PROFILE 1 Masters of Esthetic Dentistry FIBER-REINFORCED INLAY FIXED PARTIAL DENTURES: MAXIMUM PRESERVATION OF DENTAL HARD TISSUE Felix Lutz, MD, DMD, PhD Dr. Felix Lutz - ____._ Cumnt Occupation Full-time Academic Faculty, University of Zurich, Dental Institute. Clinic of Preventative Dentistry, Periodontology, and Cariology Education MD (1969) DMD (1972) PhD in Dentistry (1982) Affiliations Professor and Chairman, Department of Preventative Dentistry, Periodontology, and Cariology Fellowships Academy of Dental Materials, Academy of Operative Dentistry, IADR, SSO, SSP, SVPR Professional Memberships International Association for Dental Research Academy of Operative Dentistry Academy of Dental Materials Swiss Dental Society (SSO) Swiss Society for Preventative and Restorative Dentistry (SVPR) Publications Three books (in German) in accordance with the newly adopted Swiss Quality Guidelines (tooth-colored direct posterior restorations, tooth-colored indirect restorations, and tooth-colored anterior restorations) Research Projects Noninvasive restorations. fiber-free resin-based inlay fixed partial dentures, new approach in pulp-capping Till N. Gohring, DMD he teeth adjacent to a single- T tooth edentulous area fre- quently may have one-, two-, or three-surface restorations, or have initial dental carious lesions.’ In this clinical situation, a single miss- ing tooth can be restored with a * conservative inlay-anchored bonded fixed partial denture (IFPD).2,3 The anticipated durable resolution to this problem may now be a reality with the recent advances in glass fiber-reinforced composite technol- ogy and the use of a carefully exe- cuted bonding te~hnique.~ A glass fiber-reinforced composite system comprising prefabricated glass fiber reinforcement elements and processing and curing equipment (Targis-Vectris, Ivoclar, Schaan, Principality of Liechtenstein) was introduced in 1996.4 Using a simi- lar system, a recent in vitro study reported high fracture strength of approximately 700 N of fiber- reinforced adhesive IFPDS.~ High marginal quality also has been achieved in vitro and ~linically,~.’ using a high-viscosity insertion technique with restoration compos- ite (TetridTetric-Ceram, Vivadent, Schaan, Principality of Liechtenstein), ultrasonic power (Mini Piezon with SP Tip, Electro Medical Systems [EMS], Nyon, Switzerland), and a selective bonding technique. MATERIALS AND METHODS Between March 1997 and January 1999,60 glass fiber-reinforced com- posite IFPDs were inserted. Patients were instructed verbally and in writ- ing about the materials and tech- nique used to restore missing teeth. Informed consent was obtained from all patients. The Ethics Com- mittee of the University of Zurich approved the study. All patients submitted to a comprehensive oral diagnosis, including dental, peri- odontal, functional, and radiologic examinations, prior to treatment. An average of 14.6 months after IFPD insertion, 18 patients (25 IFPDs) were examined. The 2-year post-procedure examinations of the patients started in May 1999 and are still in progress. 164 JOURNAL OF ESTHETIC DENTISTRY
Transcript
PROFILE 1 Masters of Esthetic Dentistry
FIBER-REINFORCED INLAY FIXED PARTIAL DENTURES: MAXIMUM PRESERVATION OF DENTAL HARD TISSUE
Felix Lutz, MD, DMD, PhD Dr. Felix Lutz - ____._
Cumnt Occupation Full-time Academic Faculty, University of Zurich, Dental Institute. Clinic of Preventative Dentistry, Periodontology, and Cariology
Education MD (1969) DMD (1972) PhD in Dentistry (1982)
Affiliations Professor and Chairman, Department of Preventative Dentistry, Periodontology, and Cariology
Fellowships Academy of Dental Materials, Academy of Operative Dentistry, IADR, SSO, SSP, SVPR
Professional Memberships International Association for Dental Research Academy of Operative Dentistry Academy of Dental Materials Swiss Dental Society (SSO) Swiss Society for Preventative and Restorative Dentistry (SVPR)
Publications Three books (in German) in accordance with the newly adopted Swiss Quality Guidelines (tooth-colored direct posterior restorations, tooth-colored indirect restorations, and tooth-colored anterior restorations)
Research Projects Noninvasive restorations. fiber-free resin-based inlay fixed partial dentures, new approach in pulp-capping
Till N. Gohring, DMD
he teeth adjacent to a single- T tooth edentulous area fre- quently may have one-, two-, or three-surface restorations, or have initial dental carious lesions.’ In this clinical situation, a single miss- ing tooth can be restored with a
* conservative inlay-anchored bonded fixed partial denture (IFPD).2,3 The anticipated durable resolution to this problem may now be a reality with the recent advances in glass fiber-reinforced composite technol- ogy and the use of a carefully exe- cuted bonding te~hnique.~
A glass fiber-reinforced composite system comprising prefabricated glass fiber reinforcement elements and processing and curing equipment (Targis-Vectris, Ivoclar, Schaan, Principality of Liechtenstein) was introduced in 1996.4 Using a simi- lar system, a recent in vitro study reported high fracture strength of approximately 700 N of fiber- reinforced adhesive IFPDS.~ High marginal quality also has been achieved in vitro and ~linically,~.’ using a high-viscosity insertion
technique with restoration compos- ite (TetridTetric-Ceram, Vivadent, Schaan, Principality of Liechtenstein), ultrasonic power (Mini Piezon with SP Tip, Electro Medical Systems [EMS], Nyon, Switzerland), and a selective bonding technique.
MATERIALS A N D METHODS
Between March 1997 and January 1999,60 glass fiber-reinforced com- posite IFPDs were inserted. Patients were instructed verbally and in writ- ing about the materials and tech- nique used to restore missing teeth. Informed consent was obtained from all patients. The Ethics Com- mittee of the University of Zurich approved the study. All patients submitted to a comprehensive oral diagnosis, including dental, peri- odontal, functional, and radiologic examinations, prior to treatment.
An average of 14.6 months after IFPD insertion, 18 patients (25 IFPDs) were examined. The 2-year post-procedure examinations of the patients started in May 1999 and are still in progress.
164 J O U R N A L OF ESTHETIC D E N T I S T R Y
M A S T E R S OF E S T H E T I C D E N T I S T R Y
T O O T H PREPARATION OF A B U T M E N T S
The design of each IFPD followed the philosophy of maximal preserva- tion of sound tooth substance. Pre- existing restorations were removed and their cavity preparations were used for retention in the tooth abut- ments (Figure 1). In cases of primary carious lesions, cavity preparation was minimally invasive, but ade- quate for inlay retention. Dental caries was excavated and gross tooth preparations were made using 80-pm diamond burs (No. 8113R, No. 8113NR Intensiv SA, Viganello, Switzerland). All the dentin surfaces of the cavity preparations were sealed with a threetomponent enamel-dentin adhesive system . ( Syntac-Classid-ieliobond,
Vivadent). Later, for insertion, the restorations were bonded selectively to the cavity margins. In practice, this procedure has various advantages. First, the dentin is sealed and protected immediately after prepara- tion; therefore, postoperative sen- sitivity during temporization can be virtually eliminated. Second, the con- figuration-factor (C-factor): the ratio of bonded to free unbonded restora- tion surfaces, can be reduced using a selective bonding techniq~e.~.~ The third advantage of selective bonding is the protection of the dentin: in the case of marginal imperfections, the adhesive functions as a second barrier against the penetration of bacteria into the dentin. Fourth, it is difficult to replace a failed inserted restoration with total bonding.'O
Extensively undermined cusps were strengthened with fine hybrid com- posite (Tetric-Ceram, Vivadent). The cavity margins were finished occlusally with diamond-coated (25 pm) finishing diamond burs (3113R, 3117, Intensiv). The cavity margins of the proximal boxes were finished using ultra- sonic diamond-coated instruments (VIP-Set 4294, Komet, Besigheim, Germany) and an ultrasonic power unit (Mini Piezon, EMS). The shape of the diamond-coated tips activated by ultrasonic power automatically generated a 15-degree bevel at the cervical margins. After an elastomeric impression was obtained:,' all tooth preparations were restored with provisional IFPDs made of
Figure 1 . A, Common single-tooth edentulous area. B, Rubber dam placed before preparation. C , Amalgam removed, with care taken to avoid losing more tooth hard tissue than necessary.
V O L U M E 12 , N U M B E R 3 , 2000 165
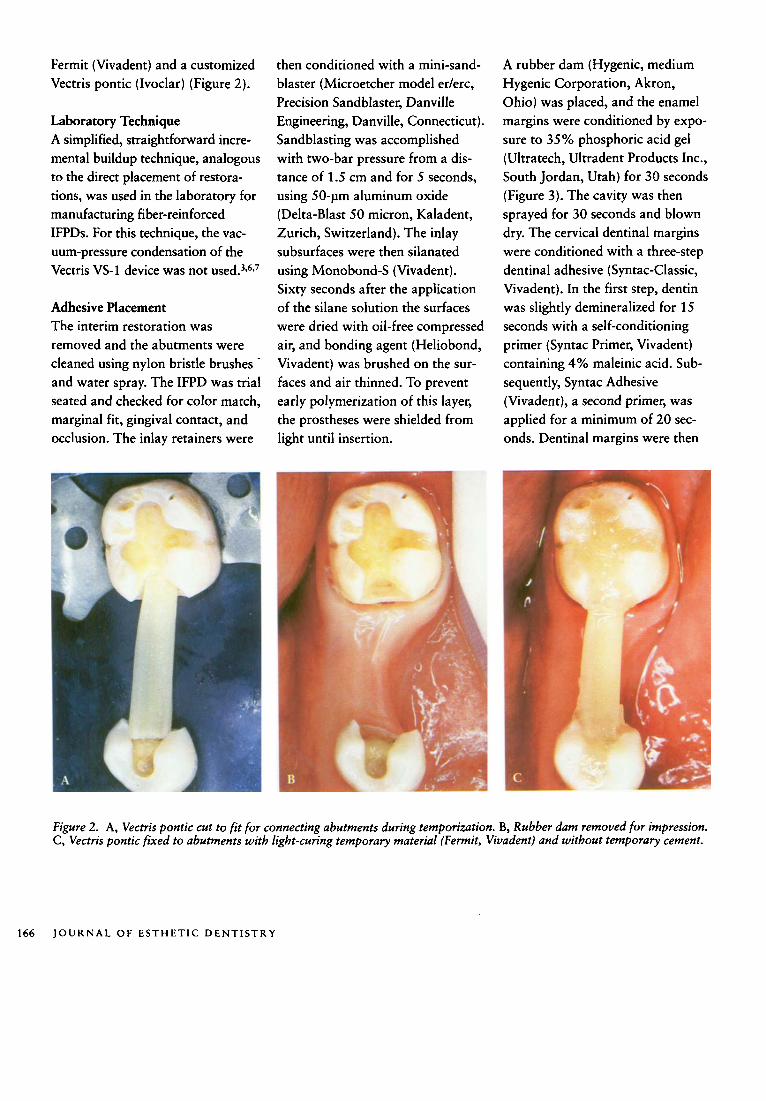
Fermit (Vivadent) and a customized Vectris pontic (Ivoclar) (Figure 2).
Laboratory Technique A simplified, straightforward incre- mental buildup technique, analogous to the direct placement of restora- tions, was used in the laboratory for manufacturing fiber-reinforced IFPDs. For this technique, the vac- uum-pressure condensation of the Vectris VS-1 device was not ~sed .~ ,~ , ’
Adhesive Placement The interim restoration was removed and the abutments were cleaned using nylon bristle brushes and water spray. The IFPD was trial seated and checked for color match, marginal fit, gingival contact, and occlusion. The inlay retainers were
then conditioned with a mini-sand- blaster (Microetcher model er/erc, Precision Sandblaster, Danville Engineering, Danville, Connecticut). Sandblasting was accomplished with two-bar pressure from a dis- tance of 1.5 cm and for 5 seconds, using SO-pm aluminum oxide (Delta-Blast 50 micron, Kaladent, Zurich, Switzerland). The inlay subsurfaces were then silanated using Monobond-S (Vivadent). Sixty seconds after the application of the silane solution the surfaces were dried with oil-free compressed air, and bonding agent (Heliobond, Vivadent) was brushed on the sur- faces and air thinned. To prevent early polymerization of this layer, the prostheses were shielded from light until insertion.
A rubber dam (Hygenic, medium Hygenic Corporation, Akron, Ohio) was placed, and the enamel margins were conditioned by expo- sure to 35% phosphoric acid gel (Ultratech, Ultradent Products Inc., South Jordan, Utah) for 30 seconds (Figure 3). The cavity was then sprayed for 30 seconds and blown dry. The cervical dentinal margins were conditioned with a three-step dentinal adhesive (Syntac-Classic, Vivadent). In the first step, dentin was slightly demineralized for 15 seconds with a self-conditioning primer (Syntac Primer, Vivadent) containing 4% maleinic acid. Sub- sequently, Syntac Adhesive (Vivadent), a second primer, was applied for a minimum of 20 sec- onds. Dentinal margins were then
Figure 2. A, Vectris pontic cut to fit for connecting abutments during temporization. B, Rubber dam removed for impression. C , Vectris pontic fixed to abutments with light-curing temporary material (Fermit, Vivadent) and without temporary cement.
166 J O U R N A L OF E S T H E T I C D E N T I S T R Y
M A S T E R S OF E S T H E T I C D E N T I S T R Y
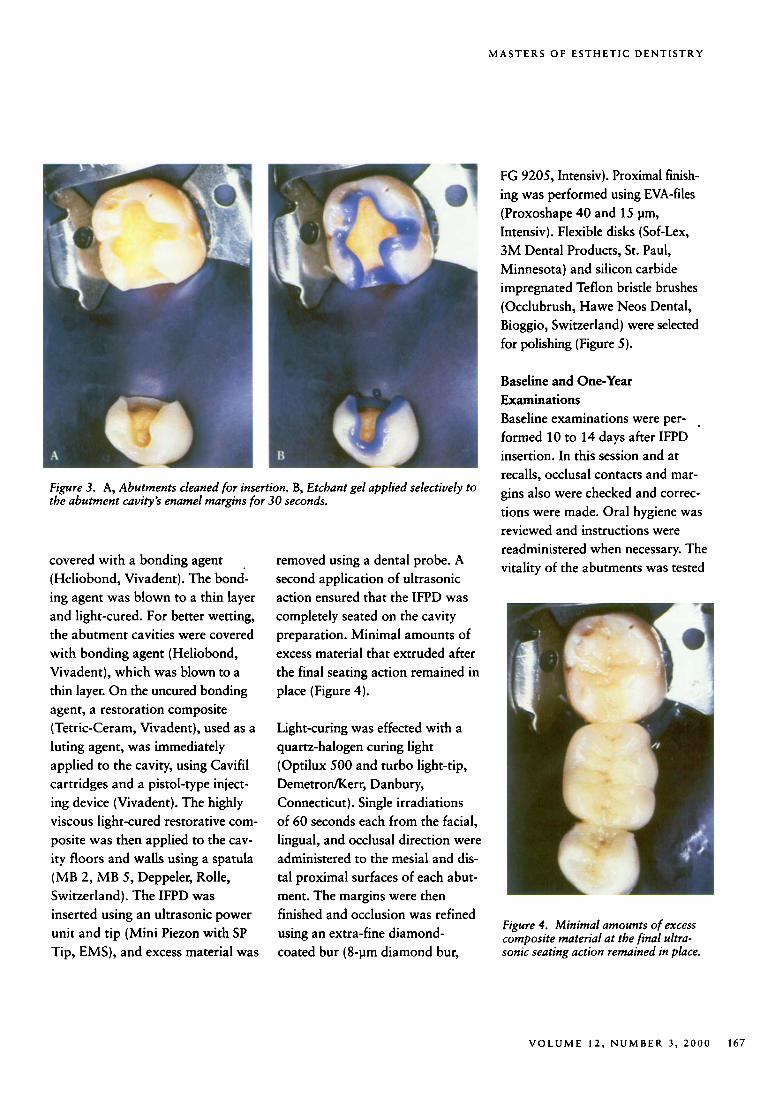
Figure 3. A, Abutments cleaned for insertion. B, Etchant gel applied selectively to the abutment cavity’s enamel margins for 30 seconds.
covered with a bonding agent (Heliobond, Vivadent). The bond- ing agent was blown to a thin layer and light-cured. For better wetting, the abutment cavities were covered with bonding agent (Heliobond, Vivadent), which was blown to a thin layer. On the uncured bonding agent, a restoration composite (Tetric-Ceram, Vivadent), used as a luting agent, was immediately applied to the cavity, using Cavifil cartridges and a pistol-type inject- ing device (Vivadent). The highly viscous light-cured restorative com- posite was then applied to the cav- ity floors and walls using a spatula (MB 2, MB 5, Deppeler, Rolle, Switzerland). The IFPD was inserted using an ultrasonic power unit and tip (Mini Piezon with SP Tip, EMS), and excess material was
removed using a dental probe. A second application of ultrasonic action ensured that the IFPD was completely seated on the cavity preparation. Minimal amounts of excess material that extruded after the final seating action remained in place (Figure 4).
Light-curing was effected with a quartz-halogen curing light (Optilux 500 and turbo light-tip, Demetromerr, Danbury, Connecticut). Single irradiations of 60 seconds each from the facial, lingual, and occlusal direction were administered to the mesial and dis- tal proximal surfaces of each abut- ment. The margins were then finished and occlusion was refined using an extra-fine diamond-
FG 9205, Intensiv). Proximal finish- ing was performed using EVA-files (Proxoshape 40 and 15 pm, Intensiv). Flexible disks (Sof-Lex, 3M Dental Products, St. Paul, Minnesota) and silicon carbide impregnated Teflon bristle brushes (Occlubrush, Hawe Neos Dental, Bioggio, Switzerland) were selected for polishing (Figure 5).
Baseline and One-Year Examinations Baseline examinations were per- . formed 10 to 14 days after IFPD insertion. In this session and at recalls, occlusal contacts and mar- gins also were checked and correc- tions were made. Oral hygiene was reviewed and instructions were readministered when necessary. The vitality of the abutments was tested
Figure 4. Minimal amounts of excess composite material at the final ultra-
coated bur (8-pm diamond bur, sonic seating action remained in place.
V O L U M E 12, N U M B E R 3 , 2000 167
with frozen Cot , and the IFPDs were rated according to United States Public Health Service (USPHS) criteria,” by two cali- brated examiners. The clinical rat- ing was performed in the same manner as at the 1- and the on- going 2-year examinations. Plaque growth at the gingival pontic sur- faces, abutment inlays, and contra- lateral control teeth, also was mea- sured, using the Plaque Index (PI).I2 Gingival health was recorded at the proximal abutment inlays, mid- pontic area, and contralateral con- trol teeth, using the Gingival Index (GI).I3 For statistical analysis of GI and PI, the sign test was used.
Impressions were made of the occlusal and proximal surfaces of the abutments’(President fast, light body surface activated fast,
Coldne, Altstatten, Switzerland). Replicas were manufactured at ran- dom using epoxy resin (Stycast 1266, Emerson and Cuming, West- erlo, Belgium). The replicas were sputter-coated with gold (Sputter SCD 030, Balzers Union, Balzers, Principality of Liechtenstein). Mar- ginal adaptation at the interfaces between the tooth and luting com- posite, as well as between the luting composite and the restorations, was examined quantitatively with SEM (Amray lSlO/r, Amray Inc., Bed- ford, Massachusetts), at 200 times magnification, according to Krejci (Figure 6).14 Margins were rated “excellent” when a smooth transi- tion with no interruption of conti- nuity was found. Every separation of the components due to cohesive or adhesive failure was rated as “noncontinuous margin. ”
Figure 5. A, Excess composite material was removed with 8-pm finishing diamond burs and Eva-tips. B, After the occlusion was checked, the IFPD was polished and the enamel was remineralized with fluoride.
In Vitro Evaluation Before clinical evaluation, in vitro tests were carried out with 18 human canines and 18 human molars with slot-inlay preparations located in enamel, anchoring for unit IFPDs. Preparation, laboratory technique, adhesive placement, replica manu- facture, and SEM evaluation were identical to those in the clinical pro- cedure. The specimens were loaded in a computer-controlled masticator (CoCoM 1, PPK, Zurich, Switzerland) simultaneously with 1,200,000 occlusal loadings of 49 N at 1.7 Hz and 3000 thermocycles of type 5”C, SO”C, 5°C. The margins were subsequently analyzed with SEM, using a replica technique, as described for clinical procedure, and the same criteria.6
RESULTS
The clinical ratings after 1 year, using USPHS criteria, can be sum- marized as follows:
There was no breakage at the pon- tics, inlay retainers, or inlay margins.
There was no debonding between retainer inlays and cavity preparations.
The IFPDs were rated “alfa” with respect to color and color match with one exception. One single IFPD was rated “bravo” at baseline and at the 1-year examination, because the Vectris Pontic fiber ele- ment shone occlusally through a thin layer of enamel composite. Surface texture was rated “bravo”
168 JOURNAL OF ESTHETIC DENTISTRY
MASTERS OF ESTHETIC DENTISTRY
in two instances because of exposed glass fibers, but there was no dis- coloration of these two IFPDs. In another case, one marginal section was rated “bravo” because of a slight marginal discrepancy. Discol- oration of inlay and luting material was not observed, and there was no secondary caries (Table 1).
All abutments initially diagnosed as vital remained vital after 1 year. At baseline examination, two patients reported increased postoperative sensitivity. In one instance, increased sensitivity vanished after approxi- mately 6 weeks; in the other, increas- ed sensitivity diminished after 3 to 4 months. No postoperative sensi- tivity was reported at the 1-year examination. Plaque growth was moderate (Table 2). The sign test revealed no significant difference in plaque growth between abutments and pontics, or between pontic areas and contralateral control teeth. Sig- nificantly more plaque was located only on distal abutments compared to mesial abutments ( p c .05). All patients judged their IFPDs as being very good from the point of view of esthetics, surface texture, and com- fort during mastication at baseline and a t the 1-year and the ongoing 2-year e~amination.~,’
Clinical and SEM examinations did not reveal any excessive wear of the abutment inlays or pontic surfaces. There were occlusal contacts in cen- tric occlusion on all occlusal surfaces of the inlays and pontics. All proxi- mal contacts of abutment inlays
Figure 6. Marginal section of a bonded composite inlay retainer showing excellent marginal adaptation at tooth-luting composite interface and at restoration-composite luting material interface after I year. (Original mag- nification, x 200)
remained strong at the 1-year exami- nation. Quantitative SEM examina- tion revealed 91.6 5% excellent margins at the luting composite- tooth interface, and 86.1 = 7.6% excellent margins at the luting com- posite-restoration interface.’
In the ongoing 2-year examinations, no changes from the clinical ratings and SEM analysis derived a t 1 year have been detected to date. But it is too early for a conclusive judgment. Data will be presented when the 2-year examinations are completed.
In the in vitro pretests, an average of 92.1 12.3% of excellent margins at the canines and 92.7 2 3.5% at the molars was achieved after long- term mechanical loading at the lut- ing composite-tooth interface. At the luting composite-restoration interface, 96.1 2 6.4% of excellent
margin at the canines and 96.4 2
4.7% at the molars were achieved.‘
1) I s<:uss I 0 s
The advantages of polymer-based reconstructions have been well doc- umented since the early 1 9 7 0 ~ . ” . ’ ~ However, their insufficient fracture resistance has caused significant problems.” Now, optimized fiber- reinforced polymer systems have apparently overcome this limiting flaw. These products allow clini- cians to construct tooth-friendly and cost-conscious restorations and reconstructions.‘
To date, separation of the veneering composite from the fiber substruc- ture has not been observed in iabo- ratory evaluation. This type of sep- aration was reported in an earlier experimental study using a labora- tory multistep technique similar to
V O L U M E 12, N U M B E R 3 , 2000 169
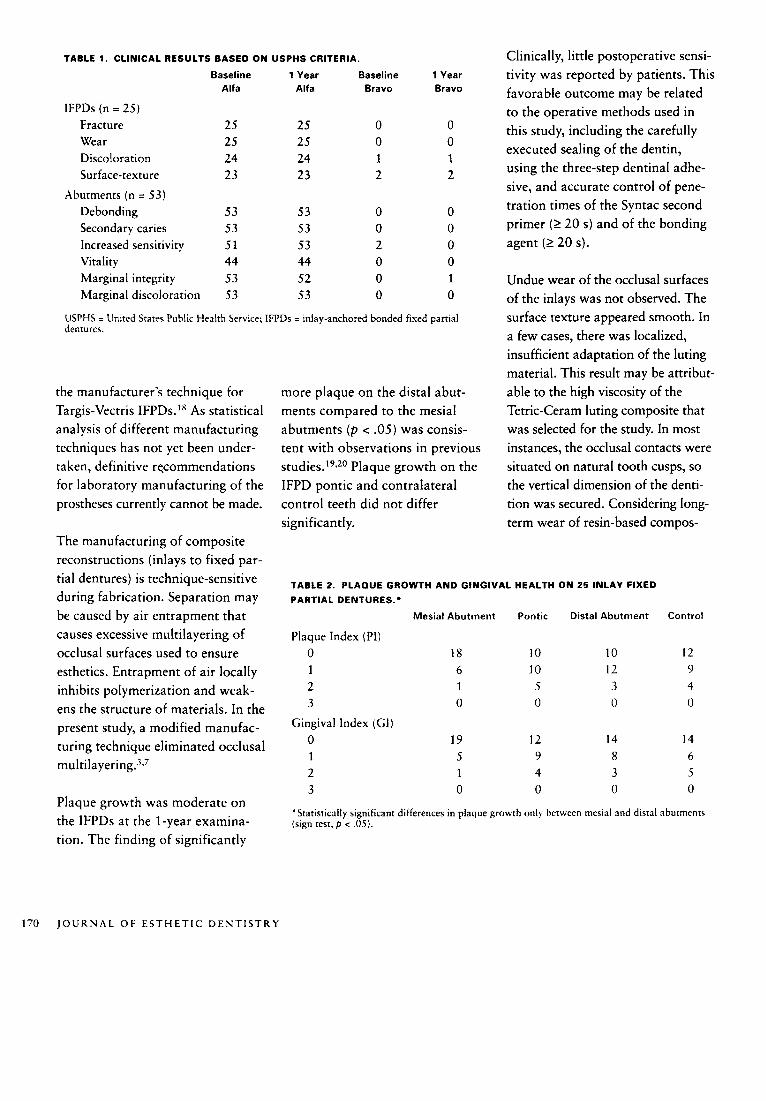
TABLE 1. CLINICAL RESULTS BASED O N USPHS CRITERIA. Clinically, little postoperative sensi- Baseline 1 Year Baseline 1 Year tivity was reported by patients. This
favorable outcome may be related to the oDerative methods used in
Alfa Alfa Bravo Bravo
IFPDs (n = 25)
Fracture 25 25 0 0 this study, including the carefully executed sealing of the dentin, Wear 25 25 0 0
Discoloration 24 24 1 1 using the three-step dentinal adhe- Surface-texture 23 23 2 2 sive, and accurate control of pene- tration times of the Syntac second Debonding 53 53 0 0
Secondary caries 53 53 0 0 primer (2 20 s) and of the bonding
Abutments (n = 53)
Increased sensitivity 51 53 2 0 agent (2 20 s). Vitality 44 44 0 0 Marginal integrity 53 52 0 1 Undue wear of the occlusal surfaces Marginal discoloration 53 53 0 0 of the inlays was not observed. The
surface texture appeared smooth. In a few cases, there was localized, insufficient adaptation of the luting material. This result may be attribut- able to the high viscosity of the Tetric-Ceram luting composite that was selected for the study. In most instances, the occlusal contacts were situated on natural tooth cusps, so the vertical dimension of the denti- tion was secured. Considering long- term wear of resin-based compos-
USPHS = United Srares Public Health Service; IFPDs = inlay-anchored bonded fised partial dentures.
the manufacturer’s technique for Targis-Vectris IFPDs.’* As statistical analysis of different manufacturing techniques has not yet been under- taken, definitive recommendations for laboratory manufacturing of the prostheses currently cannot be made.
The manufacturing of composite reconstructions (inlays to fixed par-
during fabrication. Separation may be caused by air entrapment that Mesial Abutment Pontic Distal Abutment Control
causes excessive multilayering of occlusal surfaces used to ensure 0 18 10 10 12
more plaque on the distal abut- ments compared to the mesial abutments ( p < .05) was consis- tent with observations in previous s t ~ d i e s . ’ ~ , ~ ~ Plaque growth on the IFPD pontic and contralateral control teeth did not differ significantly.
tial dentures) is technique-sensitive TABLE 2. PLAQUE GROWTH AND GINGIVAL HEALTH O N 25 INLAY FIXED
PARTIAL DENTURES:
Plaque Index (PI)
esthetics. Entrapment of air locally 1 6 10 12 9 inhibits polymerization and weak- 2 1 5 3 4
3 0 0 0 0 ens the structure of materials. In the present study, a modified manufac- turing technique eliminated occlusal m~ltilayering.~*’
‘Statistically significant differences in plaque growth only between mesial and distal abutments (sign test, p < .05).
Plaque growth was moderate on
tion. The finding of significantly the IFPDs at the 1-year examina-
170 J O U R N A L O F E S T H E T I C D E N T I S T R Y
M A S T E R S O F E S T H E T I C D E N T I S T R Y
ites, it appears that the current tech- nique of using a conservative bonded IFPD may be successful. After 1 year, an overall clinical alfa rating for most criteria of the conser- vative bonded IFPDs as well as results from SEM analysis showed that the marginal quality was high. Because of the unique ease with which polymer-based reconstruc- tions are incorporated, these systems enable a level of acceptance that has, to date, been ~nattainable.~ Conse- quently, new options in reconstruc- tive dentistry have been generated that should definitely be considered.
Although the observation period of this study was short, it provided similar results to the clinical information provided by other researchers. Continuing monitoring of the survival rates of IFPDs made of fiber-reinforced composite is nec- essary and more data will be col- lected for this study during the next 5 years. The ongoing 2-year exami- nations are promising, and to date, appear to confirm the results of the 1-year examinations. But it is too early for a conclusive judgment. With the present in vitro data and the preliminary results of a descrip- tive study, no generalization about IFPDs currently can be made. More clinical experience must be docu- mented to create a sound basis for final assessment of this method. However, it is the impression of the authors that fiber-reinforced com- posite constructions have the poten- tial to satisfy the requirements for durable, conservative IFPDs.
CONCLUSION
Based on the results of in vitro tests and the descriptive clinical study, glass fiber-reinforced composite IFPDs have a potential to satisfy the requirements for durable, conserva- tive bonded IFPDs.
ACKNOWLEDGMENTS
The authors thank Mr. David Sagesser for his consistent high quality work and care in the labo- ratory fabrication of the glass fiber- reinforced inlay dentures.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
9.
Giitschow F. Untersuchungen zur Hau- figkeit der Indikation fiir Adhasivbriicken. Dtsch Stomatol 1991; 41:89-91.
Krejci I, Boretti R, Giezendanner P, Lutz, F. Adhesive crowns and FPDs fabricated of ceromer/FRC clinical and laboratory procedures. Pract Periodont Aesthet Dent 1998; 10:487498.
Gohring TN, Krejci I, Lutz F. Adhasive Inlaybrucken aus glasfaserverstarktem Komposit. Step by Step-Beschreibung der klinischen Anwendung. Schweiz Monatss- chr Zahnmed 1999; 109:369-379.
Behr M, Rosentritt A, Leibrock S, Schnei- der-Feyrer S, Handel G. In vitro study of fracture strength and marginal adaptation of fiber-reinforced adhesive fixed partial inlay dentures. J Dent 1999; 27163-168.
Gohring TN, Peters 0, Lutz F. Marginal adaptation of bonded slot-inlays anchor- ing four-unit inlay FPDs. J Prosthet Dent 2000. (Accepted for publication)
Gohring TN, Mormann W, Lun F. Clini- cal and scanning electron microscopic eval- uation of fiber-reinforced fixed partial den- tures. J Prosthet Dent 1999; 82:662-668.
Feilzer AJ, De Gee AJ, Davidson CL. Set- ting stress in composite resin in relation to configuration of the restoration. J Dent Res 1987; 66:1636-1639.
Lutz F, Krejci I, Barbakow F. Quality and durability of marginal adaptation in bonded composite restorations. Dent Mater 1991; 7:107-113.
10. Krejci I, Lieber CM, Lutz F. Time required to remove totally bonded tooth-colored posterior restorations and related tooth substance loss. Dent Mater 1995; 11:3440.
11 . Ryge G, Snyder M. Evaluating the clinical quality of restorations. J Am Dent Assoc 1973; 87:369-377.
12. Loe H, Silness J. Periodontal disease in pregnancy. Prevalence and severity. Acta Odontol Scand 1963; 21533-551.
13. Silness J, Loe H. Periodontal disease in pregnancy. 11. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 1964; 22:121-135.
16. McDermott T, Lutz F, Lufi A, Schmid U, Miihlemann HR. Quantitative evaluation of in vivo occlusal wear of acrylic resin bridges and wear resistance of three differ- ent materials: results after six months. Helv Odont Acta 1981; 91:lOOl-1024.
17. Beuchat M, Krejci I, Lutz F. Minimally invasive unreinforced adhesive composite bridges: the clinical procedure. Schweiz Monatsschr Zahnmed 1999; 109507-51 9.
18. Altieri JV, Burstone CJ, Goldberg AJ, Patel AP. Longitudinal clinical evaluation of fiber-reinforced composite FPDs: a pilot study. J Prosthet Dent 1994; 71:16-22.
19. Cumming BR, Liie H. Consistency of plaque distribution in individuals without special home care instruction. J Periodont Res 1973; 8:94-100.
20. Furuichi Y, Lindhe J, Ramberg P, Volpe AR. Patterns of de novo plaque formation in human dentition. J Clin Periodontol 1992; 19:423433.
Reprint requests: Till N. Gohring, DMD, Department of Preuentiue Dentistry, Periodontology, and Cariology, Center for Dental and Oral Medicine, University of Zurich, Plattenstrasse 1 1 , CH-8028 Zurich, Switzerland; e-mail: [email protected] 02000 B.C. Decker fnc.