29
Community Nutrition Dept. of Public Health and Preventive Medicine FMUP
| Date post: | 19-Dec-2015 |
| Category: |
Documents |
| View: | 236 times |
| Download: | 9 times |
Community Nutrition
Dept. of Public Health and Preventive MedicineFMUP
Epidemiology
Developing countries >> Low socioeconomic status Reproductive women Deficiency Fe main cause of anemia Genetic Deficiency folic acid
IRON DEFICIENCY ANEMIA (IDA)
Fe Deficiency abnormal biochemistry of Fe with or without anemia, caused by;
-decrease bioavailibility of Fe intake. -increase need of Fe(pregnant,lactation ) -increase blood loss (ankylostoma)
Anemia by Fe deficiency occur in severe anemia make the body can not maintain body temperature and could be fatal.
IRON DEFICIENCY ANEMIA (IDA)
Severe anemia (Hb< 4 g/dl) post delivery stress O2 function decreased death.
In pregnant woman low birth weight, prematurity.
Influence also O2 transportation work capacity and productivity decrease
In baby and children influence behavior and intelligence
Factors influence anemia 1. Lack of Fe intake In average woman need 6,5 ug/ day. Inhibitor fitat and polifenol ( in
cereal,peanut, coffee, tea, vegetable)
Enhancer ascorbic acid, and animal protein (cow & chicken meat, fish)
2. Increase physiological need Increase during pregnant, for increasing blood volume, for fetus and placenta, and blood loss during delivery.
Factors.....................cont 3. Excessive blood loss Blood loss can be occurred during operation, disease, menstruation. In average a woman lost 27 cc of blood per menstruation cycle. About 10% lost
more than 80 cc. IUD increase lost of blood 2X, Pill can
decrease amount of menstruation blood 1,5X.
FACTORS..................cont
Placenta praevia and placenta abruption become the risk of lost of blood after delivery process
In average during delivery a woman lost 500 cc blood
Exclusive breast feeding prolong amenorrhae of mother.
Infection /parasitic infection like hook-worm corelate positively with anemia
Blooding can also occurred caused by drug consumption like adrenocorticosteroid, aspirin
Factors.................contLaboratory Increase Hb > 1 g/dl after 1 month Fe
suplementation Fe deficiency anemia Serum feritin < 12mg/cc Fe deficiency Fe status analysis can use concentration of
ferritin serum, saturation transferin, erithrocyt protophorfirin, transferin receptor concentration.
Serum feritin is specific indicator for Fe deficiency during low Fe level.
During infection and edema serum feritin also increase.
Prevention and therapy of IDA
PREVENTION : maintain equilibrium between Fe intake with the need and lost of Fe.
To increase Fe input increase food consumption contain heme-iron.
If not enough from diet Fe supplement Fe supplementation need discipline of the patient. Side effect of Fe is gastric disturbance
Fortification of cereal product is one of strategy for increasing Fe consumption in community.
Prevention............cont
SCREENING Screening is very important to identify
woman group to be treated for reducing anemia morbidity.
CDC Atlanta suggest that woman (youth and adult not pregnant) should be screened every 5-10 years.
If there is risk for developing anemia, screening is conducted yearly.
For pregnant woman screening should be conducted during PNC.
Prevention................cont
THERAPY: Anemia patient should consume 60-120
mg Fe per day and increase consumption of Fe through diet. Check after 1 month, Hb should increase minimal 1g/dl.
Pregnant woman with mild anemia should treated with Fe 60-120mg /day .
After Hb and Haematocrit normal 30 mg/day.
IODINE DEFICIENCY
Deficiency can develop since prenatal stage until old age .
Before, known as Enlargement of Thyroid (Gondok Ind) Can cause abortion, still birth, cretin,
hypothyroid.
ECOLOGY AND DEMOGRAPHY
Not all country have Iodine mineral resources. Most of natural iodine are in the sea and in
the soil. Iodine in soil as I and at the sea as I2
In sea water 50-60ug/l, air 0,7 ug/l, rain water 1,8-8,5 ug/l
Ecology...................cont
Yodium easy to evaporate and sensitive to the light. Yodium from sea water evaporate to
the air to soil with rain or snow. If soil can not keep water to river then to
the sea. In area which cannot keep water
endemic area of deficiency yodium
The cycle
ETIOLOGY OF YODIUM DEFICIENCY
In general nutrition problems can be divided into two :
-Primary: No equilibrium b/w the need and the input. -Secondary: Body cannot use nutrient eg caused by inborn defect metabolism.
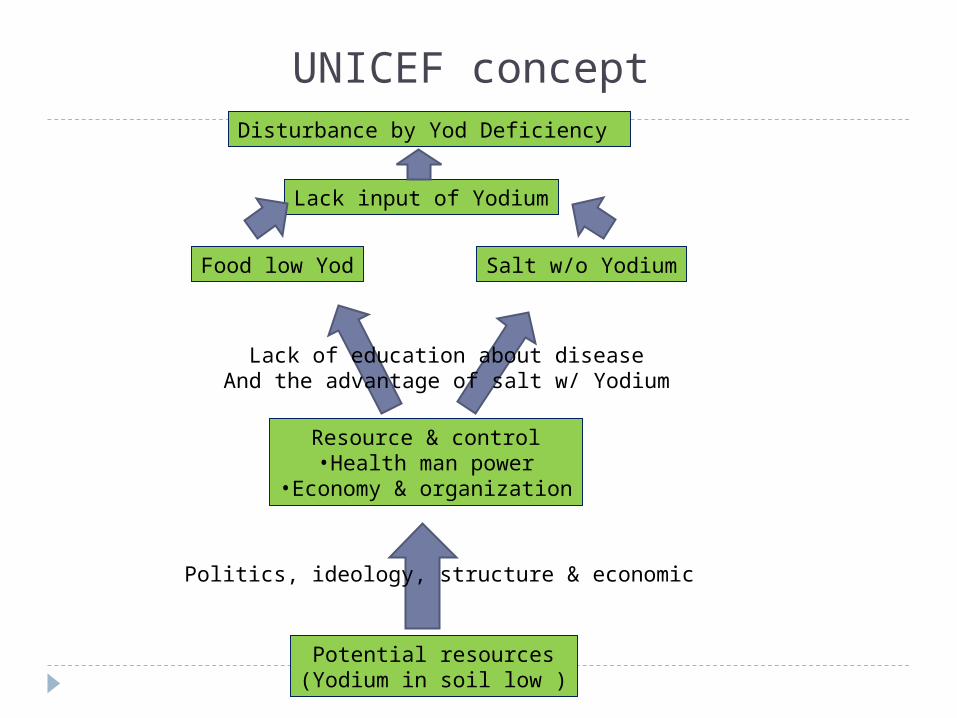
UNICEF conceptDisturbance by Yod Deficiency
Lack input of Yodium
Food low Yod Salt w/o Yodium
Lack of education about diseaseAnd the advantage of salt w/ Yodium
Resource & control•Health man power
•Economy & organization
Politics, ideology, structure & economic
Potential resources(Yodium in soil low )
Toxicity and hyperthyroid
According to Wolf (WHO 1996) excess of iodine can be
divided into 4 groups. Moderate excess of iodine increase absorption
of iodine in thyroid gland and increase production of organic iodine.
Big enough excess of iodine will inhibit release of iodine from thyroxin in and from thyroid gland where release of iodine increased by TSH .
Big excess of iodine inhibit production of organic iodine Goiter
Very big excess will saturate active transportation mechanism of iodine ion
Intake more than 2000 ug Iodine / day dangerous .
Big intake from sea do not dangerous, like in Japan/ china
- thyroid function is normal although more or less than
30 mg/day
- incidence of non-toxic diffuse goiter and toxic goiter
will decreased.
- incidence of Graves and Hashimoto do not influence
by high intake of iodine.
- high intake of iodine will induce hypothyroid and
inhibit effect of thioamide drug.
CRETIN Cretin is caused by irreversible iodine
deficiency. Most dangerous deficiency of iodine. IQ in cretin below standard. Become a burden for a long time (until dead) In general Cretin is developed, if during
organogenesis there is iodine deficiency. Cretin can be seen clearly after the age of baby
more than 12 months Prevalence in baby with breast feeding is less
than baby with formula milk.
Diagnosis Diagnosed based on damage of central nervous
system Symptoms : mental retardation, bilateral
perceptive deaf, neuro-motoric damage. Hypothyroid obstacle of height and weight
development In severe hypothyroid myxoedema In mild hypothyroid ossification inhibition
Early sign & symptoms Weak and sleepy (lethargic) Growth problems Constipation Swollen face and dumb expression Chink-eyes Thick and big tongue Rough and dry hair. Fat deposit at fossa supraclavicularis and neck. Big belly and hernia umbilical Short and fat, dry skin and low body temperature Non pitting edema.
Iodine status examination Biochemistry : - creatinin in urine ; normal = more than 50ug I2/g creatinin hypothyroid = 25-50 ug I2/g creatinin cretin = < 25 ug I2/ g creatinin Thyroid gland enlargement 2 stages stage II can be seen in normal head position stage I cannot be seen in normal head position but visible when the head in lift up position.
Indicator for thyroid gland enlargement
Total Goiter rate (TGR) and Visible Goiter Rate (VGR)
TGR= Group I + Group II / children examine x 100
VGR= Group II / children examine x 100 Mild TGR 5,0 – 19,0% Medium TGR 20,0 – 29,0% Severe- TGR > 30%
Program
In mild area salt iodization and economic development,
In medium area salt iodization 20-40 ppm and iodine oil capsules
In severe area iodine oil capsules
Program steps Situation analyses of disorder cause by
deficiency of Iodine. Communicate data to health and public
health professionals . Plan of action by MOH. Socialization of program in local language Organization development and partnership with local government. Monitoring & evaluation.
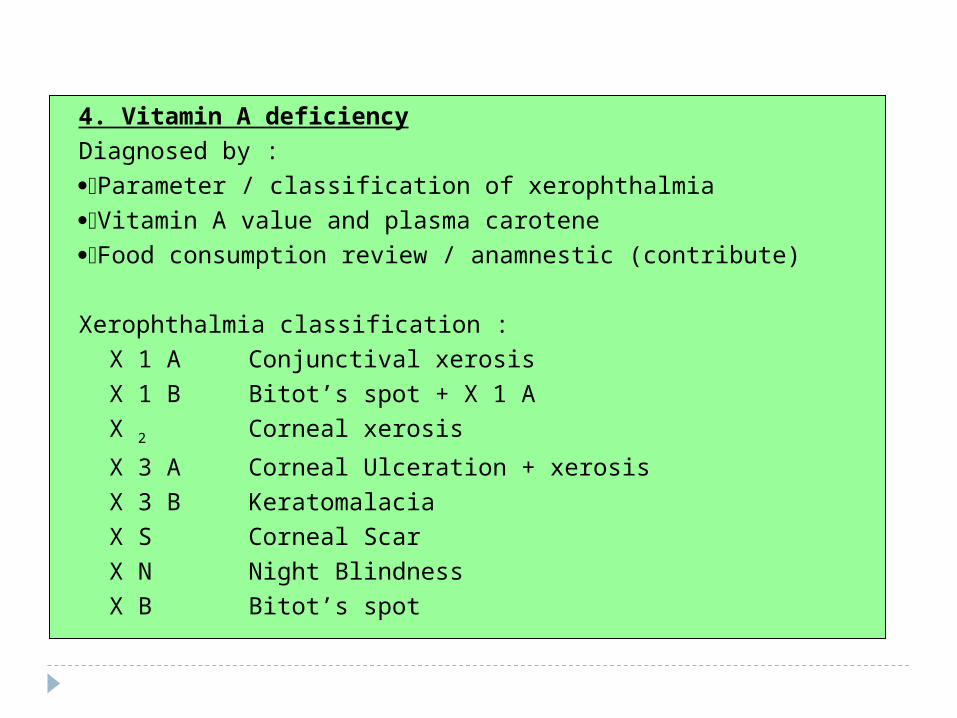
4. Vitamin A deficiency
Diagnosed by :
Parameter / classification of xerophthalmia
Vitamin A value and plasma carotene
Food consumption review / anamnestic (contribute)
Xerophthalmia classification :
X 1 A Conjunctival xerosis
X 1 B Bitot’s spot + X 1 A
X 2 Corneal xerosis
X 3 A Corneal Ulceration + xerosis
X 3 B Keratomalacia
X S Corneal Scar
X N Night Blindness
X B Bitot’s spot
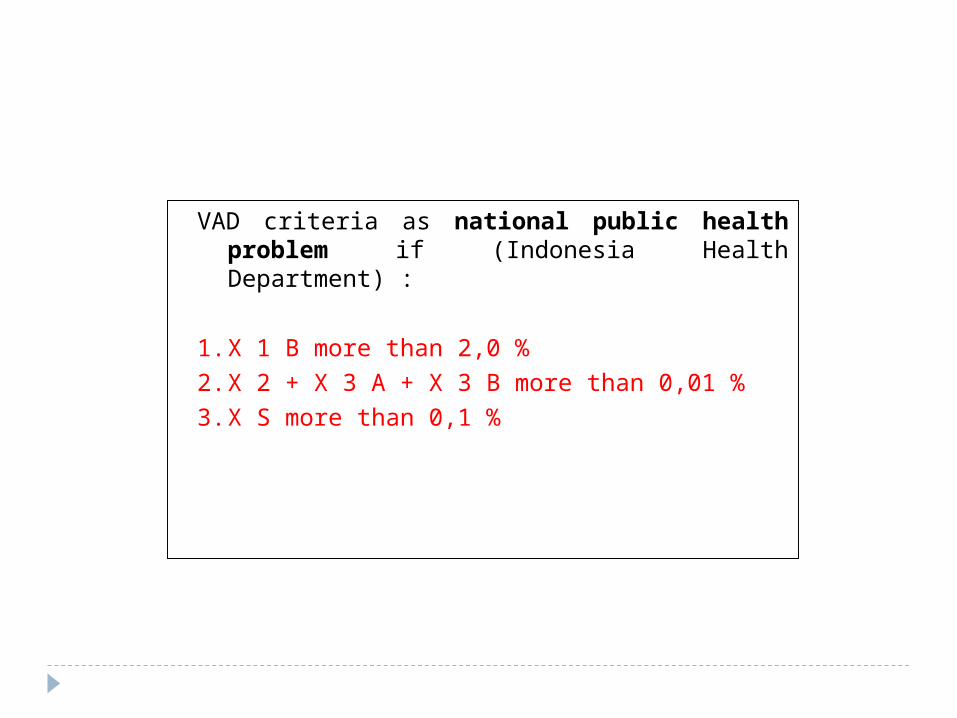
VAD criteria as national public health problem if (Indonesia Health Department) :
1. X 1 B more than 2,0 %
2. X 2 + X 3 A + X 3 B more than 0,01 %
3. X S more than 0,1 %
Thank you

















