Drinking Water and Cancer Robert D. Morris Department of Family and Community Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin Any and all chemicals generated by human activity can and will find their way into water supplies. The types and quantities of carcinogens present in drinking water at the point of consumption will differ depending on whether they result from contamination of the source water, arise as a consequence of treatment processes, or enter as the water is conveyed to the user. Source-water contaminants of concern include arsenic, asbestos, radon, agricultural chemicals, and hazardous waste. Of these, the strongest evidence for a cancer risk involves arsenic, which is linked to cancers of the liver, lung, bladder, and kidney. The use of chlorine for water treatment to reduce the risk of infectious disease may account for a substantial portion of the cancer risk associated with drinking water. The by-products of chlorination are associated with increased risk of bladder and rectal cancer, possibly accounting for 5000 cases of bladder cancer and 8000 cases of rectal cancer per year in the United States. Fluoridation of water has received great scrutiny but appears to pose little or no cancer risk. Further research is needed to identify and quantify risks posed by contaminants from drinking-water distribution pipes, linings, joints, and fixtures and by biologically active micropollutants, such as microbial agents. We need more cost-effective methods for monitoring drinking-water quality and further research on interventions to minimize cancer risks from drinking water. - Environ Health Perspect 1 03(Suppl 8):225-232 (1995) Key words: arsenic, asbestos, bladder cancer, cancer, chlorination, environment, fluoridation, rectal cancer, water Introduction Few things tie humans so directly to the natural environment as drinking water. The contamination of water is a direct reflection of the degree of contamination of the environment. After flushing airborne pollutants from the skies, rainwater literally washes over the entire human landscape before running into the aquifers, streams, rivers, and lakes that supply our drinking- water. Any and all of the chemicals gener- ated by human activity can and will find their way into water supplies. Evaluating possible links between drinking water and cancer means identifying those chemi- cals that appear in enough water supplies at sufficient concentrations to pose a substantial attributable cancer risk. Contaminants may enter water supplies at many points before reaching the tap. The types and quantities of carcinogens present in drinking water at the point of consump- tion may result from contamination of the This paper was presented at the President's Cancer Panel Conference on Avoidable Causes of Cancer held 7-8 April 1994 in Bethesda, Maryland. Manuscript received 9 March 1995; manuscript accepted 24 March 1995. The author gratefully acknowledges R. Munasinghe for his assistance in preparation of the maps included in this paper. Address correspondence to Dr. Robert D. Morris, Department of Family and Community Medicine, Medical College of Wisconsin, 8701 Watertown Plank Road, Milwaukee, WI 53226. Telephone: (414) 456-8382. Fax: (414) 266-8502. E-mail: [email protected]Abbreviations: IARC, International Agency for Research on Cancer; DDT, dichlorodiphenyl- trichloroethane. source water, arise as a consequence of treatment processes, or enter as the water is conveyed to the user. Many different car- cinogens may contaminate source waters, but they usually exist in drinking water at low concentrations. On the other hand, chemicals that enter drinking water during the course of water treatment are limited in number, but these chemicals appear in drinking-water supplies with greater fre- quency than most source water contami- nants. Finally, the compounds contained in the pipes, joints, and fixtures of the water distribution system may contaminate treated water on its way to the consumer. Similarities in the construction of drinking- water distribution systems mean that any carcinogen entering through this pathway may be widespread and can pose substantial attributable risks of cancer. The following discussion reviews the attributable risks for contaminants entering at each of these points. Data gaps are identified and emerging areas of concern are discussed. Source-Water Contaminants Except for naturally occurring minerals such as calcium carbonate, contaminants that enter the water supply through the source water generally occur at low con- centration levels. Source-water contami- nants of concern either are sufficiently potent carcinogens to pose risks at extremely low concentrations or cause local contamination at high concentra- tions. The source-water contaminants that have been the focus of concern among those individuals investigating environmental cancer risks include arsenic, asbestos, radon, agricultural chemicals, and hazardous waste. Some of the strongest evidence for a cancer risk associated with source-water contamination involves arsenic. Epidemi- ologic studies from Taiwan have suggested that arsenic in drinking water poses sub- stantial risks of liver, lung, bladder, and kidney cancer as listed in Table 1 (1,2). Although toxicologic studies do not pro- vide unequivocal evidence of carcinogenic- ity (3), occupational studies, as well as other epidemiologic studies, support the findings of the Taiwanese studies(4). Estimates of attributable risk based on the data in Table 1 suggest that an average level of arsenic 2.5 pg/l in drinking water in the United States of causes approxi- mately 3000 cases of cancer per year (4). Although asbestos is a proven carcino- gen, the attributable risks associated with asbestos in drinking water do not appear to be substantial. An early study in California (5) suggested that there may be an Table 1. Estimated mortality risk ratios by arsenic levels in drinking water in Taiwan. Cancer Back- Water levels, pg/l p-Value site Sex ground 170 470 800 for trend Liver M 1.0 1.2 1.5 2.5 <0.001 F 1.0 1.6 2.1 3.6 <0.001 Lung M 1.0 1.8 3.3 4.5 <0.001 F 1.0 2.8 4.3 8.8 <0.001 Bladder M 1.0 5.1 12.1 28.7 <0.001 F 1.0 11.9 25.1 65.4 <0.001 Kidney M 1.0 4.9 11.9 19.6 <0.001 F 1.0 4.0 13.9 37.0 <0.001 Data from Chen et al. ( 1). Environmental Health Perspectives 225
Transcript
Drinking Water and CancerRobert D. MorrisDepartment of Family and Community Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin
Any and all chemicals generated by human activity can and will find their way into water supplies. The types and quantities of carcinogens present indrinking water at the point of consumption will differ depending on whether they result from contamination of the source water, arise as aconsequence of treatment processes, or enter as the water is conveyed to the user. Source-water contaminants of concern include arsenic,asbestos, radon, agricultural chemicals, and hazardous waste. Of these, the strongest evidence for a cancer risk involves arsenic, which is linked tocancers of the liver, lung, bladder, and kidney. The use of chlorine for water treatment to reduce the risk of infectious disease may account for asubstantial portion of the cancer risk associated with drinking water. The by-products of chlorination are associated with increased risk of bladderand rectal cancer, possibly accounting for 5000 cases of bladder cancer and 8000 cases of rectal cancer per year in the United States. Fluoridation ofwater has received great scrutiny but appears to pose little or no cancer risk. Further research is needed to identify and quantify risks posed bycontaminants from drinking-water distribution pipes, linings, joints, and fixtures and by biologically active micropollutants, such as microbial agents.We need more cost-effective methods for monitoring drinking-water quality and further research on interventions to minimize cancer risks fromdrinking water. - Environ Health Perspect 1 03(Suppl 8):225-232 (1995)
IntroductionFew things tie humans so directly to thenatural environment as drinking water.
The contamination of water is a directreflection of the degree of contaminationof the environment. After flushing airbornepollutants from the skies, rainwater literallywashes over the entire human landscapebefore running into the aquifers, streams,rivers, and lakes that supply our drinking-water. Any and all of the chemicals gener-
ated by human activity can and will findtheir way into water supplies. Evaluatingpossible links between drinking water
and cancer means identifying those chemi-cals that appear in enough water suppliesat sufficient concentrations to pose a
substantial attributable cancer risk.Contaminants may enter water supplies
at many points before reaching the tap. Thetypes and quantities of carcinogens presentin drinking water at the point of consump-tion may result from contamination of the
This paper was presented at the President'sCancer Panel Conference on Avoidable Causes ofCancer held 7-8 April 1994 in Bethesda, Maryland.Manuscript received 9 March 1995; manuscriptaccepted 24 March 1995.
The author gratefully acknowledges R. Munasinghefor his assistance in preparation of the maps includedin this paper.
Address correspondence to Dr. Robert D. Morris,Department of Family and Community Medicine,Medical College of Wisconsin, 8701 WatertownPlank Road, Milwaukee, WI 53226. Telephone:(414) 456-8382. Fax: (414) 266-8502. E-mail:[email protected]
Abbreviations: IARC, International Agency forResearch on Cancer; DDT, dichlorodiphenyl-trichloroethane.
source water, arise as a consequence oftreatment processes, or enter as the water isconveyed to the user. Many different car-cinogens may contaminate source waters,but they usually exist in drinking water atlow concentrations. On the other hand,chemicals that enter drinking water duringthe course of water treatment are limited innumber, but these chemicals appear indrinking-water supplies with greater fre-quency than most source water contami-nants. Finally, the compounds contained inthe pipes, joints, and fixtures of the waterdistribution system may contaminatetreated water on its way to the consumer.Similarities in the construction of drinking-water distribution systems mean that anycarcinogen entering through this pathwaymay be widespread and can pose substantialattributable risks of cancer. The followingdiscussion reviews the attributable risksfor contaminants entering at each of thesepoints. Data gaps are identified andemerging areas of concern are discussed.
Source-Water ContaminantsExcept for naturally occurring mineralssuch as calcium carbonate, contaminantsthat enter the water supply through thesource water generally occur at low con-centration levels. Source-water contami-nants of concern either are sufficientlypotent carcinogens to pose risks atextremely low concentrations or causelocal contamination at high concentra-tions. The source-water contaminantsthat have been the focus of concernamong those individuals investigatingenvironmental cancer risks include arsenic,
Some of the strongest evidence for acancer risk associated with source-watercontamination involves arsenic. Epidemi-ologic studies from Taiwan have suggestedthat arsenic in drinking water poses sub-stantial risks of liver, lung, bladder, andkidney cancer as listed in Table 1 (1,2).Although toxicologic studies do not pro-vide unequivocal evidence of carcinogenic-ity (3), occupational studies, as well asother epidemiologic studies, support thefindings of the Taiwanese studies(4).Estimates of attributable risk based on thedata in Table 1 suggest that an averagelevel of arsenic 2.5 pg/l in drinking waterin the United States of causes approxi-mately 3000 cases of cancer per year (4).
Although asbestos is a proven carcino-gen, the attributable risks associated withasbestos in drinking water do not appear tobe substantial. An early study in California(5) suggested that there may be an
Table 1. Estimated mortality risk ratios by arseniclevels in drinking water in Taiwan.
Cancer Back- Water levels, pg/l p-Valuesite Sex ground 170 470 800 for trend
elevation in colorectal cancer risk associ-ated with asbestos in drinking water. Itappears that these findings are limited tosituations in which naturally occurring lev-els are high. A subsequent, more detailedstudy of asbestos in source water, togetherwith studies of asbestos leached from waterdistribution systems, suggests that, whenasbestos is present at levels commonlyfound in drinking water, it does not pose amajor cancer risk (6,7).
Radon is also a known carcinogen;however, the evidence linking consumptionof radon-contaminated water to humancancer is weak (8). The relationshipbetween ionizing radiation and cancer iswell understood. This information, coupledwith measured levels of radon in drinkingwater, suggests that fewer than 100 cases ofcancer occur each year in the United Statesas a consequence of consuming radon indrinking water (9).
Farm runoff containing agriculturalchemicals and manure may lead to local orregional contamination of source waterswith insecticides, fungicide, rodenticides,herbicides, and fertilizers, which containphosphorous and nitrogen. Although somepesticides are carcinogens, drinking-watercontamination resulting from their agricul-tural application has not been directly asso-ciated with cancer in epidemiologic studies.Emerging evidence, however, indicates thatfertilizers may pose cancer risks.
Studies in China among populationsexposed to high levels of nitrates in drink-ing water have suggested links betweennitrate contamination and stomach andliver cancer (10). In these studies, thehistology of the gastric lesions has beenlinked to the level of nitrates in the water(11) and cancer rates increased with the invitro mutagenicity of the drinking water(12). Nitrates may act as carcinogensthrough the formation of N-nitroso com-pounds (13). When human volunteerswere given proline, which is a secondaryamine, those participants in areas withhigher levels of nitrate in their drinkingwater had higher levels of N-nitrosoprolinein their urine than volunteers residing inplaces with low nitrate levels in their drink-ing water (14). Although an epidemiologi-cal study in France failed to demonstratean association between nitrates in drinkingwater and cancer (15), current evidence issufficient to warrant further study of thispotential carcinogen.
Few examples of significant linksbetween hazardous waste in drinking waterand cancer have been reported. Elevated
cancer risks are difficult to detect becauseof the relatively low incidence of site-specific neoplasms and the typically smallsize of exposed populations (16). An eco-logic study in New Jersey found weak evi-dence for a positive association betweenvolatile organic compounds in drinkingwater and leukemia (17). In a nationalecologic study, Griffith et al. (18) foundevidence of elevated cancer rates in thevicinity of hazardous waste sites. Limita-tions on ecologic data urge caution in theinterpretation of such findings. Contami-nation of wells associated with hazardouswaste disposal in Woburn, Massachusetts,was ultimately linked to elevations in theirincidence of leukemia (19). Although thisinvestigation was arguably the most thor-ough study of this kind, questions wereraised about the magnitude of the risk(20). There are numerous factors thatmake it difficult, if not impossible, to esti-mate the attributable risks associated withhazardous wastes on a national level,including the wide variety of chemicalspresent in hazardous waste sites, thedifficulties in assessing exposure, the obsta-cles to establishing links between exposureand cancer even when links are present, thesmall size of exposed populations, and theuncertainties concerning future risks.
Cancer Risks Associatedwith Water TreatmentUntil this century, concerns about thecleanliness of drinking water focusedalmost exclusively on the presence orabsence of pathogens. Ironically, the chlo-rine used to reduce the risk of infectiousdisease may account for a substantial por-tion of the cancer risk associated withdrinking water.
Chlorination of drinking water played acentral role in the reduction in the mortal-ity rates associated with waterbornepathogens. Water chlorination was firstintroduced at the Jersey City Water Worksin Boonton, New Jersey. The relative easeof use of water chlorination, together withits potent bactericidal action, lead to therapid dissemination of this treatment tech-nology throughout the United States.Overshadowed by the clear benefits topublic health, the potential health risksassociated with water chlorination receivedlittle attention. This view is evident in anarticle heralding the opening of theBoonton waterworks, which appeared onthe back page of the New York Times (21).The brief article claimed that, with thisprocess, "any municipal water supply can
be made as pure as mountain spring water.Chlorination destroys all animal andmicrobial life, leaving no trace of itselfafterwards" (21).
This statement represented the prevail-ing wisdom until about 20 years ago whenhalogenated organic compounds, particu-larly chloroform, were identified in chlori-nated drinking water (22). A subsequentsurvey of water supplies showed that thesecompounds were common in water sup-plies throughout the United States and thatconcentrations were far higher in treatedsurface water than in treated groundwater(23). With these revelations came a shift inthe basis of our definition of cleanliness indrinking water. New concerns about cancerrisks associated with chemical contamina-tion from chlorination by-products havegiven rise to 25 epidemiologic studies.
Table 2 summarizes the results of ametaanalysis of the cohort and case-controlstudies that have been conducted to evalu-ate the association between consumptionof chlorinated drinking water and cancer atvarious sites (24). For each cancer site, thepooled results from available studies showelevations in risk, and the risk estimatesachieved statistical significance for bladderand rectal cancer. Further analyses in thisstudy suggested that risks increased withincreasing exposure and that improvementsin exposure assessment yielded higherestimates of risk. Confounding could con-ceivably explain the observed pattern ofassociation, but stratification into studiesthat adjusted or did not adjust for con-founders does not support such an asser-tion. Studies that adjusted for populationdensity, smoking, or occupation, did notdemonstrate a difference in relative riskestimates. Although it is still possible thatthe pattern of associations could represent
Table 2. Results from metaanalysis of chlorinationby-products and cancer.
Relative risk 95% ConfidenceSite n8 estimate interval p
'Number of studies evaluating specific cancer site.
Environmental Health Perspectives226
DRINKING WATERAND CANCER
some systematic bias in the available studies,no specific bias has emerged to explain theobserved results.
In summary, the available studies gen-erally support the notion that by-productsof chlorination are associated withincreased cancer risks. The precise charac-terization of these risks is somewhat lessclear. The broad category of chlorinationby-products includes many different com-pounds, and the carcinogens among thesecompounds have not been clearly identi-fied. Trihalomethanes are the most preva-lent compounds and, given the evidencesuggesting that they are animal carcino-gens, have been the focus of research andregulation. The chlorination by-productsthat have been specifically identified, how-ever, account for only about half of thebound chlorine in finished drinking water.Other compounds present in far smallerquantities may pose substantial cancer risksby virtue of high potency (25).
The goal of precise characterization ofthe cancer risk posed by each of the chlori-nation by-products will probably prove tobe unrealistic. A quantitative dose-responserelationship has not been well described forany individual compound, much less theentire complex mixture. The relative con-tributions of different exposure pathwaysvary among the by-products and have notbeen well characterized. Nonetheless, giventhe large number of people who consumechlorinated surface water, the number ofcases of cancer potentially attributable tothis exposure is substantial. The numbersderived from the metaanalysis suggest that5000 (95% CI = 2000-7000) cases of blad-der cancer per year and 8000 cases of rectalcancer per year (95% CI = 200-14,000)may be associated with consumption ofchlorinated drinking water. Although thesefigures do not provide a precise estimate ofrisk, the true risk is probably within anorder of magnitude of these values.
Since the publication of the meta-analysis, a number of other studies havebeen completed. McGeehin et al. (26)found an elevated risk for bladder cancercomparable in magnitude to the summaryestimate of the metaanalysis. Kuovaslo etal. (27) found a similar estimate of risk forbladder cancer but did not find an elevatedrisk for rectal cancer. Kantor (28), on theother hand, found a risk for rectal cancersimilar to that in the metaanalysis, but anincrease in bladder cancer risk associatedwith chlorination by-products was onlyobserved among smokers. Including thesefindings within the metaanalysis does not
change its results. Nonetheless, theseapparent inconsistencies may reflect impor-tant differences in the carcinogenicity ofthe exposures experienced among thevarious study populations. The complexmixture of compounds that comprise chlo-rination by-products, the multiple path-ways of exposure to those compounds, andthe potential for synergy with diet andother exposures may well explain the appar-ent inconsistencies that exist among thestudies included in the metaanalysis.
To stop chlorination of drinking-waterto eliminate the elevated cancer risks fromchlorination by-products would be fool-hardy. Nonetheless, the data provide strongevidence to support expanded efforts inresearch and development of alternatives tochlorination for the disinfection of drink-ing-water. Chlorination is particularly effec-tive in preventing recontamination duringdistribution. Alternatives must provide asimilar level of protection. The capacity ofchemical disinfectants to kill pathogens gen-erally reflects their strong tendency to reactwith organic chemicals. The production ofby-products may, therefore, be inherent tothe chemical disinfection of drinking water.For example, ozone produces aldehydesincluding formaldehyde and bromate ifthe source waters contain bromine. Thesecompounds pose a cancer risk that is notyet fully quantified (29). Before the wide-spread introduction of any new method ofwater treatment, the carcinogenicity ofby-products should be carefully evaluated.
Of the other compounds routinelyadded during the course of drinking-watertreatment, fluoride has received the greatestscrutiny as a potential carcinogen. TheInternational Agency for Research onCancer ([ARC) Working Group on CancerRisks from Fluoridated Drinking Water hasconcluded that available ecologic studieshave been consistent in finding no risk butstopped short of suggesting that flouridewas not carcinogenic because the studieswere all ecologic in design (30). One ani-mal study (31) and one case-control study(32) suggested that fluoridated water couldbe linked with osteosarcoma, but thesefindings will require further confirmationto be considered suggestive of causality. Itappears that if flouride poses any cancerrisk, the attributable risk is relatively small.
Cancer Risks Associated withDrinking-Water DistributionThe chemical components of pipes, joints,and fixtures can contaminate drinkingwater after treatment. A broad range of
materials are used in these systems. Pipescan be made from metals, primarily iron,copper and lead; plastics, such as polyvinylchloride and polyethylene; and concrete orasbestos/concrete aggregates. These pipesmay be plated or lined with a variety ofcompounds including zinc, coal tar,asphalt, or vinyl. In addition, bacteria andorganic matter frequently coat the inside ofpipes within the distribution systems (33).All of these can be sources of new contami-nation, or they can combine with chemicalsalready in the water to alter the health risksposed by drinking water. In 1979, a studyof several medium-size water systemsdemonstrated increases in mutagenicity ofdrinking water after passage through thedistribution system (34). This study didnot isolate specific contaminants that mightbe responsible. Perhaps the most extensivelystudied contaminant associated with drink-ing water distribution is asbestos, which canleach from asbestos-concrete pipes. Theavailable research suggests that asbestosfrom this source does not pose significanthuman cancer risks (35-37). A study byAshengrau et al. (38) showed an increase inleukemia in association with trichlorethyl-ene, which had leached from a plastic linerused in concrete pipes. Other than thenegative results of the asbestos studies, theavailable research does not allow for strongconclusions concerning the magnitude ofcancer risks relating to contamination fromthe distribution system. Further research isneeded to identify and quantify risks posedby contamination that occurs duringdrinking-water distribution.
Emerging Concerns andPotential Cancer RisksWater is among the most basic require-ments for human survival, therefore,emerging health threats related to drinking-water contamination demand careful con-sideration. Although the identification ofpotential threats to human health requires acertain degree of speculation, protection ofpublic health requires a willingness to occa-sionally err in the name of caution. Cancerrisks may emerge from the micropollutantsand microbial contaminants that can enterour drinking-water supply. Less directeffects may also pose risks.
One focus of current concerns aboutthe potential for micropollutants to causecancer involves those compounds thatmimic naturally occurring, biologicallyactive compounds. Biologically activemicropollutants or endocrine disruptersappear to have the ability to disturb normal
Volume 103, Supplement 8, November 1995 227
R.D. MORRIS
intercellular communications. For example,evidence from wildlife biologists, toxi-cologists, endocrinologists, and epidemiol-ogists demonstrate the potential forestrogenic effects of environmental conta-minants among humans (39,40). Meta-bolites of DDT are estrogenic in vivo andhave been associated with the developmentof breast cancer in epidemiologic studies(41,42). Nonyl-phenol, a common chemi-cal surfactant, increases proliferation inbreast tumor cell cultures (43). The poten-tial risks from drinking-water contami-nants acting through these mechanismshave not been evaluated.
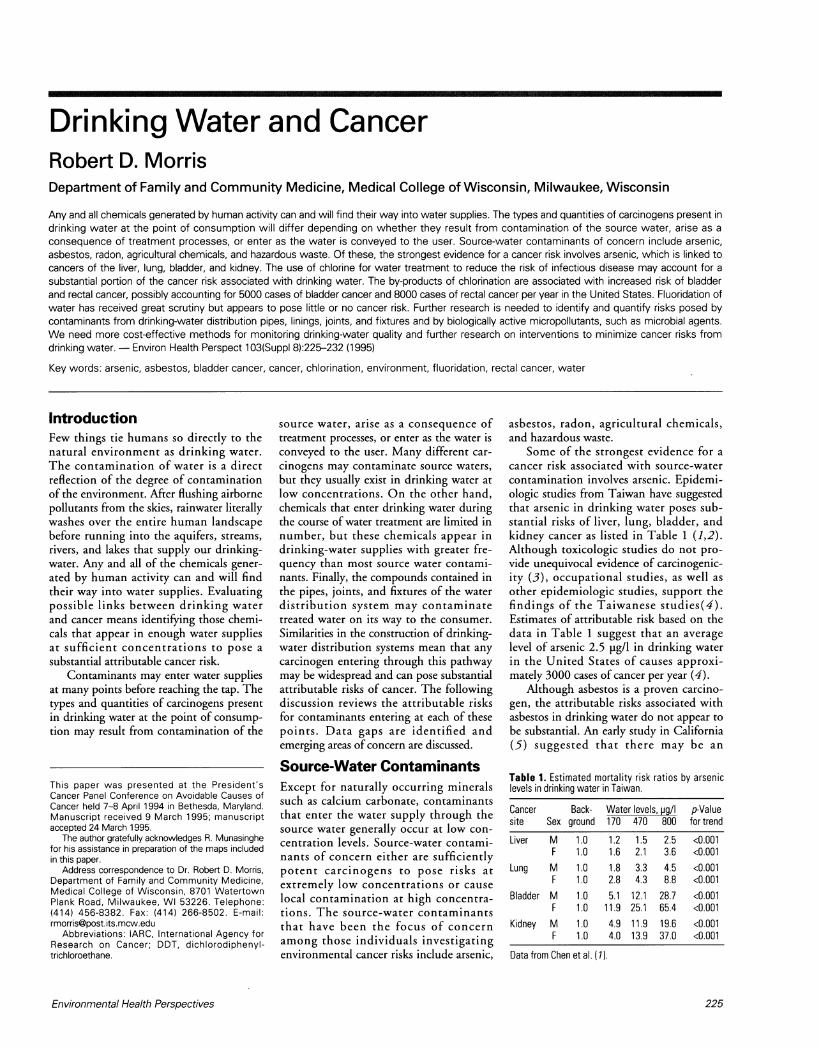
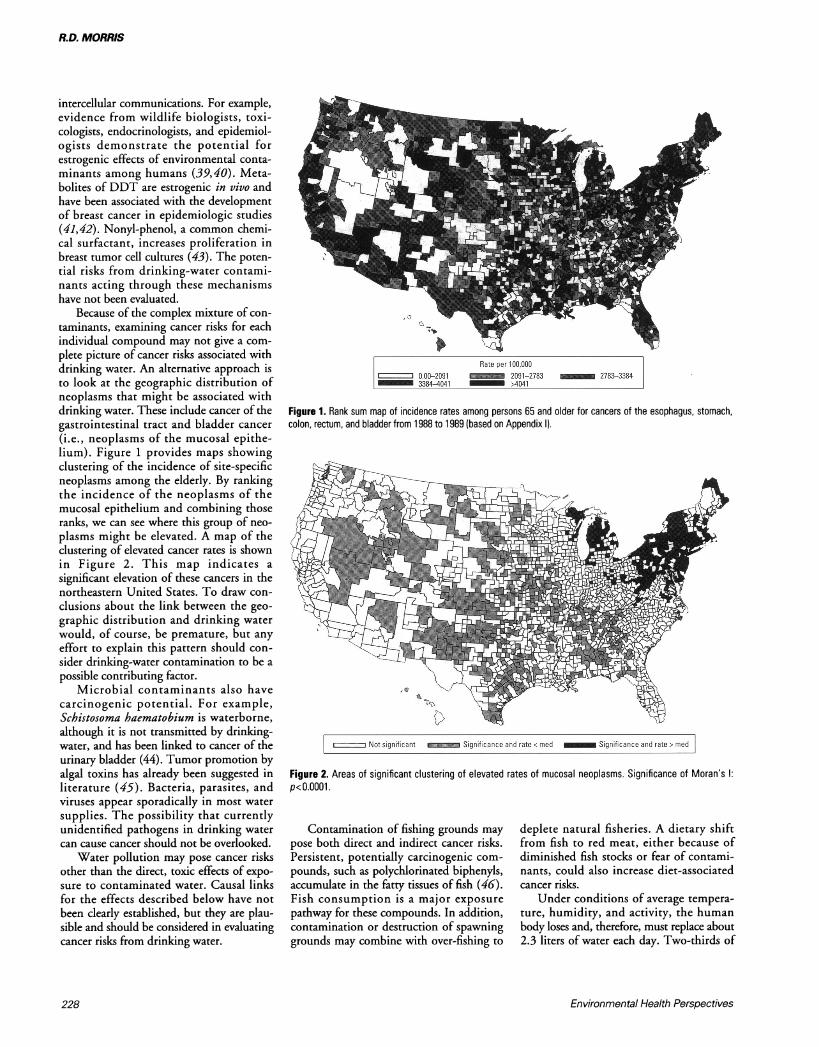
Because of the complex mixture of con-taminants, examining cancer risks for eachindividual compound may not give a com-plete picture of cancer risks associated withdrinking water. An alternative approach isto look at the geographic distribution ofneoplasms that might be associated withdrinking water. These include cancer of thegastrointestinal tract and bladder cancer(i.e., neoplasms of the mucosal epithe-lium). Figure 1 provides maps showingclustering of the incidence of site-specificneoplasms among the elderly. By rankingthe incidence of the neoplasms of themucosal epithelium and combining thoseranks, we can see where this group of neo-plasms might be elevated. A map of theclustering of elevated cancer rates is shownin Figure 2. This map indicates asignificant elevation of these cancers in thenortheastern United States. To draw con-clusions about the link between the geo-graphic distribution and drinking waterwould, of course, be premature, but anyeffort to explain this pattern should con-sider drinking-water contamination to be apossible contributing factor.
Microbial contaminants also havecarcinogenic potential. For example,Schistosoma haematobium is waterborne,although it is not transmitted by drinking-water, and has been linked to cancer of theurinary bladder (44). Tumor promotion byalgal toxins has already been suggested inliterature (45). Bacteria, parasites, andviruses appear sporadically in most watersupplies. The possibility that currentlyunidentified pathogens in drinking watercan cause cancer should not be overlooked.
Water pollution may pose cancer risksother than the direct, toxic effects of expo-sure to contaminated water. Causal linksfor the effects described below have notbeen clearly established, but they are plau-sible and should be considered in evaluatingcancer risks from drinking water.
- -~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.-
'Ic
~~~~~~~~o-
| Rate per 100,0000.00-2091 2091-2783 _ 2783-33843384-4041 >4041
Figure 1. Rank sum map of incidence rates among persons 65 and older for cancers of the esophagus, stomach,colon, rectum, and bladder from 1988 to 1989 (based on Appendix I).
,-- ----Not significant miSignificance and ratec med _ Significance and rate > med
Figure 2. Areas of significant clustering of elevated rates of mucosal neoplasms. Significance of Moran's l:p<O.OOOl
Contamination of fishing grounds maypose both direct and indirect cancer risks.Persistent, potentially carcinogenic com-pounds, such as polychlorinated biphenyls,accumulate in the fatty tissues of fish (46).Fish consumption is a major exposurepathway for these compounds. In addition,contamination or destruction of spawninggrounds may combine with over-fishing to
deplete natural fisheries. A dietary shiftfrom fish to red meat, either because ofdiminished fish stocks or fear of contami-nants, could also increase diet-associatedcancer risks.
Under conditions of average tempera-ture, humidity, and activity, the humanbody loses and, therefore, must replace about2.3 liters of water each day. Two-thirds of
Environmental Health Perspectives228
DRINKING WATERAND CANCER
this consumption is in the form of water orsome other beverage. Concerns about thehealth risks or taste of drinking water mayinduce those who consume tap water toshift to bottled water, or other beverages.These beverages may include sweetened softdrinks and alcoholic beverages, which canpose health risks greater than those associ-ated with drinking water. In addition, theproduction and disposal of containers foralternative beverages, including bottledwater, may lead to the release of carcinogens.Summary and PreventionStrategiesThe cancer risks associated with the majorcontaminants of drinking water are listedin Table 3. The weight of the evidencesuggests that chlorination by-products posesubstantial cancer risks that should bereduced. A growing body of evidence sup-ports the possibility that arsenic in drink-ing water may also carry unacceptablecancer risks. The cancer risks from radonand asbestos in drinking water are less sub-stantial but may require remediation wherelocal conditions dictate. The availableevidence does not support assertions ofcancer risks associated with fluoridation ofdrinking water.
For most other compounds present indrinking water, the attributable cancer
risks are not clear. Hazardous waste andpesticides may contaminate waters locallyand regionally, but the attributable cancerrisk is difficult to quantify. Nitrates aremore widespread contaminants and moreclosely linked to human cancer, but evi-dence is incomplete. Contamination dur-ing drinking-water distribution may posecancer risks, but the epidemiologicevidence is extremely limited. Less conven-tional cancer risk factors, such as biologi-cally active micro pollutants and pathogens,only present the possibility of risk atpresent but may emerge as importantcarcinogens in the future.
Cancer-prevention strategies must focuson source-water purity. In particular,strong source-water protection efforts pro-vide a barrier to emerging cancer risks thathave not been identified or fully character-ized. Furthermore, failure to protect sourcewater purity will necessitate more extensivewater treatment and, in most cases, heavierchlorination. Drinking-water treatmenttechnologies should be evaluated withextreme care and should be reevaluated ona regular basis. The concept of continuousquality improvement should be fully inte-grated into drinking-water treatment andshould include ongoing efforts to develop,evaluate, and implement new treatmenttechnologies. More cost-effective methods
Table 3. Carcinogenic risk associated with majorcontaminants of drinking water.
Attributable risk Contaminant Point of Entry
Substantial Chlorination Treatmentby-products
Arsenic Source waterSmall to Asbestos Source water,moderate distribution
Radionuclides Source waterLittle or none Fluoride TreatmentUnknown Hazardous waste Source water
distributionBiologically active Source water,micropollutants distribution (?)
for monitoring drinking-water quality needto be aggressively developed. Finally,drinking-water research should be a prior-ity. The consequences of a lack of vigilancewith respect to emerging threats in drink-ing water were felt with devastating impactin Milwaukee, Wisconsin, in 1993, when400,000 people fell ill during a waterborneoutbreak of cryptosporidiosis (47). Weshould view this as a warning and anopportunity for timely intervention tominimize health risks from drinking water.
Appendix IThe map of cancer incidence rates formucosal cancer was based on the applica-tion of the method described below.
Assessing Cancer Incidence RatesThe incidence of cancer of the esophagus,stomach, colon, and urinary bladder forpersons over 64 years of age for the period1988 through 1989 was estimated usingMedicare hospital admissions data. Themethod used to estimate cancer incidencewith this database is reported elsewhere(1-3). Briefly stated, all patients with a hos-pital admission for cancer were identified.Patients with no admissions for the sitespecific cancer diagnosis in the previous 4years were considered to represent incidentcases. From these, age and sex adjusted,race-specific cancer rates were determined.
Localizing Diseawe ClustersA disease cluster can be defined as a groupof geographic areas that are close to oneanother with disease rates that are simi-larly increased or decreased relative to
surrounding areas. This can be expressedquantitatively for each analytic area i, as theweighted covariance of its disease rate (xi)with the rates for the rest of the analyticareas in the study region (xj) as given by
wij(xi-X-)(xj-X-) [1]
n-1
where the weights (w,1) are the inverse ofthe distance between population centroidsof the analytic areas (4).
If the sizes of the study areas are nothomogeneous across the study regions,the weights corresponding to two adjacentareas will vary according to the size ofthose areas. After modification to accom-modate variations in region size, theregional spatial autocorrelation coefficient(RSAC) for analytic area i, Ri, becomes
E(xi )2x(wii )
Ri= (xi--E _2(Wi_)
The mean and standard deviation of thedistribution of RSAC can be reasonablyapproximated by a normal distributionwith an expectation of zero and a standarddeviation of a/(n-2)1/2 where a is the stan-dard deviation of xi and n is the number ofanalytic areas.
The RSAC was calculated for each ana-lytic area, and the theoretical mean andstandard deviation were used to test forsignificance. Analytic areas that havesignificantly high RSACs were furtherclassified into two groups based onwhether their disease rates were greater orless than the median rate. Analytic areaswith significant RSACs and disease ratesgreater than the median were defined asanalytic areas with clustering of elevateddisease rates or high clusters. These ana-lytic areas were shaded black in the map.Analytic areas with significant RSACs anddisease rates less than the median weredefined as analytic areas with clustering oflow disease rates or low clusters. Whenthe value of the RSAC was not significant,analytic areas were not shaded and
Volume 103, Supplement 8, November 1995 229
R.D. MORRIS
A B~~~~~~~~~~~~~~~~~~~~~~~C D
Not significant _ Significance and rate < med Significance and rate > med
Figure Al. Regional spatial autocorrelation coefficient (RSAC) maps showing localized areas containing statistically significant disease clusters. (A) Malignant neoplasm ofthe esophagus. (B) Malignant neoplasm of the bladder. (C) Malignant neoplasm of the colon. (D) Malignant neoplasm of the stomach. Significance of Moran's l: p<O.OOOl.
represented random spatial structures.Maps depicting the results of these analy-ses (RSAC maps) were created to evaluatethe use of this method as a visual aid tolocalize areas that contain disease clusters.These methods are described in detail else-where (1,4). The resulting maps areshown in Figure Al.
Appendix References1. Morris RD, Munasinghe RL.
Aggregation of existing geographicregions to diminish spurious variabil-ity of disease rates. Stat in Med12:1915-1929 (1993).
2. McBean AM, Babish JD, Warren JL.Determination of lung cancerincidence in the elderly usingMedicare claims data. Am J Epidemiol
137(2):226-234 (1993).3. Whittle J, Steinberg EP. Accuracy of
Medicare claims data for estimation ofcancer incidence and resection ratesamong elderly Americans. Med Care29(12):1226-1236 (1991).
4. Munasinghe RL, Morris RD.Localization of disease clusters usingregional measures of spatial autocorre-lation. Stat Med (in press).
REFERENCES
1. Chen CJ, Kuo TL, Wu MM. Arsenic and cancers (letter).Lancet:1(8582)414-415 (1988).
2. Wu MM, Kuo TL, Hwang YH, Chen CJ. Dose-response rela-tion between arsenic well water and mortality from cancer. AmJ Epidemiol 130:1123-1132 (1989).
3. IARC. IARC Monographs on Evaluation of Carcinogenic Risksof Chemicals to Humans; Overall Evaluation of Carcinogenicity:an Updating of IARC Monographs, Vols 1-42, Suppl 7.Lyon:International Agency for Research on Cancer, 1987.
4. Smith AH, Hopenhayn-Rich C, Bates MN, Goeden HM,
Hertz-Picciotto I, Duggan HM, Woed R, Kosnett M, SmithMT. Cancer risks from arsenic in drinking water. EnvironHealth Perspect 97:259-267 (1992).
5. Kanarek MS, Conforti PM, Jackson LA, Cooper RC, MurchioJC. Asbestos in drinking water and cancer incidence in the SanFrancisco Bay area. Am J Epidemiol 112:54-72 (1980).
6. Polissar L, Severson RK, Boatman ES. A case-control study ofasbestos drinking water and cancer risk. Am J Epidemiol119:456-471 (1984).
7. U.S. Department of Health and Human Services Working
230 Environmental Health Perspectives
DRINKING WATERAND CANCER
Group. Report on cancer risks associated with the ingestion ofasbestos. Environ Health Perspect 72:253-265 (1987).
8. Neuberger JS. Residential radon exposure and lung cancer: anoverview of published studies. Cancer Detect Prev 15:435-443(1991).
9. Crawford-Brown DJ, Cothern CR. A Bayesian analysis or sci-entific judgment of uncertainties in estimating risk due to222Rn in U.S. public drinking-water supplies. Health Phys53:11-21 (1987).
10. Tao XG, Zhu HG. Yu SZ, Zhao ZY, Wang JR, Wu GD, YouXF, Li C, Zhi WL, Bao JP, Sun ZQ. Effects of drinking waterfrom the lower reaches of the Huangpu River on the risk ofmale stomach and liver cancer death. Public Health Rev19:229-236 (1991-1992).
11. Xu G, Song P, Reed PI. The relationship between gastricmucosal changes and nitrate intake via drinking water in ahigh-risk population for gastric cancer in Moping County,China. Eur J Cancer Prev 1:437-443 (1992).
12. Tao XG, Zhu HG, Yu SZ, Zhao QY, Wang JR, Wu GD, YouXF, Li C, Zhi WL, Bao JP, Sun ZQ. Pilot study on the rela-tionship between male stomach and liver cancer death and themutagenicity of drinking water in the Huangpu River area.Public Health Rev 19:219-227 (1991-1992).
13. Mirvish SS, Huang Q, Chen SC, Birt DF, Clark GW, HinderRA, Amyrk TC, DeMeester TR. Metabolism of carcinogenicnitrosamines in the rat and human esophagus and induction ofesophageal adenocarcinoma in rats. Endoscopy 25:627-631(1993).
14. Mirvish SS, Grandjean AC, Moller H, Fike S, Maynard T,Jones L, Rosinsky S, Nie G. N-Nitrosoproline excretion byrural Nebraskans drinking water of varied nitrate content.Cancer Epidemiol Biomarkers Prev 1:455-461 (1992).
15. Leclerc H, Vincent P, Vandevenne P. Nitrates de l'eau de bois-son et cancer. Ann Gastroenterol Hepatol 27:326-32 (1991).
16. National Research Council. Environmental Epidemiology. Vol1: Public Health and Hazardous Wastes. Washington:NationalAcademy Press, 1991.
17. Fagliano JM, Berry M, Bove F, Burke T. Drinking-water cont-amination and the incidence of leukemia: an ecologic study.AmJ Public Health 80:1209-1212 (1990).
18. Griffith J, Duncan RC, Riggan WB, Pellom AC. Cancer mor-tality in US countries with hazardous waste sites and groundwater pollution. Arch Environ Health 44:69-74 (1989).
19. Lagakos SW, Wessen BJ, Zelen M. An analysis of contami-nated well water and health effects in Woburn, Massachusetts.J Am Stat Assoc 81:583-596 (1986).
20. MacMahon B. Comment. J Am Stat Assoc 81:597-599 (1986).21. Anonymous. New water purifier: chlorine used in reservoir that
supplies Jersey City. New York Times, 7 December 1908; 16.22. Rook JJ. Formation of halogforms during chlorination of nat-
ural waters. Soc Water Treat Exam 23:234-243 (1974).23. Symons JM, Bellar TA, Carswell JK, DeMarco J, Kropp KL,
Robeck GG, Seeger DR, Slocum CJ, Smith BL, Stevens AA.National organics reconnaissance survey for halogenated organ-ics. Am Water Works Assoc 67:634-646 (1975).
24. Morris RD, Audet AM, Angelillo IF, Chalmers TC, MostellerF. Chlorination, chlorination by-products, and cancer: a meta-analysis. Am J Public Health 82:955-963 (1992).
25. Kronberg L, Holmboom B, Tikkanen L. Identification of thestrong mutagen 3-chloro-4-(dichloromethyl)-5-hydroxy-2(5H)-furanone and its geometric isomer E-2-chloro-3-(dichloromethyl)-4-oxy-butenoic acid in mutagenic fractions ofchlorine-treated humic water and in drinking water. In: WaterChlorination Chemistry, Environmental Impact and HealthEffects (Jolley RL, ed). Chelsea, MI:Lewis Publishers,1987;153-159.
26. McGeehin MA, ReifJS, Becher JC, Mangione EJ. Case-controlstudy of bladder cancer and water disinfection methods inColorado. Am J Epidemiol 138:492-501 (1993).
27. Koivausalo M, Jaakkola JJ, Varitiainen T, Jakulinen T,Karjalainen S, Pukkala E, Tuomisto J. Drinking-water muta-genicity and gastrointestinal and urinary tract cancers: an ecologi-cal study in Finland. Am J Public Health 84:1223-1228 (1994).
28. Kantor KP, Lynch CF, Hildesheim M. Chlorinated drinkingwater and risk of bladder, colon, and rectal cancers: a case-control study in Iowa, USA. Epidemiology 6:S30 (1995).
29. Bull RJ, Kopfler KC. Health Effects of Disinfectants andDisinfectant By-products. Denver:American Water WorksAssociation, 1992.
30. IARC. Inorganic fluorides used in drinking water and dentalpreparations. In: IARC Monographs on the Evaluation ofCarcinogenic Risks to Humans. Vol 27: Some AromaticAmines, Anthraquinones and Nitroso Compounds, andInorganic Fluorides Used in Drinking Water and DentalPreparations. Lyon:International Agency for Research onCancer, 1982.
31. Bucher JR, Hejtmancik MR, Toft JD, Persing RL, Eustis SL,Haseman JK. Results and conclusions of the NationalToxicology Program's rodent carcinogenicity studies withsodium fluoride. Int J Cancer 48:733-737 (1991).
32. Cohn, P. Osteosarcoma and Chlorinated Drinking Water.Trenton, NJ:New Jersey Department of Health, 1993.
33. National Academy of Science. Biological quality of water in thedistribution system. In: Drinking Water and Health. Vol 4.Washington:National Academy Press, 1982.
34. Schwartz DJ, Saxena J, Kopfler FC. Water distribution system,a new source of mutagens in drinking waters. Environ SciTechnol 13:1138-1141 (1979).
35. Harrington JM, Craun GF, Meigs JW, Landrigan PJ, FlanneryJT, Woodhull RS. An investigation of the use of asbestoscement pipe for public water supply and the incidence of gas-trointestinal cancer in Connecticut, 1935-1973. Am JEpidemiol 107:96-103 (1978).
36. Howe HL, Wolfgang PE, Burnett WS, Nasca PC, YoungbloodL. Cancer incidence following exposure to drinking water withasbestos leachate. Public Health Rep 104:251-256 (1989).
37. Sadler TD, Rom WN, Lyon JL, Mason JO. The use ofasbestos-cement pipe for public water supply and the incidenceof cancer in selected communities in Utah. J Commun Health9:285-293 (1984).
38. Aschengrau A, Ozonoff D, Paulu C, Coogan P, Vezina R,Heeren T, Zhang Y. Cancer risk and tetrachforoethylene-cont-aminated drinking water in Massachusetts. Arch EnvironHealth 48:284-297 (1993).
39. Colborn T, Vom Saal FS, Soto AM. Developmental effects ofendocrine-disrupting chemicals in wildlife and humans.Environ Health Perspect 101:378-384 (1993).
40. Davis DL, Bradlow HL, Wolff M, Woodruff T, Hoel G,Anton-Culver H. Medical hypothesis: xenoestrogens as pre-ventable causes of breast cancer. Environ Health Perspect101:372-377 (1993).
41. Falck F Jr, Ricci A Jr, Wolff MS, Godbold J, Deckers P.Pesticides and polychlorinated biphenyl residues in humanbreast lipids and their relation to breast cancer. Arch EnvironHealth 47:143-146 (1992).
42. Wolff MS, Toniolo PG, Lee EW, Rivera M, Dubin N. Bloodlevels of organochlorine residues and risk of breast cancer. JNatl Cancer Inst 85:648-652 (1993).
43. Soto AM, Justicia H, Wray JW, Sonnenschein C. p-Nonyl-phenol: an estrogenic xenobiotic released from "modified"polystyrene. Environ Health Perspect 92:167-173 (1991).
44. Gelfand M, Weinberg RW, Castle WM. Relation between car-cinoma of the bladder and infestation with Schistosoma haema-tobium. Lancet 502:1249-1251 (1967).
45. Falconer IR, Buckley TH. Tumor promotion by Microcystis sp.,a blue-green alga occurring in water supplies [letter]. Med JAust 150:351 (1989).
46. U.S. EPA. National Study of Chemical Residues in Fish.EPA/823-R-92-008b. Washington:US EnvironmentalProtection Agency, 1992.
47. Mackenzie WR, Hoxie NJ, Proctor ME, Gradus MS, Blair KA,Peterson DE, Kazmierczak JJ, Addiss DG, Fox KR, Rose JB,Davis JP. A massive outbreak in Milwaukee of Crypotosporidiuminfection transmitted through the public water supply. N Engl JMed 331:161-167 (1994).