16
Abridged Version Case study from Indonesia PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
Abridged Version
Case study from Indonesia
PRIMARY HEALTH CARE SYSTEMS (PRIMASYS)
WHO/HIS/HSR/17.7
© World Health Organization 2017
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Primary health care systems (PRIMASYS): case study from Indonesia, abridged version. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
The named authors alone are responsible for the views expressed in this publication.
Editing and design by Inís Communication – www.iniscommunication.com
Overview of primary health care system in Indonesia
Quality of life and equal access to health care are basic human rights1 in Indonesia, in line with the five fundamental principles (or “Pancasila”) of Indonesian national ideology, and in accordance with Article 34 of the National Constitution of 1945 and National Health Act No. 36 of 2009. Indonesia is the largest archipelago country in the world, and the fourth most populated country. It comprises more than 17 000 islands, the largest being Java, Sumatera, Kalimantan/Borneo, Sulawesi/Celebes, and Papua. Indonesia has 255 461 million inhabitants linked by one official language, Bahasa Indonesia, while there are more than 700 local languages. Administratively, the country has 34 provinces, 514 districts, more than 7000 subdistricts, and more than 80 000 villages. Though it has a stable life expectancy, Indonesia is still challenged by poverty, and 11% of the population is living below the poverty line.2
Indonesia is facing a triple burden of health care problems due to (a) the ineffective control of infectious diseases such as malaria, multidrug-resistant tuberculosis, dengue fever and other infections; (b) the rise of chronic diseases into the list of top five catastrophic disorders in the country, leading to increased risk of metabolic disorders, such as diabetes mellitus, hypertension, dyslipidaemia, and cancers, in addition to cardiovascular problems, trauma and injuries; and (c) re-emerging diseases such as polio and diphtheria, due to challenges in the distribution and scope of child immunization, and risky cultural attitudes. The maternal mortality rate (MMR) has decreased since
1 United Nations Declaration of Human Rights, 1948.
2 Statistical Yearbook of Indonesia 2016. Republic of Indonesia Statistics Centre Bureau (https://www.bps.go.id/index.php/publikasi/4238, accessed 16 February 2017).
1990, from 390 to 228 per 100 000 live births. However, unlike the under-5 mortality rate, the MMR did not meet the Millennium Development Goal (MDG) target for Indonesia by 2015.3 This complex setting is intertwined by inequalities, with a Gini coefficient of 0.41, and also an unequal distribution of health workers. The gross domestic product (GDP) per capita is US$ 3834.06, which is among the lowest in the world. The educational background of the Indonesian population is about 25% elementary school, 25% secondary school, 25% high school, and only 8% with higher education. Consequently, Indonesia’s Human Development Index for 2014 was 0.684, ranking it 110 out of 188 countries, low compared to other countries in the Association of South-East Asian Nations (ASEAN).
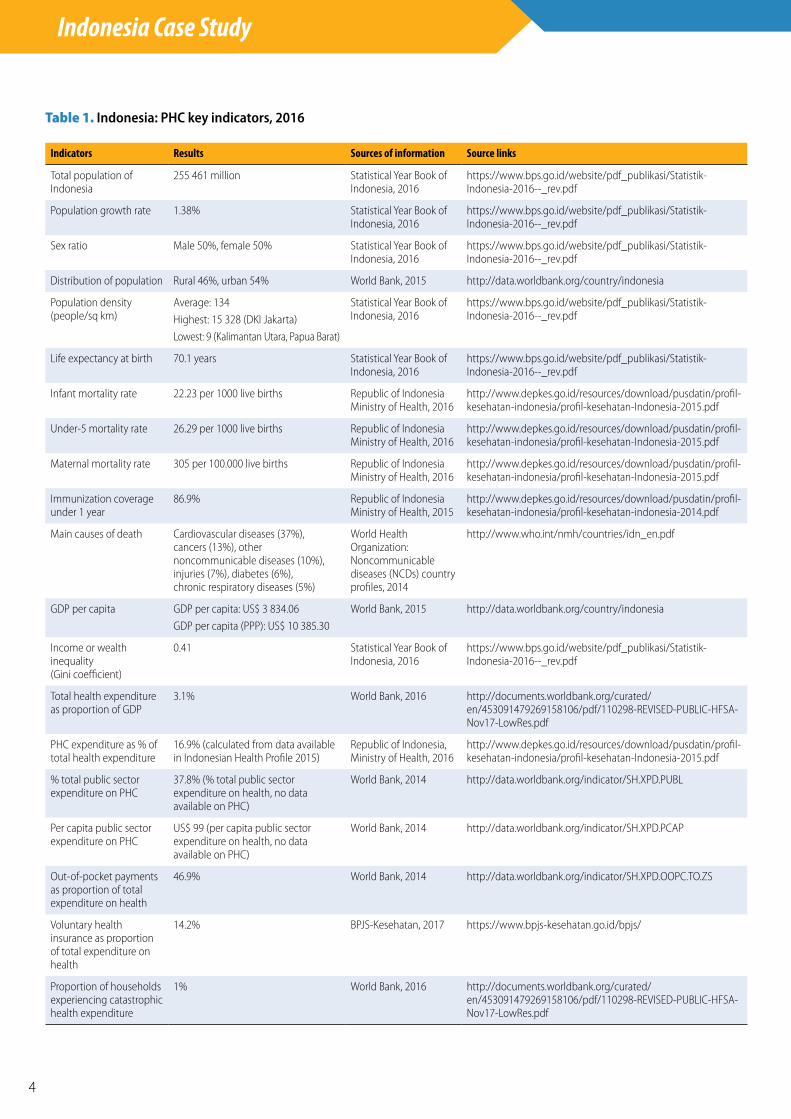
During 2016, Indonesian Government spending on health met the target stipulated by Health Act No. 36 of 2009, which is 5% of the State budget. However, this proportion is still very low, given the complexity and disparity of the health problems facing Indonesia. As a result, the government contribution to public health expenditure is limited, and the proportion of out-of-pocket expenditure is relatively high. Significant levels of poverty occur because households are faced with catastrophic expenditure on health care. Indonesia’s primary health care (PHC) key indicators for 2016 are shown in Table 1.
3 Indonesia Health Profile 2015. Republic of Indonesia Ministry of Health; 2016.
Case study from Indonesia
Primary Health Care Systems (PRIMASYS)
4
Indonesia Case Study
Table 1. Indonesia: PHC key indicators, 2016
Indicators Results Sources of information Source links
Total population of Indonesia
255 461 million Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Population growth rate 1.38% Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Sex ratio Male 50%, female 50% Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Distribution of population Rural 46%, urban 54% World Bank, 2015 http://data.worldbank.org/country/indonesia
Population density (people/sq km)
Average: 134
Highest: 15 328 (DKI Jakarta)
Lowest: 9 (Kalimantan Utara, Papua Barat)
Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Life expectancy at birth 70.1 years Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Infant mortality rate 22.23 per 1000 live births Republic of Indonesia Ministry of Health, 2016
http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-Indonesia-2015.pdf
Under-5 mortality rate 26.29 per 1000 live births Republic of Indonesia Ministry of Health, 2016
http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-Indonesia-2015.pdf
Maternal mortality rate 305 per 100.000 live births Republic of Indonesia Ministry of Health, 2016
http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-Indonesia-2015.pdf
Immunization coverage under 1 year
86.9% Republic of Indonesia Ministry of Health, 2015
http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-indonesia-2014.pdf
Main causes of death Cardiovascular diseases (37%), cancers (13%), other noncommunicable diseases (10%), injuries (7%), diabetes (6%), chronic respiratory diseases (5%)
World Health Organization: Noncommunicable diseases (NCDs) country profiles, 2014
http://www.who.int/nmh/countries/idn_en.pdf
GDP per capita GDP per capita: US$ 3 834.06
GDP per capita (PPP): US$ 10 385.30
World Bank, 2015 http://data.worldbank.org/country/indonesia
Income or wealth inequality (Gini coefficient)
0.41 Statistical Year Book of Indonesia, 2016
https://www.bps.go.id/website/pdf_publikasi/Statistik-Indonesia-2016--_rev.pdf
Total health expenditure as proportion of GDP
3.1% World Bank, 2016 http://documents.worldbank.org/curated/en/453091479269158106/pdf/110298-REVISED-PUBLIC-HFSA-Nov17-LowRes.pdf
PHC expenditure as % of total health expenditure
16.9% (calculated from data available in Indonesian Health Profile 2015)
Republic of Indonesia, Ministry of Health, 2016
http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-Indonesia-2015.pdf
% total public sector expenditure on PHC
37.8% (% total public sector expenditure on health, no data available on PHC)
World Bank, 2014 http://data.worldbank.org/indicator/SH.XPD.PUBL
Per capita public sector expenditure on PHC
US$ 99 (per capita public sector expenditure on health, no data available on PHC)
World Bank, 2014 http://data.worldbank.org/indicator/SH.XPD.PCAP
Out-of-pocket payments as proportion of total expenditure on health
46.9% World Bank, 2014 http://data.worldbank.org/indicator/SH.XPD.OOPC.TO.ZS
Voluntary health insurance as proportion of total expenditure on health
14.2% BPJS-Kesehatan, 2017 https://www.bpjs-kesehatan.go.id/bpjs/
Proportion of households experiencing catastrophic health expenditure
1% World Bank, 2016 http://documents.worldbank.org/curated/en/453091479269158106/pdf/110298-REVISED-PUBLIC-HFSA-Nov17-LowRes.pdf
5
PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
Evolution of PHC policies
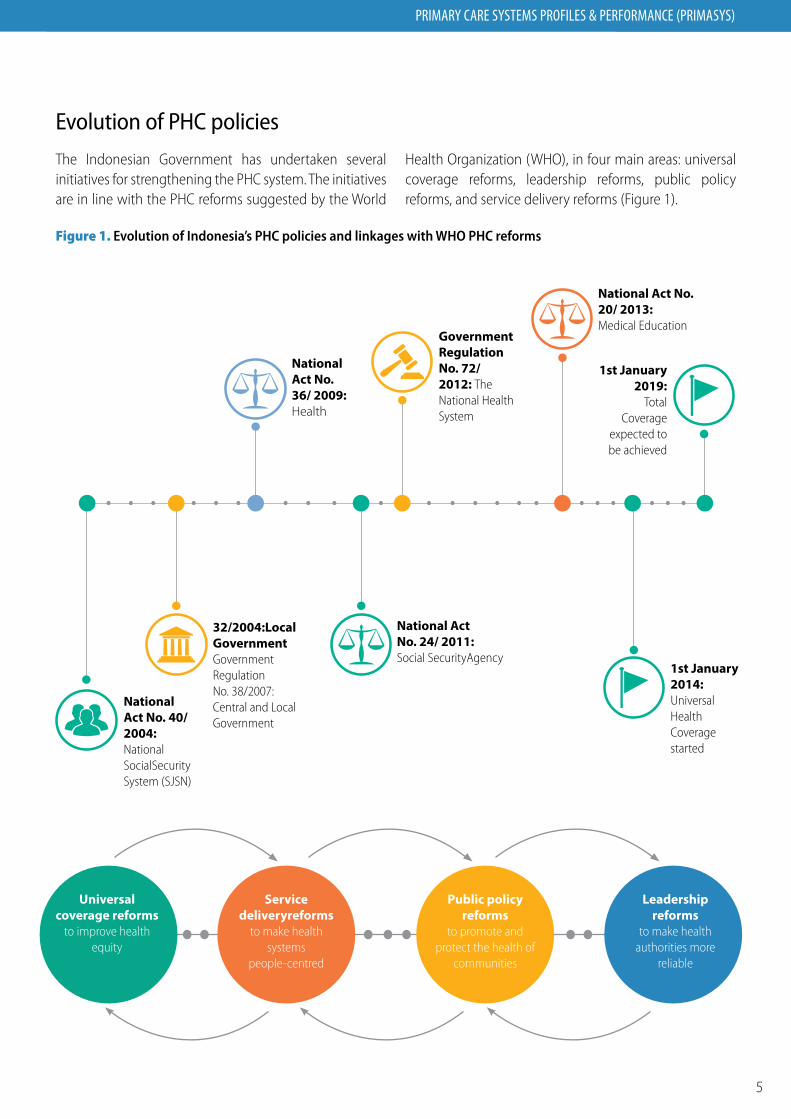
The Indonesian Government has undertaken several initiatives for strengthening the PHC system. The initiatives are in line with the PHC reforms suggested by the World
Health Organization (WHO), in four main areas: universal coverage reforms, leadership reforms, public policy reforms, and service delivery reforms (Figure 1).
Figure 1. Evolution of Indonesia’s PHC policies and linkages with WHO PHC reforms
National Act No. 40/ 2004: National SocialSecurity System (SJSN)
32/2004:Local Government Government Regulation No. 38/2007: Central and Local Government
National Act No. 24/ 2011: Social SecurityAgency
1st January 2014: Universal Health Coverage started
1st January 2019:
Total Coverage
expected to be achieved
National Act No. 36/ 2009: Health
Government Regulation No. 72/ 2012: The National Health System
National Act No. 20/ 2013: Medical Education
Universal coverage reforms
to improve health equity
Service deliveryreforms
to make health systems
people-centred
Public policy reforms
to promote and protect the health of
communities
Leadership reforms
to make health authorities more
reliable
6
Indonesia Case Study
Governance
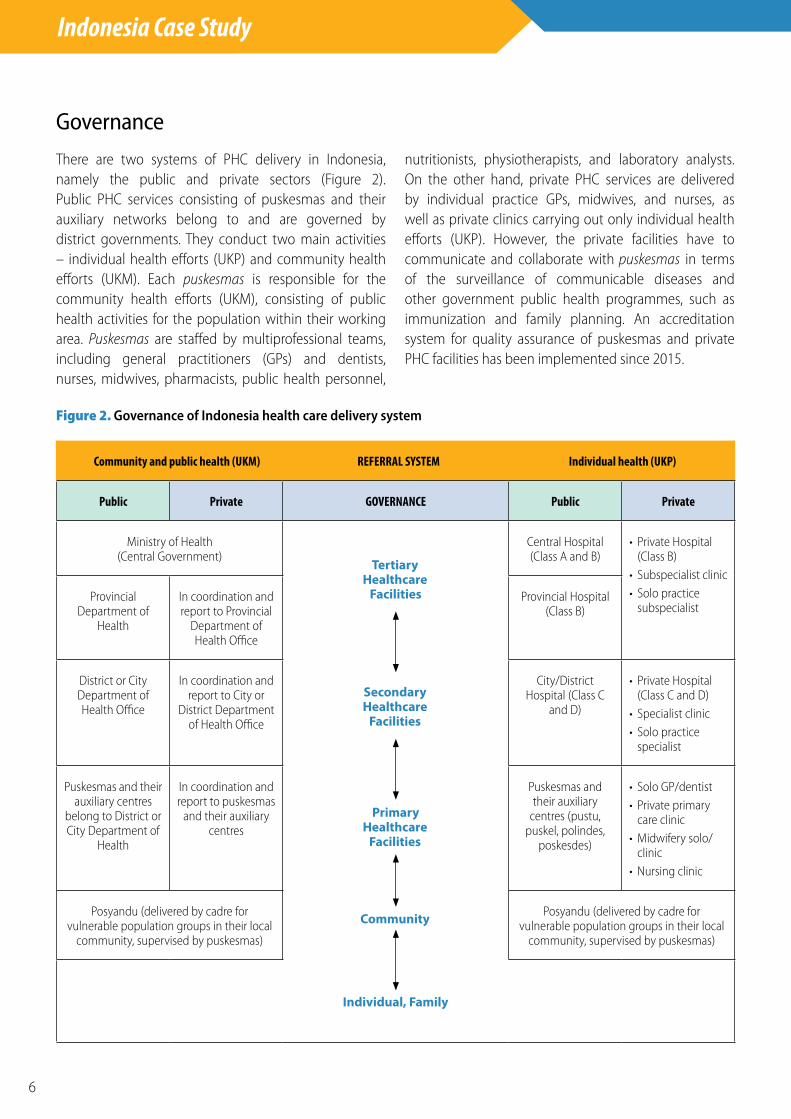
There are two systems of PHC delivery in Indonesia, namely the public and private sectors (Figure 2). Public PHC services consisting of puskesmas and their auxiliary networks belong to and are governed by district governments. They conduct two main activities – individual health efforts (UKP) and community health efforts (UKM). Each puskesmas is responsible for the community health efforts (UKM), consisting of public health activities for the population within their working area. Puskesmas are staffed by multiprofessional teams, including general practitioners (GPs) and dentists, nurses, midwives, pharmacists, public health personnel,
nutritionists, physiotherapists, and laboratory analysts. On the other hand, private PHC services are delivered by individual practice GPs, midwives, and nurses, as well as private clinics carrying out only individual health efforts (UKP). However, the private facilities have to communicate and collaborate with puskesmas in terms of the surveillance of communicable diseases and other government public health programmes, such as immunization and family planning. An accreditation system for quality assurance of puskesmas and private PHC facilities has been implemented since 2015.
Figure 2. Governance of Indonesia health care delivery system
Community and public health (UKM) REFERRAL SYSTEM Individual health (UKP)
Public Private GOVERNANCE Public Private
Ministry of Health (Central Government)
Central Hospital (Class A and B)
• Private Hospital (Class B)
• Subspecialist clinic• Solo practice
subspecialistProvincial
Department of Health
In coordination and report to Provincial
Department of Health Office
Provincial Hospital (Class B)
District or City Department of Health Office
In coordination and report to City or
District Department of Health Office
City/District Hospital (Class C
and D)
• Private Hospital (Class C and D)
• Specialist clinic• Solo practice
specialist
Puskesmas and their auxiliary centres
belong to District or City Department of
Health
In coordination and report to puskesmas
and their auxiliary centres
Puskesmas and their auxiliary
centres (pustu, puskel, polindes,
poskesdes)
• Solo GP/dentist• Private primary
care clinic• Midwifery solo/
clinic• Nursing clinic
Posyandu (delivered by cadre for vulnerable population groups in their local
community, supervised by puskesmas)
Posyandu (delivered by cadre for vulnerable population groups in their local
community, supervised by puskesmas)
Individual, Family
Tertiary Healthcare
Facilities
Primary Healthcare
Facilities
Community
Secondary Healthcare
Facilities
7
PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
By the universal coverage system that started in 2014, the national systematic referral system was implemented. The referral and referral back system is based on the diagnoses listed in the primary care online medical record system (P-Care), which guides the primary care physicians and hospital specialists on whether to refer or not to refer patients with certain diseases. In reality, this system is widely known by all physicians at primary, secondary and tertiary care levels, though there are still many areas where improvement can be achieved, based on clinical pathways, key performance indicators and rates of contact with patients. By December 2014 there were 9731 puskesmas, staffed by one or two GPs on average, while 38.53% of puskesmas had more GPs than the average. However, 25.57% of puskesmas had a shortage of GPs. As a result, midwives and nurses have to take over GPs’ work, as a consequence of which patients fail to get proper PHC services. The number of health professionals staffing puskesmas needs to be sufficient and appropriate to support both the UKP and UKM functions of puskesmas. Moreover, the government needs to recognize private PHC facilities as a part of its PHC system and treat them equally with puskesmas in terms of support, control and involvement, thus removing the inequity related to the perception that “puskesmas is for the poor and private practice is for the rich.”
Financing
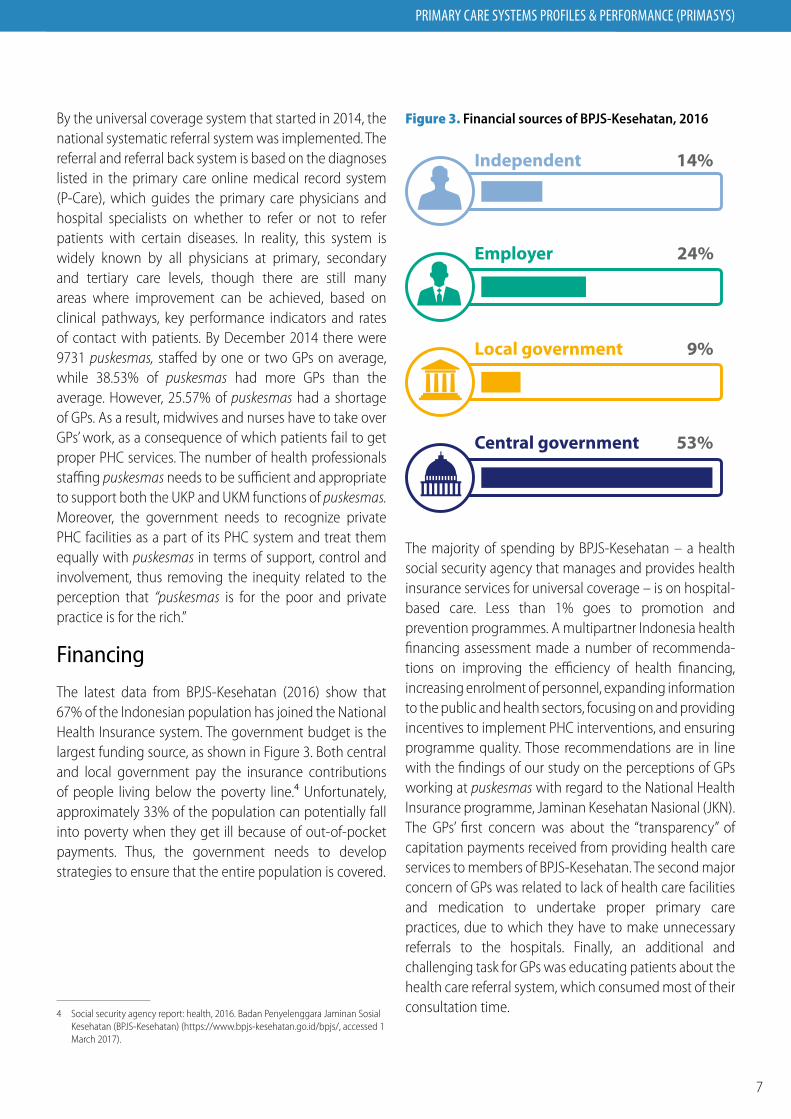
The latest data from BPJS-Kesehatan (2016) show that 67% of the Indonesian population has joined the National Health Insurance system. The government budget is the largest funding source, as shown in Figure 3. Both central and local government pay the insurance contributions of people living below the poverty line.4 Unfortunately, approximately 33% of the population can potentially fall into poverty when they get ill because of out-of-pocket payments. Thus, the government needs to develop strategies to ensure that the entire population is covered.
4 Social security agency report: health, 2016. Badan Penyelenggara Jaminan Sosial Kesehatan (BPJS-Kesehatan) (https://www.bpjs-kesehatan.go.id/bpjs/, accessed 1 March 2017).
Figure 3. Financial sources of BPJS-Kesehatan, 2016
Independent 14%
Employer 24%
Local government 9%
Central government 53%
The majority of spending by BPJS-Kesehatan – a health social security agency that manages and provides health insurance services for universal coverage – is on hospital-based care. Less than 1% goes to promotion and prevention programmes. A multipartner Indonesia health financing assessment made a number of recommenda-tions on improving the efficiency of health financing, increasing enrolment of personnel, expanding information to the public and health sectors, focusing on and providing incentives to implement PHC interventions, and ensuring programme quality. Those recommendations are in line with the findings of our study on the perceptions of GPs working at puskesmas with regard to the National Health Insurance programme, Jaminan Kesehatan Nasional (JKN). The GPs’ first concern was about the “transparency” of capitation payments received from providing health care services to members of BPJS-Kesehatan. The second major concern of GPs was related to lack of health care facilities and medication to undertake proper primary care practices, due to which they have to make unnecessary referrals to the hospitals. Finally, an additional and challenging task for GPs was educating patients about the health care referral system, which consumed most of their consultation time.
8
Indonesia Case Study
Human resources: the transition to high quality of care in Indonesia
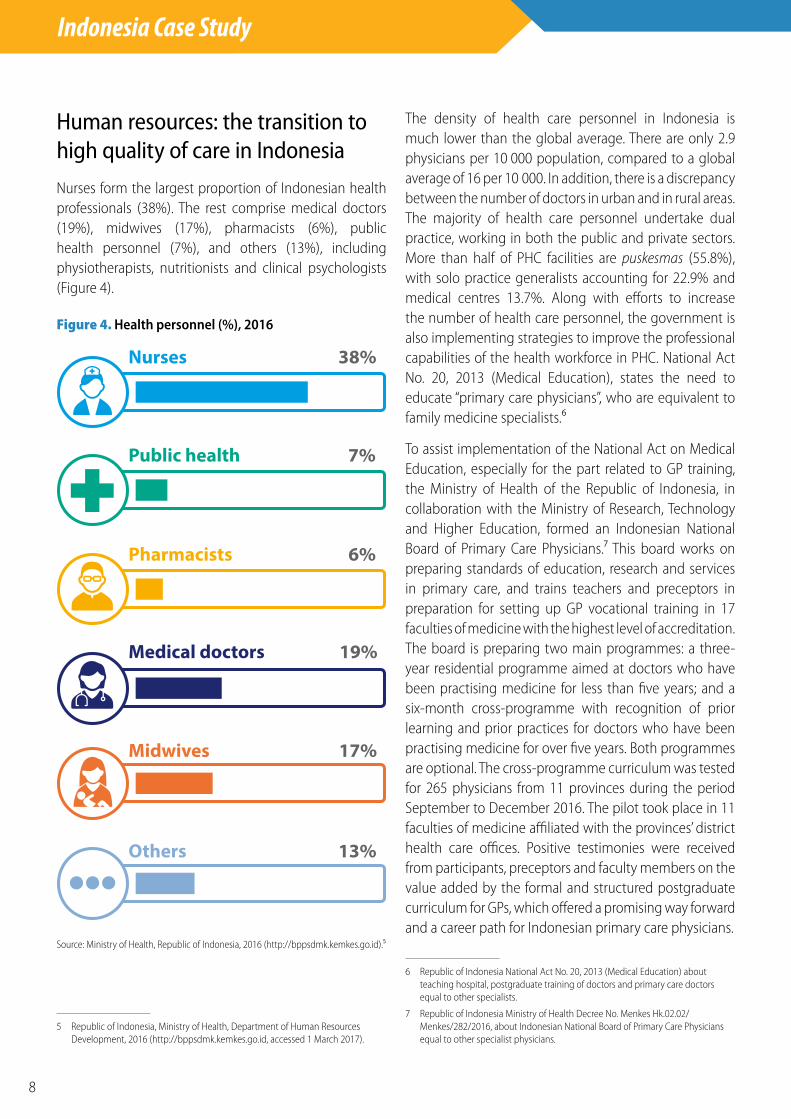
Nurses form the largest proportion of Indonesian health professionals (38%). The rest comprise medical doctors (19%), midwives (17%), pharmacists (6%), public health personnel (7%), and others (13%), including physiotherapists, nutritionists and clinical psychologists (Figure 4).
Figure 4. Health personnel (%), 2016
Public health 7%
Pharmacists 6%
Medical doctors 19%
Midwives 17%
Nurses 38%
Others 13%
Source: Ministry of Health, Republic of Indonesia, 2016 (http://bppsdmk.kemkes.go.id).5
5 Republic of Indonesia, Ministry of Health, Department of Human Resources Development, 2016 (http://bppsdmk.kemkes.go.id, accessed 1 March 2017).
The density of health care personnel in Indonesia is much lower than the global average. There are only 2.9 physicians per 10 000 population, compared to a global average of 16 per 10 000. In addition, there is a discrepancy between the number of doctors in urban and in rural areas. The majority of health care personnel undertake dual practice, working in both the public and private sectors. More than half of PHC facilities are puskesmas (55.8%), with solo practice generalists accounting for 22.9% and medical centres 13.7%. Along with efforts to increase the number of health care personnel, the government is also implementing strategies to improve the professional capabilities of the health workforce in PHC. National Act No. 20, 2013 (Medical Education), states the need to educate “primary care physicians”, who are equivalent to family medicine specialists.6
To assist implementation of the National Act on Medical Education, especially for the part related to GP training, the Ministry of Health of the Republic of Indonesia, in collaboration with the Ministry of Research, Technology and Higher Education, formed an Indonesian National Board of Primary Care Physicians.7 This board works on preparing standards of education, research and services in primary care, and trains teachers and preceptors in preparation for setting up GP vocational training in 17 faculties of medicine with the highest level of accreditation. The board is preparing two main programmes: a three-year residential programme aimed at doctors who have been practising medicine for less than five years; and a six-month cross-programme with recognition of prior learning and prior practices for doctors who have been practising medicine for over five years. Both programmes are optional. The cross-programme curriculum was tested for 265 physicians from 11 provinces during the period September to December 2016. The pilot took place in 11 faculties of medicine affiliated with the provinces’ district health care offices. Positive testimonies were received from participants, preceptors and faculty members on the value added by the formal and structured postgraduate curriculum for GPs, which offered a promising way forward and a career path for Indonesian primary care physicians.
6 Republic of Indonesia National Act No. 20, 2013 (Medical Education) about teaching hospital, postgraduate training of doctors and primary care doctors equal to other specialists.
7 Republic of Indonesia Ministry of Health Decree No. Menkes Hk.02.02/Menkes/282/2016, about Indonesian National Board of Primary Care Physicians equal to other specialist physicians.
9
PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
National Act No. 36 of 2014, on health care personnel, regulates types of personnel, educational qualifications, roles and functions, colleges, national examinations, and recertification of other health care professions. Systems are being developed to support collaboration between health professionals in the areas of continuity of care and patient safety.
Planning and implementation
According to the Republic of Indonesia Ministry of Health, the first agenda is to strengthen the PHC system through five steps, as part of the “revitalization of community health centres (puskesmas)”. The steps are: (a) enhancing educational qualifications for health professionals; (b) enhancing the capacity of primary
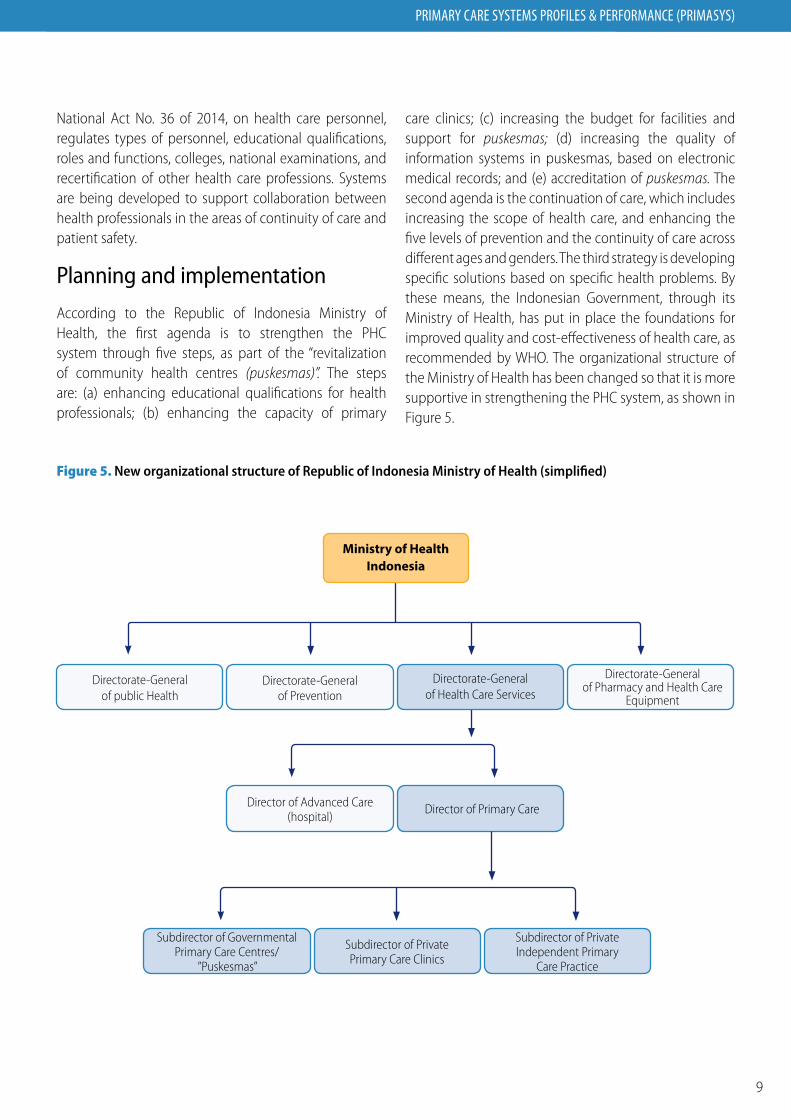
care clinics; (c) increasing the budget for facilities and support for puskesmas; (d) increasing the quality of information systems in puskesmas, based on electronic medical records; and (e) accreditation of puskesmas. The second agenda is the continuation of care, which includes increasing the scope of health care, and enhancing the five levels of prevention and the continuity of care across different ages and genders. The third strategy is developing specific solutions based on specific health problems. By these means, the Indonesian Government, through its Ministry of Health, has put in place the foundations for improved quality and cost-effectiveness of health care, as recommended by WHO. The organizational structure of the Ministry of Health has been changed so that it is more supportive in strengthening the PHC system, as shown in Figure 5.
Figure 5. New organizational structure of Republic of Indonesia Ministry of Health (simplified)
Ministry of Health Indonesia
Directorate-General of public Health
Directorate-General of Prevention
Directorate-General of Health Care Services
Directorate-General of Pharmacy and Health Care
Equipment
Director of Advanced Care (hospital)
Director of Primary Care
Subdirector of Governmental Primary Care Centres/
”Puskesmas”
Subdirector of Private Primary Care Clinics
Subdirector of Private Independent Primary
Care Practice

10
Indonesia Case Study
Regulatory processes
Ministry of Health Regulation No. 46 of 2015 requires all PHC facilities, including puskesmas, private clinics and private practices of GPs and dentists, to undergo an accreditation programme. In 2016, nearly 30% of puskesmas in Indonesia became accredited. The target was set at 50% in 2015. To date, the accreditation system has not been extended to other PHC facilities (private facilities). However, to assist achievement of the goal of universal health coverage by 2019, the private PHC facilities will undergo similar accreditation programmes to ensure quality of care. Through this quality assurance system, all PHC facilities in Indonesia will be ready to provide a high quality of first contact care, thus strengthening the provision of PHC services in Indonesia. Despite the low ratio of primary care facilities to population – which is around 1 per 15 000 people – the Ministry of Health, which coordinates the health care system across the country, is laying the foundation for the start of a new era of better health care services. To achieve better health outcomes in the coming decades, the key is continuous improvement.
Monitoring and information systems
The current National Health Insurance system provides a national online medical record system (PCare) at all primary care facilities serving BPJS-Kesehatan members. Although the form of the online medical record system is still undergoing continuous development, the aim is to put in place more integrated referral information for primary, secondary and tertiary care. A more rigorous medical record online system would provide data for health care services, researchers and health professional education agendas, ultimately leading to greater continuity of care within the primary care system for Indonesia. Reports of periodical regional health research (riset kesehatan daerah or riskesdas) also provide continuous health profiles from each province in Indonesia, which are ultimately analysed and collated into health profiles at national level. The introduction of the accreditation programme for PHC facilities will also help to ensure continuity of high-quality PHC services. Patient satisfaction is also taken into account in the accreditation standards.
WHO / SEARO /Budi Chandra
11
PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
Way forward and policy considerations
The global efforts to strengthen PHC systems are part of the agenda to strengthen all levels of care, from primary to secondary and tertiary care. The Indonesian people and health professionals should start to embrace a paradigm shift aimed at early prevention efforts in order to achieve better health outcomes, rather than simply pursuing curative programmes. The recommendations from the 2008 World health report have been implemented in Indonesia through (a) the start of universal coverage of the National Health Insurance system on 1 January 2014, with the aim of achieving universal health coverage by 2019; (b) service delivery reforms based on a more people-centred care system, including increasing the capacity of health professionals and use of general practitioners as gatekeepers (for example through initiation of a postgraduate education programme for primary care
physicians (specialists) as a regular programme for GPs practising for less than five years and a non-regular programme for GPs practising for five years and more); (c) public policy reforms in relation to strengthening the primary care system through the various regulations mentioned above; and (d) leadership reforms to enable equal access to high quality of care for all people, which is the biggest challenge (Figure 6). The new health care system requires that all actors collaborate and work together. Although the two national Acts related to human health workforce development have currently been rejected by existing physicians in professional associations – perhaps due to their perceptions of future insecurity – Indonesia has taken the firm decision to begin moving towards equity of access to health care, in line with the Alma Ata Declaration.
WHO / SEARO /Budi Chandra

12
Indonesia Case Study
Figure 6. Framework for strengthening PHC system in Indonesia
INDONESIA PHC FUTURE OVERVIEW
• Equity and equality of health care access
• Continuity of care
• Optimum comprehensive care
• Universal coverage
INDONESIA PHC CURRENT OVERVIEW
• Inequality
• Demographic transition
• Epidemiological transition
• Triple burden of health problems
• Lack of continuity of care
• Need for comprehensive coverage
COORDINATIVE CARECoordinator of care
(Graduate primary care physicians)
GOVERNANCENeeds optimum
comprehensive care
FINANCINGNeeds massive, specific and continuous
information nationally
PLANNING AND IMPLEMENTATION
Needs governmental focusMake PHC everyone’s business
GOVERNANCEPolitical will (local and central government)
PLANNING AND IMPLEMENTATION
Governmental focus towards scaling up health professionals
PHC is everyone’s responsibility
MONITORING AND EVALUATIONUse of online medical record data for communication, research and policy towards continuous improvement
MONITORING AND EVALUATIONNeeds well organized online medical
records towards coninuity and comprehensive care
FINANCING SOURCES• Insured budget for universal coverage
• Increase scope of BPJS participation
• Reducing kick-off behavior of participant
FINANCING SPENDING• Emphasize prevention
• Primary care facilities
• Variation and appropriate payment (not only single capitation methods)
• Health professionals support
The need to change
Willingness to change
HUMAN RESOURCESNeeds collaborative care and
high quality of care

13
PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
ReferencesBadan Penyelenggara Jaminan Sosial Kesehatan (BPJS-Kesehatan) / Health social security agency report, 2016 (https://www.bpjs-kesehatan.go.id/bpjs/, accessed 15 December 2016)
Chongsusivatwong V, Phua KH, Yap MT, Pocock NS, Hashim JH, Chhem R, et al. Health and health-care systems in southeast Asia: Diversity and transitions. Lancet 2011;377:429–37.
Communicable Disease Profile for Tsunami Affected Areas Indonesia., 2005., Communicable Disease team, WHO Aceh/Indonesia Regional Office for South East Asia, WHO/SEARO Communicable Disease Working Group on Emergencies, WHO/HQ.
Hernawan A. Andalkan Klinik Sebagai Ujung Tombak: SJSN Segera Dioperasikan untuk Gantikan Jamkesda: Lensaindonesia.com; 2012. Available from: http://www.lensaindonesia.com/ 2012/10/06/ssjn-segera-dioperasikan-untuk-gantikan-jamkesda.html
JAMSOS Indonesia. [Online]Available at: http://www.jamsosindonesia.com/
Kidd M, 2013. The contribution of family medicine to health care system. WONCA
Republic of Indonesia Ministry of Finance, 2014. [Online] Available at: https://www.bps.go.id/index.php/publikasi/326
Republic of Indonesia National Act No; No. 36, 2009 about Health and Wellness.
Republic of Indonesia National Act No. 40, 2004 about Universal Coverage System in Indonesia
Republic of Indonesia National Act No. 11, 2011 about the body who responsible for implementing the Universal Coverage System in Indonesia
Republic of Indonesia National Act No.20, 2013 (medical education) about Teaching Hospital, Postgraduate trainings of doctors and Primary Care Doctors equal to other specialists
Republic of Indonesia National Act No.36, 2014 about Healthcare Personnels
Republic of Indonesia Ministry of Health Decree No: Menkes Hk.02.02/Menkes/282/2016 about Indonesian National Board of Primary Care Physicians equal to other specialists physicians
Republic of Indonesia Ministry of Health, Department of Human Resources Development, 2016. Available from http://bppsdmk.kemkes.go.id
Republic of Indonesia Ministry of Health, Ministry of Health Regulation No. 46, 2015 about primary care facilities accreditation system
Republic of Indonesia Ministry of Research, Technology and Higher Education Decree No: 22/Kepmen/ 2016 about the National Committee of Ministry of Health and Ministry of Research-Technology and Higher Education on health care services and education excellences.
Republic of Indonesia, Ministry of Health Strategic Planning, 2015
http://www.depkes.go.id/resources/download/info-publik/Renstra-2015.pdf
Republic of Indonesia Ministry of Health Reports, Indonesia Health Profile-2014, published 2015
Republic of Indonesia Ministry of Health Reports, Indonesia Health Profile-2015, published 2016 http://www.depkes.go.id/resources/download/pusdatin/profil-kesehatan-indonesia/profil-kesehatan-Indonesia-2015.pdf
United Nation Declaration, 1948
United Nation Development Programme, Indonesian Report 2015
World Bank., 2014. [Online]Available at: http://data.worldbank.org/country/indonesia
World Bank., 2015. [Online]Available at: http://data.worldbank.org/country/indonesia
WHO, Alma Ata Declaration WHO, 1978
WHO, Primary Health Care is Now More than Ever, 2008
Thabrany H. Implementasi SJSN Tidak Boleh Tertunda Lagi Jakarta2011. Available from: http://www.slideshare.net/imbangbilabora/bahanpresentasipembicaradpkesehatan071211hasbullahthabrany.
Republic of Indonesia Statistics Centre Bureau, Statistical Yearbook of Indonesia 2016. Available from: https://www.bps.go.id/index.php/publikasi/4238, accessed 16 February 2017).
Syah NA, Roberts C, Jones A, Trevena L Kumar K. Perceptions of Indonesian general practitionersin maintaining standards of medical practice ata time of health reform. Family Practice, 2015, Vol. 32, No. 5, 584–590
Syah NA, Exploration of general practitioners’ experiences of maintaining standards of practice in Indonesia (PhD thesis submitted to Sydney Medical School), 2014.
Indonesia Health Financing System Assessment (2016) Spend More. Spend Right. Spend Better. Ministry of Health Republic of Indonesia, Ministry of Finance Republic of Indonesia, World Bank, Australia Government DFAT, Canada, European Union, Swiss Confederation, and The Vaccine Alliance Federation
14
Indonesia Case Study
AuthorsMora Claramita Department of Medical Education and Department of Family and Community Medicine, Faculty of Medicine, Universitas Gadjah Mada (UGM); and National Board of Indonesian Primary Care Physicians – College of Indonesian Primary Care Physicians
Nur Afrainin Syah Department of Medical Education, Faculty of Medicine, Universitas Andalas (UNAND); and National Board of Indonesian Primary Care Physicians – College of Indonesian Primary Care Physicians
Fitriana Murriya Ekawati Department of Family and Community Medicine, Faculty of Medicine, UGM
Oryzati Hilman Agrimon Department of Family Medicine and Public Health, Faculty of Medicine and Health Sciences, Universitas Muhammadiyah Yogyakarta (UMY); and National Board of Indonesian Primary Care Physicians – College of Indonesian Primary Care Physicians
Hari Kusnanto Department of Family and Community Medicine, Faculty of Medicine, UGM; and National Board of Indonesian Primary Care Physicians – College of Indonesian Primary Care Physicians

PRIMARY CARE SYSTEMS PROFILES & PERFORMANCE (PRIMASYS)
World Health Organization
Avenue Appia 20CH-1211 Genève [email protected]
http://www.who.int/alliance-hpsr
This case study was developed by the Alliance for Health Policy and Systems Research, an international partnership hosted by the World Health Organization, as part of the Primary Health Care Systems (PRIMASYS) initiative. PRIMASYS is funded by the Bill & Melinda Gates Foundation, and aims to advance the science of primary health care in low- and middle-income countries in order to support efforts to strengthen primary health care systems and improve the implementation, effectiveness and efficiency of primary health care interventions worldwide. The PRIMASYS case studies cover key aspects of primary health care systems, including policy development and implementation, financing, integration of primary health care into comprehensive health systems, scope, quality and coverage of care, governance and organization, and monitoring and evaluation of system performance. The Alliance has developed full and abridged versions of the 20 PRIMASYS case studies. The abridged version provides an overview of the primary health care system, tailored to a primary audience of policy-makers and global health stakeholders interested in understanding the key entry points to strengthen primary health care systems. The comprehensive case study provides an in-depth assessment of the system for an audience of researchers and stakeholders who wish to gain deeper insight into the determinants and performance of primary health care systems in selected low- and middle-income countries.

















