17
1 Nose & Sinuses- OSCE Leader: Maha Allhaidan Done by: Arwa Almashaan Reem Aljubab Shaikha AlDossari Tahani AlShaibani Lama Alotaibi Hind almuhaya Reem Alhefdhi
| Date post: | 10-Jan-2023 |
| Category: |
Documents |
| Upload: | khangminh22 |
| View: | 0 times |
| Download: | 0 times |
1
Nose & Sinuses- OSCE
Leader: Maha Al lhaidan
Done by:
Arwa Almashaan Reem Aljubab
Shaikha AlDossari Tahani AlShaibani
Lama Alotaibi Hind almuhaya Reem Alhefdhi
2
Nose Examination ………………………3 Nasal block history …………………….5 Sinusitis…………………………………9 Epistaxis history ……………………….12 Rhinitis history …………………………14
CONTENTS:
3
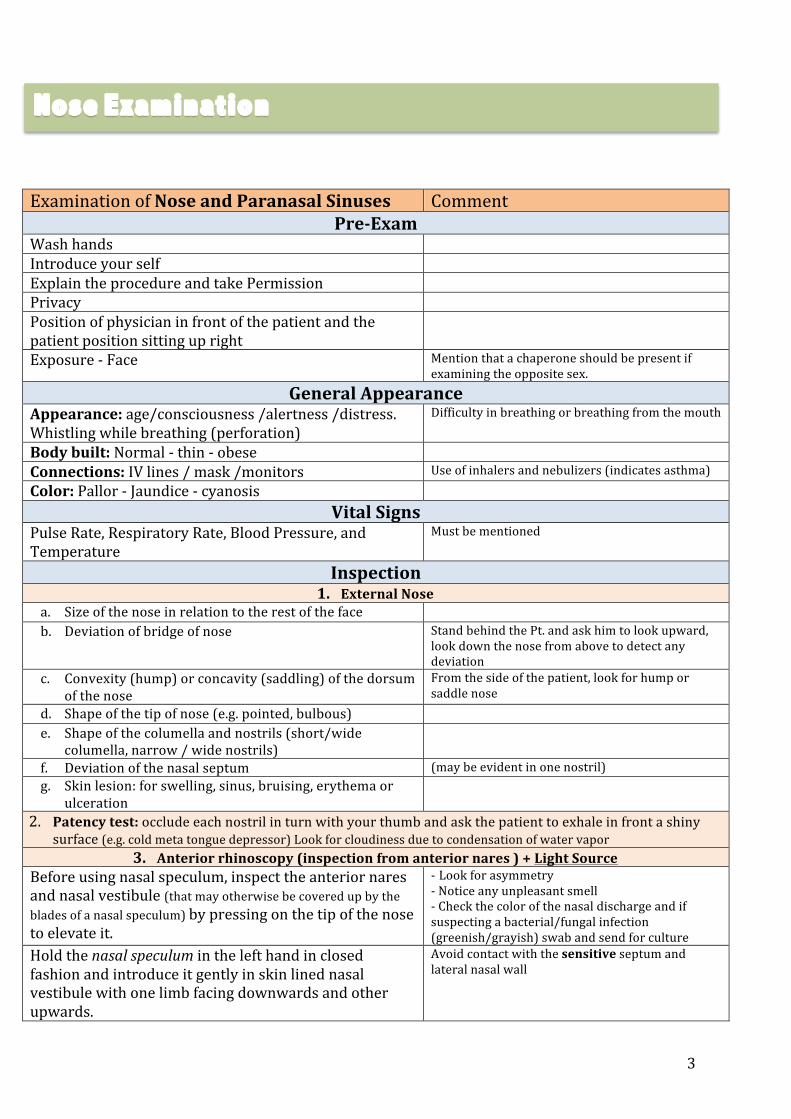
Examination of Nose and Paranasal Sinuses Comment Pre-‐Exam
Wash hands Introduce your self Explain the procedure and take Permission Privacy Position of physician in front of the patient and the patient position sitting up right
Exposure -‐ Face Mention that a chaperone should be present if examining the opposite sex.
General Appearance Appearance: age/consciousness /alertness /distress. Whistling while breathing (perforation)
Difficulty in breathing or breathing from the mouth
Body built: Normal -‐ thin -‐ obese
Connections: IV lines / mask /monitors Use of inhalers and nebulizers (indicates asthma) Color: Pallor -‐ Jaundice -‐ cyanosis
Vital Signs Pulse Rate, Respiratory Rate, Blood Pressure, and Temperature
Must be mentioned
Inspection 1. External Nose
a. Size of the nose in relation to the rest of the face b. Deviation of bridge of nose Stand behind the Pt. and ask him to look upward,
look down the nose from above to detect any deviation
c. Convexity (hump) or concavity (saddling) of the dorsum of the nose
From the side of the patient, look for hump or saddle nose
d. Shape of the tip of nose (e.g. pointed, bulbous) e. Shape of the columella and nostrils (short/wide
columella, narrow / wide nostrils)
f. Deviation of the nasal septum (may be evident in one nostril) g. Skin lesion: for swelling, sinus, bruising, erythema or
ulceration
2. Patency test: occlude each nostril in turn with your thumb and ask the patient to exhale in front a shiny surface (e.g. cold meta tongue depressor) Look for cloudiness due to condensation of water vapor
3. Anterior rhinoscopy (inspection from anterior nares ) + Light Source Before using nasal speculum, inspect the anterior nares and nasal vestibule (that may otherwise be covered up by the blades of a nasal speculum) by pressing on the tip of the nose to elevate it.
-‐ Look for asymmetry -‐ Notice any unpleasant smell -‐ Check the color of the nasal discharge and if suspecting a bacterial/fungal infection (greenish/grayish) swab and send for culture
Hold the nasal speculum in the left hand in closed fashion and introduce it gently in skin lined nasal vestibule with one limb facing downwards and other upwards.
Avoid contact with the sensitive septum and lateral nasal wall
Nose Examination
4
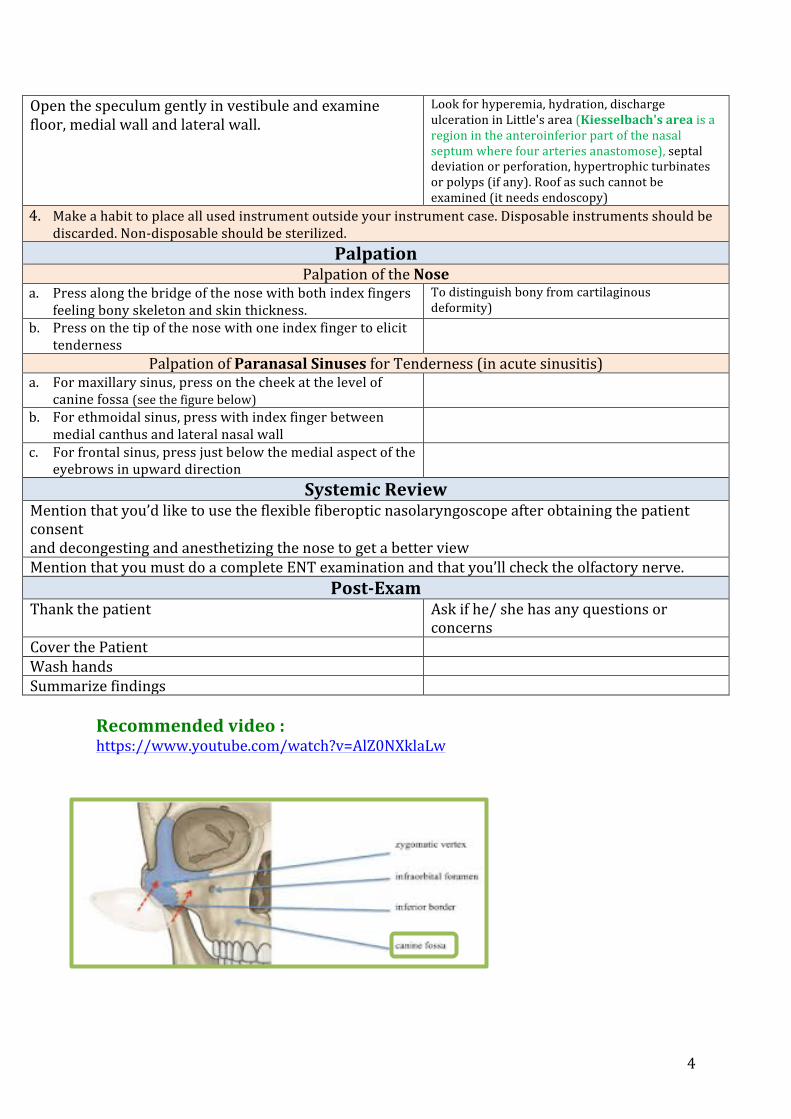
Open the speculum gently in vestibule and examine floor, medial wall and lateral wall.
Look for hyperemia, hydration, discharge ulceration in Little's area (Kiesselbach's area is a region in the anteroinferior part of the nasal septum where four arteries anastomose), septal deviation or perforation, hypertrophic turbinates or polyps (if any). Roof as such cannot be examined (it needs endoscopy)
4. Make a habit to place all used instrument outside your instrument case. Disposable instruments should be discarded. Non-‐disposable should be sterilized.
Palpation Palpation of the Nose
a. Press along the bridge of the nose with both index fingers feeling bony skeleton and skin thickness.
To distinguish bony from cartilaginous deformity)
b. Press on the tip of the nose with one index finger to elicit tenderness
Palpation of Paranasal Sinuses for Tenderness (in acute sinusitis) a. For maxillary sinus, press on the cheek at the level of
canine fossa (see the figure below)
b. For ethmoidal sinus, press with index finger between medial canthus and lateral nasal wall
c. For frontal sinus, press just below the medial aspect of the eyebrows in upward direction
Systemic Review Mention that you’d like to use the flexible fiberoptic nasolaryngoscope after obtaining the patient consent and decongesting and anesthetizing the nose to get a better view Mention that you must do a complete ENT examination and that you’ll check the olfactory nerve.
Post-‐Exam Thank the patient Ask if he/ she has any questions or
concerns Cover the Patient Wash hands Summarize findings
Recommended video : https://www.youtube.com/watch?v=AlZ0NXklaLw
5
Items
Introduction Personal data Chief complaint History of presenting Illness (HPI) Site unilateral (suggesting structural causes) or bilateral (suggesting mucosal causes) Onset & Duration Pattern, progression, pain, previously Intermittent with respect to: -‐Daily time course -‐Body position -‐Seasonality -‐Exposures to environmental stimuli (eg, cigarette smoke, particulate matter, pets, chemicals) Aggravating and Reliving factors Time course -‐Temporal course of symptoms, including diurnal and seasonal variation suggesting an allergic process. -‐Nasal septal deviation or bony inferior turbinate hypertrophy typically worsen slowly over time. Recent: URTI, Hx of sinusitis, or use of topical nasal decongestants >5 days. Samter’s triad (nasal polyps, aspirin sensitivity, asthma) Severity Associated symptoms -‐ Changes in sense of taste and smell (hyposmia)
-‐ Persistent postnasal drip -‐ Symptoms suggesting malignancy: Facial deformity, cranial nerve dysfunction (eg, facial numbness), and unexplained epistaxis, middle ear effusion (nasopharyngeal ca) -‐ Symptoms of rhinosinusitis: Facial pain or pressure, nasal congestion, dysosmia, headache, purulent nasal discharge -‐ Intranasal drug use: Intranasal cocaine or overuse of topical nasal decongestant, such as oxymetazoline or neosynephrine -‐ Oral medications: Oral contraceptives, antithyroid medication, antihypertensive medication, antidepressants, and benzodiazepines -‐ Constitutional: Fever, Weight loss, Loss of appetite
Past medical Past Medical Conditions: Asthma and obstructive sleep apnea, Wegener’s granulomatosis, cystic fibrosis (associated with nasal polyposis), sarcoidosis, and syphilis. Past Surgeries/Trauma: rhinoplasty Past Hospital admission
Social history
Nasal block history:
6
Household pets Smoking, alcohol Allergies, medication, blood transfusions. Family history
Asthma, OSA, nasal polyps.
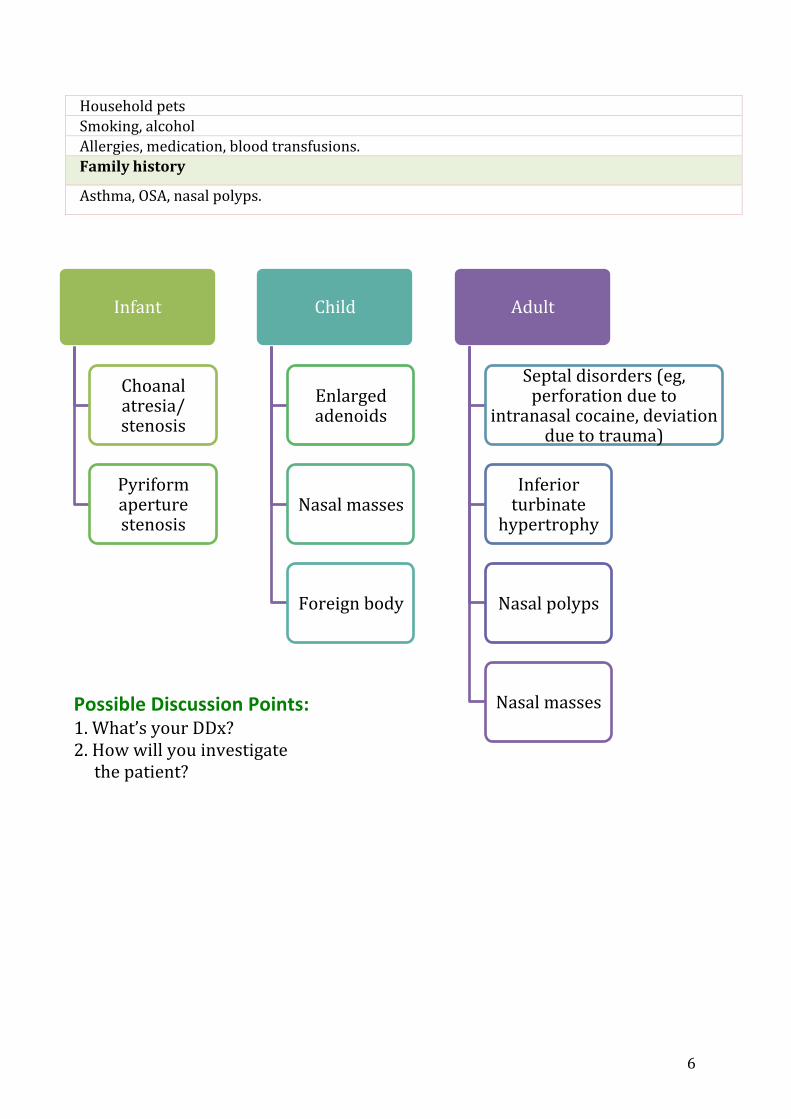
Infant
Choanal atresia/stenosis
Pyriform aperture stenosis
Child
Enlarged adenoids
Nasal masses
Foreign body
Adult
Septal disorders (eg, perforation due to
intranasal cocaine, deviation due to trauma)
Inferior turbinate
hypertrophy
Nasal polyps
Nasal masses Possible Discussion Points: 1. What’s your DDx? 2. How will you investigate the patient?
7
1. History of: -‐Hx of atopy, URTIs, enlarged adenoids, deviated septum. -‐Recurrent sinusitis -‐Nasal trauma/ surgery -‐Having household pets -‐Exposure to poor air quality 2. Family history of nasal polyposis. 3. Use of topical nasal decongestants >5 days.
Congestion, stuffiness, or blockage within the nose, and/or difficulty sleeping/breathing.
In the case of rhinosinusitis: +Facial congestion, facial pain or pressure, dysosmia, rhinorrhea, postnasal discharge, cough, pruritic conjunctivitis, sneezing, or throat irritation/itching. -‐Obstructive Sleep Apnea. -‐Asthma flare-‐ups. -‐Sinus infections and its complications.
1. Anterior rhinoscopy. -‐Performed with a nasal speculum or with an otoscope, along with a bright light source to improve visualization. -‐Allows for optimal visualization of each vestibule, the nasal turbinates, septum, and mucosal surfaces. -‐Provides assessment of the size and caliber of the inferior turbinates and the position of the anterior to mid-‐nasal septum. -‐Possible Findings: -‐Occluded nasal passageways caused by boggy, red nasal mucosa may develop as a result of allergies, nonallergic rhinitis, or overuse of nasal decongestants. -‐Ulcerated, friable mucosa may indicate granulomatous disease. -‐Polyps at the level of the middle turbinate or mid-‐nasal cavity may be visible. -‐Purulent nasal discharge is helpful in identifying cases of rhinosinusitis. 2. Fiberoptic nasal endoscopy. -‐Posterior nasal structures are best visualized with nasal endoscopy. -‐Done after preparation of the nose with topical decongestant and/or topical anesthetic spray.
Investigations
Complications
Signs & Symptoms
Risk Factors
Rhinitis medicamentosa (or RM) is a condition of rebound nasal congestion brought on by extended use of topical decongestants (e.g., oxymetazoline, phenylephrine, xylometazoline, and naphazoline nasal sprays)
8
3. CT scan. 4. Other testing. • Allergy testing
-‐should be particularly considered in patients with concurrent asthma. • Acoustic rhinometry
-‐ a simple, noninvasive measure of cross-‐sectional area of the nasal cavity longitudinally along the nasal passageway.
• Peak nasal airflow -‐ a noninvasive measure indicating peak nasal airflow in liters per minute achieved during maximal forced nasal inspiration.
• Rhinomanometry -‐a computerized, functional assessment of airflow.
Mucosal biopsy is indicated for cases of suspected malignancy and may be helpful in the diagnosis of infection or inflammatory disease.
Depending on the underlying cause.
Management
9
Definition Acute sinusitis:
• Usually unilateral and after an URTI • Symptoms usually last <4 weeks
Chronic sinusitis: • Pain is less of a feature • Symptoms last >3 months
Fungal sinusitis: • Usually the patients are immunocompromised due to diabetes, cancer, HIV, organ transplantation or using systemic or intranasal glucocorticoids.
Presentation • Presentation is often non-‐specific • Nasal congestion • Purulent discharge • Facial pain with headache • Dental pain (maxillary sinus) • Alteration in sense of smell • Pain may be exacerbated by leaning forward or head movement
NB. Facial pain in the absence of nasal symptoms is unlikely to be sinusitis.
Complications • Complications can be life threatening • Osteomyelitis • Orbital cellulitis • Intracranial involvement
Investigations: • Diagnosis depend on clinical history and physical examination. • Sinuses culture: not for all patients (persistence infection despite antibiotics treatment or immunocompromised).
• Imaging may be warranted in the case of recurrent episodes of sinusitis, suspected anatomical abnormalities, or if an alternative diagnosis is suspected such as migraine headache or malignancy. ü Nasal endoscopy: mucosal erythema, purulent discharge. ü CT Sinuses (non-‐contrast): identifies extent of sinus disease, abnormal
anatomical structures. Management:
• Cases are usually self-limiting • Analgesia and decongestants • Antibiotics • Topical nasal steroids • Surgery: FESS
Sinusitis:
10
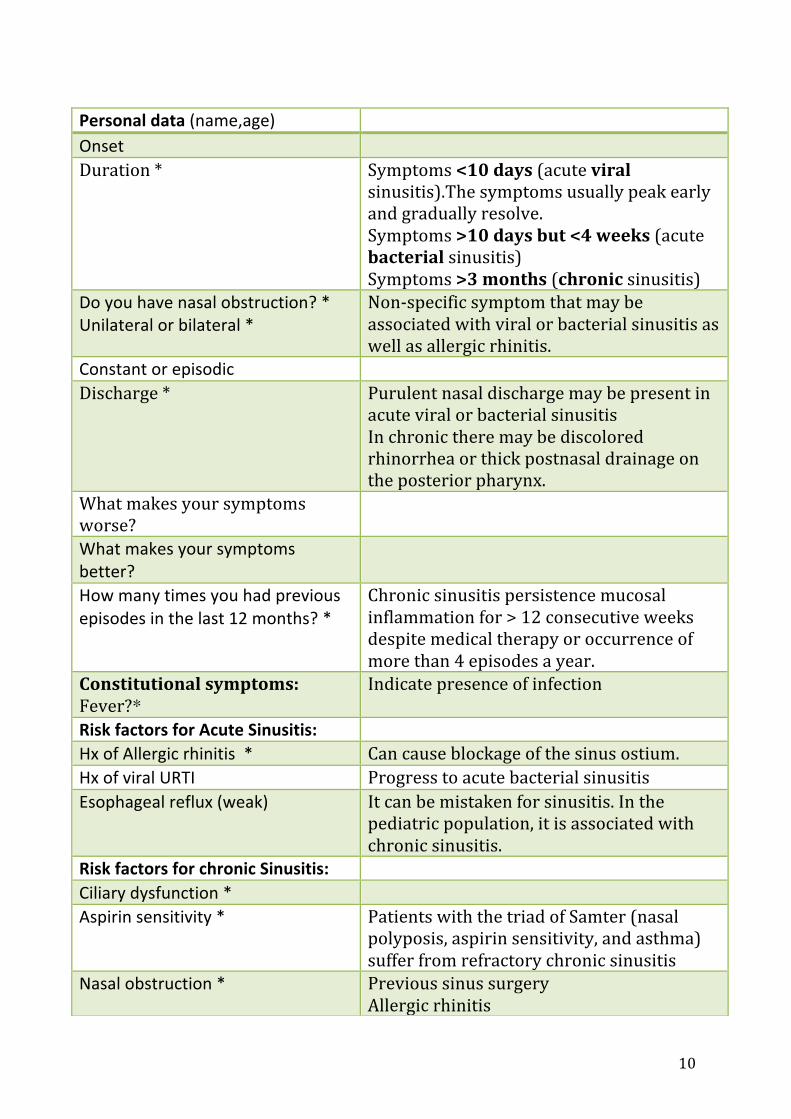
Personal data (name,age) Onset Duration * Symptoms <10 days (acute viral
sinusitis).The symptoms usually peak early and gradually resolve. Symptoms >10 days but <4 weeks (acute bacterial sinusitis) Symptoms >3 months (chronic sinusitis)
Do you have nasal obstruction? * Unilateral or bilateral *
Non-‐specific symptom that may be associated with viral or bacterial sinusitis as well as allergic rhinitis.
Constant or episodic Discharge * Purulent nasal discharge may be present in
acute viral or bacterial sinusitis In chronic there may be discolored rhinorrhea or thick postnasal drainage on the posterior pharynx.
What makes your symptoms worse?
What makes your symptoms better?
How many times you had previous episodes in the last 12 months? *
Chronic sinusitis persistence mucosal inflammation for > 12 consecutive weeks despite medical therapy or occurrence of more than 4 episodes a year.
Constitutional symptoms: Fever?*
Indicate presence of infection
Risk factors for Acute Sinusitis: Hx of Allergic rhinitis * Can cause blockage of the sinus ostium. Hx of viral URTI Progress to acute bacterial sinusitis Esophageal reflux (weak) It can be mistaken for sinusitis. In the
pediatric population, it is associated with chronic sinusitis.
Risk factors for chronic Sinusitis: Ciliary dysfunction * Aspirin sensitivity * Patients with the triad of Samter (nasal
polyposis, aspirin sensitivity, and asthma) suffer from refractory chronic sinusitis
Nasal obstruction * Previous sinus surgery Allergic rhinitis
11
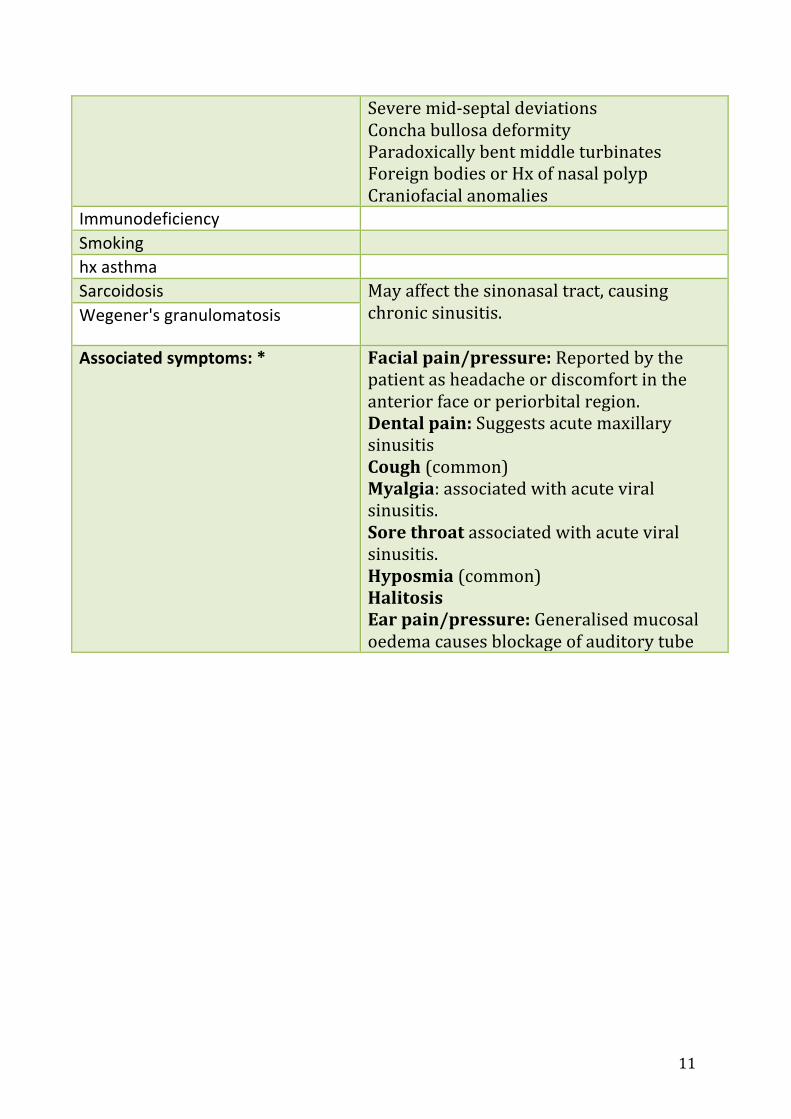
Severe mid-‐septal deviations Concha bullosa deformity Paradoxically bent middle turbinates Foreign bodies or Hx of nasal polyp Craniofacial anomalies
Immunodeficiency Smoking hx asthma Sarcoidosis May affect the sinonasal tract, causing
chronic sinusitis.
Wegener's granulomatosis
Associated symptoms: *
Facial pain/pressure: Reported by the patient as headache or discomfort in the anterior face or periorbital region. Dental pain: Suggests acute maxillary sinusitis Cough (common) Myalgia: associated with acute viral sinusitis. Sore throat associated with acute viral sinusitis. Hyposmia (common) Halitosis Ear pain/pressure: Generalised mucosal oedema causes blockage of auditory tube
12
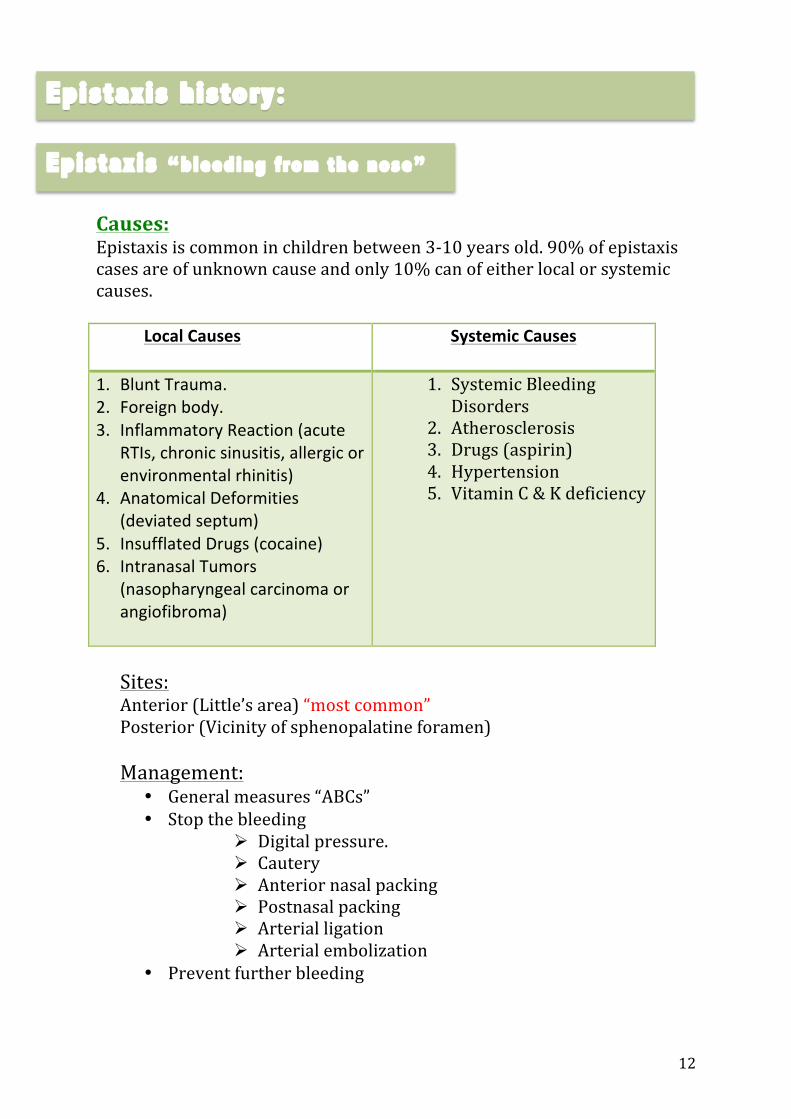
Causes: Epistaxis is common in children between 3-‐10 years old. 90% of epistaxis cases are of unknown cause and only 10% can of either local or systemic causes.
Local Causes
Systemic Causes
1. Blunt Trauma. 2. Foreign body. 3. Inflammatory Reaction (acute
RTIs, chronic sinusitis, allergic or environmental rhinitis)
4. Anatomical Deformities (deviated septum)
5. Insufflated Drugs (cocaine) 6. Intranasal Tumors
(nasopharyngeal carcinoma or angiofibroma)
1. Systemic Bleeding Disorders
2. Atherosclerosis 3. Drugs (aspirin) 4. Hypertension 5. Vitamin C & K deficiency
Sites: Anterior (Little’s area) “most common” Posterior (Vicinity of sphenopalatine foramen) Management:
• General measures “ABCs” • Stop the bleeding
Ø Digital pressure. Ø Cautery Ø Anterior nasal packing Ø Postnasal packing Ø Arterial ligation Ø Arterial embolization
• Prevent further bleeding
Epistaxis history:
Epistaxis “bleeding from the nose”
13
• Introduction. • Personal Data. • Chief Complaint.
History of presenting illness:
• Side. • Onset. • Frequency. • Duration. • Color. • Triggers “sneezing, nose blowing or picking” or “weather changes” • Aggravating and relieving factors. • Severity and estimated blood loss. • Any previous episodes. • Family history or bleeding disorder. • Recent trauma, URTIs or sinusitis.
Review of Systems: Ask about symptoms of excessive bleeding (easy bruising, bloody stools, hemoptysis, blood in urine, and excess bleeding with tooth brushing, phlebotomy, or minor trauma) and symptoms of anemia. Past Medical History:
• Hypertension. • Coagulopathies or any vascular abnormalities. • Cirrhosis, HIV.
Past Surgical History:
• Any nasal surgeries. Medications:
• Aspirin or other NSAIDs. • Antiplatelet drugs (clopidogrel) • Aspirin and warfarin.
Social History: • Smoking • Allergies and blood transfusion
History..
14
Definition: inflammation of the mucosa of the nasal cavity Allergic Rhinitis: Common, IgE mediated hypersensitivity response, associated allergic conjunctivitis and asthma may occur
1. Intermittent (Seasonal) less that 4 days/week or less than 4 weeks at a time 2. Persistent (Perennial) 4 or more days/week and 4 or more weeks
Clinical features: - Sneezing may be in paroxysm.
- Rhinorrhea - Nasal obstruction and loss of smell
- Itchiness of nose, palate
- Tearing, itching, redness of eyes
- Burning sensation in the throat.
- Symptom related to asthma
Risk factors: • Age: usually at childhood • Family hx : genetic component. • Environmental exposure to allergens : pollen, house dust mite, pets Pathophysiology phases: 1. Sensitization 2. Subsequent reaction to allergen– early phase 3. Late phase reaction 4. Systemic activation
Rhinitis:
15
Investigations: 1-‐ Skin Tests: it’s a primary tool in allergy investigation. 2-‐Laboratory tests:
-‐Nasal cytology, eosinophil counts in nasal secretion -‐Blood IgE level measurement (confirmatory but it is neither sensitive nor specific )
Treatment: • Prevention: hygiene and avoidance of allergen • Nasal irrigation with saline • Antihistamines • Oral decongestants (pseudoephedrine) • Topical decongestant • Other topicals: steroids (fluticasone, beclomethazone,), antihistamines, and ipratropium bromide • Oral steroids if severe • Desensitization by allergen immunotherapy • Surgery: polypectomy, Reduction of inferior turbinate Complications: Sinusitis, Otitis media, Nasal polyps, Sleep apnea, Dental overbite, Palate malformations caused by mouth breathing Rhinitis medicamentosa: Rebound congestion due to the overuse of intranasal vasoconstrictors. For prevention, use of these medications for only 5-‐7 d is recommended. *Congestion reduces nasal airflow and allows the nose to repair itself (i.e. washes away the irritants). Treatment should focus on the initial insult rather than target this defense mechanism. Vasomotor Rhinitis • Neurovascular disorder of nasal parasympathetic system affecting mucosal blood vessels • Nonspecific reflex hypersensitivity of nasal mucosa Caused by: -‐Temperature change, Alcohol, dust, smoke, Stress, anxiety, neurosis, hypothyroidism, pregnancy, menopause, Parasympathomimetic drugs Clinical Features: • Chronic intermittent nasal obstruction, varies from side to side • Rhinorrhea: thin, watery • Mucosa and turbinates: swollen • Nasal allergy must be ruled out Treatment: • Elimination of irritant factors
16
• Parasympathetic blocker • Steroids • Surgery (often of limited lasting benefit): electrocautery, cryosurgery, laser treatment or removal of inferior or middle turbinates • Symptomatic relief with exercise (increased sympathetic tone) Infectious rhinitis
Specific Non-‐specific
Acute Common cold & influenza
-‐Virus: rhinovirus, coronavirus, adenovirus, Para influenza virus, respiratory syncytial virus, enterovirus -‐Nasal obstruction: Pyrexia -‐Bacterial: strep. Pneumonia, strept. Pyogen *Prophylactic: avoid contact with patient *Therapeutic: Rest, Analgesics, Decongestant, Antibiotic
Chronic Syphilis, Wegner’s granuloma, Medline lethal granuloma, Sarcoidosis, Mycobacteria, Atrophic rhinitis
*Etiology: -‐Not fully known -‐Infection -‐Endocrine or vitamin disturbance *Types: -‐Primary (without any interference) -‐Secondary (usually related to surgery)
History:
• What is your main symptom? Describe your symptom?
• How old were you when you first had these symptoms?
• Is there anything that makes it worse? • What time of year and what time of day do you have these symptoms?
• How much does it bother you? How often do you have these symptoms, and how long do your symptoms last?
• Do you have trouble sleeping or have you missed school or work because of your symptoms?
Allergic rhinitis traid: sneezing +nose itching+ rhinorrhea They may also have: Nasal or air obstruction
17
- Associated symptoms? : See the box, post nasal drip, smell sensation, cough or throat clearing, eye (itching, redness, tearing), fatigue and malaise (in children), Symptoms of upper respiratory infection (makes allergic etiology less likely)
- Constitutional Symptoms? Fever, Weight loss and Loss of appetite
• Symptom related to asthma (cough, shortness off breath, wheeze)
• If nasal block: do you need to breathe from your mouth? • If rhinorrhea: color? (Clear or colored may exist, though colored rhinorrhea may indicate a co-‐morbid disease process with AR) unilateral or bilateral (uni: could be obstruction or foreign body. Bi: could be rhinitis or sinusitis) alternating or constant (alternating is normal nasal cycle)
• Symptom related to ear infection? • Does anyone else in your family have same problems, including allergic asthma, eczema?
• Do you have other medical conditions that are related to allergies, such asthma, eczema, or rhinitis?
• Did you have allergies as a child? Allergy to pollen, house dust mite, food, pets?
• What medicines, including over-‐the-‐counter medicines and dietary supplements, are you taking now? Do these medicines help your symptoms?
• Have you ever had surgery on your nose, throat, or ears? - Social History : Smoking or Passive smoking - Alcohol consumption - Traveling
For mistakes or feedback

















