Journal of Behavioral 3/ledicine, Vol. 7, No. 4, 1984 Coping and Adjustment To Genital Herpes Sharon Manne ~ and Irwin Sandier ~ Accepted for publication." January 20, 1984 The current study examined how individuals deal with genital herpes, a recurrent, incurable disease with a great psychological impact. An assess- ment battery composed of cognitive and problem-focused coping, attribu- tion, and social support mechanisms was employed. These coping mechanisms were correlated with measures of psychological adjustment." self-esteem, depression, sexual adjustment, and amount upset by herpes. Subjects were 152 people with herpes recruited from self-help groups and people from the community who volunteered to participate in the study. Results supported several hypotheses derived from previous research on coping with life stressors. Cognitive coping mechanisms, especially negative thoughts, along with wishful thinking and characterological self-blame, were significant predictors of poor psychological adjustment. Social sup- port was correlated with better psychological adjustment. In addition, the repeated use of disease management strategies was found to correlate with poor psychological adjustment. Further research in the area of coping with chronic illness is suggested. KEY WORDS: coping; adjustment; herpes; chronic illness. INTRODUCTION The past decade of medical research has seen a dramatic increase in the ability of the medical community to decrease the number of people who die from acute and deadly illnesses. However, with these technological ad- vances, there has also been a price to pay. Diseases that used to be fatal are nowchronic and degenerative (i.e., cancer and heart disease) and have be- ~Arizona State University, Tempe, Arizona 85287. 391 0160 7715/84/1200 0391503.50/0 =~ 1984Plenum Publishing Corporation
Transcript
Journal o f Behavioral 3/ledicine, Vol. 7, No. 4, 1984
Coping and Adjustment To Genital Herpes
S h a r o n M a n n e ~ and Irwin S a n d i e r ~
Accepted for publication." January 20, 1984
The current study examined how individuals deal with genital herpes, a recurrent, incurable disease with a great psychological impact. An assess- ment battery composed o f cognitive and problem-focused coping, attribu- tion, and social support mechanisms was employed. These coping mechanisms were correlated with measures o f psychological adjustment." self-esteem, depression, sexual adjustment, and amount upset by herpes. Subjects were 152 people with herpes recruited from self-help groups and people from the community who volunteered to participate in the study. Results supported several hypotheses derived from previous research on coping with life stressors. Cognitive coping mechanisms, especially negative thoughts, along with wishful thinking and characterological self-blame, were significant predictors o f poor psychological adjustment. Social sup- port was correlated with better psychological adjustment. In addition, the repeated use o f disease management strategies was found to correlate with poor psychological adjustment. Further research in the area o f coping with chronic illness is suggested.
The past decade of medical research has seen a dramatic increase in the ability of the medical communi ty to decrease the number of people who die f rom acute and deadly illnesses. However, with these technological ad- vances, there has also been a price to pay. Diseases that used to be fatal are nowchron ic and degenerative (i.e., cancer and heart disease) and have be-
come leading causes of death (Vital Statistics of the US., 1974). Chronic, nonfatal illnesses such as arthritis, kidney disease, and diabetes have be- come more prominent. Living with a chronic illness is a task which requires skills beyond those of dealing with an acute or short-term illness. People with chronic illnesses face stressors, such as changes in life-style necessitated by the illness, disruption Of vocational and social roles, threats to self- esteem and body image, and a variety of psychological responses including anxiety, depression, anger, and helplessness (Abram, 1972; Doehrman, 1977; Visotsky et al., 1961; Westbrook and Viney, 1982). Adjustment to an illness which is chronic may require considerable coping effort. Evidence of the effort needed to cope with chronic illnesses is provided by the increasing frequency of support groups for such diseases as diabetes and heart disease. However, the strategies employed to cope with chronic illness have received littleattention to date.
The purpose of the current study is to examine these coping mechan- isms involved in chronic illness. Because coping is a complex and mul- tifaceted process the current study employs an assessment battery to investigate a range of coping strategies.
Coping is defined as "any and all responses made by an individual who encounters a potentially harmful outcome" (Silver and Wortman, 1980). Lazarus defines two major functions of coping, coping that is directed at managing or changing the source of the stress and coping that is directed at managing the emotional response to the problem. These two types of coping are called problem-focused and emotion-focused coping, respective- ly (Folkman and Lazarus, 1980). These two functions can include both cog- nitive and behavioral strategies. Although there have been a few efforts to assess Lazarus' coping paradigm, such research is in its early stages. Lazarus has developed a structured scale, the Ways of Coping scale, based on his theoretic framework and classifications provided by Sidle et al. (1969), Weisman and Worden (1976), and Mechanic (1962). Folkman and Lazarus (1980) employed this scale to assess coping with stressful episodes monthly for 1 year. Results indicated that both problem-focused and emotion- focused coping was used in 98% of the stressful episodes. Work-related epi- sodes were more significantly related to a greater frequency of problem- focused coping, and health episodes with increased emotion-focused cop- ing. Aldwin et al. (1980) factor-analyzed the Ways of Coping scale into seven subscales. Coyne et al. (1981) administered this factor-analyzed scale to the same sample, divided into depressed and nondepressed subjects, and assessed coping for a 1-year period. Results indicated that depressed sub- jects used significantly more wishful thinking and seeking of emotional sup- port. Item-level analyses indicated that depressives were more likely to go
Coping with Herpes 393
over a problem again and again, to wish they were a stronger person, to wish they could change the way they felt, and to talk to someone about the way they felt.
In addition to the basic coping strategies assessed by Lazarus, four ad- ditional approaches to coping were considered important. Social support has been considered a major mediator between stress and its effects (Pearlin et al., 1981). While social support is a complex construct, there is evidence that it is the subjective belief that one is supported, satisfaction with sup- port, that decreases psychological stress (Cohen and McKay, 1983; Sandler and Barrera, 1984). When the stressor is a chronic illness, the emotional support provided by interpersonal relationships is a significant resource in coping with the threat to self-esteem and emotional well-being presented by the stressor. Berle et al. (1962) found that the emotional support from par- ents and spouses was related to improvement in physical symptoms in pa- tients with various stress diseases (asthma, migraine headache, peptic ulcer). Higher levels of social support were associated with lower doses of medica- tion for people with asthma, and these subjects also had a better prognosis, as measured by a number of symptoms (De Araujo et al., 1976). DeNour and Czackes (1976) found that the opportunity for expression of feelings was a crucial factor in adjustment to l(idney dialysis, and Diamond (1979) also found social support (family cohesion, spouse support, and expression of feelings in the family) significantly positively correlated with measures of morale and social functioning. Other investigators have found support to be an important factor in adjustment to mastectomy (Bloom et al., 1979) and major burns (Davidson et al., 1979).
Another coping strategy that may be important in coping with chronic illness is causal attribution. Bulman and Wortman (1977) initially inves- tigated the influence of attribution on adjustment, examining people who had been paralyzed in serious accidents. Level of adjustment was assessed by the judgments of the social worker assigned to each subject. Results in- dicated that attribution of blame to others was the best predictor of poor coping. However, self-blame was positively correlated with effective cop- ing. This result contradicted other literature, which suggested self-blame is correlated with depression (Abramson et al., 1978). Janoff-Bulman (1979) explained this incongruity by differentiating two types of blame, charac- terological and behavioral. Characterological self-blame (CSB) is attribut- ing causality to uncontrollable, nonmodifiable traits of one's character, and behavioral self-blame (BSB) is attributing blame to controllable, modifiable behaviors. Janoff-Bulman (1979) proposes that it is characterological self- blame that is associated with depression, not behavioral self-blame. Research by Jar/off-Bulman (1979) Peterson et al. (1979), and Feather
394 Manne and Sandier
(1983) indicates that CSB is employed more by depressed than nondepressed people and is correlated highly with low self-esteem.
Cognitive coping has an important part in restoring psychological health (Horowitz, 1976). Recent evidence has indicated that negative thoughts may have a more important role in predicting psychological symp- tomatology. Sandler (1982) assessed stressful cognitions and coping or posi- tive cognitions and their relationship with psychological measures. Stress and coping thoughts both correlated positively With symptomatology, but stress thoughts were a stronger predictor. Goodhardt (1982) assessed posi- tive and negative thinking about event outcomes and correlated them with measures of well-being, measured longitudinally. Negative thinking was a stronger predictor of well-being over time than positive thinking. Similar results have been reported by Vinokur and Selzer (1975) and Beckham and Adams (1982).
A final important way of coping is the use of disease management strategies. This is a term introduced by the authors. It is a subset of Lazarus' concept of problem-focused coping, applied to the situation of coping with illness. Disease management strategies are defined as efforts to control a disease. One application of this concept is to the situation of chronic illness, when a person may engage in many types of life-style changes in order to manage a disease. For example, when a person has diabetes, he/she needs to make dietary changes in order to manage the diabetes. However, some- times a person with a chronic illness may attempt to cure the disease by con- tinual and repeated attempts to treat it. Often the probability o f the success of these efforts is low. When the person continues to focus on treating his/her disease, these efforts may begin to interfere with other, productive aspects of his/her life. These efforts to control may effect the person's ad- justment in two ways. On the one hand, they may reduce feelings of depres- sion or hopelessness, because the person feels he/she is taking action to deal with the problem. However, as Bulman and Brickman (1982) have pointed out, persistence in efforts to control an uncontrollable outcome can also lead to serious negative effects including increased stress and stress-related diseases, not engaging in more productive alternative behaviors, and wast- ing a great deal of time and energy.
When considering a chronic illness to examine, the authors wanted to choose an incurable illness which represented some unique psychological problems. Genital herpes represented such a situation. In addition to being incurable, it is sexually transmitted, is probably stress related, and can have a great deal of emotional impact upon the person who contracts it. Although the topic of a plethora of popular literature, empirical studies delineating the effects of coping strategies have been negligible.
Coping with Herpes 395
During the past 6 years, the incidence of genital herpes has increased to epidemic proportions. The Center of Disease Control has recently esti- mated that 3 to 20 million people suffer with genital herpes, with an esti- mated 400,000 cases added to the total annually (Genital Herpes Infec- t i o n - U n i t e d States, 1966-1979, 1982). Genital herpes is caused by a virus named herpes simplex virus hominis. It is a recurrent virus, in the majority of the people with herpes, and the virus relocates to the base of the spinal cord between recurrences. There are two major medical problems associat- ed with herpes, both pertaining to women. Cervical cancer is five to eight times more f requent in women with genital herpes (Rawls et al., 1969) and herpes simplex carl be passed on to a newborn child by a mother who has an active cervical or external outbreak during deli.very. The mortality rate of these infants is about 50% (Nahmias et al., 1971).
Many aspects of the disease can cause psychological effects. Luby and Gillespie (1981) described a sequence of responses to herpes observed by cli- nicians: (1) initial shock and emotional numbing; (2) a frantic search for an immediate cure; (3) a sense of isolation and loneliness when the person be- comes aware of the chronicity of the disease; (4) anger directed at the person who is the source of the infection; (5) fear about the consequence of the dis- ease upon sexuality; (6) a leper effect, feelings of ugliness and contamina- tion; (7) feelings of depression over time; and (8) reactivation of underlying psychopathology, in rare cases (Luby and Gillespie, 1981).
Stubbs (1981) has studied psychological reactions to herpes. The majority of those studied perceived herpes as having a negative effect on their self-worth. Most felt herpes had decreased their enjoyment of sexual activities and their perception of themselves as sexually desirable; 38% of the subjects indicated herpes caused them to be "very depressed" at times.
It is apparent that herpes is a stressful experience for many of those who contract it. It also seems that herpes represents an appropriate paradigm for the application of the concepts of coping with chronic illness. The present study has two purposes: (1) to investigate how people cope with herpes and (2) to correlate these coping mechanisms with measures of ad- justment. There are some basic predictions that will be investigated and cor- related with adjustment. Higher levels of psychological symptomatology are predicted to be correlated with the coping strategies of characterological self-blame, wishful thinking, use of disease management strategies, "stress thoughts," and the perception that family, friends, and others have a nega- tive attitude toward the subject. Females are predicted to have higher levels of symptomatology, because herpes poses a greater medical threat to wom- en. Lower levels of pathology are predicted to be related to using the strate- gy of minimizing the threat posed by herpes, the use of problem-focused
396 Manne and Sandier
coping, and a higher perceived frequency of and satisfaction with social support. In addition, those with less severe herpes infections and those who have had herpes a greater length of time will evidence lower levels of psy- chological symptomatology.
M E T H O D
Subjects and P r o c e d u r e
Subjects were drawn from herpes self-help groups and volunteer sub- jects not affiliated with self-help groups, Self-help-group members were from eight different groups around the country, Volunteers were people who responded to newspaper advertisements in the Phoenix area. There were 116 self-help-group subjects and 36 volunteers, making a total of 152 subjects in the study. Approximately 70 help-group members were ad- ministered the questionnaire at meetings of their help groups. The re- mainder of the help-group subjects and all volunteers were sent the questionnaires through the mail,
lns l rumentat ion
Basic Information. Demographic information was collected pertain- ing to age, gender, race, marital status, and income level. Information was also collected on the subject's herpes disease: the source of their infection, how long they had herpes, the average number of outbreaks per year, and the average length of time the herpes outbreaks lasted. The subjects were asked how many different sexual partners they had in the year previous to contracting herpes. They were also asked about the amount of information they read or saw on television concerning herpes before they contracted it. On this scale, subjects were given a choice on a six-point scale, from a little to a great deal of information concerning herpes.
Attitude of Others. The attitude of others toward the subject who has herpes was assessed by a six-point rating scale of (1) how coldly the other person acted, (2) how much the person blamed the subject for getting herpes, and (3) how accepting of the subject the person was. Subjects rated family, friends, and medical workers on this scale.
Social Support. The amount of perceived social support in relation to herpes was assessed by having the subject rate how much support he/she had received from family, friends, spouse, doctors, and community resources. Each source of support was rated separately. The subjects also rated how helpful the social support was that they received.
Coping with Herpes 397
Coping Variables. Three coping variables were assessed: wishful thinking, minimization of threat, and problem-focused coping. The items were derived from the Ways of Coping scale (Folkman and Lazarus, 1980). Items were selected if they fit three criteria: (1) loading above 0.30 on its factor in the factor analysis done by Aldwin et al. (1980); (2) being chosen by the author as appropriate to coping with herpes and rewritten to make the item role relevant [for example, the item, "wished the situation would go away or somehow be over with" was changed to add, "wished the situa- tion (having herpes) would go away or somehow be over with"]; and (3) be- ing rated by 80~ of 25 graduate students at Arizona State University as fitting the operational definition of either wishful thinking, problem- focused coping, or minimization of threat. Eight items were included on the wishful thinking scale, nine on the problem-focused coping scale, and eight on the minimization of threat scale. An example of a problem-focused cop- ing item is, "Changed something so things would turn out better." An exam- ple of a minimization of threat item is, "Didn't let it get to you."
Disease Management Strategies. Disease management was defined as efforts to treat or manage herpes. The items for this scale were composed by the first author and based on a review of the literature on treatment ef- forts of herpes patients. Subjects were asked to list the number of treat- ments, stress reduction techniques, and number of dietary changes tried, as well as the number of doctors and clinics visited in the past year concerning herpes.
Attribution o f Blame. Attribution was divided into internal and exter- nal attribution, characterological self-blame (CSB) and behavioral self- blame (BSB) were internal attributions, and blame on bad luck and blame on the person who gave the subject herpes were external attributions. All items were generated by the first author. Five items each were on the CSB scale and BSB scales, one item assessed bad luck, and one item assessed ex- ternal blame. For example, characterological self-blame was assessed by an item, "I am a loose or promiscuous person." Items were rated from 0 ("never think this is a reason why I got herpes") to 3 ("often think this is a reason why I got herpes").
Stress Thoughts. The stress thoughts scale was developed to assess how often subjects thought about negative aspects of having herpes. Items for this scale were composed by the first author and consisted of common concerns associated with having herpes (i.e., "I worry others know I have herpes, when they do not know I have it"). There were 14 items on this scale. Subjects rated how frequently they had engaged in these worries dur- ing the previous month on a four-point scale.
Adjustment Measures. Four measures of adjustment were employed in the present study: measures of self-esteem, depression, sexual problems, and degree to which the subject is bothered by having herpes.
398 Manne and Sandier
Self-Esteem. Self-esteem was assessed by the Rosenberg self-esteem scale (Rosenberg, 1965). The scale measures the self-acceptance component of self-esteem. It is a widely used 10-item Guttman scale, with items mea- sured on a four-point continuum from "strongly agree" to "strongly dis- agree." Reliability of the scale has been found to be satisfactory [internal consistency = 0.92; test-retest reliability over a 2-week period = 0.85 (Rosenberg, 1965)]. The Rosenberg scale correlated from 0.56 with clinical interview results, and Robinson and Shaver (1973) report correlations from 0.27 to 0.66 with other self-image scales. The scale was scored by summing across the entire 10 items to yield a single total score. This method of scor- ing the scale is recommended as one of the valid alternatives by Crandall (cited by Robinson and Shaver, 1973).
Depression. The current study employed the Beck Depression Invento- ry (Beck et al., 1961). It is a self-report inventory with 21 items of symptoms and attitudes related to depression. Split-half reliability of the scale was reported by Beck et al. (1961) using 226 psychiatric outpatients, with coeffi- cients ranging from 0.86 to 0.93. Validation of the inventory against clinical ratings of depth of depression indicated a progressively higher mean score on the Beck Depression Inventory as clinical ratings of depression became more severe. Scoring of the inventory is a simple summation of the category item scores to a total score. The cutoff for a diagnosis of clinical depression is 17 (Beck et al., 1961).
Sexual Problems. This scale assessed difficulties in sexual functioning, sexual satisfaction, and self-perceptions about sexuality. Eight of the items from this scale were drawn from Stubbs' (1981) survey of herpes subjects. Two items were constructed by the first author in order to 'assess aspects of sexual functioning not addressed by Stubbs (1981). Each item was rated on a five-point scale, with ratings ranging from "greatly decreased" to "greatly increased." The items were summed to compose a total score on the scale.
Amount Bothered by Herpes. The degree to which each subject was bothered by having herpes was assessed by a single seven-point scale, which ranged from "This is only a minor annoyance" to "This is the worst thing that's ever happened to me." A higher score indicated that the subject was more upset by herpes.
Reliability o f Measures. Because many of the scales were composed by the authors especially for this study, it was necessary to assess the psycho- metric properties of the scales. Coefficient alpha estimates of these scales ranged from 0.43 to 0.89; with the perceived social support scale producing the lowest estimate and the stress thoughts and sexual problems scales producing the highest alpha. The social support scale had the lowest relia- bility estimate because the scale was based on ratings from different sources of support, and ratings varied widely. The reliability of each of the scales is as follows: social support, 0.43; helpfulness of support, 0.65; minimiza-
Coping with Herpes 399
tion of threat, 0.58; problem-focused coping, 0.68; wishful thinking, 0.77; characterological self-blame, 0.65; behavioral self-blame, 0.71; stress thoughts, 0.89; sexual problems, 0.89; and attitude of others toward the subject, 0.76.
Preliminary Analysis
Characteristics of the Sample. Over half of the sample was female (61%). Ha l f of the sample was single, and 36% were divorced or separated. The mean age was 33.4 years. The majori ty o f the sample was Caucasian (91%). The mean amount of time for having herpes was 62 months; however, a few subjects who contracted herpes at an early age biased the sample. The median of 50 months is a more accurate representation of the central tendency. The mean number of herpes outbreaks per year for sub- jects who had herpes less than a year was 8, and for subjects who had herpes more than a year, the mean was 10. The mean duration of herpes outbreaks was 9.5 days, with a median of 7 days.
Adjustment Scale. Because of the high intercorrelations between the dependent measures (7 = 0.42), the four dependent variables were Con- verted into z scores and summed into a single overall "adjustment" scale. Higher scores on the scale indicate more difficulty adjusting to herpes.
Demographic Characteristics. Of 60 comparisons made, only five sig- nificant relationships were found between coping strategies and demo- graphic variables. Females reported more external blame on the person f rom whom they contracted herpes (r = 0.14, P < 0.05). Older subjects engaged in less wishful thinking (r = 0.15, P < 0.05). Partialing out the effect of length of infection and external blame (r = 0.13, P < 0.05) decreased both correlations to nonsignificant levels. Older subjects engaged in less CSB, and this relationship remained significant after the length of infection was partialed out (r = 0.21, P < 0.01). Married subjects received significantly more social support than single or divorced subjects (F = 5.85, df = 144, P < 0.01). Post hoc comparison of groups using the Tukey test indicated that married subjects had significantly better adjustment than sin- gle or divorced subjects (F = 3.6, df = 143, P < 0.05).
Help vs. Volunteer Subject Comparisons. Self-help-group members were significantly older (r = - 0 . 3 2 , P < 0.01), were more educated (Mann-Whi tney Utes t , z = - 2 . 1 5 , P < 0.05), and had a higher level of income (Mann-Whi tney U test, z = 4.1, P < 0.001). Help-group members coped differently than volunteers. They received more social support, did more problem-focused coping and more wishful thinking, and used more disease management strategies, more CSB and more blame on others. However, no differences on any adjustment measures were found.
Tab
le I
. C
orr
ela
tio
ns
Am
on
g
Ind
ep
en
de
nt
Var
iab
les
SS
H
elp
P
F
WT
M
IN
Man
age
CS
B
BS
B
Lu
ck
Oth
er
ST
Soc
ial
Su
pp
ort
(S
S)
Hel
pfu
lnes
s (H
elp
) 0
.57
**
*
Pro
ble
m-F
ocu
sed
Co
pin
g (
PF
) 0
.25
**
W
ish
ful
Th
ink
ing
(W
T)
0.0
9
Min
imiz
atio
n (
MIN
) -
0.16
* D
isea
se M
anag
emen
t (M
anag
e)
- 0.
10
Ch
arac
tero
log
ical
S
elf-
Bla
me
(CS
B)
0.1
0
Beh
avio
ral
Sel
f-B
lam
e (B
SB
) 0.
05
Bla
me
on
B
ad
Lu
ck (
Lu
ck)
0.0
2
Bla
me
on
Oth
er P
erso
n (
Oth
er)
0.0
8
Str
ess
Th
ou
gh
ts (
ST
) -
0.1
7"
0.20
".
- 0
.18
" 0
.27
**
*
- 0.
10
- 0.
02
0.07
0.
01
0.24
**
0.3
4*
**
0
.06
0.12
0.
02
0.5
3*
**
0.
12
0.3
5*
**
0.
05
0.0
6
0.1
9
0.11
0
.08
0
.02
0
.10
0
.55
**
*
0.08
0
.16
" -0
.05
0.
13
0.3
9*
**
0.
05
0.05
-
0.11
0
.06
0
.54
**
*
0.0
6
0.3
4*
**
0.4
5*
**
0
.38
**
*
0.0
4
0.3
2*
**
0
.30
**
*
0.22
**
0.4
5*
**
0
.27
**
*
0.2
7*
**
0
.43
***
*P
<
0
.05
. *
*P
<
0
.01
. *
**
P
<
0.0
01
.
Coping with Herpes 401
Since there were some differences between heip-group members and volunteers, the correlational analyses were initially done separately. However, since the zero-order correlations were very similar across the two groups, the results from the total combined sample will be presented.
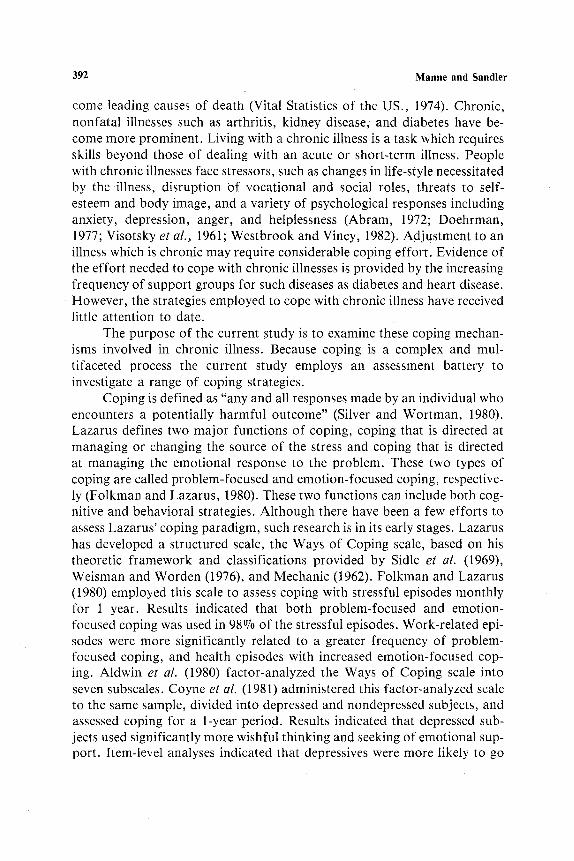
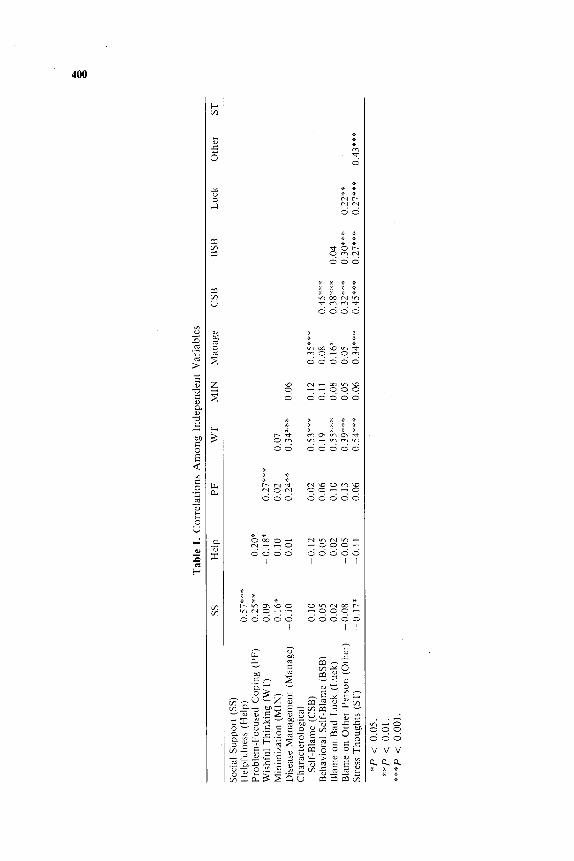
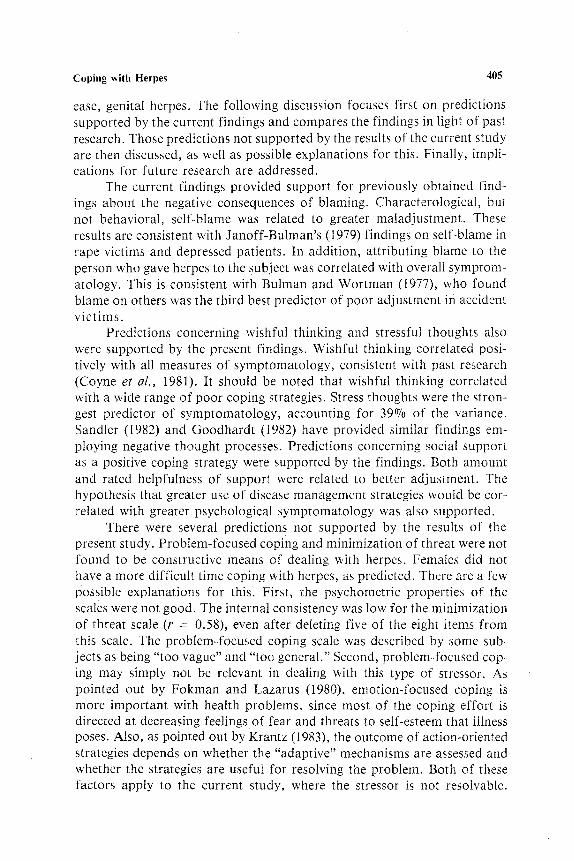
Correlations Among Coping Variables. Of 55 correlations, 16 were significant. Table I shows the intercorreIations among the coping variables. The social support variables are highly intercorrelated (r = 0.57, P < 0.001). Most of the attribution variables, except for behavioral self-blame, were significantly intercorrelated. These attribution variables were corre- lated with wishful thinking and stress thoughts. Wishful thinking and stress thoughts were significantly correlated (r = 0.54, P < 0.001). Perceived amount of social support and stress thoughts were negatively correlated (r = -0 .17 , P < 0.05).
Relationship of Coping to Adjustment
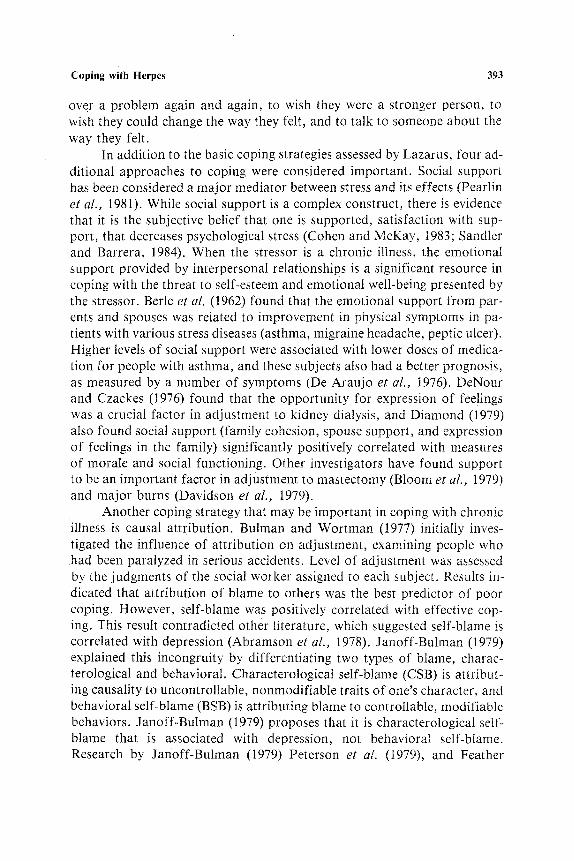
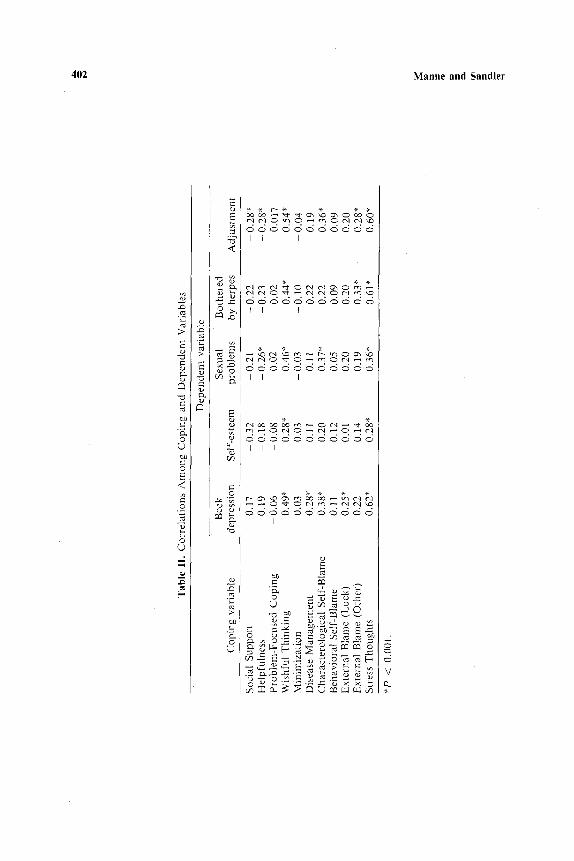
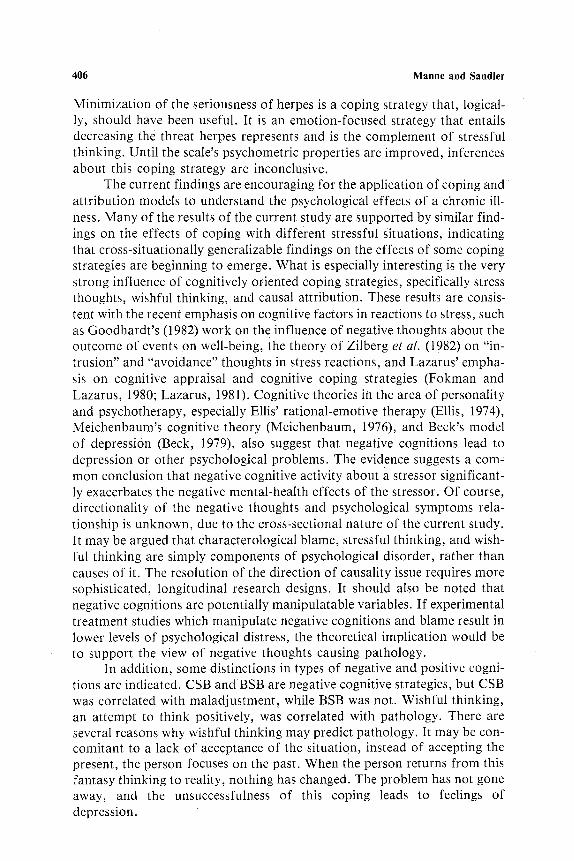
Correlations between the 11 independent variables and the 5 depen- dent variables (including overall adjustment) were carried out, making a to- tal of 55 correlations. In order to control for Type I error introduced by these multiple correlations, the multistage Boneferoni procedure (Larzelere and Mulaik, 1977) was employed. This procedure is performed by dividing the significance level for each test (0.05) by the number of correlations done, to determine a significance level. If none of the tests in the group is significant at this level, the procedure is discontinued. However, if one finds a significant test, then a second stage is begun. The significance level is reset to the initial significance level divided by the number of correlations re- maining after stage one. With this procedure, the probability of a Type I error is controlled at a level no greater than 0.05. Employing this procedure, the final significance level was 0.0015. Of 55 comparisons between coping and adjustment, 21 were significant, as can be seen in Table lI. Higher lev- els of social support were correlated with less symptomatology and better self-esteem. The perceived helpfulness of support was correlated with better overall adjustment and fewer sexual problems. In addition, those who per- ceived the attitude of family, friends, and medical workers as more negative reported a greater degree of depression (r = 0.24, P < 0.05), more sexual problems (r = 0.27, P < 0.05), poorer self-esteem (r = 0.32, P < 0.01), and poorer overall adjustment (r = 0.26, P < 0.05). Problem-focused cop- ing and minimization of threat were not correlated significantly with any of the adjustment measures. Wishful thinking was highly correlated with all measures of maladjustment. Depression was significantly correlated with engaging in a high level of disease management strategies (P < 0.0015). Greater use of disease management strategies was not correlated significant-
a~
1,4
Tab
le
I1.
Co
rrel
atio
ns
Am
on
g
Co
pin
g
and
D
epen
den
t V
aria
ble
s
Co
pin
g
var
iab
le
Dep
end
ent
var
iab
le
Bec
k
Sex
ual
B
oth
ered
d
epre
ssio
n
Sel
f-es
teem
p
rob
lem
s b
y h
erp
es
Ad
just
men
t
So
cial
S
up
po
rt
- 0
.17
0
.32
0.
21
- 0
.22
-
0.2
8*
H
elp
fuln
ess
0.1
9
0.18
-
0.2
6*
-
0.23
-
0.2
8*
P
rob
lem
-Fo
cuse
d
Co
pin
g
- 0
.06
-
0.0
8
0.0
2
0.0
2
0.0
17
W
ish
ful
Th
ink
ing
0.
49*
0.28
* 0
.46
*
0.4
4*
0
.54
*
Min
imiz
atio
n
0.0
3
0.03
-
0.0
3
- 0
.10
-
0.0
4
Dis
ease
M
anag
emen
t 0
.28
*
0.11
0.
11
0,2
2
0.1
9
Ch
arac
tero
log
ical
S
elf-
Bla
me
0.38
* 0
.20
0
.37
*
0.2
2
0.3
6*
B
ehav
iora
l S
elf-
Bla
me
0.11
0
.12
0
.05
0
.09
0
.09
E
xte
rnal
B
lam
e (L
uck
) 0
.25
*
0.01
0
.20
0
.20
0
.20
E
xte
rnal
B
lam
e (O
ther
) 0
,22
0
.14
0
.19
0
.33
*
0.2
8*
S
tres
s T
ho
ug
hts
0
.62
*
0.2
8*
0
.36
*
0,61
*
0.6
0*
*P
<
0.00
1.
m_
m_
Coping with Herpes 403
ly with overall maladjustment at the P < 0.0015 level, but the relationship was significant at the P < 0.05 level.
Relationship of Causal Attribution to Adjustment
Characterological self-blame was correlated positively with all mea- sures of symptomatology. Behavioral self-blame was not significantly cor- related with any measure of adjustment. There was a significant difference between the characterological and behavioral self-blame correlations and the Beck Depression score (Hotelling's t test, t = 3.37, P < 0.005) and the sexual problems scale (Hotelling's t test, t = 4.0, P < 0.005). Attr ibution of blame to the person who gave the subject herpes was correlated signifi- cantly with maladjustment .
Relationship of Stress Thoughts to Adjustment
Stress thoughts were significantly correlated with all measures of maladjustment, as can be seen in Table II. More stress thoughts concern- ing herpes correlated with greater levels of depression, poorer self-esteem, more sexual problems, and being more bothered by herpes.
Effects of Greater Severity of Herpes Infection
Results indicate that, the longer the subjects had herpes, the less depressed and less bothered they were by it (r = - 0.17, P < 0.05). These sub- jects also used less stress thoughts (r = - 0 . 2 4 , P < 0.01). The average number of outbreaks per year did not contribute to any differences in ad- justment when the subject had contracted herpes less than a year ago. More outbreaks in the first year of contracting herpes were correlated with a greater number of stress thoughts. In those who had herpes more than a year, more outbreaks correlated with more depression (r = 0.17, P < 0.05) and poorer self-esteem (r = 0.16, P < 0.05). There were no differences in adjustment in those subjects with a greater duration of herpes outbreaks.
Regression Analyses
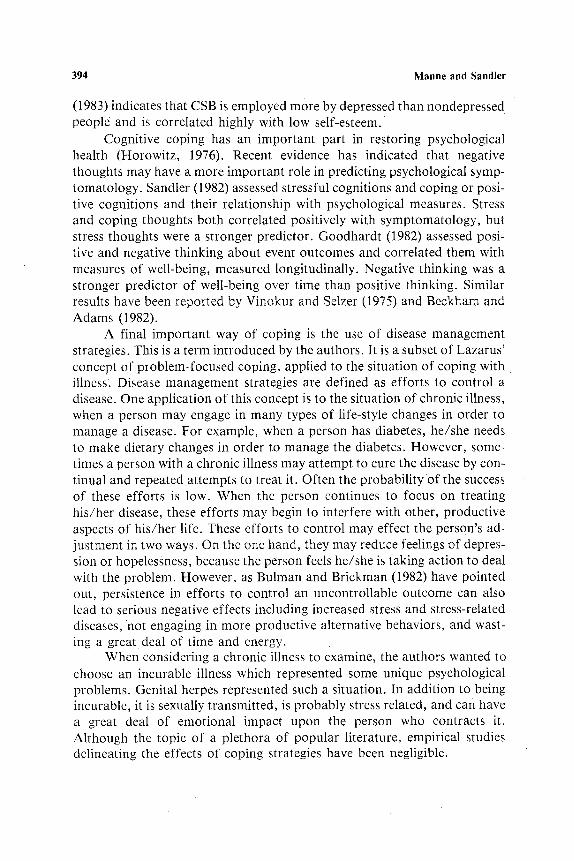
Regression analyses were conducted to determine how well the total group of coping variables could predict symptomatology. Results for the to- tal sample are shown in Table III . Regression analysis indicated that stress
404 Manne and Sandier
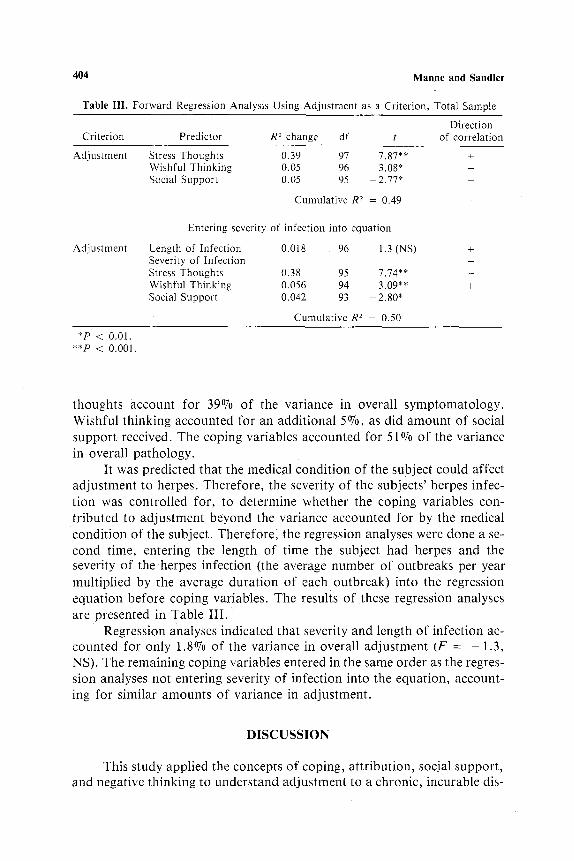
Table II1. Forward Regression Analysis Using Adjustment as a Criterion, Total Sample
Direction Criterion Predictor R 2 change df t of correlation
Adjustment Stress Thoughts 0.39 97 7.87** + Wishful Thinking 0.05 96 3.08* + Social Support 0.05 95 - 2.77* -
Adjustment
Cumulative R 2 = 0.49
Entering severity of infection into equation
Length of Infection 0.018 96 - 1.3 (NS) + Severity of Infection Stress Thoughts 0.38 95 7.74** - Wishful Thinking 0.056 94 3.09** + Social Support 0.042 93 2.80*
Cumulative R 2 = 0.50
*P < 0.01. **P < 0.001.
thoughts account for 39% of the variance in overall symptomatology. Wishful thinking accounted for an additional 5~ as did amount of social support, received. The coping variables accounted for 51% of the variance in overall pathology.
It was predicted that the medical condition of the subject could affect adjustment to herpes. Therefore, the severity of the subjects' herpes infec- tion was controlled for, to determine whether the coping variables con- tributed to adjustment beyond the variance accounted for by the medical condition of the subject. Therefore; the regression analyses were done a se- cond time, entering the length of time the subject had herpes and the severity of the herpes infection (the average number of outbreaks per year multiplied by the average duration of each outbreak) into the regression equation before coping variables. The results of these regression analyses are presented in Table III.
Regression analyses indicated that severity and length of infection ac- counted for only 1.8% of the variance in overall adjustment (F = - 1.3, NS). The remaining coping variables entered in the same order as the regres- sion analyses not entering severity of infection into the equation, account- ing for similar amounts of variance in adjustment.
D I S C U S S I O N
This study applied the concepts of coping, attribution, soc.ial support, and negative thinking to understand adjustment to a chronic, incurable dis-
Coping with Herpes 405
ease, genital herpes. The following discussion focuses first on predictions supported by the current findings and compares the findings in light of past research. Those predictions not supported by the results of the current study are then discussed, as well as possible explanations for this. Finally, impli- cations for future research are addressed.
The current findings provided support for previously obtained find- ings about the negative consequences of blaming. Characterological, but not behavioral, self-blame was related to greater maladjustment. These results are consistent with Janoff-Bulman's (1979) findings on self-blame in rape victims and depressed patients. In addition, attributing blame to the person who gave herpes to the subject was correlated with overall symptom- atology. This is consistent with Bulman and Wortman (1977), who found blame on others was the third best predictor of poor adjustment in accident vict ims.
Predictions concerning wishful thinking and stressful thoughts also were supported by the present findings. Wishful thinking correlated posi- tively with all measures of symptomatology, consistent with past research (Coyne et al., 1981). It should be noted that wishful thinking correlated with a wide range of poor coping strategies. Stress thoughts were the stron- gest predictor of symptomatology, accounting for 39% of the variance. Sandler (1982) and Goodhardt (1982) have provided similar findings em- ploying negative thought processes. Predictions concerning social support as a positive coping strategy were supported by the findings. Both amount and rated helpfulness of support were related to better adjustment. The hypothesis that greater use of disease management strategies would be cor- related with greater psychological symptomatology was also supported.
There were several predictions not supported by the results of the present study. Problem-focused coping and minimization of threat were not found to be constructive means of dealing with herpes. Females did not have a more difficult time coping with herpes, as predicted. There are a few possible explanations for this. First, the psychometric properties of the scales were not good. The internal consistency was low for the minimization of threat scale (r = 0.58), even after deleting five of the eight items from this scale. The problem-focused coping scale was described by some sub- jects as being "too vague" and "too general." Second, problem-focused cop- ing may simply not be relevant in dealing with this type of stressor. As pointed out by Fokman and Lazarus (1980), emotion-focused coping is more important with health problems, since most of the coping effort is directed at decreasing feelings of fear and threats to self-esteem that illness poses. Also, as pointed out by Krantz (1983), the outcome of action-oriented strategies depends on whether the "adaptive" mechanisms are assessed and whether the strategies are useful for resolving the problem. Both of these factors apply to the current study, where the stressor is not resolvable.
406 Manne and Sandier
Minimization of the seriousness of herpes is a coping strategy that, logical- ly, should have been useful. It is an emotion-focused strategy that entails decreasing the threat herpes represents and is the complement of stressful thinking. Until the scale's psychometric properties are improved, inferences about this coping strategy are inconclusive.
The current findings are encouraging for the application of coping and attribution models to understand the psychological effects of a chronic ill- ness. Many of the results of the current study are supported by similar find- ings on the effects of coping with different stressful Situations, indicating that cross-situationally generalizable findings on the effects of some coping strategies are beginning to emerge. What is especially interesting is the very strong influence of cognitively oriented coping strategies, specifically stress thoughts, wishful thinking, and causal attribution. These results are consis- tent with the recent emphasis on cognitive factors in reactions to stress, such as Goodhardt's (1982) work on the influence of negative thoughts about the outcome of events on well-being, the theory of Zilberg et al. (1982) on "in- trusion" and "avoidance" thoughts in stress reactions, and Lazarus' empha- sis on cognitive appraisal and cognitive coping strategies (Fokman and Lazarus, 1980; Lazarus, 1981). Cognitive theories in the area of personality and psychotherapy, especially Ellis' rational-emotive therapy (Ellis, 1974), Meichenbaum's cognitive theory (Meichenbaum, 1976), and Beck's model of depression (Beck, 1979), also suggest that negative cognitions lead to depression or other psychological problems. The evidence suggests a com- mon conclusion that negative cognitive activity about a stressor significant- ly exacerbates the negative mental-health effects of the stressor. Of course, directionality of the negative thoughts and psychological symptoms rela- tionship is unknown, due to the cross-sectional nature of the current study. It may be argued that characterological blame, stressful thinking, and wish- ful thinking are simply components of psychological disorder, rather than causes of it. The resolution of the direction of causality issue requires more sophisticated, longitudinal research designs. It should also be noted that negative cognitions are potentially manipulatable variables. If experimental treatment studies which manipulate negative cognitions and blame result in lower levels of psychological distress, the theoretical implication would be to support the view of negative thoughts causing pathology.
In addition, some distinctions in types of negative and positive cogni- tions are indicated. CSB and BSB are negative cognitive strategies, but CSB was correlated with maladjustment, while BSB was not. Wishful thinking, an attempt to think positively, was correlated with pathology. There are several reasons why wishful thinking may predict pathology. It may be con- comitant to a lack of acceptance of the situation, instead of accepting the present, the person focuses on the past. When the person returns from this fantasy thinking to reality, nothing has changed. The problem has not gone away, and the unsuccessfulness of this coping leads to feelings of depression.
Coping with Herpes 407
The number of disease management strategies employed was a new coping mechanism introduced in this study. Results indicated that one can try too many ways to resolve a problem, or "obsessively" cope with a problem, when the means of coping is not likely to resolve the stressor. It may relate to psychopathology because, like wishful thinking, it signals a lack of acceptance of the situation. The attempts to gain control of herpes, and the repeated failures to do so, may lead to increased feelings of stress, helplessness, and depression, creating a "learned helplessness" situation (Seligman, 1975). Similar to the suggestion of Bulman and Brickman (1982), the findings suggest that doing something is not always a positive way of coping; on the contrary, it can be detrimental, when the actions taken do not impact on the stressor.
The results of this study have implications for individuals with genital herpes. Those teaching herpes sufferers how to deal with herpes may get better results by training people how not to focus on the negative aspects of herpes, instead of how to think positively. For example, to encounter the characterological self-blame, "Herpes means I'm a loose or promiscuous person." one would teach the rational thought, "Having herpes means noth- ing about my personality. It may be embarrassing, but it does not mean i am a shameful person," approaches similar to the therapy of Beck et al.
1979) or Ellis and Harper (1975). They also suggest that providing social support that is perceived as helpful and not condeming the person for hav- ing herpes are important considerations for treating those upset by herpes. Also, teaching the person not to focus on the past and wish he/she did not get herpes may be helpful. These findings also have implications for treat- ment of people who have encountered stressful events in general. Training individuals to "fight off" negative thoughts may be productive in decreasing feelings of depression and loss of self-esteem. In the specific area of genital herpes, this was one of the first empirical efforts to examine how people deal with herpes. Additional research needs to assess coping over a period of time, as in time-series designs (Cook and Campbell, 1979). Longitudinal assessment would also allow investigation of "stages" of coping over time (Silver and Wortman, 1982).
Further research needs to investigate whether the coping concepts em- ployed in this study apply to other stressors, especially other chronic ill- nesses. There are differences between herpes and other chronic diseases that may impede generalization. Herpes is less painful than many other diseases, it has more social stigma, and there are more psychological factors involved than diseases such as arthritis or heart disease. These differences may make a difference in the generalizability of the findings of this study.
The interrelationship among coping behaviors, psychol()gical sym- ptomatology, and physical symptoms also needs to be addressed. In the cur- rent study, coping behaviors were better predictors of psychological symptoms than was physical symptomatology. These relationships may be different for other diseases, where the social stigma is less, the pain is great-
408 Manne and Sandier
er, or physical degeneration is more of an issue. For example, where physi- cal symptoms also imply that the individual is degenerating, they may have greater psychological impact. Thus, although the current results are consis- tent with literature on coping with other stressors, it may be that different factors are important in coping with different physical illnesses. Identifying the effects of different coping behaviors across a range of chronic diseases is an important priority for future research.
ACKNOWLEDGMENTS
This article is based on a master's thesis submitted in partial fulfill- ment of the requirements for the master's degree at Arizona State Universi- ty. Appreciation is extended to Sandy Braver, Alex Zautra, and John Reich, members of the master's committee.
REFERENCES
Abram, H. (1972). The psychology of chronic illness. J. Chron. Dis. 25: 659-664. Abramson, L., Seligman, M., and Teasdale, J. (1978). Learned helplessness in humans: Cri-
tique and reformulation. J. Abnorm. Psychol. 87: 49-74. Aldwin, C., Folkman, S., Schaefer, C., Coyne, J., and Lazarus, R. (1980). Ways of coping:
A process measure. Paper presented at the American Psychological Association Meet- ing, Montreal.
Beck, A. (1967). Depression: Causes and Treatment, University of Pennsylvania Press, Philadelphia.
Beck, A., Rush, A., Shaw, B., and Emery, G. (1979). Cognitive Therapy o f Depression, Guil- ford Press, New York.
Beck, A., Ward, C., Mendelson, M., Mock, J., and Erbaugh, J. (1961). An inventory for mea- suring depression. Arch. Gen. Psychiat. 4: 561-571.
Beckham, E., and Adams, R. (1982). Measurement of coping behaviors in depression: A report on a new scale. Paper presented at the meeting of the American Psychological Associa- tion, Washington, D.C.
Berle, B., Pinsky, R., Wolf, S., and Wolff, H. (1952). A clinical guide to prognosis in stress diseases. JAMA 149: 1624-1626.
Bloom, J., Ross, R., and Burnell, G. (1979). The effect of social support on patient adjustment after breast surgery. Pat. Counsel. Health Educ. 2: 50-56.
Bulman, R. J., and Brickman, P. (1982). Expectations and what people learn from failure. In Feather, N. T. (ed.), Expectancy, Incentive and Action, Erlbaum, Hillsdale, N.J.
Bulman, R., and Wortman, C. (1977). Attributions of blame and coping in the "real world": Severe accident victims react to their lot. J. Personal. Soc. Psychol. 35: 351-363.
Cohen, S., and McKay, G. (1983). Social support, stress and the buffering hypothesis: An em- pirical review. In Baum, A., et al. (eds.), Handbook o f Psychology and Health, Vol. IV, Erlbaum, Hillsdale, N.J.
Cook, T., and Campbell, D. (1979). Quasi-Experimentation: Design and Analysis for FieM Set- tings, Houghton-Mifflin, Boston.
Coyne, J., Aldwin, C., and Lazarus, R. (1981). Depression and coping in stressful episodes. J. Abnorm. Psychol. 90: 439-447.
Coping with Herpes 409
Davidson, T., Bowden, L., and Tholen, D. (1979). Social support as a moderator of burn re- habilitation. Arch. Phys. Med. Rehab. 60: 556.
De Araujo, G., van Arsdael, P., Holmes, T., and Dudley, D. (1973). Life change, coping abili- ty and chronic intrinsic asthma. J. Psychosom. Res. 17: 359-353.
De Nour, A., and Czackes, J. (1976). The influence of patient's personality on adjustment to chronic dialysis. J. Nerv. Mont. Dis. 162: 323-333.
Dimond; M. (1979). Social support and adaptation to chronic illness: The case of maintenance hemodialysis. Res. Nuts. Health 2: t01-108.
Doehrman, S. (1977). Psychosocial aspects of recovery from heart disease: A review. Sac. Sci. Meal. 11: 199-218.
Ellis, A. (1974). Rational-emotive therapy. In Burton, A. fed.), Operational Theories o f Perso- nality, Brunner-Mazel, New York.
Ellis, A., and Harper, R. (1975). A New Guide to Rational Living, Prentice*Hall, Englewood Cliffs, N.J.
Feather, N. (1983). Some correlates of attributional style. Personal. Sac. Psychol. Bull. 9: 125-135. Folkman, S., and Lazarus, R. (1980). An analysis of coping in a middle-aged community sam-
ple. J. Health Sac. Behav. 21: 219-239. Genital Herpes Infection-United States, 1966-t979 (I982). Morbid. Mortal Week. Rep. 3i:
137-139. Goodhardt, D. (1982). Some psychological effects associated with positive and negative think-
ing about stressful event outcomes: Was Pollyanna right? Unpublished manuscript. Horowitz, M. (1976). Stress Response Syndromes, Aronson, New York. Janoff-Bulman, R. (1979). Characterological versus behavioral self-blame: Inquiries into depres-
sion and rape. J, Personal. Sac. Psychol. 37: 1798-1809. Krantz, S. (t983). Cognitive appraisals and problem-directed coping: A prospective study of
stress. J. Personal. Sac. Psychol. 14: 638-643. Larzelere, R., and Mulaik, S. (1977). Single sample tests for many correlations. Psychol. Bull.
84: 557-569. Lazarus, R. (1981). The stress and coping paradigm. In Eisdorfer, C., Cohen, D., Kleinman,
A., and Maxim, P. (eds.), Models for Clinical Psychopathology, Spectrum, New York. Luby, E., and Gillespie, O. (1981). Psychological responses to genital herpes. Helper 3: 2-3. Mechanic, D. (1962). Students Under Stress: A Study in the Social Psychology o f Adaptation,
The Free Press, Glencoe, Ill. Meichenbaum, D. (1976). Cognitive behavior modification. In Spence, J., Carson, R., and
Thibaut, J. (eds.), Behavioral Approaches to Therapy, General Learning Press, Mor- ristown, N.J.
Nahmias, A., Josey, W., and Naib, Z. (1971). Perinalal risk associated with maternal genital herpes simplex virus infection. Am. J. Obstet. Gylwco/. It0: 825-834.
Pearlin, L., Lieberman, M., Menaghen, E., and Mullah, J. (1981). The stress process. J. Health Sac. Behav. 22: 337-356.
Peterson, C., Schwartz, L., and Seligman, M. (1981). Self-blame and depressive symptoms. J. Personal. Sac. Psychol. 41: 253-259.
Rawls, W., Tompkins, W., and Melnick, J. (1969). The association of herpes virus Type 2 and carcinoma of the uterine cervix. Am. J. Epidemiol. 89: 547-554.
Rosenberg, M. (1965). Society and the Adolescent Self-Image, Princeton University Press, Prince- ton, N.J.
Sandler, I. (1982). Cognitive correlates of negative ]ire events and social support as an approach to understanding the stress buffering effect, la Caplan, R. (Chair), Social Support as a Stress Buffer, Symposium presented at the meeting of the American Psychological As- sociation, Washington, D.C.
Sandler, I , and Barrera, M. (1984). Social support as a stress buffer: A multlmethod investiga- tion. Am. J. Comrnun. Psychol. 12: 37-52.
Seligman, M. (1975). Helplessness: On Depression, Development and Death, Freeman Press, San Francisco.
Sidle, A., Moos, R., Adams, J., and Cady, P. (1969). Development of a coping scale. Arch. Gen. Psychiat. 20: 226-232.
410 Manne and Sandier
Silver, R. and Wortman, C. (1980). Coping with undesirable life events. In Garber, E., and Seligman, M. (eds.), Human Helplessness, Academic Press, New York.
Stubbs, J. (1981). Psychological and social consequences of recurrent genital herpes, Unpub- lished manuscript.
Vinokur, A., and Selzer, M. (1975). Desirable versus undesirable life events: Their relation- ship to stress and mental distress. J. Personal. Soc. Psychol. 32: 329-337.
Visatsky, B., Hamburg, D., Goss, M., and Libovits, B. (1961). Coping behavior under extreme stress. Arch. Gen. Psychiat. 5: 27-52.
Vital Statistics of the U.S. (1974). VoI. 22 (No. 13). Westbrook, M., and Viney, L. (1982). Psychological reactions to the onset of chronic illness.
Soc. Sci. Med. 16: 899-905. Weisman, W., and Worden, J. (1976). The existential plight in cancer: Significance of the first
100 days. Int. J. Psychiat. Med. 7: 1-15. Zilberg, N., Weiss, D., and Horowitz, M. (1982). Impact of event scale: A cross-validation
study of some empirical evidence suggesting a conceptual model of stress response syn- dromes. J. Clin. Consult. Psychol. 50: 407-416.