Prepared by Dr n. med. Radosław Blok – I Katedra Gin - Poł. AM Wrocław Faculty of Medicine Wrocław,Gynaecology & Obstetrics Depart. Pathologies Pathologies of the of the amniotic fluid amniotic fluid volume volume .
Transcript
Prepared by Dr n. med. Radosław Blok – I Katedra Gin - Poł. AM Wrocław
Faculty of Medicine Wrocław,Gynaecology & Obstetrics Depart.
Pathologies of the Pathologies of the amniotic fluid amniotic fluid volumevolume
.
Amniotic fluidAmniotic fluid
Amniotic fluid volume measures is one of the important aspects in perinatal diagnosis.
Excess or less amount of amniotic Excess or less amount of amniotic fluid in pregnancy can be a sign of fluid in pregnancy can be a sign of serious pathology such as serious pathology such as polyhydramnios or oligohydramnios.polyhydramnios or oligohydramnios.
Life and growth of the fetus for the whole Life and growth of the fetus for the whole period of pregnancy is depending on period of pregnancy is depending on amniotic fluid which is one of the factors amniotic fluid which is one of the factors for a proper growth.for a proper growth.Since the period of Hipokrates until the Since the period of Hipokrates until the beginning of XX century, it has been beginning of XX century, it has been believed that amniotic fluid is a fetus believed that amniotic fluid is a fetus urine, which only: urine, which only: 1. acts as a shock absorber protecting the 1. acts as a shock absorber protecting the fetus from possible extraneous injury.fetus from possible extraneous injury.2.maintenanse an even temperature.2.maintenanse an even temperature.3.the fluid extends the amniotic sac and 3.the fluid extends the amniotic sac and thereby allows for growth and free thereby allows for growth and free movement of the fetus.movement of the fetus.4.its nutrietive values is negligible 4.its nutrietive values is negligible because of small amount of protien and because of small amount of protien and salt content, however, water supply to salt content, however, water supply to the feuts is quite adequate.the feuts is quite adequate.
We also know that the amniotic fluid We also know that the amniotic fluid plays a metabolic role, and its plays a metabolic role, and its contents has a significant contents has a significant information about fetus wellbeing. information about fetus wellbeing. The amniotic fluid The amniotic fluid pH values are pH values are responsible for the implimentation of responsible for the implimentation of the fetus acid-base balance as follows:the fetus acid-base balance as follows:Before the 20th week-7.23Between 25th-31st week-7.17At labour 7.11
In the amniotic fluid we can find the In the amniotic fluid we can find the following constituents:following constituents:OrganicOrganic:-Protein- 0.3 mg%, Glucose- :-Protein- 0.3 mg%, Glucose- 20mg%, Urea-30mg%, Uric acid-4mg%, 20mg%, Urea-30mg%, Uric acid-4mg%, Creatinine-2mg%, Total lipids-50mg%, Creatinine-2mg%, Total lipids-50mg%, Hormones (Prolactin,insulin and renin)Hormones (Prolactin,insulin and renin) InorganicInorganic:-The concetration of sodium, :-The concetration of sodium, chloride and potassium is almost the chloride and potassium is almost the same as the maternal blood.same as the maternal blood.The amniotic fluid has a bacteriostatic The amniotic fluid has a bacteriostatic nature guaranteed by lizozomes, nature guaranteed by lizozomes, properidine and protein-zinc complex as properidine and protein-zinc complex as well as immunogloblins. well as immunogloblins.
In the first half of pregnancy most of In the first half of pregnancy most of the amniotic fluid contents are the amniotic fluid contents are transported through the fetus skin, but transported through the fetus skin, but after the 24-26 week that is after the after the 24-26 week that is after the fetal skin fetal skin keratinizationkeratinization that path of that path of transport becomes impossible with an transport becomes impossible with an except of the low density substances except of the low density substances dissolved in lipids.dissolved in lipids.
The amniotic fluid volume changes as the The amniotic fluid volume changes as the pregnancy grows, and it reaches its peak pregnancy grows, and it reaches its peak around the 32nd week. After that period around the 32nd week. After that period the volume decreases systematically.the volume decreases systematically.It’s important to note that after the 42nd It’s important to note that after the 42nd week the volume undergoes a sudden week the volume undergoes a sudden decrease being a sign of placenta decrease being a sign of placenta disability, as well as prolonged pregnancy disability, as well as prolonged pregnancy (postdate pregnancy).(postdate pregnancy).
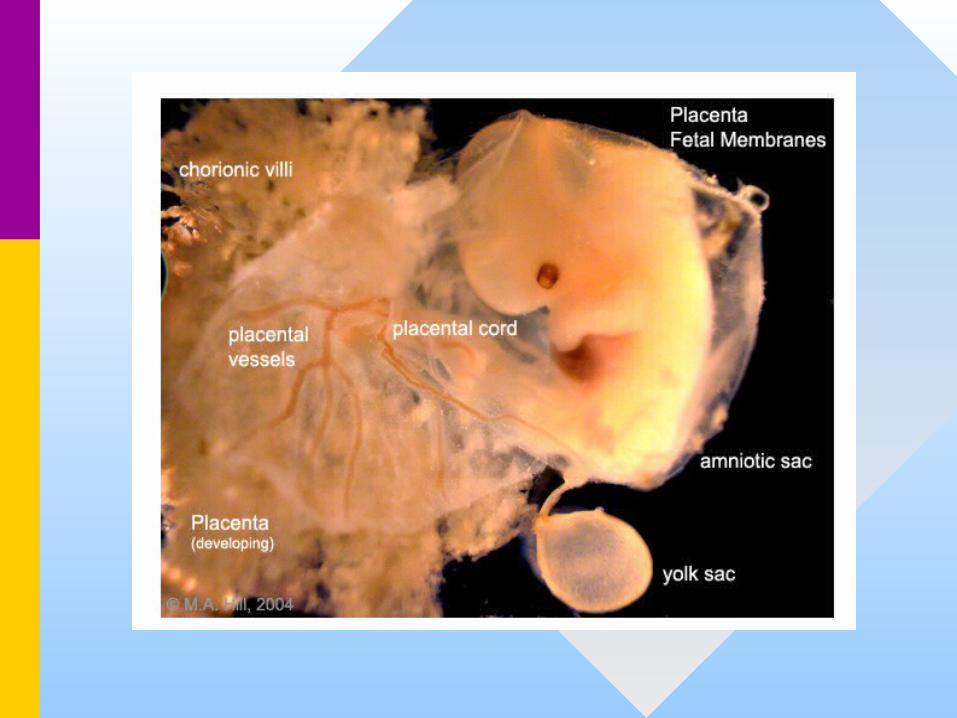
Embryo at 10 weeks – normal AFIEmbryo at 10 weeks – normal AFI
Amniotic fluid circulation after the Amniotic fluid circulation after the 20th week.20th week.
The amniotic fluid production is as follows• Fetal kidney 500 - 1000 ml • Fetal lungs 170 ml• Fetal saliva 25 ml
Reabsorbtion of amniotic fluid• By swallowing 500 - 1000 ml• Fetal lungs 170 ml• Intra-membrane transport to the fetus 200 - 500 ml• The fetus-maternal membrane transport only 10 ml
Oligohydroamnion is severe deficiency of amniotic fluid (sometimes defined as maximum vertical pocket < 1cm determined by sonography) oligohydramnion measures below 200ml.
Anhydramnion should be diagnosed when the AFI is below 50ml.
Clinical signs as follows: low uterine volume, lack of fetal free movements, a low abdominal circumference, low body weight, easy palpapable fetal parts and weak fetal movements.
Maximum vertical pocketMaximum vertical pocket
The causes of oligohydroamnionThe causes of oligohydroamnion• Developmental defects, especially in the urinary system• Preterm rupture of membranes• Hypotrophy• Postterm pregnancy• Multiple pregnancy transfusion syndrome• Drugs:Prostaglandin synthesis inhibitors Angiotensin-converting enzyme inhibitors • Mother’s diseases with microangiopathy with high blood
• Amniotic fluid index - AFI < 5• Low value biochemical profiles – Manningas test• Low or lack of fetus movements• Difficulties in fetus anatomical analysis.• Pathological fetus measurements due to
compression
Complications caused by oligohydramnion
• Hipotrophy• Fetus lung hipoplasia • Fetus deformation syndrome• Intrauterine infection• Severe fetal condition after birth• Intrauterine fetal death
Complications caused by Anhydramnion
Fetus deformation syndrome• Dysmorphism of facial skeleton • Pathological limb location• Hip dislocation• Excessive skin• Minor thorax causing fetus hypoplastic lung
Complications caused by Anhydramnion
Intrauterine fetal asphyxia• umbilical cord compression• an increase in meconium aspiration syndrom• pathological KTG• a decrease in biophysical profile• poor vessel blood flow - doppler• an icrease in cesarean sections • poor newborns state < 7 points
Management in oligohydramnion Preconception management in women with :• hypertension• chronic kidney diseases• autoimmunological diseases• diabetes mellitus type R and F• obstetrical load
Management in oligohydramnion care during pregnancy :• early diagnosis• proper treatment of common diseases in time • infection prophylaxis• water and electrolite balance• bedrest • the use of tocolytic agents• adequate hydration
Management in oligohydramnion
Care during labor :• Intensive care: KTG, doppler-flows,
• prostaglandyn syntetaze blocker• it increases fetal breathing rate by 50% • it as well increases fetus membrane permeable ability• it changes membrane character from secretion to
resorbtion• it reduces the fetus urine production
Treatment continued Indometacyna
• The first dose 50 mg in suppository• Next dose 25mg p.o. every 6 hours• Fetus ECC at a 3 days interval• AFI level every after 7 days• daily blood pressure control
Treatment continued The side effects of Indomethacin use
• nausea, abdominal discomfort, gastric ulcers• headache and dizzness• It causes hypertention effects as it is a hypotensive
drugs antagonist• It causes a duretic decrease in pregnant women• It also causes platelets disbalance
The side effects of Indomethacin use in the fetus
• the newborn colon inflammation • fetal aterial stenosis• right ventricle hypertrophy• an increase in pulmonary artery blood pressure• a decrease in stroke volume
Care in polyhydramnion
during labour:• intensive care: KTG, flows, gasometry,
puls rate control • Care during amniocentesis
The placentaThe placenta
• The placenta (Greek, The placenta (Greek, plakuosplakuos = flat = flat cake) named on the basis of this cake) named on the basis of this organs appearance. The placenta a organs appearance. The placenta a mateno-fetal organ which begins mateno-fetal organ which begins developing at implantation of the developing at implantation of the blastocyst and is delivered with the blastocyst and is delivered with the fetus at birth. fetus at birth.
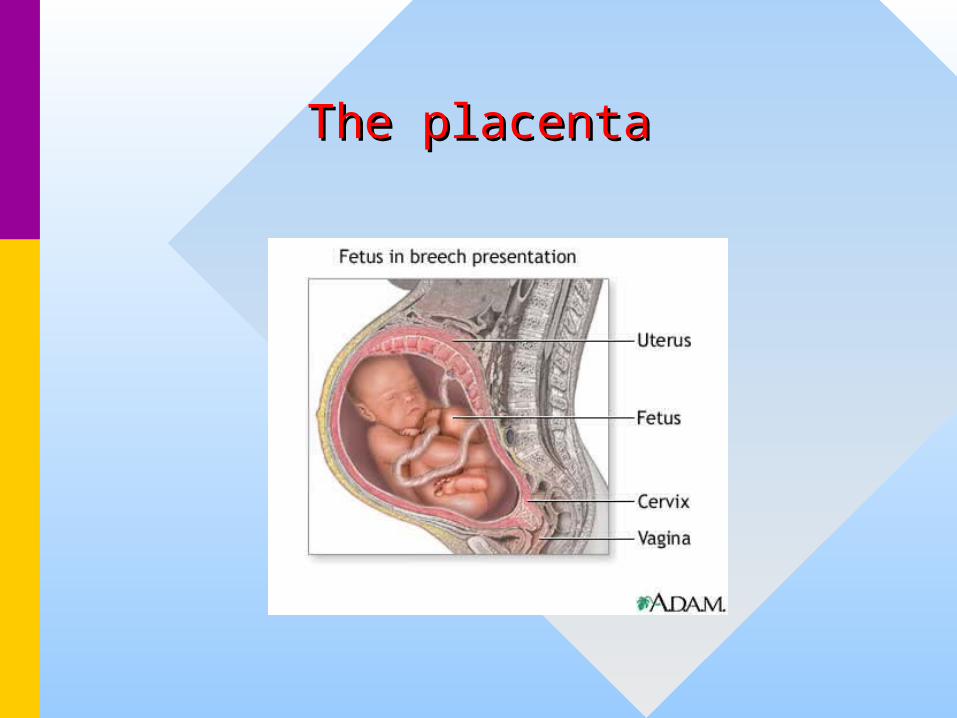
The placentaThe placenta
The placentaThe placenta
• During that 9 month period it During that 9 month period it provides nutrition, gas exchange, provides nutrition, gas exchange, waste removal, endocrine and waste removal, endocrine and immune support for the developing immune support for the developing fetus. fetus.
The placenta - developmentThe placenta - development • embryonic/maternal organ embryonic/maternal organ • villous chorion/decidua basalis villous chorion/decidua basalis • continuous with amniotic and chorionic sacks continuous with amniotic and chorionic sacks • Dimensions Dimensions
– discoid up to 20cm diameter and 3 cm thick (in term) discoid up to 20cm diameter and 3 cm thick (in term) – weighs 500-600 gm weighs 500-600 gm
• maternal and embryonic surface maternal and embryonic surface • delivered at parturition delivered at parturition • retention may cause uterine hemorrhage retention may cause uterine hemorrhage
The placenta - developmentThe placenta - development
• Maternal SurfaceMaternal Surface • Cotyledons - form cobblestone appearance Cotyledons - form cobblestone appearance • originally placental septa formed grooves originally placental septa formed grooves • covered with maternal decidua basalis covered with maternal decidua basalis • Fetal SurfaceFetal Surface • umbilical cord attachment umbilical cord attachment • cord 1-2 cm diameter, 30-90cm long cord 1-2 cm diameter, 30-90cm long • covered with amniotic attached to chorionic plate covered with amniotic attached to chorionic plate • umbilical vessels branch into chorionic vessels which umbilical vessels branch into chorionic vessels which
anastomose anastomose
Placental functionPlacental function
• 3 main functions 3 main functions • metabolism metabolism • transport transport • endocrine endocrine
• provides nutrient and energy provides nutrient and energy
Placental TransportPlacental Transport • gases and nutrition gases and nutrition • oxygen, carbon dioxide, carbon monoxide oxygen, carbon dioxide, carbon monoxide • water, glucose, vitamins water, glucose, vitamins • hormones, mainly steroid not protein hormones, mainly steroid not protein • electrolytes electrolytes • maternal antibodies maternal antibodies • waste products waste products • urea, uric acid, bilirubin urea, uric acid, bilirubin • drugs and their metabolites drugs and their metabolites • fetal drug addiction fetal drug addiction • infectious agents infectious agents • cytomegalovirus, rubella, measles, microorganismscytomegalovirus, rubella, measles, microorganisms
Placental EndocrinePlacental Endocrine
• Human chorionic gonadotrophin (hCG) Human chorionic gonadotrophin (hCG) like leutenizing hormone, supports corpus luteum like leutenizing hormone, supports corpus luteum • Human chorionic somatommotropin (hCS) Human chorionic somatommotropin (hCS) or placental lactogen or placental lactogen hormone level increases in maternal blood through hormone level increases in maternal blood through
• Human chorionic thyrotropin (hCT) Human chorionic thyrotropin (hCT) (hCT) Peptide placental hormone, similar to anterior (hCT) Peptide placental hormone, similar to anterior
pituitary released thyroid stimulating hormone (TSH), pituitary released thyroid stimulating hormone (TSH), which along with human chorionic gonadotrophin which along with human chorionic gonadotrophin (hCG) is thought to act on maternal thyroid. There is (hCG) is thought to act on maternal thyroid. There is little recent research published on this hormone, its little recent research published on this hormone, its level and activities. level and activities.
• Human chorionic corticotropin (hCACTH) Human chorionic corticotropin (hCACTH) placental hormone thought to have corticotropin placental hormone thought to have corticotropin
• Steroid Hormones Steroid Hormones • progestins - progesterone, support of the progestins - progesterone, support of the
endometrium and suppress uterine smooth muscle endometrium and suppress uterine smooth muscle contractility. contractility.
• estrogens - estriol, stimulate growth of the estrogens - estriol, stimulate growth of the myometrium and mammary gland development. myometrium and mammary gland development.
• both hormones support maternal endometrium both hormones support maternal endometrium • Relaxin – Humans high levels early in pregnancy than Relaxin – Humans high levels early in pregnancy than
at birth promotes angiogenesis probably plays a role at birth promotes angiogenesis probably plays a role in development of the uterus/ placenta than in the in development of the uterus/ placenta than in the birth process birth process
Human chorionic gonadotrophin Human chorionic gonadotrophin (hCG)(hCG)
• After implantation cells within the After implantation cells within the developing placenta (syncitiotrophoblasts) developing placenta (syncitiotrophoblasts) synthesize and secrete Human chorionic synthesize and secrete Human chorionic gonadotrophin (hCG) into the maternal gonadotrophin (hCG) into the maternal bloodstream. The main function of serum bloodstream. The main function of serum hCG is to maintain the corpus luteum in hCG is to maintain the corpus luteum in the maternal ovary and therefore maintain the maternal ovary and therefore maintain the early pregnancy, that is block the the early pregnancy, that is block the menstrual cycle.menstrual cycle.
UltrasonographyUltrasonography
• A methodical sonographic evaluation of A methodical sonographic evaluation of the placenta should include: location, the placenta should include: location, visual estimation of the size (and, if visual estimation of the size (and, if appearing abnormal, measurement of appearing abnormal, measurement of thickness and/or volume), implantation, thickness and/or volume), implantation, morphology, anatomy, as well as a search morphology, anatomy, as well as a search for anomalies, such as additional lobes for anomalies, such as additional lobes and tumors. Additional assessment for and tumors. Additional assessment for multiple gestations consists of multiple gestations consists of examining the intervening membranes examining the intervening membranes (if present). (if present).
Placenta – the both sidesPlacenta – the both sides
• The umbilical cord (also called the The umbilical cord (also called the birth cord or funiculus umbilicalis) is birth cord or funiculus umbilicalis) is the connecting cord from the the connecting cord from the developing embryo or fetus to the developing embryo or fetus to the placenta. Developed from the same placenta. Developed from the same zygotre as the fetus, the human zygotre as the fetus, the human umbilical cord normally contains two umbilical cord normally contains two arteries and one vein, buried within arteries and one vein, buried within Wharton’s jelly. Wharton’s jelly.
• The umbilical cord develops from and contains The umbilical cord develops from and contains remnants of the yolk sac and allantois (and is remnants of the yolk sac and allantois (and is therefore derived from the same zygote as the therefore derived from the same zygote as the fetus). It forms by the fifth week of fetal fetus). It forms by the fifth week of fetal development, replacing the yolk sac as the development, replacing the yolk sac as the source of nutrients for the fetus. The umbilical source of nutrients for the fetus. The umbilical cord in a full term neonate is usually about 50 cord in a full term neonate is usually about 50 centimeters long and about 2 centimetres centimeters long and about 2 centimetres diameter. This diameter decreases rapidly diameter. This diameter decreases rapidly within the placenta.within the placenta.
• The umbilical vein supplies the fetus with The umbilical vein supplies the fetus with oxygeneted, nutrietent-rich blood from the oxygeneted, nutrietent-rich blood from the placenta. Conversely, the umbilical arteries placenta. Conversely, the umbilical arteries return the deoxygenated, nutrient-depleted return the deoxygenated, nutrient-depleted bloodblood
• Occasionally, only two vessels (one vein and Occasionally, only two vessels (one vein and one artery) are present in the umbilical cord. one artery) are present in the umbilical cord. This is sometimes related to fetal This is sometimes related to fetal abnormalities, but it may also occur without abnormalities, but it may also occur without accompanying problems.accompanying problems.
• It is unusual for a vein to carry oxygenated It is unusual for a vein to carry oxygenated blood, and for arteries to carry deoxygenated blood, and for arteries to carry deoxygenated blood (the only other examples being blood (the only other examples being the pulmonary veins and arteries, connecting the pulmonary veins and arteries, connecting the lungs to the heart). However, this naming the lungs to the heart). However, this naming convention reflects the fact that the umbilical convention reflects the fact that the umbilical vein carries blood towards the fetus's heart, vein carries blood towards the fetus's heart, whilst the umbilical arteries carry blood whilst the umbilical arteries carry blood away.away.
Placenta – umbilical cordPlacenta – umbilical cordConnection to fetal circulatory Connection to fetal circulatory
systemsystem • The umbilical vein continues towards the transverse The umbilical vein continues towards the transverse
fissure of the liver, where it splits into two. One of fissure of the liver, where it splits into two. One of these branches joins with the hepatic portal vein these branches joins with the hepatic portal vein (connecting to its left branch), which carries blood (connecting to its left branch), which carries blood into the liver. The second branch (known as the into the liver. The second branch (known as the ductus venosus) allows the majority of the incoming ductus venosus) allows the majority of the incoming blood (approximately 80%) to bypass the liver and blood (approximately 80%) to bypass the liver and flow via the left hepatic vein into the inferior vena flow via the left hepatic vein into the inferior vena cava, which carries blood towards the heart.cava, which carries blood towards the heart.
• The two umbilical arteries branch from the internal The two umbilical arteries branch from the internal iliac arteries, and pass on either side of the urinary iliac arteries, and pass on either side of the urinary bladder before joining the umbilical cord.bladder before joining the umbilical cord.
Shortly after birth, upon exposure to Shortly after birth, upon exposure to temperature change, the gelatinous temperature change, the gelatinous Wharton's Jelly substance undergoes a Wharton's Jelly substance undergoes a physiological change that collapses physiological change that collapses previous structure boundaries and in previous structure boundaries and in effect creates a natural clamp on the effect creates a natural clamp on the umbilical cord which halts placental blood umbilical cord which halts placental blood return to the neonate. This process will return to the neonate. This process will take as little as five minutes if left to take as little as five minutes if left to proceed naturally.proceed naturally.