2
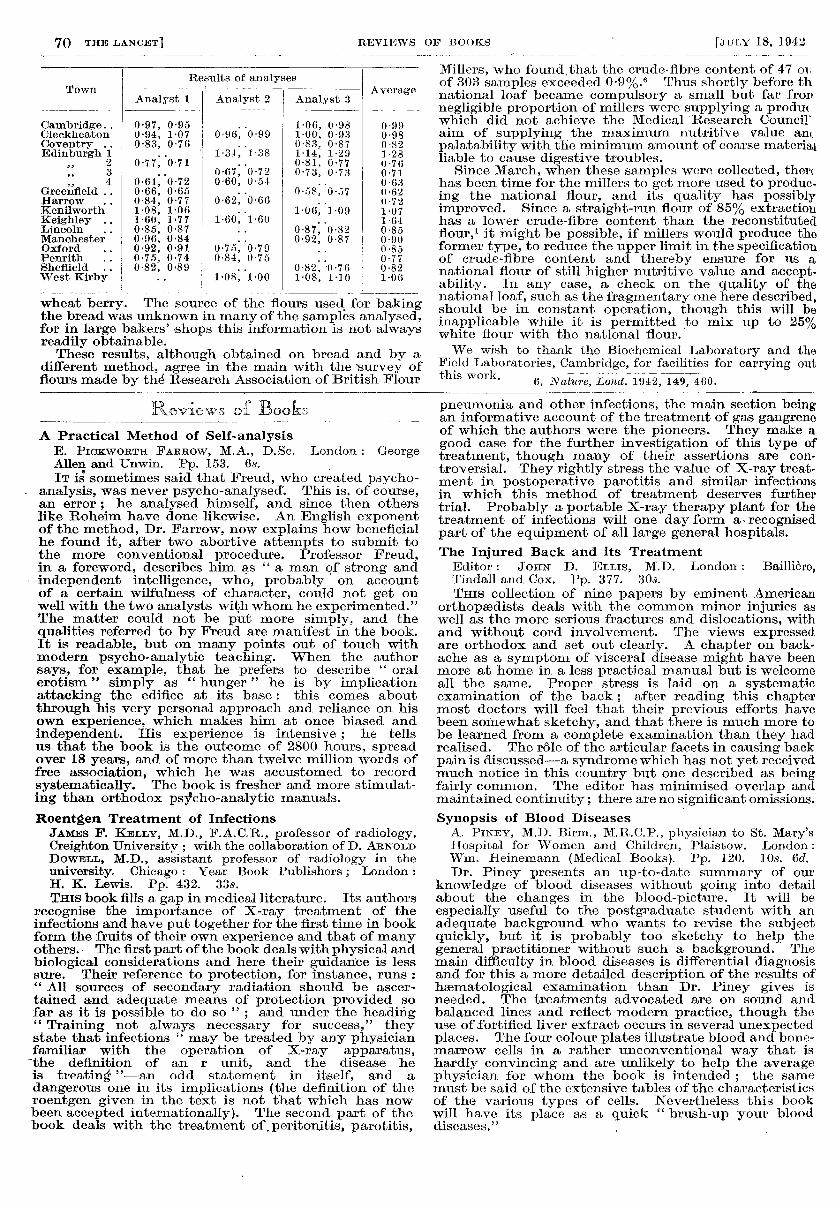
70 wheat berry. The source of the flours used for baking the bread was unknown in many of the samples analysed, for in large bakers’ shops this information is not always readily obtainable. These results, although obtained on bread and by a different method, agree in the main with the survey of flours made by the Research Association of British Flour Millers, who found, that the crude-fibre content of 47 on of 303 samples exceeded 0.9%.6 Thus shortly before th. national loaf became compulsory a small but far frop negligible proportion of millers were supplying a produ< which did not achieve the Medical -Research Council aim of supplying the maximum nutritive value a,m palatability with the minimum amount of coarse material liable to cause digestive troubles. Since March, when these samples were collected, ther( has been time for the millers to get more used to produc- ing the national flour, and its quality has possibly improved. Since a straight-run flour of 85% extraction has a lower crude-fibre content than the reconstituted flour,! it might be possible, if millers would produce the former type, to reduce the upper limit in the specification of crude-fibre content and thereby ensure for us a national flour of still higher nutritive value and accept- ability. In any case, a check on the quality of the national loaf, such as the fragmentary one here described, should be in constant operation, though this will be inapplicable while it is permitted to mix up to 25% white flour with the national flour. We wish to thank the Biochemical Laboratory and the Field Laboratories, Cambridge, for facilities for carrying out 6. Nature, Lond. 1942, 149, 460. Reviews of Books A Practical Method of Self-analysis E. PiCKWORTH FARROW, M.A., D.Se. London : George Allen and Unwin. Pp. 153. 6s. IT is sometimes said that Freud, who created psycho- analysis, was never psycho-analysed. This is, of course, an error ; he analysed himself, and since then others like Roheim have done likewise. An English exponent of the method, Dr. Farrow, now explains how beneficial he found it, after two abortive attempts to submit to the more conventional procedure. Professor Freud, in a foreword, describes him as " a man of strong and independent intelligence, who, probably on account of a certain wilfulness of character, could not get on well with the two analysts with whom he experimented." The matter could not be put more simply, and the qualities referred to by Freud are manifest in the book. It is readable, but on many points out of touch with modern psycho-analytic teaching. When the author says, for example, that he prefers to describe " oral erotism " simply as " hunger " he is by implication attacking the edifice at its base : this comes about through his very personal approach and reliance on his own experience, which makes him at once biased and independent. His experience is intensive ; he tells us that the book is the outcome of 2800 hours, spread over 18 years, and of more than twelve million words of free association, which he was accustomed to record systematically. The book is fresher and more stimulat- ing than orthodox psycho-analytic manuals. Roentgen Treatment of Infections JAMES F. KELLY, M.D., F.A.C.R., professor of radiology, Creighton University ; with the collaboration of D. ARNOLD DowELL, M.D., assistant professor of radiology in the university. Chicago : Year Book Publishers ; London : H. K. Lewis. Pp. 432. 33s. THIS book fills a gap in medical literature. Its authors recognise the importance of X-ray treatment of the infections and have put together for the first time in book form the fruits of their own experience and that of many others. The first part of the book deals with physical and biological considerations and here their guidance is less sure. Their reference to protection, for instance, runs : " All sources of secondary radiation should be ascer- tained and adequate means of protection provided so far as it is possible to do so " ; and under the heading " Training not always necessary for success," they state that infections " may be treated by any physician familiar with the operation of X-ray apparatus, - the definition of an r unit, and the disease he is treating "-an odd statement in itself, and a dangerous one in its implications (the definition of the roentgen given in the text is not that which has now been accepted internationally). The second part of the book deals with the treatment of, periton,itis, parotitis, pneumonia and other infections, the main section being an informative account of the treatment of gas gangrene of which the authors were the pioneers. They make a good case for the further investigation of this type of treatment, though many of their assertions are con- troversial. They rightly stress the value of X-ray treat- ment in postoperative parotitis and similar infections in which this method of treatment deserves further trial. Probably a portable X-ray therapy plant for the treatment of infections will one day form a- recognised part of the equipment of all large general hospitals. The Injured Back and its Treatment Editor: JOHN D. ELLIS, M.D. London: Baillière, Tindall and Cox. Pp. 377. 30.9. Tms collection of nine papers by eminent American orthopsedists deals with the common minor injuries as well as the more serious fractures and dislocations, with and without cord involvement. The views expressed are orthodox and set out clearly. A chapter on back- ache as a symptom of visceral disease might have been more at home in a less practical manual but is welcome all the same. Proper stress is laid on a systematic examination of the back ; after reading this chapter most doctors will feel that their previous efforts have been somewhat sketchy, and that there is much more to be learned from a complete examination than they had realised. The role of the articular facets in causing back pain is discussed-a syndrome which has not yet received much notice in this country but one described as being fairly common. The editor has minimised overlap and maintained continuity; there are no significant omissions. Synopsis of Blood Diseases A. PINEY, M.D. Birm., M.R.C.P., physician to St. Mary’s Hospital for Women and Children, Plaistow. London: Wm. Heinemann (Medical Books). Pp. 120. 10s. 6d. Dr. Piney presents an up-to-date summary of our knowledge of blood diseases without going into detail about the changes in the blood-picture. It will be especially useful to the postgraduate student with an adequate background who wants to revise the subject quickly, but it is probably too sketchy to help the general practitioner without such a background. The main difficulty in blood diseases is differential diagnosis and for this a more detailed description of the results of haematological examination than Dr. Piney gives is needed. The treatments advocated are on sound and balanced lines and reflect modern practice, though the use of.fortified liver extract occurs in several unexpected places. The four colour plates illustrate blood and bone- marrow cells in a rather unconventional way that is hardly convincing and are unlikely to help the average physician for whom the book is intended ; the same must be said of the extensive tables of the characteristics of the various types of cells. Nevertheless this book will have its place as a quick " brush-up your blood diseases."