Board of Directors Public, 18 December 2014, confirmed minutes Version 1.1 Author: Sally Willcox Department: Corporate Page 1 of 13 Date produced: 19 th December 2014 Retention period: 30 years confirmed Minutes of the Board of Directors – Public Session held on Thursday 18 December in the Conference Room, Library, Sergeants Walk, St Andrew’s Street North, Bury St Edmunds, IP33 1TZ Present: Gary Page: Trust Chair (Chair) Hadrian Ball: Medical Director Bohdan Solomka: Medical Director Designate John Brierley: Non-Executive Director (09.15) Andrew Hopkins: Director of Finance Peter Jefferys: Non-Executive Director Tim Newcomb: Non-Executive Director Brian Parrott: Non-Executive Director Marion Saunders: Non-Executive Director Jane Sayer: Director of Nursing, Quality & Patient Safety Michael Scott: Chief Executive Stuart Smith: Non-Executive Director Adrian Stott: Non-Executive Director Debbie White: Director of Operations (Norfolk & Waveney) Graham Creelman: Non-Executive Director ( 9.15) Sara Fletcher: Physical Health Team Leader (for item 14.171 viii) In attendance: Ian Young: Associate Director Robert Nesbitt: Trust Secretary Sally Willcox: Acting Assistant Trust Secretary (minutes) There were 8 governors and 1 member of staff in attendance. Meeting commenced at: 0900 There was a break: 11.26 – 11.38 / 12.30 – 13.00 Date: 22 nd January 2015 A Item: 15.03
Transcript
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 1 of 13 Date produced: 19th
December 2014 Retention period: 30 years
confirmed
Minutes of the Board of Directors – Public Session
held on Thursday 18 December in the Conference Room, Library, Sergeants Walk, St Andrew’s Street North, Bury St Edmunds, IP33 1TZ
Present:
Gary Page: Trust Chair (Chair)
Hadrian Ball: Medical Director
Bohdan Solomka: Medical Director Designate
John Brierley: Non-Executive Director (09.15)
Andrew Hopkins: Director of Finance
Peter Jefferys: Non-Executive Director
Tim Newcomb: Non-Executive Director
Brian Parrott: Non-Executive Director
Marion Saunders: Non-Executive Director
Jane Sayer: Director of Nursing, Quality & Patient Safety
Michael Scott: Chief Executive
Stuart Smith: Non-Executive Director
Adrian Stott: Non-Executive Director
Debbie White: Director of Operations (Norfolk & Waveney)
Graham Creelman: Non-Executive Director ( 9.15)
Sara Fletcher: Physical Health Team Leader (for item 14.171 viii)
There were 8 governors and 1 member of staff in attendance.
Meeting commenced at: 0900
There was a break: 11.26 – 11.38 / 12.30 – 13.00
Date: 22nd
January 2015 A
Item: 15.03
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 2 of 13 Date produced: 19th
December 2014 Retention period: 30 years
14.166 Chair’s welcome, notification of any urgent business and apologies for absence
Gary Page opened the meeting with an apology for the length of the Board agenda and asked that any interventions be kept brief and pertinent so as to keep to the time schedule he also asked the Board to note that the Charitable Funds paper marked as AOB would be taken with the Chair’s report.
14.167 Standing Item: Declarations of Interest
Declarations of interest were present to the Board with nothing further to add.
The Board NOTED the Declarations of interest
14.168 To approve the minutes of the previous public meeting held on 23rd October 2014
The Chair asked the Board to note the minutes of the Public Board held on 23rd October.
Minutes of the Public Board held on 23rd October were APPROVED with no amendments.
14.169 Chair’s Report
The Chair asked that his report be taken as read and added that he recently attended the East of England Mental Health Chairs’ meeting and asked the Board to note that it was reported that all except one other Trust had issues with Out of Area (OOA) placements. It was noted that no other trust takes 100% of the financial risk in respect of OOA placements as the respective Clinical Commissioning Groups (CCGs) make a financial contribution. It was agreed that a firmer line should be taken with the Norfolk and Suffolk CCGs in respect of this.
The Chair further advised that all the Eastern Mental Health Trusts had indicated that their view was they would be experiencing a financial deficit within two or three years and that they had made this clear to Monitor. Brian Parrott asked if it were worth building on this and sending a joint communication to Monitor on the matter.
Tim Newcomb asked that the Board be provided with a better understanding of the political agenda in respect of Monitor and Michael Scott advised that he would provide the Board with an overview of the Five Year Vision / Plan written by Simon Stevens.
The Board NOTED the report.
Action 14.169 – Five Year Vision
Provide the board with an overview of the Five Year Plan written by Simon Stevens (Michael Scott)
14.170 CEO’s report
Michael Scott highlighted the key points of his report as follows:
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 3 of 13 Date produced: 19th
December 2014 Retention period: 30 years
There was a very positive account from Norfolk concerning the re-tendering of the IAP service journey. He advised the Board that NSFT were the only contender but were in a strong position with MIND being excellent partners.
Michael Scott asked that the Board note the changes to Directors portfolios arising from the resignation of Jane Marshall-Robb and confirmed that Jane Sayer would take education portfolio supported by Dawn Collins.
Michael Scott advised that there had been a positive resolution concerning the gentleman resident in St John’s and pointed out that the EDP had reported that this person was not a service user of the Trust.
The Board NOTED the report
14.171 Items for approval
i. Patient Safety and Quality Report (Dr Jane Sayer)
Jane Sayer advised that the timing of this report meant that it was an ‘exception’ report. She advised that the Quality Governance workshop held in November resulted in a good relationship with Locality Managers and Matrons with them acquiring an improved oversight of the quality goals of organisation.
Peter Jefferys advised that he had attended the workshop and wanted to added that the enthusiasm and commitment from staff to make the changes work going forward was very clear.
Jane Sayer advised that the Service User and Carer Involvement and Engagement Strategy Group were looking for a steer from the Board concerning their priorities.
Gary Page advised that the Board would provide a steer to the group and that he and Jane Sayer would discuss the matter.
Gary Page highlighted his concern in respect of a complaint about staff talking in front of a service users in a language they did not understand. Jane Sayer advised that the staff concerned where NHSP and that a communication would be sent out to all staff highlighting the requirements to converse in language that service users understand and asking that staff challenge directly any incident when this is not the case.
Gary Page asked how many people were currently in the community and awaiting allocation of a care co-ordinator. Debbie White advised that this applied to around 500 people who had been assessed as low risk and that additional resources of 12 Band 6 and 6 Band 4 staff was being progressed however, resolution of the issue would be some months away.
Peter Jefferys asked is a refresher communication could be sent to all those on the waiting list indicating a timeline for intervention.
Debbie White advised that service users were written to advising them of the wait and that she would write to them again with an update advising them that stress control workshops and re-assessments could be offered.
Gary Page said that he was keen to ensure that service user expectations were managed correctly and that the Trust needed to be clear on what the service can deliver and when.
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 4 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Gary Page highlighted the high levels of reporting in respect of restrictive interventions and asked what support was in place for staff. He expressed concern that the issue was a big concern and asked what more could be done to drill down into the information presented.
Jane Sayer advised that the reporting of these interventions fitted with the implementation of Department of Health (DoH) guidance on reducing restrictive interventions and that the Trust were awaiting further guidance. Currently the staff record any incident when there is any hands-on contact with staff/service users and all assaults on staff are recorded. Figures suggest that there is confusion about what should be recorded as restraint with a need to take all incidents against staff seriously.
Jane Sayer advised that staff affected receive regular support with the offer of occupational health referrals and counselling. She further advised that should a staff member concerned have a record sickness from work as result of an assault this is recorded as a RIDDOR.
John Brierley added that the figures are skewed as the forensic service is included and he asked the Board to recognise that the Learning Difficulties Inpatient service recorded a high degree of assaults.
Robert Nesbitt advised that one issue was the racial abuse of black staff by service users and work was being undertaken with the police to help resolve this. It was reported that police involvement could be helpful, particularly at the Norvic who have picked up working with the police.
Stuart Smith advised that he was pleased to see the start of the Family and Friends (F&F) test results and noted that these reports would be made to the Board monthly.
Action 14.171i
a. Staff (including NHSP staff) to be reminded not to talk in a non-English language to each other in front of patients, before January board meeting (Jane Sayer)
b. Patients on community waiting lists to be written to update on likely wait times and advise of stress reducing workshops and re-assessments (Debbie White).
ii. Safer Staffing (Dr Jane Sayer)
Jane Sayer advised that the paper was the second 6 monthly report reviewing staffing levels. She reported that no guidelines had been released by the DoH for mental health staffing levels. Jane reported that currently the trust was using a process of benchmarking with similar organisations and discussion with Ward Managers to ascertain the levels.
Brian Parrott asked how figures for 1 on 1 nursing requirements were reconciled in respect of temporary staffing needs. Jane Sayer advised that e-rostering would help with this along with Ward Managers overview of what is required.
Jane Sayer advised that more flexible working for permanent staff was being considered to better serve the needs of the Trust and that further work with Team Leaders would take place in respect of this and the need to manage with the resources given to them.
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 5 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Gary Page asked for an overview of numbers in relation to own staff verses agency and Jane Sayer advised that this varied from ward to ward. Jane also reported that the rise in HCAs was as a result of NHSP struggling to provide registered nurses. Michael Scott advised that there was not an issue of overstaffing.
Debbie White advised that 90% of HCAs are agency staff and that the clinical vacancies are now below 10%.
Tim Newcomb asked when the Board would be advised of the permanent staffing requirement of the Trust and the cost of this. Andrew Hopkins advised that the current agency spend is higher than the spend would be on permanent staff once in post. Jane Sayer advised that work was ongoing with Team Leaders in respect of staffing requirements and staffing budgets.
John Brierley raised concerns that the figures showed a lack of basic management control at an operational level. Gary Page advised that there was a need to identify areas where the staffing compliment was wrong and that there was a need to revisit the use of temporary, bank and NHSP staff. Leigh Howlett advised that the Temporary Staffing Process Board was currently looking at this.
Marion Saunders asked if there was a need to devolve budgets to the lowest possible level in order to give staff management of their own budgets. Jane Sayer reported that the Team Leaders session held on 16 December had given an indication that they wanted more autonomy in respect of staffing and budget control.
Action Min 14.171ii
For future board papers, the table showing the ration between registered nurses and HCAs (where there is over-staffing of HCAs to compensate for understaffing of registered nurses) to be presented to as to show the trend over time. (Jane Sayer)
iii. Service Governance Committee Chair’s report (Peter Jefferys )
Peter Jefferys asked that this report be taken as read advising that there was still more work to do and that the committee would be restructured in January with Lead Clinicians attending to assist with this.
Michael Scott advised that the outstanding recommendations figure actually only related to 26 different issues.
John Brierley advised that he felt that the Board should take more ownership of policies. Gary Page asked what determined policies coming to the Board.
Robert Nesbitt advised that there was no written understanding of what came to Board in respect of policies and that the key factors were risk, in respect of Board objectives, and the relationship to strategy. Robert reported the need for proper monitoring and a tightening up of the process.
It was agreed that Robert Nesbitt and Gary Page would discuss the need for the Board to own some of the policies.
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 6 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Action 14.171 iii (Service Governance Committee)
For the January BoD meeting Gary Page and Robert Nesbitt to identify which policies should come to the board for approval. (Robert Nesbitt)
iv. Finance Report M08
Andrew Hopkins introduced the Finance report advising that month 8 had seen a downturn in finances due to Out of Area placements however there had been a turnaround in performance due to fewer temporary staff being used. The Board noted that Out of Area placements were down to 24 as of 17 December 2014.
Andrew reported that the revised financial forecast showed an improvement in the cash position and that further funding would come from St Clements in March if the sale progresses.
Andrew asked that the Board note that there had been a spend of £3m capital against a plan of £6.6m and that this would be reported to Monitor.
Andrew Hopkins advised that there would be significant savings to be had once Thurne ward was open as this could reduce the Out of Area placements to zero. Further he reported that there would be additional funding coming in respect of resilience funding from the CCGs. He advised of the need to hit the improved CQUIN targets. He further advised that in non-pay terms there were a number of unspent budgets relating to maintenance and training which were being pushed back to 2015/16.
Gary Page asked what assumptions were being made in respect of Thurne Ward and Out of Area placements. Andrew Hopkins advised that the figures were based on a 50% reduction of current out of area placements.
Adrian Stott advised that 1 in 5 current inpatient service user was the responsibility of social services however, their budgets could not cope with demand. He advised that as these people were ‘bed-blocking’ a more aggressive approach with the County Council was taken on this.
v. Business Performance Report M08
Andrew Hopkins asked the Board to note that the Trust was meeting the Monitor targets however, delayed transfers had increased. He advised that in January the quarter 3 compliance to Monitor would be made.
Andrew further reported that the quality of data entry had seen good improvements.
The Board recorded appreciation to Denise and team on the work they had done on this and Michael Scott advised that he had personally done this but would reinforce the message from the Board.
Action 14.171 v
Thanks to be passed to Denise Grimes on behalf of the board for the progress on the action plan. (Michael Scott)
vi. Finance and Performance Committee Chair’s Report 16 December (Stuart Smith)
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 7 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Stuart Smith gave the following verbal report to the Board:
‘The key messages from the F&PC meeting held 2 days ago but also including thinking that emerged from an extraordinary F&PC meeting held the previous week. I will start with our financial position and outlook:
I would like to draw your attention to page 7 of the minutes (that is attachment B). The essence of what I said on the 23rd October remained true during much of November. However there is some positive news about the way we have grasped the challenges and moved on from that time.
Andrew has outlined our more immediate financial position, outlook and the importance of the Financial Recovery Plan and it is my intention to focus on the key points.
a) firstly, it is the opinion of the F&PC that the Trust can deliver a COSRR of 2 throughout the remainder of this financial year 2014/15. The likely outcome as a result of a number of financial recovery actions being a full year deficit of approx. £3.7m rather than the £5.3m previously forecast. The year-end cash balance is likely to be approx. £10m. This takes into account the ongoing difficulties with temporary staffing and OOA placements which I will come back too shortly.
b) secondly, for 2015/16 and 2016/17 our focus has been to ensure we are constantly striving for a COSRR of 2 in the next financial year, 2015/16 and a trajectory towards a 3 in 2016/17. To this end the Board have reluctantly agreed that in the light of no significant improvement to funding that an income and expenditure improvement target of approx. £15.3m in 2015/16 is necessary. So far £8.6m has been provisionally identified and so a further £6.7m is required at least and with a view to 2016/17 yet more income and expenditure improvements will be required.
To ensure that we hit these financial targets and achieve our COSRR ambition a feasibility study is being embarked upon with the intention of finding the further £6.7m plus a bit more in 2015/16 and the as yet unquantified further improvements needed for 2016/17. This feasibility study is planned to be delivered to the March F&PC and BoD and will be testing the feasibility of a series of potentially transformational initiatives amongst other things. The significance of the output from this FS should not be under estimated as it will need to take a hard look at many aspects of the Trusts operations. The FS team will be led by Cynthia Conquest who will report into Andrew Hopkins and the FRP steering committee. The F&PC have stressed the importance of giving this work priority and ensuring adequate resources are available to Cynthia In summary, the financial challenges are understood and a fresh approach to solving them is being pursued.
2 integrated Performance Report
Discussions centred on Data Completeness, IAPT and several aspects of OOA issues. An encouraging improvement in the level of data completeness and access to IAPT were noted along with further initiatives to reduce OOA
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 8 of 13 Date produced: 19th
December 2014 Retention period: 30 years
placements which will be covered more fully by other Board colleagues 3 Bi-monthly workforce update:
The current position was noted and discussion centred on the need for further improvements to the time it takes to recruit staff to assist in reducing the temporary pay spend. Whilst more can be done the general staff shortages facing the NHS cannot be ignored.
4 Report of Significant Partners:
This report remains embryonic but is nonetheless a useful prompt to discussing the health of key relationships. To this end it is considered appropriate for this report to be considered by the Board as a whole and I recommend that this is done so as soon as possible’.
A question was raised on the ‘cost base’ and Stuart Smith advised that the Board is looking much harder at its cost base with a clear willingness to do this.
Graham Creelman advised that the Board needed to concentrate on what they can fix as opposed to issues that are about the condition of the NHS which cannot be fixed locally.
Gary Page advised that the Terms of Reference had been formulated for the feasibility study and that these would be presented to the Private Board.
vii. Board Assurance Framework (BAF) (Robert Nesbitt)
Robert Nesbitt advised that the executive team had revisited the Datix risk and these had been updated on the BAF.
John Brierley raised concerns about the wording in ‘system confidence’ and Robert Nesbitt, Michael Scott and John Brierley agreed to meet to discuss and agree on wording.
Action 14.171vii
Robert Nesbitt and John Brierley to meet to consider how to divide the system confidence themes into separate themes. (Robert Nesbitt)
viii. Smoking Policy (Jane Sayer)
Sara Fletcher attended for this item and advised that Bohdan Solomka (Medical Director designate) would be the operational lead on this.
Gary Page asked for the opinion of each Board member prior to voting taking place.
Bohdan Solomka advised that the true desire of the Trust might be complicated by the fact that smoking is a legal activity and that service users feel that by being denied this ‘right’ the trust is making a punitive decision on their behalf. Further, it may introduce an extra element of stress into the scenario.
A vote took place with the following outcome:
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 9 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Recommendation A – five people in favour and eight against.
Recommendation B – thirteen people in favour
Recommendation C – seven in favour and eight against.
Recommendation B was APPROVED by the Board.
Action 17.171viii
Decision of board to adopt option B (harm reduction but without outright ban at this time) to be communicated clearly to staff. (Jane Sayer)
BREAK 11.26 – 11.38
14.172 Items for debate
i. Staff Morale (Michael Scott) incorporating Min 14.161i
Michael Scott presented this report highlighting this as the biggest single issue facing the Trust. He advised that the Board had discussed this in March, prior to his arrival, and that there were a number of good initiatives to consider. He drew the Board’s attention to the need to make better connections between them and the staff.
Michael reported that the Senior Management Forum (monthly meeting of 30 – 40 managers) was extended down to all Band 7 staff for a quarterly meeting on 16th December 2014 and that 120/130 people attended. Michael advised that attendees were delighted to be involved and learn that the Trust needs empowered staff to help them move forward.
Michael Scott advised that the change and development being undertaken was bringing staff ‘on board’ with some very positive reactions. He advised that the Board needed to re-double its efforts to ensure that staff perception became one of a Board that cared for its staff and service users as opposed to being motivated by reducing finances.
Brian Parrott endorsed this approach on behalf of the Organisational Development and Workforce committee. He advised that a workforce priorities paper would be presented to a future Board.
Hadrian Ball raised concerns over the suggestion to encourage staff to ‘email the CEO’ as a previous incarnation of this had seen the Chair inundated with emails. The Board agrees that a ‘CEO Live Chat’ online might be a more manageable option.
Jane Sayer advised that Team Leaders were keen to receive communications from the CEO and to see more high level individuals on the shop floor. Bohdan Solomka advised that engagement rather than events was more productive and promote a ‘business as usual’ message.
The Board agreed that there was a need to be open and honest with Trust staff and allowing proper time to put any new measures in place.
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 10 of 13 Date produced: 19th
December 2014 Retention period: 30 years
ii. Trust Service Strategy lessons learned (Leigh Howlett)
Leigh Howlett asked for the report to be taken as read and advised that the feedback given would be shared with Governors at their next meeting.
Michael Scott advised that the Trust Service Strategy had worked in Suffolk.
Gary Page advised that it was important to understand that there was now no Trust Service Strategy and to learn lessons from the study. He further advised that the Board should stop using this terminology and now remove it from the vocabulary but to reference back to the learnings when needed.
Action 14.172ii
Add point about a staged approach to programme implementation avoiding a ‘carry on regardless’ mind-set to be added to the TSS lessons learned paper before it goes to BoG. (Leigh Howlett)
iii. Board report format refresh (Robert Nesbitt)
Robert Nesbitt asked that the report be taken as read however he advised that a refresh of the design was necessary to ensure that the necessary information was included in the report summary encouraging briefness of the executive summary which should include the key risks.
Marion Saunders advised that previous Boards that she had served on had encouraged members to email the Directors with any questions ahead of the meeting so that the Director could immediately provide any answers.
Michael Scott asked that this process be followed in the future.
Gary Page advised that more focus was needed on what needed to be discusses and that Board members needed to be more disciplined on speaking at the meeting.
Action 17.172ii
a. Add ‘risk of not accepting recommendation’ to the template. (Robert Nesbitt)
b. All directors / NEDs to email queries on BoD papers to director authors so that these can be addresses in the introduction to the paper at the board meeting itself.
14.173 Items for Information
i. Update of Fit and Proper Person test and Duty of Candour (Robert Nesbitt / Jane Sayer)
Robert Nesbitt asked that the report be taken as read.
Marion Saunders asked that an addition be made to include an annual statement from Directors that nothing had happened in the previous 12 months to affect them being a ‘fit and proper’ person.
The Board AGREED this decision.
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 11 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Action 14.173i
Add annual statement of FPPT position to workplan for BoD. (Robert Nesbitt)
LUNCH – 1230 - 1300
ii. Update learning disability service strategy including access to MH services for people with a learning disability incorporating Min 14.49ii (Jane Sayer)
Jane Sayer asked that the report be taken as read advising that the information relating to Suffolk was vague as negotiations are presently underway with the County Council and CCG slow to decide on their input.
Hadrian Ball advised that the Trust were not commissioned to undertake mental health services for people with a learning disabilities however, he reported that the Trust does undertake the treatment of service users who have a learning difficulty along with a mental health illness.
Peter Jefferys advised that people with a learning difficulty should have access to expertise regardless of their LD diagnosis. Bohdan Solomka advised that in Central Norfolk a lot of work had been done in respect of people diagnosed with a learning difficulty with a secondary mental health diagnosis.
Brian Parrott advised that at least two other mental health trusts would be interested in the contract if NSFT did not complete on this and that confidence needed to be built with the County Council and the CCGs.
Michael Scott advised that Executives would discuss access to medicine to LD diagnosed patients.
The Board APPROVED the report.
Action 14.173ii
a. Cost implications for the LD strategy (including capex) to be included in the report to F&P next committee. (Jane Sayer)
b. Email note to be circulated to the BoD on the context and organisational boundaries for mental health services for people with a LD in Norfolk. (Bohdan Solomka)
iii. Report on PLACE (Patient-led Assessments of the Care Environment) (Leigh Howlett)
Leigh Howlett asked that the report be taken as read and confirmed that there had been no material breaches in respect of single sex accommodation.
The Board NOTED the report
iv. Audit and Risk Committee Chair’s Report from 10th December 2014 meeting (John Brierley)
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 12 of 13 Date produced: 19th
December 2014 Retention period: 30 years
John Brierley asked that the report be taken as read and advised that agreement had been made with KPMG to finalise the risks with an agreement that limited assurances would be taken up by the Executive team.
The Board NOTED the report.
v. Communications Committee Chair’s report from meeting 9th December 2014 (Graham Creelman)
Graham Creelman asked that the report be taken as read highlighting the fact that negative publicity had reduced and reporting was showing as neutral.
The Board NOTED the report and the positive trend.
vi. Investment Committee Chair’s report from meeting 16th December 2014 (Adrian Stott)
Adrian Stott gave a verbal report to the meeting for information.
The Board NOTED the report.
vii. OD and Workforce Committee Chair’s Report from 11 December 2014 (Brian Parrott)
Brian Parrott asked that the report be taken as read and requested that the additional paper be circulated to the Board.
He added that there had been good improvement on appraisals in general but not everywhere which could cause problems next year where there are gaps.
The Board NOTED the report.
Action 14.173vii
Circulate the current workforce priority documents (From OD&WRC) to BoD. Sally Willcox
viii. Remuneration and Terms of Service Committee / Joint Rem ToRs / Nom Ctte Chair’s Report from meeting 1st December 2014 (Gary Page)
Gary Page advised that the Terms of Reference needed to be formally approved. Robert Nesbitt advised that he would provide a narrative to the Board in January as to how the ToRs fitted together.
The Board APPROVED the Terms of Reference.
Action 14.173 viii
a. Amend reference to Dir. OD&WF from 6.2 Tor. (Robert Nesbitt)
b. Narrative of how the ToRs fit together to be provided to January board. (Robert Nesbitt)
ix. Charitable Funds Committee Chair’s Report from meeting 8th December 2014 (Graham Creelman)
Board of Directors Public, 18 December 2014, confirmed minutes
Version 1.1
Author: Sally Willcox
Department: Corporate
Page 13 of 13 Date produced: 19th
December 2014 Retention period: 30 years
Graham Creelman asked that the report be taken as read. He advised that the Committee had examined in detail the Charitable Funds Annual Accounts which were brought to the meeting under AOB for approval.
The Board APPROVED the Charitable Funds Annual Accounts.
Gary Page took this moment to extend publicly the Board’s thanks to the work undertaken by Hadrian Ball, the outgoing Medical Director.
14.175 Any other urgent business, previously notified to the Chair
i. The item of AOB was taken under 14.173 ix.
14.146 Date, time and location of the next meeting
The next public meeting of the Board of Directors will be held on Thursday 22nd January 2-15 at 09.30 in the Main Hall, Hellesdon Hospital, Drayton High Road, Norwich, NR6 5BE
Meeting closed at: 1.26
Chair: ……...…..…………………
Date: ……....…………………………….
Page 1 of 2
Matters Arising from Public BoD 18th December 2014
Action Min 14.169 (Chair’s Report)
Provide the board with an overview of the Five Year Plan written by Simon Stevens (Michael Scott)
Provided for strategy day
Action Min 14.171i (Patient Safety and Quality Report)
a. Staff (including NHSP staff) to be reminded not to talk in a non-English language to each other in front of patients, before Jan board meeting. (Jane Sayer)
b. Patients on Community waiting lists to be written to update on likely wait times and advise of stress reducing workshops and re-assessments. (Debbie White)
Complete
Action Min 14.171ii (Safe Staffing)
For future board papers, the table showing the ratio between registered nurses and HCAs (where there is over-staffing of HCAs to compensate for understaffing of registered nurses) to be presented to as to show the trend over time. (Jane Sayer)
On agenda
Action Min 14.171iii (Service Governance Committee)
For the January BoD meeting Gary Page and Robert Nesbitt to identify which policies should come to the board for approval. (Robert Nesbitt)
On agenda
Action Min 14.171v (Business Performance Report)
Thanks to be passed to Denise Grimes on behalf of the board for the progress on action plan. (Michael Scott)
Complete
Action 14.171vii (BAF)
Robert Nesbitt and John Brierley to meet to consider how to divide the system confidence themes into separate themes. (Robert Nesbitt)
Complete
Action 14.171viii (Smoking Policy)
Decision of board to adopt option B (harm reduction but without outright ban at this time) to be communicated clearly to staff. (Jane Sayer).
Complete
Action 14.172ii (TSS lessons learned)
Add point about a staged approach to programme implementation avoiding a ‘carry on regardless’ mind-set to be added to the TSS lessons learned paper before it goes to the BoG. (Leigh Howlett).
Complete
Date: 22nd January 2015
B Item: 15.04
Page 2 of 2
Action 14.172iii (Board Format Refresh)
a. Add ‘risk of not accepting recommendation’ to the template. (Robert Nesbitt)
b. All directors / NEDs to email queries on BoD papers to director authors so that these can be addressed in the introduction to the paper at the board meeting itself.
Complete
Action 14.173i (FPPT)
Add annual statement on FPPT position to the workplan for the BoD. (Robert Nesbitt)
Complete
Action 14.173ii (LD strategy)
a. Cost implications for the LD strategy (including capex) to be included in the report to F&PC next committee, (Jane Sayer)
b. Email note to be circulated to the BoD on the context and organisational boundaries for mental health services for people with a LD in Norfolk. (Bohdan Solomka).
Action 14.173vii (OD&WF)
Circulate the current workforce priority documents (from OD&WFC) to BoD. (Sally Willcox).
Complete.
Action 14.173viii (RemToS)
a. Amend reference to Dir. OD&WF from 6.2 ToR (Robert Nesbitt).
b. Narrative of how the ToRs fit together to be provided to January board. (Robert Nesbitt)
Complete.
On agenda.
Board of Directors Meeting - 22nd
January 2015 Chairs Report
Version 1.0
Author: Gary Page Department: Corporate
Page 1 of 3 Date produced: 13th
January 2015
Retention period: 30 years
Report To: Board of Directors Meeting
Public
Meeting Date: 22nd January 2015
Title of Report: Chairs Report
Action Sought: For Information
Estimated time: 15 Minutes
Author: Gary Page, Chair
Executive Summary:
The report details my most significant meetings and my key observations over the last month.
1.0 Interaction with External Organisations
1.1 I met with Nicholas Gould, (Cognitive Behavioural Therapist) from the Suffolk Well-being Service on the 7th January. Amongst other things we discussed the recent developments in the Wellbeing service
1.2 I met with Toni Lawton (Project Manager) from Sweet Arts a third sector organisation providing creative activities to promote physical, emotional and mental wellbeing of women in Norfolk. 42% of their referrals come from NSFT.
1.3 I met with Julie Meikle CQC inspector to discuss the draft report and also participated in a conference call with Monitor.
1.4 I met with Chris Hedges and the Newmarket Integrated Delivery Team. I was shadowed by a Youth Council member on this visit.
1.5 I am meeting with the Chairs of Norfolk NHS provider organisations on Friday 16th and will provide a verbal update at the Board.
1.6 I have a scheduled meeting with the Chair of Norfolk Health Overview and Scrutiny Committee and will provide a verbal report at the Board.
Date: 22nd January 2015
C Item: 15.05
Board of Directors Meeting - 22nd
January 2015 Chairs Report
Version 1.0
Author: Gary Page Department: Corporate
Page 2 of 3 Date produced: 13th
January 2015
Retention period: 30 years
2.0 Interaction with Services and Staff
2.1 I attended the new Governors meeting on the 6th January 2015 and welcomed the new Governors to the Trust; they are two new public Governors, two new staff Governors and one new service user Governor from Norfolk
2.2 I went to the Trust’s services at Northgate, where I visited NRP and met with Jillian Sinclair and staff. I also met with Dr Larry Ayuba, Lead Clinician and visited the wards at Northgate.
2.3 I went to Lowestoft and, visited 44 Kirkley Cliff where I met with Sari Kelsey and the team and then visited the Community Teams at Victoria House. Morale seemed significantly better than my previous visit and staff commented on a more honest and open approach from the Board.
2.4 I attended the Planning and Performance Sub Group Committee where the main topic was the working of the Service Governance Sub Committee.
2.5 I attended the Equality Leads meeting and gave a presentation on my role as an Equality Lead on the Board.
2.6 I met with the staff Governors (old and new) as part of my initiative to meet with Governors in their constituency’s to discuss areas of particular concerns.
3.0 Interactions with Service Users
3.1 I met with Kevin Pull Chief Executive of Aspire, which works with service users and carers in Great Yarmouth and Waveney. They are keen to find new ways of working with the Trust and are particularly interested in the Resource Centres. Kevin has recently joined the Service User and Carer Trust Partnership.
3.2 I Chaired the Service User and Carers Forum on the 19th December 2014.
4.0 Key Observations
4.1 On my day in Yarmouth and Waveney two of the teams I visited both commented that for the first time in 2 years they were fully staffed with permanent staff. Both said how positive this was for morale and that it was enabling them to look forward and to start thinking about planning. This reinforces just how important the recruitment drive is.
4.2 The issue of Service User and Carer Engagement has been a big theme this month – at the Board of Governors, trust partnership and in a number of bilateral discussions across Norfolk and Suffolk. There is no doubt about the commitment of the Board to Service User and Carer Engagement. There are many examples of it in practice and I was struck at 44 Kirkley Cliff and Northgate Ward how it is happening on the ground outside of the formal structures we have in place. However as Jane Sayer and I have discussed there is an urgent need for structures to be formalised, the strategy completed and communicated so that we
Board of Directors Meeting - 22nd
January 2015 Chairs Report
Version 1.0
Author: Gary Page Department: Corporate
Page 3 of 3 Date produced: 13th
January 2015
Retention period: 30 years
can evidence this on the ground. There is a feeling that communications between the Trust and Service Users and Carers have deteriorated. There are many initiatives which can help us – Lorenzo, Triangle of Care, the refreshed Involvement Strategy. This needs to have greater priority.
5.0 Recommendations
5.1 The Board is asked to note the report.
Gary Page Chair
Board of Directors – 22 Jan 15 Chief Executive Update
Version 1.0
Author MSC/CWC Department: Corporate
Page 1 of 2 Date produced: 8 Jan15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Chief Executive Update
Action Sought: For Information
Estimated time: 10 minutes
Author: Michael Scott, CEO
Director: Michael Scott, CEO
Executive Summary:
This report provides an update on the main issue, insights, observations and activities undertaken by the Chief Executive for the month
1.0 Director of Operations – Suffolk:
1.1 Welcome to Alison Armstrong who many of you may have already met over the past few weeks as she joins the executive team.
2.0 Christmas/New Year visits:
2.1 I met with a number of staff and visited various wards over the Christmas/New Year period which included Kings Lynn, Hammerton Court and Hellesdon Hospital wards and teams.
2.2 Whilst in the Kings Lynn I took the opportunity to meet with Dr Ian Mack and had a general discussion around the challenges to the system in West Norfolk. I have proposed that we consider a whole systems management arrangement in support of the west Norfolk Alliance.
3.0 CQC update:
3.1 The CQC draft report was received just before Christmas. Factual corrections were submitted on the 16th January 2015. A quality summit will take place on 2nd February 2015 with publication of the report the following day.
Date: 22nd January 2015
D Item: 15.06
Board of Directors – 22 Jan 15 Chief Executive Update
Version 1.0
Author MSC/CWC Department: Corporate
Page 2 of 2 Date produced: 8 Jan15 Retention period: 30 years
4.0 Trustwide Medical Staffing Committee
4.1 I attended both LNC and Medical Advisory meeting which were held at Lynford Hall both on one day together with the majority of clinicians from the Trust. A constructive dialogue has commenced with both bodies. Whilst there is considerable pressure on our medical staff they reported feeling more supported.
5.0 Stowmarket visit:
5.1 I visited our offices in Stowmarket. Concerns has been expressed that the more to better quality accommodation in Haymills was delayed. I was able to assure colleagues that the work is out to tender and the move should be complete by October 2015.
6.0 Risks / mitigation in relation to the Trust objectives
6.1 None.
7.0 Recommendations
7.1 The Board is asked to note the content of this report.
Michael Scott Chief Executive
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 1 of 10 Date produced: 12th January 2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Patient Safety and Quality Report, December 2014
Action Sought: For Approval
Estimated time: 10 Minutes
Author: Dr Jane Sayer, Director of Nursing, Quality and Patient Safety
Director: Dr Jane Sayer. Director of Nursing, Quality and Patient Safety
Executive Summary:
This is a report on current quality and patient safety issues. Information is reported on key areas of concern or activity since the last report to the Board in December 2014. The main messages for the Board to note in this report relate to:
• Friends and Family Test progress, and details of respondents. Although the overall response remains very positive, the response rate has fallen to 12 teams in December 2014, and actions taken to raise the rate are summarised.
• Safe Staffing report, including trends for staffing levels, and details of highest and lowest staffing areas. Information from the reporting is used locally to prioritise areas for recruitment, and has been used in the latest establishment assessments.
1.0 Report contents
2.0 Service user safety indicators, including serious incidents, harm free care, and Duty of Candour.
3.0 Service user and carer experience indicators including complaints, initial results from the Friends and Family Test, and an update on Triangle of Care.
4.0 Clinical assurance, including audit and external reports.
5.0 Safe staffing.
6.0 Quality dashboard.
Date: 22nd January 2015
E Item: 15.07i
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 2 of 10 Date produced: 12th January 2015 Retention period: 30 years
2.0 Service User Safety Indicators
2.1 Serious Incidents
During December there were 19 SIs reported. The number of reported Serious Incidents during December is three more than the previous month of November reported at 16. The most reported category was Unexpected Deaths of which there were 14.
Chart 1: Trustwide serious incidents reported, April 2012 – October 2014
2.2 Inquests
Inquests since the last report are detailed in Table 1.
Table 1: Summary of Inquests, December 2014
RCA Locality Inquest Verdict
424 Central Open
482 Central Hanged himself; his intention at the time is not known
435 Central Suicide
415 Great Yarmouth Took own life
471 NRP Drug related death
399 West Norfolk Open
434 Great Yarmouth Died following complications following drug use
The Trust received a Regulation 28 report in December 2014 following an inquest into the unexpected death of a service user. The Coroner asked the Trust to
April May June July Aug Sept Oct Nov Dec Jan Feb March
12 13 14 18 10 14 17 15 17 12 9 11 13 11
13 14 15 7 21 25 8 18 17 9 15 15 8 14
14 15 20 10 25 13 27 16 15 16 19
0
5
10
15
20
25
30
Number of SIs reported
Comparison of SIs reported from April 2012
12 13
13 14
14 15
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 3 of 10 Date produced: 12th January 2015 Retention period: 30 years
consider how the Trust's community services responds when service users appear to be disengaging from treatment. A response to the Coroner is being completed.
2.3 Duty of Candour
In response to the implementations required following the Francis Inquiry regarding Duty of Candour NSFT has applied the process in 76 cases since it’s implementation in October 2014. The threshold applied has been based on reported levels of harm, and incidents recorded at moderate or above have led to the application of Duty of Candour. The implementation of Duty of Candour is still in it’s infancy, there remains a lack of guidance for Mental Health Services in relation to it’s thresholds and application.
2.4 Safety Thermometer (ST)
The national Safety Thermometer tool provides monthly point prevalence data on harm-free care in the later life wards which participate in data submission. As it is a point prevalence survey, it does not correlate with information reported on the incidence of harms. In December 2014, 94% of patients received harm-free care in relation to pressure ulcers, falls, catheter associated urinary tract infections and venous-thromboembolisms (VTEs). The results demonstrated that six patients had harms at the time of the survey, but no apparent trends were noted.
2.5 Infection prevention and control
There have been no reported outbreaks of Norovirus on any NSFT in-patient area; however there have been significant problems in local general acute Trusts. Information on any local outbreak is provided for the Modern Matrons to support risk assessments when admitting patients.
2.6 Flu vaccination programme 2014-2015
The final flu vaccination figures have been reported to the Department of Health. These show 35% uptake by clinical staff which is lower than last year. This is despite considerable effort from various flu crew members, continual coverage in the Trust Update and reminder emails out to all areas. A survey will be completed for learning from this year’s programme and reported back.
3.0 Service User and Carer Experience Indicators 3.1 Complaints
There were 55 complaints received in December 2014. This is an increase of 16 from the previous month.
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 4 of 10 Date produced: 12th January 2015 Retention period: 30 years
Chart 2: Number of Complaints received monthly from April 2013
In December 2014 there was no identified trend according to service and type. Overarching themes of complaints in this period referred to communication and points of discharge from services. These will be addressed through locality governance and further training on discharge processes.
3.2 Triangle of Care
The deadline for completed self-assessments for submission to the Carers Trust is end of May 2015. Eighty percent of completed self-assessments from our in-patient and CRHT/HT teams will need to be submitted in line with the Triangle of Care membership scheme terms and conditions, by the end of May 2015. As a Trust we are on schedule to meet this target at the end of May. NSFT has a further two years to ensure that all other areas (service lines) have completed the self-assessments. However, all teams across the Trust are being encouraged to start their self-assessments even though they may not be due for submission to the Carers Trust until 2017.
Monitoring of the self-assessments continues to take place in the Carers Leads Advisory Group (CLAG). Service lines are being encouraged to develop their own local monitoring groups whereby teams can monitor their own specific assessments. Those local groups will then elect a member of the team to represent their service line at the CLAG meeting. The set up of the local monitoring groups varies in each locality.
3.3 Friends and Family 3.3.1 Developments Post October 2014
The Friends and Family Test was implemented across the Norfolk and Suffolk NHS Foundation Trust on 1 October 2014. At the time of submitting this report, the FFT has been running for a total of 12 weeks. At this stage there have not been any specific themes or trends with regard to service delivery noted. Comments from the two supplementary questions remain positive for the majority of respondents, who
45
26
7166
4450
63
39
55
0
10
20
30
40
50
60
70
80
April May June July Aug Sept Oct Nov Dec Jan Feb Mar
No of complaints
Period
Chart to show Complaints received from April 2013
13-14
14-15
13-14ave
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 5 of 10 Date produced: 12th January 2015 Retention period: 30 years
described dedicated and supportive staff, people being treated with dignity and respect in a safe and caring environment (Appendix 1).
With regard to the number of respondents and the breakdown of percentages for people who would recommend the services of NSFT, the following are noted for the first three months of implementation (Table 2). Table 2: FFT Responses, October – December 2014
Number of responses
% recommending services
Number (%) of teams participating
October 2014 162 52.2 51 (49)
November 2014 44 56 18 (17)
December 2014 44 72.7 12 (11)
Overall participation for October, November and up until 20 December 2014; out of 105 teams, 51 teams (49%) have participated in the test (Appendix 2).
3.3.2 Improving the Response Rate
Although the test is available in all services across the Norfolk and Suffolk NHS Foundation Trust, the figures suggest a decline in the number of responses after the initial implementation in October 2014. A suggestion for this would be the timescales set for asking the question. If in-patient services were not discharging as many people during the month, this would have some bearing on the number of responses. Given the nature of services provided by NSFT, a service user may decline the opportunity to take part in the test, even though they had been willing to do so the in the previous months.
To improve the number of responses;
• Associate Directors of Operations for Norfolk and Suffolk are discussing results with individual teams.
• The Service User and Carer Experience Lead is visiting all Locality Governance meetings to promote the test and outline the reason for the FFT and look at any extra support that may be required for staff to enable them to support service users with the FFT.
• Friends and family Test cards are available in a timely manner, NSFT are developing a monthly ordering procedure which will ensure that services have sufficient supplies of the leaflets.
• Although service users are able to access the forms ‘on line’ only one person has used this facility. CQUIN Lead to liaise with Free Range people to discuss alternative options with regard to asking the question.
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 6 of 10 Date produced: 12th January 2015 Retention period: 30 years
4.0 Clinical Assurance 4.1 Care Quality Commission
Following the comprehensive inspection in October 2014 the Trust has now received the draft report for comment on accuracy and two MHA reports, one for Catton Ward at the Norvic Clinic and one for Lark ward at Woodlands. The accuracy response is due back to the CQC by the 16 January and the action plans for the MHA reports are due by the 15 January. The issues raised in the MHA reports are as follows: Lark Ward
• Lack of involvement of patients in care planning
• No evidence that seclusion was being managed
• No evidence that pts were informed of their rights to an IMHA
• Section 132 rights not being repeated in accordance with Code of Practice
• Section 17 leave forms not fully completed
• Door handles were not anti ligature
• Risks arising from visitors entering the ward without going through an air lock
• The presence of informal patients on a PICU unit not being informed of their rights to leave
• Inconsistent physical health monitoring
• Inconsistent practice under sec 58 that the statutory consultee had recorded their conversation with the second opinion appointed doctor
• No evidence that the RC had communicated the results of the SOAD assessment to the patient
• T2 and T3 forms, authorised treatment did not correlate with the prescription Catton Ward
• AMHP reports not available
• No record that patients were provided with a copy of their Sec17 leave authority
• Lack of involvement of patients in care planning
• Secluded patients not being examined by the duty doctor
• Incident forms for restraint did not identify the length of time for the prone/supine restraint
• Physical health care not being monitored or managed
• Hinges were not anti ligature
• Individual issues required patient B asking for access to physio and Patient C unhappy
All these issues are being responded to by services. Monitoring of actions in response to these points will be included in the CQC action plan.
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 7 of 10 Date produced: 12th January 2015 Retention period: 30 years
5.0 Safe Staffing 5.1 In line with the Government’s requirements as set out in Hard Truths, the Trust
continues to submit data via the National reporting system Unify 2. The figures reported for November 2014 are attached for the Board’s information (Appendix 3). Table 3 summarises the fill rates reported since the Trust began monitoring staffing levels in May 2014, and this is represented graphically in Chart 3. Table 3: Average Staffing Rates reported to Unify, May – November 2014
Average % fill rate RNs days
Average % fill rate CSWs days
Average % fill rate RNs nights
Average % fill rate CSWs days
May 96.80% 119.50% 89.90% 125.00%
June 102.70% 117.40% 88.80% 132.00%
July 99.80% 122.50% 92.50% 134.20%
August 98.60% 125.10% 90.50% 138.10%
September 99.10% 119.50% 88.80% 137.90%
October 98.80% 121.80% 86.80% 140.40%
November 99.9% 125% 90.2% 140.1%
Chart 3: Average Staffing Rates, May - November 2014
Average fill rates, by month, May to November 2014
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
120.0%
140.0%
160.0%
May June July August September October November
Month
Pe
rce
nta
ge
fil
l ra
te
Registered nurses,
by day
Care staff, by day
Registered nurses,
by night
Care staff, by night
5.2. Chart 4 below demonstrates the six month staffing rate across NSFT in-patient
areas during the six month reporting period and the average rates of Registered Nurses and Support Workers during this period. Information within these graphs indicates ongoing pressure regarding registered nurses fill rates in specific clinical
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 8 of 10 Date produced: 12th January 2015 Retention period: 30 years
areas and services and during key shift times such as night shifts. These shortfalls continue to be mitigated against with the use of support workers, and are monitored centrally and concerns raised with local managers.
Chart 4: Average Staffing Rates by Ward, May – November 2014
Average fill rates by ward for RNs, CSWs and all staff,
May to Nov 2014
0.0
20.0
40.0
60.0
80.0
100.0
120.0
140.0
160.0
180.0
200.0
So
uth
ga
te W
ard
5 A
ire
y C
lose
Wh
itli
ng
ha
m W
ard
Gla
ve
n W
ard
Ca
tto
n W
ard
Ya
re W
ard
Wa
ve
ne
y A
cu
te S
erv
ice
s
Ch
urc
hil
l W
ard
Fo
xg
lov
e W
ard
7 A
ire
y C
lose
Th
orp
e W
ard
Ab
be
yg
ate
Wa
rd
Wa
ve
ne
y W
ard
Sw
ee
tbri
ar
Wa
rd
Wa
lke
r C
lose
Dra
yto
n W
ard
6 A
ire
y C
lose
Fo
xh
all
Ho
use
Ea
ton
Wa
rd
No
rth
ga
te W
ard
Sa
nd
rin
gh
am
Wa
rd
Ac
le W
ard
Po
pp
y W
ard
Av
oc
et
Wa
rd
Fe
rnw
oo
d W
ard
Wil
low
s W
ard
Lark
Wa
rd
Ro
lle
sby
Wa
rd
Gre
at
Ya
rmo
uth
Ac
ute
Se
rvic
es
Bli
ck
lin
g W
ard
Ro
se W
ard
Re
ed
Wa
rd
Ward
Pe
rce
nta
ge
fil
l ra
te
Fill rate for RNs
Fill rate for CSWs
Fill rate for al l staff
5.3 The five wards reporting the lowest staffing rates of all staff groups during this
period of time as below (Table 4). Of note only the Southgate CSW fill rate falls below the 80% reporting level.
Table 4: Wards With Lowest Fill Rates Overall, May – November 2014
Name of Ward RN Fill Rate CSW Fill Rate Total fill rate
Southgate 103.9% 79.4% 91.6%
5 Airey Close 86.3% 99.9% 93.7%
Whitlingham Ward 91.1% 102% 97.6%
Glaven Ward 102.5% 97.2% 99.3%
Catton Ward 98.7% 101.6% 100.4%
The five wards reporting the highest staffing rates are reported below (Table 5).
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 9 of 10 Date produced: 12th January 2015 Retention period: 30 years
Table 5: Wards with Highest Fill Rates Overall, May – November 2014
Name of Ward RN Fill Rate CSW Fill Rate Total fill rate
Rollesby 113.3% 140.6% 130.8%
Northgate Ward 122.1% 139.3% 131.5%
Blickling Ward 91% 159.4% 135.3%
Rose Ward 83.6% 177.9% 141.6%
Reed Ward 78.5% 190.5% 147.4%
The five wards reporting the lowest and highest fill rates of Registered Nurses are as below (Table 6) with three out of the five wards below the required 80% reporting level. Foxhall House, Reed Ward, 6 Airey Close and Rose were also in the top 4 wards for lowest fill rates for CSWs, with only Foxhall being marginally below the required reporting rate at 79.4% overall fill rate. Rollesby, 7 Airey Close and Reed all reported significant overfill rates of CSWs, reporting 159%, 177% and 190% fill rates respectively.
Table 6: Five Wards with Highest and Lowest Rates of RN Staffing
Name of Ward RN’s Fill Rate Name of Ward RN’s Fill Rate
Foxhall House 63.2% Foxglove 110.3%
Acle Ward 78% Churchill Ward 111.1%
Reed Ward 78.5% Rollesby Ward 113.3%
6 Airey Close 82.2% 7 Airey Close 115.6%
Rose Ward 83.6% Rose Ward 122.1%
6.0 Quality Dashboard The newly formatted Quality dashboard attached represents the number of
incidents recorded across localities in relation to the number of occupied bed days and contacts. Narrative is contained alongside the data provided to provide assurance and rational related to incidents recorded (Appendix 4).
7.0 Risks / Mitigation in Relation to the Trust Objectives (Implications for Board Assurance Framework)
7.1 Quality and patient safety issues are fundamental to the delivery of Trust objectives, and the Board’s ability to manage the performance of the Trust. Relevant mitigating action is included above, and residual risks are noted.
Board of Directors, Public - 22nd
January 2015 Patient Safety and Quality
Version 1.0
Author: Jane Sayer Department: Director of Nursing
Page 10 of 10 Date produced: 12th January 2015 Retention period: 30 years
8.0 Recommendations
8.1 The Board of Directors is asked to note and approve the contents of this report.
Jane Sayer Director of Nursing and Quality 12th January 2015
Background Papers / Information Appendix 1 – FFT - Overall Report Appendix 2 – FFT Participation Report Appendix 3 – In-Patient Staffing Actual versus Budget Appendix 4 – Quality and Safety Dashboard, December 2014-15 version 1.0
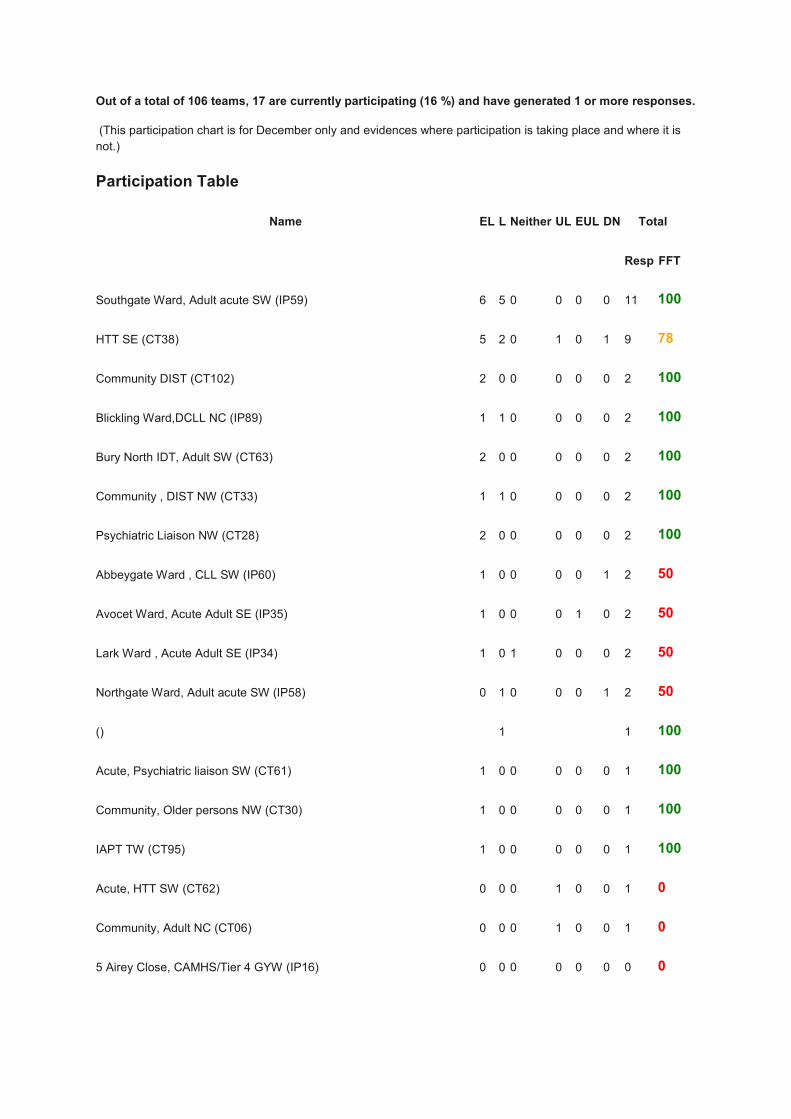
Out of a total of 106 teams, 17 are currently participating (16 %) and have generated 1 or more responses.
(This participation chart is for December only and evidences where participation is taking place and where it is
Promoter and detractor break-down for December 2014: 56.8% extremely likely to recommend 25% likely to recommend 2.3% neither likely nor unlikely to recommend 6.8% unlikely to recommend 2.3% extremely unlikely to recommend 6.8% Don’t know
Promoters (extremely likelies, likelies)
IP59
1
09/01/2015
The staff on Southgate were nothing but respectful and had time to listen no matter how busy they were.
Awesome team!!
Improvements: No
CT38
1
09/01/2015
The response and care of the home treatment team over Xmas period was absolutely brilliant.
Improvements: Nothing. Everything was excellent.
CT38
1
08/01/2015
Very kind and gave helpful advice. Came at time or rang to say would be delayed.
IP60
1
08/01/2015
Staff were helpful and considerate and sincere.
Improvements: Nothing.
IP59
2
07/01/2015
Good staff
IP34
1
06/01/2015
Staff very friendly and understanding. Dignity respected. Better smoking area, Poppy ward got smoking area too.
No females in Lark Ward. Rooms better. More time to relax and chill out.
Improvements: Nothing! I was extremely happy on Lark ward. Enjoyed my stay!
CT38
1
06/01/2015
The home treatment service came and gave me all the confidence I needed to be at home. Stayed with me for
quite a while, discussed all the things I was needing to cope with. Many thanks.
Improvements: No
CT38
1
05/01/2015
Very pleased with the service and care I received.
2
03/01/2015
Staff friendly, treatment explained. Smoking are in the garden also on Poppy ward peaceful no females as
patients.
Improvements: More input needed to the taking of medication as patient doesnt need mood stablisers like
Depacote, not appropriate for schizophrenic disorder. Staff treated patients on lark ward with disrespect and
sometimes staff condescending.
CT33
2
31/12/2014
The home treatment team helped me to get back on my feet after a month long spent with depression. Have
suffered from chronic depression on and off for many years. Being treated at home seems on the whole a better
alternative to being in hospital although I was sceptical at first.
Improvements: Better liaison between patient and team by phone. I never know who I was talking to on the
phone when ringing for advice. It would be good if patient knows where speaking to social worker, CPN or
support worker. I found it very confusing.
CT28
1
30/12/2014
Very understanding, extremely helpful.
Improvements: None that I can think of.
IP59
1
27/12/2014
Its helped me with a new train of thought and given me space to also sort my head out.
Improvements: Nothing
IP59
1
27/12/2014
I learnt new ways to deal with situations and cope better with things.
Improvements: Certain members of staff need to be less grumpy and that will make them more appropriate!
CT102
1
27/12/2014
Very, very good, excellent.
IP59
1
27/12/2014
They helped with my wellbeing.
Improvements: No
IP35
1
15/12/2014
The staff are awesome.
Improvements: The bed.
IP59
2
15/12/2014
We understand the difficulty with mental health as everyone's needs are different, but dealing with someone who
suffers from this can be very draining and could do with more support but the staff have been very nice.
Improvements: More space to go outside, more staff to cope. The staff have been very good but you can see
they are stressed and more time to discuss with family as its very hard dealing with someone with mental health
issues.
CT38
2
15/12/2014
Your were so kind and supportive.
Improvements: Better care plan and more regular visits with the same person/people.
CT38
1
15/12/2014
I was at my lowest ebb and your team got me on my feet and functioning again, much to the relief and pleasure
of my family. it has been a very worrying and frightening time. I do not want to be there again. With the support
and visits from the team I am sure that I will make it!
Improvements: I prefer one to one. Two ladies however nice they were I felt better with one concentrating on
me.
CT102
1
11/12/2014
During extremely stressful time the help and support given to both my mother and myself was excellent. The
team supported us throughout and in the weeks that followed and I know should the need arise I could contact
them. Thank you all.
Improvements: Nothing
CT38
2
11/12/2014
Brilliant alternative to hospital treatment. Most nurses make you feel very comfortable.
Improvements: Limit amount of different people visiting.
CT95
1
11/12/2014
NHS OK
CT30
1
11/12/2014
the people involved with the visit today were patient, informative, keen to listen to everything that I had to say.
Improvements: I was very satisfied so nothing extra was needed.
IP89
2
10/12/2014
Family photographer in room. Very likely to recommend. Food looks good, nice and clean.
Improvements: My own clothes every day.
CT28
1
10/12/2014
Tammy gave me first class care and so understanding and was warm to my feelings, made me feel better by her
talking to me.
Improvements: Could not have been better as it was brilliant by all the staff, thank you.
IP89
1
09/12/2014
Good care, smiling staff.
Improvements: Cup of tea.
IP58
2
08/12/2014
Good service
Improvements: Ok as it is.
CT63
1
04/12/2014
Valve the craft group on a Wednesday with Karen and Iona.
CT63
1
03/12/2014
Because it was educational and enjoyable. I had time off from my busy life caring for my disabled husband and I
met other people with mental health issues.
Improvements: I would like to see more people attending craft groups but I do not think that my visits could be
improved upon.
IP59
1
03/12/2014
Crazy people in Newmarket.
Improvements: Nothing
CT33
1
03/12/2014
Your staff are friendly, knowledgeable and very professional. They went to great lengths to help us and I am very
happy with their work with us, in particular Caroline Britton and Paul Collier have been very helpful.
Improvements: A cure for alzheimers disease.
CT61
1
02/12/2014
Although hospital was busy, wasnt too long until I was seen to. Reassured me, gave me words of advice and
sorted everything out to get me some help.
Improvements: Nothing.
Detractors (unlikelies, extremely unlikelies)
CT62
4
03/01/2015
Whilst those who came were positive in their response they seemed unconfident in their role and at times made
wildly optimistic statements that were not realistic. A sleep hygiene specialist did not make clear who she was
and what she was there for, making the experience distressing for me. A course of action was agreed with a
psychiatrist, which was to take place during the following week. It was subsequently found out that the person
concerned was on holiday so I was advised to discharge myself from this service and self refer to the Wellbeing
Service. Having done that, the Wellbeing Service phoned a week later and were more interested in filling in their
forms and my sexual orientation rather that what I was suffering from and what woulc be best to remedy it. A
week later the Wellbeing Service phoned me up to say that the: disagreed with the course of action suggested by
the psychiatrist above. Having stood my ground they capitulated and agreed to continue with what was
suggested by the psychiatrist.
Improvements: Being seen by confident and positive people who make realistically optimistic statements and
explain who they are, what they are doing there and what to expect. It is very important when someone is in the
state that I was in to have clear pathways to follow. Each minute is difficult to get through let alone each day. To
chop and change procedures and people is very distressing. In my view, the important thing is to remember that
the person in distress is a human being and any fixation on form filling, ethnicity or sexual orientation is not
relevant at this time.
IP35
5
31/12/2014
Did not get help I expected to be provided with. Being kicked out only being here a couple of days.
Improvements: Stay and get better.
CT38
4
24/12/2014
Care in hospital was lacking and in outside team. The whole service needs more money spent on staffing. And
more time is needed on patients. There is too larger a jump from 5/10 minutes care from home treatment to 24
hour admission to a ward.
Improvements: More 1:1 time in and out of hospital. Less violent patients who were not controlled quick enough
in hospital. It upset the entire ward and hinder chances of getting well.
CT06
4
03/12/2014
At this moment in time I feel I have been left dangling.
Improvements: Getting a visit?
Neutral/Passives
IP60
6
05/01/2015
Depends entirely on state of health of person concerned.
Improvements: Better initial indication of why I was coming into hospital.
IP58
6
29/12/2014
Improvements: Less unnecessary restrictions.
FFT Participation Report for All Dates
Out of a total of 105 teams, 51 are currently participating (49 %) and have generated 1 or more responses.
Quality and Safety Dashboard(graphic version)December 2014-2015 version 1.0
Data Collated and Published by: Informatics Source of Data: Datix Page 1 of 6
Report Published 08/01/2015Risk Management by Region December 2014
0
20
40
60
80
100
120
140
160
DSH Assault Restraint STF Abscon. Compl. Med. Pr. Ulcer SI ward SI comm.
Trust
0
10
20
30
40
50
60
70
DSH Assault Restraint STF Abscon. Compl. Med. Pr. Ulcer SI ward SI comm.
Norfolk
0
10
20
30
40
50
60
70
DSH Assault Restraint STF Abscon. Compl. Med. Pr. Ulcer SI ward SI comm.
GT Yarmouth & Waveney
0
10
20
30
40
50
60
70
DSH Assault Restraint STF Abscon. Compl. Med. Pr. Ulcer SI ward SI comm.
Suffolk
0
10
20
30
40
50
60
70
DSH Assault Restraint STF Abscon. Compl. Med. Pr. Ulcer SI ward SI comm.
Secure Services
Commentary: Whilst the Trust is a high reporter of incidents, levels of harm have been recorded lower than national levels through the National Reporting and Learning System. One area where the Trust is seen as recording high levels of activities is Restraint, the levels of recording relate to intervention in service user behaviour, from placing hands on and guiding away from an escalating event to full preventative managed aggression (PMA) by trained staff. The Risk Manager is working with the PMA lead to identify assurance that training records reflect the management of the risk in the environment. It is noted that more self harm events and restraint events are recorded in Suffolk. Physical assaults between service users, fluctuate between 40 to 70 events each month, however moderate harm is recorded in only 2 events in December. In all cases where it is considered that the assailant is likely to have capacity, statements are requested from the clinical team and outcomes are reviewed with the Police. Outcomes are higher with Norfolk Police than Suffolk Police currently, although a new service agreement is being signed within the Suffolk Police region, which will bring greater common practice across both counties.
Key: DSH - deliberate self harm STF - slips, trips & falls Abscon. - absconsions Compl. - complaints Med. - medication errors (administration and prescription) Pr. Ulcer - pressure ulcers SI ward - serious incidents (ward based patients) SI comm. - serious incidents (community & office)
Data Collated and Published by: Informatics Source of Data: Datix Page 2 of 6
Report Published 08/01/2015Physical Assault by Locality December 2014
GT Yarmouth and Waveney
Norfolk Central
Norfolk West NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
-5
0
5
10
15
20
25
30
35
Inci
den
ts
Physical assault by locality Balloon size is based on community contacts and occupied bed days
0
5
10
15
20
25
30
35
40
45
Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Dec 14
0
10
20
30
40
50
60
70
80
Loca
litie
s
Tru
st
Physical assault over 12 months by locality
Trust
GT Yarmouth and Waveney
Norfolk Central
Norfolk West
NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
Commentary: With the exception of West Norfolk, physical assaults have been recorded more frequently on Older Persons services, the Julian Hospital, where recording is consistent, are taking part in a risk trail, to review factors in relation to service user assaults. Most areas of harm occur on the Secure Services and Acute wards and all are reviewed to identify if clinical intervention was appropriately applied.
Data Collated and Published by: Informatics Source of Data: Datix Page 3 of 6
Report Published 08/01/2015Absconsions by Locality December 2014
GT Yarmouth and Waveney
Norfolk Central
Norfolk West NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
-1
0
1
2
3
Inci
den
ts
Absconsions by locality Balloon size is based on community contacts and occupied bed days
0
2
4
6
8
10
Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Dec 14
0
2
4
6
8
10
Loca
litie
s
Tru
st
Absconsions over 12 months by locality
Trust
GT Yarmouth and Waveney
Norfolk Central
Norfolk West
NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
Commentary: Absconsions have reduced in Acute services in Norfolk since the changes to environmental controls (fencing). Recent Health and Safety Executive (HSE) guidance re: ‘Lincolnshire Partnership NHS Foundation Trust has been fined for safety failings after a vulnerable mental health patient was left paralysed after diving off a roof.’ Has been shared with the Directors of Operations and Localities reminded to record their controls of stopping service users accessing roofs in their risk assessments.
Data Collated and Published by: Informatics Source of Data: Datix Page 4 of 6
Report Published 08/01/2015Medication Errors by Locality December 2014
GT Yarmouth and Waveney
Norfolk Central
Norfolk West
NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
-1
0
1
2
3
4
5
6
Inci
den
ts
Medication errors by locality Balloon size is based on community contacts and occupied bed days
0
2
4
6
8
10
12
14
16
18
20
Jan 14 Feb 14 Mar 14 Apr 14 May 14 Jun 14 Jul 14 Aug 14 Sep 14 Oct 14 Nov 14 Dec 14
0
5
10
15
20
25
30
35
Loca
litie
s
Tru
st
Medication errors over 12 months by locality
Trust
GT Yarmouth and Waveney
Norfolk Central
Norfolk West
NRP
Secure Services
Suffolk CountyWide
Suffolk East
Suffolk West
Commentary: The Risk Manager is to discuss with the Matron at West Norfolk as to why repeated medication concerns were being reported up to November 2014. There were some recording concerns highlighted in Suffolk East in May 2014 and Norfolk Central consistently report low levels, with no identified link in location or type of event (prescribing or administration etc). Trust levels reported are still lower than the national average and harm is much lower in the National Reporting and Learning System. The Medical Safety Officers (MSO) group (Risk Manager, Chief Pharmacist and Clinical Pharmacist) take part in online medication error conferences and will be working with other MSOs to ensure common reported errors are learnt from.
Data Collated and Published by: Informatics Source of Data: Datix Page 5 of 6
Report Published 08/01/2015Workforce by Region November 2014
3874.48
0%
20%
40%
60%
0
1000
2000
3000
4000
FTE Vacancies Turnover Absence Sick >= 21 d Appraisals Wellbeing
Pe
rfo
rman
ce
FTE
Trust Commentary:
0%
20%
40%
60%
0
500
1000
1500
FTE Vacancies Turnover Absence Sick >= 21 d Appraisals Wellbeing
GT Yarmouth & Waveney 1586.16
0%
20%
40%
60%
0
500
1000
1500
FTE Vacancies Turnover Absence Sick >= 21 d Appraisals Wellbeing
Norfolk
401.91
0%
20%
40%
60%
0
500
1000
1500
FTE Vacancies Turnover Absence Sick >= 21 d Appraisals Wellbeing
Secure Services
1022.15
0%
20%
40%
60%
0
500
1000
1500
FTE Vacancies Turnover Absence Sick >= 21 d Appraisals Wellbeing
Suffolk
Key: FTE - Full time equivalent Vacancies - as % of FTE Turnover - Leavers as % of FTE Absence - days as % of FTE x days (in last 12 months) Sick >= 21 d - spell over 21 days duration as % of episodes Appraisals - Staff appraised in last 12 months as % of FTE Wellbeing - Staff having a wellbeing discussion in last 12 months as % of FTE
Data Collated and Published by: Informatics Source of Data: Datix Page 6 of 6
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 1 of 9 Date produced: 13th January 2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 22nd January 2015
Title of Report: Quality Account update
Action Sought: For Information and approval
Estimated time: 10 minutes
Author: Sue Barrett: Head of Governance
Executive Dr Jane Sayer: Director of Nursing Quality and Patient Safety
Executive Summary:
This paper updates the Board of Directors (BoD) on the progress made towards achieving the Quality Account priorities 2014/15 approved by the Board in February 2014. The Board is asked to approve the recommendations in regard to priorities 2,4,5and 8
1.0 Summary
This paper provides an update on the quality priorities which will be reported in the annual Quality Account due for publication in June 2015.
2.0 Progress against Quality Account priorities – Quarter 3 2014/15
Priority 1: Patient Safety 2013-14 To implement a system which ensures that all patients in contact with mental health services access relevant physical healthcare screening and services. (2013-14) Board Lead: Jane Sayer, Sara Fletcher Q3 Update The Trust now has a physical health strategy group chaired by Dr Kapil Bakshi and this group aims to coordinate all of the physical health initiatives across the Trust.
Date: 22nd January 2015
F Item: 15.07ii
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 2 of 9 Date produced: 13th January 2015 Retention period: 30 years
This includes:
• Linking with the recovery college to produce a physical health module
• Links with public health leads to address physical health needs of community patients
• Physical Health monitoring in Clozapine Clinics and for depot injections
• Cardio-metabolic assessment for patients with schizophrenia as required from the National Audit of Schizophrenia.
• Supporting the use of the Rethink document. The East Norfolk pilot scheme that was originally proposed in response to the first round of the National Audit of Schizophrenia, has been subsumed into the physical health strategy group work. Specific work liaising with GP’s was undertaken as part of the public consultation.
Progress RAG rating GREEN
Priority 2: Patient Safety 2014-15 Being able to access services quickly Board lead: Operations Directors Q3 Update Following discussion with the informatics team, the following format is suggested to be included in the Quality Account. This format is designed to give a view of the waiting times which will be accessible for the public in the terms that are usually referred to.
Complete waits for treatment - 2014 - 2015 Q3
Secondary Care Services - seen within 18 weeks of referral
Month GT Yarmouth & Waveney Norfolk Suffolk Trust
Oct 99.45% 99.52% 98.66% 99.23%
Nov 99.51% 99.59% 99.84% 99.65%
Dec 99.74% 99.54% 98.92% 99.40%
Qtr 99.57% 99.55% 99.14% 99.42%
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 3 of 9 Date produced: 13th January 2015 Retention period: 30 years
Complete waits for treatment - 2014 - 2015 Q3
IAPT Services - seen within 28 days of referral
Month GT Yarmouth & Waveney Norfolk Suffolk Trust
Oct 90.16% 80.71% 99.50% 89.04%
Nov 75.28% 79.38% 99.41% 86.07%
Dec 72.84% 80.08% 99.39% 85.42%
Qtr 79.50% 80.06% 99.44% 87.03%
The board is asked to approve this format for use in the Quality Account.
Progress RAG rating Amber
Priority 3: Patient Safety 2014-15
Being confident that the Trust learns from mistakes and puts in plans to reduce similar risks
Board lead: Jane Sayer, Michael Lozano Q3 Update The duty of candour policy is now in place and reported on by the patient safety team. This action will be reported as complete in the Quality Account.
Progress RAG rating GREEN
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 4 of 9 Date produced: 13th January 2015 Retention period: 30 years
Priority 4: Patient Experience 2014-15 Being able to contact a mental health worker out of hours.
Board lead: Operations Directors Q3 Update Access to a support line in Norfolk Following negotiations with MIND and CCGs for funding to ensure that all Norfolk areas will be covered, the support line is due to commence on the 26th January.
The inclusion of emergency contact details in crisis plans for service users subject to CPA or contingency plans for those on non CPA
The Q3 audit covered the central locality and showed that:
• 18/40 (45%) had a crisis or contingency plan
• For CPA only 5/13 people had a crisis plan and of these only 3 plans contained contact details
• For non CPA only 13/27 people had a contingency plan and of these only 3 plans contained contact details
This is demonstrating that the Trust continues to struggle to ensure that service users have a crisis plan. With the implementation of Lorenzo it should be possible to provide more up to date timely information on the status of crisis plans but without a specific focus on this target, progress will not be made. The board is asked to consider the Trust response to this priority and the actions to be taken to improve performance.
Progress RAG rating AMBER
Priority 5: Patient Experience 2013-14
All inpatient areas will have a programme of activities which will be available over seven days and include evenings
Board lead: Operations directors
Q3 Update This priority was identified for 2013-14 and despite the Trust being in the top 20% for the provision of activities (in patient survey) it was reported by one service user group that there were insufficient activities. It was therefore agreed to continue monitoring this priority but without a clear goal we cannot measure
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 5 of 9 Date produced: 13th January 2015 Retention period: 30 years
progress or declare completion. Following a meeting with the allied health professions (AHP) lead, it is clear there is no national guidance on how much activity is required. All in patient areas have an activity programme consisting of both structured and unstructured activity. Daily meetings enable service users to discuss activities for the day and for the staff to tailor the programme accordingly. It is noted that the expected level of activity is subjective and dependent on the individual. It has therefore been identified that an individual monitoring form will be introduced for all in patients (appendix 1). This will demonstrate the activity that is available and taken up by the service user and may also be used in reviews to identify changes in mental state. The Board is asked to approve the implementation of this form as the measure for this priority, enabling the Trust to move towards achievement.
Progress RAG rating AMBER
Priority 6: Patient Experience 2014-15 Having carers needs taken into consideration. Board Lead: Jane Sayer Q3 Update This is reported in the Director Nursing update. A full summary of achievement will be presented in the Q4 update
Progress RAG rating GREEN
Priority 7: Clinical Effectiveness 2013-14 When a new medication is prescribed, the prescriber should always discuss this with the service user first. Information leaflets should be given and this should be recorded in the service user’s record. Board lead: Medical Director Q3 Update Dr Solomka has been asked to take over this priority and discuss with prescribers. An audit is currently underway and will be reported in the end of year report.
Progress RAG rating AMBER
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 6 of 9 Date produced: 13th January 2015 Retention period: 30 years
Priority 8: Clinical Effectiveness 2014-15 Having a care coordinator who gets to know you and can ensure continuity of your care. Board Lead: Operations Directors Q3 Update As reported in the October report, there is no obvious metric with which to report achievement of this priority. Following discussion with Informatics, the regular reports regarding unallocated cases are received and the current figures for Norfolk are as follows:
Unallocated cases December 2014
Locality Number of cases
Central adult 283
Central youth 96
Coast adult 79
Coast DCLL 33
Coast memory team 29
West 163
The Board is asked to approve this information as the metric for reporting progress. The Board is asked to discuss how this priority can be measured in Suffolk.
Progress RAG rating RED
3.0 Quality implications
3.1 As the stated quality priorities for the Trust, there is a clear link with quality if the individual priorities are not achieved.
3.2 Due to the roll over of quality priorities from 2013-14, there is an imperative that progress is made in 2014-15. A failure to do so will reflect negatively on the reputation of the Trust.
4.0 Risks / mitigation in relation to the Trust objectives
4.1 As noted above, a failure to deliver the quality priorities will have a negative impact on the reputation of the Trust and the Trust aim to “improve our focus on quality”
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 7 of 9 Date produced: 13th January 2015 Retention period: 30 years
Commissioners in response to the Quality Account published in June 2014, commented on the Trust failure to deliver some of the quality priorities and the governors have also recently raised concern about a lack of progress.
The risk can be mitigated through a determined focus on the objectives in the final months of the financial year, particularly with regard to priorities 2,4,7 and 8.
5.0 Recommendations
5.1 The board is asked to approve the recommendations in relation to priorities 2,4,5 and 8. If the recommendations are not approved, this will probably lead to a failure to achieve the stated priorities and lead to a lack of quality improvement and therefore a failure to meet the stated Trust aim. It will also lead to a loss of reputation as the priorities are reported publicly.
Sue Barrett Head of Governance
Background Papers / Information Give details of any background papers / information Appendix 1
Board of Directors – Public January 2015
Version 1.0
Author: Sue Barrett Department: Governance
Page 8 of 9 Date produced: 13th January 2015 Retention period: 30 years
Reasons for non-attendance:
A = Asleep
C = Community Leave
M = In a m
eeting
PI = Physical Illness
SC = Session Clash
SL = Staffing levels
DMH = Deterioration in Mental Health
S = Seclusion
O= Other – Please Specify
Patient Initials:
Ward:
Date:
Session Offered:
Attended
Y or N
Reason if did not
attend: (see Key)
Staff Initials
Offered Session
Duration
Actual Session
Duration
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 1 of 6 Date produced: 13.01.15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Equality delivery system objectives update
Action Sought: For Information
Estimated time: 10 minutes
Author: Ravi Seenan: Equalities and Engagement Manager
Executive: Robert Nesbitt: Trust Secretary
Executive Summary:
This paper updates the Board of Directors (BoD) on progress in achieving the equality delivery system (EDS) objectives 2014/2015 that were approved by the Board in April 2014. The EDS objectives help us to fulfil our responsibilities under the Equality Act (2010). Good progress has been made in developing the equality leads arrangements and community engagement in Suffolk. Understanding of the rationale for equalities focussed practice remains mixed across the Trust, evidenced by the clinical audit on spiritual needs assessment and care planning. The pressure on staff time means that training on equality and diversity issues is not prioritised at this time.
1.0 Introduction
1.1 At its meeting in October 2014 the Board asked that the EDS report be presented separately rather than part of the quarterly quality report. This report format is based on the four equality goals within the EDS. Two of these relate to services (service access and experience) and two to staff (staff development / support and leadership). The Trust has identified 5 objectives that relate to these goals.
1.2 The Trust has a three-fold public equality statutory duty to eliminate unlawful discrimination, advance equality of opportunity and foster good relations between people who share a protected characteristic and those who do not share it.
1.2 Areas where we have made significant improvement are as follows:
Date: 22nd January 2015
G Item: 15.07iii
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 2 of 6 Date produced: 13.01.15 Retention period: 30 years
• Staff involvement with the equality lead network.
• Engagement with BME communities and key stake holders.
• NSFT published a report of the findings and recommendations from the ‘Open Mind Workshop’
• A diversity team is now established by bringing together the Spiritual and Pastoral Care leads in Suffolk and Norfolk, the Engagement and Membership Officer and the Equalities and Engagement Manager.
2.0 Progress against Equality delivery system objectives- Quarter 3- 2014/15
Objective 1: Improving our equality monitoring data
“To improve equality monitoring information so that we can improve individual care and plan for service improvements.”
Rationale: In the absence of monitoring information we cannot know what is happening in the Trust and rely on anecdotal accounts. Unless practitioners are able to explain how monitoring information improves personalised care, service users may not feel comfortable about sharing information about their relationships, beliefs and cultural preferences. The same principle applies to staff information as it relates to recruitment and promotion.
UPDATE
1. Following the launch of the ‘Why ask monitoring questions?’ booklet for staff and leaflet for service users, equality leads are preparing to deliver small training/workshop session to their colleagues in team meetings using these materials. Equality leads received presentation skills training as part of their equality leads programme on 16.01.15 to enable them to complete this task in the next quarter.
2. We now have over 60 equality leads covering the following localities and areas and these are:
• East Suffolk: 15
• West Suffolk: 6
• Norfolk West: 9
• Great Yarmouth and Waveney: 5
• Norfolk Central: 8
• Secure services (Norfolk and Suffolk): 12
• HR & Workforce: 3
• IT/Lorenzo:1
• Trust management/coporate:8
• SUF: 1
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 3 of 6 Date produced: 13.01.15 Retention period: 30 years
Ravi Seenan has been working closely with a training provider in delivering a comprehensive training programme for the equality leads and the training included the following topics.
1. Equality legislations and tackling discrimination 2. Equality assessment, monitoring and action learning sets 3. Presentation and training skills
The training has been very well received and all leads that were able to attend have found the network to be very supportive and useful. Many equality leads have been unable to attend the lessons consistently because their managers have been unable to free them from other work commitments. The modest amount of funding that was available to set the programme up has now come to an end and Ravi Seenan will also explore other methods to deliver some of training via video conferencing. The development of the equality leads network is encouraging with the caveats that there is still somewhat patchy coverage, that they are often unable to attend, and that even where the training delivery does take place it cannot substitute for broader experiential equalities training. 3. The network meets monthly and going forward will focus on the objectives agreed at the Performance Review Group (PRG) meeting in July 2014 (focussed on using equalities information to improve services). The network will continue as a forum to share information and learn from each other with opportunities where possible to invite external speakers and trainers to attend the meeting.
Objective 2: Monitoring experience
“To use feedback from service users who share protected characteristics to understand their experiences better so as to be able to improve accessibility and quality of services.”
Rationale: We do not know how people from protected characteristics groups experience our services and whether there are barriers to access.
UPDATE
1. Community Engagement. Ravi Seenan has now published the report on the
findings of the October 2014 BME workshop entitled “Open Mind” and this is now being distributed to all stake holders including voluntary and statutory organisations. Copies are available by emailing [email protected]. Ravi Seenan is also engaging with the CCG’s and make sure they are aware of the
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 4 of 6 Date produced: 13.01.15 Retention period: 30 years
findings of the report and recommendations within.
2. Work between NSFT and Healthwatch Suffolk on the survey of BME people who do not use mental health services is progressing well and regular meetings are scheduled to take place between now and April 2015. We are now at a stage where the details of questionnaire are being finalised and a BME service user forum is being established to work alongside us in developing this piece of work.
3. Service experience. Sharon Picken (Service user and carer experience lead) has liaised with the organisation (Free-range) who designed the family and friend online survey and as a result demographics questions have now been included. Unfortunately, this remains problematic as the monitoring questions are not linked to the feedback and therefore it is not possible to analyse the feedback by protected characteristic. Ravi Seenan will now liaise with the company to see how flexible the system is and whether it can be slightly modified to adapt to our needs. This highlights a wider issue which is that usually, when surveys are carried out in the Trust, no monitoring information is collected. This implies that managers often do not understand the Public Sector Equality Duty and means that the Trust is unable to demonstrate compliance with the Equality Act. More importantly it means that the time spent gathering information gathered through such surveys is ineffective since it is does not produce useful insights into services. Ravi Seenan has written a piece for staff update highlighting this issue.
4. At present there is no way of analysing complaints information, or staff training data, by protected characteristic and consideration is being given as to how to do so.
5. A clinical audit on how well assessment and care planning addresses the spiritual needs of service users took place in 2014. This was part of the 3 year spirituality strategy launched in February 2013. The findings show very poor compliance in asking about the spiritual needs of service users. If the results of the audit are generalizable they indicates that service users are not normally asked whether they have any spiritual life which might feed into their recovery plan and this may also reflect a lack of awareness of the need to consider cultural, spiritual and personal recovery goals within services. A plan to try to address these issues is under development, although the key issue of staff awareness may be a training issue.
6. The NHS BME Network is now analysing the figures that informatics have provided about the demographics of the population who access our services. Once they have completed the analysis they will propose a way forward to implementing the values based commissioning tool and that means for NSFT staff to develop ways of empowering and working alongside bme service users in improving services.
7. The NHS BME network has also offered NSFT the opportunity to take part in their annual conference later this year to share the initiaitives that the Trust is taking forward.
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 5 of 6 Date produced: 13.01.15 Retention period: 30 years
Objective 3: Optimising training
“To optimise the delivery equality and diversity training so that it supports the Trust’s objectives”. Rationale: Research shows that using a blended approach to training is a more effective way of delivering equality and diversity training. This includes using face to face sessions, e-learning training as well as embedding equality aspects across all other training. By using such an approach, we are more likely to have a stronger impact on quality
UPDATE
1. E&D e-learning training although mandatory, is only required as a one-off requirement for staff to show as ‘green’ on LARA with no updates and no face to face training. The OD&WF committee reviewed whether this could be changed but due to the competing priorities for staff time this is not possible at this time. This remains a weakness in the Trust’s approach to equality and diversity. 2. Ravi Seenan is working with a training provider to train equality leads with basic training and presentation skills to be able to carry out ‘bite size’ training in their teams. Whilst this is positive, it is important not to view this work as a substitute for experiential training (see caveats in Objective 1).
Objective 4: Supporting staff
“To strengthen the Trust’s approach and policies in tackling bullying, harassment and discrimination in order to improve the experiences of staff in the Trust”.
UPDATE
1. Work is still in progress between Ravi Seenan and Risk Department to look at
confidential and anonymous reporting of discrimination incident through datix.
2. HR plan to review the discrimination by service user policy.
3. The Equality Leads Network has had very good feedback in so far that staff who have joined the network have found this very useful and beneficial to them and their team. The network which is led by the Equalities and Engagement manager will be working closely together in the aim to also organise a conference in November 2015.
4. The board will receive a staff presentation by representatives of the BME Employee Network Group at the start of the private session today highlighting common experiences of what it is like to work in the Trust as black member of staff.
BoD - Public 22Jan 2015 EDS update
Version 1.0
Author: Ravi Seenan Department: Corporate
Page 6 of 6 Date produced: 13.01.15 Retention period: 30 years
Objective 5 Objective 5 Leadership
“For board members and senior leaders to regularly demonstrate their continuing support and commitment to promoting equality in their day to day business”. Rationale: Board members play an important leadership role in highlighting organisational priorities through the focus of their enquiries and discussions.
Update
The board is keen to continue to demonstrate their commitment by supporting key equality initiatives such:
1. Gary Page continues to support both the BME network and the Equality lead network.
2. We now have two more senior manager members (Dawn Collins and Alison Armstrong) and one non-executive director member (Marion Saunders) who have joined the equality lead network.
3. The Board remains committed in addressing BME and mental health issues by supporting by working closely with Healthwatch and NHS BME Network.
4. All board report includes a section of equality implications which means that all responsible in reporting to the board have to consider how equality is addressed in their practice.
3.0 Equality implications / summary of consultation
This report is solely focussed on the topic of equality and diversity.
4.0 Risks / mitigation in relation to the Trust objectives
The risk is that equality work is perceived as separate to the wider quality agenda which impacts on the Trust’s compliance with the public sector equality duties and on service quality. The challenge for the organisation is how to efficiently manage a wide range of competing priorities for staff time and resources in a way that maximises quality of care. This is mitigated by the work undertaken as part of the EDS objectives.
5.0 Recommendations
5.1 Directors are asked to note the progress made against the equality objectives 2014/2015 and to continue to support these initiatives.
Ravi Seenan Equalities and Engagement Manager
Background Papers / Information – None
Board of Directors – Public 22Jan2014 Board Assurance Framework
Version 1.0 Author: Robert Nesbitt Department: Corporate
Page 1 of 2 Date produced: 09Jan2014 Retention period: 30 years
Report To: Board of Directors – public
Meeting Date: 22nd January 2015
Title of Report: Board Assurance Framework
Action Sought: For Approval
Estimated time: 10 minutes
Author: Robert Nesbitt: Trust Secretary
Executive: Robert Nesbitt: Trust Secretary
Executive Summary:
The outcomes of the 18th December 2014 board discussion have been incorporated into the January 2015 report (see appendix 1) and themes cross referenced with the risk register. At the December 2014 meeting the Board considered that all the main risks to the Trust’s objectives had been captured in the BAF and noted that almost all of the board agenda was focussed on actions to reduce these risks to acceptable levels, however, it was also suggested that the presentation could be improved. Following discussion with John Brierley, a trial version of a new format will be presented at the February 2015 board using a ‘butterfly’ diagram. NB: The mitigation RAAG rating is based on Monitor’s Governance Risk Rating system which is set out below. This 4 point scale is used as a guide only for the use of the Board. A Red ‘likely risk of breach’ is the highest level of unmitigated risk but needs to be understood in the context of the additional actions set out in the BAF and elsewhere in board papers. It does not mean that a breach is necessarily imminent but flags the most serious issues. ‘Red’ (the mitigation is so weak that there is likely risk of a breach to the provider license), ‘Red / Amber’ (the mitigation is such that there are material concerns of a breach to the provider license), ‘Amber Green’ (the mitigation leaves limited concerns of a breach). ‘Green’ (the mitigation is so strong as to mean that there are no material concerns of a breach). Scores shown are ‘Consequence x Likelihood’ as recorded on Datix. The executive owner is not always the risk owner on Datix (this is intentional).
Date: 22nd January 2015
H Item: 15.07iv
Board of Directors – Public 22Jan2014 Board Assurance Framework
Version 1.0 Author: Robert Nesbitt Department: Corporate
Page 2 of 2 Date produced: 09Jan2014 Retention period: 30 years
1.0 Conclusion
1.1 Board members are to review the BAF themes and consider whether any additional actions are required to provide assurance on management of the risks.
1.2 The Board is also asked to consider whether there are additional significant risks that have come to light but which are not represented in the BAF at present.
Robert Nesbitt Trust Secretary
Appendix 1 – Board Assurance Framework
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 1 of 10 Date produced: 02Jan2015 Retention period: 30 years
1. Name of risk theme (board committee with oversight)
Staffing (OD and WF Committee)
1.1 Relevant Trust objectives:
Implementation of Hard Truths recommendations so agreed inpatient staffing levels are achieved, maintained and published weekly from June 2014.
To agree recording and monitoring process for safe caseloads levels by October 2014.
Delivery of a Workforce and OD strategy.
1.2 What is the nature of the risk? The risk is that shortage of staff capacity impacts on safety. The key drivers for this risk include mistakes that were made in the modelling for community team establishments as part of the N&W Trust Service Strategy with underestimates of care coordinator numbers and loss of experienced staff who were able to safely manage risk. Teams which have been fragmented or reconstituted can experience a shift in risk tolerance which moves service pressure into Crisis Teams and OOAs. In inpatient areas risks can arise through a shortage of qualified staff on shifts, staff without the right skills (such as Prevention and Management of Aggression (PMA) training) or staff who have not yet built up experience in supporting people with complex needs.
1.3 How is the risk controlled and mitigated? In community services, the risk is mitigated by the FACT model being introduced across all teams, additional support worker resource being provided by MIND to enhance community capacity, admission prevention service being provided by Julian Support/West Norfolk MIND and a Robust duty worker system in place in all community teams. There is a plan to introduce the “Waves” model for service users with a diagnosis of Personality Disorder in Norfolk and Waveney. A bespoke crisis support telephone line for service users is about to be introduced (operated by MIND). Recording and monitoring safe caseloads: Implementation of a caseload weighting tool was due for completion 31/12/14. A review of the access and assessment function is underway with a plan to deploy those staff into community teams. As an immediate mitigation in inpatient areas, where qualified staff are not available shifts are strengthened with unqualified but experienced support workers. See the Safe Staffing report on the Board agenda this month. Managers allocate staff and move people to other areas so as to prioritise risk. The overspend on temporary staffing may indicate that patient safety is prioritised. Staff are encouraged to report staffing shortages using Datix, and they do so, which means that action can be taken by managers to mitigate risks. Risk owner for these aspects are Debbie White Director of Operations N&W and Alison Armstrong as Director of Operations Suffolk. In the longer term, the Flexible Working Strategy includes specific measures to improve staffing levels. Some
Confidence level in mitigation:
Red/Amber
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 2 of 10 Date produced: 02Jan2015 Retention period: 30 years
progress has been made in filling vacancies although retention remains a challenge. See also Staff Engagement report on the agenda this month. The risk owner for this aspect is Leigh Howlett
1.4 What additional actions are required? None in addition to those set out above.
1.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix 1116 (vacancy impact on services) = 4x3=12 Leigh Howlett Datix 1141 Inability to deliver corporate services safely due to high level of vacancies 3 x 3 = 9 Leigh Howlett Datix 1133 (difficulty recruiting in West Suffolk). 3x4 =12. Alison Armstrong. Datix 1155 (accessing PMA staff via NHSP) 4x5=20 Alison Armstrong. Datix 1123 (high caseloads W, Norfolk adult) was 3 x 4 = 12 (reduced to 3 x 3 from 16.12.14 but under review). Datix 1065 (high caseloads W, Norfolk OPMH) 3 x 4 = 12 Owner Debbie White. Datix 1033 3 x 5 = 15 (unallocated cases in Central Norfolk) Owner Debbie White.
1.6 What is the timeline for the mitigation confidence level to reach ‘green’? To address the N&W community capacity shortages contract negotiations with CCGs have flagged the need for additional funding for care coordinators. This will feed into the 2015/16 contracts. Delivery of the Workforce and OD strategy is part of the two year operational plan and five year strategic plan. The business care for e-rostering bas been approved and will be rolled out by year end with a full implementation date of March 2016. However, it is recognised that whilst e-rostering is a foundation for pre effective use of staff, the behavioural aspects that will deliver changes in practice will need to be promoted by managers and clinicians in order to deliver improvements.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 3 of 10 Date produced: 02Jan2015 Retention period: 30 years
2. Name of risk theme (board committees with oversight)
System confidence (Finance and Performance Committee / Comms Committee)
2.1 Relevant Trust objectives:
For the 2014/15 financial year: delivery of all operational targets including receiving 100% CQUIN and the avoidance of any operational and financial penalties from commissioners in the final quarter of the year.
Engage with the wider health economy, third and voluntary sector to ensure the Trust is a known and trusted partner evidenced by a 10% increase in new business with external parties by March 2015, evidenced by financial turnover.
We will look for, and exploit, opportunities to work on prevention and anti-stigma by development and delivery of a robust communication plan, evidenced by monthly positive media messages from launch in September 2014.
2.2 What is the nature of the risk? The Monitor investigation has raised the risk of a loss of system confidence in the management of the Trust. If regulatory action follows it could impact on the ability of the Trust to retain and win contracts, and would impact on management capacity. It could also weaken the public’s confidence in the quality of the service which might inhibit people from seeking help who need our support. A critical CQC report based on the inspection visit in October 2014 could weaken patient (and wider) confidence in the Trust. In addition, the loss of some CQUIN income in Q1 and Q2 means that receiving 100% of CQUIN income as set out in the Trust objective above is not achievable which risks undermining confidence in the Trust’s ability to deliver.
2.3 How is the risk controlled and mitigated?
1. Constructive response to the Monitor investigation to assist the Trust’s recovery plans 2. Prioritisation of meeting performance standards and addressing problems quickly. The Business Performance
Report indicates improvements across several areas, but note the cross-reference with financial performance which continues to fall short (see 7. Finance)
3. Positive attempts to reach out to the Campaign so as to find common ground in our joint desire to protect and improve services.
4. The draft CQC report was received for comment on 19.12.14 and the Trust will use its best endeavours to try to ensure that the report is an accurate representation of Trust services.
5. There has been recognition in local media of the excellent work of our staff through the work of the communications team.
6. Endeavours to improve CQUIN performance for Q3 – 4 so as to maximise income and system confidence in ability of Trust to deliver. This is supported by moving CQUIN to the Trust’s contracting function and a dedicated resource to support delivery.
7. There are plans in place to increase new business (such as peri-natal mental health and eating disorders) although this does not yet amount to 10% (by turnover).
Confidence level in mitigation:
Red
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 4 of 10 Date produced: 02Jan2015 Retention period: 30 years
2.4 What additional actions are required? None in addition to those set out above.
2.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix ID 1112(Risk of damage to Trust reputation) 4 x 3 = 12 Owner Michael Scott. Datix ID 1144 (Risk of poor CQC report affecting confidence in Trust) 4 x 3 = 12 Owner Jane Sayer.
2.6 What is the timeline for the mitigation confidence level to reach ‘green’? System confidence is closely linked to the other risk themes on the BAF, and so the finance recovery plan which runs over 18 months sets the outer milestone. However, this could be impacted by the CQC inspection report, the first draft of which is expected on 18.12.14 to for accuracy checking and with the report being published in March 2015.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 5 of 10 Date produced: 02Jan2015 Retention period: 30 years
3. Name of risk theme (board committees with oversight)
Quality (Service Governance Committee / Finance and Performance Committee)
3.1 Relevant Trust objectives:
Achieve zero out of area non specialist bed placements by March 2015.
Achieve a positive CQC review in 2014 and effectively addressing any issues that arise as part of this.
3.2 What is the nature of the risk? Risks to quality are made up of several factors including operational performance and clinical and corporate governance. Service pressures may lead to safety risks to patients and, as a result, to very high stress staff levels. Service user and carer experience may be compromised by service delays and mistakes. Caseload pressures partly as a result of the S.75 changes in N&W and partly because of problems with the TSS modelling assumptions have quality implications across the care pathway including bed pressures. SGC has also flagged that slippage on the work on Restrictive Interventions and weak assurance from an IA report on clinical supervision give rise to quality risks. Weaknesses in the board in having a clear line of sight to services may compromise the ability of the board to provide leadership and to prioritise effectively.
3.3 How is the risk controlled and mitigated? 1. Out of area acute capacity placements in N&W remain high (c.30) but have reduced from their high 40s level earlier in the autumn of 2014. Planning is underway to open 10 additional beds in February 2015. 2. Whilst caseloads in many N&W community teams are unsustainably high there is mitigation in that the whole care pathway is being reviewed to balance resources and improve community services capacity. This cross-references to staff recruitment and retention. 3. There is a risk that learning from incidents is not adequately shared so that lessons are not learned. Mitigation: The DoN and MD scrutinise every report, identifying themes and reporting these to the Senior Mgt Forum. Clinical audit reviews how well embedded lessons are. The Service Governance Ctte continues to flag this as a concern. See SGC report. The Board received an update report on Restrictive Interventions in November 2014. 4. There is a S.75 transitional plan to assist in the managing the caseload pressures. See also 1. Staffing. 5. A working group on clinical supervision will report to SGC in January 2015 6. The external board evaluation identified some weaknesses in the board’s leadership on quality. Mitigation: There is a timed action plan that is implementing the evaluation recommendations.
Confidence level in mitigation:
Red/Amber
3.4 What additional actions are required? None in addition to those set out above.
3.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix 914 (mandatory training) 4 x 4 = 16. Owner Jane Sayer Datix 1062 (bed management) 4 x 3= 12 Owner Debbie White. (this has reduced from 4 x 4 = 16 in Dec 2014 but remains under review) Datix 1145 (risk of not learning from RCAs) 3 x 3 = 9. Owner Jane Sayer. (This has reduced from 4 x 3 = 12, and is being reviewed to increase it).
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 6 of 10 Date produced: 02Jan2015 Retention period: 30 years
Datix 1163 (well-led) 5 x 4 = 20 Owner Gary Page. Datix 1123 (High demand for community services in West Norfolk) 3 x 4 = 12 Owner Debbie White Datix 1160 (Impact of S.75 changes on caseloads on quality) 4 x 4 = 16 Owner Debbie White Datix 1169 (Restrictive interventions practice implementation) 5 x 3 = 15 Owner Jane Sayer
3.6 What is the timeline for the mitigation confidence level to reach ‘green’? This risk area is made up of several inter-connected elements. The CQC and board evaluation action plans provide a substantial part of this detail. Whilst immediate improvements can be made in some areas, it is likely that the rebalancing of the care pathway to substantially reduce OOA placements will take several months, particularly where additional care coordinators are required in Norfolk as this may be contingent on negotiations with commissioners.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 7 of 10 Date produced: 02Jan2015 Retention period: 30 years
4. Name of risk theme (board committees with oversight)
Staff morale (OD & WF Committee)
4.1 Relevant Trust objectives:
Delivery of WF & OD strategy
Vacancies recruited to point of offer within 8 weeks by March 2015
Plans to delivery 7 days services by end of financial year.
Roll out of e-rostering by March 2016
4.2 What is the nature of the risk? Low morale impacts on quality of care and staff well-being. It can impact on staff sickness which increases stress for other staff. Low morale can make it more difficult to attract and retain high calibre staff. For operational staff, this cross-references to the service pressures set out in 3 above, and for corporate and support staff, low morale may impact on the support to front line services.
4.3 How is the risk controlled and mitigated? 1. The Trust is rolling out a staff engagement plan, developed in partnership with Staff Side, as part of the OD strategy and with an emphasis on local ownership. 2.Executive team members have set up engagement sessions to hear staff concerns and to answer questions about the rationale for the changes. 3.The staff appraisal system changes will help staff to see where their role contributes to the Trust’s work in supporting service users and will enable better feedback to staff on their performance. 4.The staff FFT includes 3 staff engagement measures which provides a tool to monitor progress. This reports to OD&WFC.
Confidence level in mitigation:
Red
4.4 What additional actions are required? None in addition to those set out above.
4.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix ID 1164 (Staff Morale) 4 x 5 = 20 Owner Leigh Howlett
4.6 What is the timeline for the mitigation confidence level to reach ‘green’? The Friends and Family Test is quarterly. However, the executive team recognise that the challenges in this area are medium to long term issues and so the expectation is that it will take 12 – 18 months for changes now being implemented to feed through into some measurable improvement. Following the trial of a new central lean recruitment process for three months this is now being rolled out and delivery of the recruitment KPIs is anticipated by March 2016. Enhanced management of sickness absence will be introduced over the next quarter and the results should be seen by March 2016. The position on appraisals had not improved and the backlog appeared to be growing. The target for a stable turnover rate of 10% is March 2016.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 8 of 10 Date produced: 02Jan2015 Retention period: 30 years
5. Name of risk theme (board committees with oversight)
Maintaining and growing business (Investment Committee)
5.1 Relevant Trust objectives:
By October 2014, delivery of a Commercial Strategy to protect current services and develop new business.
Engage with the wider health economy, third and voluntary sector to ensure the Trust is a known and trusted partner evidenced by a 10% increase in new business with external parties by March 2015, evidenced by financial turnover.
5.2 What is the nature of the risk? Growth increases the ability of the Trust to bear fixed costs / overheads. Loss of income will destabilise the organisation. Loss of key contracts where we are the incumbent could also damage our reputation since they could be interpreted as a loss of commissioner confidence. The development of the Commercial Strategy has been delayed. Developing bids and winning contracts requires an increasingly specialised skill set where demand is variable and where competitors are continually raising the bar. Successful bids require evidence of a track record of delivery which has been variable in recent months. For an organisation of our size it is a challenge to be able to maintain a strong bid capability with the right skills on tap that is also cost-effective during quieter periods. A bid development team need access to specialist service knowledge in the context of clinical managers who are already short of capacity. Formal regulatory action could affect the Trust’s ability to get past PQQ stage for a bid.
5.3 How is the risk controlled and mitigated? 1. Resources to support improved bidding capability have been set aside for 2014/15. In the interim project support and plans are in place for reviewing and securing current / new business.
Confidence level in mitigation:
Red / Amber
5.4 What additional actions are required? The implementation of the corporate restructure so as to provide a stable platform for the Commercial Strategy.
5.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? This is not represented on the risk register given that there is no specific risk at this time related to a bid.
5.6 What is the timeline for the mitigation confidence level to reach ‘green’? The corporate restructure is being designed in September / October and consultation began at the end of November 2014. The project plans for reviewing and securing new business as set out in 5.3 have their own timeframes.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 9 of 10 Date produced: 02Jan2015 Retention period: 30 years
6. Name of risk theme (board committees with oversight)
Maintaining a CoSRR of 3 in 2014/15 (Finance and Performance Committee)
6.1 Relevant Trust objectives:
Delivery of the 2014/15 financial plan so the Trust achieves a COSRR of 3 as a foundation for 2015/16
Delivery of the 2014/15 CIP and capital programmes
Develop a new strategy for procurement by end of 2014/15 financial year
For the 2014/15 financial year: delivery of all operational targets including receiving 100% CQUIN and the avoidance of any operational and financial penalties from commissioners in the final quarter of the year.
6.2 What is the nature of the risk? Following the Board’s Monitor Declaration in October 2014 that the Trust would be unable to maintain at CoSRR of 3, and the analysis which shows that delivery of CIPS is significantly behind plan, the risk is that our ability to provide a stable financial footing will affect our future ability to provide services. Monitor have announced that they will be carrying out an investigation into this issue. Financial pressures that are due to out of area placements and use of temporary staffing reflect in part the priority given to patient safety, but are major factors driving the deficit.
6.3 How is the risk controlled and mitigated? 1. Details on the mitigation arrangements are set out in the financial report to the Board. Dedicated resources have been allocated to the financial recovery / CIPs programme including the appointment of Cynthia Conquest (formerly acting Director of Finance).
Confidence level in mitigation:
Red
6.4 What additional actions are required? Reduction in use of temporary staffing including rationalisation of use of locums. Rebalancing of care pathway to reduce use of OOA beds. Generation of new CIPS programmes to fill gaps in current plans. Implementation of the corporate restructure. Maximisation of income through remaining CQUIN targets.
6.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix ID (inability to realise TSS savings) Owner Andrew Hopkins. Datix ID 1084 5 x 4 = 20 and 1090 CIPS delivery 5x4=20. Owner Andrew Hopkins.
6.6 What is the timeline for the mitigation confidence level to reach ‘green’? The finance report presented at this meeting sets out progress on actions underway to address these issues. The timeline back to a secure CoSRR of 3 is likely to take 18 months.
Board Assurance Framework January 2015
Board of Directors – Public 22Jan2015
Board Assurance Framework
Version 1.0
Author: Robert Nesbitt
Department: Corporate
Page 10 of 10 Date produced: 02Jan2015 Retention period: 30 years
7. Name of risk theme (board committees with oversight)
ICT weaknesses (Investment Committee)
7.1 Relevant Trust objectives:
Delivery of an ICT strategy which supports engagement with service users and carers in a convenient and timely way and makes best use of clinicians time (e.g. reduce travel) by October 2014
7.2 What is the nature of the risk? The risk is that patient safety and business continuity is compromised by weaknesses in ICT infrastructure.
7.3 How is the risk controlled and mitigated? 1. Following a report to the Investment Committee on 5th June 2014 investment has taken place in data backup and ICT infrastructure.
Confidence level in mitigation:
Amber
7.4 What additional actions are required? There will be an independent audit of ICT capability be the end of the calendar year to confirm that risks have been mitigated, but see below (7.6) for Disaster Recovery updated timetable.
7.5 How do these risks show on the Trust’s Risk Register? Who owns these risks? Datix ID 1101 (data back-up) 5 x 2 = 10. Datix ID 1100 (Disaster Recovery) 5 x 4 = 20 (increased from 15), Datix ID 1095 (ICT infrastructure) 4 x 3 = 12. Leigh Howlett.
7.6 What is the timeline for the mitigation confidence level to reach ‘green’? ICT are starting to implement the new data backup solution. Its expected completion date is 31 Jan 2015. This is dependent upon the support of external contractors. ICT infrastructure work is due for completion at year end. The Disaster Recovery Capability work has had to be retendered which will delay resolution until mid-2015 discussions are underway with suppliers.
Board of Directors - 22nd January 2015 Month 9 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 1 of 3 Date produced: 9th January 2015 Retention period: 1 year
Report To: Board of Directors - Public
Meeting Date: 22nd January 2015
Title of Report: 2014/15 Financial Performance Report (for the nine month period ending 31st December 2014)
Action Sought: For Information
Estimated time: 15 minutes
Author: Adrian Brooke – Business Accounting & Reporting Manager
Director: Andrew Hopkins, Finance Director
Executive Summary:
The purpose of this report is to inform the Board of Directors of the Trust’s financial performance for the period 1 April 2014 to 31 December 2014. Key headlines for the month include:
• A deficit of £3.77m leading to a revised forecast year-end deficit of £4.6m, which has increased from the £3.7m plan due to additional expenditure being incurred in Month 9. Expenditure plans in the final quarter are being reviewed to identify further measures to bring the outturn back on track and to maintain a COSRR of 2 at year-end.
• A reported Continuity of Service Risk Rating (COSRR) of 2 for December which is forecast to continue to the end of the year based on the financial recovery actions being addressed.
• Temporary staffing expenditure levels have increased this month to £2.10m (£1.83m November). The year to date expenditure now stands at £18.97m.
• Cash position remains ahead of plan by £2.9m as at the end of December. This favourable position is forecast to reduce over the last 3 months of the year and will drop below plan by the year end. Current forecast position indicates that the year-end cash position will be £8.7m which is £12.7m behind original plan.
• A reduction in the number of bed days for acute out of area (OOA) placements in the month. Forecast assumptions have been revised this month to account for this change and the effect of the opening of the Assessment Ward in February 2015.
• Year to date capital expenditure of £3.95m against an original plan of £7.26m.
Date: 22nd January 2015
I Item: 15.07v
Board of Directors - 22nd January 2015 Month 9 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 2 of 3 Date produced: 9th January 2015 Retention period: 1 year
1.0 Financial Position
The following power-point document details the overall Trust Financial Performance
as at the end of December 2014. A summarised position is also attached to this
paper in Appendix 1.
2.0 Recommendations
The Board of Directors is asked to review and note the report.
Adrian Brooke Business Accounting & Reporting Manager 9th January 2015
Appendix 1
Board of Directors - 22nd January 2015 Month 9 Financial Performance Report
Version 1.0
Author: Adrian Brooke Department: Finance
Page 3 of 3 Date produced: 9th January 2015 Retention period: 1 year
Other clinical income 3,028 3,954 926 4,038 5,270 1,233
NHS Mental Health activity Income, Total 145,313 145,662 348 192,991 194,668 1,677
Research and Development 669 1,426 757 892 1,737 845
Education and Training 2,515 2,648 133 3,353 3,536 183
Misc. Other Operating 5,261 8,095 2,834 7,015 10,622 3,607
Other Operating income, Total 8,445 12,170 3,725 11,260 15,896 4,636
Operating Income, Total 153,759 157,831 4,073 204,251 210,564 6,313
Income – Clinical
Block Contracts – (£249k) lower than plan:
• (£356k) under-occupancy provision for CAMHS Tier 4 and Secure Services,
• (£637k) CQUIN provision,
• £427k of Additional Observations for Suffolk CCG’s,
• £295k Additional Income for QEH Liaison and winter pressures
• £21k of other contract variations and budget phasing.
Clinical Partnerships – (£340k) lower than plan:
• (£150k) reduction in the Section 75 NCC and NRP contracts, and
• (£62k) reclassifying of NCA monies to a block contract with Cambridge & Peterborough CCG
• (£155k) re-phasing of NRP innovation monies. The latter will be recovered at the end of the year and
• £27k of other contract movement.
Other Clinical Income - £926k increase to plan: key contributors are:
• £551k agreed contracts over original Annual Plan assumptions
• £375k – Other contract variations including Norfolk Constabulary and System Wide CQUIN
9
Income – Non Clinical income The graph below shows the breakdown of miscellaneous other income against plan.
The deferred/other income variance continues to be due to the conservative assumptions
used when setting the Annual Plan. All of the income achieved is matched with pay and
non pay expenditure.
ICT trading accounts also reflect increased activity against planned assumptions, by
£736k. Figures evidence that trading accounts for these services are making a minimal
profit overall against the level of turnover generated in the year.
Estates trading income is below plan by £379k YTD due to lost contracts. Where this
applies, there are matching pay and non pay favourable variances to plan with no loss to
the Trust overall.
12
Expenditure – Summary Vacancy levels continue to remain high across the Trust, however progress has once again
been made over net recruitment this month to a number of clinical and admin roles across
the Trust. December vacancy levels now stand at 450 WTE’s. It should also be noted that
this vacancy level does not take account of any overtime hours that are regularly worked,
as the WTE of these hours is not captured. The Finance team is looking to implement a
change to this data capture for next financial year...
Temporary pay expenditure continues to exceed the funding available from the vacant roles
(see graphical presentation of forecast Pay position overleaf). Total temporary pay
expenditure in the month was £2.10m (£1.83m November), pushing up YTD costs to
£18.97m.
A decrease in bed days and costs for Out of Area Placements is reported this month and a
further revision of the forecast has been made as a result.
Other non pay expenditure categories remain broadly in line against original plan, with the
exception of Drugs, Public Dividend Capital and Depreciation.
15
Expenditure – PayAgainst original plan, Pay costs report an
adverse variance YTD of £5.14m.
Of the variance, total medical related roles
overspend accounts for £1.14m. ongoing
review of these personnel and the
vacancies they are covering has seen
some positive movement in terms of
reduced expenditure over the year on
locum spend. It is anticipated now that the
forecast overspend in this area will reduce
to £1.5m from an original £1.7m.
The chart shows total spend by pay type
with a forecast level of expenditure.
The forecast position now accounts for the
additional spend relating to the new
Assessment Ward which will open in
February 2015.
The bank and agency ratio (excluding
medical locum agency) worsened this
month with reduced Bank expenditure
assumed to be due to less availability over
the festive period, which in turn increased
Agency costs across DCS localities
Increases in ICT and Lorenzo programme
temporary pay costs, where not met by
additional income, were the result of
infrastructure and service-desk requirements.
Bank expenditure only accounted for 40% this
month (51% last month) of the total bank and
agency expenditure level.
16
Expenditure – Non Pay 1
The YTD adverse position for Drugs has increased this month, to £0.36m, as costs for
December have come in higher than had been forecast.
Training and Education expenditure in the month was broadly in line with forecast
expectation, which is part of the agreed financial recovery plan to reduce expenditure level
by £0.2m against original plan. Discussions continue across the Trust, particularly within
DCS localities, in order to assess training needs for the remainder of the year.
An improved forecast position for Public Dividend Capital (PDC) has been calculated and
reflected in the overall deficit positon this month, which is a £0.3m improvement on previous
forecast assumptions. Current full year cost pressure has subsequently reduced to £0.24m.
The favourable position reported for depreciation continues to be reported due to the Capital
programme being considerably behind the Trust’s original plan. Both the YTD and forecast
out turn depreciation is expected to be favourable by £0.36m which is dependant on Q4
Capital expenditure levels.
17
Expenditure – Non Pay 2
(Specialist and OOA Placements)
Total spend on Specialist and Out of Area placements YTD now amounts to £4.89m.
Specialist placement expenditure in Norfolk accounts for £1.35m of this total but as can be
seen in the graph overleaf, expenditure levels have reduced from earlier in the year and
have largely remained static since June 2014. The slight increase these last 2 months was
due to placements rising by two, to 10, all of which are considered longer term care. Three
of these placements have been identified as very long term and are currently being
reviewed to assess their appropriateness.
A drop in the number of bed days during December, to 846 days (November 1,221,
October 872) for Acute out of area (OOA) placements has seen expenditure levels drop
back to £0.40m for the month. There were 17 admissions in total during the month but 36
discharges. As at the end of the month, 18 patients remain in placements, of which 15 are
in the Central locality, 1 in GY&W and 2 in the West. As a result of the improvement during
December and accounting for the opening of the new Assessment Ward in February, a
further review of the forecast position has been reflected. Total YTD costs now stand at
£2.73m with a forecast level of £3.80m being predicted. As no specific funding for these
placements currently exists, it is these that is placing the biggest cost pressure on the Trust
finances.
There were just 10 days of activity on PICU placements this month.. YTD expenditure
therefore is now £0.43m. NHS Funded care costs for December was in line with
expectation, pushing the YTD expenditure to £0.37m.
18
Expenditure – Non Pay 2 (Placements)
19
Capital
23
The cumulative capital position at the end of month 9 is 54% against the revised target
(month 8 42%). The in-month spend is 81% of target (month 8 – 77%).
The Trust capital expenditure must remain between £5.53m and £7.48m at year end in
order to meet Monitors acceptable range of 85%-115%.
Currently £3.4m of the capital programme is forecast to be spent in the last three months of
the year, of which £1.6m (47%) relates to ICT expenditure. Assurances have been received
form the Head of ICT that these monies will be spent, although there is still a risk of
slippage on these projects.
Balance Sheet
At the end of month 9, the Trust held cash of
£15.2m, £2.9m higher than planned. The
variance is predominantly due to the continuing
low level of capital expenditure but the current
rate of cash being spent in month is high,
leading to a forecast year end position of
£8.7m, £12.7m below plan.
Net current liabilities continue to be higher
(£5.9m) than planned due to higher than
anticipated accruals and holding higher levels
of provisions being held for possible HMRC
liabilities.
Trade receivables are slightly ahead of plan.
This is due primarily to issues with CQUIN
invoices being in query, and non payment of a
number of invoices by Norfolk County Council.
24
Cash flow
The forecast cash position is currently £8.7m at 31st March 2015 against a plan of
£21.41m. The forecast level of revenue expenditure results in the cash position continuing
to be challenging and will continue to be under high scrutiny for the remainder of the year
and going forward.
25
COSRR headroom
27
Below is an indication of the necessary capital services and liquidity headroom to achieve a
COSRR of 2.
This forecast is based on the current forecast plan, and takes into account the adjustments
to the capital expenditure programme and the revised income statement at month 9.
An increase in revenue available for capital service or in the cash for COS liquidity
purposes is required to achieve a 2 for the year end..
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 1 of 8 Date produced: 09th
January 2015 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Business Performance Report – M09 2014/15
Action Sought: For Approval
Estimated time: 10 Minutes
Author: Tim Walsh: Business Intelligence Manager
Director: Andrew Hopkins: Director of Finance
Executive Summary:
The Business Performance report shows that the Trust is compliant across all seven of the key performance standards under the Monitor Risk Assessment Framework. This is shown in the monitor targets section. The overall COSRR rating remains at 2. This paper is for Approval and the Board is requested to consider the Trust’s performance as described within the Business Performance Report.
1. Report contents
1.1 The Business Performance Report is submitted to the Board for month 09 2014/15 and contains details of performance against key Monitor Compliance Framework targets and KPIs for Organisational Delivery, Quality, Safety & Experience and Workforce Development & Effectiveness.
1.2 The Trust remains at an overall COSRR of 2.
Date: 22nd January 2015
J Item: 15.07vi
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 2 of 8 Date produced: 09th
January 2015 Retention period: 30 years
2. Monitor Targets
2.1 Monitor Performance Summary
Ref Measure Target Quarter 3 to Date (M09)
M01 CPA patients receiving follow up within 7 days of discharge
95% 98% 221 out of 225 discharges
M02 CPA patients having formal review within 12 months
95% 97% 1,924 out of 1,985 reviews
M03 Minimising Delayed Transfers of Care
7.5% 4.7% 1878 delayed days out of 39,923 bed days
M04 Admissions to inpatient services had access to Crisis Resolution and Home Treatment (CRHT) teams
95% 98% 324 out of 331 admissions gate-kept
M05 Meeting commitment to serve new psychosis cases by Early Intervention teams
95% 130% 165 new cases against target of 127
M06 Data completeness: Identifiers 97% 99%
219,922 valid entries out of 221,292 possible data fields
M07 Data completeness: Outcomes 50% 82%
8,449 valid records out of 10,302 records
3. Performance
3.1 Director of Operations Norfolk and Waveney Summary
The main areas to highlight in Norfolk and Waveney are:
• Out of area placements have decreased in December. Addressing the number of out of area placements remains a priority.
• Performance in terms of the timeliness of data entry dipped slightly in central Norfolk but remained at 96% in West Norfolk.
• DTOC remained below the 7.5% threshold in December reporting at 6.08% in Central Norfolk.
• The IAPT service continued to report below the 15% access trajectory.
• The locality is continuing to interview and recruit but they do have an issue with recruiting to certain staff bands which means that teams have to carry vacancies which increases pressure on the service. This is particularly an issue in the Access and Assessment service.
• 18 week waits decreased by 19 in Central Norfolk in December.
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 3 of 8 Date produced: 09th
January 2015 Retention period: 30 years
3.2 Director of Operations Suffolk Summary
The main areas to highlight in Suffolk are:
• DTOCs in Suffolk East remain high at 9% in December however this represents a 3% reduction from the position reported in November.
• Performance against the IAPT 15% access target in Suffolk is showing a further improvement in December and was achieved in West Suffolk.
• The number of 18 week waits increased by 6 in Suffolk in December.
3.3 Minimising delayed transfers of care (DTOC)
In December the DTOC position for the trust improved and was reported at 4.7%. This is below the 7.5% threshold. In the Central locality the DTOCs reduced in December from 6.79% to 6.08%. In Norfolk on a weekly basis the DTOCs and potential DTOCs are discussed and agreed with operational staff and a social care lead. It has been identified that there is an insufficient number of beds outside of NSFT which causes pressure on NSFT acute areas. If NSFT look at discharging service users there is often a waiting list for accommodation that has been identified and this means that when funding is agreed the delay is still possible.
Suffolk East were reporting above the threshold at 9.21%.In Suffolk the service is continuing to work in conjunction with Social services to look at the delays especially service users who are awaiting placements in residential care especially the Learning Disability patients. In the last week of December, of the 9 delays, two were for LD service users.
Please refer also to Appendix 1 and Appendix 2. These items list all of the current delays reported in Norfolk and Great Yarmouth and Waveney as at 9th January 2015, split by whether the delay is due to the NHS and Social Care.
3.4 Percentage of qualifying patients with a MHCT cluster (OD07)
In December the trust reported at 97% against a 99% target. Suffolk East and Suffolk West are the lowest performing localities against this metric. In Suffolk East and West a number of data errors had been identified which are now being corrected by the locality business support manager. The locality will also be monitoring the referrals coming from AAT(Access and Assessment Team) into the IDT (Integrated Delivery Team) to ensure they have a cluster and to return to AAT if it is missing.
3.5 Data quality including timely entry (OD09)
The trust performance dipped against this metric for December from 94% to 93%. Further improvements were seen in previous months in Central Norfolk however this locality reported at 88% for December. This will be raised at the performance review meetings for the locality. Suffolk West showed an improvement in December reporting at 97% up 2% from November’s position.
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 4 of 8 Date produced: 09th
January 2015 Retention period: 30 years
3.7 Percentage of IAPT patients who have depression and or anxiety disorders who receive psychological therapy
Access rates continue to be below the target trajectory for December reporting at 8.81% against a target of 11.25%. At a locality level, Suffolk West achieved their target for the second month running and Suffolk East missed the target by 0.9%. Norfolk Central missed the target by 3.7%. In Great Yarmouth and Waveney the IAPT service reported at 8.5% against a target of 11.25%. Action plans are in place across all localities to meet the 15% access rate by the end of quarter 4 2014/15. Weekly reports have been requested by all commissioners during quarter 4 in order to monitor the progress against plan at a regional level.
3.8 Medium and Low Secure Bed Occupancy Rate The low secure bed occupancy increased to 94% in December, a further increase of 4% from last month. Medium secure bed occupancy remained at 79%, this is below the 90% target. The occupancy rate in these units is being monitored by the service and by commissioners.
3.9 Waiting times in completed pathways breaching standard and Number of incomplete pathways waiting over 18 weeks
The number of 18 week waits decreased from 80 to 72 for the trust between November and December. The numbers of 18 week waits decreased in Central Norfolk from 34 to 15. In Suffolk West, the number of 18 week waits increased from 18 in November to 22 in December. They also increased from 3 to 9 in West Norfolk. This will be monitored in the locality action plans.
3.10 Patient Safety Thermometer (QU14)
The trust reported at 99% for the patient safety thermometer in December. There was one fall reported as part of the safety thermometer submission. The fall was in Sweetbriar bungalow in Great Yarmouth and Waveney locality.
3.11 Bed occupancy, out of locality and out of area acute placements
There were 18 out of area placements reported in Norfolk and Great Yarmouth and Waveney as of the end of December. This figure has decreased further from the position reported in November. Assessors remain in place to review the out of area cases in Norfolk. Bed occupancy remains high across the adult acute areas and this was reflective of demand in December.
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 5 of 8 Date produced: 09th
January 2015 Retention period: 30 years
3.12 Access and Assessment
Norfolk
The Access and Assessment performance in November 2014 showed that all Emergency referrals received an assessment within 4 hours. 89.9% of Urgent referrals were seen within 72 hours and 78% of Routine referrals were seen within 28 days. Both the Routine and Urgent referrals report against a 95% target. A Contract Query Notice has been issued by the CCGs in Norfolk because of the performance against the Routine referrals. This is being addressed at the locality performance meetings internally. The December 2014 performance was not available at the time this report was issued.
Suffolk
In Suffolk in November 2014, the Access and Assessment service reported at 100% against both Emergency and Urgent over 18 referrals. For Routine referrals which should be seen within 28 days, there were 21 breaches which resulted in a performance of 91% against a 95% target.
3.13 Norfolk Recovery Partnership (NRP) and Suffolk Alcohol Service
The Norfolk Recovery Partnership has completed all of the actions on the Remedial Action Plan and this has now been signed off by commissioners. October was the first month that the new contract report was submitted to NRP commissioners and the new report was positively received.
NDTMS data is showing an improvement in NRP’s performance especially around the areas that the commissioners were expressing concerns. Now that the local performance management framework has been agreed, this should result in more beneficial local data to not only monitor performance against the contract but also inform service delivery.
With regard to the Suffolk Alcohol Service, performance is robust and constant with no areas of concern. The contract finishes on the 31st March 2015.
3.14 Research Performance Indicators
The Key Performance Indicators as set by the National Institute of Health Research are being reviewed internally by the Research Manager and a full report will be provided in the board report issued in February 2015.
4. Section 75 Partnership
Suffolk
There have been no notable high level developments with regard to the Suffolk Section 75 Partnership. New procedural arrangements have been implemented across all teams and are subject to on-going monitoring with a more detailed review scheduled for spring 2015.
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 6 of 8 Date produced: 09th
January 2015 Retention period: 30 years
5. Workforce Development and Effectiveness
5.1 Vacancies
The Trusts current vacancy rate (WD08) is 11.54%. This is a decrease of 0.11% in the month. In real terms at M9 the Trust had an establishment of 3895.61 and 449.67 vacant posts.
Vacancy rates continue to be above 10% in Corporate Services (-1.82%, at 19.09%), Suffolk Access and Assessment (no change, 14.75%), Suffolk West (-0.38%, at 17.24%), Secure Services (+1.11% at 10.33%) and West Norfolk (+4.82%, at 11.82%). All other localities are below 10%.
5.2 Turnover
At M9 staff turnover (WD09) within the Trust is currently at 15.48%, a reduction of -1.09% in the month.
Turnover within Central Norfolk (-2.74% at 16.45%), Great Yarmouth and Waveney (-1.75% at 10.85%), Secure Services (-0.41% at 12.59%), Suffolk West (-2.48% at 16.78%) and Norfolk West (-2.48% at 19.91%) have all reduced in the month. Turnover within Corporate (+0.21% at 20.37%) and Substance Misuse (+3.26% at 13.08%) have increased in the month.
5.3 Temporary Resourcing
The percentage of nursing shifts that NHSP filled decreased from 69.01% to 66.04% in the month. During December, agency staff covered a further 22.04% of available nursing shifts. 11.6% of vacant shifts went unallocated.
5.4 Absence
Overall, the Trusts rolling 12 month sickness absence rate (WD01) has decreased in the month from 5.09% in November 2014 to 5.03% in December 2014.
5.5 Workforce development
Since April 2014, 65.71% of staff who have had an appraisal due, have had an appraisal completed.
5.6 Employee Relations Currently there are 32 active disciplinary cases within the Trust (no change within the month). There are 9 grievance matters on-going within the Trust (+1 within the month). Across all localities, there are 3 formal capability matters (no change within the month). There are 134 absence cases being managed (-3 in month).
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 7 of 8 Date produced: 09th
January 2015 Retention period: 30 years
6. Recommendations
6.1 The Board is requested to consider the Trust’s performance as described within the Business Performance Report.
Tim Walsh Business Intelligence Manager 09
th January 2015
Appendix 1
The table below summarises all Delayed Transfers of Care for NSFT attributable to Social Care as at 9th January 2015 for Norfolk and GY&W.
Locality Ward Delayed
Description
Total delayed days on
09-01-2015
Commentary for Board Report
Central Glaven Social Care-
Awaiting public funding
0
Patient accepted at Omnia on 11/12/14. Should have gone on 15/12/14 but the
Social Worker needed 2 weeks to prepare a report. Next panel date was
given as 29th January 2015. Trust requested that this was brought forward
to January 12th and this request was granted. Due to Social Worker and
panel delays this was reported as a DTOC due to B - Awaiting Public
Funding Social Care on 09-01-2015
GT Yarmouth
and Waveney
Acute Services Centre
Yarmouth
Social Care -Awaiting public
funding 84
Accepted at Coach House but they require funding for one month. This has
gone back to Social Services (02-01-2015) to agree extra funding
Central Glaven
Social Care -Awaiting residential
home placement/availability
63
Patient accepted at Old Vicarage on 11/12/14 (whilst awaiting a vacancy at Devonshire Place). Request to transfer
agreed funding from Omnia to Old Vicarage was not made on 15/12/14 because the panel requested more
information. The social worker was sent additional information on 29/01/14 and is
still awaiting panel decision 09-01-15.
GT Yarmouth
and Waveney
Foxglove Ward
Social Care -Awaiting residential
home placement/availability
84
On waiting list for Oulton Park since 05/12/14 other facilities have assessed and declined and it has been requested that the social worker keeps looking for
alternatives.
GT Yarmouth
and Waveney
Foxglove Ward
Social Care -Awaiting residential
home placement/availability
42
Social worker failed to find a placement since 28/11/14 with a vacancy prepared
to assess. The ward have been contacting the social worker regularly.
Central Sandringham
Ward
Social Care -Awaiting Nursing
home placement/availability
99 Accepted at Buckingham Lodge, to be
discharged on 11-01-2015
Board of Directors – Public 22
nd January 2015
Business Performance Report
Version 2 2
Author: Tim Walsh Department: Informatics
Page 8 of 8 Date produced: 09th
January 2015 Retention period: 30 years
Locality (Contd..)
Ward Delayed
Description
Total delayed days on
09-01-2015
Commentary for Board Report
GT Yarmouth
and Waveney
Fernwood Ward
Social Care -Awaiting residential
home placement/availability
21 Social worker seeking placement since
19/12/14.
Appendix 2
The table below summarises all Delayed Transfers of Care for NSFT attributable to the NHS as at 9th January 2015 for Norfolk and GY&W.
Locality Ward Delayed
Description
Total delayed days on
09-01-2015
Commentary for Board Report
Central Rollesby
PICU NHS - Awaiting public funding
0
Need neuro psych. unit due to complexity, North Norfolk CCG funding
panel turned down 18-12-14. NSFT going back to panel again with more
information for a specialist placement at Warwick Lodge (place being held for
patient) however this is not an approved North Norfolk CCG provider. The social worker has been contacted by contracts on 09-01-15 for clarification as to current
position.
Central Waveney
Ward NHS - Awaiting
further non-acute 109
Patient accepted at Cygnet, New Dawn facility on 22-08-14, medically fit for
transfer on 22-09-14, Cygnet said bed would be available before Christmas.
The wait continues because there is still no bed on 08-01-15 New Dawn said it would be a minimum of 8 weeks. NHS
England has asked New Dawn to expedite. BMDFT(Bed management) asked for a referral to Milestones or
Springbank however this would require NSFT external placements panel to
agree funding.
GY&W NCC
Rollesby PICU
NHS - Awaiting further non-acute
0 Accepted for LSU 08-01-2015, there is a vacancy in Trust LSU in Suffolk but has
to go through NHS England.
GT Yarmouth
and Waveney
Sweet Briar Ward
NHS -Awaiting Nursing home
placement/availability 78
First on list for Oulton Park since 04-12-2014. CHC contacted weekly for
progress report.
Business Performance ReportDecember 2014 version 2.0
NSFT Informatics
1 BPR December 2014 v2.0/Front
Monitor
Ref Metric Period Value Apr-14 May-14 Jun-14 Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15
FM07 CIPs % of planned CYE (R&NR) savings achieved
Month YTD
FM05Creditors > 90 days past due account for more than 5% of the total creditor balances
Month YTD
FM06 CAPEX % of plan spent Month YTD
FM03 Liquidity rating Month YTD
FM04 Debtors > 90 days past due account for more than 5% of the total debtor base
Month YTD
FM01 Continuity of Service Risk Rating Month YTD
FM02 Capital Service Cover rating Month YTD
BPR December 2014 v2.0/KPI Financials 14_15
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 1 of 8 Date produced: 09th January 2015 Retention period: 30 years
Report To: Board of Directors - Public
Meeting Date: 22nd January 2015
Title of Report: Monitor Compliance Framework – 3rd Quarter 2014/15
Action Sought: For Approval
Estimated time: 10 Minutes
Author: Tim Walsh: Business Intelligence Manager
Director: Andrew Hopkins: Director of Finance
Executive Summary:
This report summarises the Monitor targets and data relating to those targets for Quarter 3 2014/15. The Board of Directors are required to declare an assurance level for Finance, Governance and Quality which references Monitor’s Compliance Framework 2014/15. The Board of Directors is aware that the Trust is under investigation by Monitor and is such this is shown on the Monitor website under the Governance Rating.
1.0 SUMMARY OF REPORT 1.1 The Board of Directors are required to declare an assurance level for Finance,
Governance and Quality which references Monitor’s Compliance Framework 2014/15.
1.2 For the 3rd Quarter the Trust met the threshold for all of the eight governance KPIs.
Compliance against Monitor’s Governance Risk Rating score is 0.0 for Quarter 3. A risk rating of 0.0 gives the Trust a status of ‘GREEN’.
1.3 Please refer to the Finance and Quality reports for detail to support the Finance and
Quality declarations.
Date: 22nd January 2015
K Item: 15.07ix
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 2 of 8 Date produced: 09th January 2015 Retention period: 30 years
2.0 DETAILS OF TARGETS
2.1
Target Threshold Actual
CPA patients receiving follow-up within 7 days of discharge from hospital
95% 98.22%
Data 225 discharges 221 followed up within 7 days 4 followed up not within 7 days
2.2
Target Threshold Actual
CPA patients having formal review within 12 months
95% 96.93%
Data 1,985 qualifying patients 1,924 patients with a contact with care coordinator 61 patients with no contact with care coordinator
2.3
Target Threshold Actual
Minimising delayed transfers of care
<7.50% 4.70%
Data Sum of bed days occupying a bed for each day of period = 39,923 Sum of bed days delayed for each day of period = 1,878
2.4
Target Threshold Actual
Admissions to inpatient services had access to crisis resolution home treatment teams
95% 97.89%
Data 331 admissions 324 via CRHTs 7 via other means including emergency mental health assessment
2.5
Target Threshold Actual
Meeting commitment to serve new psychosis cases by early intervention teams
95% 129.92%
Data NHS Norfolk & NHS Great Yarmouth & Waveney and NHS Suffolk: Target 127 NHS Norfolk & NHS Great Yarmouth & Waveney and NHS Suffolk: Actual 165
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 3 of 8 Date produced: 09th January 2015 Retention period: 30 years
2.6
Target Threshold Actual
Data completeness: identifiers
97% 99.38%
Data NHS Number (%) 96.88 Date of Birth (%) 99.99 Postcode (%) 99.64 Current gender (%) 99.97 Registered GP code (%) 99.88 Commissioner code (%) 99.92
2.7
Target Threshold Actual
Data completeness: outcomes
50% 82.01%
Data With employment status (%) 84.80 With accommodation status (%) 84.57 HoNOS assessment in last 12 months (%) 76.67
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 4 of 8 Date produced: 09th January 2015 Retention period: 30 years
2.8
Target Threshold Actual
Self-certification against compliance with requirements regarding access to health care for people with a learning disability
Compliant in 6 of 6 criteria
Compliant in 6 of 6 criteria
Data The Board of Directors agreed to self-certify that the Trust met all six criteria of compliance for Quarter 1 2013/14 on 25th July 2013.
a) Does the NHS foundation trust have a mechanism in place to identify and flag patients with learning disabilities and protocols that ensure that pathways of care are reasonably adjusted to meet the health needs of these patients? b) Does the NHS foundation trust provide readily available and comprehensible information to patients with learning disabilities about the following criteria: • treatment options; • complaints procedures; and • appointments? c) Does the NHS foundation trust have protocols in place to provide suitable support for family carers who support patients with learning disabilities? d) Does the NHS foundation trust have protocols in place to routinely include training on providing healthcare to patients with learning disabilities for all staff? e) Does the NHS foundation trust have protocols in place to encourage representation of people with learning disabilities and their family carers? f) Does the NHS foundation trust have protocols in place to regularly audit its practices for patients with learning disabilities and to demonstrate the findings in routine public reports? Note: NHS foundation trust boards are required to certify that their trusts meet requirements a) to f) above at the annual plan stage and in each quarter. Failure to do so will result in the application of the service performance score for this indicator.
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 5 of 8 Date produced: 09th January 2015 Retention period: 30 years
3.0 RISKS TO AUTHORISATION
3.1 NHS foundation trusts are required to provide reports for risks to compliance with the Authorisation (including in relation to all the items on this list). These reports are required only by exception, i.e. if there is an issue.
3.2 Finance
� Unplanned significant reductions in income or significant increases in costs � Requirements for additional working capital facilities beyond those incorporated
in the prudential borrowing limit (“PBL”) Failure to comply with the NHS Foundation Trust Annual Reporting Manual
� Discussions with external auditors which may lead to a qualified audit report � Transactions potentially affecting the financial risk rating and/or resulting in an � ‘investment adjustment’ � Proposed disposals of protected assets (or removal of protected status – see
Protection of Assets: Guidance for NHS Foundation Trusts) 3.3 Governance
� Removal of director(s) for significant contractual or non-contractual dispute with another NHS body
� Adverse report from internal auditors � Risk of a failure to maintain registration with the Care Quality Commission � Significant third party investigations that suggest material issues with
governance e.g., fraud, Care Quality Commission reports of “significant failings”, National Patient Safety Agency reports
� Care Quality Commission responsive or planned reviews � Outcomes or findings of Care Quality Commission responsive or planned
reviews � Proposals to vary the Authorisation � Other patient safety issues which may impact the Authorisation (e.g. serious
incidents) � Proposals to vary mandatory service provision or dispose of assets, including: –
cessation or suspension of mandatory service(s) – variation of Authorisation or asset protection processes
� Loss of accreditation of a mandatory service � Reporting of breaches in information governance (including data losses) � Performance penalties to commissioners
3.4 Other Risks
Enforcement notices from other bodies implying potential or actual significant breach of any other requirement in the Authorisation, e.g.:
� Health and Safety Executive or fire authority notices � Material issues impacting the trust’s reputation � Adverse reports from overview and scrutiny committees � Patient group concerns
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 6 of 8 Date produced: 09th January 2015 Retention period: 30 years
4.0 EXCEPTION REPORTS
4.1 Exception reports that make a request for a variation to the Authorisation should cover:
4.2 Nature of request
� A description of the issue that has arisen, identifying the area(s) of the Authorisation to which it applies.
� An assessment of the time frame in which it will come into effect, if approved � Details of the background and reasons for the request. � Overview of implications of the application for a variation (both operational and
financial).
4.3 Proposed Action � A summary of the proposed actions that are required to be put in place (if any) � Required approvals to be received from other third parties (if required)
4.4 Next Steps
� A list of the third parties that the NHS foundation trust has and intends to notify of the issue.
� Evidence of required approvals (if not already provided).
5.0 DECLARATIONS REQUIRED
5.1 The performance to date shows that governance targets are all being met, however the current governance rating is acknowledged as “Under Investigation”. The Board can sign up to the second declaration that all targets should continue to be met over the next year.
5.2 For Finance, the Board is declaring a COSRR of 2 and therefore cannot sign the first declaration regarding a COSRR of 3 for the next 12 months. Wording will be agreed in the return to identify that the board expects a COSRR of 2 over the next 12 months as recovery actions are put in place.
5.3 Please note that the Trust has shared all significant third party reports with Monitor.
Tim Walsh Business Intelligence Manager 09
th January 2015
Board of Directors – Private / Public 22nd January 2015 Monitor Compliance Framework Quarter 3 2014 / 15
Version 2.2
Author: Tm Walsh Department: Informatics
Page 7 of 8 Date produced: 09th January 2015 Retention period: 30 years
Appendix 1 – Governance Declarations.
Date: 22nd January 2015
K Item: 15.07ix Appendix 1
Worksheet "Governance Statement"Click to go to index
In Year Governance Statement from the Board of Norfolk and Suffolk
The board are required to respond "Confirmed" or "Not confiirmed" to the following statements (see notes below)
For finance, that: Board Response
4
For governance, that:
11
Otherwise:
Consolidated subsidiaries:
Signed on behalf of the board of directors
Signature Signature
Name Name
Capacity [job title here] Capacity [job title here]
Date Date
4
Notes:
A
B
C
The board anticipates that the trust will continue to maintain a Continuity of Service risk rating of at least 3 over the next 12 months.
The board is satisfied that plans in place are sufficient to ensure: ongoing compliance with all existing targets (after the application of thresholds) as
set out in Appendix A of the Risk Assessment Framework; and a commitment to comply with all known targets going forwards.
The board confirms that there are no matters arising in the quarter requiring an exception report to Monitor (per the Risk Assessment Framework
page 22, Diagram 6) which have not already been reported.
Number of subsidiaries included in the finances of this return. This template should not include the results of your NHS charitable funds.
Monitor will accept either 1) electronic signatures pasted into this worksheet or 2) hand written signatures on a paper printout of this declaration posted to
In the event than an NHS foundation trust is unable to confirm these statements it should NOT select 'Confirmed’ in the relevant box. It must provide a
This may include include any significant prospective risks and concerns the foundation trust has in respect of delivering quality services and effective quality
Monitor may adjust the relevant risk rating if there are significant issues arising and this may increase the frequency and intensity of monitoring for the NHS
The board is unable to make one of more of the confirmations in the section above on this page and accordingly responds:
Board of Directors – Private / Public
22nd January 2015
Monitor Compliance Framework
Quarter 3 2014 / 15
Version 2.2
Author: Tm W
alsh
Department: Informatics
Page 8 of 8
Date produced: 09th January 2015
Retention period: 30 years
NS
FT
Qu
art
erl
y M
on
ito
r S
ub
mis
sio
n D
ece
mb
er
20
14
A
ctio
n
Ple
ase
ca
n t
he
Bo
ard
be
ma
de
aw
are
th
at
this
in
form
ati
on
wil
l su
bm
itte
d w
ith
th
e M
on
ito
r re
po
rt f
or
Qu
art
er
3.
Su
mm
ary
NS
FT
su
bm
it a
qu
art
erl
y r
ep
ort
to
Mo
nit
or.
In
th
e s
ub
mis
sio
n d
ocu
me
nt
for
Qu
art
er
3 2
01
4/1
5 t
he
Tru
st w
ill r
esp
on
d t
o t
he
CQ
C c
om
plia
nce
qu
est
ion
s a
s fo
llo
ws:
Ta
rge
t o
r In
dic
ato
r R
esp
on
se
Risk of, or actual, failure to deliver Commissioner Requested Services
N
o
CQC compliance action outstanding (as at time of submission)
Ye
s
CQC enforcement action within last 12 months (as at time of submission)
No
CQC enforcement action (including notices) currently in effect (as at time of submission)
No
Moderate CQC concerns or impacts regarding the safety of healthcare provision (as at time of submission)
Ye
s
Major CQC concerns or impacts regarding the safety of healthcare provision (as at time of submission)
No
Trust unable to declare on-going compliance with minimum standards of CQC registration
Ye
s
Th
e f
oll
ow
ing
te
xt w
ill b
e a
dd
ed
in
th
e s
ect
ion
of
the
Mo
nit
or
rep
ort
th
at
en
ab
les
the
tru
st t
o a
dd
co
mm
en
tary
. T
he
te
xt h
as
be
en
su
pp
lie
d b
y S
erv
ice
Go
ve
rna
nce
.
“Cu
rre
nt
CQ
C c
om
pli
an
ce o
uts
tan
din
g a
s o
f 9
th J
an
ua
ry 2
01
4:
Wo
od
lan
ds
ref
INS
1-8
54
74
11
29
da
te o
f v
isit
12
th N
ov
20
13
: U
pd
ate
d o
n t
he
13
/08
/14
, co
mp
leti
on
du
e O
ct 1
4.
1 m
ino
r im
pa
ct r
eco
rde
d f
or
reco
rds.
He
lle
sdo
n r
ef
INS
1-8
54
71
55
52
da
te o
f v
isit
8th
& 9
th J
an
20
14
: u
pd
ate
d o
n t
he
24
.09
.14
.
1 m
ino
r im
pa
ct f
or
resp
ect
ing
an
d i
nv
olv
ing
pe
op
le w
ho
use
se
rvic
es,
1 m
od
era
te i
mp
act
fo
r ca
re a
nd
we
lfa
re o
f p
eo
ple
wh
o u
se s
erv
ice
s.”
Date:
22nd January 2015
K
Item:
15.07ix Appendix 2
Board of Directors - 22.01.15 Constitution change partner govs
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 1 of 3 Date produced: 12.01.15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Proposed change to the Constitution (Partner Governors)
Action Sought: For Approval
Estimated time: 10 mins
Author: Robert Nesbitt: Trust Secretary
Executive: Robert Nesbitt: Trust Secretary
Executive Summary:
The purpose of this paper is to seek approval for a time-limited change to the make-up of the partner governor constituency for the Trust so as to compensate for reduced representation of elected service user and carer governors for Suffolk following the 2014/15 election. The Board of Governors (BoG) approved this change and their meeting on 08.01.15. The Board of Directors are also required to approve changes to the Constitution.
1.0 Proposal
1.1 The proposal is that two partner governor seats are created which exist from 01.02.15 until 31.01.16. The rationale for these seats is shown in appendix .1
1.2 The seats are for Suffolk User Forum (SUF) and Suffolk Family Carers (SFC). Both organisations have said that they would welcome the opportunity to field governor representatives.
1.3 The amendment to the constitution to read,
By Appointment (including partnership organisations) Norfolk County Council 1 Governor Suffolk County Council 1 Governor Norfolk CCG 1 Governor Julian Housing Support Trust Limited 1 Governor
Date: 22nd January 2015
L Item: 15.07x
Board of Directors - 22.01.15 Constitution change partner govs
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 2 of 3 Date produced: 12.01.15 Retention period: 30 years
Norfolk and Suffolk Constabularies 1 Governor University of East Anglia 1 Governor University Campus Suffolk 1 Governor Suffolk Family Carers (01.02.15 until 31.01.16) 1 Governor Suffolk User Forum (01.02.15 until 31.01.16) 1 Governor
Norfolk and Suffolk NHS Foundation Trust’s Youth Council (Suffolk) 1 Governor Norfolk and Suffolk NHS Foundation Trust’s Youth Council (Norfolk) 1 Governor
2.0 Quality implications
2.1 The change will enable a stronger voice for Suffolk services users and carers on the BoG. It will also provide an opportunity to increase the membership of the elected governor constituencies for Suffolk users and carers so as to be in a better position to hold a contested election in 2015/16 for governors to take up their seats from 01.12.16.
6.0 Equality implications / summary of consultation
6.1 The proposal assists in the work of the Trust in its Public Sector Equality Duty of promoting understanding of protected characteristics groups.
6.2 The Board of Governors approved the proposal and both SUF and SFC welcome the move.
6.3 These changes will require ratification at the AGM members’ meeting but their implementation is not delayed by this step.
7.0 Risks / mitigation in relation to the Trust objectives
7.1 There are no risks to the Trust objectives from this proposal.
8.0 Recommendations
8.1 Directors are asked to approve the change to the Constitution. The consequence of not approving the change would be that Suffolk service user and carer voices would be under-represented on the Board of Governors.
Robert Nesbitt Trust Secretary
Board of Directors - 22.01.15 Constitution change partner govs
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 3 of 3 Date produced: 12.01.15 Retention period: 30 years
Background Papers / Information
Proposed Board of Governors – from 01 Feb 2015
Public 13, Staff 4
Service User 4, Carer 2
Appointed 11
Service User (4) Public – Suffolk (6) Norfolk Suffolk
Norfolk
� Siobhan Leviton
� Kevin James
Suffolk
� Paul Gaffney (Suffolk)
� Vacant (Suffolk)
� Paddy Fielder
� Susie Enoch
� Jane Millar
� Guenever Pachent (Lead)
� Andrew Good
� Kathleen Ben Rabha
� Pip Coker – Julian Support
� Rosie Doy – University of East Anglia
� Cllr Sue Whitaker – Norfolk County Council
� David Skevington – Suffolk Constabulary (covering for Norfolk Constabulary too)
� Ann Donkin (Norfolk CCG rep)
� Vacant – University Campus Suffolk
� Cllr Tony Goldson – Suffolk County Council
� Vacant – Youth Council (Norfolk)
� Vacant – Youth Council (Suffolk)
� Suffolk User Forum
� Suffolk Family Carers
Carer (2)
� Vacant (Suffolk)
� Mary Rose Roe (Norfolk)
Public – Norfolk (7)
� Sheila Preston
� Stephen Fletcher
� Ronald French
� Elizabeth Witt
� Pat Southgate
� Catherine Wells
� Hilary Hanbury
Staff (4)
� Dr Nanayakkara De Silva
� Dr Karen O’Sullivan
� Howard Tidman
� Linda Weatherley
See Appendix 1 for Board of Governor report (08.01.15)
Board of Governors – Public 08Jan 2015 Governor vacancies
Version 1.1 Author: Robert Nesbitt Department: Corporate
Page 1 of 2 Date produced: 15Dec2014 Retention period: 30 years
Report To: Board of Governors
Meeting Date: 8th January 2015
Title of Report: Action regarding governor vacancies
Action Sought: For approval
Estimated time: 10 minutes
Author: Robert Nesbitt – Trust Secretary
Executive: Robert Nesbitt – Trust Secretary
1.0 Summary of Report
1.1 The outcomes of the governor elections 2014/15 are reported under item 15.01. It can be seen that there were no nominations for the Suffolk Carer vacancy, and only one nomination for the two Suffolk service user vacancies. The Board of Governors will be light on service user and carer views in the next period (beginning 01.02.15).
1.2 This paper sets out the options and recommends that there is a concentrated effort to build the pool of user and carer members over the coming year so that when we hold the next elections there is better chance of a (preferably contested) election.
1.3 The paper also introduces a suggestion to mitigate the lower level of Suffolk service user and carer governor voices in the interim by creating temporary partner governor roles for representatives from Suffolk User Forum and Suffolk Family Carers.
2.0 Governor vacancies – the position and options
2.1 The constitution does allow for elections to be held mid-term, however, there are three reasons why waiting might be preferable:
First, all Suffolk service user and carer members who have expressed an interest in being a governor received a personal letter from Gary Page in November 2014 inviting them to consider standing and to attend an information session. However, the pool of prospective members from which to draw service user and carer governors is quite small compared to the Suffolk public constituency. If we run the election again now we will in effect be fishing in the same pool. Having asked Electoral Reform Services for their opinion, they suggest concentrating efforts on expanding the number of members and prospective governors rather than simply running the election again with the same Iimited pool. We could, for example, offer
Date: 22nd January 2015
Li Item: 15.07x Appendix 1
Board of Governors – Public 08Jan 2015 Governor vacancies
Version 1.1 Author: Robert Nesbitt Department: Corporate
Page 2 of 2 Date produced: 15Dec2014 Retention period: 30 years
to run targeted membership campaigns with Suffolk Family Carers mental health project and Suffolk User Forum to build the membership.
Second, the annual cycle of new governors starting in February each year makes it possible to organise induction programmes for each cohort. Staggering elections so that new people start mid-year means that this will not be possible and it would also be potentially confusing for people to know when terms start and end.
Third, running the elections is a significant time commitment. It would put considerable pressure on the Trust Secretariat to organise the pre-election publicity, information sessions and coordinate the data transfers twice a year instead of once.
2.2 The downside of waiting a year, however, is that we will continue to have no named governor voice for Suffolk carers and only one service user governor for Suffolk. This is mitigated by the fact that many public governors (and probably some partner governors) have user and carer experience.
2.3 An additional option for the Board of Governors is to create temporary partner governor seats for SUC and SFC until the February 2016 intake. Informal contact with both organisations has been encouraging but it would require a formal decision by their Trustees in order to implement this. If the Board of Governors agree then these discussions can be taken forward with a view to updating the constitution from March 2015.
3.0 Recommendation
3.1 Governors are asked to consider the above options and agree a way forward.
Robert Nesbitt Trust Secretary
Background Papers / Information Current membership for Suffolk
Carer Service User Public
399 142 5672
BoD Public - 22.01.15 Policies to BoD
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 1 of 3 Date produced: 09.01.15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22 January 2015
Title of Report: Policies that need to come to the Board
Action Sought: For Approval
Estimated time: 10 minutes
Author: Robert Nesbitt: Trust Secretary
Executive: Robert Nesbitt: Trust Secretary
Executive Summary:
This paper is coming to the board as requested at the December 2014 BoD meeting. The purpose is to clarify which policies require board approval. The paper sets out proposed criteria to identify policies and then applies these to existing policies. Directors are asked to consider and approve the criteria and confirm or amend the list.
1.0 Criteria for policies to require board approval
1.1 If governance arrangements within board committees and operational management groups are functioning appropriately then in almost all cases they should have the authority and capability to authorise policies for the Trust. However, there is a case to argue that a small number of policies are so critical to the organisation (either from a culture or risk / reputation point of view) that the board may not want to delegate approval.
1.2 It is important for the board to be assured that there is a system in place to identify the need to create a policy, that it is fit for purpose and reviewed at an appropriate period. If the board is not confident that this is the case then the solution, of course, is not to pull the work into the board, but rather direct that the systems are made fit for purpose and can be seen to be so.
1.3 The point has been made that the distinction between policies (short statements of principle), procedures (operationalisation of a policy – the who, why, where or what), and protocols (mandatory processes or rules) is often blurred and many of our policies currently also include procedures and protocols.
Date: 22nd January 2015
M Item: 15.07xi
BoD Public - 22.01.15 Policies to BoD
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 2 of 3 Date produced: 09.01.15 Retention period: 30 years
1.4 The proposed criteria for policies that require board approval are that:
a. they are so core to setting the culture of the organisation that the board has a legitimate role in approving the policy and being seen to lead on it, or b. they relate to a risk which is of significant importance in relation to the Trust’s objectives that the board wishes to be directly assured as to its suitability, or c. that there is an externally mandated requirement that the board accepts as appropriate, or d. that they are controversial or carry reputational risk.
3.1 If the criteria are set and applied appropriately the board should add value to the quality of Trust services and the understanding of its role by the organisation is augmented. See also risks (5). Certain policies will be approved by Board committees (such as counter-fraud, and business conduct by the Audit and Risk Committee).
4.0 Equality implications / summary of consultation
4.1 There are no equality implications, the Chair and Chair of Audit and Risk have been consulted on this paper.
5.0 Risks / mitigation in relation to the Trust objectives
5.1 The risk of setting the criteria too low is that the board uses its limited time inefficiently and therefore is unable to adequately address the bigger issues.
5.2 This is mitigated by ensuring that where a policy does come to the board, it is in a finished state and requires little or no discussion. No draft reports should ever come to the board for debate or comment; this work should take place in committees or operational management groups.
6.0 Recommendations
6.1 That directors approve the criteria of policies that come to the board.
6.2 That directors agree the list below as the set of policies that are identified by the criteria.
BoD Public - 22.01.15 Policies to BoD
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 3 of 3 Date produced: 09.01.15 Retention period: 30 years
6.3 The risk of not accepting 6.1 is that, unless an alternative is agreed, there continues to be uncertainty about the role of the board in policy approval. The risk of not accepting the list of policies below is marginal (assuming that the criteria are agreed) as this can be rectified before the next board meeting.
Robert Nesbitt Trust Secretary
Background Papers / Information Policies that set the culture and that are proposed as coming to the board for approval Being Open - C104 Duty of Candour – Q06 Public Interest Disclosure Whistle-blowing policy HRP006 Equality and Diversity – HR-013 Policies that relate to risk Health and Safety – Q23 Fire - Q03 Ligature and suicide risk - Q46 Risk Management Strategy – Q18 Standing Financial Instructions Safeguarding children - C89 Safeguarding vulnerable adults – C90 Policies which may be contentious (this will change over time) Smoking – Q49
Note – The SFIs / Scheme of Delegation will always come to the board.
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 1 of 6 Date produced: 13.01.15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Board of Director committee structure and terms of reference
Action Sought: For Approval
Estimated time: 10 mins
Author: Robert Nesbitt: Trust Secretary
Executive: Robert Nesbitt: Trust Secretary
Executive Summary:
Following the Foresight Partnership board evaluation, the board of directors agreed to streamline the committee structure so as to provide a clearer line of sight into the organisation and to create capacity for a refocus of non-executive director time. The Healthy NHS Board (2013) notes that, “effective boards minimise the number of standing board committees.” (p.16). The new structure was approved at the board meeting in November 2014 and this paper brings together the terms of reference for the new committee structure. The number of committees is reduced by two and much work has already been undertaken in refining the terms of reference for the Service Governance Committee including its relationship to the Audit and Risk Committee structure. The paper sets out the key changes, including the role of the operational management groups that will take up existing elements of work from the current Investment and Communications Committees. There is a risk in changing a governance structure, that new gaps or overlaps are created and the paper sets out how the work of those committees that will end from 31.03.15 is captured either by other committees or within the operational management groups structure. Whilst good governance is built on a foundation of appropriate structures, such structures do not in themselves lead to good outcomes. They are there to support effective behaviours and therefore these changes are part of a wider board development plan.
Date: 22nd January 2015
N Item: 15.07xii
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 2 of 6 Date produced: 13.01.15 Retention period: 30 years
1.0 Constitutional requirements and overarching principles
1.1 NSFT’s constitution Annex 8 S.34 requires that the Board establish an Audit and Risk Committee and Remuneration and Terms of Service Committee as well as the Charitable Funds Committee. It permits the establishment of any other committees required to discharge the Trust’s responsibilities.
1.2 The Board makes appointments to these committees and the constitution stipulates that only non-executive directors may be members of the Remuneration and Terms of Service Committee and the Audit and Risk Committee (one of whom must have recent and relevant financial experience). The Board can delegate executive powers to committees that are formally constituted.
1.3 The principles applied to the structure are based on The Healthy NHS Board 2013.
o The board leads on the strategic process in collaboration with partners.
o There is a clear structure and sufficient capacity to hold the organisation to account for the delivery of the strategy.
o The board has time to develop a shared ethos (based on openness, learning, transparency, accountability and candour) through which it can shape the culture of the organisation.
2.0 Investment
2.1 Board committee oversight of the investment strategies (including estates and ICT strategies given that these are constrained by capex considerations) and approval of decisions within delegated limits set out under the Standing Financial Instructions moves to the Finance Committee (re-named from Finance and Performance). The investment committee will cease to exist from 31.03.15. The SFIs will be amended to reflect this. At present the financial thresholds for the investment committee as set out in the SFIs are:
i. the proposed annual additional revenue cost is in excess of £500,000
within the first two years; and/or
ii. the capital cost of the development exceeds £100,000 (excluding VAT);
Decisions on capital investment projects in excess of £1m are reserved to the Board of Directors. Directors may wish to review these levels.
Consideration of decisions to bid for new contracts or to disinvest will move to the Finance Committee which, where required, will make recommendations to the Board of Directors in line with SFI thresholds or where the risk / reputational issues indicate the need to do so.
2.2 The work that did take place within the Investment Committee in checking and scrutinising business cases will become an executive responsibility within an Investment Appraisal Group led by the Director of Finance. The Director of Finance will work closely with other executive directors, particularly the Director of
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 3 of 6 Date produced: 13.01.15 Retention period: 30 years
Strategy and Resources, but would be the accountable officer for investment appraisal.
The purposes of this operational management function are to:
o Check that business cases are aligned with Trust’s overall strategy, locality clinical priorities, the Estates Strategy, the ICT strategy and within the approved capital expenditure plan.
o Ensure that there is an integrated approach to investment decisions so that synergies can be maximised and waste minimised,
o Allocate funds efficiently,
o Ensure that business cases are robust with an appropriate level of detail on options, costs, payback periods and risks.
o Provide a clear audit trail for investment decisions,
o Escalate problematic or potentially controversial issues to the Finance Committee.
o Where appropriate, track multi-staged investment programmes to ensure that they remain within agreed tolerances,
o Prepare the annual capital expenditure plan for approval by the Finance Committee in line with the business cycle.
o Provide exception reporting to the Finance Committee on the capex plan and on ICT and Estates Strategies implementation within tolerances approved by that committee.
2.3 On this basis none of the functions currently carried out by the Investment Committee will be lost, and the workloads for the Director of Finance and Director of Strategy and Resources should remain unchanged, but the non-executive directors will have additional capacity to focus on the wider strategic aspects of Finance (and the work of the board as described in 1.3).
3.0 Communications
3.1 The communications committee was put in place partly in response to a period of sustained external pressure in 2014 at a time of internal change when additional support was needed. The board considered at the time that this might only be needed on a temporary basis and with the appointment of the new head of communications who took up her role this month, the functions of the committee can now be part of the operational management of the communications team.
3.2 The objectives of the committee, which formed part of the terms of reference approved in June 2014 remain relevant and are mapped on to the following functions in the table below
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 4 of 6 Date produced: 13.01.15 Retention period: 30 years
Communications Committee ToR How taken up
Communicate the vision of the Trust
and support implementation of the
Trust’s strategic objectives and service
development plans
This would be part of the objectives for
the head of communications, and may
also figure in executive director
objectives for the coming year.
Actively engage staff, service users,
carers, Governors, the wider health
economy, local population, regulators
and stakeholders (such as MPs, DoH
and Trade Unions) in the work of Trust
This was always a challenge for a
committee. The stakeholder analysis
work of the Director of Strategy and
Resources will provide the basis for a
SMART approach to stakeholder
engagement.
Ensures forthcoming and emerging
issues are appropriately managed and
the outcomes are evaluated
This is a function of the communications
team supported by executive
colleagues.
Ensures Trust staff are aware of the
communication function, their role and
how to communicate both positive and
negative activity
This relates closely to the values and
behaviours work which will inform
personal objectives for staff for the
coming year.
Assures that any consultation or event
is well managed and evaluated for
success
Formal consultation (under S.242)
should be picked up within the
programme plan for the change. Event
management and evaluation is a
function of the communications team
supported by Trust colleagues.
Establishes and evaluates whether the
Trust is developing a positive profile
and brand recognition is increasing
amongst its staff and key stakeholders
Brand profile tracking and management
is a function of communications and
marketing functions.
4.0 Committee structure and terms of reference
4.1 The revised committee structure from 01.14.15 is shown in appendix 1.
4.2 A proposed set of changes to the Finance Committee to take account of the Investment Committee changes, reflecting S.2 above is shown in appendix 2
4.3 The terms of reference for the core committees are set out in appendix 3.These are included to make it easier for directors to cross-check assurance arrangements and the overall scope of the new structure.
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 5 of 6 Date produced: 13.01.15 Retention period: 30 years
4.4 The exception to this is the ToR for the Remuneration and Terms of Service Committee. The FTN Compendium of Best Practice recommends that CEOs should be members of the committees (although not of course involved in setting their own terms and conditions). However, to be consistent with the Trust’s constitution, the CEO should attend the committee but not as a voting member of it. This anomaly requires that alignment and it is proposed at this stage the ToR be amended to be consistent with the constitution, and that the RemToS committee then considers whether or not to recommend a change to the constitution to the board of governors.
5.0 Transitional arrangements
5.1 There is a risk that in changing structures important work is lost. This is mitigated by the Chair of the former Investment Committee being a member of the Finance Committee. However, the final IC meeting minutes and its workplan for 2014 should be reviewed by the Finance Committee to check that no issues are overlooked.
5.2 Chairs of committees will of course continue to refer items between committees and discuss issues of common relevance.
6.0 Quality implications
6.1 These changes are intended to streamline the work of the board committees so as to free up capacity to concentrate on the key board roles of formulating strategy, shaping culture, and ensuring accountability.
7.0 Equality implications / summary of consultation
7.1 There are no equality implications. This paper is based on deliberations at board and subsequent discussions. An area that may need further consideration by the board is how performance can be effectively scrutinised in order to assist the board in gaining assurance.
8.0 Risks / mitigation in relation to the Trust objectives
8.1 The key risk in changing governance arrangements is that they create new fault-lines or gaps which impact on quality. This is mitigated by mapping the work of the committees that are dissolved into the new structure as set out in this report.
8.2 A secondary risk is that an assumption is made that changing the structure will itself improve accountability. This is mitigated by the parallel board development work based on the Foresight Partnership recommendations.
9.0 Recommendations
9.1 Directors are asked to approve the changes. The next stages will then be for the Finance Committee to review the terms of reference with its wider membership
Board of Directors - 22.01.15 Committee Structure
Version 1.1
Author: Robert Nesbitt Department: Corporate
Page 6 of 6 Date produced: 13.01.15 Retention period: 30 years
and adopt them if no further changes are required. The executive team will ensure that the investment and communications committee changes are implemented.
9.2 The consequence of not approving the changes will be a delay to the implementation of the structure agreed in November 2014, but as the timetable for the introduction of the new structure is April 2014 there is some latitude on this.
Robert Nesbitt Trust Secretary
Background Papers / Information Appendix 1 – New governance structure diagram from 01.04.15 Appendix 2 – Proposed changes to the Finance ToR to take account of the IC changes (for approval) Appendix 3 – ToR for: I. Investment Committee II. Communications Committee III. Remuneration and Terms of Service (amended for approval) IV. OD and Workforce (no change) V. Audit and Risk (no change) VI. Service Governance (no change)
Service Governance Ctte
KEY
Board of Directors
Board of Governors
Nominations Ctte Planning &
Performance
Membership /
comms
Education
Finance Ctte
MHA Hosp Mgrs Ctte
Local People
SU and Carer Trust
Partnership
Drugs and
Therapeutics Ctte
Research
Governance Ctte
Infection Prev. &
Control Ctte
Medical Advisory
Ctte
MH Law Forum
H&S Ctte
Clinical
Effectiveness &
Policy Group
Equality and
Diversity Group
Locality / Service
Governance
Groups
Executive Team
Information Gov
Sub-Ctte
Flexible WF Prog.
Board
Perf Review
Group
Trust Partnership
Forum / LNC
Clinical Cabinet BoG Group
BoD Ctte
Operational
bod bog ctte and subgroup structure 2015 11dec2014
amended
Reporting
Consulting /
Liaising ICT Strategy
Programme Board
Lorenzo
Programme Board
Nursing
Workforce Council
Remuneration
Ctte
Audit & Risk Ctte
Investment
Group
OD and Workforce
Ctte
Charitable
funds
Communications
Group
Committee structure from April 2015
Board of Directors - 22.01.15 Committee Structure App 2
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 1 of 3 Date produced: 13.01.15 Retention period: 30 years
FINANCE COMMITTEE
Terms of Reference for approval – January 2015
1.0 Constitution
The Board of Directors hereby resolves to establish a Committee of the Board to be known as the Finance Committee (The Committee).
The Committee is a non-executive committee of the Board of Directors and has no executive powers, other than those specifically delegated to it in these Terms of Reference.
2.0 Authority
The Committee is authorised by the Board of Directors to scrutinise any activity within its Terms of Reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board of Directors to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
3.0 Role of the Finance Committee
The Finance Committee is specifically charged with undertaking the following roles:
� To provide oversight to the development and effectiveness of the Trust’s integrated performance management systems.
� To monitor the integrated performance, including financial performance, of the Trust.
� To approve the annual capital expenditure plan ensuring that it is aligned to the Trust’s overall strategy
� To set and monitor the risk tolerances for the capital expenditure plan, and for strategies reporting to the committee.
� To receive exception reports from the executive on the implementation of the Capex Plan and the Estates and ICT strategies.
� To monitor the development and implementation of the cost improvement programme
Date: 22nd
January 2015
Nii Item: 15.07xii
Board of Directors - 22.01.15 Committee Structure App 2
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 2 of 3 Date produced: 13.01.15 Retention period: 30 years
� To review and monitor the integrated performance of all significant partnership arrangements.
� To approve specific investment / disposal business cases where the commitment is at or above the level set out in the standing financial instructions or where there are non-financial risks (such as reputation) that require consideration.
� To decide whether to bid or re-bid for contracts within SFI thresholds, referring decisions to the Board of Directors where appropriate.
� To consider any areas of risk that may impact on the Trust objectives and to escalate these for inclusion in the Board Assurance Framework, or update the BAF where appropriate.
� To share information with other board committees, referring issues as appropriate.
� The committee may require project highlight and post-implementation reviews as appropriate.
� The committee adhere to regulatory requirements and will take account of guidance issued by regulators and the Treasury in its work.
4.0 Membership
The Committee shall be appointed by the Board of Directors from amongst the Directors and comprise:
� Non-Executive Director Chair
� Two other Non-Executive Directors
� Chief Executive
� Director of Finance
� Director of Strategy and Resources
� Directors of Operations for N&W and Suffolk
The Non-Executive Directors will normally be designated but can, from time-to-time be substituted by any other Non-Executive Director as agreed with the Chair.
A quorum shall be four members: two Non-Executive Directors and two Executive Directors.
5.0 Attendance
The Committee may require the attendance of other Executive Directors or other Trust staff as required (such as technical advisors from within or outside the Trust).
There is no minimum attendance requirement in order to remain a member of the Committee.
The Trust Secretary, or whoever covers these duties, shall be Secretary to the Committee and shall attend to take minutes of the meeting and provide appropriate support and advice to the Chairman and committee members.
6.0 Frequency of meetings and reporting to Board of Directors
Board of Directors - 22.01.15 Committee Structure App 2
Version 1.0
Author: Robert Nesbitt Department: Corporate
Page 3 of 3 Date produced: 13.01.15 Retention period: 30 years
The Committee will meet at least six times per annum.
The Chair will prepare a written report summarising the key areas of discussion / outcomes for the next Board of Directors’ meeting. Minutes of the Committee will also be available to all members of the Board of Directors.
7.0 Agenda
The agenda will be set by the Chair in conjunction with the Director of Finance and circulated seven days prior to the meeting. Items for inclusion must be informed to the Trust Secretariat at least fourteen days before the circulation of the agenda.
8.0 Minutes
The Trust Secretary shall arrange administrative support to the Committee which will include the following duties:
� Agreement of agenda with the Chair and attendees and collation of papers;
� Taking the minutes and keeping a record of matters arising and issues to be carried forward; and
� Advising the Committee on pertinent areas.
The minutes will be prepared by the Meetings Secretary and distributed no later than ten working days after the meeting, and ratified at the following meeting, in accordance with Trust standards
9.0 Other functions
The Committee may undertake additional work as delegated from time-to-time by the Board of Directors. This will require formal variation to the Terms of Reference at a Board of Directors’ meeting.
10.0 Review of performance of the committee and its terms of reference
The committee will consider its performance against the terms of reference and will review the terms of reference on an annual basis and report the outcome of this to the board of directors.
Original 22Jan2015
Terms of Reference & Constitution version 1 Approved - BoD 27Feb2014 Investment Committee Page 1 of 4
Investment Committee Terms of Reference
1. Purpose of the Committee
The Committee is authorised by the Board of Directors to consider, and within delegated powers approve, proposed major capital investment decisions for new business, acquisitions and disposals including any associated revenue consequences within the authorities delegated to the Committee by the Board of Directors, under the Trust’s Scheme of Delegation. The Committee will provide assurance to the Board that business cases for investment have been properly prepared and that it fully and fairly describes the costs and benefits both financial and non-financial over the life of the investment. It will also consider all post project evaluation reports on capital investments. The committee will provide assurance that best value is being delivered on all asset sales with a value greater than £250,000. The committee will be advisory to the Board and review compliance with financing agreements and covenants and the operation of treasury management policies.
2. Functions
a. The Committee’s primary role is to evaluate proposals for new major
business developments (capital and associated revenue consequences), and to make considered judgement as to whether they should proceed or not to implementation. The Committee will approve proposals within its delegated limits or make recommendations to the Board of Directors as appropriate.
b. This will relate to all business developments that require financial investment by the Trust or from outside, if either:
i. the proposed annual additional revenue cost is in excess of £500,000 within the first two years; and/or
ii. the capital cost of the development exceeds £100,000 (excluding VAT); and / or
Date: 22nd January 2015
Niii Item: 15.07xii Appendix 3i
Terms of Reference & Constitution version 1 Approved - BoD 27Feb2014 Investment Committee Page 2 of 4
iii. the nature of the business development is of strategic importance and/or requires a new business, organisational or legal structure (e.g. joint ventures).
c. The Committee will evaluate all disposal or divestment proposals in accordance with the determined limits as set in the Trust’s SFI’s.
d. The Committee shall receive quarterly highlight and financial reports on all approved business cases including those approved by the Board of Directors.
e. The Committee will formally consider post project evaluation reports on significant capital investments (as defined above).
f. The Committee will be responsible for drafting clear guidance as to the expected structure and content of a Business Case, and individual members (or technical advisors) may be called upon to assist in the development of such cases prior to the case coming to the Committee.
g. The Committee will be able to give advice on preliminary outline business cases or business opportunities where it is difficult to judge whether it is worth proceeding with a business venture. It will not be the Committee’s role to develop a venture but it will give feedback on preliminary cases.
h. The Committee will receive reports from the Estates, ICT and Facilities Group.
i. The Committee will take account of the guidance published by Monitor, “Risk Evaluation for Investment Decisions by NHS Foundation Trusts”
j. The Committee will review Treasury investment decisions and reporting guidance.
3. Accountability & Reporting Procedures
The Investment Committee is a sub-committee of, and accountable to, the Board of Directors.
The Investment Committee will formally report in writing to the Board after each meeting. The Committee will prepare and submit a summary Annual Report of its activities to the Board of Directors.
At least once a year the Committee will review its own performance and terms of reference to ensure that it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board of Directors for approval.
The Committee is authorised to seek any information it requires from any employee, and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised to obtain outside legal advice or other professional advice and to secure the attendance of outsiders with relevant experience if it considers this necessary to support its deliberations.
Terms of Reference & Constitution version 1 Approved - BoD 27Feb2014 Investment Committee Page 3 of 4
4. Delegated Limits
Capital Expenditure Delegated Limits Delegated Limit per project
Board of Directors > £2m
Investment Committee > £100,000 < £1m
Director of Finance and other Director < £100,000
5. Membership
A Non-Executive Director, preferably with a financial and / or commercial background, will chair the Committee.
The membership of the Committee shall be: � Non-Executive Director (Chair) � Non-Executive Director (Vice-Chair) � Director of Finance & Performance � Commercial Director � Medical Director (or deputy) � Director of Operations
Members of the Audit and Risk Committee should not normally be members of the Investment Committee.
Business case sponsors may be invited to attend by exception.
The Committee may ask any or all of those who normally attend but who are not members to withdraw to facilitate open and frank discussion of particular matters.
The Board of Directors will review membership of the Committee annually. 6. Technical Advisors to the Committee
The Technical Advisors to the Committee (who will attend for items as appropriate) shall be:
� Deputy Director of Finance � Head of Strategic Estates � Head of Maintenance Services � Head of Facilities � Head of Finance � Operational Managers – Direct Care Services � Head of ICT
The Committee may invite staff of the Trust, staff from partner organisations and internal or external audit to attend meetings as necessary to assist with discussions on any particular matter.
Terms of Reference & Constitution version 1 Approved - BoD 27Feb2014 Investment Committee Page 4 of 4
7. Quorum
A quorum shall exist if three voting members are present, one of who must be a Non-Executive Director. In the absence of the Director of Finance, the Deputy Director of Finance shall be a voting member.
8. Deputies
Deputies are not normally allowed, except for Formal Deputies in accordance with the Compliance Framework.
9. Meetings
Meetings will be held bimonthly. Additional meetings may be called as appropriate.
10. Agenda
The agenda will be set by the Commercial Director, in consultation with the Chair, and circulated seven days prior to the meeting. Items for inclusion must be informed to the Director of Finance at least fourteen days before the circulation of the agenda. This is in accordance with Trust standards
11. Minutes
The minutes will be prepared by the Meetings Secretary and distributed no later than ten working days after the meeting, and ratified at the following meeting, in accordance with Trust standards.
12. Review of the Terms of Reference
These will be reviewed annually, or more frequently if appropriate, and submitted to the Board of Directors for consideration.
Last Review: 1st November 2012, 7th November 2013,
Approved at BoD 27 Feb 2014
Board of Directors – Pvt 26Jun 2014 –
Draft Comms Ctte ToR
Version 0.1 Author: Leigh Howlett
Department: Commercial Directorate
Page 1 of 2 Date produced: 09Jun2014 Retention period: 30 years
Communication Committee
Terms of Reference
1. Purpose
To support implementation of a robust communication and engagement strategy for
the Trust which will ensure staff, stakeholders, service users, carers and the public
are systematically engaged in service planning, prioritisation and monitoring.
To ensure the Trust listens to feedback received from staff, service users, carers, the
public and wider health economy, and that any actions taken as a consequence are
clearly communicated. This will include acting on learning from complaints and Trust
communication activity.
2. Membership
The core membership of the group is:
Non-executive Director (Chair)
Commercial Director
Director of Workforce and Organisational Development
Head of Communication.
(possibility of second NED)
The group may request others to attend its meetings for the purpose of providing
guidance and advice.
3. Accountability and Relationship to Other Committees
The Communications Committee will be accountable to the Trust Board
Date: 22nd January 2015
Niv Item: 15.07xii Appendix 3ii
Board of Directors – Pvt 26Jun 2014 –
Draft Comms Ctte ToR
Version 0.1 Author: Leigh Howlett
Department: Commercial Directorate
Page 2 of 2 Date produced: 09Jun2014 Retention period: 30 years
4. Frequency of Meetings
Meetings will be held monthly.
5. Objectives
The committee is formed to evaluate communication activity not undertake specific
delivery. It aims to ensure NSFT has arrangements in place that:
1. Communicate the vision of the Trust and support implementation of the
Trust’s strategic objectives and service development plans
2. Actively engage staff, service users, carers, Governors, the wider health
economy, local population, regulators and stakeholders (such as MPs, DoH
and Trade Unions) in the work of Trust
3. Ensures forthcoming and emerging issues are appropriately managed and the
outcomes are evaluated
4. Ensures Trust staff are aware of the communication function, their role and
how to communicate both positive and negative activity
5. Assures that any consultation or event is well managed and evaluated for
success
6. Establishes and evaluates whether the Trust is developing a positive profile
and brand recognition is increasing amongst its staff and key stakeholders.
6. Quorum
The meeting shall be quorate when at least three members are present.
7. Attendance
Members are expected to regularly attend meetings and contribute to the
discussions.
8. Review
The Terms of Reference will be reviewed annually.
Terms of Reference 14Mar08: Reviewed 7Sept09, Reviewed 27Jan2011. Reviewed 03Dec2012. Approved by BoD 22Dec2012, Approved BoD 15Jan2014 Page 1 of 4
Remuneration & Terms of Service Committee (RemToS)
Terms of Reference
1.0 Authority
1.1 The RemToS committee is constituted as a standing committee of the Trust’s board of directors.
1.2 The RemToS committee is authorised to act within its terms of reference in order to identify and appoint candidates for all executive director positions, and to determine their remuneration and terms of service.
1.3 The RemToS committee is authorised by the board of directors to instruct professional advisors and to request the attendance of individuals from outside the Trust with relevant skills and expertise in order to exercise its functions.
1.4 The RemToS committee is authorised to obtain such internal information it needs to fulfil its functions. All members of staff are directed to cooperate with any such request made by the RemToS committee.
1.5 When appointing the chief executive, the committee shall be the committee described in Schedule 7, 17(3) of the NHS Act (2006) (the Act). When appointing other executive directors the committee shall be the committee described in Schedule 7,17(4) of the Act.
2.0 Supporting Principles
2.1 Where Executive Directors or Senior Managers are involved in advising the Remuneration & Terms of Service Committee, care must be taken to avoid conflict of interests.
2.2 The Remuneration & Terms of Service Committee will work with the Board of Governors (Nominations Committee) in evaluating the skills, knowledge and experience of the whole Board and regularly review the structure, size and composition of the whole Board. At least annually a joint meeting will be held between the Remuneration and Terms of Service Committee and the Nominations Committee.
2.3 In all its work the RemToS committee will adhere to relevant laws, regulations and Trust policies, and will take into account best practice.
3.0 Appointments role
3.1 The RemToS committee will regularly review the structure, size and composition (skills, knowledge, experience and diversity) of the board, acting on the output of the board evaluation process as appropriate and making recommendations to the board of directors or board of governors, as applicable, as to any changes.
3.2 The RemToS committee will consider and make plans for succession planning for the chief executive and other executive directors, taking into account the challenges and
Date: 22nd
January 2015
Nv Item: 15.07xii Appendix 3iii
Terms of Reference 14Mar08: Reviewed 7Sept09, Reviewed 27Jan2011. Reviewed 03Dec2012, Reviewed 16Dec2013, Reviewed 01Dec2014, Reviewed 22Jan2015 Page 2 of 4
opportunities facing the organisation and the balance of skills and expertise needed on the board for the future.
3.3 The RemToS committee will keep the leadership needs of the Trust under review at executive level to ensure the continued ability of the Trust to operate effectively in the health and social care economy.
3.4 The RemToS committee is responsible for identifying and appointing candidates to fill posts within its remit.
3.5 When a vacancy arises, the RemToS committee will evaluated the requirements of the board and prepare or update a job description and person specification setting out the requirements for the appointment.
3.6 The RemToS committee may use recruitment consultants to facilitate the search for suitable candidates but will always advertise the vacancy publicly.
3.7 Throughout the recruitment process candidates will be considered on their merits against objective criteria derived from the needs of the Trust.
3.8 Should an executive director candidate have significant commitments, these will be disclosed to the RemToS committee before appointment, and any changes will be reported to the board of directors as they arise.
3.9 Should an executive director candidate have any past, current or known future business interests that may give rise to a conflict of interest (or a perception of a conflict of interest) then these will be disclosed to the RemToS committee before an appointment is made. Any changes to interests will be reported to the board of directors as they arise.
3.10 In the case of any matter related to an executive director being suspended, or having their service terminated, then the RemToS committee will consider this matter, subject to any legal provision and the individual’s employment contract.
4.0 Remuneration role
4.1 The RemToS committee will establish a remuneration policy in respect of executive directors, and any senior managers on locally determined pay below board level, and keep this under review. As part of this policy the committee will consult with the chief executive over proposals related to the remuneration of other executive directors.
4.2 The scope of the remuneration policy will include:
• Salary, including performance related pay or bonus payments if applicable,
• Provision for other benefits including pensions and cars,
• Allowances
• Payable expenses
• Compensation payments
4.3 An underlying principle of this policy will be to establish sufficient levels of remuneration so as to attract and motivate executive directors of the required quality to lead the Trust, without paying more than is necessary for this purpose, and at a level affordable for the organisation. In doing so, the RemToS committee will draw on national guidance and market benchmarking analysis in any determination of executive director pay (and any senior managers on locally determined pay). The RemToS committee will ensure that no director or senior manager on locally determined pay
Terms of Reference 14Mar08: Reviewed 7Sept09, Reviewed 27Jan2011. Reviewed 03Dec2012, Reviewed 16Dec2013, Reviewed 01Dec2014, Reviewed 22Jan2015 Page 3 of 4
receives an increase in remuneration where the Trust or the individuals’ performance does not justify such an increase. The RemToS committee will take into account and be sensitive to the pay and conditions of staff in the wider Trust in setting the remuneration policy and in making specific decisions based upon it.
4.4 The RemToS committee will monitor and assess the performance appraisal of individual executive directors and consider this information when reviewing changes to remuneration packages.
4.5 The RemToS committee will oversee contractual arrangements for executive directors (including termination payments) so as to avoid rewarding poor performance.
5.0 Membership and Quoracy
5.1 The RemToS committee shall consist of the Chair of the Board of Directors and all Non-Executive Directors. The Trust Chair will chair the committee.
5.2 Four members of the RemToS committee, including the Chair, shall constitute a quorum.
5.3 Only members of the RemToS committee have a right to attend meetings.
5.4 The composition of the Remuneration & Terms of Service Committee shall be recorded in the Annual Report.
6.0 Attendance
6.1 The Chief Executive is invited to all meetings.
6.2 Lead director for HR, or other managers may be asked to attend.
6.3 The RemToS committee may invite representatives of the Nominations Committee to attend meetings.
6.4 Any member of the committee, including the Trust Secretary, will be required to leave the committee when their own remuneration or terms of service are the subject of discussion.
7.0 Secretariat support
7.1 The Trust Secretary, or their nominated deputy, shall be responsible for minuting meetings and providing administrative support to the RemToS committee.
7.2 The Trust Secretary will arrange with HR for the completion of payroll documentation following decisions made by the RemToS committee.
8.0 Reporting
8.1 The Chair will report to the board of directors following each meeting.
8.2 Minutes of the RemToS committee shall normally be reserved to members of the Committee.
8.3 The RemToS committee will ensure that disclosure of executive director remuneration is included in the Trust’s Annual Report in line with reporting requirements.
Terms of Reference 14Mar08: Reviewed 7Sept09, Reviewed 27Jan2011. Reviewed 03Dec2012, Reviewed 16Dec2013, Reviewed 01Dec2014, Reviewed 22Jan2015 Page 4 of 4
9.0 Frequency of meeting
9.1 The RemToS committee will meet at least two times a year. Meetings may be called as required.
10 Review
10.1 These Terms of Reference shall be reviewed annually, unless otherwise required.
10.2 The performance of the RemToS committee will be reviewed as part of the annual board performance review process, taking into account these Terms of Reference.
Robert Nesbitt
17.11.14
Approved by BoD on 18.12.14
Membership amended for BoD approval 22.01.15
OD & Workforce Committee Terms of Reference Final April 2014 Page 1 of 3
ORGANISATIONAL DEVELOPMENT AND WORKFORCE COMMITTEE Terms of Reference – April 2014
1.0 Constitution
The Board of Directors hereby resolves to establish a Committee of the Board to be known as the OD and Workforce Committee (The Committee). The Committee is a non-executive committee of the Board of Directors and has no executive powers, other than those specifically delegated to it in these Terms of Reference.
The Trust Secretary shall provide administrative support to the Committee and will include the following duties:
� Agreement of agenda with the Chair and attendees and collation of papers;
� Taking the minutes and keeping a record of matters arising and issues to be carried forward; and
� Advising the Committee on pertinent areas.
2.0 Role of the OD and Workforce Committee
The Board of Directors has responsibility for ensuring the effective management of all of the Trust’s affairs, including management and development of the Trust’s workforce.
The OD and Workforce Committee is specifically charged with undertaking the following roles:
� To approve, monitor and review the Trusts 5 year OD and Workforce strategy
� To monitor the development of the Workforce implications of service redesign.
� To provide an oversight of all employee related matters including but not limited to:
� Workforce remuneration and terms and conditions
� Employee / Staff side consultation
� Bids and Tenders - a periodic review of workforce impacts
� Staff engagement and its impact across the Trust
Date: 22nd January 2015
Nvi Item: 15.07xii Appendix 3iv
OD & Workforce Committee Terms of Reference Final April 2014 Page 2 of 3
� To sponsor and support employee wellbeing including monitoring the staff survey action plan.
� To monitor employee development and training including:
� Statutory and mandatory requirements
� Performance management and appraisals
� To monitor all employee related risks
3.0 Membership
The Committee shall be appointed by the Board of Directors from amongst the Directors and comprise:
� Non-Executive Director Chair
� One other Non-Executive Director
� Both Associate Directors of Operations
� Director of Workforce & OD
� Director of Nursing
� Deputy Medical Director
The Non-Executive Directors will normally be designated but can, from time-to-time be substituted by any other Non-Executive Director as agreed with the Chair.
A quorum shall be four members: One Non-Executive Director and three Executive Directors (one to be the Director of Workforce & OD or nominated deputy)
4.0 Attendance
The Committee may require the attendance of the Chief Executive, other Executive Directors or other Trust staff as appropriate.
The Trust Secretary, or whoever covers these duties, shall be Secretary to the Committee and shall attend to take minutes of the meeting and provide appropriate support and advice to the Chairman and committee members.
5.0 Authority
The Committee is authorised by the Board of Directors to scrutinise any activity within its Terms of Reference. It is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised by the Board of Directors to obtain outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary.
OD & Workforce Committee Terms of Reference Final April 2014 Page 3 of 3
6.0 Frequency of meetings and reporting to Board of Directors
The Committee will meet at least six times per annum.
The Chair will prepare a written report summarising the key areas of discussion / outcomes for the next Board of Directors’ meeting. Minutes of the Committee will also be available to all members of the Board of Directors.
7.0 Agenda
The agenda will be set by the Chair in conjunction with the Director of Workforce & OD and circulated seven days prior to the meeting. Items for inclusion must be informed to the Trust Secretary at least fourteen days before the circulation of the agenda. This is in accordance with Trust standards.
8.0 Minutes
The minutes will be prepared by the Meetings Secretary and distributed no later than ten working days after the meeting, and ratified at the following meeting, in accordance with Trust standards
9.0 Other Functions
The Committee may undertake additional work as delegated from time-to-time by the Board of Directors. This will require formal variation to the Terms of Reference at a Board of Directors’ meeting.
10.0 Review of Terms of Reference
These terms of reference are to be reviewed on an annual basis. Date of last review: July 2012
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 1 of 13 Date produced: 03Jan2014 Retention period: 30 years
Audit & Risk Committee
Terms of Reference – May 2014
Note: The relevant sections of the Monitor Code of Governance are included in brackets and at the end of this document for ease of reference
The NHS LA Monitoring Statement is enclosed at the end of this document for ease of reference
1. Constitution
1.1 The Board of Directors hereby resolves to establish a Committee of the Board of Directors to be known as the Audit and Risk Committee (“the Committee”) (F3).
1.2 The Committee is a non-executive committee of the Board of Directors and has no executive powers, other than those specifically delegated to it in these Terms of Reference.
1.3 The Committee shall be supported administratively by the Trust Secretary, or their nominee, whose duties in this respect will include:
1.3.1 Agreement of agenda with Chair and attendees and collation of papers;
1.3.2 Taking the minutes and keeping a record of matters arising and issues to be carried forward;
1.3.3 Following-up outstanding items;
1.3.4 Advising the Committee on pertinent areas; and
1.3.5 Assisting the Chair with relevant reports (for example – Annual Report)
2. Role of the Audit and Risk Committee
2.1 The Board of Directors has responsibility for ensuring the effective internal control of all of the Trust’s affairs, including management of the Trust’s activities in accordance with laws and regulations, the establishment and maintenance of the system of internal control designed to ensure that assets are safeguarded, waste or inefficiency avoided and reliable financial information produced, and that “value for money” is continuously sought.
2.2 The Committee will provide the Board of Directors and Board of Governors with the means of independent and objective review, and assurance (F3.3). Its main roles and responsibilities being:
Date: 22nd January 2015
Nvii Item: 15.07xii Appendix 3v
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 2 of 13 Date produced: 03Jan2014 Retention period: 30 years
2.2.1 to ensure the Trust has effective systems of internal control and risk management, including clinical risk management;
2.2.2 to provide the Board of Directors with assurance on governance arrangements across the Trust;
2.2.3 to ensure the Board Assurance Framework is properly established and monitored;
2.2.4 to advise on, and approve, the Annual Governance Statements;
2.2.5 to review and monitor Financial Control systems and financial information used by the Trust, including returns to Regulators;
2.2.6 to review and monitor Quality Control systems and clinical information used by the Trust, including returns to Regulators;
2.2.7 to ensure the Annual Accounts are produced in accordance with all relevant legislative and accounting requirements and that sufficient review has been undertaken by management;
2.2.8 to ensure the Quality Account is produced in accordance with all relevant legislative and accounting requirements and that sufficient review has been undertaken by management;
2.2.9 to ensure both Internal, and External Audit deliver their planned activity, and to review the appropriateness of the planned activity. To ensure recommendations arising from such work are acted on by management. To monitor the joint work of Clinical and Internal Audit; and
2.2.10 to provide an Annual Report of the Committee’s work to the Board of Directors (see Section 17).
3. Membership (F3.1)
3.1 Members of the Committee shall be appointed by the Board of Directors, on the recommendation of the Nominations Committee in consultation with the Chair of the Committee. The Committee shall be made up of at least three members. The members will attend at least 50% of meetings during a 12-month period.
3.2 All members of the Committee shall be independent Non-Executive Directors at least one of whom shall have recent and relevant financial experience. The Chair of the Board of Directors shall not be a member of the Committee.
3.3 Only members of the Committee have the right to attend Committee meetings. However, other individuals such as the Chair, the Chief Executive, the Director of Finance, other Directors, the heads of risk and internal audit and representatives from the finance function will be invited to attend all or part of any meeting, as and when appropriate.
3.4 The External Auditors will be invited to attend meetings of the Committee on a regular basis.
3.5 Appointments to the Committee shall be for a period of up to three years, which may be extended for two further three-year periods provided the Non-Executive Director remains independent.
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 3 of 13 Date produced: 03Jan2014 Retention period: 30 years
3.6 The membership of the Committee should be refreshed to ensure that undue reliance is not placed on particular individuals. (A3)
3.7 The Board of Directors shall appoint the Committee Chair who shall be an independent Non-Executive Director. In the absence of the Committee Chair the remaining members present shall elect one of themselves to chair the meeting.
3.8 Governors are formally invited to attend the meeting at which the review of the external auditors is considered. Governors are welcome to attend as observers by prior arrangement with the Chair of the committee and the Board of Governors may wish to nominate a governor (ideally a member of the governors’ Planning and Performance Subgroup) to attend regularly in order to provide continuity of feedback to the Board of Governors.
4. Quorum
4.1 The necessary quorum for the transaction of business shall be two members. A duly convened meeting of the Committee at which a quorum is present shall be competent to exercise all or any of the authorities, powers and discretions vested in or exercisable by the Committee.
5. Attendance
5.1 At least once a year the Committee should meet privately with the External and Internal Auditors (separate meetings). (See paragraph 3.3 and 3.4)
5.2 The Chief Executive and other Executive Directors should be invited to attend meetings, particularly when the Committee is discussing areas of risk or operation that are the responsibility of that director.
5.3 The Chief Executive should be invited to attend meetings at least annually, to discuss with the Committee the process for assurance that supports the Annual Governance Statements.
6. Authority
6.1 The Committee is authorised by the Board of Directors to scrutinise any activity within its terms of reference.
6.2 The Committee is authorised to seek any information it requires from any employee and all employees are directed to co-operate with any request made by the Committee.
6.3 The Committee is authorised by the Board of Directors to obtain outside legal or other independent professional advice and to secure the attendance of people with relevant experience and expertise if it considers this necessary.
7. Frequency of meetings
7.1 The Committee will meet bi-monthly. The Chair’s report will be presented at the next full meeting of the Board of Directors highlighting matters requiring the attention of the full Board of Directors. Additional meetings for specific tasks may be arranged with due notice (see paragraph 8).
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 4 of 13 Date produced: 03Jan2014 Retention period: 30 years
8 Notice of Meetings
8.1 Meetings of the Committee shall be summoned by the Secretary of the Committee at the request of any of its members or at the request of the External or Internal Auditors, if they consider it necessary.
8.2 Unless otherwise agreed, notice of each meeting confirming the venue, time and date together with an agenda of items to be discussed, shall be forwarded to each member of the Committee, any other persons required to attend and all Non-Executive Directors, no later that five working days before the date of the meeting. Supporting papers shall be sent to the Committee members and to other attendees as appropriate, at the same time.
9. Minutes of Meetings
9.1 The Trust Secretary, or their nominee, shall minute the proceedings and resolutions of all meetings of the Committee, including recording the names of those present and in attendance.
9.2 The Trust Secretary, or their nominee, shall ascertain, at the beginning of each meeting, the existence of any conflicts of interest and minute them accordingly.
9.3 Minutes of the Committee’s meetings shall be circulated according to the Trust’s Standards for Meetings to all members of the Committee and, a report to all members of the Board of Directors.
10. Reporting Responsibilities
10.1 The Committee Chair shall report formally to the Board of Directors on its proceedings after each meeting on all matters within its duties and responsibilities.
10.2 The Committee shall make whatever recommendations to the Board of Directors it deems appropriate on any area within its remit where action or improvement is needed.
10.3 The Committee shall hold one meeting per year which the governors will be invited to attend
10.4 The Committee shall report on its activities in the Trust’s Annual Report.
11. Duties of the Committee
11.1 Governance, Risk Management and Internal Control
11.1.1 The Committee shall monitor the integrity of the establishment and maintenance of an effective system of integrated governance, risk management and internal control, across the whole of the organisation’s activities (both clinical and non-clinical), which supports the achievement of the organisation’s objectives (F3.2).
11.1.2 In particular, the Committee will review the adequacy of:
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 5 of 13 Date produced: 03Jan2014 Retention period: 30 years
� all risk and control-related disclosure statements (in particular the Annual Governance Statements), together with any accompanying Head of Internal Audit opinion, External Audit opinion or other appropriate independent assurances, prior to endorsement by the Board of Directors;
� the underlying assurance processes that indicate the degree of the achievement of corporate objectives, the effectiveness of the management of principal risks and the appropriateness of the above disclosure statements;
� the policies for ensuring compliance with relevant regulatory, legal and code of conduct requirements;
� the structures, processes and responsibilities for identifying and managing key risks facing the organization, including the Board Assurance Framework;
� the operational effectiveness of policies and procedures;
� monitor and review the Risk Register; and
� review and approve the statements to be included in the Annual Report concerning internal controls and risk management
11.1.3 In carrying out this work the Committee will primarily utilise the work of Internal Audit, External Audit and other assurance functions, , but will not be limited to these audit functions. It will also seek reports and assurances from Directors and managers as appropriate, concentrating on the over-arching systems of integrated governance, risk management and internal control, together with indicators of their effectiveness.
11.1.4 This will be evidenced through the Committee’s use of an effective Assurance Framework to guide its work and that of the audit and assurance functions that report to it.
11.2 Management
11.2.1 The Committee shall request and review reports and positive assurances from Directors and managers on the overall arrangements for governance, risk management and internal control.
11.2.2 The Committee may also request specific reports from individual functions within the organisation (e.g. clinical audit), as they may be appropriate to the overall arrangements.
12 Financial Reporting
12.1 The Committee shall review the Annual Report and Financial Statements before submission to the Board of Directors, focusing particularly on:
12.1.1 the wording in the Annual Governance Statement and other disclosures relevant to the Terms of Reference of the Committee;
12.1.2 changes in, and compliance with, accounting policies and practices;
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 6 of 13 Date produced: 03Jan2014 Retention period: 30 years
12.1.3 unadjusted mis-statements in the financial statements;
12.1.4 major judgemental areas; and
12.1.5 significant adjustments resulting from external audits.
12.2 The Committee should also ensure that the systems for financial reporting to the Board of Directors, including those of budgetary control, are subject to review as to completeness and accuracy of the information provided to the Board of Directors.
12.3 The Committee should also ensure that the systems for reporting on the Quality Account to the Board of Directors are subject to review as to completeness and accuracy of the information provided to the Board of Directors.
14. Internal Audit
14.1 The Committee shall ensure that there is an effective Internal Audit function, established by management, which meets mandatory NHS Internal Audit Standards and provides appropriate independent assurance to the Audit and Risk Committee, Chief Executive and Board. This will be achieved by:
14.1.1 consideration of the provision of the Internal Audit service, the cost of the audit and any questions of resignation and dismissal;
14.1.2 review and approval of the Internal Audit strategy, operational plan and more detailed programme of work, ensuring that this is consistent with the audit needs of the organisation as identified in the Board Assurance Framework
14.1.3 review and monitor management’s responsiveness to the findings and recommendations of the Internal Auditor;
14.1.4 ensuring that the Internal Audit function is adequately resourced and has appropriate standing within the organisation;
14.1.5 annual review of the effectiveness of Internal Audit;
14.1.6 reviewing the annual report of the Head of Internal Audit and reporting relevant matters to the Board of Directors;
14.1.7 to receive from the Director of Finance (annually) an appraisal on the performance of Internal Audit; and
14.1.8 reviewing promptly all reports prepared by Internal Audit.
15. External Audit
15.1 The Committee should make recommendations to the Board of Governors in relation to the appointment, re-appointment and removal of the external auditor and approve the remuneration and terms of engagement of the external auditor (F3.2, F3.4, F3.5, F3.6)
15.2 The Committee shall develop and implement a policy on the engagement of the external auditor for audit and non-audit services (F3.2, F3.4, F3.6)
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 7 of 13 Date produced: 03Jan2014 Retention period: 30 years
15.3 The Committee shall review the work and findings of the External Auditor appointed by the Board of Governors and consider the implications and management’s responses to their work. This will be achieved by:
15.3.1 discussion and agreement with the External Auditor, before an audit commences, of the nature and scope of the audit as set out in the Annual Plan, and ensure co-ordination, as appropriate, with other External Auditors in the local health economy;
15.3.2 discussion with the External Auditors of their local evaluation of audit risks and assessment of the Trust and associated impact on the audit fee;
15.3.3 review all External Audit reports, including agreement of the Annual Audit Letter before submission to the Board of Directors and any work carried outside the annual audit plan, together with the appropriateness of management responses;
15.3.4 to assess the extent of the reliance placed on Internal Audit by External Audit;
15.3.5 to discuss problems and reservations arising from the External Auditor’s work and any matters that the External Auditor may wish to discuss in order to brief the Board of Directors; and
15.3.6 to consider the content of any report involving the Trust issued by the Public Accounts Committee or Comptroller and Auditor General and reviewing management’s proposed response before presentation to the Board of Directors.
16. Public Disclosure / Whistleblowing (F3.9)
16.1 The Committee shall ensure that the Trust’s arrangements for its employees to raise concerns, in confidence, about possible improprieties in matters of financial reporting and control, clinical quality, patient safety or other matters are overseen by the Service Governance Committee.
16.2 The Committee shall ensure that these arrangements allow proportionate and independent investigation of such matters and appropriate follow-up action.
17. Other Assurance Functions
17.1 The Committee shall review the findings of other significant assurance functions, both internal and external to the organisation, and consider the implications to the governance of the organisation. These will include, but will not be limited to, and any reviews by Department of Health Arms Length Bodies or Regulators / Inspectors (e.g., NHS Litigation Authority etc).
17.2 The Committee will review the work of other board committees within the organisation, whose work can provide relevant assurance to the Committee’s own scope of work. This will particularly include the Service Governance Committee. Minutes from these meetings may form part of the agenda for the Committee.
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 8 of 13 Date produced: 03Jan2014 Retention period: 30 years
17.3 The Committee will ensure that the Trust has policies and procedures for all work relating to Fraud and Corruption as set out in the Secretary of State’s Directions and as required by the NHS Protect.
17.4 The Committee will receive relevant reports from the Trust’s Local Counter Fraud Specialist, including their Annual Report.
17.5 The Committee will review any proposed changes to Standing Orders and Standing Financial Instructions, and examining circumstances associated with each occasion when Standing Orders are waived.
17.6 The Committee will review schedules of losses and compensations.
17.7 The Committee will review the Register of Hospitality at least annually.
17.8 The Committee will annually review its own performance, constitution and terms of reference to ensure it is operating at maximum effectiveness and recommend any changes it considers to the Board of Directors for approval.
18.0 Annual Report of the Committee
18.1 The Committee is required to provide an annual report, which will include (F3.3, F3.5, F3.8):
18.1.1 a specific statement confirming that the draft Annual Governance Statements are consistent with the view of the Committee on the organisation’s system of internal control and that it supports the Board of Director’s approval of the statement, subject to any reasonable limitations that the Committee may draw attention to;
18.1.2 that the system of risk management in the organisation is adequate in identifying risks and allowing the Board of Directors to understand the appropriate management of those risks;
18.1.3 that the Committee has reviewed and used the Board Assurance Framework and believes that it is fit for purpose;
18.1.4 that there are no areas of significant duplication or omission in the systems of governance in the organisation that have come to the Committee’s attention and not been adequately resolved; and
18.1.5
18.2 In addition, the report should highlight to the Board of Directors the main areas that the Committee has reviewed and any particular concerns or issues that it has addressed. These should include:
18.2.1 the financial position and financial reporting systems of the organisation;
18.2.2 any major breakdown in internal control that has led to a significant loss in one form or another; and
18.2.3 any major weakness in the governance systems that has exposed, or continues to expose, the organisation to an unacceptable risk.
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 9 of 13 Date produced: 03Jan2014 Retention period: 30 years
19. Annual General Meeting of the Trust
19.1 The Chair of the Committee, or his / her representative, shall attend the Annual General Meeting and be prepared to respond to any Stakeholder’s questions on the Committee’s activities.
20. Other Matters
20.1 The Committee shall:
20.1.1 have access to sufficient resources in order to carry out its duties, including access to the Trust secretariat for assistance as required;
20.1.2 be provided with appropriate and timely training, both in the form of an induction programme for new members and on an ongoing basis for all members;
20.1.3 give due consideration to the laws and regulations, the provisions of the Combined Code and the regulator, Monitor;
20.1.4 review arrangements for the co-ordination of the Internal and External Auditors;
20.1.5 oversee any investigation of activities which are within its terms of reference and act as a court of last resort.
21. Review of the Terms of Reference
21.1 Unless otherwise required, these Terms of Reference will be reviewed every two years.
Robert Nesbitt Trust Secretary 03
th February 2014
Version Control Amended to take account of creation of Service Governance Committee February 2014 Amended to remove “sub” from Service Governance Committee May 2014 BoD Approved: May 2014, Aug 2013, Oct 2011, Aug2010, Aug2009, Apr2008, Oct2006, Aug2006, Jun2006, Nov2004, Oct2003, Jul2002, Jul2001, Apr2000, Jan1998 Original: September 1994
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 10 of 13 Date produced: 03Jan2014 Retention period: 30 years
Monitor: The NHS Foundation Trust Code of Governance (March 2013)
Section B: Effectiveness The board of directors and its committees should have the appropriate balance of skills, experience, independence and knowledge of the NHS foundation trust to enable them to discharge their respective duties and responsibilities effectively. B.1.e The value of ensuring that committee membership is refreshed and that undue reliance is not placed on particular individuals should be taken into account in deciding chairpersonship and the membership of committees.
C.3 Audit committee and auditors Main principle C.3.a The board of directors should establish formal and transparent arrangements for considering how they should apply the corporate reporting and risk management and internal control principles and for maintaining an appropriate relationship with the NHS foundation trust’s auditors. Monitor’s publications, Audit Code for NHS Foundation Trusts and Your statutory duties: A reference guide for NHS foundation trust governors, provide further guidance. Code provision C.3.1. The board of directors should establish an audit committee composed of at least three members who are all independent non-executive directors. The board should satisfy itself that the membership of the audit committee has sufficient skills to discharge its responsibilities effectively, including ensuring that at least one member of the audit committee has recent and relevant financial experience. The chairperson of the trust should not chair or be a member of the audit committee. He can, however, attend meetings by invitation as appropriate. C.3.2. The main role and responsibilities of the audit committee should be set out in publicly available, written terms of reference. The council of governors should be consulted on the terms of reference, which should be reviewed and refreshed regularly. It should include details of how it will:
• Monitor the integrity of the financial statements of the NHS foundation trust, and any formal announcements relating to the trust’s financial performance, reviewing significant financial reporting judgements contained in them;
• Review the NHS foundation trust’s internal financial controls and, unless expressly addressed by a separate board risk committee composed of independent directors, or by the board itself, review the trust’s internal control
and risk management systems; • Monitor and review the effectiveness of the NHS foundation trust's internal audit function, taking into consideration relevant UK professional and
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 11 of 13 Date produced: 03Jan2014 Retention period: 30 years
regulatory requirements;
• Review and monitor the external auditor’s independence and objectivity and the effectiveness of the audit process, taking into consideration relevant UK professional and regulatory requirements;
• Develop and implement policy on the engagement of the external auditor to supply non-audit services, taking into account relevant ethical guidance regarding the provision of non-audit services by the external audit firm; and
• Report to the council of governors, identifying any matters in respect of which it considers that action or improvement is needed and making recommendations as to the steps to be taken. C.3.3. The council of governors should take the lead in agreeing with the audit committee the criteria for appointing, re-appointing and removing external auditors. The council of governors will need to work hard to ensure they have the skills and knowledge to choose the right external auditor and monitor their performance. However, they should be supported in this task by the audit committee, which provides information to the governors on the external auditor’s performance as well as overseeing the NHS foundation trust’s internal financial reporting and internal auditing. C.3.4. The audit committee should make a report to the council of governors in relation to the performance of the external auditor, including details such as the quality and value of the work and the timeliness of reporting and fees, to enable to council of governors to consider whether or not to re-appoint them. The audit committee should also make recommendation to the council of governors about the appointment, re-appointment and removal of the external auditor and approve the remuneration and terms of engagement of the external auditor. C.3.5 If the council of governors does not accept the audit committee’s recommendation, the board of directors should include in the annual report a statement from the audit committee explaining the recommendation and should set out reasons why the council of governors has taken a different position. C.3.6. The NHS foundation trust should appoint an external auditor for a period of time which allows the auditor to develop a strong understanding of the finances, operations and forward plans of the NHS foundation trust. The current best practice is for a three- to five-year period of appointment. C.3.7. When the council of governors ends an external auditor’s appointment in disputed circumstances, the chairperson should write to Monitor informing it of the reasons behind the decision. C.3.8. The audit committee should review arrangements that allow staff of the NHS foundation trust and other individuals where relevant, to raise, in confidence, concerns about possible improprieties in matters of financial reporting and control, clinical quality, patient safety or other matters. The audit committee’s objective should be to ensure that arrangements are in place for the proportionate and independent investigation of such matters and for appropriate follow-up action. This should include ensuring safeguards for those who raise concerns are in place and operating effectively. Such processes should enable individuals or groups to draw formal attention to practices that are unethical or violate internal or external policies, rules or regulations and to ensure that valid concerns are promptly addressed. These processes should also reassure individuals raising concerns that they will be protected from potential negative repercussions. C.3.9. A separate section of the annual report should describe the work of the
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 12 of 13 Date produced: 03Jan2014 Retention period: 30 years
committee in discharging its responsibilities. The report should include:
• the significant issues that the committee considered in relation to financial statements, operations and compliance, and how these issues were addressed;
• an explanation of how it has assessed the effectiveness of the external audit process and the approach taken to the appointment or re-appointment of the external auditor, the value of external audit services and information on the length of tenure of the current audit firm and when a tender was last conducted; and
• if the external auditor provides non-audit services, the value of the non-audit services provided and an explanation of how auditor objectivity and
independence are safeguarded. Monitoring Compliance with this Terms of Reference
Process for Reporting Arrangements to the Audit and Risk Committee (A & RC)
A & R Committee
Board of Directors
A & R C Chair’s Report after each meeting
Reports:
° Governance, Risk Management and Internal Control
° Internal Audit
° External Audit
° Other Assurance Functions
° Management
° Ad Hoc reports as stated in the A&RC Work Plan
(Frequency: As specified in the A & R C Work Plan)
Audit and Risk Ctte May2014
ToR
Version 1.1
Editor: Robert Nesbitt
Department: Corporate
Page 13 of 13
Date produced: 03Jan2014
Retention period: 30 years
Aspects of the
TOR to be
monitored
Monitoring M
ethod
Individual / team
responsible for
the m
onitoring
Frequency
Findings: Group /
committee that will receive
the findings / monitoring
report
Action: Group / committee responsible for
ensuring actions are in place
Reporting
arrangements to
the Board
Audit of 25% of Board
minutes (over 12 month
period) to evidence the
Audit and Risks Chairs
report to BoD highlighting
matters requiring attention
from the BoD
Assurance
Manager
Annual
Assurance Managers
annual report of High Level
Risk Committee
Governance to the Audit
and Risk Committee
Audit and Risk Committee
Reporting
arrangements to
the high level
committee
Audit of Audit and Risk
Committee minutes for the
past 12 month period to
show evidence reporting to
the Committee as shown
in the process and detailed
in the A&RC Work Plan
Assurance
Manager
Annual
Assurance Managers
annual report of High Level
Risk Committee
Governance to the Audit
and Risk Committee
Audit and Risk Committee
Board of Directors – Public 23Oct2014 SGC Terms of Reference
Version Author: Peter Jefferys Department: Corporate
Page 1 of 6 Date produced: 12Oct2014 Retention period: 30 years
Service Governance Committee Terms of Reference
1. Purpose of the Committee
The main role of the Committee is to provide assurance to the Board of Directors on the delivery of the Trust’s Quality Strategy. Its focus will therefore be on the quality and effectiveness of care provided to service users and carers by NSFT services. Development of the Trust’s strategy for service and clinical quality is a core objective. The latter requires promotion of an organisational culture that enables high quality and compassionate care, using the Trust’s Vision and Values to guide behaviour and decision making. To achieve this the Committee will enable and monitor the contribution of senior clinical staff from all professions to quality strategy development and monitoring of standards.
• Progress against other quality targets e.g. CQUINS
• Performance against CQC’s essential standards of quality b. Risk identification & mitigation
• Identify risks related to service and clinical quality and seek assurance that principal risks threatening quality are being reported and managed appropriately at all levels within the Trust
• Examine failures in service quality and ensure action plans are devised and implemented which address learning and development issues with a positive impact on quality of patient care
• Monitor progress against action plans with appropriate outcome audit
• Seek assurance that major service transformation (operational or strategic) & significant QIPP and CIP programmes will not have a detrimental impact on service quality for patients
c. Governance assurance – overall
• Ensure resources to deliver quality improvement & governance are effectively deployed and monitored via functions such as:
o Clinical audit o Clinical effectiveness
Date: 22nd January 2015
Nviii Item: 15.07xii Appendix 3vi
Board of Directors – Public 23Oct2014 SGC Terms of Reference
Version Author: Peter Jefferys Department: Corporate
Page 2 of 6 Date produced: 12Oct2014 Retention period: 30 years
o Patient safety o Complaints function o Safeguarding o Use of relevant Risk Management data (e.g. Datix)
• Ensure there are processes in place to monitor quality effectively
• Approve Trust policies relating to all aspects of quality d. Governance assurance – locality & specialist services
• Critical review of reports / minutes from established locality / specialist services governance groups to provide assurance that they robustly address Trust’s quality strategy.
• To identify priorities for locality / specialist services quality initiatives / governance tasks & learning events consistent with Trust’s quality strategy.
• Review assurance and actions by Trust groups which report to Committee, e.g. Infection Control Subcommittee, Physical Health Committee, Mental Health Law Forum, Equality & Diversity etc.
e. Response to external organisations
• To receive and consider impact of national policy & strategy on safety, effectiveness & patient experience within the Trust
• To receive reports from external organizations & ensure appropriate response & monitoring / review, including:
o Commissioners (CCG’s & NHS England) o Monitor / CQC o Healthwatch o Health & Scrutiny Committees o HM Coroner o NHSLA
f. Service Users, Carers & Youth
• To ensure that effective channels exist for quality concerns to be raised by Service Users / Carers / Youth Council
3. Accountability & Reporting Procedures
The Service Governance Committee is a committee of, and accountable to, the Board of Directors.
The Service Governance Committee Chair will formally report in writing to the Board and to the Audit and Risk Committee after each meeting; urgent issues will be reported verbally by the Chair if necessary. The Chair and Director of Nursing will consider whether any risks need adding to the BAF after each meeting, and action accordingly.
The Committee will prepare and submit a summary Annual Report of its activities to the Board of Directors and Audit & Risk Committee.
At least once a year the Committee will review its own performance and terms of reference to ensure that it is operating at maximum effectiveness and recommend any changes it considers necessary to the Board of Directors for approval.
Board of Directors – Public 23Oct2014 SGC Terms of Reference
Version Author: Peter Jefferys Department: Corporate
Page 3 of 6 Date produced: 12Oct2014 Retention period: 30 years
The Committee is authorised to seek any information it requires from any employee, and all employees are directed to co-operate with any request made by the Committee. The Committee is authorised to obtain outside legal advice or other professional advice and to secure the attendance of outsiders with relevant experience if it considers this necessary to support its deliberations.
5. Membership
A Non-Executive Director, preferably with a clinical or practitioner background, will chair the Committee.
The membership of the Committee shall be:
� Non-Executive Director (Chair) � Non-Executive Director (Vice-Chair) � Director of Nursing and Governance – Executive Lead � Medical Director � Lead Clinicians x 7 *
[* Lead Clinician / Modern Matron from 5 localities + NRP + Secure Services]
� Deputy Director of Nursing & Practice Excellence � Head of Governance
Governors may attend as observers with prior notification to the Chair. A Service User representative, carer representative and Youth Council representative may attend as observers. For the avoidance of doubt, governors and service user / carer / youth council representatives may contribute to discussions at meetings but do not take part in formal decisions.
The Committee’s annual work plan will follow three broad themes central to NSFT’s quality strategy. Each will be covered four times each year (monthly meetings), with focused reports and attendance dependent on theme:
• Safe Services (attendance by Head of Pharmacy, Head of Patient Safety, Trust Secretary)
• Caring & Responsive Services (attendance by Service User & Care Engagement Lead, Health of Patient Safety, Head of Service User Experience)
• Effective Services (attendance by Research & Development, Head of Physical Health & Infection Control)
Other Directors, managers & clinicians will be invited to attend to address specific issues as appropriate.
The Board of Directors will review membership of the Committee annually.
7. Quorum
The committee will be quorate when there are a total of two Board Directors present, including one Non-Executive Director.
Board of Directors – Public 23Oct2014 SGC Terms of Reference
Version Author: Peter Jefferys Department: Corporate
Page 4 of 6 Date produced: 12Oct2014 Retention period: 30 years
8. Deputies
Deputies are not normally allowed, except for Formal Deputies in accordance with the Compliance Framework.
9. Meetings
Meetings will be monthly. Additional meetings may be called as appropriate.
10. Agenda
The agenda will be set by the Chair, in consultation with the Director of Nursing and Governance, and circulated seven days prior to the meeting. Items for inclusion must be informed to the Chair at least fourteen days before the circulation of the agenda. This is in accordance with Trust standards
11. Minutes
The minutes will be prepared by the Nursing and Governance Team PA and ratified at the following meeting, in accordance with Trust standards.
12. Review of meeting effectiveness & Terms of Reference
The Chair, Director of Nursing and Secretary will review the effectiveness of the committee after each meeting. The Terms of Reference will be reviewed annually, or more frequently if appropriate, and submitted to the Board of Directors for consideration.
Last Review: Date
Board of Directors – Public 23Oct2014
SGC Terms of Reference
Version
Author: Peter Jefferys
Department: Corporate
Page 5 of 6
Date produced: 12Oct2014
Retention period: 30 years
Annual Workplan
Safe
Caring & Responsive
Effective
Jan
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Serious Incidents
Safeguarding
Prevention and management of
aggression
Medicines management annual report
Safeguarding annual report
Feb
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Service user experience
Complaints
PLACE annual report
Ma
r Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Clinical audit
Physical health
Mental Health Act
Learning Disability strategy annual
report
Apr
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Serious Incidents
Safeguarding
Prevention and management of
aggression
Risk management annual report
May Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Service user experience
Complaints
Complaints annual report
Safe staffing biannual review
Jun Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Clinical audit
Physical health
Mental Health Act
NICE guidelines annual report
Personality Disorder strategy annual
report
Jul
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Serious Incidents
Safeguarding
Prevention and management of
aggression
Serious incident annual report
Ligature annual report
Aug
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Service user experience
Complaints
ANNUAL REVIEW OF SGC
EFFECTIVENESS
Sep
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Clinical audit
Physical health
Mental Health Act
ASD strategy annual report
R&D governance annual report
Board of Directors – Public 23Oct2014
SGC Terms of Reference
Version
Author: Peter Jefferys
Department: Corporate
Page 6 of 6
Date produced: 12Oct2014
Retention period: 30 years
Oct
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Serious Incidents
Safeguarding
Prevention and management of
aggression
Suicide strategy annual report
Nov
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Service user experience
Complaints
Safe staffing annual review
De
c
Quality Dashboard
Regulatory compliance
Risk review
Policy ratification
Clinical audit
Physical health
Mental Health Act
Clinical supervision annual report
Board of Directors - 22/01/15, Impact of S75 changes
Version 0.1
Author: Debbie White Department: Corporate
Page 1 of 3 Date produced: 13/01/15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Impact of S75 changes in Norfolk
Action Sought: For Debate
Estimated time: 10 minutes
Author: Debbie White - Director of Operations Norfolk and Waveney
Director: Debbie White - Director of Operations Norfolk and Waveney
Executive Summary:
The purpose of this report is to update the Trust Board on the impact of the changes to the S75 arrangements in Norfolk which took place on 1st October 2014 when the majority of social workers previously employed by NSFT transferred their employment to Norfolk County Council. At the point of transfer it was agreed that there would be a transition plan to ensure the safe transfer of service users where necessary and appropriate. This transition plan extends until 31st March 2015 and whilst some progress has been made there are still a number of service users who require transition to either a health or social care caseload. There have been a number of technical teething problems, particularly in relation to access to Care First for social workers and use of the Care first webform for referrals but both organisations have worked jointly to successfully overcome these issues. Capacity remains an issue for both organisations due to a high number of vacancies for Assistant Practitioners within NCC and insufficient care co-ordinator capacity within NSFT. Additional investment in the NSFT adult community service line in central Norfolk has been agreed and recruitment is underway for additional care co-ordinators but unfortunately these capacity issues are impacting on the ability to provide social care packages in a timely fashion in some instances.
1.0 Report contents
1.1 Some progress has been made with transferring cases to the appropriate organisation with transfer of all the health only cases being completed by 5th December 2014. There are, however, a number of joint health and social care
Date: 22nd January 2015
O Item: 15.08i
Board of Directors - 22/01/15, Impact of S75 changes
Version 0.1
Author: Debbie White Department: Corporate
Page 2 of 3 Date produced: 13/01/15 Retention period: 30 years
cases which still need to be allocated to the most appropriate professional. In West Norfolk and Gt Yarmouth this work is being jointly managed by NCC Team managers and NSFT service managers.
1.2 In central Norfolk where the numbers are higher a NSFT service manager has been seconded to focus on this work and is reviewing all of the caseloads still open to social workers on IPM. This work is expected to be complete by the end of March 2015 but the ability to allocate cases to a health worker will be dependent on recruitment to the additional 12 B6 care co-ordinator posts in central Norfolk which are currently out to advert. The number of unallocated cases in the central Norfolk adult service line was 283 at the end of December. This number has been compounded by the changes to the s75 arrangements.
1.3 Relationships between NCC and NSFT staff at all levels remain positive with a focus on problem solving and negotiation. A joint operational meeting between NCC and NSFT is planned and this will be the arena to discuss any ongoing areas of concern.
1.4 Social work teams are structured on a locality basis with the exception of CRHT, NRP, Forensic and Youth/EI. The location of social workers in the central Norfolk CRHT has proved problematic and two of the three social workers in that team have been successful in applying for B6 assessor roles within the Trust and will transfer back to the employment of NSFT at the end of January 2015. This will provide an opportunity to review the efficacy of these roles and discussions are underway as to whether social workers would be of more benefit linking to inpatient areas, in particular the new assessment unit, Thurne ward, when this opens in March. A review of progress within NRP is planned for early 2015 with Forensic and Youth/EI scheduled for March 2015.
1.5 A significant amount of work has occurred between the AMHP team manager and NSFT managers to improve interface issues such as the clarity of the AMHP role and appropriate thresholds for Mental Health Act assessments. Some confusion at the beginning of the s75 changes appears to have contributed to a steep rise in the number of out of area placements during October and November but a more recent reduction in these numbers seems to demonstrate that there is now a shared understanding between NCC and NSFT.
1.6 There are a number of areas of ongoing concern such as delays in accessing social care packages and delays in social workers being allocated to present to the residential and nursing care panel. Both of these issues are impacting on timely discharge from inpatient units and have a financial impact on NSFT when people are placed out of area. A meeting between Alison Simpkin, Head of Social Care for NCC, Clive Rennie, Assistant Director Integrated Commissioning Mental Health and Learning Disability and The NSFT Director of Operations has been arranged to discuss these matters and any outstanding issues will be escalated to the next Mental Health Programme Board which is scheduled to meet in February.
1.0 Risks/mitigation in relation to the Trust objectives
The main risks are:
Board of Directors - 22/01/15, Impact of S75 changes
Version 0.1
Author: Debbie White Department: Corporate
Page 3 of 3 Date produced: 13/01/15 Retention period: 30 years
• Inability to recruit to the required 12 B6 posts by the end of March 2015
• Unacceptably high levels of unallocated cases
• Delays in providing social care packages leading to delayed lengths of stay in hospital
• The solution to these risks will be dependent on the successful recruitment of Assistant Practitioners for NCC and additional care co-ordinators for NSFT. NCC will continue to have capacity issues until social workers have been able to transfer all of the predominately health cases back to NSFT as this will impact on their ability to allocate new cases. Whilst it is regrettable that the new arrangements are causing some delays, there is a strong commitment from both organisations to work together to overcome these issues.
3.0 Recommendations
3.1 The Board is asked to note the content of this report.
Debbie White Director of Operations Norfolk and Waveney
Background Papers / Information - none
Board of Directors Meeting -22/01/15, MH Concordat
Version 1.0
Author: Debbie White Department: Corporate
Page 1 of 3 Date produced: 13/01/15 Retention period: 30 years
Report To: Board of Directors – Public
Meeting Date: 22nd January 2015
Title of Report: Update on system-wide action plan for Mental Health Concordat
Action Sought: For Information
Estimated time: 10 minutes
Author: Debbie White – Director of Operations Norfolk and Waveney
Director: Debbie White – Director of Operations Norfolk and Waveney
Executive Summary:
The purpose of this report is to update the Board on progress in relation to the Mental Health Crisis Care Concordat in both counties. The Concordat was launched by the Government in February 2014 and lists a set of core principles and a national action plan agreed by all of the organisations which have signed the Concordat. The crisis care concordat focuses on four core areas:
• Access to support before crisis point – making sure people with mental help problems can get help 24 hours a day and that when they ask for help they are taken seriously
• Urgent and emergency access to crisis care – making sure that a mental health crisis is treated with the same urgency as a physical health emergency
• Quality of treatment and care when in crisis – making sure that people are treated with dignity and respect in a therapeutic environment
• Recovery and staying well – preventing future crisis by making sure people are referred to appropriate services.
Suffolk submitted their declaration on improving outcomes for people experiencing mental health crisis in August 2014 and Norfolk submitted their declaration in July 2014. NSFT were signatories in both counties.
1.0 Report contents
1.1 The Norfolk Mental Health Strategic Board has been meeting since June 2014 to steer the development of the local declaration and action plan and a comprehensive action plan (appendix 1) was submitted to the national project team in December 2014. A stakeholder consultation event was held in July 2014 to identify any gaps and areas for development and these are reflected in the action
Date: 22nd January 2015
P Item: 15.09i
Board of Directors Meeting -22/01/15, MH Concordat
Version 1.0
Author: Debbie White Department: Corporate
Page 2 of 3 Date produced: 13/01/15 Retention period: 30 years
plan. There is also a monthly operational Mental Health and Learning Disability Steering Group which reports to the Strategic Board. NSFT are represented at both of these meetings.
1.2 NSFT is involved in a number of new initiatives to support delivery of the Concordat in Norfolk including:
• The establishment of a dedicated mental health team within the Norfolk Constabulary Contact and Control room.
• Community based admission prevention schemes in partnership with MIND, Stonham Housing and Julian Support.
• Enhanced psychiatric liaison services at the Norfolk and Norwich University Hospital and Queen Elizabeth Hospital.
Full staffing of the s136 suites at Hellesdon Hospital and the Fermoy unit.
All of the above initiatives will be fully evaluated but early feedback demonstrates reductions in the number of detentions under s136, reductions in the number of repeat calls to the Contact and Control room, reduction in front line attendances by police officers to calls from people with mental ill health and a reduction in the number of critical incidents involving those with mental ill health. Another noticeable benefit is enhanced working relationships between NSFT, Norfolk Constabulary and other partner organisations.
1.3 Suffolk have held two workshops with a range of stakeholders and have produced a draft action plan (appendix 2) which will be reviewed at the Health and Wellbeing Board on 19th January prior to being submitted to the national project team. Further work is required to amalgamate the work underway in the Suffolk East and West CCG areas with Waveney.
Notable initiatives in Suffolk include:
• The police triage car pilot where NSFT clinicians accompany police in patrol cars to assist in the identification of people with mental health issues and support diversion away from detention under s136. The scheme has been evaluated and has resulted in a reduction of Sec 136 detentions.
• Significant development of psychiatric liaison services at both Ipswich and West Suffolk Hospitals
• Increasing the provision of alternative to admission services.
1.4 The developments in both counties compare favourably to other parts of the country and there is a strong commitment from all organisations locally to work together to improve the experiences of people in crisis because of a mental health condition.
2.0 Risks/mitigation in relation to the Trust objectives
2.1 A number of the service developments outlined in the Crisis Care Concordat action plans are funded on a fixed term basis and in some cases are part of CQUIN
Board of Directors Meeting -22/01/15, MH Concordat
Version 1.0
Author: Debbie White Department: Corporate
Page 3 of 3 Date produced: 13/01/15 Retention period: 30 years
funding. If the evaluation process demonstrates that there are system wide benefits to these developments then it will be vital that funding is made available on a recurrent basis.
3.0 Recommendations
The Board is requested to note the content of this report.
Debbie White Director of Operations Norfolk and Waveney
Background Papers / Information Appendix 1 Appendix 2
Norfolk Action Plan to Enable Delivery of Shared Goals of the Mental Health Crisis Care Concordat
ACTION TIMESCALEFINANCIAL
IMPLICATIONLED BY OUTCOMES PROGRESS & MILESTONES RAG
NATIONA
L REF.1
1.1 To review the monitoring of use of section 135 and bring this within
existing monitoring processes;
Mar-15 NoneNorfolk Constabulary / NSFT /
NCC
Local monitoring arrangements are in place for Section 135 and
136. Data which quantifies the demand for responses for people in
mental health crisis and provides clearer evidence on which to base
local commissioning is accurate and available.
Daily, monthly and quarterly monitoring in place for section 136