E L S E V I E R Clinica Chimica Acta 256 (1996) 151 164
Osteocalcin detection in aging serum and whole blood: stability of different osteocalcin fractions
Marjo H.J. Knapen a, Hans-Georg Eisenwiener b, Cees Vermeer"'*
"Cardiovascular Research Institute and Department of Biochemistry, University of Limburg, P.O. Box 616, 6200 MD Maastricht, The Netherlands bHoffmann-La Roche Diagnostics, Basle, Switzerland
Received II March 1996; revised 29 July 1996; accepted 7 August 1996
[1,2]. The only known function of Gla-residues in proteins is the strong and selective binding of calcium ions. Two major sources of Gla-proteins are the hepatocytes in liver (production of blood coagulation factors) [3] and the osteoblasts in bone (synthesis of osteocalcin, matrix-Gla-protein, and protein S) [4-6]. Osteocalcin (also known as bone Gla-protein, BGP) is the most abundant Gla-protein known thus far and it is widely used as a bone formation marker [4,5,7]. Following its biosynthesis and cellular secretion, the main part of osteocalcin is bound to the hydroxyapatite matrix of bone; about 20% of the de novo synthesized material, however, is set free in the blood, where it is available for detection by immuno-affinity techniques [8].
In all mammals investigated thus far, osteocalcin contains three Gla- residues [4,9]. Human osteocalcin, however, seems to occur in the normal form as well as in various states of undercarboxylation (Gla-deficiency). Notably the most N-terminal Gla-residue (position 17) is frequently under- carboxylated, suggesting a local vitamin K-deficiency in bone tissue [10,11]. Since the physiological importance of osteocalcin is still a matter of debate, it is unknown whether the reduced number of Gla-residues hampers its biological function. Subjects with high levels of circulating undercarboxy- lated osteocalcin were reported to have a lower bone mass [12], and a sixfold increased femur neck fracture risk [13] than age- and sex-matched controls. Moreover, it was shown in postmenopausal women that vitamin K-supplementation increased the serum markers for bone formation (os- teocalcin and bone alkaline phosphatase), and decreased the urinary excre- tion of hydroxyproline (marker for bone resorption) and calcium [14,15].
Several commercial kits are available for measuring the immunoreactive serum osteocalcin (irOC) concentration in humans. Based on an earlier described technique in rats [16], we have developed a method to fractionate total human serum irOC (irOCtot,1) into a fraction with high (irOCbo,nd) and a fraction with low (irOCfree) affinity for hydroxyapatite [14,15]. It is generally assumed that these fractions are similar to normally carboxylated (3 Gla) osteocalcin and undercarboxylated (0-2 Gla) osteocalcin, but since they have not yet been chemically characterized we prefer to designate both fractions as irOCbounO and irOCfree, respectively. In a cross-sectional study among 229 women, we have recently found a high correlation between irOCbound with bone alkaline phosphatase, whereas irOCfreo inversely corre- lates with bone mass (Knapen et al., unpublished data). This demonstrates the importance of developing simple and rapid detection methods for both osteocalcin fractions.
Problems related to the commercial test kits presently available for osteocalcin detection are: (i) when using kits from different origin, the absolute irOC concentration measured in the same serum sample may vary 10-fold; this hampers the comparison of data from one laboratory to
another [8,17,18]; (ii) the stability of serum irOC is frequently reported to be poor [19,20]; and (iii) it is unclear whether and to what extent the various kits detect undercarboxylated osteocalcin and osteocalcin degradation products. In this paper, we have compared six different osteocalcin kits: two radioimmunoassays (RIA), two immunoradiometric assays (IRMA), and two enzyme-linked immunosorbent assays (ELISA). With these tests, we have determined the stability at different tem- peratures of the various irOC fractions in serum and in whole blood, and the relative proportion of both fractions in serum from normal adults.
2. Materials and methods
2. I. Sample preparation
2. I. 1. Serum collection Five normal, healthy adults (two men, three women, mean age 32
years) were recruited; serum samples from the same subjects were used for all experiments. Blood was taken by venipuncture and collected in glass tubes. Unless indicated otherwise, serum was prepared by incubat- ing the samples for 20 min at room temperature, and subsequently cen- trifuging them for 15 min at 3000 x g. In all experiments reported below the serum concentrations were calculated from duplicate measure- ments for each participant separately, the means of individual values _+ SEM are given in Table 2 and in Figs. 1-3. For the experiment with samples outside the normal range, we used: the five normal subjects mentioned above, 10 hemodialysis patients, 15 postmenopausal, 10 pa- tients under oral anticoagulant treatment, and five cord sera.
2.1.2. Fractionation o f serum osteocalcin Fifty milligrams of hydroxyapatite (BDH, Poole, UK) was added to
0.5 ml of serum, and rotated end over end at room temperature for 30 min. Subsequently the hydroxyapatite was removed by centrifugation (5 rain, 10000 × g) and irOC was measured in the serum before and after the extraction step. The resulting values were designated as irOCtot~ and irOCfree, respectively. IrOCbound was calculated by subtracting irOCfree from irOCtotab and the hydroxyapatite binding capacity of os- teocalcin (HBC) was calculated by expressing irOCbo,nj as a percentage of irOC~ot~,l.
All test kits were used according to the manufacturers' protocols. A short summary of the characteristics of each kit is given in Table 1.
Osteocalcin 125I RIA Kit: for the quantitative determination of osteocalcin (Incstar, Stillwater, MN). This assay is based on a competitive reaction b e t w e e n 125I bovine osteocalcin, sample (human serum) osteocalcin, and rabbit anti-bovine osteocalcin antibodies (polyclonal). After an overnight incubation (16-24 h at 2-8°C) phase separation occurs by the addition of
E 32 O'J
" 24 C
o 8
0 0
.A - - r -
_
2 3 4 5 6
Assay number
A
v
O m "I"
100
80
60
40
20
0
B
1 2 3 4 5 6
Assay number
Fig. 1. Immunoreactive osteocalcin detected by various test kits. All measurements were made in freshly prepared serum from five donors, and the values are given + SEM. The different tests are referred to with numbers: 1, Incstar; 2, Henning; 3, Cis Bio International; 4, Nichols; 5, Metra; 6, Osteometer. A: each bar represents the total immunoreactive osteocalcin as measured by the various kits, subdivided into irOCfree (hatched part of bars) and irOCboun d (open part of bars). B: the hydroxyapatite binding capacity (HBC) is calculated by expressing the irOfboun,t as a percentage of irOCtota 1.
Assay number Fig. 2. Stability of serum osteocalcin during storage at room temperature. The depicted storage periods were 6 h (open bars) and 10 days (hatched bars). All values are expressed as a percentage of those obtained with the same kit in freshly prepared serum. A, irOCtotal; B, irOCbo.na; C, irOCfree. Further details are as in the legend to Fig. 1.
Temperature (C) Fig. 3. Stability of serum osteocalcin at increased temperatures. All incubation periods were 1 h; the data obtained at the incubation temperatures of 22, 37, and 56°C are expressed as a percentage of those at 4°C. Three kits were compared: Cis Bio International (open bars), Osteometer (wide hatching), and Nichols (narrow hatching). A, irOCtotal; B, irOCbound; C, irOCf~.
M . H , J . Knapen et a l . / Clinica Chimica Ac ta 256 (1996) 151--164 I 5 7
a complex of goat anti-rabbit antibodies, rabbit serum, and polyethylene glycol.
Oscatest Osteocalcin (BGP): RIA for the determination of intact os- teocalcin (BGP) in human serum (Henning, Berlin, Germany). Tubes are coated with sheep polyclonal antibodies against human osteocalcin frag- ment 37-49. Sample osteocalcin competes with 125I human osteocalcin fragment 37-49 during an overnight incubation step at 2-8°C. Excess of tracer is then removed by aspirating the liquid phase.
ELSA-OSTEO IRMA: A solid-phase 'sandwich' immunoradiometric as- say with two monoclonal antibodies against human osteocalcin (Cis Bi0 International, Gif-sur-Yvette, France). The first monoclonal antibody against human osteocalcin fragment 25-37 is coated on the solid phase. Sample and J25I-labeled second monoclonal antibody against human os- teocalcin fragment 5-13 antibody are added and incubation occurs for 2 h at room temperature. Excess of unbound tracer is removed after an extensive washing procedure.
Human Osteocalcin Kit: IRMA for the Quantitative Determination of Osteocalcin Levels in Human Serum (Nichols Institute, Immutopics, Inc., San Clemente, USA). A polyclonal antibody against human osteocalcin fragment 20-49 is immobilized onto plastic beads and captures sample osteocalcin. The detection is performed with the aid of a ~25I-labeled second antibody against human osteocalcin fragment 1-19. After an incubation period of 3 h at room temperature, excess unbound antibody is removed by a washing procedure.
NovoCalcin Kit: ELISA for the determination of 'de novo osteocalcin' in serum or tissue culture medium (serum free) to quantify bone turnover (Metra Biosystems, Inc., Palo Alto, CA). Human osteocalcin is coated to the wells of a microtiter plate, and competes with sample osteocalcin for the monoclonal antibody against bovine osteocalcin during a 2-h incubation at room temperature. After washing the plate, an enzyme-linked antibody is added, followed by a 1-h incubation period and subsequent washing. Detection occurs within half an hour after adding of the substrate to the wells.
Two-site N-MID hOsteocalcin ELISA: For the quantitative determination of osteocalcin in human serum (Osteometer A/S, Copenhagen, Denmark). Wells of a microtiter plate have been pre-coated with a monoclonal anti- body against human osteocalcin fragment 20-43. Sample osteocalcin and a second (peroxidase-conjugated) monoclonal antibody against human os- teocalcin fragment 1-19 are added to the wells and incubated for 2 h at room temperature. Detection occurs within 15 min after adding the sub- strate to the washed wells.
3.1. Comparison of different test kits in freshly prepared serum
Blood was taken from five healthy volunteers, and used for the prepara- tion of serum. Six kits were compared with respect to their ability to detect irOCtotal, and irOCfre~ in the same serum samples, and from these data, the irOCbound was calculated. Using the test-specific standards as a reference, large variations were found in the absolute values for each of these variables (Fig. 1), with irOCtota~ ranging from 3.9-27.0 ng/ml, irOCfre~ from 0.8-16.9 ng/ml and irOCbound from 3.1-14.5 ng/ml. Remarkably, the relative amounts of irOCbouna (expressed as HBC) were very similar (70-80%) in five out of six kits. With the Osteometer kit, high amounts of irOCfr~ were detected, leading to low HBC values (36%).
3.2. Stability of osteocalcin fractions during storage of serum at room temperature
The same samples as mentioned above were kept at room temperature and the osteocalcin determinations were repeated after varying periods of time. Fig. 2 summarizes the measurements after 6 h and after 10 days of incubation at room temperature. The decrease of immunoreactive antigen was very small after 6 h, and only in the case of the Henning kit was the decrease marginally significant (p = 0.06). After 10 days at room tempera- ture, 70-80% of the original irOCtotal concentrations were detectable with the Cis and the Osteometer kit (Fig. 2A). With other kits these values were lower. Both irOCbound and irOCrree had decreased, except in one case (Cis) where we observed a substantial increase of irOCfree (Fig. 2B,C). This suggests that irOCfre~ can be formed from irOCbouna, and since the design of this assay excludes the detection of osteocalcin fragments, the conversion of irOCbou~j into irOCfr~ may be brought about by a conformational change rather than by degradation of the molecule. Similar experiments were performed in which the whole blood clot was incubated for the indicated periods of time, followed by serum preparation shortly before testing. In this way it was demonstrated that the stability of the various osteocalcin fractions in whole blood is comparable to that in serum (data not shown).
3.3. Stability of osteocalcin fractions at different temperatures
Freshly prepared serum samples (n = 5) were incubated for 1 h at different temperatures (4, 22, 37, and 56°C) and cooled in ice before the various osteocalcin fractions were assessed with three different kits. As was
to be expected, the values remained unchanged at 4°C, and the data obtained at higher temperatures were expressed as a percentage of the corresponding time points at 4°C. The data are shown in Fig. 3, and it is clear that no significant losses occurred during 1-h incubations up to 37°C. At higher temperatures significant amounts of irOCbound (Fig. 3B) are lost in all three tests, whereas only in the Osteometer test, irOCfree also decreased dramatically at 56°C (Fig. 3C). It should be remembered, however, that the absolute value of irOCfre~ detected with this kit is much higher than with other kits, resulting in an abnormally low HBC-value. After incubation at high temperature the HBC-values measured with all kits were closely similar (about 50%). Apparently the extra antigen detected with the Osteometer kit was lost at 56°C.
3.4. Correlation between different kits in patient sera
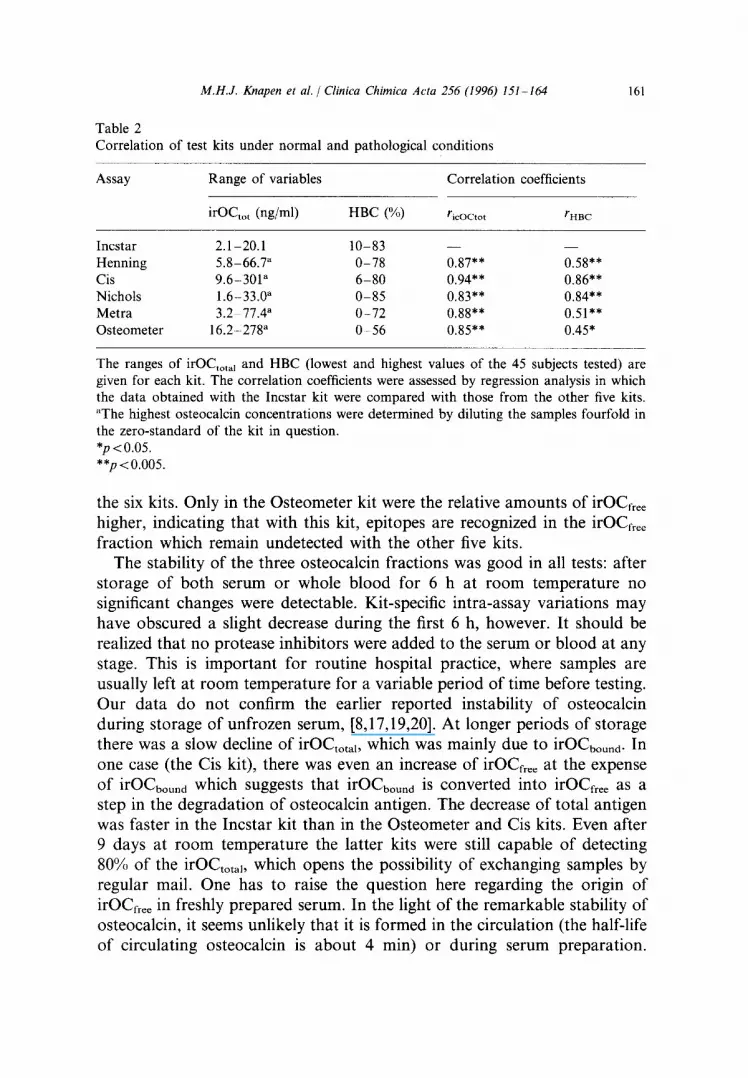
To test the performance of the various kits over a wide range of osteocalcin concentrations and HBC values, the group of five normal subjects mentioned above was supplemented with: 10 hemodialysis patients (known to have very high osteocalcin levels), 15 postmenopausal women (mildly elevated osteocalcin levels, partly undercarboxylated), 10 patients under oral anticoagulant treatment (low-normal serum osteocalcin antigen, substantially undercarboxylated), and five cord sera (high serum osteocal- cin, extreme undercarboxylation). In these 45 samples, we assessed both the irOftota 1 and the HBC values and we calculated the correlation between the data obtained with the Incstar and the other five kits. The results are summarized in Table 2 and show the wide test ranges for both irOCtotal and for HBC. A satisfactory correlation between the various kits for total osteocalcin antigen was found over the whole test range. For HBC, the data obtained with the Incstar kit correlated well with those from Cis and Nichols, but the correlation was less consistent for the other kits, notably with both ELISA-based ones (Metra and Osteometer).
4. Discussion
Commercial kits are based on either one of three different detection techniques: radioimmunoassay [21], immunoradiometric assay [22], and enzyme-linked immunosorbent assay [23,24]. Two kits from each group were selected and used for the assessment of irOCtotal, irOCbound, and irOCfroe in the same serum samples. Large variations were found in the absolute concentrations, but the relative amounts of irOCbound and irOCfre~ (expressed as a percentage of irOCtota~) were remarkably similar in five of
Table 2 Correlation of test kits under normal and pathological conditions
Assay Range of variables Correlation coefficients
irOCto t (ng/ml) HBC (%) ricocto t rHnc
Incstar 2.1-20.1 10-83 - - - - Henning 5.8-66.7 a 0-78 0.87** 0.58** Cis 9.6-301 a 6-80 0.94** 0.86** Nichols 1.6-33.0 a 0-85 0.83** 0.84** Metra 3.2 77.4" 0-72 0.88** 0.51"* Osteometer 16.2-278 a 0-56 0.85"* 0.45"
The ranges of irOCtota I and HBC (lowest and highest values of the 45 subjects tested) are given for each kit. The correlation coefficients were assessed by regression analysis in which the data obtained with the Incstar kit were compared with those from the other five kits. aThe highest osteocalcin concentrations were determined by diluting the samples fourfold in the zero-standard of the kit in question. *p <0.05. **p<0.005.
the six kits. Only in the Osteometer kit were the relative amounts of irOCfree higher, indicating that with this kit, epitopes are recognized in the irOCfvee fraction which remain undetected with the other five kits.
The stability of the three osteocalcin fractions was good in all tests: after storage of both serum or whole blood for 6 h at room temperature no significant changes were detectable. Kit-specific intra-assay variations may have obscured a slight decrease during the first 6 h, however. It should be realized that no protease inhibitors were added to the serum or blood at any stage. This is important for routine hospital practice, where samples are usually left at room temperature for a variable period of time before testing. Our data do not confirm the earlier reported instability of osteocalcin during storage of unfrozen serum, [8,17,19,20]. At longer periods of storage there was a slow decline of irOCtotal , which was mainly due to irOCuouna. In one case (the Cis kit), there was even an increase of irOCfr~e at the expense of irOCbound which suggests that irOCbound is converted into irOCfree as a step in the degradation of osteocalcin antigen. The decrease of total antigen was faster in the Incstar kit than in the Osteometer and Cis kits. Even after 9 days at room temperature the latter kits were still capable of detecting 80% of the i rOCtotab which opens the possibility of exchanging samples by regular mail. One has to raise the question here regarding the origin of irOCfree in freshly prepared serum. In the light of the remarkable stability of osteocalcin, it seems unlikely that it is formed in the circulation (the half-life of circulating osteocalcin is about 4 min) or during serum preparation.
Alternatively, it might be a product from the bone resorption process, in which case it could be used as an independent bone resorption marker.
Three of the selected kits are based on the antigen competition principle (Incstar, Henning, and Metra), the other three (Cis, Osteometer and Nichols) on the dual antibody ('sandwich') principle, which is a more direct and sensitive method for osteocalcin detection than antigen competition [22]. Moreover this technique seems to rule out the detection of osteocalcin fragments. To be able to interpret our data unequivocally, we have decided to focus our attention on the latter three kits. Not only in time, but also at increased temperatures were the osteocalcin fractions remarkably stable: only at 56°C did we find a detectable decrease of irOCtotal. When measured with the Nichols and Cis kits, there was a slight decrease of the irOCbouna, whereas irOCfree remained stable. The same samples measured with the Osteometer kit showed a marked decrease of both the irOCbound and the irOCfree fractions, suggesting that the extent to which both fractions are recognized by the various kits may differ substantially. Another argument to support this hypothesis was obtained in the correlation study (Table 2), where a better correlation was found between HBC values assessed with the kits from Cis and Nichols, than between each of these values and those obtained with the Osteometer kit.
From our data, it is clear that total osteocalcin, measured with all kits tested, consists of several fractions. A first separation of these fractions may be based on the relative affinities for hydroxyapatite, but key questions are, what is the molecular structure of these fractions, and can they be used as separate markers for different processes in bone? Recent data have shown a high correlation between irOCbound and bone alkaline phosphatase, another marker for osteoblastic bone formation. IrOCf~e~, on the other hand, showed an inverse correlation with bone mass (r = 0.65), notably in post- menopausal women (Knapen, unpublished data). Several arguments may be put forward to support the hypothesis that the fraction referred to as irOCbound is similar to highly carboxylated, mature osteocalcin. In previous studies we have shown that treatment with vitamin K of a group of healthy postmenopausal women increased the serum irOCbound concentration, sug- gesting that an increased intake of vitamin K stimulates the osteoblastic production of fully carboxylated osteocalcin [14,15]. In the same studies, we found that the administration of pharmacological doses of vitamin K during at least several weeks did not significantly alter the serum irOCfr~e concentration, which seems to exclude the possibility that irOCfr~e originates f rom de novo synthesis of undercarboxylated osteocalcin. In dialysis exper- iments with flesh and aging serum most of the irOCfr~ was retained in the dialysis bag, which does not suggest that a major part of irOCfree consists of low molecular weight degradation products (data not shown). From a
chemical point of view, the spontaneous decarboxylation of osteocalcin either in the circulation or in serum seems highly unlikely. Our working hypothesis is therefore that the main part of irOCfreo originates from bone resorption, and differs from irOCboun d by mation rather than by its primary amino
We have shown here that circulating
its secondary or tertiary confor- acid sequence. osteocalcin consists of different
fractions, which differ from each other by their physico-chemical character- istics. It is probable that these fractions also differ from each other with respect to their origin, and that they may be used as markers for different metabolic bone processes. Obviously, (i) a more precise definition of the various circulating osteocalcin fractions, and (ii) the development of sepa- rate tests, each with a high specificity for only one osteocalcin fraction, are absolute requirements for the optimal use of osteocalcin as a diagnostic tool for metabolic bone disorders.
References
[1] Vermeer C. Gamma-carboxyglutamate-containing proteins and the vitamin K-depen- dent carboxylase. Biochem J 1990;266:625-636.
[2] Suttie JW. Vitamin K-dependent carboxylase. Annu Rev Biochem 1985;54:459-477. [3] Furie B, Furie BC. Molecular and cellular biology of blood coagulation. New Engl J
Med 1992;326:800-806. [4] Hauschka PV, Lian JB, Cole DEC, Gundberg CM. Osteocalcin and matrix Gla protein:
vitamin K dependent proteins in bone. Phys Rev 1989;69:990-1047. [5] Vermeer C, Knapen MHJ, Jie K-SG. Role of vitamin K in bone metabolism. Annu Rev
Nutr 1995;15:1-22. [6] Maillard C, Berruyer M, Serre CM, Dechavanne M, Delmas PD. Protein S, a vitamin
K-dependent protein, is a bone matrix component synthesized and secreted by os- teoblasts. Endocrinology 1992;130:1599-1604.
[7] Slovik RM, Gundberg CM, Neer RM, Lian JB. Clinical evaluation of bone turnover by serum osteocalcin measurements. J Clin Endocrinol Metab 1984;59:228-230.
[8] Power M J, Fotrell PF. Osteocalcin: diagnostic methods and clinical applications. Crit Rev Clin Lab Sci 1991;28:287-335.
[9] Price PA. Role of vitamin K-dependent proteins in bone metabolism. Annu Rev Nutr 1988;8:565-583.
[10] Poser JW, Esch FS, Ling NC, Price PA. Isolation and sequence of the vitamin K-dependent protein from human bone. J Biol Chem 1980;255:8685-8691.
[11] Cairns JR, Price PA. Direct demonstration that the vitamin K-dependent bone Gla protein is incompletely y-carboxylated in humans. J Bone Miner Res 1994;9:1989-1997.
[12] Szulc P, Arlot M, Chapuy M-C, Duboeuf F, Meunier PJ, Delmas PD. Serum undercar- boxylated osteocalcin correlates with hip bone mineral density in elderly women. J Bone Miner Res 1994;9:1591-1595.
[13] Szulc P, Chapuy M-C, Meunier PJ, Delmas PD. Serum undercarboxylated osteocalcin is a marker of the risk of hip fracture in elderly women. J Clin Invest 1993;91:1769- 1774.
[14] Knapen MHJ, Hamulyak K, Vermeer C. The effect of vitamin K supplementation on circulating osteocalcin (bone Gla protein) and urinary calcium excretion. Ann Intern Med 1989; 111:1001-1005.
[15] Knapen MHJ, Jie K-SG, Hamuly~ik K, Vermeer C. Vitamin K-induced changes in markers for osteoblast activity and urinary calcium loss. Calcif Tissue Int 1993;53:81- 85.
[16] Price PA, Williamson MK, Lothringer JW. Origin of the vitamin K-dependent bone protein found in plasma and its clearance by kidney and bone. J Biol Chem 1981;256:12760-!2766.
[17] Diaz Diego EM, Guerrero R, de la Piedra C. Six osteocalcin assays compared. Clin Chem 1994;40:2071-2077.
[18] Masters PW, Jones RG, Purves DA, Cooper EH, Cooney JM. Commercial assays for serum osteocalcin give clinically discordant results. Clin Chem 1994;40:358-363.
[19] Banff G, Daveno R. In vitro stability of osteocalcin. Clin Chem 1994;40:833-834. [20] Blumsohn A, Harmon RA, Eastell R. Apparent instability of osteocalcin in serum as
measured with different commercially available immunoassays. Clin Chem 1995;41:318- 319.
[21] Price PA, Nishimoto SK. Radioimmunoassay for the vitamin K-dependent protein of bone and its recovery in plasma. Proc Natl Acad Sci USA 1980;77:2234-2238.
[22] Garnero P, Grimaux M, Demiaux B, Preaudat C, Seguin P, Delmas PD. Measurement of serum osteocalcin with a human-specific two-site immunoradiometric assay. J Bone Miner Res 1992;7:1389-1398.
[23] Power M J, F0trell PF. Solid-phase enzymoimmunoassay for osteocalcin in human serum or plasma with use of monoclonal antibody. Clin Chem 1989;5:2087-2092.
[24] Egsmose C, Dangaard H, Lund B. Detection of bone Gla protein (osteocalcin) by enzyme-linked immunosorbent assay. Clin Chim Acta 1989;184:279-288.