88
Dr. Gitalisa Andayani, SpM Department of Opthalmology F K UI/R S C M 1 SUMMARY OF EYE PROBLEMS
Dr. G ita lis a Andayani, S pMDepartment of Opthalmology
FKUI/RS CM1
SUMMARY OF EYE
PROBLEMS

EYE PROBLEMS
• Red eyes (normal and decreased vision) • Chronic visual (progressive) loss• Acute visual (persistent) loss• Trauma• Abnormalities in ocular alignment and
motility• Refractive disorders

- Congestion of conjunctival blood vessels- If clarity of media disturbedvision decreased
- In developing countries accounts for 40% eye problems
RED EYES
Red Eyes, normal vision
Conjunctivitis (bacterial/viral/chlamidyal/allergic)
Pterygium Subconjunctival hemorrhage Episcleritis and scleritis

CONJUNCTIVITISClinical presentation Nonspecific:
watery eyes, irritation, stinging, foreign body sensation, photophobia or itchiness
Discharge: watery, mucoid, purulent or mucopurulent
Conjunctival injection Eyelid swelling Tarsal conjunctiva:
papillae/follicles/membrane Cornea and pupils usually normal

CONJUNCTIVITIS

CONJUNCTIVITIS

CONJUNCTIVITIS
Conjunctivitis Bacterial Conjunctivitis
Chlamidial conjunctivitis (trachoma) Allergic/vernal conjunctivitis

CONJUNCTIVITISManagement
- Can be done by GP
- Eye hygiene
- Eyedrops:
viral self-limiting, antibiotics
bacterial antibiotics
allergic/vernal antiallergy, steroids(!)
- 3 days w/o improvement: refer
PTERYGIUM
• growth of triangular fibrovaskular tissue invading the cornea
• patients in hot climate, chronic dryness and high sunlight exposure
• difference from pinguekula: yellow-white deposit at nasal/temporal from limbus (collagen degeneration, calcification)
• apex always in the cornea side, often with Fe deposits

PTERIGIUM
PTERYGIUM
Management:
• Excision with conjuctical graft
• Lamellar keratoplasty

SUBCONJUNCTIVAL HEMORRHAGE
• No pain, no discharge
• Well-demarcated
• Self-limiting within 2 weeks

EPISCLERITIS AND SCLERITIS
• Sclera covered by 3 vascular layers:
- Conjungtival blood vessels
- Superfisial episcleral vessels
(in Tenon layer);
with phenilephrin: blanching
- Deep vascular plexus
EPISCLERITIS AND SCLERITIS
Episcleritis:
• common, benign, self-limiting
• young adult
• related to systemic disease
• types: - simple (sectoral,diffuse)
- nodular

EPISCLERITIS AND SCLERITIS
Scleritis:
• granulomatous inflammation
• rheumatoid arthritis, connective tissue disorder
• less common
• severity: mild-severe (necrotizing)• types: - anterior scleritis (non-necrotizing / necrotizing)
- scleritis posterior

EPISCLERITIS AND SCLERITIS
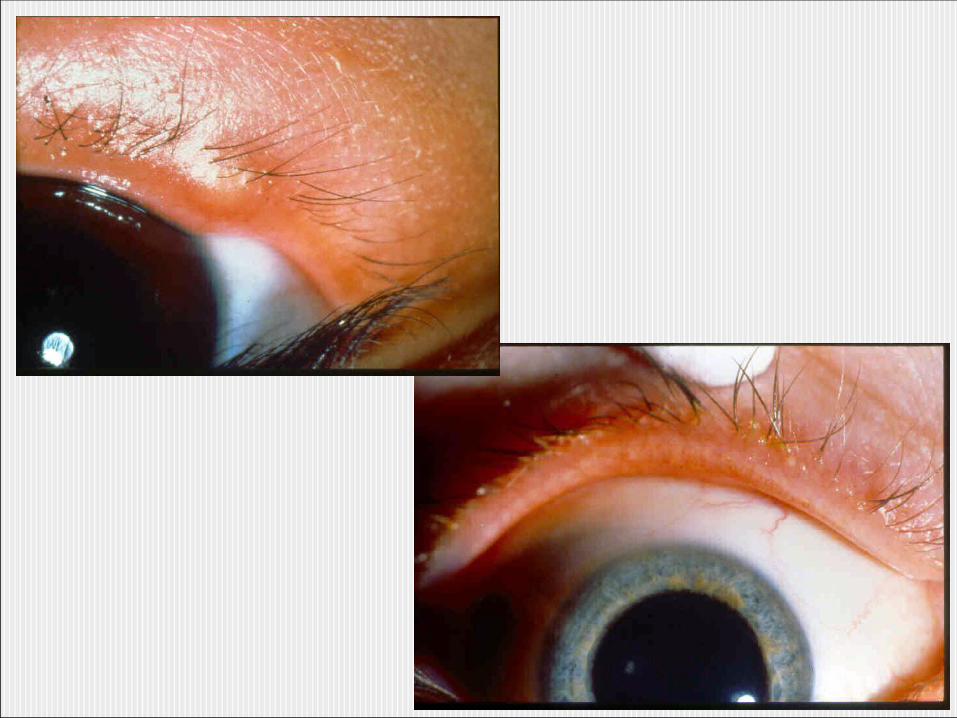
Simple, sectoral episcleritis non-necrotizing, diffuse scleritis
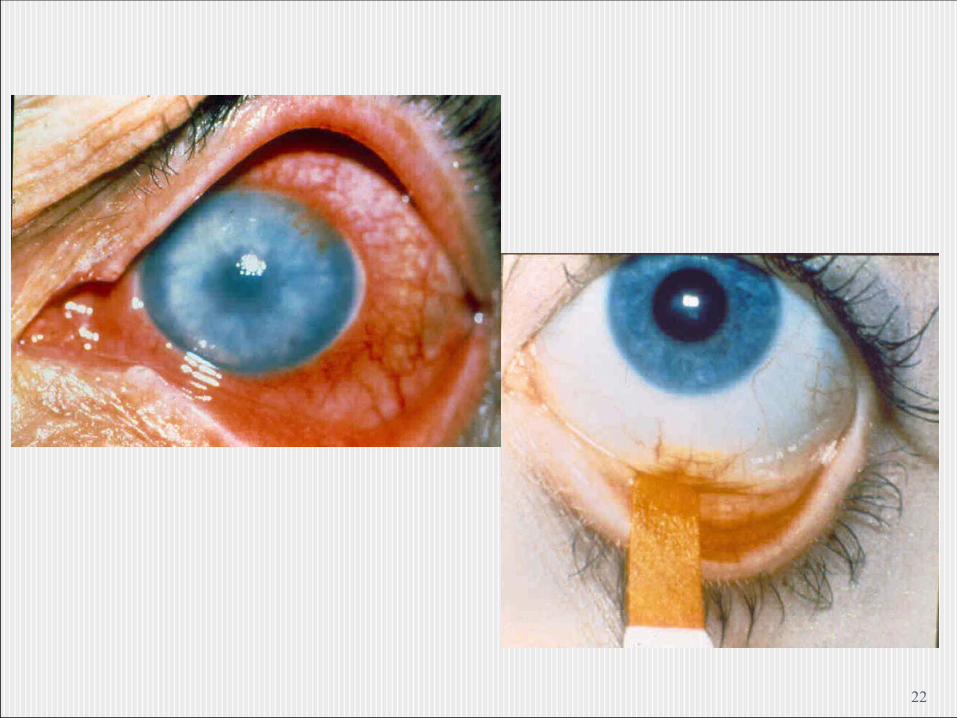
early necrotizing scleritis Scleral necrosis
Episcleritis and Scleritis
Management:Episcleritis - Steroids/NSAID eyedrops
- Systemic ibuprofen/flurbiprofen
Scleritis- Oral NSAID
- Oral Steroid
- Combination
19

20

21
22

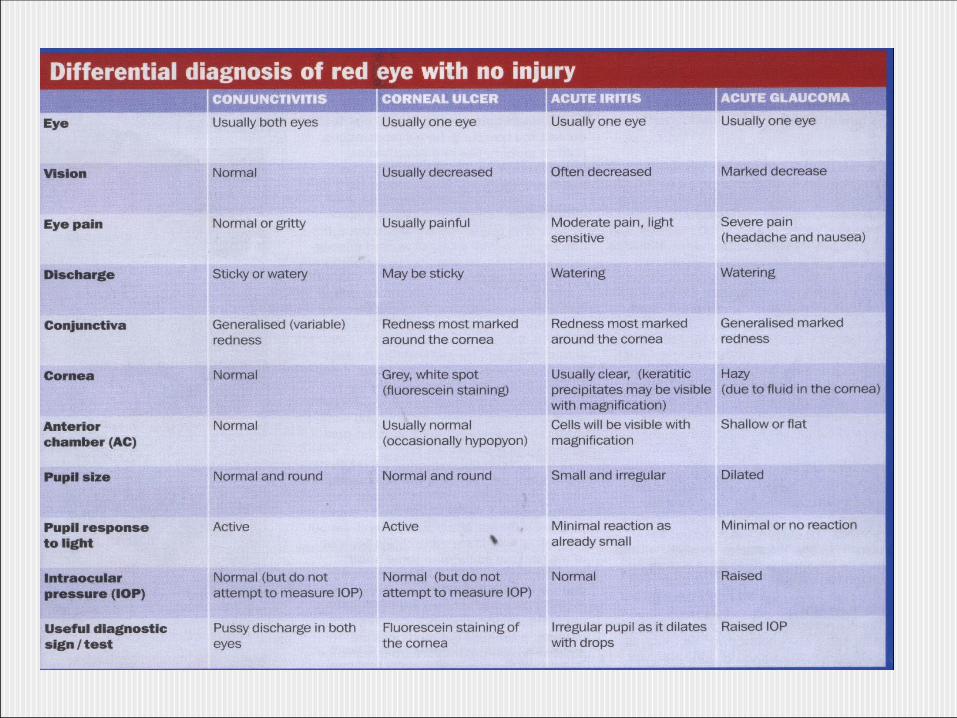
Red Eyes, Decreased Vision
Keratitis
Cornea Ulcer
Anterior Uveitis (iritis, iridocyclitis)
Acute Glaucoma
Endophthalmitis
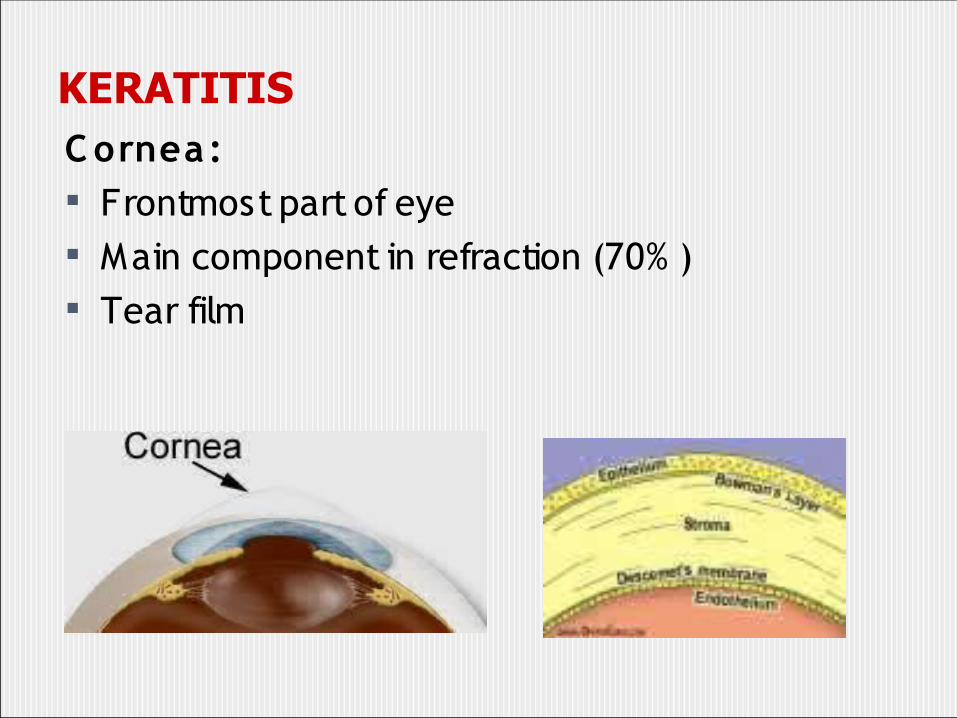
KERATITISC ornea: Frontmost part of eye Main component in refraction (70% ) Tear film

KERATITIS
Keratitis: Inflammatory cells infiltration Corneal opacity Superficial / deep Cause: Infection (Viral/bacterial/fungal) Also: Dry eyes, trauma, drug toxicity, UV exposure,
contact lens irritation, allergy, immunogenic states, chronic conjunctivitis
May progress to cornea ulcer
KERATITIS-CORNEAL ULCER
Clinical presentation
- photophobia
- periocular pain
- foreign body sensation
- ciliary flush
- corneal opacity
Diagnosis : - reduced cornea sensibility
- fluorescein test
- assessment of corneal regularity
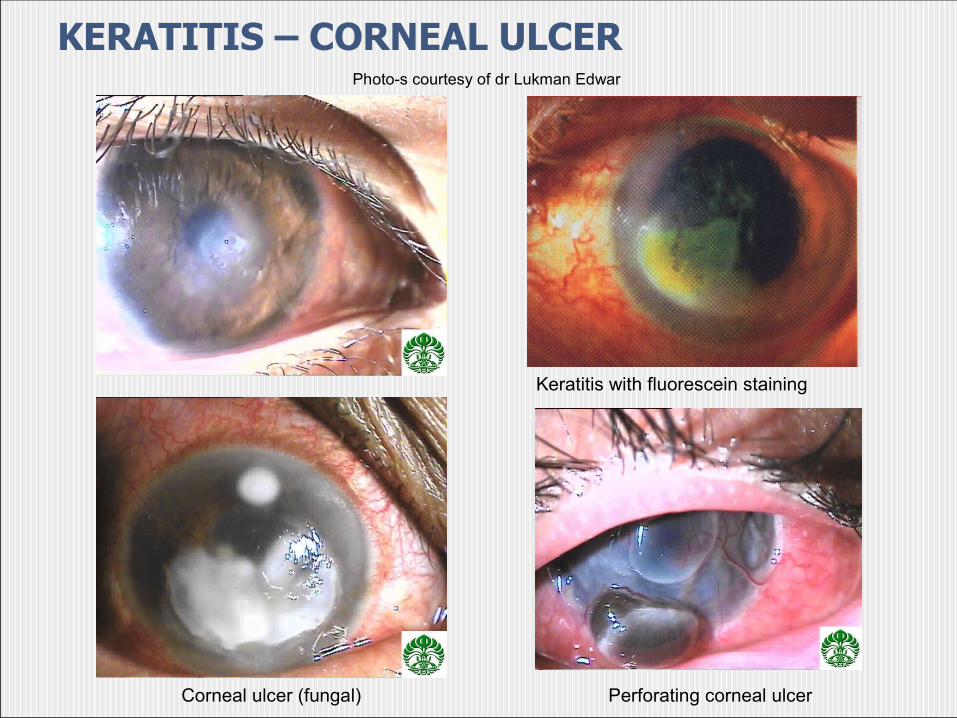
KERATITIS – CORNEAL ULCER
Keratitis with fluorescein staining
Corneal ulcer (fungal) Perforating corneal ulcer
Photo-s courtesy of dr Lukman Edwar

Corneal Ulcer
Cause Pseudomonas Strepcococcus pneumonia
Virus Fungi Allergy
Location central central central central central
Excavation + + - - -
Color greenish yellow yellow abcess satelites infiltrates
Hypopion + + -/+ + -
Appearence purulent discharge purulent discharge
quiet abcess Diffuse
Sensibility normal normal decreased increased normal
Perforation frequent frequent rare frequent none
KERATITIS – CORNEAL ULCER
Management:
- Refer to ophthalmologist
- Medication based on causative microorganism
virus antiviral
bacteria antibiotics
fungi antifungal
- Corneal scar

ANTERIOR UVEITIS
• Inflammation of iris and ciliary body• Usually auto-immune• Isolated or part of systemic condition:
- ankylosing spondilitis- juvenile rheumatoid arthritis- Reiter Syndrome- sarcoidosis- herpes simpleks- herpes zoster- Behçet Syndrome (with stomatitis aftosa)

ANTERIOR UVEITIS
Clinical presentation:- periocular pain- photophobia- usually mild decrease of vision- ciliary flush- small, irregular pupil, due to adhesion to
lens surface permukaan lensa

ANTERIOR UVEITIS
Clinical presentation:- indistinct iris crypts- cornea opacity- cells and flare in AC keratic precipitates, hypopion- IOP changes

Posterior synechia
Iris nodules
Hypopion
ANTERIOR UVEITISPhoto-s courtesy of dr Lukman Edwar
Normal iris
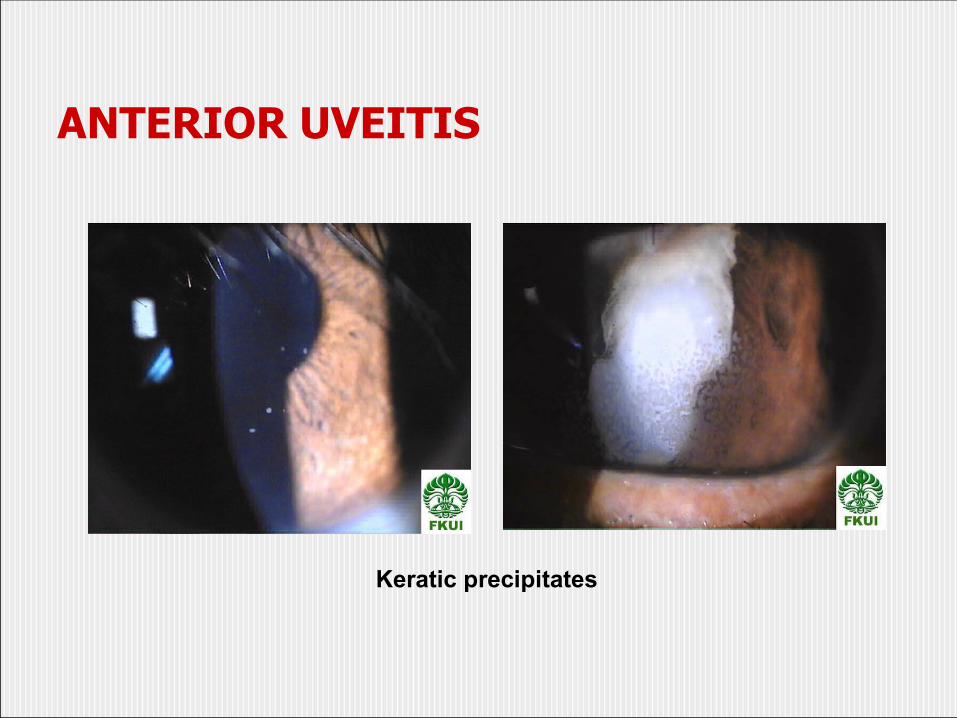
ANTERIOR UVEITIS
Keratic precipitates

ANTERIOR UVEITIS
Management:- Refer to Ophthalmologist- Work-up- Medication: - cycloplegics eyedrops - corticosteroids eyedrops - oral corticosteroids oral (prn) - Glaucoma drugs

ACUTE GLAUCOMA
• ocular emergency• sudden IOP elevation• block of aqueous humor outflow• elder patients• Asians >>
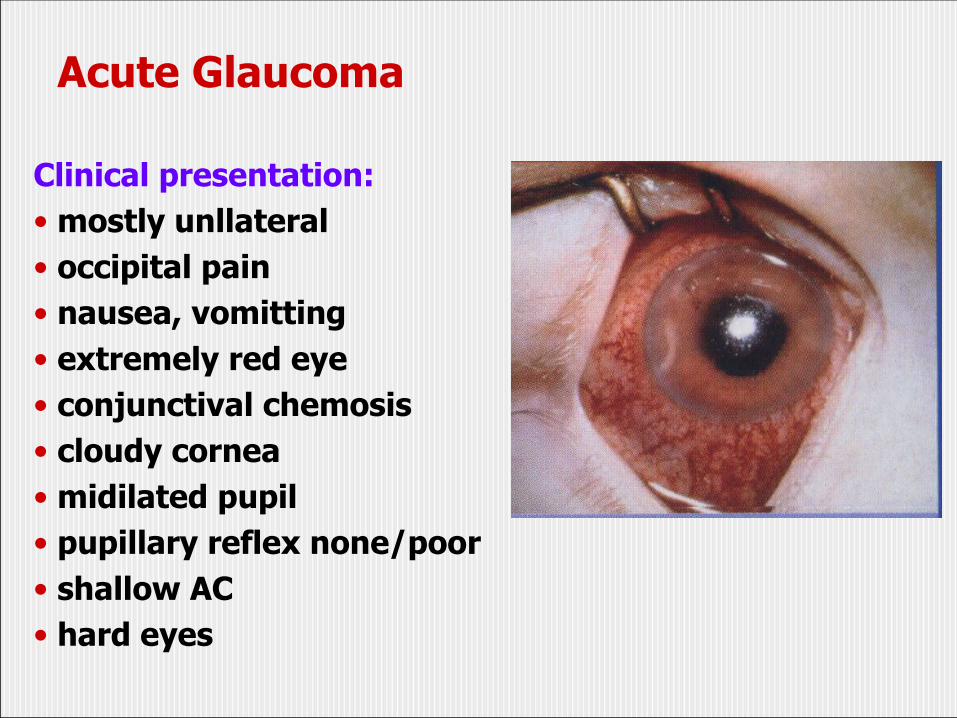
Acute Glaucoma
Clinical presentation:• mostly unllateral• occipital pain• nausea, vomitting• extremely red eye• conjunctival chemosis• cloudy cornea• midilated pupil• pupillary reflex none/poor• shallow AC• hard eyes
38

Acute Glaucoma
Management:- Refer to ophthalmologist- Immediately lower IOP: Pilocarpine 2% Timolol 0.5% Asetazolamid Oral glycerin /IV manitol surgery / laser iridotomy

ENDOPHTHALMITIS
• Purulent intraocular infection• Caused by infection through the cornea, trauma post-surgery (mainly: cataract surgery), or endogenous• Bacterial/fungal• Most common: staphylococcus aureus, proteus and pseudomonas• If with extraocular infection: panophtalmitis

Endophthalmitis
Clinical presentation:- periocular pain - chemosis - eyelid swelling- corneal opacity- anterior uveitis- hypopion

Endophthalmitis
Management:- Refer to ophthalmologist- Aqueos / vitreous tap- intravitreal antibiotic/antifungal- systemic antibiotic - Panoftalmitis: evisceration
Chronic visual loss
cataract
glaucoma (chronic: open and closed angle)
Retinopathies (mainly: diabetic retinopathy)
Macular Degeneration
(AMD=age-related macular degeneration) Others: e.g. retinitis pigmentosa

Cataract
Lens opacity Penyebab:
- degeneration: senile/age-related- complication of ocular disease / metabolic / drug-induced(komplikata)- congenital- traumatic
cataract

Cataract
Symptoms Early
- no symptoms- fog- glare- difficulty in reading
Late- blur of vision- leucocoria

CataractManagement Depend on patient’s demand; if interfering
with daily activity: Cataract surgery
Technique:- Intracapsular Cataract Extraction(ICCE) now rarely done- Extracapsular Cataract Extraction(ECCE)- Phacoemulsification- Small-incision
Phacoemulsification

Glaucoma
• Optic neuropathy, mainly caused by chronic IOP elevation due to increased outflow resistance• visual field defects• 2 types: - open angle glaucoma
- closed angle glaucoma
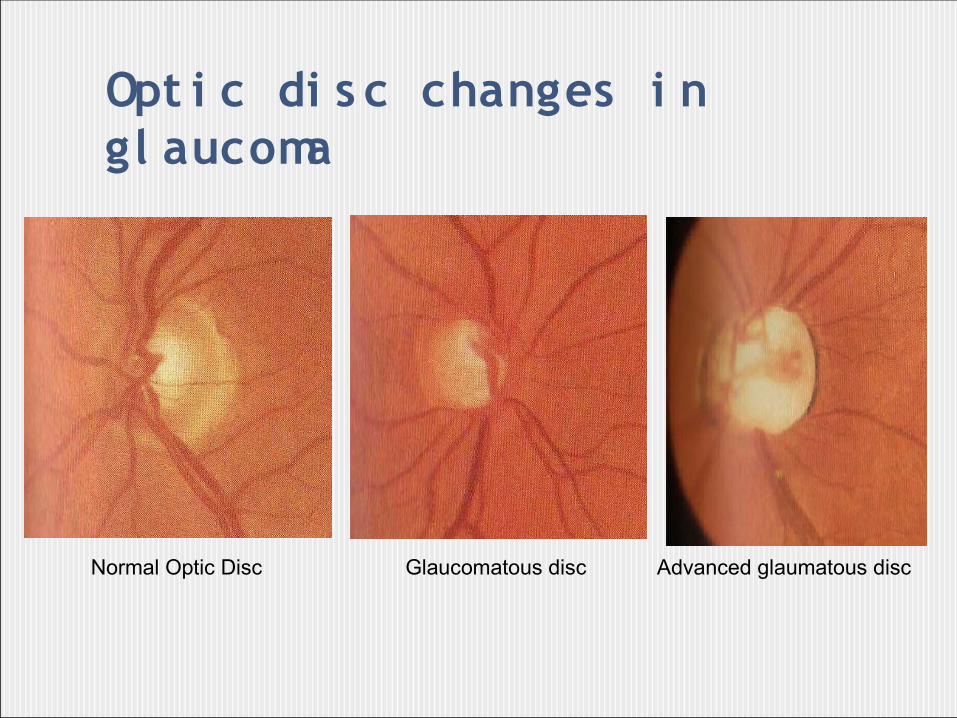
Opt i c di s c changes i n gl aucoma
Normal Optic Disc Glaucomatous disc Advanced glaumatous disc

Glaucoma
Symptoms • IOP > 21 mmHg (normal 10-21)• Open angle: asymptomatic; if there is indicating late stages (frequently bumping, rainbow halo, periocular pain)• Closed angle: predisposition to acute glaucoma• Constricted visual field

Glaucoma
Management• Observation• Glaucoma drugs: - beta-blocker
- acetazolamid - pilocarpine
• Laser (iridotomy, trabeculotomy, trabeculoplasty)• Surgery (iridectomy, trabeculektomy, implant)
RETINOPATHIES
N on-inflammatory retina dis orders
2 mos t c ommon:
- hypertensive retinopathy
- diabetic retinopathy

Retina anatomy
Sklera
Koroid
Membran Bruch
RPE=epitel
pigmen retina
Fotoreseptor
Lapisan serabut saraf

Hypertensive retinopathy
• caused by chronic hypertension• depend on onset• - Grade I: narrowing of vessels - Grade II: + narrowing of veins at crossing - Grade III: + intraretinal hemorrhages, exudates - Grade IV: optic disc edema, star figured
macular exudates

55
Hypertensive retinopathy
Cotton-wool spots and macular star
Disc oedema
Focal Generalized
Arteriolar constriction
Extravascular signs
Flame-shaped retinal haemorrhages
Arteriolosclerosis (A-V changes)

56
Grading of arteriolosclerosis

Diabetic retinopathy
Complication of diabetesComplication of diabetes Chronic hyperglycemiaChronic hyperglycemia damage to microvasculars Chronic visual lossChronic visual loss Main cause of blindness in DM 50% of diabetics within 10 yrs will have retinopathy

Mekanisme kebutaan pada diabetic retinopathy
leakage of exudates, lipid and blood to the retina
Macular edeme
Decreased blood flow to the retina
iskemia
neovascularization PDR
-vitreous hemorrhage- Fibrovascular scar
- retinal traction retinal detachment
7

Diabetic retinopathy
7
Normal retina
PDR vitreuous hemorrhage Fibrovascular scar in PDR
Early PDR FFA
NPDR

AMD=age-related macular degeneration
7
• Chronic visual loss caused by changes of the macula
• bilateral
AMD=age-related macular degeneration
7
• Problem world wide
• 4 th in global cause blindness
• Treatment:
- Photodynamic therapy
- Anti-VEGF
- others

Acute (persistent) visual loss
retinal detachment
vitreous hemorrhage
retinal vein occlusion
Retinal artery occlusion
Optic neuritis
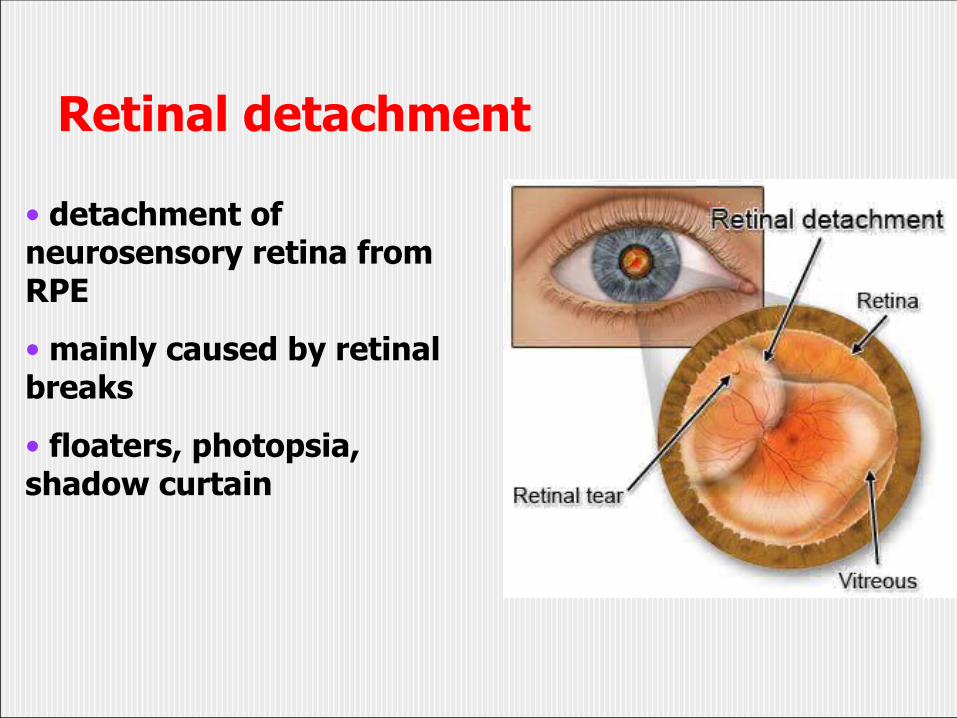
Retinal detachment
• detachment of neurosensory retina from RPE
• mainly caused by retinal breaks
• floaters, photopsia, shadow curtain

retinal detachmentManagement• pneumatic retinopexy• vitreoretina surgery
- Scleral buckling- Vitrectomy
Scleral buckling (SB) Vitrectomy

Vitreous hemorrhage
• Blood in the vitreous
• Rupture of blood vessels
• Cause: trauma, retinal breaks, DM, hypertension
• On examination: fundus reflex absent
• Vitrectomy maybe needed
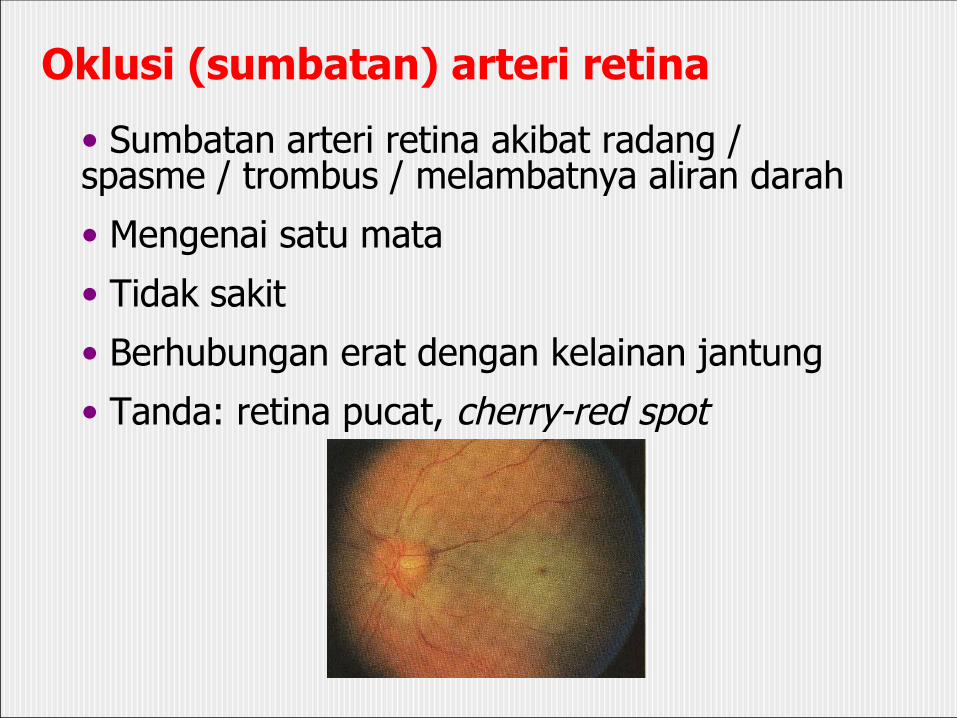
Oklusi (sumbatan) arteri retina
• Sumbatan arteri retina akibat radang / spasme / trombus / melambatnya aliran darah
• Mengenai satu mata
• Tidak sakit
• Berhubungan erat dengan kelainan jantung
• Tanda: retina pucat, cherry-red spot

Retinal vein occlusion
• Central/branch
• Unilateral
• Painless
• Systemic risk factors
• flame-shaped hemorrhages, cotton wool spots

Optic neuritis• inflammation/intoxication/demyelination of the optic nerve
• may be accompanied by pain
• unilateral
• sluggish pupil reflex, RAPD +

OCULAR TRAUMA
• Chemical/thermal burn• Corneal erosion• Corneal and conjunctival foreign body• Blunt trauma• Penetrating/perforating trauma• Hyphema• Intraocular foreign body• Orbital wall fracture

Chemical burn
• Alkali:- pestisides- household products (cleaners, etc)
• Asam (acid):- batteries
→ damage to cornea• Thermal:
- flame- hot water- metal liquid, etc
→ usually milder
Chemical burn
Penatalaksanaan:
• immediate
• topical anesthetics
• Corneal edema/chemosis? Opacity?
• Irigate eyeball with 1-2 liter water/ NaCl
Chemical burn
Managenment
• Clean the eyelid sac from debris
• Topical medications (steroid+antibiotics,
EDTA, tetracycline)
• Bandage lens if necessary
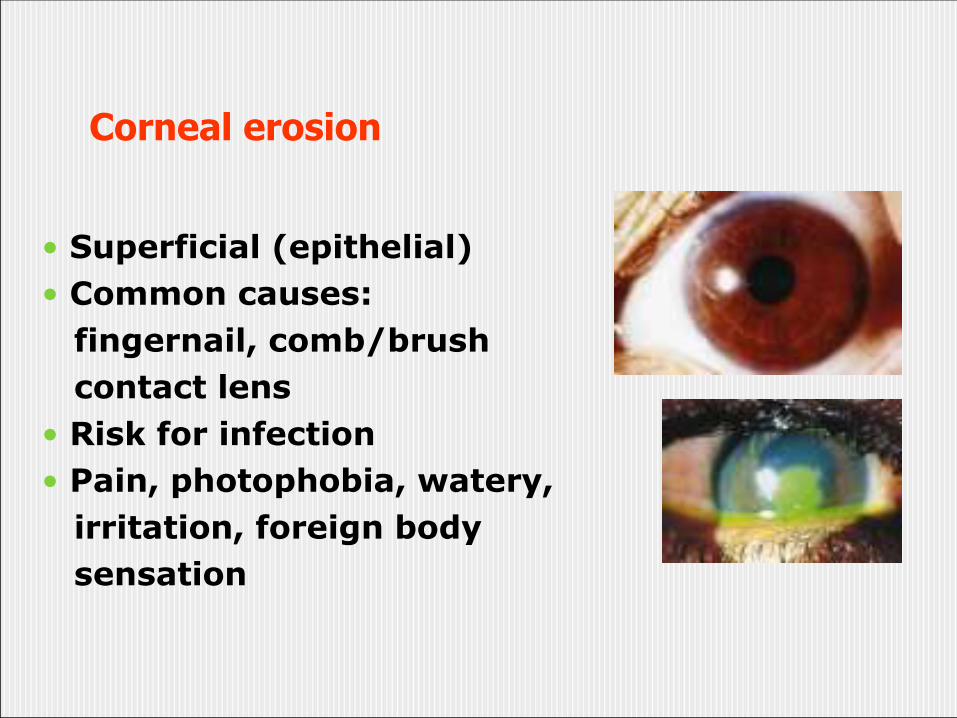
Corneal erosion
• Superficial (epithelial)• Common causes: fingernail, comb/brush contact lens• Risk for infection• Pain, photophobia, watery, irritation, foreign body sensation

Corneal erosion
Management:• Topical anesthetics• Fluorescein test• Check tarsal conjunctiva of upper eyelid
→ retained foreign body? • Antibiotics eyedrop• Bandage lens/patching• Re-epithelisation) within 24-48 jam

Conjunctival/corneal foreign body
Conjunctival foreign body Corneal foreign body
• Dust, occupational, etc• Photophobia, watery, foreign body sensation• Management: foreign body extraction
Blunt trauma
• Eyelid hematoma
• Hyphema
• Subconjunctival hemorrhage
• Vitreous/Retinal hemorrhage
• Orbital fracture
• Retinal commotion

Blunt trauma
Hematoma + subconjunctival subhemorrhage RE
(good eye movement)

Hyphema
Hyphema(clotting) Hyphema occupying ½ AC
Full hyphema
Hyphema
Management:
• hospitalization (risk: visual loss, IOP
elevation, re-bleeding in 30% cases)
• bed-rest, semi-fowler position
• tranexamic acid (e.g Transamin)

Lens subluxation

Iridodialisis

Kommosio retina
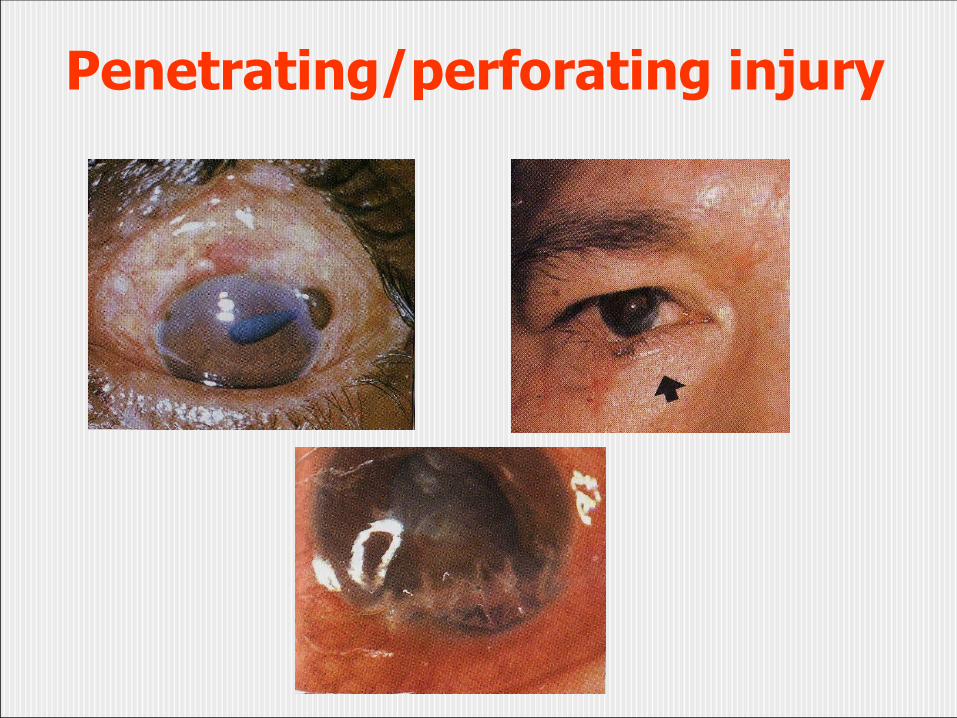
Penetrating/perforating injury
Penetrating/perforating injury
Management:
• refer to ophthalmologist
• antibiotics eyedrop
• oral antibiotics
• ATS, TT
• patch eyes
• primary repair

Laceration/ruptur of eyelid and face
- ATS, TT
- NaCl / Betadine compress
- Immediate repair
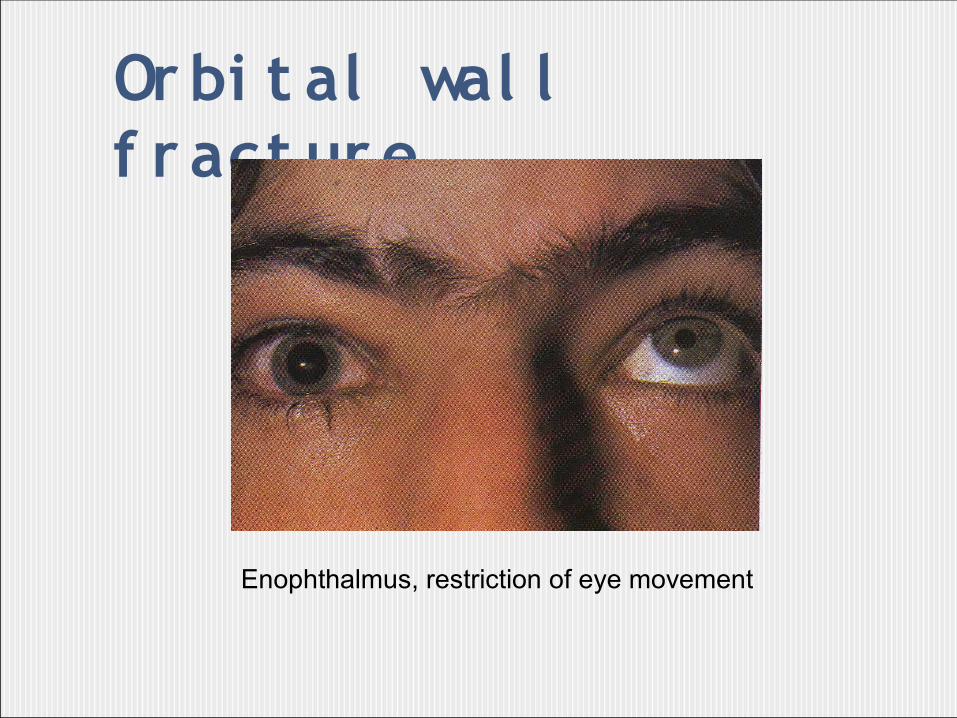
Or bi t al wal l f r act ur e
Enophthalmus, restriction of eye movement

I nt r aocul ar f or ei gn bi dy
Management:
-Immediate extraction for foreign body
-Oral and intravitreal foreign body
-Corticosteroids


















