ED, Spanos WJJr., Tapley ND, Fletcher GH, Oswald MJ(1982). Bilateral breast cancer in patientswith initial stage I and II disease. Cancer50: 1191-1194. 2556. Schernhammer ES, Laden F, SpeizerFE, Willett WC, Hunter DJ, Kawachi I,Colditz GA (2001). Rotating night shifts andrisk of breast cancer in women participat-ing in the nurses' health study. J NatlCancer Inst 93: 1563-1568. 2556a. Schildkraut JM, Risch N, ThompsonWD (1989). Evaluating genetic associationamong ovarian, breast, and endometrialcancer: evidence for a breast/ovarian can-cer relationship. Am J Hum Genet 45: 521-529. 2 5 5 7 . Schildkraut JM, Thompson WD(1988). Familial ovarian cancer: a popula-tion-based case-control study. Am JEpidemiol 128: 456-466. 2558. Schlesinger C, Kamoi S, Ascher SM,Kendell M, Lage JM, Silverberg SG (1998).Endometrial polyps: a comparison study ofpatients receiving tamoxifen with two con-trol groups. Int J Gynecol Pathol 17: 302-311.

413References
2559. Schlesinger C, Silverberg SG (1999).Endocervical adenocarcinoma in situ oftubal type and its relation to atypical tubalmetaplasia. Int J Gynecol Pathol 18: 1-4. 2560. Schmidt-Kittler O, Ragg T, DaskalakisA, Granzow M, Ahr A, Blankenstein TJ,Kaufmann M, Diebold J, Arnholdt H, MullerP, Bischoff J, Harich D, Schlimok G,Riethmuller G, Eils R, Klein CA (2003). Fromlatent disseminated cells to overt metasta-sis: genetic analysis of systemic breastcancer progression. Proc Natl Acad SciUSA 100: 7737-7742. 2561. Schmitt FC, Ribeiro CA, Alvarenga S,Lopes JM (2000). Primary acinic cell-likecarcinoma of the breast--a variant withgood prognosis? Histopathology 36: 286-289. 2562. Schmitz MJ, Hendricks DT, Farley J,Taylor RR, Geradts J, Rose GS, Birrer MJ(2000). p27 and cyclin D1 abnormalities inuterine papillary serous carcinoma.Gynecol Oncol 77: 439-445. 2563. Schmutte C, Marinescu RC, CopelandNG, Jenkins NA, Overhauser J, Fishel R(1998). Refined chromosomal localizationof the mismatch repair and hereditary non-polyposis colorectal cancer genes hMSH2and hMSH6. Cancer Res 58: 5023-5026. 2564. Schnarkowski P, Kessler M, ArnholdtH, Helmberger T (1997). Angiosarcoma ofthe breast: mammographic, sonographic,and pathological findings. Eur J Radiol 24:54-56. 2 5 6 5 . Schneider A, de Villiers EM,Schneider V (1987). Multifocal squamousneoplasia of the female genital tract: sig-nificance of human papillomavirus infec-tion of the vagina after hysterectomy.Obstet Gynecol 70: 294-298. 2566. Schneider C, Wight E, Perucchini D,Haller U, Fink D (2000). Primary carcinomaof the fallopian tube. A report of 19 caseswith literature review. Eur J GynaecolOncol 21: 578-582. 2567. Schneider JA (1989). Invasive papil-lary breast carcinoma: mammographic andsonographic appearance. Radiology 171:377-379. 2568. Schneider V, Zimberg ST, Kay S(1981). The pigmented portio: benign lenti-go of the uterine cervix. Diagn GynecolObstet 3: 269-272. 2569. Schnitt SJ (1997). Morphologic riskfactors for local recurrence in patientswith invasive breast cancer treated withconservative surgery and radiation thera-py. Breast J. 3: 261-266. 2570. Schnitt SJ, Connolly JL, Recht A,Silver B, Harris JR (1989). Influence of infil-trating lobular histology on local tumorcontrol in breast cancer patients treatedwith conservative surgery and radiothera-py. Cancer 64: 448-454. 2571. Schnitt SJ, Connolly JL, Tavassoli FA,Fechner RE, Kempson RL, Gelman R, PageDL (1992). Interobserver reproducibility inthe diagnosis of ductal proliferative breastlesions using standardized criteria. Am JSurg Pathol 16: 1133-1143. 2 5 7 2 . Schnuch A (1993). [Post hoc orpropter hoc? On the heuristics of side-effects in the example of gynecomastia].Dtsch Med Wochenschr 118: 796-803. 2 5 7 3 . Schorge JO, Lee KR, Sheets EE(2000). Prospective management of stageIA(1) cervical adenocarcinoma by coniza-tion alone to preserve fertility: a prelimi-nary report. Gynecol Oncol 78: 217-220.
2574. Schorge JO, Miller YB, Qi LJ, MutoMG, Welch WR, Berkowitz RS, Mok SC(2000). Genetic alterations of the WT1 genein papillary serous carcinoma of the peri-toneum. Gynecol Oncol 76: 369-372. 2575. Schorge JO, Muto MG, Lee SJ,Huang LW, Welch WR, Bell DA, Keung EZ,Berkowitz RS, Mok SC (2000). BRCA1-relat-ed papillary serous carcinoma of the peri-toneum has a unique molecular pathogen -esis. Cancer Res 60: 1361-1364. 2576. Schorge JO, Muto MG, Welch WR,Bandera CA, Rubin SC, Bell DA, BerkowitzRS, Mok SC (1998). Molecular evidence formultifocal papillary serous carcinoma ofthe peritoneum in patients with germlineBRCA1 mutations. J Natl Cancer Inst 90:841-845. 2577. Schottenfeld D, Lilienfeld AM,Diamond H (1963). Some observations onthe epidemiology of breast cancer amongmales. Am J Publ Hlth 53: 890-897. 2578. Schrager CA, Schneider D, GruenerAC, Tsou HC, Peacocke M (1998). Clinicaland pathological features of breast dis-ease in Cowden's syndrome: an underrec -ognized syndrome with an increased riskof breast cancer. Hum Pathol 29: 47-53. 2579. Schuh ME, Nemoto T, Penetrante RB,Rosner D, Dao TL (1986). Intraductal carci -noma. Analysis of presentation, pathologicfindings, and outcome of disease. ArchSurg 121: 1303-1307. 2580. Schultz DM (1957). A malignant, mel-onotic neoplasm of the uterus, resemblingthe "retinal anlage" tumours. Arch Pathol28: 524-532. 2581. Schurch W, Potvin C, Seemayer TA(1985). Malignant myoepithelioma (myoep -ithelial carcinoma) of the breast: an ultra-structural and immunocytochemical study.Ultrastruct Pathol 8: 1-11. 2582. Schuuring E, Verhoeven E, vanTinteren H, Peterse JL, Nunnink B,Thunnissen FB, Devilee P, Cornelisse CJ,Van de Vijver MJ, Mooi WJ, MichalidesRJAM. (1992). Amplification of genes with -in the chromosome 11q13 region is indica-tive of poor prognosis in patients withoperable breast cancer. Cancer Res 52:5229-5234. 2583. Schwartz GF, Feig SA, Rosenberg AL,Patchefsky AS, Schwartz AB (1984).Staging and treatment of clinically occultbreast cancer. Cancer 53: 1379-1384. 2584. Schwartz GF, Patchefsky AS,Finklestein SD, Sohn SH, Prestipino A, FeigSA, Singer JS (1989). Nonpalpable in situductal carcinoma of the breast. Predictorsof multicentricity and microinvasion andimplications for treatment. Arch Surg 124:29-32. 2585. Schwartz IS, Strauchen JA (1990).Lymphocytic mastopathy. An autoimmunedisease of the breast? Am J Clin Pathol 93:725-730. 2586. Schwartz PE (2000). Surgery of germcell tumours of the ovary. Forum (Genova)10: 355-365. 2587. Schwartz PE, Chambers SK,Chambers JT, Kohorn E, McIntosh S (1992).Ovarian germ cell malignancies: the YaleUniversity experience. Gynecol Oncol 45:26-31. 2588. Schwartz PE, Smith JP (1976).Treatment of ovarian stromal tumors. Am JObstet Gynecol 125: 402-411.
2589. Schweizer P, Moisio AL, KuismanenSA, Truninger K, Vierumaki R, Salovaara R,Arola J, Butzow R, Jiricny J, Peltomaki P,Nystrom-Lahti M (2001). Lack of MSH2 andMSH6 characterizes endometrial but notcolon carcinomas in hereditary nonpolypo-sis colorectal cancer. Cancer Res 61: 2813-2815. 2590. Scopsi L, Andreola S, Pilotti S,Bufalino R, Baldini MT, Testori A, Rilke F(1994). Mucinous carcinoma of the breast.A clinicopathologic, histochemical, andimmunocytochemical study with specialreference to neuroendocrine differentia-tion. Am J Surg Pathol 18: 702-711. 2591. Scopsi L, Andreola S, Saccozzi R,Pilotti S, Boracchi P, Rosa P, Conti AR,Manzari A, Huttner WB, Rilke F (1991).Argyrophilic carcinoma of the male breast.A neuroendocrine tumor containing pre-dominantly chromogranin B (secre-togranin I). Am J Surg Pathol 15: 1063-1071. 2592. Scott SP, Bendix R, Chen P, Clark R,Dork T, Lavin MF (2002). Missense muta-tions but not allelic variants alter the func -tion of ATM by dominant interference inpatients with breast cancer. Proc NatlAcad Sci USA 99: 925-930. 2593. Scully R, Anderson SF, Chao DM, WeiW, Ye L, Young RA, Livingston DM, ParvinJD (1997). BRCA1 is a component of theRNA polymerase II holoenzyme. Proc NatlAcad Sci USA 94: 5605-5610. 2594. Scully R, Chen J, Ochs RL, Keegan K,Hoekstra M, Feunteun J, Livingston DM(1997). Dynamic changes of BRCA1 subnu -clear location and phosphorylation stateare initiated by DNA damage. Cell 90: 425-435. 2595. Scully R, Chen J, Plug A, Xiao Y,Weaver D, Feunteun J, Ashley T,Livingston DM (1997). Association ofBRCA1 with Rad51 in mitotic and meioticcells. Cell 88: 265-275. 2596. Scully R, Ganesan S, Brown M, DeCaprio JA, Cannistra SA, Feunteun J,Schnitt S, Livingston DM (1996). Location ofBRCA1 in human breast and ovarian can-cer cells. Science 272: 123-126. 2597. Scully R, Ganesan S, Vlasakova K,Chen J, Socolovsky M, Livingston DM(1999). Genetic analysis of BRCA1 functionin a defined tumor cell line. Mol Cell 4:1093-1099. 2598. Scully RE (1970). Gonadoblastoma. Areview of 74 cases. Cancer 25: 1340-1356. 2599. Scully RE (1970). Sex cord tumor withannular tubules a distinctive ovarian tumorof the Peutz-Jeghers syndrome. Cancer 25:1107-1121. 2600. Scully RE, Bell DA, Abu-Jawdeh GM(1995). Update on early ovarian cancer andcancer developing in benign ovariantumors. In: Ovarian Cancer 3, P Mason, FSharp, T Blackett, J Berek (eds.),Chapman and Hall: London, pp. 139-144.2601. Scully RE, Bonfiglio TA, Kurman RJ,Silverberg SG, Wilkinson EJ (1994). WorldHealth Organization: Histological Typing ofFemale Tract Tumours. 2nd ed. Springer-Verlag: Berlin.2602. Scully RE, Bonfiglio TA, Kurman RJ,Silverberg SG, Wilkinson EJ (1994). Uterinecorpus. In: World Health Organization:Histological Typing of Female GenitalTract Tumors, Springer-Verlag: New York ,pp. 13-31.2603. Scully RE, Galdabini JJ, McNeely BU(1976). Case records of the MassachusettsGeneral Hospital. Weekly clinicopathologi-cal exercises. Case 14-1976. N Engl J Med294: 772-777.
2604. Scully RE, Sobin LH (1999). WorldHealth Organization: Histological Typing ofOvarian Tumours. 2nd ed. Spinger-Verlag:Berlin.2605. Scully RE, Young RH, Clement PB(1998). Atlas of Tumor Pathology Tumorsof the Ovary, Maldeveloped Gonads,Fallopian Tube, and Broad Ligament. 3rded. AFIP: Washington,D.C.2606. Scurry J, Beshay V, Cohen C, Allen D(1998). Ki67 expression in lichen sclerosusof vulva in patients with and without asso-ciated squamous cell carcinoma.Histopathology 32: 399-404. 2607. Scurry J, Brand A, Planner R,Dowling J, Rode J (1996). Vulvar Merkelcell tumor with glandular and squamousdifferentiation. Gynecol Oncol 62: 292-297. 2608. Scurry J, Craighead P, Duggan M(2000). Histologic study of patterns of cer-vical involvement in FIGO stage II endome-trial carcinoma. Int J Gynecol Cancer 10:497-502. 2609. Scurry J, Planner R, Grant P (1991).Unusual variants of vaginal adenosis: achallenge for diagnosis and treatment.Gynecol Oncol 41: 172-177. 2610. Scurry JP, Brown RW, Jobling T(1996). Combined ovarian serous papillaryand hepatoid carcinoma. Gynecol Oncol63: 138-142. 2611. Sebek BA (1984). Cavernous heman-gioma of the female breast. Cleve Clin Q 51:471-474. 2612. Seckl MJ, Mulholland PJ, Bishop AE,Teale JD, Hales CN, Glaser M, Watkins S,Seckl JR (1999). Hypoglycemia due to aninsulin-secreting small-cell carcinoma ofthe cervix. N Engl J Med 341: 733-736. 2613. Secreto G, Zumoff B (1994). Abnormalproduction of androgens in women withbreast cancer. Anticancer Res 14: 2113-2117. 2614. Sedlis A (1961). Primary carcinoma ofthe Fallopian tube. Obstet Gynecol Surv 16:209-226. 2615. Segal GH, Hart WR (1992). Ovarianserous tumors of low malignant potential(serous borderline tumors). The relation-ship of exophytic surface tumor to peri-toneal "implants". Am J Surg Pathol 16: 577-583. 2616. Segawa T, Sasagawa T, Yamazaki H,Sakaike J, Ishikawa H, Inoue M (1999).Fragile histidine triad transcription abnor-malities and human papillomavirus E6-E7mRNA expression in the development ofcervical carcinoma. Cancer 85: 2001-2010. 2617. Seidman JD (1994). Mucinous lesionsof the fallopian tube. A report of sevencases. Am J Surg Pathol 18: 1205-1212. 2618. Seidman JD (1996). Prognosticimportance of hyperplasia and atypia inendometriosis. Int J Gynecol Pathol 15: 1-9. 2619. Seidman JD (1996). Unclassifiedovarian gonadal stromal tumors. A clinico-pathologic study of 32 cases. Am J SurgPathol 20: 699-706. 2620. Seidman JD, Abbondanzo SL,Bratthauer GL (1995). Lipid cell (steroidcell) tumor of the ovary: immunophenotypewith analysis of potential pitfall due toendogenous biotin-like activity. Int JGynecol Pathol 14: 331-338. 2621. Seidman JD, Ashton M, Lefkowitz M(1996). Atypical apocrine adenosis of thebreast: a clinicopathologic study of 37patients with 8.7-year follow-up. Cancer77: 2529-2537.

414 References
2622. Seidman JD, Borkowski A, Aisner SC,Sun CC (1993). Rapid growth of pseudoan-giomatous hyperplasia of mammary stro-ma in axillary gynecomastia in an immuno-suppressed patient. Arch Pathol Lab Med117: 736-738. 2623. Seidman JD, Elsayed AM, Sobin LH,Tavassoli FA (1993). Association of muci-nous tumors of the ovary and appendix. Aclinicopathologic study of 25 cases. Am JSurg Pathol 17: 22-34. 2624. Selim AG, Wells CA (1999).Immunohistochemical localisation ofandrogen receptor in apocrine metaplasiaand apocrine adenosis of the breast: rela-tion to oestrogen and progesterone recep-tors. J Clin Pathol 52: 838-841. 2625. Seltzer VL, Levine A, Spiegel G,Rosenfeld D, Coffey EL (1990).Adenofibroma of the uterus: multiplerecurrences following wide local excision.Gynecol Oncol 37: 427-431. 2626. Seltzer VL, Molho L, Fougner A, HongP, Kereszti B, Gero M, Spitzer M (1988).Parovarian cystadenocarcinoma of low-malignant potential. Gynecol Oncol 30: 216-221. 2627. Semczuk A, Baranowski W, BerbecH, Marzec B, Skomra D, Miturski R (1999).Analysis of p53 and K-ras genes and theirproteins in a sarcoma botryoides of theuterine cervix. Eur J Gynaecol Oncol 20:311-314. 2628. Sengupta BS (1981). Vulval cancerfollowing or co-existing with chronic gran-ulomatous diseases of vulva. An analysisof its natural history, clinical manifestationand treatment. Trop Doct 11: 110-114. 2629. Senzaki H, Kiyozuka Y, Mizuoka H,Yamamoto D, Ueda S, Izumi H, Tsubura A(1999). An autopsy case of hepatoid carci-noma of the ovary with PIVKA-II produc-tion: immunohistochemical study and liter -ature review. Pathol Int 49: 164-169. 2630. Seong C, Kirby RW (1987). Leydig-celltumour of the ovary en a multipleendocrine neoplasia syndrome. J ObstetGynaecol 7: 295-296. 2631. Serova OM, Mazoyer S, Puget N,Dubois V, Tonin P, Shugart YY, Goldgar D,Narod SA, Lynch HT, Lenoir GM (1997).Mutations in BRCA1 and BRCA2 in breastcancer families: are there more breastcancer-susceptibility genes? Am J HumGenet 60: 486-495. 2632. Shabb NS, Tawil A, Mufarrij A, ObeidS, Halabi J (1997). Mammary carcinomawith osteoclastlike giant cells cytologicallymimicking benign breast disease. A casereport. Acta Cytol 41: 1284-1288. 2633. Shanks JH, Harris M, Banerjee SS,Eyden BP, Joglekar VM, Nicol A, HasletonPS, Nicholson AG (2000). Mesotheliomaswith deciduoid morphology: a morphologicspectrum and a variant not confined toyoung females. Am J Surg Pathol 24: 285-294. 2634. Sharma A, Pratap M, Sawhney VM,Khan IU, Bhambhani S, Mitra AB (1999).Frequent amplification of C-erbB2 (HER-2/Neu) oncogene in cervical carcinoma asdetected by non-fluorescence in situhybridization technique on paraffin sec-tions. Oncology 56: 83-87. 2635. Shashi V, Golden WL, Kap-Herr C,Andersen WA, Gaffey MJ (1994).Interphase fluorescence in situ hybridiza-tion for trisomy 12 on archival ovarian sexcord-stromal tumors. Gynecol Oncol 55:349-354.
2636. Shatz P, Bergeron C, Wilkinson EJ,Arseneau J, Ferenczy A (1989). Vulvarintraepithelial neoplasia and skinappendage involvement. Obstet Gynecol74: 769-774. 2637. Shaw JA, Dabbs DJ, Geisinger KR(1992). Sclerosing stromal tumor of theovary: an ultrastructural and immunohisto-chemical analysis with histogenetic con-siderations. Ultrastruct Pathol 16: 363-377. 2638. Sheikh MS, Rochefort H, Garcia M(1995). Overexpression of p21WAF1/CIP1induces growth arrest, giant cell formationand apoptosis in human breast carcinomacell lines. Oncogene 11: 1899-1905. 2639. Shen JT, d'Ablaing G, Morrow CP(1982). Alveolar soft part sarcoma of thevulva: report of first case and review of lit -erature. Gynecol Oncol 13: 120-128. 2640. Shen T, Zhuang Z, Gersell DJ,Tavassoli FA (2000). Allelic Deletion of VHLGene Detected in Papillary Tumors of theBroad Ligament, Epididymis, andRetroperitoneum in von Hippel-LindauDisease Patients. Int J Surg Pathol 8: 207-212. 2641. Shenson DL, Gallion HH, Powell DE,Pieretti M (1995). Loss of heterozygosityand genomic instability in synchronousendometrioid tumors of the ovary andendometrium. Cancer 76: 650-657. 2642. Shepherd JH (1989). Revised FIGOstaging for gynaecological cancer. Br JObstet Gynaecol 96: 889-892. 2643. Shepherd JJ, Wright DH (1967).Burkitt's tumour presenting as bilateralswelling of the breast in women of child-bearing age. Br J Surg 54: 776-780. 2644. Sheppard DG, Libshitz HI (2001). Post-radiation sarcomas: a review of the clinicaland imaging features in 63 cases. ClinRadiol 56: 22-29. 2645. Sherman JE, Smith JW (1981).Neurofibromas of the breast and nipple-areolar area. Ann Plast Surg 7: 302-307. 2646. Sherman ME, Bitterman P,Rosenshein NB, Delgado G, Kurman RJ(1992). Uterine serous carcinoma. A mor-phologically diverse neoplasm with unify-ing clinicopathologic features. Am J SurgPathol 16: 600-610. 2647. Sherman ME, Bur ME, Kurman RJ(1995). p53 in endometrial cancer and itsputative precursors: evidence for diversepathways of tumorigenesis. Hum Pathol 26:1268-1274. 2648. Sherman ME, Sturgeon S, Brinton LA,Potischman N, Kurman RJ, Berman ML,Mortel R, Twiggs LB, Barrett RJ, WilbanksGD (1997). Risk factors and hormone levelsin patients with serous and endometrioiduterine carcinomas. Mod Pathol 10: 963-968. 2649. Sheth NA, Saruiya JN, Ranadive KJ,Sheth AR (1974). Ectopic production ofhuman chorionic gonadotrophin by humanbreast tumours. Br J Cancer 30: 566-570. 2650. Sheth S, Hamper UM, Kurman RJ(1993). Thickened endometrium in the post-menopausal woman: sonographic-patho-logic correlation. Radiology 187: 135-139. 2651. Sheu BC, Lin HH, Chen CK, Chao KH,Shun CT, Huang SC (1995). Synchronousprimary carcinomas of the endometriumand ovary. Int J Gynaecol Obstet 51: 141-146. 2652. Shevchuk MM, Fenoglio CM, LattesR, Frick HC, Richart RM (1978). Malignantmixed tumor of the vagina probably arisingin mesonephric rests. Cancer 42: 214-223.
2653. Sheyn I, Mira JL, Bejarano PA,Husseinzadeh N (2000). Metastatic femaleadnexal tumor of probable Wolffian origin:a case report and review of the literature.Arch Pathol Lab Med 124: 431-434. 2654. Shidara Y, Karube A, Watanabe M,Satou E, Uesaka Y, Matsuura T, Tanaka T(2000). A case report: verrucous carcino-ma of the endometrium--the difficulty ofdiagnosis, and a review of the literature. JObstet Gynaecol Res 26: 189-192. 2655. Shigematsu T, Kamura T, Arima T,Wake N, Nakano H (2000). DNA polymor-phism analysis of a pure non-gestationalchoriocarcinoma of the ovary: case report.Eur J Gynaecol Oncol 21: 153-154. 2656. Shigeta H, Taga M, Kurogi K,Kitamura H, Motoyama T, Gorai I (1999).Ovarian strumal carcinoid with severeconstipation: immunohistochemical andmRNA analyses of peptide YY. Hum Pathol30: 242-246. 2657. Shih HA, Couch FJ, Nathanson KL,Blackwood MA, Rebbeck TR, ArmstrongKA, Calzone K, Stopfer J, Seal S, StrattonMR, Weber BL (2002). BRCA1 and BRCA2mutation frequency in women evaluated ina breast cancer risk evaluation clinic. JClin Oncol 20: 994-999. 2 6 5 8 . Shih IM, Kurman RJ (1998).Epithelioid trophoblastic tumor: a neo-plasm distinct from choriocarcinoma andplacental site trophoblastic tumor simulat -ing carcinoma. Am J Surg Pathol 22: 1393-1403. 2659. Shih IM, Kurman RJ (2001). Thepathology of intermediate trophoblastictumors and tumor-like lesions. Int JGynecol Pathol 20: 31-47. 2660. Shiloh Y, Kastan MB (2001). ATM:genome stability, neuronal development,and cancer cross paths. Adv Cancer Res83: 209-254. 2 6 6 1 . Shin SJ, DeLellis RA, Rosen PP(2001). Small cell carcinoma of the breast--additional immunohistochemical studies.Am J Surg Pathol 25: 831-832. 2662. Shin SJ, DeLellis RA, Ying L, RosenPP (2000). Small cell carcinoma of thebreast: a clinicopathologic and immuno-histochemical study of nine patients. Am JSurg Pathol 24: 1231-1238. 2663. Shin SJ, Kanomata N, Rosen PP(2000). Mammary carcinoma with promi-nent cytoplasmic lipofuscin granules mim -icking melanocytic differentiation.Histopathology 37: 456-459. 2664. Shivas AA, Douglas JG (1972). Theprognostic significance of elastosis inbreast carcinoma. J R Coll Surg Edinb 17:315-320. 2665. Shokeir MO, Noel SM, Clement PB(1996). Malignant mullerian mixed tumor ofthe uterus with a prominent alpha-fetopro-tein-producing component of yolk sactumor. Mod Pathol 9: 647-651. 2666. Shoker BS, Jarvis C, Clarke RB,Anderson E, Munro C, Davies MP, SibsonDR, Sloane JP (2000). Abnormal regulationof the oestrogen receptor in benign breastlesions. J Clin Pathol 53: 778-783. 2667. Shoker BS, Jarvis C, Sibson DR,Walker C, Sloane JP (1999). Oestrogenreceptor expression in the normal and pre-cancerous breast. J Pathol 188: 237-244. 2668. Shousha S, Backhous CM,Alaghband-Zadeh J, Burn I (1986). Alveolarvariant of invasive lobular carcinoma ofthe breast. A tumor rich in estrogen recep-tors. Am J Clin Pathol 85: 1-5.
2669. Shousha S, Coady AT, Stamp T,James KR, Alaghband-Zadeh J (1989).Oestrogen receptors in mucinous carcino-ma of the breast: an immunohistologicalstudy using paraffin wax sections. J ClinPathol 42: 902-905. 2670. Shousha S, Schoenfeld A, Moss J,Shore I, Sinnett HD (1994). Light and elec-tron microscopic study of an invasive crib-riform carcinoma with extensive microcal-cification developing in a breast withsilicone augmentation. Ultrastruct Pathol18: 519-523. 2671. Sieinski W (1989). Lipomatousneometaplasia of the uterus. Report of 11cases with discussion of histogenesis andpathogenesis. Int J Gynecol Pathol 8: 357-363. 2 6 7 2 . Sigurdsson K, Hrafnkelsson J,Geirsson G, Gudmundsson J, SalvarsdottirA (1991). Screening as a prognostic factorin cervical cancer: analysis of survival andprognostic factors based on Icelandicpopulation data, 1964-1988. Gynecol Oncol43: 64-70. 2673. Sijmons RH, Kiemeney LA, Witjes JA,Vasen HF (1998). Urinary tract cancer andhereditary nonpolyposis colorectal can-cer: risks and screening options. J Urol160: 466-470. 2674. Sillman FH, Fruchter RG, Chen YS,Camilien L, Sedlis A, McTigue E (1997).Vaginal intraepithelial neoplasia: risk fac-tors for persistence, recurrence, and inva-sion and its management. Am J ObstetGynecol 176: 93-99. 2675. Silva EG, Jenkins R (1990). Serouscarcinoma in endometrial polyps. M o dPathol 3: 120-128. 2676. Silva EG, Robey-Cafferty SS, SmithTL, Gershenson DM (1990). Ovarian carci-nomas with transitional cell carcinomapattern. Am J Clin Pathol 93: 457-465. 2677. Silva EG, Tornos C, Bailey MA, MorrisM (1991). Undifferentiated carcinoma ofthe ovary. Arch Pathol Lab Med 115: 377-381. 2678. Silver SA, Cheung AN, Tavassoli FA(1999). Oncocytic metaplasia and carcino-ma of the endometrium: an immunohisto-chemical and ultrastructural study. Int JGynecol Pathol 18: 12-19. 2679. Silver SA, Devouassoux-ShisheboranM, Mezzetti TP, Tavassoli FA (2001).Mesonephric adenocarcinomas of theuterine cervix: a study of 11 cases withimmunohistochemical findings. Am J SurgPathol 25: 379-387. 2680. Silver SA, Tavassoli FA (1998).Mammary ductal carcinoma in situ withmicroinvasion. Cancer 82: 2382-2390. 2 6 8 1 . Silver SA, Tavassoli FA (1998).Primary osteogenic sarcoma of the breast:a clinicopathologic analysis of 50 cases.Am J Surg Pathol 22: 925-933. 2 6 8 2 . Silver SA, Tavassoli FA (2000).Glomus tumor arising in a mature teratomaof the ovary: report of a case simulating ametastasis from cervical squamous carci-noma. Arch Pathol Lab Med 124: 1373-1375. 2683. Silver SA, Tavassoli FA (2000).Pleomorphic carcinoma of the breast: clin-icopathological analysis of 26 cases of anunusual high-grade phenotype of ductalcarcinoma. Histopathology 36: 505-514. 2684. Silver SA, Wiley JM, Perlman EJ(1994). DNA ploidy analysis of pediatricgerm cell tumors. Mod Pathol 7: 951-956. 2685. Silverberg SG (1971). Brenner tumorof the ovary. A clinicopathologic study of60 tumors in 54 women. Cancer 28: 588-596.

415References
2686. Silverberg SG (1999). Protocol for theexamination of specimens from patientswith carcinomas of the endometrium: abasis for checklists. Cancer Committee,College of American Pathologists. ArchPathol Lab Med 123: 28-32. 2687. Silverberg SG (2000). Histopathologicgrading of ovarian carcinoma: a reviewand proposal. Int J Gynecol Pathol 19: 7-15. 2688. Silverberg SG (2000). Problems in thedifferential diagnosis of endometrialhyperplasia and carcinoma. Mod Pathol13: 309-327. 2689. Silverberg SG, Chitale AR (1973).Assessment of significance of proportionsof intraductal and infiltrating tumor growthin ductal carcinoma of the breast. Cancer32: 830-837. 2690. Silverberg SG, Kay S, Koss LG (1971).Postmastectomy lymphangiosarcoma:ultrastructural observations. Cancer 27:100-108. 2691. Silverberg SG, Kurman RJ (1992).Atlas of Tumour Pathology. Tumours of theuterine corpus and gestational trophoblas-tic disease, AFIP: Washington DC.2692. Silverberg SG, Major FJ, Blessing JA,Fetter B, Askin FB, Liao SY, Miller A (1990).Carcinosarcoma (malignant mixed meso-dermal tumor) of the uterus. A GynecologicOncology Group pathologic study of 203cases. Int J Gynecol Pathol 9: 1-19. 2693. Silverberg SG, Willson MA, Board JA(1971). Hemangiopericytoma of the uterus:an ultrastructural study. Am J ObstetGynecol 110: 397-404. 2694. Silverman EM, Oberman HA (1974).Metastatic neoplasms in the breast. SurgGynecol Obstet 138: 26-28. 2695. Silverstein MJ, Gierson ED, ColburnWJ, Rosser RJ, Waisman JR, Gamagami P(1991). Axillary lymphadenectomy for intra-ductal carcinoma of the breast. S u r gGynecol Obstet 172: 211-214. 2696. Silverstein MJ, Lewinsky BS,Waisman JR, Gierson ED, Colburn WJ,Senofsky GM, Gamagami P (1994).Infiltrating lobular carcinoma. Is it differentfrom infiltrating duct carcinoma? Cancer73: 1673-1677. 2697. Simkin PH, Ramirez LA, Zweizig SL,Afonso SA, Fraire AE, Khan A, Dunn AD,Dunn JT, Braverman LE (1999).Monomorphic teratoma of the ovary: a rarecause of triiodothyronine toxicosis.Thyroid 9: 949-954. 2698. Simpson JF, Page DL, Dupont WD(1990). Apocrine adenosis - a mimmic ofmammary carcinoma. Surgical Pathology3: 289-299. 2699. Simpson JF, Page DL, Dupont WD(1990). Apocrine adenosis - an occasionalmimicker of breast carcinoma. Mod Pathol3. 2700. Simpson JF, Quan DE, O'Malley F,Odom-Maryon T, Clarke PE (1997).Amplification of CCND1 and expression ofits protein product, cyclin D1, in ductal car-cinoma in situ of the breast. Am J Pathol151: 161-168. 2701. Simpson JL, Michael H, Roth LM(1998). Unclassified sex cord-stromaltumors of the ovary: a report of eightcases. Arch Pathol Lab Med 122: 52-55. 2702. Simpson RH, Cope N, Skalova A,Michal M (1998). Malignant adenomyoep-ithelioma of the breast with mixedosteogenic, spindle cell, and carcinoma-tous differentiation. Am J Surg Pathol 22:631-636.
2703. Simpson T, Thirlby RC, Dail DH (1992).Surgical treatment of ductal carcinoma insitu of the breast. 10- to 20-year follow-up.Arch Surg 127: 468-472. 2704. Simsek T, Trak B, Tunc M, Karaveli S,Uner M, Sonmez C (1998). Primary purechoriocarcinoma of the ovary in reproduc -tive ages: a case report. Eur J GynaecolOncol 19: 284-286. 2705. Singer A, Monaghan J (2000). LowerGenital Tract Precancer. Colposcopy,Pathology and Treatment. 2nd ed.Blackwell Science Ltd: Oxford.2706. Singer G, Kurman RJ, Chang HW, ChoSK, Shih I (2002). Diverse tumorigenic path-ways in ovarian serous carcinoma. Am JPathol 160: 1223-1228. 2707. Singer G, Oldt R, III, Cohen Y, WangBG, Sidransky D, Kurman RJ, Shih I (2003).Mutations in BRAF and KRAS characterizethe development of low-grade ovarianserous carcinoma. J Natl Cancer Inst 95:484-486. 2708. Singh TT, Hopkins MP, Price J,Schuen R (1992). Myxoid liposarcoma ofthe broad ligament. Int J Gynecol Cancer 2:220-223. 2709. Singhal S, Sharma S, De S, Kumar L,Chander S, Rath GK, Gupta SD (1990). Adultembryonal rhabdomyosarcoma of the vagi-na complicating pregnancy: a case reportand review of the literature. Asia OceaniaJ Obstet Gynaecol 16: 301-306. 2710. Sinkre P, Albores-Saavedra J, MillerDS, Copeland LJ, Hameed A (2000).Endometrial endometrioid carcinomasassociated with Ewing sarcoma/peripheralprimitive neuroectodermal tumor. Int JGynecol Pathol 19: 127-132. 2711. Sinkre P, Miller DS, Milchgrub S,Hameed A (2000). Adenomyofibroma of theendometrium with skeletal muscle differ-entiation. Int J Gynecol Pathol 19: 280-283. 2712. Sinniah R, O'Brien FV (1973).Pigmented progonoma in a dermoid cyst ofthe ovary. J Pathol 109: 357-359. 2713. Siriaunkgul S, Robbins KM,McGowan L, Silverberg SG (1995). Ovarianmucinous tumors of low malignant poten-tial: a clinicopathologic study of 54 tumorsof intestinal and mullerian type. Int JGynecol Pathol 14: 198-208. 2714. Sirota RL, Dickersin GR, Scully RE(1981). Mixed tumors of the vagina. A clini -copathological analysis of eight cases.AmJ Surg Pathol 5: 413-422. 2715. Sit AS, Price FV, Kelley JL, ComerciJT, Kunschner AJ, Kanbour-Shakir A,Edwards RP (2000). Chemotherapy formalignant mixed Mullerian tumors of theovary. Gynecol Oncol 79: 196-200. 2 7 1 6 . Sjostedt S, Whalen T (1961).Prognosis of granulosa cell tumours. ActaObstet Gynecol Scand 40(suppl 6): 3-26. 2717. Skelton H, Smith KJ (2001). Spindlecell epithelioma of the vagina showsimmunohistochemical staining supportingits origin from a primitive/progenitor cellpopulation. Arch Pathol Lab Med 125: 547-550. 2718. Skinnider BF, Clement PB,MacPherson N, Gascoyne RD, ViswanathaDS (1999). Primary non-Hodgkin's lym-phoma and malakoplakia of the vagina: acase report. Hum Pathol 30: 871-874. 2719. Slamon DJ, Clark GM, Wong SG,Levin WJ, Ullrich A, McGuire WL (1987).Human breast cancer: correlation ofrelapse and survival with amplification ofthe HER-2/neu oncogene. Science 2 3 5 :177-182.
2720. Slanetz PJ, Whitman GJ, Halpern EF,Hall DA, McCarthy KA, Simeone JF (1997).Imaging of fallopian tube tumors. AJR AmJ Roentgenol 169: 1321-1324. 2720a. Slattery ML, Kerber RA (1993). Acomprehensive evaluation of family historyand breast cancer risk. The UtahPopulation Database. JAMA 270: 1563-1568. 2721. Sloan D (1988). Diagnosis of a tumorwith an unusual presentation in the pelvis.Am J Obstet Gynecol 159: 826-827. 2722. Sloane JP (2001). Biopsy Pathologyof the Breast. 2nd ed. Arnold: London.2723. Sloane JP, Amendoeira I,Apostolikas N, Bellocq JP, Bianchi S,Boecker W, Bussolati G, Coleman D,Connolly CE, Dervan P, Eusebi V, DeMiguel C, Drijkoningen M, Elston CW,Faverley D, Gad A, Jacquemier J, LacerdaM, Martinez-Penuela J, Munt C, PeterseJL, Rank F, Sylvan M, Tsakraklides V,Zafrani B (1998). Consistency achieved by23 European pathologists in categorizingductal carcinoma in situ of the breastusing five classifications. EuropeanCommission Working Group on BreastScreening Pathology. Hum Pathol 29: 1056-1062. 2724. Sloane JP, Amendoeira I,Apostolikas N, Bellocq JP, Bianchi S,Boecker W, Bussolati G, Coleman D,Connolly CE, Eusebi V, De Miguel C,Dervan P, Drijkoningen R, Elston CW,Faverly D, Gad A, Jacquemier J, LacerdaM, Martinez-Penuela J, Munt C, PeterseJL, Rank F, Sylvan M, Tsakraklides V,Zafrani B (1999). Consistency achieved by23 European pathologists from 12 coun-tries in diagnosing breast disease andreporting prognostic features of carcino-mas. European Commission WorkingGroup on Breast Screening Pathology.Virchows Arch 434: 3-10. 2725. Sloane JP, Mayers MM (1993).Carcinoma and atypical hyperplasia inradial scars and complex sclerosinglesions: importance of lesion size andpatient age. Histopathology 23: 225-231. 2726. Sloboda J, Zaviacic M, Jakubovsky J,Hammar E, Johnsen J (1998).Metastasizing adenocarcinoma of thefemale prostate (Skene's paraurethralglands). Histological and immunohisto-chemical prostate markers studies andfirst ultrastructural observation. P a t h o lRes Pract 194: 129-136. 2727. Slomovitz BM, Caputo TA, Gretz HF,III, Economos K, Tortoriello DV,Schlosshauer PW, Baergen RN, Isacson C,Soslow RA (2002). A comparative analysisof 57 serous borderline tumors with andwithout a noninvasive micropapillary com -ponent. Am J Surg Pathol 26: 592-600. 2728. Smit VT, Cornelisse CJ, De Jong D,Dijkshoorn NJ, Peters AA, Fleuren GJ(1988). Analysis of tumor heterogeneity in apatient with synchronously occurringfemale genital tract malignancies by DNAflow cytometry, DNA fingerprinting, andimmunohistochemistry. Cancer 62: 1146-1152. 2 7 2 9 . Smith-Warner SA, Spiegelman D,Yaun SS, van den Brandt PA, Folsom AR,Goldbohm RA, Graham S, Holmberg L,Howe GR, Marshall JR, Miller AB, PotterJD, Speizer FE, Willett WC, Wolk A, HunterDJ (1998). Alcohol and breast cancer inwomen: a pooled analysis of cohort stud-ies. JAMA 279: 535-540.
2 7 3 0 . Smith BH, Taylor HB (1969). Theoccurrence of bone and cartilage in mam-mary tumors. Am J Clin Pathol 51: 610-618. 2 7 3 1 . Smith DR, Ji CY, Goh HS (1996).Prognostic significance of p53 overexpres-sion and mutation in colorectal adenocar-cinomas. Br J Cancer 74: 216-223. 2732. Smith HO, Qualls CR, Romero AR,Webb JC, Dorin MH, Padilla LA, Key CR(2002). Is there a difference in survival forIA1 and IA2 adenocarcinoma of the uterinecervix? Gynec Oncol 85: 229-241. 2733. Smith J, Munoz N, Herrero R, Eluf-Neto J, Ngelangel C, Franceschi S, BoschFX, Walboomers JM, Peeling RW (2002).Evidence for Chlamydia trachomatis as ahuman papillomavirus cofactor in the etiol-ogy of invasive cervical cancer in Braziland the Philippines. J Infect Dis 185: 324-331. 2734. Smith JS, Herrero R, Bosetti C,Munoz N, Bosch FX, Eluf-Neto J,Castellsague X, Meijer CJ, van den BruleAJ, Franceschi S, Ashley R (2002). Herpessimplex virus-2 as a human papillomaviruscofactor in the etiology of invasive cervicalcancer. J Natl Cancer Inst 94: 1604-1613. 2735. Smith TM, Lee MK, Szabo CI, JeromeN, McEuen M, Taylor M, Hood L, King MC(1996). Complete genomic sequence andanalysis of 117 kb of human DNA contain-ing the gene BRCA1. Genome Res 6: 1029-1049. 2736. Smith YR, Quint EH, Hinton EL (1998).Recurrent benign mullerian papilloma ofthe cervix. J Pediatr Adolesc Gynecol 11:29-31. 2737. Snyder RR, Norris HJ, Tavassoli F(1988). Endometrioid proliferative and lowmalignant potential tumors of the ovary. Aclinicopathologic study of 46 cases. Am JSurg Pathol 12: 661-671. 2738. Soares J, Tomasic G, Bucciarelli E,Eusebi V (1994). Intralobular growth ofmyoepithelial cell carcinoma of the breast.Virchows Arch 425: 205-210. 2739. Sobin LH, Wittekind CH (1997). BreastTumours in TNM. 5th ed. Wiley-Liss: NewYork.2740. Sodha N, Houlston RS, Bullock SL,Yuille MA, Chu C, Turner G, Eeles RA(2002). Increasing evidence that germlinemutations in CHEK2 do not cause Li-Fraumeni syndrome. Hum Mutat 20: 460-462. 2741. Sodha N, Houlston RS, Williams R,Yuille MA, Mangion J, Eeles RA (2002). Arobust method for detecting CHK2/RAD53mutations in genomic DNA. Hum Mutat 19:173-177. 2742. Sodha N, Williams R, Mangion J,Bullock SL, Yuille MR, Eeles RA (2000).Screening hCHK2 for mutations. Science289: 359. 2743. Soga J, Osaka M, Yakuwa Y (2000).Carcinoids of the ovary: an analysis of 329reported cases. J Exp Clin Cancer Res 19:271-280. 2 7 4 4 . Solin LJ, Fowble BL, Yeh IT,Kowalyshyn MJ, Schultz DJ, Weiss MC,Goodman RL (1992). Microinvasive ductalcarcinoma of the breast treated withbreast-conserving surgery and definitiveirradiation. Int J Radiat Oncol Biol Phys 23:961-968. 2745. Somasundaram K, Zhang H, Zeng YX,Houvras Y, Peng Y, Zhang H, Wu GS, LichtJD, Weber BL, El Deiry WS (1997). Arrest ofthe cell cycle by the tumour-suppressorBRCA1 requires the CDK-inhibitorp21WAF1/CiP1. Nature 389: 187-190.

416 References
2746. Somerville JE, Clarke LA, Biggart JD(1992). c-erbB-2 overexpression and histo-logical type of in situ and invasive breastcarcinoma. J Clin Pathol 45: 16-20. 2747. Sonnendecker HE, Cooper K, KalianKN (1994). Primary fallopian tube adeno-carcinoma in situ associated with adjuvanttamoxifen therapy for breast carcinoma.Gynecol Oncol 52: 402-407. 2748. Sonoda Y, Saigo PE, Federici MG,Boyd J (2000). Carcinosarcoma of theovary in a patient with a germline BRCA2mutation: evidence for monoclonal origin.Gynecol Oncol 76: 226-229. 2749. Sood AK, Sorosky JI, Gelder MS,Buller RE, Anderson B, Wilkinson EJ,Benda JA, Morgan LS (1998). Primary ovar-ian sarcoma: analysis of prognostic vari-ables and the role of surgical cytoreduc-tion. Cancer 82: 1731-1737. 2 7 5 0 . Soomro S, Shousha S, Taylor P,Shepard HM, Feldmann M (1991). c-erbB-2expression in different histological types ofinvasive breast carcinoma. J Clin Pathol44: 211-214. 2751. Sorbe B, Risberg B, Thornthwaite J(1994). Nuclear morphometry and DNAflow cytometry as prognostic methods forendometrial carcinoma. Int J GynecolCancer 4: 94-100. 2752. Sordillo PP, Chapman R, Hajdu SI,Magill GB, Golbey RB (1981). Lymph-angiosarcoma. Cancer 48: 1674-1679. 2753. Soreide JA, Anda O, Eriksen L, HolterJ, Kjellevold KH (1988). Pleomorphic ade-noma of the human breast with localrecurrence. Cancer 61: 997-1001. 2754. Sorensen FB, Paulsen SM (1987).Glycogen-rich clear cell carcinoma of thebreast: a solid variant with mucus. A lightmicroscopic, immunohistochemical andultrastructural study of a case.Histopathology 11: 857-869. 2755. Sorensen HT, Friis S, Olsen JH,Thulstrup AM, Mellemkjaer L, Linet M,Trichopoulos D, Vilstrup H, Olsen J (1998).Risk of breast cancer in men with liver cir -rhosis. Am J Gastroenterol 93: 231-233. 2756. Sorlie T, Perou CM, Tibshirani R, AasT, Geisler S, Johnsen H, Hastie T, EisenMB, van de Rijn M, Jeffrey SS, Thorsen T,Quist H, Matese JC, Brown PO, Botstein D,Eystein LP, Borresen-Dale AL (2001). Geneexpression patterns of breast carcinomasdistinguish tumor subclasses with clinicalimplications. Proc Natl Acad Sci USA 98:10869-10874. 2757. Sorlie T, Tibshirani R, Parker J, HastieT, Marron JS, Nobel A, Deng S, Johnsen H,Pesich R, Geisler S, Demeter J, Perou CM,Lonning PE, Brown PO, Borresen-Dale AL,Botstein D (2003). Repeated observation ofbreast tumor subtypes in independentgene expression data sets. Proc Natl AcadSci USA 100: 8418-8423. 2758. Soslow RA, Rouse RV, HendricksonMR, Silva EG, Longacre TA (1996).Transitional cell neoplasms of the ovaryand urinary bladder: a comparativeimmunohistochemical analysis. Int JGynecol Pathol 15: 257-265. 2759. Soussi T (1996). The p53 tumour sup-pressor gene: a model for molecular epi-demiology of human cancer. Mol MedToday 2: 32-37. 2760. Soussi T, Beroud C (2001). AssessingTP53 status in human tumours to evaluateclinical outcome. Nat Rev Cancer 1: 233-240.
2761. Soussi T, Dehouche K, Beroud C(2000). p53 website and analysis of p53gene mutations in human cancer: forging alink between epidemiology and carcino-genesis. Hum Mutat 15: 105-113. 2762. Spagnolo DV, Shilkin KB (1983).Breast neoplasms containing bone andcartilage. Virchows Arch A Pathol AnatHistopathol 400: 287-295. 2763. Spatz A, Bouron D, Pautier P,Castaigne D, Duvillard P (1998). Primaryyolk sac tumor of the endometrium: a casereport and review of the literature.Gynecol Oncol 70: 285-288. 2764. Spiegel GW (1995). Endometrial car-cinoma in situ in postmenopausal women.Am J Surg Pathol 19: 417-432. 2765. Spitz DJ, Reddy VB, Gattuso P (1999).Fine-needle aspiration of pseudoangioma -tous stromal hyperplasia of the breast.Diagn Cytopathol 20: 323-324. 2766. Spitzer M (1999). Lower genital tractintraepithelial neoplasia in HIV-infectedwomen: guidelines for evaluation andmanagement. Obstet Gynecol Surv 54: 131-137. 2767. Sreenan JJ, Hart WR (1995).Carcinosarcomas of the female genitaltract. A pathologic study of 29 metastatictumors: further evidence for the dominantrole of the epithelial component and theconversion theory of histogenesis. Am JSurg Pathol 19: 666-674. 2768. Srigley JR, Colgan TJ (1988).Multifocal and diffuse adenomatoid tumorinvolving uterus and fallopian tube.Ultrastruct Pathol 12: 351-355. 2769. Srivatsa PJ, Keeney GL, Podratz KC(1994). Disseminated cervical adenomamalignum and bilateral ovarian sex cordtumors with annular tubules associatedwith Peutz-Jeghers syndrome. G y n e c o lOncol 53: 256-264. 2 7 7 0 . Ssali JC, Gakwaya A, Katongole-Mbidde F (1995). Risk factors for breastcancer in Ugandan women: a case-controlstudy. East Central Afr J Surg 1: 9-13. 2771. Staebler A, Heselmeyer-Haddad K,Bell K, Riopel M, Perlman E, Ried T,Kurman RJ (2002). Micropapillary serouscarcinoma of the ovary has distinct pat-terns of chromosomal imbalances by com-parative genomic hybridization comparedwith atypical proliferative serous tumorsand serous carcinomas. Hum Pathol 33: 47-59. 2772. Staebler A, Lax SF, Ellenson LH(2000). Altered expression of hMLH1 andhMSH2 protein in endometrial carcinomaswith microsatellite instability. Hum Pathol31: 354-358. 2773. Stalsberg H, Blom PE, Bostad LH,Westgaard G (1983). An InternationalSurvey of Distributions of Histologic Typesof Tumours of the Testis and Ovary(Ovarian tumours and endometriosis inNorway General Hospital material). UICC:Geneva.2774. Stambolic V, Suzuki A, de la PompaJL, Brothers GM, Mirtsos C, Sasaki T,Ruland J, Penninger JM, Siderovski DP,Mak TW (1998). Negative regulation ofPKB/Akt-dependent cell survival by thetumor suppressor PTEN. Cell 95: 29-39.
2775. Stankovic T, Kidd AM, Sutcliffe A,McGuire GM, Robinson P, Weber P,Bedenham T, Bradwell AR, Easton DF,Lennox GG, Haites N, Byrd PJ, Taylor AM(1998). ATM mutations and phenotypes inataxia-telangiectasia families in the BritishIsles: expression of mutant ATM and therisk of leukemia, lymphoma, and breastcancer. Am J Hum Genet 62: 334-345. 2775a. Stapleton JJ, Holser MH, Linder LE(1981). Paramesonephric papillary serouscystadenocarcinoma. A case report withscanning electron microscopy. Acta Cytol25: 310-316. 2776. Starink TM, van der Veen JP, ArwertF, de Waal LP, de Lange GG, Gille JJ,Eriksson AW (1986). The Cowden syn-drome: a clinical and genetic study in 21patients. Clin Genet 29: 222-233. 2777. Steck PA, Pershouse MA, Jasser SA,Yung WK, Lin H, Ligon AH, Langford LA,Baumgard ML, Hattier T, Davis T, Frye C,Hu R, Swedlund B, Teng DH, Tavtigian SV(1997). Identification of a candidate tumoursuppressor gene, MMAC1, at chromosome10q23.3 that is mutated in multipleadvanced cancers. Nat Genet 15: 356-362. 2778. Steeper TA, Piscioli F, Rosai J (1983).Squamous cell carcinoma with sarcoma-like stroma of the female genital tract.Clinicopathologic study of four cases.Cancer 52: 890-898. 2779. Steeper TA, Rosai J (1983).Aggressive angiomyxoma of the femalepelvis and perineum. Report of nine casesof a distinctive type of gynecologic soft-tis-sue neoplasm. Am J Surg Pathol7: 463-475. 2780. Steeper TA, Wick MR (1986). Minimaldeviation adenocarcinoma of the uterinecervix ("adenoma malignum"). An immuno-histochemical comparison with microglan-dular endocervical hyperplasia and con-ventional endocervical adenocarcinoma.Cancer 58: 1131-1138. 2781. Stefani M, Speranza N (1970). [A caseof cylindroma of the vagina]. Riv AnatPatol Oncol 36: 77-105. 2782. Stehman FB, Bundy BN, Disaia PJ,Keys HM, Larson JE, Fowler WC (1991).Carcinoma of the cervix treated with radi-ation therapy. I. A multi-variate analysis ofprognostic variables in the GynecologicOncology Group. Cancer 67: 2776-2785. 2783. Stehman FB, Bundy BN, DvoretskyPM, Creasman WT (1992). Early stage Icarcinoma of the vulva treated with ipsilat-eral superficial inguinal lymphadenectomyand modified radical hemivulvectomy: aprospective study of the GynecologicOncology Group. Obstet Gynecol 79: 490-497. 2784. Steingaszner LC, Enzinger FM, TaylorHB (1965). Hemangiosarcoma of thebreast. Cancer 18: 352-361. 2785. Stenkvist B, Bengtsson E, DahlqvistB, Eklund G, Eriksson O, Jarkrans T, NordinB (1982). Predicting breast cancer recur-rence. Cancer 50: 2884-2893. 2786. Stenwig JT, Hazekamp JT, BeechamJB (1979). Granulosa cell tumors of theovary. A clinicopathological study of 118cases with long-term follow-up. GynecolOncol 7: 136-152. 2787. Stephenson TJ, Mills PM (1986).Adenomatoid tumours: an immunohisto-chemical and ultrastructural appraisal oftheir histogenesis. J Pathol 148: 327-335. 2788. Sternberg WH, Barclay DL (1966).Luteoma of pregnancy. Am J ObstetGynecol 95: 165-184.
2789. Sternberg WH, Roth LM (1973).Ovarian stromal tumors containing Leydigcells. I. Stromal-Leydig cell tumor and non-neoplastic transformation of ovarian stro-ma to Leydig cells. Cancer 32: 940-951. 2790. Stettner AR, Hartenbach EM, SchinkJC, Huddart R, Becker J, Pauli R, Long R,Laxova R (1999). Familial ovarian germ cellcancer: report and review. Am J MedGenet 84: 43-46. 2791. Stevens RG (1987). Electric poweruse and breast cancer: a hypothesis. Am JEpidemiol 125: 556-561. 2792. Stewart CJ, Nandini CL, Richmond JA(2000). Value of A103 (melan-A) immunos-taining in the differential diagnosis of ovar-ian sex cord stromal tumours.J Clin Pathol53: 206-211. 2793. Stewart FW, Treves N (1949).Lymphangiosarcoma in postmastectomylymphedema. A report of six cases of ele-phantiasis chirurgica. Cancer 1: 64-81. 2794. Stock RJ, Zaino R, Bundy BN, AskinFB, Woodward J, Fetter B, Paulson JA,Disaia PJ, Stehman FB (1994). Evaluationand comparison of histopathologic gradingsystems of epithelial carcinoma of theuterine cervix: Gynecologic OncologyGroup studies. Int J Gynecol Pathol 13: 99-108. 2795. Stocks LH, Patterson FM (1976).Inflammatory carcinoma of the breast.Surg Gynecol Obstet 143: 885-889. 2796. Stomper PC, Connolly JL (1992).Ductal carcinoma in situ of the breast: cor-relation between mammographic calcifi-cation and tumor subtype. AJR Am JRoentgenol 159: 483-485. 2797. Stone GC, Bell DA, Fuller A, DickersinGR, Scully RE (1986). Malignant schwanno-ma of the ovary. Report of a case. Cancer58: 1575-1582. 2798. Storm HH, Jensen OM (1986). Risk ofcontralateral breast cancer in Denmark1943-80. Br J Cancer 54: 483-492. 2799. Storm HH, Olsen J (1999). Risk ofbreast cancer in offspring of male breast-cancer patients. Lancet 353: 209. 2800. Stratton JF, Gayther SA, Russell P,Dearden J, Gore M, Blake P, Easton D,Ponder BA (1997). Contribution of BRCA1mutations to ovarian cancer. N Engl J Med336: 1125-1130. 2801. Stratton JF, Pharoah P, Smith SK,Easton D, Ponder BA (1998). A systematicreview and meta-analysis of family historyand risk of ovarian cancer. Br J ObstetGynaecol 105: 493-499. 2802. Stratton JF, Thompson D, Bobrow L,Dalal N, Gore M, Bishop DT, Scott I, EvansG, Daly P, Easton DF, Ponder BA (1999).The genetic epidemiology of early-onsetepithelial ovarian cancer: a population-based study. Am J Hum Genet 65: 1725-1732. 2803. Straughn JM Jr., Richter HE, ConnerMG, Meleth S, Barnes MN (2001).Predictors of outcome in small cell carci-noma of the cervix--a case series.Gynecol Oncol 83: 216-220. 2804. Sturgeon SR, Brinton LA, Devesa SS,Kurman RJ (1992). In situ and invasive vul-var cancer incidence trends (1973 to 1987).Am J Obstet Gynecol 166: 1482-1485. 2805. Sturgeon SR, Sherman ME, KurmanRJ, Berman ML, Mortel R, Twiggs LB,Barrett RJ, Wilbanks GD, Brinton LA (1998).Analysis of histopathological features ofendometrioid uterine carcinomas and epi-demiologic risk factors. Cancer EpidemiolBiomarkers Prev 7: 231-235.

417References
2806. Stutz JA, Evans AJ, Pinder S, Ellis IO,Yeoman LJ, Wilson AR, Sibbering DM(1994). The radiological appearances ofinvasive cribriform carcinoma of thebreast. Nottingham Breast Team. C l i nRadiol 49: 693-695. 2807. Su TH, Wang JC, Tseng HH, ChangCP, Chang TA, Wei HJ, Chang JG (1998).Analysis of FHIT transcripts in cervical andendometrial cancers. Int J Cancer 76: 216-222. 2808. Su Y, Swift M (2000). Mortality ratesamong carriers of ataxia-telangiectasiamutant alleles. Ann Intern Med 133: 770-778. 2809. Su Y, Swift M (2001). Outcomes ofadjuvant radiation therapy for breast can-cer in women with ataxia-telangiectasiamutations. JAMA 286: 2233-2234. 2810. Su YN, Cheng WF, Chen CA, Lin TY,Hsieh FJ, Cheng SP, Hsieh CY (1999).Pregnancy with primary tubal placentalsite trophoblastic tumor--A case reportand literature review. Gynecol Oncol 73:322-325. 2811. Suarez A, Palacios J, Burgos E,Gamallo C (1993). Signet-ring stromaltumor of the ovary: a histochemical,immunohistochemical and ultrastructuralstudy. Virchows Arch A Pathol AnatHistopathol 422: 333-336. 2812. Suarez VD, Gimenez PA, Rio SM(1990). Vaginal rhabdomyoma and adeno-sis. Histopathology 16: 393-394. 2813. Sugiyama T, Ohta S, Nishida T, OkuraN, Tanabe K, Yakushiji M (1998). Two casesof endometrial adenocarcinoma arisingfrom atypical polypoid adenomyoma.Gynecol Oncol 71: 141-144. 2814. Sullivan JJ, Magee HR, Donald KJ(1977). Secretory (juvenile) carcinoma ofthe breast. Pathology 9: 341-346. 2815. Sumpio BE, Jennings TA, Merino MJ,Sullivan PD (1987). Adenoid cystic carcino-ma of the breast. Data from theConnecticut Tumor Registry and a reviewof the literature. Ann Surg 205: 295-301. 2816. Suster S, Moran CA, Hurt MA (1991).Syringomatous squamous tumors of thebreast. Cancer 67: 2350-2355. 2817. Suzuki A, de la Pompa JL, StambolicV, Elia AJ, Sasaki T, del Barco Barrantes I,Ho A, Wakeham A, Itie A, Khoo W,Fukumoto M, Mak TW (1998). High cancersusceptibility and embryonic lethalityassociated with mutation of the PTENtumor suppressor gene in mice. Curr Biol 8:1169-1178. 2818. Swanson GP, Dobin SM, Arber JM,Arber DA, Capen CV, Diaz JA (1997).Chromosome 11 abnormalities in Bowendisease of the vulva. Cancer GenetCytogenet 93: 109-114. 2819. Swift M, Morrell D, Massey RB,Chase CL (1991). Incidence of cancer in 161families affected by ataxia-telangiectasia.N Engl J Med 325: 1831-1836. 2820. Swift M, Reitnauer PJ, Morrell D,Chase CL (1987). Breast and other cancersin families with ataxia-telangiectasia. NEngl J Med 316: 1289-1294. 2821. Switzer JM, Weckstein ML, CampbellLF, Curtis KL, Powaser JT (1984). Ovarianhydatidiform mole. J Ultrasound Med 3:471-473. 2822. Sworn MJ, Hammond GT, BuchananR (1979). Mixed mesenchymal sarcoma ofthe broad ligament: case report. Br JObstet Gynaecol 86: 403-406.
2823. Symonds RP, Habeshaw T, Paul J,Kerr DJ, Darling A, Burnett RA, Sotsiou F,Linardopoulos S, Spandidos DA (1992). Nocorrelation between ras, c-myc and c-junproto-oncogene expression and prognosisin advanced carcinoma of cervix. Eur JCancer 28A: 1615-1617. 2824. Szabo CI, King MC (1997). Populationgenetics of BRCA1 and BRCA2. Am J HumGenet 60: 1013-1020. 2825. Szabo CI, Wagner LA, Francisco LV,Roach JC, Argonza R, King MC, OstranderEA (1996). Human, canine and murineBRCA1 genes: sequence comparisonamong species. Hum Mol Genet 5: 1289-1298. 2 8 2 6 . Szarewski A, Cuzick J (1998).Smoking and cervical neoplasia: a reviewof the evidence. J Epidem Biostat 3: 229-256. 2827. Szukala SA, Marks JR, Burchette JL,Elbendary AA, Krigman HR (1999). Co-expression of p53 by epithelial and stromalelements in carcinosarcoma of the femalegenital tract: an immunohistochemicalstudy of 19 cases. Int J Gynecol Cancer 9:131-136. 2828. Szulman AE, Surti U (1978). The syn-dromes of hydatidiform mole. I.Cytogenetic and morphologic correlations.Am J Obstet Gynecol 131: 665-671. 2829. Szulman AE, Surti U (1978). The syn-dromes of hydatidiform mole. II.Morphologic evolution of the complete andpartial mole. Am J Obstet Gynecol 132: 20-27. 2830. Szych C, Staebler A, Connolly DC, WuR, Cho KR, Ronnett BM (1999). Moleculargenetic evidence supporting the clonalityand appendiceal origin of Pseudomyxomaperitonei in women. Am J Pathol 154: 1849-1855. 2831. Szyfelbein WM, Young RH, Scully RE(1994). Cystic struma ovarii: a frequentlyunrecognized tumor. A report of 20 cases.Am J Surg Pathol 18: 785-788. 2832. Szyfelbein WM, Young RH, Scully RE(1995). Struma ovarii simulating ovariantumors of other types. A report of 30 cases.Am J Surg Pathol 19: 21-29. 2833. Tagaya N, Kodaira H, Kogure H,Shimizu K (1999). A case of phyllodes tumorwith bloody nipple discharge in juvenilepatient. Breast Cancer 6: 207-210. 2834. Tai LH, Tavassoli FA (2002).Endometrial polyps with atypical (bizarre)stromal cells. Am J Surg Pathol 26: 505-509. 2835. Takahashi M, Kigawa J, Ishihara K,Shimada M, Kamei T, Terakawa N (2002).Hydrotubation for diagnosing carcinoma insitu of the fallopian tube. A case report.Acta Cytol 46: 735-737. 2836. Takahashi O, Shibata S, Hatazawa J,Takisawa J, Sato H, Ota H, Tanaka T (1998).Mature cystic teratoma of the uterine cor-pus. Acta Obstet Gynecol Scand 77: 936-938. 2837. Takahashi T, Moriki T, Hiroi M,Nakayama H (1998). Invasive lobular carci-noma of the breast with osteoclastlikegiant cells. A case report. Acta Cytol 42:734-741. 2838. Takemori M, Nishimura R, Yasuda D,Sugimura K (1997). Carcinosarcoma of theuterus: magnetic resonance imaging.Gynecol Obstet Invest 43: 139-141. 2839. Takeshima N, Tabata T, Nishida H,Furuta N, Tsuzuku M, Hirai Y, Hasumi K(2001). Peripheral primitive neuroectoder-mal tumor of the vulva: report of a casewith imprint cytology. Acta Cytol 45: 1049-1052.
2840. Takeuchi K, Murata K, Funaki K, FujitaI, Hayakawa Y, Kitazawa S (2000).Liposarcoma of the uterine cervix: casereport. Eur J Gynaecol Oncol 21: 290-291. 2841. Takeuchi S (1982). Nature of invasivemole and its rational management. SeminOncol 9: 181-186. 2842. Takeuchi S, Ishihara N, Ohbayashi C,Itoh H, Maruo T (1999). Stromal Leydig celltumor of the ovary. Case report and litera-ture review. Int J Gynecol Pathol 18: 178-182. 2843. Talamonti MS (1996). Management ofductal carcinoma in situ. Semin SurgOncol 12: 300-313. 2 8 4 4 . Talerman A (1972). A distinctivegonadal neoplasm related to gonadoblas-toma. Cancer 30: 1219-1224. 2845. Talerman A (1972). A mixed germcell-sex cord stroma tumor of the ovary ina normal female infant. Obstet Gynecol 40:473-478. 2846. Talerman A (1974). Gonadoblastomaassociated with embryonal carcinoma.Obstet Gynecol 43: 138-142. 2847. Talerman A (1980). The pathology ofgonadal neoplasms composed of germcells and sex cord stroma derivatives.Pathol Res Pract 170: 24-38. 2848. Talerman A (1994). Germ cell tumoursof the ovary. In: Blaustein's Pathology ofthe Female Genital Tract, RJ Kurman (ed.),4th ed. Springer-Verlag: New York, pp.849-914.2849. Talerman A (2002). Mixed germ cell-sex cord stromal tumours. In: Haines andTaylor, Gynaecological and ObstetricalPathology, 5th ed. Churchill Livingstone:Edingburgh.2850. Talerman A (2002). Mixed germ celltumors of the ovary. In: Blaustein'sPathology of the Female Genital Tract, RJKurman, A Blaustein (eds.), 5th ed.Springer Verlag: New York.2851. Talerman A, Auerbach WM, vanMeurs AJ (1981). Primary chondrosarcomaof the ovary. Histopathology 5: 319-324. 2852. Talerman A, van der Harten JJ (1977).Mixed germ cell-sex cord stroma tumor ofthe ovary associated with isosexual preco-cious puberty in a normal girl. Cancer 40:889-894. 2853. Tallini G, Price FV, Carcangiu ML(1993). Epithelioid angiosarcoma arising inuterine leiomyomas. Am J Clin Pathol 100:514-518. 2 8 5 4 . Tallini G, Vanni R, Manfioletti G,Kazmierczak B, Faa G, Pauwels P,Bullerdiek J, Giancotti V, Van den BergheH, Dal Cin P (2000). HMGI-C and HMGI(Y)immunoreactivity correlates with cytoge-netic abnormalities in lipomas, pulmonarychondroid hamartomas, endometrialpolyps, and uterine leiomyomas and iscompatible with rearrangement of theHMGI-C and HMGI(Y) genes. Lab Invest80: 359-369. 2855. Talwar S, Prasad N, Gandhi S, PrasadP (1999). Haemangiopericytoma of theadult male breast. Int J Clin Pract 53: 485-486. 2856. Tambouret R, Bell DA, Young RH(2000). Microcystic endocervical adeno-carcinomas: a report of eight cases. Am JSurg Pathol 24: 369-374. 2 8 5 7 . Tamimi HK, Bolen JW (1984).Enchondromatosis (Ollier's disease) andovarian juvenile granulosa cell tumor.Cancer 53: 1605-1608.
2858. Tamura S, Enjoji M (1988). Elastosis inneoplastic and non-neoplastic tissuesfrom patients with mammary carcinoma.Acta Pathol Jpn 38: 1537-1546. 2859. Tanaka Y, Sasaki Y, Nishihira H,Izawa T, Nishi T (1992). Ovarian juvenilegranulosa cell tumor associated withMaffucci's syndrome. Am J Clin Pathol 97:523-527. 2860. Tang CK, Toker C, Ances IG (1979).Stromomyoma of the uterus. Cancer 43:308-316. 2861. Tariel D, Body G, Fetissof F, MenardF, Lansac J (1986). [Postoperative vaginalpseudosarcoma. Apropos of a case]. JGynecol Obstet Biol Reprod (Paris) 15: 769-771. 2862. Taruscio D, Carcangiu ML, Ward DC(1993). Detection of trisomy 12 on ovariansex cord stromal tumors by fluorescencein situ hybridization. Diagn Mol Pathol 2:94-98. 2 8 6 3 . Tashiro H, Isacson C, Levine R,Kurman RJ, Cho KR, Hedrick L (1997). p53gene mutations are common in uterineserous carcinoma and occur early in theirpathogenesis. Am J Pathol 150: 177-185. 2864. Tasseron EW, van der Esch EP, HartAA, Brutel de la Riviere G, Aartsen EJ(1992). A clinicopathological study of 30melanomas of the vulva. Gynecol Oncol 46:170-175. 2 8 6 5 . Tateno H, Sasano N (1983). AnInternational Survey of Distribution ofHistologic Types Tumours of the Testis andOvary (Ovarian Tumours in Sendai Japan.General Hospital Material). UICCTechnical Report Series: Genova.2866. Tavassoli FA (1986). Melanotic para-ganglioma of the uterus. Cancer 58: 942-948. 2867. Tavassoli FA (1988). Serous tumor oflow malignant potential with early stromalinvasion (serous LMP with microinvasion).Mod Pathol 1: 407-414. 2868. Tavassoli FA (1991). Myoepitheliallesions of the breast. Myoepitheliosis, ade-nomyoepithelioma, and myoepithelial car-cinoma. Am J Surg Pathol 15: 554-568. 2869. Tavassoli FA (1992). Carcinoma withosteoclastic giant cells. In: Pathology ofthe Breast, Appleton and Lange: Norwalk,Connecticut.2870. Tavassoli FA (1992). Glycogen-rich(clear-cell) carcinoma. In: Pathology ofthe Breast, Appleton and Lange: Norwalk,Connecticut .2871. Tavassoli FA (1992). Mesenchymallesions. In: Pathology of the Breast,Tavassoli FA, ed., First edition ed.Appleton and Lange: Norwalk , pp. 557-558.2872. Tavassoli FA (1992). Metastatic car-cinoma. In: Pathology of the Breast,Appleton and Lange: Norwalk,Connecticut.2873. Tavassoli FA (1992). Papillary lesions.In: Pathology of the Breast, Appleton andLange: Stamford , pp. 193-228.2874. Tavassoli FA (1992). Pathology of theBreast. Appleton and Lange: Stanford.2875. Tavassoli FA (1999). Myoepitheliallesions. In: Pathology of the Breast, 2nd ed.Appleton and Lange: Hartford, pp. 763-791.2876. Tavassoli FA (1999). Pathology of theBreast. 2nd ed. Appleton-Lange: Stamford.2877. Tavassoli FA, Andrade R, Merino M(1990). Retiform wolffian adenoma. In:Progress in Surgical Pathology, C MFenoglio-Preiser, M Wolfe, F Rilke (eds.),Field & Wood Medica Publishers inc: NewYork, pp. 121-136.

418 References
2878. Tavassoli FA, Andradre R, Merino M(1990). Retiform wolffian adenoma.Progress in Surgical Pathology. Field &Wood Medical Publishers: New York.2879. Tavassoli FA, Norris HJ (1979).Smooth muscle tumors of the vagina.Obstet Gynecol 53: 689-693. 2 8 8 0 . Tavassoli FA, Norris HJ (1979).Smooth muscle tumors of the vulva. ObstetGynecol 53: 213-217. 2 8 8 1 . Tavassoli FA, Norris HJ (1980).Secretory carcinoma of the breast.Cancer45: 2404-2413. 2882. Tavassoli FA, Norris HJ (1980). Sertolitumors of the ovary. A clinicopathologicstudy of 28 cases with ultrastructuralobservations. Cancer 46: 2281-2297. 2 8 8 3 . Tavassoli FA, Norris HJ (1981).Mesenchymal tumours of the uterus. VII. Aclinicopathological study of 60 endometrialstromal nodules. Histopathology 5: 1-10. 2 8 8 4 . Tavassoli FA, Norris HJ (1983).Microglandular adenosis of the breast. Aclinicopathologic study of 11 cases withultrastructural observations. Am J SurgPathol 7: 731-737. 2 8 8 5 . Tavassoli FA, Norris HJ (1986).Mammary adenoid cystic carcinoma withsebaceous differentiation. A morphologicstudy of the cell types. Arch Pathol LabMed 110: 1045-1053. 2886. Tavassoli FA, Norris HJ (1990). Acomparison of the results of long-term fol-low-up for atypical intraductal hyperplasiaand intraductal hyperplasia of the breast.Cancer 65: 518-529. 2 8 8 7 . Tavassoli FA, Norris HJ (1994).Intraductal apocrine carcinoma: a clinico-pathologic study of 37 cases.Mod Pathol 7:813-818. 2888. Tavassoli FA, Purcell CA, BratthauerGL, Man Y (1996). Androgen receptorexpression along with loss of bcl-2, ER andPR expression in benign and malignantapocrine lesions of the breast: implicationsfor therapy. Breast Jour 2: 261-269. 2 8 8 9 . Tavassoli FA, Weiss S (1981).Hemangiopericytoma of the breast. Am JSurg Pathol 5: 745-752. 2890. Tavassoli FA, Yeh IT (1988). Surgicalpathology of the ovary: a review of select-ed tumors. Mod Pathol 1: 140-167. 2891. Tavtigian SV, Simard J, Rommens J,Couch F, Shattuck-Eidens D, Neuhausen S,Merajver S, Thorlacius S, Offit K, Stoppa-Lyonnet D, Belanger C, Bell R, Berry S,Bogden R, Chen Q, Davis T, Dumont M,Frye C, Hattier T, Jammulapati S, JaneckiT, Jiang P, Kehrer R, Leblanc JF, MitchellJT, McArthur Morrisson J, Nguyen K, PengY, Samson C, Shroeder M, Snyder SC,Steele L, Stringfellow M, Stroup C,Swedlund B, Swensen J, Teng D, ThomasA, Tran T, Tran T, Tranchant M, WeaverFeldhaus J, Wong AKC, Shizuya H, EyfjordJE, Cannon Albright L, Labrie F, SkolnickMH, Weber B, Kamb A, Goldgar DE (1996).The complete BRCA2 gene and mutationsin chromosome 13q-linked kindreds. NatGenet 12: 333-337.2892. Taxy JB, Trujillo YP (1994). Breastcancer metastatic to the uterus. Clinicalmanifestations of a rare event. A r c hPathol Lab Med 118: 819-821. 2893. Taylor CE, Tuttle HK (1944).Melanocarcinoma of the cervix uteri andvaginal vault. Arch Pathol 38: 60-61. 2894. Taylor HB, Robertson A.G. (1965).Adenomas of the nipple. Cancer 18: 995-1002.
2894a. Taylor HCJ (1929). Malignant andsemimalignant tumors of the ovary. SurgGynecol Obstet 48: 204-230. 2895. Taylor RN, Lacey CG, Shuman MA(1985). Adenocarcinoma of Skene's ductassociated with a systemic coagulopathy.Gynecol Oncol 22: 250-256. 2896. Teilum G (1965). Endodermal sinus ofthe ovary and testis: comparative morpho -genesis of the so-called mesonephromaovarii (Schiller) and extraembryonic (yolksac allantoic) structures of the rat's pal-centa. Cancer 12: 1091-1105. 2897. Teixeira MR, Kristensen GB, AbelerVM, Heim S (1999). Karyotypic findings intumors of the vulva and vagina. CancerGenet Cytogenet 111: 87-91. 2898. Tempany CM, Zou KH, Silverman SG,Brown DL, Kurtz AB, McNeil BJ (2000).Staging of advanced ovarian cancer: com-parison of imaging modalities--report fromthe Radiological Diagnostic OncologyGroup. Radiology 215: 761-767. 2899. Terada S, Suzuki N, Uchide K, ShozuM, Akasofu K (1993). Parovarian fibromawith heterotopic bone formation of proba-ble wolffian origin. Gynecol Oncol 50: 115-118. 2900. Terzakis JA, Opher E, Melamed J,Santagada E, Sloan D (1990). Pigmentedmelanocytic schwannoma of the uterinecervix. Ultrastruct Pathol 14: 357-366. 2901. Tetu B, Bonenfant JL (1991). Ovarianmyxoma. A study of two cases with long-term follow-up. Am J Clin Pathol 95: 340-346. 2902. Tetu B, Silva EG, Gershenson DM(1987). Squamous cell carcinoma of theovary. Arch Pathol Lab Med 111: 864-866. 2903. Tewari K, Cappuccini F, Disaia PJ,Berman ML, Manetta A, Kohler MF (2000).Malignant germ cell tumors of the ovary.Obstet Gynecol 95: 128-133. 2904. Thakur S, Zhang HB, Peng Y, Le H,Carroll B, Ward T, Yao J, Farid LM, CouchFJ, Wilson RB, Weber BL (1997).Localization of BRCA1 and a splice variantidentifies the nuclear localization signal.Mol Cell Biol 17: 444-452. 2905. The European Commission (1996).European Guidelines for QualityAssurance in Mammography Screening.2nd ed. The European Commission:Luxembourg.2906. Thomas DB, Jimenez LM, McTiernanA, Rosenblatt K, Stalsberg H, StemhagenA, Thompson WD, Curnen MG, SatarianoW, Austin DF, et al. (1992). Breast cancer inmen: risk factors with hormonal implica-tions. Am J Epidemiol 135: 734-748. 2907. Thomas EJ, Campbell IG (2000).Molecular genetic defects in endometrio-sis. Gynecol Obstet Invest 50 Suppl 1: 44-50. 2908. Thomas GM (2000). Concurrentchemotherapy and radiation for locallyadvanced cervical cancer: the new stan-dard of care. Semin Radiat Oncol 10: 44-50. 2909. Thomas HV, Key TJ, Allen DS, MooreJW, Dowsett M, Fentiman IS, Wang DY(1997). A prospective study of endogenousserum hormone concentrations and breastcancer risk in premenopausal women onthe island of Guernsey. Br J Cancer 75:1075-1079. 2910. Thomas JP, Timbal Y, Wannin G,Dumurgier C (1973). [Schwannoglioma ofthe broad ligament]. J Urol Nephrol (Paris)79: 933-935.
2911. Thomas M, Pim D, Banks L (1999).The role of the E6-p53 interaction in themolecular pathogenesis of HPV.Oncogene 18: 7690-7700. 2912. Thomas NA, Choong DY, JokubaitisVJ, Neville PJ, Campbell IG (2001).Mutation of the ST7 tumor suppressorgene on 7q31.1 is rare in breast, ovarianand colorectal cancers. Nat Genet 29: 379-380. 2912a. Thomason RW, Rush W, Dave H(1995). Transitional cell carcinoma arisingwithin a paratubal cyst: report of a case.Int J Gynecol Pathol 14: 270-273. 2913. Thompson D, Easton D (2001).Variation in cancer risks, by mutation posi-tion, in BRCA2 mutation carriers. Am JHum Genet 68: 410-419. 2914. Thompson D, Easton D (2002).Variation in BRCA1 cancer risks by muta-tion position. Cancer Epidemiol BiomarkersPrev 11: 329-336. 2915. Thompson D, Easton DF (2002).Cancer incidence in BRCA1 mutation carri-ers. J Natl Cancer Inst 94: 1358-1365. 2916. Thompson M, Husemeyer R (1981).Carcinofibroma--a variant of the mixedMullerian tumour. Case report. Br J ObstetGynaecol 88: 1151-1155. 2917. Thompson ME, Jensen RA,Obermiller PS, Page DL, Holt JT (1995).Decreased expression of BRCA1 acceler-ates growth and is often present duringsporadic breast cancer progression. NatGenet 9: 444-450. 2918. Thompson WD, Schildkraut JM(1991). Family history of gynaecologicalcancers: relationships to the incidence ofbreast cancer prior to age 55. Int JEpidemiol 20: 595-602. 2919. Thor AD, Young RH, Clement PB(1991). Pathology of the fallopian tube,broad ligament, peritoneum, and pelvicsoft tissues. Hum Pathol 22: 856-867. 2920. Thorlacius S, Sigurdsson S,Bjarnadottir H, Olafsdottir G, Jonasson JG,Tryggvadottir L, Tulinius H, Eyfjord JE(1997). Study of a single BRCA2 mutationwith high carrier frequency in a small pop -ulation. Am J Hum Genet 60: 1079-1084. 2921. Thorlacius S, Struewing JP, Hartge P,Olafsdottir GH, Sigvaldason H,Tryggvadottir L, Wacholder S, Tulinius H,Eyfjord JE (1998). Population-based studyof risk of breast cancer in carriers ofBRCA2 mutation. Lancet 352: 1337-1339. 2922. Thurlbeck WM, Scully RE (1960).Solid teratoma of the ovary. A clinico-pathological analysis of 9 cases. Cancer13: 804-811. 2923. Tietze L, Gunther K, Horbe A, PawlikC, Klosterhalfen B, Handt S, Merkelbach-Bruse S (2000). Benign metastasizingleiomyoma: a cytogenetically balanced butclonal disease. Hum Pathol 31: 126-128. 2924. Tiltman AJ (1980). Adenomatoidtumours of the uterus. Histopathology 4:437-443. 2925. Tiltman AJ (1998). Leiomyomas of theuterine cervix: a study of frequency. Int JGynecol Pathol 17: 231-234. 2926. Tiltman AJ, Allard U (2001). Femaleadnexal tumours of probable Wolffian ori-gin: an immunohistochemical study com-paring tumours, mesonephric remnantsand paramesonephric derivatives.Histopathology 38: 237-242.
2927. Tirkkonen M, Kainu T, Loman N,Johannsson OT, Olsson H, Barkardottir RB,Kallioniemi OP, Borg A (1999). Somaticgenetic alterations in BRCA2-associatedand sporadic male breast cancer. GenesChromosomes Cancer 24: 56-61. 2928. Tjarks M, Van Voorhis BJ (2000).Treatment of endometrial polyps. ObstetGynecol 96: 886-889. 2929. Tobon H, Murphy AI (1977). Benignblue nevus of the vagina. Cancer 40: 3174-3176. 2930. Todorov S (1980). Polyposis of theuterine cervix. Jugosl Ginekol Opstet 19:183-186. 2931. Tohya T, Katabuchi H, Fukuma K,Fujisaki S, Okamura H (1991). Angio-sarcoma of the vagina. A light and elec-tronmicroscopy study. Acta ObstetGynecol Scand 70: 169-172. 2932. Toikkanen S (1981). Primary squa-mous cell carcinoma of the breast. Cancer48: 1629-1632. 2933. Toikkanen S, Eerola E, Ekfors TO(1988). Pure and mixed mucinous breastcarcinomas: DNA stemline and prognosis.J Clin Pathol 41: 300-303. 2934. Toikkanen S, Kujari H (1989). Pureand mixed mucinous carcinomas of thebreast: a clinicopathologic analysis of 61cases with long-term follow-up. H u mPathol 20: 758-764. 2935. Toikkanen S, Pylkkanen L, Joensuu H(1997). Invasive lobular carcinoma of thebreast has better short- and long-term sur-vival than invasive ductal carcinoma. Br JCancer 76: 1234-1240. 2936. Toki T, Kurman RJ, Park JS, Kessis T,Daniel RW, Shah KV (1991). Probable non-papillomavirus etiology of squamous cellcarcinoma of the vulva in older women: aclinicopathologic study using in situhybridization and polymerase chain reac-tion. Int J Gynecol Pathol 10: 107-125. 2937. Toki T, Zhai Y-L, Park JS, Fujii S(1999). Infrequent occurence of high-riskhuman papillomavirus and of p53 mutationin minimal deviation adenocarcinoma ofthe cervix. Int J Gynecol Pathol 18: 215-219. 2938. Tokunaga M, Land CE, Yamamoto T,Asano M, Tokuoka S, Ezaki H, Nishimori I(1987). Incidence of female breast canceramong atomic bomb survivors, Hiroshimaand Nagasaki, 1950-1980. Radiat Res 112:243-272. 2938a. Tommasino M (2001). Early genes ofhuman papillomaviruses. In: EncyclopedicReference of Cancer. Springer-Verlag:Heidelberg, p. 270.2939. Tonin P, Moslehi R, Green R, RosenB, Cole D, Boyd N, Cutler C, Margolese R,Carter R, McGillivray B, Ives E, Labrie F,Gilchrist D, Morgan K, Simard J, Narod SA.(1995). Linkage analysis of 26 Canadianbreast and breast-ovarian cancer families.Hum Genet 95: 545-550.2940. Topalovski M, Crisan D, Mattson JC(1999). Lymphoma of the breast. A clinico-pathologic study of primary and secondarycases. Arch Pathol Lab Med 123: 1208-1218. 2941. Tornos C, Silva EG, Khorana SM,Burke TW (1994). High-stage endometrioidcarcinoma of the ovary. Prognostic signifi-cance of pure versus mixed histologictypes. Am J Surg Pathol 18: 687-693.

419References
2942. Tornos C, Silva EG, Ordonez NG,Gershenson DM, Young RH, Scully RE(1995). Endometrioid carcinoma of theovary with a prominent spindle-cell com-ponent, a source of diagnostic confusion.A report of 14 cases. Am J Surg Pathol 19:1343-1353. 2943. Tot T (2000). The cytokeratin profile ofmedullary carcinoma of the breast.Histopathology 37: 175-181. 2944. Towfighi J, Simmonds MA, DavidsonEA (1983). Mucin and fat emboli in muci-nous carcinomas. Cause of hemorrhagiccerebral infarcts. Arch Pathol Lab Med107: 646-649. 2945. Traiman P, Bacchi CE, De Luca LA,Uemura G, Nahas NJ, Nahas EA, Pontes A(1999). Vulvar carcinoma in young patientsand its relationship with genital warts. EurJ Gynaecol Oncol 20: 191-194. 2946. Treffers PE, Hanselaar AG,Helmerhorst TJ, Koster ME, van LeeuwenFE (2001). [Consequences of diethylstilbe-strol during pregnancy; 50 years later still asignificant problem]. Ned TijdschrGeneeskd 145: 675-680. 2947. Treilleux T, Mignotte H, Clement-Chassagne C, Guastalla P, Bailly C (1999).Tamoxifen and malignant epithelial-nonep-ithelial tumours of the endometrium: reportof six cases and review of the literature.Eur J Surg Oncol 25: 477-482. 2 9 4 8 . Tremblay G, Pearse AGE (2001).Histochemistry of oxidative enzyme sys-tems in human thyroid with special refer-ence to Askanazy cells. J Pathol Bacteriol80: 353-358. 2949. Trimble EL (1996). Melanomas of thevulva and vagina. Oncology (Huntingt) 10:1017-1023. 2950. Trimble EL, Lewis JL Jr., Williams LL,Curtin JP, Chapman D, Woodruff JM, RubinSC, Hoskins WJ (1992). Management ofvulvar melanoma. Gynecol Oncol 45: 254-258. 2951. Trivedi P, Dave K, Shah M, Karelia N,Patel D, Wadhwa M (1998). Hepatoid carci-noma of the ovary--a case report. Eur JGynaecol Oncol 19: 167-169. 2952. Trojani M, De Mascarel I, Coquet M,Coindre JM, De Mascarel A (1989).[Osteoclastic type giant cell carcinoma ofthe breast]. Ann Pathol 9: 189-194. 2953. Trojani M, Guiu M, Trouette H, DeMascarel I, Cocquet M (1992). Malignantadenomyoepithelioma of the breast. Animmunohistochemical, cytophotometric,and ultrastructural study of a case withlung metastases. Am J Clin Pathol 98: 598-602. 2954. Troncone G, Martinez JC, PalombiniL, De Rosa G, Mugica C, Rodriguez JA,Zeppa P, Di Vizio D, Lucariello A, Piris MA(1998). Immunohistochemical expressionof mdm2 and p21WAF1 in invasive cervicalcancer: correlation with p53 protein andhigh risk HPV infection. J Clin Pathol 51:754-760. 2955. Tsang WY, Chan JK (1996). Endocrineductal carcinoma in situ (E-DCIS) of thebreast: a form of low-grade DCIS with dis-tinctive clinicopathologic and biologiccharacteristics. Am J Surg Pathol 20: 921-943. 2956. Tsang WYW, Chan JKC (1996).Endocrine ductal carcinoma in situ (E-DCIS) of the breast: a form of low-gradeDCIS with distinctive clinicopathologic andbiologic characteristics. Am J Surg Pathol20: 921-943.
2957. Tseng CJ, Pao CC, Tseng LH, ChangCT, Lai CH, Soong YK, Hsueh S, Jyu-Jen H(1997). Lymphoepithelioma-like carcinomaof the uterine cervix: association withEpstein-Barr virus and human papillo-mavirus. Cancer 80: 91-97. 2958. Tsongalis GJ, Ried A Jr. (2001). HER2:the neu prognostic marker for breast can-cer. Crit Rev Clin Lab Sci 38: 167-182. 2959. Tsou HC, Teng DH, Ping XL,Brancolini V, Davis T, Hu R, Xie XX,Gruener AC, Schrager CA, Christiano AM,Eng C, Steck P, Ott J, Tavtigian SV,Peacocke M (1997). The role of MMAC1mutations in early-onset breast cancer:causative in association with Cowden syn-drome and excluded in BRCA1-negativecases. Am J Hum Genet 61: 1036-1043. 2 9 6 0 . Tsuda H, Callen DF, Fukutomi T,Nakamura Y, Hirohashi S (1994). Allele losson chromosome 16q24.2-qter occurs fre-quently in breast cancers respectively ofdifferences in phenotype and extent ofspread. Cancer Res 54: 513-517. 2961. Tsuda H, Takarabe T, Susumu N,Inazawa J, Okada S, Hirohashi S (1997).Detection of numerical and structuralalterations and fusion of chromosomes 16and 1 in low-grade papillary breast carci-noma by fluorescence in situ hybridization.Am J Pathol 151: 1027-1034. 2962. Tsuda HH (2001). Prognostic and pre-dictive value of c-erbB-2 (HER-2/neu) geneamplification in human breast cancer.Breast Cancer 8: 38-44. 2963. Tsuji T, Kawauchi S, Utsunomiya T,Nagata Y, Tsuneyoshi M (1997).Fibrosarcoma versus cellular fibroma ofthe ovary: a comparative study of their pro-liferative activity and chromosome aberra-tions using MIB-1 immunostaining, DNAflow cytometry, and fluorescence in situhybridization. Am J Surg Pathol 21: 52-59. 2964. Tsukamoto N, Nakamura M,Ishikawa H (1976). Case report: sclerosingstromal tumor of the ovary. Gynecol Oncol4: 335-339. 2965. Tsuura Y, Hiraki H, Watanabe K,Igarashi S, Shimamura K, Fukuda T, SuzukiT, Seito T (1994). Preferential localization ofc-kit product in tissue mast cells, basalcells of skin, epithelial cells of breast, smallcell lung carcinoma and seminoma/dys-germinoma in human: immunohistochemi-cal study on formalin-fixed, paraffin-embedded tissues. Virchows Arch 4 2 4 :135-141. 2966. Tuncer ZS, Vegh GL, Fulop V, GenestDR, Mok SC, Berkowitz RS (2000).Expression of epidermal growth factorreceptor-related family products in gesta-tional trophoblastic diseases and normalplacenta and its relationship with develop-ment of postmolar tumor. Gynecol Oncol77: 389-393. 2967. Twiggs LB, Okagaki T, Phillips GL,Stroemer JR, Adcock LL (1981).Trophoblastic pseudotumor-evidence ofmalignant disease potential. G y n e c o lOncol 12: 238-248. 2968. Tyagi SP, Saxena K, Rizvi R, LangleyFA (1979). Foetal remnants in the uterusand their relation to other uterine hetero-topia. Histopathology 3: 339-345. 2969. Uchiyama M, Iwasaka T, Matsuo N,Hachisuga T, Mori M, Sugimori H (1997).Correlation between human papillo-mavirus positivity and p53 gene overex-pression in adenocarcinoma of the uterinecervix. Gynecol Oncol 65: 23-29.
2970. Ueda G, Fujita M, Ogawa H, SawadaM, Inoue M, Tanizawa O (1993).Adenocarcinoma in a benign cystic ter-atoma of the ovary: report of a case with along survival period. Gynecol Oncol 48:259-263. 2971. Ueda H, Togashi K, Konishi I, KataokaML, Koyama T, Fujiwara T, Kobayashi H,Fujii S, Konishi J (1999). Unusual appear-ances of uterine leiomyomas: MR imagingfindings and their histopathologic back-grounds. Radiographics 19 Spec No: S131-S145. 2972. Uehara T, Izumo T, Kishi K, TakayamaS, Kasuga T (1991). Stromal melanocyticfoci ("blue nevus") in step sections of theuterine cervix. Acta Pathol Jpn 41: 751-756. 2973. Uehara T, Takayama S, Takemura T,Kasuga T (1991). Foci of stromalmelanocytes (so-called blue naevus) of theuterine cervix in Japanese women.Virchows Arch A Pathol Anat Histopathol418: 327-331. 2974. Uehira K, Hashimoto H, TsuneyoshiM, Enjoji M (1993). Transitional cell carci-noma pattern in primary carcinoma of thefallopian tube. Cancer 72: 2447-2456. 2975. Ueki M, Sano T, Okamura S, Iito Y,Kitsuki K, Sugimoto O (1982). [Clinical diag-nosis of well differentiated cervical adeno-carcinoma with plentiful mucous secre-tion]. Nippon Sanka Fujinka Gakkai Zasshi34: 1846-1852. 2976. UICC (2002). TNM classification ofmalignant tumors. Sixth ed. John Wiley &Sons: New York.2977. Ulbright TM, Alexander RW, Kraus FT(1981). Intramural papilloma of the vagina:evidence of Mullerian histogenesis.Cancer 48: 2260-2266. 2978. Ulbright TM, Roth LM (1985).Metastatic and independent cancers ofthe endometrium and ovary: a clinico-pathologic study of 34 cases. Hum Pathol16: 28-34. 2979. Ulbright TM, Roth LM, BrodheckerCA (1986). Yolk sac differentiation in germcell tumors. A morphologic study of 50cases with emphasis on hepatic, enteric,and parietal yolk sac features. Am J SurgPathol 10: 151-164. 2980. Ulbright TM, Roth LM, Stehman FB(1984). Secondary ovarian neoplasia. Aclinicopathologic study of 35 cases.Cancer 53: 1164-1174. 2981. Underwood PB Jr., Smith RT (1971).Carcinoma of the vagina. JAMA 217: 46-52. 2982. Unkila-Kallio L, Tiitinen A, WahlstromT, Lehtovirta P, Leminen A (2000).Reproductive features in women develop-ing ovarian granulosa cell tumour at a fer-tile age. Hum Reprod 15: 589-593. 2983. Uziel T, Savitsky K, Platzer M, Ziv Y,Helbitz T, Nehls M, Boehm T, Rosenthal A,Shiloh Y, Rotman G (1996). GenomicOrganization of the ATM gene. Genomics33: 317-320. 2984. Vahteristo P, Bartkova J, Eerola H,Syrjakoski K, Ojala S, Kilpivaara O,Tamminen A, Kononen J, Aittomaki K,Heikkila P, Holli K, Blomqvist C, Bartek J,Kallioniemi OP, Nevanlinna H (2002). ACHEK2 genetic variant contributing to asubstantial fraction of familial breast can-cer. Am J Hum Genet 71: 432-438. 2985. Vaizey C, Burke M, Lange M (1999).Carcinoma of the male breast - a review of91 patients from the JohannesburgHospital breast clinics. S Afr J Surg 37: 6-8.
2986. van't Veer LJ, Dai H, Van de VijverMJ, He YD, Hart AA, Mao HL, van der KooyK, Marton MJ, Witteveen AT, SchreiberGJ, Kerkhoven RM, Roberts C, Linsley PS,Bernards R, Friend SH (2002). Gene expres-sion profiling predicts clinical outcome ofbreast cancer. Nature 415: 530-536. 2987. van Belzen MJ, Hiel JA, WeemaesCM, Gabreels FJ, van Engelen BG, SmeetsDF, van den Heuvel LP (1998). A doublemissense mutation in the ATM gene of aDutch family with ataxia telangiectasia.Hum Genet 102: 187-191. 2988. Van Bogaert LJ, Maldague P (1977).Histologic variants of lipid-secreting carci-noma of the breast. Virchows Arch APathol Anat 375: 345-353. 2989. Van de Vijver MJ (1999). The patholo-gy of familial breast cancer: The pre-BRCA1/BRCA2 era: historical perspec-tives. Breast Cancer Res 1: 27-30. 2990. Van de Vijver MJ, He YD, van't VeerLJ, Dai H, Hart AA, Voskuil DW, SchreiberGJ, Peterse JL, Roberts C, Marton MJ,Parrish M, Atsma D, Witteveen A, Glas A,Delahaye L, van der Velde T, Bartelink H,Rodenhuis S, Rutgers ET, Friend SH,Bernards R (2002). A gene-expression sig-nature as a predictor of survival in breastcancer. N Engl J Med 347: 1999-2009. 2991. van der Putte SC (1994). Mammary-like glands of the vulva and their disorders.Int J Gynecol Pathol 13: 150-160. 2992. van der Putte SC, van Gorp LH (1994).Adenocarcinoma of the mammary-likeglands of the vulva: a concept unifyingsweat gland carcinoma of the vulva, carci-noma of supernumerary mammary glandsand extramammary Paget's disease. JCutan Pathol 21: 157-163. 2993. van Diest PJ, Baak JPA (1991). Themorphometric prognostic index is thestrongest prognosticator in pre-menopausal lymph node-negative andlymph node-positive breast cancerpatients. Hum Pathol 22: 326-330. 2994. Van Dorpe J, De Pauw A, Moerman P(1998). Adenoid cystic carcinoma arising inan adenomyoepithelioma of the breast.Virchows Arch 432: 119-122. 2995. Van Hoeven KH, Drudis T, Cranor ML,Erlandson RA, Rosen PP (1993). Low-gradeadenosquamous carcinoma of the breast.A clinocopathologic study of 32 cases withultrastructural analysis. Am J Surg Pathol17: 248-258. 2996. van Ingen G, Schoemaker J, Baak JP(1991). A testosterone-producing tumour inthe mesovarium. Pathol Res Pract 187: 362-370. 2997. Vanderstichele S, Elhage A, Verbert-Scherrer A, Robert Y, Querleu D, Crepin G(1996). [Granulosa cell tumors: a caselocated in the broad ligament of the uteruswith normal ovaries]. J Gynecol ObstetBiol Reprod (Paris) 25: 47-52. 2998. Vang R, Kempson RL (2002).Perivascular epithelioid cell tumor('PEComa') of the uterus: a subset of HMB-45-positive epithelioid mesenchymal neo-plasms with an uncertain relationship topure smooth muscle tumors. Am J SurgPathol 26: 1-13. 2999. Vang R, Medeiros LJ, Fuller GN,Sarris AH, Deavers M (2001). Non-Hodgkin's lymphoma involving the gyneco-logic tract: a review of 88 cases. Adv AnatPathol 8: 200-217. 3000. Vang R, Medeiros LJ, Ha CS, DeaversM (2000). Non-Hodgkin's lymphomasinvolving the uterus: a clinicopathologicanalysis of 26 cases. Mod Pathol 13: 19-28.

420 References
3001. Vang R, Medeiros LJ, Silva EG,Gershenson DM, Deavers M (2000). Non-Hodgkin's lymphoma involving the vagina:a clinicopathologic analysis of 14 patients.Am J Surg Pathol 24: 719-725. 3002. Vang R, Taubenberger JK, MannionCM, Bijwaard K, Malpica A, Ordonez NG,Tavassoli FA, Silver SA (2000). Primary vul-var and vaginal extraosseous Ewing's sar -coma/peripheral neuroectodermal tumor:diagnostic confirmation with CD99immunostaining and reverse transcrip-tase-polymerase chain reaction. Int JGynecol Pathol 19: 103-109. 3003. Vang R, Whitaker BP, Farhood AI,Silva EG, Ro JY, Deavers MT (2001).Immunohistochemical analysis of clearcell carcinoma of the gynecologic tract.Int J Gynecol Pathol 20: 252-259. 3004. Vanni R, Faa G, Dettori T, Melis GB,Dumanski JP, O'Brien KP (2000). A case ofdermatofibrosarcoma protuberans of thevulva with a COL1A1/PDGFB fusion identi-cal to a case of giant cell fibroblastoma.Virchows Arch 437: 95-100. 3005. Vardi JR, Tovell HM (1980).Leiomyosarcoma of the uterus: clinico-pathologic study. Obstet Gynecol 56: 428-434. 3006. Varga Z, Kolb SA, Flury R, Burkhard R,Caduff R (2000). Sebaceous carcinoma ofthe breast. Pathol Int 50: 63-66. 3007. Vasen HF (2000). Clinical diagnosisand management of hereditary colorectalcancer syndromes. J Clin Oncol 18: 81S-92S. 3008. Vasen HF, Mecklin JP, Khan PM,Lynch HT (1991). The InternationalCollaborative Group on Hereditary Non-Polyposis Colorectal Cancer (ICG-HNPCC).Dis Colon Rectum 34: 424-425. 3009. Vasen HF, Stormorken A, Menko FH,Nagengast FM, Kleibeuker JH, Griffioen G,Taal BG, Moller P, Wijnen JT (2001). MSH2mutation carriers are at higher risk of can -cer than MLH1 mutation carriers: a studyof hereditary nonpolyposis colorectal can-cer families. J Clin Oncol 19: 4074-4080. 3010. Vasen HF, Watson P, Mecklin JP,Lynch HT (1999). New clinical criteria forhereditary nonpolyposis colorectal cancer(HNPCC, Lynch syndrome) proposed by theInternational Collaborative group onHNPCC. Gastroenterology 116: 1453-1456. 3011. Vasen HF, Wijnen JT, Menko FH,Kleibeuker JH, Taal BG, Griffioen G,Nagengast FM, Meijers-Heijboer EH,Bertario L, Varesco L, Bisgaard ML, MohrJ, Fodde R, Khan PM (1996). Cancer risk infamilies with hereditary nonpolyposis col-orectal cancer diagnosed by mutationanalysis. Gastroenterology 110: 1020-1027. 3012. Vaughn JP, Cirisano FD, Huper G,Berchuck A, Futreal PA, Marks JR, IglehartJD (1996). Cell cycle control of BRCA2.Cancer Res 56: 4590-4594. 3013. Vega de la G. (1976). Signet ring cellcarcinoma of the uterine cervix. Patologia14: 193-196. 3014. Vegh GL, Fulop V, Liu Y, Ng SW,Tuncer ZS, Genest DR, Paldi-Haris P, FoldiJ, Mok SC, Berkowitz RS (1999).Differential gene expression patternbetween normal human trophoblast andchoriocarcinoma cell lines: downregula-tion of heat shock protein-27 in choriocar-cinoma in vitro and in vivo. Gynecol Oncol75: 391-396.
3015. Velasco-Oses A, Alonso-Alvaro A,Blanco-Pozo A, Nogales FF Jr. (1988).Ollier's disease associated with ovarianjuvenile granulosa cell tumor. Cancer 62:222-225. 3016. Veliath AJ, Hannah P, Ratnakar C,Jayanthi K, Aurora AL (1978). Primaryliposarcoma of the cervix: a case report.Int J Gynaecol Obstet 16: 75-79. 3017. Venable JG, Schwartz AM,Silverberg SG (1990). Infiltrating cribriformcarcinoma of the breast: a distinctive clin-icopathologic entity. Hum Pathol 21: 333-338. 3018. Venkitaraman AR (2002). Cancer sus-ceptibility and the functions of BRCA1 andBRCA2. Cell 108: 171-182. 3019. Venkitaraman AR (2003). A growingnetwork of cancer-susceptibility genes. NEngl J Med 348: 1917-1919. 3020. Vergier B, Trojani M, De Mascarel I,Coindre JM, Le Treut A (1991). Metastasesto the breast: differential diagnosis fromprimary breast carcinoma. J Surg Oncol48: 112-116. 3021. Verhest A, Nedoszytko B, Noel JC,Dangou JM, Simon P, Limon J (1992).Translocation (6;16) in a case of granulosacell tumor of the ovary. Cancer GenetCytogenet 60: 41-44. 3022. Verhoog LC, Brekelmans CT,Seynaeve C, van den Bosch LM, DahmenG, van Geel AN, Tilanus-Linthorst MM,Bartels CC, Wagner A, van den OuwelandA, Devilee P, Meijers-Heijboer EJ, Klijn JG(1998). Survival and tumour characteristicsof breast-cancer patients with germlinemutations of BRCA1. Lancet 351: 316-321. 3023. Verhoog LC, van den Ouweland AM,Berns E, Veghel-Plandsoen MM, vanStaveren IL, Wagner A, Bartels CC,Tilanus-Linthorst MM, Devilee P,Seynaeve C, Halley DJ, Niermeijer MF,Klijn JG, Meijers-Heijboer H (2001). Largeregional differences in the frequency ofdistinct BRCA1/BRCA2 mutations in 517Dutch breast and/or ovarian cancer fami-lies. Eur J Cancer 37: 2082-2090. 3024. Veridiano NP, Gal D, Delke I, Rosen Y,Tancer ML (1980). Gestational choriocarci-noma of the ovary. Gynecol Oncol 10: 235-240. 3025. Viacava P, Naccarato AG, Nardini V,Bevilacqua G (1995). Breast carcinomawith osteoclast-like giant cells: immuno-histochemical and ultrastructural study ofa case and review of the literature. Tumori81: 135-141. 3026. Vicandi B., Jimenez-Hefferman J.A.,Lopez-Ferrer P., Ortega L., Viguer J.M.(1998). Nodular pseudoangiomatous stro-mal hyperplasia of the breast. Cytologicfeatures. Acta Cytol 42: 335-341.3027. Vivian JB, Tan EG, Frayne JR, WatersED (1993). Bilateral liposarcoma of thebreast. Aust N Z J Surg 63: 658-659. 3028. Vizcaino AP, Moreno V, Bosch FX,Munoz N, Barros-Dios XM, Parkin DM(1998). International trends in the inci-dence of cervical cancer: I. Adeno-carcinoma and adenosquamous cell carci-nomas. Int J Cancer 75: 536-545. 3029. Vizcaino I, Torregrossa AHV, MoroteV, Crenades A, Torres V, Olmos S, Molins C(2001). Metastasis to the breast from extra-mammary malignancies: a report of fourcases and a review of literature. E u rRadiol 11: 802-806.
3030. Vleminckx K, Vakaet L Jr., Mareel M,Fiers W, van Roy F (1991). Genetic manipu-lation of E-cadherin expression by epithe-lial tumor cells reveals an invasion sup-pressor role. Cell 66: 107-119. 3031. Voet RL, Lifshitz S (1982). Primaryclear cell adenocarcinoma of the fallopiantube: light microscopic and ultrastructuralfindings. Int J Gynecol Pathol 1: 292-298. 3032. Vortmeyer AO, Devouassoux-Shisheboran M, Li G, Mohr V, Tavassoli F,Zhuang Z (1999). Microdissection-basedanalysis of mature ovarian teratoma. Am JPathol 154: 987-991. 3033. Vos A, Oosterhuis JW, de Jong B,Castedo SM, Hollema H, Buist J, AaldersJG (1990). Karyotyping and DNA flowcytometry of metastatic ovarian yolk sactumor. Cancer Genet Cytogenet 44: 223-228. 3034. Vos CB, Cleton-Jansen AM, Berx G,de Leeuw WJ, ter Haar NT, van Roy F,Cornelisse CJ, Peterse JL, Van de VijverMJ (1997). E-cadherin inactivation in lobu-lar carcinoma in situ of the breast: an earlyevent in tumorigenesis. Br J Cancer 76:1131-1133. 3035. Vos CB, ter Haar NT, Peterse JL,Cornelisse CJ, Van de Vijver MJ (1999).Cyclin D1 gene amplification and overex-pression are present in ductal carcinomain situ of the breast. J Pathol 187: 279-284. 3036. Vos CB, ter Haar NT, Rosenberg C,Peterse JL, Cleton-Jansen AM, CornelisseCJ, Van de Vijver MJ (1999). Genetic alter-ations on chromosome 16 and 17 areimportant features of ductal carcinoma insitu of the breast and are associated withhistologic type. Br J Cancer 81: 1410-1418. 3037. Vuitch MF, Rosen PP, Erlandson RA(1986). Pseudoangiomatous hyperplasia ofmammary stroma. Hum Pathol 17: 185-191. 3038. Wadhwa J, Dawar R, Kumar L (1999).Ovarian carcinoma metastatic to thebreast. Clin Oncol (R Coll Radiol ) 11: 419-421. 3039. Wagner A, Hendriks Y, Meijers-Heijboer EJ, de Leeuw WJ, Morreau H,Hofstra R, Tops C, Bik E, Brocker-VriendsAH, van der Meer C, Lindhout D, Vasen HF,Breuning MH, Cornelisse CJ, van KrimpenC, Niermeijer MF, Zwinderman AH, WijnenJ, Fodde R (2001). Atypical HNPCC owingto MSH6 germline mutations: analysis of alarge Dutch pedigree. J Med Genet 38: 318-322. 3040. Wagner I, Bettendorf U (1980).Extraovarian Brenner tumor. Case reportand review. Arch Gynecol 229: 191-196. 3041. Waha A, Sturne C, Kessler A, Koch A,Kreyer E, Fimmers R, Wiestler OD, vonDeimling A, Krebs D, Schmutzler RK (1998).Expression of the ATM gene is significant -ly reduced in sporadic breast carcinomas.Int J Cancer 78: 306-309. 3042. Wahner-Roedler DL, Sebo TJ,Gisvold JJ (2001). Hamartomas of thebreast: clinical, radiologic, and pathologicmanifestations. Breast J 7: 101-105. 3043. Waite KA, Eng C (2002). ProteanPTEN: form and function. Am J Hum Genet70: 829-844. 3044. Walboomers JM, Jacobs MV, ManosMM, Bosch FX, Kummer JA, Shah KV,Snijders PJ, Peto J, Meijer CJ, Munoz N(1999). Human papillomavirus is a neces-sary cause of invasive cervical cancerworldwide. J Pathol 189: 12-19.
3045. Waldman FM, Devries S, Chew KL,Moore DH, Kerlikowske K, Ljung BM(2000). Chromosomal alterations in ductalcarcinomas in situ and their in situ recur-rences. J Natl Cancer Inst 92: 313-320. 3046. Waldman FM, Hwang ES, Etzell J,Eng C, Devries S, Bennington J, Thor A(2001). Genomic alterations in tubularbreast carcinomas. Hum Pathol 32: 222-226. 3047. Walford N, ten Velden J (1989).Histiocytoid breast carcinoma: an apoc-rine variant of lobular carcinoma.Histopathology 14: 515-522. 3048. Walker RA, Jones JL, Chappell S,Walsh T, Shaw JA (1997). Molecularpathology of breast cancer and its applica-tion to clinical management. C a n c e rMetastasis Rev 16: 5-27. 3049. Walsh MM, Bleiweiss IJ (2001).Invasive micropapillary carcinoma of thebreast: eighty cases of an underrecog-nized entity. Hum Pathol 32: 583-589. 3050. Walt H, Hornung R, Fink D, Dobler-Girdziunaite D, Stallmach T, Spycher MA,Maly F, Haller U, Burki N (2001).Hypercalcemic-type of small cell carcino-ma of the ovary: characterization of a newtumor line. Anticancer Res 21: 3253-3259. 3051. Walter A (1982). Benign teratoma ofthe Fallopian tube. Aust N Z J ObstetGynaecol 22: 245-247. 3052. Wang H, Douglas W, Lia M,Edelmann W, Kucherlapati R, PodsypaninaK, Parsons R, Ellenson LH (2002). DNA mis-match repair deficiency acceleratesendometrial tumorigenesis in Pten het-erozygous mice. Am J Pathol 160: 1481-1486. 3053. Wang WW, Spurdle AB, KolachanaP, Bove B, Modan B, Ebbers SM, SuthersG, Tucker MA, Kaufman DJ, Doody MM,Tarone RE, Daly M, Levavi H, Pierce H,Chetrit A, Yechezkel GH, Chenevix-TrenchG, Offit K, Godwin AK, Struewing JP (2001).A single nucleotide polymorphism in the 5'untranslated region of RAD51 and risk ofcancer among BRCA1/2 mutation carriers.Cancer Epidemiol Biomarkers Prev 10: 955-960. 3054. Wang Y, Cortez D, Yazdi P, Neff N,Elledge SJ, Qin J (2000). BASC, a supercomplex of BRCA1-associated proteinsinvolved in the recognition and repair ofaberrant DNA structures. Genes Dev 14:927-939. 3055. Ward BA, McKhann CF, RavikumarTS (1992). Ten-year follow-up of breastcarcinoma in situ in Connecticut. A r c hSurg 127: 1392-1395. 3056. Ward BE, Cooper PH, Subramony C(1989). Syringomatous tumor of the nipple.Am J Clin Pathol 92: 692-696. 3057. Ward BE, Saleh AM, Williams JV, ZitzJC, Crum CP (1992). Papillary immaturemetaplasia of the cervix: a distinct subsetof exophytic cervical condyloma associat -ed with HPV-6/11 nucleic acids. M o dPathol 5: 391-395. 3058. Ward RM, Evans HL (1986).Cystosarcoma phyllodes. A clinicopatho-logic study of 26 cases. Cancer 58: 2282-2289. 3059. Wargotz ES, Deos PH, Norris HJ(1989). Metaplastic carcinomas of thebreast. II. Spindle cell carcinoma. HumPathol 20: 732-740. 3060. Wargotz ES, Norris HJ (1989).Metaplastic carcinomas of the breast. I.Matrix-producing carcinoma. Hum Pathol20: 628-635.

421References
3061. Wargotz ES, Norris HJ (1990).Metaplastic carcinomas of the breast. IV.Squamous cell carcinoma of ductal origin.Cancer 65: 272-276. 3062. Wargotz ES, Norris HJ (1990).Metaplastic carcinomas of the breast: V.Metaplastic carcinoma with osteoclasticgiant cells. Hum Pathol 21: 1142-1150. 3063. Wargotz ES, Norris HJ, Austin RM,Enzinger FM (1987). Fibromatosis of thebreast. A clinical and pathological study of28 cases. Am J Surg Pathol 11: 38-45. 3064. Wargotz ES, Silverberg SG (1988).Medullary carcinoma of the breast: a clini-copathologic study with appraisal of cur-rent diagnostic criteria. Hum Pathol 19:1340-1346. 3065. Warner E, Foulkes W, Goodwin P,Meschino W, Blondal J, Paterson C,Ozcelik H, Goss P, Allingham-Hawkins D,Hamel N, Di Prospero L, Contiga V, SerruyaC, Klein M, Moslehi R, Honeyford J, LiedeA, Glendon G, Brunet JS, Narod S (1999).Prevalence and penetrance of BRCA1 andBRCA2 gene mutations in unselectedAshkenazi Jewish women with breast can-cer. J Natl Cancer Inst 91: 1241-1247. 3066. Warner NE (1969). Lobular carcinomaof the breast. Cancer 23: 840-846. 3067. Watanabe Y, Nakajima H, Nozaki K,Ueda H, Obata K, Hoshiai H, Noda K (2001).Clinicopathologic and immunohistochemi-cal features and microsatellite status ofendometrial cancer of the uterine isthmus.Int J Gynecol Pathol 20: 368-373. 3068. Waterhouse J, Muir CS, Correa P,Powell J (1976). Cancer Incidence in FiveContinents (IARC Scientific Publicationsn°15). IARC: Lyon.3069. Watkin W, Silva EG, Gershenson DM(1992). Mucinous carcinoma of the ovary.Pathologic prognostic factors. Cancer 69:208-212. 3070. Watson P, Lin KM, Rodriguez-BigasMA, Smyrk T, Lemon S, Shashidharan M,Franklin B, Karr B, Thorson A, Lynch HT(1998). Colorectal carcinoma survivalamong hereditary nonpolyposis colorectalcarcinoma family members. Cancer 8 3 :259-266. 3071. Watson P, Vasen HF, Mecklin JP,Jarvinen H, Lynch HT (1994). The risk ofendometrial cancer in hereditary nonpoly-posis colorectal cancer. Am J Med 96: 516-520. 3072. Watt AC, Haggar AM, Krasicky GA(1984). Extraosseous osteogenic sarcomaof the breast: mammographic and patho-logic findings. Radiology 150: 34. 3073. Waxman M (1979). Pure and mixedBrenner tumors of the ovary: clinicopatho-logic and histogenetic observations.Cancer 43: 1830-1839. 3074. Waxman M, Vuletin JC, Urcuyo R,Belling CG (1979). Ovarian low-grade stro-mal sarcoma with thecomatous features: acritical reappraisal of the so-called "malig-nant thecoma". Cancer 44: 2206-2217. 3075. Way S (1948). Primary carcinoma ofthe vagina. J Obstet Br Emp 55: 739. 3076. Webb JC, Key CR, Qualls CR, SmithHO (2001). Population-based study ofmicroinvasive adenocarcinoma of theuterine cervix. Obstet Gynecol 97: 701-706. 3077. Webb LA, Young JR (1996). Casereport: haemangioma of the breast--appearances on mammography and ultra-sound. Clin Radiol 51: 523-524. 3078. Webb MJ, Symmonds RE, WeilandLH (1974). Malignant fibrous histiocytomaof the vagina. Am J Obstet Gynecol 119:190-192.
3079. Weber AM, Hewett WF, GajewskiWH, Curry SL (1993). Malignant mixed mul-lerian tumors of the fallopian tube.Gynecol Oncol 50: 239-243. 3080. Wei LH, Huang CY, Cheng SP, ChenCA, Hsieh CY (2001). Carcinosarcoma ofovary associated with previous radiothera-py. Int J Gynecol Cancer 11: 81-84. 3081. Weidner N (1990). Benign breastlesions that mimic malignant tumors:analysis of five distinct lesions. S e m i nDiagn Pathol 7: 90-101. 3082. Weidner N, Semple JP (1992).Pleomorphic variant of invasive lobularcarcinoma of the breast. Hum Pathol 23:1167-1171. 3083. Weigand RA, Isenberg WM, Russo J,Brennan MJ, Rich MA (1982). Blood vesselinvasion and axillary lymph node involve-ment as prognostic indicators for humanbreast cancer. Cancer 50: 962-969. 3084. Weinberg E, Hoisington S, EastmanAY, Rice DK, Malfetano J, Ross JS (1993).Uterine cervical lymphoepithelial-like car-cinoma. Absence of Epstein-Barr virusgenomes. Am J Clin Pathol 99: 195-199. 3085. Weir MM, Bell DA, Young RH (1997).Transitional cell metaplasia of the uterinecervix and vagina: an underrecognizedlesion that may be confused with high-grade dysplasia. A report of 59 cases. AmJ Surg Pathol 21: 510-517. 3086. Weiss SW (1994). Histological Typingof Soft Tissue Tumours. 2nd ed. Springer:Berlin Heidelberg, New York.3087. Weiss SW, Tavassoli FA (1988).Multicystic mesothelioma. An analysis ofpathologic findings and biologic behaviorin 37 cases. Am J Surg Pathol 12: 737-746. 3088. Weissberg JB, Huang DD, Swift M(1998). Radiosensitivity of normal tissues inataxia-telangiectasia heterozygotes . Int JRadiat Oncol Biol Phys 42: 1133-1136. 3089. Weitmann HD, Knocke TH, Kucera H,Potter R (2001). Radiation therapy in thetreatment of endometrial stromal sarcoma.Int J Radiat Oncol Biol Phys 49: 739-748. 3090. Weitzner S, Nascimento AG, ScanlonLJ (1979). Intramammary granular cellmyoblastoma. Am Surg 45: 34-37. 3091. Wellings SR, Jensen HM, MarcumRG (1975). An atlas of subgross pathologyof the human breast with special referenceto possible precancerous lesions. J NatlCancer Inst 55: 231-273. 3092. Wells CA, Ferguson DJ (1988).Ultrastructural and immunocytochemicalstudy of a case of invasive cribriformbreast carcinoma. J Clin Pathol 41: 17-20. 3093. Wells CA, McGregor IL, MakunuraCN, Yeomans P, Davies JD (1995).Apocrine adenosis: a precursor of aggres -sive breast cancer? J Clin Pathol 48: 737-742. 3094. Wells CA, Nicoll S, Ferguson DJ(1986). Adenoid cystic carcinoma of thebreast: a case with axillary lymph nodemetastasis. Histopathology 10: 415-424. 3095. Wen WH, Reles A, Runnebaum IB,Sullivan-Halley J, Bernstein L, Jones LA,Felix JC, Kreienberg R, el Naggar A, PressMF (1999). p53 mutations and expression inovarian cancers: correlation with overallsurvival. Int J Gynecol Pathol 18: 29-41. 3096. Weng L, Brown J, Eng C (2001). PTENinduces apoptosis and cell cycle arrestthrough phosphoinositol-3-kinase/Akt-dependent and -independent pathways.Hum Mol Genet 10: 237-242.
3097. Weng LP, Brown JL, Baker KM,Ostrowski MC, Eng C (2002). PTEN blocksinsulin-mediated ETS-2 phosphorylationthrough MAP kinase, independently of thephosphoinositide 3-kinase pathway. HumMol Genet 11: 1687-1696. 3098. Weng LP, Smith WM, Brown JL, EngC (2001). PTEN inhibits insulin-stimulatedMEK/MAPK activation and cell growth byblocking IRS-1 phosphorylation and IRS-1/Grb-2/Sos complex formation in a breastcancer model. Hum Mol Genet 10: 605-616. 3099. Werling RW, Hwang H, Yaziji H, GownAM (2003). Immunohistochemical distinc-tion of invasive from noninvasive breastlesions: a comparative study of p63 versuscalponin and smooth muscle myosin heavychain. Am J Surg Pathol 27: 82-90. 3100. Werner M, Mattis A, Aubele M,Cummings M, Zitzelsberger H, Hutzler P,Hofler H (1999). 20q13.2 amplification inintraductal hyperplasia adjacent to in situand invasive ductal carcinoma of thebreast. Virchows Arch 435: 469-472. 3101. Werness BA, Dicioccio RA (2002).Transitional cell ovarian carcinoma in aBRCA1 mutation carrier. Obstet Gynecol100: 385. 3102. Werness BA, Ramus SJ, WhittemoreAS, Garlinghouse-Jones K, Oakley-GirvanI, Dicioccio RA, Tsukada Y, Ponder BA,Piver MS (2000). Histopathology of familialovarian tumors in women from familieswith and without germline BRCA1 muta-tions. Hum Pathol 31: 1420-1424. 3103. Werness BA, Ramus SJ, WhittemoreAS, Garlinghouse-Jones K, Oakley-GirvanI, Dicioccio RA, Tsukada Y, Ponder BA,Piver MS (2000). Primary ovarian dysger-minoma in a patient with a germline BRCA1mutation. Int J Gynecol Pathol 19: 390-394. 3104. West M, Blanchette C, Dressman H,Huang E, Ishida S, Spang R, Zuzan H, OlsonJA Jr., Marks JR, Nevins JR (2001).Predicting the clinical status of humanbreast cancer by using gene expressionprofiles. Proc Natl Acad Sci USA 98: 11462-11467. 3 1 0 4 a . Westenend PJ, Liem SJ (2001).Adenosis tumor of the breast containingductal carcinoma in situ, a pitfall in coreneedle biopsy. Breast J 7: 200-201. 3105. Wheeler DT, Bell KA, Kurman RJ,Sherman ME (2000). Minimal uterineserous carcinoma: diagnosis and clinico-pathologic correlation. Am J Surg Pathol24: 797-806. 3106. Wheeler JE, Enterline HT (1976).Lobular carcinoma of the breast in situ andinfiltrating. Pathol Annu 11: 161-188. 3107. Wheeler JE, Enterline HT, RosemanJM, Tomasulo JP, McIlvaine CH, Fitts WTJr., Kirshenbaum J (1974). Lobular carcino-ma in situ of the breast. Long-term fol-lowup. Cancer 34: 554-563. 3108. Wheelock JB, Goplerud DR, Dunn LJ,Oates JF, III (1984). Primary carcinoma ofthe Bartholin gland: a report of ten cases.Obstet Gynecol 63: 820-824. 3109. Wheelock JB, Krebs HB, SchneiderV, Goplerud DR (1985). Uterine sarcoma:analysis of prognostic variables in 71cases. Am J Obstet Gynecol 151: 1016-1022. 3110. Whiteman DC, Murphy MF,Verkasalo PK, Page WF, Floderus B,Skytthe A, Holm NV (2000). Breast cancerrisk in male twins: joint analyses of fourtwin cohorts in Denmark, Finland, Swedenand the United States. Br J Cancer 83:1231-1233.
3111. WHO Technical Report Series (1983).WHO Scientific Group: Gestional tro-phoblastic diseases. WHO: 3112. Wick MR, Goellner JR, Wolfe JT, III,Su WP (1985). Vulvar sweat gland carcino-mas. Arch Pathol Lab Med 109: 43-47. 3113. Wick MR, Lillemoe TJ, Copland GT,Swanson PE, Manivel JC, Kiang DT (1989).Gross cystic disease fluid protein-15 as amarker for breast cancer: immunohisto-chemical analysis of 690 human neo-plasms and comparison with alpha-lactal-bumin. Hum Pathol 20: 281-287. 3114. Wijnen J, de Leeuw W, Vasen H, vander Klift H, Moller P, Stormorken A,Meijers-Heijboer H, Lindhout D, Menko F,Vossen S, Moslein G, Tops C, Brocker-Vriends A, Wu Y, Hofstra R, Sijmons R,Cornelisse C, Morreau H, Fodde R (1999).Familial endometrial cancer in female car-riers of MSH6 germline mutations. NatGenet 23: 142-144. 3115. Wijnen J, Khan PM, Vasen H, MenkoF, van der Klift H, van den Broek M,Leeuwen-Cornelisse I, Nagengast F,Meijers-Heijboer EJ, Lindhout D, GriffioenG, Cats A, Kleibeuker J, Varesco L, BertarioL, Bisgaard ML, Mohr J, Kolodner R, FoddeR (1996). Majority of hMLH1 mutationsresponsible for hereditary nonpolyposiscolorectal cancer cluster at the exonicregion 15-16. Am J Hum Genet 58: 300-307. 3116. Wijnen J, van der Klift H, Vasen H,Khan PM, Menko F, Tops C, Meijers HH,Lindhout D, Moller P, Fodde R (1998). MSH2genomic deletions are a frequent cause ofHNPCC. Nat Genet 20: 326-328. 3117. Wijnen JT, Vasen HF, Khan PM,Zwinderman AH, van der Klift H, Mulder A,Tops C, Moller P, Fodde R (1998). Clinicalfindings with implications for genetic test-ing in families with clustering of colorectalcancer. N Engl J Med 339: 511-518. 3118. Wijnmaalen A, van Ooijen B, van GeelBN, Henzen-Logmans SC, Treurniet-Donker AD (1993). Angiosarcoma of thebreast following lumpectomy, axillarylymph node dissection, and radiotherapyfor primary breast cancer: three casereports and a review of the literature. Int JRadiat Oncol Biol Phys 26: 135-139. 3119. Wilkinson EJ (2000). Protocol for theexamination of specimens from patientswith carcinomas and malignantmelanomas of the vulva: a basis for check-lists. Cancer Committee of the AmericanCollege of Pathologists. Arch Pathol LabMed 124: 51-56. 3120. Wilkinson EJ (2002). Premalignantand Malignant Tumours of the vulva. In:Blaustein's Pathology of the FemaleGenital Tract. 5th ed. Springer-Verlag:New York.3121. Wilkinson EJ, Brown H (2002). VulvarPaget disease of urothelial origin: a reportof three cases and proposed classificationof vulvar Paget disease. Hum Pathol 33:549-554. 3122. Wilkinson EJ, Croker BP, Friedrich EGJr., Franzini DA (1988). Two distinct patho-logic types of giant cell tumor of the vulva.A report of two cases. J Reprod Med 33:519-522. 3123. Wilkinson EJ, Friedrich EG Jr., Fu YS(1981). Multicentric nature of vulvar carci-noma in situ. Obstet Gynecol 58: 69-74. 3124. Wilkinson EJ, Stone IK (1994). Atlasof Vulvar Disease. Williams and WIlkins:Baltimore, Maryland.

422 References
3125. Willemsen W, Kruitwagen R,Bastiaans B, Hanselaar T, Rolland R (1993).Ovarian stimulation and granulosa-celltumour. Lancet 341: 986-988. 3126. Willen R, Bekassy, Carlen B, BozokyB, Cajander S (1999). Cloacogenic adeno-carcinoma of the vulva. Gynecol Oncol 74:298-301. 3127. Willett GD, Kurman RJ, Reid R,Greenberg M, Jenson AB, Lorincz AT(1989). Correlation of the histologicappearance of intraepithelial neoplasia ofthe cervix with human papillomavirustypes. Emphasis on low grade lesionsincluding so-called flat condyloma. Int JGynecol Pathol 8: 18-25. 3128. Williamson JD, Colome MI, Sahin A,Ayala AG, Medeiros LJ (2000). PagetoidBowen disease: a report of 2 cases thatexpress cytokeratin 7. Arch Pathol LabMed 124: 427-430. 3129. Willsher PC, Leach IH, Ellis IO, BellJA, Elston CW, Bourke JB, Blamey RW,Robertson JF (1997). Male breast cancer:pathological and immunohistochemicalfeatures. Anticancer Res 17: 2335-2338. 3130. Wilson CA, Ramos L, Villasenor MR,Anders KH, Press MF, Clarke K, Karlan B,Chen JJ, Scully R, Livingston D, Zuch RH,Kanter MH, Cohen S, Calzone FJ, SlamonDJ (1999). Localization of human BRCA1and its loss in high-grade, non-inheritedbreast carcinomas. Nat Genet 21: 236-240. 3131. Wilson RB, Hunter JSJ, Dockerty MB(1961). Chorioadenoma destruens. Am JObstet Gynecol 81: 546-559. 3132. Wilson TM, Ewel A, Duguid JR, EbleJN, Lescoe MK, Fishel R, Kelley MR (1995).Differential cellular expression of thehuman MSH2 repair enzyme in small andlarge intestine. Cancer Res 55: 5146-5150. 3133. Winchester DJ, Chang HR, GravesTA, Menck HR, Bland KI, Winchester DP(1998). A comparative analysis of lobularand ductal carcinoma of the breast: pres-entation, treatment, and outcomes. J AmColl Surg 186: 416-422. 3134. Wingren S, van den Heuvel A, GentileM, Olsen K, Hatschek T, Soderkvist P(1997). Frequent allelic losses on chromo-some 13q in human male breast carcino-mas. Eur J Cancer 33: 2393-2396. 3135. Winkler B, Alvarez S, Richart RM,Crum CP (1984). Pitfalls in the diagnosis ofendometrial neoplasia. Obstet Gynecol 64:185-194. 3136. Wiseman C, Liao KT (1972). Primarylymphoma of the breast. Cancer 29: 1705-1712. 3137. Wohlfahrt J, Melbye M (2001). Age atany birth is associated with breast cancerrisk. Epidemiology 12: 68-73. 3138. Wolber RA, Talerman A, WilkinsonEJ, Clement PB (1991). Vulvar granular celltumors with pseudocarcinomatous hyper-plasia: a comparative analysis with well-differentiated squamous carcinoma. Int JGynecol Pathol 10: 59-66. 3139. Wolfson AH, Wolfson DJ, Sittler SY,Breton L, Markoe AM, Schwade JG,Houdek PV, Averette HE, Sevin BU,Penalver M, Duncan RC, Ganjei P. (1994). Amultivariate analysis of clinicopathologicfactors for predicting outcome in uterinesarcomas. Gynecol Oncol 52: 56-62.3140. Wong JH, Kopald KH, Morton DL(1990). The impact of microinvasion on axil-lary node metastases and survival inpatients with intraductal breast cancer.Arch Surg 125: 1298-1301.
3141. Wong SY, Kernohan NM, Walker F(1990). Breast cancers with extremely highoestrogen receptor protein status.Histopathology 16: 125-132. 3142. Woodard BH, Brinkhous AD,McCarty KS, Sr., McCarty KS Jr. (1980).Adenosquamous differentiation in mam-mary carcinoma: an ultrastructural andsteroid receptor study. Arch Pathol LabMed 104: 130-133. 3143. Woodman CB, Collins S, Winter H,Bailey A, Ellis J, Prior P, Yates M, RollasonTP, Young LS (2001). Natural history of cer-vical human papillomavirus infection inyoung women: a longitudinal cohort study.Lancet 357: 1831-1836. 3144. Woodruff JD, Dietrich D, Genadry R,Parmley TH (1981). Proliferative and malig -nant Brenner tumors. Review of 47 cases.Am J Obstet Gynecol 141: 118-125. 3 1 4 5 . Woodruff JD, Julian CG (1969).Multiple malignancy in the upper genitalcanal. Am J Obstet Gynecol 103: 810-822. 3146. Woodruff JD, Rauh JT, Markley RL(1966). Ovarian struma. Obstet Gynecol 27:194-201. 3 1 4 7 . Woods DB, Vousden KH (2001).Regulation of p53 function. Exp Cell Res264: 56-66. 3148. Woods ER, Helvie MA, Ikeda DM,Mandell SH, Chapel KL, Adler DD (1992).Solitary breast papilloma: comparison ofmammographic, galactographic, andpathologic findings. AJR Am J Roentgenol159: 487-491. 3149. Woodward AH, Ivins JC, Soule EH(1972). Lymphangiosarcoma arising inchronic lymphedematous extremities.Cancer 30: 562-572. 3150. Woolas R, Smith J, Paterson JM,Sharp F (1997). Fallopian tube carcinoma:an under-recognized primary neoplasm.Int J Gynecol Cancer 7: 284-288. 3151. Woolcott RJ, Henry RJ, Houghton CR(1988). Malignant melanoma of the vulva.Australian experience. J Reprod Med 33:699-702. 3152. Wooster R, Mangion J, Eeles R, SmithS, Dowsett M, Averill D, Barrett-Lee P,Easton DF, Ponder BA, Stratton MR (1992).A germline mutation in the androgenreceptor gene in two brothers with breastcancer and Reifenstein syndrome. N a tGenet 2: 132-134. 3153. World Cancer ResearchFund.American Institute for CancerResearch (1997). Food, Nutrition and thePrevention of Cancer: a GlobalPerspective. American Institute for CancerResearch: Washington DC.3 1 5 4 . World Health Organization (1981).International Histological Classification ofTumours: Histologic Types of BreastTumours. Geneva.3155. World Health Organization (2000).World Health Organisation 1997-1999World Health Statistics Annual.http://www who int/whosis. 3156. Worsham MJ, Van Dyke DL,Grenman SE, Grenman R, Hopkins MP,Roberts JA, Gasser KM, Schwartz DR,Carey TE (1991). Consistent chromosomeabnormalities in squamous cell carcinomaof the vulva. Genes Chromosomes Cancer3: 420-432. 3157. Wotherspoon AC, Finn TM, IsaacsonPG (1995). Trisomy 3 in low-grade B-celllymphomas of mucosa-associated lym-phoid tissue. Blood 85: 2000-2004.
3158. Wrba F, Ellinger A, Reiner G, Spona J,Holzner JH (1988). Ultrastructural andimmunohistochemical characteristics oflipid-rich carcinoma of the breast.Virchows Arch A Pathol Anat Histopathol413: 381-385. 3159. Wright CV, Shier MR (2000).Colposcopy of Adenocarcinoma in situ andAdenocarcinoma of the Cervix.Differentiation from Other CervicalLesions. Biomedical Communications:Houston.3160. Wu Y, Berends MJ, Mensink RG,Kempinga C, Sijmons RH, Der Zee AG,Hollema H, Kleibeuker JH, Buys CH,Hofstra RM (1999). Association of heredi-tary nonpolyposis colorectal cancer-relat -ed tumors displaying low microsatelliteinstability with MSH6 germline mutations.Am J Hum Genet 65: 1291-1298. 3161. Wu Y, Berends MJ, Post JG, MensinkRG, Verlind E, Van Der Sluis T, Kempinga C,Sijmons RH, van der Zee AG, Hollema H,Kleibeuker JH, Buys CH, Hofstra RM (2001).Germline mutations of EXO1 gene inpatients with hereditary nonpolyposis col-orectal cancer (HNPCC) and atypicalHNPCC forms. Gastroenterology 120: 1580-1587. 3 1 6 2 . Wu Y, Berends MJ, Sijmons RH,Mensink RG, Verlind E, Kooi KA, Van DerSluis T, Kempinga C, dDer Zee AG, HollemaH, Buys CH, Kleibeuker JH, Hofstra RM(2001). A role for MLH3 in hereditary non-polyposis colorectal cancer. Nat Genet 29:137-138. 3163. Wurdinger S, Schutz K, Fuchs D,Kaiser WA (2001). Two cases of metas-tases to the breast on MR mammography.Eur Radiol 11: 802-806. 3164. Wyatt SW, Lancaster M, Bottorff D,Ross F (2001). History of tobacco useamong Kentucky women diagnosed withinvasive cervical cancer: 1997-1998. J KyMed Assoc 99: 537-539. 3165. Wysocka B, Serkies K, Debniak J,Jassem J, Limon J (1999). Sertoli cell tumorin androgen insensitivity syndrome--acase report. Gynecol Oncol 75: 480-483. 3166. Xu B, Kim S, Kastan MB (2001).Involvement of Brca1 in S-phase and G(2)-phase checkpoints after ionizing irradia-tion. Mol Cell Biol 21: 3445-3450. 3167. Xu X, Wagner KU, Larson D, WeaverZ, Li C, Ried T, Hennighausen L, Wynshaw-Boris A, Deng CX (1999). Conditional muta -tion of Brca1 in mammary epithelial cellsresults in blunted ductal morphogenesisand tumour formation. Nat Genet 22: 37-43. 3168. Yaghsezian H, Palazzo JP, Finkel GC,Carlson JA Jr., Talerman A (1992). Primaryvaginal adenocarcinoma of the intestinaltype associated with adenosis. GynecolOncol 45: 62-65. 3169. Yakirevich E, Izhak OB, Rennert G,Kovacs ZG, Resnick MB (1999). Cytotoxicphenotype of tumor infiltrating lympho-cytes in medullary carcinoma of thebreast. Mod Pathol 12: 1050-1056. 3170. Yakirevich E, Maroun L, Cohen O,Izhak OB, Rennert G, Resnick MB (2000).Apoptosis, proliferation, and Fas (APO-1,CD95)/Fas ligand expression in medullarycarcinoma of the breast. J Pathol 192: 166-173. 3171. Yamamoto Y, Akagi A, Izumi K, Kishi Y(1995). Carcinosarcoma of the uterine bodyof mesonephric origin. Pathol Int 45: 303-309.
3172. Yamashita K, Wake N, Araki T,Ichinoe K, Makoto K (1979). Human lym-phocyte antigen expression in hydatidi-form mole: androgenesis following fertil-ization by a haploid sperm. Am J ObstetGynecol 135: 597-600. 3173. Yamauchi H, Stearns V, Hayes DF(2001). When is a tumor marker ready forprime time? A case study of c-erbB-2 as apredictive factor in breast cancer. J ClinOncol 19: 2334-2356. 3174. Yanai-Inbar I, Scully RE (1987).Relation of ovarian dermoid cysts andimmature teratomas: an analysis of 350cases of immature teratoma and 10 casesof dermoid cyst with microscopic foci ofimmature tissue. Int J Gynecol Pathol 6:203-212. 3175. Yang B, Hart WR (2000). Vulvarintraepithelial neoplasia of the simplex(differentiated) type: a clinicopathologicstudy including analysis of HPV and p53expression. Am J Surg Pathol 24: 429-441. 3176. Yang WT, Suen M, Metreweli C(1997). Sonographic features of benignpapillary neoplasms of the breast: reviewof 22 patients. J Ultrasound Med 16: 161-168. 3177. Yannacou N, Gerolymatos A, Parissi-Mathiou P, Chranioti S, Perdikis T (2000).Carcinosarcoma of the uterine cervix com-posed of an adenoid cystic carcinoma andan homologous stromal sarcoma. A casereport. Eur J Gynaecol Oncol 21: 292-294. 3178. Yarden RI, Pardo-Reoyo S, SgagiasM, Cowan KH, Brody LC (2002). BRCA1 reg-ulates the G2/M checkpoint by activatingChk1 kinase upon DNA damage. Nat Genet30: 285-289. 3 1 7 9 . Yazigi R, Sandstad J, Munoz AK(1988). Breast cancer metastasizing to theuterine cervix. Cancer 61: 2558-2560. 3180. Yaziji H, Gown AM (2001).Immunohistochemical analysis of gyneco-logic tumors. Int J Gynecol Pathol 20: 64-78. 3181. Yaziji H, Gown AM, Sneige N (2000).Detection of stromal invasion in breastcancer: the myoepithelial markers. AdvAnat Pathol 7: 100-109. 3182. Yilmaz AG, Chandler P, Hahm GK,O'Toole RV, Niemann TH (1999). Melanosisof the uterine cervix: a report of two casesand discussion of pigmented cervicallesions. Int J Gynecol Pathol 18: 73-76. 3183. Yip CH, Wong KT, Samuel D (1997).Bilateral plasma cell granuloma (inflamma-tory pseudotumour) of the breast. Aust N ZJ Surg 67: 300-302. 3184. Yokoyama Y, Sato S, Futagami M,Saito Y (2000). Solitary metastasis to theuterine cervix from the early gastric can-cer: a case report. Eur J Gynaecol Oncol21: 469-471. 3185. Yoonessi M (1979). Carcinoma of thefallopian tube. Obstet Gynecol Surv 34:257-270. 3186. Yoonessi M, Abell MR (1979).Brenner tumors of the ovary. O b s t e tGynecol 54: 90-96. 3187. Yoshino K, Enomoto T, Nakamura T,Nakashima R, Wada H, Saitoh J, Noda K,Murata Y (1998). Aberrant FHIT transcriptsin squamous cell carcinoma of the uterinecervix. Int J Cancer 76: 176-181. 3188. Yoshino K, Enomoto T, Nakamura T,Sun H, Ozaki K, Nakashima R, Wada H,Saitoh J, Watanabe Y, Noda K, Murata Y(2000). FHIT alterations in cancerous andnon-cancerous cervical epithelium. Int JCancer 85: 6-13.

423References
3189. Yoshioka T, Tanaka T (2000). Maturesolid teratoma of the fallopian tube: casereport. Eur J Obstet Gynecol Reprod Biol89: 205-206. 3190. Yoshiura K, Kanai Y, Ochiai A,Shimoyama Y, Sugimura T, Hirohashi S(1995). Silencing of the E-cadherin inva-sion-suppressor gene by CpG methylationin human carcinomas. Proc Natl Acad SciUSA 92: 7416-7419. 3191. Young JLJr, Percy CL, Asire AJ(1981). Surveillance, Epidemiology and Endresults: Incidence and mortality data:1973-1977. NCI Monogr.3192. Young RH, Clement PB (1988).Adenomyoepithelioma of the breast. Areport of three cases and review of the lit-erature. Am J Clin Pathol 89: 308-314. 3193. Young RH, Clement PB (2000).Endocervicosis involving the uterinecervix: a report of four cases of a benignprocess that may be confused with deeplyinvasive endocervical adenocarcinoma.Int J Gynecol Pathol 19: 322-328. 3194. Young RH, Clement PB, Scully RE(1988). Calcified thecomas in youngwomen. A report of four cases. Int JGynecol Pathol 7: 343-350. 3195. Young RH, Dickersin GR, Scully RE(1984). Juvenile granulosa cell tumor of theovary. A clinicopathological analysis of 125cases. Am J Surg Pathol 8: 575-596. 3196. Young RH, Dudley AG, Scully RE(1984). Granulosa cell, Sertoli-Leydig cell,and unclassified sex cord-stromal tumorsassociated with pregnancy: a clinico-pathological analysis of thirty-six cases.Gynecol Oncol 18: 181-205. 3197. Young RH, Gersell DJ, Clement PB,Scully RE (1992). Hepatocellular carcinomametastatic to the ovary: a report of threecases discovered during life with discus-sion of the differential diagnosis of hepa-toid tumors of the ovary. Hum Pathol 23:574-580. 3198. Young RH, Gersell DJ, Roth LM,Scully RE (1993). Ovarian metastases fromcervical carcinomas other than pure ade-nocarcinomas. A report of 12 cases.Cancer 71: 407-418. 3199. Young RH, Gilks CB, Scully RE (1991).Mucinous tumors of the appendix associ-ated with mucinous tumors of the ovaryand pseudomyxoma peritonei. A clinico-pathological analysis of 22 cases support-ing an origin in the appendix. Am J SurgPathol 15: 415-429. 3200. Young RH, Hart WR (1989).Metastases from carcinomas of the pan-creas simulating primary mucinous tumorsof the ovary. A report of seven cases. AmJ Surg Pathol 13: 748-756. 3201. Young RH, Kleinman GM, Scully RE(1981). Glioma of the uterus. Report of acase with comments on histogenesis. AmJ Surg Pathol 5: 695-699. 3202. Young RH, Kurman RJ, Scully RE(1988). Proliferations and tumors of inter-mediate trophoblast of the placental site.Semin Diagn Pathol 5: 223-237. 3203. Young RH, Kurman RJ, Scully RE(1990). Placental site nodules and plaques.A clinicopathologic analysis of 20 cases.Am J Surg Pathol 14: 1001-1009. 3204. Young RH, Oliva E, Scully RE (1994).Small cell carcinoma of the ovary, hyper-calcemic type. A clinicopathologicalanalysis of 150 cases. Am J Surg Pathol 18:1102-1116.
3205. Young RH, Prat J, Scully RE (1980).Epidermoid cyst of the ovary. A report ofthree cases with comments on histogene-sis. Am J Clin Pathol 73: 272-276. 3206. Young RH, Prat J, Scully RE (1982).Ovarian endometrioid carcinomas resem-bling sex cord-stromal tumors. A clinico-pathological analysis of 13 cases. Am JSurg Pathol 6: 513-522. 3207. Young RH, Prat J, Scully RE (1982).Ovarian Sertoli-Leydig cell tumors withheterologous elements. I. Gastrointestinalepithelium and carcinoid: a clinicopatho-logic analysis of thirty-six cases. Cancer50: 2448-2456. 3208. Young RH, Prat J, Scully RE (1984).Endometrioid stromal sarcomas of theovary. A clinicopathologic analysis of 23cases. Cancer 53: 1143-1155. 3209. Young RH, Scully RE (1983). OvarianSertoli-Leydig cell tumors with a retiformpattern: a problem in histopathologic diag -nosis. A report of 25 cases. Am J SurgPathol 7: 755-771. 3210. Young RH, Scully RE (1983). Ovariansex cord-stromal tumors with bizarrenuclei: a clinicopathologic analysis of 17cases. Int J Gynecol Pathol 1: 325-335. 3211. Young RH, Scully RE (1983). Ovarianstromal tumors with minor sex cord ele-ments: a report of seven cases. Int JGynecol Pathol 2: 227-234. 3212. Young RH, Scully RE (1983). Ovariantumors of probable wolffian origin. A reportof 11 cases. Am J Surg Pathol 7: 125-135. 3213. Young RH, Scully RE (1984).Endodermal sinus tumor of the vagina: areport of nine cases and review of the lit-erature. Gynecol Oncol 18: 380-392. 3214. Young RH, Scully RE (1984).Fibromatosis and massive edema of theovary, possibly related entities: a report of14 cases of fibromatosis and 11 cases ofmassive edema. Int J Gynecol Pathol 3:153-178. 3215. Young RH, Scully RE (1984). OvarianSertoli cell tumors: a report of 10 cases.IntJ Gynecol Pathol 2: 349-363. 3216. Young RH, Scully RE (1984). Well-dif-ferentiated ovarian Sertoli-Leydig celltumors: a clinicopathological analysis of 23cases. Int J Gynecol Pathol 3: 277-290. 3217. Young RH, Scully RE (1985). OvarianSertoli-Leydig cell tumors. A clinicopatho-logical analysis of 207 cases. Am J SurgPathol 9: 543-569. 3218. Young RH, Scully RE (1987). Ovariansteroid cell tumors associated withCushing's syndrome: a report of threecases. Int J Gynecol Pathol 6: 40-48. 3219. Young RH, Scully RE (1988).Mucinous ovarian tumors associated withmucinous adenocarcinomas of the cervix.A clinicopathological analysis of 16 cases.Int J Gynecol Pathol 7: 99-111. 3220. Young RH, Scully RE (1988). Urothelialand ovarian carcinomas of identical celltypes: problems in interpretation. A reportof three cases and review of the literature.Int J Gynecol Pathol 7: 197-211. 3221. Young RH, Scully RE (1990). Ovarianmetastases from carcinoma of the gall-bladder and extrahepatic bile ducts simu-lating primary tumors of the ovary. A reportof six cases. Int J Gynecol Pathol 9: 60-72. 3222. Young RH, Scully RE (1990).Sarcomas metastatic to the ovary: a reportof 21 cases. Int J Gynecol Pathol 9: 231-252.
3223. Young RH, Scully RE (1991).Malignant melanoma metastatic to theovary. A clinicopathologic analysis of 20cases. Am J Surg Pathol 15: 849-860. 3224. Young RH, Scully RE (1992). Uterinecarcinomas simulating microglandularhyperplasia. A report of six cases. Am JSurg Pathol 16: 1092-1097. 3225. Young RH, Scully RE (1993). Minimal-deviation endometrioid adenocarcinomaof the uterine cervix. A report of five casesof a distinctive neoplasm that may be mis-interpreted as benign. Am J Surg Pathol17: 660-665. 3226. Young RH, Scully RE (1994). Metastictumours of the ovary. In: B l a u s t e i n ' sPathology of the Female Genital Tract,Kurman RJ, ed., 4th ed. Springer-Verlag:New York , pp. 939-974.3227. Young RH, Scully RE, McCluskey RT(1985). A distinctive glomerular lesion com-plicating placental site trophoblastictumor: report of two cases. Hum Pathol 16:35-42. 3228. Young RH, Treger T, Scully RE (1986).Atypical polypoid adenomyoma of theuterus. A report of 27 cases. Am J ClinPathol 86: 139-145. 3 2 2 9 . Young TW, Thrasher TV (1982).Nonchromaffin paraganglioma of theuterus. A case report. Arch Pathol LabMed 106: 608-609. 3 2 3 0 . Youngs LA, Taylor HB (1967).Adenomatoid tumors of the uterus and fal -lopian tube. Am J Clin Pathol 48: 537-545. 3231. Youngson BJ, Cranor M, Rosen PP(1994). Epithelial displacement in surgicalbreast specimens following needling pro-cedures. Am J Surg Pathol 18: 896-903. 3232. Yu GH, Fishman SJ, Brooks JS (1993).Cellular angiolipoma of the breast. ModPathol 6: 497-499. 3233. Yuan CC, Wang PH, Lai CR, Yen MS,Chen CY, Juang CM (1998). Prognosis-pre -dicting system based on factors related tosurvival of cervical carcinoma. Int JGynaecol Obstet 63: 163-167. 3234. Zabernigg A, Muller-Holzner E, GascJM, Gattringer C (1997). An unusual case ofa renin-producing tumour of the fallopiantube. Eur J Cancer 33: 1709. 3235. Zafrani B, Aubriot MH, Mouret E, deCremoux P, De Rycke Y, Nicolas A, BoudouE, Vincent-Salomon A, Magdelenat H,Sastre-Garau X (2000). High sensitivity andspecificity of immunohistochemistry forthe detection of hormone receptors inbreast carcinoma: comparison with bio-chemical determination in a prospectivestudy of 793 cases. Histopathology 37: 536-545. 3236. Zahradka M, Zahradka W, Mach S(1989). [Stromal sarcoma of the vagina].Zentralbl Gynakol 111: 1450-1454. 3237. Zaidi SN, Conner MG (2001). Primaryvulvar adenocarcinoma of cloacogenicorigin. South Med J 94: 744-746. 3238. Zaino RJ, Kurman RJ, Diana KL,Morrow CP (1995). The utility of the revisedInternational Federation of Gynecologyand Obstetrics histologic grading ofendometrial adenocarcinoma using adefined nuclear grading system. AGynecologic Oncology Group study.Cancer 75: 81-86. 3239. Zaino RJ, Unger ER, Whitney C (1984).Synchronous carcinomas of the uterinecorpus and ovary. Gynecol Oncol 19: 329-335.
3240. Zaki I, Dalziel KL, Solomonsz FA,Stevens A (1996). The under-reporting ofskin disease in association with squamouscell carcinoma of the vulva. Clin ExpDermatol 21: 334-337. 3241. Zaloudek C, Hayashi GM, Ryan IP,Powell CB, Miller TR (1997). Micro-glandular adenocarcinoma of theendometrium: a form of mucinous adeno-carcinoma that may be confused withmicroglandular hyperplasia of the cervix.Int J Gynecol Pathol 16: 52-59. 3242. Zaloudek C, Norris HJ (1982).Granulosa tumors of the ovary in children:a clinical and pathologic study of 32 cases.Am J Surg Pathol 6: 503-512. 3243. Zaloudek C, Norris HJ (1984). Sertoli-Leydig tumors of the ovary. A clinicopatho-logic study of 64 intermediate and poorlydifferentiated neoplasms. Am J SurgPathol 8: 405-418. 3244. Zaloudek C, Oertel YC, Orenstein JM(1984). Adenoid cystic carcinoma of thebreast. Am J Clin Pathol 81: 297-307. 3245. Zaloudek CJ, Norris HJ (1981).Adenofibroma and adenosarcoma of theuterus: a clinicopathologic study of 35cases. Cancer 48: 354-366. 3246. Zaloudek CJ, Tavassoli FA, Norris HJ(1981). Dysgerminoma with syncytiotro-phoblastic giant cells. A histologically andclinically distinctive subtype of dysgermi-noma. Am J Surg Pathol 5: 361-367. 3247. Zamecnik M, Michal M (1998).Endometrial stromal nodule with retiformsex-cord-like differentiation. Pathol ResPract 194: 449-453. 3248. Zamecnik M, Michal M, Curik R(2000). Adenoid cystic carcinoma of theovary. Arch Pathol Lab Med 124: 1529-1531. 3249. Zanella M, Falconieri G, Lamovec J,Bittesini L (1998). Pseudoangiomatoushyperplasia of the mammary stroma: trueentity or phenotype? Pathol Res Pract 194:535-540. 3250. Zanetta G, Rota SM, Lissoni A, ChiariS, Bratina G, Mangioni C (1999).Conservative treatment followed bychemotherapy with doxorubicin and ifos-famide for cervical sarcoma botryoides inyoung females. Br J Cancer 80: 403-406. 3251. Zanetta GM, Webb MJ, Li H, KeeneyGL (2000). Hyperestrogenism: a relevantrisk factor for the development of cancerfrom endometriosis. Gynecol Oncol 79: 18-22. 3252. Zhang J, Young RH, Arseneau J,Scully RE (1982). Ovarian stromal tumorscontaining lutein or Leydig cells (luteinizedthecomas and stromal Leydig cell tumors)--a clinicopathological analysis of fiftycases. Int J Gynecol Pathol 1: 270-285. 3253. Zhao S, Kato N, Endoh Y, Jin Z, AjiokaY, Motoyama T (2000). Ovariangonadoblastoma with mixed germ celltumor in a woman with 46, XX karyotypeand successful pregnancies. Pathol Int 50:332-335. 3254. Zhao X, Wei YQ, Kariya Y,Teshigawara K, Uchida A (1995).Accumulation of gamma/delta T cells inhuman dysgerminoma and seminoma:roles in autologous tumor killing and gran-uloma formation. Immunol Invest 24: 607-618. 3255. Zheng L, Pan H, Li S, Flesken-NikitinA, Chen PL, Boyer TG, Lee WH (2000).Sequence-specific transcriptional core-pressor function for BRCA1 through anovel zinc finger protein, ZBRK1. Mol Cell6: 757-768.

424 References
3256. Zheng W, Khurana R, Farahmand S,Wang Y, Zhang ZF, Felix JC (1998). p53immunostaining as a significant adjunctdiagnostic method for uterine surface car-cinoma: precursor of uterine papillaryserous carcinoma. Am J Surg Pathol 22:1463-1473. 3257. Zheng W, Wolf S, Kramer EE, Cox KA,Hoda SA (1996). Borderline papillaryserous tumour of the fallopian tube. Am JSurg Pathol 20: 30-35. 3258. Zhong Q, Chen CF, Li S, Chen Y, WangCC, Xiao J, Chen PL, Sharp ZD, Lee WH(1999). Association of BRCA1 with thehRad50-hMre11-p95 complex and the DNAdamage response. Science 285: 747-750. 3259. Zhou H, Kuang J, Zhong L, Kuo WL,Gray JW, Sahin A, Brinkley BR, Sen S(1998). Tumour amplified kinaseSTK15/BTAK induces centrosome amplifi-cation, aneuploidy and transformation. NatGenet 20: 189-193. 3260. Zhou X, Hampel H, Thiele H, GorlinRJ, Hennekam RC, Parisi M, Winter RM,Eng C (2001). Association of germlinemutation in the PTEN tumour suppressorgene and Proteus and Proteus-like syn-dromes. Lancet 358: 210-211.
3261. Zhou XP, Kuismanen S, Nystrom-Lahti M, Peltomaki P, Eng C (2002). DistinctPTEN mutational spectra in hereditarynon-polyposis colon cancer syndrome-related endometrial carcinomas comparedto sporadic microsatellite unstable tumors.Hum Mol Genet 11: 445-450. 3262. Zhou XP, Woodford-Richens K,Lehtonen R, Kurose K, Aldred M, HampelH, Launonen V, Virta S, Pilarski R,Salovaara R, Bodmer WF, Conrad BA,Dunlop M, Hodgson SV, Iwama T, JarvinenH, Kellokumpu I, Kim JC, Leggett B, MarkieD, Mecklin JP, Neale K, Phillips R, Piris J,Rozen P, Houlston RS, Aaltonen LA,Tomlinson IP, Eng C (2001). Germline muta-tions in BMPR1A/ALK3 cause a subset ofcases of juvenile polyposis syndrome andof Cowden and Bannayan-Riley-Ruvalcabasyndromes. Am J Hum Genet 69: 704-711. 3263. Zhu WY, Leonardi C, Penneys NS(1992). Detection of human papillomavirusDNA in seborrheic keratosis by poly-merase chain reaction. J Dermatol Sci 4:166-171.
3264. Zhu XL, Hartwick W, Rohan T, KandelR (1998). Cyclin D1 gene amplification andprotein expression in benign breast dis-ease and breast carcinoma. Mod Pathol11: 1082-1088. 3265. Zhuang Z, Merino MJ, Chuaqui R,Liotta LA, Emmert-Buck MR (1995).Identical allelic loss on chromosome 11q13in microdissected in situ and invasivehuman breast cancer. Cancer Res 55: 467-471. 3266. Ziegler RG, Hoover RN, Pike MC,Hildesheim A, Nomura AM, West DW, Wu-Williams AH, Kolonel LN, Horn-Ross PL,Rosenthal JF, Hyer MB. (1993). Migrationpatterns and breast cancer risk in Asian-American women. J Natl Cancer Inst 85:1819-1827. 3267. Zollo JD, Zeitouni NC (2000). TheRoswell Park Cancer Institute experiencewith extramammary Paget's disease. Br JDermatol 142: 59-65. 3268. Zotalis G, Nayar R, Hicks DG (1998).Leiomyomatosis peritonealis disseminata,endometriosis, and multicystic mesothe-lioma: an unusual association. Int JGynecol Pathol 17: 178-182.
3269. Zou A, Marschke KB, Arnold KE,Berger EM, Fitzgerald P, Mais DE,Allegretto EA (1999). Estrogen receptorbeta activates the human retinoic acidreceptor alpha-1 promoter in response totamoxifen and other estrogen receptorantagonists, but not in response to estro-gen. Mol Endocrinol 13: 418-430. 3270. Zuntova A, Motlik K, Horejsi J,Eckschlager T (1992). Mixed germ cell-sexcord stromal tumor with heterologousstructures. Int J Gynecol Pathol 11: 227-233. 3271. Zweemer RP, van Diest PJ, VerheijenRH, Ryan A, Gille JJ, Sijmons RH, JacobsIJ, Menko FH, Kenemans P (2000).Molecular evidence linking primary cancerof the fallopian tube to BRCA1 germlinemutations. Gynecol Oncol 76: 45-50. 3272. Zweemer RP, Verheijen RH, Gille JJ,van Diest PJ, Pals G, Menko FH (1998).Clinical and genetic evaluation of thirtyovarian cancer families. Am J ObstetGynecol 178: 85-90. 3273. Zwijsen RM, Wientjens E,Klompmaker R, van der Sman J, BernardsR, Michalides RJ (1997). CDK-independentactivation of estrogen receptor by cyclinD1. Cell 88: 405-415.

425References
Subject index
A
Acantholytic variant, squamous cell car-cinoma, 38, 40, 41
Acanthosis nigricans, 189Acinic cell carcinoma, 45Acquired melanocytic naevus, 331, 332Adenocarcinoma in situ, 232, 272, 273,
275, 276Adenocarcinoma of Skene gland origin,
324Adenocarcinoma of the rete ovarii, 180Adenocarcinoma with spindle cell meta-
plasia, 38Adenocystic basal cell carcinoma, 44Adenofibroma, 122, 124, 125, 127, 130,
196, 209, 245, 248, 284, 285Adenohibernoma, 103Adenoid basal carcinoma, 267, 277-
279, 301Adenoid cystic carcinoma, 28, 44, 57,
86, 182, 184, 185, 228, 267, 277-279, 301, 321-323
Adenolipoma, 94, 103Adenoma malignum, 273Adenoma of minor vestibular glands,
324Adenoma of the rete ovarii, 181Adenomatoid tumour, 197, 199, 211,
243, 244, 310Adenomatous hyperplasia of the rete
ovarii, 181Adenomyoepithelial adenosis, 82, 86, 87Adenomyoepithelioma, 44, 46, 82, 86, 87Adenomyoma, 134, 188, 215, 235, 245,
249, 273, 284-286, 321, 323Adenosarcoma, 130, 133, 210, 212,
215, 244-248, 281, 282, 284-286,306, 307
Adenosis, 78, 81-83, 85, 87, 104, 295,297, 299, 300
Adenosis with apocrine metaplasia, 82Adenosquamous carcinoma, 39-41,
130, 174, 266, 273, 277, 278, 301,321, 322
A d re n o c o rtical carcinoma, 351, 352, 354Adult granulosa cell tumour, 131, 146AFP, see alpha-fetoprotein
Aggressive angiomyxoma, 305, 329Aggressive T-cell leukaemia, 361Akt, 231, 357Alpha lactalbumin, 41, 43Alpha-fetoprotein, 138, 155, 156, 165-
168, 184, 207, 246, 309Alveolar rhabdomyosarcoma, 215, 244,
282Alveolar soft part sarcoma, 215, 244,
280-282, 304, 326, 327Alveolar variant, lobular carcinoma, 24, 32Amenorrhea, 154, 157, 175, 190Amylase, 45Androblastoma, 153Androgen insensitivity syndrome, 157Androgen receptor gene, 112, 154Angiogenesis, 22Angiolipoma, 93Angiomyofibroblastoma, 327, 329, 330Angiosarcoma, 40, 89, 91, 94-96, 175,
188, 244, 280, 282, 304Apocrine adenoma, 85Apocrine adenosis, 82Apocrine carcinoma, 36, 37, 47, 71Apocrine cell, 36, 37, 47, 65APPBP2, 51Argyrophilia, 33, 80A-T complementation, 361Ataxia telangiectasia, ,27, 342, 350,
353, 361-363ATM see Ataxia telangiectasia Atypical adenosis, 299, 300Atypical carcinoid, 277, 279Atypical columnar change, 66Atypical cystic lobules, 63, 66Atypical ductal hyperplasia, 20, 63, 64,
66, 78Atypical hyperplasia, 63, 84, 136, 210,
221, 222, 228, 229, 232, 359Atypical intraductal hyperplasia, 66, 78Atypical leiomyoma, 236, 241Atypical lobular hyperplasia, 60Atypical lobules, type A, 66Atypical medullary carcinoma, 28, 338Atypical melanocytic naevus of the geni-
tal type, 332
Atypical papilloma, 78Atypical polypoid adenomyoma, 249,
285, 286Atypical proliferative serous tumour, 121Atypical vulvar naevus, 332Aurora-A, 51
BB72.3 (TAG-72) antibody, 119, 131, 138,
187Bannayan-Riley-Ruvalcaba syndrome,
357BARD1, 342Barr bodies, 171Bartholin gland adenoma, 323Bartholin gland carcinoma, 322Bartholin gland nodular hyperplasia,
323Bartholin gland tumour, 321, 322Basal cell carcinoma, 151, 174, 175,
184, 185, 316, 318, 319Basal cell tumour, 182, 184, 185Basaloid carcinoma, 267, 316Basaloid squamous cell carcinoma, 267,
278, 279, 317BASC, see BRCA1-associated surveil-
lance complex Bcl-2, 58, 92, 108, 109, 250BEK, 51Benign mesothelioma, 199Benign metastasizing leiomyoma, 237,
242Benign mixed epithelial tumour, 144Benign mixed tumour, 85, 306, 307Benign peripheral nerve sheath tumour,
92, 94Benign sclerosing ductal proliferation, 83Beta-catenin, 131Bethesda Criteria, 358ß-hCG, 22, 164, 165, 167, 168, 207,
250, 251, 252Bilateral breast carcinoma, 23, 48
425Subject Index
426 Subject Index
Biphasic teratomas, 168BLM, 341, 342Bloom syndrome, 349Blue naevus, 287, 288, 308, 309, 331,
332Blunt duct adenosis, 82BMPR1A, type 1A receptor of bone mor-
phogenetic proteins (BMP) 357Body mass index, 111Borderline Brenner tumour, 140, 142Borderline clear cell adenofibromas with
intraepithelial carcinoma, 139Borderline clear cell adenofibromatous
tumour, 139Borderline mixed epithelial tumour, 144Bowenoid papulosis, 319, 320BRAF, 120BRCA1, 14, 20, 29, 53- 56, 118, 120,
202, 207, 208, 337- 348, 350, 351,353, 354, 362
BRCA1-associated genome surveillancecomplex, 341, 342
BRCA2, 20, 29, 53-56, 112, 118, 133,207, 208, 337- 351, 354
Brenner tumour, 140-145, 172, 190, 196,212
Brenner tumour of low malignant poten-tial, 142
BRUSH-1, 112BTAK /aurora2 /STK15, centrosome-
associated serine/threonine kinase,51
Burkitt lymphoma, 107, 108, 191, 196
C
CA125, 109, 119, 130, 138, 141, 180,181, 184, 202, 272, 322, 340, 341,347, 348
CA19-9, carbohydrate antigen 19-9, 109Call-Exner bodies, 131, 145, 147, 177Calponin, 45, 75, 86, 91, 243Calretinin, 119, 147, 157, 180, 185, 198,
213, 244, 255, 275Cambium layer, 230, 283, 297, 302, 303Carcinoembryonic antigen, 106, 138,
164, 187, 224, 272, 276, 322, 332Carcinofibroma, 245, 248Carcinoid, 171, 172, 196, 277, 279, 301Carcinoid syndrome, 172Carcinoma adenoides cysticum, 44Carcinoma of the male breast, 110Carcinoma with choriocarcinomatous
features, 22Carcinoma with melanotic features, 22
Carcinoma with osteoclastic giant cells,21
Carcinosarcoma, 37, 40, 127, 133, 174,230, 236, 245-247, 255, 284, 285,306, 347
CCND1, 51, 59, 72, 73CD10, 108, 109, 135, 180, 187, 213,
233, 235, 240, 243, 248, 275CD30, 108, 166, 167CD31, 91, 95, 269, 282CD34, 91, 92, 95, 269, 282, 307, 327CD68, 22, 91, 98, 161, 192, 196, 311CD99, 92, 147, 157, 174, 183, 188, 234,
255, 307, 309, 334CD117, 164Cdc25A, 354Cdc25C, 354CDH1, 53CDKN2A, 52CEA, 164, 341, 348Cellular angiofibroma, 327, 329, 330
Cellular fibroma, 149-151Cellular leiomyoma, 235, 236, 239, 240Cellular variant, blue naevus, 308, 309Central papilloma, 76-78
C-erbB, 250, 266Cervical intraepithelial neoplasia, 63,
262, 264-273, 276, 279, 294, 295, 319Charcot-Böttcher filaments, 157CHEK2, 350, 351, 353, 354, 362Chloroacetate esterase, 196, 311Chloroma, 192, 196, 311
Chondrolipoma, 94Choriocarcinoma, 168, 186, 210, 250-
252, 311Chorionic gonadotrophin, 22
Chromogranin A, 30Chromosomal double-strand breaks,
342Chymotrypsin, 45Ciliated cell variant, endometrioid ade-
nocarcinoma, 221, 224CIN, s e e Cervical intraepithelial neoplasia c-Jun, 352CK 5,6, 61, 92CK14, 86CK34BE12, 38, 61, 65CK5, 38, 65, 86CK5/6, 38CK7, 38, 226, 227C-kit, 164
Clear cell adenocarcinofibroma, 137
Clear cell adenocarcinoma, 137-139,188, 195, 206, 207, 212, 221, 223-226, 272, 274, 276, 297-300
Clear cell adenofibroma, 137, 139Clear cell adenofibromatous tumour of
borderline malignancy, 139Clear cell carcinoma, 46, 137, 138, 160,
166, 196, 212, 228, 339Clear cell cystadenofibroma, 137Clear cell cystadenoma, 137Clear cell hidradenoma, 46, 325Clear cell leiomyoma, 241Clinging carcinoma, 63, 66c-Myc, 72, 266Coagulative necrosis, 164Cobblestone-like papules, 356COL1A1/PDGFB, 327Collagenous spherulosis, 44, 60, 78Colloid carcinoma, 30, 272Columnar cell mucinous carcinoma, 30, 31Complete hydatidiform mole, 252-254Complex (adenomatous) hyperplasia of
the endometrium, 229Complex sclerosing lesion, 27, 81-83Condylomatous squamous cell carcino-
ma, 267Congenital melanocytic naevus, 331,
332Cotyledonoid dissecting leiomyoma,
216, 241Cowden syndrome, 232, 355CSE1L/CAS, 51CTNNB1 (beta-catenin), 131Cushing syndrome, 160, 175Cyclin D1, 51, 73, 338Cylindromatous carcinoma, 44CYP24, 51Cystadenocarcinoma, 145Cystic lymphangioma, 199Cytokeratin 7, 25, 33, 45, 106, 109, 119,
129, 141, 147, 156, 195, 226, 268, 275Cytokeratin 14, 45Cytokeratin 20, 33, 119, 143, 187, 213,
226, 341, 348, Cytokeratin 34betaE12, 86, 187, 213Cytokeratin AE1/AE3, 21, 47, 119, 161Cytokeratin CAM5.2, 21, 119, 187Cytotrophoblast, 164, 167, 168, 186,
251, 252
D
DAM1, 50
427Subject Index
DCIS, see Ductal carcinoma in situ 20,25, 26, 28, 32, 33, 35, 60, 61, 63-73, 75, 77-81, 101, 106, 112, 338,346, 347, 356
Deciduoid mesothelioma, 197Deep angiomyxoma, 304, 305, 327,
329, 330Dermatofibrosarcoma protuberans, 327Dermoid cyst, 127, 129, 143, 163, 169-
175, 188, 196, 215, 287, 288, 310DES, 274, 297, 298, 299Desmoid tumour, 92Desmoplastic small round cell tumour,
197, 200Diethylstilbestrol, 274, 297Diffuse angioma, 89Diffuse large B-cell lymphoma, 108Diffuse leiomyomatosis, 237, 241Diffuse malignant mesothelioma, 197,
198Diffuse peritoneal leiomyomatosis, 200DIN, 63, 64, 66, 67Dissecting leiomyoma, 241Disseminated peritoneal adenomuci-
nosis, 128DNA ploidy, 53, 54Ductal adenoma, 77, 85Ductal carcinoma in situ, 20, 25, 26, 28,
32, 33, 35, 40, 44, 58, 60, 61, 63-75, 77-81, 101, 106, 112, 338, 346,347, 356
Dysgerminoma, 138, 163-166, 168, 176-179, 191, 196, 340
Dyskeratosis, 270Dysplasia, 254, 269, 284, 294, 295, 319,
345Dysplasia/carcinoma-in-situ, 269Dysplastic melanocytic naevus, 331,
333
E
E6, 262, 265, 318E7, 262, 263Early invasive adenocarcinoma, 272, 275Early invasive squamous cell carcino-
ma, 268EBV, see Epstein-Barr Virus E-cadherin, 24, 25, 29, 33, 53, 61, 62,
65, 71, 72, 112, 252Ectopic decidua, 189, 198EGFR, 27, 50, 58, 202, 250EIN, 231, 232EMA, see Epithelial membrane antigen
Embryoid bodies, 167Embryonal carcinoma, 163, 166-168Embryonal rhabdomyosarcoma, 97,
211, 215, 248, 281, 302, 303, 326EMK, 112Enchondromatosis, 149Encysted papillary carcinoma, 79Endocervical polyp, 276, 277Endocervical-like borderline tumour,
126, 127Endocrine carcinoma, 32Endodermal sinus tumour, 165, 288,
309, 333Endometrial hyperplasia, 131, 132, 137,
146, 152, 187, 221, 222, 225, 228,229, 231, 232, 359
Endometrial polyp, 209, 230, 245, 246,249
Endometrial stromal nodule, 233-236Endometrial stromal sarcoma, 149, 190,
196, 216, 233, 234, 245, 247, 281,309
Endometrioid adenocarcinoma, 130,143, 206, 207, 212, 221-226, 230,232, 249, 272-275, 297, 300
Endometrioid borderline tumour, 130,135, 136
Endometrioid polyp, 209Endometrioid stromal sarcoma, 130,
134, 135, 147, 215, 235, 280, 281,302, 303
Endometrioid tumour of borderlinemalignancy, 135
Endometrioid tumour of low malignantpotential, 135
Endometriosis, 127, 130-137,143, 145,180, 190, 195, 200, 210, 212, 215,235, 281, 300, 303, 324
Endometriosis with smooth musclemetaplasia, 215
E n d o m e t roid yolk sac tumour,1 6 6
Endomyometriosis, 215Endosalpingiosis, 123, 210Endosalpinx, 340, 347Ependymoma, 171, 174, 212, 213Epidermoid cyst, 144, 175Epithelial membrane antigen, 21, 22, 43,
45, 91, 119, 131, 138, 147, 154,156, 157, 161, 180, 182, 187, 200,213, 255, 275, 332,
Epithelioid leiomyoma, 236, 241Epithelioid leiomyosarcoma, 238, 241,
252, 280, 281Epithelioid trophoblastic tumour, 251,
252Epitheliosis, 65, 104
Epstein-Barr virus, 17, 29, 108, 268, 311ERß receptor, 58ERBB2, 23, 25, 27, 29, 35, 48, 51, 53,
58-60, 66, 72, 73, 106, 112, 202,338, 341, 346
ERBB3, 51, 202ERBB4, 51, 202Erosive adenomatosis, 104Ewing tumour, 174, 200, 211, 244, 255,
309, 333, 334EWS/FLI1, 174, 309, 334EWS-WT1, 200, 201Exaggerated placental site,
2 5 4Exonic splicing enhancer, 350Extranodal marginal-zone
B-cell lymphoma, 108
F
Factor VIII protein, 91FANCA, 52FANCD1, 346, 350Fanconi anaemia, 342, 349, 350Fanconi anaemia D2 protein,
342Fetiform teratoma, 163, 170FGFR1, 50, 59FGFR2, 51FHIT, 27, 52, 265Fibroadenoma, 30, 81, 84, 90, 98,
99, 253Fibrocystic disease, 355, 356Fibroepithelial polyp, 271, 297, 302,
303, 320, 321, 329, 330Fibroma, 134, 135, 149-153, 158, 187,
190, 215, 325Fibromas of the oral mucosa, 356Fibromatosis, 39, 40, 88, 92, 190Fibrosarcoma, 40, 101, 135, 151, 175,
188, 304Fibrosis mammae virilis,
110Fibrothecomatous stroma,
147, 148Flat epithelial atypia, 26, 63, 65, 66FLG, 50Florid papillomatosis, 104Follicular lymphoma,
107, 109, 191Folliculome lipidique, 157Fragile histidine triad, 265
428 Subject Index
G
GADD45, 343, 353GCDFP-15, 25, 33, 36, 37, 44, 45Gelatinous carcinoma, 30Genital rhabdomyoma, 282, 304Gestational choriocarcinoma, 168, 182,
186, 210, 251, 334Gestational trophoblastic disease, 210, 250GFAP, 86, 174Glandular dysplasia, 265, 276Glassy cell carcinoma, 228, 277, 279Glioblastoma, 171, 174Gliomatosis peritonei, 170Glomus tumour, 171, 175, 283, 330Glycogen-rich carcinoma, 46Goblet cell, 124-127, 156, 173, 195,
206, 224, 272Goldenhar syndrome, 149Gonadoblastoma, 163, 164, 167, 176-
179Grading of invasive carcinoma, 18Granular cell tumour, 36, 37, 94, 283,
327, 330Granulocytic sarcoma, 109, 191, 192,
196, 311, 334Granulosa cell tumour, 131, 134, 145-
151, 159, 160, 183, 196, 215Granulosa-stromal cell tumours, 160GRB7, 53Gynaecomastia, 90, 91, 110, 111Gynandroblastoma, 158, 159
H
5-HIAA, 5-hydroxyindoleacetic acid, 173Haemangioblastoma, 94Haemangioma, 89, 94, 244, 283, 330Haemangiomatosis, 149, 357Haemangiopericytoma, 90, 244Haemangiosarcoma, 94Haematoperitoneum, 186Haematosalpinx, 206Haemorrhagic cellular leiomyoma, 240HAIR-AN syndrome, 189Hamartoma, 98, 100, 355, 357H a m a rtomatous polyps of the colon, 356HBME1, 244H-caldesmon, 234, 235, 240, 243Hepatocellular carcinoma, 184, 353Hepatoid carcinoma, 182, 184Hepatoid yolk sac tumour, 165, 184
HER2, 51, 58Herceptin, 58, 73Hereditary breast-ovarian cancer syn-
drome, 208Hereditary colorectal endometrial can-
cer syndrome, 358Hereditary defective mismatch repair
syndrome, 358Hereditary fallopian tube carcinoma,
340, 347
Hereditary nonpolyposis colon cancersyndrome, 53, 118, 132, 232, 337,358-360
Hibernoma, 94HIC1, 52Hilus cell tumour, 161Hirsutism, 154, 157, 190Histiocytoid carcinoma, 46HIV, 262, 269, 319, 320HMB45, 106, 109HMGIC, 230, 242HMGIY, 230, 242HNPCC, see Hereditary non-polyposis
colon cancer Homunculus, 170HPV, see Human papilloma virus hRad50-hMre11-NBS1p95 (R/M/N) com-
plex, 342
HRAS1, 343Human papillomavirus, 226, 227, 262,
265-271, 293, 295, 296, 311, 316-321Hydatidiform mole, 182, 186, 210, 250-
252, 254Hydrosalpinx, 206Hypercalcaemia, 137, 138, 148, 182Hyperoestrinism, 146, 221, 222, 225Hyperplasia of the usual type, 65Hyperplasias without atypia of the
endometrium 229Hyperreactio luteinalis, 189
I
IGF2R, 52IGF-binding proteins, 16Immature teratoma, 166, 169-171, 174,
188Infiltrating ductal carcinoma, 19, 20, 22,
23, 28, 31Infiltrating epitheliosis, 83Infiltrating myoepithelioma, 88Infiltrating syringomatous adenoma, 39, 105Inflammatory carcinoma, 47
Inflammatory myofibroblastic tumour,92, 93
I n f l a m m a t o ry pseudotumour, 93Inhibin, 131, 135, 138, 147, 148, 150,
151, 154, 156, 157, 159-161, 174,180, 182, 187, 188, 213, 234, 243,255
Insulin-growth factor-I, 16Intercellular adhesion molecule-1, 29Intestinal-type borderline tumour, 127,
129Intracystic papillary carcinoma, 34, 79, 80Intraductal carcinoma, 27, 46, 67, 105,
106Intraductal hyperplasia, 65Intraductal papillary carcinoma, 76, 78,
79, 80Intraductal papillary neoplasms, 76Intraductal papilloma, 76, 78, 81, 85Intraductal proliferative lesions, 63, 64, 77Intravenous leiomyomatosis, 216, 235,
237, 241, 242Invasive breast carcinoma, 13, 18, 58,
63, 64, 71, 78, 96, 112, 362Invasive cribriform carcinoma, 22, 27, 28Invasive ductal carcinoma, 18-20, 35,
57, 64, 72, 73, 353Invasive ductal carcinoma, no specific
type, 19Invasive ductal carcinoma, not otherwise
specified, 19Invasive hydatidiform mole, 254Invasive lobular carcinoma, 20, 23, 32,
36, 42, 49, 51, 61, 62, 338, 346Invasive micropapillary carcinoma, 35Invasive papillary carcinoma, 34, 35Inverted follicular keratosis, 321
J
JAZF1, JJAZ1, 234Juvenile carcinoma, 42Juvenile fibroadenoma, 99Juvenile granulosa cell tumour, 146, 148,
174, 182
K
Keratinizing type squamous cell carci-noma, 266, 267, 316, 317
Keratoacanthoma, 317, 321Ki-67, 57, 270, 272
429References
Koilocytosis, 267, 270, 271, 294, 295,296, 320, 321
KRAS, 120, 125, 129, 145, 202, 231,281
Krukenberg tumour, 153, 190, 193-196
L
Lactating adenoma, 84Laminin, 27, 28, 44, 53, 81, 82, 278Large cell keratinizing squamous cell
carcinoma, 38Large cell neuroendocrine carcinoma,
33, 184, 279Large duct papilloma, 76LCIS, see Lobular carcinoma in situ Leiomyoblastoma, 238, 241Leiomyoma, 98, 215, 216, 233-237,
239-242, 244, 256, 281, 282, 304,327, 330, 355
Leiomyomatosis peritonealis dissemina-ta, 200
Leiomyosarcoma, 98, 175, 196, 211,215, 233, 236-240, 245, 280, 281,283, 302, 303, 305, 326, 330
Leukaemia, 49, 109, 191, 192, 196, 211,289, 311, 334, 351, 361
Leukoplakia, 264Leuprolide, 238Leydig cell tumour, 131, 154, 158, 160,
161Leydig cell tumour, non-hilar type, 161Lichen sclerosus, 316Li-Fraumeni syndrome, 65, 67, 351, 352,
354LIN, s e e Lobular intraepithelial neoplasia Lipid cell tumour, 160Lipid secreting carcinoma, 41Lipid-rich carcinoma, 41Lipofuscin, 22, 154, 160, 161Lipoleiomyoma, 237, 241, 244Lipoma, 93, 94, 103, 175, 244, 283, 330Lipomatosis, 357Liposarcoma, 40, 96, 97, 101, 211, 215,
244, 246, 282, 326, 327, 329Lobular carcinoma in situ, 23-25, 53, 60,
61, 74, 338, 346Lobular intraepithelial neoplasia, 60-62,
81, 101, 106, 112Lobular neoplasia, 20, 26, 60, 71, 75,
338Louis-Bar Syndrome, 361Low grade adenosquamous carcinoma,
39, 105
Luteinized thecoma, 149, 150, 158Luteoma of pregnancy, 160, 188, 189,
196Ly m p h a n g i o s a rcoma, 94, 188Lymphoblastic lymphoma, 107Lymphoedema, 95, 96, 263Lymphoepithelioma, 29, 207, 266-268Lymphoepithelioma-like carcinoma, 207,
267, 268Lymphoma, 108, 191, 289, 310Lynch syndrome, 358Lysozyme, 45, 196, 311
M
M6P/IGF2R, 52Macrocephaly, 355, 357Maffucci syndrome, 149, 151Major duct papilloma, 76Malignant Brenner tumour, 140, 142Malignant fibrous histiocytoma, 96, 175,
244, 282, 304Malignant lymphoma, 107, 109, 112,
183, 191, 192, 211, 256, 311, 334Malignant melanoma, 22, 23, 106, 109,
112, 160, 171, 196, 287, 308, 317,331-334, 353
Malignant mesodermal mixed tumour,133, 245, 306
Malignant mesothelioma, 182, 185, 197-199
Malignant mixed epithelial tumour, 144Malignant müllerian mixed tumour, 130,
133, 149, 156, 188, 210, 245, 284,306
Malignant myoepithelioma, 86, 88Malignant peripheral nerve sheath
tumour, 188, 244, 280-282, 304Malignant pigmented neuroectodermal
tumour of infancy, 244Malignant rhabdoid tumour, 244, 327Malignant struma, 171, 172Malignant sweat gland tumour, 324MALT lymphoma, 108, 109Mammary hamartoma, 103Mammary osteogenic sarcoma, 97Masculinization, 189Maspin, 86Massive ovarian oedema, 190Matrix producing carcinoma, 37, 40Mature cystic teratoma, 163, 170, 174,
287, 288, 310Mature teratoma, 168-171, 174, 175,
215, 288
MDM2, 53, 250, 352, 353Medullary carcinoma, 20, 28, 34, 57,
109, 338Medulloblastoma, 174Medulloepithelioma, 174Megencephaly, 355Meigs syndrome, 151, 172, 215Melan A, 188, 332Melanocytic naevus, 171, 175, 308,
309, 331, 333Melanocytic tumours, 175, 308, 331Melanotic paraganglioma, 255Menometrorrhagia, 154, 157, 221Mental retardation, 355Merkel cell tumour, 333Mesonephric adenocarcinoma, 272,
274, 275, 284, 297, 300Metaplastic carcinoma, 37, 39-41, 85,
97, 133, 245, 246, 284, 306Metaplastic papillary tumour, 209Metastasizing leiomyoma, 242Metastatic hydatidiform mole, 254MIB-1, 57MIC2, 174, 183Microglandular adenosis, 27, 82Microinvasive carcinoma, 49, 74, 75,
269, 316Microinvasive squamous cell carcino-
ma, 268, 269Micropapillary pattern, 26, 70, 123Micropapillomatosis labialis, 320Microsatellite instability, 53, 131, 132,
231, 232, 358, 360Microscopic papilloma, 77Minimal deviation adenocarcinoma, 265,
272, 273, 285, 286Mismatch repair, 53, 132, 232, 337, 358,
360Mitotically active leiomyoma, 240Mixed ductal-lobular carcinoma, 25Mixed endometrial stromal and smooth
muscle tumour, 235, 242Mixed epithelial tumour, 143, 144Mixed germ cell-sex cord-stromal
tumour, 176, 178, 179Mixed gonadal dysgenesis, 177Mixed type carcinoma, 21, 24, 27MLH1, 53, 118, 131, 132, 337, 342,
358-361MLH3, 359, 360MMR, 358, 360Monoclonality, 265Monodermal teratoma, 171, 175
430 Subject Index
MPNST, see Malignant peripheral nervesheath tumour
MRE11, 341MSH2, 53, 118, 132, 337, 342, 358-361MSH6, 53, 337, 342, 358-361MSI, 53, 359-361MSI-H, 360, 361Mucin producing carcinoma,
30Mucinous adenocarcinoma, 124, 206,
212, 221, 224, 272, 273, 297, 300Mucinous borderline tumour, 124-126,
128, 145, 193Mucinous borderline tumour, intestinal
type, 125Mucinous carcinoid, 171, 173, 195Mucinous carcinoma, 30, 31, 34, 35, 57,
80, 124-126, 128, 195, 206, 226,339
Mucinous cystadenocarc i n o f i b roma, 124Mucinous cystadenocarcinoma, 30-32,
145Mucinous cystadenoma, 124-127, 129,
143, 156, 175, 209, 212Mucinous cystic tumours with mural
nodules, 127Mucinous tumour of borderline malig-
nancy, endocervical-like, 126Mucinous tumour of borderline malig-
nancy, intestinal type, 125Mucinous tumour of low malignant
potential, endocervical-like, 126Mucinous tumour of low malignant
potential, intestinal type, 125Mucocoele-like lesion, 31Mucoepidermoid carcinoma, 39, 277Mucoid carcinoma, 30, 42Mucosal/acral lentiginous melanoma,
331Muir-Torre syndrome, 132MUL, 51Müllerian papilloma,
276, 300Multicystic mesothelioma, 197, 198Multilocular peritoneal inclusion cyst, 198Multinodular goitre, 356Multinucleated giant cells, 92, 99, 207Multiple facial trichilemmomas, 356Multiple hamartoma syndrome, 355MutL homologue 1, 359MutL homologue 3, 359MutS homologue 2, 359MutS homologue 6, 359Myc, 250, 266Myoepithelial carcinoma, 40, 86, 88, 92
Myoepitheliosis, 86Myofibroblastoma, 91Myoglobin, 246, 302Myoid hamartoma, 103Myxoid leiomyoma, 236, 241Myxoid leiomyosarcoma, 238Myxoma, 182, 187, 244
N
NCOA3 (AIB1), 51, 343, 350Neuroblastoma, 51, 174, 334Neuroendocrine carcinoma, 30, 43, 184,
279, 333N e u roendocrine tumours, 32, 144, 277, 279Neurofibroma, 94, 329, 330Neuron-specific enolase, 200, 255Nevoid basal cell carcinoma syndrome,
151NFKB / NF-kappaB, 352, 362Nipple adenoma, 81, 104Nipple discharge, 68, 74, 76, 77, 85,
92, 97, 101, 112Nipple duct adenoma, 104Nodular adenosis with apocrine meta-
plasia, 85Nodular hidradenoma, 324, 325Nodular melanoma, 331Nodular theca-lutein hyperplasia of
pregnancy, 188Non-encapsulated sclerosing lesion, 83Non-gestational choriocarcinoma, 163,
167, 168Non-keratinizing, squamous cell carci-
noma, 266, 267, 316, 317Non-medullary thyroid cancer,
355Nuclear grooves, 86, 147
O
O6-Methylguanine DNA ethyltransferase(O6MGMT) 353
Ollier disease, 149Oncocytic carcinoma, 43Ordinary intraductal hyperplasia, 65Osteosarcoma, 40, 97, 98, 101, 175,
188, 244, 246, 282Ovarian tumour of probable wolffian
origin, 186Ovarian wolffian tumour,
182, 186
P
p14ARF, 353p16/CDKN2a/p16INK4, 270, 353p21, 250, 341, 348p27, 58p63, 86p73, 362Paget disease, 23, 35, 41, 63, 68, 105,
112, 174, 319, 321, 322, 324, 332,352
Paget disease of the nipple, 35, 41, 105Pagetoid spread, 332, 333Paneth cell, 45, 125-127, 272, 276Papillary adenoma, 104Papillary carcinoma, non-invasive, 78Papillary ductal carcinoma in situ, 79Papillary hidradenoma, 321, 323Papillary intraductal carcinoma, 32, 34,
79Papillary squamous cell carcinoma, 267Papilloma, 76-79, 119, 209, 296Papillomatosis, 76, 104, 271, 296Papillomatosis of the nipple, 104Paraganglioma, 182, 187, 255, 283Parasitic leiomyoma, 239Parathyroid hormone-related protein,
138Partial hydatidiform mole, 254PAT1, 51PDGFRL, 52Peau d’orange, 48PEComa, 243Peptide YY, 172Periductal stromal sarcoma, 100, 102Peripheral papilloma, 76-78, 83Peripheral primitive neuroectodermal
tumour, 244, 255, 309, 334Peritoneal mesothelioma, 185,197, 199Peritoneal mucinous carcinomatosis,
128Peritoneal tumours, 197Perivascular epithelioid cell tumour, 243Peutz-Jeghers syndrome, 156-158, 208,
273Phaeochromocytoma, 187Phosphoinositol-3-kinase, 357Phyllodes tumour, 96, 97, 99-101, 103,
247, 352Pigmented progonoma, 175PIVKA-II (protein induced by vitamin K
absence), 184Placental alkaline phosphatase, 196
431Subject Index
Placental site nodule, 211, 252, 254Placental site trophoblastic tumour, 210,
250-252Placental-like alkaline phosphatase
(PLAP) 164, 168, 191, 252Plasma cell granuloma, 93Plasmacytoma, 192Pleomorphic adenoma, 41, 85, 86, 88,
307, 324Pleomorphic carcinoma, 21, 41Pleomorphic lobular carcinoma, 24, 25Plexiform leiomyoma, 241PMS1, 53, 360PMS2, 53, 359, 360PNET, see Primitive neuroectodermal
tumour P o l y e m b ryoma, 163, 167, 168Polypoid adenofibroma, 209Polyvesicular vitelline tumour,
165Postmeiotic segregation 2, 359Postoperative spindle cell nodule, 244,
281, 283, 305, 326Post-radiotherapy angiosarcoma, 96Potter syndrome, 149Primary peritoneal borderline tumour,
197, 202Primary peritoneal carcinoma, 197, 201Primitive neuro e c t o d e rmal tumour,
171,174, 309, 310Proliferating trichilemmal tumour,
325Prophylactic bilateral mastectomy,
345Prophylactic bilateral salpingo-
oophorectomy, 345Proteus syndrome, 357Protocadherin 9, 112Proximal-type epithelioid sarcoma,
326pS2, 72Psammocarcinoma, 201, 202Psammoma bodies, 68, 119, 122, 198,
202, 210, 214, 224, 225, 255, 274,276
Pseudoangiomatous hyperplasia, 103Pseudoangiomatous stromal hyperpla-
sia, 90Pseudocarcinomatous hyperplasia, 209Pseudomyxoma ovarii,
129Pseudomyxoma peritonei, 126, 128,
129, 208PTEN, 131, 132, 145, 230-232, 318,
354-357, 359
R
Rad50, 341RAD51, 341-343, 348-351Radial scar, 26, 27, 39, 60, 78, 81-83Radial sclerosing lesion, 83RASSF1A (Ras association domain fam-
ily 1A gene), 52RB1CC1 (RB1-inducible Coiled-Coil 1),
52Reichert membrane, 165Reifenstein syndrome, 112Reinke crystals, 154, 158, 160, 161,
176, 177Renin, 157, 207Rete cyst, 124Rete ovarii adenocarcinoma, 180Rete ovarii adenoma, 180Retiform Sertoli-Leydig cell tumour, 156Retiform wolffian adenocarcinoma, 212Retiform wolffian adenoma, 212Retiform wolffian tumour, 186Retinal anlage tumour, 171, 175Revised Amsterdam Criteria, 358Rhabdoid tumour, 244Rhabdomyoma, 244, 282, 305, 330Rhabdomyosarcoma, 40, 97, 101, 109,
135, 155, 175, 188, 244, 302, 309,311, 326
RING domain, 342Rokitansky protuberance, 163, 171RPS6KB1, 51
S
Salpingitis isthmica nodosa, 210Sarcoma botryoides, 155, 248, 280,
281, 283, 297, 302, 303, 305, 309,326
Sarcoma family syndrome of Li andFraumeni, 351
Schiller-Duval bodies, 165Schwannoma, 94, 283, 304, 330Scleroelastotic scar, 83Sclerosing adenosis, 27, 39, 60, 61, 78,
81-83, 86, 98, 99, 104Sclerosing papillary lesion, 39, 83Sclerosing papilloma, 77, 85, 104S c l e rosing papillomatosis, 104S c l e rosing peritonitis, 149, 150Sclerosing stromal tumour, 149, 152SCTAT, see Sex cord tumor with annular
tubules
Sebaceous adenoma, 171, 175Sebaceous carcinoma, 37, 46, 47, 171,
175, 324Sebocrine cell, 47Seborrheic keratosis, 321Secretory carcinoma, 42
Secretory variant, endometrioid adeno-carcinoma, 130, 221, 223
Seminoma, 163, 164, 176, 177Serotonin, 143, 173, 272, 279Serous adenocarcinoma, 119, 141, 201,
206, 212, 221, 224-226, 272, 274,339
Serous adenofibroma, 119Serous borderline adenofibroma, 122Serous borderline tumour, 119, 120,
121, 127, 144, 202, 209Serous borderline tumour with microin-
vasion, 120Serous cystadenoma, 119, 124, 209,
212Serous papillary cystadenoma, 119Serous psammocarcinoma, 119, 120Serous surface borderline tumour, 122Serous tumour of borderline malignancy,
120, 121Serous tumour of borderline malignancy
with microinvasion, 120Serous tumour of low malignant poten-
tial with microinvasion, 120Serous tumour of low malignant
potential,, 121Sertoli cell tumour, 153, 156-159, 179,
196, 213Sertoli cell tumour, annular tubular vari-
ant, 158Sertoli-Leydig cell tumour, 131, 153,
157, 159, 172, 180, 188, 196, 213Sertoli-Leydig tumour with heterologous
elements, 155Sex cord tumour with annular tubules,
157-159, 179, 273Sex hormone-binding globulin, 16Signet ring cell carcinoma, 30, 32, 42Signet-ring cell, 138, 272, 273
Signet-ring cell adenocarcinoma, 193,273
Signet-ring stromal tumour, 153Simple atypical hyperplasia of the
endometrium, 229Simple hyperplasia of the endometrium,
229Site specific early onset breast cancer
syndrome, 346SIX1 homeobox gene, 72
432 Subject Index
Small cell / oat cell carcinoma, 32Small cell carcinoma, 32-34, 145, 148,
174, 182, 183, 196, 207, 221, 227,266, 267, 277-279, 301, 309, 321,323
Small cell carcinoma of neuroendocrinetype, 183, 227
Small cell carcinoma hypercalcaemictype, 145. 182
Small cell carcinoma, pulmonary type,183
Smooth muscle myosin, 75, 86Smooth muscle tumour of uncertain
malignant potential, 238Solid neuroendocrine carcinoma, 32Spangaro bodies, 157Speckled penis, 357Spindle cell carcinoma, 37, 88, 92Spindle cell epithelioma, 307Spindle cell lipoma, 93Spindle cell variant, adenomyoepithe-
lioma, 87Spindle cell variant, squamous cell car-
cinoma 38Squamotransitional carcinoma, 268Squamous intraepithelial lesion, 269,
270, 294Squamous papilloma, 266, 271, 272,
293, 296S-T syndrome, 95, 96ST7, 52Stellate scar, 83Sternberg tumour, 216Steroid cell tumour, 138, 160, 188, 196,
216Stewart Treves syndrome, 95STK11, 273STK15, 51Stromal hyperplasia, 189, 190Stromal hyperthecosis, 161, 189, 190Stromal luteoma, 160, 161Stromal polyp, 271, 297Stromal tumour with minor sex cord ele-
ments, 152Stromal-Leydig cell tumour, 158Struma ovarii, 138, 157, 160, 171, 172Strumal carcinoid, 171-173Subareolar duct papillomatosis, 104Superficial angiomyxoma, 327, 329Superficial spreading melanoma, 331Supernumerary ring chromosome, 327Sustentacular cell, 187Symplastic leiomyoma, 241
Synaptophysin, 30, 33, 34, 173, 279, 334Syncytial growth pattern, 28Syncytiotrophoblast, 164, 167, 168, 186,
207, 251, 252, 254Synovial sarcoma, 304, 307Syringoma, 81, 324, 325Syringomatous adenoma, 104, 105Syringomatous squamous tumour, 39
T
Tamoxifen-related lesions, 230TBX2, 51Terminal duct lobular unit (TDLU) 13,
17, 19, 60, 63, 66, 76, 79, 81Thecoma, 135, 147, 149, 150, 152, 158,
187, 215Thyroglobulin, 138, 172Thyroid transcription factor-1, 34TP53, see Li-Fraumeni syndrome TP73, 52, 352Transforming growth factor alpha, 58Transitional cell carcinoma, 140-142,
145, 174, 196, 206, 207, 226, 267,268, 311, 321, 322, 339, 361
Transitional cell metaplasia, 207, 268,270, 295
TRAP240, 51Trastuzumab, 58Trichilemmoma, 324, 325, 355Trichoepithelioma, 324, 325TTF-1 (thyroid transcription factor-1), 34Tubal epithelial hyperplasia, 209Tubular adenoma, 84, 87, 300Tubular carcinoma, 19, 23, 24, 26-28,
35, 73, 105, 336, 338, 356Tubulo-lobular carcinoma, 24, 346Tubulovillous adenoma, 300Tumour associated macrophages, 22Turcot syndrome, 360Turner syndrome, 176, 249
U
Ubiquitin ligase, 342Ubiquitin-mediated degradation, 53Ulex europaeus agglutinin-1, 91Unclassified sex cord - s t romal tumour, 160Undifferentiated carcinoma of non-small
cell neuroendocrine type, 184
Undifferentiated endocervical sarcoma,280, 281
Undifferentiated endometrial sarcoma,233, 234, 236
Undifferentiated ovarian sarcoma, 134,135
Undifferentiated uterine sarcoma, 236Undifferentiated vaginal sarcoma, 302,
303Uterus-like mass, 215
V
Vaginal intraepithelial neoplasia (VAIN),293- 296
Vaginal micropapillomatosis, 296VATER, 357Verrucous carcinoma, 267, 294, 316,
317Vestibular micropapillomatosis, 320Vestibular papilloma, 316, 320VHL, see von-Hippel Lindau disease
214, 215Villoglandular variant, adenocarcinoma,
221, 223, 273Villous adenoma, 300VIN, see Vulvar intraepithelial neoplasia Virilization, 152, 156, 188-190von Hippel-Lindau disease, 212, 214,
215Vulvar intraepithelial neoplasia (VIN),
316, 318-320, 324
W
Walthard cell nests, 144Warty type, squamous cell carcinoma,
266, 267, 294, 316, 317Well differentiated papillary mesothe-
lioma, 197, 198Wilms tumour, 169, 182, 187, 200, 256,
284, 285Wolffian adnexal tumour, 207, 212, 213,
215WT1, 200, 202
YYolk sac tumour, 137, 138, 156, 163-
166, 168, 170, 215, 246, 256, 287,288, 309, 333
ZZNF217, 51Zymogen-like granule, 45

















