84
23-1 Respiratory System
| Date post: | 17-Dec-2015 |
| Category: |
Documents |
| Upload: | chester-james |
| View: | 218 times |
| Download: | 1 times |

23-1
Respiratory System

23-2
Respiration• Ventilation: Movement of air into and out
of lungs• External respiration: Gas exchange
between air in lungs and blood• Transport of oxygen and carbon dioxide in
the blood• Internal respiration: Gas exchange between
the blood and tissues

23-3
Respiratory System Functions • Gas exchange: Oxygen enters blood and carbon
dioxide leaves• Regulation of blood pH: Altered by changing
blood carbon dioxide levels• Voice production: Movement of air past vocal
folds makes sound and speech• Olfaction: Smell occurs when airborne
molecules drawn into nasal cavity• Protection: Against microorganisms by
preventing entry and removing them

23-4
Respiratory System Divisions• Upper tract
–Nose, pharynx and associated structures
• Lower tract–Larynx,
trachea, bronchi, lungs

23-5
Nose and Pharynx• Nose–External nose–Nasal cavity
• Functions–Passageway for air–Cleans the air–Humidifies, warms air–Smell–Along with paranasal
sinuses are resonating chambers for speech
• Pharynx–Common opening
for digestive and respiratory systems
–Three regions• Nasopharynx• Oropharynx• Laryngopharynx

23-6
Larynx
• Functions–Maintain an open passageway for air
movement–Epiglottis and vestibular folds prevent
swallowed material from moving into larynx
–Vocal folds are primary source of sound production

23-7
Vocal Folds

23-8
Trachea
• Windpipe• Divides to
form–Primary
bronchi
Insert Fig 23.5 all but b

23-9
Tracheobronchial Tree• Conducting zone
–Trachea to terminal bronchioles which is ciliated for removal of debris
–Passageway for air movement–Cartilage holds tube system open and
smooth muscle controls tube diameter• Respiratory zone
–Respiratory bronchioles to alveoli–Site for gas exchange

23-10
Tracheobronchial Tree

23-11
Bronchioles and Alveoli

23-12
Lungs• Two lungs: Principal
organs of respiration–Right lung: Three lobes–Left lung: Two lobes
• Divisions–Lobes,
bronchopulmonary segments, lobules

23-13
Ventilation
• Movement of air into and out of lungs
• Air moves from area of higher pressure to area of lower pressure
• Pressure is inversely related to volume

23-14
Alveolar Pressure Changes
• Basic Chest X-Ray Interpretation
• Deb Updegraff, C.N.S., PICU
• X-rays- describe radiation which is part of the• spectrum which includes visible light, gamma rays
and cosmic radiation.
• Unlike visible light, radiation passes through stuff.
• When you shine a beam of X-Ray at a person • and put a film on the other side of them a shadow
is produced of the inside of their body.

• Different tissues in our body absorb X-rays at different extents:
• Bone- high absorption (white)
• Tissue- somewhere in the middle absorption (grey)
• Air- low absorption (black)

Film Quality
• First determine is the film a PA or AP view.
PA- the x-rays penetrate through the back of the patient on to the film
AP-the x-rays penetrate through the front of the patient on to the film.
All x-rays in the PICU are portable and are AP view

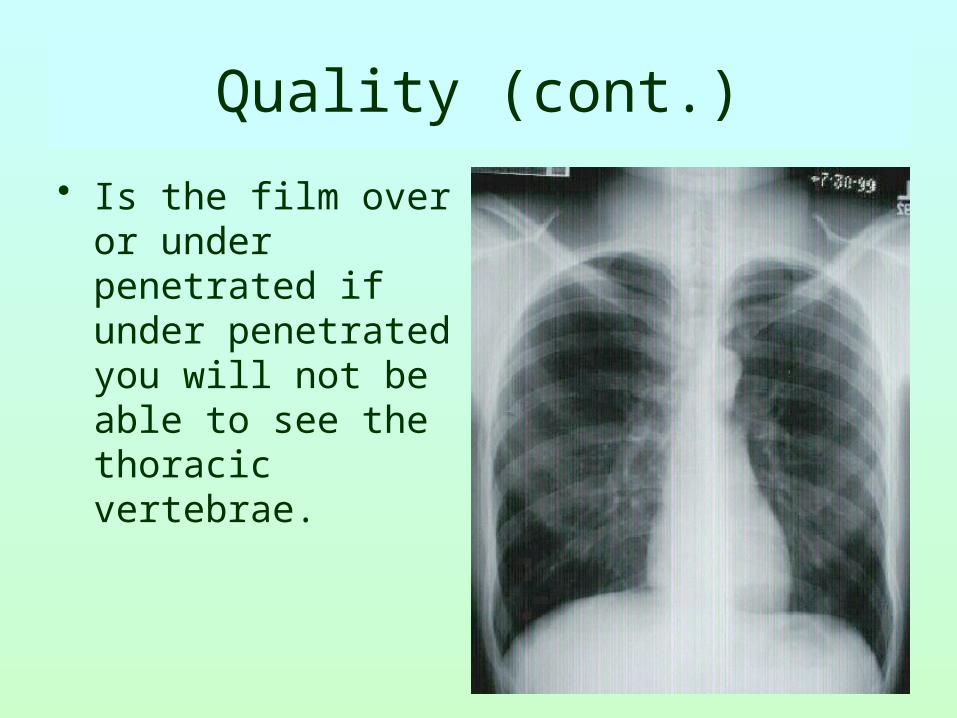
Quality (cont.)
• Is the film over or under penetrated if under penetrated you will not be able to see the thoracic vertebrae.

Quality (cont)
• Check for rotation
– Does the thoracic spine align in the center of the sternum and between the clavicles?
– Are the clavicles level?


LUNG VOLUMES• The total volume contained in the lung at
the end of a maximal inspiration is subdivided into volumes and subdivided into capacities.
• There are four volume subdivisions which:
• do not overlap.• can not be further divided.• when added together equal total lung
capacity.

Capacities
• Lung capacities are subdivisions of total volume that include two or more of the 4 basic lung volumes.
Basic lung volumes (memorize)
• Tidal Volume (TV). The amount of gas inspired or expired with each breath.
• Inspiratory Reserve Volume (IRV). Maximum amount of additional air that can be inspired from the end of a normal inspiration.

Basic lung volumes (memorize)
• Expiratory Reserve Volume (ERV). The maximum volume of additional air that can be expired from the end of a normal expiration.
• Residual Volume (RV). The volume of air remaining in the lung after a maximal expiration. This is the only lung volume which cannot be measured with a spirometer.

Basic lung capacities (memorize)
• Total Lung Capacity (TLC). The volume of air contained in the lungs at the end of a maximal inspiration. Called a capacity because it is the sum of the 4 basic lung volumes. TLC=RV+IRV+TV+ERV

Basic lung capacities (memorize)
• Vital Capacity (VC). The maximum volume of air that can be forcefully expelled from the lungs following a maximal inspiration. Called a capacity because it is the sum of inspiratory reserve volume, tidal volume, and expiratory reserve volume. VC=IRV+TV+ERV=TLC-RV

Basic lung capacities (memorize)
• Functional Residual Capacity (FRC). The volume of air remaining in the lung at the end of a normal expiration. Called a capacity because it equals residual volume plus expiratory reserve volume. FRC=RV+ERV

Basic lung capacities (memorize)
• Inspiratory Capacity (IC). Maximum volume of air that can be inspired from end expiratory position. Called a capacity because it is the sum of tidal volume and inspiratory reserve volume. This capacity is of less clinical significance than the other three. IC=TV+IRV

Now you are ready
• Look at the diaphram:
for tenting
free air
abnormal elevation• Margins should be sharp
(the right hemidiaphram is usually slightly higher than
the left)

Check the Heart
• Size• Shape• Silhouette-margins should be sharp• Diameter (>1/2 thoracic diameter is
enlarged heart)
Remember: AP views make heart appear larger than it
actually is.

• Cardiac Silhouette
1. R Atrium
2. R Ventricle• 3. Apex of L Ventricle
4. Superior Vena Cava
5. Inferior Vena Cava
• 6. Tricuspid Valve
7. Pulmonary Valve
8. Pulmonary Trunk• 9. R PA 10. L PA



Check the costophrenic angles
• Margins should• be sharp

• Loss of Sharp Costophrenic Angles

Check the hilar region
• The hilar – the large blood vessels going to and from the lung at the root of each lung where it meets the heart.
• Check for size and shape of aorta, nodes,enlarged vessels


Finally, Check the Lung Fields
• Infiltrates• Increased interstitial markings• Masses• Absence of normal margins• Air bronchograms• Increased vascularity













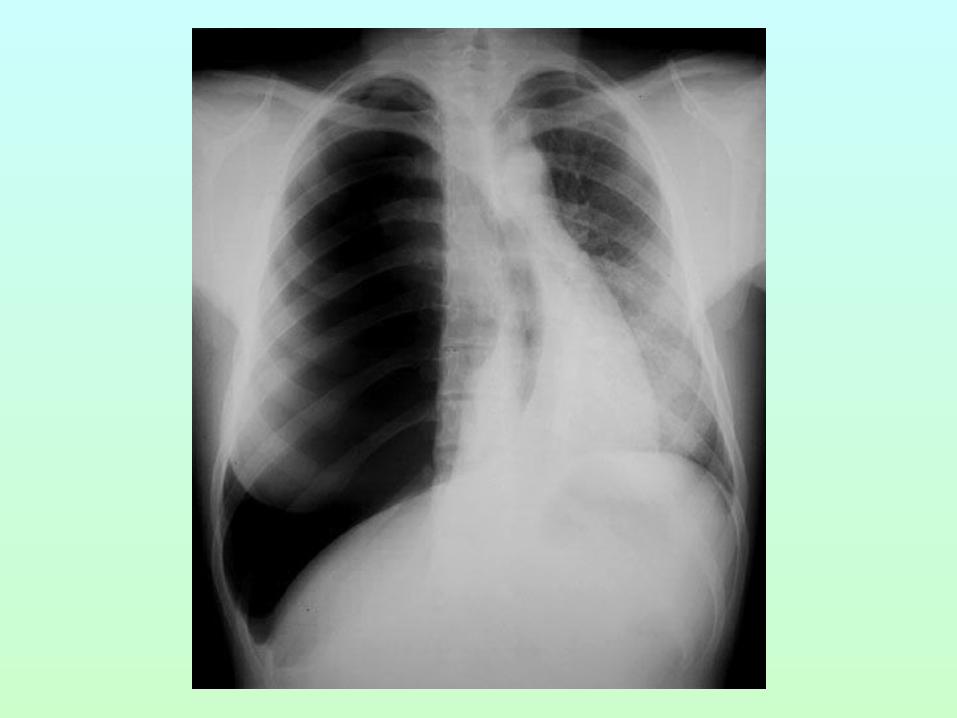
Hemothorax


23-59
Changing Alveolar Volume
• Lung recoil– Causes alveoli to collapse resulting from
• Elastic recoil and surface tension– Surfactant: Reduces tendency of lungs to collapse
• Pleural pressure– Negative pressure can cause alveoli to expand– Pneumothorax is an opening between pleural
cavity and air that causes a loss of pleural pressure
23-60
Pulmonary Volumes• Tidal volume
– Volume of air inspired or expired during a normal inspiration or expiration
• Inspiratory reserve volume– Amount of air inspired forcefully after inspiration of normal tidal
volume
• Expiratory reserve volume– Amount of air forcefully expired after expiration of normal tidal
volume
• Residual volume– Volume of air remaining in respiratory passages and lungs after the
most forceful expiration

23-61
Pulmonary Capacities
• Inspiratory capacity– Tidal volume plus inspiratory reserve volume
• Functional residual capacity– Expiratory reserve volume plus the residual volume
• Vital capacity– Sum of inspiratory reserve volume, tidal volume, and expiratory
reserve volume
• Total lung capacity– Sum of inspiratory and expiratory reserve volumes plus the tidal
volume and residual volume

23-62
Spirometer and Lung Volumes/Capacities

23-63
Minute and Alveolar Ventilation• Minute ventilation: Total amount of air moved
into and out of respiratory system per minute• Respiratory rate or frequency: Number of
breaths taken per minute• Anatomic dead space: Part of respiratory
system where gas exchange does not take place• Alveolar ventilation: How much air per minute
enters the parts of the respiratory system in which gas exchange takes place

23-64
Physical Principles of Gas Exchange
• Partial pressure– The pressure exerted by each type of gas in a mixture– Dalton’s law– Water vapor pressure
• Diffusion of gases through liquids– Concentration of a gas in a liquid is determined by its
partial pressure and its solubility coefficient– Henry’s law
23-65
Physical Principles of Gas Exchange
• Diffusion of gases through the respiratory membrane– Depends on membrane’s thickness, the diffusion coefficient
of gas, surface areas of membrane, partial pressure of gases in alveoli and blood
• Relationship between ventilation and pulmonary capillary flow– Increased ventilation or increased pulmonary capillary blood
flow increases gas exchange– Physiologic shunt is deoxygenated blood returning from
lungs

23-66
Oxygen and Carbon Dioxide Diffusion Gradients
• Oxygen– Moves from alveoli into
blood. Blood is almost completely saturated with oxygen when it leaves the capillary
– P02 in blood decreases because of mixing with deoxygenated blood
– Oxygen moves from tissue capillaries into the
tissues
• Carbon dioxide– Moves from tissues
into tissue capillaries
– Moves from pulmonary capillaries into the alveoli

23-67
Changes in Partial Pressures
23-68
Hemoglobin and Oxygen Transport
• Oxygen is transported by hemoglobin (98.5%) and is dissolved in plasma (1.5%)
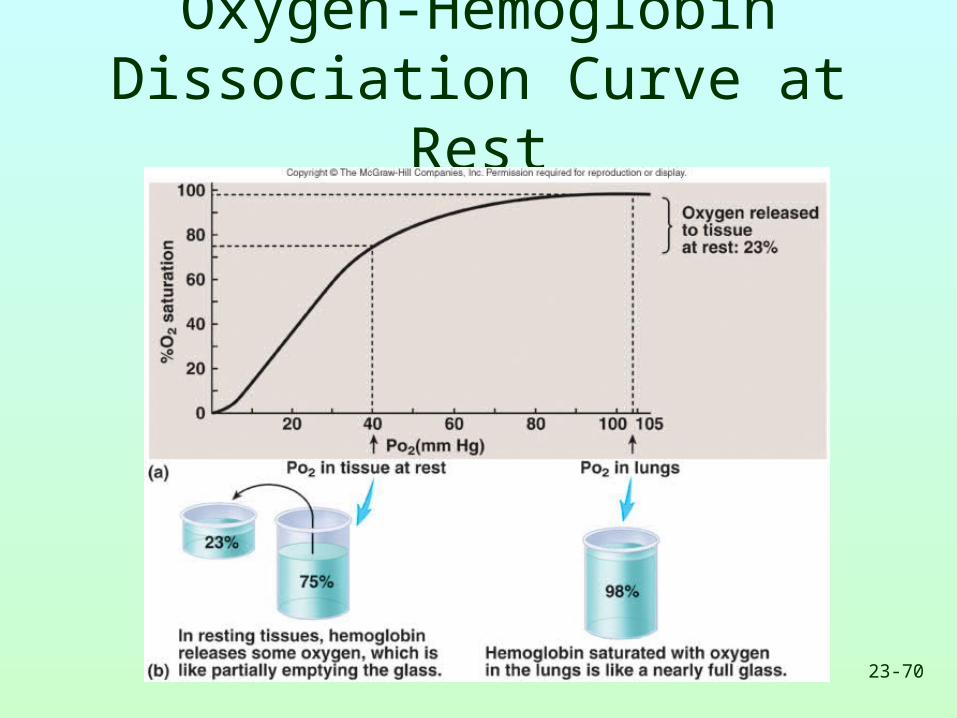
• Oxygen-hemoglobin dissociation curve shows that hemoglobin is almost completely saturated when P02 is 80 mm Hg or above. At lower partial pressures, the hemoglobin releases oxygen.
• A shift of the curve to the left because of an increase in pH, a decrease in carbon dioxide, or a decrease in temperature results in an increase in the ability of hemoglobin to hold oxygen

23-69
Hemoglobin and Oxygen Transport
• A shift of the curve to the right because of a decrease in pH, an increase in carbon dioxide, or an increase in temperature results in a decrease in the ability of hemoglobin to hold oxygen
• The substance 2.3-bisphosphoglycerate increases the ability of hemoglobin to release oxygen
• Fetal hemoglobin has a higher affinity for oxygen than does maternal
23-70
Oxygen-HemoglobinDissociation Curve at Rest

23-71
Oxygen-HemoglobinDissociation Curve during Exercise
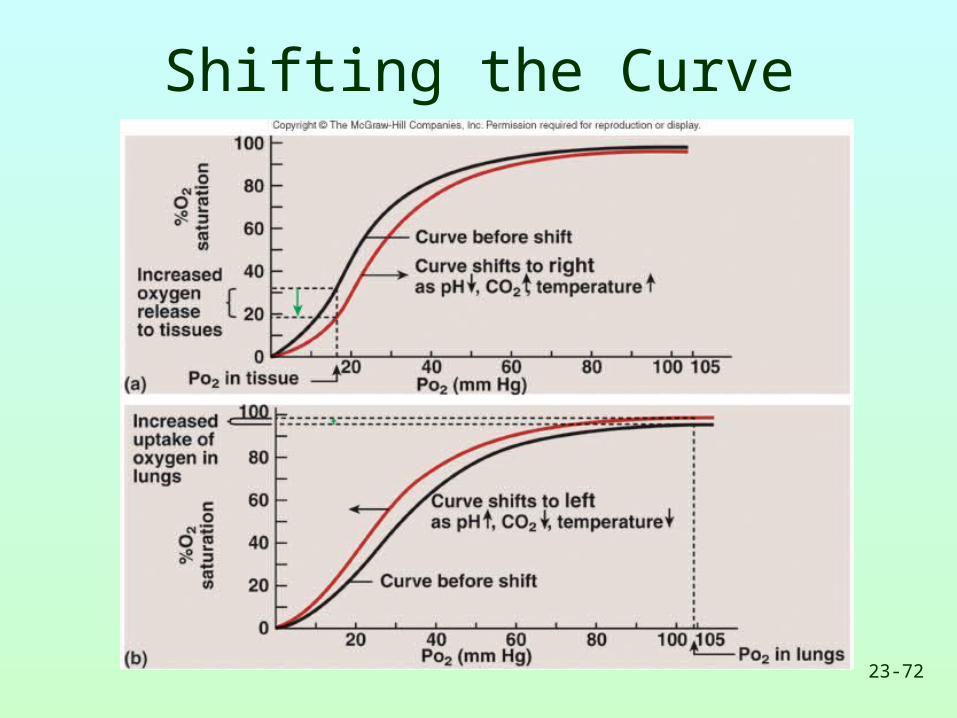
23-72
Shifting the Curve

23-73
Transport of Carbon Dioxide
• Carbon dioxide is transported as bicarbonate ions (70%) in combination with blood proteins (23%) and in solution with plasma (7%)
• Hemoglobin that has released oxygen binds more readily to carbon dioxide than hemoglobin that has oxygen bound to it (Haldane effect)
• In tissue capillaries, carbon dioxide combines with water inside RBCs to form carbonic acid which dissociates to form bicarbonate ions and hydrogen ions

23-74
Transport of Carbon Dioxide
• In lung capillaries, bicarbonate ions and hydrogen ions move into RBCs and chloride ions move out. Bicarbonate ions combine with hydrogen ions to form carbonic acid. The carbonic acid is converted to carbon dioxide and water. The carbon dioxide diffuses out of the RBCs.
• Increased plasma carbon dioxide lowers blood pH. The respiratory system regulates blood pH by regulating plasma carbon dioxide levels

23-75
Carbon Dioxide Transportand Chloride Movement

23-76
Respiratory Areas in Brainstem
• Medullary respiratory center– Dorsal groups stimulate the diaphragm– Ventral groups stimulate the intercostal and
abdominal muscles
• Pontine (pneumotaxic) respiratory group– Involved with switching between inspiration
and expiration

23-77
Respiratory Structures in Brainstem

23-78
Rhythmic Ventilation
• Starting inspiration– Medullary respiratory center neurons are continuously active– Center receives stimulation from receptors and simulation from parts of
brain concerned with voluntary respiratory movements and emotion– Combined input from all sources causes action potentials to stimulate
respiratory muscles
• Increasing inspiration– More and more neurons are activated
• Stopping inspiration– Neurons stimulating also responsible for stopping inspiration and
receive input from pontine group and stretch receptors in lungs. Inhibitory neurons activated and relaxation of respiratory muscles results in expiration.

23-79
Modification of Ventilation
• Cerebral and limbic system– Respiration can be
voluntarily controlled and modified by emotions
• Chemical control– Carbon dioxide is
major regulator• Increase or decrease
in pH can stimulate chemo- sensitive area, causing a greater rate and depth of respiration
– Oxygen levels in blood affect respiration when a 50% or greater decrease from normal levels exists

23-80
Modifying Respiration

23-81
Regulation of Blood pH and Gases

23-82
Herring-Breuer Reflex
• Limits the degree of inspiration and prevents overinflation of the lungs– Infants
• Reflex plays a role in regulating basic rhythm of breathing and preventing overinflation of lungs
– Adults• Reflex important only when tidal volume large as in
exercise

23-83
Ventilation in Exercise• Ventilation increases abruptly
– At onset of exercise– Movement of limbs has strong influence– Learned component
• Ventilation increases gradually– After immediate increase, gradual increase occurs
(4-6 minutes)– Anaerobic threshold is highest level of exercise
without causing significant change in blood pH• If exceeded, lactic acid produced by skeletal muscles

23-84
Effects of Aging
• Vital capacity and maximum minute ventilation decrease
• Residual volume and dead space increase• Ability to remove mucus from respiratory
passageways decreases• Gas exchange across respiratory membrane
is reduced

















