41
Aplasie médullaire Physiopathologie Gérard Socié Hôpital St Louis / Université Paris VII Remerciements: - NS Young - A Risitano - J Maciewsky

Aplasie médullaire Physiopathologie
Gérard SociéHôpital St Louis / Université Paris VII
Remerciements:- NS Young- A Risitano- J Maciewsky

Aplasie médullaire Physiopathologie
Les 2 problèmes !moelle vide maladie rare
Takaku et al, Blood 2010
AA

Moelle osseuse
Thymus
Tiss
u pé
riph
ériq
ue
Cellules souches
ProgéniteurMyélo-érythroïde
CFU-GEMM
Progéniteurlymphoïde
Pro-B
Pro-NK
Pro-T
Pré-B Lymphocyte BPlasmocyte
NK
Cellule dendritique
Pré-T
T auxiliaire
T cytotoxique
Compartiment des cellules souches
Compartiment des progéniteurs
Compartiment de maturation Précurseurs et cellules matures
sang
Cellules dendritiques
CFU-GM
CFU-M Pro-Monocyte Monocyte
Macrophage
CFU-G neutrophile neutrophile
éosinophileCFU-Eo éosinophile
basophileCFU-Baso basophileMastocyte
BFU-MK
BFU-E
Mégacaryocyte Plaquettes
Érythroblaste Érythrocyte
Myé
locy
tes
Gra
nulo
cyte
s
ProgéniteurLympho-myéloïde
Aplasie médullaire Physiopathologie

CSH humaines
CSH
SRC
Cultures à long terme
Prog
énit
eurs
LTC-ICMy, Ly
Tests clonogéniques
CFC
Cellu
les
en c
ours
de m
atur
atio
n
Caractéristiques phénotypiques
Aplasie médullaire Physiopathologie

Aplasie médullaire Physiopathologie
Références Nbre patients Résultats
Marsh et al.1990 32
Bacigalupo et al.1992 46
Stark et al.1993 17
Diminution des CFC n=31
Diminution des CFC n= 46
Diminution des CFC n=15
Progéniteurs déterminés

Aplasie médullaire Physiopathologie
Progéniteurs primitifs
Moelle totale; LTC-IC
CD34

Aplasie médullaire Physiopathologie
Maciejewski, Blood, 1996
Nombre /105 CMN MoelleCD34+ CFC LTC-IC LTC-IC /CD34+
Control 2890+200 210+120 1,95+0,5 1/1280
AA modérée 854+400 27+10 0,29+0,13 1/1220
AA sévère 230+50 1,5+1 0,19+0,03 1/1242
Diminution des LTC-IC corrélée avec la diminution des cellules CD34+
Progéniteurs primitifs

Aplasie médullaire Physiopathologie
Progéniteurs primitifs
Maciejewski, Blood, 1996
Clonogénicité Nombre CFC/ 1 LTC-IC des CD34+purifiées
Control 1/13 (8-20%) 4,3+1
AA modérée 1/60 (1-2%) 2+0,4
AA sévère 1/133 (1%) 1,27+0,1
Capacité de prolifération des CD34+ et des LTC-IC diminués

Aplasie médullaire Physiopathologie
Progéniteurs primitifs
Stroma irradié Mo normale
CD34+ Mo d’AA CD34+ Mo normale
Stroma irradié Mo d’AA
CD34+ Mo normale
Stroma irradié Mo normale
P<0,001
2 3 4 5 6
1 000
100
10
Nom
bre
CFU
-GM
/ p
uits
Normal
CD34 Nl/stroAA
CD34 AA/stro Nl
Marsh, BJH, 1996Semaines
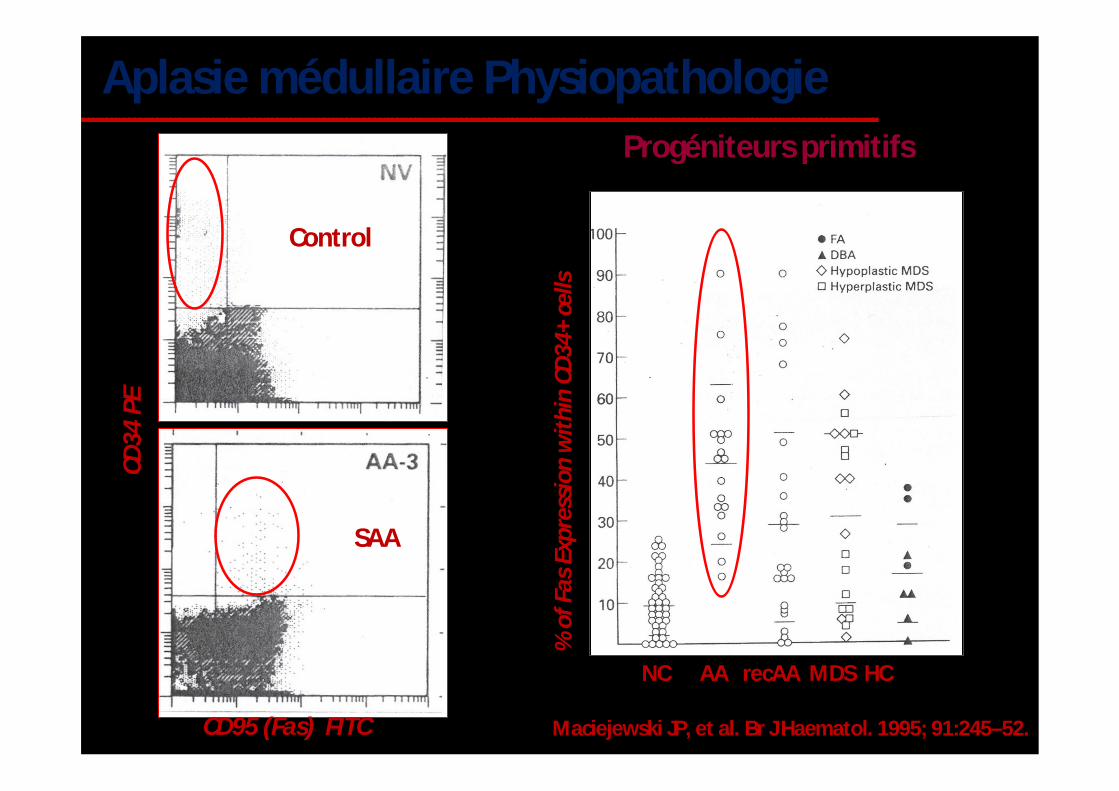
Aplasie médullaire PhysiopathologieProgéniteurs primitifs
Maciejewski JP, et al. Br J Haematol. 1995; 91:245–52.
Control
SAA
CD95 (Fas) FITC
CD34
PE
% o
f Fas
Exp
ress
ion
wit
hin
CD34
+ ce
lls
NC AA recAA MDS HC

Aplasie médullaire Physiopathologie

Aplasie médullaire Physiopathologie
Over-expressed
• Apoptosis
• Stress response
• Cytokine/chemokine transduction
• Defense/immune response genes
• Cell cycle/proliferation inhibitors
Down-expressed
• Cell cycle/proliferation promoters
CD34
“…the transcriptome analysis of HSC in AA is consistent with the presence of stressed, immunologically activated or dying target cells rather than of an intrinsically abnormal population.“
“…the transcriptome analysis of HSC in AA is consistent with the presence of stressed, immunologically activated or dying target cells rather than of an intrinsically abnormal population.“

Aplasie médullaire Physiopathologie
Maladie dysimunitaire
Clinique Reconstitution autologue après allogreffe de moelle Traitement de référence = Immunosuppresseurs
Biologie Lymphocytes T activés (sang et moelle) Phénotype Th1 Action directe cytotoxique ou indirecte (IFN, TNF, MIP1 )
Young, ASH, 2012

Aplasie médullaire PhysiopathologieCIRCULATING ACTIVATED SUPPRESSOR T LYMPHOCYTES IN APLASTIC ANEMIAN.C. Zoumbos, P. Gascon, J.Y. Djeu, S.R. Trost, and N.S. YoungVolume 312 January 31, 1985 Number 5
Perf
orin
PE
Gra
nzym
e B
PE
CD8 PECY5 CD8 PECY5

Aplasie médullaire PhysiopathologieAnti-IFN mAb may restore impaired growth of hematopoietic progenitors in vitro
γ-IFN and TNF-α induce apoptosis of hematopoietic progenitors in vitro
Bone marrow stromal cells transduced with γ-IFN impair hematopoiesis by inducing apoptosis of hematopoietic progenitors

Aplasie médullaire Physiopathologie
Normal control
SAA patient

Aplasie médullaire Physiopathologie
Maladie dysimunitaire
Young, N. S. et al. Blood 2006;108:2509-2519

Aplasie médullaire Physiopathologie
T-bet•T-box family transcription factor essential for Th1 development
•acts downstream Itk and PKC (mostly PKC-Θ)
T-bet

Aplasie médullaire Physiopathologie
Treg Solomou et al., Blood 2007
Peffault de Latour et al., Blood 2010Th17
•Increased in AA patients
•Correlate with disease status
•Normalize after treatment in good responders only

Aplasie médullaire Physiopathologie
Tregs Th1 Th2 Th17Severe vs. non-severe AA
Decreased but not statistically different in severe AA
Tregs Th1 Th2 Th17Aplastic anemia vs. controls
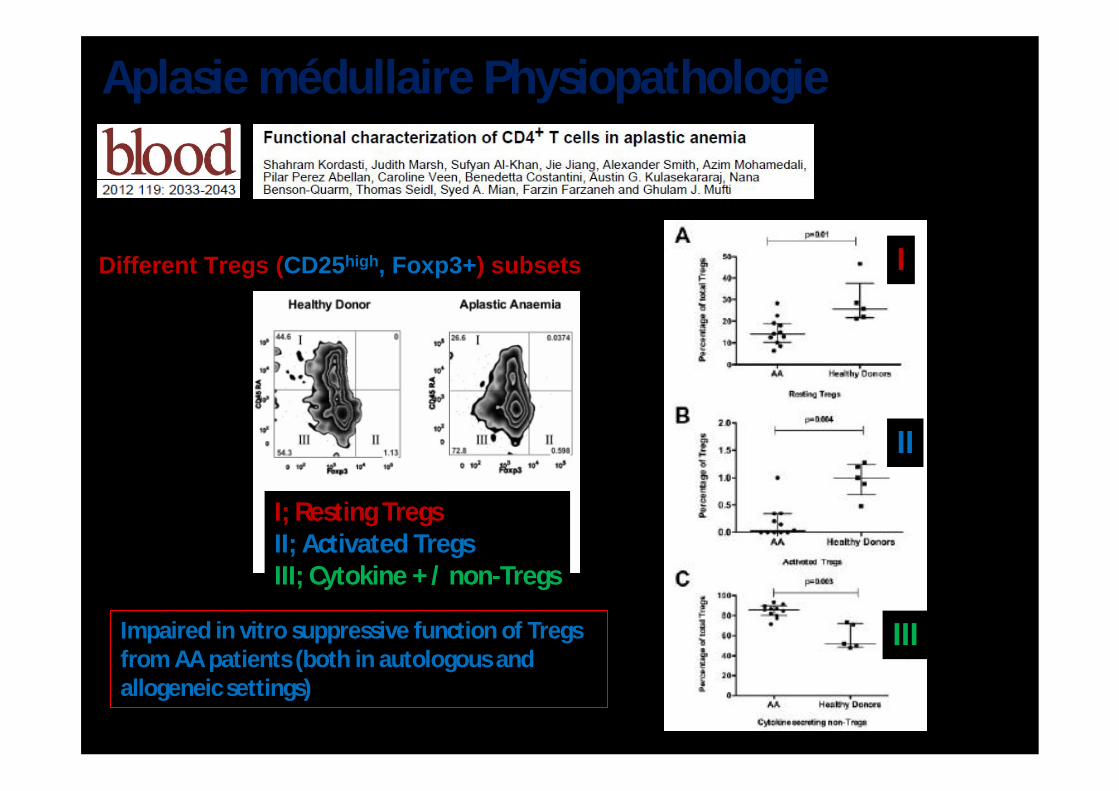
Aplasie médullaire Physiopathologie
Different Tregs (CD25high, Foxp3+) subsets
Impaired in vitro suppressive function of Tregs from AA patients (both in autologous and allogeneic settings)
I
II
III
I; Resting TregsII; Activated TregsIII; Cytokine + / non-Tregs

Aplasie médullaire Physiopathologie
Maladie dysimunitaire

Aplasie médullaire Physiopathologie
Représentation anormale de lymphocytes T CD4 à distribution clonale
Zeng, JCI, 2001

Aplasie médullaire Physiopathologie
Zeng, JCI, 2001
Cytotoxicité(CD34+)
Restreint par HLA-DR
Inhibition des Progéniteurs déterminés
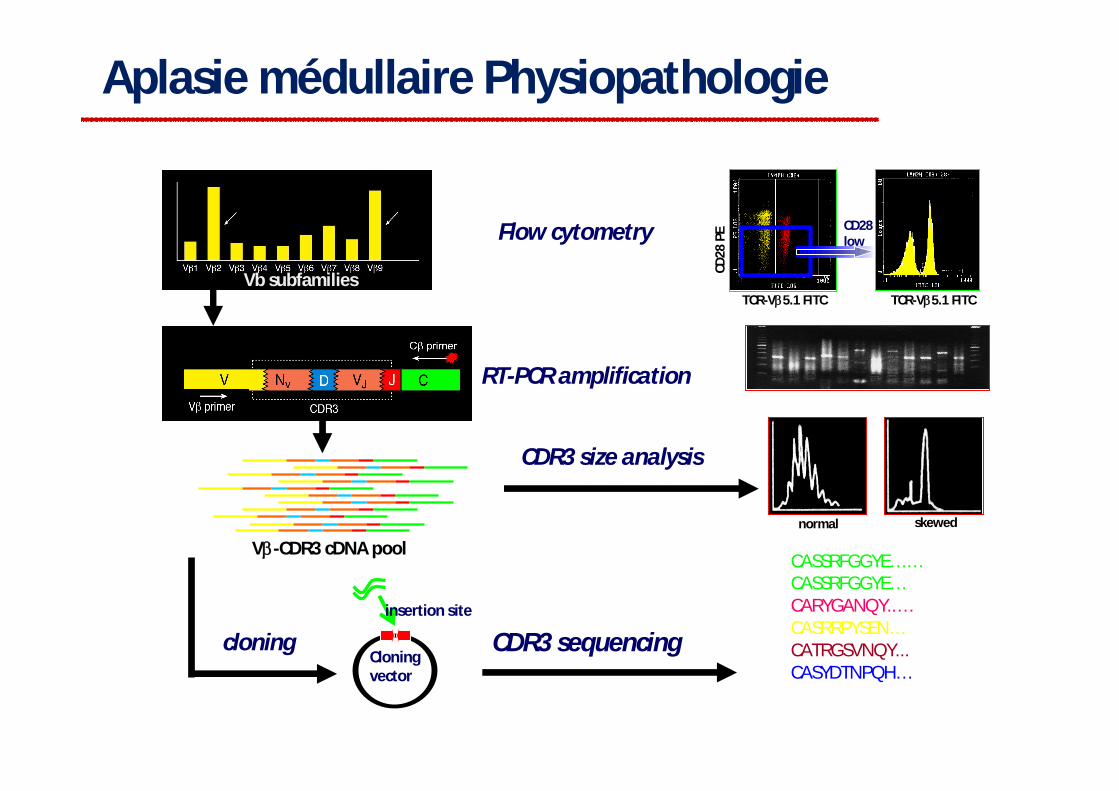
Aplasie médullaire Physiopathologie
Vb subfamilies
V-CDR3 cDNA pool
Flow cytometry
RT-PCR amplification
CDR3 size analysis
insertion site
Cloning vector
cloning CDR3 sequencing
CASSRFGGYE… …CASSRFGGYE…CARYGANQY..…CASRRPYSEN…CATRGSVNQY...CASYDTNPQH…
TCR-V5.1 FITC TCR-V5.1 FITC
normal skewed
CD28 low
CD28
PE

Aplasie médullaire Physiopathologie
BMMNCCD33+CD34+

Aplasie médullaire Physiopathologie
TCR diversity and clonality (on CD4+ subsets)
DiversityDominance
ClonalPolyclonal/oligoclonal

Aplasie médullaire Physiopathologie
Haematologica | 2013; 98(9)

Aplasie médullaire Physiopathologie
1. A pathogenic antibody-mediated autoimmune response?
2. Non-pathogenic antibodies as markers of the underlying immune derangement?
3. An Ag-specific B-cell response interplaying with a T-cell response?
These putative auto-Ag may trigger (as whole proteins or derived epitopes) a cytotoxic T-cell response in vitro (but Ag-specific T-cells were never demonstrated in vivo in AA patients)

T-cell poolEscape from self-tolerance maintenance mechanisms
Newly expressed Ags (exogenous, mutated, cross-reacting, tissue specific)
oligoclonal T-cell response
TCR
hematopoietic stem cells
mature blood cells
Immune pathophysiology of aplastic anemia

T-cell poolEscape from self-tolerance maintenance mechanisms
Newly expressed Ags (exogenous, mutated, cross-reacting, tissue specific)
effector mechanisms— Fas— IFN-g
— TNF-a— Perforin mature blood cellsoligoclonal T-cell response
TCR
hematopoietic stem cells
Immune pathophysiology of aplastic anemia

Aplasie médullaire Physiopathologie
HEMATOLOGY/HEMATOPOIESIS IN“NORMAL” FAMILY MEMBERS WITH TERC MUTATIONS
Hematology
normal peripheral blood counts
mild anemia with macrocytosis
mild thrombocytopenia
Hematopoiesisseverely hypoplastic↓CD34 number↓colony formation↑erythropoietin, thrombopoietin
proband affected sister affected niece unaffected brother

Aplasie médullaire Physiopathologie
0
2
4
6
8
10
12
14
16
0 20 40 60 80 100
controls
age, years
telo
mer
e le
ngth
, kb
His 412 Tyr
Val 694 MetAla 202 Thr
Cys 772 Tyr
Val 1090 Met
patients
TELOMERE LENGTH IN TERT MUTATION LEUCOCYTES

Aplasie médullaire Physiopathologie
C204G
TERTA202TH412YV694MY772C
Dyskerin
Pseudoknotdomain
5’5’
CR7 domain
Template
Box
H/A
C A
dom
ain
CR4-
CR5
dom
ain
TERC
G143AA117C
C116T
110-113
GC107-108AG
C72G130 kD
96-97
378-451
C408G
1-316
G305A
G322A
NHP222 kD
NOP1010 kD
GAR125 kD
L37L37
L321VL321V
57 kD
A353VA353V
A2VA2V
T66AT66A
P40RP40RF36VF36V
E41KE41K
L72YL72Y
M350T/IM350T/IG402EG402E
R65TR65T
K39EK39E
TERC
TELOMERASE COMPLEX GENE MUTATIONS AND BONE MARROW FAILURE

TELOMERE DISEASES
EtOH
smoking
immune, virus ,toxin
envi
ronm
ent
LiverLung
BM
genetic penetrance
physiologic aging
Skin/mucosa
DKC Complex Disease Risk Factors
cirrhosis
pulmonary fibrosis
marrow failure
TERT, TERC+ /-
Calado RT, Young NS, NEJM 2009; 361:2353

Aplasie médullaire Physiopathologie
J. Exp. Med. 2013Vol. 210 No. 7 1311-1329

Aplasie médullaire Physiopathologie
J. Exp. Med. 2013; Vol. 210 No. 7 1311-1329

Toxic agentsViruses
TPO-RDNA damage
Effector T-cells
Apoptosis
Cycling blockade
Proliferation and survival
Cell cyclingGF-Rs
Growth factors
SBDS
c-mpl
?
Perforine/granzyme
Immune polymorphisms?
Autoantigen, altered protein
TCR
Fas-LFas-R Self-
renewal
DNA repair
Telomerase complex genes
FA genes
Lysis
HLA
Mechanisms of hematopoietic stem cell damage
Risitano AM, et al. Curr Stem Cell Res Ther. 2007;2:39–52.
IFN-γ Reactive oxygen species
NO
TRAIL-Rs
TNF-R
IFN-R
TRAIL
TNF-α
+ inflammatory cytokines

ONSET
immune response
incitingevent
Time
RECOVERY
responses, complete/partial
LATE DISEASE
abnormal clone
relapse of pancytopenia
MDS, AML
Hematopoietic stem cells
Peripheral blood counts
clinical presentation
ACQUIRED APLASTIC ANEMIAN
umbe
r

Aplasie médullaire PhysiopathologieJerez A et al. Blood 2013;122:2453-2459

Aplasie médullaire Physiopathologie
ARRAY-BASED KARYOTYPING
Chr 7 Chr X
Loss of heterozygozity
Chromosome 7
D7S1842
1
0.48D7S2471
Copy number
1
0.5RQ
CD3+ Bone marrow






![Prophylaxie des infections post-allogreffe : recommandations ......post-allogreffe) est recommandée [35]. Il n'y a pas de bénéfice d'une seconde dose de vaccin [36]. Recommandation](https://static.documents.pub/doc/80x56/60869edafb35b40e44139f19/prophylaxie-des-infections-post-allogreffe-recommandations-post-allogreffe.jpg)










